
Epididymoorchitis
For patient information click here Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Dima Nimri, M.D. [2]
Overview
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Dima Nimri, M.D. [2]
Overview
Epididymoorchitis refers to the inflammation of the epididymis and/or testes, with or without infection. It is a major cause of acute scrotum and must be differentiated from other common causes, such as testicular torsion and torsion of the testicular appendage. While the pathogenesis is not fully understood, infectious epididymoorchitis is thought to be due to retrograde reflux of infected urine into the epididymis, which then spreads to the testes. The causes of epididymoorchitis can be divided into idiopathic, infectious and non-infectious causes. Most common cases are due to infectious causes, which are mostly due to N. gonorrhea, C. trachomatis and E. Coli. Data on epidemiology of epididymoorchitis is scarce, however, epididymoorchitis is the 5th most common genitourinary diagnosis made and disease is more prevalent among U.S. military men. Peak incidence of the disease is in men between the ages of 20 to 29 years. The main symptoms of epididymoorchitis are scrotal pain and swelling. Other symptoms such as fever, nausea, vomiting and lower UTI symptoms may be present. The main focus of physical examination in patients with epididymoorchitis is scrotal and testicular examination. Signs that may be present include testicular swelling, tenderness on palpation, as well as erythema. Other signs include relief of pain upon elevation of the testis. Unlike patients with testicular torsion, patients with epididymoorchitis have an intact cremasteric reflex. A color Doppler ultrasound is mainly done to rule out testicular torsion and is the diagnostic imaging of choice in evaluating cases of acute scrotum. Epididymoorchitis might show a thickened epididymis with normal to increased Doppler wave pulsations, consistent with normal to increased blood flow. Management of epididymoorchitis consists mainly of conservative measures, including bed rest and limitation of physical activity, use of cold packs, analgesia and non-steroidal anti-inflammatory drugs (NSAIDs). In addition, appropriate antibiotic therapy should be initiated if the cause of epididymoorchitis is bacterial.
Historical Perspective
Cases of epididymoorchitis were described in literature as early as 1841.[1] It was believed that epididymitis was caused by chemical irritation caused by urine reflux. However, by 1979, a study showed that bacteria were responsible for more cases.[2]
Classification
Epididymoorchitis can be classified based on the extent of involvement into isolated cases of epididymitis, isolated cases of orchitis or cases of epididymoorchitis. Another means of classifying the disease is based on duration into acute or chronic epididymoorchitis. Finally, it can also be classified according to the causative agent into infectious, non-infectious and idiopathic causes.[2][3]
Pathophysiology
Epididymoorchitis refers to the inflammation of the epididymis and/or testes, with or without infection. While the pathogenesis is not fully understood, infectious epididymoorchitis is thought to be due to retrograde reflux of infected urine into the epididymis, which then spreads to the testes.[2][3]
Causes
The causes of epididymoorchitis can be divided into idiopathic, infectious and non-infectious causes.[4][3]
Differentiating Epididymoorchitis from other Diseases
Epididymoorchitis is a major cause of acute scrotum. Other causes of acute scrotum which must be differentiated from epididymoorchitis include testicular torsion and torsion of the testicular appendage.[2][5][4][6]
Epidemiology and Demographics
Data on epidemiology of epididymoorchitis is scarce, however, epididymoorchitis is the 5th most common genitourinary diagnosis made and disease is more prevalent among U.S. military men. Peak incidence of the disease is in men between the ages of 20 to 29 years.[4]
Risk Factors
Risk factors for epididymoorchitis include sexual activity and sexually transmitted diseases, surgery or instrumentation of the bladder, as well as anatomic abnormalities of the urinary tract and obstruction to the normal flow of urine.[2]
Screening
There are no screening recommendations for epididymoorchitis.[7]
Natural History, Complications and Prognosis
The prognosis of epididymoorchitis is usually excellent, with the majority of cases resolving within 30 days of initiation of medical therapy. However, some cases can progress to chronic epididymoorchitis. Other complications of epididymoorchitis include abscess formation, testicular infarction, sepsis and infertility.
History and Symptoms
The main symptoms of epididymoorchitis are scrotal pain and swelling. Other symptoms such as fever, nausea, vomiting and lower UTI symptoms may be present.[2][8][5][4]
Physical Examination
The main focus of physical examination in patients with epididymoorchitis is scrotal and testicular examination. Signs that may be present include testicular swelling, tenderness on palpation, as well as erythema. Other signs include relief of pain upon elevation of the testis. Unlike patients with testicular torsion, patients with epididymoorchitis have an intact cremasteric reflex.
Laboratory Findings
In patients with epididymoorchitis, laboratory investigations include a urinalysis, urine culture, as well as urethral Gram stain and PCR testing for N. gonorrhea and C. trachomatis.
There are no x-ray findings associated with epididymoorchitis.
Imaging studies, such as CT scan, are usually not done in the case of epididymoorchitis. The diagnostic modality of choice is a scrotal ultrasound.
Imaging studies, such as MRI, are usually not done in the case of epididymoorchitis. The diagnostic modality of choice is a scrotal ultrasound.
A color Doppler ultrasound is mainly done to rule out testicular torsion[3] and is the diagnostic imaging of choice in evaluating cases of acute scrotum.[4] Epididymoorchitis might show a thickened epididymis with normal to increased Doppler wave pulsations, consistent with a normal to increased blood flow.
Other Imaging Findings
A scrotal radionuclide scintigraphy has a high specificity and sensitivity in distinguishing between testicular torsion and epididymoorchitis. In testicular torsion, there is decreased or absent uptake of radionuclide, while uptake is increased in cases of epididymoorchitis.[3]
Other Diagnostic Studies
There are no other diagnostic studies for epididymoorchitis.
Medical Therapy
Management of epididymoorchitis consists mainly of conservative measures, including bed rest and limitation of physical activity, use of cold packs, analgesia and non-steroidal anti-inflammatory drugs (NSAIDs). In addition, appropriate antibiotic therapy should be initiated if the cause of epididymoorchitis is bacterial.[2][8][3]
Surgery
There is no role for surgery in treating uncomplicated cases of epididymoorchitis.
