
Cardiology
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]
Cardiology is the branch of medicine pertaining to the heart.
Cardiac pacemaker (Electrical system of the heart)
- Electrical conduction system of the heart
- Sinoatrial node
- Atrioventricular node
- Bundle of His
- Purkinje fibers
Basic cardiac physiology
Disorders of the coronary circulation
Disorders of the coronary circulation
- Atherosclerosis
- Restenosis
- Coronary heart disease (Ischaemic heart disease, Coronary artery disease)
- Acute coronary syndrome
- Angina
- Myocardial infarction (Heart attack)
Sudden cardiac death (The abrupt cessation of blood flow, leading to death)
Sudden cardiac death (The abrupt cessation of blood flow, leading to death)
Treatment of sudden cardiac death
For patient information click here
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editors-In-Chief: Sara Zand, M.D.[2] Cafer Zorkun, M.D., Ph.D. [3]; M.Umer Tariq [4]; Edzel Lorraine Co, DMD, MD[5] Nehal Eid, M.D.[6]
Related Chapters
Disorders of the myocardium (muscle of the heart)
Disorders of the myocardium (muscle of the heart)
- Cardiomyopathy
- Ischemic cardiomyopathy
- Nonischemic cardiomyopathy
- Amyloid cardiomyopathy
- Hypertrophic cardiomyopathy (HCM)
- Hypertrophic obstructive cardiomyopathy (HOCM) (Idiopathic hypertrophic subaortic stenosis (IHSS))
- Apical hypertrophic cardiomyopathy
- Dilated cardiomyopathy
- Alcoholic cardiomyopathy
- Tachycardia induced cardiomyopathy
- Takotsubo cardiomyopathy (Transient apical ballooning, stress-induced cardiomyopathy)
- Arrhythmogenic right ventricular dysplasia (Arrhythmogenic right ventricular cardiomyopathy)
- Restrictive cardiomyopathy
- Congestive heart failure
- Ventricular hypertrophy
- Primary tumors of the heart
- Myocardial rupture
Disorders of the pericardium (outer lining of the heart)
Disorders of the pericardium (outer lining of the heart)
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Assistant Editor(s)-in-Chief: Rim Halaby
Overview
The pericardium is a double-walled sac that contains the heart and the roots of the great vessels. Morphologically, it is a conical-shaped, double-walled fibro-serous membrane. It rests posteriorly to the sternum at the level of second to sixth costal cartilages and T5-T8 vertebrae.
Layers
- The pericardium is made up of two layers:
- Fibrous pericardium
- Serous pericardium
- Smooth internal layer made up of 2 components:
- Parietal: reflects onto fibrous pericardium
- Visceral: reflects onto heart and great vessels and forms the epicardium, the external layer of the heart wall
- Smooth internal layer made up of 2 components:
- Pericardial cavity: Potential space between parietal and visceral layers. It contains a serous fluid film that occupies the cavity and functions as lubricant against friction by all chest movements.[1][2][3]
Pericardial Sinuses
- There are two small chambers or sinuses located where the visceral and parietal pericardia are continuous with one another within the pericardial cavity.
- Transverse sinus:
- Located posterior to the pulmonary trunk and ascending aorta at the level between the superior vena cava and aortic arch
- Formed after dorsal mesocardium rupture embryonically
- Functional role is to allow the unhindered expansion of great arteries posteriorly during cardiac systole
- Utilized surgically to pass surgical clamps or place ligatures around great arteries.
- Oblique sinus:
- A blind recess (cul-de-sac) posterior to the left atrium between superior vena cava, right and left pulmonary veins inferior to the transverse sinus
- Formed embryonically by the incorporation of the pulmonary vein tributaries into the left atrium
- Functional role believed to be the expansion of the left atrium upon normal collapse of the thorax[4][5][6]


Diseases of the Pericardium
- Pericarditis is an inflammatory condition of the pericardium.
- Pericardial effusion is fluid accumulation in the pericardial sac.
- Constrictive pericarditis occurs when there is a scar encasing, the heart that chronically constricts the filling of the heart.
- Cardiac tamponade is a medical emergency in which fluid in the pericardial sac acutely restricts the filling of the heart. This requires surgical drainage or pericardiocentesis.
Additional Images
-
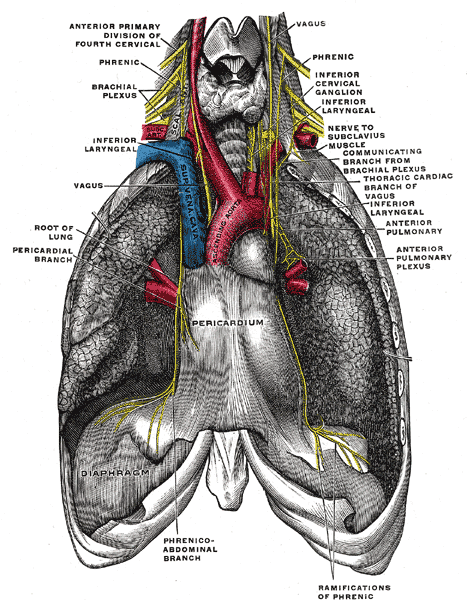 The phrenic nerve and its relations with the vagus nerve.
