
Aortic stenosis
For patient information, click here
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-In-Chief: Cafer Zorkun, M.D., Ph.D. [2]; Mohammed A. Sbeih, M.D. [3]; Lakshmi Gopalakrishnan, M.B.B.S. [4]; Rim Halaby, M.D. [5]; Usama Talib, BSc, MD [6]; Seyedmahdi Pahlavani, M.D. [7]; Arzu Kalayci, M.D. [8]; Mandana Chitsazan, M.D. [9]
Synonyms and keywords: AS; critical AS; tight AS; aortic valve stenosis; calcific aortic stenosis; senile calcific aortic stenosis; degenerative calcific aortic stenosis
Overview
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-In-Chief: Mohammed A. Sbeih, M.D. [2]; Lakshmi Gopalakrishnan, M.B.B.S. [3]; Usama Talib, BSc, MD [4] Assistant Editor-In-Chief: Kristin Feeney, B.S. [5]
Overview
The aortic valve ensures that the blood moves forward from the left ventricle into the aorta and that it does not leak backwards during diastole. When functioning appropriately, the aortic valve does not impede the flow of blood between the left ventricle and the aorta and it does not leak. Under some circumstances, the aortic valve becomes narrower than normal impeding the flow of blood. This is known as aortic valve stenosis, or aortic stenosis, often abbreviated as AS.
Classification
Aortic stenosis can be classified broadly into four main categories:
ACC/AHA staging system (Stages A-D)
Stage A = at risk;
Stage B = progressive (mild-moderate);
Stage C = asymptomatic severe (C1 = normal LVEF, C2 = LVEF <50%);
Stage D = symptomatic severe (D1 = high-gradient, D2 = low-flow low-gradient with reduced LVEF, D3 = paradoxical low-flow low-gradient with normal LVEF). [1][2]
Pathophysiology
Aortic stenosis is the progressive narrowing of the aortic valve. aortic sclerosis (leaflet thickening without obstruction) is the earliest pathological stage, affecting approximately 25% of people over 65, with an approximately 2% annual rate of progression to AS[3]. While early disease shares features with atherosclerosis (lipid infiltration, inflammation), the current understanding is that disease initiation and disease progression are distinct processes. Progression is primarily driven by fibrosis, calcification, and biomineralization rather than a purely atherosclerotic process. This distinction is clinically important because it explains why statins failed to slow AS progression [4]. In contrast, rheumatic aortic stenosis is due to fusion of the commissures with valvular scarring and calcification.[5] Aortic stenosis causes an impedance to the antegrade blood flow not only at the level of the aortic valve itself, but also at the subvalvular (below the aortic valve) or supravalvular (above the aortic valve) levels. As a result, chronic pressure overload develops in the left ventricle. The left ventricle undergoes hypertrophy as an initial adaptive mechanism to overcome the increased afterload. This compensatory mechanism ends up being maladaptive by causing apoptosis of the hypertrophied myocytes and subsequent heart failure. [6] Hence, aortic stenosis is a progressive valvular disease which progression depends mainly on the degree of the narrowing of the aortic valve as well as on the maladaptive ventricular wall response.[7]
Causes
The frequency of causes of aortic stenosis varies with the age of the patient. calcific degeneration of a trileaflet valve is the most common cause of stenosis overall, and bicuspid aortic valve (present in 1-2% of the population) is the most common congenital predisposition. [3]
Differentiating Aortic Stenosis from other Disorders
Aortic stenosis must be differentiated from other cardiac or pulmonary causes of dyspnea, weakness, and dizziness. Furthermore, if there is left ventricular outflow tract obstruction, it is critical to identify whether the obstruction is subvalvular, valvular or supravalvular or due to hypertrophic cardiomyopathy (HOCM).
Epidemiology and Demographics
Aortic stenosis primarily affects older adults and the majority of cases are due to calcific degeneration. AS affects 1% to 2% of persons aged 65 years or older and approximately 12% of those older than 75 years. Calcific AS affects approximately 12.6 million people globally and accounts for more than 100,000 deaths annually.[2] AS is the most common valvular heart disease in high-income countries, and its global prevalence increased 124% between 1990 and 2017. [8]
Risk Factors
The most common risk factor for the subsequent development of aortic stenosis is congenital bicuspid aortic valve. Rheumatic fever is another risk factor for the subsequent development of aortic stenosis (rheumatic heart disease). Risk factors that may speed up the progression of degenerative calcific aortic stenosis include: hypertension, diabetes mellitus, hyperlipoproteinemia, uremia and smoking.
Elevated lipoprotein(a) [Lp(a)] a recognized risk factor for both the development and progression of AS. Mendelian randomization studies and meta-analyses have established Lp(a) as a causal, genetically determined risk factor for calcific aortic valve disease. Patients in the highest Lp(a) tertile demonstrate 41% faster hemodynamic progression of AS. The 2022 European Atherosclerosis Society consensus statement identifies Lp(a) as causally associated with both aortic valve microcalcification and macrocalcification.[4][5][6][7]
Chronic kidney disease/end-stage renal disease is also a significant risk factor, as recognized by the AHA scientific statement on AS in CKD.[9]
Male sex and older age (≥65 years) are independent risk factors. [2]
Natural History, Complications and Prognosis
Left untreated, aortic valve stenosis can lead to angina, syncope, congestive heart failure, atrial fibrillation, endocarditis, and sudden cardiac death. Surgical treatment of aortic stenosis also carries risks and potential complications that include vascular complications and mitral valve injury.
Diagnosis
History and Symptoms
The main symptoms of aortic stenosis include angina, syncope and congestive heart failure. The current literature emphasizes that symptomatic severe AS is associated with an annual mortality rate as high as 50% if not treated with valve replacement, and the 1-year mortality was 50.7% with standard medical care in the PARTNER trial[2]. Other symptoms include dyspnea on exertion, orthopnea and paroxysmal nocturnal dyspnea.
Physical Examination
Aortic stenosis is most often diagnosed when it is asymptomatic and can sometimes be detected during routine examination of the heart and circulatory system. The major signs include pulsus parvus et tardus (a slow-rising, small volume carotid pulse), a lag time between apical and carotid impulses, and a distinct systolic ejection murmur.
Electrocardiogram
The electrocardiogram in the patient with moderate to severe aortic stenosis may reveal left ventricular hypertrophy and heart block.
Cardiac Stress Test
Exercise testing should not be performed in symptomatic patients with severe AS (Stage D1, aortic velocity ≥4.0 m/s or mean gradient ≥40 mm Hg) because of the risk of severe hemodynamic compromise (Class III: Harm). However, in asymptomatic patients with severe AS (Stage C1), exercise testing is reasonable (Class IIa) to assess physiological changes and confirm the absence of symptoms.[1]
Chest X-ray
Chest X-ray may be used as a diagnostic tool in the evaluation of aortic stenosis. Findings associated with aortic stenosis include left ventricular hypertrophy and calcification of the aortic valve.
CT Scan
CT Aortic Valve Calcium Scoring
Noncontrast CT aortic valve calcium scoring is now recommended by both ACC/AHA and ESC/EACTS guidelines as a key adjunctive tool to adjudicate AS severity, particularly in patients with discordant echocardiographic findings (e.g., low-flow, low-gradient AS). Sex-specific calcium score thresholds have been established: ≥2,065 Agatston units (AU) in men and ≥1,274 AU in women indicate severe AS. CT calcium scoring is also recommended in paradoxical low-flow low-gradient AS with preserved LVEF.[10]
MRI
Cardiac MRI (CMR) has an expanding role in AS evaluation, particularly for: Myocardial fibrosis assessment via late gadolinium enhancement (LGE) and T1 mapping/extracellular volume (ECV) quantification. LGE-detected midwall fibrosis is independently associated with a 2.14-fold increased risk of all-cause mortality in AS patients.[11]
The EVOLVED trial (2025) randomized asymptomatic patients with severe AS and midwall LGE to early intervention vs. conservative management, establishing CMR-detected fibrosis as a biomarker for risk stratification.[12]
CMR is the reference standard for LV mass and volume assessment and can detect subclinical myocardial damage before LVEF declines.[13]
Echocardiography
Echocardiography is the best non-invasive test to evaluate the aortic valve anatomy and function. TTE is indicated in patients with signs or symptoms of AS or a bicuspid aortic valve for accurate diagnosis (Class I) [1]. Doppler echocardiography allows the measurement of the maximum jet velocity and can be used to estimate the effective orifice area of the aortic valve as well as the gradient across the aortic valve using the modified Bernoulli equation (gradient = 4 x velocity2). The flow must be constant, so as the velocity increases, the valve area decreases proportionally. severe AS is defined by aortic Vmax ≥4 m/s or mean gradient ≥40 mm Hg, with AVA typically ≤1.0 cm² (or indexed AVA ≤0.6 cm²/m²), but a high velocity or high gradient alone meets the definition of severe AS — AVA is not required [1]. Moreover , the role of global longitudinal strain (GLS) by speckle tracking echocardiography as a more sensitive indicator of subclinical myocardial dysfunction than LVEF, with prognostic value in asymptomatic severe AS[14]
Attention to technical details is important as they may lead to underestimation of the severity of the aortic stenosis.[5] Echocardiography can also be used to assess the severity of left ventricular hypertrophy.
Cardiac Catheterization
Left and right heart catheterization as well as angiography may be useful in the assessment of the patient prior to aortic valve replacement surgery. invasive hemodynamic assessment is one option but is no longer the primary recommended approach for discordant findings. CT calcium scoring and dobutamine stress echocardiography are now the preferred noninvasive methods for adjudicating severity in discordant cases. Cardiac catheterization is primarily performed for coronary angiography prior to planned valve intervention, not routinely for hemodynamic assessment of AS severity[1]
Aortic Valve Area
The aortic valve area is the size of the orifice for blood to flow from the left ventricle to the aorta. The aortic valve area is reduced in aortic stenosis, and the aortic valve area is the metric that is used to gauge the need for aortic valve replacement surgery. The pressure gradient across a narrowed aortic valve cannot be used to gauge the need for valve replacement as the gradient may be low in patients with impaired left ventricular function.
Aortic Valve Area Calculation
The calculation of the aortic valve area is an indirect method used to determine the area of the aortic valve. The calculated aortic valve orifice area is currently one of the measures for evaluating the severity of aortic stenosis. An aortic valve having an area ≤1.0 cm² (or indexed AVA ≤0.6 cm²/m²) considered to be severe aortic stenosis.[1]
There are many ways to calculate the aortic valve area. The most commonly used methods involve measurements taken during echocardiography. For interpretation of these values, the aortic valve area is generally divided by the body surface area.
Treatment
General Approach
Choice of SAVR vs. TAVR
AVR (either SAVR or TAVR) is recommended for symptomatic severe AS. The choice between SAVR and TAVR should be made by a multidisciplinary heart valve team based on age, surgical risk, anatomy, comorbidities, and patient preference — not simply based on whether the patient “can tolerate surgery[2][15]. If severe left ventricular dysfunction is present in the setting of aortic stenosis, it is of utmost importance to differentiate between true severe aortic stenosis and pseudo-severe aortic stenosis as these two entities have different pathophysiologies and different outcomes after aortic valve replacement. Medical therapy reduces symptoms but does not prolong life. TAVR is a Class I recommendation for patients ≥80 years or with life expectancy <10 years, and either SAVR or TAVR is Class I for patients aged 65-80 years. SAVR is preferred for patients <65 years with life expectancy >20 years[2][10]. Aortic valvuloplasty can be considered in those patients who are too sick for surgery or transcatheter aortic valve implantation.The section should mention the concept of shared decision-making (Class I, ACC/AHA) in choosing between SAVR and TAVR, considering expected patient longevity vs. valve durability.[10]
Discussion of early intervention in asymptomatic severe AS:
For asymptomatic severe AS, current guidelines now recognize several Class I and IIa indications for AVR even without symptoms: LVEF <50%, symptoms on exercise testing, very severe AS (Vmax ≥5 m/s), BNP >3× normal, and rapid progression (≥0.3 m/s/year). The RECOVERY trial (10-year follow-up, 2026) and AVATAR trial demonstrated survival benefit with early surgery in asymptomatic very severe AS.[1][2][10][16]
Medical Therapy
While medical therapy may improve the symptoms of patients with aortic stenosis, medical therapy does not prolong life expectancy. Aortic valve replacement remains the definitive treatment for symptomatic aortic stenosis and it improves both the symptoms and life expectancy of the patients. When pharmacological therapies are used, extreme caution must be taken in the administration of vasodilators as an excess in vasodilation may lead to hypotension, a reduction in perfusion pressure to the heart, a further decline in cardiac output and further hypotension. This vicious circle can be fatal and must be avoided at all costs.
The 2020 ACC/AHA guidelines give a Class IIb recommendation for renin-angiotensin-aldosterone system (RAAS) blockade in patients undergoing TAVR, based on observational data showing lower 1-year mortality.[1]
Surgery
Surgical intervention may be a necessary component of treatment for symptomatic severe aortic stenosis. Aortic valve replacement is the mainstay of treatment of symptomatic aortic stenosis, as it improves both the symptoms and life expectancy in aortic stenosis patients, in contrast to medical therapy alone which may improve the symptoms without prolonging life expectancy.[12]
Percutaneous Aortic Balloon Valvotomy (PABV) or Aortic Valvuloplasty
Surgical aortic valve replacement is the mainstay of the treatment of aortic stenosis as it improves both symptoms and life expectancy. However, some patients may not be surgical candidates due to coexisting comorbidities. Hence, minimally invasive treatment such as percutaneous aortic balloon valvotomy (PABV) maybe an alternative to surgery as a palliative strategy. PABV is a procedure during which one or more balloons are placed across a stenotic valve and then inflated in order to cause a decrease the severity of aortic stenosis. This is to be distinguished from transcatheter aortic valve implantation (TAVI) which is a different method that involves replacement of the valve percutaneously.