Primary Prevention
In men aged 14 to 35 years, cases of epididymoorchitis are mainly due to sexually transmitted infections. Hence, the importance of condom use to prevent the disease should be emphasized.[2]
Secondary Prevention
Secondary prevention of epididymoorchitis mainly consists on emphasizing on the importance of completion of the antibiotic course if prescribed, screening and treating comorbid sexually transmitted infections in both the patient and his partners.[2][4][9][10][11]
References
- ↑ Taylor AJ (1841). “On the utility of compression in epididymitis: With cases”. Prov Med Surg J (1840). 3 (53): 8–10. PMC 2489278. PMID 21379715.
- ↑ 2.0 2.1 2.2 2.3 2.4 2.5 2.6 2.7 2.8 Trojian TH, Lishnak TS, Heiman D (2009). “Epididymitis and orchitis: an overview”. Am Fam Physician. 79 (7): 583–7. PMID 19378875.
- ↑ 3.0 3.1 3.2 3.3 3.4 3.5 Tracy CR, Steers WD, Costabile R (2008). “Diagnosis and management of epididymitis”. Urol. Clin. North Am. 35 (1): 101–8, vii. doi:10.1016/j.ucl.2007.09.013. PMID 18061028.
- ↑ 4.0 4.1 4.2 4.3 4.4 4.5 Luzzi GA, O’Brien TS (2001). “Acute epididymitis”. BJU Int. 87 (8): 747–55. PMID 11350430.
- ↑ 5.0 5.1 Kadish HA, Bolte RG (1998). “A retrospective review of pediatric patients with epididymitis, testicular torsion, and torsion of testicular appendages”. Pediatrics. 102 (1 Pt 1): 73–6. PMID 9651416.
- ↑ Ciftci AO, Senocak ME, Tanyel FC, Büyükpamukçu N (2004). “Clinical predictors for differential diagnosis of acute scrotum”. Eur J Pediatr Surg. 14 (5): 333–8. doi:10.1055/s-2004-821210. PMID 15543483.
- ↑ The U.S. Preventive Services Task Force https://www.uspreventiveservicestaskforce.org/BrowseRec/Search?s=epididymoorchitis. Accessed on Dec. 28, 2016.
- ↑ 8.0 8.1 Stewart A, Ubee SS, Davies H (2011). “Epididymo-orchitis”. BMJ. 342: d1543. PMID 21490048.
- ↑ Berger RE, Alexander ER, Harnisch JP, Paulsen CA, Monda GD, Ansell J, Holmes KK (1979). “Etiology, manifestations and therapy of acute epididymitis: prospective study of 50 cases”. J. Urol. 121 (6): 750–4. PMID 379366.
- ↑ Mulcahy FM, Bignell CJ, Rajakumar R, Waugh MA, Hetherington JW, Ewing R, Whelan P (1987). “Prevalence of chlamydial infection in acute epididymo-orchitis”. Genitourin Med. 63 (1): 16–8. PMC 1193999. PMID 3817820.
- ↑ Grant JB, Costello CB, Sequeira PJ, Blacklock NJ (1987). “The role of Chlamydia trachomatis in epididymitis”. Br J Urol. 60 (4): 355–9. PMID 3690209.
Historical Perspective
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Dima Nimri, M.D. [2]
Overview
Cases of epididymoorchitis were described in literature as early as 1841.[1]It was believed that epididymitis was caused by chemical irritation caused by urine reflux. However, by 1979, a study showed that bacteria were responsible for more cases. [2]
Historical Perspective
- Cases of epididymoorchitis were described in literature as early as 1841.[1]
- In 1841, A. J. Taylor described the effects of compression (i.e., applying pressure on the testicles) in the treatment of epididymitis.[1] In 1847, Wills GF suggests the same modality of treatment for orchitis.[3]
- In 1906, Francis R. Hagner described operative treatment of acute epididymitis caused by N. gonorrhea.[4]
- It was believed that epididymitis was caused by chemical irritation caused by urine reflux. However, by 1979, a study showed that bacteria were responsible for more cases. [2]
References
- ↑ 1.0 1.1 1.2 Taylor AJ (1841). “On the utility of compression in epididymitis: With cases”. Prov Med Surg J (1840). 3 (53): 8–10. PMC 2489278. PMID 21379715.
- ↑ 2.0 2.1 Trojian TH, Lishnak TS, Heiman D (2009). “Epididymitis and orchitis: an overview”. Am Fam Physician. 79 (7): 583–7. PMID 19378875.
- ↑ Wills GF (1847). “Observations on the Treatment of Orchitis by Compression”. Prov Med Surg J. 11 (6): 148–51. PMC 2487178. PMID 20794182.
- ↑ Hagner FR (1908). “X. A Further Report of the Operative Treatment of Acute Gonorrhoeal Epididymitis”. Ann. Surg. 48 (6): 876–82. PMC 1407051. PMID 17862275.
Classification
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Dima Nimri, M.D. [2]
Overview
Epididymoorchitis can be classified based on the extent of involvement into isolated cases of epididymitis, isolated cases of orchitis or cases of epididymoorchitis. Another means of classifying the disease is based on duration into acute or chronic epididymoorchitis. Finally, it can also be classified according to the causative agent into infectious, non-infectious and idiopathic causes.[1][2]
Classification
Epididymoorchitis can be classified based on the extent of involvement, duration or cause of the disease.[1][2]
Extent of Involvement
- Epididymitis
- Orchitis
- Epididymoorchitis
Based on Duration
Epididymoorchitis can be divided into acute and chronic epididymoorchitis based on duration of the illness:
- Acute epididymoorchitis: are cases lasting less than 6 weeks in duration
- Chronic epididymoorchitis: are cases lasting more than 3 months in duration
Based on Cause
There are several etiological factors to epididymoorchitis and these include:
- Infectious causes
- Noninfectious causes
- Idiopathic epididymoorchitis
For more on the causative agents of epididymoorchitis, click here
References
- ↑ 1.0 1.1 Trojian TH, Lishnak TS, Heiman D (2009). “Epididymitis and orchitis: an overview”. Am Fam Physician. 79 (7): 583–7. PMID 19378875.
