
List of subjects in Gray's Anatomy: II. Osteology
Introduction (Template:GraySubject)
Introduction (Template:GraySubject)
- classes
- classes
- Surfaces of bones
- articular eminences
- articular depressions
- non-articular eminences
- tuberosity, protuberance, or process
- tubercle
- spine
- ridge, crest, or line
- non-articular depressions
- perforation/passage
Development of the Skeleton
- Skull
- membranous cranium
- chondrocranium
- chordal or vertebral portion
- prechordal or prevertebral portion
- trabeculae cranii
- parachordal cartilages
bone (Template:GraySubject)
- Structure and Physical Properties
- Marrow
- Vessels and Nerves of Bone
- Vessels and Nerves of Bone
- Minute Anatomy
- Minute Anatomy
- primary or fundamental lamellæ
- secondary or special lamellæ
- Haversian canals
- lamellæ
- perforating fibers
- Lacunæ
- Minute Anatomy
- Ossification
- Ossification
- osteoblasts, or bone-formers
- osteoclasts, or bone-destroyers
- secondary areolæ or medullary spaces
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]
Overview

Bones are rigid organs that form part of the endoskeleton of vertebrates. They function to move, support, and protect the various organs of the body, produce red and white blood cells and store minerals. Because bones come in a variety of shapes and have a complex internal and external structure, they are lightweight, yet strong and hard, in addition to fulfilling their many other functions. One of the types of tissues that makes up bone is the mineralized osseous tissue, also called bone tissue, that gives it rigidity and honeycomb-like three-dimensional internal structure. Other types of tissue found in bones include marrow, endosteum and periosteum, nerves, blood vessels and cartilage. There are 206 bones in the adult body, and about 300 bones in a infants body.
Functions
Bones have eight main functions:
- Protection — Bones can serve to protect internal organs, such as the skull protecting the brain or the ribs protecting the heart and lungs.
- Shape — Bones provide a frame to keep the body supported.
- Blood production — The marrow, located within the medullary cavity of long bones and the interstices of cancellous bone, produces blood cells in a process called haematopoiesis.
- Mineral storage — Bones act as reserves of minerals important for the body, most notably calcium and phosphorus.
- Movement — Bones, skeletal muscles, tendons, ligaments and joints function together to generate and transfer forces so that individual body parts or the whole body can be manipulated in three-dimensional space. The interaction between bone and muscle is studied in biomechanics.
- Acid-base balance — Bone buffers the blood against excessive pH changes by absorbing or releasing alkaline salts.
- Detoxification — Bone tissues can also store heavy metals and other foreign elements, removing them from the blood and reducing their effects on other tissues. These can later be gradually released for excretion.
- Sound transduction — Bones are important in the mechanical aspect of hearing.
Characteristics
The primary tissue of bone, osseous tissue, is a relatively hard and lightweight composite material, formed mostly of calcium phosphate in the chemical arrangement termed calcium hydroxylapatite (this is the osseous tissue that gives bones their rigidity). It has relatively high compressive strength but poor tensile strength, meaning it resists pushing forces well, but not pulling forces. While bone is essentially brittle, it does have a significant degree of elasticity contributed chiefly by collagen. All bones consist of living cells embedded in the mineralised organic matrix that makes up the osseous tissue.
Macrostructure
Bone is not a uniformly solid material, but rather has some spaces between its hard elements.

Compact bone
The hard outer layer of bones is composed of compact bone tissue, so-called due to its minimal gaps and spaces. This tissue gives bones their smooth, white, and solid appearance, and accounts for 80% of the total bone mass of an adult skeleton. Compact bone may also be referred to as dense bone or cortical bone.
Trabecular bone
Filling the interior of the organ is the trabecular bone tissue (an open cell porous network also called cancellous or spongy bone) which is comprised of a network of rod- and plate-like elements that make the overall organ lighter and allowing room for blood vessels and marrow. Trabecular bone accounts for the remaining 20% of total bone mass, but has nearly ten times the surface area of compact bone.
Cellular structure
There are several types of cells constituting the bone;
- Osteoblasts are mononucleate bone-forming cells which descend from osteoprogenitor cells. They are located on the surface of osteoid seams and make a protein mixture known as osteoid, which mineralizes to become bone. Osteoid is primarily composed of Type I collagen. Osteoblasts also manufacture hormones, such as prostaglandins, to act on the bone itself. They robustly produce alkaline phosphatase, an enzyme that has a role in the mineralisation of bone, as well as many matrix proteins. Osteoblasts are the immature bone cells.
- Bone lining cells are essentially inactive osteoblasts. They cover all of the available bone surface and function as a barrier for certain ions.
- Osteocytes originate from osteoblasts which have migrated into and become trapped and surrounded by bone matrix which they themselves produce. The spaces which they occupy are known as lacunae. Osteocytes have many processes which reach out to meet osteoblasts probably for the purposes of communication. Their functions include to varying degrees: formation of bone, matrix maintenance and calcium homeostasis. They possibly act as mechano-sensory receptors—regulating the bone’s response to stress. They are mature bone cells.
- Osteoclasts are the cells responsible for bone resorption (remodeling of bone to reduce its volume). Osteoclasts are large, multinucleated cells located on bone surfaces in what are called Howship’s lacunae or resorption pits. These lacunae, or resorption pits, are left behind after the breakdown of bone and often present as scalloped surfaces. Because the osteoclasts are derived from a monocyte stem-cell lineage, they are equipped with engulfment strategies similar to circulating macrophages. Osteoclasts mature and/or migrate to discrete bone surfaces. Upon arrival, active enzymes, such as tartrate resistant acid phosphatase, are secreted against the mineral substrate.
Molecular structure
Matrix
The matrix is the major constituent of bone, surrounding the cells. It has inorganic and organic parts.
Inorganic
The inorganic is mainly crystalline mineral salts and calcium, which is present in the form of hydroxyapatite. The matrix is initially laid down as unmineralized osteoid (manufactured by osteoblasts). Mineralisation involves osteoblasts secreting vesicles containing alkaline phosphatase. This cleaves the phosphate groups and acts as the foci for calcium and phosphate deposition. The vesicles then rupture and act as a centre for crystals to grow on.
Organic
The organic part of matrix is mainly Type I collagen. This is made intracellularly as tropocollagen and then exported. It then associates into fibrils. Also making up the organic part of matrix include various growth factors, the functions of which are not fully known. Other factors present include glycosaminoglycans, osteocalcin, osteonectin, bone sialo protein and Cell Attachment Factor. One of the main things that distinguishes the matrix of a bone from that of another cell is that the matrix in bone is hard.
