
Chagas disease
For patient information click here
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Yazan Daaboul, M.D., Huda A. Karman, M.D. Raviteja Guddeti, M.B.B.S. [2], Tamar Sifri [3]
Synonyms and keywords: Chagas’ disease; American trypanosomiasis; Trypanosoma cruzi infection
Overview
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Yazan Daaboul, M.D. Raviteja Guddeti, M.B.B.S. [2]
Overview
Chagas disease (American trypanosomiasis) is an infectious disease caused by the flagellate protozoan parasite, T. cruzi. The global incidence of Chagas disease is estimated to be 5-8 million with global incidence of Chagas disease of approxiamtely 100-400 per 100,000 individuals. The majority of cases are reported in South America, where Chagas disease is considered the most common parasitic infection. The most common mode of transmission of Chagas disease is vectorborne via exposure to feces/urine of infected triatomine (Riduvid) insects. The incubation period of T. cruzi is 1-2 weeks following transmission. The majority (90%-95%) of infected individuals remain asymptomatic in the acute phase following Chagas disease infection. Nonetheless, patients typically remain chronically infected and demonstrate clinical manifestation several years/decades following infection. Approximately 1/3 of patients develop manifestations of the chronic Chagas disease, namely cardiac conduction system dysfunction, GI denervation with esophageal and/or colonic dysfunction (megaesophagus and megacolon). Acute Chagas disease is often diagnosed by peripheral blood smear following the visual detection of T. cruzi parasite. In contrast, the diagnosis of chronic Chagas disease is more difficult and requires serial serological or PCR testing. Benznidazole and nifurtimox are the only antimicrobial therapies with proven efficacy against T. cruzi infection. Neither drug is FDA-approved, but can be obtained under investigational protocol. Either benznidazole or nifurtimox may be used to manage congenital infection, acute infection, and chronic infection (only among young patients < 50-55 years) including those with early cardiomyopathy. Chronic Chagas’ disease leads to congestive heart failure. These patients commonly have right bundle branch block and/or other arrhythmias. These hearts are dilated and hypertrophied, have areas of fibrosis especially in the apex, and often contain mural thrombi. The myocardium is infiltrated with lymphocytes and macrophages and there is interstitial edema and fibrosis. This inflammatory reaction is most severe around the area of the right bundle branch. Patients may also develop megaesophagus and/or megacolon.
Historical Perspective
The discovery of T. cruzi, the parasite that causes Chagas disease, dates back to pre-Columbian times in South America. Carlos Chagas,a Brazilian bacteriologist, was the first to discover the association between the Riduvid insect and T. cruzi. Carlos Chagas named the pathogen T. cruzi in honor of his mentor, Oswaldo Cruz. In 1966, Benznidazole was introduced and was the first antimicrobial agent against T. cruzi infections.
Pathophysiology
The most common mode of transmission of Chagas disease is vectorborne via exposure to feces/urine of infected triatomine insects. Nonetheless, other modes of transmission, such as via blood transfusion, organ transplant, oral ingestion, breast milk, and vertical transmission, are possible. The hallmark of Chagas disease is inflammation. Acutely following transmission, a state of parasitemia, characterized by parasitic replication and host immune responses, is responsible for the development of clinical manifestations. Following the acute phase, it is thought that Chagas disease causes a state of low-grade persistent inflammation that eventually results in the development of chronic disease, manifested by multisystem involvement. The pathogenesis of chronic Chagas disease is poorly understood, but is thought to be caused by either persistent parasites that were not eliminated by the host during the acute phase or development of autoimmune destructive processes. On gross pathology, acute Chagas disease is characterized by inflammation, whereas chronic disease often demonstrates tissue dilation and congestion, along with evidence of fibrosis and wall thickening. On microscopic histopathological analysis, acute Chagas disease demonstrates mononuclear and lymphocytic infiltration in infected tissue, which chronically result in tissue denervation and fibrous scar formation.
Chagas disease in the heart:
The histologic diagnosis of Chronic Chagas cardiomyopathy (CCM) consists of a diffuse and patchy chronic myocarditis, interstitial mononuclear cell infiltrates, and myocardial fiber destruction with fibrotic replacement. Grossly enlarged hearts have been found in autopsy studies in subjects with end stage of Chagas disease. Left ventricular apical aneurysms are also frequently found on autopsy.
Causes
Chagas disease is a human tropical parasitic disease usually caused by Trypanosoma cruzi, a flagellate protozoa.
Differentiating Chagas disease from other Diseases
Chagas disease must be differentiated from other diseases the cause cardiomyopathy, hepatosplenomegaly, or esophageal/colonic dysfunction, such as electrophysiological cardiac diseases, GI hypomotility disorders, and malignancies.
Epidemiology and Demographics
The global incidence of Chagas disease is estimated to be 5-8 million with global incidence of Chagas disease of approxiamtely 100-400 per 100,000 individuals. The majority of cases are reported in South America, where Chagas disease is considered the most common parasitic infection. Individuals of all age groups may acquire Chagas disease, including neonates due to risk of vertical transmission. Elderly patients often demonstrate clinical manifestations of chronic Chagas disease. Although there is no evidence that suggests racial predilection to the acquisition of the disease, the majority of cases are reported among individuals of Hispanic origin due to the endemicity of the disease in South America. The majority of cases outside South America are among South American immigrants.
Risk Factors
Risk factors for Chagas disease include residence in Central or South America, living in old houses with either mud and sticks wall constructions or straw roofs, ingestion of contaminated water, or receiving blood transfusions / organ donation from individuals in regions with high endemicity. Neonatal risk is highest among those who breastfeed from bleeding / cracked nipples of infected mothers and those who are delivered from seropositive mothers with active disease.
Natural History, Complications and Prognosis
The incubation period of T. cruzi is 1-2 weeks following transmission. The majority (90%-95%) of infected individuals remain asymptomatic in the acute phase following Chagas disease infection. Nonetheless, patients typically remain chronically infected and demonstrate clinical manifestations several years/decades following infection. Approximately 1/3 of patients develop manifestations of the chronic Chagas disease, namely cardiac conduction system dysfunction, GI denervation with esophageal and/or colonic dysfunction (megaesophagus and megacolon). Chagas cardiomyopathy is the most common chronic manifestation of the disease and accounts for approximately 80-90% of chronic manifestations. The majority of patients with Chagas cardiomyopathy die within 2 years of symptom onset.
Diagnosis
Symptoms
The majority of patients with acute Chagas disease infection are asymptomatic. Clinical manifestations of the acute phase of infection commonly non-specific symptoms, such as fever, myalgia, fatigue, and anorexia. Less commonly, patients may present with more severe disease that may be suggestive of early Chagas myocarditis or meningoencephalitis. Chronic symptoms are generally manifestations of Chagas either cardiomyopathy or GI disease.
Physical Examination
On physical examination, Chagas disease may manifest with fever, tachycardia, cardiac rhythm abnormalities, hepatosplenomegaly, and lymphadenopathy. Romaña’s sign, a classical sign of Chagas disease, is characterized by eyelid sweilling at the site of parasitic entry. Other signs on physical examination are usually due to either cardiac or GI manifestations of the disease.
Laboratory Findings
Acute Chagas disease is often diagnosed by peripheral blood smear following the visual detection of T. cruzi parasite. Serology is often helpful for chronic cases only, where assay positivity of both “whole parasite lysate” and “recombinant antigen” is usually required for the diagnosis. Although PCR is sensitive in acute cases (e.g. exposure following organ transplantation), its sensitivity and specificity are variable in the chronic state and highly depend on the pre-test probability.
Electrocardiography
RBBB and AV block are common findings on ECG among patients with Chagas disease cardiomyopathy.
Treatment
Medical Therapy
Benznidazole and nifurtimox are the only antimicrobial therapies with proven efficacy against T. cruzi infection. Neither drug is FDA-approved, but can be obtained under investigational protocol. Either benznidazole or nifurtimox may be used to manage congenital infection, acute infection, and chronic infection (only among young patients < 50-55 years) including those with early cardiomyopathy.
