
The Physical Examination in Cardiovascular Disease:The Neck
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]
Carotid Bruit
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Ogheneochuko Ajari, MB.BS, MS [2]
Overview
A carotid bruit is a bruit or sound heard over the carotid artery area, usually by a nurse or physician during auscultation. It is usually the result of a stenosis of the carotid artery, and is unlikely to be heard if the stenosis occludes less than 40% of the diameter of the artery. Likewise, a stenosis of greater than 90% may not be heard, as the flow may be too low.
Causes
Life Threatening Causes
Life-threatening causes include conditions which may result in death or permanent disability within 24 hours if left untreated.
Common Causes
Causes by Organ System
Diagnosis
Many carotid bruits are discovered incidentally in an otherwise asymptomatic patient. A carotid duplex ultrasound may be useful in determining the origin of the bruit, the severity of the stenosis causing it, and the bruit’s hemodynamic effects.
- Carotid bruits are best heard with the bell of the stethoscope.
- Carotid bruits are a blowing sound or murmur over the carotid artery
- Are usually associated with carotid stenosis, secondary to atherosclerosis
- Depending on degree of stenosis, may imply an increased risk of stroke
History and Symptoms
- Special attention should paid to symptoms suggestive of:
- Transient ischemic attack (TIA) symptoms
- Cardiac risk factors
Physical Examination
Heart
- It is critical to assess if there is a heart murmur that is radiating to the carotids.
Abdomen
- The presence of a carotid bruit may indicate that a renal bruit is present as well.
Extremities
- The presence of a carotid bruit may indicate that a femoral artery bruit will be present as well. The distal pulses should be evaluated carefully.
Neurologic
- Neurologic exam should document and focal neurologic findings that might suggest a prior stroke.
Laboratory Findings
- Complete blood count (CBC)
- Lipid panel
- Folate levels
- Vitamin B12
- Thyroid stimulating hormone (TSH)
- Glucose
- Homocysteine level
- Erythrocyte sedimentation rate (ESR)
Echocardiography or Ultrasound
- The degree of stenosis can be evaluated by carotid duplex ultrasound.
- A CT scan may be indicated for patients with ultrasound-proven carotid disease who are at a higher risk for cerebrovascular accidents such as stroke.
Other Imaging Findings
- To evaluate symptomatic stenosis that may require surgery:
- Computerized tomographic angiography (CTA)
- Magnetic resonance angiogram (MRA)
- Carotid arteriography
Treatment
- Treat underlying atherosclerotic disease proceses.
- Smoking cessation
Pharmacotherapy
Acute Pharmacotherapies
- Aspirin and/or antiplatelet therapy is recommended for asymptomatic patients
Chronic Pharmacotherapies
- Aspirin and/or antiplatelet therapy is recommended for asymptomatic patients
Surgery and Device Based Therapy
- Symptomatic patients with stenosis of 50-69% benefit more from surgery than medical therapies
- Symptomatic patients with stenosis of greater than 70% should consider endarterectomy
Future or Investigational Therapies
- Carotid angioplasty is under investigation for a possible future treatment
References
- ↑ Sailer, Christian, Wasner, Susanne. Differential Diagnosis Pocket. Hermosa Beach, CA: Borm Bruckmeir Publishing LLC, 2002:77 ISBN 1591032016
- ↑ Kahan, Scott, Smith, Ellen G. In A Page: Signs and Symptoms. Malden, Massachusetts: Blackwell Publishing, 2004:68 ISBN 140510368X
- ↑ Sauvé J, Laupacis A, Østbye T, Feagan B, Sackett DL. Original article: does this patient have a clinically important carotid bruit? In: Simel DL, Rennie D, eds. The Rational Clinical Examination: Evidence-Based Clinical Diagnosis. New York, NY: McGraw-Hill; 2009. http://www.jamaevidence.com/content/3476758. Accessed 1/7/2015
- ↑ Demiryoguran NS, Karcioglu O, Topacoglu H, Aksakalli S (2006). “Painless aortic dissection with bilateral carotid involvement presenting with vertigo as the chief complaint”. Emerg Med J. 23 (2): e15. doi:10.1136/emj.2005.027862. PMC 2564071. PMID 16439729.