The phrenic nerve and its relations with the vagus nerve. -
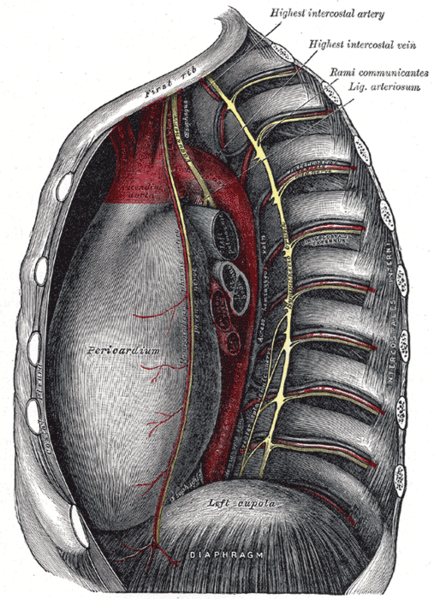 Thoracic portion of the sympathetic trunk.
Thoracic portion of the sympathetic trunk. -
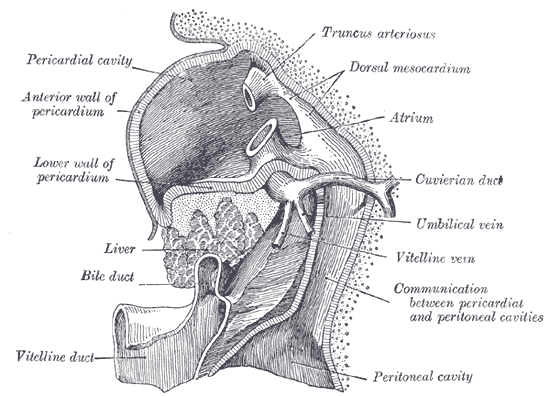 Liver with the septum transversum. Human embryo 3 mm long.
Liver with the septum transversum. Human embryo 3 mm long. -
 The thymus of a full-time fetus, exposed in situ.
The thymus of a full-time fetus, exposed in situ.




References
- ↑ Kishore, K. (2003). The Heart of Structural Development: The Functional Basis of the Location and Morphology of the Human Vascular Pump. J Postgrad Med, 49:282-4.
- ↑ Moore, K. L., Agur, A. M., & Dalley, A. F. (2011). Essential Clinical Anatomy – Fourth Edition. Lippincott Williams & Wilkins.
- ↑ Tank, P. W. (2009). Grant’s Dissector – Fourteenth Edition. Lippincott Williams & Wilkins.
- ↑ Kishore, K. (2003). The Heart of Structural Development: The Functional Basis of the Location and Morphology of the Human Vascular Pump. J Postgrad Med, 49:282-4.
- ↑ Moore, K. L., Agur, A. M., & Dalley, A. F. (2011). Essential Clinical Anatomy – Fourth Edition. Lippincott Williams & Wilkins.
- ↑ Tank, P. W. (2009). Grant’s Dissector – Fourteenth Edition. Lippincott Williams & Wilkins.
de:Herzbeutel it:Pericardio la:Pericardium ms:Perikardium nl:Pericard nn:Hjartepose fi:Perikardium
Disorders of the heart valves
Disorders of the heart valves
- Aortic valve disorders
- Mitral valve disorders
- Pulmonary valve disorders
- Congenital pulmonic stenosis
- Tricuspid valve disorders

Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]
Overview
In anatomy, the heart valves are valves in the heart that maintain the unidirectional flow of blood by opening and closing depending on the difference in pressure on each side. The mechanical equivalent of the heart valves would be the reed valves.
There are four valves of the heart (not counting the valve of the coronary sinus and valve of the inferior vena cava):
- The two atrioventricular (AV) valves ensure blood flows from the atria to the ventricles, and not the other way.
- The two semilunar (SL) valves are present in the arteries leaving the heart, and they prevent blood flowing back from the arteries into the ventricles.
The sound of the heart valves shutting causes the heart sounds.
Atrioventricular valves
The atrioventricular valves are large, multicusped valves that prevent backflow from the ventricles into the atria during systole. They are anchored to the wall of the ventricle by chordae tendinae, that prevent the valve from inverting.
The chordae tendinae are attached to papillary muscles that cause tension to better hold the valve. Together, the papillary muscles and the chordae tendinae are known as the subvalvular apparatus. The function of the subvalvular apparatus is to keep the valves from prolapsing into the atria when they close. The subvalvular apparatus have no effect on the opening and closure of the valves, however. This is caused entirely by the pressure gradient across the valve.
Mitral valve
Also known as the bicuspid valve, the mitral valve gets its name from the resemblance to a bishop’s mitre (a type of hat). It prevents blood flowing from the left ventricle into the left atrium. It is on the left side of the heart and has two leaflets.
A common complication of rheumatic fever is thickening and stenosis of the mitral valve.
Tricuspid valve
The tricuspid valve is on the right side of the heart, between the right atrium and the right ventricle.