Both ACC/AHA and ESC/EACTS give PABV a Class IIb recommendation only as a bridge to SAVR or TAVR, or before urgent noncardiac surgery. It is not recommended as a definitive or standalone palliative therapy due to high restenosis rates.[10]
Transcatheter Aortic Valve Implantation
TAVR has been FDA-approved for all surgical risk categories (including low risk) since 2019, based on the PARTNER 3 and Evolut Low Risk trials [15]. In Transcatheter Aortic Valve Implantation (TAVI) also known as Percutaneous Aortic Valve Replacement (PAVR), a synthetic valve is advanced to the heart through a small hole made in the groin. This procedure is similar in its mechanism to the insertion of a stent, or performing balloon angioplasty albeit with much larger equipment. Traditional aortic valve replacement is an invasive surgical procedure, with considerable mortality and morbidity, especially in more fragile patients. In the newly developed TAVI procedure, the dysfunctional aortic valve is replaced percutaneously, which obviates the need for open heart surgery. TAVR has lower 30-day risk of atrial fibrillation (10% vs. 33%) and major bleeding compared to SAVR, but higher rates of permanent pacemaker implantation (15% vs. 6%) and paravalvular regurgitation. Long-term durability data for TAVR extend up to 10 years in older patients, compared to >20 years for surgical bioprosthetic valves.[2]
Follow Up
Follow up is recommended for all patients with operated and unoperated aortic stenosis. Asymptomatic patients with aortic stenosis should undergo follow up since aortic stenosis is an ongoing disease that progresses with time. The Follow Up time is following:
Severe AS (Stage C1): every 6-12 months
Moderate AS: every 1-2 years
Mild AS: every 3-5 years[2][1]
Prevention
Aortic stenosis associated with rheumatic heart disease can be minimized with antibiotic therapy in patients with documented streptococcal pharyngitis (strep throat).[15]Bicuspid aortic valve disease is a congenital variant and cannot be prevented. Three large RCTs (SALTIRE, SEAS, ASTRONOMER) and a Cochrane systematic review conclusively demonstrated that statins do not slow the progression of calcific AS or reduce the need for valve replacement. The 2020 ACC/AHA guidelines explicitly state there are no data to support statins for prevention of AS progression.[2][1]
Currently, no medical therapies have been proven to slow AS progression. Medications targeting calcification (bisphosphonates, denosumab) have also been ineffective. Lp(a)-lowering therapies are under investigation but no published data yet support their use for AS[2]
Precautions and Prophylaxis
The 2020 ACC/AHA guidelines do not recommend routine antibiotic prophylaxis for native valve AS (including bicuspid aortic valve). Prophylaxis is recommended only for the highest-risk groups: prosthetic cardiac valves (including TAVR), prosthetic material used for valve repair, previous IE, unrepaired cyanotic congenital heart disease, and cardiac transplant with valve regurgitation. The 2021 AHA scientific statement specifically considered and rejected expanding prophylaxis to patients with native valve AS, bicuspid aortic valve, or rheumatic heart disease. [1][2]
Clindamycin is no longer recommended for IE prophylaxis due to increased risk of Clostridium difficile infection. Preferred alternatives for penicillin-allergic patients include cephalexin, azithromycin, or doxycycline.[16]
Patients with severe aortic stenosis should avoid strenuous exercise and any exercise that greatly increases afterload such as weight lifting.
References
- ↑ 1.00 1.01 1.02 1.03 1.04 1.05 1.06 1.07 1.08 1.09 1.10 https://www.jacc.org/doi/10.1016/j.jacc.2020.11.018
- ↑ 2.00 2.01 2.02 2.03 2.04 2.05 2.06 2.07 2.08 2.09 2.10 2.11 doi:10.1001/jama.2024.16477
- ↑ 3.0 3.1 doi:10.1001/jama.2024.16477
- ↑ 4.0 4.1 doi:10.1001/jamacardio.2022.0987
- ↑ 5.0 5.1 5.2 DOI: 10.1093/eurheartj/ehac361
- ↑ 6.0 6.1 https://pubmed.ncbi.nlm.nih.gov/37078819/DOI: 10.1093/cvr/cvad062
- ↑ 7.0 7.1 https://jamanetwork.com/journals/jamacardiology/fullarticle/2820718?utm_source=openevidence&utm_medium=referral
- ↑ https://pubmed.ncbi.nlm.nih.gov/35241220/
- ↑ https://www.ahajournals.org/doi/full/10.1161/CIR.0000000000000979?rfr_dat=cr_pub++0pubmed&url_ver=Z39.88-2003&rfr_id=ori%3Arid%3Acrossref.org
- ↑ 10.0 10.1 10.2 10.3 10.4 https://pubmed.ncbi.nlm.nih.gov/37587584/
- ↑ https://pubmed.ncbi.nlm.nih.gov/35113967/
- ↑ 12.0 12.1 https://jamanetwork.com/journals/jama/fullarticle/2825540?utm_source=openevidence&utm_medium=referral
- ↑ https://pubmed.ncbi.nlm.nih.gov/32828787/
- ↑ https://jamanetwork.com/journals/jamacardiology/article-abstract/2824468?utm_source=openevidence&utm_medium=referra
- ↑ 15.0 15.1 15.2 https://jamanetwork.com/journals/jama/article-abstract/2781245?utm_source=openevidence&utm_medium=referral
- ↑ 16.0 16.1 https://www.aafp.org/pubs/afp/issues/2026/0200/infective-endocarditis.html
Historical Perspective
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Mandana Chitsazan, M.D. [2]
Overview
Aortic stenosis was probably first described by Lazare Riviere, a French physician in 1663.
Historical Perspective
- In 1663, the earliest description of calcific aortic stenosis was made by a french physician named Lazare Rivière. He identified left ventricular hypertrophy and large caruncle-like masses obstructing the left ventricular outflow in an autopsy report from a patient with palpitations, progressive dyspnea, and loss of peripheral pulses.[1][2]
- The first transcatheter aortic valve replacement procedure in the world was performed on 16 April 2002 in a 57-year-old inoperable patient with severe aortic stenosis. The procedure was done by the Interventional Cardiologist Professor Alain Cribier at the Charles Nicolle University Hospital in Rouen, France. [3] [4]
References
- ↑ Leopold, Jane A. (2012). “Cellular Mechanisms of Aortic Valve Calcification”. Circulation: Cardiovascular Interventions. 5 (4): 605–614. doi:10.1161/CIRCINTERVENTIONS.112.971028. ISSN 1941-7640.
- ↑ Lerman DA, Prasad S, Alotti N (2015). “Calcific Aortic Valve Disease: Molecular Mechanisms and Therapeutic Approaches”. Eur Cardiol. 10 (2): 108–112. doi:10.15420/ecr.2015.10.2.108. PMC 4888946. PMID 27274771.
- ↑ “15 Years in TAVI”.
- ↑ “Harold on History: The Evolution of Transcatheter Aortic Valve Replacement – American College of Cardiology”.
Classification
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Mandana Chitsazan, M.D. [2]
Overview
According to the 2020 AHA/ACC Guideline for the Management of Patients With Valvular Heart Disease, there are 4 stages of aortic stenosis based on the valve anatomy, valve hemodynamics, the left ventricular and vascular consequences of aortic obstruction, and the symptoms. The stages include at risk of AS, progressive hemodynamic obstruction, severe asymptomatic AS, and symptomatic AS.
Classification
According to the 2020 AHA/ACC Guideline for the Management of Patients With Valvular Heart Disease, there are 4 stages of aortic stenosis based on the valve anatomy, valve hemodynamics, the left ventricular and vascular consequences of aortic obstruction, and the symptoms of the patient:
- A: Patient at risk of AS
- B: Progressive hemodynamic obstruction
- C: Severe asymptomatic AS
- D: Symptomatic AS
Hemodynamic severity is assessed by transaortic maximum velocity or mean pressure gradient in the presence of a normal transaortic flow rate. However, some patients with AS have a low transaortic flow rate due to:
- LV systolic dysfunction with a reduced LV ejection fraction (designated as D2)
- Small hypertrophied LV with a low stroke volume (designated as D3) [1]
| Stage | Definition | Valve Anatomy | Valve Hemodynamics | Hemodynamic Consequences | Symptoms |
|---|---|---|---|---|---|
| A | At risk of AS |
|
|
|
|
| B | Progressive AS |
|
|
|
|
| C: | Asymptomatic severe AS | ||||
| C1 | Asymptomatic severe AS |
|
|
|
|
| C2 | Asymptomatic severe AS with LV dysfunction |
|
|
|
|
| D: | Symptomatic severe AS | ||||
| D1 | Symptomatic severe high-grade AS |
|
|
|
|
| D2 | Symptomatic severe low-flow/low-gradient AS with reduced LVEF |
|
|
|
|
| D3 | Symptomatic severe low-gradient AS with normal LVEF or paradoxical low-flow severe AS |
|
|
|
|
References
- ↑ Otto CM, Nishimura RA, Bonow RO, Carabello BA, Erwin JP, Gentile F, Jneid H, Krieger EV, Mack M, McLeod C, O’Gara PT, Rigolin VH, Sundt TM, Thompson A, Toly C (February 2021). “2020 ACC/AHA Guideline for the Management of Patients With Valvular Heart Disease: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines”. Circulation. 143 (5): e72–e227. doi:10.1161/CIR.0000000000000923. PMID 33332150 Check
|pmid=value (help).
Pathophysiology
Narrowing of the Aortic Valve | Left Ventricular Hypertrophy | Early Diastolic Dysfunction | Late Systolic Dysfunction | Atrial Fibrillation | Hemodynamics of Aortic Stenosis | Low Flow, Low Gradient Aortic Stenosis | Gross Pathology | Microscopic Pathology
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-In-Chief: Mohammed A. Sbeih, M.D. [2], Lakshmi Gopalakrishnan, M.B.B.S. [3]; Usama Talib, BSc, MD [4] , Claudia P. Hochberg, M.D. [5], Abdul-Rahman Arabi, M.D. [6], Keri Shafer, M.D. [7], Priyamvada Singh, MBBS [8], Aysha Anwar, M.B.B.S[9] Cafer Zorkun, M.D., Aysha Anwar, M.B.B.S[10] Mandana Chitsazan, M.D. [11] Assistant Editor-In-Chief: Kristin Feeney, B.S. [12]; Rim Halaby
Overview
Aortic stenosis is the progressive narrowing of the aortic valve. Calcific aortic stenosis, in particular, is an active atherosclerotic pathology where inflammation, fibrosis, and calcification are involved in the progressive narrowing of the effective aortic valve area in the absence of any commissural fusion. In contrast, rheumatic aortic stenosis is due to the fusion of the commissures with valvular scarring and calcification. Aortic stenosis causes an impedance to the antegrade blood flow not only at the level of the aortic valve itself but also at the subvalvular (below the aortic valve) or supravalvular (above the aortic valve) levels. As a result, chronic pressure overload develops in the left ventricle. The left ventricle undergoes hypertrophy as an initial adaptive mechanism to overcome the increased afterload. This compensatory mechanism ends up being maladaptive by causing apoptosis of the hypertrophied myocytes and subsequent heart failure. Hence, aortic stenosis is a progressive valvular disease which progression depends mainly on the degree of the narrowing of the aortic valve as well as on the maladaptive ventricular wall response. Gross anatomy dissection may be used as a diagnostic tool in the evaluation of aortic stenosis. Common findings associated with aortic stenosis include left ventricular hypertrophy and heart block.
Pathophysiology
- Aortic stenosis in the progressive narrowing of the aortic valve.[1]
- The decrease in aortic valve area does not cause a change in the antegrade velocity unless the area is decreased by at least half. Aortic stenosis causes an impedance to the antegrade blood flow not only at the level of the aortic valve itself but also at the subvalvular (below the aortic valve) or supravalvular (above the aortic valve) levels. As a result, chronic pressure overload develops in the left ventricle. As a result, chronic pressure overload develops in the left ventricle.[2]
- Slow compensatory mechanisms occur in the heart to adapt to the pressure changes caused by aortic stenosis. The most prominent adaptive mechanism is ventricular hypertrophy which leads early on to diastolic dysfunction and later on to systolic dysfunction.[3][4]
Shown below is an image summarizing the pathophysiology of aortic stenosis:[4]

Associated Conditions
Heyde’s Syndrome
- In Heyde’s syndrome, aortic stenosis is associated with angiodysplasia of the colon. Presenting symptoms include:[5]
Von Willebrand Disease
- Aortic stenosis may result in a form of von Willebrand disease due to an increased turbulence around the stenosed aortic valve which subsequently triggers the break down of coagulation factor VIII-associated antigen, (also called von Willebrand factor) and thus results in a variant of von Willebrand disease.[6][7]
Narrowing of the Aortic Valve
Calcific Aortic Stenosis
Calcific aortic stenosis has long been thought to be the result of prolonged wear and tear mechanism and age-related degeneration of the valvular cusps as opposed to cusp fusion of the aortic valve in rheumatic heart disease. However, recent studies have revealed that the underlying pathophysiology of calcific aortic stenosis is active inflammation, fibrosis, and calcification. Genetic predisposition plays a role in the rate of progression of aortic stenosis. The stages of the formation of the calcific aortic stenosis are the following:[4]
- Endothelial Damage:
- Endothelial damage is the initial event starting the cascade of events in calcific aortic stenosis.
- It results from increased mechanical stress and decreased shear stress.
- Endothelial damage happens at a faster rate in bicuspid aortic valves than in tricuspid aortic valves as a result of the difference in distribution of stress forces on the valvular cusps.[4]
- Inflammation:
- Endothelial damage triggers accumulation of lipids (LDL and lipoprotens) that subsequently undergo oxidative changes.
- As a result, inflammation is accentuated by:
- Elevated CRP in patients with aortic stenosis is an evidence of inflammation[8]
- Fibrosis:
- Inflammation eventually leads to activation of fibroblasts and remodeling of the extracellular matrix[9]
- Calcification:
- Calcification is induced by long standing inflammation and fibrosis.
- The following disorders of mineral metabolism accelerates calcification:[4][10][11][12][13]
- Hemodialysis
- Osteoporosis
- Paget’s disease
- Vitamin D receptor polymorphism
- Calcification starts at the base of the cusps and then reaches the leaflets. Calcification results in a decrease in the leflet motion and hence decrease in the effective valve area in the absence of any fusion of the commissures.[14]
- Calcification is coordinated by osteoblasts in the context of a highly regulated mechanism similar to bone formation.[4]
Rheumatic Aortic Stenosis
- Rheumatic aortic stenosis is due to the fusion of the valve commissures and subsequent scarring and calcification. Rheumatic aortic stenosis is always accompanied by mitral regurgitation.[14]
- Rheumatic fever which depends on a prior autoimmunological stimulation, is a systemic disease affecting the peri-arteriolar connective tissue and can occur after an untreated Group A streptococcal pharyngeal infection. It is believed to be caused by antibody cross-reactivity which is a type II hypersensitivity reaction and is termed ‘molecular mimicry’.
- Chronic rheumatic heart disease is characterized by repeated inflammation with fibrinous resolution. The cardinal anatomic changes of the valve include leaflet thickening, commissural fusion and shortening and thickening of the tendinous cords.[15]Rheumatic heart disease may lead to up to 99% stenosis of the aortic valve often resulting in a “fish mouth” gross appearance.
Congenital Aortic Stenosis
Congenital malformation of the aortic valve is one of the less common causes of aortic stenosis.[16]Congenital aortic stenosis is detected in young adults.
Left Ventricular Hypertrophy
- Long-standing aortic stenosis exposes the left ventricle to prolonged pressure overload which leads to concentric hypertrophy as a compensatory mechanism to preserve left ventricular function.[17][18][19] The left ventricular wall increases in thickness (i.e. concentric hypertrophy occurs) as a result of the parallel replication of the sarcomeres
- However, left ventricle hypertrophy ends up being a maladpative mechanism and a marker of a bad prognosis. Hypertrophied myocardial cells undergo apoptosis at a rate larger to that of regeneration.[4] In fact, angiotensin II promotes the apoptosis of the hypertrophied vessels, thus angiotensin receptor blockers (ARB) paly a role in the treatment of heart failure secondary to aortic stenosis even without having a great role in decreasing the blood pressure.[20]
- Left ventricular hypertrophy weakly relates to the degree of stenosis itself but rather to advanced age, male sex and obesity. Other factors that participate in the hypertrophy of the left ventricle are hypertension and increased arterial stiffness.
