
Pulmonary edema
For patient information click here
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor-In-Chief: Farnaz Khalighinejad, MD [2]
Synonyms and keywords: Pulmonary edema; lung edema; lung congestion; lung water; pulmonary congestion
Overview
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1] Associate Editor(s)-in-Chief: Farnaz Khalighinejad, MD [2]
Overview
Pulmonary edema is fluid accumulation in the lungs. This fluid accumulation leads to impaired gas exchange and hypoxia.
Historical Perspective
Pulmonary edema was first described as a result of heart failure by Andreas Nerlich. In 1891 the first case of high altitude pulmonary edema was reported. In 1908, W. T. Shanahan noted acute pulmonary edema as an adverse effect of epileptic seizures.
Classification
Pulmonary edema can be classified on the basis of etiology into 2 subtypes, including cardiogenic pulmonary edema (left ventricular failure, myocardial infarction, left ventricle hypertrophy cardiomyopathy) and, noncardiogenic pulmonary edema (acute respiratory distress syndrome, pneumonia, pulmonary embolism, chest trauma).
Pathophysiology
Pulmonary edema is due to either failure of the heart to remove fluid from the lung circulation (“cardiogenic pulmonary edema”), or due to a direct injury to the lung parenchyma or increased permeability or leakiness of the capillaries (“noncardiogenic pulmonary edema”).
Causes
Common causes of cardiogenic pulmonary edema are cardiomyopathy, congestive heart failure, coronary heart disease, aortic regurgitation, aortic stenosis. Common causes of noncardiogenic pulmonary edema are acute respiratory distress syndrome, high altitude pulmonary edema, pulmonary embolism.
Differentiating Pulmonary edema from Other Diseases
Pulmonary edema should be distinguished from other conditions that cause dyspnea, orthopnea, cough.
Epidemiology and Demographics
The prevalence of pulmonary edema was estimated to be 75000-83000 cases per 100,000 individuals among heart failure patients with reduced ejection fraction. Pulmonary edema commonly affects individuals older than 65 years of age. Males are more commonly affected by pulmonary edema than woman.
Risk Factors
The risk factors in pulmonary edema refer to the risk factors for the underlying disease that cause pulmonary edema. Risk factors of cardinogenic pulmonary edema include high blood pressure, hyperlipidemia, atherosclerosis, diabetes mellitus, obesity. And risk factors for noncardiogenic pulmonary edema include sepsis, aspiration, pneumonia.
Screening
There is insufficient evidence to recommend routine screening for pulmonary edema.
Natural History, Complications and Prognosis
Some patients may need to use a breathing machine for a long time, which may lead to damage to lung tissue.Kidney failure and damage to other major organs may occur if blood and oxygen flow are not restored promptly. If not treated, this condition can be fatal. If left untreated, acute pulmonary edema can lead to coma and even death, generally due to its main complication of hypoxia.
Diagnosis
Pulmonary artery catheterization is the gold standard test for the diagnosis of pulmonary edema. Elevated pulmonary-artery pressure indicates cardiogenic pulmonary edema or pulmonary edema due to volume overload.
History and Symptoms
The history of a patient with pulmonary edema varies according to the underlying cause. The most common symptom of pulmonary edema is shortness of breath (dyspnea). Depending on the cause, it may occur acutely or have a gradual onset. When pulmonary edema is due to an acute myocardial infarction chest pain is common symptom.
Physical Examination
Patients with pulmonary edema usually appear agitated. Physical examination of patients with pulmonary edema is usually remarkable for dyspnea, tachypnea. The presence of abnormal cardiac examination on physical examination is diagnostic of cardiogenic pulmonary edema. Patients with noncardiogenic pulmonary edema may have warm extremities, whereas patients with cardiogenic pulmonary edema may have cool extremities.
Laboratory Findings
Chest X Ray
The diagnosis is confirmed on X-ray of the lungs, which shows increased fluid in the alveolar walls. Kerley B lines, increased vascular filling, pleural effusions, upper lobe diversion (increased blood flow to the higher parts of the lung) may be indicative of cardiogenic pulmonary edema, while patchy alveolar infiltrates with air bronchograms are more indicative of noncardiogenic edema
Electrocardiography
Although there is no diagnostic criteria of pulmonary edema on the EKG, there may be signs of the underlying cardiogenic cause of pulmonary edema.
CT
Thoracic CT scan may be helpful in the diagnosis of pulmonary edema. Findings on CT scan diagnostic of hydrostatic pulmonary edema include cardiomegaly, vascular engorgment, pleural effusions.
MRI
There are no MRI findings associated with pulmonary edema.
Echocardiography
Echocardiography is useful in confirming a cardiac or no-cardiac cause of pulmonary edema. Echocardiography may identify the presence and severity of valvular causes of pulmonary edema. Echocardiography is helpful in diagnosis of ischemia or myocardial infarction, cardiomyopathy as an underlying cause of pulmonary edema. Echocardiography is less sensitive in identifying diastolic dysfunction. Thus, a normal echocardiogram may not rule out cardiogenic pulmonary edema.
Other imaging findings
There are no additional imaging findings associated with pulmonary edema.
Other diagnostic findings
Pulmonary artery catheterization is the gold standard test for the diagnosis of pulmonary edema. Elevated pulmonary-artery pressure indicates cardiogenic pulmonary edema or pulmonary edema due to volume overload.
Treatment
Medical Therapy
Pulmonary edema classified into cardiogenic and non-cardiogenic pulmonary edema, each requires different management and has a different prognosis. The main goal of a treatment are alleviate symptoms and improving hemodynamics. The initial management of patients is following the ABCs of resuscitation, that is, airway, breathing, and circulation. Medical treatment of cardiogenic pulmonary edema focuses on preload reduction, afterload reduction and inotropic support.
