
Cardiac tumors
For patient information click here
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-In-Chief: Cafer Zorkun, M.D., Ph.D. [2]; Varun Kumar, M.B.B.S. Syed Hassan A. Kazmi BSc, MD [3]
Overview
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]
Overview
The primary tumors of the heart are tumors that arise from the normal tissues that make up the heart. This is in contrast to secondary tumors of the heart, which are typically either metastatic from another part of the body, or infiltrate the heart via direct extension from the surrounding tissues.
History and Symptoms
Cardiac tumors present with a wide variety of symptoms. Many patients remain asymptomatic, and the tumor is an incidental finding. Some patients may present with symptoms of mimicking those of valve abnormalities such as mitral stenosis. Patients may also present with rhythm disturbances,endocarditis or even heart failure.
Physical Examination
A “tumor plop” (a sound related to movement of the tumor), abnormal heart sounds, or murmur may be heard. These sounds may change when the patient changes position.
Electrocardiogram
There are no specific ECG abnormalities associated with heart tumors. The ECG changes vary depending on the location of the tumor and aid in the diagnosis of tumors when used in conjunction with other diagnostic modalities.
Historical Perspective
As early as 1559, Dr. Realdo Colombo wrote about heart tumors, and the first successful surgery to remove a left atrial myxoma was performed in 1954 by Dr. Clarence Crafoord. After the discovery of cardiac tumors, new chemotherapeutic agents and treatments have been developed.
Classification
Based on their origin, cardiac tumors are classed as either primary or secondary. Primary cardiac tumors are classified as either benign, malignant, or intermediate.
Pathophysiology
Cardiac tumors’ exact pathogenesis remains an enigma. Some cardiac tumors are linked to genetic predispositions or are a part of syndromes.
- Cardiac rhabdomyomas are linked to “Tuberous sclerosis,” an autosomal dominant disorder characterized by the development of several organ hamartomas.
- Cardiac fibromas may be related with Gorlin syndrome, an autosomal dominant disorder characterized by congenital anomalies and a predisposition to tumorigenesis.
- Cardiac myxomas may be related with Carney complex, an autosomal dominant disorder.
- Histiocytoid cardiomyopathy is occasionally inherited, however the underlying genetic abnormalities are still unclear.
- The majority of undifferentiated cardiac sarcomas share the same genetic profile as pulmonary artery intimal sarcomas, which are defined by recurrent mutations in the MDM2, PDGFRA, and CDKN2A genes.
- Papillary fibroelastomas have been reported following cardiac instrumentation and thoracic irradiation.
Causes
Numerous genetic abnormalities are linked to cardiac tumors however no direct causes have been established as of yet. Some genetic disorders closely related with a high incidence of cardiac tumors are Tuberous Sclerosis, Gorlin Syndrome, and Carneys Triad.
Differentiating Cardiac Tumors from other Diseases
Common cardiac tumor symptoms include fever, weight loss, and other constitutional symptoms. Each tumor has unique traits that distinguish it from others.
Risk Factors
There are no recognized cardiac tumor risk factors. However, HIV increases the risk of Kaposi sarcoma of the heart. Certain disorders, including Gorlin syndrome, Tuberous Sclerosis, LAMB, NAME, and Paragangliomas, are linked to an elevated risk of cardiac tumors. The presence of other tumors also increases the risk of secondary tumors in heart
Screening
The USPSTF does not suggest screening for heart tumors routinely. Transthoracic echocardiography (TTE) is the preferred screening tool for cardiac cancers. Valvular lesions are frequently detected by Transesophageal echocardiography (TEE).
Natural History, Complications and Prognosis
Cardiac tumors can originate in numerous ways, resulting in a variety of clinical manifestations. Regardless of the type of heart tumor, cardiac symptoms depend mostly on tumor location and size. Patients with cardiac tumors can experience systemic constitutional symptoms, such as fever, tiredness, and joint issues. Depending on the location of tumors, particular symptoms may develop. The prognosis for benign cardiac tumors is good, but recurrence is possible, whereas the prognosis for malignant tumors is dismal.
Diagnosis
Multiple cardiovascular imaging techniques could be utilized to outline the anatomy of the cardiac mass and its potential functional consequences.
The primary purpose of cardiovascular imaging is to assess the location, extent, and vascularity of the tumor, as well as any hemodynamic consequences and myopericardial invasion.
All patients should receive two-dimensional transthoracic echocardiography (TTE). A biopsy provides the definitive diagnosis. The technique for a final diagnosis is carried out using percutaneous cardiac biopsy and transvenous cardiac biopsy, guided by echocardiography, mediastinoscopy, or thoracotomy.
Staging | History and Symptoms | Physical Examination | Laboratory Findings | Electrocardiogram | Chest X Ray | CT | MRI | Echocardiography | Other Imaging Findings | Other Diagnostic Studies
Treatment
The vast majority of cardiac tumors are treated surgically. Primary malignant cardiac tumors have a propensity for fast metastatic dissemination.
Systemic neoadjuvant therapy should be vigorously sought in hemodynamically stable patients with localized disease because it permits: (a) faster removal by lowering the size of the tumor, and (b) a reduction in the likelihood of systemic recurrence.
In certain instances, surgery may be an option for malignant tumors. Patients with a solitary heart problem and a controlled primary tumor are the best candidates. The tumor must be amenable to excision while preserving sufficient heart function to sustain life.
Medical Therapy | Surgery | Primary Prevention | Secondary Prevention | Cost-Effectiveness of Therapy | Future or Investigational Therapies
Case Studies
Case #1 | Case #2: Cardiac lymphoma
References
Historical Perspective
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Dheeraj Makkar, M.D.[2]
Overview
- Realdo Colombo initially reported cardiac tumors in 1559, and Dr. Clarence Crafoord performed the first successful surgical resection of left atrial myxoma in 1954. New chemotherapy drugs and treatment have been developing after the discovery of cardiac tumors.
Historical Perspective
- Cardiac Tumors were first described by Realdo Colombo in 1559.[1]
- In 1936, Beck and Maurer were the first to resect right ventricular teratoma. They also resected a left ventricular lipoma in 1951.[2]
- Dr. William Norris was the first to describe a “melanotic heart” with secondary metastases to the heart in 1820.[3]
- In 1952, left atrial myxoma was successfully excised by Bahnson and Newman through a right atriotomy. Unfortunately, the patient succumbed to the procedure after 24 days.[4]
Landmark events in the development of treatment strategies
- In 1954, Dr. Clarence Crafoord from Sweden reported the first successful removal of left atrial myxoma in a 40-year-old female presenting with dizziness and transient hemiparesis caused by myxoma.The patient survived for more than 40 years after her surgery.[1]
- Dr. Senning and his team developed perfusion system to ease cardiac surgeries. The Perfusion system comprised of hypothermia, flow, and ventricular fibrillation to prevent embolism.[1]
- In July 1954, they used it for the first time in the excision of left atrial myxoma, performed by Dr. Crafoord. This was a milestone surgery in developing Extracorporeal perfusion system.[1]
References
- ↑ 1.0 1.1 1.2 1.3 Chitwood WR (1992). “Clarence Crafoord and the first successful resection of a cardiac myxoma”. Ann Thorac Surg. 54 (5): 997–8. doi:10.1016/0003-4975(92)90676-u. PMID 1417305.