Semilunar valves
The semilunar vlalves are positioned on the pulmonary artery and the aorta. These valves do not have chordae tendinae, but are more similar to valves in veins.
Aortic valve
The aortic valve lies between the left ventricle and the aorta. The aortic valve has three cusps. During ventricular systole, pressure rises in the left ventricle. When the pressure in the left ventricle rises above the pressure in the aorta, the aortic valve opens, allowing blood to exit the left ventricle into the aorta. When ventricular systole ends, pressure in the left ventricle rapidly drops. When the pressure in the left ventricle decreases, the aortic pressure forces the aortic valve to close. The closure of the aortic valve contributes the A2 component of the second heart sound (S2).
The most common congenital abnormality of the heart is the bicuspid aortic valve. In this condition, instead of three cusps, the aortic valve has two cusps. This condition is often undiagnosed until the person develops calcific aortic stenosis. Aortic stenosis occurs in this condition usually in patients in their 40s or 50s, an average of over 10 years earlier than in people with normal aortic valves.
Pulmonic valve
The pulmonic valve lies between the right ventricle and the pulmonary artery and also has three cusps.
Pathology of the valves
- Endocarditis – inflammation of the inner layer of the endocardium.
- Stenosis – a constricture of the heart valve, making it hard for blood to get through.
- Insufficiency (also regurgitation or incompetence) – the inability of the heart valve to close properly, meaning some blood can flow the wrong way.
-
 An artificial heart valve may be used to surgically replace a patient’s damaged valve.
An artificial heart valve may be used to surgically replace a patient’s damaged valve. -
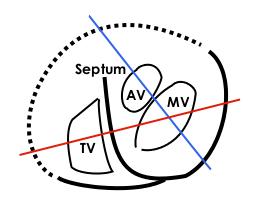 MV: Mitral valve, TV: Tricuspid valve, AV: Aortic valve, Septum: Interventricular septum. Continuous lines demarkates septum and free wall seen in echocardiogram, dotted line is a suggestion of where the free wall of the right ventricle should be. The red line represents where the upper left loop in the echocardiogram transects the 3D-loop, the blue line represents the lower loop.
MV: Mitral valve, TV: Tricuspid valve, AV: Aortic valve, Septum: Interventricular septum. Continuous lines demarkates septum and free wall seen in echocardiogram, dotted line is a suggestion of where the free wall of the right ventricle should be. The red line represents where the upper left loop in the echocardiogram transects the 3D-loop, the blue line represents the lower loop.


See also
- Disorders of the valves (Valvular heart disease)
- Aortic valve disorders:
- Mitral valve disorders
- Pulmonic valve disorders
- Tricuspid valve disorders
- Cardiac fibrosis
- Congenital heart disease
- Endocarditis
- Heart sounds
- Artificial heart valve

External links
- Mitral Valve Repair at The Mount Sinai Hospital – “Mitral Valve Anatomy”
Additional Reading
- Moss and Adams’ Heart Disease in Infants, Children, and Adolescents Hugh D. Allen, Arthur J. Moss, David J. Driscoll, Forrest H. Adams, Timothy F. Feltes, Robert E. Shaddy, 2007 ISBN 0781786843
- Hurst’s the Heart, Fuster V, 12th ed. 2008, ISBN 978-0-07-149928-6
- Willerson JT, Cardiovascular Medicine, 3rd ed., 2007, ISBN 978-1-84628-188-4
de:Herzklappe
eo:Korvalvo
he:שסתום הלב
it:Valvola cardiaca
nl:Hartklep
nn:Hjarteklaff
Disorders of the electrical system of the heart (Cardiac electrophysiology)
Disorders of the electrical system of the heart (Cardiac electrophysiology)
- Tachycardia
- Cardiac arrhythmias
- Supraventricular tachycardia (Fast rhythms that originate above the ventricles)
- Atrial fibrillation
- Atrial flutter
- Atrial tachycardia
- Sick sinus syndrome (Tachy-Brady syndrome)
- AV nodal reentrant tachycardia (AVNRT)
- AV reentrant tachycardia (AVRT)
- Bigeminy
- Premature ventricular contraction
- Ventricular tachycardia
- Ventricular fibrillation
- Sick sinus syndrome
- Bundle branch block
- Heart block
- Supraventricular tachycardia (Fast rhythms that originate above the ventricles)
- Specific diseases of the electrical system of the heart
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Assistant Editor(s)-in-Chief: Rim Halaby; Serge Korjian
Overview
- Cardiac electrophysiology (also referred to as clinical cardiac electrophysiology , or electrophysiology) is the science of the mechanisms, functions, and performance of the electrical activities of specific regions of the heart.
- The normal electrical conduction in the heart allows the impulse that is generated by the sinoatrial node (SA node) of the heart to be propagated to (and stimulate) the myocardium (Cardiac muscle). The myocardium contracts after stimulation. It is the ordered stimulation of the myocardium that allows efficient contraction of the heart, thereby allowing blood to be pumped throughout the body.
Cardiac Conduction System
- Proper cardiac function heavily depends on the ability of the cardiomyocytes to receive and propagate an electrical impulse allowing the heart to contract.