- ↑ Sauvé J, Laupacis A, Østbye T, Feagan B, Sackett DL. Original article: does this patient have a clinically important carotid bruit? In: Simel DL, Rennie D, eds. The Rational Clinical Examination: Evidence-Based Clinical Diagnosis. New York, NY: McGraw-Hill; 2009. http://www.jamaevidence.com/content/3476758. Accessed 1/7/2015
- ↑ Rymer JA, Anderson LL, Posenau JT, Jones WS (2013). “Remote Stab Wound Resulting in AV Fistula and High-Output Heart Failure”. Case Rep Cardiol. 2013: 902719. doi:10.1155/2013/902719. PMC 4008354. PMID 24826298.
- ↑ Bavinzski G, Richling B, Killer M, Gruber A, Levy D (1996). “Evolution of different therapeutic strategies in the treatment of cranial dural arteriovenous fistulas–report of 30 cases”. Acta Neurochir (Wien). 138 (2): 132–8. PMID 8686535.
- ↑ Lawrence PF, Oderich GS (2002). “Ophthalmologic findings as predictors of carotid artery disease”. Vasc Endovascular Surg. 36 (6): 415–24. PMID 12476231.
- ↑ Hill SL, Holtzman GL, Berry R, Arnold JF (1997). “The appropriate use of the duplex scan in carotid arterial disease”. Am Surg. 63 (8): 720–5. PMID 9247441.
- ↑ Chambers BR, Norris JW (1985). “Clinical significance of asymptomatic neck bruits”. Neurology. 35 (5): 742–5. PMID 3887214.
- ↑ Wu HC, Chen YC, Chen CJ, Chen ST, Lee TH (2006). “Spontaneous bilateral internal carotid artery dissection with acute stroke in young patients”. Eur Neurol. 56 (4): 230–4. doi:10.1159/000096491. PMID 17057383.
- ↑ Lindsay FW, Mullin D, Keefe MA (2003). “Subacute hypoglossal nerve paresis with internal carotid artery dissection”. Laryngoscope. 113 (9): 1530–3. doi:10.1097/00005537-200309000-00022. PMID 12972929.
- ↑ Santilli JD, Santilli SM, Rodnick JE (1996). “Prevention of stroke caused by carotid bifurcation stenosis”. Am Fam Physician. 53 (2): 549–56, 559–60. PMID 8629537.
- ↑ 14.0 14.1 Morales-Gisbert SM, Plaza-Martínez Á, Sala-Almonacil VA, Olmos-Sánchez D, Gomez-Palonés FJ, Ortiz-Monzón E (2013). “[Natural history of moderate-degree carotid stenosis in patients with peripheral artery disease]”. Med Clin (Barc). 140 (8): 337–42. doi:10.1016/j.medcli.2012.06.031. PMID 23339889.
- ↑ Lacerda Gde C, Pedrosa RC, Lacerda RC, Santos MC, Perez Mde A, Teixeira AB; et al. (2008). “Cardioinhibitory carotid sinus hypersensitivity: prevalence and predictors in 502 outpatients”. Arq Bras Cardiol. 90 (3): 148–55. PMID 18392392.
- ↑ Ebina K, Iwabuchi T (1978). “[Closure of traumatic internal carotid-cavernous fistula with an improved type of captive embolus (author’s transl)]”. No Shinkei Geka. 6 (1): 59–66. PMID 628507.
- ↑ Garland SD, Maloney PL, Doku HC (1977). “Carotid-cavernous sinus fistula after trauma to the head”. J Oral Surg. 35 (10): 832–5. PMID 269234.
- ↑ Subramani KS, Kolhari VB, Manjunath CN, Bhairappa S (2013). “Familial hypercholesterolaemia presenting with coronary artery disease in a young patient”. BMJ Case Rep. 2013. doi:10.1136/bcr-2013-008718. PMID 23519510.
- ↑ Frost PH, Davis BR, Burlando AJ, Curb JD, Guthrie GP, Isaacsohn JL; et al. (1996). “Coronary heart disease risk factors in men and women aged 60 years and older: findings from the Systolic Hypertension in the Elderly Program”. Circulation. 94 (1): 26–34. PMID 8964114.
- ↑ 20.0 20.1 Taddio A, Maschio M, Martelossi S, Barbi E, Ventura A (2013). “Crohn’s disease and Takayasu’s arteritis: an uncommon association”. World J Gastroenterol. 19 (35): 5933–5. doi:10.3748/wjg.v19.i35.5933. PMC 3793150. PMID 24124342.