- ↑ Beck CS (1942). “AN INTRAPERICARDIAL TERATOMA AND A TUMOR OF THE HEART: BOTH REMOVED OPERATIVELY”. Ann Surg. 116 (2): 161–74. doi:10.1097/00000658-194208000-00001. PMC 1543811. PMID 17858078.
- ↑ Gibbs P, Cebon JS, Calafiore P, Robinson WA (1999). “Cardiac metastases from malignant melanoma”. Cancer. 85 (1): 78–84. PMID 9921977.
- ↑ BAHNSON HT, NEWMAN EV (1953). “Diagnosis and surgical removal of intracavitary myxoma of the right atrium”. Bull Johns Hopkins Hosp. 93 (3): 150–63. PMID 13094264.
Classification
Primary cardiac tumors | Secondary cardiac tumors
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Dheeraj Makkar, M.D.[2]
Overview
- Cardiac tumors are classified as either primary or secondary based on their origin.
- Primary tumors can be categorized as benign, malignant, or intermediate.
Classification
In 2015, the World Health Organization (WHO) changed the classification of cardiac neoplasms, including benign tumors, tumor-like lesions, malignant tumors, and pericardial tumors. [1]
- Now, cardiac tumors are categorized into primary and secondary.
| Cardiac Tumors | |||||||||||||||||||||||||||||||||||||||||||
| Primary | Secondary | ||||||||||||||||||||||||||||||||||||||||||
| Malignant | Benign | Intermediate | |||||||||||||||||||||||||||||||||||||||||
| Low grade Sarcoma/Myxofibroma | High Grade sarcoma/Undifferentiated Pleomorphic Sarcoma | ||||||||||||||||||||||||||||||||||||||||||
| Congenital | Childhood | Adult | |||||||||||||||||||||||||||||||||||||||||
| Neoplastic benign | Non-neoplastic | ||||||||||||||||||||||||||||||||||||||||||
Classification
Primary Cardiac Tumors
- Myxoma
- Papillary fibroelastoma
- Fibroma
- Rhabdomyoma
- Hemangioma
- Teratoma
- Lipoma
- Paraganglioma
- Pericardial cysts
- Rhabdomyosarcoma
Secondary Cardiac Tumors
- The Heart in Breast Cancer
- The Heart in Central and Peripheral Nervous System Cancers
- The Heart in Gastrointestinal, Hepatobilier & Pancreatic Tumors
- The Heart in Gynecologic Tumors
- The Heart in Head and Neck Tumors
- The Heart in Leukemias
- The Heart in Lung Cancers
- The Heart in Lymphomas
- The Heart in Multiple Myeloma
- The Heart in Osteosarcomas
- The Heart in Peritoneal and Mesothelial Tumors
- The Heart in Skin Cancers
- The Heart in Thyroid and Parathyroid Cancers
- The Heart in Urinary System Tumors
- The Heart in Tumors that Originated from Vascular Structure
- The Heart in Primary Myocardial Tumors
References
- ↑ Travis WD, Brambilla E, Nicholson AG, Yatabe Y, Austin JHM, Beasley MB; et al. (2015). “The 2015 World Health Organization Classification of Lung Tumors: Impact of Genetic, Clinical and Radiologic Advances Since the 2004 Classification”. J Thorac Oncol. 10 (9): 1243–1260. doi:10.1097/JTO.0000000000000630. PMID 26291008.
Pathophysiology
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-In-Chief: Cafer Zorkun, M.D., Ph.D. [2]; Varun Kumar, M.B.B.S. Dheeraj Makkar, M.D.[3]
Overview
The precise pathophysiology of cardiac tumors is unknown. Some cardiac tumors are associated with genetic predispositions or are components of genetic disorders.
- Cardiac rhabdomyomas are associated with Tuberous sclerosis, an autosomal dominant condition characterized by the development of various organ hamartomas.
- Cardiac fibromas may be associated with Gorlin syndrome, an autosomal dominant condition marked by congenital abnormalities and a propensity for neoplasia.
- Cardiac myxomas may be associated with the autosomal dominant condition Carney complex.
- Histiocytoid cardiomyopathy is sometimes inherited, however the underlying genetic disorders remain unknown.
- Most cardiac undifferentiated sarcomas share the same genetic profile as pulmonary artery intimal sarcomas, characterized by recurrent mutations in the MDM2, PDGFRA, and CDKN2A genes.
- There have been reports of papillary fibroelastomas following cardiac instrumentation and thoracic irradiation.
Pathophysiology
| Tumor | Macroscopic appearance | Microscopic appearance | Remarks |
|---|---|---|---|
| Myxoma(Images B, C) | Two Types Solid(round with a smooth, lustrous, undulating surface)/Villous(frequently fragile papillary surfaces) | Cells have eosinophilic cytoplasm and an oval or round nucleus. | Embolization is frequent.[1] |
| Cardiac Lipoma | Isolated lumps that are yellow, soft, smooth, well-circumscribed, and encapsulated | Fat cells exhibit minimal to no atypia, fibrous capsule | They can cause arrhythmias or conduction system disorders and heart failure symptoms.[2] |
| Papillary fibroelastoma(Images F,G) | Round, whitish appearance and soft consistency, sea anemone-like” appearance[3] | Thin avascular papillary fronds that frequently display complicated branching | Embolization is frequent.
|
| Rhabdomyomas | Nodular, unencapsulated, whitish, or grey, range in size from millimeters to several centimeters | Large vacuolated cells with transparent cytoplasm due to glycogen deposition, spider cells also present | Heart block or ventricular tachyarrhythmias, ventricular tachyarrhythmias may develop[4]
|
| Cardiac Fibromas(Image D) | Solitary well-defined formation, | Monomorphic fibroblasts exhibiting minimal or no atypia *Resembles fibromatosis or uterine leiomyomas | May manifest like heart failure, ventricular tachyarrhythmia, Can present as Sudden Cardiac Death[5]
|
| Angiosarcoma | Darkish brown or black hemorrhagic aggregates with invading margins | Vascular conduits, infiltrating cardiac muscle, anastomosing, uneven, *Pleomorphic lining cells displaying numerous mitotic figures[6] | Most commonly involves right atrium |
| Secondary Cardiac Tumors(Image A) | Direct tumor infiltration from the mediastinum or hematogenous spread[7] | Same as underlying Malignancy | Pericardial effusion is one of the most frequent findings in individuals with secondary tumors.