Woven or lamellar

Bone is first deposited as woven bone, in a disorganized structure with a high proportion of osteocytes in young and in healing injuries. Woven bone is weaker, with a small number of randomly oriented collagen fibers, but forms quickly. It is replaced by lamellar bone, which is highly organized in concentric sheets with a low proportion of osteocytes. Lamellar bone is stronger and filled with many collagen fibers parallel to other fibers in the same layer. The fibers run in opposite directions in alternating layers, much like plywood, assisting in the bone’s ability to resist torsion forces. After a break, woven bone quickly forms and is gradually replaced by slow-growing lamellar bone on pre-existing calcified hyaline cartilage through a process known as “bony substitution.”
Five types of bones

There are five types of bones in the human body: long, short, flat, irregular and sesamoid.
- Long bones are longer than they are wide, consisting of a long shaft (the diaphysis) plus two articular (joint) surfaces, called epiphyses. They are comprised mostly of compact bone, but are generally thick enough to contain considerable spongy bone and marrow in the hollow centre (the medullary cavity). Most bones of the limbs (including the three bones of the fingers) are long bones, except for the kneecap (patella), and the carpal, metacarpal, tarsal and metatarsal bones of the wrist and ankle. The classification refers to shape rather than the size.
- Short bones are roughly cube-shaped, and have only a thin layer of compact bone surrounding a spongy interior. The bones of the wrist and ankle are short bones, as are the sesamoid bones.
- Flat bones are thin and generally curved, with two parallel layers of compact bones sandwiching a layer of spongy bone. Most of the bones of the skull are flat bones, as is the sternum.
- Irregular bones do not fit into the above categories. They consist of thin layers of compact bone surrounding a spongy interior. As implied by the name, their shapes are irregular and complicated. The bones of the spine and hips are irregular bones.
- Sesamoid bones are bones embedded in tendons. Since they act to hold the tendon further away from the joint, the angle of the tendon is increased and thus the force of the muscle is increased. Examples of sesamoid bones are the patella and the pisiform
Formation
The formation of bone during the fetal stage of development occurs by two methods: intramembranous and endochondral ossification.
Intramembranous ossification
Intramembranous ossification mainly occurs during formation of the flat bones of the skull; the bone is formed from mesenchyme tissue. The steps in intramembranous ossification are:
- Development of ossification center
- Calcification
- Formation of trabeculae
- Development of periosteum
Endochondral ossification

Endochondral ossification, on the other hand, occurs in long bones, such as limbs; the bone is formed from cartilage. The steps in endochondral ossification are:
- Development of cartilage model
- Growth of cartilage model
- Development of the primary ossification center
- Development of medullary cavity
- Development of the secondary ossification center
- Formation of articular cartilage and epiphyseal plate
Endochondral ossification begins with points in the cartilage called “primary ossification centers.” They mostly appear during fetal development, though a few short bones begin their primary ossification after birth. They are responsible for the formation of the diaphyses of long bones, short bones and certain parts of irregular bones. Secondary ossification occurs after birth, and forms the epiphyses of long bones and the extremities of irregular and flat bones. The diaphysis and both epiphyses of a long bone are separated by a growing zone of cartilage (the epiphyseal plate). When the child reaches skeletal maturity (18 to 25 years of age), all of the cartilage is replaced by bone, fusing the diaphysis and both epiphyses together (epiphyseal closure).
Bone marrow
There are two types of bone marrow, yellow and red, most commonly seen is red Bone marrow can be found in almost any bone that holds cancellous tissue. In newborns, all such bones are filled exclusively with red marrow (or hemopoietic marrow), but as the child ages it is mostly replaced by yellow, or fatty marrow. In adults, red marrow is mostly found in the flat bones of the skull, the ribs, the vertebrae and pelvic bones.
Remodeling
Remodeling or bone turnover is the process of resorption followed by replacement of bone with little change in shape and occurs throughout a person’s life. Osteoblasts and osteoclasts, coupled together via paracrine cell signalling, are referred to as bone remodeling units.
Purpose
The purpose of remodeling is to regulate calcium homeostasis, repair micro-damaged bones (from everyday stress) but also to shape and sculpture the skeleton during growth.
Calcium balance
The process of bone resorption by the osteoclasts releases stored calcium into the systemic circulation and is an important process in regulating calcium balance. As bone formation actively fixes circulating calcium in its mineral form, removing it from the bloodstream, resorption actively unfixes it thereby increasing circulating calcium levels. These processes occur in tandem at site-specific locations.
Repair
Repeated stress, such as weight-bearing exercise or bone healing, results in the bone thickening at the points of maximum stress (Wolff’s law). It has been hypothesized that this is a result of bone’s piezoelectric properties, which cause bone to generate small electrical potentials under stress.
Medical conditions related to bones
Osteology
The study of bones and teeth is referred to as osteology. It is frequently used in anthropology, archeology and forensic science for a variety of tasks. This can include determining the nutritional, health, age or injury status of the individual the bones were taken from. Preparing fleshed bones for these types of studies can involve maceration – boiling fleshed bones to remove large particles, then hand-cleaning.
Typically anthropologists and archeologists study bone tools made by Homo sapiens and Homo neanderthalensis. Bones can serve a number of uses such as projectile points or artistic pigments, and can be made from endoskeletal or external bones such as antler or tusk.
Alternatives to bony endoskeletons
There are several evolutionary alternatives to mammilary bone; though they have some similar functions, they are not completely functionally analogous to bone.
- Exoskeletons offer support, protection and levers for movement similar to endoskeletal bone. Different types of exoskeletons include shells, carapaces (consisting of calcium compounds or silica) and chitinous exoskeletons.
- A true endoskeleton (that is, protective tissue derived from mesoderm) is also present in Echinoderms. Porifera (sponges) possess simple endoskeletons that consist of calcareous or siliceous spicules and a spongin fiber network.
Exposed bone
Bone penetrating the skin and being exposed to the outside can be both a natural process in some animals, and due to injury:
- A deer’s antlers are composed of bone
- The extinct predatory fish Dunkleosteus, instead of teeth, had sharp edges of hard exposed bone along its jaws
- A compound fracture occurs when the edges of a broken bone punctures the skin
- Though not strictly speaking exposed, a bird’s beak is primarily bone covered in a layer of keratin
Terminology
Several terms are used to refer to features and components of bones throughout the body:
| Bone feature | Definition |
|---|---|
| articular process | A projection that contacts an adjacent bone. |
| articulation | The region where adjacent bones contact each other—a joint. |
| canal | A long, tunnel-like foramen, usually a passage for notable nerves or blood vessels. |
| condyle | A large, rounded articular process. |
| crest | A prominent ridge. |
| eminence | A relatively small projection or bump. |
| epicondyle | A projection near to a condyle but not part of the joint. |
| facet | A small, flattened articular surface. |
| foramen | An opening through a bone. |
| fossa | A broad, shallow depressed area. |
| fovea | A small pit on the head of a bone. |
| labyrinth | A cavity within a bone. |
| line | A long, thin projection, often with a rough surface. Also known as a ridge. |
| malleolus | One of two specific protuberances of bones in the ankle. |
| meatus | A short canal. |
| process | A relatively large projection or prominent bump.(gen.) |
| ramus | An arm-like branch off the body of a bone. |
| sinus | A cavity within a cranial bone. |
| spine | A relatively long, thin projection or bump. |
| suture | Articulation between cranial bones. |
| trochanter | One of two specific tuberosities located on the femur. |
| tubercle | A projection or bump with a roughened surface, generally smaller than a tuberosity. |
| tuberosity | A projection or bump with a roughened surface. |
Several terms are used to refer to specific features of long bones:
| Bone feature | Definition |
|---|---|
| diaphysis | The long, relatively straight main body of a long bone; region of primary ossification. Also known as the shaft. |
| epiphysis | The end regions of a long bone; regions of secondary ossification. |
| epiphyseal plate | Also known as the growth plate or physis. In a long bone it is a thin disc of hyaline cartilage that is positioned transversely between the epiphysis and metaphysis. In the long bones of humans, the epiphyseal plate disappears by twenty years of age. |
| head | The proximal articular end of the bone. |
| metaphysis | The region of a long bone lying between the epiphysis and diaphysis. |
| neck | The region of bone between the head and the shaft. |
References
- Marieb, E.N. (1998). Human Anatomy & Physiology, 4th ed. Menlo Park, California: Benjamin/Cummings Science Publishing.
