
Anaplastic thyroid cancer
For patient information, click here.
To review the wikidoc page on thyroid cancer , click here.
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Ammu Susheela, M.D. [2]
Synonyms and keywords: anaplastic thyroid cancer; Anaplastic thyroid carcinoma; Anaplastic thyroid carcinoma; Anaplastic carcinoma of the thyroid; Anaplastic carcinoma of thyroid gland; Undifferentiated thyroid carcinoma; Sarcomatoid thyroid carcinoma
Overview
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Ammu Susheela, M.D. [2]
Overview
In 1811, the first thyroid cancer case was reported. Thyroid cancer was first described by William Stewart Halsted, an American surgeon in the late nineteenth century. Anaplastic thyroid cancer arises from cells of thyroid, which are normally involved in production and secretion of thyroid hormones, thyroxine (T4) and triiodothyronine (T3) and is always considered as stage IV. Genes involved in the pathogenesis of follicular thyroid cancer include P53 and BRAF. Anaplastic thyroid cancer must be differentiated from other diseases that cause neck masses such as goiter, Grave’s disease, Hurthle cell carcinoma, follicular thyroid cancer, papillary thyroid carcinoma, follicular adenoma, sarcoma, and medullary thyroid carcinoma.[1]. Depending on the extent of the tumor at the time of diagnosis, the prognosis of anaplastic thyroid cancer may vary. However, the prognosis is generally regarded as poor. The presence of metastasis is associated with a particularly poor prognosis among patients with anaplastic thyroid cancer. According to the American Joint Committee on Cancer (AJCC)[2] there are 4 stages of anaplastic thyroid cancer based on the clinical features and findings on imaging. Each stage is assigned a letter and a number that designate the tumor size, number of lymph node regions involved, and metastasis. The hallmark of anaplastic thyroid cancer is swelling in the neck. A positive history of irradiation of head and neck, rapid growth of the nodule, and family history of anaplastic thyroid carcinoma is suggestive of anaplastic thyroid cancer. The most common symptoms of anaplastic thyroid cancer include swelling in the neck, pain in the front of the neck, and hoarseness of voice. Surgery is the mainstay of treatment for anaplastic thyroid cancer.
Historical Perspective
In 1811, the first thyroid cancer case was reported. Thyroid cancer was first described by William Stewart Halsted, an American surgeon in the late nineteenth century.
Pathophysiology
Anaplastic thyroid cancer arises from cells of thyroid, which are secretory cells that are normally involved in production and secretion of thyroid hormones, thyroxine (T4) and triiodothyronine (T3) and is always considered as stage IV. Genes involved in the pathogenesis of follicular thyroid cancer include P53 and BRAF.
Causes
Genetic mutation is suspected to be the main cause of anaplastic thyroid cancer.
Differential Diagnosis
Anaplastic thyroid cancer must be differentiated from other diseases that cause neck masses such as goiter, Grave’s disease, Hurthle cell carcinoma, follicular thyroid cancer, papillary thyroid carcinoma, follicular adenoma, sarcoma, and medullary thyroid carcinoma.[3]
Epidemiology and Demographics
Females are more commonly affected with follicular thyroid cancer than males. The incidence of follicular thyroid cancer increases with age; the median age at diagnosis is 6th to 7th decades.
Risk Factors
Common risk factors in the development of anaplastic thyroid cancer are iodine deficiency, family history of thyroid cancer, and radiation exposure.
Natural history, Complications and Prognosis
Depending on the extent of the tumor at the time of diagnosis, the prognosis of anaplastic thyroid cancer may vary. However, the prognosis is generally regarded as poor. The presence of metastasis is associated with a particularly poor prognosis among patients with anaplastic thyroid cancer.
Staging
According to the American Joint Committee on Cancer (AJCC)[4] there are 4 stages of anaplastic thyroid cancer based on the clinical features and findings on imaging. Each stage is assigned a letter and a number that designate the tumor size, number of lymph node regions involved, and metastasis.
History and Symptoms
The hallmark of anaplastic thyroid cancer is swelling in the neck. A positive history of irradiation of head and neck, rapid growth of the nodule, and family history of anaplastic thyroid carcinoma is suggestive of anaplastic thyroid cancer. The most common symptoms of anaplastic thyroid cancer include swelling in the neck, pain in the front of the neck, and hoarseness of voice.