|
Papillary fibroelastoma
- Primary tumor of the heart that typically involves one of the valves of the heart
- Papillary fibroelastoma is generally considered benign, and represents 10% of all primary tumors of the heart
- Papillary fibroelastoma are the third most common type of primary tumor of the heart, behind cardiac myxomas and cardiac fibromas.[8]
- The pathogenesis of papillary fibroelastoma is characterised by the mechanical effects of the tumor and the transient occlusion of the left main coronary artery (by the tumor), while a heart attack or sudden cardiac death may be due to embolisation of a portion of the tumor into a coronary artery.[9]
Gross Pathology
Image shown below is courtesy of Professor Peter Anderson DVM PhD and published with permission. © PEIR, University of Alabama at Birmingham, Department of Pathology
-
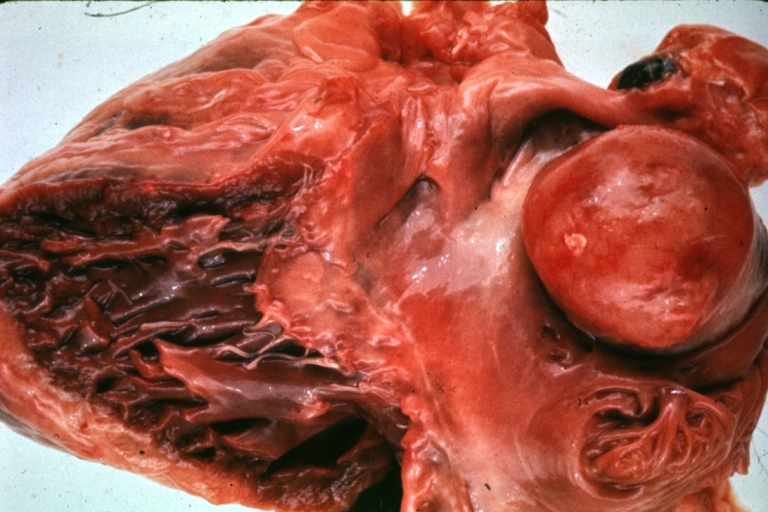 Image A HEART: Metastatic Tumor: Gross very unusual large metastatic carcinoid in right atrium
Image A HEART: Metastatic Tumor: Gross very unusual large metastatic carcinoid in right atrium -
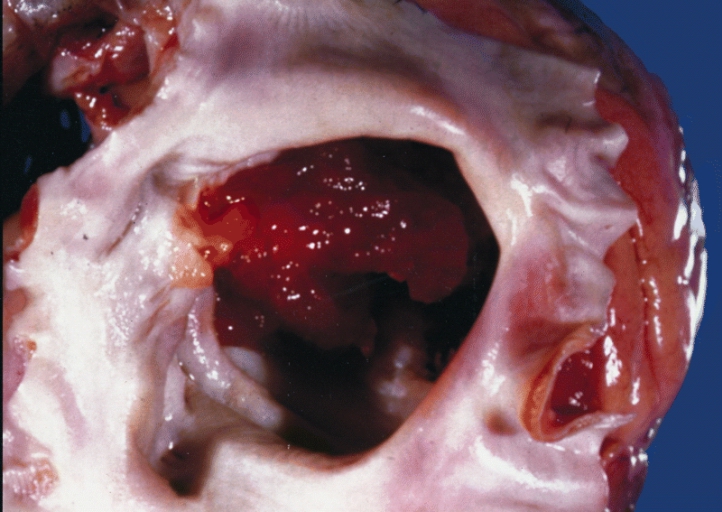 Image B Cardiac Myxoma A gelatinous tumor is attached by a narrow pedicle to the atrial septum. The myxoma has an irregular surface and nearly fills the left atrium.
Image B Cardiac Myxoma A gelatinous tumor is attached by a narrow pedicle to the atrial septum. The myxoma has an irregular surface and nearly fills the left atrium.


-
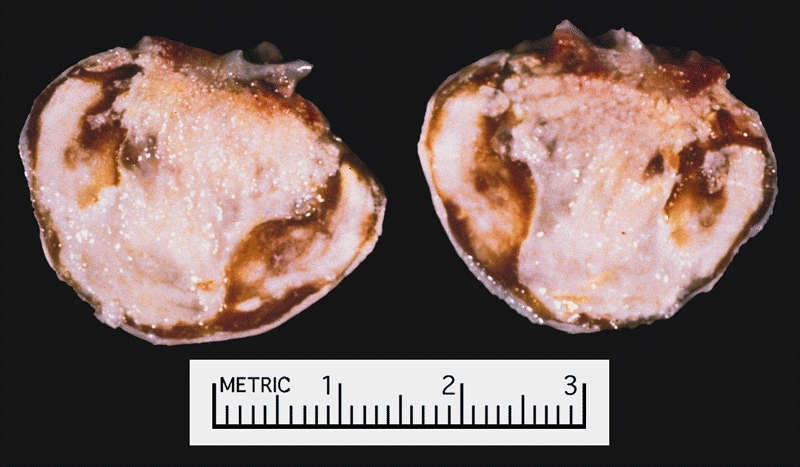 Image C Cardiac Myxoma There was a calcified right atrial mass on the X ray of a 47-year-old man. Resection demonstrated a smooth-surfaced tumor. The gritty material seen microscopically on cut section was calcified and ossified myxoma.
Image C Cardiac Myxoma There was a calcified right atrial mass on the X ray of a 47-year-old man. Resection demonstrated a smooth-surfaced tumor. The gritty material seen microscopically on cut section was calcified and ossified myxoma. -
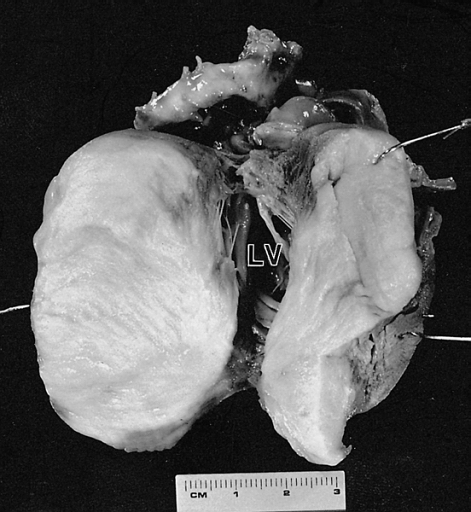 Image D Cardiac Fibroma Cut surface of the tumor shown in figure 6-2. The left ventricular (LV) cavity is present behind the mass. The patient was a 4-month-old child who died suddenly without a previous medical history.
Image D Cardiac Fibroma Cut surface of the tumor shown in figure 6-2. The left ventricular (LV) cavity is present behind the mass. The patient was a 4-month-old child who died suddenly without a previous medical history.


-
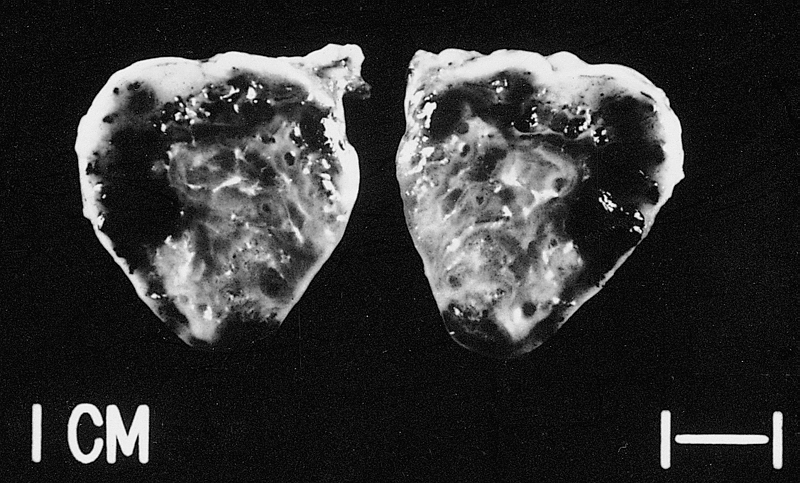 Image E This tumor was resected from the right atrium of a 1-year-old boy with pericardial effusions. Note areas of hemorrhage and dilated vessels. The patient was well 49 months postoperatively.
