
Mitral valve prolapse
For patient information click here
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor-In-Chief: Cafer Zorkun, M.D., Ph.D. [2]
Synonyms and keywords: Barlow syndrome; floppy mitral valve; systolic click—murmur syndrome; redundant cusp syndrome; billowing mitral valve syndrome
Overview
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]
Overview
Mitral valve prolapse (MVP) is a valvular heart disease characterized by the displacement of an abnormally thickened mitral valve leaflet into the left atrium during systole. In its nonclassic form, MVP carries a low risk of complications. In severe cases of classic MVP, complications include mitral regurgitation and infective endocarditis.
References
Historical Perspective
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]
Overview
Historical Perspective
The term mitral valve prolapse was coined by J. Michael Criley in 1966 and gained acceptance over the other descriptor of “billowing” of the mitral valve, as originally described by JB Barlow.[1]. Barlow had postulated that mitral valve prolapse was due to an aneurysm of the mitral leaflet and Criley demonstrated that it was instead due to displacement of the leaflet that led to the condition.
For many years, mitral valve prolapse was a poorly understood anomaly associated with a wide variety of both related and seemingly unrelated signs and symptoms, including late systolic murmurs, inexplicable panic attacks, and polythelia (extra nipples). Recent studies suggest that these symptoms were incorrectly linked to MVP because the disorder was simply over-diagnosed at the time. Continuously-evolving criteria for diagnosis of MVP with echocardiography have made the diagnosis more rigorous and specific. As a result, there may have been many patients who would not currently be classified as having MVP who were included in original studies of the disorder and its prevalence. In fact, some modern studies report that as many as 55% of the population would be diagnosed with MVP if older, less specific criteria for the diagnosis of MVP, such as M-mode echocardiography—were applied today.
In recent years, new objective diagnostic criteria for MVP have been proposed based upon two- and three-dimensional echocardiography. The disorder has also been classified into a number of subtypes with respect to these echocardiographic criteria.
-
 St. Zenon of Verona wearing a mitre.
St. Zenon of Verona wearing a mitre.

References
Classification
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]
Overview
Classification
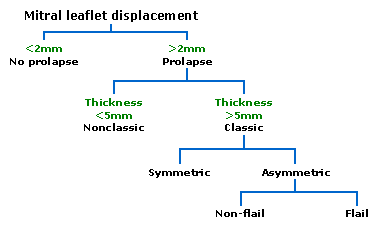
Prolapsed mitral valves are classified into several subtypes, based on leaflet thickness, concavity, and type of connection to the mitral annulus. Subtypes can be described as classic, nonclassic, symmetric, asymmetric, flail, or non-flail.
Note: all measurements below refer to adult patients and applying them to children may be misleading.
-
 Diagnosis of mitral valve prolapse is based on modern echocardiographic techniques which can pinpoint abnormal leaflet thickening and other related pathology.
Diagnosis of mitral valve prolapse is based on modern echocardiographic techniques which can pinpoint abnormal leaflet thickening and other related pathology.

Classic versus nonclassic
Prolapse occurs when the mitral valve leaflets are displaced more than 2 mm above the mitral annulus high points. The condition can be further divided into classic and nonclassic subtypes based on the thickness of the mitral valve leaflets: up to 5 mm is considered nonclassic, while anything beyond 5 mm is considered classic MVP.
Symmetric versus asymmetric
Classic MVP may be subdivided into symmetric and asymmetric, referring to the point at which leaflet tips join the mitral annulus. In symmetric coaptation, leaflet tips meet at a common point on the annulus. Asymmetric coaptation is characterized by one leaflet being displaced toward the atrium with respect to the other. Patients with asymmetric prolapse are susceptible to severe deterioration of the mitral valve, with the possible rupture of the chordae tendineae and the development of a flail leaflet.
Flail versus non-flail
Asymmetric prolapse is further subdivided into flail and non-flail prolapse. Flail prolapse occurs when a leaflet tip turns outward, becoming concave toward the left atrium, causing the deterioration of the mitral valve. The severity of flail leaflet varies, ranging from tip eversion to chordal rupture. Dissociation of leaflet and chordae tendineae provides for unrestricted motion of the leaflet (hence “flail leaflet”). Thus patients with flail leaflets have a higher prevalence of mitral regurgitation than those with the non-flail subtype.