Primary Prevention
Methods of primary prevention of Chagas disease include use of insecticides to control the vector, use of new construction compounds in building walls and roofs, and organ/blood testing prior to donation.
Future or Investigational Therapies
Although novel investigational drugs are being studied for chronic Chagas disease, to date no new pharmacologic therapy has proven to be effective compared with the current standard of care (either benznidazole or nifurtimox therapy)
References
Historical Perspective
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Yazan Daaboul, M.D., Raviteja Guddeti, M.B.B.S. [2]
Overview
The discovery of T. cruzi, the parasite that causes Chagas disease, dates back to pre-Columbian times in South America. Carlos Chagas,a Brazilian bacteriologist, was the first to discover the association between the Riduvid insect and T. cruzi. Carlos Chagas named the pathogen T. cruzi in honor of his mentor, Oswaldo Cruz. In 1966, Benznidazole was introduced and was the first antimicrobial agent against T. cruzi infections.
Historical Perspective
- The earliest evidence of Chagas disease infection dates to pre-Columbian times (9000 years ago) in South America, where positive PCR DNA sequences were discovered among Chinchorro mummies.[1]
- The vector for T. cruzi, the Reduvius (kissing/assassin) bug, was first described by Charles Darwin during his voyage of the Beagle.[2]
- Carlos Chagas,a Brazilian bacteriologist, was the first to discover the association between the triatomine Riduvid insect and T. cruzi. Carlos Chagas named the pathogen T. cruzi in honor of his mentor, Oswaldo Cruz.[3]
- Further contributions to the characteristization of T. cruzi were made by microbiological identification of the parasite were made by Stanislaus von Prowazek (microbiological characteristics of the parasite), Gaspara de Oliveria Vianna (intracellular life cycle), Alexandre Joseph Emile Brumpt (mode of vector transmission of the parasite), and Salvador Mazza (blood transfusion transmission and clinical description of the disease).[3]
- Benznidazole, introduced in 1966, was the first medical therapy for Chagas disease. In 1970, nifurtimox was introduced.[4]
- In 1940, vector control was attempted using organochloride insecticides, but these compounds proved to be ineffective against triatomines. It was not until 1980 that effective vector control by pyrethroid insecticides was introduced.[5]
References
- ↑ Aufderheide AC, Salo W, Madden M, Streitz J, Buikstra J, Guhl F; et al. (2004). “A 9,000-year record of Chagas’ disease”. Proc Natl Acad Sci U S A. 101 (7): 2034–9. doi:10.1073/pnas.0307312101. PMC 357047. PMID 14766963.
- ↑ Miles MA (2004). “The discovery of Chagas disease: progress and prejudice”. Infect Dis Clin North Am. 18 (2): 247–60, table of contents. doi:10.1016/j.idc.2004.01.005. PMID 15145379.
- ↑ 3.0 3.1 Steverding D (2014). “The history of Chagas disease”. Parasit Vectors. 7: 317. doi:10.1186/1756-3305-7-317. PMC 4105117. PMID 25011546.
- ↑ Rodriques Coura J, de Castro SL (2002). “A critical review on Chagas disease chemotherapy”. Mem Inst Oswaldo Cruz. 97 (1): 3–24. PMID 11992141.
- ↑ Dias J, Schofield C (1999). “The evolution of Chagas disease (American trypanosomiasis) control after 90 years since Carlos Chagas discovery”. Mem Inst Oswaldo Cruz. 94 Suppl 1: 103–21. PMID 10677697.
Classification
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief:
Overview
There is no established system for the classification of Chagas disease. We can classify Chagas disease based on the transmission route of Trypanosoma cruzi or based on the clinical manifestations (acute, chronic, congenital, cardiac, and digestive).
Classification
There is no established system for the classification of Chagas disease. However, we can classify Chagas disease based on the following: [1]
- Based on the etiology transmission routes:
- Vector-borne transmission
- Congenital transmission
- Blood-borne transmission.
- Organ-derived transmission
- Oral transmission
- Based on the clinical manifestations:
References
- ↑ Bern C, Kjos S, Yabsley MJ, Montgomery SP (2011). “Trypanosoma cruzi and Chagas’ Disease in the United States”. Clin Microbiol Rev. 24 (4): 655–81. doi:10.1128/CMR.00005-11. PMC 3194829. PMID 21976603.
Pathophysiology
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Yazan Daaboul, M.D., Raviteja Guddeti, M.B.B.S. [2]
Overview
The most common mode of transmission of Chagas disease is vectorborne via exposure to feces/urine of infected triatomine insects. Nonetheless, other modes of transmission, such as via blood transfusion, organ transplant, oral ingestion, breast milk, and vertical transmission, are possible. The hallmark of Chagas disease is inflammation. Acutely following transmission, a state of parasitemia, characterized by parasitic replication and host immune responses, is responsible for the development of clinical manifestations. Following the acute phase, it is thought that Chagas disease causes a state of low-grade persistent inflammation that eventually results in the development of chronic disease, manifested by multisystem involvement. The pathogenesis of chronic Chagas disease is poorly understood, but is thought to be caused by either persistent parasites that were not eliminated by the host during the acute phase or development of autoimmune destructive processes. On gross pathology, acute Chagas disease is characterized by inflammation, whereas chronic disease often demonstrates tissue dilation and congestion, along with evidence of fibrosis and wall thickening. On microscopic histopathological analysis, acute Chagas disease demonstrates mononuclear and lymphocytic infiltration in infected tissue, which chronically result in tissue denervation and fibrous scar formation. The histologic diagnosis of Chronic Chagas cardiomyopathy (CCM) consists of a diffuse and patchy chronic myocarditis, interstitial mononuclear cell infiltrates, and myocardial fiber destruction with fibrotic replacement. Grossly enlarged hearts have been found in autopsy studies in subjects with end stage of Chagas disease. Left ventricular apical aneurysms are also frequently found on autopsy.
Pathophysiology
Transmission
- Chagas disease usually has a vector-borne transmission. Triatomine insects, the Riduvid (kissing/assassin) bugs, suck blood from an infected individual and are subsequently infected themselves.
- The insects carry the pathogen in their feces and urine. Human infection with T. cruzi occurs following exposure to feces/urine of infected insects. The pathogen typically enters the host either through a wound induced by the host’s scratching following the insect bite or through the conjunctival mucus membranes.
- Other modes of transmission include organ transplantation, blood transfusions, vertical transmission, breast milk, and oral transmission following ingestion of infected foods.[1][2][3][4]
- The incubation period following transmission is typically 1-2 weeks following transmission.

Cellular Pathogenesis
Acute infection
- Following transmission, trypomastigotes invade host cells via a unique transmigration process that involves bradykinin and CCL2 chemokine.
- Unlike African trypanosomes, the bloodstream trypomastigotes are unable to replicate. Instead, they differentiate into intracellular amastigotes intracellularly.
- The amastigotes multiply by binary fission and re-transform into trypomastigotes, which are released again into the blood and lymphatic circulations. These newly formed trypomastigotes are then able to infect new host tissues (macrophages, fibroblasts, skeletal and cardiac myocytes, and endothelial cells), which often accounts for the high grade parasitemia and the multisystem complications associated with Chagas disease.
- Inflammation is the hallmark of Chagas disease. Early host immune responses include the activation of B-cell and T-cell (CD4+ and CD8+) lymphocytes that result in the production of anti-trypanosoma antibodies and direct cytotoxicity. It is thought that host immune mechanisms simultaneously contribute to the elimination of the parasite and host tissue damage. The early response causes a state of systemic inflammation reaction that either subsides and resolves or persists as a low-grade silent inflammation and manifests as a chronic disease.[5][6]
Chronic infection
- The true mechanism that result in chronic manifestations of the disease is poorly understood, but it is thought that chronic Chagas disease may be caused by either pathogenic inflammatory responses against residual and persistent T. cruzi pathogens or autoimmune mechanisms.[7][8][9]
- Host immune cells, namely mononuclear cells, play an important role in the chronic host tissue destruction. Other involved immune cells include activated neutrophils and eosinophils.