- Netter, Frank H. (1987), Musculoskeletal system: anatomy, physiology, and metabolic disorders, Summit, New Jersey: Ciba-Geigy Corporation.
- Tortora, G. J. (1989), Principles of Human Anatomy, 5th ed. New York: Harper & Row, Publishers.
See also
External links
- Review (including references) of piezoelectricity and bone remodelling
- A good basic overview of bone biology from the Science Creative Quarterly
- Bone Health at Got Bones?
- Osteopathic physicians
Template:Bone and cartilage Template:Facial bones Template:Cranium Template:Sutures Template:Bones of upper extremity Template:Spine Template:Bones of lower extremity Template:Pelvis
af:Been
ar:عظم
ay:Ch’aka
bs:Kosti
br:Askorn
bg:Кост
ca:Os
cs:Kost
cy:Asgwrn
da:Knogle (anatomi)
de:Knochen
el:Οστό
eo:Osto
eu:Hezur
gd:Cnàmh
gl:Óso
ko:뼈
hr:Kosti
io:Osto
id:Tulang
is:Bein
it:Osso
he:עצם
la:Os (ossis – anatomia)
lv:Kauli
lt:Kaulas
ln:Mokúwa
hu:Csont
mk:Коска
nl:Bot (anatomie)
qu:Tullu
simple:Bone
sk:Kosť
sl:Kost
sr:Кост
sh:Kosti
su:Tulang
fi:Luu
sv:Ben (skelett)
tl:Buto (anatomiya)
ta:எலும்பு
th:กระดูก
uk:Кістка
the vertebral column (Template:GraySubject)
- Columna Vertebralis; Spinal column
general characteristics of a vertebra (Template:GraySubject)
- typical vertebra
- vertebral foramen
- intervertebral foramina
- body of vertebra (corpus vertebræ)
- body of vertebra (corpus vertebræ)
- vertebral arch or neural arch (posterior part)
- pedicle of vertebral arch (radices arci vertebræ)
- lamina of the vertebral arch
- processes of vertebra
- 1 Spinous process (processus spinosus)
- 4 Articular processes
- 2 Transverse processes (processus transversi)
- upper surface
- lower surface
- pedicles
- laminae
- vertebral foramen
- spinous process
- superior articular process
- inferior articular process
- transverse processes
- foramen transversarium
- costal process or costal element
- anterior tubercle
- posterior tubercle
- First thoracic vertebra
- Ninth thoracic vertebra
- Tenth thoracic vertebra
- Eleventh thoracic vertebra
- Twelfth thoracic vertebra
the sacral and coccygeal vertebrae (Template:GraySubject)
- Sacrum (os sacrum)
- Pelvic surface of sacrum (facies pelvina)
- Dorsal surface of sacrum (facies dorsalis)
- Dorsal surface of sacrum (facies dorsalis)
- Lateral surface of sacrum
- base of the sacrum (basis oss. sacri)
- base of the sacrum (basis oss. sacri)
- Apex of the sacrum (apex oss. sacri)
- Vertebral canal (canalis sacralis; sacral canal)
- Differences in the Sacrum of the Male and Female
- Coccyx (os coccygis)
- Ossification of the Vertebral column
- Ossification of the Vertebral column
the vertebral column as a whole (Template:GraySubject)


Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]
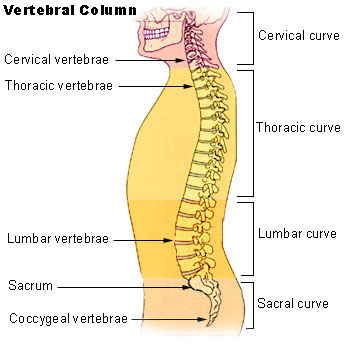
In human anatomy, the vertebral column (backbone or spine) is a column of 33 vertebrae, the sacrum, intervertebral discs, and the coccyx situated in the dorsal aspect of the torso, separated by spinal discs. It houses the spinal cord in its spinal canal.
Curves
Viewed laterally the vertebral column presents several curves, which correspond to the different regions of the column, and are called cervical, thoracic, lumbar, and pelvic.
The cervical curve, convex forward, begins at the apex of the odontoid (tooth-like) process, and ends at the middle of the second thoracic vertebra; it is the least marked of all the curves.
The thoracic curve, concave forward, begins at the middle of the second and ends at the middle of the twelfth thoracic vertebra. Its most prominent point behind corresponds to the spinous process of the seventh thoracic vertebra. This curve is known as a tt curve.
The lumbar curve is more marked in the female than in the male; it begins at the middle of the last thoracic vertebra, and ends at the sacrovertebral angle. It is convex anteriorly, the convexity of the lower three vertebrae being much greater than that of the upper two. This curve is described as a lordotic curve.
The pelvic curve begins at the sacrovertebral articulation, and ends at the point of the coccyx; its concavity is directed downward and forward.
The thoracic and pelvic curves are termed primary curves, because they alone are present during fetal life. In the early embryo, the vertebral column is C-shaped, and the cervical and lumbar curvatures are not yet present in a newborn infant. The cervical and lumbar curves are compensatory or secondary, and are developed after birth, the former when the child is able to hold up its head (at three or four months) and to sit upright (at nine months), the latter at twelve or eighteen months, when the child begins to walk.
The thoracic portion of the vertebral column also has a slight lateral curvature, the convexity of which is directed toward the right side. This may be produced by muscular action, most persons using the right arm in preference to the left, especially in making long-continued efforts, when the body is curved to the right side. In support of this explanation it has been found that in one or two individuals who were left-handed, the convexity was to the left side. This curvature is regarded by others as being produced by the aortic arch and upper part of the descending thoracic aorta – a view which is supported by the fact that in cases of situs inversus where the viscera are transposed and the aorta is on the right side, the convexity of the curve is directed to the left side.