Physical Examination
Patients with anaplastic thyroid cancer usually appear thin and cachectic. Physical examination of patients with anaplastic thyroid cancer is usually remarkable for thyromegaly, lymphadenopathy and anxiety.
Laboratory Findings
Laboratory findings consistent with the diagnosis of anaplastic thyroid cancer include elevated T3, elevated T4, and decreased thyroid stimulating hormone.
Chest x-ray
Chest x ray may be helpful in the diagnosis of anaplastic thyroid cancer.
CT
CT scan may be helpful in the diagnosis of anaplastic thyroid cancer.
MRI
MRI may be helpful in the diagnosis of anaplastic thyroid cancer. MRI may also be performed to detect metastases of anaplastic thyroid cancer to brain and bones.
Echocardiography or Ultrasound
Neck ultrasound may be performed to detect anaplastic thyroid cancer.
Other Imaging Findings
PET may be helpful in the diagnosis of anaplastic thyroid cancer. PET may also be performed to detect metastases of anaplastic thyroid cancer to brain and bones.[5]
Other Diagnostic Studies
Other diagnostic studies for anaplastic thyroid cancer include laryngoscopy, which demonstrates vocal cord immobility.
Biopsy
On biopsy, anaplastic thyroid cancer is characterized by trabecular or solid follicular tumor cells that invade tumor capsule and surrounding vascular structures.
Medical Therapy
Pharmacologic medical therapies for anaplastic thyroid cancer include radioactive iodine therapy and adjuvant radiotherapy.
Surgery
Surgery is the mainstay of treatment for anaplastic thyroid cancer.
Prevention
Effective measures for the prevention of anaplastic thyroid cancer include avoidance of diets low in iodine and avoidance of ultraviolet exposure.
Reference
- ↑ Thyroid Cancer Cancer.gov (2015). http://www.cancer.gov/types/thyroid/hp/thyroid-treatment-pdq#section/_6- Accessed on October, 29 2015
- ↑ Stage Information for Thyroid Cancer Cancer.gov (2015). http://www.cancer.gov/types/thyroid/hp/thyroid-treatment-pdq#link/stoc_h2_2- Accessed on October, 29 2015
- ↑ Thyroid Cancer Cancer.gov (2015). http://www.cancer.gov/types/thyroid/hp/thyroid-treatment-pdq#section/_6- Accessed on October, 29 2015
- ↑ Stage Information for Thyroid Cancer Cancer.gov (2015). http://www.cancer.gov/types/thyroid/hp/thyroid-treatment-pdq#link/stoc_h2_2- Accessed on October, 29 2015
- ↑ Thyroid Cancer Canadian Cancer Society (2015). http://www.cancer.ca/en/cancer-information/cancer-type/thyroid/diagnosis/?region=sk- Accessed on November, 19 2015
Historical Perspective
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Ammu Susheela, M.D. [2]
Overview
In 1811, the first thyroid cancer case was reported. Thyroid cancer was first described by William Stewart Halsted, an American surgeon in the late nineteenth century.
Historical Perspective
Discovery
- The first case of thyroid cancer was described by William Stewart Halsted.[1]
- In 1951, head and neck irradiation was demonstrated to cause thyroid cancer in children.
Landmark Events in the Development of Treatment Strategies
- In 1884, thyroidectomies were introduced to successfully treat thyroid disorders.
- Theodore Kocher (1841-1917) was considered an expert in thyroidectomy in Switzerland.
- Charles Horace Mayo was considered as an expert in thyroidectomies in United States.
- Murray discovered that patients with hypothyroidism respond well to injecting thyroid extracts to them.
Famous Cases
- William Rehnquist, Chief Justice of the United States (1986-2005) passed away on September 3, 2005 from anaplastic thyroid cancer.
Reference
Pathophysiology
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Ammu Susheela, M.D. [2]
Overview
Anaplastic thyroid cancer arises from cells of the thyroid, which are normally involved in production and secretion of thyroid hormones, thyroxine (T4) and triiodothyronine (T3). Anaplastic thyroid tumor is always considered as stage IV. Genes involved in the pathogenesis of follicular thyroid cancer include P53 and BRAF.