- These impulses, known as action potentials, originate and travel through the cardiac conduction system.
- A time-ordered propagation of the electrical impulse through the myocardium allows efficient contraction of all four chambers of the heart, starting with the atria pumping the blood toward the ventricles, followed by the ventricles which contribute to the pulmonary and systemic circulation.
The Components of the Cardiac Conduction System:
- The sinus (sinoatrial) node
- The internodal tracts
- The atrioventricular (AV) node
- The His/AV bundle
- The right and left bundle branches,
- The Purkinje fibers.
The Direction of Propagation of the Action Potential:
- The initial cardiac impulse, produced by pacemaker cells, originates in the sinoatrial (SA) node at the intersection of the right atrium and the superior vena cava.
- This action potential is the trigger of every cardiac cycle, initiating the atrial then ventricular contractions; it is henceforth responsible for the rhythmic beating of the heart.
- This action potential then propagates as a wave of depolarization through the internodal tracts initiating atrial contraction and then converging at the AV node.
- The convergence occurs because, in a normal heart, the AV node is the only electrical connection between the atria and the ventricles.
- The conduction of this potential is delayed at the AV node mainly due to the slower depolarization in these cells.
- This delay is represented as the PR interval of the ECG.
- The electrical impulse then moves to the ventricles by means of the AV or His bundle located in the superior portion of the interventricular septum.
- It then continues moving apically and propagating through both [[]]ventricles via the right and left bundle branches, and the Purkinje fibers.[1][2][3][4]
-
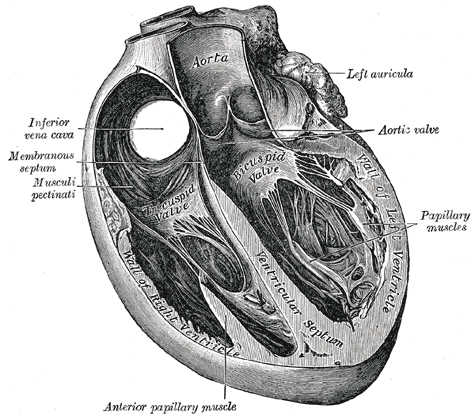 Section of the heart showing the ventricular septum.
Section of the heart showing the ventricular septum. -
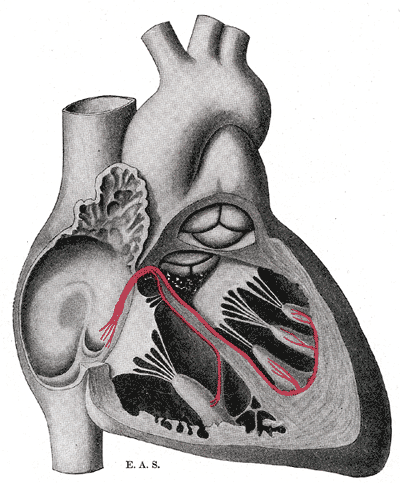 Schematic representation of the atrioventricular bundle of His.
Schematic representation of the atrioventricular bundle of His.

- Similarly to skeletal muscle cells which are also striated muscles, the cardiomyocytes contract in response to a rapid alteration in the cell membrane’s potential.
- However, the cardiomyocytes differ from skeletal muscle cells by three important variations that are essential for cardiac function:
- 1) They can self-generate a change in cell membrane potential.
- 2) The action potential can be transmitted directly from cell to cell.
- 3) The action potentials have a significantly longer duration.
The Resting Membrane Potential
- All cells including cardiomyocytes have a resting membrane potential that is maintained assuming there is no electrical charge crossing the membrane from the intracellular towards the extracellular milieu or vice versa.
- This potential is estimated to be –80 to –90 mV.
- The most crucial ions that determine this resting potential are:
- Sodium (Na+)
- Calcium (Ca2+)
- Potassium (K+)
- Sodium (Na+) and calcium (Ca2+) are most present in the interstitial fluid, while potassium (K+) is more present in intracellularly.
- These ions are lipid insoluble which prevents them from crossing the lipid bilayer or the cell membrane.
- Alternatively, ions cross via specific protein structures in the cell membrane that may be either: ion channels, ion pumps, or ion exchangers.
- These transmembrane proteins are highly specific and allow only one type of ion to pass through which allows good maintenance of the membrane potential.
- Ion channels can be opened, inactivated or closed depending on complex factors that modulate their activity.
The Cardiac Action Potential
- The cardiac contraction action potential is divided into 5 phases.
Phase 0: Depolarization
- The initial rapid increase in the transmembrane potential from -80mV to approximately +30mV constitutes the Phase 0 or the depolarization phase.
- This depolarization results from a rapid increase in the membrane permeability to Na+ ions via opening of voltage-dependent fast Na+ channels allowing Na+ ions to move intracellularly according to their electrochemical gradient.
- Following the conduction of an action potential, a recovery phase is attained where a large number of Na+ channels are inactivated, preventing the conduction of a second action potential.
- When the membrane is fully repolarized, these channels are reactivated and allow the conduction of the following action potential.
Phase I: Initial Repolarization
- The phase I of the action potential, known as the initial rapid repolarization ensues, resulting from K+ and Cl- ion flux across the membrane.