Names of individual vertebrae
Individual vertebrae named according to region and position, from superior to inferior
- Cervical – 7 vertebrae (C1-C7)
- C1 is known as “atlas” and supports the head, C2 is known as “axis”
- Possesses bifid spinous processes, which is absent in C7
- Small-bodied
- Thoracic – 12 vertebrae (T1-T12)
- Distinguished by the presence of costal facets for the articulation of the heads of ribs
- Body is intermediate in size between the cervical and lumbar vertebrae
- Lumbar – 5 vertebrae (L1-L5)
- Has a large body
- Does not have costal facets nor transverse process foramina
- Sacral – 5 (fused) vertebrae (S1-S5)
- Coccygeal – 4 (fused) vertebrae (Co1-Co4)
Surfaces
Anterior surface
When viewed from in front, the width of the bodies of the vertebrae is seen to increase from the second cervical to the first thoracic; there is then a slight diminution in the next three vertebrae; below this there is again a gradual and progressive increase in width as low as the sacrovertebral angle. From this point there is a rapid diminution, to the apex of the coccyx.

Posterior surface
The posterior surface of the vertebral column presents in the median line the spinous processes. In the cervical region (with the exception of the second and seventh vertebrae) these are short and horizontal, with bifid extremities. In the upper part of the thoracic region they are directed obliquely downward; in the middle they are almost vertical, and in the lower part they are nearly horizontal. In the lumbar region they are nearly horizontal. The spinous processes are separated by considerable intervals in the lumbar region, by narrower intervals in the neck, and are closely approximated in the middle of the thoracic region. Occasionally one of these processes deviates a little from the median line — a fact to be remembered in practice, as irregularities of this sort are attendant also on fractures or displacements of the vertebral column. On either side of the spinous processes is the vertebral groove formed by the laminae in the cervical and lumbar regions, where it is shallow, and by the laminae and transverse processes in the thoracic region, where it is deep and broad; these grooves lodge the deep muscles of the back. Lateral to the vertebral grooves are the articular processes, and still more laterally the transverse processes. In the thoracic region, the transverse processes stand backward, on a plane considerably behind that of the same processes in the cervical and lumbar regions. In the cervical region, the transverse processes are placed in front of the articular processes, lateral to the pedicles and between the intervertebral foramina. In the thoracic region they are posterior to the pedicles, intervertebral foramina, and articular processes. In the lumbar region they are in front of the articular processes, but behind the intervertebral foramina.
Lateral surfaces
The lateral surfaces are separated from the posterior surface by the articular processes in the cervical and lumbar regions, and by the transverse processes in the thoracic region. They present, in front, the sides of the bodies of the vertebrae, marked in the thoracic region by the facets for articulation with the heads of the ribs. More posteriorly are the intervertebral foramina, formed by the juxtaposition of the vertebral notches, oval in shape, smallest in the cervical and upper part of the thoracic regions, and gradually increasing in size to the last lumbar. They transmit the spinal nerves and are situated between the transverse processes in the cervical region, and in front of them in the thoracic and lumbar regions.

T3 is at level of medial part of spine of scapula. T7 is at inferior angle of the scapula. L4 is at highest point of iliac crest. S2 is at the level of posterior superior iliac spine. T12 can be found by identifying the lowest pair of ribs and tracing them to their thoracic attachment.[1] Furthermore, C7 is easily localized as a prominence at the lower part of the neck. [2]
Vertebral canal
The vertebral canal follows the different curves of the column; it is large and triangular in those parts of the column which enjoy the greatest freedom of movement, such as the cervical and lumbar regions; and is small and rounded in the thoracic region, where motion is more limited.
Abnormalities
Occasionally the coalescence of the laminae is not completed, and consequently a cleft is left in the arches of the vertebrae, through which a protrusion of the spinal membranes (dura mater and arachnoid), and generally of the spinal cord (medulla spinalis) itself, takes place, constituting the malformation known as spina bifida. This condition is most common in the lumbosacral region, but it may occur in the thoracic or cervical region, or the arches throughout the whole length of the canal may remain incomplete.
The following abnormal curvatures may occur in some people:
- Kyphosis is an exaggerated kyphotic (posterior) curvature in the thoracic region. This produces the so-called “humpback” or “dowager’s hump”, a condition commonly observed in osteoporosis.
- Lordosis is an exaggerated lordotic (anterior) curvature of the lumbar region, “swayback”. Temporary lordosis is common among pregnant women.
- Scoliosis, lateral curvature, is the most common abnormal curvature, occurring in 0.5% of the population. It is more common among females and may result from unequal growth of the two sides of one or more vertebrae. It can also be caused by pulmonary atelectasis (partial or complete deflation of one or more lobes of the lungs) as observed in asthma or pneumothorax.
Additional images
-
 Vertebral column.
Vertebral column. -
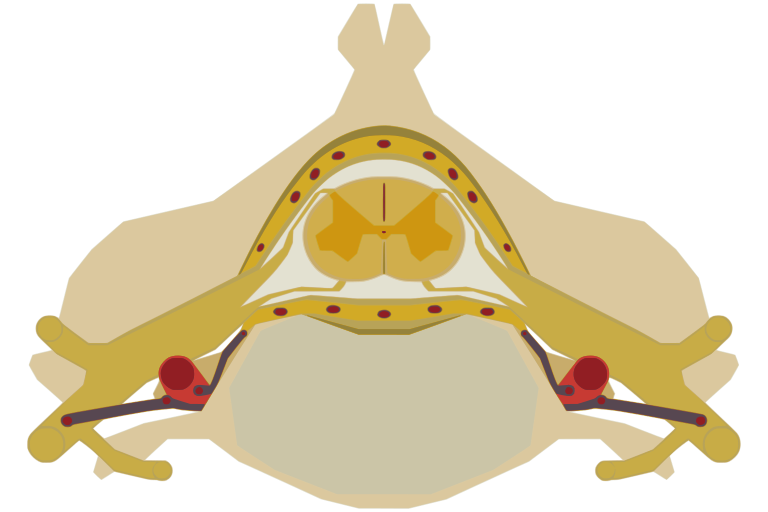 The spinal cord nested in the vertebral column.