Image E This tumor was resected from the right atrium of a 1-year-old boy with pericardial effusions. Note areas of hemorrhage and dilated vessels. The patient was well 49 months postoperatively. -
 Image F Papillary fibroelastomas are often on the arterial surface and may project into the coronary ostium, causing ostial occlusion. This tumor is in the noncoronary sinus.
Image F Papillary fibroelastomas are often on the arterial surface and may project into the coronary ostium, causing ostial occlusion. This tumor is in the noncoronary sinus. -
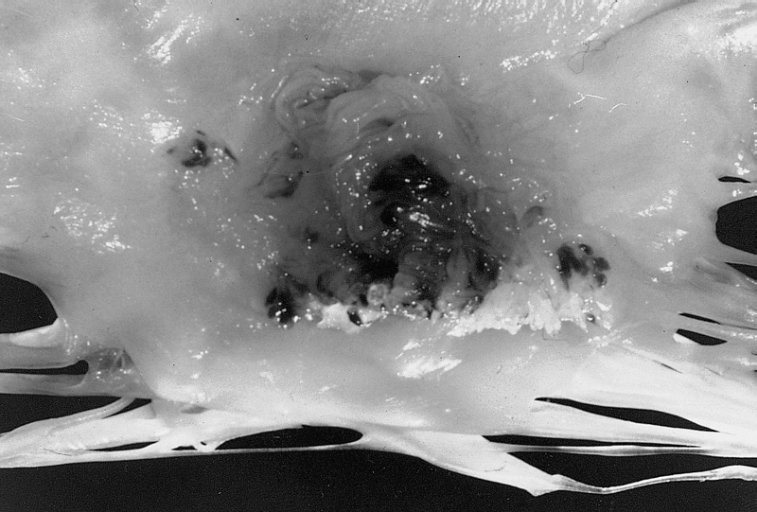 Image G Papillary Fibroelastoma: When located on the mitral valve, these tumors are usually on the anterior leaflet of the atrial surface.
Image G Papillary Fibroelastoma: When located on the mitral valve, these tumors are usually on the anterior leaflet of the atrial surface.



References
- ↑ Pinede L, Duhaut P, Loire R (2001). “Clinical presentation of left atrial cardiac myxoma. A series of 112 consecutive cases”. Medicine (Baltimore). 80 (3): 159–72. doi:10.1097/00005792-200105000-00002. PMID 11388092.
- ↑ Benvenuti LA, Mansur AJ, Lopes DO, Campos RV (1996). “Primary lipomatous tumors of the cardiac valves”. South Med J. 89 (10): 1018–20. doi:10.1097/00007611-199610000-00020. PMID 8865802.
- ↑ Burke A, Tavora F (2016). “The 2015 WHO Classification of Tumors of the Heart and Pericardium”. J Thorac Oncol. 11 (4): 441–52. doi:10.1016/j.jtho.2015.11.009. PMID 26725181.
- ↑ Basso C, Valente M, Poletti A, Casarotto D, Thiene G (1997). “Surgical pathology of primary cardiac and pericardial tumors”. Eur J Cardiothorac Surg. 12 (5): 730–7, discussion 737-8. doi:10.1016/s1010-7940(97)00246-7. PMID 9458144.
- ↑ Pacini D, Careddu L, Pantaleo A, Berretta P, Leone O, Marinelli G; et al. (2012). “Primary benign cardiac tumours: long-term results”. Eur J Cardiothorac Surg. 41 (4): 812–9. doi:10.1093/ejcts/ezr067. PMID 22219403.
- ↑ Orlandi A, Ferlosio A, Roselli M, Chiariello L, Spagnoli LG (2010). “Cardiac sarcomas: an update”. J Thorac Oncol. 5 (9): 1483–9. doi:10.1097/JTO.0b013e3181e59a91. PMID 20651614.
- ↑ Fred HL, van Dijk HA (2017). “Cardiac Metastases from Malignant Melanoma: The “Charcoal Heart““. Methodist Debakey Cardiovasc J. 13 (4): 254–255. doi:10.14797/mdcj-13-4-254. PMC 5935287. PMID 29744020.
- ↑ Matsumoto N, Sato Y, Kusama J, Matsuo S, Kinukawa N, Kunimasa T, Ichiyama I, Takahashi H, Kimura S, Orime Y, Saito S. (2007). “Multiple papillary fibroelastomas of the aortic valve: case report”. Int J Cardiol. 122 (1): e1–3. PMID 17196273.
- ↑ Takada A, Saito K, Ro A, Tokudome S, Murai T. (2000). “Papillary fibroelastoma of the aortic valve: a sudden death case of coronary embolism with myocardial infarction”. Forensic Sci Int. 113 (1–3): 209–14. PMID 10978627.
Causes
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Dheeraj Makkar, M.D.[2]
Overview
- Numerous genetic disorders are associated with cardiac tumors however, till now no direct causes have been identified.
Causes
- Many genetic conditions are strongly associated with a large number of heart tumors. Some of them are as follows:[1]
| Tumor | Syndrome | Gene Associated with syndrome |
|---|---|---|
| Rhabdomyoma | Tuberous Sclerosis | TSC1 or hamartin
TSC2 or tuberin |
| Fibroma | Gorlin Syndrome | PATCHED gene |
| Myxoma | Carney Complex | Inactivating mutation of PRKARA1A
Activating pathogenic variant of PRKACA gene |
| Paraganglioma | Carney triad | No known gene associations |
| Paraganglioma | Hereditary Paraganglioma | Mutation of succinate dehydrogenase subunit
SDHAF2 gene, and possibly MAX gene but these mutations are rare |
| Paraganglioma | Von Hippel Lindau | VHL gene |
| Paraganglioma | Neurofibromatosis type 1 | NF1 gene |
References
- ↑ Lee E, Mahani MG, Lu JC, Dorfman AL, Srinivasan A, Agarwal PP (2018). “Primary cardiac tumors associated with genetic syndromes: a comprehensive review”. Pediatr Radiol. 48 (2): 156–164. doi:10.1007/s00247-017-4027-2. PMID 29214333.
Differentiating Cardiac Tumors from other Diseases
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1] Associate Editor(s)-in-Chief: Syed Hassan A. Kazmi BSc, MD [2]
Overview
- The cardiac tumors have some common features like fever, weight loss, and other constitutional symptoms. Each tumor has its peculiar characteristics that sets it apart from other tumors.
Differenting Cardiac Tumors from Other Diseases
- Primary cardiac tumors have been divided into two categories: benign and malignant.
- Both benign and malignant tumors can be differentiated based on age of presentation, location, morphological features on echocardiography and MRI findings.