- ↑ 2.0 2.1 Tracy CR, Steers WD, Costabile R (2008). “Diagnosis and management of epididymitis”. Urol. Clin. North Am. 35 (1): 101–8, vii. doi:10.1016/j.ucl.2007.09.013. PMID 18061028.
Pathophysiology
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Dima Nimri, M.D. [2]
Overview
Epididymoorchitis refers to the inflammation of the epididymis and/or testes, with or without infection. While the pathogenesis is not fully understood, infectious epididymoorchitis is thought to be due to retrograde reflux of infected urine into the epididymis, which then spreads to the testes.[1][2]
Pathophysiology
Pathogenesis
Epididymoorchitis refers to the inflammation of the epididymis and/or testes, with or without infection. While the pathogenesis is not fully understood, the following are the proposed mechanisms behind epididymoorchitis:[1][2]
- The retrograde ascent of infectious pathogens is the usual route of infection. Most cases of epididymoorchitis start with inflammation of the epididymis (i.e., epididymitis), which then spread to the adjacent testicle (i.e., orchitis). Because orchitis tends to occur in patients with concurrent epididymitis, cases are mostly referred to as epididymoorchitis.
- Isolated cases of orchitis are usually due to mumps virus and in isolated cases of orchitis, blood-borne dissemination is the usual route of infection.
- Retrograde flow of infected urine into the ejaculatory duct is thought to cause epididymoorchitis.
- For infectious cases of epididymoorchitis that are not associated with an STD or UTI, it is believed that these cases may be related a post-infectious inflammatory reaction. When taking viral cultures of throat, stool and urine, it was found that patients with epididymoorchitis had elevated titers to certain pathogens, as compared to controls. Most notably, patients with epididymoorchitis had elevated titers to M. pneumonia and adenovirus.
- The mechanism behind non-infectious epididymoorchitis remains unclear.
Gross Pathology
-
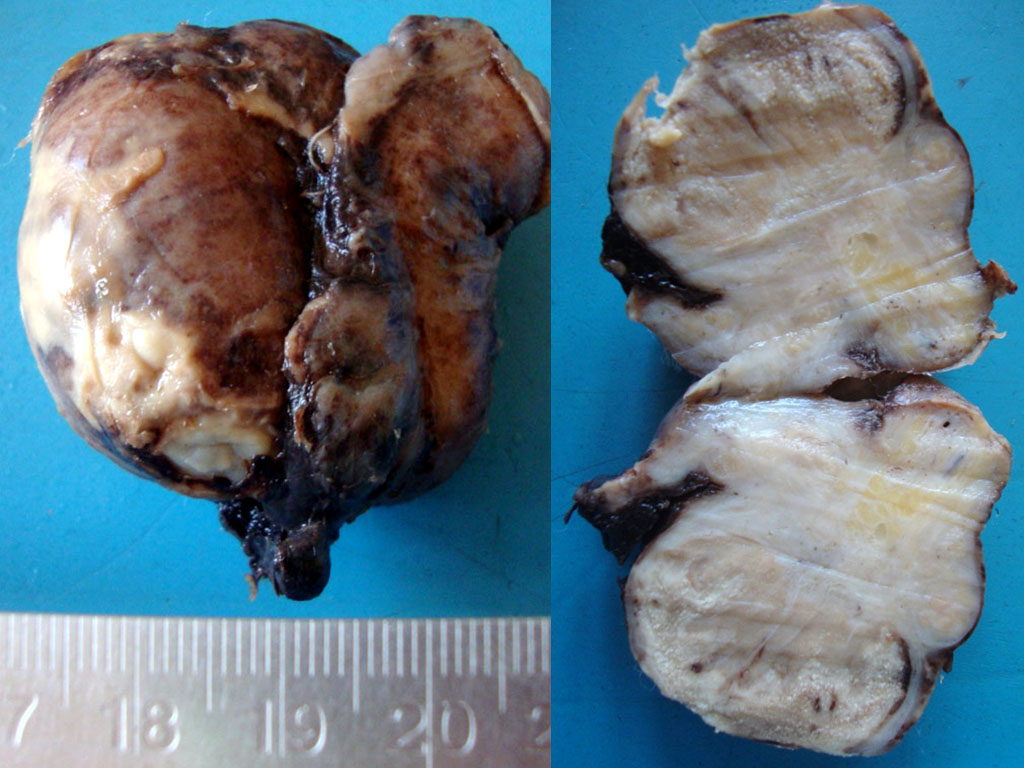 Image on the left shows evidence of acute inflammation and exudates on the surface of the testicle. Image to the right is a cut section showing exudates and dense fibrosis in the epididymis. Adapted from https://commons.wikimedia.org/wiki/Category:Gross_pathology_of_epididymo-orchitis#/media/File:Acute_epidydimoorchitis_Gross_Pathology.jpg. Accessed on Jan 3rd, 2017.
Image on the left shows evidence of acute inflammation and exudates on the surface of the testicle. Image to the right is a cut section showing exudates and dense fibrosis in the epididymis. Adapted from https://commons.wikimedia.org/wiki/Category:Gross_pathology_of_epididymo-orchitis#/media/File:Acute_epidydimoorchitis_Gross_Pathology.jpg. Accessed on Jan 3rd, 2017. -
 Cut-section through the testicle following orchidectomy showing a lesion in the epidydimis with fibrosis and caseous necrosis, following chronic epididymoorchitis caused by Mycobacterium tuberculosis. Adapted from https://commons.wikimedia.org/wiki/Category:Gross_pathology_of_tuberculous_epididymo-orchitis#/media/File:Tuberculous_epididymoorchitis_gross_pathology.jpg. Accessed on Jan 3rd, 2017.