The spinal cord nested in the vertebral column. -
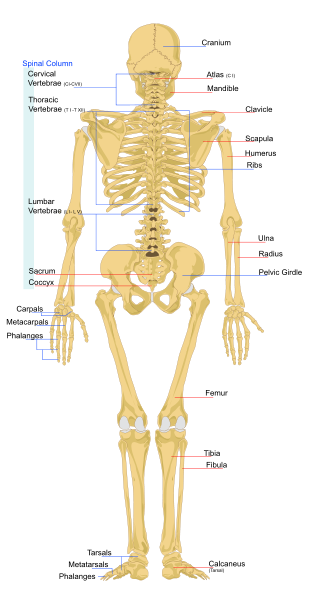 Human skeleton back
Human skeleton back -
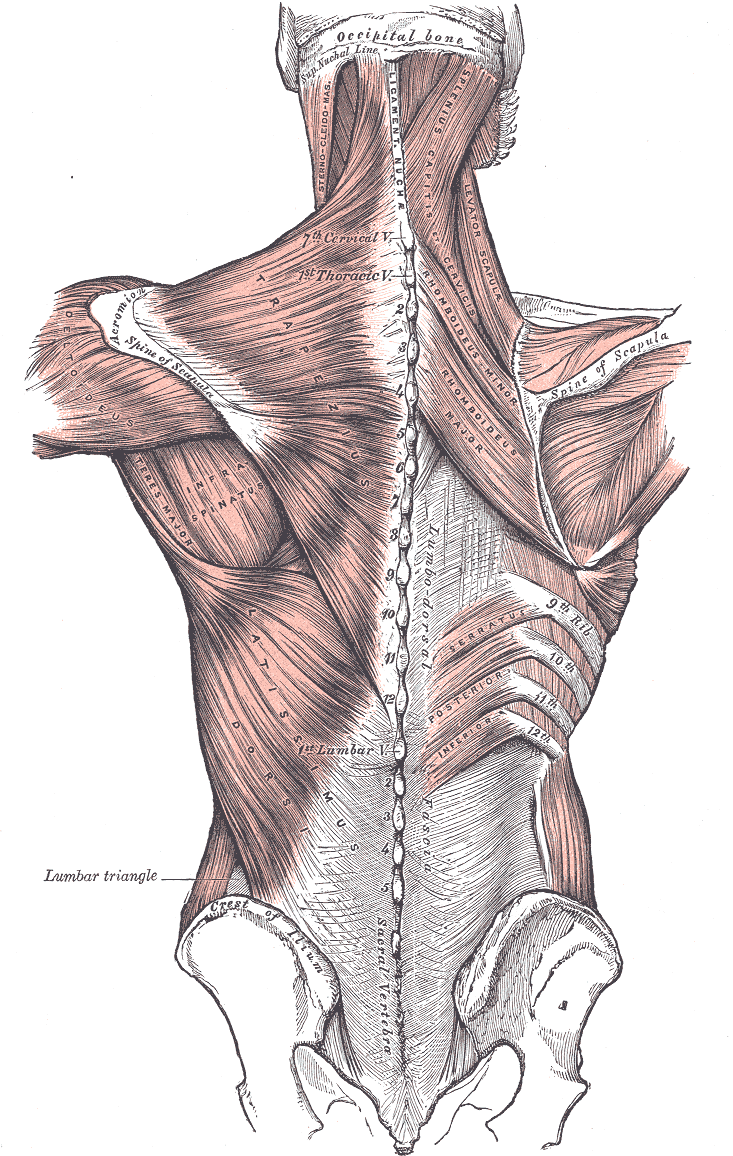 Relation of the vertebral column to the surrounding muscles.
Relation of the vertebral column to the surrounding muscles.




References
See also
External links
- North American Spine Society is a multidisciplinary medical organization that advances quality spine care through education, research and advocacy.
- Spinal Cord Injuries Australia (formerly Australian Quadriplegic Association AQA, established 1967) provides information about the disability and services for affected people, advocacy, accommodation, employment, peer support.
- Spinal Cord Injury Peer SupportPeer support for those living with spinal injuries.
- Vertebral column basics
- Spinal Term Glossary
Template:Vertebral column and spinal cord Template:Human anatomical features
ar:عمود فقري
ay:Jikhani k’ili
br:Gwalenn ar c’hein
bg:Гръбначен стълб
ca:Columna vertebral
cs:Páteř
cy:Asgwrn cefn
da:Rygsøjlen
de:Wirbelsäule
eo:Vertebraro
fa:ستون مهرهها
ko:등뼈
is:Hryggsúla
it:Colonna vertebrale
he:עמוד השדרה
ku:Masiya piştê
la:Columna vertebralis
lv:Mugurkauls
lt:Stuburas
ln:Mokesa
nl:Wervelkolom
no:Ryggsøyle
nn:Ryggsøyle
scn:Cutruzzu
simple:Vertebral column
sk:Chrbtica
sl:Hrbtenica
su:Tulang tonggong
fi:Selkäranka
sv:Ryggrad
tl:Gulugod
te:వెన్నెముక
th:กระดูกสันหลัง
uk:Хребет
fiu-vro:Sälgruuts
yi:רוקן ביין
the thorax (Template:GraySubject)
the thorax (Template:GraySubject)
- Thorax: boundaries of:
- Thorax: skeleton of:
- upper opening of the thorax
the sternum (Template:GraySubject)
- Manubrium (manubrium sterni)
- Body of sternum (corpus sterni; gladiolus)
- Body of sternum (corpus sterni; gladiolus)
- sternal foramen
- sternal angle (angulus Ludovici)
- Xiphoid process (processus xiphoideus; ensiform or xiphoid appendix)
the ribs (Template:GraySubject)
- costal cartilages (Cartilagines Costales)

Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]
Overview
The chest is a part of the anatomy of humans and various other animals.
Human chest anatomy
In human, the chest is the region of the body between the neck and the abdomen, along with its internal organs and other contents. It is mostly protected and supported by the ribcage, spine, and shoulder girdle. Contents of the chest include the following:
- organs
- muscles
- internal structures
- arteries and veins

- bones
- the shoulder socket containing the upper part of the humerus
- scapula
- sternum
- thoracic portion of the spine
- collarbone
- ribcage
- Floating ribs
- external structures
- thoracic abdomen (stomach, kidney/adrenal, pancreas, spleen, and lower oesophagus)
In humans, the portion of the chest protected by the ribcage is also called the thorax.
Chest injury
Injury to the chest (also referred to as chest trauma, thoracic injury, or thoracic trauma) results in up to ¼ of all deaths due to trauma in the United States.[1]
In the human body, the chest is the body region between the neck and diaphragm in the front of the body. The corresponding area in an animal can be referred to as the chest. The chest holds many important internal, and is protected by the ribcage.
It is important to realize that the shape of the chest does not correspond to that of the bony thorax which encloses the heart and lungs; all the breadth of the shoulders is due to the shoulder girdle, and contains the axilla and the head of the humerus. In the middle line the suprasternal notch is seen above, while about three fingers’ breadth below it a transverse ridge can be felt, which is known as (Ludovic’s angle) and marks the junction between the manubrium and gladiolus of the sternum. Level with this line the second ribs join the sternum, and when these are found the lower ribs may be easily counted in a moderately thin subject. At the lower part of the sternum, where the seventh or last true ribs join it, the ensiform cartilage begins, and over this there is often a depression popularly known as the pit of the stomach.