References
Pathophysiology
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]
Overview
Pathophysiology
The mitral valve, so named because of its resemblance to a bishop’s miter, is the heart valve that prevents the backflow of blood from the left ventricle into the left atrium. It is composed of two leaflets (one anterior, one posterior) that close when the left ventricle contracts.[1]
Each leaflet is composed of three layers of tissue: the atrialis, fibrosa, and spongiosa. Patients with classic mitral valve prolapse have excess connective tissue that thickens the spongiosa and separates collagen bundles in the fibrosa. This is due to an excess of dermatan sulfate, a glycosaminoglycan. This weakens the leaflets and adjacent tissue, resulting in increased leaflet area and elongation of the chordae tendineae. Elongation of the chordae may be associated with chordae rupture, and is commonly found in the chordae tendineae attached to the posterior leaflet. Advanced lesions — also commonly involving the posterior leaflet — lead to leaflet folding, inversion, and displacement toward the left atrium.
Associated Conditions
Mitral valve prolapse syndrome
Mitral valve prolapse syndrome (MVP Syndrome), also referred to as mitral valve prolapse dysautonomia, is thought to represent an imbalance of the autonomic nervous system in association with mitral valve prolapse. The underlying etiology that causes both autonomic dysregulation and the structural abnormalities present in mitral valve prolapse is unknown. Most patients who suffer from mitral valve prolapse syndrome may have an underlying dysautonomia as the cause of their symptoms. In particular, supraventricular arrhythmias such as those observed with MVP syndrome are associated with increased parasympathetic tone.[2]
Symptoms generally attributed to MVP syndrome include palpitations, shortness of breath, and syncope. Because of the low specificity of these symptoms, and the fact that there is significant overlap in the causes of these symptoms with sequelae of significant mitral regurgitation often seen with mitral valve prolapse, MVP syndrome is most likely over-diagnosed.[3] The uncertainty regarding the frequency of this syndrome may in part be due to the fact that there is no consensus criteria to diagnose MVP syndrome.
References
- ↑ Women’s Heart Foundation, Inc. “Mitral Valve Prolapse”. Retrieved 2007-07-11.
- ↑ Terechtchenko L, Doronina SA, Pochinok EM, Riftine A. (2003). “Autonomic tone in patients with supraventricular arrhythmia associated with mitral valve prolapse in young men”. Pacing Clin Electrophysiol. 26 (1 Pt 2): 444–6. PMID 12687863.
- ↑ Fogoros, Richard N. “Mitral Valve Prolapse (MVP)”. Heart Disease. About.com. Retrieved 2007-07-11.
Causes
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Farman Khan, MD, MRCP [2]
Overview
Mitral valve prolapse (MVP) is a valvular heart disease that is considered to be mainly hereditary. Myxomatous degeneration of the mitral valve is a common cause of MVP. Other less common causes of MVP include connective tissue diseases such as Marfan’s syndrome, Ehlers Danlos syndrome and osteogenesis imperfecta, as well as damage to the mitral valve secondary to infarction, rheumatic heart disease, hypertrophic cardiomyopathy and trauma.