- Fibrosis is an integral component of the myocardial hypertrophy.[4]
Early Diastolic Dysfunction
During the initial period of concentric hypertrophy, the left ventricle is not dilated and there is preservation of the left ventricular systolic function. Diastolic function, however, may be reduced due to a reduction in diastolic compliance.[21][22][23]
This diastolic dysfunction may in turn lead to a rise in pulmonary capillary wedge pressure and consequently lead to dyspnea. Cardiac output may also be reduced as a result of diastolic dysfunction and impaired filling of the left ventricle. Early in the course of aortic stenosis, there may be a failure to augment cardiac output during exercise resulting in dyspnea on exertion.
Late Systolic Dysfunction
Later in the course of aortic stenosis, left ventricular dysfunction may develop due to a variety of pathophysiological processes. Systolic dysfunction is associated with a poor prognosis and it often does not partially or fully reverse following operative repair.[22]
Excess Hypertrophy Causes Systolic Dysfunction
The massive concentric hypertrophy, characterized by a reduced diastolic radius-to-wall thickness ratio, has shown to initially counter balance the increased systolic left ventricular pressure; nevertheless, if this process continues, an inverse relationship has been observed such that the ejection fraction eventually goes down as the left ventricular mass increases beyond a certain point.[24][22][25][26]
Myocardial Ischemia
The hypertrophied left ventricle and the prolonged ejection time (the time for the heart to eject blood) result in an increase in the myocardial oxygen requirements. In addition, the elevated diastolic filling pressure reduces the gradient between the aorta and the right atrium (“the height of the waterfall”) which normally drives coronary blood flow. There may be a relative reduction in the density of the capillary network. The hypertrophied ventricle may also compress the capillaries. All of the above lead to a reduction in coronary blood flow even in the absence of obstructive epicardial stenosis. This may lead to subendocardial ischemia during stress or exercise.[27][28]
Myocardial Fibrosis
Myocardial scarring or fibrosis may develop with prolonged aortic stenosis, probably due to chronic subendocardial ischemia or increased wall stress. [29]
Dyssynchronous Contraction
Another factor that may contribute to the reduced left ventricular systolic function is the dyssynchronous contraction subsequent to regional wall motion abnormalities, fibrosis or ischemia.[30]
Atrial Fibrillation
The stiff non-compliant left ventricle can become increasingly dependent on the left atrium for filling, which predisposes to atrial fibrillation. The presence of atrial fibrillation and the associated loss of atrial contractility can result in reduced left ventricular filling and reduced cardiac output.[31]
Hemodynamics of Aortic Stenosis
Pressure Gradient and Valve Area
When the aortic valve becomes stenosed, it can result in the formation of a pressure gradient between the left ventricle (LV) and the aorta.[32] The more constricted the valve is, the bigger the gradient between the LV and the aorta is.
For instance, the pressure gradient in patients with mild AS might be 20 mmHg. This means that, at peak systole, while the LV may generate a pressure of 140 mmHg, the pressure that is transmitted into the aorta will only be 120 mmHg. Therefore, while a blood pressure cuff may measure a normal systolic blood pressure the actual pressure generated by and inside the LV would be considerably higher. As the left ventricle fails, it may no longer be able to mount the contractility necessary to generate a large gradient across the aortic valve.
Therefore, the absence of a large gradient across the aortic valve does not exclude the presence of critical aortic stenosis. The presence of a low gradient and a low ejection results in a low flow aortic stenosis. It is for this reason that the best measure of the severity of aortic stenosis is the aortic valve area and not the aortic valve gradient.
Read in detail by clicking on the topics:
Subvalvular Gradients in AS in the Absence of Anatomic Obstruction
Subvalvular pressure gradients are often present in patients with severe aortic stenosis in the absence of an anatomic subvalvular obstruction. In fact, the subvalvular pressure gradients constitute around 50% of the total measured transvalvular gradient. The extent of increase in cardiac output during exercise is inversely related to the magnitude of subvalvular gradient.[33]
Flow Velocity
If the left ventricular function and contractility are preserved, a flow velocity across the stenosed valve of at least 2.6 m/sec is deemed consistent with aortic stenosis. This is based on the echocardiographic estimation of the aortic jet velocity, the aortic valve area and the mean transvalvular gradient. The aortic valve becomes calcified in aortic valve sclerosis (not stenosis); however, the aortic jet velocity is ≤ 2.5 m/sec (without a significant gradient). Aortic valve sclerosis is commonly characterized by a focal thickening of the aortic cusps with calcific nodules generally at the base of leaflets and a transvalvular velocity within the normal range (Vmax <2 m/s). Until a few years ago, aortic valve sclerosis was considered to be a physiologic process related to aging without any clinical relevance. However, aortic valve sclerosis is not observed in about 50% of people over 80 years old. Furthermore, several experimental and clinical studies have demonstrated that aortic valve sclerosis could represent an active phenomenon significantly related to the risk factors of atherosclerosis.[34][35]
Relationship of Hemodynamic Severity to Symptoms of Aortic Stenosis
- Patients with aortic stenosis become symptomatic when:[36][37]
- The valve area is less than 1.0 cm2.
- The jet velocity is over 4.0 m/sec.
- Mean transvalvular pressure gradient exceeds 40 mm Hg.
- However, many patients develop symptoms only when more severe valve obstruction is present, other patients become symptomatic at a less severe degree of stenosis, particularly if there is coexisting aortic regurgitation.
ACC/AHA Guidelines – Severity Classification [36]
Indicator Mild Moderate Severe Jet velocity (m per s) Less than 3.0 3.0–4.0 Greater than 4.0 Mean gradient (mm Hg)† Less than 25 25–40 Greater than 40 Valve area (cm2) Greater than 1.5 1.0–1.5 Less than 1.0 Valve area index (cm2 per m2) Less than 0.6
† Valve gradients are flow-dependent. They should be assessed with knowledge of cardiac output or antegrade flow across the valve when used to estimate of the severity of valve stenosis.
Low Flow, Low Gradient Aortic Stenosis
- In aortic stenosis, as the aortic orifice area decreases the transvalvular gradient increases. In fact, when the aortic valve effective orifice area decreases below 1.0 cm2 the mean transvalvular gradient is expected to be larger than 40 mm Hg. The transvalvular gradient is highly dependent on the flow of blood through the valve.
- However, when severe systolic or/and diastolic myocardial dysfunction coexist with the aortic stenosis, there is a decrease in the flow through the valve leading to a prominent decrease in the transvalvular gradient. This is called low flow, low gradient aortic stenosis (LFLG AS).
- LFLG AS is a challenging diagnosis that must be done in order to tailor the management plan. It is important to recognize these entities because they might cause either underestimation or overestimation of the degree of severity of the aortic stenosis.
- Two various scenarios occur in the setting of LFLG AS depending on the status of the left ventricular ejection fraction:
- LFLG AS with low LVEF
- LFLG AS with normal LVEF[38]
Shown below is a table depicting the differences between LFLG AS with low LVEF and LFLG AS with normal LVEF:
| LFLG AS | Percentage of the Cases of Severe AS Caused by LFLG AS | Pathophysiology | Diagnostic Challenges |
|---|---|---|---|
| LFLG AS with low LVEF | 5-10% of severe aortic stenosis | Decreased systolic function:
Dilated left ventricle Decreased contractility |
Differentiation between severe aortic stenosis and pseudo-severe aortic stenosis |
| LFLG AS with normal LVEF | 10-25% of severe aortic stenosis | Decreased diastolic function:
Small left ventricle Decreased compliance |
Underestimation of the severity of aortic stenosis
Differentiation from confounding measurement errors and small ventricle body size |
