
Congestive heart failure chest x ray
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-In-Chief: Lakshmi Gopalakrishnan, M.B.B.S. [2] Edzel Lorraine Co, DMD, MD[3]
Overview
Overview
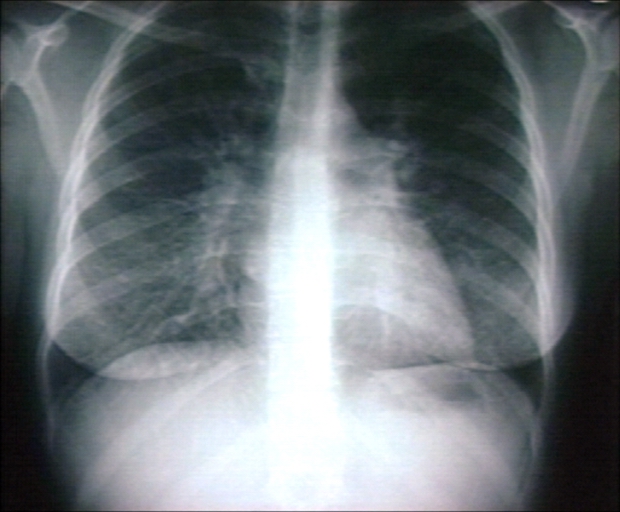
Chest x-ray in a patient with heart failure shows cardiomegaly (cardiac enlargement and pulmonary congestion (Kerley B lines, and in some cases pleural effusion).
Chest X Ray
Chest X Ray
- Since the left ventricle often dilates in the anteroposterior direction, the cardiac silhouette may appear deceptively normal.
- Chest x-ray findings include:
- Kerley B lines or thickening of the interlobular septa
- Peribronchial cuffing
- Thickening of the fissures
- Cephalization
- Increased vascular markings
- Interstitial edema
- Pleural effusions
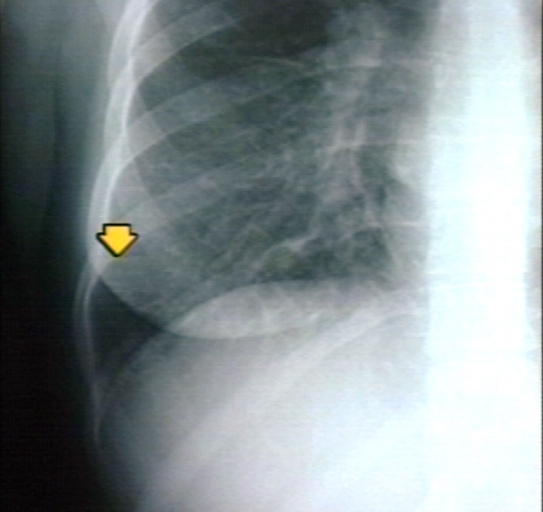
Kerley B Lines
Kerley B lines are short parallel lines at the lung periphery. These lines represent distended interlobular septa, which are usually less than 1 cm in length and parallel to one another at right angles to the pleura. They are located peripherally in contact with the pleura, but are generally absent along fissural surfaces. They may be seen in any zone but are most frequently observed at the lung bases at the costophrenic angles on the PA radiograph, and in the substernal region on lateral radiographs.
-
 Plain film: Mitral stenosis, Kerley B lines
Plain film: Mitral stenosis, Kerley B lines -
 Plain film: Mitral stenosis, Kerley B lines
Plain film: Mitral stenosis, Kerley B lines -
 Plain film: Mitral stenosis, Kerley B lines
Plain film: Mitral stenosis, Kerley B lines



Peribronchial Cuffing

Peribronchial cuffing is an abnormality on a chest x-ray whereby the usually thin bronchial walls are thickened and take on a doughnut-like appearance.

Cephalization refers to the redistribution of blood into the upper lobe vessels. It has been hypothesized that once the hydrostatic pressure exceeds 10 mm Hg, then fluid begins to leak into the interstitium of the lung. This excess fluid initially compresses the lower lobe vessels, perhaps as a result of gravity. After this, the upper lobe vessels are recruited to distribute a greater volume of blood. In order to carry a greater volume of blood, the upper lobe vessels increase in size.