- Chronic inflammation typically results in end-organ damage by inducing local and diffuse tissue necrosis and fibrosis.
- Denervation is characteristic of Chagas disease, whereby host organs lose sympathethic and parasympathetic nerve endings (neuronolysis) within the walls of infected tissue. The denervation process results in clinical manifestations (e.g. GI hypomotility).[10]
Gross Pathology
- On goss pathology, infected organs, such as the heart, the colon, lymph nodes, or the esophagus, demonstrate the following characteristic features[10]:
- Expansion in size
- Dilation with flabby-appearing tissue
- Tissue congestion and engorgement
- Tissue effacement and aneurysm formation (e.g. left ventricle apical effacement in Chagas cardiomyopathy) typically followed by life-threatening thrombus formation
- Whitish “soldier’s” patches (early) and diffuse fibrosis (late) suggestive of tissue fibrosis in chronic states
Microscopic Pathology
Microscopic histopathological analysis of organs infected with Chagas disease often demonstrate the following characteristic features[10]:
Acute Phase
- Pseudocyst formation in muscle fibers and histiocytes
- Mononuclear and lymphocytic cellular infiltrate
- Host cell lysis (eg. [myocyte]]s, neurons, endothelial cells, brain astrocytes) with or without any evidence of parasite presence (especially in acute phase)
- Evidence of T. cruzi parasite in the cytoplasm of host cells, such as cardiac myocytes or neurons. The parasite typically appear to be adhering to cellular microfilaments.
- Palisading mononuclear cells around meningeal blood vessels (in Virchow-Robin spaces)
Indeterminate Phase
- Low-grade inflammation in host tissue
Chronic Phase
- Evidence of mononuclear and lymphocytic cellular infiltrate and host cell lysis
- Replacement of destroyed tissue by fibrous scars, which typically appear locally then become more diffuse
Chagas heart disease
The pathogenesis of Chagas cardiomyopathy is incompletely understood, it may involve several mechanisms (Hypothesis), including:
- Parasite-dependent myocardial damage,
- Immune-mediated myocardial injury (induced by the parasite itself and by self-antigens)
- Microvascular and neurogenic disturbances.
There are two phases for Chagas heart disease, acute and chronic.
Organ damage can occur as a result of intense parasitaemia and tissue parasitism, with superimposed immune-inflammatory response to the parasite. Although any organ can harbour the parasites, experimental Trypanosoma cruzi infection has a typical predilection for the muscle system in the heart, oesophagus and colon, and for the central nervous system. An in vitro model using human cell lines in culture to observe T. cruzi passage through the vascular barrier showed that there is usually no disruption of the endothelial monolayer, as the parasite uses a special transmigration process that is facilitated by bradykinin and CCL2 chemokine. It is not fully clear though that such phenomenon also occurs in vivo.
Histopathology:
prominent inflammatory changes in the vicinity of ruptured infected cells in tissues from both right and left cardiac chambers
Myocarditis is intense and diffuse with myocyte necrosis, interstitial oedema, vasculitis and capillary dilation, and mononuclear and polymorphonuclear infiltration
The immunological reaction is thought to control the active parasite multiplication through various host innate mechanisms that play a role in detecting and controlling parasite tissue invasion – a powerful reaction involving CD4+ and CD8+ T-cells and B-cells activation that induces direct antitrypanosoma cytotoxicity, cytokine secretion and production of specific antibodies against the parasite. The neuronal depopulation of the Meissner and Auerbach plexuses that occurs in esophageal and colon tissues during the acute phase are a key factor in the pathogenesis of megaoesophagus and megacolon in the chronic phase. Direct damage of smooth muscle may also be a contributory factor, but this hypothesis has not been adequately explored in humans and animal models of Chagas disease.
Chronic Chagas cardiomyopathy:
The pathogenic mechanisms responsible for cardiac lesions developing during the chronic phase of Chagas disease are not completely understood. However, four mechanisms are believed to play a role, neurogenic disturbances, microvascular derangements, parasite-dependent damage, and immune-mediated tissue injury. The first two mechanisms probably play only an ancillary role in the development of the cardiac lesions and clinical complications observed in patients with chronic Chagas cardiomyopathy. By contrast, most investigators now believe that parasite persistence is a critical factor in causing inflammation and in initiating and progressing chronic myocarditis. This concept emphesizes on the notion that chronic Chagas disease is indeed an infectious entity, in which the parasite is not completely eliminated, despite the multiple and proteiform reactions developed by the host systems against it.
Acute form of Chagas Disease: Myocarditis is infrequent, appearing in only 1-5% of patients whose having the acute phase of Chagas Disease (1-5 of every 10,000 infected subjects).
Chronic form of Chagas Disease: The histologic diagnosis of Chronic Chagas cardiomyopathy (CCM) consists of a diffuse and patchy chronic myocarditis, interstitial mononuclear cell infiltrates, and myocardial fiber destruction with fibrotic replacement. Grossly enlarged hearts have been found in autopsy studies in subjects with end stage of Chagas disease. Left ventricular apical aneurysms are also frequently found on autopsy.
The degree of myocardial fibrosis increases progressively from the mildest to the most severe disease stages. Additionally, myocardial fibrosis correlates inversely with left ventricular ejection fraction and clinical status.
Cardiac MRI may demonstrate myocardial involvement (hyperenhancement) among seropositive patients without clinical symptoms or left ventricular wall motion abnormalities.
Across groups A-D, coronary angiography is usually normal or shows minimally obstructive disease.
Case Example: Heart Involvement in Chagas Disease
Clinical Summary
A 12-year-old boy, whose family had recently emigrated from Brazil, presented to the emergency room with a three-day history of malaise, fever, anorexia, and edema of the face and upper extremities.
On physical examination the patient had generalized lymphadenopathy and hepatosplenomegaly.
The patient was tachycardic and dysgenic with signs of congestive heart failure.
A cardiac biopsy was performed which revealed an active myocarditis with leishmanial forms of parasitic organisms within cardiac myocytes.
Close examination of peripheral blood smears revealed occasional circulating trypomastigotes. A complement fixation test for antibodies to Trypanosoma cruzi was strongly positive.
Gallery
-
![Life cycle of Trypanosoma cruzi, the causal agent of American Trypanosomiasis. From Public Health Image Library (PHIL). [11]](https://www.wikidoc.org/images/9/9e/Chagas03.jpeg) Life cycle of Trypanosoma cruzi, the causal agent of American Trypanosomiasis. From Public Health Image Library (PHIL). [11]
Life cycle of Trypanosoma cruzi, the causal agent of American Trypanosomiasis. From Public Health Image Library (PHIL). [11] -
![Trypanosoma cruzi in monkey heart. From Public Health Image Library (PHIL). [11]](https://www.wikidoc.org/images/9/9a/Chagas09.jpeg) Trypanosoma cruzi in monkey heart. From Public Health Image Library (PHIL). [11]
Trypanosoma cruzi in monkey heart. From Public Health Image Library (PHIL). [11]
![Life cycle of Trypanosoma cruzi, the causal agent of American Trypanosomiasis. From Public Health Image Library (PHIL). [11]](https://www.wikidoc.org/index.php/File%3AChagas03.jpeg)
![Trypanosoma cruzi in monkey heart. From Public Health Image Library (PHIL). [11]](https://www.wikidoc.org/index.php/File%3AChagas09.jpeg)
</gallery>
-
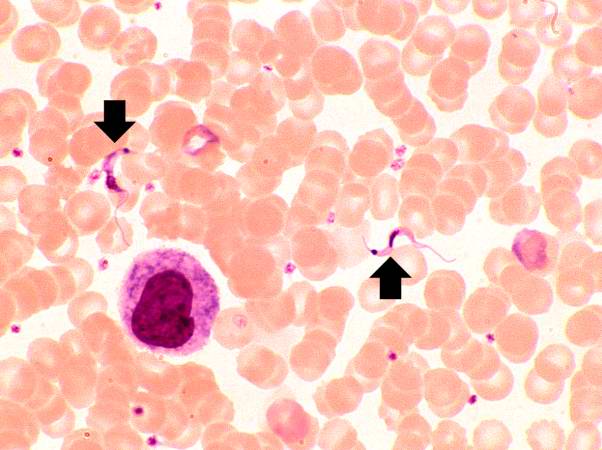 This peripheral blood smear from the patient shows two trypomastigotes of Trypanosoma cruzi.