- Cardiac MRI is the most useful assessment tool.[1]
| Benign | Malignant |
|---|---|
| Myxoma | Rhabdomyosarcoma |
| Rhabdomyoma | Angiosarcoma |
| Fibroelastoma | Fibrosarcoma |
| Cardiac Lipoma | Lymphoma |
| Cardiac Hemangioma | |
| Cardiac Fibroma | |
| Atrioventricular tumors | |
| Paragangliomas |
Differential Diagnosis of Cardiac Mass
Cardiac tumors present as a cardiac mass on imaging. The following are the differentials of cardiac mass:[2][3][4][5][6][7][8][9][10][11][12][13][14][15][16][17][18][19][20][21][22][23][24][25][26][27][28][29][30][31][32][33][34][35][36][37][38][39][40][41][42][43][44][45][46][47][48]
| Site of Tumor | Malignant Potential | Type of Tumor | Tissue of Origin | Age of Presentation | Location | Morphology | Signs and Symptoms | MRI Findings | ||
|---|---|---|---|---|---|---|---|---|---|---|
| Systemic Manifestations | Cardiac Manifestations | Embolic Manifestations | ||||||||
| Primary Cardiac Tumor | Primary Benign | Myxoma |
|
|
|
|
|
| ||
| Rhabdomyoma |
|
|
|
|
| |||||
| Fibroma |
|
|
|
| ||||||
| Fibroelastoma |
|
|
|
|
| |||||
| Hemangioma |
|
|
|
|
| |||||
| Lipoma |
|
|
|
|
| |||||
| Paraganglioma |
|
|
|
|
|
|
|
| ||
| Atrioventricular Node Tumor |
|
|
|
|
|
| ||||
| Lipomatous hypertrophy of the interatrial septum |
|
|
|
|
– |
| ||||
| Primary Malignant | Fibrosarcoma |
|
|
|
|
|
| |||
| Angiosarcoma |
|
|
|
| ||||||
| Rhabdomyosarcoma |
|
|
|
| ||||||
| Lymphoma |
|
|
|
|
| |||||
| Secondary Cardiac Tumor | Metastastatic Malignant | Metastasis |
|
|
|
|
| |||
References
- ↑ Hoffmeier A, Sindermann JR, Scheld HH, Martens S (2014). “Cardiac tumors–diagnosis and surgical treatment”. Dtsch Arztebl Int. 111 (12): 205–11. doi:10.3238/arztebl.2014.0205. PMC 3983698. PMID 24717305.
- ↑ Mankad R, Herrmann J (December 2016). “Cardiac tumors: echo assessment”. Echo Res Pract. 3 (4): R65–R77. doi:10.1530/ERP-16-0035. PMC 5292983. PMID 27600455.
- ↑ Zaragoza-Macias E, Zaragosa-Macias E, Chen MA, Gill EA (February 2012). “Real time three-dimensional echocardiography evaluation of intracardiac masses”. Echocardiography. 29 (2): 207–19. doi:10.1111/j.1540-8175.2011.01627.x. PMID 22283202.
- ↑ Larrieu AJ, Jamieson WR, Tyers GF, Burr LH, Munro AI, Miyagishima RT, Gerein AN, Allen P (March 1982). “Primary cardiac tumors: experience with 25 cases”. J. Thorac. Cardiovasc. Surg. 83 (3): 339–48. PMID 7062746.
- ↑ Molina JE, Edwards JE, Ward HB (August 1990). “Primary cardiac tumors: experience at the University of Minnesota”. Thorac Cardiovasc Surg. 38 Suppl 2: 183–91. doi:10.1055/s-2007-1014064. PMID 2237900.
- ↑ Tazelaar HD, Locke TJ, McGregor CG (October 1992). “Pathology of surgically excised primary cardiac tumors”. Mayo Clin. Proc. 67 (10): 957–65. PMID 1434856.
- ↑ Sarjeant JM, Butany J, Cusimano RJ (2003). “Cancer of the heart: epidemiology and management of primary tumors and metastases”. Am J Cardiovasc Drugs. 3 (6): 407–21. doi:10.2165/00129784-200303060-00004. PMID 14728061.
- ↑ St John Sutton MG, Mercier LA, Giuliani ER, Lie JT (June 1980). “Atrial myxomas: a review of clinical experience in 40 patients”. Mayo Clin. Proc. 55 (6): 371–6. PMID 7382545.
- ↑ Pinede L, Duhaut P, Loire R (May 2001). “Clinical presentation of left atrial cardiac myxoma. A series of 112 consecutive cases”. Medicine (Baltimore). 80 (3): 159–72. PMID 11388092.
- ↑ Reynen K (December 1995). “Cardiac myxomas”. N. Engl. J. Med. 333 (24): 1610–7. doi:10.1056/NEJM199512143332407. PMID 7477198.
- ↑ Javed A, Zalawadiya S, Kovach J, Afonso L (March 2014). “Aortic valve myxoma at the extreme age: a review of literature”. BMJ Case Rep. 2014. doi:10.1136/bcr-2013-202689. PMC 3962858. PMID 24642215.
- ↑ Lee VH, Connolly HM, Brown RD (August 2007). “Central nervous system manifestations of cardiac myxoma”. Arch. Neurol. 64 (8): 1115–20. doi:10.1001/archneur.64.8.1115. PMID 17698701.
- ↑ Carney JA, Gordon H, Carpenter PC, Shenoy BV, Go VL (July 1985). “The complex of myxomas, spotty pigmentation, and endocrine overactivity”. Medicine (Baltimore). 64 (4): 270–83. PMID 4010501.
- ↑ McAllister HA, Hall RJ, Cooley DA (February 1999). “Tumors of the heart and pericardium”. Curr Probl Cardiol. 24 (2): 57–116. PMID 10028128.
- ↑ Klarich KW, Enriquez-Sarano M, Gura GM, Edwards WD, Tajik AJ, Seward JB (September 1997). “Papillary fibroelastoma: echocardiographic characteristics for diagnosis and pathologic correlation”. J. Am. Coll. Cardiol. 30 (3): 784–90. PMID 9283541.
- ↑ Tamin SS, Maleszewski JJ, Scott CG, Khan SK, Edwards WD, Bruce CJ, Oh JK, Pellikka PA, Klarich KW (June 2015). “Prognostic and Bioepidemiologic Implications of Papillary Fibroelastomas”. J. Am. Coll. Cardiol. 65 (22): 2420–9. doi:10.1016/j.jacc.2015.03.569. PMID 26046736.
- ↑ Gowda RM, Khan IA, Nair CK, Mehta NJ, Vasavada BC, Sacchi TJ (September 2003). “Cardiac papillary fibroelastoma: a comprehensive analysis of 725 cases”. Am. Heart J. 146 (3): 404–10. doi:10.1016/S0002-8703(03)00249-7. PMID 12947356.
- ↑ Beghetti M, Gow RM, Haney I, Mawson J, Williams WG, Freedom RM (December 1997). “Pediatric primary benign cardiac tumors: a 15-year review”. Am. Heart J. 134 (6): 1107–14. PMID 9424072.