Differentiating Cardiogenic Versus Noncardiogenic Pulmonary Edema
Differentiating Cardiogenic Versus Noncardiogenic Pulmonary Edema

Cardiogenic pulmonary edema can be distinguished from noncardiogenic pulmonary edema by the presence of redistribution of blood flow to the upper lobes (increased blood flow to the higher parts of the lung) and interstitial edema.
Noncardiogenic Pulmonary Edema

In contrast, patchy alveolar infiltrates with air bronchograms are more indicative of noncardiogenic edema.
Correlation of Chest X-Ray Findings with Pulmonary Capillary Wedge Pressure
Correlation of Chest X-Ray Findings with Pulmonary Capillary Wedge Pressure
- Normal: 5-10 mm Hg
- Cephalization: 10-15 mm Hg
- Kerley B Lines: 15-20 mm Hg
- Pulmonary Interstitial Edema: 20-25 mm Hg
- Pulmonary Alveolar Edema: > 25 mm Hg

Template:Interventions infobox
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]
Overview
A chest X-ray, commonly abbreviated CXR, is a projection radiograph (X-ray), taken by a radiographer, of the thorax which is used to diagnose problems with that area.
Problems identified through chest x-rays
Examples of such problems include but are not limited to:
- Pneumothorax, sometimes tension pneumothorax (though this is usually diagnosed clinically because of its acute nature)
- Rib fracture
- Air space disease/consolidation (e.g. pneumonia)
- Interstitial lung disease (e.g. idiopathic pulmonary fibrosis (IPF), lung cancer, active tuberculosis)
- Cardiac silhouette enlargement – congestive heart failure, pericardial effusion, hypertrophic cardiomyopathies
- Pleural effusion
- Peritonitis
- Hiatal hernia
- Emphysema
- Pulmonary embolism (rarely) – usually CXR is normal
- Dissecting aortic aneurysm (due to trauma, advanced/untreated syphilis, connective tissue disorders)
Chest X-Rays are among the most common films taken, being diagnostic of so many important problems.
Features that are typically examined on a chest X-ray
Every doctor will have a different approach to examining chest X-rays. A commonly used mnemonic for what to look for on a chest X-ray is: It May Prove Quite Right (but) Stop And Be Certain How Lungs Appear:
- I = Identification (name, age, sex, indication for X-ray)
- M = Markers (differentiate left from right – diagnose dextrocardia)
- P = Position – the spinous process of T4 should be between the heads of the clavicle (if it isn’t the body is rotated)
- Q = Quality – is the film penetrated properly. In a properly penetrated film the vertebral interspaces should be visible behind the central (cardiac) shadow
- R = Respiration – chest X-rays are typically done with full inspiration
- (but)
- S = Soft tissue – look for subcutaneous emphysema (suggestive of trauma), soft tissue swelling
- A = Abdomen – look for free abdominal air (suggests penetrating trauma, peritonitis, or recent surgery)
- B = Bone – look for fractures (these tend to be at the lateral aspects because of the mechanics – bending moment largest at lateral aspect)
- C = Central shadow (cardiac silhouette) – greater than 50% of lateral distance in frontal view at the diaphragm suggests cardiac enlargement (usually secondary to heart failure) or a pericardial effusion). A widened mediastinum may suggest aortic dissection.
- H = Hila (of the lungs) – can be affected in lung disease, malignant processes and infection (hilar lymphadenopathy).
- L = Lungs – for consolidation, interstitial lung disease (reticular, nodular or reticulonodular), honeycombing, miliary pattern, granulomas, lung masses
- A = Absent structures/Apices of the lung (for pneumothorax)
Another approach is to examine first any major abnormality, and then “review areas”:
- the apices,
- the hila,
- behind the heart (it must be remembered that lung can be seen through the heart),
- the cardiophrenic angles,
- the costophrenic angles,
- beneath the diaphragm, and then
- bone and soft tissues.