This peripheral blood smear from the patient shows two trypomastigotes of Trypanosoma cruzi. -
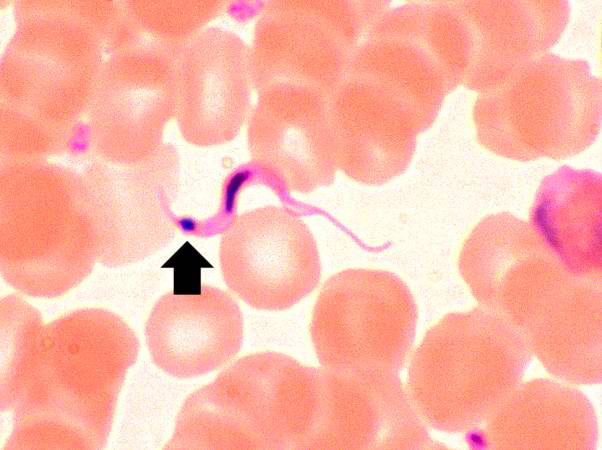 This peripheral blood smear from the patient shows a higher power view of a Trypanosoma cruzi trypomastigote. Note the prominent kinetoplast (arrow).
This peripheral blood smear from the patient shows a higher power view of a Trypanosoma cruzi trypomastigote. Note the prominent kinetoplast (arrow).


-
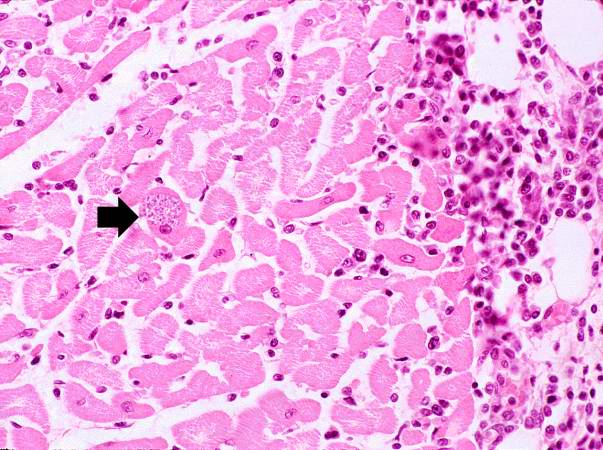 This is a low-power photomicrograph of an H & E stained section from the heart biopsy of this patient. Note the organisms within a myocyte (arrow) and the adjacent inflammatory response.
This is a low-power photomicrograph of an H & E stained section from the heart biopsy of this patient. Note the organisms within a myocyte (arrow) and the adjacent inflammatory response. -
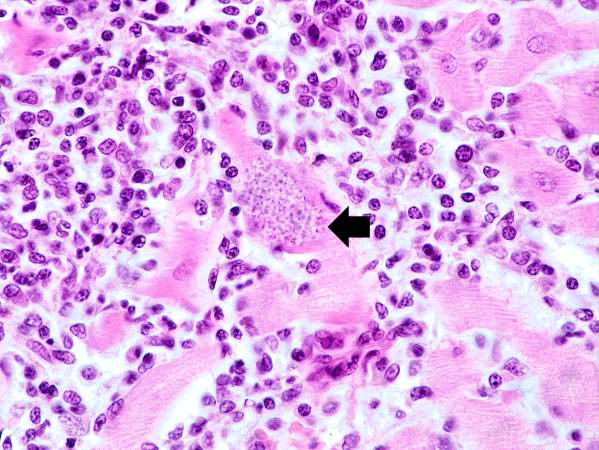 This is a higher-power photomicrograph of an H & E stained heart biopsy from this patient. Again, note the organisms within a myocyte (arrow) and the inflammatory response.
This is a higher-power photomicrograph of an H & E stained heart biopsy from this patient. Again, note the organisms within a myocyte (arrow) and the inflammatory response.


-
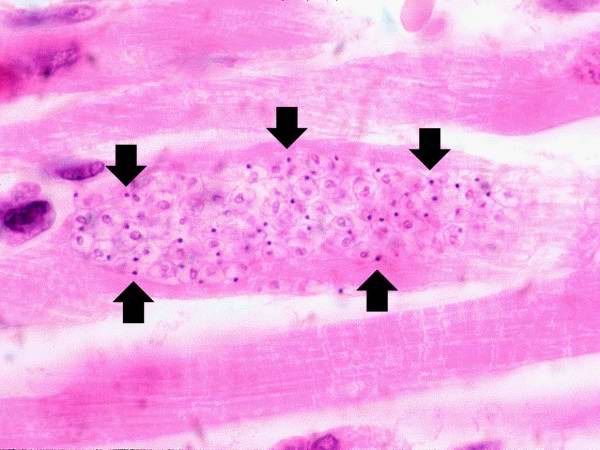
 This is a higher-power photomicrograph of an H & E stained heart biopsy from this patient. At this magnification the organisms within a myocyte (arrows) and the adjacent inflammatory response are more clearly seen. The individual organisms within the myocyte are called amastigotes.
This is a higher-power photomicrograph of an H & E stained heart biopsy from this patient. At this magnification the organisms within a myocyte (arrows) and the adjacent inflammatory response are more clearly seen. The individual organisms within the myocyte are called amastigotes. -
 This is a higher-power photomicrograph of an H & E stained heart biopsy from this patient. Note the T. cruzi amastigotes (arrows) within this longitudinal section of a myocyte.
This is a higher-power photomicrograph of an H & E stained heart biopsy from this patient. Note the T. cruzi amastigotes (arrows) within this longitudinal section of a myocyte.


References
- ↑ Santos Ferreira C, Amato Neto V, Gakiya E, et al. “Microwave treatment of human milk to prevent transmission of Chagas disease.” Rev Inst Med Trop São Paulo. 2003 Jan-Feb;45(1):41-2. PMID 12751321
- ↑ WHO. Chagas. Accessed 24 September 2006.
- ↑ da Silva Valente S, de Costa Valente V, Neto H. “Considerations on the epidemiology and transmission of Chagas disease in the Brazilian Amazon.” Mem Inst Oswaldo Cruz 94 Suppl 1: 395-8. PMID 10677763
- ↑ UK Health Protection Agency (HPA).Chagas’ disease (American trypanosomiasis) in southern Brazil. Accessed 24 September 2006.
- ↑ Coates BM, Sullivan DP, Makanji MY, Du NY, Olson CL, Muller WA; et al. (2013). “Endothelial transmigration by Trypanosoma cruzi”. PLoS One. 8 (12): e81187. doi:10.1371/journal.pone.0081187. PMC 3846899. PMID 24312535.
- ↑ Tarleton RL, Koller BH, Latour A, Postan M (1992). “Susceptibility of beta 2-microglobulin-deficient mice to Trypanosoma cruzi infection”. Nature. 356 (6367): 338–40. doi:10.1038/356338a0. PMID 1549177.