Pathogenesis
- Anaplastic tumors have a high mitotic rate and lymphovascular invasion. It rapidly invades surrounding tissues (such as the trachea).
- Most patients with anaplastic thyroid cancer have distant metastasis at the time of diagnosis because of the rapid growth and aggressive nature of this type of cancer.
- Common sites of metastasis include the lungs, pleura, bones, and brain.
Genetics
Associated Conditions
- Anaplastic thyroid cancer may be associated with the following conditions:
Gross Pathology
- Macroscopic features of anaplastic thyroid cancer include:
- Unencapsulated, fleshy, tan-white tumor
- Soft-tissue infiltration of the neck
Microscopic Pathology
- Three types of histologic variety will be expected in anaplastic thyroid cancer:
- Spindle cell
- Giant cell
- Squamoid cell
- Features include:
- Cytologically malignant:
- Huge nuclear-cytoplasmic ratio
- Mitoses
- Presence or absence of necrosis
Immunohistochemistry
- Anaplastic thyroid cancer may be positive for the following markers:
- Pankeratin (AE1/AE3)
- High molecular weight keratins
- TTF-1
- PAX8
- P53
- B-catenin
-
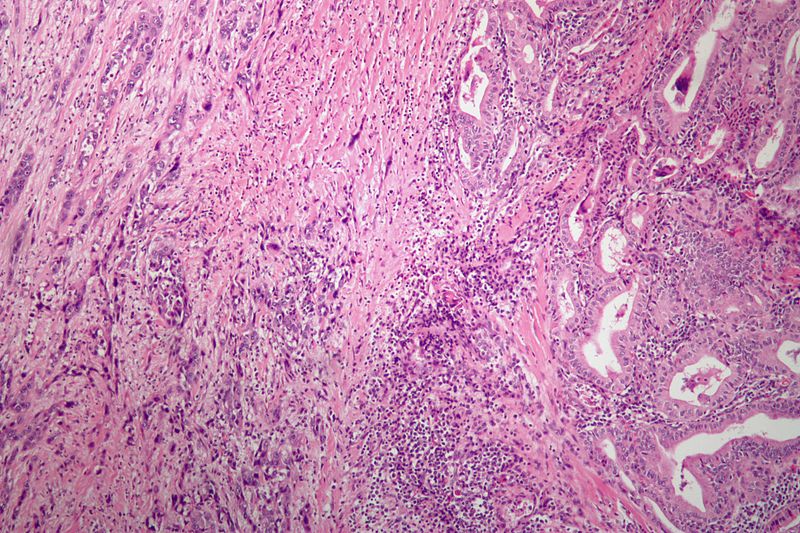 Anaplastic thyroid carcinoma with a component of PTC. (WC)
Anaplastic thyroid carcinoma with a component of PTC. (WC)
References
- ↑ Patel KN, Shaha AR (2006). “Poorly differentiated and anaplastic thyroid cancer”. Cancer Control. 13 (2): 119–28. PMID 16735986.
- ↑ Quiros RM, Ding HG, Gattuso P, Prinz RA, Xu X (June 2005). “Evidence that one subset of anaplastic thyroid carcinomas are derived from papillary carcinomas due to BRAF and p53 mutations”. Cancer. 103 (11): 2261–8. doi:10.1002/cncr.21073. PMID 15880523.
Causes
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Ammu Susheela, M.D. [2]
Overview
- Genetic mutation is suspected to be the main cause of anaplastic thyroid cancer. Genes involved in the pathogenesis of follicular thyroid cancer include P53 and BRAF.
Causes
Common Causes
- Genetic mutations are suspected to be the main cause of anaplastic thyroid cancer. Genes involved in the pathogenesis of follicular thyroid cancer include P53 and BRAF.[1]
References
- ↑ Patel KN, Shaha AR (2006). “Poorly differentiated and anaplastic thyroid cancer”. Cancer Control. 13 (2): 119–28. PMID 16735986.