A third approach is:
- Inspection of chest
- Centralized – Check whether the Xray is centralized. In a well centralized film the clavicle is equidistant from the spines of the vertebral body. It is important when we are commenting on the comparative radiolucency of the lung field, cardiomegaly and mediastenal shift.
- Compare the lung field on upper, middle, and lower zone to check for radiolucency on both side of lungs at equal levels.
- Check the apical area (just behind the clavicle) for the changes due to tuberculosis.
- Check for any cervical rib in cases of bony deformities
- Check for cardiophrenic and costophrenic angles. These are sharp and curved in healthy individuals. The right diaphragm is .5 – 1.5 cm higher than the left diaphragm.
- Check the hila for any hilar lymphadenopathy. The left hilum is slightly higher than the right
- Trace trachea up to the carina to check for any deviation.
- Inspection of the cardiac silhouette
- Check the cardiac borders. Left cardiac border is formed by aorta, pulmonary conus, left atrium, and right atrium from top to bottom. The right border is formed by superior vena cava and right atrium
- Measure the cardio-thoracic ratio to rule out any cardiomegaly. To measure the cardiothoracic ratio draw a vertical line through the spine of the vertebrae. Draw lines perpendicular from this line to the maximum width of the left (say for e.g. a) and right heart borders (say for e.g. b). The summation of a and b should be less than half of the maximum transverse diameter of the chest (say for e.g. c). Thus a+b = or < C/2
- Inspection of bones
- Check ribs for crowding, spreading and bony lesions
- Check clavicle, scapula, and shoulder joints
- Inspection of soft tissue
- Check chest muscles, subcutaneous tissue, and breast in females
Views
Typical views
- Frontal (view)
- PA (posterior-anterior)
- AP (anterior-posterior) – these are typically done in the ICU
- Lateral (view)
The most common view is the PA (posterior-anterior) and is frequently done with a left lateral view (so one can identify the location of abnormalities in 3-D space). PA views are generally preferred to AP views (which are often done with mobile/portable X-ray equipment), but much less convenient in the ICU setting or when a patient cannot otherwise leave their bed. PA views are preferred because the central shadow is better defined, the magnification of the heart is reduced, and less of the lungs obscured by the heart/pericardial sac.
Additional views
- Decubitus – useful for differentiating pleural effusions from consolidation (e.g. pneumonia). In effusions, the fluid layers out (by comparison to an up-right view, when it often accumulates in the costophrenic angles).
- Lordotic view – used to visualize the apex of the lung, to pick-up abnormalities such as a Pancoast tumour.
- Expiratory view – helpful for the diagnosis of pneumothorax
- Obliques
Chest X Ray findings in some common lung diseases
Abnormalities
Nodule
A nodule is a discrete opacity in the lung which may be caused by:
- Neoplasm: benign or malignant
- Granuloma: tuberculosis
- Infection: round pneumonia
- Vascular: infarction, varix, Wegener’s granulomatosis, rheumatoid arthritis
There are a number of features that are helpful in suggesting the diagnosis:
- rate of growth
- Doubling time of less than one month: sarcoma/infection/infarction/vascular
- Doubling time of six to 18 months: benign tumour/malignant granuloma
- Doubling time of more than 24 months: benign nodule
- calcification
- margin
- smooth
- lobulated
- presence of a corona radiata
- shape
- site
If the nodules are multiple, the differential is then smaller:
- infection: tuberculosis, fungal infection, septic emboli
- neoplasm: e.g., metastases, lymphoma, harmatoma
- sarcoidosis
- alveolitis
- auto-immune disease: e.g., Wegener’s granulomatosis, rheumatoid arthritis
- inhalation (e.g., pneumoconiosis)
Cavities
A cavity is a walled hollow structure within the lungs. Diagnosis is aided by noting:
- wall thickness
- wall outline
- changes in the surrounding lung
The causes include:
- cancer (usually malignant)
- infarction (usually from a pulmonary embolus)
- infection: e.g., Staphylococcus aureus, tuberculosis, Gram negative bacteria (especially Klebsiella pneumoniae), and anaerobic bacteria.