Low Flow, Low Gradient Aortic Stenosis with Low Ejection Fraction
- When ventricular systolic dysfunction is present, the myocardium can not contract strongly enough to pump blood with a lot of pressure. In that case, low flow and subsequent low transvalvular gradient are present and this entity is called LFLG AS with low LVEF.
- LFLG AS with low LVEF is defined as:[36][37][38]
- An aortic valve areas < 1.0 cm2
- A left ventricular ejection fraction < 40%
- A mean pressure difference or gradient across the aortic valve of < 30 mm Hg
- When low flow, low gradient aortic stenosis is present, the challenge is to differentiate whether the LFLG AS with low LVEF is a true severe aortic stenosis or a pseudo-severe aortic stenosis. It is very important to differentiate between these two entities as they have different outcomes following aortic valve replacement.[38]
True Severe Aortic Stenosis
- The aortic stenosis is so severe that it caused secondary left ventricular dysfunction. This systolic dysfunction causes decreased contractility and hence causes decreased ejection force and low transvalvular flow and gradient.[38]
Pseudo-Severe Aortic Stenosis
The aortic stenosis in Pseudo-Severe Aortic Stenosis is mild or moderate but it co-exists with another myocardial disease that is independent from the aortic stenosis. Overestimation of the severity of the aortic stenosis happens in this context.
- The presence of fibrosis in the left ventricle may cause an incomplete recovery after aortic valve replacement[22].
- This scenario can also occur among patients in whom there is a history of myocardial infarction due to the absence of sufficient contractility to mount an aortic gradient.
- It may also occur when myocardial fibrosis develops due to longstanding aortic stenosis.[38]
Low Flow, Low Gradient Aortic Stenosis with Normal Ejection Fraction
LFLG AS with normal ejection fraction has been recently described and it is usually an advanced stage of valvular and myocardial diseases.
- LFLG AS with normal ejection fraction has a lot of similarities with normal ejection fraction diastolic heart failure. In fact, it is usually present in older females in the context of systemic hypertension. The underlying pathophysiology is a restrictive myocardium.
- The characteristics of LFLG AS with normal ejection fraction is the presence of extensive remodeling due to predominant diastolic dysfunction as well as systolic dysfunction. However, the decrease in the systolic performance of the left ventricle does not show a decrease in the ejection fraction.[38]
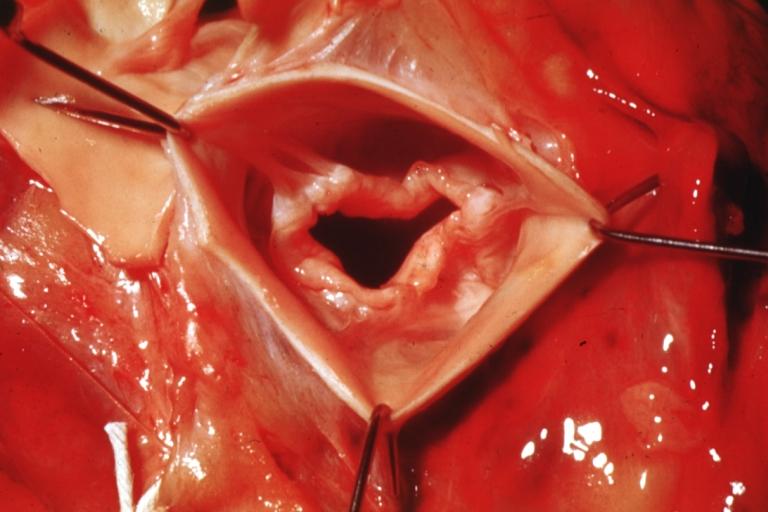
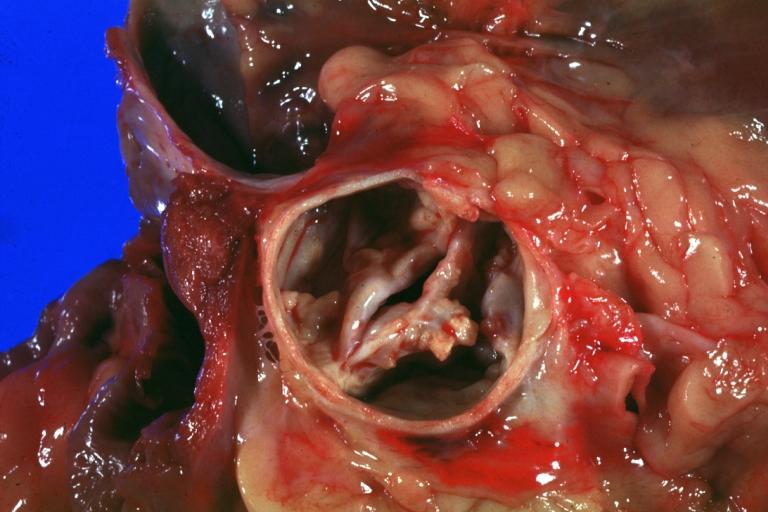
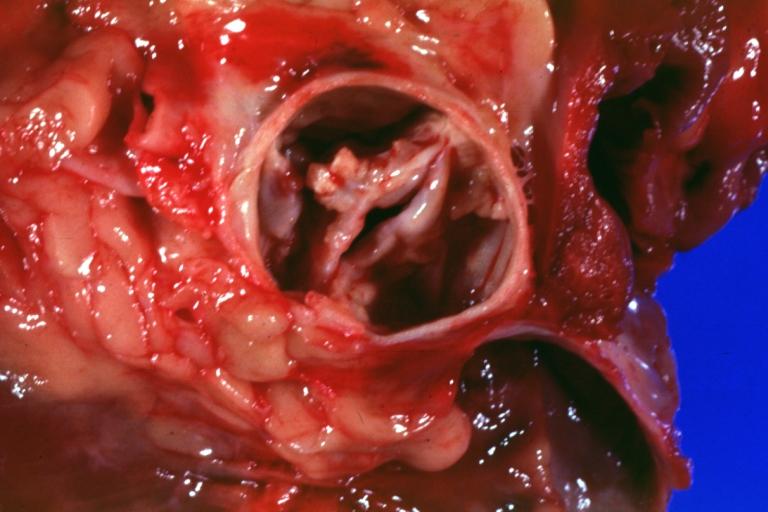
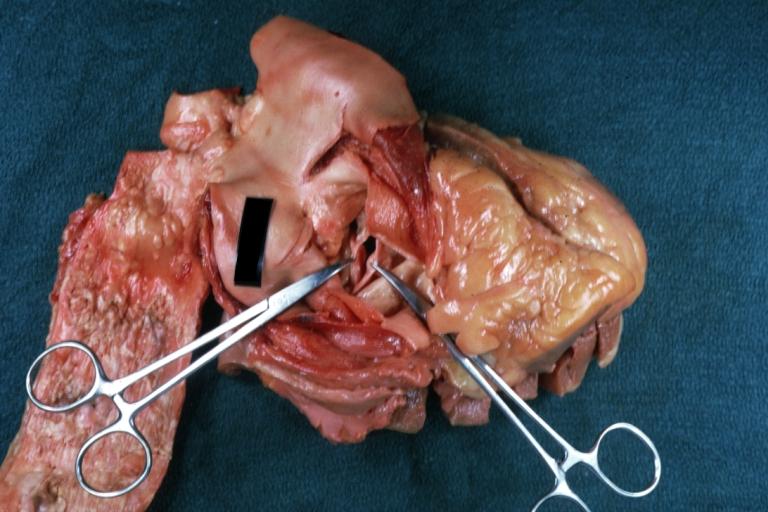
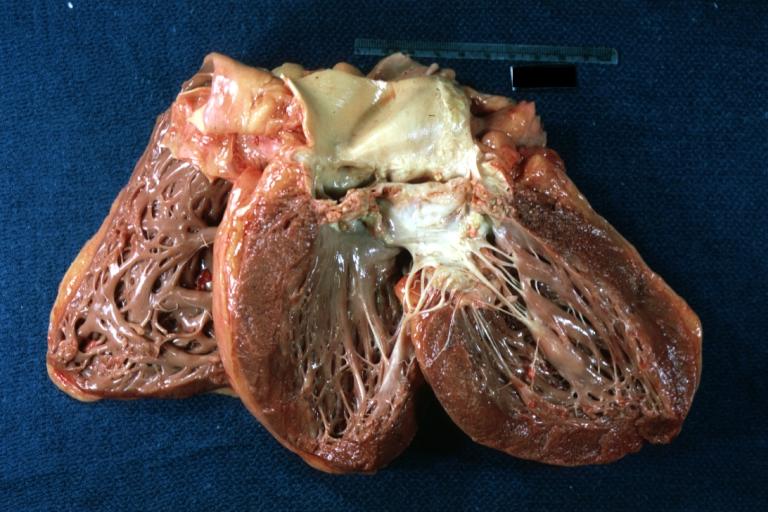
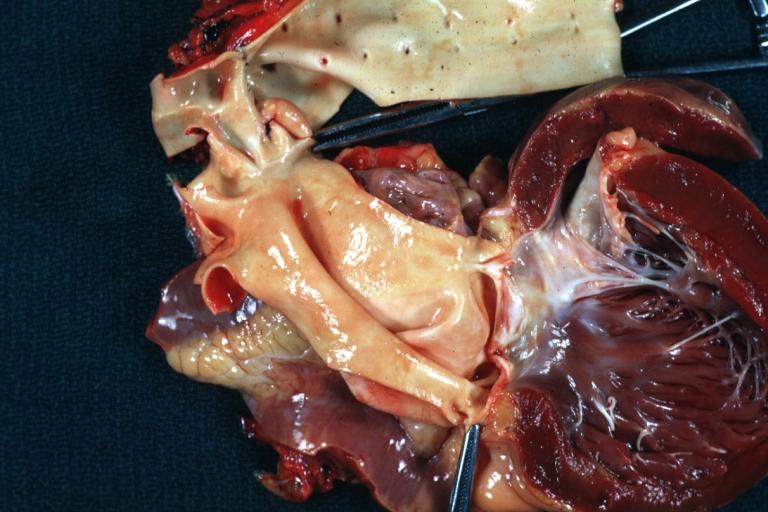
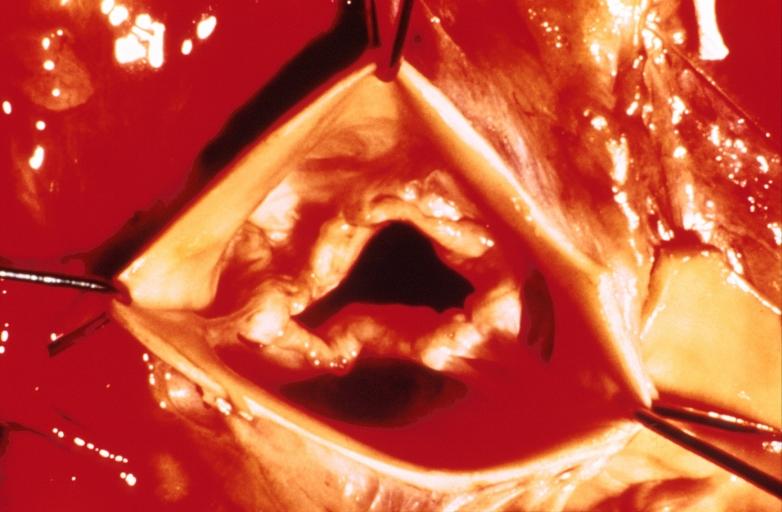
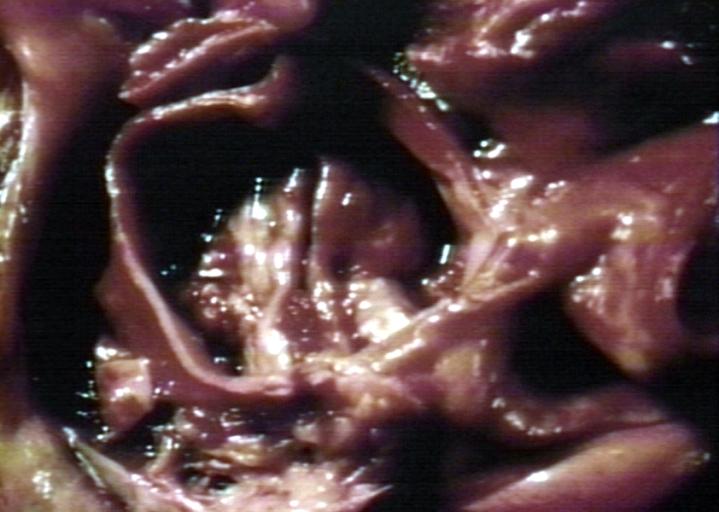
Gross Pathology
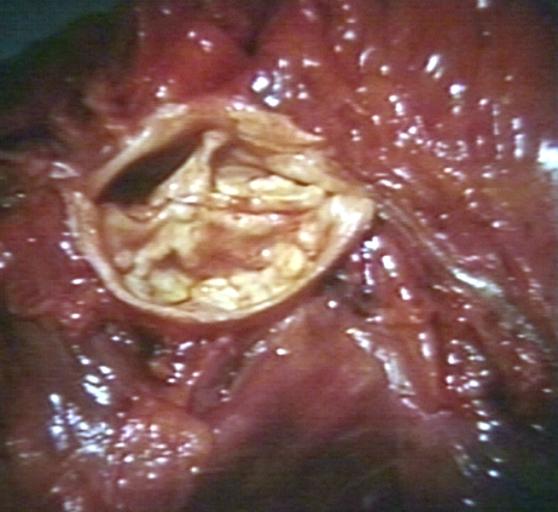
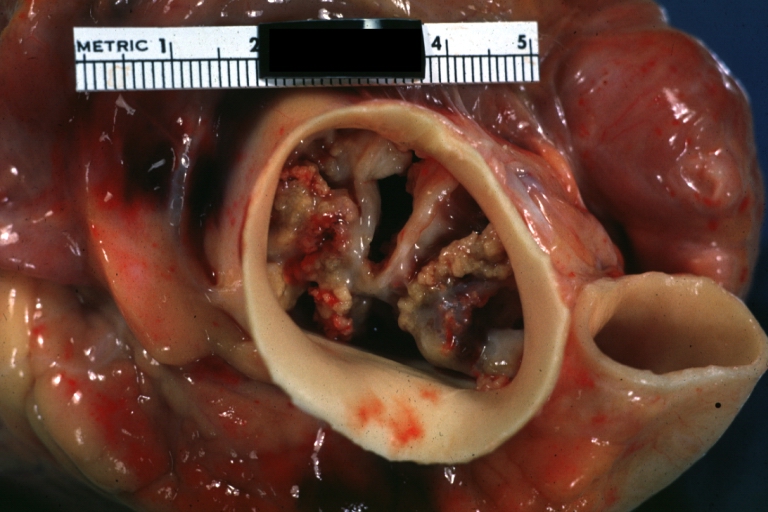
Pathological findings of congenital or acquired aortic stenosis in adults result in thickening and calcification of aortic valve. The following patterns may be seen:[39]
- Calcified bicuspid valve involving anterior or posterior cusps
- Calcified aortic valve cusps with the fusion of commissures seen in post rheumatic cases
- Degenerative calcific aortic stenosis which shows sinuses of Valsalva filled with calcium deposits seen in age >70
Images shown below are courtesy of Professor Peter Anderson DVM Ph.D. and published with permission. © PEIR, the University of Alabama at Birmingham, Department of Pathology
-
 Aortic Stenosis, Bicuspid valve: Gross; excellent image of bicuspid and calcific valve showing a false raphe.
Aortic Stenosis, Bicuspid valve: Gross; excellent image of bicuspid and calcific valve showing a false raphe. -
 Aortic Stenosis, Bicuspid valve: Gross; good example of bicuspid valve
Aortic Stenosis, Bicuspid valve: Gross; good example of bicuspid valve -
 Aortic Stenosis, Bicuspid valve: Gross; image of bicuspid aortic valve, an excellent example
Aortic Stenosis, Bicuspid valve: Gross; image of bicuspid aortic valve, an excellent example -
 Aortic Stenosis, Bicuspid valve: Gross; close-up image of bicuspid aortic valve.
Aortic Stenosis, Bicuspid valve: Gross; close-up image of bicuspid aortic valve. -
 Aortic Stenosis, Bicuspid valve: Gross; close-up image of bicuspid aortic valve.
Aortic Stenosis, Bicuspid valve: Gross; close-up image of bicuspid aortic valve. -
 Bicuspid aortic valve
Bicuspid aortic valve -
 Gross natural color opened first portion aortic arch with bicuspid aortic valve shows stenosis and aortic root is dilated
Gross natural color opened first portion aortic arch with bicuspid aortic valve shows stenosis and aortic root is dilated -
 Aortic Stenosis Bicuspid: Gross; natural color opened left ventricular outflow tract with calcific masses on valve as well as anterior leaflet mitral valve probably did not cause significant stenosis
Aortic Stenosis Bicuspid: Gross; natural color opened left ventricular outflow tract with calcific masses on valve as well as anterior leaflet mitral valve probably did not cause significant stenosis -
 Bicuspid Aortic Valve with Repaired Aorta Coarctation: Gross natural color opened left ventricular outflow tract with uncomplicated bicuspid aortic valve repaired coarctation barely visible ruptured postoperative young female with ovaries Turner mosaic not ruled out
Bicuspid Aortic Valve with Repaired Aorta Coarctation: Gross natural color opened left ventricular outflow tract with uncomplicated bicuspid aortic valve repaired coarctation barely visible ruptured postoperative young female with ovaries Turner mosaic not ruled out -
 Bicuspid Aortic Stenosis: Gross; fixed tissue
Bicuspid Aortic Stenosis: Gross; fixed tissue -
 Aortic Stenosis, Bicuspid: Gross; fixed tissue view of stenotic valve through ventricular outlet track
Aortic Stenosis, Bicuspid: Gross; fixed tissue view of stenotic valve through ventricular outlet track -
 Aortic Stenosis Bicuspid: Gross; fixed tissue. Bicuspid valve and false raphe classical
Aortic Stenosis Bicuspid: Gross; fixed tissue. Bicuspid valve and false raphe classical -
 Bicuspid aortic valve
Bicuspid aortic valve -
 Bicuspid aortic valve
Bicuspid aortic valve -
 Bicuspid aortic valve
Bicuspid aortic valve -
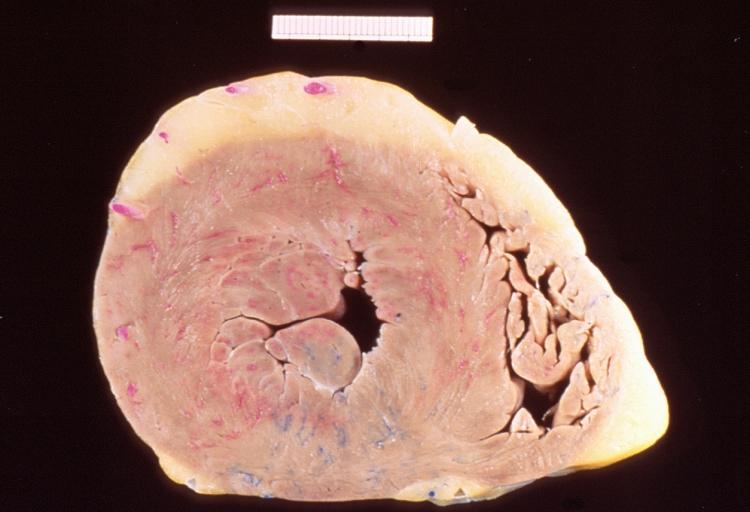 Left ventricular hypertrophy due to bicuspid aortic valve
Left ventricular hypertrophy due to bicuspid aortic valve -
 Congenital aortic stenosis: Gangrene toe In Infant: Gross, natural color, 1-month-old child with congenital aortic stenosis
Congenital aortic stenosis: Gangrene toe In Infant: Gross, natural color, 1-month-old child with congenital aortic stenosis -
 Unicuspid aortic stenosis
Unicuspid aortic stenosis


















Microscopic Pathology
On microscopic histopathological analysis, the calcific aortic stenosis shows pink amorphous material around the calcific foci indicating deposition of calcium. Congenital and calcific aortic stenosis show the areas of fibrosis, thickening, fat cell infiltration and elastosis.[40]
References
- ↑ Galli D, Manuguerra R, Monaco R, Manotti L, Goldoni M, Becchi G; et al. (2016). “Understanding the structural features of symptomatic calcific aortic valve stenosis: A broad-spectrum clinicopathologic study in 236 consecutive surgical cases”. Int J Cardiol. 228: 364–374. doi:10.1016/j.ijcard.2016.11.180. PMID 27866029.
- ↑ Joseph J, Naqvi SY, Giri J, Goldberg S (2016). “Aortic stenosis: pathophysiology, diagnosis and therapy”. Am J Med. doi:10.1016/j.amjmed.2016.10.005. PMID 27810479.
- ↑ Otto CM, Prendergast B (2014). “Aortic-valve stenosis–from patients at risk to severe valve obstruction”. N Engl J Med. 371 (8): 744–56. doi:10.1056/NEJMra1313875. PMID 25140960.
- ↑ 4.0 4.1 4.2 4.3 4.4 4.5 4.6 4.7 4.8 Dweck MR, Boon NA, Newby DE (2012). “Calcific aortic stenosis: a disease of the valve and the myocardium”. J Am Coll Cardiol. 60 (19): 1854–63. doi:10.1016/j.jacc.2012.02.093. PMID 23062541.
- ↑ Ledingham D (2013). “Heyde’s syndrome: exploring the link between aortic stenosis and an acquired bleeding disorder”. BMJ Case Rep. 2013. doi:10.1136/bcr-2013-009306. PMC 3645074. PMID 23605838.
- ↑ Vincentelli A, Susen S, Le Tourneau T, Six I, Fabre O, Juthier F; et al. (2003). “Acquired von Willebrand syndrome in aortic stenosis”. N Engl J Med. 349 (4): 343–9. doi:10.1056/NEJMoa022831. PMID 12878741.