Cut-section through the testicle following orchidectomy showing a lesion in the epidydimis with fibrosis and caseous necrosis, following chronic epididymoorchitis caused by Mycobacterium tuberculosis. Adapted from https://commons.wikimedia.org/wiki/Category:Gross_pathology_of_tuberculous_epididymo-orchitis#/media/File:Tuberculous_epididymoorchitis_gross_pathology.jpg. Accessed on Jan 3rd, 2017.


Microscopic Pathology
Acute epididymoorchitis is characterized by infiltration of neutrophils. Chronic cases of epididymoorchitis, such as in sarcoidosis or tuberculosis, are characterized by granulomatous inflammation.
-
 Microscopy showing hyalinised residual seminiferous tubules and dense infilitrate of neutrophils. Adapted from https://commons.wikimedia.org/wiki/Category:Histopathology_of_epididymo-orchitis#/media/File:Suppurative_epidydimo_orchitis_histopathology.jpg. Accessed on Jan 3rd, 2017.
Microscopy showing hyalinised residual seminiferous tubules and dense infilitrate of neutrophils. Adapted from https://commons.wikimedia.org/wiki/Category:Histopathology_of_epididymo-orchitis#/media/File:Suppurative_epidydimo_orchitis_histopathology.jpg. Accessed on Jan 3rd, 2017. -
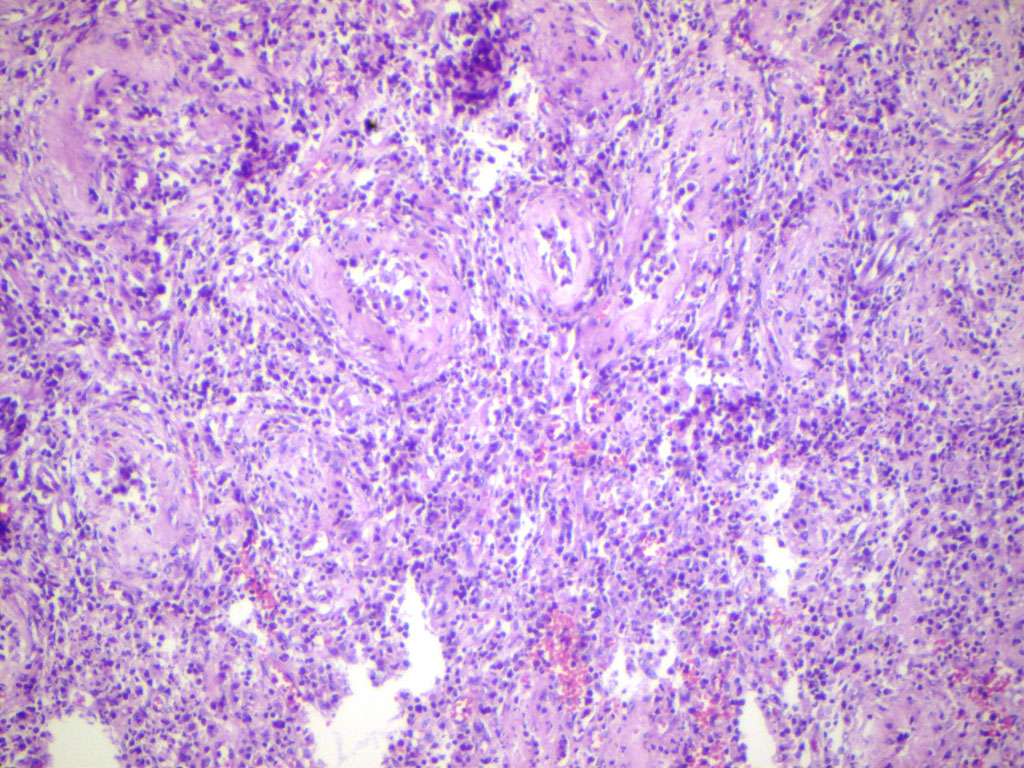
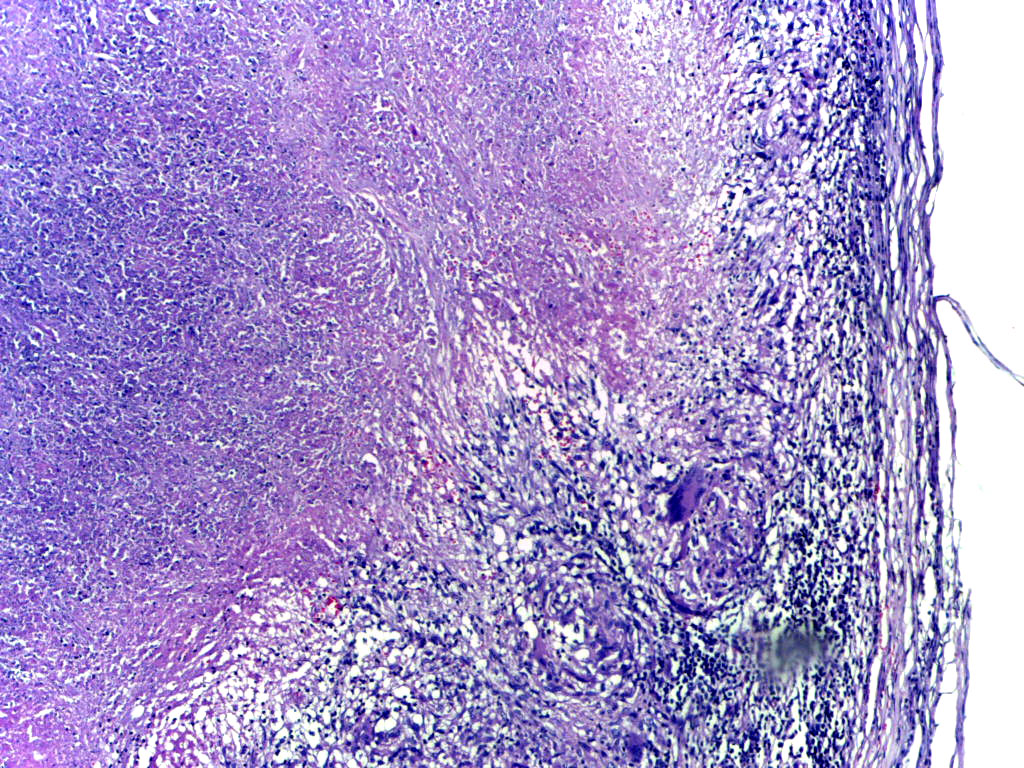 Low-power microscopy showing tuberculous epididymitis; caseous necrosis surrounded by epithelioid cells and giant cells with a mantle of lymphocytes. Adapted from https://commons.wikimedia.org/wiki/Category:Histopathology_of_tuberculous_epididymitis#/media/File:Tuberculous_epididymitis_Low_Power.jpg. Accessed on Jan 3rd, 2017.