Pleural abnormalities
Fluid in space between the lung and the chest wall is termed a pleural effusion. There needs to be at least 75ml of pleural fluid in order to blunt the costophrenic angle on the lateral chest X-ray, and 200ml on the posteroanterior chest X-ray. On a lateral decubitus, amounts as small as 5ml of fluid are possible. Pleural effusions typically have a meniscus visible on an erect chest X-ray, but loculated effusions (as occur with an empyema) may have a lenticular shape (the fluid making an obtuse angle with the chest wall).
Pleural thickening may cause blunting of the costophrenic angle, but is distinguished from pleural fluid by the fact that is occurs as a linear shadow ascending vertically and clinging to the ribs.
Diffuse shadowing
The differential for diffuse shadowing is very broad and can defeat even the most experienced radiologist. It is seldom possible to reach a diagnosis on the basis of the chest X-ray alone: high-resolution CT of the chest is usually required and sometimes a lung biopsy. The following features should be noted:
- type of shadowing (lines, dots or rings)
- reticular (crisscrossing lines)
- nodular (lots of small dots)
- rings or cysts
- ground glass
- consolidation (diffuse opacity with air bronchograms)
- location (where is the lesion worst?)
- upper zone (e.g., sarcoid, tuberculosis, silicosis/pneumoconiosis, ankylosing spondylitis, Langerhans cell histiocytosis)
- lower zone (e.g., cryptogenic fibrosing alveolitis, connective tissue disease, asbestosis, drug reactions)
- central (e.g., pulmonary oedema, alveolar proteinosis, lymphoma, Kaposi’s sarcoma, PCP)
- peripheral (e.g., cryptogenic fibrosing alveolitis, connective tissue disease,chronic eosinophilic pneumonia, bronchiolitis obliterans organizing pneumonia)
- lung volume
- increased (e.g., Langerhans cell histiocytosis, lymphangioleiomyomatosis, cystic fibrosis, allergic bronchopulmonary aspergillosis)
- decreased (e.g., fibrotic lung disease, chronic sarcoidosis, chronic extrinsic allergic alveolitis)
Pleural effusions may occur with cancer, sarcoid, connective tissue diseases and lymphangioleiomyomatosis. The presence of a pleural effusion argues against pneumocystis pneumonia.
- Reticular (linear) pattern
- (sometimes called “reticulonodular” because of the appearance of nodules at the intesection of the lines, even though there are no true nodule present)
- cryptogenic fibrosing alveolitis
- connective tissue disease
- sarcoidosis
- radiation fibrosis
- asbestosis
- lymphangitis carcinomatosis
- Nodular pattern
- Cystic
-
- cryptogenic fibrosing alveolitis (late stage “honeycomb lung”)
- cystic bronchiectasis
- Langerhans cell histocytosis
- lymphangioleiomyomatosis
- Consolidation
-
- Alveolar haemorrhage
- Alveolar cell carcinoma
- vasculitis
- chronic eosinophilic pneumonia
Limitations
It must be remembered that while the chest X-ray is a cheap and safe method of investigating diseases of the chest, there are a number of serious chest conditions that may be associated with a normal chest X-ray and other means of assessment may be necessary to make the diagnosis:
- Asthma
- Chronic obstructive pulmonary disease
- Pneumocystis jiroveci pneumonia (PCP)
- Pulmonary embolism
- Smoke inhalation
- Foreign body inhalation
Signs
Silhouette Sign
- The silhouette sign is especially helpful in localizing lung lesions. (e.g., loss of right heart border in right middle lobe pneumonia),[1]
Air Bronchogram Sign
- The air bronchogram sign, where branching radiolucent columns of air corresponding to bronchi is seen, usually indicates air-space (alveolar) disease, as from blood, pus, mucus, cells, protein surrounding the air bronchograms. This is seen in Respiratory distress syndrome[1]
Bean Sign
- The “bean” sign first described by Professor Keval Pandya is the appearance of a sharply circumscribed bean shaped nodule on chest X-ray which has a high sensitivity and specificity (92% and 88%) for the presence of miliary TB.