Surgery
The mainstay of treatment for pulmonary edema is medical therapy. Surgery is usually reserved for patients who experienced cardiogenic shock following acute cardiogenic pulmonary edema.
Primary Prevention
Effective measures for the primary prevention of cardiogenic pulmonary edema include maintaining a healthy lifestyle, avoid tobacco, treat dyslipidemia, low salt diet, controlling hypertension, avoid cardiotoxic agents, controling diabetes. Effective measures for the primary prevention of high-altitude pulmonary edema include, encourage healthy lifestyle and exercise, gradual ascent, preacclimization, avoiding alcohol ingestion, high carbohydrate in diet, adequate hydration, vigorous exertion during the first few days at high altitude, oxygen enrichment.
Secondary Prevention
The major complications of cardiogenic pulmonary edema are respiratory failure and sudden cardiac death secondary to cardiac arrhythmia. Prompt diagnosis and treatment are effective for secondary prevention in cardiogenic pulmonary edema.
References
Historical Perspective
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1] Associate Editor(s)-in-Chief: Farnaz Khalighinejad, MD [2]
Overview
Pulmonary edema was first described as a result of heart failure by Andreas Nerlich. In 1891 the first case of high altitude pulmonary edema was reported. In 1908, W. T. Shanahan noted acute pulmonary edema as an adverse effect of epileptic seizures.
Historical Perspective
- Pulmonary edema was first described as a result of heart failure by Andreas Nerlich, a pathologist from Munich, Germany.[1]
- In 1891 the first case of high altitude pulmonary edema was reported.[2]
- In 1913, TH Ravenhill suggested first diagnostic framework for high altitude pulmonary edema.[2]
- In 1908, W. T. Shanahan noted acute pulmonary edema as an adverse effect of epileptic seizures.[3][4]
- During WWI, francois Moutier noted the sudden onset of pulmonary edema among soldiers shot in the head.[3][4]
- In the Vietnam War, alveolar edema and hemorrhage seen in the lungs of soldiers dying after isolated bullet head wounds.[5]
Landmark Events in the Development of Treatment Strategies
- In 1953, intra-aortic balloon pumping (IABP) was described by Kantrowitz.[6]
- In 1962, the modern intra-aortic counterpulsation device was described by Moulopoulos et al at the Cleveland Clinic.[7]
- In 1969 intra-aortic balloon pumping (IABP) was first used clinically in a patient with cardiogenic shock.
- Since the 1980s, IABP has been increasingly used in stabilizing patient with cardiogenic pulmonary edema before definitive therapy.
References
- ↑ Bianucci R, Loynes RD, Sutherland ML, Lallo R, Kay GL, Froesch P, Pallen MJ, Charlier P, Nerlich AG (September 2016). “Forensic Analysis Reveals Acute Decompensation of Chronic Heart Failure in a 3500-Year-Old Egyptian Dignitary”. J. Forensic Sci. 61 (5): 1378–81. doi:10.1111/1556-4029.13138. PMID 27362779.
- ↑ 2.0 2.1 Gensini GF, Conti AA (March 2003). “A historical perspective on high altitude pulmonary edema”. Monaldi Arch Chest Dis. 60 (1): 45–7. PMID 12827832.
- ↑ 3.0 3.1 Davison DL, Terek M, Chawla LS (December 2012). “Neurogenic pulmonary edema”. Crit Care. 16 (2): 212. doi:10.1186/cc11226. PMC 3681357. PMID 22429697.
- ↑ 4.0 4.1 Izumida H, Homma K, Sasaki J, Hori S (April 2017). “Pulmonary edema following tonic-clonic seizure”. Acute Med Surg. 4 (2): 221–222. doi:10.1002/ams2.251. PMC 5667274. PMID 29123866.
- ↑ Simmons RL, Heisterkamp CA, Collins JA, Genslar S, Martin AM (July 1969). “Respiratory insufficiency in combat casualties. 3. Arterial hypoxemia after wounding”. Ann. Surg. 170 (1): 45–52. PMC 1387602. PMID 5789529.
- ↑ Ali, Jason M.; Abu-Omar, Yasir (2018). “The intra-aortic balloon pump and other methods of mechanical circulatory support”. Surgery (Oxford). 36 (2): 68–74. doi:10.1016/j.mpsur.2017.11.002. ISSN 0263-9319.
- ↑ MOULOPOULOS SD, TOPAZ S, KOLFF WJ (May 1962). “Diastolic balloon pumping (with carbon dioxide) in the aorta–a mechanical assistance to the failing circulation”. Am. Heart J. 63: 669–75. PMID 14476645.