The nipple in the male is situated in front of the fourth rib or a little below; vertically it lies a little external to a line drawn down from the middle of the clavicle; in the female it is not so constant. A little below it the lower limit of the great pectoral muscle is seen running upward and outward to the axilla; in the female this is obscured by the breast, which extends from the second to the sixth rib vertically and from the edge of the sternum to the mid-axillary line laterally. The female nipple is surrounded for half an inch by a more or less pigmented disc, the areola. The apex of a normal heart is in the fifth left intercostal space, three and a half inches from the mid-line.
References
- ↑ Shahani, Rohit, MD. (2005). Penetrating Chest Trauma. eMedicine. Retrieved 2005-02-05.
See also
- Thoracic cavity
- Pectus excavatum
- Pectus carinatum
- Breast
- Chest hair
- Barechested
Template:Human anatomical features Template:Torso general
ar:صدر
ay:Ñuñu
de:Brust
ln:Bontólo
qu:Qhasqu
simple:Chest
sk:Hrudník
fi:Rinta
sv:Bröst (könsneutralt)
tl:Dibdib
yi:ברוסט קאסטען
[[zh:胸]
the skull (Template:GraySubject)
the skull (Template:GraySubject)
the cranial bones
- Basilar part of occipital bone (pars basilaris)
- Foramen magnum
- Angles
- Borders
- Ossification of occipital bone
- external surface
- parietal eminence (tuber parietale)
- external surface
- internal surface
- Borders
- Borders
- Angles
- Squama (squama frontalis)
- metopic suture
- frontal eminence (tuber frontale)
- superciliary arches
- glabella
- supraorbital margin
- Squama (squama frontalis)
- Orbital or Horizontal Part (pars orbitalis)
- Orbital or Horizontal Part (pars orbitalis)
- border of the squama
- posterior borders of the orbital plates
- Ossification of frontal bone
- Squama (squama temporalis)
- temporal line, or supramastoid crest
- zygomatic process
- anterior root and posterior root
- articular tubercle (eminentia articularis)
- parietal notch
- antero-inferior border
- Mastoid portion (pars mastoidea)
- Mastoid portion (pars mastoidea)
- Petrous portion (pars petrosa)
- Petrous portion (pars petrosa)
- Trigeminal impression
- posterior surface
- inferior surface
- Petrous portion (pars petrosa)
- Petrous portion (pars petrosa)
- angles
- jugular foramen
- anterior angle
- petrosquamous suture
- septum canalis musculotubarii (processus cochleariformis)
- angles
- Tympanic part (pars tympanica)
- Styloid process (processus styloideus)
- Ossification of temporal bone
- anterior surface of sphenoid
- inferior surface of sphenoid
- sphenoidal rostrum
- vaginal process
- Great wings (alæ magnæ) (ali-sphenoids)
- Great wings (alæ magnæ) (ali-sphenoids)
- Great wings (alæ magnæ) (ali-sphenoids)
- Small wings (alæ parvæ)
- Surfaces
- Borders
- Pterygoid processes (processus pterygoidei)
- Pterygoid processes (processus pterygoidei)
- Sphenoidal conchæ (conchæ sphenoidales; sphenoidal turbinated processes)
- Cribiform plate (lamina cribrosa; horizontal lamina)
- Perpendicular plate (lamina perpendicularis; vertical plate)
- Labyrinth or Lateral mass (labyrinthus ethmoidalis)
- Surfaces
- upper surface
- anterior and posterior ethmoidal canals
- posterior surface
- upper surface
- Surfaces
- lateral surface
- Surfaces
- sutural or Wormian bones
the facial bones
the maxillæ (upper jaw) (Template:GraySubject)
- Body of maxilla (corpus maxillæ)
- Body of maxilla (corpus maxillæ)
- Body of maxilla (corpus maxillæ)
- Maxillary sinus or Antrum of Highmore (sinus maxillaris)
- Body of maxilla (corpus maxillæ)
- Zygomatic process (processus zygomaticus; malar process)
- Frontal process (processus frontalis; nasal process)
- Alveolar process (processus alveolaris)
- Palatine process (processus palatinus; palatal process)
- Palatine process (processus palatinus; palatal process)
- Ossification of maxilla
- posterior lacrimal crest
- lacrimal sulcus (sulcus lacrimalis)
- lacrimal hamulus
- lesser lacrimal bone
- Processes
- Processes
- Processes
- Borders
- Articulations
- Horizontal part of palatine bone (pars horizontalis; horizontal plate of palatine bone)
- Vertical part of palatine bone (pars perpendicularis; perpendicular plate of palatine bone)
- Vertical part of palatine bone (pars perpendicularis; perpendicular plate of palatine bone)
- processes
- Pyramidal process of palatine bone or Tuberosity (processus pyramidalis)
- Orbital process of palatine bone (processus orbitalis)
- processes
- Sphenoidal process of palatine bone (processus sphenoidalis)
- sphenopalatine notch
- Ossification of sphenoid
the vomer (Template:GraySubject)
the mandible (lower jaw) (Template:GraySubject)
- Body of mandible (corpus mandibulae)
- Body of mandible (corpus mandibulae)
- Ramus of mandible (ramus mandibulae; perpendicular portion of mandible)
- Ramus of mandible (ramus mandibulae; perpendicular portion of mandible)
- angle of the mandible
- Coronoid process (processus coronoideus)
- Condyloid process (processus condyloideus)
- mandibular notch
- Greater Cornua or Thyrohyals (cornua majora)
- Lesser Cornua or Ceratohyals (cornua minora)
- Norma verticalis
- coronal sutures
- sagittal sutures
- lambdoidal suture
- bregma
- lambda
- parietal eminence and parietal foramen
- obelion
- glabella
- superciliary arches
- frontal eminences
- frontal suture
- temporal lines
- incisive foramen
- incisive canals (foramina of Stenson)
- foramina of Scarpa
- greater palatine foramen
- pyramidal process of the palatine bone
- lesser palatine foramina
- posterior nasal spine
- choanæ
- pharyngeal canals
- pterygoid canal
- scaphoid fossa
- hamulus
- pharyngeal tubercle
- foramen ovale
- foramen spinosum
- spina angularis (sphenoidal spine)
- mandibular fossa
- petrotympanic fissure
- articular tubercle
- styloid process
- stylomastoid foramen
- tympanomastoid fissure
- mastoid notch
- occipital groove
- foramen lacerum
- pterygoid canal
- carotid canal
- sulcus tubæ auditivæ
- petrosphenoidal fissure
- carotid canal
- aquæductus cochleæ
- jugular foramen
- inferior tympanic canaliculus
- mastoid canaliculus
- petroöccipital fissure
- foramen magnum
- jugular process
- basion
- opisthion
- condyloid fossa
- Norma lateralis
- zygomaticotemporal suture
- zygomaticofrontal suture
- sphenozygomatic suture
- sphenofrontal suture
- sphenoparietal suture
- sphenosquamosal suture
- pterion
- squamosal suture
- parietomastoid suture
- coronal suture and lambdoidal suture
- occipitomastoid suture
- mastoid foramen
- asterion