- This forms the notch seen in the action potential following the depolarization.
Phase II: Plateau
- Phase II, almost exclusive to cardiomyocytes, represents a plateau in the membrane potential as an outcome of the equilibrium between Ca2+ influx and K+ outflow.
- The channels responsible for this Ca2+ influx are known as the L-type calcium channels, which are activated rapidly when the membrane potential reaches -50mV, but are slowly inactivated thereafter.
- Throughout this plateau phase, few Na+ channels also remain active.
- These are Na+/Ca2+ exchangers that allow 1 ion of calcium to move outside the cell for every 3 molecules of sodium moving inside the cell.
Phase III: Repolarization
- The third phase, also known as rapid repolarization, depicts the restoration of a resting membrane potential.
- It is initiated by inactivation of the L-type calcium channels and an increase in K+ outflow.
- This change in potassium across the membrane is related to 3 K+ currents:
- 1) Inwardly rectifying K+ current (IK1) à Produces the resting membrane potential
- 2) Transient outward K+ current (ITO) à Accounts for initial part of repolarization
- 3) Delayed outward K+ current (IK) à Responsible for final part of repolarization
- After repolarization has occurred, intracellular Na+ and extracellular K+ are rearranged via the Na+/K+ ATPase pump.
- The ATPase moves 3 sodium ions out for every 2 potassium ions moved intracellularly.
- Equilibrium of ions across the membrane is also achieved via the Na+/Ca2+ exchangers.
Phase IV: Diastolic depolarization
- The phase IV of the action potential is characterized by a diastolic depolarization that is both spontaneous and slow.
- This phase provides cardiac cells with features of automaticity.
- In a normal functioning heart, only the sinoatrial node is able to reach a threshold potential during phase IV making it the pacemaker of the heart.
- Nevertheless other cells including those in the AV node, the His bundle, and the Purkinje fibers are able to reach a threshold and fire automatically if they are not suppressed by the SA node, which is true in some disease entities.
The factors responsible for the initial diastolic depolarization in the SA node are:
- Inward Ca2+ current
- Delayed outward K+ current
- IF Currents – Inward sodium-potassium currents activated if membrane repolarizes below the If threshold
- T-type Ca2+ channel – Releases calcium from internal stores
The rate of impulse generation by the SA node is determined by 3 factors:
- 1) The slope of diastolic depolarization
- 2) The maximal diastolic potential
- 3) The threshold potential
- All these factors are controlled by the autonomic nervous system allowing for the modulation of the rate of SA node firing and subsequently the heart rate.[1][5][3][4]
Electrophysiology Studies and Therapeutic Modalities
Overview
- An electrophysiologic study is a term used to describe a number of invasive (intracardiac) and non-invasive recording of spontaneous electrical activity as well as of cardiac responses to programmed electrical stimulation.
- These studies are performed to assess arrhythmias, elucidate symptoms, evaluate abnormal electrocardiograms, assess risk of developing arrhythmias in the future, and design treatment.
- These procedures increasingly include therapeutic methods (typically radiofrequency ablation) in addition to diagnostic and prognostic procedures.
- Other therapeutic modalities employed in this field include antiarrhythmic drug therapy and implantation of pacemakers and implantable cardioverter-defibrillators.
- A specialist in cardiac electrophysiology is known as a cardiac electrophysiologist, or (more commonly) simply an electrophysiologist. Cardiac electrophysiology is considered a subspecialty of cardiology, and in most countries requires two or more years of fellowship training beyond a general cardiology fellowship. They are trained to perform interventional cardiac EP procedures as well as surgical device implantations.
Diagnostic Testing
- Ambulatory electrocardiographic monitoring (Holter recording and interpretation; loop recording and interpretation)
- Tilt table testing
- Signal-averaged electrocardiogram (SAECG) interpretation, also referred to as “late potentials” reading
- Electrophysiologic study (EPS)
- Pacing and recording electrodes are inserted either in the esophagus (intra-esophageal EPS) or, through blood vessels, directly into the heart chambers (intra-cardiac EPS) in order to measure electrical properties of the heart. In addition, intra-cardiac EPS electrically stimulates the heart and induces arrhythmias for diagnostic purposes (“programmed electrical stimulation”).
Medical Treatment
Electrophysiologists play a role in:
- The initial administration and monitoring of the effect of drugs for treatment of heart rhythm disorders
- The management of severe or life threatening arrhythmias
- The management of arrythmias requiring multiple drugs use
Catheter Ablation
- Ablation therapy is the catheter based creation of lesions in the heart with radiofrequency energy, cryotherapy (destructive freezing), or ultrasound energy in order to cure or control arrhythmias (see radiofrequency ablation). Ablation is usually performed during the same procedure as the electrophysiology study which induces and confirms the diagnosis of the arrhythmia for which ablation therapy is sought.
Non-complex ablation
- It includes ablation for arrhythmias such as: AV nodal reentrant tachycardia, accessory pathway mediated tachycardia and atrial flutter.
- This procedure is usually performed using intracardiac catheters , fluoroscopy (a real-time X-ray camera), and electrical recordings from the inside of the heart.
