
Cholangitis
For patient information click here
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1] Assosciate Editor(s)-In-Chief: Amandeep Singh M.D.[2], Prashanth Saddala M.B.B.S, Farwa Haideri [3]
Synonyms and keywords: Cholangitis; bile duct infection; bile duct inflammation; common bile duct inflammation; common bile duct infection
Overview
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Amandeep Singh M.D.[2],Farwa Haideri [3]
Overview
Cholangitis is an infection of the bile duct, which transports bile from the liver to the intestines and the gallbladder. Symptoms include fever, right upper quadrant pain, and jaundice due to the infection of the bile duct and inflammation of the biliary tree, which is usually the result of obstruction and stasis.
Historical Perspective
- Dr. Jean-Martin Charcot, a French physician, is credited with discovering the disease in the late 19th century. He referred to the condition as “hepatic fever.”
- Charcot’s triad of fever, jaundice, and right upper quadrant abdominal pain is the classical presentation of cholangitis.
- By adding septic shock and mental status changes to the list of symptoms, Dr. B. M. Reynolds and Dr. Everett L. Dargan changed Charcot’s triad to Reynold’s pentad.
- Until 1968, the mainstay of treatment of cholangitis was surgery, with exploration of the bile duct and excision of gallstones, until the advent of endoscopic retrograde cholangiopancreatography (ERCP).
Classification
Acute cholangitis is classified into grade I, II, or III, depending on the severity of the condition.
Pathophysiology
Cholangitis involves two main factors: an increase in the bacterial presence and elevated intraductal pressure in the bile duct, both of which allow for the translocation of bacteria or endotoxins in the vascular system. Bacterial contamination alone does not usually result in cholangitis. Increased pressure in the biliary system, from obstruction in the bile duct, widens the spaces between the cells lining the duct, which brings bacterially contaminated bile into the bloodstream.
Causes
Cholangitis is usually caused by a bacterial infection, which can occur due to blockage in the duct, such as from a gallstone or tumor. The infection causing this condition may also spread to the liver.
Differential Diagnosis
Cholangitis must be differentiated from other causes of infection in the common bile duct, as well as from inflammation and infection of cholecystitis.
Epidemiology and Demographics
Cholangitis is most prevalent in adults, with roughly 20% of the adult population suffering from some form of abdominal pain from gallstones passing through the bile duct into the digestive tract.
Risk Factors
Common risk factors in the development of cholangitis are gallstones, sclerosing cholangitis, and HIV. Variations in treatment and risk factors influence mortality rates in patients with cholangitis, and these rates underscore the necessity for standardized diagnostic, treatment, and severity assessment criteria.
Screening
There are no established screening processes for cholangitis or cholangiocarcinoma, a cancer associated with this disease. There are methods to detect the early onset of both diseases.
Natural History, Complications, and Prognosis
Patients who show early signs of multiple organ failure (renal failure, disseminated intravascular coagulation, alterations in the level of consciousness, and shock) or evidence of acute cholangitis, as well as those who do not respond to conservative treatment, should receive systemic antibiotics and undergo emergent biliary drainage. Unless early and appropriate biliary drainage is performed and systemic antibiotics are administered, death will occur. Prognosis is usually good with treatment, but poor without it.
Diagnosis
History and Symptoms
A positive history of gallstones and common bile duct stones, recent cholecystectomy, endoscopic manipulation or endoscopic retrograde cholangiopancreatography (ERCP), cholangiogram and history of HIV or AIDS. Symptoms of cholangitis include fever, abdominal pain, nausea and vomiting, jaundice/yellowish discoloration of skin, acholic stools/pale stools, pruritus, malaise, and confusion
Physical Examination
Charcot’s triad, which includes abdominal pain, jaundice, and fever, describes three common findings in cholangitis. Reynold’s pentad, which includes Charcot’s triad and two other symptoms, septic shock and mental confusion, also provides common markers in a physical examination for cholangitis. Cholangitis is associated with significant morbidity and mortality.
Laboratory Findings
Laboratory tests provide useful clues in the diagnosis of cholangitis. Some commonly conducted tests include complete blood count, basic metabolic panel, liver function tests, blood culture, and other body fluid cultures.
X-Ray
There are no x-ray findings associated with acute cholangitis.
CT
CT scans may be helpful in locating, with high sensitivity, the site of the obstruction responsible for a case of cholangitis.
MRI
There are no MRI findings associated with acute cholangitis.
Ultrasound
Ultrasounds (US) are the primary imaging modality for cholangitis. An US is both sensitive and specific in demonstrating biliary dilatation.
Other Imaging Findings
There are no other imaging findings associated with cholangitis
Other Diagnostic Studies
Endoscopic retrograde cholangiopancreatography (ERCP) is considered a gold standard test for biliary obstruction. Magnetic resonance cholangiopancreatography (MRCP) and Percutaneous transhepatic cholangiography (PTCA) are the most sensitive techniques to correctly determine the underlying cause and level of biliary obstruction in patients with acute cholangitis when ERCP fails.
Diagnostic Criteria
Shown below are the diagnostic criteria for acute cholangitis according to Tokyo guidelines:
- The diagnosis is “suspected” in the case of the presence of one item in systemic inflammation with one item in either cholestasis or imaging findings.
- The diagnosis is “definite” in the case of the presence of one item in systemic inflammation, one item in cholestasis, and one item in imaging.
| Clinical Manifestations | Changes from the baseline |
|---|---|
| Systemic inflammation | ♦ Fever >38℃ and/or shaking chills ♦ Evidence of inflammatory response: – WBC (×1000/μl) <4, or >10 – CRP (mg/dl) ≥1 |
| Cholestasis | ♦ Jaundice with total bilirubin ≥2 (g/dl) ♦ Abnormal liver function tests: – ALP (IU) >1.5×STD – γGTP (IU) >1.5×STD – AST (IU) >1.5×STD – ALT (IU) >1.5×STD |
| Imaging findings | ♦ Biliary dilatation ♦ Evidence of the etiology (stricture, stone, stent, etc.) on imaging (abdominal X-ray: KUB, abdominal USG, CT scan, MRI, MRCP, and HIDA scan) |
Severity Assessment Criteria
The severity assessment criteria for acute cholangitis according to Tokyo guidelines are as follows:
Grade III Acute Cholangitis
Grade III, or severe acute cholangitis, is characterized by the onset of dysfunction in at least one of the following:
- Cardiovascular system: decreased blood pressure that necessitates the administration of dopamine (>5 μg/kg/min) or norepinephrine
- Neurological system: abnormal consciousness
- Respiratory system: PaO2/FiO2 ratio <300
- Renal system: serum creatinine >2.0 mg/dl, decreased urine output
- Hepatic system: PT-INR >1.5
- Hematological system: platelet count < 100,000/mm3
Grade II Acute Cholangitis
Grade II, or moderate acute cholangitis, is characterized by the presence of any two of the following:
- Abnormal WBC count: >12,000/mm3, <4,000/mm3
- Fever ≥39°C
- Age ≥75 years
- Elevated total bilirubin ≥5 mg/dl
- Decreased albumin level <0.7 x STD
Grade I Acute Cholangitis
Grade I, or mild acute cholangitis, does not meet the criteria of either grade II (moderate) or grade III (severe) acute cholangitis.