- ↑ Olin JW, Sealove BA (2011). “Diagnosis, management, and future developments of fibromuscular dysplasia”. J Vasc Surg. 53 (3): 826–36.e1. doi:10.1016/j.jvs.2010.10.066. PMID 21236620.
- ↑ Sauvé J, Laupacis A, Østbye T, Feagan B, Sackett DL. Original article: does this patient have a clinically important carotid bruit? In: Simel DL, Rennie D, eds. The Rational Clinical Examination: Evidence-Based Clinical Diagnosis. New York, NY: McGraw-Hill; 2009. http://www.jamaevidence.com/content/3476758. Accessed 1/7/2015
Acknowledgements
The content on this page was first contributed by Editor-In-Chief: C. Michael Gibson, M.S., M.D. [3]
List of contributors:
Suggested Reading and Key General References
Suggested Links and Web Resources
For Patients
Hepatojugular Reflux
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]
Synonyms and keywords: Abdominojugular test, AJR, HJR
Overview
The abdominojugular test (AJR), also known as hepatojugular reflux or HJR is used as an alternate test for measuring jugular venous pressure (JVP) through the distension or swelling of the jugular vein. A positive AJR best correlates with the pulmonary capillary wedge pressure although it also correlates with the right heart pressure and the left heart ejection fraction [1].
Procedure
The doctor presses firmly over either the Right upper quadrant (liver) or over the center of the abdomen [1] for 10-60 seconds with a pressure of 20 to 35 mm Hg while observing the internal jugular vein in the neck and also observing to be sure the patient does not Valsalva [2].
The internal jugular vein can be distinguished from the carotid artery by
- Having a biphasic waveform
- Falling pressure during inspiration
- Rising with abdominal pressure, and
- Being compressible with direct pressure [2].
When the meniscus of the internal jugular vein cannot be determined, one study found the height of the meniscus in the external jugular vein correlated with the right atrial pressure [3].

- Negative Result: On an otherwise healthy individual, the jugular venous pressure remains constant or temporarily rises for a heartbeat or two, before returning to normal. This negative result would be indicated by a lack of swelling of the jugular vein.
- Positive Result: A positive result is variously defined as either a sustained rise in the JVP of at least 4cm or more [2] or a fall of 4 cm or more [1] after the examiner releases pressure. The AJR has a reported sensitivity of 24% [4] to 72% [1] and a specificity of 96% to 93%. The large discrepancy in sensitivity may be explained by the higher value being reported during performance in optimal conditions of a cardiac lab while the lower value was from a study in an emergency room.
Below is a video demonstrating hepato-jugular reflux {{#ev:youtube|B8OX3T4c7PU}}>
References
- ↑ 1.0 1.1 1.2 1.3 Ewy G (1988). “The abdominojugular test: technique and hemodynamic correlates”. Ann Intern Med. 109 (6): 456–60. PMID 3415106.
- ↑ 2.0 2.1 2.2 Cook D, Simel D (1996). “The Rational Clinical Examination. Does this patient have abnormal central venous pressure?”. JAMA. 275 (8): 630–4. PMID 8594245.
- ↑ Stoelting R (1973). “Evaluation of external jugular venous pressure as a reflection of right atrial pressure”. Anesthesiology. 38 (3): 291–4. PMID 4698149.
- ↑ Marantz P, Kaplan M, Alderman M (1990). “Clinical diagnosis of congestive heart failure in patients with acute dyspnea”. Chest. 97 (4): 776–81. PMID 2182296.
Jugular Venous Pressure
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1] Associate Editor(s)-in-Chief: Mitra Chitsazan, M.D.[2] Mandana Chitsazan, M.D. [3]
Synonyms and keywords: Jugular venous distention; elevated JVP; JVD; elevated neck veins; distended neck veins
Overview
The jugular venous pressure (JVP, sometimes referred to as jugular venous pulse) is the indirectly observed pressure over the venous system. It can be useful in the differentiation of various forms of heart and lung disease.
Classically three upward deflections (waves) and two downward deflections (toughs) have been described. The upward deflections are the “a” (atrial filling), “c” (ventricular contraction and resulting bulging of tricuspid into the right atrium during isovolumic systole), and “v” (atrial venous filling) waves, and the downward deflections are the “x”(when tricuspid opens and ventricular filling occurs) and the “y” descents (filling of ventricle after tricuspid opening).
