
Hypoplastic left heart syndrome
For patient information click here
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-In-Chief: Priyamvada Singh, M.B.B.S.[2], Cafer Zorkun, M.D., Ph.D. [3], Keri Shafer, M.D. [4]; Assistant Editor(s)-In-Chief: Kristin Feeney, B.S.[5]
Synonyms and keywords: HLHS
Overview
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-In-Chief: Priyamvada Singh, M.B.B.S.[2], Cafer Zorkun, M.D., Ph.D. [3], Keri Shafer, M.D. [4]; Assistant Editor(s)-In-Chief: Kristin Feeney, B.S.[5]
Overview
Hypoplasia can affect the heart, which typically results in the failure of either the right ventricle or the left ventricle to develop adequately, leaving only one side of the heart capable of pumping blood to the body and lungs. Hypoplasia of the heart is rare but is the most serious form of congenital heart defect; it is called hypoplastic left heart syndrome when it affects the left side of the heart and hypoplastic right heart syndrome when it affects the right side of the heart. In both conditions, the presence of a patent ductus arteriosus (and, when hypoplasia affects the right side of the heart, a patent foramen ovale) is vital to the infant’s ability to survive until emergency heart surgery can be performed, since without these pathways blood cannot circulate to the body (or lungs, depending on which side of the heart is defective). Hypoplasia of the heart is generally a cyanotic heart defect.
Hypoplastic left heart syndrome is a rare congenital heart defect in which the left side of the heart is severely underdeveloped. In babies with HLHS, the aorta and left ventricle are very small, and the aortic and mitral valves are either too small to allow sufficient blood flow or are atretic (closed) altogether. As blood returns from the lungs to the left atrium, it must pass through an atrial septal defect to the right side of the heart. [1] [2] [3] [4] [5] [6] [7] [8] [9] [10] [11] [12] [13]
Pathophysiology
In patients with hypoplastic left heart syndrome, the left side of the heart is unable to send enough blood to the body. As a result, the right side of the heart must maintain the circulation for both the lungs and the body. The right ventricle can support the circulation to both the lungs and the body for a while, but this extra workload eventually causes the right side of the heart to fail.
Causes
As with most congenital heart defects, there is no known cause. Approximately 10% of patients with hypoplastic left heart syndrome also have other birth defects.
Differentiating Hypoplastic left heart syndrome from other Diseases
Signs and symptoms of hypoplastic left heart syndrome may be similar to other conditions. A differential diagnosis is essential to definitively diagnose hypoplastic left heart syndrome from associated conditions.
Risk Factors
Hypoplastic left heart is more common in males than in females.
Natural History, Complications and Prognosis
Failure to treat hypoplastic left heart syndrome can be fatal for the infant. However, with treatment, infants have a good chance at survival well into late adulthood. Potential complications may develop such as heart failure, arrhythmias, and even neurological complications.
Diagnosis
History and Symptoms
At first, a newborn with hypoplastic left heart may appear normal. Symptoms usually occur in the first few hours of life, although it may take up to a few days to develop symptoms. Common symptoms include cyanosis, dyspnea, and poor circulation.
Physical Examination
A physical examination is an integral part of diagnosing hypoplastic left heart syndrome. During a routine visit, a doctor may find signs of right ventricle enlargement, presence of additional birth defects, and hemodynamic imbalances.
Laboratory Findings
Laboratory studies that should be ordered include a complete blood count, and an arterial blood gas.
Electocardiogram
An electrocardiogram should be ordered if hypoplastic left heart syndrome is suspected. Findings that may be depicted are right axis deviation, right ventricular hypertrophy, and prominent p waves.
Chest X Ray
Findings on chest x ray include increased markings of pulmonary vasculature, and cardiomegaly.
Echocardiography
The echocardiogram is of high diagnostic value in the assessment of hypoplastic left heart syndrome. Doppler echocardiography will also help in visualizing the flow in the ventricles.
Treatment
Medical Therapy
Failure to treat hypoplastic left heart syndrome can be fatal for the infant. Medical therapy can be used prior to surgical intervention to allow the ductus to open and promote bloodflow. It is only a temporary solution, surgical intervention is needed to ultimately repair hypoplastic left heart syndrome.
Surgery
Failure to treat hypoplastic left heart syndrome can be fatal for the infant. Surgical therapy is the only true way to treat and permanently fix hypoplastic left heart syndrome. Two main methods exist for treatment: transplantation and a three-stage surgical procedure.
References
- ↑ Atz AM, Feinstein JA, Jonas RA, et al. Preoperative management of pulmonary venous hypertension in hypoplastic left heart syndrome with restrictive atrial septal defect. Am J Cardiol. Apr 15 1999;83(8):1224-8.