Treatment
Medical Therapy
Antimicrobial therapy is indicated for acute cholangitis. Patients with community-acquired mild-to-moderate disease are treated with Cephalosporins. All other patients are treated with a combination of Metronidazole and either Imipenem-Cilastatin, Meropenem, Doripenem, Piperacillin-Tazobactam, Ciprofloxacin, Levofloxacin, or Cefepime.
Surgery
Surgery is not recommended for the treatment of cholangitis.
Primary Prevention
Although re-establishing biliary drainage is the main focus of treatment, antibiotics play an important role in the management of cholangitis.
Secondary Prevention
Secondary prevention strategies for cholangitis include continued treatment of predisposing causes in appropriate patients.
Cost-Effectiveness of Therapy
The most cost-effective technique to diagnose cholangitis is an ultrasound.
References
Historical Perspective
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Amandeep Singh M.D.[2], Farwa Haideri [3]
Overview
Dr. Jean-Martin Charcot, a French physician, is credited with discovering cholangitis in the late 19th century. He referred to the condition as “hepatic fever.” Charcot’s triad of fever, jaundice, and right upper quadrant abdominal pain is the classical presentation of cholangitis. By adding septic shock and mental status changes to the list of symptoms, Dr. B. M. Reynolds and Dr. Everett L. Dargan changed Charcot’s triad to Reynold’s pentad. Until 1968, the mainstay of treatment of cholangitis was surgery, with the exploration of the bile duct and excision of gallstones, until the advent of endoscopic retrograde cholangiopancreatography (ERCP).
Historical Perspective
- In 1877, at the Salpêtrière Hospital in Paris, France, Dr. Jean-Martin Charcot was first credited with describing cholangitis.[1]
- He initially referred to this condition as a triad of three symptoms: abdominal pain, fever, and jaundice.
- In 1959, American surgeon Dr. Benedict M. Reynolds ignited interest in the condition with his report with colleague Dr. Everett L. Dargan.[2]
- The report discussed how the condition was generally treated by surgeons, as an exploration of the bile duct and excision of gallstones.
- Reynolds and Dargan recognized that septic shock and mental status changes portended a poor outcome.[3][4][5][6]
- The addition of these two symptoms gave rise to the Reynold’s pentad, which is commonly used in clinical practice nowadays.
- In 1968, endoscopic retrograde cholangiopancreatography (ERCP) was first used for the diagnosis and management of acute cholangitis.
- In modern times, seventy to eighty percent of cases of acute cholangitis are resolved by antibiotics; some cases may require ERCP to achieve surgical decompression.[1][7]
References
- ↑ 1.0 1.1 Kimura Y, Takada T, Kawarada Y, Nimura Y, Hirata K, Sekimoto M, Yoshida M, Mayumi T, Wada K, Miura F, Yasuda H, Yamashita Y, Nagino M, Hirota M, Tanaka A, Tsuyuguchi T, Strasberg SM, Gadacz TR (2007). “Definitions, pathophysiology, and epidemiology of acute cholangitis and cholecystitis: Tokyo Guidelines”. J Hepatobiliary Pancreat Surg. 14 (1): 15–26. doi:10.1007/s00534-006-1152-y. PMC 2784509. PMID 17252293.
- ↑ REYNOLDS BM, DARGAN EL (1959). “Acute obstructive cholangitis; a distinct clinical syndrome”. Ann. Surg. 150 (2): 299–303. PMC 1613362. PMID 13670595.
- ↑ Kadakia S. Biliary Tract Emergencies. Med Clin North Amer. 1993, 77(5) 1015-1036. PMID 8371614
- ↑ Carpenter H. Bacterial and Parasitic Cholangitis. May Clin Proc. 1998, 73:473-478. PMID 9581592
- ↑ Leese T, Neoptolemos JP, Baker AR. Management of acute cholangitis and the impact of endoscopic sphincterotomy. Br J Surg. 1986, 73:988. PMID 3790964
- ↑ Lai ECS, Mok FPT, Tan ESY. Endoscopic biliary drainage for severe acute cholangitis. NEJM 1992, 326:1582-6. PMID 1584258
- ↑ Hui CK, Lai KC, Yuen MF, Ng M, Lai CL, Lam SK (2001). “Acute cholangitis–predictive factors for emergency ERCP”. Aliment. Pharmacol. Ther. 15 (10): 1633–7. PMID 11564004.
Classification
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Amandeep Singh M.D.[2], Vendhan Ramanujam M.B.B.S [3], Farwa Haideri [4]
Overview
Acute cholangitis may be classified into grade I, II, or III, depending on the severity of the condition.
Classification
The severity of cholangitis can be classified into three grades, based on the onset of organ dysfunction and the patient’s response to the initial medical treatment:[1][2][3]
- Mild (grade I)
- Moderate (grade II)
- Severe (grade III)
The severity assessment criteria for acute cholangitis according to Tokyo guidelines is as follows:[4][5][6]
| Severity assessment of cholangitis | |||
|---|---|---|---|
| Criterion | Severity | ||
| Mild (grade I) | Moderate (grade II) | Severe (grade III) | |
| Onset of organ dysfunction | – | – | + |
| Response to medical treatment | + | – | – |
Grade I acute cholangitis
Grade I, or mild acute cholangitis, don’t meet the criteria of neither grade II (moderate) nor grade III (severe) acute cholangitis. The patient responds to initial medical treatment.
Grade II acute cholangitis
Grade II, or moderate acute cholangitis, is characterized by the presence of any two of the following:
- Abnormal white blood cell (WBC) count: >12,000/mm3, <4,000/mm3
- Fever ≥39°C
- Age ≥75 years
- Elevated total bilirubin ≥5 mg/dl
- Decreased albumin level <0.7 x standard
Grade III acute cholangitis
Grade III, or severe acute cholangitis, is characterized by the onset of dysfunction in at least one of the following:
- Cardiovascular system: decreased blood pressure that necessitates the administration of dopamine (>5 μg/kg/min) or norepinephrine
- Neurological system: abnormal consciousness
- Respiratory system: PaO2/FiO2 ratio <300
- Renal system: serum creatinine >2.0 mg/dl, decreased urine output
- Hepatic system: PT-INR >1.5
- Hematological system: platelet count < 100,000/mm3
References
- ↑ Wada K, Takada T, Kawarada Y, Nimura Y, Miura F, Yoshida M, Mayumi T, Strasberg S, Pitt HA, Gadacz TR, Büchler MW, Belghiti J, de Santibanes E, Gouma DJ, Neuhaus H, Dervenis C, Fan ST, Chen MF, Ker CG, Bornman PC, Hilvano SC, Kim SW, Liau KH, Kim MH (2007). “Diagnostic criteria and severity assessment of acute cholangitis: Tokyo Guidelines”. J Hepatobiliary Pancreat Surg. 14 (1): 52–8. doi:10.1007/s00534-006-1156-7. PMC 2784515. PMID 17252297.