- ↑ Tamura T, Horiuchi H, Imai M, Tada T, Shiomi H, Kuroda M; et al. (2015). “Unexpectedly High Prevalence of Acquired von Willebrand Syndrome in Patients with Severe Aortic Stenosis as Evaluated with a Novel Large Multimer Index”. J Atheroscler Thromb. 22 (11): 1115–23. doi:10.5551/jat.30809. PMID 26269004.
- ↑ Galante A, Pietroiusti A, Vellini M, Piccolo P, Possati G, De Bonis M; et al. (2001). “C-reactive protein is increased in patients with degenerative aortic valvular stenosis”. J Am Coll Cardiol. 38 (4): 1078–82. PMID 11583885.
- ↑ Frantz C, Stewart KM, Weaver VM (2010). “The extracellular matrix at a glance”. J Cell Sci. 123 (Pt 24): 4195–200. doi:10.1242/jcs.023820. PMC 2995612. PMID 21123617.
- ↑ Ureña P, Malergue MC, Goldfarb B, Prieur P, Guédon-Rapoud C, Pétrover M (1999). “Evolutive aortic stenosis in hemodialysis patients: analysis of risk factors”. Nephrologie. 20 (4): 217–25. PMID 10480155.
- ↑ Aksoy Y, Yagmur C, Tekin GO, Yagmur J, Topal E, Kekilli E; et al. (2005). “Aortic valve calcification: association with bone mineral density and cardiovascular risk factors”. Coron Artery Dis. 16 (6): 379–83. PMID 16118543.
- ↑ Strickberger SA, Schulman SP, Hutchins GM (1987). “Association of Paget’s disease of bone with calcific aortic valve disease”. Am J Med. 82 (5): 953–6. PMID 3578364.
- ↑ Ortlepp JR, Hoffmann R, Ohme F, Lauscher J, Bleckmann F, Hanrath P (2001). “The vitamin D receptor genotype predisposes to the development of calcific aortic valve stenosis”. Heart. 85 (6): 635–8. PMC 1729782. PMID 11359741.
- ↑ 14.0 14.1 Bonow RO, Carabello BA, Chatterjee K, de Leon AC, Faxon DP, Freed MD; et al. (2008). “2008 Focused update incorporated into the ACC/AHA 2006 guidelines for the management of patients with valvular heart disease: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Revise the 1998 Guidelines for the Management of Patients With Valvular Heart Disease): endorsed by the Society of Cardiovascular Anesthesiologists, Society for Cardiovascular Angiography and Interventions, and Society of Thoracic Surgeons”. Circulation. 118 (15): e523–661. doi:10.1161/CIRCULATIONAHA.108.190748. PMID 18820172.
- ↑ Kumar RK, Tandon R (2013). “Rheumatic fever & rheumatic heart disease: the last 50 years”. Indian J Med Res. 137 (4): 643–58. PMC 3724245. PMID 23703332.
- ↑ Mordi I, Tzemos N (2012). “Bicuspid aortic valve disease: a comprehensive review”. Cardiol Res Pract. 2012: 196037. doi:10.1155/2012/196037. PMC 3368178. PMID 22685681.
- ↑ Sasayama S, Ross J, Franklin D, Bloor CM, Bishop S, Dilley RB (1976). “Adaptations of the left ventricle to chronic pressure overload”. Circulation Research. 38 (3): 172–8. PMID 129304. Retrieved 2012-04-10. Unknown parameter
|month=ignored (help) - ↑ Gaasch WH (1979). “Left ventricular radius to wall thickness ratio”. The American Journal of Cardiology. 43 (6): 1189–94. PMID 155986. Unknown parameter
|month=ignored (help);|access-date=requires|url=(help) - ↑ Spann JF, Bove AA, Natarajan G, Kreulen T (1980). “Ventricular performance, pump function and compensatory mechanisms in patients with aortic stenosis”. Circulation. 62 (3): 576–82. PMID 6446989. Retrieved 2012-04-10. Unknown parameter
|month=ignored (help) - ↑ González A, López B, Ravassa S, Querejeta R, Larman M, Díez J; et al. (2002). “Stimulation of cardiac apoptosis in essential hypertension: potential role of angiotensin II”. Hypertension. 39 (1): 75–80. PMID 11799082.
- ↑ Gaasch WH, Levine HJ, Quinones MA, Alexander JK (1976). “Left ventricular compliance: mechanisms and clinical implications”. The American Journal of Cardiology. 38 (5): 645–53. PMID 136186. Unknown parameter
|month=ignored (help);|access-date=requires|url=(help) - ↑ 22.0 22.1 22.2 22.3 Hess OM, Ritter M, Schneider J, Grimm J, Turina M, Krayenbuehl HP (1984). “Diastolic stiffness and myocardial structure in aortic valve disease before and after valve replacement”. [[]]: 855–65. Retrieved 2012-04-10. Unknown parameter
|month=ignored (help) - ↑ Gaasch WH (1994). “Diagnosis and treatment of heart failure based on left ventricular systolic or diastolic dysfunction”. JAMA : the Journal of the American Medical Association. 271 (16): 1276–80. PMID 8151903. Unknown parameter
|month=ignored (help);|access-date=requires|url=(help) - ↑ Krayenbuehl HP, Hess OM, Ritter M, Monrad ES, Hoppeler H (1988). “Left ventricular systolic function in aortic stenosis”. European Heart Journal. 9 Suppl E: 19–23. PMID 2969811. Retrieved 2012-04-10. Unknown parameter
|month=ignored (help) - ↑ Gunther S, Grossman W (1979). “Determinants of ventricular function in pressure-overload hypertrophy in man”. Circulation. 59 (4): 679–88. PMID 154367. Retrieved 2012-04-10. Unknown parameter
|month=ignored (help) - ↑ Huber D, Grimm J, Koch R, Krayenbuehl HP (1981). “Determinants of ejection performance in aortic stenosis”. Circulation. 64 (1): 126–34. PMID 7237709. Retrieved 2012-04-10. Unknown parameter
|month=ignored (help) - ↑ Marcus ML, Doty DB, Hiratzka LF, Wright CB, Eastham CL (1982). “Decreased coronary reserve: a mechanism for angina pectoris in patients with aortic stenosis and normal coronary arteries”. N Engl J Med. 307 (22): 1362–6. doi:10.1056/NEJM198211253072202. PMID 6215582.
- ↑ Carabello BA (2002). “Clinical practice. Aortic stenosis”. N Engl J Med. 346 (9): 677–82. doi:10.1056/NEJMcp010846. PMID 11870246.
- ↑ Yarbrough WM, Mukherjee R, Ikonomidis JS, Zile MR, Spinale FG (2012). “Myocardial remodeling with aortic stenosis and after aortic valve replacement: mechanisms and future prognostic implications”. J Thorac Cardiovasc Surg. 143 (3): 656–64. doi:10.1016/j.jtcvs.2011.04.044. PMC 3210937. PMID 21762938.
- ↑ Jin XY, Pepper JR, Gibson DG (1996). “Effects of incoordination on left ventricular force-velocity relation in aortic stenosis”. Heart (British Cardiac Society). 76 (6): 495–501. PMC 484601. PMID 9014797. Retrieved 2012-04-10. Unknown parameter
|month=ignored (help) - ↑ Burup Kristensen C, Jensen JS, Sogaard P, Carstensen HG, Mogelvang R (2012). “Atrial fibrillation in aortic stenosis–echocardiographic assessment and prognostic importance”. Cardiovasc Ultrasound. 10: 38. doi:10.1186/1476-7120-10-38. PMC 3517318. PMID 23006976.
- ↑ Lilly LS (editor) (2003). Pathophysiology of Heart Disease (3rd ed. ed.). Lippincott Williams & Wilkins. ISBN 0-7817-4027-4.
- ↑ Laskey WK, Kussmaul WG (2001). “Subvalvular gradients in patients with valvular aortic stenosis: prevalence, magnitude, and physiological importance”. Circulation. 104 (9): 1019–22. PMID 11524395. Retrieved 2012-04-12. Unknown parameter
|month=ignored (help) - ↑ Branch KR, O’Brien KD, Otto CM (2002). “Aortic valve sclerosis as a marker of active atherosclerosis”. Curr Cardiol Rep. 4 (2): 111–7. PMID 11827633.
- ↑ {{Faggiano P, D’Aloia A, Antonini-Canterin F, Pinamonti B, DiLenarda A, Brentana L, Metra M, Nodari S, Dei Cas L. Usefulness of cardiac calcification on two-dimensional echocardiography for distinguishing ischemic from nonischemic dilated cardiomyopathy: a preliminary report. J Cardiovasc Med. 2006.}}
- ↑ 36.0 36.1 36.2 Bonow RO, Carabello BA, Chatterjee K, de Leon AC, Faxon DP, Freed MD; et al. (2008). “2008 focused update incorporated into the ACC/AHA 2006 guidelines for the management of patients with valvular heart disease: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to revise the 1998 guidelines for the management of patients with valvular heart disease). Endorsed by the Society of Cardiovascular Anesthesiologists, Society for Cardiovascular Angiography and Interventions, and Society of Thoracic Surgeons”. J Am Coll Cardiol. 52 (13): e1–142. doi:10.1016/j.jacc.2008.05.007. PMID 18848134.
- ↑ 37.0 37.1 Vahanian A, Alfieri O, Andreotti F, Antunes MJ, Baron-Esquivias G, Baumgartner H; et al. (2013). “[Guidelines on the management of valvular heart disease (version 2012). The Joint Task Force on the Management of Valvular Heart Disease of the European Society of Cardiology (ESC) and the European Association for Cardio-Thoracic Surgery (EACTS)]”. G Ital Cardiol (Rome). 14 (3): 167–214. doi:10.1714/1234.13659. PMID 23474606.
- ↑ 38.0 38.1 38.2 38.3 38.4 38.5 Pibarot P, Dumesnil JG (2012). “Low-flow, low-gradient aortic stenosis with normal and depressed left ventricular ejection fraction”. J Am Coll Cardiol. 60 (19): 1845–53. doi:10.1016/j.jacc.2012.06.051. PMID 23062546.
- ↑ Normand J, Loire R, Zambartas C (1988). “The anatomical aspects of adult aortic stenosis”. Eur Heart J. 9 Suppl E: 31–6. PMID 3402479.
- ↑ Towler DA (2013). “Molecular and cellular aspects of calcific aortic valve disease”. Circ Res. 113 (2): 198–208. doi:10.1161/CIRCRESAHA.113.300155. PMC 4057916. PMID 23833294.
Causes
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-In-Chief: Mohammed A. Sbeih, M.D. [2]; Lakshmi Gopalakrishnan, M.B.B.S. [3]; Vendhan Ramanujam M.B.B.S [4]; Usama Talib, BSc, MD [5] Mandana Chitsazan, M.D. [6] Assistant Editor-In-Chief: Kristin Feeney, B.S. [7]
Overview
Aortic stenosis can be either congenital or acquired, and its common causes vary between different age groups and between different populations. Rheumatic heart disease remains the most common cause of aortic stenosis worldwide. Calcification of the aortic valve is the most common cause of aortic stenosis in North America and Europe. While calcification of congenital bicuspid aortic valve is the most common cause of aortic stenosis in people less than 70 years of age, acquired degenerative calcific aortic stenosis is the most common cause in older patients above the age of 70 years.
Causes
Life Threatening Causes
Life-threatening causes include conditions which may result in death or permanent disability within 24 hours if left untreated. Aortic stenosis is a progressive disease and does not have a life threatening cause. However, complications resulting from untreated disease name is common.
Common Causes
Common causes of aortic stenosis may include:[1][2][3][4]
- Calcific aortic valve disease
- A congenitally abnormal aortic valve with superimposed calcification (unicuspid or bicuspid).
- Rheumatic heart disease
Causes by Location of Stenosis
Valvular Aortic Stenosis
- Acquired
- Congenital
- Bardet-Biedl syndrome[11]
- Bicuspid aortic valve[2]
- Fabry’s disease[12]
- Familial hypercholesterolemia[13]
- Familial thoracic aortic aneurysm syndrome[14]
- Hypoplastic aortic annulus[15]
- Subaortic stenosis short stature syndrome (Onat syndrome) [16]
- Quadricuspid aortic valve[17]
- Singleton-Merten syndrome[18]
- Sweet syndrome[19]
- Tricuspid aortic valve with commissural fushion[20]
- Turner syndrome[21]
- Unicuspid aortic valve[22]
Subvalvular Aortic Stenosis
- Familial subvalvular aortic stenosis[23]
- Hypertrophic cardiomyopathy[24]
- Idiopathic hypertrophic subaortic stenosis[25]
Supravalvular Aortic Stenosis
- Aortitis[26]
- Familial supravalvular aortic stenosis[27]
- Homozygous familial hypercholesterolemia[28]
- Hypoplastic left heart syndrome[29]
- Williams syndrome[30][31]
Causes by Age Groups
Under Age 70
- Bicuspid aortic valve[32]
- Rheumatic heart disease[33]
- Degenerative calcification[34]
- Uni-commissural aortic valve[22]
- Hypoplasia of the annulus[35]
Over Age 70
- Degenerative calcification[34]
- Bicuspid aortic valve[2]
- Rheumatic heart disease[36]
- Hypoplasia of the annulus[35]
Causes by Organ System
Causes in Alphabetical Order
References
- ↑ O’Brien KD (2006). “Pathogenesis of calcific aortic valve disease: a disease process comes of age (and a good deal more)”. Arteriosclerosis, Thrombosis, and Vascular Biology. 26 (8): 1721–8. doi:10.1161/01.ATV.0000227513.13697.ac. PMID 16709942. Retrieved 2012-04-11. Unknown parameter
|month=ignored (help) - ↑ 2.0 2.1 2.2 Mordi I, Tzemos N (2012). “Bicuspid aortic valve disease: a comprehensive review”. Cardiol Res Pract. 2012: 196037. doi:10.1155/2012/196037. PMC 3368178. PMID 22685681.
- ↑ Lugiano, CA. (2013). “Aortic stenosis”. JAAPA. 26 (11): 46–7. doi:10.1097/01.JAA.0000436518.69169.8e. PMID 24153092. Unknown parameter
|month=ignored (help) - ↑ 4.0 4.1 VOC=VITIUM ORGANICUM CORDIS, a compendium of the Department of Cardiology at Uppsala Academic Hospital. By Per Kvidal September 1999, with revision by Erik Björklund May 2008
- ↑ Hannoush H, Introne WJ, Chen MY, Lee SJ, O’Brien K, Suwannarat P; et al. (2012). “Aortic stenosis and vascular calcifications in alkaptonuria”. Mol Genet Metab. 105 (2): 198–202. doi:10.1016/j.ymgme.2011.10.017. PMC 3276068. PMID 22100375.