- ↑ Smythe JF, Dyck JD, Smallhorn JF, Freedom RM (November 1990). “Natural history of cardiac rhabdomyoma in infancy and childhood”. Am. J. Cardiol. 66 (17): 1247–9. PMID 2239731.
- ↑ Jacobs JP, Konstantakos AK, Holland FW, Herskowitz K, Ferrer PL, Perryman RA (November 1994). “Surgical treatment for cardiac rhabdomyomas in children”. Ann. Thorac. Surg. 58 (5): 1552–5. PMID 7979700.
- ↑ Elbardissi AW, Dearani JA, Daly RC, Mullany CJ, Orszulak TA, Puga FJ, Schaff HV (September 2008). “Survival after resection of primary cardiac tumors: a 48-year experience”. Circulation. 118 (14 Suppl): S7–15. doi:10.1161/CIRCULATIONAHA.107.783126. PMID 18824772.
- ↑ Basu S, Folliguet T, Anselmo M, Greengart A, Sabado M, Cunningham JN, Jacobowitz IJ (April 1994). “Lipomatous hypertrophy of the interatrial septum”. Cardiovasc Surg. 2 (2): 229–31. PMID 8049952.
- ↑ Simpson L, Kumar SK, Okuno SH, Schaff HV, Porrata LF, Buckner JC, Moynihan TJ (June 2008). “Malignant primary cardiac tumors: review of a single institution experience”. Cancer. 112 (11): 2440–6. doi:10.1002/cncr.23459. PMID 18428209.
- ↑ Vander Salm TJ (April 2000). “Unusual primary tumors of the heart”. Semin. Thorac. Cardiovasc. Surg. 12 (2): 89–100. PMID 10807431.
- ↑ Petersen CD, Robinson WA, Kurnick JE (1976). “Involvement of the heart and pericardium in the malignant lymphomas”. Am. J. Med. Sci. 272 (2): 161–5. PMID 1008078.
- ↑ Ragland MM, Tak T (March 2006). “The role of echocardiography in diagnosing space-occupying lesions of the heart”. Clin Med Res. 4 (1): 22–32. PMC 1447535. PMID 16595790.
- ↑ Miguel CE, Bestetti RB (June 2011). “Primary cardiac lymphoma”. Int. J. Cardiol. 149 (3): 358–63. doi:10.1016/j.ijcard.2010.02.016. PMID 20227122.
- ↑ Grebenc ML, Rosado de Christenson ML, Burke AP, Green CE, Galvin JR (2000). “Primary cardiac and pericardial neoplasms: radiologic-pathologic correlation”. Radiographics. 20 (4): 1073–103, quiz 1110–1, 1112. doi:10.1148/radiographics.20.4.g00jl081073. PMID 10903697.
- ↑ Grinda JM, Couetil JP, Chauvaud S, D’Attellis N, Berrebi A, Fabiani JN, Deloche A, Carpentier A (January 1999). “Cardiac valve papillary fibroelastoma: surgical excision for revealed or potential embolization”. J. Thorac. Cardiovasc. Surg. 117 (1): 106–10. PMID 9869763.
- ↑ Webb DW, Thomas RD, Osborne JP (March 1993). “Cardiac rhabdomyomas and their association with tuberous sclerosis”. Arch. Dis. Child. 68 (3): 367–70. PMC 1793857. PMID 8466239.
- ↑ Yoshitake I, Hata M, Sezai A, Niino T, Unosawa S, Shimura K, Kasamaki Y, Minami K (September 2009). “Cardiac angiosarcoma with cardiac tamponade diagnosed as a ruptured aneurysm of the sinus valsalva”. Jpn. J. Clin. Oncol. 39 (9): 612–5. doi:10.1093/jjco/hyp044. PMID 19493870.
- ↑ Parissis H, Akbar MT, Young V (October 2010). “Primary leiomyosarcoma of the right atrium: a case report and literature update”. J Cardiothorac Surg. 5: 80. doi:10.1186/1749-8090-5-80. PMC 2964688. PMID 20939891.
- ↑ Gulati G, Sharma S, Kothari SS, Juneja R, Saxena A, Talwar KK (2004). “Comparison of echo and MRI in the imaging evaluation of intracardiac masses”. Cardiovasc Intervent Radiol. 27 (5): 459–69. doi:10.1007/s00270-004-0123-4. PMID 15383848.
- ↑ Narin B, Arman A, Arslan D, Simşek M, Narin A (February 2010). “Assessment of cardiac masses: magnetic resonance imaging versus transthoracic echocardiography”. Anadolu Kardiyol Derg. 10 (1): 69–74. PMID 20150010.
- ↑ “academic.oup.com”.
- ↑ Ismail I, Al-Khafaji K, Mutyala M, Aggarwal S, Cotter W, Hakim H, Khosla S, Arora R (2015). “Cardiac lipoma”. J Community Hosp Intern Med Perspect. 5 (5): 28449. doi:10.3402/jchimp.v5.28449. PMC 4612478. PMID 26486106.
- ↑ D’Souza J, Shah R, Abbass A, Burt JR, Goud A, Dahagam C (January 2017). “Invasive Cardiac Lipoma: a case report and review of literature”. BMC Cardiovasc Disord. 17 (1): 28. doi:10.1186/s12872-016-0465-2. PMC 5237479. PMID 28088193.
- ↑ Yadav, Pradeep K.; Baquero, Giselle A.; Malysz, Jozef; Kelleman, John; Gilchrist, Ian C. (2014). “Cardiac Paraganglioma”. Circulation: Cardiovascular Interventions. 7 (6): 851–856. doi:10.1161/CIRCINTERVENTIONS.114.001856. ISSN 1941-7640.
- ↑ Tahir M, Noor SJ, Herle A, Downing S (2009). “Right atrial paraganglioma: a rare primary cardiac neoplasm as a cause of chest pain”. Tex Heart Inst J. 36 (6): 594–7. PMC 2801953. PMID 20069088.
- ↑ Hamilton BH, Francis IR, Gross BH, Korobkin M, Shapiro B, Shulkin BL, Deeb CM, Orringer MB (January 1997). “Intrapericardial paragangliomas (pheochromocytomas): imaging features”. AJR Am J Roentgenol. 168 (1): 109–13. doi:10.2214/ajr.168.1.8976931. PMID 8976931.
- ↑ Shih, Wei-Jen; McCullough, Scott; Smith, Mary (1993). “Diagnostic imagings for primary cardiac fibrosarcoma”. International Journal of Cardiology. 39 (2): 157–161. doi:10.1016/0167-5273(93)90028-F. ISSN 0167-5273.
- ↑ Arai T, Kurashima C, Wada S, Chida K, Ohkawa S (November 1998). “Histological evidence for cell proliferation activity in cystic tumor (endodermal heterotopia) of the atrioventricular node”. Pathol. Int. 48 (11): 917–23. PMID 9832064.
- ↑ Wolf PL, Bing R (November 1965). “The smallest tumor which causes sudden death”. JAMA. 194 (6): 674–5. PMID 5897246.
- ↑ Burke AP, Anderson PG, Virmani R, James TN, Herrera GA, Ceballos R (October 1990). “Tumor of the atrioventricular nodal region. A clinical and immunohistochemical study”. Arch. Pathol. Lab. Med. 114 (10): 1057–62. PMID 2222148.