- ↑ Zimmer V, Lammert F (June 2015). “Acute Bacterial Cholangitis”. Viszeralmedizin. 31 (3): 166–72. doi:10.1159/000430965. PMC 4569195. PMID 26468310.
- ↑ Lee JG (September 2009). “Diagnosis and management of acute cholangitis”. Nat Rev Gastroenterol Hepatol. 6 (9): 533–41. doi:10.1038/nrgastro.2009.126. PMID 19652653.
- ↑ Mayumi, T.; Someya, K.; Ootubo, H.; Takama, T.; Kido, T.; Kamezaki, F.; Yoshida, M.; Takada, T. (2013). “Progression of Tokyo Guidelines and Japanese Guidelines for management of acute cholangitis and cholecystitis”. J UOEH. 35 (4): 249–57. PMID 24334691.
- ↑ Takada T, Strasberg SM, Solomkin JS, Pitt HA, Gomi H, Yoshida M, Mayumi T, Miura F, Gouma DJ, Garden OJ, Büchler MW, Kiriyama S, Yokoe M, Kimura Y, Tsuyuguchi T, Itoi T, Gabata T, Higuchi R, Okamoto K, Hata J, Murata A, Kusachi S, Windsor JA, Supe AN, Lee S, Chen XP, Yamashita Y, Hirata K, Inui K, Sumiyama Y (2013). “TG13: Updated Tokyo Guidelines for the management of acute cholangitis and cholecystitis”. J Hepatobiliary Pancreat Sci. 20 (1): 1–7. doi:10.1007/s00534-012-0566-y. PMID 23307006.
- ↑ Dinc T, Kayilioglu SI, Coskun F (2017). “Evaluation and Comparison of Charcot’s Triad and Tokyo Guidelines for the Diagnosis of Acute Cholangitis”. Indian J Surg. 79 (5): 427–430. doi:10.1007/s12262-016-1512-z. PMID 29089703.
Pathophysiology
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Amandeep Singh M.D.[2], Farwa Haideri [3]
Overview
Cholangitis involves two main factors: an increased bacterial presence and elevated intraductal pressure in the bile duct, both of which allow for translocation of bacteria or endotoxins in the vascular system. Bacterial contamination alone does not usually result in cholangitis. Increased pressure in the biliary system, from obstruction in the bile duct, widens the spaces between the cells lining the duct, which brings bacterially contaminated bile into the bloodstream.
Pathophysiology
 |
The onset of cholangitis involves two factors: increased bacteria in the bile duct and elevated intraductal pressure in the bile duct that allows translocation of bacteria or endotoxins into the vascular system. Because of its anatomical characteristics, the biliary system is likely to be affected by elevated intraductal pressure. With the elevated intraductal biliary pressure, the bile ductules tend to become more permeable to bacteria and toxins. This can result in serious;even fatal infections, such as hepatic abscesses and sepsis.[2] Functional changes in sinusoidal lining cells are also common.[3][2]
Pathogenesis
Bile, which is produced by the liver, serves to eliminate cholesterol and bilirubin from the body, as well as to emulsify fats to make them more soluble in water and aid in their digestion. It is formed in the liver by hepatocytes and excreted into the common hepatic duct. Some bile is stored in the gallbladder and can be released at time of digestion. All bile reaches the duodenum through the common bile duct and the ampulla of Vater.[4]
The biliary tree is usually relatively free of bacteria because of certain protective mechanisms:
- The sphincter of Oddi acts as a mechanical barrier.
- The biliary system normally has low pressure and allows bile to flow freely through. This flushes bacteria, if present, into the duodenum, and does not allow for the establishment of an infection.[4]
Increased pressure within the biliary system resulting from obstruction in the bile duct widens spaces between the cells lining the duct, bringing bacterially contaminated bile in contact with the bloodstream. Increased biliary pressure decreases production of immunoglobulins (e.g., IgA) in the bile. This results in bacteremia and gives rise to the systemic inflammatory response syndrome (SIRS), which is comprised of fever (often with rigors), tachycardia, increased respiratory rate, and increased white blood cell count.[5][6][2]
Bacterial contamination alone, in absence of obstruction, does not usually result in cholangitis.
Gross Pathology

- On gross pathology following are characteristic findings of cholangitis[8]:
- Thickening of bile ducts
- Bile stasis (cholestasis) as shown by greenish discoloration of parenchyma
- Abscesses or pus in bile duct, as seen in the picture (seen more commonly in acute suppurative cholangits)
- Erosions or ulcers in the bile duct
Microscopic Pathology
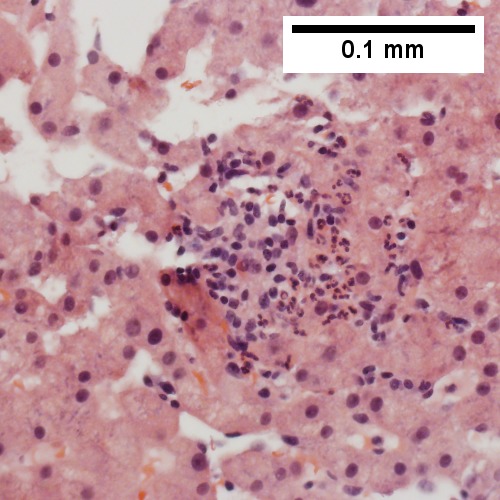
On microscopic histopathological analysis, following features are characteristic findings of acute cholangitis[9]:
- Cholestasis of bile canaliculi and/or ducts with or without neutrophils
- Presence of neutrophils in the ductular walls and lumina.