The interpretation of JVP findings can be challenging and is becoming a lost art, as much of the subtle information previously obtained by careful observation of the JVP can now be gained easily with echocardiography and/or EKG. Certain waveform abnormalities include “Cannon a-waves“, which result when the atrium contracts against a closed tricuspid valve, due to complete heart block (3rd-degree heart block), or even in ventricular tachycardia. Another abnormality, “c-v waves“, can be a sign of tricuspid regurgitation.
An elevated JVP is the classic sign of venous hypertension (e.g. right-sided heart failure). The paradoxical increase of the JVP with inspiration (instead of the expected decrease) is referred to as the Kussmaul sign and indicates impaired filling of the right ventricle. The differential diagnosis of Kussmaul’s sign includes constrictive pericarditis, restrictive cardiomyopathy, pericardial effusion, and severe right-sided heart failure.
Anatomy
- Right and left internal jugular veins (IJVs):
- Paired neck veins draining the head and neck.
- Originate from the dural venous sinuses and leave the skull via the jugular foramen, then descend through the neck alongside and lateral to the internal carotid arteries.
- Then join the subclavian veins (at the base of the neck) to form the brachiocephalic vein.
- The IJVs lies deep to the skin and soft tissues; therefore, they are not directly visible and identification only is possible via visualization of pulsations transmitted to the surface of the neck.
- Additionally, these blood vessels are under much lower pressure than the adjacent, pulsating carotid artery. It, therefore, takes a sharp eye to identify the relatively weak, transmitted venous impulses.
- Right internal jugular vein
- It directly Communicates with the right atrium via the superior vena cava
- The right IJV can therefore function as a manometer, with distention indicating an elevation of Central venous pressure (CVP).
- This in turn is an important marker of intravascular volume status and related cardiac function.
- Right and left external jugular veins (EJV):
- These veins drain superficial scalp and face structures
- They descend the lateral neck, pass diagonally over the top of the sternocleidomastoid muscles and empty into the subclavian veins
- The EJVs are valved, and not directly in the line with the right atrium or superior vena cava; therefore, are less preferred for estimation of JVP compared to the left IJV.
Technique

- A classical method for quantifying the JVP was described by Borst & Molhuysen in 1952.[1] It has since been modified in various ways. [2] [3] [4]
- The patient is positioned under 45°, and the filling level of the jugular vein is determined. In healthy people, it is a maximum of several (3-4) centimeters above the sternal angle. Some physicians employ a venous arc, an instrument to measure the JVP more accurately. A pen-light can aid in discerning the jugular filling level.
Visualization of the JVP
The JVP is easiest to observe if one looks along the surface of the sternocleidomastoid muscle, as it is easier to appreciate the movement relative to the neck when looking from the side (as opposed to looking at the surface at a 90-degree angle). Like judging the movement of an automobile from a distance, it is easier to see the movement of an automobile when it is crossing one’s path at 90 degrees (i.e. moving left to right or right to left), as opposed to coming toward one. Remember, tangential light is critical.
A few things to remember:
- Think anatomically
- The right internal jugular vein (IJV) runs between the two heads (sternal and clavicular) of the sternocleidomastoid muscle (SCM) and up in front of the ear.
- This muscle can be identified by asking the patient to turn their head to the left and into your hand while you provide resistance to the movement.
- The two heads form the sides of a small triangle, with the clavicle making up the bottom edge. You should be able to feel a shallow defect formed by the borders of these landmarks.
- Note, you are trying to identify impulses originating from the IJV and transmitted to the overlying skin in this area. You can’t actually see the IJV.
- The external jugular vein (EJV) runs in an oblique direction across the sternocleidomastoid muscle and, in contrast to the IJV, can usually be directly visualized.
- If the EJV is not readily apparent, have the patient look to the left and do a Valsalva manuver. This usually makes it quite obvious.
- EJV distention is not always a reliable indicator of elevated CVP as valves, designed to prevent the retrograde flow of blood, can exist within this vessel causing it to appear engorged even when CVP is normal. It also makes several turns before connecting with the central venous system and is thus not in a direct line with the right atrium.
- Take your time.
- Look at the area in question for several minutes while the patient’s head is turned to the left.
- The carotid artery is adjacent to the IJV, lying just medial to it.