Classification
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1] Associate Editor(s)-in-Chief: Farnaz Khalighinejad, MD [2]
Overview
Pulmonary edema can be classified on the basis of etiology into 2 subtypes, including cardiogenic pulmonary edema (left ventricular failure, myocardial infarction, left ventricle hypertrophy cardiomyopathy) and, noncardiogenic pulmonary edema (high altitude pulmonary edema, neurogenic pulmonary edema, reperfusion pulmonary edema, re-expansion pulmonary edema)
Classification
Pulmonary edema may be classified according to etiology into 2 groups:
- Cardiogenic pulmonary edema, which can be secondary to:[1]
- Left ventricular failure
- Dysrhythmia
- Left ventricular hypertrophy cardiomyopathy
- Volume overload
- Myocardial Infarction
- Left ventricular outflow obstruction
- Non-cardiogenic pulmonary edema which can be secondary to:[2]
- Acute respiratory distress syndrome (ARDS)
- High altitude pulmonary edema
- Neurogenic pulmonary edema
- Reperfusion pulmonary edema
- Re-expansion pulmonary edema
- Others(opioid overdose, salicylate toxicity, viral infections)
Pulmonary edema Cardiogenic Non-cardiogenic LV failure Dysrhythmia LV hypertrophy and cardiomyopathy Volume overload Myocardial Infarction LV outflow obstruction Direct injury to lung Hematogenous injury to lung Lung injury plus elevated hydrostatic pressure Chest trauma,pulmonary contusion Aspiration Smoke inhalation Pneumonia Oxygen toxicity Pulmonary embolism,reperfusion High altitude pulmonary edema Neurogenic pulmonary edema Reexpansion pulmonary edema Sepsis Pancreatitis Nonthoracic trauma Multiple transfusions Intravenous drug use. e.g. heroin References
- ↑ Attias D, Mansencal N, Auvert B, Vieillard-Baron A, Delos A, Lacombe P, N’Guetta R, Jardin F, Dubourg O (2010). “Prevalence, characteristics, and outcomes of patients presenting with cardiogenic unilateral pulmonary edema”. Circulation. 122 (11): 1109–15. doi:10.1161/CIRCULATIONAHA.109.934950. PMID 20805429.
- ↑ Calenoff L, Kruglik GD, Woodruff A (1978). “Unilateral pulmonary edema”. Radiology. 126 (1): 19–24. doi:10.1148/126.1.19. PMID 619405.
Pathophysiology
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1] Associate Editor(s)-in-Chief: Farnaz Khalighinejad, MD [2]
Overview
Pulmonary edema is due to either failure of the heart to remove fluid from the lung circulation (“cardiogenic pulmonary edema”), or due to a direct injury to the lung parenchyma or increased permeability or leakiness of the capillaries (“noncardiogenic pulmonary edema”).
Pathophysiology
It is understood that pulmonary edema is the abnormal increase in extravascular lung water (EVLW). This condition may be caused by the following underlying physiologic changes:[1][2][3]
- Imbalance of staling force
- Altered valvular capillary membrane permeability
- Lymphatic insufficiency
- Other factors
These factors have been described bellow:
Imbalance of starling force
The flux of fluid across the capillary wall is controlled by a balance between hydrostatic pressure and osmotic pressure gradients between the capillaries and interstitial space that can be calculated via Starling equation:
JV = K.S.([Pmv-Ppmv]-σd[πmv-πpmv])
where:
- JV = volume flow across the capillary bed
- K = filtration coefficient of the capillary wall
- S = surface area of the capillary bed
- Pmv = microvascular hydrostatic pressure
- Ppmv = perimicrovascular (interstitial) hydrostatic pressure
- πmv = plasma colloid osmotic pressure
- πpmv = perimicrovascular (interstitial) colloid osmotic pressure
- σd = protein reflection coefficient
- Increase pulmonary capillary pressure
- In cardiogenic pulmonary edema, the most common mechanism for a rise in transcapillary filtration is an increase in pulmonary capillary pressure.
- Left ventricular failure
- Left ventricular outflow obstruction
- Mitral stenosis
- In cardiogenic pulmonary edema, the most common mechanism for a rise in transcapillary filtration is an increase in pulmonary capillary pressure.
- Increase negative interstitial pressure
- Negative-pressure pulmonary edema (NPPE) or postobstructive pulmonary edema[4]
- It is understood that postobstructive pulmonary edema is caused by highly negative intrathoracic pressure that create by forceful attempts to inhale against an obstruction, this causes elevated venous return, declined cardiac output and fluid transudation into the alveolar space.
- Negative-pressure pulmonary edema (NPPE) or postobstructive pulmonary edema[4]
Altered alveolar-capillary membrane permeability (acute respiratory distress syndrome)
Following are a few important aspects about altered alveolar capillary membrane permeability leading to pulmonary edema:
- In noncardiogenic pulmonary edema, the most common mechanism for a rise in transcapillary filtration is an increase in capillary permeability.
- This increase in permeability damages the alveolar-capillary membrane, causing increased movement of water and proteins from the intravascular space to the interstitial space.
- In most cases of noncardiogenic pulmonary edema, the concentration of protein in the interstitium exceeds 60 percent of the plasma value, compared to less than 45 percent in cardiogenic pulmonary edema.