References
- ↑ 1.0 1.1 Chest X-Ray, OB-GYN 101: Introductory Obstetrics & Gynecology. © 2003, 2004, 2005, 2008 Medical Education Division, Brookside Associates, Ltd. Retrieved 9 February 2010.
Evaluation With Cardiac Imaging 2022 AHA/ACC/HFSA Heart Failure Guideline (DO NOT EDIT) [1]
Evaluation With Cardiac Imaging 2022 AHA/ACC/HFSA Heart Failure Guideline (DO NOT EDIT) [1]
| Class I |
| “1. In patients with suspected or new-onset HF, or those presenting with acute decompensated HF, a chest X-ray should be performed to assess heart size and pulmonary congestion and to detect alternative cardiac, pulmonary, and other diseases that may cause or contribute to the patient‘s symptoms. [2][3](Level of Evidence: C-LD) ” |
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; David E. Winchester M.D. M.S.
This chapter presents a brief overview of cardiac imaging techniques. For a detailed discussion of each of the imaging technoloies, please view the chapter on that imaging technology.
Assessment of LV function
- Least expensive, most versatile.
- Portable, immediately available
- Preferred initial technique to diagnose heart muscle disease of unknown etiology.
- Regional thickening can be assessed on ECHO and not other techniques and this is a better marker of regional function than is regional wall motion (cant be seen on nuclear or angio studies, MRI can assess though)
- ECHO is not as good at assessing quantitative ejection fraction (SPECT, angio, RVG are better at this).
- More sensitive than EKG in diagnosis of LVH.
- Excellent in estimating LV mass
- Good for quantitating LV and RV EFs. Excellent for following the wall motion in patients treated with chemotherapeutic agents.
- Good for wall motion.
- In MI does not tell you about infarct expansion, MR, LV thrombus, regional thickening abnormalities.
- Permits evaluation of regional thickening, global LV function and myocardial perfusion.
- Good regional and global cardiac function.
- With contrast agents, good perfusion data
- Superior for congenital, aortic disease, anomalous coronary arteries, and RV dysplasia
- Cost benefit ratios of echo and nuclear make them superior for LV function assessment
- May be best technique for quantitating LV mass
- As a research tool may be useful in the assessment of LV remodeling
- Gold standard in the assessment of wall motion but not in the assessment of wall thickening.
- LVEF and absolute volumes are highly reproducible
- LVH and LV mass are better quantitated with echo and MRI
- Left to right shunts are most accurately quantitated with cardiac cath over echo and MRI
Techniques to Assess CAD and Prognosis
- Strengths
- Low cost
- Short duration
- Functional status evaluation
- High sensitivity in 3 VD or left main disease
- Useful prognostic information
- Limitations
- Suboptimal sensitivity in the detection of single vessel disease (50%), 85% in the presence of three vessel disease
- In all patients, overall sensitivity 68%, specificity 77%
- Beta blocker use is associated with a higher rate of false negatives (fail to achieve rate pressure product)
- Non diagnostic in patients with abnormal baseline EKG (dig, LVH, WPW)
- Poor specificity in certain patient populations: premenopausal women, LVH, dig, IVCD, hypokalemia, hyperventilation, severe hypertension, resting ST abnormalities
- The negative predictive value in women of low to intermediate risk is high, the positive predictive value in men is high
- Need to achieve > 85% of maximum heart rate for maximizing accuracy
- Its main values lies in excluding CAD in patients with a low pre test probability of CAD based on gender and age.