- ↑ Backer CL, Bove EL, Zales VR. Hypoplastic left heart syndrome. In: Cardiac Surgery. New York, NY: Churchill Livingstone;1994:442-53.
- ↑ Bailey L, Concepcion W, Shattuck H, Huang L. Method of heart transplantation for treatment of hypoplastic left heart syndrome. J Thorac Cardiovasc Surg. Jul 1986;92(1):1-5.
- ↑ Barber G. Hypoplastic left heart syndrome. In: Garson A Jr, Bricker JT, Fisher DJ, Neish SR, eds. The Science and Practice of Pediatric Cardiology. 2nd ed. Philadelphia, Pa: Lippincott Williams & Wilkins; 1998: 1625-45.
- ↑ Bove EL, Lloyd TR. Staged reconstruction for hypoplastic left heart syndrome. Contemporary results. Ann Surg. Sep 1996;224(3):387-94; discussion 394-5.
- ↑ Bove EL. Current status of staged reconstruction for hypoplastic left heart syndrome. Pediatr Cardiol. Jul-Aug 1998;19(4):308-15.
- ↑ Day RW, Barton AJ, Pysher TJ, Shaddy RE. Pulmonary vascular resistance of children treated with nitrogen during early infancy. Ann Thorac Surg. May 1998;65(5):1400-4.
- ↑ Fontan F, Baudet E. Surgical repair of tricuspid atresia. Thorax. May 1971;26(3):240-8.
- ↑ Freedom RM, Benson LN. Hypoplastic left heart syndrome. In: Moss and Adams Heart Disease in Infants, Children, and Adolescents. 5th ed. 1995: 1133-1153.
- ↑ Norwood WI, Kirklin JK, Sanders SP. Hypoplastic left heart syndrome: experience with palliative surgery. Am J Cardiol. Jan 1980;45(1):87-91.
- ↑ Norwood WI, Lang P, Hansen DD. Physiologic repair of aortic atresia-hypoplastic left heart syndrome. N Engl J Med. Jan 6 1983;308(1):23-6.
- ↑ Pizarro C, Malec E, Maher KO, et al. Right ventricle to pulmonary artery conduit improves outcome after stage I Norwood for hypoplastic left heart syndrome. Circulation. Sep 9 2003;108(10 Suppl 1):II155-II160.
- ↑ Talner CN. Report of the New England Regional Infant Cardiac Program, by Donald C. Fyler, MD, Pediatrics, 1980; 65(suppl):375-461. Pediatrics. Jul 1998;102(1 Pt 2):258-9.
Historical Perspective
Please help WikiDoc by adding content here. It’s easy! Click here to learn about editing.
References
Pathophysiology
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-In-Chief: Priyamvada Singh, M.B.B.S.[2], Cafer Zorkun, M.D., Ph.D. [3], Keri Shafer, M.D. [4]; Assistant Editor(s)-In-Chief: Kristin Feeney, B.S.[5]
Overview
In patients with hypoplastic left heart syndrome, the left side of the heart is unable to send enough blood to the body. As a result, the right side of the heart must maintain the circulation for both the lungs and the body. The right ventricle can support the circulation to both the lungs and the body for a while, but this extra workload eventually causes the right side of the heart to fail.
Pathophysiology
The only possibility of survival is a connection between the right and the left side of the heart, or between the arteries and pulmonary arteries (the blood vessels that carry blood to the lungs).In babies with HLHS, the aorta and left ventricle are very small, and the aortic and mitral valves are either too small to allow sufficient blood flow or are atretic (closed) altogether. As blood returns from the lungs to the left atrium, it must pass through an atrial septal defect to the right side of the heart. In a healthy human, the left side of the heart receives oxygen-rich blood from the lungs and pumps it out to the rest of the body; with these structures underdeveloped, they cannot circulate blood to other organs, and the right ventricle must pump blood to both the lungs, as it would normally, and to the rest of the body, a situation which cannot be sustained for long.
In cases of HLHS, the right side of the heart often must pump blood to the body through a patent ductus arteriosus. As the ductus arteriosus usually closes within eleven days after birth, blood flow is severely restricted and eventually cut off, leading to dangerously low circulation and eventually to shock.
Genetics
HLHS appears to be genetically sporadic and multiple loci have been implicated.