- ↑ Aronow, WS. (2013). “A review of the pathophysiology, diagnosis, and treatment of aortic valve stenosis in elderly patients”. Hosp Pract (1995). 41 (4): 66–77. doi:10.3810/hp.2013.10.1082. PMID 24145591. Unknown parameter
|month=ignored (help) - ↑ Moura LM, Maganti K, Puthumana JJ, Rocha-Gonçalves F, Rajamannan NM (2007). “New understanding about calcific aortic stenosis and opportunities for pharmacologic intervention”. Curr Opin Cardiol. 22 (6): 572–7. doi:10.1097/HCO.0b013e3282f0dae6. PMID 17921746.
- ↑ Strickberger SA, Schulman SP, Hutchins GM. Association of Paget’s disease of bone with calcific aortic valve disease. Am J Med 1987;82:953-6.
- ↑ Ong DS, Aertker RA, Clark AN, Kiefer T, Hughes GC, Harrison JK; et al. (2013). “Radiation-associated valvular heart disease”. J Heart Valve Dis. 22 (6): 883–92. PMID 24597417.
- ↑ Bert JS, Abdullah M, Dahle TG, Gertner E (2013). “Transcatheter aortic valve replacement for advanced valvular disease in active SLE and APS”. Lupus. 22 (10): 1046–9. doi:10.1177/0961203313498797. PMID 23884983.
- ↑ Beales PL, Elcioglu N, Woolf AS, Parker D, Flinter FA (1999). “New criteria for improved diagnosis of Bardet-Biedl syndrome: results of a population survey”. J Med Genet. 36 (6): 437–46. PMC 1734378. PMID 10874630.
- ↑ Nakao S, Takenaka T, Maeda M, Kodama C, Tanaka A, Tahara M; et al. (1995). “An atypical variant of Fabry’s disease in men with left ventricular hypertrophy”. N Engl J Med. 333 (5): 288–93. doi:10.1056/NEJM199508033330504. PMID 7596372.
- ↑ Sprecher DL, Schaefer EJ, Kent KM, Gregg RE, Zech LA, Hoeg JM; et al. (1984). “Cardiovascular features of homozygous familial hypercholesterolemia: analysis of 16 patients”. Am J Cardiol. 54 (1): 20–30. PMID 6331147.
- ↑ Loscalzo ML, Goh DL, Loeys B, Kent KC, Spevak PJ, Dietz HC (2007). “Familial thoracic aortic dilation and bicommissural aortic valve: a prospective analysis of natural history and inheritance”. Am J Med Genet A. 143A (17): 1960–7. doi:10.1002/ajmg.a.31872. PMID 17676603.
- ↑ REEVE, R.; ROBINSON, SJ. (1964). “HYPOPLASTIC ANNULUS–AN UNUSUAL TYPE OF AORTIC STENOSIS: A REPORT OF THREE CASES IN CHILDREN”. Dis Chest. 45: 99–102. PMID 14114644. Unknown parameter
|month=ignored (help) - ↑ “Subaortic stenosis short stature syndrome | Genetic and Rare Diseases Information Center (GARD) – an NCATS Program”.
- ↑ Yamagishi Y, Yuda S, Tsuchihashi K, Saitoh S, Miura T, Ura N; et al. (2007). “Quadricuspid aortic valve associated with aortic stenosis and regurgitation: report of a case and a review of the literature”. J Med Ultrason (2001). 34 (4): 197–200. doi:10.1007/s10396-007-0148-9. PMID 27278482.
- ↑ Feigenbaum A, Müller C, Yale C, Kleinheinz J, Jezewski P, Kehl HG; et al. (2013). “Singleton-Merten syndrome: an autosomal dominant disorder with variable expression”. Am J Med Genet A. 161A (2): 360–70. doi:10.1002/ajmg.a.35732. PMID 23322711.
- ↑ Cohen PR, Kurzrock R (2003). “Sweet’s syndrome revisited: a review of disease concepts”. Int J Dermatol. 42 (10): 761–78. PMID 14521689.
- ↑ Bedynek JL, Galioto FM, Leon DF (2000). “Tricuspid aortic valve with partial commissural fusion: prelminary report of an apparently common cause of aortic ejection sounds with potential for serious sequelae, illustrated by two cases”. Tex Heart Inst J. 27 (2): 201–5. PMC 101056. PMID 10928509.
- ↑ Noonan JA (1968). “Hypertelorism with Turner phenotype. A new syndrome with associated congenital heart disease”. Am J Dis Child. 116 (4): 373–80. PMID 4386970.
- ↑ 22.0 22.1 Kwon HJ, Park JH, Kim SS, Sun BJ, Jin SA, Kim JH; et al. (2016). “Severe Aortic Stenosis Associated with Unicommissural Unicuspid Aortic Valve in a Middle Aged Male”. J Cardiovasc Ultrasound. 24 (3): 247–250. doi:10.4250/jcu.2016.24.3.247. PMC 5050315. PMID 27721957.
- ↑ Stern, JA.; Meurs, KM.; Nelson, OL.; Lahmers, SM.; Lehmkuhl, LB. (2012). “Familial subvalvular aortic stenosis in golden retrievers: inheritance and echocardiographic findings”. J Small Anim Pract. 53 (4): 213–6. doi:10.1111/j.1748-5827.2011.01187.x. PMID 22417094. Unknown parameter
|month=ignored (help) - ↑ Varma PK, Neema PK (2014). “Hypertrophic cardiomyopathy: part 1 – introduction, pathology and pathophysiology”. Ann Card Anaesth. 17 (2): 118–24. doi:10.4103/0971-9784.129841. PMID 24732610.
- ↑ Clark CE, Henry WL, Epstein SE (1973). “Familial prevalence and genetic transmission of idiopathic hypertrophic subaortic stenosis”. N Engl J Med. 289 (14): 709–14. doi:10.1056/NEJM197310042891402. PMID 4737963.
- ↑ Sharma S, Bahl VK, Rajani M (1997). “Stent treatment of obstructing dissection after percutaneous transluminal angioplasty of aortic stenosis caused by nonspecific aortitis”. Cardiovasc Intervent Radiol. 20 (5): 377–9. PMID 9271649.
- ↑ Chiarella, F.; Bricarelli, FD.; Lupi, G.; Bellotti, P.; Domenicucci, S.; Vecchio, C. (1989). “Familial supravalvular aortic stenosis: a genetic study”. J Med Genet. 26 (2): 86–92. PMID 2918546. Unknown parameter
|month=ignored (help) - ↑ Giannakoulas, G.; Mouratoglou, SA.; Kelekis, A.; Hatzimiltiades, S.; Karvounis, H. “Supravalvular aortic stenosis in homozygous familial hypercholesterolemia”. Hellenic J Cardiol. 54 (5): 392–3. PMID 24100183.
- ↑ Norwood WI, Lang P, Casteneda AR, Campbell DN (1981). “Experience with operations for hypoplastic left heart syndrome”. J Thorac Cardiovasc Surg. 82 (4): 511–9. PMID 6168869.
- ↑ Deo, SV.; Burkhart, HM.; Dearani, JA.; Schaff, HV. (2013). “Supravalvar aortic stenosis: current surgical approaches and outcomes”. Expert Rev Cardiovasc Ther. 11 (7): 879–90. doi:10.1586/14779072.2013.811967. PMID 23895031. Unknown parameter
|month=ignored (help) - ↑ Morris CA, Demsey SA, Leonard CO, Dilts C, Blackburn BL (1988). “Natural history of Williams syndrome: physical characteristics”. J Pediatr. 113 (2): 318–26. PMID 2456379.
- ↑ Siu SC, Silversides CK (2010). “Bicuspid aortic valve disease”. J Am Coll Cardiol. 55 (25): 2789–800. doi:10.1016/j.jacc.2009.12.068. PMID 20579534.
- ↑ Kumar RK, Tandon R (2013). “Rheumatic fever & rheumatic heart disease: the last 50 years”. Indian J Med Res. 137 (4): 643–58. PMC 3724245. PMID 23703332.
- ↑ 34.0 34.1 Pawade TA, Newby DE, Dweck MR (2015). “Calcification in Aortic Stenosis: The Skeleton Key”. J Am Coll Cardiol. 66 (5): 561–77. doi:10.1016/j.jacc.2015.05.066. PMID 26227196.
- ↑ 35.0 35.1 Philip F, Faza NN, Schoenhagen P, Desai MY, Tuzcu EM, Svensson LG; et al. (2015). “Aortic annulus and root characteristics in severe aortic stenosis due to bicuspid aortic valve and tricuspid aortic valves: implications for transcatheter aortic valve therapies”. Catheter Cardiovasc Interv. 86 (2): E88–98. doi:10.1002/ccd.25948. PMID 25914355.
- ↑ Marijon E, Mirabel M, Celermajer DS, Jouven X (2012). “Rheumatic heart disease”. Lancet. 379 (9819): 953–64. doi:10.1016/S0140-6736(11)61171-9. PMID 22405798.
Differentiating Aortic Stenosis from other Diseases
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editors-In-Chief: Mohammed A. Sbeih, M.D. [2]; Usama Talib, BSc, MD [3] Assistant Editor-In-Chief: Kristin Feeney, B.S. [4]
Overview
Aortic stenosis must be differentiated from other cardiac or pulmonary causes of dyspnea, weakness, and dizziness. Furthermore, when left ventricular outflow tract obstruction is present, it is critical to identify whether the obstruction is subvalvular, valvular or supravalvular and whether there is hypertrophic cardiomyopathy (HOCM) or not.[1]
Differentiating Aortic Stenosis from other Diseases
Aortic stenosis must be differentiated from the following:[2][3][4][5][6][7][8][9][10][11][12][13][14][15][16][17][18][19][20][21][22][23][24]
| Diseases | History | Symptoms | Physical Examination | Murmur | Diagnosis | Other Findings | |||
|---|---|---|---|---|---|---|---|---|---|
| ECG | CXR | Echocardiogram | Cardiac Catheterization | ||||||
| Aortic stenosis |
|
|
|
|
Left ventricular hypertrophy:
|
|
|
Left heart catheterization:
|
|
| Mitral Stenosis |
|
|
|
|
|
|
|
Right heart catheterization:
Left heart catheterization:
|
|
| Mitral Regurgitation |
|
|
Palpation
Auscultation
|
|
|
Acute MR
Chronic MR
|
|
|
|
| Atrial septal defect |
|
|
Inspection
Palpation
Auscultation
|
|
|
|
|
|
|
| Left Atrial Myxoma |
|
|
Skin
Auscultation:
|
|
|
Rare findings:
|
|
|
|
| Prosthetic Valve Obstruction |
|
|
Ausculation
Muffling of murmur |
|
− | − |
|
Causes:
| |
| Cor Triatriatum |
|
|
Auscultation
Other findings
|
|
Non specific but may have
|
|
|
|
Types
|
| Congenital Mitral Stenosis |
|
Infants:
Older patients:
|
Auscultation
Other findings
|
Mild-Moderate
Severe
|
|
|
|
Very rare condition | |
| Supravalvular Ring Mitral Stenosis |
|
|
Auscultation:
Lungs: Fine, crepitant rales and rhonchi or wheezes may be present Heart: Murmur |
|
|
Supramitral ring:
Intramitral ring:
(Difficult to visualize membrane <1mm in size) |
|
Types
It is attached between the opening of the atrial appendage and the mitral annulus which helps in differentiating with Cor triatriatum sinister.
| |
References
- ↑ Cleland JG, Swedberg K, Follath F, Komajda M, Cohen-Solal A, Aguilar JC, Dietz R, Gavazzi A, Hobbs R, Korewicki J, Madeira HC, Moiseyev VS, Preda I, van Gilst WH, Widimsky J, Freemantle N, Eastaugh J, Mason J (2003). “The EuroHeart Failure survey programme– a survey on the quality of care among patients with heart failure in Europe. Part 1: patient characteristics and diagnosis”. European Heart Journal. 24 (5): 442–63. PMID 12633546. Retrieved 2012-04-11. Unknown parameter
|month=ignored (help) - ↑ Nassar PN, Hamdan RH (2011). “Cor Triatriatum Sinistrum: Classification and Imaging Modalities”. Eur J Cardiovasc Med. 1 (3): 84–87. doi:10.5083/ejcm.20424884.21. PMC 3286827. PMID 22379596.
- ↑ Roudaut R, Serri K, Lafitte S (2007). “Thrombosis of prosthetic heart valves: diagnosis and therapeutic considerations”. Heart. 93 (1): 137–42. doi:10.1136/hrt.2005.071183. PMC 1861363. PMID 17170355.
- ↑ Apostolakis EE, Baikoussis NG (2009). “Methods of estimation of mitral valve regurgitation for the cardiac surgeon”. J Cardiothorac Surg. 4: 34. doi:10.1186/1749-8090-4-34. PMC 2723095. PMID 19604402.
- ↑ Alboliras ET, Edwards WD, Driscoll DJ, Seward JB (1987). “Cor triatriatum dexter: two-dimensional echocardiographic diagnosis”. J Am Coll Cardiol. 9 (2): 334–7. PMID 3805524.
- ↑ Gibson DG, Honey M, Lennox SC (1974). “Cor triatriatum. Diagnosis by echocardiography”. Br Heart J. 36 (8): 835–8. PMC 458901. PMID 4412638.
- ↑ Cor triatrium https://radiopaedia.org/articles/cor-triatriatum (2016) Accessed on November 29, 2016
- ↑ Sosland RP, Vacek JL, Gorton ME (2007). “Congenital mitral stenosis: a rare presentation and novel approach to management”. J Thorac Cardiovasc Surg. 133 (2): 572–3. doi:10.1016/j.jtcvs.2006.10.025. PMID 17258606.
- ↑ Driscoll DJ, Gutgesell HP, McNamara DG (1978). “Echocardiographic features of congenital mitral stenosis”. Am J Cardiol. 42 (2): 259–66. PMID 685838.
- ↑ Bonou M, Lampropoulos K, Barbetseas J (2012). “Prosthetic heart valve obstruction: thrombolysis or surgical treatment?”. Eur Heart J Acute Cardiovasc Care. 1 (2): 122–7. doi:10.1177/2048872612451169. PMC 3760527. PMID 24062899.
- ↑ Maganti K, Rigolin VH, Sarano ME, Bonow RO (2010). “Valvular heart disease: diagnosis and management”. Mayo Clin Proc. 85 (5): 483–500. doi:10.4065/mcp.2009.0706. PMC 2861980. PMID 20435842.
- ↑ DEXTER L (1956). “Atrial septal defect”. Br Heart J. 18 (2): 209–25. PMC 479579. PMID 13315850.
- ↑ Webb G, Gatzoulis MA (2006). “Atrial septal defects in the adult: recent progress and overview”. Circulation. 114 (15): 1645–53. doi:10.1161/CIRCULATIONAHA.105.592055. PMID 17030704.
- ↑ Geva T, Martins JD, Wald RM (2014). “Atrial septal defects”. Lancet. 383 (9932): 1921–32. doi:10.1016/S0140-6736(13)62145-5. PMID 24725467.
- ↑ Demir M, Akpinar O, Acarturk E (2005). “Atrial myxoma: an unusual cause of myocardial infarction”. Tex Heart Inst J. 32 (3): 445–7. PMC 1336732. PMID 16392241.
