
Mast cell tumor
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1];Associate Editor(s)-in-Chief: Suveenkrishna Pothuru, M.B,B.S. [2]
Synonyms and keywords: Mastocytosis; Systemic mastocytosis; Cutaneous mastocytosis; Systemic mast cell tumor; Cutaneous mast cell tumor; Mastocytoma; Mast cell neoplasm; Localized mastocytosis; Maculopapular cutaneous mastocytosis; Diffuse cutaneous mastocytosis; Mastocytoma of skin; Indolent systemic mastocytosis; Smoldering systemic mastocytosis; Isolated bone marrow mastocytosis; Aggressive systemic mastocytosis; Mast cell sarcoma; Extracutaneous mastocytoma; Mastocyte tumor
Overview
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1];Associate Editor(s)-in-Chief: Suveenkrishna Pothuru, M.B,B.S. [2]
Overview
Mast cell tumor is a rare and heterogeneous disease characterized by the presence of excessive numbers of mast cells in various organs, mainly the skin and the bone marrow that manifests with an unusually broad spectrum of clinical and morphological appearances. Based on the affected organ(s), mast cell tumor may be classified into either cutaneous mastocytosis or systemic mastocytosis. Mast cell tumor may be classified into seven subtypes based on WHO classification system. Cutaneous mastocytosis is more common in children and the disease manifest itself in the first year of life in over 80% of cases. There is no sex predilection and race predilection to the mast cell tumor. Mast cell tumor arises from the mast cell, which is a type of white blood cell involved in the inflammatory process. The progression to mast cell tumor usually involves the uncontrolled stimulation of the receptor for stem cell factor following mutation of C-kit cell surface receptor. On microscopic histopathological analysis, mast cells in the superficial and mid dermis that are lymphocyte like with dense granular cytoplasm which tend to be more abundant around blood vessels is characteristic finding of mast cell tumor. Mast cell tumor must be differentiated from other diseases that cause flushing,such as: phaeochromocytoma and carcinoid syndrome. Mast cell tumor must be differentiated from other diseases that cause elevated serum tryptase levels and cytopenia, such as: myelodysplastic syndrome, primary myelofibrosis, essential thrombocythemia, and chronic eosinophilic leukemia. Common complications of mast cell tumor include episodes of anaphylaxis, osteoporosis, and progression to malignant mastocytosis or mast cell leukemia. The prognosis of mast cell tumor varies with the subtype, location, and extent of the tumor. The cutaneous mastocytosis is associated with the most favorable prognosis and mast cell leukemia is associated with poor prognosis. The diagnosis of systemic mastocytosis is based on the presence of one major criterion and one minor criterion or three minor criteria. Major criteria include the presence of multifocal dense infiltrates of mast cells observed in bone marrow sections or other extra cutaneous organs. Four minor criteria include the presence of >25% abnormal spindle-shaped mast cells in bone marrow and/or tissues, detection of Kit mutation at codon 816 in bone marrow or extracutaneous organ(s), the expression of CD2 and CD25 surface markers in C-kit positive mast cells from bone marrow or other organs, and elevated serum tryptase levels >20 ng/mL. Physical examination for mast cell tumor include inspection for a large assortment of types of skin lesions, testing for dermatographism (Darier’s sign), and palpating for hepatosplenomegaly and lymphadenopathy. Laboratory tests that may be helpful for diagnosis of mast cell tumor include complete blood count, serum tryptase levels, plasma and urinary histamine levels, and coagulation profile. Biopsy of affected organ may be performed to detect possible accumulation of mast cells in an involved tissue. Other imaging studies for evaluation of mast cell tumor include sonography of internal organs, gastroscopy and colonoscopy with biopsy, and DXA scan of bones. The mainstay of therapy for mast cell tumor is avoidance of triggering factors and symptomatic therapy. Chemotherapy is indicated for aggressive form of mast cell tumor.
Historical Perspective
Mast cell activation was first described by Dr. Nettleship and Tay in 1869. Dr. Sezary and other french scientists reported the first case of mast cell tumor in 1936.
Classification
Based on the affected organ(s), mast cell tumor may be classified into either cutaneous mastocytosis or systemic mastocytosis. Mast cell tumor may be classified into seven subtypes based on WHO classification system.
Pathophysiology
Mast cell tumor arises from the mast cell, which is a type of white blood cell involved in the inflammatory process. The progression to mast cell tumor usually involves the uncontrolled stimulation of the receptor for stem cell factor following mutation of C-kit cell surface receptor. On microscopic histopathological analysis, mast cells in the superficial and mid dermis that are lymphocyte like with dense granular cytoplasm which tend to be more abundant around blood vessels is characteristic finding of mast cell tumor.
Causes
There are no established causes for mast cell tumor.
Differentiating Mast Cell Tumor from other Diseases
Mast cell tumor must be differentiated from other diseases that cause flushing,such as: phaeochromocytoma and carcinoid syndrome. Mast cell tumor must be differentiated from other diseases that cause elevated serum tryptase levels and cytopenia, such as: myelodysplastic syndrome, primary myelofibrosis, essential thrombocythemia, and chronic eosinophilic leukemia.
Epidemiology and Demographics
Mast cell tumor is a rare disease and considered to be an “orphan disease” affecting 200,000 or fewer people in the United States. There are no definite data regarding the prevalence of mast cell tumor among the US general population. Cutaneous mastocytosis is more common in children and the disease manifest itself in the first year of life in over 80% of cases. There is no sex predilection and race predilection to the mast cell tumor.
Risk Factors
Common risk factors in the development of mast cell tumor are age and mutation of C-kit receptor.
Natural History, Complications and Prognosis
Common complications of mast cell tumor include episodes of anaphylaxis, osteoporosis, and progression to malignant mastocytosis or mast cell leukemia. The prognosis of mast cell tumor varies with the subtype, location, and extent of the tumor. The cutaneous mastocytosis is associated with the most favorable prognosis and mast cell leukemia is associated with poor prognosis.
Diagnostic Criteria
The diagnosis of systemic mastocytosis is based on the presence of one major criterion and one minor criterion or three minor criteria. Major criteria include the presence of multifocal dense infiltrates of mast cells observed in bone marrow sections or other extra cutaneous organs. Four minor criteria include the presence of >25% abnormal spindle-shaped mast cells in bone marrow and/or tissues, detection of Kit mutation at codon 816 in bone marrow or extracutaneous organ(s), the expression of CD2 and CD25 surface markers in C-kit positive mast cells from bone marrow or other organs, and elevated serum tryptase levels >20 ng/mL.
Diagnosis
Staging
There is no established system for the staging of mast cell tumor.
History and Symptoms
Physical Examination
Physical examination for mast cell tumor include inspection for a large assortment of types of skin lesions, testing for dermatographism (Darier’s sign), and palpating for hepatosplenomegaly and lymphadenopathy.
Laboratory Findings
Laboratory tests that may be helpful for diagnosis of mast cell tumor include complete blood count, serum tryptase levels, plasma and urinary histamine levels, and coagulation profile.
Biopsy
Biopsy of affected organ may be performed to detect possible accumulation of mast cells in an involved tissue.
Other Imaging Findings
Other imaging studies for evaluation of mast cell tumor include sonography of internal organs, gastroscopy and colonoscopy with biopsy, and DXA scan of bones.
Treatment
Medical Therapy
The mainstay of therapy for mast cell tumor is avoidance of triggering factors and symptomatic therapy. Chemotherapy is indicated for aggressive form of mast cell tumor.
Surgery
Surgical intervention is not recommended for the management of mast cell tumor.
References
Historical Perspective
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Ahmed Elsaiey, MBBCH [2]
Overview
Mast cell activation was first described by Dr. Nettleship and Tay in 1869. Dr. Sezary and other french scientists reported the first case of mast cell tumor in 1936.
Historical Perspective
Discovery
- In 1869, Dr. Nettleship and Tay were the first ever to discuss the mast cell activation and it was in a case of urticaria pigmentosa.[1]
- In 1936, Dr. Sézary and other french scientists reported the first case of systemic mastocytosis or mast cell tumor.
- Dr. Sezary describes the systemic mastocytosis as aberrant mast cell proliferation which is characterized by release of immense vasoactive amines.[2]
References
- ↑ Scherber RM, Borate U (2018). “How we diagnose and treat systemic mastocytosis in adults”. Br J Haematol. 180 (1): 11–23. doi:10.1111/bjh.14967. PMID 29048112.
- ↑ Scherber RM, Borate U (2018). “How we diagnose and treat systemic mastocytosis in adults”. Br J Haematol. 180 (1): 11–23. doi:10.1111/bjh.14967. PMID 29048112.