- ↑ Kalil J, Cunha-Neto E (1996). “Autoimmunity in chagas disease cardiomyopathy: Fulfilling the criteria at last?”. Parasitol Today. 12 (10): 396–9. PMID 15275290.
- ↑ Tarleton RL (2001). “Parasite persistence in the aetiology of Chagas disease”. Int J Parasitol. 31 (5–6): 550–4. PMID 11334941.
- ↑ Kierszenbaum F (1999). “Chagas’ disease and the autoimmunity hypothesis”. Clin Microbiol Rev. 12 (2): 210–23. PMC 88915. PMID 10194457.
- ↑ 10.0 10.1 10.2 Teixeira AR, Nitz N, Guimaro MC, Gomes C, Santos-Buch CA (2006). “Chagas disease”. Postgrad Med J. 82 (974): 788–98. doi:10.1136/pgmj.2006.047357. PMC 2653922. PMID 17148699.
- ↑ 11.0 11.1 “Public Health Image Library (PHIL)”.
Causes
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Yazan Daaboul, M.D.
Overview
Chagas disease (American tryponosomiasis) is a human tropical parasitic disease usually caused by Trypanosoma cruzi, a flagellate protozoa.
Causes
Etiologic Agent
- Chagas disease (American trypanosomiasis) is a human tropical parasitic disease usually caused by Trypanosoma cruzi, a flagellate protozoa.
Transmission
- Chagas disease usually has a vector-borne transmission. Triatomine insects, the Riduvid (kissing/assassin) bugs, suck blood from an infected individual and are subsequently infected themselves.
- The insects carry the pathogen in their feces and urine. Human infection with T. cruzi occurs following exposure to feces/urine of infected insects. The pathogen typically enters the host either through a wound induced by the host’s scratching following the insect bite or through the conjunctival mucus membranes.
- Triatomine insects may also be referred to as benchuca, vinchuca, kissing bug, chipo, chupança and barbeiro. Other insect species that may be vectors for T. cruzi are insects of the families Rhodnius and Panstrongylus
- Other modes of transmission include organ transplantation, blood transfusions, vertical transmission, breast milk, and oral transmission following ingestion of infected foods.[1][2][3][4]
Life Cycle
The following figure illustrates the life cycle of T. cruzi, the causative pathogen of Chagas disease.
Gallery
-
![Triatoma infestans or the “Kissing Bug”, “Assassin Bug”, or “Cone-Nose Bug”, is a vector for Chagas' Disease. From Public Health Image Library (PHIL). [5]](https://www.wikidoc.org/images/6/68/Chagas06.jpeg) Triatoma infestans or the “Kissing Bug”, “Assassin Bug”, or “Cone-Nose Bug”, is a vector for Chagas’ Disease. From Public Health Image Library (PHIL). [5]
Triatoma infestans or the “Kissing Bug”, “Assassin Bug”, or “Cone-Nose Bug”, is a vector for Chagas’ Disease. From Public Health Image Library (PHIL). [5] -
![Dorsal view of the “kissing bug”, Triatoma infestans, a vector for Chagas disease. From Public Health Image Library (PHIL). [5]](https://www.wikidoc.org/images/3/3c/Chagas02.jpeg) Dorsal view of the “kissing bug”, Triatoma infestans, a vector for Chagas disease. From Public Health Image Library (PHIL). [5]
Dorsal view of the “kissing bug”, Triatoma infestans, a vector for Chagas disease. From Public Health Image Library (PHIL). [5] -
![Dorsal view of the Eastern bloodsucking conenose, or the Mexican bed bug, Triatoma sanguisuga. From Public Health Image Library (PHIL). [5]](https://www.wikidoc.org/images/0/0d/Chagas01.jpeg) Dorsal view of the Eastern bloodsucking conenose, or the Mexican bed bug, Triatoma sanguisuga. From Public Health Image Library (PHIL). [5]
Dorsal view of the Eastern bloodsucking conenose, or the Mexican bed bug, Triatoma sanguisuga. From Public Health Image Library (PHIL). [5]
![Triatoma infestans or the “Kissing Bug”, “Assassin Bug”, or “Cone-Nose Bug”, is a vector for Chagas' Disease. From Public Health Image Library (PHIL). [5]](https://www.wikidoc.org/index.php/File%3AChagas06.jpeg)
![Dorsal view of the “kissing bug”, Triatoma infestans, a vector for Chagas disease. From Public Health Image Library (PHIL). [5]](https://www.wikidoc.org/index.php/File%3AChagas02.jpeg)
![Dorsal view of the Eastern bloodsucking conenose, or the Mexican bed bug, Triatoma sanguisuga. From Public Health Image Library (PHIL). [5]](https://www.wikidoc.org/index.php/File%3AChagas01.jpeg)
References
- ↑ Santos Ferreira C, Amato Neto V, Gakiya E, et al. “Microwave treatment of human milk to prevent transmission of Chagas disease.” Rev Inst Med Trop São Paulo. 2003 Jan-Feb;45(1):41-2. PMID 12751321
- ↑ WHO. Chagas. Accessed 24 September 2006.
- ↑ da Silva Valente S, de Costa Valente V, Neto H. “Considerations on the epidemiology and transmission of Chagas disease in the Brazilian Amazon.” Mem Inst Oswaldo Cruz 94 Suppl 1: 395-8. PMID 10677763
- ↑ UK Health Protection Agency (HPA).Chagas’ disease (American trypanosomiasis) in southern Brazil. Accessed 24 September 2006.
- ↑ 5.0 5.1 5.2 “Public Health Image Library (PHIL)”.
Differentiating Chagas disease from other Diseases
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Raviteja Guddeti, M.B.B.S. [2]
Overview
Chagas disease must be differentiated from other diseases the cause cardiomyopathy, hepatosplenomegaly, or esophageal/colonic dysfunction, such as electrophysiological cardiac diseases, GI hypomotility disorders, and malignancies.
Differentiating Chagas disease from other Diseases
Chagas disease is more common among immunocompromised patients who are at high risk for other fungal, bacterial, and viral infections. It should be differentiated from the following diseases:
| Disease | Differentiating signs and symptoms | Differentiating tests |
|---|---|---|
| CNS lymphoma[1] |
|
|
| Disseminated tuberculosis[2] |
|
|
| Aspergillosis[3] |
|
|
| Cryptococcosis |
|
|
| Chagas disease[4] |
|
|
| CMV infection[5] |
|
|
| HSV infection[6] |
|
|
| Varicella Zoster infection[7] |
|
|
| Brain abscess[8][9] |
|
|
| Progressive multifocal leukoencephalopathy[10] |
|
Chagas disease should also be differentiated from the following diseases:
- Achalasia
- Atrioventricular Block
- Cardiomyopathy, Dilated
- Cardiomyopathy, Hypertrophic
- Colonic obstruction
- Constipation
- Encephalopathy, Hypertensive
- Esophageal Cancer
- Esophageal motility disorders
- Esophageal rupture
- Esophageal spasm
- Esophagitis
- Gastroesophageal reflux disease
- Megacolon
- Myocardial infarction
- Myocardial ischemia
- Myocarditis
- Pulmonary edema, cardiogenic
- Pulmonary embolism
- Sinus node dysfunction
- Splenomegaly
- Sudden cardiac death
- Toxoplasmosis
References
- ↑ Gerstner ER, Batchelor TT (2010). “Primary central nervous system lymphoma”. Arch. Neurol. 67 (3): 291–7. doi:10.1001/archneurol.2010.3. PMID 20212226.
- ↑ von Reyn CF, Kimambo S, Mtei L, Arbeit RD, Maro I, Bakari M, Matee M, Lahey T, Adams LV, Black W, Mackenzie T, Lyimo J, Tvaroha S, Waddell R, Kreiswirth B, Horsburgh CR, Pallangyo K (2011). “Disseminated tuberculosis in human immunodeficiency virus infection: ineffective immunity, polyclonal disease and high mortality”. Int. J. Tuberc. Lung Dis. 15 (8): 1087–92. doi:10.5588/ijtld.10.0517. PMID 21740673.