- ↑ MacGowan SW, Sidhu P, Aherne T, Luke D, Wood AE, Neligan MC; et al. (1993). “Atrial myxoma: national incidence, diagnosis and surgical management”. Ir J Med Sci. 162 (6): 223–6. PMID 8407260.
- ↑ Circulation http://circ.ahajournals.org/content/119/7/1034 (2016) Accessed on December 7, 2016
- ↑ Alphonso N, Nørgaard MA, Newcomb A, d’Udekem Y, Brizard CP, Cochrane A (2005). “Cor triatriatum: presentation, diagnosis and long-term surgical results”. Ann Thorac Surg. 80 (5): 1666–71. doi:10.1016/j.athoracsur.2005.04.055. PMID 16242436.
- ↑ circulation http://circ.ahajournals.org/content/36/1/101 (1967) Accessed on 7 December, 2016
- ↑ Moore P, Adatia I, Spevak PJ, Keane JF, Perry SB, Castaneda AR; et al. (1994). “Severe congenital mitral stenosis in infants”. Circulation. 89 (5): 2099–106. PMID 8181134.
- ↑ Uva MS, Galletti L, Gayet FL, Piot D, Serraf A, Bruniaux J; et al. (1995). “Surgery for congenital mitral valve disease in the first year of life”. J Thorac Cardiovasc Surg. 109 (1): 164–74, discussion 174-6. doi:10.1016/S0022-5223(95)70432-9. PMID 7815793.
- ↑ Banerjee A, Kohl T, Silverman NH (1995). “Echocardiographic evaluation of congenital mitral valve anomalies in children”. Am J Cardiol. 76 (17): 1284–91. PMID 7503011.
- ↑ Sullivan ID, Robinson PJ, de Leval M, Graham TP (1986). “Membranous supravalvular mitral stenosis: a treatable form of congenital heart disease”. J Am Coll Cardiol. 8 (1): 159–64. PMID 3711511.
- ↑ Subramaniam V, Herle A, Mohammed N, Thahir M (2011). “Ortner’s syndrome: case series and literature review”. Braz J Otorhinolaryngol. 77 (5): 559–62. PMID 22030961.
Epidemiology and Demographics
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-In-Chief: Mohammed A. Sbeih, M.D. [2]; Lakshmi Gopalakrishnan, M.B.B.S. [3]; Usama Talib, BSc, MD [4] Assistant Editor-In-Chief: Kristin Feeney, B.S. [5]
Overview
Aortic stenosis is a major health problem that primarily affects the elderly. The majority of cases of aortic stenosis is due to calcific degeneration. Aortic stenosis tends to affect approximately 1% of patients over the age of 65, 2% of patients over the age of 75, and 4% of patients over the age 85.[1] As North American and European populations continue to live longer, aortic stenosis has major public health implications. Abnormalities of aortic valve morphology and function represent the most common valvular lesion in the elderly.[2]
Epidemiology and Demographics
Prevalence
- The prevalence of aortic stenosis is approximately 3% in adults over 75 years.[3]
- According to the Cardiovascular Health Study, the prevalence of aortic stenosis among patients more than 65 years of age is approximately 2% in the United States.[1]
- Based on the results from the EuroHeart Failure survey programme, 4.8% of patients with acute coronary syndrome had significant valve disease, in particular calcific aortic stenosis.[4]
Age
The prevalence of aortic stenosis increases with age. Less than 1% of all live births exhibit symptoms of severe aortic stenosis. Approximately 1% of patients over the age of 65, 2% of patients over the age of 75, and 4% of patients over the age of 85 have aortic stenosis.[1][5]
Gender
Calcific degenerative aortic stenosis is more common in males.[6]
Developed Countries
In North America and Europe, a linear relationship exists between the increase in the incidence of aortic stenosis and the increase in aging population.[7]
References
- ↑ 1.0 1.1 1.2 Stewart BF, Siscovick D, Lind BK, Gardin JM, Gottdiener JS, Smith VE, Kitzman DW, Otto CM (1997). “Clinical factors associated with calcific aortic valve disease. Cardiovascular Health Study”. Journal of the American College of Cardiology. 29 (3): 630–4. PMID 9060903. Retrieved 2012-04-11. Unknown parameter
|month=ignored (help) - ↑ Iivanainen AM, Lindroos M, Tilvis R, Heikkilä J, Kupari M (1996). “Natural history of aortic valve stenosis of varying severity in the elderly”. Am J Cardiol. 78 (1): 97–101. PMID 8712130.
- ↑ Carità P, Coppola G, Novo G, Caccamo G, Guglielmo M, Balasus F; et al. (2016). “Aortic stenosis: insights on pathogenesis and clinical implications”. J Geriatr Cardiol. 13 (6): 489–98. doi:10.11909/j.issn.1671-5411.2016.06.001. PMC 4987417. PMID 27582763.
- ↑ Cleland JG, Swedberg K, Follath F, Komajda M, Cohen-Solal A, Aguilar JC, Dietz R, Gavazzi A, Hobbs R, Korewicki J, Madeira HC, Moiseyev VS, Preda I, van Gilst WH, Widimsky J, Freemantle N, Eastaugh J, Mason J (2003). “The EuroHeart Failure survey programme– a survey on the quality of care among patients with heart failure in Europe. Part 1: patient characteristics and diagnosis”. European Heart Journal. 24 (5): 442–63. PMID 12633546. Retrieved 2012-04-11. Unknown parameter
|month=ignored (help) - ↑ Lindroos M, Kupari M, Heikkilä J, Tilvis R (1993). “Prevalence of aortic valve abnormalities in the elderly: an echocardiographic study of a random population sample”. Journal of the American College of Cardiology. 21 (5): 1220–5. PMID 8459080. Retrieved 2012-04-11. Unknown parameter
|month=ignored (help) - ↑ Townsend CM, et al. Sabiston Textbook of Surgery. 18th ed. Saunders; 2008:1841-1844.
- ↑ Otto CM, Prendergast B (2014). “Aortic-valve stenosis–from patients at risk to severe valve obstruction”. N Engl J Med. 371 (8): 744–56. doi:10.1056/NEJMra1313875. PMID 25140960.
Risk Factors
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editors-In-Chief: Mohammed A. Sbeih, M.D. [2]; Usama Talib, BSc, MD [3] Assistant Editor-In-Chief: Kristin Feeney, B.S. [4]
Overview
The most common risk factor for the development of aortic stenosis is the presence of a congenital bicuspid aortic valve. Risk factors that may speed up the progression of aortic stenosis include the same risk factors as atherosclerosis.
Risk Factors
Common Risk Factors
Common risk factors in the development of aortic stenosis include:[1][2][3][4]
- Congenital bicuspid aortic valve that may subsequently become calcified later in life
- Acute rheumatic fever
- Age-related progressive calcification of the normal tricuspid aortic valve
Less common Risk Factors
Less common risk factors in the development of aortic stenosis include:[5][6][7][8]
Other Risk Factors
Some other risk factors of aortic stenosis include:[9][10][11]
- Radiation therapy for cancer, such as breast cancer or lymphoma
- High lipoprotein a
- Disorders of calcium metabolism
References
- ↑ Siu SC, Silversides CK (2010). “Bicuspid aortic valve disease”. J Am Coll Cardiol. 55 (25): 2789–800. doi:10.1016/j.jacc.2009.12.068. PMID 20579534.
- ↑ Mylonakis E, Calderwood SB (2001). “Infective endocarditis in adults”. N Engl J Med. 345 (18): 1318–30. doi:10.1056/NEJMra010082. PMID 11794152.
- ↑ Lugiano, CA. (2013). “Aortic stenosis”. JAAPA. 26 (11): 46–7. doi:10.1097/01.JAA.0000436518.69169.8e. PMID 24153092. Unknown parameter
|month=ignored (help) - ↑ Pawade TA, Newby DE, Dweck MR (2015). “Calcification in Aortic Stenosis: The Skeleton Key”. J Am Coll Cardiol. 66 (5): 561–77. doi:10.1016/j.jacc.2015.05.066. PMID 26227196.
- ↑ Aronow WS, Schwartz KS, Koenigsberg M (1987). “Correlation of serum lipids, calcium, and phosphorus, diabetes mellitus and history of systemic hypertension with presence or absence of calcified or thickened aortic cusps or root in elderly patients”. Am J Cardiol. 59 (9): 998–9. PMID 3565291.
- ↑ Lindroos M, Kupari M, Valvanne J, Strandberg T, Heikkilä J, Tilvis R (1994). “Factors associated with calcific aortic valve degeneration in the elderly”. Eur Heart J. 15 (7): 865–70. PMID 7925504.
- ↑ Olsson M, Thyberg J, Nilsson J (1999). “Presence of oxidized low density lipoprotein in nonrheumatic stenotic aortic valves”. Arterioscler Thromb Vasc Biol. 19 (5): 1218–22. PMID 10323772.
- ↑ Maher ER, Pazianas M, Curtis JR (1987). “Calcific aortic stenosis: a complication of chronic uraemia”. Nephron. 47 (2): 119–22. PMID 3696315.
- ↑ Hull MC, Morris CG, Pepine CJ, Mendenhall NP (2003). “Valvular dysfunction and carotid, subclavian, and coronary artery disease in survivors of hodgkin lymphoma treated with radiation therapy”. JAMA. 290 (21): 2831–7. doi:10.1001/jama.290.21.2831. PMID 14657067.
- ↑ Gotoh T, Kuroda T, Yamasawa M, Nishinaga M, Mitsuhashi T, Seino Y; et al. (1995). “Correlation between lipoprotein(a) and aortic valve sclerosis assessed by echocardiography (the JMS Cardiac Echo and Cohort Study)”. Am J Cardiol. 76 (12): 928–32. PMID 7484833.
- ↑ Linefsky JP, O’Brien KD, Katz R, de Boer IH, Barasch E, Jenny NS; et al. (2011). “Association of serum phosphate levels with aortic valve sclerosis and annular calcification: the cardiovascular health study”. J Am Coll Cardiol. 58 (3): 291–7. doi:10.1016/j.jacc.2010.11.073. PMC 3147295. PMID 21737022.
Natural History, Complications and Prognosis
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editors-In-Chief: Mohammed A. Sbeih, M.D. [2]; Lakshmi Gopalakrishnan, M.B.B.S. [3]; Usama Talib, BSc, MD [4]
Overview
Left untreated, aortic valve stenosis can lead to angina, syncope, congestive heart failure, atrial fibrillation, endocarditis, and sudden cardiac death. Surgical treatment of aortic stenosis also carries risks and potential complications that include vascular complications and mitral valve injury. When aortic stenosis is left untreated, the average survival is 5 years after the onset of angina, 3 years after the onset of syncope, and 1 year after the onset of congestive heart failure.[1][2][3]
Natural History, Complications, and Prognosis
Natural History
Degenerative Calcific Aortic Stenosis
- Aortic stenosis due to the degeneration of a calcified aortic valve has a prolonged latent period during which symptoms are minimal or even lacking. This form of aortic stenosis presents later in life, usually after the age of 75. [4][5]
- Once moderate aortic stenosis is present and symptomatic, the average rate of progression of the valvular stenosis is a decrease in the valve area of 0.1 cm2 per year.[5][6]
- In addition, there is an increase in the jet velocity of 0.3 m/second per year and an increase in the mean pressure gradient of 7 mm Hg per year.[7][8][9]
- There is a tremendous individual variability in the rate of progression of aortic stenosis. Risk factors for atherosclerosis (such as age, smoking, hypertension, obesity and diabetes, lipid abnormalities, chronic renal failure and dialysis) and atherosclerotic disease itself (such as concomitant coronary artery disease) are associated with more rapid rates of progression of the severity of the aortic stenosis.[10]
Aortic Stenosis Due to Rheumatic Heart Disease
- The aortic stenosis due to rheumatic heart disease is amongst the most common causes of aortic stenosis. It is calculated to be around 24% of the total prevalence.[11]
Bicuspid Aortic Valve Disease
- Bicuspid aortic valve stenosis presents one or two decades earlier than the tricuspid aortic valve.
- The rate of progression of degenerative aortic stenosis can be faster in patients with bicuspid aortic valve than in those with congenital or rheumatic disease.[12][13]
- Bicuspid aortic valve functions without any significant pressure gradient during childhood. However, the thickening and calcification of the valves may be detectable pathologically and on echocardiography by the second decade.[14]
- Approximately 75% of bicuspid aortic valves progress into aortic stenosis requiring operative correction.[15][16]
- Bicuspid aortic stenosis progressively leads to heart failure, arrythmias, angina and other symptoms. These symptoms generally manifests between 40 to 60 years of age, which is relatively a younger age than that of the manifestation of the symptoms caused by aortic stenosis. However, children who develop early pathological changes in bicuspid aortic valve are more likely to develop aortic insufficiency than stenosis.[15]
Aortic Sclerosis
- Aortic sclerosis (defined as aortic valve thickening without obstruction to ventricular outflow) may progress to narrowing of the aortic valve or aortic stenosis. The decrease in pulse pressure or upstroke of the pulse in a patient with aortic sclerosis is a sign of progression to aortic stenosis.[17]
Complications
Degenerative Calcific Aortic Stenosis
If left untreated, aortic stenosis may lead to complications such as angina, syncope, or heart failure. A complete list of complications of aortic stenosis includes the following:[18][19][20][21][22]
- Congestive heart failure, particularly left-sided heart failure or systolic dysfunction[23][24][25][26][27][28]
- Left ventricular hypertrophy[29][30][31][32]
- Angina
- Arrhythmias
- Bleeding: Impaired platelet function and coagulation abnormalities, as decreased levels of Von Willebrand factor, can be seen in most patients with severe AS. This resolves after valve replacement procedure. 20% of patients have clinical bleeding, most often epistaxis or ecchymoses. Aortic stenosis may result in a form of von Willebrand disease due to an increased turbulence around the stenosed aortic valve which subsequently triggers a break down of coagulation factor VIII-associated antigen, (also called von Willebrand factor) and results in a variant of von Willebrand disease.
- Hypertension
- Endocarditis
- Fainting or syncope: Since the stenosed aortic valve may limit the heart’s output, people with aortic stenosis are at risk of syncope and dangerously low blood pressure with the use of some common medications. Ironically, these same medicines are used to treat a variety of cardiovascular diseases, many of which may co-exist with aortic stenosis. Examples include nitroglycerin, nitrates, ACE inhibitors, terazosin (Hytrin), and hydralazine. Note that all of these substances lead to peripheral vasodilation. Normally, however, in the absence of aortic stenosis, the heart is able to increase its output and thereby offset the effect of the dilated blood vessels. However, some cases of aortic stenosis can be associated with outflow blood obstruction which can prevent an increase of the cardiac output. Hence, low blood pressure or syncope may ensue.