Classification
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1];Associate Editor(s)-in-Chief: Suveenkrishna Pothuru, M.B,B.S. [2]
Overview
Based on the affected organ(s), mast cell tumor may be classified into either cutaneous mastocytosis or systemic mastocytosis. Mast cell tumor may be classified into seven subtypes based on WHO classification system.[1]
Classification
Based on the affected organ(s), mast cell tumor may be classified into two subtypes:
- Cutaneous mastocytosis
- Limited to the skin where mast cells infiltrate the skin
- Systemic mastocytosis
- Systemic mastocytosis is caused by mast cells accumulating in the tissues and can affect organs such as the liver, spleen, bone marrow, and small intestine
- Localized mastocytosis
Mast cell tumor may be classified according to WHO classification into seven subtypes:[1]
- Cutaneous mastocytosis
- Urticaria pigmentosa
- Maculopapular cutaneous mastocytosis
- Diffuse cutaneous mastocytosis
- Mastocytoma of skin
- Indolent systemic mastocytosis
- Smoldering systemic mastocytosis
- Isolated bone marrow mastocytosis
- Systemic mastocytosis with an associated (clonal) hematologic non–mast cell lineage disease
- Aggressive systemic mastocytosis
- Lymphadenopathic systemic mastocytosis with eosinophilia
- Mast cell leukemia
- Typical mast cell leukemia
- Aleukemic mast cell leukemia
- Mast cell sarcoma
- Extracutaneous mastocytoma
References
- ↑ 1.0 1.1 Patnaik MM, Rindos M, Kouides PA, Tefferi A, Pardanani A (2007). “Systemic mastocytosis: a concise clinical and laboratory review”. Arch Pathol Lab Med. 131 (5): 784–91. doi:10.1043/1543-2165(2007)131[784:SMACCA]2.0.CO;2. PMID 17488167.
Pathophysiology
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1];Associate Editor(s)-in-Chief: Suveenkrishna Pothuru, M.B,B.S. [2]
Overview
Mast cell tumor arises from the mast cell, which is a type of white blood cell involved in the inflammatory process. The progression to mast cell tumor usually involves the uncontrolled stimulation of the receptor for stem cell factor following mutation of C-kit cell surface receptor. On microscopic histopathological analysis, mast cells in the superficial and mid dermis that are lymphocyte like with dense granular cytoplasm which tend to be more abundant around blood vessels is characteristic finding of mast cell tumor.
Pathophysiology
Mast Cell
- Mast cells are bone marrow derived multi-functional immune cells and are normally found throughout the connective tissue of the body.
- It is a normal component of the immune system and as it releases histamine it is associated with allergic reactions.
- Mast cell granules contain histamine, heparin, platelet-activating factor, leukotrienes, prostaglandins, cytokines and proteases.[1][2]
- It is thought that the effects of mast cell tumor relate at least in part to mediator release.
- The clinical features of mast cell tumor arise from release of mast cell mediators, inflitration of tissues by mast cells, local build-up of mast cells and associated neoplasms.[3]
- In systemic mastocytosis, abnormal proliferation and microscopic infiltration of mast cells involves skin, bone marrow, gastrointestinal tract, liver, and spleen.[4][5]
Genetics
- Mutations in kinases (especially in the tyrosine kinase Kit) and in enzymes and receptors (histamine H4 receptor, PDGFRα, JAK2, RASGRP4, Src-kinases, c-Cbl-encoded E3 ligase) which are essentially involved in the regulation of proliferation and differentiation of mast cell, and are required to establish a clonal mast cell population.[6]
- Mast cells express a cell surface receptor, C-kit (CD117), which is the receptor for stem cell factor. In laboratory studies, stem cell factor appears to be important for the proliferation of mast cells.[7][8]
- Mutations of the C-kit receptor, leading to uncontrolled stimulation of the receptor, is a cause for the disease.[9]
- The D816V point mutation within the tyrosine kinase Kit (C-kit) that is detected in 80% of cases is considered a driver mutation causing the permanent receptor activation and consequent proliferation, and thus neoplastic expansion of the mutated mast cell clone.[10]
- The following genes are involved in the pathogenesis of mast cell tumor:[11][12][13]
Microscopic Pathology
- Lymphocyte-like with more cytoplasm that is granular
- Cells may have spindled or stellate morphology
- Tend to be more abundant around vessels
- Eosinophils may present
-
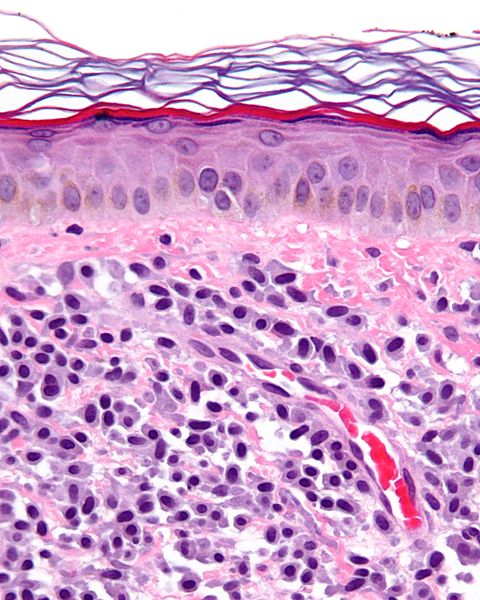 Micrograph showing a mast cell tumor.
Micrograph showing a mast cell tumor.

References
- ↑ Moon TC, Befus AD, Kulka M (2014). “Mast cell mediators: their differential release and the secretory pathways involved”. Front Immunol. 5: 569. doi:10.3389/fimmu.2014.00569. PMID 25452755.
- ↑ Krystel-Whittemore M, Dileepan KN, Wood JG (2015). “Mast Cell: A Multi-Functional Master Cell”. Front Immunol. 6: 620. doi:10.3389/fimmu.2015.00620. PMID 26779180.
- ↑ Metcalfe DD (2005). “Regulation of normal and neoplastic human mast cell development in mastocytosis”. Trans. Am. Clin. Climatol. Assoc. 116: 185–203, discussion 203–4.
- ↑ Ramsay DB, Stephen S, Borum M, Voltaggio L, Doman DB (December 2010). “Mast cells in gastrointestinal disease”. Gastroenterol Hepatol (N Y). 6 (12): 772–7. PMC 3033552. PMID 21301631.
- ↑ Ahmed M, Kesavan M, Jilani BN, Ahmed S, Deeb L (June 2016). “Systemic Mastocytosis as an Unconventional Cause of Variceal Bleeding: Think Outside the Box”. Cureus. 8 (6): e629. doi:10.7759/cureus.629. PMC 4935436. PMID 27433408.
- ↑ Molderings, Gerhard J; Brettner, Stefan; Homann, Jürgen; Afrin, Lawrence B (2011). “Mast cell activation disease: a concise practical guide for diagnostic workup and therapeutic options”. Journal of Hematology & Oncology. 4 (1): 10. doi:10.1186/1756-8722-4-10. ISSN 1756-8722.
- ↑ Longley BJ, Morganroth GS, Tyrrell L, Ding TG, Anderson DM, Williams DE, Halaban R (May 1993). “Altered metabolism of mast-cell growth factor (c-kit ligand) in cutaneous mastocytosis”. N. Engl. J. Med. 328 (18): 1302–7. doi:10.1056/NEJM199305063281803. PMID 7682288.
- ↑ Galli SJ, Tsai M, Wershil BK (April 1993). “The c-kit receptor, stem cell factor, and mast cells. What each is teaching us about the others”. Am. J. Pathol. 142 (4): 965–74. PMC 1886888. PMID 7682764.
- ↑ Chatterjee A, Ghosh J, Kapur R (July 2015). “Mastocytosis: a mutated KIT receptor induced myeloproliferative disorder”. Oncotarget. 6 (21): 18250–64. doi:10.18632/oncotarget.4213. PMID 26158763.
- ↑ Kristensen T, Vestergaard H, Møller MB (March 2011). “Improved detection of the KIT D816V mutation in patients with systemic mastocytosis using a quantitative and highly sensitive real-time qPCR assay”. J Mol Diagn. 13 (2): 180–8. doi:10.1016/j.jmoldx.2010.10.004. PMC 3279709. PMID 21354053.
- ↑ Schwaab J, Schnittger S, Sotlar K, Walz C, Fabarius A, Pfirrmann M, Kohlmann A, Grossmann V, Meggendorfer M, Horny HP, Valent P, Jawhar M, Teichmann M, Metzgeroth G, Erben P, Ernst T, Hochhaus A, Haferlach T, Hofmann WK, Cross NC, Reiter A (October 2013). “Comprehensive mutational profiling in advanced systemic mastocytosis”. Blood. 122 (14): 2460–6. doi:10.1182/blood-2013-04-496448. PMID 23958953.
- ↑ Traina F, Visconte V, Jankowska AM, Makishima H, O’Keefe CL, Elson P, Han Y, Hsieh FH, Sekeres MA, Mali RS, Kalaycio M, Lichtin AE, Advani AS, Duong HK, Copelan E, Kapur R, Olalla Saad ST, Maciejewski JP, Tiu RV (2012). “Single nucleotide polymorphism array lesions, TET2, DNMT3A, ASXL1 and CBL mutations are present in systemic mastocytosis”. PLoS ONE. 7 (8): e43090. doi:10.1371/journal.pone.0043090. PMC 3419680. PMID 22905207.