Complex ablation
- It includes ablation for arrhythmias such as: multifocal atrial tachycardia, atrial fibrillation, and ventricular tachycardia.
- In addition to the apparatus used for a “non-complex” ablation, these procedures often make use of sophisticated computer mapping systems to localize the source of the abnormal rhythm and to direct delivery of ablation lesions.
Surgical Procedures: Pacemaker and Defibrillator Implantation and Follow Up
- Implantation of single and dual chamber pacemakers and defibrillators
- Implantation of “biventricular” pacemakers and defibrillators for patients with congestive heart failure
- Implantation of loop recorders (implanted ECG recorders for long term monitoring of ECG to allow for diagnosis of an arrhythmia)
- Clinical follow up and reprogramming of implanted devices
Abnormalities in Cardiac Electrophysiology
- Mechanism of Arrhythmias
- Diseases of the Conduction System and Bradyarrhythmias
- Narrow Complex Tachycardias
- Wide Complex Tachycardias
- Ventricular Tachyarrhythmias, Cardiac Arrest and Sudden Cardiac Death
- Arrhythmias in Pregnancy
Treatment Modalities for Arrhythmia
- Antiarrhythmic Medications
- Indications for Pacemakers
- Indications for an ICD
- Cardiac Resynchronization Therapy
- Catheter ablation
See also
- Clinical cardiac electrophysiology
- Electrical conduction system of the heart
- Electrocardiogram (EKG)
- Basic Principles of ECG Interpretation
- Electrophysiologic study
- Cardiology
- Cardiac arrhythmia
External links
References
- ↑ 1.0 1.1 David E. Mohrman, L. J. (2010). Cardiovascular Physiology, 7e. The McGraw-Hill Companies, Inc.
- ↑ Kim E. Barrett, S. B. (2012). Ganong’s Review of Medical Physiology, 24e . The McGraw-Hill Companies, Inc.
- ↑ 3.0 3.1 Olson, E. N. (2004). A decade of discoveries in cardiac biology. Nature Medicine, 467 – 474.
- ↑ 4.0 4.1 Valentin Fuster, R. A. (2011). Hurst’s The Heart, 13e. The McGraw-Hill Companies, Inc.
- ↑ Kim E. Barrett, S. B. (2012). Ganong’s Review of Medical Physiology, 24e . The McGraw-Hill Companies, Inc.
Inflammation and infection of the heart
Inflammation and infection of the heart
Congenital heart disease
- Atrial septal defect
- Ventricular septal defect
- Patent ductus arteriosus
- Bicuspid aortic valve
- Tetralogy of Fallot
- Transposition of the great vessels (TGV)
- Hypoplastic left heart syndrome
For patient information, click here
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-In-Chief: Priyamvada Singh, MBBS [2] Assistant Editor(s)-In-Chief: Kristin Feeney, B.S. [3]
Synonyms and keywords: CHD; cardiac malformation
Congenital heart disease (CHD) is the most common type of birth defect, accounting for about 1% of all cases [4]. Although mild cases of CHD are not detected until after discharge, most of the critical CHD cases are identified soon after birth requiring surgery or catheter-based intervention in the first year of life. CHD is broadly classified into three major groups, namely, cyanotic CHD, ductal-dependent CHD and critical CHD. Cyanotic CHD involves defects that lead to mixing of deoxygenated blood into the systemic circulation. Ductal-dependent CHD relies on the patency of the ductus arteriosus for supply of blood to the pulmonary or systemic outflow which allows adequate mixing between the parallel circulations. Lesions requiring surgery or catheter-based intervention in the first year of life are referred to as critical CHD which includes ductal-dependent and cyanotic lesions, as well as forms of CHD that, although not requiring surgery in the neonatal period, do necessitate intervention in the first year of life, such as a big ventricular septal defect or an atrioventricular canal defect (or atrioventricular septal defect).