- Acute cholangitis in a patient with multiple bile duct procedures. After the biopsy, removal of bile duct stones released pus.[10]
-
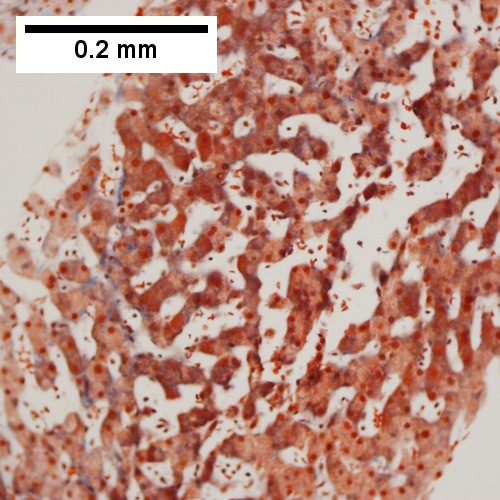
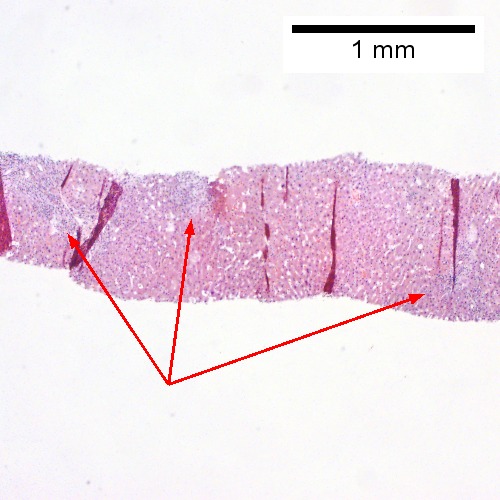 A. Rounded, clear (edematous) portal tracts (arrows) separated by hepatocytes with dilated sinusoids
A. Rounded, clear (edematous) portal tracts (arrows) separated by hepatocytes with dilated sinusoids -
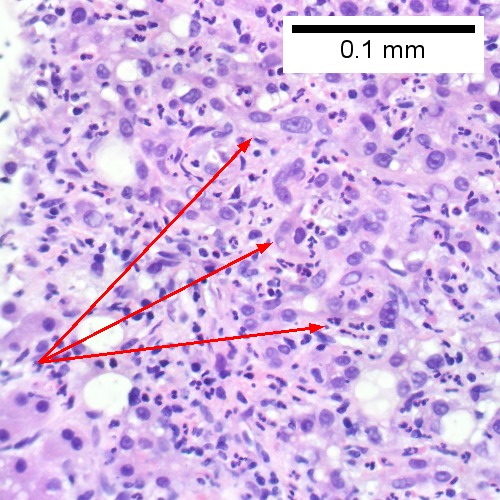
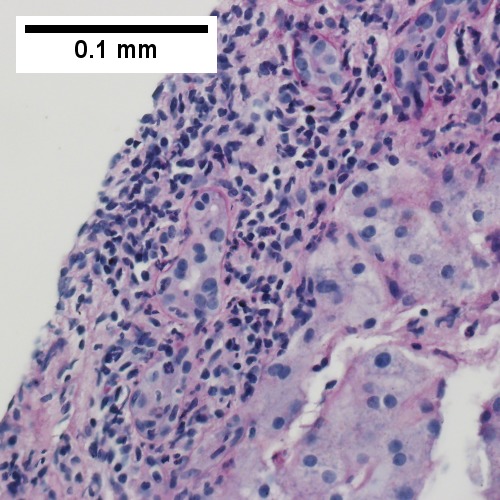
 B. Neutrophils about hepatocytes (arrows) have spilled into the lobule from a portal tract.
B. Neutrophils about hepatocytes (arrows) have spilled into the lobule from a portal tract. -
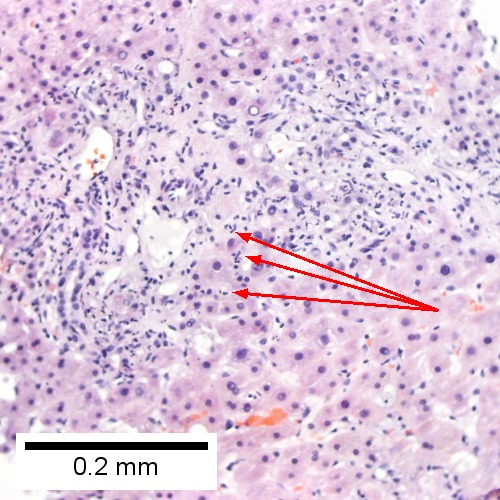
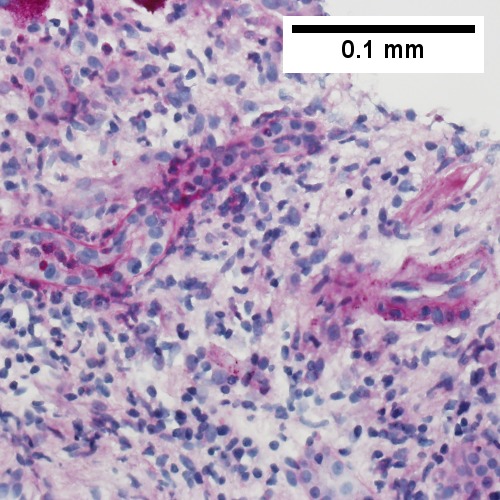
 C, Proliferated bile ductules (arrows) bearing neutrophils within epithelium and lumens are features of obstruction that should prompt a search for interlobular ducts with acute inflammation
C, Proliferated bile ductules (arrows) bearing neutrophils within epithelium and lumens are features of obstruction that should prompt a search for interlobular ducts with acute inflammation -
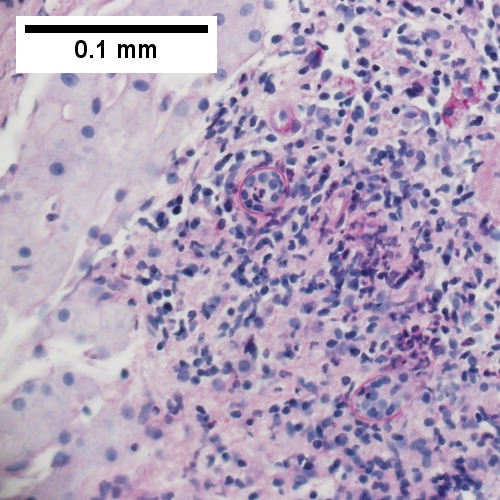
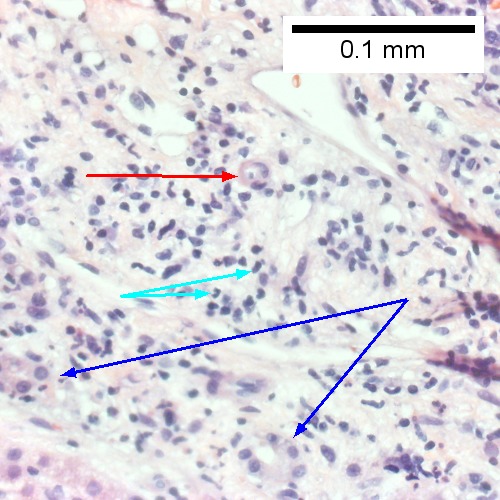 D. The epithelium of the ducts can be severely degenerated. Neutrophils (cyan arrows) invade epithelium of an interlobular duct that are recognizable mainly as a circle of rounded nuclei; the associated arteriole (red arrow) should be identified to ensure an interlobular duct is being evaluated. Note the proliferated bile ductules (blue arrows).
D. The epithelium of the ducts can be severely degenerated. Neutrophils (cyan arrows) invade epithelium of an interlobular duct that are recognizable mainly as a circle of rounded nuclei; the associated arteriole (red arrow) should be identified to ensure an interlobular duct is being evaluated. Note the proliferated bile ductules (blue arrows). -
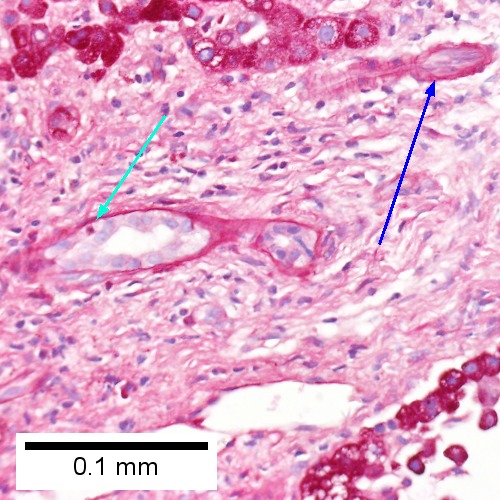 E. A PAS without diastase stain colors the arteriole (blue arrow), as well as the rim of the interlobular duct within which lies a neutrophil (cyan arrow).