- ↑ Burke A, Tavora F (April 2016). “The 2015 WHO Classification of Tumors of the Heart and Pericardium”. J Thorac Oncol. 11 (4): 441–52. doi:10.1016/j.jtho.2015.11.009. PMID 26725181.
- ↑ Tran, Thao T; Starnes, Vaughn; Wang, Xuedong; Getzen, James; Ross, Brian D (2009). “Cardiovascular magnetics resonance diagnosis of cystic tumor of the atrioventricular node”. Journal of Cardiovascular Magnetic Resonance. 11 (1): 13. doi:10.1186/1532-429X-11-13. ISSN 1532-429X.
- ↑ Tatli, Servet; O’Gara, Patrick Thomas; Lambert, Jarvis; Kwong, Raymond; Byrne, John Gerald; Yucel, E. Kent (2004). “MRI of Atypical Lipomatous Hypertrophy of the Interatrial Septum”. American Journal of Roentgenology. 182 (3): 598–600. doi:10.2214/ajr.182.3.1820598. ISSN 0361-803X.
- ↑ Saboo, Sachin S.; Krajewski, Katherine M.; Zukotynski, Katherine; Howard, Stephanie; Jagannathan, Jyothi P.; Hornick, Jason L.; Ramaiya, Nikhil (2012). “Imaging Features of Primary and Secondary Adult Rhabdomyosarcoma”. American Journal of Roentgenology. 199 (6): W694–W703. doi:10.2214/AJR.11.8213. ISSN 0361-803X.
Epidemiology and Demographics
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-In-Chief: Cafer Zorkun, M.D., Ph.D. [2]; Varun Kumar, M.B.B.S. Dheeraj Makkar, M.D.[3]
Overview
The rates of primary and secondary cardiac tumors were 0.056 and 1.23 percent, respectively, as determined by autopsy. Lung, esophageal, and lymphoma metastases are the three most prevalent malignant neoplasms impacting the heart. Nearly 90% of primary cardiac tumors are benign. Extracardiac tumors are 20–40 times greater probable than primary cardiac tumors to cause secondary heart involvement. A primary intracardiac tumor may be responsible for less than 1 percent of cardiovascular fatalities.
Epidemiology and Demographics
Prevalence
- Prevalence in autopsy series: 1/300 to 1/5900
- 80% of primary tumors are benign:
- 1/2 (40%) are myxomas
- 1/2 (40% ) are of other types
Benign Tumors of the Heart
- The most common primary tumor of the heart is the myxoma.
- Makes up as much as 77% of all primary tumors of the heart.[1] Other benign tumors of the heart include rhabdomyomas, fibromas, hemangiomas, lipomas, paragangliomas, myocytic hamartomas, and papillary fibroelastomas[2].
Primary Malignant Tumors of the Heart
About 20 percent of primary tumors of the heart are malignant in nature.[1]
- Malignant tumors of the heart include rhabdomyosarcomas, angiosarcomas, myxosarcomas, fibrosarcomas, leiomyosarcomas, reticulum cell sarcomas, and liposarcomas.
- The cardiac sarcomas may occur at any age, but are more commonly seen in individuals in their 20s to 40s.
- They occur equally in males and females.
Tumors of the Valve
A subset of the primary tumors of the heart are tumors that are found on the valves of the heart.
- Tumors that affect the valves of the heart are found in an equal distribution among the four heart valves.[2] The vast majority of these are papillary fibroelastomas.
- Primary tumors of the valves of the heart are more likely to occur in males.
- The primary tumors of the valves of the heart are mainly benign.
- The symptoms related to the valve, include neurologic symptoms and (in a few cases) sudden cardiac death.
Secondary (Metastatic) Malignant Tumors of the Heart
- 20 to 40x more common than primary cardiac tumors
- Typically carcinomas, melanomas, and leukemias/lymphomas
- Discrete tumors found in 10 to 12% of all autopsies
- Any involvement of heart by a malignancy found in 20% of all autopsies
References
- ↑ 1.0 1.1 Molina JE, Edwards JE, Ward HB (1990). “Primary cardiac tumors: Experience at the University of Minnesota”. Thorac Cardiovasc Surg. 38 Suppl 2: 183–91. PMID 2237900.
- ↑ 2.0 2.1 Edwards FH, Hale D, Cohen A, Thompson L, Pezzella AT, Virmani R. (1991). “Primary cardiac valve tumors”. Ann Thorac Surg. 52 (5): 1127–31. PMID 1953134.
Risk Factors
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Dheeraj Makkar, M.D.[2]
Overview
There are no direct risk factors for cardiac tumors. Most of them are sporadic but some are associated with certain syndromes and can be congenital.
Risk Factors
- There are no established risk factors for Cardiac tumors. But HIV predisposes to formation of Kaposi Sarcoma of heart.[1]
- Certain syndromes like Gorlin syndrome, Tuberous Sclerosis, LAMB, NAME, and Paragangliomas are associated with increased risk of cardiac tumors.[2]
- The presence of lung carcinoma, breast carcinoma, esophageal carcinoma, malignant lymphoma, malignant melanoma, and leukemia are risk factors for secondary cardiac tumors due to their propensity to spread to the heart. Renal Cell Carcinoma spreads to heart mainly via Inferior Vena Cava.[3]
- Malignant Melanoma has the most significant predisposition for hematogenous spread to the heart among all the tumors.[3]
Factors affecting Prognosis
- There are definitive risk factors influencing the prognosis of patients afflicted with cardiac tumors.
- The independent risk factors associated with poor prognosis of cardiac tumors include, conservative management, malignant nature of tumor, and ”biatrial” tumors.[4]
- It is also important to note that features like age, sex, NYHA grading, leg edema, and peripheral embolism do not affect the longevity of patients with cardiac tumors. [4]
References
- ↑ Ghosn J, Taiwo B, Seedat S, Autran B, Katlama C (2018). “HIV”. Lancet. 392 (10148): 685–697. doi:10.1016/S0140-6736(18)31311-4. PMID 30049419.
- ↑ Lee E, Mahani MG, Lu JC, Dorfman AL, Srinivasan A, Agarwal PP (2018). “Primary cardiac tumors associated with genetic syndromes: a comprehensive review”. Pediatr Radiol. 48 (2): 156–164. doi:10.1007/s00247-017-4027-2. PMID 29214333.
- ↑ 3.0 3.1 Reynen K, Köckeritz U, Strasser RH (2004). “Metastases to the heart”. Ann Oncol. 15 (3): 375–81. doi:10.1093/annonc/mdh086. PMID 14998838.
- ↑ 4.0 4.1 Maimaitiaili A, Zhang WM, Guo YZ, Elmaik D, Tang NH, Zhang ZG (2019). “Survival of Patients with Primary Cardiac Tumors in an 11-Year Single Center Study”. Heart Surg Forum. 22 (2): E097–E102. doi:10.1532/hsf.2271. PMID 31013217.
Screening
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Dheeraj Makkar, M.D.[2]
Overview
There are no screening guidelines by USPSTF for cardiac tumors.
Screening
- According to the USPSTF, routine screening for cardiac tumors is not recommended.