Aortic stenosis | Atrial septal defect (ASD) | Atrial septal defect sinus venosus | Atrioventricular canal | Atrioventricular septal defect (AVSD) | Bicuspid aortic valve | Brugada syndrome | Cardiomyopathy | Coarctation of the aorta (CoA) | dextro-Transposition of the great arteries (d-TGA) | Dextrocardia | Ebstein’s anomaly | Hypoplastic left heart syndrome (HLHS) | Hypoplastic right heart syndrome | Interrupted aortic arch (IAA) | levo-Transposition of the great arteries (l-TGA) | Lutembacher’s syndrome | Mitral stenosis | Ostium primum | Ostium secundum | Partial anomalous pulmonary venous connection (PAPVC) | Patent ductus arteriosus (PDA) | Pulmonary atresia | Pulmonary stenosis | Septum primum | Subaortic stenosis | Tetralogy of Fallot (ToF) | Total anomalous pulmonary venous connection (TAPVC) | Tricuspid atresia | Truncus arteriosus | Ventricular septal defect (VSD)
Diagnosis
Diagnostic Criteria | History and Symptoms | Physical Examination | Laboratory Findings | Electrocardiogram | Chest X Ray | MRI | CT | Echocardiography | Prenatal Ultrasound | Other Imaging Findings
Treatment
Medical Therapy | Surgery | Prevention | Outcomes | Reproduction
Case Studies
Related Chapters
Diseases of blood vessels (Vascular diseases)
Diseases of blood vessels (Vascular diseases)
- Vasculitis
- Atherosclerosis
- Aneurysm
- Varicose veins
- Economy class syndrome
- Diseases of the aorta
- Diseases of the carotid arteries
Procedures done for coronary artery disease
Procedures done for coronary artery disease
- Percutaneous coronary intervention
- Atherectomy
- Angioplasty (PTCA)
- Stenting
- Coronary artery bypass surgery (CABG)
- Enhanced external counterpulsation (EECP)
hehe
Devices used in cardiology
Devices used in cardiology
- Stethoscope
- Devices used to maintain normal electrical rhythm
- Devices used to maintain blood pressure
Diagnostic tests and procedures
- Blood tests
- Echocardiogram
- Cardiac stress test
- Auscultation (Listening with the Stethoscope)
Electrocardiogram (ECG or EKG)
- Ambulatory Holter monitor
- Electrophysiologic study
- Sphygmomanometer (Blood pressure cuff)
- Cardiac enzymes
- Coronary catheterization
- Myocardial Fractional Flow Reserve (FFRmyo)
- IVUS (IntraVascular UltraSound)
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]
The diagnostic tests in cardiology are methods of identifying heart conditions associated with healthy vs. unhealthy, pathologic, heart function.
Bedside
History
Obtaining a medical history is always the first “test”, part of understanding the likelihood of significant disease, as detectable within the current limitations of clinical medicine. Yet heart problems often produce no symptoms until very advanced, and many symptoms, such as palpitations and sensations of extra or missing heart beats correlate poorly with realtive heart health vs disease. Hence, a history alone is rarely sufficient to diagnose a heart condition.
Auscultation
Auscultation employs a stethoscope to more easily hear various normal and abnormal sounds, such as normal heart beat sounds and the usual heart beat sound changes associated with breathing versus heart murmurs.
Laboratory
Blood tests
A variety of blood tests are available for analyzing cholesterol transport behavior, HDL, LDL, triglycerides, lipoprotein little a, homocysteine, C-reactive protein, blood sugar control: fasting, after eating or averages using glycosylated albumen or hemoglobin, myoglobin, creatine kinase, troponin, brain-type natriuretic peptide, etc. to assess the evolution of coronary artery disease and evidence of existing damage. A great many more physiologic markers related to atherosclerosis and heart function are used and being developed and evaluated in research.
| Test Name | Lower/normal risk | High risk | Cost $US (approx) |
|---|---|---|---|
| Total Cholesterol | <200 mg/dL | >240 mg/dL | |
| LDL-C | <100 mg/dL | >160 mg/dL | $150* |
| HDL-C | >60 mg/dL | <40 mg/dL | |
| Triglyceride | <150 mg/dL | >200 mg/dL | |
| Blood Pressure | <120/80 mmHg | >140/90 mmHg | |
| C-reactive protein | <1 mg/L | >3 mg/L | $20 |
| Fibrinogen | <300 mg/dL | >460 mg/dL | $100 |
| Homocysteine | <10 µmol/L | >14 µmol/L | $200 |
| Fasting Insulin | <15 µIU/mL | >25 µIU/mL | $75 |
| Ferritin | male 12–300 ng/mL female 12–150 ng/mL |
$85 | |
| Lipoprotein(a) – Lp(a) | <14mg/dL | >19mg/dL | $75 |
| Calcium Heart Scan | <100 | >300 | $250-600 |
(*) due to the high cost, LDL is usually calculated instead of being measured directly
source: Beyond Cholesterol, Julius Torelli MD, 2005 ISBN 0-312-34863-0
Electrophysiology
Electrocardiogram
Electrocardiography (ECG/EKG in German vernacular. Elektrokardiogram) monitors electrical activity of the heart, primarily as recorded from the skin surface. A 12 lead recording, recording the electrical activity in three planes, anterior, posterior, and lateral is the most commonly used form. The ECG allows observation of the heart electrical activity by visualizing waveform beat origin (typically from the sinoatrial or SA node) following down the bundle of HIS and ultimately stimulating the ventricles to contract forcing blood through the body. Much can be learned by observing the QRS morphology (named for the respective portions of the polarization/repolarization waveform of the wave, P,Q,R,S,T wave). Rhythym abnormalities can also be visualized as in slow heart rate bradycardia, or fast heart rate tachycardia.
Holter monitor
A Holter monitor records a continuous EKG rhythm pattern (rarely a full EKG) for 24 hours or more. These monitors are used for suspected frequent rhythm abnormalities, especially ones the wearer may not recognize by symptoms. They are more expensive than event monitors.
Event monitor
An Event monitor records short term EKG rhythm patterns, generally storing the last 2 to 5 minutes, adding in new and discarding old data, for 1 to 2 weeks or more. There are several different types with different capabilities. When the wearer presses a button on the monitor, it quits discarding old and continues recording for a short additional period. The wearer then plays the recording, via a standard phone connection, to a center with compatible receiving and rhythm printing equipment, after which the monitor is ready to record again. These monitors are used for suspected infrequent rhythm abnormalities, especially ones the wearer does recognize by symptoms. They are less expensive than Holter monitors.