E. A PAS without diastase stain colors the arteriole (blue arrow), as well as the rim of the interlobular duct within which lies a neutrophil (cyan arrow). -
 F. A PAS with diastase stain colors the arteriole (red arrow), as well as the rim of the interlobular duct within which lies a neutrophil (cyan arrow).
F. A PAS with diastase stain colors the arteriole (red arrow), as well as the rim of the interlobular duct within which lies a neutrophil (cyan arrow).






- Patient with sepsis and acute cholangitis.[10]
-
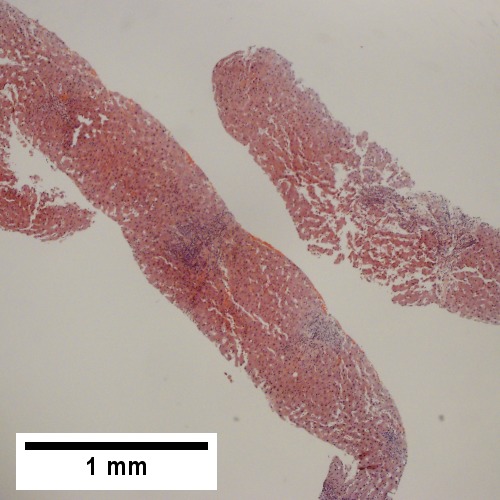 A. Low power shows variably sized inflamed portal tracts.
A. Low power shows variably sized inflamed portal tracts. -
 B. Trichrome shows dilated sinusoids and space of Disse collagenization.
B. Trichrome shows dilated sinusoids and space of Disse collagenization. -
 C. Inflammatory focus with macrophages and neutrophils.
C. Inflammatory focus with macrophages and neutrophils. -
 D. PAS with diastase shows proliferated bile ductules at edge of triad with neutrophils, which should not be used to make a definite diagnosis of acute cholangitis.
D. PAS with diastase shows proliferated bile ductules at edge of triad with neutrophils, which should not be used to make a definite diagnosis of acute cholangitis. -
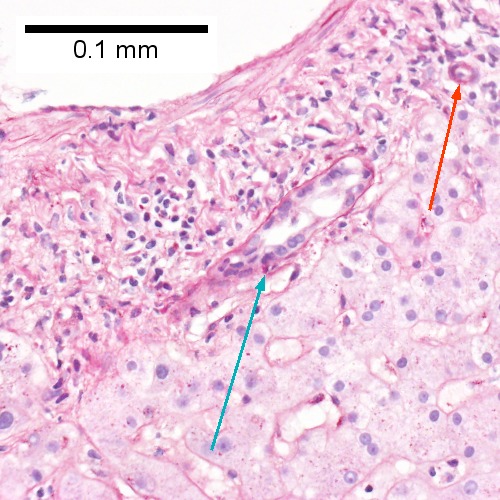
 E. PAS without diastase showing acutely inflamed bile duct, with accompanying blood vessel of similar size, diagnostic of acute cholangitis.
E. PAS without diastase showing acutely inflamed bile duct, with accompanying blood vessel of similar size, diagnostic of acute cholangitis. -
 F. PAS with diastase showing neutrophil in bille duct lumen, diagnostic of acute cholangitis.
F. PAS with diastase showing neutrophil in bille duct lumen, diagnostic of acute cholangitis.






References
- ↑ , CC BY-SA 4.0, https://commons.wikimedia.org/w/index.php?curid=56630024
- ↑ 2.0 2.1 2.2 Kimura Y, Takada T, Kawarada Y, Nimura Y, Hirata K, Sekimoto M, Yoshida M, Mayumi T, Wada K, Miura F, Yasuda H, Yamashita Y, Nagino M, Hirota M, Tanaka A, Tsuyuguchi T, Strasberg SM, Gadacz TR (2007). “Definitions, pathophysiology, and epidemiology of acute cholangitis and cholecystitis: Tokyo Guidelines”. J Hepatobiliary Pancreat Surg. 14 (1): 15–26. doi:10.1007/s00534-006-1152-y. PMC 2784509. PMID 17252293.
- ↑ Kawada, N., Takemura, Y., Minamiyama M. (1996). “Pathophysiology of acute obstructive cholangitis”. Journal of Hepato-Biliary-Pancreatic Surgery. 3 (1): 4–8. doi:10.1007/BF01212771.
- ↑ 4.0 4.1 Kinney TP (2007). “Management of ascending cholangitis”. Gastrointest. Endosc. Clin. N. Am. 17 (2): 289–306, vi. doi:10.1016/j.giec.2007.03.006. PMID 17556149.
- ↑ Sung JY, Costerton JW, Shaffer EA (1992). “Defense system in the biliary tract against bacterial infection”. Dig. Dis. Sci. 37 (5): 689–96. PMID 1563308.
- ↑ Navaneethan U, Jayanthi V, Mohan P (2011). “Pathogenesis of cholangitis in obstructive jaundice-revisited”. Minerva Gastroenterol Dietol. 57 (1): 97–104. PMID 21372774.
- ↑ https://commons.wikimedia.org/wiki/Category:Ascending_cholangitis#/media/File:Cholangitis.jpg
- ↑ Fyfe, Billie (2016). Diagnostic pathology. Philadelphia, PA: Amirsys/Elsevier. ISBN 978-0323376761.
- ↑ Fyfe, Billie (2016). Diagnostic pathology. Philadelphia, PA: Amirsys/Elsevier. ISBN 978-0323376761.
- ↑ 10.0 10.1 “Medical liver disease – Libre Pathology”.
Causes
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Amandeep Singh M.D.[2] Farwa Haideri [3]
Overview
Cholangitis is usually caused by a bacterial infection, which can occur when there is blockage in the bile duct, such as a gallstone or tumor. The infection causing this condition may also spread to the liver.
Causes
Life-threatening causes
Acute suppurative cholangitis is a life-threatening cause of cholangitis.
Common causes
Cholangitis is usually caused by bile stasis. It is the ascending infection of the bile duct by bacteria, and/or parasites.