- superciliary arch
- frontal eminence
- parietal eminence
- external occipital protuberance
- temporal lines
- Temporal fossa (fossa temporalis)
- stephanion
- zygomaticotemporal foramen
- infratemporal crest
- inferior orbital fissure or sphenomaxillary fissure
- zygomatic arch
- external acoustic meatus
- suprameatal triangle
- suprameatal spine
- mandibular fossa
- Infratemporal fossa (fossa infratemporalis; zygomatic fossa)
- zygomatic arch
- foramen ovale and foramen spinosum
- alveolar canals
- inferior orbital fissure (fissura orbitalis inferior; sphenomaxillary fissure)
- pterygomaxillary fissure
- Pterygopalatine fossa (fossa pterygopalatina; sphenomaxillary fossa)
- foramen rotundum
- pterygoid canal
- pharyngeal canal
- sphenopalatine foramen
- pterygopalatine canal
- Norma occipitalis
- sagittal suture
- lambdoidal suture
- parietomastoid suture
- occipitomastoid suture
- external occipital protuberance or inion
- planum occipitale
- planum nuchale
- mastoid foramen
- frontal eminences
- superciliary arches
- glabella
- frontal suture
- nasion
- supraorbital notch or supraorbital foramen
the interior of the skull (Template:GraySubject)
- Inner Surface of the Skull-cap
- Skull: upper surface of base of:
- Skull: fossa of:
- Anterior cranial fossa (fossa cranii anterior)
- Middle cranial fossa (fossa cranii media)
- Middle cranial fossa (fossa cranii media)
- Middle cranial fossa (fossa cranii media)
- Posterior cranial fossa (fossa cranii posterior)
- Posterior cranial fossa (fossa cranii posterior)
- The Points in the Median plane
- The Points on Either Side of the Median plane
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]

Overview
The skull is a bony structure found in many animals which serves as the general framework for the head. The skull supports the structures of the face and protects the head against injury.
The skull can be subdivided into two parts: the cranium and the mandible. A skull that is missing a mandible is only a cranium; this is the source of a very commonly made error in terminology. Those animals having skulls are called craniates.
Protection of the brain is only one part of the function of a bony skull. For example, a fixed distance between the eyes is essential for stereoscopic vision, and a fixed position for the ears helps the brain to use auditory cues to judge direction and distance of sounds. In some animals, the skull also has a defensive function (e.g. horned ungulates); the frontal bone is where horns are mounted.
Human skulls


In humans, the adult skull is normally made up of 22 bones. Except for the mandible, all of the bones of the skull are joined together by sutures, rigid articulations permitting very little movement. Eight bones form the neurocranium (braincase), a protective vault surrounding the brain. Fourteen bones form the splanchnocranium, the bones supporting the face. Encased within the temporal bones are the six ear ossicles of the middle ears, though these are not part of the skull. The hyoid bone, supporting the tongue, is usually not considered as part of the skull either, as it does not articulate with any other bones.
The skull contains the sinus cavities, which are air-filled cavities lined with respiratory epithelium, which also lines the large airways. The exact functions of the sinuses are unclear; they may contribute to lessening the weight of the skull with a minimal reduction in strength,or they may be important in improving the resonance of the voice. In some animals, such as the elephant, the sinuses are extensive. The elephant skull needs to be very large, to form an attachment for muscles of the neck and trunk, but is also unexpectedly light; the comparatively small brain-case is surrounded by large sinuses which reduce the weight. The meninges are the three layers, or membranes, which surround the structures of the nervous system. They are known as the dura mater, the arachnoid mater and the pia mater. Other than being classified together, they have little in common with each other.
In humans, the anatomical position for the skull is the Frankfurt plane, where the lower margins of the orbits and the upper borders of the ear canals are all in a horizontal plane. This is the position where the subject is standing and looking directly forward. For comparison, the skulls of other species, notably primates and hominids, may sometimes be studied in the Frankfurt plane. However, this does not always equate to a natural posture in life.
Possible types of skull fractures
Other skulls
Temporal Fenestra

The temporal fenestra are anatomical features of the amniote skull, characterised by bilaterally symmetrical holes (fenestrae) in the temporal bone. Depending on the lineage of a given animal, two, one, or no pairs of temporal fenestrae may be present, above or below the postorbital and squamosal bones. The upper temporal fenestrae are also known as the supratemporal fenestrae, and the lower temporal fenestrae are also known as the infratemporal fenestrae. The presence and morphology of the temporal fenestra is critical for taxonomic classification of the synapsids, of which mammals are part.
Physiological speculation associates it with a rise in metabolic rates and an increase in jaw musculature. The earlier amniotes of the Carboniferous did not have temporal fenestrae but the more advanced sauropsids and synapsids did. As time progressed, sauropsids’ and synapsids’ temporal fenestrae became more modified and larger to make stronger bites and more jaw muscles. Dinosaurs, which are sauropsids, have large advanced openings and their descendants, the birds, have temporal fenestrae which have been modified. Mammals, which are synapsids, possess no fenestral openings in the skull, as the trait has been modified. They do, though, still have the temporal orbit (which resembles an opening) and the temporal muscles. It is a hole in the head and is situated to the rear of the orbit behind the eye.
See also
- Bone terminology
- Anatomical terms of location
- Head and neck anatomy
- Phrenology, the pseudoscientific process of determining personality from the shape of the head.
References
- White, T.D. 1991. Human osteology. Academic Press, Inc. San Diego, CA.
External links
- Animal Skull Collection (Over 300 animal skull images compiled by U.S. high-school teacher)
- Skull terminology site by Texas A&M
- Anatomy of cranial cavity.
- Dept of Anth Skull Module
- Skull Anatomy Tutorial.