Low-power microscopy showing tuberculous epididymitis; caseous necrosis surrounded by epithelioid cells and giant cells with a mantle of lymphocytes. Adapted from https://commons.wikimedia.org/wiki/Category:Histopathology_of_tuberculous_epididymitis#/media/File:Tuberculous_epididymitis_Low_Power.jpg. Accessed on Jan 3rd, 2017.


Associated Conditions
The following conditions may be associated with epididymoorchitis:[1]
- Sexually transmitted diseases, such as N. gonorrhea and C. trachomatis
- Mumps infection may be associated with isolated cases of orchitis
- Anatomic abnormalities of the urinary tract, such as prostatic obstruction in older men (e.g., benign prostatic hyperplasia (BPH), prostatic cancer, urethral strictures)[2] and posterior urethral valves or meatal stenosis in young, prepubertal boys
References
- ↑ 1.0 1.1 1.2 Trojian TH, Lishnak TS, Heiman D (2009). “Epididymitis and orchitis: an overview”. Am Fam Physician. 79 (7): 583–7. PMID 19378875.
- ↑ 2.0 2.1 2.2 Tracy CR, Steers WD, Costabile R (2008). “Diagnosis and management of epididymitis”. Urol. Clin. North Am. 35 (1): 101–8, vii. doi:10.1016/j.ucl.2007.09.013. PMID 18061028.
Causes
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Dima Nimri, M.D. [2]
Overview
The causes of epididymoorchitis can be divided into idiopathic, infectious and non-infectious causes.[1][2]
Causes
The causes of epididymoorchitis can be divided into idiopathic, infectious and non-infectious causes:[1][2]
| Infectious | ||
|---|---|---|
| Common Pathogens | Less Common Pathogens | |
| Sexually transmitted | Neisseria gonorrhea | Ureaplasma urealyticum |
| Associated with a UTI/bacteriuria | E. Coli | Hemophilus influenza type b |
| Others | Bacterial: | |
| Viral: | ||
| Fungal: | ||
| Parasitic:
Wuchereria bancrofti (flilariasis) | ||
| Noninfectious |
| |
| Idiopathic | – | |
References
Differentiating Epididymoorchitis from other Diseases
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Dima Nimri, M.D. [2]Syed Hassan A. Kazmi BSc, MD [3]José Eduardo Riceto Loyola Junior, M.D.[4]
Overview
Epididymoorchitis is a major cause of acute scrotum. Other causes of acute scrotum which must be differentiated from epididymoorchitis include testicular torsion and torsion of the testicular appendage.[1][2][3][4]
Differentiating Epididymoorchitis From Other Diseases
Epididymoorchitis is a major cause of acute scrotum. Other causes of acute scrotum which must be differentiated from epididymoorchitis include testicular torsion and torsion of the testicular appendage:[1][2][3][4]
| Epididymoorchitis | Testicular Torsion | Torsion of the Testicular Appendage | |
|---|---|---|---|
| Swelling and redness of the scrotum | can be present | can be present | can be present |
| Location of pain/tenderness | Testicles and/or epididymis | Testicles | Superior pole of the testis |
| Onset of pain | Gradual | Sudden | N/A |
| Urinary symptoms | Can be present | Usually absent | Usually absent |
| Pain with elevation of the testis | Usually relieved | Usually exacerbated | N/A |
| Cremasteric Reflex | Usually present | Usually absent | Usually present |
| “Blue dot” sign | Absent | Absent | Can be present and indicates infarction of the testicular appendage |
| Testicular lie | Normal | can be high and transverse | Normal |
| Doppler ultrasound findings | Normal or increased flow | Decreased or absent flow | Normal or increased flow |
- If patient presents with symptoms for ≥6-weeks (symptoms of discomfort or pain in the scrotum, testicle, or epididymis), chronic epididymitis must be suspected. It is usually caused by granulomatous reaction. Mycobacterium tuberculosis is the most common granulomatous disease affecting the testicles and epididymis. Differential must include chronic noninfectious epididymitis.