Cholangitis may be caused by:
- Bile stasis
- Choledocholithiasis/dislodged gallstones (cholelithiasis)
- Biliary strictures
- Bacterial infection
- Malignancy
- Endoscopic retrograde cholangiopancreatography (ERCP)
- Biliary tract surgery with common bile duct implantment[1]e.g. resection of the carcinoma of ampulla of Vater
Less common causes
Less common causes of cholangitis include:
- Parasitic infections:
- Ascaris lumbricoides
- Clonorchis sinensis
- Opisthorchis viverrini
- Ogatpisthorchis felineus
- Taenia saginata
- Malignancy
Causes by organ system
| Cardiovascular | No underlying causes |
| Chemical/Poisoning | No underlying causes |
| Dental | No underlying causes |
| Dermatologic | No underlying causes |
| Drug Side Effect | Cidofovir, Sorafenib, Teduglutide |
| Ear Nose Throat | No underlying causes |
| Endocrine | No underlying causes |
| Environmental | No underlying causes |
| Gastroenterologic | Cholelithiasis, Biliary stricture, Pancreatic cancer, Primary sclerosing cholangitis |
| Genetic | No underlying causes |
| Hematologic | No underlying causes |
| Iatrogenic | Endoscopic retrograde cholangiopancreatography |
| Infectious Disease | Escherichia coli, Klebsiella, Enterococcus, Enterobacter, Bacteroides, Clostridia, Ascaris lumbricoides, Clonorchis sinensis, Opisthorchis viverrini, Opisthorchis felineus, Taenia saginata |
| Musculoskeletal/Orthopedic | No underlying causes |
| Neurologic | No underlying causes |
| Nutritional/Metabolic | No underlying causes |
| Obstetric/Gynecologic | No underlying causes |
| Oncologic | Cancer of the pancreatic head, Cholangiocarcinoma, Lymphoma, Hepatoma, Metastasis to bile duct |
| Ophthalmologic | No underlying causes |
| Overdose/Toxicity | No underlying causes |
| Psychiatric | No underlying causes |
| Pulmonary | No underlying causes |
| Renal/Electrolyte | No underlying causes |
| Rheumatology/Immunology/Allergy | No underlying causes |
| Sexual | No underlying causes |
| Trauma | No underlying causes |
| Urologic | No underlying causes |
| Miscellaneous | No underlying causes |
References
- ↑ https://books.google.com/books?id=Z67nCAAAQBAJ&pg=PA16&lpg=PA16&dq=paralytic+ileus+and+cholangitis&source=bl&ots=EN_c_A_D4F&sig=tzVoAltXsoltCH6_KkdcTi_qaiU&hl=en&sa=X&ved=0ahUKEwiywPaJu4zXAhVp5IMKHWZzB7AQ6AEIRjAG#v=onepage&q=paralytic%20ileus%20and%20cholangitis&f=false. Missing or empty
|title=(help) - ↑ Serradilla Martin, M.; Palomares Cano, A.; Dabán Collado, E.; Medina Cuadros, M. (2016). “Acute cholangitis secondary to main bile duct thrombi for hepatocellular carcinoma”. HPB. 18: e745–e746. doi:10.1016/j.hpb.2016.01.225. ISSN 1365-182X.
Differentiating Cholangitis from other Diseases
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Amandeep Singh M.D.[2] Farwa Haideri [3]
Overview
Cholangitis must be differentiated from other causes of infection in the common bile duct, as well as inflammation and infection of the gall bladder.and mainly from other causes of acute abdomen.
Differentiating Cholangitis from other Diseases
Cholangitis should be differentiated from the following:[1]
- Acute cholecystitis
- Acute hepatitis
- Acute pancreatitis
- Biliary stricture
- Cancer of the common bile duct
- Cholestatic liver disease
- Cirrhosis
- Duodenal ulcer
- Gastic ulcer
- Pancreatic cancer
Differentiating acute cholangitis from other causes of abdominal pain
The differential diagnosis of diseases presenting with abdominal pain, fever and jaundice are discussed below.
Abbreviations: RUQ= Right upper quadrant of the abdomen, LUQ= Left upper quadrant, LLQ= Left lower quadrant, RLQ= Right lower quadrant, LFT= Liver function test, SIRS= Systemic inflammatory response syndrome, ERCP= Endoscopic retrograde cholangiopancreatography, IV= Intravenous, N= Normal, AMA= Anti mitochondrial antibodies, LDH= Lactate dehydrogenase, GI= Gastrointestinal, CXR= Chest X ray, IgA= Immunoglobulin A, IgG= Immunoglobulin G, IgM= Immunoglobulin M, CT= Computed tomography, PMN= Polymorphonuclear cells, ESR= Erythrocyte sedimentation rate, CRP= C-reactive protein, TS= Transferrin saturation, SF= Serum Ferritin, SMA= Superior mesenteric artery, SMV= Superior mesenteric vein, ECG= Electrocardiogram
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
References
- ↑ Miura F, Takada T, Kawarada Y, Nimura Y, Wada K, Hirota M, Nagino M, Tsuyuguchi T, Mayumi T, Yoshida M, Strasberg SM, Pitt HA, Belghiti J, de Santibanes E, Gadacz TR, Gouma DJ, Fan ST, Chen MF, Padbury RT, Bornman PC, Kim SW, Liau KH, Belli G, Dervenis C (2007). “Flowcharts for the diagnosis and treatment of acute cholangitis and cholecystitis: Tokyo Guidelines”. J Hepatobiliary Pancreat Surg. 14 (1): 27–34. doi:10.1007/s00534-006-1153-x. PMC 2784508. PMID 17252294.
Epidemiology and Demographics
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Farwa Haideri [2], Amandeep Singh M.D.[3]
Overview
Cholangitis is most prevalent in adults, with roughly 20% of the population suffering from some form of abdominal pain from gallstones passing through the bile duct into the digestive tract.
Epidemiology and Demographics
Prevalence
- Within a span of ten years, 15–26% of people will suffer at least one episode of biliary colic (abdominal pain due to the passage of gallstones through the bile duct into the digestive tract).[1]
- 2–3% of people will develop complications of obstruction in the form of acute cholangitis.
- The prevalence of gallstones increases with age and body mass index.
- The risk is also increased in those who lose weight rapidly (after bariatric surgery, for example) due to alterations in the composition of the bile that makes it prone to form stones.
Mortality rate
- In 1980, the mortality rate of acute cholangitis was more than 50000 per 100,000 individuals; 10000-30000 per 100,000 individuals in 1981-1991; 2700-10000 per 100,000 individuals after the year 2000.[2][3][4]
Age
Gender
- Gallstones are slightly more common in women than in men, and pregnancy increases the risk further.[1]
- The increased prevalence of gallstones in women is due to hormonal imbalance between estrogen and progesterone.
Race
- There is no racial predilection to cholangitis.
Developed countries
- In Western countries, about 15000 per 100,000 individuals have gallstones in their gallbladder, but the majority are unaware of this and have no symptoms.[1]
- Incidence rates range between 0.41 and 1.2 per 100,000 people per year.[5]
Underdeveloped countries
- Parasites, specifically including the species Ascaris, Opisthorchis, Clonorchis, Fasciola and Echinococcus, are commonly associated with cholangitis outside of the United States.[6]
- Ascaris is thought to be the etiologic agent of recurrent pyogenic cholangitis found in Hong Kong, Southeast Asia, Columbia, Italy, and South Africa.
References
- ↑ 1.0 1.1 1.2 1.3 Bateson MC (1999). “Fortnightly review: gallbladder disease”. BMJ. 318 (7200): 1745–8. PMC 1116086. PMID 10381713.