Differentiating Anaplastic thyroid cancer from other Diseases
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Ammu Susheela, M.D. [2]
Overview
Anaplastic thyroid cancer must be differentiated from other diseases that cause neck masses such as goiter, Grave’s disease, Hurthle cell carcinoma, follicular thyroid cancer, papillary thyroid carcinoma, follicular adenoma, sarcoma, and medullary thyroid carcinoma.[1]
Differentiating Follicular thyroid cancer from other Diseases
Thyroid cancers should be differentiated from one another and from various other diseases:
| Disease Name | Age of Onset | Gender Preponderance | Signs/Symptoms | Imaging Feature(s) | Macroscopic Feature(s) | Microscopic Feature(s) | Laboratory Findings(s) | Other Feature(s) | Microscopic Appearance |
|---|---|---|---|---|---|---|---|---|---|
| Anaplastic Thyroid Cancer[2][3][4] |
|
|
|
|
|
|
 | ||
| Papillary Thyroid Cancer[5][6][7] |
|
|
|
|
|
|
|
 | |
| Follicular Thyroid Cancer[6][7][8] |
|
|
|
|
|
|
|
|
 |
| Medullary Thyroid Cancer[9][10][11][7] |
|
|
|
|
|
|
|
 | |
| Follicular Adenoma[12] |
|
|
|
|
|
|
 | ||
| Multinodular Goiter[13] |
|
|
|
|
|
|
|
 | |
| Thyroid Lymphoma[14] |
|
|
|
|
|
|
|
|
 |
Reference
- ↑ Thyroid Cancer Cancer.gov (2015). http://www.cancer.gov/types/thyroid/hp/thyroid-treatment-pdq#section/_6- Accessed on October, 29 2015
- ↑ Nagaiah G, Hossain A, Mooney CJ, Parmentier J, Remick SC (2011). “Anaplastic thyroid cancer: a review of epidemiology, pathogenesis, and treatment”. J Oncol. 2011: 542358. doi:10.1155/2011/542358. PMC 3136148. PMID 21772843.
- ↑ Chang TC, Liaw KY, Kuo SH, Chang CC, Chen FW (June 1989). “Anaplastic thyroid carcinoma: review of 24 cases, with emphasis on cytodiagnosis and leukocytosis”. Taiwan Yi Xue Hui Za Zhi. 88 (6): 551–6. PMID 2794956.
- ↑ Venkatesh YS, Ordonez NG, Schultz PN, Hickey RC, Goepfert H, Samaan NA (July 1990). “Anaplastic carcinoma of the thyroid. A clinicopathologic study of 121 cases”. Cancer. 66 (2): 321–30. doi:10.1002/1097-0142(19900715)66:2<321::aid-cncr2820660221>3.0.co;2-a. PMID 1695118.
- ↑ Fagin, James A.; Mitsiades, Nicholas (2008). “Molecular pathology of thyroid cancer: diagnostic and clinical implications”. Best Practice & Research Clinical Endocrinology & Metabolism. 22 (6): 955–969. doi:10.1016/j.beem.2008.09.017. ISSN 1521-690X.
- ↑ 6.0 6.1 Schlumberger, Martin Jean (1998). “Papillary and Follicular Thyroid Carcinoma”. New England Journal of Medicine. 338 (5): 297–306. doi:10.1056/NEJM199801293380506. ISSN 0028-4793.
- ↑ 7.0 7.1 7.2 Sipos JA (December 2009). “Advances in ultrasound for the diagnosis and management of thyroid cancer”. Thyroid. 19 (12): 1363–72. doi:10.1089/thy.2009.1608. PMID 20001718.
- ↑ Pettersson B, Adami HO, Wilander E, Coleman MP (April 1991). “Trends in thyroid cancer incidence in Sweden, 1958-1981, by histopathologic type”. Int. J. Cancer. 48 (1): 28–33. doi:10.1002/ijc.2910480106. PMID 2019455.
- ↑ Busnardo B, Girelli ME, Simioni N, Nacamulli D, Busetto E (January 1984). “Nonparallel patterns of calcitonin and carcinoembryonic antigen levels in the follow-up of medullary thyroid carcinoma”. Cancer. 53 (2): 278–85. doi:10.1002/1097-0142(19840115)53:2<278::aid-cncr2820530216>3.0.co;2-z. PMID 6690009.