- ↑ Latgé JP (1999). “Aspergillus fumigatus and aspergillosis”. Clin. Microbiol. Rev. 12 (2): 310–50. PMC 88920. PMID 10194462.
- ↑ Rassi A, Rassi A, Marin-Neto JA (2010). “Chagas disease”. Lancet. 375 (9723): 1388–402. doi:10.1016/S0140-6736(10)60061-X. PMID 20399979.
- ↑ Emery VC (2001). “Investigation of CMV disease in immunocompromised patients”. J. Clin. Pathol. 54 (2): 84–8. PMC 1731357. PMID 11215290.
- ↑ Bustamante CI, Wade JC (1991). “Herpes simplex virus infection in the immunocompromised cancer patient”. J. Clin. Oncol. 9 (10): 1903–15. doi:10.1200/JCO.1991.9.10.1903. PMID 1919640.
- ↑ Hambleton S (2005). “Chickenpox”. Curr. Opin. Infect. Dis. 18 (3): 235–40. PMID 15864101.
- ↑ Alvis Miranda H, Castellar-Leones SM, Elzain MA, Moscote-Salazar LR (2013). “Brain abscess: Current management”. J Neurosci Rural Pract. 4 (Suppl 1): S67–81. doi:10.4103/0976-3147.116472. PMC 3808066. PMID 24174804.
- ↑ Patel K, Clifford DB (2014). “Bacterial brain abscess”. Neurohospitalist. 4 (4): 196–204. doi:10.1177/1941874414540684. PMC 4212419. PMID 25360205.
- ↑ Tan CS, Koralnik IJ (2010). “Progressive multifocal leukoencephalopathy and other disorders caused by JC virus: clinical features and pathogenesis”. Lancet Neurol. 9 (4): 425–37. doi:10.1016/S1474-4422(10)70040-5. PMC 2880524. PMID 20298966.
Epidemiology and Demographics
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Raviteja Guddeti, M.B.B.S. [2]
Overview
The global incidence of Chagas disease is estimated to be 5-8 million with global incidence of Chagas disease of approxiamtely 100-400 per 100,000 individuals. The majority of cases are reported in South America, where Chagas disease is considered the most common parasitic infection. Individuals of all age groups may acquire Chagas disease, including neonates due to risk of vertical transmission. Elderly patients often demonstrate clinical manifestations of chronic Chagas disease. Although there is no evidence that suggests racial predilection to the acquisition of the disease, the majority of cases are reported among individuals of Hispanic origin due to the endemicity of the disease in South America. The majority of cases outside South America are among South American immigrants. Myocarditis is infrequent, appearing in only 1-5% of patients whose having the acute phase of Chagas Disease (1-5 of every 10,000 infected subjects).
Epidemiology and Demographics
Incidence
The global incidence of Chagas disease is estimated to be 100-400 per 100,000 individuals.[1][2][3]
Prevalence
- The estimated global prevalence of Chagas disease is estimated to be 5-8 million.[1][2][3]
- The prevalence of Chagas disease is thought to be declining following the introduction of effective infection control methods, including use of insecticides and T. cruzi serology screening in blood banks in endemic countries.
Age
- There is no age predominance for Chagas disease primary infection.
- The rate of Chagas disease is high among neonates due to risk of vertical transmission during pregnancy.
- Clinical manifestations of Chagas disease are common among elderly patients due to the natural history of the chronic disease state, whereby clinical manifestations develop several years following primary infection.
Gender
- There is no gender predominance for infection with Chagas disease.
- Male gender is thought to be associated with worse prognosis than female gender.
Race
- Given the endemicity of the disease in South America, the majority of individuals with Chagas disease are of Hispanic origin.
- However, there is no evidence to demonstrate that there is any racial predilection to the acquisition of the infection.
Developing Countries
- Chagas disease is a common parasitic infections worldwide.
- It is endemic in South America and is considered the single most common parasitic infection in that South American region.
- Chagas disease is rarely acquired locally in other parts of the world.
Developed Countries
- In USA, the prevalence of Chagas disease is approximately 300,000. The majority of those cases are among South American immigrants.[4]
- Chagas disease is rarely acquired locally in either USA or Europe.
References
- ↑ 1.0 1.1 Nouvellet P, Dumonteil E, Gourbière S (2013). “The improbable transmission of Trypanosoma cruzi to human: the missing link in the dynamics and control of Chagas disease”. PLoS Negl Trop Dis. 7 (11): e2505. doi:10.1371/journal.pntd.0002505. PMC 3820721. PMID 24244766.
- ↑ 2.0 2.1 Feliciangeli MD, Campbell-Lendrum D, Martinez C, Gonzalez D, Coleman P, Davies C (2003). “Chagas disease control in Venezuela: lessons for the Andean region and beyond”. Trends Parasitol. 19 (1): 44–9. PMID 12488226.
- ↑ 3.0 3.1 Samuels AM, Clark EH, Galdos-Cardenas G, Wiegand RE, Ferrufino L, Menacho S; et al. (2013). “Epidemiology of and impact of insecticide spraying on Chagas disease in communities in the Bolivian Chaco”. PLoS Negl Trop Dis. 7 (8): e2358. doi:10.1371/journal.pntd.0002358. PMC 3731239. PMID 23936581.
- ↑ Bern C, Montgomery SP (2009). “An estimate of the burden of Chagas disease in the United States”. Clin Infect Dis. 49 (5): e52–4. doi:10.1086/605091. PMID 19640226.
Risk Factors
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Yazan Daaboul, M.D.
Overview
Risk factors for Chagas disease include residence in Central or South America, living in old houses with either mud and sticks wall constructions or straw roofs, ingestion of contaminated water, or receiving blood transfusions / organ donation from individuals in regions with high endemicity. Neonatal risk is highest among those who breastfeed from bleeding / cracked nipples of infected mothers and those who are delivered from seropositive mothers with active disease.
Risk Factors
Risk factors for Chagas disease include:[1]
- Living in Central or South America
- Residing in a house constructed before the year 2000
- Exposure to either wall constructions composed of mud and sticks or straw roofs
- Ingestion of contaminated water
- Living in a hut where reduvid bugs live in the walls
- Poverty
- Receiving either a blood transfusion or organ transplant from a person in regions with high endemicity
- Maternal seropositivity and exacerbation of infection during pregnancy (risk of vertical transmission and development of congenital Chagas disease)
- Bleeding/cracked nipples of infected mother during breastfeeding
- Immunosuppression
References
- ↑ Bern C, Kjos S, Yabsley MJ, Montgomery SP (2011). “Trypanosoma cruzi and Chagas’ Disease in the United States”. Clin Microbiol Rev. 24 (4): 655–81. doi:10.1128/CMR.00005-11. PMC 3194829. PMID 21976603.
Natural History, Complications and Prognosis
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]
Overview
The incubation period of T. cruzi is 1-2 weeks following transmission. The majority (90%-95%) of infected individuals remain asymptomatic in the acute phase following Chagas disease infection. Nonetheless, patients typically remain chronically infected and demonstrate clinical manifestations several years/decades following infection. Approximately 1/3 of patients develop manifestations of the chronic Chagas disease, namely cardiac conduction system dysfunction, GI denervation with esophageal and/or colonic dysfunction (megaesophagus and megacolon). Chagas cardiomyopathy is the most common chronic manifestation of the disease and accounts for approximately 80-90% of chronic manifestations. The majority of patients with Chagas cardiomyopathy die within 2 years of symptom onset.