- Strengths
- Simultaneous evaluation of perfusion and function with gated SPECT
- Higher sensitivity and specificity than exercise EKG: For exercise or pharmacologic SPECT imaging with Tl or Tc, in patients with chest pain the sensitivity for the detection of CAD is 85% to 90%. Specificity for excluding CAD is in the 90% range. Good in patients with LVH, dig, IVCD etc. ST depression response higher rate pressure product than does a perfusion abnormality with tracers. Therefore they are more sensitive. Adding stress perfusion imaging to the exercise ECG stress test greatly assists in differentiating true positive from false positive ETT ST segment depression. For single vessel disease, the sensitivity is 25% higher with SPECT imaging compared with exercise testing. The sensitivity for detecting 3VD with exercise SPECT is 95% to 100%.
- High specificity with Tc labeled agents: Half life is shorter than Tl, therefore dose is higher, therefore image is brighter and better. Also allows gated assessment of LV thickening.
- Studies can be performed in almost all patients
- Significant additional prognostic information, can quantitate LV function
- Comparable accuracy with pharmacologic stress testing
- Viability and ischemia when assessed simultaneously
- Quantitative image analysis
- Limitations
- Suboptimal specificity with thallium imaging, with a high false positive rate in many labs, particularly among women and obese patients.
- Long procedure time with Tc agents, higher costs than ETT
- Radiation exposure
- Poor images in obese patients
- Pharmacologic stress testing: sensitivity and specificity are similar for persantine and adenosine. Dobutamine is used in those patients with a history of bronchospasm, or for those patients who have consumed coffee before the procedure. Pharmacologic testing is the preferred method in patients with LBBB.
- Women with chest pain who are referred for exercise or pharmacologic stress testing benefit the most from the enhanced accuracy of Tc imaging. Both Tl and Tc had a sensitivity of about 70%, but the specificity rose to 92% with Tc. Most labs now use Tc because of its improved specificity, the ability to gait the images and assess regional wall thickening. Mild non reversible defects that show preserved systolic thickening usually represent attenuation artifacts, however, if there is abnormal wall thickening, then this is most likely scar.
- Strengths
- Higher sensitivity and specificity than exercise EKG: Metanalysis showed sensitivity of 84%, specificity 86%. Marked variation across trials though, highly operator dependent. If the max heart rate is < 85% of age predicted, then sensitivity drops to 42%. Sensitivity is 10% lower in women than in men, specificity is the same across genders. In women with single vessel disease the sensitivity was only 40%, if there was 2 or 3 vessel disease, this number increased to 60%.
- Additional prognostic value over exercise EKG
- Dobutamine stress has higher sensitivity than does pharmacologic stress
- Time to complete examination is short
- Identification of co-existent structural cardiac abnormalities (valvular disease)
- Simultaneous evaluation of perfusion with contrast agents
- Relatively lower costs than with other techniques
- No radiation
- Limitations
- Decreased sensitivity for the detection of single vessel disease or mild stenosis with post exercise imaging
- Inability to image the entire ventricle in some patients
- Highly operator dependent in the analysis of images
- No quantitative image analysis
- Poor windows in patients with COPD
- Infarct zone ischemia less well detected
Comparison of exercise SPECT imaging and Exercise Echocardiography
- Both have a higher sensitivity and specificity than regular exercise EKG testing
- Both provide functional information that EKG testing does not
- Both provide information about myocardial viability, which the angiogram does not
Strengths of Stress ECHO over SPECT
- Noninvasive, safe and repeatable, no radiation exposure, quick, little sophisticated equipment and portable, low costs, can identify co-existing valvular heart disease
Limitations of Stress ECHO over SPECT
- Images are difficult to obtain at peak exercise, an ischemic response is required to observe wall motion abnormalities, wall motion can recover quickly in the presence of mild ischemia, detection of residual ischemia is difficult in an akinetic wall zone, the technique is highly operator dependent, good quality images were only acquired in 70% of cases.
Strengths of SPECT over stress ECHO
- Does not require an ischemic response to be abnormal, just requires an abnormality in flow reserve, sensitivity is slightly higher by about 8-10 percentage points (mostly because the ability to detect single vessel disease or mild stenoses of 50-70% is not as good with stress Echo), can see defects in areas that contain scar and viable myocardium, acquisition of images is not operator dependent, in virtually 100% of patients diagnostic images are obtained, with Tc simultaneous assessment of perfusion and function is obtained, resting LV ejection fraction can be obtained, vasodilator SPECT has significantly higher sensitivity than vasodilator stress ECHO, dobutamine ECHO is associated with higher sensitivity and specificity than vasodilator ECHO.