Causes
Common Causes
- Marfan’s syndrome
- Myxomatous degeneration of the mitral valve
- Papillary muscle infarction
- Papillary muscle trauma
Causes by Organ System
| Cardiovascular | myxomatous of the mitral valve, myocardial infarction, severe mitral annular calcification, damaged chordae tendineae, rheumatic heart disease, papillary muscle dysfunction, hypertrophic cardiomyopathy, forme fruste Barlow disease, Ebstein’s anomaly , cardiomegaly, bacterial endocarditis, congenital heart disease |
| Chemical/Poisoning | No underlying causes |
| Dental | No underlying causes |
| Dermatologic | No underlying causes |
| Drug Side Effect | No underlying causes |
| Ear Nose Throat | No underlying causes |
| Endocrine | Graves disease |
| Environmental | No underlying causes |
| Gastroenterologic | No underlying causes |
| Genetic | Turner Syndrome, spastic ataxia, Charlevoix-Saguenay type, osteogenesis imperfecta, X-linked familial mitral valve prolapse, autosomal dominant familial mitral valve prolapse, MASS phenotype, Marfan syndrome, Marfan-like syndrome Boileau type, Hunter-Mcdonald syndrome, Furlong-Kurczynski-Hennessy syndrome |
| Hematologic | Von Willebrand disease, sickle cell disease |
| Iatrogenic | No underlying causes |
| Infectious Disease | Infective endocarditis, acute rheumatic fever |
| Musculoskeletal/Orthopedic | Dermato-cardio-skeletal syndrome Borrone type |
| Neurologic | No underlying causes |
| Nutritional/Metabolic | Scurvy |
| Obstetric/Gynecologic | Pregnancy |
| Oncologic | No underlying causes |
| Ophthalmologic | No underlying causes |
| Overdose/Toxicity | No underlying causes |
| Psychiatric | No underlying causes |
| Pulmonary | No underlying causes |
| Renal/Electrolyte | Polycystic kidney disease |
| Rheumatology/Immunology/Allergy | SLE, pseudoxanthoma elasticum, polyarteritis nodosa, connective tissue disease, mixed connective tissue disease, Ehlers-Danlos syndrome type I, Ehlers-Danlos syndrome type II, Ehlers-Danlos syndrome Type V |
| Sexual | No underlying causes |
| Trauma | Trauma to mitral valve |
| Urologic | No underlying causes |
| Miscellaneous | Stickler Syndrome, Leopard syndrome, idiopathic, fibroelastic deficiency, Dahlberg syndrome, Beals syndrome |
Causes in Alphabetical Order
|
|
|
References
Epidemiology and Demographics
Please help WikiDoc by adding more content here. It’s easy! Click here to learn about editing.
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]
Overview
Incidence
Prior to the development of rigorous criteria for the diagnosis and classification of mitral valve prolapse, as described above, the incidence of mitral valve prolapse in the general population varied significantly. Studies estimated the incidence of mitral valve prolapse at 5 to 15 percent or even higher.[1]
Prevalence
As part of the Framingham Heart Study, more modern estimates of the prevalence of mitral valve prolapse have been lower at 2.4%. There was a near-even split between classic and nonclassic MVP, with no significant age or sex discrimination.[2] Based on data gathered in the United States, MVP is prevalent in 7% of autopsies.
References
- ↑ Levy D, Savage D. (1987). “Prevalence and clinical features of mitral valve prolapse”. Am Heart J. 113 (5): 1281–90. PMID 3554946.
- ↑ Freed LA, Levy D, Levine RA, Larson MG, Evans JC, Fuller DL, Lehman B, Benjamin EJ. (1999). “Prevalence and clinical outcome of mitral-valve prolapse”. N Engl J Med. 341 (1): 1–7. PMID 10387935.
Natural History, Complications and Prognosis
Please help WikiDoc by adding more content here. It’s easy! Click here to learn about editing.
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]
Overview
Natural History
Complications
- Infective Endocarditis
- Mitral regurgitation – Mitral valve prolapse is frequently associated with mild mitral regurgitation,[1] where blood aberrantly flows from the left ventricle into the left atrium during systole. Occasionally MVP patients experience severe regurgitation, often due to chordae tendineae rupture.[2]
- Stroke
- Clots to other areas
- Sudden death – severe mitral valve prolapse is associated with arrhythmias and atrial fibrillation that may progress and lead to sudden death. As there is no evidence that a prolapsed valve itself contributes to such arrythmias, these complications are more likely due to mitral regurgitation and congestive heart failure.
Prognosis
The major predictors of mortality are the severity of mitral regurgitation and the ejection fraction.[3] Generally, MVP is a benign disorder. However, MVP patients with a murmur, not just an isolated click, may have a poorer prognosis.
References
- ↑ Kolibash AJ (1988). “Progression of mitral regurgitation in patients with mitral valve prolapse”. Herz. 13 (5): 309–17. PMID 3053383.
- ↑ Tanser, Paul H. (March 2007). “Mitral Valve Prolapse (MVP)”. Merck. Retrieved 2007-07-11.
- ↑ Rodgers, Ellie (May 11, 2004). “Mitral Valve Regurgitation”. Healthwise, on Yahoo. Retrieved 2007-07-11.
Diagnosis
Diagnosis
History and Symptoms | Physical Examination | Chest X ray | CT | MRI | Echocardiography | Left ventriculography
Looking for the patient version?
© 2026 MyEClinic – IFTM Institut für Telematik in der Medizin GmbH