- ↑ Thompson JE, Pitt HA, Doty JE, Coleman J, Irving C (1990). “Broad spectrum penicillin as an adequate therapy for acute cholangitis”. Surg Gynecol Obstet. 171 (4): 275–82. PMID 2218831.
- ↑ Kimura Y, Takada T, Strasberg SM, Pitt HA, Gouma DJ, Garden OJ; et al. (2013). “TG13 current terminology, etiology, and epidemiology of acute cholangitis and cholecystitis”. J Hepatobiliary Pancreat Sci. 20 (1): 8–23. doi:10.1007/s00534-012-0564-0. PMID 23307004.
- ↑ Salek J, Livote E, Sideridis K, Bank S (2009). “Analysis of risk factors predictive of early mortality and urgent ERCP in acute cholangitis”. J Clin Gastroenterol. 43 (2): 171–5. doi:10.1097/MCG.0b013e318157c62c. PMID 18769362.
- ↑ “The prevalence, incidence and natural history of primary sclerosing cholangitis in an ethnically diverse population | BMC Gastroenterology | Full Text”.
- ↑ “RadioGraphics: Biliary Infections: Spectrum of Imaging Findings and Management”.
Risk Factors
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Amandeep Singh M.D.[2], Farwa Haideri [3]
Overview
The common risk factors in the development of cholangitis are dilatation of common bile duct, CBD stones, gallstones, sclerosing cholangitis, and HIV.
Risk factors
Common risk factors
Common risk factors in the development of cholangitis include:[1][2][3][4]
- Surgery of the biliary tract[5]
- Dilatation of common bile duct (CBD)
- Previous history of gallstones
- Large CBD stones
- A history of sclerosing cholangitis
- Advanced age (>70 years of age)
- Procedure like ERCP[6]
Less common risk factors
Less common risk factors in the development of cholangitis include:[1][2][3][4]
- HIV
- Neurologic disease
- Narrowing of the common bile duct due to cancer
- Traveling to countries where you might catch a worm or parasite infection
- Presence of liver abscess
- Acute renal failure
- Periampullary diverticula
The bile of healthy individuals is generally aseptic.[7]
- Bile culture is positive for microorganisms in:
- 16% of patients undergoing a non-biliary operation
- 72% of acute cholangitis patients
- 44% of chronic cholangitis patients
- 50% of patients with biliary obstruction
- The bacteria in bile are identified in 90% of patients with choledocholithiasis, accompanied by jaundice.
- Patients with incomplete obstruction of the bile duct present with a higher positive bile culture rate than those with complete obstruction of the bile duct.[7]
References
- ↑ 1.0 1.1 Lai EC, Tam PC, Paterson IA, Ng MM, Fan ST, Choi TK, Wong J (1990). “Emergency surgery for severe acute cholangitis. The high-risk patients”. Ann. Surg. 211 (1): 55–9. PMC 1357893. PMID 2294844.
- ↑ 2.0 2.1 Gigot JF, Leese T, Dereme T, Coutinho J, Castaing D, Bismuth H (1989). “Acute cholangitis. Multivariate analysis of risk factors”. Ann. Surg. 209 (4): 435–8. PMC 1493983. PMID 2930289.
- ↑ 3.0 3.1 Catalano, Onofrio A.; Sahani, Dushyant V.; Forcione, David G.; Czermak, Benedikt; Liu, Chang-Hsien; Soricelli, Andrea; Arellano, Ronald S.; Muller, Peter R.; Hahn, Peter F. (2009). “Biliary Infections: Spectrum of Imaging Findings and Management”. RadioGraphics. 29 (7): 2059–2080. doi:10.1148/rg.297095051. ISSN 0271-5333.
- ↑ 4.0 4.1 Yamamoto, Ryuichi; Ishida, Shuko; Osafune, Yasuyo; Takahashi, Masatomo; Harada, Maiko; Kato, Shingo; Nagoshi, Sumiko; Nishikawa, Ko; Yakabi, Koji (2013). “Su1416 Risk Factors for Acute Cholangitis Caused by Common Bile Duct Stone: a Single-Center Study”. Gastrointestinal Endoscopy. 77 (5): AB316–AB317. doi:10.1016/j.gie.2013.03.1069. ISSN 0016-5107.
- ↑ Cybulski Z, Solarski J, Majewski W (1994). “[Infection as a risk factor in biliary system surgery]”. Wiad Lek. 47 (15–16): 619–24. PMID 7716962.
- ↑ Sauter G, Ruckdeschel G, Sauerbruch T (1992). “[Antibiotic prevention and therapy of infectious complications in ERCP]”. Leber Magen Darm. 22 (5): 173–6. PMID 1406012.
- ↑ 7.0 7.1 Kimura Y, Takada T, Kawarada Y, Nimura Y, Hirata K, Sekimoto M, Yoshida M, Mayumi T, Wada K, Miura F, Yasuda H, Yamashita Y, Nagino M, Hirota M, Tanaka A, Tsuyuguchi T, Strasberg SM, Gadacz TR (2007). “Definitions, pathophysiology, and epidemiology of acute cholangitis and cholecystitis: Tokyo Guidelines”. J Hepatobiliary Pancreat Surg. 14 (1): 15–26. doi:10.1007/s00534-006-1152-y. PMC 2784509. PMID 17252293.
Screening
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Farwa Haideri [2]
Overview
There are no accepted screening processes for cholangitis or cholangiocarcinoma, a cancer associated with this disease. Methods do exist to detect the early onset of both diseases.
Screening
The cancer predominantly associated with cholangitis is cholangiocarcinoma. There are no accepted screening programs for either disease. However, methods for detecting early onsets of cholangitis and cholangiocarcinoma include using biochemical markers, scanning using positron emission tomography (PET) scan or magnetic resonance imaging (MRI), and endoscopic procedures such as endosonography and endoscopic retrograde cholangiopancreatography.[1]
References
- ↑ Kitiyakara T, Chapman RW (2008). “Chemoprevention and screening in primary sclerosing cholangitis”. Postgrad Med J. 84 (991): 228–37. doi:10.1136/pgmj.2007.064592. PMID 18508979.
Natural History, Complications and Prognosis
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Amandeep Singh M.D.[2],Farwa Haideri [3]
Overview
Patients who show early signs of multiple organ failure (renal failure, disseminated intravascular coagulation, alterations in the level of consciousness, and shock) or evidence of acute cholangitis, as well as those who do not respond to conservative treatment, should receive systemic antibiotics and undergo emergent biliary drainage. Unless early and appropriate biliary drainage is performed and systemic antibiotics are administered, death will occur. The prognosis is usually good with treatment but poor without treatment.