- ↑ Chan EC, Bai Y, Bandara G, Simakova O, Brittain E, Scott L, Dyer KD, Klion AD, Maric I, Gilfillan AM, Metcalfe DD, Wilson TM (October 2013). “KIT GNNK splice variants: expression in systemic mastocytosis and influence on the activating potential of the D816V mutation in mast cells”. Exp. Hematol. 41 (10): 870–881.e2. doi:10.1016/j.exphem.2013.05.005. PMID 23743299.
- ↑ Berezowska S, Flaig MJ, Ruëff F, Walz C, Haferlach T, Krokowski M, Kerler R, Petat-Dutter K, Horny HP, Sotlar K (January 2014). “Adult-onset mastocytosis in the skin is highly suggestive of systemic mastocytosis”. Mod. Pathol. 27 (1): 19–29. doi:10.1038/modpathol.2013.117. PMID 23807778.
- ↑ Tefferi A, Lim KH, Abdel-Wahab O, Lasho TL, Patel J, Patnaik MM, Hanson CA, Pardanani A, Gilliland DG, Levine RL (July 2009). “Detection of mutant TET2 in myeloid malignancies other than myeloproliferative neoplasms: CMML, MDS, MDS/MPN and AML”. Leukemia. 23 (7): 1343–5. doi:10.1038/leu.2009.59. PMC 4654626. PMID 19295549.
Causes
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1];Associate Editor(s)-in-Chief: Suveenkrishna Pothuru, M.B,B.S. [2]
Overview
There are no established causes for mast cell tumor.
Causes
There are no established causes for mast cell tumor. To view the list of risk factors in the development of bladder cancer, please click here
References
Differentiating Mast Cell Tumor from other Diseases
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1];Associate Editor(s)-in-Chief: Hannan Javed, M.D.[2] Zahir Ali Shaikh, MD[3] Suveenkrishna Pothuru, M.B,B.S. [4]
Overview
Mast cell tumor must be differentiated from other diseases that cause flushing,such as: phaeochromocytoma and carcinoid syndrome.[1] Mast cell tumor must be differentiated from other diseases that cause elevated serum tryptase levels and cytopenia, such as: myelodysplastic syndrome, primary myelofibrosis, essential thrombocythemia, and chronic eosinophilic leukemia.
Differential Diagnosis
Mast cell tumor must be differentiated from other diseases that cause flushing:[1]
Mast cell tumor must be differentiated from other diseases that cause abdominal pain and discomfort:
Mast cell tumor must be differentiated from other diseases that cause elevated serum tryptase levels and cytopenia, such as:
- Myelodysplastic syndrome
- Primary myelofibrosis
- Essential thrombocythemia
- Chronic eosinophilic leukemia
- Chronic myeloid leukemia
- Myelomastocytic leukemia
- Malignant lymphoma
Differentiating Myeloproliferative Disorders
ABBREVIATIONS
N/A: Not available, NL: Normal, FISH: Fluorescence in situ hybridization, PCR: Polymerase chain reaction, LDH: Lactate dehydrogenase, PUD: Peptic ulcer disease, EPO: Erythropoietin, LFTs: Liver function tests, RFTs: Renal function tests, LAP: Leukocyte alkaline phosphatase, LAD: Leukocyte alkaline dehydrgenase, WBCs: White blood cells.
| Myeloproliferative neoplasms (MPN) | Clinical manifestations | Diagnosis | Other features | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Symptoms | Physical examination | CBC & Peripheral smear | Bone marrow biopsy | Other investigations | |||||||||||
| WBCs | Hb | Plat- elets | |||||||||||||
| Leuko-cytes | Blasts | Left shift |
Baso- phils |
Eosino- phils |
Mono- cytes |
Others | |||||||||
| Chronic myeloid leukemia (CML), BCR-ABL1+[2][3] |
|
|
↑ | <2% | + | ↑ | ↑ | ↑ | N/A | ↓ | NL |
|
|
| |
| Chronic neutrophilic leukemia (CNL)[4][5][6] |
|
↑ | Minimal | + | NL | NL | NL | ↓ | ↓ |
|
|
| |||
| Polycythemia vera (PV)[7][8][9][10] |
|
|
NL or ↑ | None | – | ↑ or ↓ | NL or ↑ | NL | ↑↑ | NL |
|
| |||
| Primary myelofibrosis (PMF)[11][12][13][14] |
|
↓ | Erythroblasts | – | Absent | NL | NL | ↓ | ↓ |
|
| ||||
| Essential thrombocythemia (ET)[15][16][17] |
|
NL or ↑ |
None |
– |
↓ or absent |
NL |
NL |
|
↑↑ |
|
|||||
| Chronic eosinophilic leukemia, not otherwise specified (NOS)[18][19][20][21] |
|
↑ | Present | + | ↑ | ↑↑ | ↑ | ↓ | ↓ |
|
|
||||
| MPN, unclassifiable |
|
|
↑ | Variable | ± | ↑ or ↓ | ↑ or ↓ | ↑ or ↓ |
|
↓ | ↑ |
|
|
| |
| Mastocytosis[22][23][24][25] |
|
↑ | None | – | NL | ↑ | NL | ↓ | ↓ or ↑ |
|
| ||||
| Myeloid/lymphoid neoplasms with eosinophilia and rearrangement of PDGFRA, PDGFRB, or FGFR1, or with PCM1–JAK2[26][27][28][29] |
|
↑ | NL | – | NL | ↑ | ↑ |
|
NL | ↓ |
|
|
| ||
| B-lymphoblastic leukemia/lymphoma[30][31] | NL or ↑ | >25% | N/A | ↑ or ↓ | ↑ or ↓ | ↑ or ↓ | ↓ | ↓ |
|
| |||||
| Myelodysplastic syndromes (MDS)[32][33] |
↓ | Variable | – | ↓ | ↓ | ↓ |
|
↓ | ↓ |
|
| ||||
| Acute myeloid leukemia (AML) and related neoplasms[34][35] |
|
|
NL or ↑ | ↑ | N/A | ↑ or ↓ | ↑ or ↓ | ↑ or ↓ |
|
↓ | ↓ |
with dysplasia |
| ||
| Blastic plasmacytoid dendritic cell neoplasm[36][37][38][39] |
|
|
NL | ↑ | NL | NL | NL | ↓ | ↓ |
|
| ||||
| Myelodysplastic /myeloproliferative neoplasms (MDS/MPN) |
Chronic myelomonocytic leukemia (CMML)[40] |
|
↑ | < 20% | NL | ↑ | ↑↑ |
|
↓ | ↓ |
|
| |||
| Atypical chronic myeloid leukemia (aCML), BCR-ABL1-[43][44] |
|
|
↑ | <20% | + | <2% of WBCs | N/A | N/A |
|
↓ | ↓ |
|
|||
| Juvenile myelomonocytic leukemia (JMML)[45][46] |
|
↑ | ↑ | N/A | N/A | N/A | ↑ | ↓ | ↓ |
|
| ||||
| MDS/MPN with ring sideroblasts and thrombocytosis (MDS/MPN-RS-T)[47][48][49] |
|
|
NL or ↑ | NL | – | NL | N/A | N/A | ↓ | ↑ |
|
| |||
| T-lymphoblastic leukemia/ lymphoma |
T-lymphoblastic leukemia/ lymphoma[50][51][52] |
|
↑ | >25% blasts (Leukemia) | ± | ↑ or ↓ | ↑ or ↓ | ↑ or ↓ |
|
↓ | ↓ |
|
|||
| Provisional entity: Natural killer (NK) cell lymphoblastic leukemia/lymph[53] |
|
↑ | ↑ | ± | ↑ or ↓ | ↑ or ↓ | ↑ or ↓ |
|
↓ | ↓ |
|
||||
| Provisional entity: Early T-cell precursor lymphoblastic leukemia[54][55] |
|
↑ | ↑ | ± | ↑ or ↓ | ↑ or ↓ | ↑ or ↓ |
|
↓ | ↓ |
|
||||
Differentiating mast cell tumor from other causes of abdominal pain and diarrhea
Mast cell tumor must be differentiated from other causes of abdominal pain and diarrhea.
| Diseases | Clinical manifestations | Para-clinical findings | Gold standard | Additional findings | |||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Symptoms | Physical examination | ||||||||||||||||||||||||
| Lab Findings | Imaging | Histopathology | |||||||||||||||||||||||
| Abdominal pain | Diarrhea | Flushing | Dyspnea | Palpitations | Other symptoms | Wheezing | Telangiectasia | Hypotension | Tachycardia | Systolic murmur of tricuspid regurgitation | Other physical findings | Urinary 5-hydroxyindoleacetic acid (5-HIAA) | Serum Chromogranin A (CgA) | Other markers | Abdominal computed tomography (CT) | Abdominal MRI | Somatostatin receptor scintigraphy [SRS], or Octreoscan | Metaiodobenzylguanidine (MIBG) scintigraphy | Other diagnostic studies | Transthoracic echocardiography | |||||
| Carcinoid Syndrome[56][57][58][59][60][61][62][63][64] | Neuroendocrine tumor of midgut [65][66][67][68] | +
Mild |
+
|
+ | + | + |
Metastatic tumors in the liver: Right upper quadrant pain, hepatomegaly, and early satiety |
+ | +/- | +/- | + | + | – | + | + |
|
|
|
+
|
+ |
|
|
|
|
|
| Neuroendocrine tumor of lung[69][70][71][72] | + | + | + | + | + |
|
+ | +/- | +/- | + | + | – | + | + |
|
Sensitive for detection of liver metastases if present | + | + |
|
– | Typical low-grade:bland cells containing regular round nuclei with finely dispersed chromatin and inconspicuous small nucleoli.Mitotic figures are scarce and necrosis is absent.