Other Differentials
Epididymoorchitis should be differentiated from other conditions presenting with scrotal pain or lower abdominal pain, fever, nausea and vomiting. The differentials include the following:[5][6][7][8][9][10][11][12][13][14][15][16][17][18][19][20][21][22][23][24][25][26][27][28][29][30][31][32][33][34][35][36][37][38]
| Category | Disease | History | Signs and Symptoms | Physical Examination | Laboratory abnormalities | |||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Nausea/vomiting | Hematuria | Location of pain | Fever | Tachycardia | Hypotension | Hypertension | Anorexia | Constipation | Rebound abdominal tenderness | Urinary frequency/Urgency/Dysuria | Costovetebral angle tenderness | Pelvic Examination | Rectal Examination | Complete Blood Count (CBC) | Urinalysis | BUN | Creatinine | Stone analysis | Urine Beta- hCG | Abnormal Liver Function Tests (LFTs) | Serum Amylase/Lipase | Abdominal/Pelvic CT scan | Serum Parathyroid hormone levels (PTH) | |||
Renal Pathology |
Nephrolithiasis |
|
+ | + | – | + | – | – | +/- | – | – | + | – | – | – | – | – | – | – |
|
+/- | |||||
| Pyelonephritis |
|
+ | + (microscopic) |
|
+ | + | + | – | +/- | – | + | + | + | – |
|
– | – | – | – |
|
– | |||||
| Renal infarct | + | + | + | + | – | + | – | – | – | – | – | – | – | – | – | – | ||||||||||
| Renal papillary necrosis | – | + (microscopic) | + | +/- | – | + | – | – | – | + | – | – | – | – | – | – | – |
|
– | |||||||
| Renal cell carcinoma |
|
+ | + (microscopic) | – | – | – | + | + | +/- | – | – | – | – | – |
|
|
– | – | – | – |
|
– | ||||
| Uretral stricture |
|
– | +/- | – | – | – | – | – | – | – | – | + | – | – | – | – | – | – | – | – | – | – | – | |||
Prostate Pathology |
Prostatitis |
|
– | + |
|
+ | + | – | – | – | – | – | + | – | – |
|
– | – | – | – | – | – | – | |||
| Prostatic cancer |
|
– | + | – | – | – | – | – | + | – | – | + | – | – |
|
– |
|
– | – | – | – |
|
– | |||
Testicular Pathology |
Testicular torsion |
|
+ | – |
|
– | + | – | – | +/- | – | – | +/- | – |
|
– | – | – | – | – | – | – | – | – |
|
– |
| Orchitis |
|
+ | – |
|
+ | + | – | – | – | – | – | +/- | – |
|
– | – | – | – | – | – | – | – |
|
– | ||
Abdominal Pathology |
Cholecystitis |
|
+ | – | + | + | – | – | + | – | – | – | – | – | – | – | – | – |
|
– | + | +/- |
|
– | ||
| Appendicitis |
|
+ | – |
|
+ | + | – | – | + | – | + | +/- | – | – | – |
|
– | – | – | – | – | – | + (if perforation) |
|
– | |
| Diverticulitis |
|
+ | – | + | + | – | – | + | + | – | – | – | – | – | – | – | – | – | – | + (if perforation) |
|
– | ||||
| Abdominal aortic aneurysm | – | – |
|
– | + | + | – | – | – | + (if rupture) | – | – | – | – | – | – | – | – | – | – | – | – |
|
– | ||
| Portal vein thrombosis | + | – | + | + | + | – | + | – | + (if bowel ischemia or infarction-secondary to extension of thrombus to superior mesenteric vein) | – | – | – | – | – | – | – | – | + | + (if bowel infarction, perforation) |
|
||||||
| Duodenal ulcer |
|
+ | – | + | + | + | – | – | – | + (if perforation) | – | – | – | – | – | – | – | + (if bowel perforation) | – | |||||||
| Ischemic colitis |
|
+ | – |
|
+ | + | + (if necrosis and sepsis) | + | + | + | + (if transmural necrosis) | – | – | – |
|
– | – | – | – | + (if bowel perforation) |
|
– | ||||
References
- ↑ 1.0 1.1 Trojian TH, Lishnak TS, Heiman D (2009). “Epididymitis and orchitis: an overview”. Am Fam Physician. 79 (7): 583–7. PMID 19378875.
- ↑ 2.0 2.1 Kadish HA, Bolte RG (1998). “A retrospective review of pediatric patients with epididymitis, testicular torsion, and torsion of testicular appendages”. Pediatrics. 102 (1 Pt 1): 73–6. PMID 9651416.
- ↑ 3.0 3.1 Luzzi GA, O’Brien TS (2001). “Acute epididymitis”. BJU Int. 87 (8): 747–55. PMID 11350430.
- ↑ 4.0 4.1 Ciftci AO, Senocak ME, Tanyel FC, Büyükpamukçu N (2004). “Clinical predictors for differential diagnosis of acute scrotum”. Eur J Pediatr Surg. 14 (5): 333–8. doi:10.1055/s-2004-821210. PMID 15543483.
- ↑ Worcester EM, Coe FL (June 2008). “Nephrolithiasis”. Prim. Care. 35 (2): 369–91, vii. doi:10.1016/j.pop.2008.01.005. PMC 2518455. PMID 18486720.
- ↑ Semins MJ, Matlaga BR (February 2010). “Medical evaluation and management of urolithiasis”. Ther Adv Urol. 2 (1): 3–9. doi:10.1177/1756287210369121. PMC 3126068. PMID 21789078.
- ↑ Venkatesh L, Hanumegowda RK (June 2017). “Acute Pyelonephritis – Correlation of Clinical Parameter with Radiological Imaging Abnormalities”. J Clin Diagn Res. 11 (6): TC15–TC18. doi:10.7860/JCDR/2017/27247.10033. PMC 5535453. PMID 28764263.
- ↑ Garin EH, Olavarria F, Araya C, Broussain M, Barrera C, Young L (July 2007). “Diagnostic significance of clinical and laboratory findings to localize site of urinary infection”. Pediatr. Nephrol. 22 (7): 1002–6. doi:10.1007/s00467-007-0465-7. PMID 17375337.
- ↑ Lee DG, Jeon SH, Lee CH, Lee SJ, Kim JI, Chang SG (April 2009). “Acute pyelonephritis: clinical characteristics and the role of the surgical treatment”. J. Korean Med. Sci. 24 (2): 296–301. doi:10.3346/jkms.2009.24.2.296. PMC 2672131. PMID 19399273.
- ↑ Saeed K (2012). “Renal infarction”. Int J Nephrol Renovasc Dis. 5: 119–23. doi:10.2147/IJNRD.S33768. PMC 3437809. PMID 22969301.
- ↑ Mahamid M, Francis A, Abid A, Awawde M, Abu-Elhija O (2014). “Embolic renal infarction mimicking renal colic”. Int J Nephrol Renovasc Dis. 7: 157–9. doi:10.2147/IJNRD.S59745. PMC 4011809. PMID 24812524.
- ↑ Korzets Z, Plotkin E, Bernheim J, Zissin R (October 2002). “The clinical spectrum of acute renal infarction”. Isr. Med. Assoc. J. 4 (10): 781–4. PMID 12389340.
- ↑ Brix AE (2002). “Renal papillary necrosis”. Toxicol Pathol. 30 (6): 672–4. doi:10.1080/01926230290166760. PMID 12512867.