- ↑ Kebebew E, Ituarte PH, Siperstein AE, Duh QY, Clark OH (March 2000). “Medullary thyroid carcinoma: clinical characteristics, treatment, prognostic factors, and a comparison of staging systems”. Cancer. 88 (5): 1139–48. doi:10.1002/(sici)1097-0142(20000301)88:5<1139::aid-cncr26>3.0.co;2-z. PMID 10699905.
- ↑ Hofstra, Robert M. W.; Landsvater, Rudy M.; Ceccherini, Isabella; Stulp, Rein P.; Stelwagen, Tineke; Luo, Yin; Pasini, Barbara; Hoppener, Jo W. M.; van Amstel, Hans Kristian Ploos; Romeo, Giovanni; Lips, Cornells J. M.; Buys, Charles H. C. M. (1994). “A mutation in the RET proto-oncogene associated with multiple endocrine neoplasia type 2B and sporadic medullary thyroid carcinoma”. Nature. 367 (6461): 375–376. doi:10.1038/367375a0. ISSN 0028-0836.
- ↑ Mathur, Aarti; Olson, Matthew T.; Zeiger, Martha A. (2014). “Follicular Lesions of the Thyroid”. Surgical Clinics of North America. 94 (3): 499–513. doi:10.1016/j.suc.2014.02.005. ISSN 0039-6109.
- ↑ Bronshteĭn ME, Makarov AD, Artemova AM, Bazarova EN, Kozlov GI (1994). “[Morphology of the thyroid tissue in multinodular euthyroid goiter]”. Probl Endokrinol (Mosk) (in Russian). 40 (2): 36–9. PMID 8197088.
- ↑ Pedersen RK, Pedersen NT (January 1996). “Primary non-Hodgkin’s lymphoma of the thyroid gland: a population based study”. Histopathology. 28 (1): 25–32. PMID 8838117.
- ↑ Hyjek E, Isaacson PG (November 1988). “Primary B cell lymphoma of the thyroid and its relationship to Hashimoto’s thyroiditis”. Hum. Pathol. 19 (11): 1315–26. doi:10.1016/s0046-8177(88)80287-9. PMID 3141260.
- ↑ Tupchong L, Hughes F, Harmer CL (October 1986). “Primary lymphoma of the thyroid: clinical features, prognostic factors, and results of treatment”. Int. J. Radiat. Oncol. Biol. Phys. 12 (10): 1813–21. doi:10.1016/0360-3016(86)90324-x. PMID 3759532.
- ↑ Ota H, Ito Y, Matsuzuka F, Kuma S, Fukata S, Morita S, Kobayashi K, Nakamura Y, Kakudo K, Amino N, Miyauchi A (October 2006). “Usefulness of ultrasonography for diagnosis of malignant lymphoma of the thyroid”. Thyroid. 16 (10): 983–7. doi:10.1089/thy.2006.16.983. PMID 17042683.
Epidemiology and Demographics
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Ammu Susheela, M.D. [2]
Overview
The incidence of follicular thyroid cancer increases with age; the median age at diagnosis is 6th to 7th decades. Females are more commonly affected with anaplastic thyroid cancer than males.
Epidemiology and Demographics
Incidence
- The incidence of anaplastic thyroid cancer is approximately 1.2-3.8 per 100,000 individuals world wide.
- The incidence of anaplastic thyroid cancer is approximately .01 per 100,000 individuals in United States.
Age
- Anaplastic thyroid cancer typically occurs in the elderly (peak incidence in 6th to 7th decades).[1]
- The incidence of anaplastic thyroid cancer increases with age; the median age at diagnosis is 65 years.
Gender
- Females are more affected with anaplastic thyroid cancer than males.
- The female to male ratio is approximately 1.5 to 1.[2]
References
- ↑ Accessed on November, 18 2015 “Anaplastic thyroid carcinoma[Dr Matt A. Morgan and Dr Yuranga Weerakkody].Radiopedia 2015” Check
|url=value (help). - ↑ Nagaiah, Govardhanan; Hossain, Akm; Mooney, Colin J.; Parmentier, James; Remick, Scot C. (2011). “Anaplastic Thyroid Cancer: A Review of Epidemiology, Pathogenesis, and Treatment”. Journal of Oncology. 2011: 1–13. doi:10.1155/2011/542358. ISSN 1687-8450.