Intermediate-grade atypical: presence of Neuroendocrine morphology and either necrosis or 2 to 10 mitoses per 10 HPF |
| |||
| Irritable Bowel Syndrome[73][74][75][76] | +
Perioidic |
|
– | – | – | – | – | – | – | – | – | – | – | – | – | – |
|
– | – | Rome IV criteria
•Related to defecation •Associated with a change in stool frequency •Associated with a change in stool form (appearance) |
|||||
| Malignant neoplasms of small intestine[77][78][79] | +/- | +/- | – | – | +/- |
|
– | – | +/- | – | * Abdominal mass | – | + | Abdominal CT scan may be diagnostic of small intestine cancer. Findings on CT scan suggestive of small intestine cancer include intrinsic mass with a short segment of bowel wall thickening | MRI and MRI enteroscopy are other advance modalities to diagnose and stage small intestinal cancers | – | – | Enteroscopy, capsule endoscopy and double balloon enteroscopy |
|
Biopsy and histopathology | |||||
| Crohn disease[80][81][82][83] | +/- | – | – | – |
|
– | – | – | – | – |
|
– | – |
|
– | – |
|
– |
|
|
|||||
| Benign cutaneous flushing[84] | – | – | + | – | – | – | – | – | – | – | – | – | – | – | – | – | – | – | – | – | – | – | |||
| Systemic mastocytosis[85][86][87][88][89] | + | + | + | + | – | +/- | +/- | + | – | – | – | – | – | – | |||||||||||
| Asthma exacerbation[90][91][92][93] | – | – | – | + | + | + | – | – | + | – |
|
– | – | – | — | – | – | – | Chest X ray | – |
|
||||
| Anaphylaxis[94][95][96][97][98] | + | -/+ | + | + | + | +/- | – | + | + | – | – | – | – | – | – | – | – |
|
– | – | History of exposure to insect stings,food alllergy,rubber latex,food additives,,allergy to medications,physical factors such s excercise and cold | ||||
| Histaminergic Angioedema[99][100][101][102][103] | +/- | +/- | + | + | + |
|
+ | – | + | + | – | – | – | – |
|
– | – | – |
|
– | – | – |
| ||
| Medullary Thyroid Carcinoma[104][105][106][107] | – | +/- | +/- | +/- | – | – | – | – | – | – | – | – |
|
– | – | – | – |
|
– |
|
|
||||
References
- ↑ 1.0 1.1 Mastocytosis and mast cell disorders.Patient info.http://patient.info/doctor/mastocytosis-and-mast-cell-disorders#ref-20 accessed on March 7th, 2016
- ↑ Savage DG, Szydlo RM, Goldman JM (January 1997). “Clinical features at diagnosis in 430 patients with chronic myeloid leukaemia seen at a referral centre over a 16-year period”. Br. J. Haematol. 96 (1): 111–6. PMID 9012696.
- ↑ Thompson PA, Kantarjian HM, Cortes JE (October 2015). “Diagnosis and Treatment of Chronic Myeloid Leukemia in 2015”. Mayo Clin. Proc. 90 (10): 1440–54. doi:10.1016/j.mayocp.2015.08.010. PMC 5656269. PMID 26434969.
- ↑ Szuber N, Tefferi A (February 2018). “Chronic neutrophilic leukemia: new science and new diagnostic criteria”. Blood Cancer J. 8 (2): 19. doi:10.1038/s41408-018-0049-8. PMC 5811432. PMID 29440636.
- ↑ Maxson JE, Tyner JW (February 2017). “Genomics of chronic neutrophilic leukemia”. Blood. 129 (6): 715–722. doi:10.1182/blood-2016-10-695981. PMC 5301820. PMID 28028025.
- ↑ Menezes J, Cigudosa JC (2015). “Chronic neutrophilic leukemia: a clinical perspective”. Onco Targets Ther. 8: 2383–90. doi:10.2147/OTT.S49688. PMC 4562747. PMID 26366092.
- ↑ Vannucchi AM, Guglielmelli P, Tefferi A (March 2018). “Polycythemia vera and essential thrombocythemia: algorithmic approach”. Curr. Opin. Hematol. 25 (2): 112–119. doi:10.1097/MOH.0000000000000402. PMID 29194068.
- ↑ Pillai AA, Babiker HM. PMID 30252337. Missing or empty
|title=(help) - ↑ Tefferi A, Barbui T (January 2019). “Polycythemia vera and essential thrombocythemia: 2019 update on diagnosis, risk-stratification and management”. Am. J. Hematol. 94 (1): 133–143. doi:10.1002/ajh.25303. PMID 30281843.
- ↑ Rumi E, Cazzola M (February 2017). “Diagnosis, risk stratification, and response evaluation in classical myeloproliferative neoplasms”. Blood. 129 (6): 680–692. doi:10.1182/blood-2016-10-695957. PMC 5335805. PMID 28028026.
- ↑ Cervantes F, Correa JG, Hernandez-Boluda JC (May 2016). “Alleviating anemia and thrombocytopenia in myelofibrosis patients”. Expert Rev Hematol. 9 (5): 489–96. doi:10.1586/17474086.2016.1154452. PMID 26891375.
- ↑ Hoffman, Ronald (2018). Hematology : basic principles and practice. Philadelphia, PA: Elsevier. ISBN 9780323357623.
- ↑ Michiels JJ, Bernema Z, Van Bockstaele D, De Raeve H, Schroyens W (March 2007). “Current diagnostic criteria for the chronic myeloproliferative disorders (MPD) essential thrombocythemia (ET), polycythemia vera (PV) and chronic idiopathic myelofibrosis (CIMF)”. Pathol. Biol. 55 (2): 92–104. doi:10.1016/j.patbio.2006.06.002. PMID 16919893.
- ↑ Hoffman, Ronald (2018). Hematology : basic principles and practice. Philadelphia, PA: Elsevier. ISBN 9780323357623.
- ↑ Schmoldt A, Benthe HF, Haberland G (1975). “Digitoxin metabolism by rat liver microsomes”. Biochem Pharmacol. 24 (17): 1639–41. PMID http://dx.doi.org/10.1182/blood-2007-04-083501 Check
|pmid=value (help). - ↑ Daniel A. Arber, Attilio Orazi, Robert Hasserjian, Jurgen Thiele, Michael J. Borowitz, Michelle M. Le Beau, Clara D. Bloomfield, Mario Cazzola & James W. Vardiman (2016). “The 2016 revision to the World Health Organization classification of myeloid neoplasms and acute leukemia”. Blood. 127 (20): 2391–2405. doi:10.1182/blood-2016-03-643544. PMID 27069254. Unknown parameter
|month=ignored (help) - ↑ A. Tefferi, R. Fonseca, D. L. Pereira & H. C. Hoagland (2001). “A long-term retrospective study of young women with essential thrombocythemia”. Mayo Clinic proceedings. 76 (1): 22–28. doi:10.4065/76.1.22. PMID 11155408. Unknown parameter
|month=ignored (help) - ↑ Vidyadharan S, Joseph B, Nair SP (2016). “Chronic Eosinophilic Leukemia Presenting Predominantly with Cutaneous Manifestations”. Indian J Dermatol. 61 (4): 437–9. doi:10.4103/0019-5154.185716. PMC 4966405. PMID 27512192.
- ↑ Hofmans M, Delie A, Vandepoele K, Van Roy N, Van der Meulen J, Philippé J, Moors I (2018). “A case of chronic eosinophilic leukemia with secondary transformation to acute myeloid leukemia”. Leuk Res Rep. 9: 45–47. doi:10.1016/j.lrr.2018.04.001. PMC 5993353. PMID 29892549.