- ↑ Eknoyan G, Qunibi WY, Grissom RT, Tuma SN, Ayus JC (March 1982). “Renal papillary necrosis: an update”. Medicine (Baltimore). 61 (2): 55–73. PMID 7038374.
- ↑ Ng CS, Wood CG, Silverman PM, Tannir NM, Tamboli P, Sandler CM (October 2008). “Renal cell carcinoma: diagnosis, staging, and surveillance”. AJR Am J Roentgenol. 191 (4): 1220–32. doi:10.2214/AJR.07.3568. PMID 18806169.
- ↑ Ares Valdés Y, Amador Sandoval B, Morales JC, Alonso Domínguez F, Carballo Velásquez L, Fragas Valdés R, Shou Rodríguez A (September 2004). “[The role of CT scan in the diagnosis of renal cell carcinoma]”. Arch. Esp. Urol. (in Spanish; Castilian). 57 (7): 737–42. PMID 15536955.
- ↑ Leveridge MJ, Bostrom PJ, Koulouris G, Finelli A, Lawrentschuk N (June 2010). “Imaging renal cell carcinoma with ultrasonography, CT and MRI”. Nat Rev Urol. 7 (6): 311–25. doi:10.1038/nrurol.2010.63. PMID 20479778.
- ↑ Tritschler S, Roosen A, Füllhase C, Stief CG, Rübben H (March 2013). “Urethral stricture: etiology, investigation and treatments”. Dtsch Arztebl Int. 110 (13): 220–6. doi:10.3238/arztebl.2013.0220. PMC 3627163. PMID 23596502.
- ↑ Mundy AR, Andrich DE (January 2011). “Urethral strictures”. BJU Int. 107 (1): 6–26. doi:10.1111/j.1464-410X.2010.09800.x. PMID 21176068.
- ↑ Maciejewski C, Rourke K (February 2015). “Imaging of urethral stricture disease”. Transl Androl Urol. 4 (1): 2–9. doi:10.3978/j.issn.2223-4683.2015.02.03. PMC 4708283. PMID 26816803.
- ↑ Soper DE (August 2010). “Pelvic inflammatory disease”. Obstet Gynecol. 116 (2 Pt 1): 419–28. doi:10.1097/AOG.0b013e3181e92c54. PMID 20664404.
- ↑ Paavonen J (October 1998). “Pelvic inflammatory disease. From diagnosis to prevention”. Dermatol Clin. 16 (4): 747–56, xii. PMID 9891675.
- ↑ Lee MH, Moon MH, Sung CK, Woo H, Oh S (December 2014). “CT findings of acute pelvic inflammatory disease”. Abdom Imaging. 39 (6): 1350–5. doi:10.1007/s00261-014-0158-1. PMID 24802548.
- ↑ Eggert J, Sundquist K, van Vuuren C, Fianu-Jonasson A (October 2006). “The clinical diagnosis of pelvic inflammatory disease–reuse of electronic medical record data from 189 patients visiting a Swedish university hospital emergency department”. BMC Womens Health. 6: 16. doi:10.1186/1472-6874-6-16. PMC 1624808. PMID 17054801.
- ↑ Washington C, Carmichael JC (December 2012). “Management of ischemic colitis”. Clin Colon Rectal Surg. 25 (4): 228–35. doi:10.1055/s-0032-1329534. PMC 3577613. PMID 24294125.
- ↑ Chawla YK, Bodh V (March 2015). “Portal vein thrombosis”. J Clin Exp Hepatol. 5 (1): 22–40. doi:10.1016/j.jceh.2014.12.008. PMC 4415192. PMID 25941431.
- ↑ “Imaging of Abdominal Aortic Aneurysms – – American Family Physician”.
- ↑ Aggarwal S, Qamar A, Sharma V, Sharma A (2011). “Abdominal aortic aneurysm: A comprehensive review”. Exp Clin Cardiol. 16 (1): 11–5. PMC 3076160. PMID 21523201.
- ↑ Destigter KK, Keating DP (August 2009). “Imaging update: acute colonic diverticulitis”. Clin Colon Rectal Surg. 22 (3): 147–55. doi:10.1055/s-0029-1236158. PMC 2780264. PMID 20676257.
- ↑ Hameed AM, Lam VW, Pleass HC (February 2015). “Significant elevations of serum lipase not caused by pancreatitis: a systematic review”. HPB (Oxford). 17 (2): 99–112. doi:10.1111/hpb.12277. PMC 4299384. PMID 24888393.
- ↑ “Imaging for Suspected Appendicitis – – American Family Physician”.
- ↑ “CT Findings of Acute Cholecystitis and Its Complications : American Journal of Roentgenology : Vol. 194, No. 6 (AJR)”.
- ↑ “Epididymitis and Orchitis: An Overview – – American Family Physician”.
- ↑ Jia JB, Houshyar R, Verma S, Uchio E, Lall C (January 2016). “Prostate cancer on computed tomography: A direct comparison with multi-parametric magnetic resonance imaging and tissue pathology”. Eur J Radiol. 85 (1): 261–267. doi:10.1016/j.ejrad.2015.10.013. PMID 26526901.
- ↑ Bratt O, Lilja H (January 2015). “Serum markers in prostate cancer detection”. Curr Opin Urol. 25 (1): 59–64. doi:10.1097/MOU.0000000000000128. PMC 4315142. PMID 25393274.
- ↑ “Prostate Cancer (Prostate Carcinoma): Symptoms – National Library of Medicine – PubMed Health”.
- ↑ Eskicioğlu F, Özdemir AT, Turan GA, Gür EB, Kasap E, Genç M (November 2014). “The efficacy of complete blood count parameters in the diagnosis of tubal ectopic pregnancy”. Ginekol. Pol. 85 (11): 823–7. PMID 25675798.
- ↑ Sivalingam VN, Duncan WC, Kirk E, Shephard LA, Horne AW (October 2011). “Diagnosis and management of ectopic pregnancy”. J Fam Plann Reprod Health Care. 37 (4): 231–40. doi:10.1136/jfprhc-2011-0073. PMC 3213855. PMID 21727242.