Natural History
Acute cholangitis is the result of a bacterial infection that causes partial or complete obstruction of the biliary system. Patients with the disease present with a wide range of severity, from low-grade fever to severe sepsis. Patients usually present with Charcot’s triad which comprises of fever, abdominal pain and jaundice. Shock in the presence of pus within the biliary tree is indicative of acute suppurative cholangitis. Patients present with Reynold’s pentad that includes sepsis and mental confusion in addition to fever, abdominal pain and jaundice.[1] A history of biliary disease, such as gallstones, previous biliary procedures, or the placement of a biliary stent are factors that are very helpful in understanding the natural history of cholangitis.[2]
Complications
Complications related to cholangitis include:[3][4][5]
- Renal failure
- Respiratory failure
- The inability of the respiratory system to oxygenate blood and/or eliminate carbon dioxide
- Cardiac arrhythmia
- Wound infection
- Pneumonia
- Gastrointestinal bleeding
- Myocardial ischemia
- Acute cholecystitis
- Jaundice
- Pancreatitis
The risk of developing complications increased in subsequent years after gallbladder stones were first discovered, but have been decreasing since. Every year, 6-8% of patients whose symptoms progress from minor to serious undergo cholecystectomy. Fortunately, this percentage has been decreasing yearly.[4][5]
Prognosis
- Acute cholangitis bears a significant risk of death, with the leading cause being irreversible shock with multiple organ failure (which could have multiple possible complications of severe infections). Modern improvements in diagnosis and treatment have led to a reduction in mortality.
- Before 1980, the mortality rate was greater than 50%; in the past thirty years, it has decreased to 10-30%. [6][7][8] These differences in mortality can likely be attributed to improvements in early diagnosis and supportive treatment.
- Patients with signs of multiple organ failure are likely to die unless they undergo early biliary drainage and treatment with systemic antibiotics. Other causes of death following severe cholangitis include heart failure and pneumonia.[3][4][5]
- Prognosis is good in patients who have quick and adequate drainage where there is improvement in hemodynamic and inflammatory parameters.[9]
- Poor outcomes are seen if urgent surgery is required for drainage.[5][10]
- The prognosis is poor if the following five factors are present:[5][10]
- High fever
- Elderly patient
- Hyperbilirubinemia
- Leukocytosis
- Hypoalbuminemia
References
- ↑ Liu, CL & Fan, ST (2001), Surgical Treatment: Evidence-Based and Problem-Oriented (24 ed.), Munich, Germany: Zuckschwerdt
- ↑ Miura F, Takada T, Kawarada Y, Nimura Y, Wada K, Hirota M, Nagino M, Tsuyuguchi T, Mayumi T, Yoshida M, Strasberg SM, Pitt HA, Belghiti J, de Santibanes E, Gadacz TR, Gouma DJ, Fan ST, Chen MF, Padbury RT, Bornman PC, Kim SW, Liau KH, Belli G, Dervenis C (2007). “Flowcharts for the diagnosis and treatment of acute cholangitis and cholecystitis: Tokyo Guidelines”. J Hepatobiliary Pancreat Surg. 14 (1): 27–34. doi:10.1007/s00534-006-1153-x. PMC 2784508. PMID 17252294.
- ↑ 3.0 3.1 Lai EC, Tam PC, Paterson IA, Ng MM, Fan ST, Choi TK, Wong J (1990). “Emergency surgery for severe acute cholangitis. The high-risk patients”. Ann. Surg. 211 (1): 55–9. PMC 1357893. PMID 2294844.
- ↑ 4.0 4.1 4.2 Kimura Y, Takada T, Kawarada Y, Nimura Y, Hirata K, Sekimoto M, Yoshida M, Mayumi T, Wada K, Miura F, Yasuda H, Yamashita Y, Nagino M, Hirota M, Tanaka A, Tsuyuguchi T, Strasberg SM, Gadacz TR (2007). “Definitions, pathophysiology, and epidemiology of acute cholangitis and cholecystitis: Tokyo Guidelines”. J Hepatobiliary Pancreat Surg. 14 (1): 15–26. doi:10.1007/s00534-006-1152-y. PMC 2784509. PMID 17252293.
- ↑ 5.0 5.1 5.2 5.3 5.4 Kiriyama, Seiki; Takada, Tadahiro; Strasberg, Steven M.; Solomkin, Joseph S.; Mayumi, Toshihiko; Pitt, Henry A.; Gouma, Dirk J.; Garden, O. James; Büchler, Markus W.; Yokoe, Masamichi; Kimura, Yasutoshi; Tsuyuguchi, Toshio; Itoi, Takao; Yoshida, Masahiro; Miura, Fumihiko; Yamashita, Yuichi; Okamoto, Kohji; Gabata, Toshifumi; Hata, Jiro; Higuchi, Ryota; Windsor, John A.; Bornman, Philippus C.; Fan, Sheung-Tat; Singh, Harijt; de Santibanes, Eduardo; Gomi, Harumi; Kusachi, Shinya; Murata, Atsuhiko; Chen, Xiao-Ping; Jagannath, Palepu; Lee, Sung Gyu; Padbury, Robert; Chen, Miin-Fu; Dervenis, Christos; Chan, Angus C.W.; Supe, Avinash N.; Liau, Kui-Hin; Kim, Myung-Hwan; Kim, Sun-Whe (2013). “TG13 guidelines for diagnosis and severity grading of acute cholangitis (with videos)”. Journal of Hepato-Biliary-Pancreatic Sciences. 20 (1): 24–34. doi:10.1007/s00534-012-0561-3. ISSN 1868-6974.
- ↑ Thompson JE, Pitt HA, Doty JE, Coleman J, Irving C (1990). “Broad spectrum penicillin as an adequate therapy for acute cholangitis”. Surg Gynecol Obstet. 171 (4): 275–82. PMID 2218831.
- ↑ Kimura Y, Takada T, Strasberg SM, Pitt HA, Gouma DJ, Garden OJ; et al. (2013). “TG13 current terminology, etiology, and epidemiology of acute cholangitis and cholecystitis”. J Hepatobiliary Pancreat Sci. 20 (1): 8–23. doi:10.1007/s00534-012-0564-0. PMID 23307004.
- ↑ Salek J, Livote E, Sideridis K, Bank S (2009). “Analysis of risk factors predictive of early mortality and urgent ERCP in acute cholangitis”. J Clin Gastroenterol. 43 (2): 171–5. doi:10.1097/MCG.0b013e318157c62c. PMID 18769362.
- ↑ “Ascending cholangitis Prognosis – Epocrates Online”.
- ↑ 10.0 10.1 Tsuyuguchi, Toshio; Sugiyama, Harutoshi; Sakai, Yuji; Nishikawa, Takao; Yokosuka, Osamu; Mayumi, Toshihiko; Kiriyama, Seiki; Yokoe, Masamichi; Takada, Tadahiro (2012). “Prognostic factors of acute cholangitis in cases managed using the Tokyo Guidelines”. Journal of Hepato-Biliary-Pancreatic Sciences. 19 (5): 557–565. doi:10.1007/s00534-012-0538-2. ISSN 1868-6974.
Diagnosis
Diagnosis
History and Symptoms | Physical Examination | Laboratory findings | X Ray | CT | MRI | Ultrasound | Other Imaging Findings | Other Diagnostic Studies
Treatment
Treatment
Medical Therapy | Surgery | Primary Prevention | Cost-Effectiveness of Therapy | Future or Investigational Therapies
Looking for the patient version?
© 2026 MyEClinic – IFTM Institut für Telematik in der Medizin GmbH