ARDS can be seen in a number of disorders:
- Sepsis
- Acute pulmonary infection
- Non-thoracic trauma
- Disseminated intravascular coagulation
- Aspiration
Lymphatic insufficiency
Lymphatic insufficiency may follow:
- Lymphangitic carcinomatosis
- Fibrosing lymphangitis
Other factors
Various other factors contributing to the development of pulmonary edema include:
- High-altitude pulmonary edema
- It is understood that high-altitude pulmonary edema is caused by hypoxic pulmonary vasoconstriction at altitudes above 12,000 to 13,000 feet (3600 to 3900 m).[5]
- Neurogenic pulmonary edema
- It is understood that neurogenic pulmonary edema is caused by sympathetic overreactivity with massive catecholamine surges that shifts blood from the systemic to the pulmonary circulation.[6]
- Narcotic overdose
- The exact pathogenesis of narcotic overdose pulmonary edema is not fully understood. Proposed mechanisms include combination of direct toxicity of the drug, hypoxia, and acidosis secondary to hypoventilation and/or cerebral edema.[7]
- Pulmonary embolism
- It is understood that pulmonary embolism can cause pulmonary edema by damaging the pulmonary and nearby pleural systemic circulations, increasing hydrostatic pressures in pulmonary and/or systemic veins, and decreasing pleural pressure due to atelectasis.[8]
- Re-expansion pulmonary edema
- The exact pathogenesis of re-expansion pulmonary edema is not fully understood. Direct injury from surfactant dysfunction in chronic atelectatic lung, elevated transpleural pressures, or indirect injury from reperfusion has been proposed.[9]
Gross Pathology
-
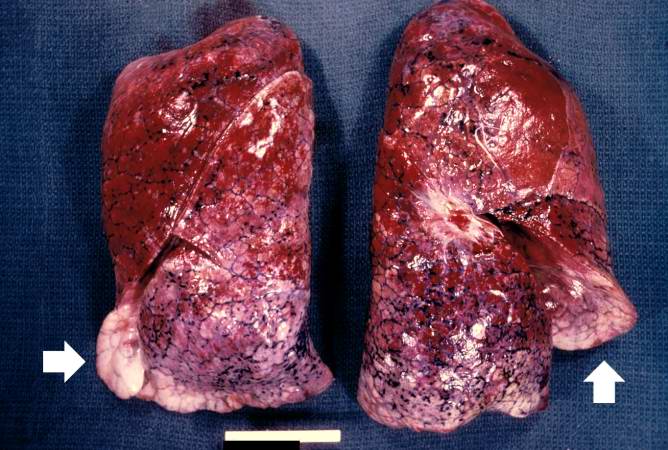 Distended and red lungs. The reddish coloration of the tissue is due to congestion. Some normal pink lung tissue is seen at the edges of the lungs (arrows).
Distended and red lungs. The reddish coloration of the tissue is due to congestion. Some normal pink lung tissue is seen at the edges of the lungs (arrows). -
 This is a gross photograph of lung demonstrating acute pulmonary congestion and edema. A frothy exudate fills the bronchus (arrow).
This is a gross photograph of lung demonstrating acute pulmonary congestion and edema. A frothy exudate fills the bronchus (arrow). -
 This gross photograph demonstrates the frothy exudate that is being extruded from the lung tissue.
This gross photograph demonstrates the frothy exudate that is being extruded from the lung tissue.



Microscopic Pathology
-
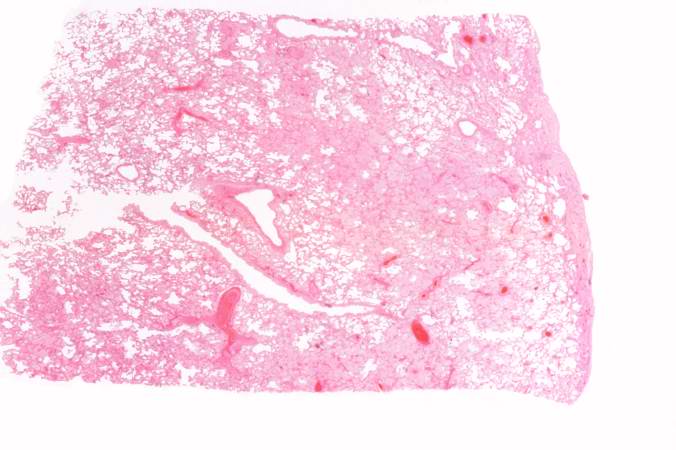 This is a low-power photomicrograph of lung from this case. The lung section has a pale-red color indicating proteinaceous material within the lung.
This is a low-power photomicrograph of lung from this case. The lung section has a pale-red color indicating proteinaceous material within the lung. -
 This is a higher-power photomicrograph of lung. The edema fluid within the alveoli is visible at this higher magnification (arrows). The thickened pleura (1) is on the left.
This is a higher-power photomicrograph of lung. The edema fluid within the alveoli is visible at this higher magnification (arrows). The thickened pleura (1) is on the left.


-
 This is a higher-power photomicrograph showing edema-filled alveoli in the right portion of this section (arrows).
This is a higher-power photomicrograph showing edema-filled alveoli in the right portion of this section (arrows). -
 This high-power photomicrograph illustrates the edema fluid within the alveoli (1) and the congestion (RBCs) in the alveolar capillaries (arrows).
This high-power photomicrograph illustrates the edema fluid within the alveoli (1) and the congestion (RBCs) in the alveolar capillaries (arrows).


References
- ↑ Sibbald WJ, Cunningham DR, Chin DN (1983). “Non-cardiac or cardiac pulmonary edema? A practical approach to clinical differentiation in critically ill patients”. Chest. 84 (4): 452–61. PMID 6617283.
- ↑ Ware LB, Matthay MA (2005). “Clinical practice. Acute pulmonary edema”. N. Engl. J. Med. 353 (26): 2788–96. doi:10.1056/NEJMcp052699. PMID 16382065.
- ↑ Pena-Gil C, Figueras J, Soler-Soler J (2005). “Acute cardiogenic pulmonary edema–relevance of multivessel disease, conduction abnormalities and silent ischemia”. Int. J. Cardiol. 103 (1): 59–66. doi:10.1016/j.ijcard.2004.08.029. PMID 16061125.
- ↑ Bhattacharya M, Kallet RH, Ware LB, Matthay MA (2016). “Negative-Pressure Pulmonary Edema”. Chest. 150 (4): 927–933. doi:10.1016/j.chest.2016.03.043. PMID 27063348.