Risk Factors
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Ammu Susheela, M.D. [2]
Overview
Common risk factors in the development of anaplastic thyroid cancer are iodine deficiency, family history of thyroid cancer, and radiation exposure.
Risk Factors
- Patients with a history of radiation administered in infancy and childhood for benign conditions of the head and neck, such as enlarged thymus, acne, or tonsillar or adenoidal enlargement, have an increased risk of cancer as well as other abnormalities of the thyroid gland. Radiation exposure as a consequence of nuclear fallout has also been associated with a high risk of thyroid cancer, especially in children.
- Other risk factors for the development of thyroid cancer include the following:
References
- ↑ Thyroid Cancer Cancer.gov(2015). http://www.cancer.gov/types/thyroid/hp/thyroid-treatment-pdq#section/_6- Accessed on October, 29 2015
Natural History, Complications, and Prognosis
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Ammu Susheela, M.D. [2]
Overview
Depending on the extent of the tumor at the time of diagnosis, the prognosis of anaplastic thyroid cancer may vary. However, the prognosis is generally regarded as poor. The presence of metastasis is associated with a particularly poor prognosis among patients with anaplastic thyroid cancer.
Natural History
Anaplastic thyroid cancer is very aggressive and can invade directly into adjacent organs, such as the trachea, larynx, esophagus, blood vessel and muscle, resulting in suffocation, vocal cord paralysis, dyspnea or dysphagia. Most patients die a few months after diagnosis because of uncontrolled neck mass and metastases, and long-term survivors are rare.[1]
Complications
- Common complications of anaplastic thyroid cancer are:
Prognosis
- The overall 5-year survival rate of anaplastic thyroid cancer has been given as 7%[2] or 14%,[3] although the latter has been criticized as being overestimated. Death is attributable to upper airway obstruction and suffocation in half of patients, and to a combination of complications from either local and distant disease or therapy, or both in the remainder.[4]
- Anaplastic thyroid cancer is extremely aggressive; in most cases death occurs in less than 1 year as a result of aggressive local growth and compromise of vital structures in the neck. Anaplastic thyroid cancer in most series has a median survival of 4 to 5 months from the time of diagnosis, with rare long-term survivors.[5]
References
- ↑ He, Xiayun; Li, Duanshu; Hu, Chaosu; Wang, Zhuoying; Ying, Hongmei; Wu, Yi (2014). “Outcome after intensity modulated radiotherapy for anaplastic thyroid carcinoma”. BMC Cancer. 14 (1): 235. doi:10.1186/1471-2407-14-235. ISSN 1471-2407.
- ↑ cancer.org > Thyroid Cancer By the American Cancer Society. In turn citing: AJCC Cancer Staging Manual (7th ed).
- ↑ Numbers from National Cancer Database in the US, from Page 10 in: F. Grünwald; Biersack, H. J.; Grںunwald, F. (2005). Thyroid cancer. Berlin: Springer. ISBN 3-540-22309-6. (Note:Book also states that the 14% 10-year survival for anaplastic thyroid cancer was overestimated)
- ↑ Anaplastic thyroid cancer Wikipedia (2015). https://en.wikipedia.org/wiki/Anaplastic_thyroid_cancer- Accessed on November, 19 2015
- ↑ Kumar V, Abbas AK, Fausto N, and Mitchel RN, “Robbins basic Pathology”, Saunders, 8th ed., 2007.
Diagnosis
Diagnosis
Staging | History and Symptoms | Physical Examination | Laboratory Findings | Chest X Ray | CT | MRI | Other Imaging Findings | Other Diagnostic Studies | Biopsy
Treatment
Treatment
Medical Therapy | Surgery | Prevention | Cost-Effectiveness of Therapy | Future or Investigational Therapies
Looking for the patient version?
© 2026 MyEClinic – IFTM Institut für Telematik in der Medizin GmbH