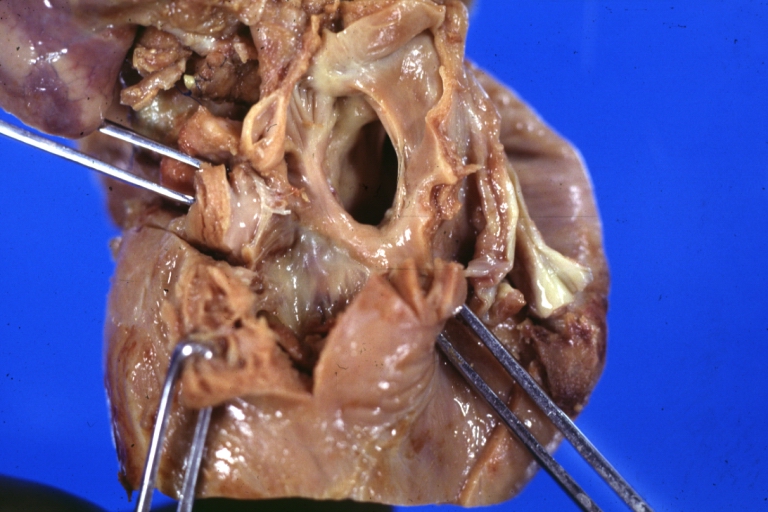
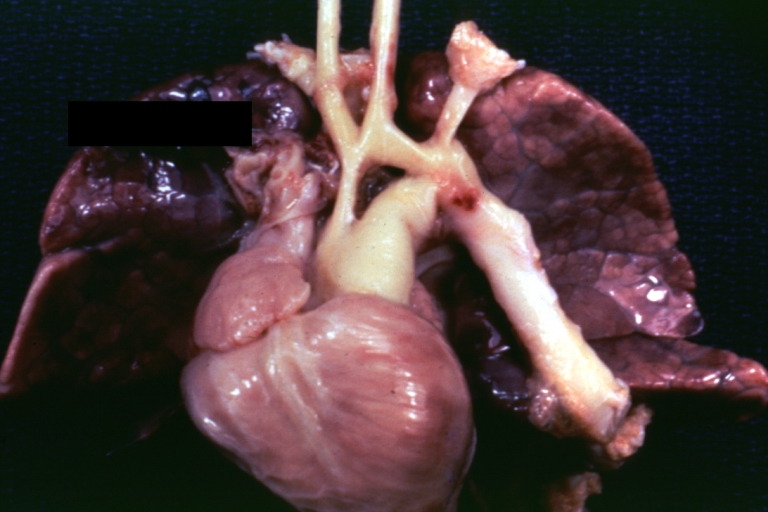
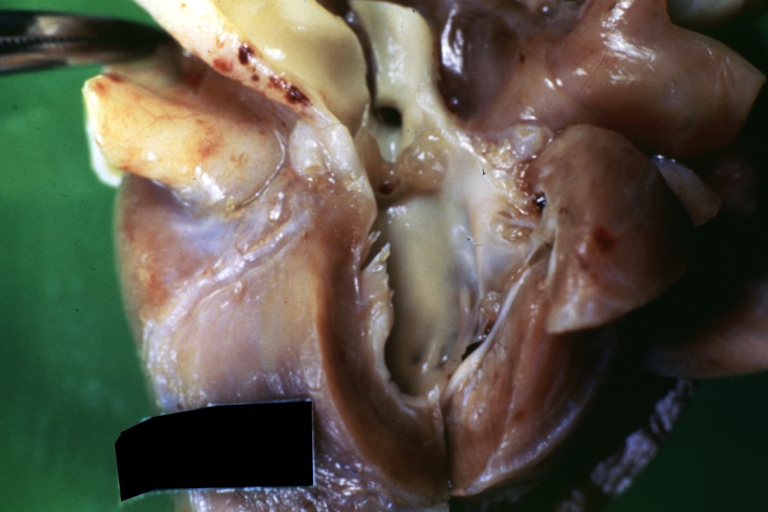
Gross Pathology
-
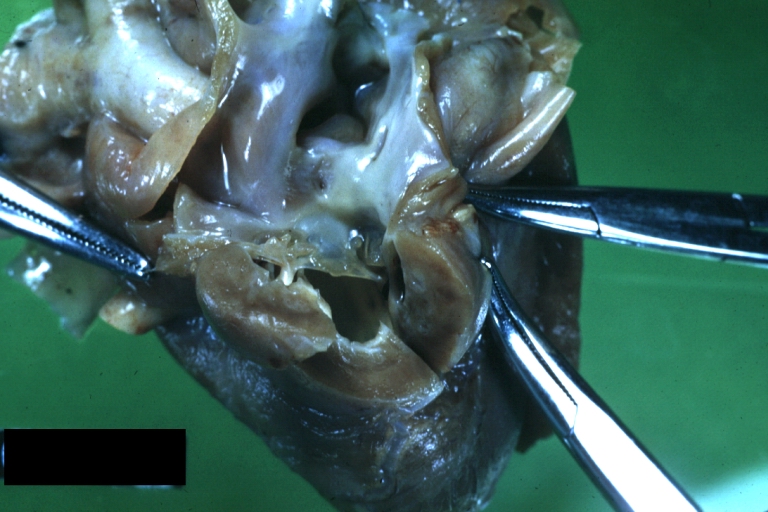 Hypoplastic left ventricle
Hypoplastic left ventricle -
 Hypoplastic left ventricle
Hypoplastic left ventricle -
 Hypoplastic left ventricle
Hypoplastic left ventricle -
 Hypoplastic left ventricle
Hypoplastic left ventricle -
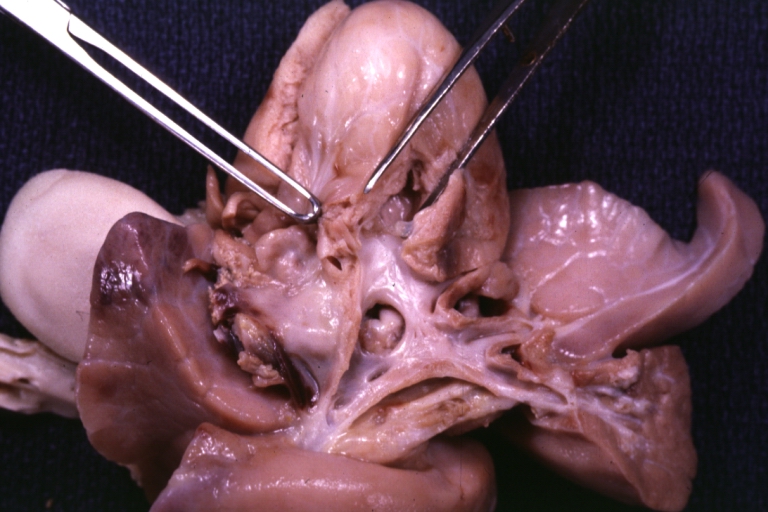 Hypoplastic left ventricle
Hypoplastic left ventricle -
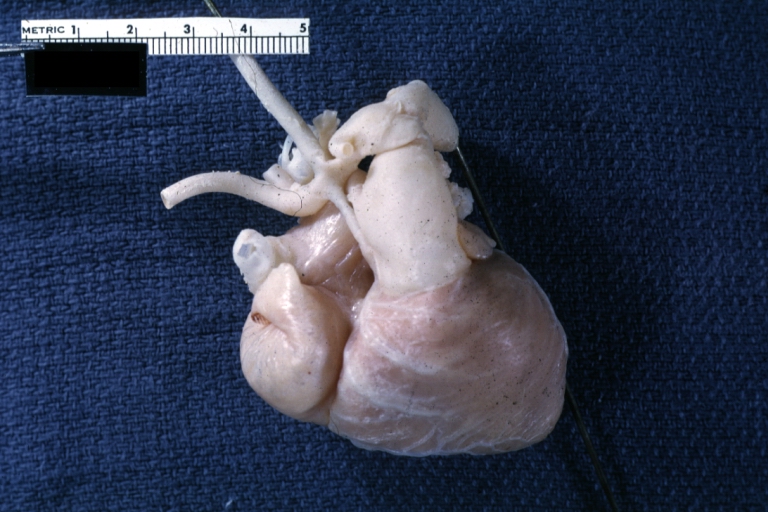 Hypoplastic left ventricle
Hypoplastic left ventricle






Associated Conditions
- HLHS is seen in patients Turner syndrome, Trisomy 18, Trisomy 13 and Jacobsen syndrome
- Anomalous pulmonary venous connection
- Coarctation of the aorta
- Complete atrioventricular canal
- Coronary artery abnormalities (especially in patients with aortic atresia and mitral stenosis)
- Persistent left superior vena cava
- Endocardial fibroelastosis (especially in patients with aortic atresia and mitral stenosis)
References
Causes
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-In-Chief: Priyamvada Singh, M.B.B.S.[2], Cafer Zorkun, M.D., Ph.D. [3], Keri Shafer, M.D. [4]; Assistant Editor(s)-In-Chief: Kristin Feeney, B.S.[5]
Overview
As with most congenital heart defects, there is no known cause. Approximately 10% of patients with hypoplastic left heart syndrome also have other birth defects.