- If you are unsure whether a pulsation is caused by the carotid artery or the IJV, place your hand on the patient’s radial artery and use this as a reference.
- The carotid impulse coincides with the palpated radial artery pulsation and is characterized by a single upstroke timed with systole.
- The venous impulse (at least when the patient is in sinus rhythm and there is no tricuspid regurgitation) has three components, each associated with a, c, and v waves. When these are transmitted to the skin, they create a series of flickers that are visible diffusely within the overlying skin.
- In contrast, the carotid artery causes a single up and down pulsation.
- Furthermore, the carotid artery is palpable, while the IJV is not palpable and can, in fact, be obliterated by applying pressure in the area where it emerges above the clavicle.
- Search along the entire projected course of the IJV as the top of the pressure wave (which is the point that you are trying to identify) may be higher than where you are looking.
- In fact, if the patient’s CVP is markedly elevated, you may not be able to identify the top of the wave unless they are positioned with their trunk elevated at 45 degrees or more (else there will be no identifiable “top” of the column as the entire IJV will be engorged).
- After you have found the top of the wave, see what effect sitting straight up and lying down flat has on the height of the column. Sitting should cause it to appear at a lower point in the neck while lying has the opposite effect. Realize that these maneuvers do not change the actual value of the central venous pressure. They simply alter the position of the top of the pulsations in relation to other structures in the neck and chest.
- Shine a penlight tangentially across the neck. This sometimes helps to accentuate the pulsations.
- If you are still uncertain, apply gentle pressure to the right upper quadrant of the abdomen for 5 to 10 seconds.
- This elicits Hepatojugular reflux which, in pathological states, will cause blood that has pooled in the liver to flow in a retrograde fashion and fill out the IJV, making the transmitted pulsations more apparent.
- Make sure that you are looking in the right area when you push as the best time to detect any change in the height of this column of blood is immediately after you apply hepatic pressure.
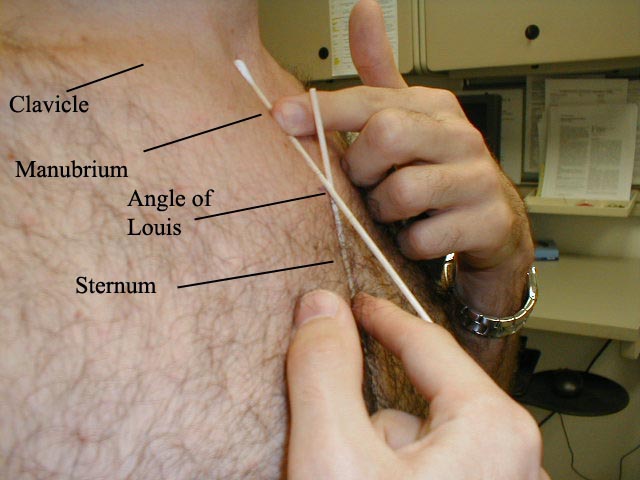
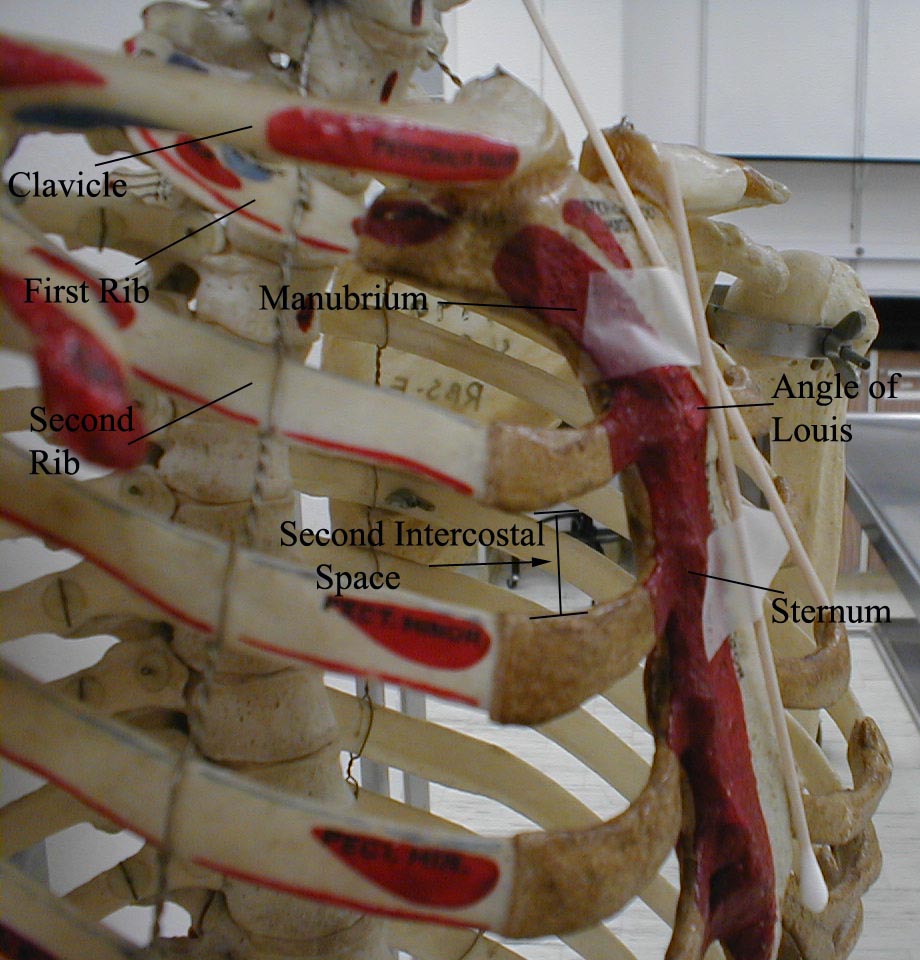
- Once you identify JVD, try to estimate how high in cm the top of the column is above the Angle of Louis.