ar:جمجمة
bg:Череп
ca:Crani
cs:Lebka
cy:Penglog
da:Kranium
de:Schädel
eo:Kranio
eu:Burezur
gl:Cranio
ko:두개골
hr:Lubanja
id:Tengkorak
os:Сæргæхц
is:Höfuðkúpa
it:Cranio
he:גולגולת
la:Calva
lt:Galvos griaučiai
hu:Koponya
nl:Schedel
no:Skalle
simple:Skull
sk:Lebka
fi:Pääkallo
sv:Kranium
th:กะโหลกศีรษะ
uk:Череп
the extremities (Template:GraySubject)
the bones of the upper extremity
the clavicle (Template:GraySubject)
- (Ossa Extremitatis Superioris) & (Clavicula; Collar bone)
- clavicle
- coracoid tuberosity (conoid tubercle)
- oblique or trapezoid ridge
- costal tuberosity (rhomboid impression)
- subclavian groove
- Sternal extremity (extremitas sternalis; internal extremity)
- Acromial extremity (extremitas acromialis; outer extremity)
- Surfaces
- Surfaces
- Spine of scapula (spina scapulæ)
- Acromion
- Borders
- Borders
- Angles
- Angles
- Coracoid process (processus coracoideus)
the humerus (Template:GraySubject)
- Upper extremity of humerus
- head of humerus (caput humeri)
- surgical neck
- Anatomical neck (collum anatomicum)
- Greater tubercle (tuberculum majus; greater tuberosity)
- Lesser tubercle (tuberculum minus; lesser tuberosity)
- intertubercular groove (bicipital groove)
- crests of the greater and lesser tubercles (bicipital ridges)
- body of humerus or shaft of humerus (corpus humeri)
- body of humerus or shaft of humerus (corpus humeri)
the ulna (Template:GraySubject)
- Upper extremity of ulna (proximal extremity of ulna)
- Olecranon (olecranon process)
- Coronoid process (processus coronoideus)
- tuberosity of the ulna
- radial notch
- Upper extremity of ulna (proximal extremity of ulna)
- Semilunar notch (incisura semilunaris; greater sigmoid cavity)
- Radial notch (incisura radialis; lesser sigmoid cavity)
- Body of ulna or Shaft of ulna (corpus ulnæ)
- Body of ulna or Shaft of ulna (corpus ulnæ)
- perpendicular line
- medial surface (facies medialis; internal surface)
- Lower extremity (distal extremity)
the radius (Template:GraySubject)
- Upper extremity of radius (proximal extremity)
- Body of radius or Shaft of radius (corpus radii)
the hand
the carpus (Template:GraySubject)
- Bones of the Proximal Row (upper row)
- Navicular bone (os naviculare manus; scaphoid bone)
- Bones of the Proximal Row (upper row)
- Lunate bone (os lunatum; semilunar bone)
- Triangular bone (os triquetum; cuneiform bone)
- Bones of the Proximal Row (upper row)
- Pisiform bone (os pisiforme)
- Bones of the Distal Row (lower row)
- Greater multangular bone (os multangulum majus; trapezium)
- Lesser multangular bone (os multangulum minus; trapezoid bone)
- Bones of the Distal Row (lower row)
- Capitate bone (os capitatum; os magnum)
- Bones of the Distal Row (lower row)
- Hamate bone (os hamatum; unciform bone)
- phalanges (Phalanges digitorum manus)
- body
- proximal extremities
- distal extremities
- ungual phalanges
- Articulations
the bones of the lower extremity
the hip bone (Template:GraySubject)
- Ossa Extremitatis Inferioris & Os Coxæ; Innominate bone
- hip bone
- acetabulum
- obturator foramen
- Ilium (os ilii)
- arcuate line
- Body of ilium (corpus oss. ilii)
- Ala (ala oss. ilii)
- Ala (ala oss. ilii)
- Ala (ala oss. ilii)
- Ischium (os ischii)
- body of ischium (corpus ossis ischii)
- body of ischium (corpus ossis ischii)
- Superior ramus (ramus superior ossis ischii; descending ramus)
- Inferior ramus (ramus inferior ossis ischii; ascending ramus)
- Pubis (os pubis)
- Body of pubis (corpus oss. pubis)
- Superior ramus (ramus superior oss. pubis; ascending ramus)
- Inferior ramus (ramus inferior oss. pubis; descending ramus)
- Acetabulum (cotyloid cavity)
- Obturator foramen (foramen obturatum; thyroid foramen)
the pelvis (Template:GraySubject)
- bones comprising pelvis
- linea terminalis (pelvic brim)
- Greater pelvis or False pelvis (pelvis major)
- Lesser pelvis or True pelvis (pelvis minor)
- Lesser pelvis or True pelvis (pelvis minor)
the femur (Template:GraySubject)
- Upper extremity of femur (proximal extremity)
- Upper extremity of femur (proximal extremity)
- Trochanters
- Greater trochanter (trochanter major; great trochanter)
- trochanteric fossa (digital fossa)
- Upper extremity of femur (proximal extremity)
- Lesser trochanter (trochanter minor; small trochanter)
- tubercle of the femur
- intertrochanteric line (spiral line of the femur)
- Upper extremity of femur (proximal extremity)
- Body of femur or Shaft of femur (corpus femoris)
- Lower extremity of femur (distal extremity)
- Lower extremity of femur (distal extremity)
the patella (Template:GraySubject)
the tibia (Template:GraySubject)
- Body of tibia or Shaft of tibia (corpus tibiæ)
- Body of tibia or Shaft of tibia (corpus tibiæ)
- Body of tibia or Shaft of tibia (corpus tibiæ)
- Lower extremity of tibia
the fibula (Template:GraySubject)
- Fibula (Calf bone)
- Upper extremity or Head of fibula (capitulum fibulœ; proximal extremity)
- Body of fibula or shaft of fibula (corpus fibulæ)
- Body of fibula or shaft of fibula (corpus fibulæ)
- Lower extremity or Lateral malleolus (malleolus lateralis; distal extremity; external malleolus)
the foot
the tarsus (Template:GraySubject)
- Tarsal bones (Ossa tarsi)
- Calcaneus (Os calcis)
- Calcaneus (Os calcis)
- Talus (Astragalus, Ankle bone)
- Talus (Astragalus, Ankle bone)
- Cuboid bone (Os cuboideum)
- Navicular bone of tarsus (Os naviculare pedis)
- Cuneiform bones
- First cuneiform bone (Os cuneiforme primum)
- Cuneiform bones
- Second cuneiform bone (Os cuneiforme secundum)
- Third cuneiform bone (Os cuneiforme tertium)
- phalanges of the foot (Phalanges Digitorum Pedis)
- ungual phalanges
comparison of the bones of the hand and foot (Template:GraySubject)
- Comparison of bones of hand and foot
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]
A limb (from the Old English lim) is a jointed, or prehensile (as octopus tentacles or new world monkey tails), appendage of the human or animal body; a large or main branch of a tree; a representative, branch or member of a group or organization.
Most animals use limbs for locomotion, such as walking, running, or climbing. Some animals can use their front limbs (or upper limbs in humans) to carry and manipulate objects. Some animals can also use hind limbs for manipulation.
In the human body, the upper and lower limbs are commonly called the arms and the legs. Human legs and feet are specialised for two-legged locomotion — most other mammals walk and run on all four limbs. Human arms are weaker, but very mobile allowing us to reach at a wide range of distances and angles, and end in specialised hands capable of grasping and fine manipulation of objects.
See also
References
Template:Human anatomical features
ca:Pota cs:Končetina de:Gliedmaßen et:Jäsemed eu:Gorputz-adar hr:Ekstremitet it:Arto nl:Ledemaat simple:Limb sv:Extremiteter uk:Кінцівки Template:Jb1 Template:WH Template:WS
Looking for the patient version?
© 2026 MyEClinic – IFTM Institut für Telematik in der Medizin GmbH