- ↑ Dunham-Snary KJ, Wu D, Sykes EA, Thakrar A, Parlow LR, Mewburn JD, Parlow JL, Archer SL (2017). “Hypoxic Pulmonary Vasoconstriction: From Molecular Mechanisms to Medicine”. Chest. 151 (1): 181–192. doi:10.1016/j.chest.2016.09.001. PMC 5310129. PMID 27645688.
- ↑ Busl KM, Bleck TP (2015). “Neurogenic Pulmonary Edema”. Crit. Care Med. 43 (8): 1710–5. doi:10.1097/CCM.0000000000001101. PMID 26066018.
- ↑ Radke JB, Owen KP, Sutter ME, Ford JB, Albertson TE (2014). “The effects of opioids on the lung”. Clin Rev Allergy Immunol. 46 (1): 54–64. doi:10.1007/s12016-013-8373-z. PMID 23636734.
- ↑ Porcel JM, Light RW (2008). “Pleural effusions due to pulmonary embolism”. Curr Opin Pulm Med. 14 (4): 337–42. doi:10.1097/MCP.0b013e3282fcea3c. PMID 18520269.
- ↑ Feller-Kopman D, Berkowitz D, Boiselle P, Ernst A (2007). “Large-volume thoracentesis and the risk of reexpansion pulmonary edema”. Ann. Thorac. Surg. 84 (5): 1656–61. doi:10.1016/j.athoracsur.2007.06.038. PMID 17954079.
Causes
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1] Associate Editor(s)-in-Chief: Farnaz Khalighinejad, MD [2]
Overview
Common causes of cardiogenic pulmonary edema are cardiomyopathy, congestive heart failure, coronary heart disease, aortic regurgitation, aortic stenosis. Common causes of noncardiogenic pulmonary edema are acute respiratory distress syndrome, high altitude pulmonary edema, pulmonary embolism.
Causes
Common Causes
- Congestive heart failure
- Coronary Heart Disease
- Aortic Regurgitation
- Aortic Stenosis
- Mitral Regurgitation
- Mitral Stenosis
- Myocarditis
- Pericardial Disease
- Infection
- Sepsis
Causes by Organ System
| Cardiovascular |
Severe Arrhythmias (tachycardia/fast heartbeat or bradycardia/slow heartbeat),Arteriovenous malformation,Anomalous pulmonary venous return, Aortic Regurgitation, Aortic Stenosis, Arrhythmia, Cardiomyopathy, Congenital pulmonary vein stenosis, Congestive heart failure, Coronary Heart Disease, Hypertensive crisis, Left Heart Failure, Left-to-Right Shunt, Mitral Regurgitation, Mitral Stenosis, Myocarditis, Pericardial Disease, Pericardial effusion with tamponade, ST elevation MI with left ventricular failure |
| Chemical / poisoning | |
| Dermatologic | No underlying causes |
| Drug Side Effect |
A variety of Drugs, particularly Chemotherapeutic agents such as anthracyclines, Bosutinib, Cytarabine, Gadobenate Dimeglumine,Gemcitabine, Hydrochlorothiazide, Meropenem, Muromonab-CD3, Oprelvekin, Phenylephrine, Pilocarpine, Pramipexole, Protamine sulfate, prednisolone |
| Ear Nose Throat | |
| Endocrine | |
| Environmental |
High altitude sickness. Ascent to high altitude occasionally causes high altitude pulmonary edema (HAPE)[1], Inhalation of toxic gases such as amonia, Water intoxication |
| Gastroenterologic |
Gastric content aspiration |
| Genetic | No underlying causes |
| Hematologic |
Blood Transfusions, Idiopathic Venoocclusive Disease, Disseminated Intravascular Coagulation, Leukemia |
| Iatrogenic |
Hyperhydration, Blood Transfusions, High altitude sickness. Ascent to high altitude occasionally causes high altitude pulmonary edema (HAPE)[2] |
| Infectious Disease |
Bacterial toxins, Malaria, Miliary Tuberculosis, Sepsis, Toxic Shock Syndrome |
| Musculoskeletal / Ortho | No underlying causes |
| Neurologic |
Neurogenic, e.g. Subarachnoid hemorrhage |
| Nutritional / Metabolic |
Hypoalbuminemia / Albumin deficiency, Water intoxication |
| Obstetric/Gynecologic | |
| Oncologic | |
| Opthalmologic | No underlying causes |
| Overdose / Toxicity | |
| Psychiatric |
Psychogenic polydipsia with hyperhydration, Water intoxication |
| Pulmonary |
Acute Bronchial Asthma, Drowning, Gastric content aspiration, Mediastinitis,Pneumonia, Pulmonary contusion, Pulmonary embolism, Reexpansion, i.e. post pneumonectomy or large volume thoracentesis, Reperfusion injury, i.e. postpulmonary thromboendartectomy or lung transplantation, Upper airway obstruction |
| Renal / Electrolyte | |
| Rheum / Immune / Allergy | |
| Sexual | No underlying causes |
| Trauma |
Drowning, Burns, Inhalation of toxic gases, Pulmonary contusion, Trauma |
| Urologic | |
| Miscellaneous |
Causes in Alphabetical Order
Cardiogenic
- Severe arrhythmias (tachycardia/fast heartbeat or bradycardia/slow heartbeat)
- Arteriovenous malformation
- Anomalous pulmonary venous return
- Aortic Regurgitation
- Aortic Stenosis
- Arrhythmia
- Cardiomyopathy
- Congenita pulmonary venous stenosis
- Congestive heart failure
- Coronary Heart Disease
- Cytarabine
- Hypertensive crisis
- Left Heart Failure
- Left-to-Right Shunt
- Mitral Regurgitation
- Mitral Stenosis
- Myocarditis
- Pericardial Disease
- Pericardial effusion with tamponade
- ST elevation MI with left ventricular failure
Non-cardiogenic
This form is contiguous with ARDS (acute respiratory distress syndrome):
- Acute Bronchial Asthma
- Acute Renal Failure
- Bacterial toxins
- Blood Transfusions
- Burns
- Chronic mediastinitis
- Decompression sickness
- Disseminated Intravascular Coagulation
- Drowning
- Drugs– Cytomegalovirus immune globulin
- Fibrotic/inflammatory disease
- Fluid overload, e.g. from kidney failure
- Gastric content aspiration
- Goodpasture’s Syndrome
- High altitude sickness. Ascent to high altitude occasionally causes high altitude pulmonary edema (HAPE)[3]
- Hyperhydration
- Hypoalbuminemia / Albumin deficiency
- Idiopathic Venoocclusive Disease
- Inhalation of toxic gases
- Infection
- Leukemia
- Malaria
- Miliary Tuberculosis
- Neurogenic, e.g. subarachnoid hemorrhage
- Oprelvekin
- Pheochromocytoma
- Pneumonia
- Pulmonary contusion, i.e. high-energy trauma
- Pulmonary Embolism
- Reexpansion, i.e. post pneumonectomy or large volume thoracentesis
- Reperfusion injury, i.e. postpulmonary thromboendartectomy or lung transplantation
- Sepsis
- Shock
- Toxic Shock Syndrome
- Multitrauma, e.g. motor vehicle accident
- Upper airway obstruction
- Uremia
References
- ↑ M Bates. “High altitude pulmonary edema”. Apex (Altitude Physiology Expeditions). Retrieved 2007-03-06.