Natural History
Acute Phase
- The incubation period of T. cruzi is 1-2 weeks following transmission. Nonetheless, the majority (90%-95%) of infected individuals remain asymptomatic in the acute phase following Chagas disease infection.[1][2]
- Some individuals may experience mild and non-specific clinical manifestations, such as fever, anorexia, and fatigue. These symptoms usually self-resolve within 4-8 weeks.[1]
- Rarely, the acute phase of Chagas disease is life-threatening, and patients may present with either myocarditis of meningoencephalitis that require hospitalization.[1]
Asymptomatic (Indeterminate) Chronic Phase
- The majority of patients are asymptomatic during the acute phase but remain chronically infected.[3]
- Early during the chronic state, patients are asymptomatic.
Symptomatic Chronic Phase
- Several years/decades following the initial acute phase, approximately 1/3 of patients develop manifestations of the chronic Chagas disease, namely cardiac conduction system dysfunction, GI denervation with esophageal and/or colonic dysfunction (megaesophagus and megacolon).[2]
- Chagas cardiomyopathy is the most common chronic manifestation of the disease and accounts for approximately 80-90% of chronic manifestations. It is highly arrhythmogenic and often manifests with right bundle branch block, AV block, tachyarrhythmia/bradyarrhythmia. Patients typically progress to congestive heart failure and may develop thromboembolic events due to thrombus formation (often due to either dilation of the left ventricle or aneurysm formation). The majority of patients with Chagas cardiomyopathy die within 6 months – 2 years of onset of cardiac symptoms.[3]
- Less commonly (10-20%), patients develop GI manifestations of chronic Chagas disease. Early esophageal Chagas disease often manifests with dysphagia, odynophagia, cough, reflux, and regurgitation. As the disease progresses, individuals experience significant weight loss and aspiration. Similarly, patients with colonic Chagas disease usually complain of constipation early in the disease that often progresses to development of fecaloma, volvolus, and ischemic bowel disease.[3]
Complications
Complications of Chagas disease include:[2][3][1]
- Myocarditis
- Tachyarrhythmia
- Bradyarrhythmia
- AV block
- RBBB
- Apical aneurysm
- Congestive heart failure
- Meningoencephalitis
- Thromboembolism
- Sudden death
- Esophagitis
- Esophageal cancer
- Fecaloma
- Volvulus of sigmoid colon
- Ischemic bowel disease
- Aspiration pneumonia
Prognosis
- Approximately 1/3 of chronically infected patients develop clinical manifestations of chronic Chagas disease.
- Development of cardiac symptoms is a poor prognostic factor. The majority of patients die within 6 months to 2 years following onset of cardiac symptoms.
- Patients with HIV are at an increased rate of developing complications, even during the early phase of Chagas disease. HIV-positivity is associated with increased risk of Chagas myocarditis and meningoencephalitis.
- The following Chagas disease prognosis index estimates the 10-year risk of Chagas disease-related mortality:[4]. Based on data from approximately 500 patients, this index incorporates individual information from the clinical aspects, X-ray findings, EKG, echocardiography and Holter.
| Clinical Feature | Points |
|---|---|
| NYHA class III or IV | 5 |
| Cardiomegaly | 5 |
| Wall motion abnormalities | 3 |
| Non-sustained ventricular tachycardia | 3 |
| Low voltage on ECG | 2 |
| Male gender | 2 |
| Total Points | 10-year Risk of Chagas Disease-related Mortality |
|---|---|
| 0–6 | 10% |
| 7–11 | 40% |
| 12–20 | 85% |
References
- ↑ 1.0 1.1 1.2 1.3 Bern C (2015). “Chagas’ Disease”. N Engl J Med. 373 (5): 456–66. doi:10.1056/NEJMra1410150. PMID 26222561.
- ↑ 2.0 2.1 2.2 Teixeira AR, Nitz N, Guimaro MC, Gomes C, Santos-Buch CA (2006). “Chagas disease”. Postgrad Med J. 82 (974): 788–98. doi:10.1136/pgmj.2006.047357. PMC 2653922. PMID 17148699.
- ↑ 3.0 3.1 3.2 3.3 Prata A (1994). “Chagas’ disease”. Infect Dis Clin North Am. 8 (1): 61–76. PMID 8021449.
- ↑ Rassi A Jr, Rassi A, Little W, Xavier S, Rassi S, Rassi A, Rassi G, Hasslocher-Moreno A, Sousa A, Scanavacca M (2006). “Development and validation of a risk score for predicting death in Chagas’ heart disease”. N Engl J Med. 355 (8): 799–808. PMID 16928995.
Diagnosis
Diagnostic Criteria | History and Symptoms | Physical Examination | Laboratory findings | Electrocardiogram | X-ray | Electrocardiogram | Echocardiography and Ultrasound | CT scan | MRI | Other Imaging Findings | Other diagnostic studies
To go back to the main page, click here.
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]Sumanth Khadke, MD[2]
Overview
In general, diagnosis (plural diagnoses) has two distinct dictionary definitions. The first definition is “the recognition of a disease or condition by its outward signs and symptoms”, while the second definition is “the analysis of the underlying physiological/biochemical cause(s) of a disease or condition”.
Diagnosis covers a broad spectrum, or spectra, of testing in some form of analysis; collective reasoning using such tests is called the method of diagnostics, leading then to the results of those tests by ideal (ethics) would then be considered a diagnosis, but not necessarily the correct one.
In medicine, diagnosis or diagnostics is the process of identifying a medical condition or disease by its signs, symptoms, and from the results of various diagnostic procedures. The conclusion reached through this process is called a diagnosis. The term “diagnostic criteria” designates the combination of symptoms which allows the doctor to ascertain the diagnosis of the respective disease.
Typically, someone with abnormal symptoms will consult a physician, who will then obtain a history of the patient‘s illness and examine him for signs of disease. The physician will formulate a hypothesis of likely diagnoses and in many cases will obtain further testing to confirm or clarify the diagnosis before providing treatment.
Medical tests commonly performed are measuring blood pressure, checking the pulse rate, listening to the heart with a stethoscope, urine tests, fecal tests, saliva tests, blood tests, medical imaging, electrocardiogram, hydrogen breath test and occasionally biopsy.
The word diagnosis is derived from the Greek words dia which means “by”, and gnosis which means “knowledge”. The verb is diagnose and a person diagnosing could be considered a diagnostician.
Relationship of diagnosis to medical practice
A physician‘s job is to know the human body and its functions in terms of normality (homeostasis). The four cornerstones of diagnostic medicine, each essential for understanding homeostasis, are: anatomy (the structure of the human body), physiology (how the body works), pathology (what can go wrong with the anatomy and physiology) and psychology (thought and behavior). Once the doctor knows what is normal and can measure the patient’s current condition against those norms, she or he can then determine the patient’s particular departure from homeostasis and the degree of departure. This is called the diagnosis. Once a diagnosis has been reached, the doctor is able to propose a management plan, which will include treatment as well as plans for follow-up. From this point on, in addition to treating the patient’s condition, the doctor educates the patient about the causes, progression, outcomes, and possible treatments of his ailments, as well as providing advice for maintaining health.
It should be noted however, that medical diagnosis in psychology or psychiatry is problematic. Apart from the fact that there are differing theoretical views toward mental conditions and that there are few “lab” tests available for various major disorders (e.g., clinical depression), a causal analysis with respect to symptomatology and disorder/disease is not always possible. As a result, most if not all mental conditions, function as both symptoms as well as disorders. There are often functional descriptions provided for psychological disorders and these are vulnerable to circular reasoning due to the etiological fuzziness inherent of these diagnostic categories. (BDG, 2006)
Diagnostic procedure
Diagnosis is a fluid process in which the physician responds to information garnered from the patient and others, from a physical examination of the patient, and from medical tests performed upon the patient.
The doctor should consider the patient in his ‘well’ context rather than simply as a walking medical condition. This entails assessing the socio-political context of the patient (family, work, stress, beliefs), in addition to the patient’s physical body, as this often offers vital clues to the patient’s condition and its management.
The process of diagnosis begins when the patient consults the doctor and presents a set of complaints (the symptoms). If the patient is unconscious, this condition is the de facto complaint. The doctor then obtains further information from the patient himself (and from those who know him, if present) about the patient’s symptoms, his previous state of health, living conditions, and so forth.