Epidemiology and Demographics
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Dima Nimri, M.D. [2]
Overview
Data on epidemiology of epididymoorchitis is scarce, however, epididymoorchitis is the 5th most common genitourinary diagnosis made and disease is more prevalent among U.S. military men. Peak incidence of the disease is in men between the ages of 20 to 29 years.[1]
Epidemiology
Data on epidemiology of epididymoorchitis is scarce, however, epididymoorchitis is the 5th most common genitourinary diagnosis made and disease is more prevalent among U.S. military men.[1]
- In 2002, 1 in 144 outpatient visits were due to epididymoorchitis.[2]
- In 2002, it has been estimated that the incidence of epididymoorchitis in the U.S. is 600,000 cases per year.[2]
The true prevalence of epididymoorchitis is unknown.[3]
Demographics
Age
- Epididymoorchitis can occur in men of any age. However, there is a bimodal distribution for the disease between 16-30 years of age and 51-70 years of age.[2]
- Peak incidence for epididymoorchitis is in men between the ages of 20-29 years.[2][1]
Race
No sufficient data exists on racial predilection of epididymoorchitis.
References
- ↑ 1.0 1.1 1.2 Luzzi GA, O’Brien TS (2001). “Acute epididymitis”. BJU Int. 87 (8): 747–55. PMID 11350430.
- ↑ 2.0 2.1 2.2 2.3 Trojian TH, Lishnak TS, Heiman D (2009). “Epididymitis and orchitis: an overview”. Am Fam Physician. 79 (7): 583–7. PMID 19378875.
- ↑ Tracy CR, Steers WD, Costabile R (2008). “Diagnosis and management of epididymitis”. Urol. Clin. North Am. 35 (1): 101–8, vii. doi:10.1016/j.ucl.2007.09.013. PMID 18061028.
Risk Factors
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Dima Nimri, M.D. [2]
Overview
Risk factors for epididymoorchitis include sexual activity and sexually transmitted diseases, surgery or instrumentation of the bladder, as well as anatomic abnormalities of the urinary tract and obstruction to the normal flow of urine.[1]
Risk Factors
Risk factors for epididymoorchitis include:[1]
- Sexual activity and infection with sexually transmitted diseases, such as C. trachomatis and N. gonorrhea
- Males who have sex with males (MSM)
- HIV is a risk factor to epididymoorchitis infections caused by viruses and fungi
- Strenuous physical activity[2][3]
- Riding motorcycles/bicycles[2][3]
- Prolonged periods of inactivity and sitting[2][3]
- Recent urinary tract surgery or instrumentation, such as cystoscopy and bladder catheterization[4]
- Anatomic abnormalities of the urinary tract, such as prostatic obstruction in older men (e.g., benign prostatic hyperplasia (BPH), prostatic cancer, urethral strictures)[5] and posterior urethral valves or meatal stenosis in young, prepubertal boys
- Mumps infection is a risk factor for isolated mumps orchitis infection
References
- ↑ 1.0 1.1 Trojian TH, Lishnak TS, Heiman D (2009). “Epididymitis and orchitis: an overview”. Am Fam Physician. 79 (7): 583–7. PMID 19378875.
- ↑ 2.0 2.1 2.2 Kaver I, Matzkin H, Braf ZF (1990). “Epididymo-orchitis: a retrospective study of 121 patients”. J Fam Pract. 30 (5): 548–52. PMID 2332745.
- ↑ 3.0 3.1 3.2 Kadish HA, Bolte RG (1998). “A retrospective review of pediatric patients with epididymitis, testicular torsion, and torsion of testicular appendages”. Pediatrics. 102 (1 Pt 1): 73–6. PMID 9651416.
- ↑ Stewart A, Ubee SS, Davies H (2011). “Epididymo-orchitis”. BMJ. 342: d1543. PMID 21490048.
- ↑ Tracy CR, Steers WD, Costabile R (2008). “Diagnosis and management of epididymitis”. Urol. Clin. North Am. 35 (1): 101–8, vii. doi:10.1016/j.ucl.2007.09.013. PMID 18061028.
Screening
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Dima Nimri, M.D. [2]
Overview
There are no screening recommendations for epididymoorchitis.[1]
Screening
There are no screening recommendations for epididymoorchitis.[1]
References
- ↑ 1.0 1.1 The U.S. Preventive Services Task Force https://www.uspreventiveservicestaskforce.org/BrowseRec/Search?s=epididymoorchitis. Accessed on Dec. 28, 2016.
Natural History, Complications and Prognosis
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Dima Nimri, M.D. [2]
Overview
The prognosis of epididymoorchitis is usually excellent, with the majority of cases resolving within 30 days of initiation of medical therapy. However, some cases can progress to chronic epididymoorchitis. Other complications of epididymoorchitis include abscess formation, testicular infarction, sepsis and infertility.
Natural History
If left untreated, acute epididymoorchitis may progress to chronic cases.[1]
Complications
Some of the complications of an acute epididymoorchitis infection include:[1]
- Progression of the infection to chronic epididymoorchitis
- Formation of a reactive hydrocele
- Abscess formation
- Infarction of the testicle
- Sepsis
- Infertility
Prognosis
The prognosis of epididymoorchitis is usually excellent. In young patients in whom epididymoorchitis is due to a sexually transmitted disease, acute epididymoorchitis usually resolves within 2 weeks of the initiation of medical therapy. In men older than the age of 40, 90% of cases of epididymitis resolve within 30 days of treatment.[2]
References
Diagnosis
Diagnosis
History and Symptoms | Physical Examination | Laboratory Findings | X ray | CT | MRI | Ultrasound | Other Imaging Findings | Other Diagnostic Studies
Treatment
Treatment
Medical therapy | Surgery | Primary Prevention | Secondary Prevention | Cost Effectiveness of Therapy | Future or Investigational Therapies
External Links
External Links
Looking for the patient version?
© 2026 MyEClinic – IFTM Institut für Telematik in der Medizin GmbH