- The angle is the site of the joint that connects the manubrium with the body of the sternum. First identify the suprasternal notch, a concavity at the top of the manubrium.
- Then walk your fingers downward until you detect a subtle change in the angle of the bone, which is approximately 4 to 5 cm below the notch.
- This is roughly at the level of the 2nd intercostal space.
- The vertical distance from the top of the column to this angle is added to 5cm, the rough vertical distance from the angle to the right atrium with the patient lying at a 45-degree angle.
- The sum is an estimate of the CVP. Normal CVP is 7-9 cm.
The CVP vs the JVP
The central venous pressure (CVP) lies approximately 5 cm above the middle of the right atrium. The CVP is therefore estimated to be the JVP in cm plus 5 cm. Normally, the CVP is 5-9 cm of H2O.
-
-
 The point at which the Q-tips cross is the Angle of Louis
The point at which the Q-tips cross is the Angle of Louis -
 Determining the CVP
Determining the CVP -
 Elevated JVP
Elevated JVP




(Images courtesy of Charlie Goldberg, M.D., UCSD School of Medicine and VA Medical Center, San Diego, California)
Differentiation of the JVP from the carotid pulse

Pulses in the JVP are rather hard to observe, but trained cardiologists do try to discern these as signs of the state of the right atrium.
The JVP and carotid pulse can be differentiated in several ways:
- Multiphasic – the JVP “beats” twice (in quick succession) in eachcardiac cycle. In other words, there are two waves in the JVP for each contraction-relaxation cycle by the heart. The first beat represents the atrial contraction (termed a wave) and the second beat represents venous filling against a closed tricuspid valve (termed vwave) and not the commonly mistaken ‘ventricular contraction‘. The carotid artery has only one beat in the cardiac cycle.
- Non-palpable – the JVP cannot be palpated. If one feels a pulse in the neck, it is generally the common carotid artery.
- Occlude – the JVP can be obliterated by occluding the internal jugular vein by lightly pressing the base of the neck.
- Varies with head-up-tilt (HUT) – the JVP varies with the angle of the neck. If a person is standing their JVP appears to be lower on the neck (or may not be seen at all because it below the sternal angle). The location of carotid pulse location does not vary with HUT.
- Varies with respiration – the JVP usually decreases with deep inspiration. Physiologically, this is a consequence of the Frank-Starling mechanism as inspiration decreases the thoracic pressure and increases blood movement into the heart (venous return), which a healthy heart moves into the pulmonary circulation.