Rather than consider the myriad diseases that could afflict the patient, the physician narrows down the possibilities to the illnesses likely to account for the apparent symptoms, making a list of only those conditions that could account for what is wrong with the patient. These are generally ranked in order of probability.
The doctor then conducts a physical examination of the patient, studies the patient’s medical record, and asks further questions as he goes, in an effort to rule out as many of the potential conditions as possible. When the list is narrowed down to a single condition, this is called the differential diagnosis, and provides the basis for a hypothesis of what is ailing the patient.
Unless the physician is certain of the condition present, further medical tests are performed or scheduled (such as medical imaging), in part to confirm or disprove the diagnosis but also to document the patient’s status to keep the patient’s medical history up to date. Consultations with other physicians and specialists in the field may be sought. If unexpected findings are made during this process, the initial hypothesis may be ruled out and the physician must then consider other hypotheses.
Despite all of these complexities, most patient consultations are relatively brief, because many diseases are obvious, or the physician’s experience may enable him to recognize the condition quickly. Another factor is that the decision trees used for most diagnostic hypothesis testing are relatively short.
Once the physician has completed the diagnosis, he explains the prognosis to the patient and proposes a treatment plan which includes therapy and follow-up (further consultations and tests to monitor the condition and the progress of the treatment, if needed), usually according to the guideline provided by the medical field on the treatment of the particular illness.
Treatment itself may indicate a need for review of the diagnosis if there is a failure to respond to treatments that would normally work.
History of medical diagnostics
The history of medical diagnosis began in earnest from the enlightened days of Hippocrates in ancient Greece but is far from perfect despite the enormous bounty of information made available by medical research including the sequencing of the human genome. The practice of diagnosis continues to be dominated by theories set down in the early 1900s.
Ancient Greece
Over two thousand years ago, Hippocrates recorded the association between disease and heredity. In similar fashion, Pythagoras noted the association between metabolism and heredity (allergy to Fava beans). The medical community, however, has only recently acknowledged the importance of genetics and its relevance to mainstream medicine.
The Oslerian ideal
The ideals of William Osler who transformed the practice of medicine in the early 1900s were based on the principles of the diagnosis and treatment of disease. According to Osler, the functions of a physician were to be able to identify disease and its manifestations, understand its mechanisms, how it may be prevented and how it may be cured. For his medical students he believed that the best textbook was the patient himself – analysis of morbid anatomy and pathology were the keys. The Oslerian ideal continues today, as the basis of the Doctor’s strategy is, “What disease does this patient have and what is the best way for treatment?” The emphasis is on the classification of the disease in order to use the remedies available for its effects to be reversed or ameliorated. The human being in question is representative of a class of people with this type of disease whereas the biological individuality of this person is not given any great weight.
Garrod’s view
The successor to William Osler as Regius Professor at Oxford was Archibald Garrod. Garrod echoed the observations of his Greek counterparts of two millennia ago, …our chemical individualities are due to our chemical merits as well as our chemical shortcomings; and it is more nearly true to say that the factors which confer upon us our predispositions to and immunities from various mishaps which are spoken of as diseases, are inherent in our very chemical structure; and even in the molecular groupings which confer upon us our individualities, and which went into the making of the chromosomes from which we sprang. Considering that the time that he formulated these ideas were the early 1900’s, and the knowledge of DNA encoding genes that in turn encoded proteins responsible for bodily structure and functions not being discovered until some fifty years later it took some time before medicine could fully appreciate the fundamental importance of his concept of diagnosis.
Present-day Oslerian practice
Whereas Osler laid the founding principles by which medicine should be practiced, Garrod placed these principles in a greater context of a chemical individuality that is inherited and is subject to the mechanisms of evolutionary selection. The Oslerian ideal of medical practice continues to dominate medical philosophy today. The patient is a collective of symptoms to be characterized and analyzed algorithmically in order to draw a diagnosis and subsequently produce a strategy of treatment. Medicine is about problems based solutions. In keeping with this philosophy, today’s pathology reports provide a momentary snapshot of the patient’s biochemical profile, highlighting the end result of the disease process.
Influence of DNA technology
Garrod’s conception of biological individuality was confirmed with the advent of the sequencing of the human genome. Finally the subtle relationship between inheritance, individuality and environment became apparent via the variations detected in DNA. In each patient’s DNA lies a script for how their bodies will change and become ill as well as how they will handle the assaults of the environment from the beginning of their life to its end. It is hoped that by knowing a patient’s genes that the biological strengths and weaknesses in respect to these assaults will be revealed and disease processes can be predicted before they have the opportunity to manifest. Although knowledge in this area is far from complete, there are already medical interventions based on this. More importantly, the physician, forewarned with this knowledge can guide the patient towards appropriate lifestyle changes to anticipate and mitigate disease processes.
See also
Lists
External links
- GPnotebook web site GPnotebook is a British medical database for GPs that provides an immediate reference resource for clinicians worldwide. The database consists of over 30,000 pages of information.
- Free 24/7 DRG & ICD-9-CM lookup powered by Flash Code at icd9coding.com
- Differential Diagnosis
- Merck Manual of Diagnosis and Therapy
als:Diagnostik bg:Диагноза de:Diagnose eu:Diagnostiko it:Diagnosi he:אבחנה ms:Diagnosis nl:Diagnose no:Diagnose nn:Diagnose simple:Diagnosis sk:Diagnóza sr:Дијагностика sh:Dijagnoza fi:Lääketieteellinen diagnoosi sv:Diagnostik ta:அறுதியிடல்
Treatment
Medical Therapy | Surgery | Primary Prevention | Secondary Prevention | Cost-Effectiveness of Therapy | Future or Investigational Therapies
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]Sumanth Khadke, MD[2], Ogechukwu Hannah Nnabude, MD
Overview
Compliance with avoidance is important. The key to avoidance is proper evaluation and detection of causative allergen. Wear appropriate clothing to protect against irritants at home and in a work environment. [1] [2]
Treatment
High-potency topical corticosteroids, e.g. clobetasol propionate 0.05% cream, may be used to reduce the inflammation. [3] As a general rule, high-potency corticosteroids should not be used on thin skin, e.g. face, genitals, intertriginous areas, to avoid the risk of skin atrophy. Antihistamines such as hydroxyzine and cetirizine are recommended to control pruritus. Systemic steroids are advised in severe cases but should be tapered gradually to prevent recurrences. Friction should be avoided as well as the use of soaps, perfumes, and dyes. Emollients are used for hydrating the skin. Tacrolimus ointment and pimecrolimus cream are immunomodulating drugs that inhibit calcineurin and are helpful in allergic contact dermatitis.
Reference
- ↑ Soltanipoor M, Kezic S, Sluiter JK, de Wit F, Bosma AL, van Asperen R; et al. (2019). “Effectiveness of a skin care programme for the prevention of contact dermatitis in healthcare workers (the Healthy Hands Project): A single-centre, cluster randomized controlled trial”. Contact Dermatitis. 80 (6): 365–373. doi:10.1111/cod.13214. PMC 6593800 Check
|pmc=value (help). PMID 30652317. - ↑ Nedorost S (2018). “A diagnostic checklist for generalized dermatitis”. Clin Cosmet Investig Dermatol. 11: 545–549. doi:10.2147/CCID.S185357. PMC 6217130. PMID 30464569.
- ↑ Vernon HJ, Olsen EA (1990). “A controlled trial of clobetasol propionate ointment 0.05% in the treatment of experimentally induced Rhus dermatitis”. J Am Acad Dermatol. 23 (5 Pt 1): 829–32. doi:10.1016/0190-9622(90)70297-u. PMID 2147698.
Looking for the patient version?
© 2026 MyEClinic – IFTM Institut für Telematik in der Medizin GmbH