- ↑ Yamada Y, Rothenberg ME, Cancelas JA (2006). “Current concepts on the pathogenesis of the hypereosinophilic syndrome/chronic eosinophilic leukemia”. Transl Oncogenomics. 1: 53–63. PMC 3642145. PMID 23662039.
- ↑ Kim TH, Gu HJ, Lee WI, Lee J, Yoon HJ, Park TS (September 2016). “Chronic eosinophilic leukemia with FIP1L1-PDGFRA rearrangement”. Blood Res. 51 (3): 204–206. doi:10.5045/br.2016.51.3.204. PMID 27722133.
- ↑ Carter MC, Metcalfe DD, Komarow HD (February 2014). “Mastocytosis”. Immunol Allergy Clin North Am. 34 (1): 181–96. doi:10.1016/j.iac.2013.09.001. PMC 3863935. PMID 24262698.
- ↑ Macri A, Cook C. PMID 29494109. Missing or empty
|title=(help) - ↑ Lladó AC, Mihon CE, Silva M, Galzerano A (2014). “Systemic mastocytosis – a diagnostic challenge”. Rev Bras Hematol Hemoter. 36 (3): 226–9. doi:10.1016/j.bjhh.2014.03.003. PMC 4109736. PMID 25031064.
- ↑ Valent P, Akin C, Metcalfe DD (March 2017). “Mastocytosis: 2016 updated WHO classification and novel emerging treatment concepts”. Blood. 129 (11): 1420–1427. doi:10.1182/blood-2016-09-731893. PMC 5356454. PMID 28031180.
- ↑ Kumar, Kirthi R.; Chen, Weina; Koduru, Prasad R.; Luu, Hung S. (2015). “Myeloid and Lymphoid Neoplasm With Abnormalities of FGFR1 Presenting With Trilineage Blasts and RUNX1 Rearrangement”. American Journal of Clinical Pathology. 143 (5): 738–748. doi:10.1309/AJCPUD6W1JLQQMNA. ISSN 1943-7722.
- ↑ Paolo Strati, Guilin Tang, Dzifa Y. Duose, Saradhi Mallampati, Rajyalakshmi Luthra, Keyur P. Patel, Mohammad Hussaini, Abu-Sayeef Mirza, Rami S. Komrokji, Stephen Oh, John Mascarenhas, Vesna Najfeld, Vivek Subbiah, Hagop Kantarjian, Guillermo Garcia-Manero, Srdan Verstovsek & Naval Daver (2018). “Myeloid/lymphoid neoplasms with FGFR1 rearrangement”. Leukemia & lymphoma. 59 (7): 1672–1676. doi:10.1080/10428194.2017.1397663. PMID 29119847. Unknown parameter
|month=ignored (help) - ↑ Ximena Montenegro-Garreaud, Roberto N. Miranda, Alexandra Reynolds, Guilin Tang, Sa A. Wang, Mariko Yabe, Wei Wang, Lianghua Fang, Carlos E. Bueso-Ramos, Pei Lin, L. Jeffrey Medeiros & Xinyan Lu (2017). “Myeloproliferative neoplasms with t(8;22)(p11.2;q11.2)/BCR-FGFR1: a meta-analysis of 20 cases shows cytogenetic progression with B-lymphoid blast phase”. Human pathology. 65: 147–156. doi:10.1016/j.humpath.2017.05.008. PMID 28551329. Unknown parameter
|month=ignored (help) - ↑ Paola Villafuerte-Gutierrez, Montserrat Lopez Rubio, Pilar Herrera & Eva Arranz (2018). “A Case of Myeloproliferative Neoplasm with BCR-FGFR1 Rearrangement: Favorable Outcome after Haploidentical Allogeneic Transplantation”. Case reports in hematology. 2018: 5724960. doi:10.1155/2018/5724960. PMID 30647980.
- ↑ Kamiya-Matsuoka C, Garciarena P, Amin HM, Tremont-Lukats IW, de Groot JF (December 2013). “B lymphoblastic leukemia/lymphoma presenting as seventh cranial nerve palsy”. Neurol Clin Pract. 3 (6): 532–534. doi:10.1212/CPJ.0b013e3182a78ef0. PMC 6082360. PMID 30107017.
- ↑ Zhang X, Rastogi P, Shah B, Zhang L (September 2017). “B lymphoblastic leukemia/lymphoma: new insights into genetics, molecular aberrations, subclassification and targeted therapy”. Oncotarget. 8 (39): 66728–66741. doi:10.18632/oncotarget.19271. PMC 5630450. PMID 29029550.
- ↑ Germing U, Kobbe G, Haas R, Gattermann N (November 2013). “Myelodysplastic syndromes: diagnosis, prognosis, and treatment”. Dtsch Arztebl Int. 110 (46): 783–90. doi:10.3238/arztebl.2013.0783. PMC 3855821. PMID 24300826.
- ↑ Gangat N, Patnaik MM, Tefferi A (January 2016). “Myelodysplastic syndromes: Contemporary review and how we treat”. Am. J. Hematol. 91 (1): 76–89. doi:10.1002/ajh.24253. PMID 26769228.
- ↑ Islam A, Catovsky D, Goldman JM, Galton DA (September 1985). “Bone marrow biopsy changes in acute myeloid leukaemia. I: Observations before chemotherapy”. Histopathology. 9 (9): 939–57. PMID 3864727.
- ↑ Orazi A (2007). “Histopathology in the diagnosis and classification of acute myeloid leukemia, myelodysplastic syndromes, and myelodysplastic/myeloproliferative diseases”. Pathobiology. 74 (2): 97–114. doi:10.1159/000101709. PMID 17587881.
- ↑ F. Julia, T. Petrella, M. Beylot-Barry, M. Bagot, D. Lipsker, L. Machet, P. Joly, O. Dereure, M. Wetterwald, M. d’Incan, F. Grange, J. Cornillon, G. Tertian, E. Maubec, P. Saiag, S. Barete, I. Templier, F. Aubin & S. Dalle (2013). “Blastic plasmacytoid dendritic cell neoplasm: clinical features in 90 patients”. The British journal of dermatology. 169 (3): 579–586. doi:10.1111/bjd.12412. PMID 23646868. Unknown parameter
|month=ignored (help) - ↑ Livio Pagano, Caterina Giovanna Valentini, Alessandro Pulsoni, Simona Fisogni, Paola Carluccio, Francesco Mannelli, Monia Lunghi, Gianmatteo Pica, Francesco Onida, Chiara Cattaneo, Pier Paolo Piccaluga, Eros Di Bona, Elisabetta Todisco, Pellegrino Musto, Antonio Spadea, Alfonso D’Arco, Stefano Pileri, Giuseppe Leone, Sergio Amadori & Fabio Facchetti (2013). “Blastic plasmacytoid dendritic cell neoplasm with leukemic presentation: an Italian multicenter study”. Haematologica. 98 (2): 239–246. doi:10.3324/haematol.2012.072645. PMID 23065521. Unknown parameter
|month=ignored (help) - ↑ Joseph D. Khoury (2018). “Blastic Plasmacytoid Dendritic Cell Neoplasm”. Current hematologic malignancy reports. 13 (6): 477–483. doi:10.1007/s11899-018-0489-z. PMID 30350260. Unknown parameter
|month=ignored (help) - ↑ Shinichiro Sukegawa, Mamiko Sakata-Yanagimoto, Ryota Matsuoka, Haruka Momose, Yusuke Kiyoki, Masayuki Noguchi, Naoya Nakamura, Rei Watanabe, Manabu Fujimoto, Yasuhisa Yokoyama, Hidekazu Nishikii, Takayasu Kato, Manabu Kusakabe, Naoki Kurita, Naoshi Obara, Yuichi Hasegawa & Shigeru Chiba (2018). “[Blastic plasmacytoid dendritic cell neoplasm accompanied by chronic myelomonocytic leukemia successfully treated with azacitidine]”. [[[Rinsho ketsueki] The Japanese journal of clinical hematology]]. 59 (12): 2567–2573. doi:10.11406/rinketsu.59.2567. PMID 30626790.
- ↑ Patnaik MM, Tefferi A (June 2016). “Chronic myelomonocytic leukemia: 2016 update on diagnosis, risk stratification, and management”. Am. J. Hematol. 91 (6): 631–42. doi:10.1002/ajh.24396. PMID 27185207.
- ↑ Parikh SA, Tefferi A (June 2012). “Chronic myelomonocytic leukemia: 2012 update on diagnosis, risk stratification, and management”. Am. J. Hematol. 87 (6): 610–9. doi:10.1002/ajh.23203. PMID 22615103.
- ↑ Benton CB, Nazha A, Pemmaraju N, Garcia-Manero G (August 2015). “Chronic myelomonocytic leukemia: Forefront of the field in 2015”. Crit. Rev. Oncol. Hematol. 95 (2): 222–42. doi:10.1016/j.critrevonc.2015.03.002. PMC 4859155. PMID 25869097.