Cardiac stress testing
Cardiac stress testing is used to determine to assess cardiac function and to disclose evidence of exertion-related cardiac hypoxia. Radionuclide testing using thallium or technetium can be used to demonstrate areas of perfusion abnormalities. With a maximal stress test the level of exercise is increased until the patient heart rate will not increase any higher, despite increased exercise. A fairly accurate estimate of the target heart rate, based on extensive clinical research, can be estimated by the formula 220 beats per minute minus patient’s age. This linear relation is accurate up to about age 30, after which it mildly underestimates typical maximum attainable heart rates achievable by healthy individuals. Other formulas exist, such as that by Miller (217 – (0.85 × Age)) and others[2]. Achieving a high enough heart rate at the end of exercise is critical to improving the sensitivity of the test to detect high grade heart artery stenosis.
Medical imaging
Coronary catheterization
Coronary catheterization uses pressure monitoring and blood sampling through a catheter inserted into the heart through blood vessels in the leg to determine the functioning of the heart, and, following injections of radiocontrast dye, uses X-ray fluoroscopy, typically at 30 frames per second, to visualize the position and size of blood within the heart chambers and arteries. Coronary angiography is used to determine the patency and configuration of the coronary artery lumens.
Echocardiogram
Echocardiography uses ultrasonic waves for continuous heart chamber and blood movement visualization. In recent times, it has become one of the most commonly used tools in diagnosis of heart problems, as it allows non-invasive visualization of the heart and the blood flow through the heart, using a technique known as Doppler.
Intravascular ultrasound
Intravascular ultrasound, an imaging methodology using specially designed, long, thin, complex manufactured catheters attached to computerized ultrasound equipment to visualize the lumen and the interior wall of blood vessels.
Positron emission tomography
Positron emission tomography, an imaging methodology for positron emitting radioisotopes. PET enables visual image analysis of multiple different metabolic chemical processes and is thus one of the most flexible imaging technologies. Cardiology uses are growing very slowly due to technical and relative cost difficulties. Most uses are for research, not clinical purposes. Appropriate radioisotopes of elements within chemical compounds of the metabolic pathway being examined are used to make the location of the chemical compounds of interest visible in a PET scanner constructed image.
Computed Tomography Angiography
Computed Tomography Angiography (CTA), an imaging methodology using a ring-shaped machine with an X-Ray source spinning around the circular path so as to bathe the inner circle with a uniform and known X-Ray density. Cardiology uses are growing with the incredible developments in CT technology. Currently, multidetector CT, specially the 64 detector-CT are allowing to make cardiac studies in just a few seconds (less than 10 seconds, depending on the equipment and protocol used). This images are reconstructed using algorithms and software. Great development and growth will be seen in the short term, allowing radiologists to diagnose cardiac artery disease without anesthesia and in a non-invasive way.
Magnetic resonance imaging
Magnetic resonance imaging (originally called nuclear magnetic resonance imaging), an imaging methodology based on aligning the spin axis of nuclei within molecules of the object being visualized using both powerful superconducting magnets and radio frequency signals and detectors. Cardiology uses are growing, especially since MRI differentiates soft tissues better than CT. The principle difficulty with current implementations, for Cardiology uses, is the difficulty of imaging the ever moving heart structures, more so than with CT because MRI is much slower. However, there is a promising future in cardiac MRI.
See also
Cardiac pharmaceutical agents
Cardiac pharmaceutical agents
The followings are medications commonly prescribed in cardiology:
- Antiarrhythmic agents
- Type I (sodium channel blockers)
- Type Ia
- Type Ib
- Type Ic
- Type II (beta blockers)
- Type III (potassium channel blockers)
- Type IV (slow calcium channel blockers)
- Type V
- Type I (sodium channel blockers)
- ACE inhibitors
- Angiotensin II receptor antagonists
- Beta blocker
- Calcium channel blocker
See also
See also
- Interventional cardiology
- Clinical cardiac electrophysiology
- Heart Failure Society of America
External links
External links
- European Society of Cardiology
- U.S. National Institute of Health (NIH)
- American College of Cardiology
- American Heart Association
- National Heart Foundation Australia
- Coronary heart disease
- Virtual Cardiac Centre – latest comprehensive information on the field of Cardiology.
- Cardiovascular Physiology – comprehensive explanation of basic concepts in cardiology.
- Preventive Cardiology
ast:Cardioloxía ca:Cardiologia de:Kardiologie eu:Kardiologia hr:Kardiologija id:Kardiologi it:Cardiologia he:קרדיולוגיה la:Cardiologia nl:Cardiologie no:Kardiologi nds:Kardiologie sq:Kardiologjia sl:Kardiologija sh:Kardiologija sv:Kardiologi uk:Кардіологія
Template:WikiDoc Sources
CME Category::Cardiology
CME Category::Cardiology
Looking for the patient version?
© 2026 MyEClinic – IFTM Institut für Telematik in der Medizin GmbH