- ↑ M Bates. “High altitude pulmonary edema”. Apex (Altitude Physiology Expeditions). Retrieved 2007-03-06.
- ↑ M Bates. “High altitude pulmonary edema”. Apex (Altitude Physiology Expeditions). Retrieved 2007-03-06.
Differentiating Pulmonary Edema from other Diseases
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1] Associate Editor(s)-in-Chief: Farnaz Khalighinejad, MD [2]
Overview
Pulmonary edema should be distinguished from other conditions that cause dyspnea, orthopnea, cough.
Differentiating Pulmonary edema from Other Diseases
Pulmonary edema should be differentiated from other diseases presenting with dyspnea, orthopnea, cough.
The differentials include the following:
Abbreviations: ABG (arterial blood gas); ACE (angiotensin converting enzyme); BMI (body mass index); CBC (complete blood count); CSF (cerebrospinal fluid); CXR (chest X-ray); DOE (dyspnea on exercise); ECG (electrocardiogram); FEF (forced expiratory flow rate); FEV1 (forced expiratory volume); FVC (forced vital capacity); JVD (jugular vein distention); MCV (mean corpuscular volume); Plt (platelet); RV (residual volume); SIADH (syndrome of inappropriate antidiuretic hormone); TSH (thyroid stimulating hormone); Vt (tidal volume); WBC (white blood cell);
References
- ↑ Bernstein JA, Cremonesi P, Hoffmann TK, Hollingsworth J (2017). “Angioedema in the emergency department: a practical guide to differential diagnosis and management”. Int J Emerg Med. 10 (1): 15. doi:10.1186/s12245-017-0141-z. PMC 5389952. PMID 28405953.
- ↑ Bjornsson HM, Graffeo CS (2010). “Improving diagnostic accuracy of anaphylaxis in the acute care setting”. West J Emerg Med. 11 (5): 456–61. PMC 3027438. PMID 21293765.
- ↑ O’Horo JC, Rogus-Pulia N, Garcia-Arguello L, Robbins J, Safdar N (2015). “Bedside diagnosis of dysphagia: a systematic review”. J Hosp Med. 10 (4): 256–65. doi:10.1002/jhm.2313. PMC 4607509. PMID 25581840.
- ↑ Bjornson CL, Johnson DW (2013). “Croup in children”. CMAJ. 185 (15): 1317–23. doi:10.1503/cmaj.121645. PMC 3796596. PMID 23939212.
- ↑ Negus VE (1927). “The Function of the Epiglottis”. J Anat. 62 (Pt 1): 1–8. PMC 1250045. PMID 17104162.
- ↑ Meltzer EO, Hamilos DL (2011). “Rhinosinusitis diagnosis and management for the clinician: a synopsis of recent consensus guidelines”. Mayo Clin Proc. 86 (5): 427–43. doi:10.4065/mcp.2010.0392. PMC 3084646. PMID 21490181.
- ↑ Wood RP, Milgrom H (September 1996). “Vocal cord dysfunction”. J. Allergy Clin. Immunol. 98 (3): 481–5. PMID 8828523.
- ↑ Hodder R, Lougheed MD, Rowe BH, FitzGerald JM, Kaplan AG, McIvor RA (2010). “Management of acute asthma in adults in the emergency department: nonventilatory management”. CMAJ. 182 (2): E55–67. doi:10.1503/cmaj.080072. PMC 2817338. PMID 19858243.
- ↑ Cantin, Luce; Bankier, Alexander A.; Eisenberg, Ronald L. (2009). “Bronchiectasis”. American Journal of Roentgenology. 193 (3): W158–W171. doi:10.2214/AJR.09.3053. ISSN 0361-803X.
- ↑ Molis MA, Molis WE (2010). “Exercise-induced bronchospasm”. Sports Health. 2 (4): 311–7. doi:10.1177/1941738110373735. PMC 3445098. PMID 23015953.