- Abdominal jugular reflux (AJR) (also hepatojugular reflux) – the JVP changes with abdominal pressure. If the JVP is elevated 4 cm, it usually returns to its baseline level within 10 seconds. If the JVP remains elevated for a longer period of time it suggests heart failure.
| Diffenetiating the jugular venous pulse from the carotid pulse | ||
| Feature | Internal Jugular vein | Carotid artery |
| Appearance of pulse |
|
|
| Palpability |
|
|
| Changes during inspiration |
|
|
| Effects of pressure |
|
|
Hepatojugular reflux, sometimes incorrectly referenced as a “reflex”,[5] is an expanded form of the JVP measurement. By pressing on the liver (hepato-) for 15-30 seconds, venous blood is advanced into the circulation. The JVP increases in a normal person, and distention should appear more pronounced. However, a slow decrease of the JVP after checking for hepatojugular reflux can indicate right ventricular failure.
Video Instruction
This video contains a detailed explanation of what the JVP is, how it is measured, and what are the diagnostic considerations of JVP, in terms of interpreting various JVP waveforms.
{{#ev:youtube|https://https://www.youtube.com/watch?v=O1MfBEmNj2s}}
Causes of Elevated Jugular Venous Pressure
- Heart failure
- Constrictive pericarditis (JVP increases on inspiration– called Kussmaul’s sign)
- Cardiac tamponade
- Right ventricular myocardial infarction
- Fluid overload (eg, renal disease)
- Superior vena cava obstruction (no JVP pulsation)
- To view a complete list of causes of elevated jugular venous pressure, click here.’
JVP waveform
The normal jugular venous pressure changes during different stages of cardiac cycles as a result of phasic pressure changes in the right atrium. It consists of two (and sometimes three) positive waves and two negative troughs.[2] [3] [4]
- “a” wave: This presystolic wave is caused by venous distension due to the right atrial contraction. During inspiration, increased venous return to the right atrium may accentuate this wave.
- “c” wave: This wave may sometimes be noted as a distinctive positive waveform. During early systole, right ventricular isovolumetric contraction bulges the tricuspid valve into the right atrium, leading to the appearance of the “c” wave. In addition, the increased carotid artery pressure during early systole may impact the adjacent jugular vein.
- “X” descend: The X descend is caused by atrial relaxation and downward displacement of the tricuspid valve into the right ventricle.
- “v” wave: This late-systolic wave is caused by the increasing volume of blood accumulating in the right atrium during the ventricular systole while the tricuspid valve is closed.
- “Y” descend: The Y descend results from the opening of the tricuspid valve and rapid inflow of blood into the right ventricle.
Components of the JVP Waveform

Abnormal JVP waveforms
| Abnormal JVP waveform | Associated Conditions |
| Absent “a” wave | |
| Large “a” wave
(caused by increased atrial contraction pressure) |
|
| Cannon “a” wave
(caused by contraction of the right atrium against the closed tricuspid valve) |
|
| Decreased nadir of “x” descent | |
| Obliteration or reversed nadir of “x” descent | |
| Accentuated “x” descent | |
| Prominent “v” wave
(caused by the backflow of blood to the right atrium during ventricular systole) |
|
| Slow “Y” descent
(caused by slow emptying of the right atrium) |
|
| Rapid, deep “Y” descent |
|
| Sharp “Y” descent with a deep “Y” trough and a rapid ascent to the baseline (referred to as Friedreich’s sign) | |
| Slow “Y” descent
(caused by obstruction to right ventricular filling) |
|
| Absent “Y” descent |
References
- ↑ Borst J, Molhuysen J (1952). “Exact determination of the central venous pressure by a simple clinical method”. Lancet. 2 (7): 304–9. PMID 14955978.
- ↑ 2.0 2.1 2.2 2.3 Perloff, Joseph (2009). Physical examination of the heart and circulation. Shelton, CT: People’s Medical Pub. House. ISBN 978-1-60795-023-3.
- ↑ 3.0 3.1 3.2 3.3 Bickley, Lynn (2017). Bates’ guide to physical examination and history taking. Philadelphia: Wolters Kluwer. ISBN 9781469893419.
- ↑ 4.0 4.1 4.2 4.3 Zipes, Douglas (2019). Braunwald’s heart disease : a textbook of cardiovascular medicine. Philadelphia, PA: Elsevier/Saunders. ISBN 978-0323463423.
- ↑ Aronson J (1999). “Hepatojugular reflux”. BMJ. 318 (7192): 1172. PMID 10221938. Free Full Text.
Looking for the patient version?
© 2026 MyEClinic – IFTM Institut für Telematik in der Medizin GmbH