Causes
While many authorities believe the cause of hypoplastic left heart syndrome (HLHS) is unknown,[1] [2][3] recent research indicates that HLHS may be due to genetic factors. [4][5] There is evidence associates hypoplastic left heart syndrome with gap junction protein, alpha 1.[6]
References
- ↑ “Hypoplastic Left Heart Syndrome Causes – Mayo Clinic”. Retrieved 2008-01-09.
- ↑ Hypoplastic Left Heart Syndrome : Article by P Syamasundar Rao, MD at eMedicine
- ↑ MedlinePlus Encyclopedia Hypoplastic left heart
- ↑ “Hypoplastic left heart syndrome likely caused by genetic factors”. Retrieved 2008-01-09.
- ↑ Dasgupta C, Martinez AM, Zuppan CW, Shah MM, Bailey LL, Fletcher WH (2001). “Identification of connexin43 (alpha1) gap junction gene mutations in patients with hypoplastic left heart syndrome by denaturing gradient gel electrophoresis (DGGE)”. Mutat. Res. 479 (1–2): 173–86. doi:10.1016/S0027-5107(01)00160-9. PMID 11470490.
- ↑ Online Mendelian Inheritance in Man (OMIM) HYPOPLASTIC LEFT HEART SYNDROME -241550
Differentiating Hypoplastic left heart syndrome from other Diseases
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-In-Chief: Priyamvada Singh, M.B.B.S.[2], Cafer Zorkun, M.D., Ph.D. [3], Keri Shafer, M.D. [4]; Assistant Editor(s)-In-Chief: Kristin Feeney, B.S.[5]
Overview
Signs and symptoms of hypoplastic left heart syndrome may be similar to other conditions. A differential diagnosis is essential to definitively diagnose hypoplastic left heart syndrome from associated conditions.
Differentiating Hypoplastic left heart syndrome from other Diseases
Several conditions produce signs and symptoms that are similar to those produce by hypoplastic left heart syndrome. To definitively diagnose hypoplastic left heart syndrome, a differential diagnosis must be done to rule out the following:
- Valvular aortic stenosis
- Viral myocarditis
- Unbalanced atrioventricular septal defect
- Total anomalous pulmonary venous connection
- Cardiac tumors
- Coarctation of the aorta
- Interrupted aortic arch
References
Epidemiology and Demographics
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-In-Chief: Priyamvada Singh, M.B.B.S.[2], Cafer Zorkun, M.D., Ph.D. [3], Keri Shafer, M.D. [4]; Assistant Editor(s)-In-Chief: Kristin Feeney, B.S.[5]
Please help WikiDoc by adding more content here. It’s easy! Click here to learn about editing.
Epidemiology and Demographics
Prevalence
It accounts for 2-3% of the all congenital heart disease.
Gender
Slightly more prevalent in males with male:female ratio of 1.5:1
References
Natural History, Complications, and Prognosis
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-In-Chief: Priyamvada Singh, M.B.B.S.[2], Cafer Zorkun, M.D., Ph.D. [3], Keri Shafer, M.D. [4]; Assistant Editor(s)-In-Chief: Kristin Feeney, B.S.[5]
Please help WikiDoc by adding more content here. It’s easy! Click here to learn about editing.
Overview
Failure to treat hypoplastic left heart syndrome can be fatal for the infant. However, with treatment, infants have a good chance at survival well into late adulthood. Potential complications may develop such as heart failure, arrhythmias, and even neurological complications.
Complications
- Irregular, fast heart rhythms (arrhythmias)
- Chronic diarrhea (due to protein loosing enteropathy)
- Heart failure
- Ascites and pleural effusion
- Blockage of the artificial shunt
- Strokes and other neurological complications
- Sudden death
Prognosis
While infants successfully treated for HLHS have a good chance of survival, they may experience chronic health problems for the rest of their lives. The 3-stage surgeries were developed in the early 1980’s with no survivors prior to that time. Therefore, the earliest survivors are in their early 20’s and the long term prognosis is unknown. However, the advances in surgical and medical techniques have helped increase the survival rate dramatically since the surgeries were first developed.
As is true for patients with other types of heart defects involving malformed valves, HLHS patients run a high risk of endocarditis, and must be monitored by a cardiologist for the rest of their lives to check on their heart function.
References
Diagnosis
Diagnosis
History and Symptoms | Physical Examination | Laboratory Findings | Electrocardiogram | Chest X Ray | Echocardiography | Other Imaging Findings
Treatment
Treatment
Medical Therapy | Surgery | Primary Prevention | Cost-Effectiveness of Therapy | Future or Investigational Therapies
Related Chapters
Related Chapters
Looking for the patient version?
© 2026 MyEClinic – IFTM Institut für Telematik in der Medizin GmbH