- ↑ Dao KH, Tyner JW (2015). “What’s different about atypical CML and chronic neutrophilic leukemia?”. Hematology Am Soc Hematol Educ Program. 2015: 264–71. doi:10.1182/asheducation-2015.1.264. PMC 5266507. PMID 26637732.
- ↑ Muramatsu H, Makishima H, Maciejewski JP (February 2012). “Chronic myelomonocytic leukemia and atypical chronic myeloid leukemia: novel pathogenetic lesions”. Semin. Oncol. 39 (1): 67–73. doi:10.1053/j.seminoncol.2011.11.004. PMC 3523950. PMID 22289493.
- ↑ Aricò M, Biondi A, Pui CH (July 1997). “Juvenile myelomonocytic leukemia”. Blood. 90 (2): 479–88. PMID 9226148.
- ↑ Hasle H (March 1994). “Myelodysplastic syndromes in childhood–classification, epidemiology, and treatment”. Leuk. Lymphoma. 13 (1–2): 11–26. doi:10.3109/10428199409051647. PMID 8025513.
- ↑ Patnaik MM, Tefferi A (March 2017). “Refractory anemia with ring sideroblasts (RARS) and RARS with thrombocytosis (RARS-T): 2017 update on diagnosis, risk-stratification, and management”. Am. J. Hematol. 92 (3): 297–310. doi:10.1002/ajh.24637. PMID 28188970.
- ↑ Alshaban A, Padilla O, Philipovskiy A, Corral J, McAlice M, Gaur S (2018). “Lenalidomide induced durable remission in a patient with MDS/MPN-with ring sideroblasts and thrombocytosis with associated 5q- syndrome”. Leuk Res Rep. 10: 37–40. doi:10.1016/j.lrr.2018.08.001. PMID 30186759.
- ↑ Bouchla A, Papageorgiou SG, Tsakiraki Z, Glezou E, Pavlidis G, Stavroulaki G, Bazani E, Foukas P, Pappa V (2018). “Plasmablastic Lymphoma in an Immunocompetent Patient with MDS/MPN with Ring Sideroblasts and Thrombocytosis-A Case Report”. Case Rep Hematol. 2018: 2525070. doi:10.1155/2018/2525070. PMC 6247723. PMID 30524760.
- ↑ You MJ, Medeiros LJ, Hsi ED (September 2015). “T-lymphoblastic leukemia/lymphoma”. Am. J. Clin. Pathol. 144 (3): 411–22. doi:10.1309/AJCPMF03LVSBLHPJ. PMID 26276771.
- ↑ Patel KJ, Latif SU, de Calaca WM (March 2009). “An unusual presentation of precursor T cell lymphoblastic leukemia/lymphoma with cholestatic jaundice: case report”. J Hematol Oncol. 2: 12. doi:10.1186/1756-8722-2-12. PMC 2663564. PMID 19284608.
- ↑ Elreda L, Sandhu M, Sun X, Bekele W, Cohen AJ, Shah M (2014). “T-cell lymphoblastic leukemia/lymphoma: relapse 16 years after first remission”. Case Rep Hematol. 2014: 359158. doi:10.1155/2014/359158. PMC 4005062. PMID 24822133.
- ↑ Sedick Q, Alotaibi S, Alshieban S, Naheet KB, Elyamany G (2017). “Natural Killer Cell Lymphoblastic Leukaemia/Lymphoma: Case Report and Review of the Recent Literature”. Case Rep Oncol. 10 (2): 588–595. doi:10.1159/000477843. PMID 28868017.
- ↑ Jain N, Lamb AV, O’Brien S, Ravandi F, Konopleva M, Jabbour E, Zuo Z, Jorgensen J, Lin P, Pierce S, Thomas D, Rytting M, Borthakur G, Kadia T, Cortes J, Kantarjian HM, Khoury JD (April 2016). “Early T-cell precursor acute lymphoblastic leukemia/lymphoma (ETP-ALL/LBL) in adolescents and adults: a high-risk subtype”. Blood. 127 (15): 1863–9. doi:10.1182/blood-2015-08-661702. PMC 4915808. PMID 26747249.
- ↑ Haydu JE, Ferrando AA (July 2013). “Early T-cell precursor acute lymphoblastic leukaemia”. Curr. Opin. Hematol. 20 (4): 369–73. doi:10.1097/MOH.0b013e3283623c61. PMC 3886681. PMID 23695450.
- ↑ Rubin de Celis Ferrari AC, Glasberg J, Riechelmann RP (August 2018). “Carcinoid syndrome: update on the pathophysiology and treatment”. Clinics (Sao Paulo). 73 (suppl 1): e490s. doi:10.6061/clinics/2018/e490s. PMC 6096975. PMID 30133565.
- ↑ Hegyi J, Schwartz RA, Hegyi V (January 2004). “Pellagra: dermatitis, dementia, and diarrhea”. Int. J. Dermatol. 43 (1): 1–5. PMID 14693013.
- ↑ Savelli G, Lucignani G, Seregni E, Marchianò A, Serafini G, Aliberti G, Villano C, Maccauro M, Bombardieri E (May 2004). “Feasibility of somatostatin receptor scintigraphy in the detection of occult primary gastro-entero-pancreatic (GEP) neuroendocrine tumours”. Nucl Med Commun. 25 (5): 445–9. PMID 15100502.
- ↑ Savelli G, Lucignani G, Seregni E, Marchianò A, Serafini G, Aliberti G, Villano C, Maccauro M, Bombardieri E (May 2004). “Feasibility of somatostatin receptor scintigraphy in the detection of occult primary gastro-entero-pancreatic (GEP) neuroendocrine tumours”. Nucl Med Commun. 25 (5): 445–9. PMID 15100502.
- ↑ Bora, ManashKumar; Vithiavathi, S (2012). “Primary bronchial carcinoid: A rare differential diagnosis of pulmonary koch in young adult patient”. Lung India. 29 (1): 59. doi:10.4103/0970-2113.92366. ISSN 0970-2113.
- ↑ Yazıcıoğlu A, Yekeler E, Bıcakcıoğlu P, Ozaydın E, Karaoğlanoğlu N (December 2012). “Synchronous bilateral multiple typical pulmonary carcinoid tumors: a unique case with 10 typical carcinoids”. Balkan Med J. 29 (4): 450–2. doi:10.5152/balkanmedj.2012.081. PMC 4115868. PMID 25207053.
- ↑ Krausz Y, Keidar Z, Kogan I, Even-Sapir E, Bar-Shalom R, Engel A, Rubinstein R, Sachs J, Bocher M, Agranovicz S, Chisin R, Israel O (November 2003). “SPECT/CT hybrid imaging with 111In-pentetreotide in assessment of neuroendocrine tumours”. Clin. Endocrinol. (Oxf). 59 (5): 565–73. PMID 14616879.
- ↑ van der Lely, Aart J.; Herder, Wouter W. de (2005). “Carcinoid syndrome: diagnosis and medical management”. Arquivos Brasileiros de Endocrinologia & Metabologia. 49 (5): 850–860. doi:10.1590/S0004-27302005000500028. ISSN 0004-2730.
- ↑ Halperin DM, Shen C, Dasari A, Xu Y, Chu Y, Zhou S, Shih YT, Yao JC (April 2017). “Frequency of carcinoid syndrome at neuroendocrine tumour diagnosis: a population-based study”. Lancet Oncol. 18 (4): 525–534. doi:10.1016/S1470-2045(17)30110-9. PMC 6066284. PMID 28238592.
- ↑ Sjöblom SM (September 1988). “Clinical presentation and prognosis of gastrointestinal carcinoid tumours”. Scand. J. Gastroenterol. 23 (7): 779–87. PMID 3227292.
- ↑ Ganeshan D, Bhosale P, Yang T, Kundra V (October 2013). “Imaging features of carcinoid tumors of the gastrointestinal tract”. AJR Am J Roentgenol. 201 (4): 773–86. doi:10.2214/AJR.12.9758. PMID 24059366.
- ↑ Signs and symptoms of carcinoid syndrome. National Cancer Institute. http://www.cancer.gov/types/gi-carcinoid-tumors/patient/gi-carcinoid-treatment-pdq
- ↑ Modlin IM, Kidd M, Latich I, Zikusoka MN, Shapiro MD (May 2005). “Current status of gastrointestinal carcinoids”. Gastroenterology. 128 (6): 1717–51. PMID 15887161.
- ↑ Gustafsson BI, Kidd M, Chan A, Malfertheiner MV, Modlin IM (July 2008). “Bronchopulmonary neuroendocrine tumors”. Cancer. 113 (1): 5–21. doi:10.1002/cncr.23542. PMID 18473355.
- ↑ Jeung, Mi-Young; Gasser, Bernard; Gangi, Afshin; Charneau, Dominique; Ducroq, Xavier; Kessler, Romain; Quoix, Elisabeth; Roy, Catherine (2002). “Bronchial Carcinoid Tumors of the Thorax: Spectrum of Radiologic Findings”. RadioGraphics. 22 (2): 351–365. doi:10.1148/radiographics.22.2.g02mr01351. ISSN 0271-5333.