- ↑ Holbro A, Lehmann T, Girsberger S, Stern M, Gambazzi F, Lardinois D, Heim D, Passweg JR, Tichelli A, Bubendorf L, Savic S, Hostettler K, Grendelmeier P, Halter JP, Tamm M (2013). “Lung histology predicts outcome of bronchiolitis obliterans syndrome after hematopoietic stem cell transplantation”. Biol. Blood Marrow Transplant. 19 (6): 973–80. doi:10.1016/j.bbmt.2013.03.017. PMID 23562737.
- ↑ Qureshi H, Sharafkhaneh A, Hanania NA (2014). “Chronic obstructive pulmonary disease exacerbations: latest evidence and clinical implications”. Ther Adv Chronic Dis. 5 (5): 212–27. doi:10.1177/2040622314532862. PMC 4131503. PMID 25177479.
- ↑ Dela Cruz CS, Tanoue LT, Matthay RA (2011). “Lung cancer: epidemiology, etiology, and prevention”. Clin Chest Med. 32 (4): 605–44. doi:10.1016/j.ccm.2011.09.001. PMC 3864624. PMID 22054876.
- ↑ Simonetti AF, Viasus D, Garcia-Vidal C, Carratalà J (2014). “Management of community-acquired pneumonia in older adults”. Ther Adv Infect Dis. 2 (1): 3–16. doi:10.1177/2049936113518041. PMC 4072047. PMID 25165554.
- ↑ Currie GP, Alluri R, Christie GL, Legge JS (2007). “Pneumothorax: an update”. Postgrad Med J. 83 (981): 461–5. doi:10.1136/pgmj.2007.056978. PMC 2600088. PMID 17621614.
- ↑ Bĕlohlávek J, Dytrych V, Linhart A (2013). “Pulmonary embolism, part I: Epidemiology, risk factors and risk stratification, pathophysiology, clinical presentation, diagnosis and nonthrombotic pulmonary embolism”. Exp Clin Cardiol. 18 (2): 129–38. PMC 3718593. PMID 23940438.
- ↑ Swart E, Laratta J, Slobogean G, Mehta S (February 2017). “Operative Treatment of Rib Fractures in Flail Chest Injuries: A Meta-analysis and Cost-Effectiveness Analysis”. J Orthop Trauma. 31 (2): 64–70. doi:10.1097/BOT.0000000000000750. PMID 27984449.
- ↑ 18.0 18.1 Bruyninckx R, Aertgeerts B, Bruyninckx P, Buntinx F (2008). “Signs and symptoms in diagnosing acute myocardial infarction and acute coronary syndrome: a diagnostic meta-analysis”. Br J Gen Pract. 58 (547): 105–11. doi:10.3399/bjgp08X277014. PMC 2233977. PMID 18307844.
- ↑ Gaggin, Hanna K.; Januzzi, James L. (2013). “Biomarkers and diagnostics in heart failure”. Biochimica et Biophysica Acta (BBA) – Molecular Basis of Disease. 1832 (12): 2442–2450. doi:10.1016/j.bbadis.2012.12.014. ISSN 0925-4439.
- ↑ van Steijn JH, Sleijfer DT, van der Graaf WT, van der Sluis A, Nieboer P (2002). “How to diagnose cardiac tamponade”. Neth J Med. 60 (8): 334–8. PMID 12481882.
- ↑ Martindale, Jennifer L.; Noble, Vicki E.; Liteplo, Andrew (2013). “Diagnosing pulmonary edema”. European Journal of Emergency Medicine. 20 (5): 356–360. doi:10.1097/MEJ.0b013e32835c2b88. ISSN 0969-9546.
- ↑ Peter JV, Sudarsan TI, Moran JL (2014). “Clinical features of organophosphate poisoning: A review of different classification systems and approaches”. Indian J Crit Care Med. 18 (11): 735–45. doi:10.4103/0972-5229.144017. PMC 4238091. PMID 25425841.
- ↑ Chin RL, Olson KR, Dempsey D (2007). “Salicylate toxicity from ingestion and continued dermal absorption”. Cal J Emerg Med. 8 (1): 23–5. PMC 2859737. PMID 20440389.
- ↑ Lane TR, Williamson WJ, Brostoff JM (2008). “Carbon monoxide poisoning in a patient with carbon dioxide retention: a therapeutic challenge”. Cases J. 1 (1): 102. doi:10.1186/1757-1626-1-102. PMC 2533003. PMID 18710551.
- ↑ Westerberg DP (March 2013). “Diabetic ketoacidosis: evaluation and treatment”. Am Fam Physician. 87 (5): 337–46. PMID 23547550.
Epidemiology and Demographics
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1] Associate Editor(s)-in-Chief: Farnaz Khalighinejad, MD [2]
Overview
The prevalence of pulmonary edema was estimated to be 75000-83000 cases per 100,000 individuals among heart failure patients with reduced ejection fraction. Pulmonary edema commonly affects individuals older than 65 years of age. Males are more commonly affected by pulmonary edema than woman.
Epidemiology and Demographics
Incidence
- The incidence of neurogenic pulmonary edema is approximately 2000 to 42900 per 100,000 individuals in patients with subarachnoid hemorrhage.[1][2]
- The incidence of neurogenic pulmonary edema is approximately 20000 per 100,000 individuals in patients with traumatic brain injury.[3]
Prevalence
- The prevalence of pulmonary edema was estimated to be 75000-83000 cases per 100,000 individuals among heart failure patients with reduced ejection fraction.[4]
Mortality rate
- The mortality rate of pulmonary edema is approximately 12000 per 100000 among in-hospital patients.[5]
- The median time from the pulmonary edema until death is approximately 10 days.