- Left ventricular hypertrophy
- Myocardial infarction
Bicuspid Aortic Valve Disease
Bicuspid aortic valve disease is associated with the following complications:[15][16][33][34][35][36]
- Aortic stenosis in the majority of patients (75%)
- Aortic insufficiency
- Endocarditis
- Aortic aneurysm
- Aortic dissection
- Sudden death can occur in children during and immediately after exertion especially among those with pressure gradient > 50 mm Hg across the aortic valve
Prognosis
Asymptomatic Patients
- The prognosis of patients with aortic stenosis who do not have symptoms is quite good. The annual mortality rate is < 1% per year in asymptomatic patients.ref>Lancellotti P, Magne J, Donal E, et al. Clinical outcome in asymptomatic severe aortic stenosis insights from the new proposed aortic stenosis grading classification. J Am Coll Cardiol. Jan 17 2012;59(3):235-43.</ref>
- Only 4% of sudden cardiac deaths that occur in patients with aortic stenosis occur in those patients who are asymptomatic.
Symptomatic Patients
- Medical treatment of newly diagnosed moderate to severe symptomatic aortic stenosis is associated with a 25% mortality at one year and a 50% mortality at two years. Half of the deaths are due to sudden cardiac death.[1][37][38]
- When aortic stenosis is left untreated, the average survival is 5 years after the onset of angina, 3 years after the onset of syncope, and 1 year after the onset of congestive heart failure.[1][2][3]
Low Flow, Low Gradient Aortic Stenosis with Low Ejection Fraction
In low flow, low gradient, low ejection fraction aortic stenosis, the aortic valve area should increase to more than 1.2 cm2 and the mean pressure gradient should rise above 30 mm Hg following infusion with dobutamine. While early surgical mortality is 32–33% in patients who fail to achieve these improvements with dobutamine infusions, it is only 5–7% in patients who demonstrate an increase in their contractility and gradient. Five years survival after surgery was 88% in patients with improved contractility and only 10–25% in patients with unimproved contractility after dobutamine infusion.[39]
References
- ↑ 1.0 1.1 1.2 Ross J, Braunwald E (1968). “Aortic stenosis”. Circulation. 38 (1 Suppl): 61–7. PMID 4894151.
- ↑ 2.0 2.1 Kelly TA, Rothbart RM, Cooper CM, Kaiser DL, Smucker ML, Gibson RS (1988). “Comparison of outcome of asymptomatic to symptomatic patients older than 20 years of age with valvular aortic stenosis”. Am J Cardiol. 61 (1): 123–30. PMID 3337000.
- ↑ 3.0 3.1 Iivanainen AM, Lindroos M, Tilvis R, Heikkilä J, Kupari M (1996). “Natural history of aortic valve stenosis of varying severity in the elderly”. Am J Cardiol. 78 (1): 97–101. PMID 8712130.
- ↑ Townsend CM, et al. Sabiston Textbook of Surgery. 18th ed. Saunders; 2008:1841-1844.
- ↑ 5.0 5.1 Faggiano P, Aurigemma GP, Rusconi C, Gaasch WH (1996). “Progression of valvular aortic stenosis in adults: literature review and clinical implications”. Am Heart J. 132 (2 Pt 1): 408–17. PMID 8701905.
- ↑ Baumgartner H, Hung J, Bermejo J, Chambers JB, Evangelista A, Griffin BP; et al. (2009). “Echocardiographic assessment of valve stenosis: EAE/ASE recommendations for clinical practice”. J Am Soc Echocardiogr. 22 (1): 1–23, quiz 101-2. doi:10.1016/j.echo.2008.11.029. PMID 19130998.
- ↑ Cheitlin MD, Gertz EW, Brundage BH, Carlson CJ, Quash JA, Bode RS (1979). “Rate of progression of severity of valvular aortic stenosis in the adult”. Am Heart J. 98 (6): 689–700. PMID 495418.
- ↑ Jonasson R, Jonsson B, Nordlander R, Orinius E, Szamosi A (1983). “Rate of progression of severity of valvular aortic stenosis”. Acta Med Scand. 213 (1): 51–4. PMID 6829320.
- ↑ Peter M, Hoffmann A, Parker C, Lüscher T, Burckhardt D (1993). “Progression of aortic stenosis. Role of age and concomitant coronary artery disease”. Chest. 103 (6): 1715–9. PMID 8404089.
- ↑ Mohler ER, Sheridan MJ, Nichols R, Harvey WP, Waller BF (1991). “Development and progression of aortic valve stenosis: atherosclerosis risk factors–a causal relationship? A clinical morphologic study”. Clin Cardiol. 14 (12): 995–9. PMID 1841025.
- ↑ Passik CS, Ackermann DM, Pluth JR, Edwards WD (1987). “Temporal changes in the causes of aortic stenosis: a surgical pathologic study of 646 cases”. Mayo Clin Proc. 62 (2): 119–23. PMID 3807436.
- ↑ Kamath AR, Pai RG (2008). “Risk factors for progression of calcific aortic stenosis and potential therapeutic targets”. Int J Angiol. 17 (2): 63–70. PMC 2728414. PMID 22477390.
- ↑ Rosenhek R, Binder T, Porenta G, Lang I, Christ G, Schemper M; et al. (2000). “Predictors of outcome in severe, asymptomatic aortic stenosis”. N Engl J Med. 343 (9): 611–7. doi:10.1056/NEJM200008313430903. PMID 10965007.
- ↑ Beppu S, Suzuki S, Matsuda H, Ohmori F, Nagata S, Miyatake K (1993). “Rapidity of progression of aortic stenosis in patients with congenital bicuspid aortic valves”. The American Journal of Cardiology. 71 (4): 322–7. PMID 8427176. Unknown parameter
|month=ignored (help);|access-date=requires|url=(help) - ↑ 15.0 15.1 15.2 Fenoglio JJ, McAllister HA, DeCastro CM, Davia JE, Cheitlin MD (1977). “Congenital bicuspid aortic valve after age 20”. The American Journal of Cardiology. 39 (2): 164–9. PMID 835475. Unknown parameter
|month=ignored (help);|access-date=requires|url=(help) - ↑ 16.0 16.1 Lewin MB, Otto CM (2005). “The bicuspid aortic valve: adverse outcomes from infancy to old age”. Circulation. 111 (7): 832–4. doi:10.1161/01.CIR.0000157137.59691.0B. PMID 15723989. Retrieved 2012-04-10. Unknown parameter
|month=ignored (help) - ↑ Di Minno MN, Di Minno A, Songia P, Ambrosino P, Gripari P, Ravani A; et al. (2016). “Markers of subclinical atherosclerosis in patients with aortic valve sclerosis: A meta-analysis of literature studies”. Int J Cardiol. 223: 364–370. doi:10.1016/j.ijcard.2016.08.122. PMID 27543711.
- ↑ S. Frank, A. Johnson & J. Jr Ross (1973). “Natural history of valvular aortic stenosis”. British heart journal. 35 (1): 41–46. PMID 4685905. Unknown parameter
|month=ignored (help) - ↑ Charlotte Burup Kristensen, Jan Skov Jensen, Peter Sogaard, Helle Gervig Carstensen & Rasmus Mogelvang (2012). “Atrial fibrillation in aortic stenosis–echocardiographic assessment and prognostic importance”. Cardiovascular ultrasound. 10: 38. doi:10.1186/1476-7120-10-38. PMID 23006976. Unknown parameter
|month=ignored (help) - ↑ R. R. Wolfe, D. J. Driscoll, W. M. Gersony, C. J. Hayes, J. F. Keane, L. Kidd, W. M. O’Fallon, D. R. Pieroni & W. H. Weidman (1993). “Arrhythmias in patients with valvar aortic stenosis, valvar pulmonary stenosis, and ventricular septal defect. Results of 24-hour ECG monitoring”. Circulation. 87 (2 Suppl): I89–101. PMID 8425327. Unknown parameter
|month=ignored (help) - ↑ “Abstracts of the 36th Annual Meeting of the Society of General Internal Medicine. April 24-27, 2013. Denver, Colorado, USA”. J Gen Intern Med. 28 Suppl 1: S1–489. 2013. doi:10.1007/s11606-013-2436-y. PMC 3654146. PMID 23625304.
- ↑ Vincentelli A, Susen S, Le Tourneau T, Six I, Fabre O, Juthier F; et al. (2003). “Acquired von Willebrand syndrome in aortic stenosis”. N Engl J Med. 349 (4): 343–9. doi:10.1056/NEJMoa022831. PMID 12878741.
- ↑ Antonini-Canterin F, Popescu BA, Popescu AC, Beladan CC, Korcova R, Piazza R; et al. (2008). “Heart failure in patients with aortic stenosis: clinical and prognostic significance of carbohydrate antigen 125 and brain natriuretic peptide measurement”. Int J Cardiol. 128 (3): 406–12. doi:10.1016/j.ijcard.2007.05.039. PMID 17662495.
- ↑ C. M. Otto, I. G. Burwash, M. E. Legget, B. I. Munt, M. Fujioka, N. L. Healy, C. D. Kraft, C. Y. Miyake-Hull & R. G. Schwaegler (1997). “Prospective study of asymptomatic valvular aortic stenosis. Clinical, echocardiographic, and exercise predictors of outcome”. Circulation. 95 (9): 2262–2270. PMID 9142003. Unknown parameter
|month=ignored (help) - ↑ Kim YJ (2016). “BR 02-1 MANAGEMENT OF HYPERTENSION IN SEVERE AORTIC STENOSIS”. J Hypertens. 34 Suppl 1 – ISH 2016 Abstract Book: e30. doi:10.1097/01.hjh.0000499936.94867.5f. PMID 27753861.
- ↑ W. M. Gersony, C. J. Hayes, D. J. Driscoll, J. F. Keane, L. Kidd, W. M. O’Fallon, D. R. Pieroni, R. R. Wolfe & W. H. Weidman (1993). “Bacterial endocarditis in patients with aortic stenosis, pulmonary stenosis, or ventricular septal defect”. Circulation. 87 (2 Suppl): I121–I126. PMID 8425318. Unknown parameter
|month=ignored (help) - ↑ Taneja I, Marney A, Robertson D (2004). “Aortic stenosis and autonomic dysfunction: co-conspirators in syncope”. Am J Med Sci. 327 (5): 281–3. PMID 15166752.
- ↑ S. Frank, A. Johnson & J. Jr Ross (1973). “Natural history of valvular aortic stenosis”. British heart journal. 35 (1): 41–46. PMID 4685905. Unknown parameter
|month=ignored (help) - ↑ Markku Kupari, Heikki Turto & Jyri Lommi (2005). “Left ventricular hypertrophy in aortic valve stenosis: preventive or promotive of systolic dysfunction and heart failure?”. European heart journal. 26 (17): 1790–1796. doi:10.1093/eurheartj/ehi290. PMID 15860517. Unknown parameter
|month=ignored (help) - ↑ Markku Kupari, Heikki Turto & Jyri Lommi (2005). “Left ventricular hypertrophy in aortic valve stenosis: preventive or promotive of systolic dysfunction and heart failure?”. European heart journal. 26 (17): 1790–1796. doi:10.1093/eurheartj/ehi290. PMID 15860517. Unknown parameter
|month=ignored (help) - ↑ Zasada W, Chyrchel M, Bobrowska B, Dudek D (2013). “Non-ST elevation myocardial infarction in a patient with severe degenerative aortic stenosis”. Kardiol Pol. 71 (9): 986–7. doi:10.5603/KP.2013.0239. PMID 24065303.
- ↑ C. M. Otto, I. G. Burwash, M. E. Legget, B. I. Munt, M. Fujioka, N. L. Healy, C. D. Kraft, C. Y. Miyake-Hull & R. G. Schwaegler (1997). “Prospective study of asymptomatic valvular aortic stenosis. Clinical, echocardiographic, and exercise predictors of outcome”. Circulation. 95 (9): 2262–2270. PMID 9142003. Unknown parameter
|month=ignored (help) - ↑ Keane MG, Wiegers SE, Plappert T, Pochettino A, Bavaria JE, Sutton MG (2000). “Bicuspid aortic valves are associated with aortic dilatation out of proportion to coexistent valvular lesions”. Circulation. 102 (19 Suppl 3): III35–9. PMID 11082359. Retrieved 2012-04-10. Unknown parameter
|month=ignored (help) - ↑ Roberts WC, Morrow AG, McIntosh CL, Jones M, Epstein SE (1981). “Congenitally bicuspid aortic valve causing severe, pure aortic regurgitation without superimposed infective endocarditis. Analysis of 13 patients requiring aortic valve replacement”. The American Journal of Cardiology. 47 (2): 206–9. PMID 7468467. Unknown parameter
|month=ignored (help);|access-date=requires|url=(help) - ↑ Gersony WM, Hayes CJ, Driscoll DJ, Keane JF, Kidd L, O’Fallon WM, Pieroni DR, Wolfe RR, Weidman WH (1993). “Bacterial endocarditis in patients with aortic stenosis, pulmonary stenosis, or ventricular septal defect”. Circulation. 87 (2 Suppl): I121–6. PMID 8425318. Unknown parameter
|month=ignored (help);|access-date=requires|url=(help) - ↑ Keane JF, Driscoll DJ, Gersony WM, Hayes CJ, Kidd L, O’Fallon WM, Pieroni DR, Wolfe RR, Weidman WH (1993). “Second natural history study of congenital heart defects. Results of treatment of patients with aortic valvar stenosis”. Circulation. 87 (2 Suppl): I16–27. PMID 8425319. Unknown parameter
|month=ignored (help);|access-date=requires|url=(help) - ↑ Chizner MA, Pearle DL, deLeon AC (1980). “The natural history of aortic stenosis in adults”. Am Heart J. 99 (4): 419–24. PMID 7189084.
- ↑ Rashedi N, Otto CM (2015). “Aortic Stenosis: Changing Disease Concepts”. J Cardiovasc Ultrasound. 23 (2): 59–69. doi:10.4250/jcu.2015.23.2.59. PMC 4486179. PMID 26140146.
- ↑ Nishimura RA, Grantham JA, Connolly HM, Schaff HV, Higano ST, Holmes DR (2002). “Low-output, low-gradient aortic stenosis in patients with depressed left ventricular systolic function: the clinical utility of the dobutamine challenge in the catheterization laboratory”. Circulation. 106 (7): 809–13. PMID 12176952.
Diagnosis
Diagnosis
History and Symptoms | Physical Examination | Cardiac Stress Test | Electrocardiogram | Chest X Ray | CT | MRI | Echocardiography | Cardiac Catheterization | Aortic Valve Area | Aortic Valve Area Calculation
Treatment
Treatment
General Approach | Medical Therapy | Surgery | Percutaneous Aortic Balloon Valvotomy (PABV) or Aortic Valvuloplasty | Transcatheter aortic valve implantation (TAVI) | TAVI Procedure Guide | Lankmark Trials | Follow Up | Prevention | Precautions and Prophylaxis | Cost-Effectiveness of Therapy | Future or Investigational Therapies | Appropriate Use Criteria
Related Chapters
Related Chapters
Looking for the patient version?
© 2026 MyEClinic – IFTM Institut für Telematik in der Medizin GmbH