- ↑ Nessi R, Basso Ricci P, Basso Ricci S, Bosco M, Blanc M, Uslenghi C (April 1991). “Bronchial carcinoid tumors: radiologic observations in 49 cases”. J Thorac Imaging. 6 (2): 47–53. PMID 1649924.
- ↑ Melmon KL, Sjoerdsma A, Mason DT (October 1965). “Distinctive clinical and therapeutic aspects of the syndrome associated with bronchial carcinoid tumors”. Am. J. Med. 39 (4): 568–81. PMID 5831899.
- ↑ Ford AC, Forman D, Bailey AG, Axon AT, Moayyedi P (May 2008). “Irritable bowel syndrome: a 10-yr natural history of symptoms and factors that influence consultation behavior”. Am. J. Gastroenterol. 103 (5): 1229–39, quiz 1240. doi:10.1111/j.1572-0241.2007.01740.x. PMID 18371141.
- ↑ Simren M, Palsson OS, Whitehead WE (April 2017). “Update on Rome IV Criteria for Colorectal Disorders: Implications for Clinical Practice”. Curr Gastroenterol Rep. 19 (4): 15. doi:10.1007/s11894-017-0554-0. PMC 5378729. PMID 28374308.
- ↑ “American Gastroenterological Association medical position statement: irritable bowel syndrome”. Gastroenterology. 123 (6): 2105–7. December 2002. doi:10.1053/gast.2002.37095b. PMID 12454865.
- ↑ Mearin F, Lacy BE, Chang L, Chey WD, Lembo AJ, Simren M, Spiller R (February 2016). “Bowel Disorders”. Gastroenterology. doi:10.1053/j.gastro.2016.02.031. PMID 27144627.
- ↑ McLaughlin PD, Maher MM (July 2013). “Primary malignant diseases of the small intestine”. AJR Am J Roentgenol. 201 (1): W9–14. doi:10.2214/AJR.12.8492. PMID 23789703.
- ↑ Hatzaras I, Palesty JA, Abir F, Sullivan P, Kozol RA, Dudrick SJ, Longo WE (March 2007). “Small-bowel tumors: epidemiologic and clinical characteristics of 1260 cases from the connecticut tumor registry”. Arch Surg. 142 (3): 229–35. doi:10.1001/archsurg.142.3.229. PMID 17372046.
- ↑ Lepage C, Bouvier AM, Manfredi S, Dancourt V, Faivre J (December 2006). “Incidence and management of primary malignant small bowel cancers: a well-defined French population study”. Am. J. Gastroenterol. 101 (12): 2826–32. doi:10.1111/j.1572-0241.2006.00854.x. PMID 17026561.
- ↑ Hara AK, Swartz PG (2009). “CT enterography of Crohn’s disease”. Abdom Imaging. 34 (3): 289–95. doi:10.1007/s00261-008-9443-1. PMID 18649092.
- ↑ Baumgart, Daniel C; Sandborn, William J (2012). “Crohn’s disease”. The Lancet. 380 (9853): 1590–1605. doi:10.1016/S0140-6736(12)60026-9. ISSN 0140-6736.
- ↑ Feuerstein, Joseph D.; Cheifetz, Adam S. (2017). “Crohn Disease: Epidemiology, Diagnosis, and Management”. Mayo Clinic Proceedings. 92 (7): 1088–1103. doi:10.1016/j.mayocp.2017.04.010. ISSN 0025-6196.
- ↑ García-Bosch, O.; Ordás, I.; Aceituno, M.; Rodríguez, S.; Ramírez, A. M.; Gallego, M.; Ricart, E.; Rimola, J.; Panes, J. (2016). “Comparison of Diagnostic Accuracy and Impact of Magnetic Resonance Imaging and Colonoscopy for the Management of Crohn’s Disease”. Journal of Crohn’s and Colitis. 10 (6): 663–669. doi:10.1093/ecco-jcc/jjw015. ISSN 1873-9946.
- ↑ Izikson, Leonid; English, Joseph C.; Zirwas, Matthew J. (2006). “The flushing patient: Differential diagnosis, workup, and treatment”. Journal of the American Academy of Dermatology. 55 (2): 193–208. doi:10.1016/j.jaad.2005.07.057. ISSN 0190-9622.
- ↑ Hartmann, Karin; Escribano, Luis; Grattan, Clive; Brockow, Knut; Carter, Melody C.; Alvarez-Twose, Ivan; Matito, Almudena; Broesby-Olsen, Sigurd; Siebenhaar, Frank; Lange, Magdalena; Niedoszytko, Marek; Castells, Mariana; Oude Elberink, Joanna N.G.; Bonadonna, Patrizia; Zanotti, Roberta; Hornick, Jason L.; Torrelo, Antonio; Grabbe, Jürgen; Rabenhorst, Anja; Nedoszytko, Boguslaw; Butterfield, Joseph H.; Gotlib, Jason; Reiter, Andreas; Radia, Deepti; Hermine, Olivier; Sotlar, Karl; George, Tracy I.; Kristensen, Thomas K.; Kluin-Nelemans, Hanneke C.; Yavuz, Selim; Hägglund, Hans; Sperr, Wolfgang R.; Schwartz, Lawrence B.; Triggiani, Massimo; Maurer, Marcus; Nilsson, Gunnar; Horny, Hans-Peter; Arock, Michel; Orfao, Alberto; Metcalfe, Dean D.; Akin, Cem; Valent, Peter (2016). “Cutaneous manifestations in patients with mastocytosis: Consensus report of the European Competence Network on Mastocytosis; the American Academy of Allergy, Asthma & Immunology; and the European Academy of Allergology and Clinical Immunology”. Journal of Allergy and Clinical Immunology. 137 (1): 35–45. doi:10.1016/j.jaci.2015.08.034. ISSN 0091-6749.
- ↑ Lee, Jason K; Whittaker, Scott J; Enns, Robert A; Zetler, Peter (2008). “Gastrointestinal manifestations of systemic mastocytosis”. World Journal of Gastroenterology. 14 (45): 7005. doi:10.3748/wjg.14.7005. ISSN 1007-9327.
- ↑ Horan RF, Austen KF (March 1991). “Systemic mastocytosis: retrospective review of a decade’s clinical experience at the Brigham and Women’s Hospital”. J. Invest. Dermatol. 96 (3): 5S–13S, discussion 13S–14S. PMID 2002264.
- ↑ Sokol, Harry; Georgin-Lavialle, Sophie; Grandpeix-Guyodo, Catherine; Canioni, Danielle; Barete, Stéphane; Dubreuil, Patrice; Lortholary, Olivier; Beaugerie, Laurent; Hermine, Olivier (2010). “Gastrointestinal involvement and manifestations in systemic mastocytosis”. Inflammatory Bowel Diseases. 16 (7): 1247–1253. doi:10.1002/ibd.21218. ISSN 1078-0998.
- ↑ Bedeir A, Jukic DM, Wang L, Mullady DK, Regueiro M, Krasinskas AM (November 2006). “Systemic mastocytosis mimicking inflammatory bowel disease: A case report and discussion of gastrointestinal pathology in systemic mastocytosis”. Am. J. Surg. Pathol. 30 (11): 1478–82. doi:10.1097/01.pas.0000213310.51553.d7. PMID 17063092.
- ↑ Fuhlbrigge A, Peden D, Apter AJ, Boushey HA, Camargo CA, Gern J, Heymann PW, Martinez FD, Mauger D, Teague WG, Blaisdell C (March 2012). “Asthma outcomes: exacerbations”. J. Allergy Clin. Immunol. 129 (3 Suppl): S34–48. doi:10.1016/j.jaci.2011.12.983. PMC 3595577. PMID 22386508.
- ↑ Limb SL, Brown KC, Wood RA, Wise RA, Eggleston PA, Tonascia J, Adkinson NF (December 2005). “Irreversible lung function deficits in young adults with a history of childhood asthma”. J. Allergy Clin. Immunol. 116 (6): 1213–9. doi:10.1016/j.jaci.2005.09.024. PMID 16337448.
- ↑ Aldington S, Beasley R (May 2007). “Asthma exacerbations. 5: assessment and management of severe asthma in adults in hospital”. Thorax. 62 (5): 447–58. doi:10.1136/thx.2005.045203. PMC 2117186. PMID 17468458.
- ↑ Dougherty RH, Fahy JV (February 2009). “Acute exacerbations of asthma: epidemiology, biology and the exacerbation-prone phenotype”. Clin. Exp. Allergy. 39 (2): 193–202. doi:10.1111/j.1365-2222.2008.03157.x. PMC 2730743. PMID 19187331.
- ↑ Peavy RD, Metcalfe DD (August 2008). “Understanding the mechanisms of anaphylaxis”. Curr Opin Allergy Clin Immunol. 8 (4): 310–5. doi:10.1097/ACI.0b013e3283036a90. PMC 2683407. PMID 18596587.