- Higher in-hospital mortality rate are associated with left ventricular myocardial function.
Age
- Pulmonary edema commonly affects individuals older than 65 years of age.[5]
Race
- Blacks have the highest risk for heart failure as underlying cause of pulmonary edema.[6]
Gender
- Males are more commonly affected by pulmonary edema than woman.[5]
References
- ↑ Fontes RB, Aguiar PH, Zanetti MV, Andrade F, Mandel M, Teixeira MJ (April 2003). “Acute neurogenic pulmonary edema: case reports and literature review”. J Neurosurg Anesthesiol. 15 (2): 144–50. PMID 12658001.
- ↑ Solenski NJ, Haley EC, Kassell NF, Kongable G, Germanson T, Truskowski L, Torner JC (June 1995). “Medical complications of aneurysmal subarachnoid hemorrhage: a report of the multicenter, cooperative aneurysm study. Participants of the Multicenter Cooperative Aneurysm Study”. Crit. Care Med. 23 (6): 1007–17. PMID 7774210.
- ↑ Bratton SL, Davis RL (April 1997). “Acute lung injury in isolated traumatic brain injury”. Neurosurgery. 40 (4): 707–12, discussion 712. PMID 9092843.
- ↑ Platz E, Jhund PS, Campbell RT, McMurray JJ (September 2015). “Assessment and prevalence of pulmonary oedema in contemporary acute heart failure trials: a systematic review”. Eur. J. Heart Fail. 17 (9): 906–16. doi:10.1002/ejhf.321. PMC 4725064. PMID 26230356.
- ↑ 5.0 5.1 5.2 Edoute Y, Roguin A, Behar D, Reisner SA (February 2000). “Prospective evaluation of pulmonary edema”. Crit. Care Med. 28 (2): 330–5. PMID 10708162.
- ↑ Yancy CW, Jessup M, Bozkurt B, Butler J, Casey DE, Drazner MH, Fonarow GC, Geraci SA, Horwich T, Januzzi JL, Johnson MR, Kasper EK, Levy WC, Masoudi FA, McBride PE, McMurray JJ, Mitchell JE, Peterson PN, Riegel B, Sam F, Stevenson LW, Tang WH, Tsai EJ, Wilkoff BL (October 2013). “2013 ACCF/AHA guideline for the management of heart failure: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines”. J. Am. Coll. Cardiol. 62 (16): e147–239. doi:10.1016/j.jacc.2013.05.019. PMID 23747642.
Risk Factors
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1] Associate Editor(s)-in-Chief: Farnaz Khalighinejad, MD [2]
Overview
The risk factors in pulmonary edema refer to the risk factors for the underlying disease that cause pulmonary edema. Risk factors of cardinogenic pulmonary edema include high blood pressure, hyperlipidemia, atherosclerosis, diabetes mellitus, obesity. And risk factors for noncardiogenic pulmonary edema include sepsis, aspiration, pneumonia.
Risk Factors
The risk factors in pulmonary edema refer to the risk factors for the underlying disease that cause pulmonary edema. Heart failure patients are the most at risk for pulmonary edema.[1]
Cardiogenic:
Common Risk Factors:
Less Common Risk Factors:
- Excessive alcohol intake
- Dietary choices
Noncardiogenic:
Common Risk Factors:
Less Common Risk Factors:
- Trauma
- Inhaled toxins
- Disseminated intravascular coagulation
References
Natural History, Complications and Prognosis
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1] Associate Editor(s)-in-Chief: Farnaz Khalighinejad, MD [2]
Overview
Some patients may need to use a breathing machine for a long time, which may lead to damage to lung tissue. Kidney failure and damage to other major organs may occur if blood and oxygen flow are not restored promptly. If not treated, this condition can be fatal. If left untreated, acute pulmonary edema can lead to coma and even death, generally due to its main complication of hypoxia.
Natural History
- If left untreated, acute pulmonary edema can lead to respiratory arrest, coma and death, generally due to its main complication of hypoxia[1]
- Some patients may need to use a breathing machine for a long time, which may lead to damage to lung tissue
Complications
Common complications of pulmonary edema include:[1]
- Leg swelling (edema)
- Abdominal swelling (ascites)
- Pleural effusion
- Congestion of liver
- Myocardial infarction (MI)
- Cardiogenic shock
- Arrhythmias
- Electrolyte disturbances
- Mesenteric insufficiency
- Protein enteropathy
- Death
Prognosis
Prognosis of non-cardiogenic pulmonary edema is generally good and responds well to treatment, while cardiogenic pulmonary edema has a variable mortality rate.
- In-hospital mortality rates in a high-acuity setting, are 15-20%.
The prognosis for patients with acute pulmonary edema depends on the:[1]
- Underlying cause
- The patient’s age
- Comorbidities
- Prompt diagnosis
- Initiation of effective treatment
The following features are associated with a worse outcome:[1]
- Advanced Age
- Wide QRS complex
- Hyponatremia
- Low Left Ventricular Ejection Fraction
- Hypotension
- Precipitated by ischaemia
- Previous hospitalisation for heart failure
- Marked BNP elevation
- Elevated troponin
References
Diagnosis
Diagnosis
History and Symptoms | Physical Examination | Laboratory Findings | X Ray | CT | Echocardiography | Other Diagnostic Studies
Treatment
Treatment
Medical Therapy | | Surgery | Primary Prevention | Secondary Prevention | Cost-Effectiveness of Therapy | Future or Investigational Therapies
Looking for the patient version?
© 2026 MyEClinic – IFTM Institut für Telematik in der Medizin GmbH