- Transthoracic echocardiography (TTE) continues to be the method of choice for screening for cardiac malignancies. Transesophageal echocardiogram (TEE) is commonly used for valvular lesions.[1]
- Emerging technologies such as contrast echocardiography and three-dimensional echocardiogram may substantially improve the diagnostic accuracy of echocardiography.[2]
- The diagnostic accuracy of echocardiography is 80%. After initial diagnosis on TTE, cardiac CT/MRI are commonly used to stage and further evaluate the tumors.[3]
- In patients undergoing myxoma resection, routine echocardiography screening must be performed one year following removal of myxoma and then every five years.[1]
- Pediatric patients with tuberous sclerosis require monitoring because of the risk of rhabdomyoma.
- At the initial diagnosis, electrocardiograms and echocardiography must be performed on all kids with tuberous sclerosis.
- Periodic monitoring of electrocardiograms are advised every three to five years due to the lifetime risk of arrhythmia regardless of the presence early-onset cardiac rhabdomyoma. [4]
References
- ↑ 1.0 1.1 Lamba G, Frishman WH (2012). “Cardiac and pericardial tumors”. Cardiol Rev. 20 (5): 237–52. doi:10.1097/CRD.0b013e31825603e7. PMID 22447042.
- ↑ Mankad R, Herrmann J (2016). “Cardiac tumors: echo assessment”. Echo Res Pract. 3 (4): R65–R77. doi:10.1530/ERP-16-0035. PMC 5292983. PMID 27600455.
- ↑ Nomoto N, Tani T, Konda T, Kim K, Kitai T, Ota M; et al. (2017). “Primary and metastatic cardiac tumors: echocardiographic diagnosis, treatment and prognosis in a 15-years single center study”. J Cardiothorac Surg. 12 (1): 103. doi:10.1186/s13019-017-0672-7. PMC 5704631. PMID 29183343.
- ↑ Hinton RB, Prakash A, Romp RL, Krueger DA, Knilans TK, International Tuberous Sclerosis Consensus Group (2014). “Cardiovascular manifestations of tuberous sclerosis complex and summary of the revised diagnostic criteria and surveillance and management recommendations from the International Tuberous Sclerosis Consensus Group”. J Am Heart Assoc. 3 (6): e001493. doi:10.1161/JAHA.114.001493. PMC 4338742. PMID 25424575.
Natural History, Complications and Prognosis
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-In-Chief: Cafer Zorkun, M.D., Ph.D. [2] Dheeraj Makkar, M.D.[3]
Overview
Patients with heart tumors may develop systemic constitutional symptoms like fever, fatigue, and joint problems. Depending on the location of tumors, specific symptoms may manifest. The prognosis for benign cardiac tumors is favorable, but there is a potential of recurrence, but the prognosis for malignant tumors is poor.
Natural History
Cardiac tumors can arise in a multitude of ways, resulting in diverse clinical presentations. Irrespective of cardiac tumor type, cardiac symptoms primarily depend on tumor position and extent.[1]
- Patients may develop systemic symptoms including fever, fatigue, and joint pains but can be asymptomatic as well. Myxomas were asymptomatic in 72% cases in a study by Dias et al.[2]
- Tumors can impede blood flow, causing hemodynamic abnormalities, poor cardiac output, or heart failure.
- Malignant tumors may especially cause weight loss, anorexia, and exhaustion.
- In addition, valvular disease can lead to stenosis or regurgitation.[3]
- Local infiltration of the cardiac conduction system could result in arrhythmias.
- Non-specific features like pericardial effusion and compression of nearby structures, such as the coronary arteries, might develop.
- Clinically, the tumor type (benign or malignant), anatomical location, time duration of receiving treatment and available treatment options are the most critical clinical criteria in determining a cardiac tumor patient’s natural history of disease.
- The relapse rate of benign cardiac tumors is minimal. In some familial types of benign tumors, such as familial myxomas, however, incidence rates of tumor recurrence can reach as high as 22%.[4] In certain syndromes like Tuberous Sclerosis the rhabdomyomas disappear and have a good prognosis.
- In contrast, malignant tumors often have a poorer prognosis and are difficult to treat due to their more invasive behavior, metastatic origin, and high recurrence rate. Malignant tumors have a much greater mortality rate. Most of the patients succumb to the tumor within an year even with treatment[4]
Complications
- Emboli into coronary arteries
- Retrograde flow through cardiac lymphatics
- Direct extension from mediastinum
- Emboli or spread via great veins => endocardial metastases
- Hypernephroma
- Testicular sarcoma
- IVC leiomyosarcoma
- Ovarian cancer
- Colon cancer
Prognosis
The vast majority of the tumors of the heart have a benign course and are not directly fatal. However, even the benign tumors of the heart can be lethal due to either direct extension into the electrical conduction system of the heart (causing complete heart block or a fatal dysrhythmia), or due to emboli from the tumor mass that may have lethal sequelae.
The malignant tumors of the heart have a worse prognosis. Cardiac sarcomas generally lead to death within 2 years of diagnosis, due to rapid infiltration of the myocardium of the heart and obstruction of the normal flow of blood within the heart.[5][6]
References
- ↑ Paraskevaidis IA, Michalakeas CA, Papadopoulos CH, Anastasiou-Nana M (2011). “Cardiac tumors”. ISRN Oncol. 2011: 208929. doi:10.5402/2011/208929. PMC 3195386. PMID 22091416.
- ↑ Dias RR, Fernandes F, Ramires FJ, Mady C, Albuquerque CP, Jatene FB (2014). “Mortality and embolic potential of cardiac tumors”. Arq Bras Cardiol. 103 (1): 13–8. doi:10.5935/abc.20140096. PMC 4126756. PMID 25029470.
- ↑ Avakian SD, Takada JY, Mansur Ade P (2012). “Giant obstructive left atrial myxoma resembling mitral valve stenosis”. Clinics (Sao Paulo). 67 (7): 853–4. doi:10.6061/clinics/2012(07)25. PMC 3400890. PMID 22892935.
- ↑ 4.0 4.1 Palaskas N, Thompson K, Gladish G, Agha AM, Hassan S, Iliescu C; et al. (2018). “Evaluation and Management of Cardiac Tumors”. Curr Treat Options Cardiovasc Med. 20 (4): 29. doi:10.1007/s11936-018-0625-z. PMID 29556752.
- ↑ Burke AP, Cowan D, Virmani R (1992). “Primary sarcomas of the heart”. Cancer. 69 (2): 387–95. PMID 1728367.
- ↑ Burke AP, Virmani R (1991). “Osteosarcomas of the heart”. Am J Surg Pathol. 15 (3): 289–95. PMID 1705103.
Diagnosis
Diagnosis
Staging | History and Symptoms | Physical Examination | Laboratory Findings | Electrocardiogram | Chest X Ray | CT | MRI | Echocardiography | Other Imaging Findings | Other Diagnostic Studies
Treatment
Treatment
Medical Therapy | Surgery | Primary Prevention | Secondary Prevention | Cost-Effectiveness of Therapy | Future or Investigational Therapies
Looking for the patient version?
© 2026 MyEClinic – IFTM Institut für Telematik in der Medizin GmbH