- ↑ Tupper J, Visser S (October 2010). “Anaphylaxis: A review and update”. Can Fam Physician. 56 (10): 1009–11. PMC 2954079. PMID 20944042.
- ↑ Kemp SF, Lockey RF (September 2002). “Anaphylaxis: a review of causes and mechanisms”. J. Allergy Clin. Immunol. 110 (3): 341–8. PMID 12209078.
- ↑ Bjornsson HM, Graffeo CS (December 2010). “Improving diagnostic accuracy of anaphylaxis in the acute care setting”. West J Emerg Med. 11 (5): 456–61. PMC 3027438. PMID 21293765.
- ↑ “Usefulness and Limitations of Sequential Serum Tryptase for the Diagnosis of Anaphylaxis in 102 Patients – FullText – International Archives of Allergy and Immunology 2013, Vol. 160, No. 2 – Karger Publishers”.
- ↑ Busse PJ, Smith T (August 2017). “Histaminergic Angioedema”. Immunol Allergy Clin North Am. 37 (3): 467–481. doi:10.1016/j.iac.2017.03.001. PMID 28687103.
- ↑ Hahn J, Hoffmann TK, Bock B, Nordmann-Kleiner M, Trainotti S, Greve J (July 2017). “Angioedema”. Dtsch Arztebl Int. 114 (29–30): 489–496. doi:10.3238/arztebl.2017.0489. PMC 5569554. PMID 28818177.
- ↑ Bernstein JA, Cremonesi P, Hoffmann TK, Hollingsworth J (December 2017). “Angioedema in the emergency department: a practical guide to differential diagnosis and management”. Int J Emerg Med. 10 (1): 15. doi:10.1186/s12245-017-0141-z. PMC 5389952. PMID 28405953.
- ↑ Bernstein JA, Moellman J (November 2012). “Emerging concepts in the diagnosis and treatment of patients with undifferentiated angioedema”. Int J Emerg Med. 5 (1): 39. doi:10.1186/1865-1380-5-39. PMC 3518251. PMID 23131076.
- ↑ Kaplan AP (June 2008). “Angioedema”. World Allergy Organ J. 1 (6): 103–13. doi:10.1097/WOX.0b013e31817aecbe. PMC 3651192. PMID 23282406.
- ↑ Pacini F, Castagna MG, Cipri C, Schlumberger M (August 2010). “Medullary thyroid carcinoma”. Clin Oncol (R Coll Radiol). 22 (6): 475–85. doi:10.1016/j.clon.2010.05.002. PMID 20627492.
- ↑ Roy M, Chen H, Sippel RS (2013). “Current understanding and management of medullary thyroid cancer”. Oncologist. 18 (10): 1093–100. doi:10.1634/theoncologist.2013-0053. PMC 3805151. PMID 24037980.
- ↑ Mian C, Perrino M, Colombo C, Cavedon E, Pennelli G, Ferrero S, De Leo S, Sarais C, Cacciatore C, Manfredi GI, Verga U, Iacobone M, De Pasquale L, Pelizzo MR, Vicentini L, Persani L, Fugazzola L (May 2014). “Refining calcium test for the diagnosis of medullary thyroid cancer: cutoffs, procedures, and safety”. J. Clin. Endocrinol. Metab. 99 (5): 1656–64. doi:10.1210/jc.2013-4088. PMID 24552221.
- ↑ Bae YJ, Schaab M, Kratzsch J (2015). “Calcitonin as Biomarker for the Medullary Thyroid Carcinoma”. Recent Results Cancer Res. 204: 117–37. doi:10.1007/978-3-319-22542-5_5. PMID 26494386.
Epidemiology and Demographics
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1];Associate Editor(s)-in-Chief: Suveenkrishna Pothuru, M.B,B.S. [2]
Overview
Mast cell tumor is a rare disease and considered to be an “orphan disease” affecting 200,000 or fewer people in the United States. There are no definite data regarding the prevalence of mast cell tumor among the US general population. Cutaneous mastocytosis is more common in children and the disease manifest itself in the first year of life in over 80% of cases. There is no sex predilection and race predilection to the mast cell tumor.
Epidemiology and Demographics
Mast cell tumor is a rare disease characterized by abnormal growth and accumulation of mast cells in various organs. It is considered to be an “orphan disease” affecting 200,000 or fewer people in the United States.[1]
Incidence
- There are no definite data regarding the exact incidence and prevalence of mast cell tumor among the US general population.[2]
Age
- Patients of all age groups may develop mast cell tumor.
- Urticaria pigmentosa, the cutaneous mastocytosis is more common in children and the disease manifest itself in the first year of life in over 80% of cases.[3]
- Second smaller peak of incidence is observed in adults in the third to fourth decade.[3]
- Systemic mastocytosis generally occurs in middle age.
Gender
- There is no sex predilection to the mast cell tumor.
Race
- There is no racial predilection to the mast cell tumor.
References
- ↑ Koenig, Martial; Morel, Jérôme; Reynaud, Jacqueline; Varvat, Cécile; Cathébras, Pascal (2008). “An unusual cause of spontaneous bleeding in the intensive care unit – mastocytosis: a case report”. Cases Journal. 1 (1): 100. doi:10.1186/1757-1626-1-100. ISSN 1757-1626.
- ↑ Brockow K (2014). “Epidemiology, prognosis, and risk factors in mastocytosis”. Immunol Allergy Clin North Am. 34 (2): 283–95. doi:10.1016/j.iac.2014.01.003. PMID 24745674.
- ↑ 3.0 3.1 Ferrante, Giuliana; Scavone, Valeria; Muscia, Maria; Adrignola, Emilia; Corsello, Giovanni; Passalacqua, Giovanni; La Grutta, Stefania (2015). “The care pathway for children with urticaria, angioedema, mastocytosis”. World Allergy Organization Journal. 8 (1): 5. doi:10.1186/s40413-014-0052-x. ISSN 1939-4551.
Risk Factors
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1];Associate Editor(s)-in-Chief: Suveenkrishna Pothuru, M.B,B.S. [2]
Overview
Common risk factors in the development of mast cell tumor are age and mutation of C-kit receptor.
Risk Factors
- Age
- Infants and children are at high risk to develop mast cell tumor.
- C-kit receptor mutation
- C-kit receptor is a surface protein that binds to stem cell factor which is a chemical entity that fosters the growth of certain types of cells.
References
Screening
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief:
Overview
There is insufficient evidence to recommend routine screening for mast cell tumor.
Screening
There is insufficient evidence to recommend routine screening for mast cell tumor.
References
Natural History, Complications and Prognosis
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1];Associate Editor(s)-in-Chief: Suveenkrishna Pothuru, M.B,B.S. [2]
Overview
Common complications of mast cell tumor include episodes of anaphylaxis, osteoporosis, and progression to malignant mastocytosis or mast cell leukemia. The prognosis of mast cell tumor varies with the subtype, location, and extent of the tumor. The cutaneous mastocytosis is associated with the most favorable prognosis and mast cell leukemia is associated with poor prognosis.
Natural History
- Mast cell tumor usually occurs as a sporadic disease that is often transient and limited in children and progressive in adults.[1]
- Systemic mastocytosis may develop in childhood cases of urticaria pigmentosa that persist beyond puberty, and in approximately 40% of adults with urticaria pigmentosa, usually of long standing.
- Patients with mast cell tumor often initially have symptom-free intervals interspersed among symptomatic periods.
- Over time, symptom-free intervals shorten, and finally symptoms become chronic with intensity which fluctuates but with an overall trend toward steadily increasing intensity.
Complications
Common complications of mast cell tumor include:[1]
- Anaphylaxis
- Osteoporosis
- Systemic mastocytosis may progress to malignant mastocytosis and/ or mast cell leukemia
Prognosis
The prognosis varies with the location and extent of the tumor:[1]
| Subtype | Prognosis |
|---|---|
|
Cutaneous mastocytosis |
|
|
Systemic mastocytosis |
Prognosis varies with degree of hematological and organ involvement
|
|
Localized mastocytosis |
|
References
- ↑ 1.0 1.1 1.2 Mastocytosis and mast cell disorders.Patient info.http://patient.info/doctor/mastocytosis-and-mast-cell-disorders#ref-20 accessed on March 7th, 2016
Diagnosis
Diagnosis
Diagnostic Criteria | Staging | History and Symptoms | Physical Examination | Laboratory Findings | Electrocardiogram | X-Ray Findings | Echocardiography and Ultrasound | CT-Scan Findings | MRI Findings | Biopsy | Other Imaging Findings | Other Diagnostic Studies
Treatment
Treatment
Medical Therapy | Surgery | Cost-Effectiveness of Therapy | Future or Investigational Therapies
Looking for the patient version?
© 2026 MyEClinic – IFTM Institut für Telematik in der Medizin GmbH