Limitations of SPECT imaging in relation to stress ECHO
- Longer imaging protocols, greater expense of equipment, must inject and store radiopharmaceuticals, inability to visualize the heart in real time, lower spatial resolution than ECHO, higher costs to patients.
In general, the sensitivity is lower for stress ECHO while the specificity is higher.
Prognosis
Exercise Tolerance Testing
- 1 mm or more of horizontal or downsloping ST depression is associated with a poor prognosis
- Failure to achieve 6 METS is associated with an elevated mortality rate over the next 2.5 years.
- Failure of heart rate to rise is associated with higher mortality, even after adjusting for perfusion defects.
- Failure to reach 85% of age adjusted max HR is associated with a RR of 1.85 in mortality.
- Limitation of ETT is the fact that the magnitude of ST depression is not strongly associated with the extent of CAD
- Exercise testing alone has excellent prognostic ability among patients with atypical chest pain or non anginal pain who have a normal EKG at baseline. If these patients have a normal ETT, the prognosis is excellent.
Nuclear Stress Myocardial Perfusion
- Nuclear Stress Myocardial Perfusion Imaging, often abbreviated MPI or MPS, is a technique for measuring perfusion of myocardial tissue using externally injected radioactive tracers. Photons, or positrons emitted from these tracers are then detected with specialized imaging equipment and software. The most common methods are single photon emission computed tomography (SPECT) and positron emission tomography (PET). SPECT can be performed with radiotracers based on thallium or technetium 99-m. PET is commonly performed with rubidium-82, although some centers use ammonia (NH3) or radiolabeled oxygen in water. Cardiac PET with fluorodeoxyglucose (FDG) is useful for other investigations such as evaluation of infections, sarcoidosis activity, and viability/hibernation. Flurpiridaz, is a PET tracer based on fluorine-18 (F-18) and was approved for use by the FDA in 2025.
- The following are associated with a poor prognosis:
- 20% of the LV is a perfusion defect
- Defects in more than one distribution suggestive of multivessel CAD
- A large number of non reversible defects
- Transient LV cavitary dilation
- Increased lung uptake
- Resting LVEF of < 40%
- Normal thallium: Mortality 1% per year
- Normal Tc: annual mortality 0.6%, 12 fold higher if there is a Tc defect
- The positive predictive value of stress myocardial perfusion imaging and stress ECHO is low: That is the percentage of people who die or sustain an MI is low among patients with abnormal findings. On the other hand the negative predictive value is high and exceeds 95%.
Techniques used to Assess Myocardial Viability
- Tl Imaging
- Rest and delayed redistribution is the most common radionuclide method used to assess viability. Uptake of Tl is related not only to blood flow, but also to membrane integrity. Myocardial stunning or hibernation does not result in a reduction in Tl extraction as long as the sarcolemmal membrane does not sustain irreversible ischemic damage. 60 to 70% of asynergistic segments will show > a 50% improvement after revascularization.
- Tc Imaging
- Same as above, as usual a better signal with Tc, can also assess regional wall thickening. If thickening is present, then viability is likely.
- PET
- Considered by many to be the gold standard. Can be used to assess perfusion and metabolism simultaneously. If there is mismatch in perfusion and metabolism, then the tissue is viable. If there is a match, then there is scar.
Dobutamine: Enhanced systolic contractility with low dose dobutamine is associated with recovery.
Vote on and Suggest Revisions to the Current Guidelines
Vote on and Suggest Revisions to the Current Guidelines
Sources
Sources
- 2022 AHA/ACC/HFSA Guideline for the Management of Heart Failure: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines[4]
- The ACC/AHA 2005 Guideline Update for the Diagnosis and Management of Chronic Heart Failure in the Adult [5]
- 2009 focused update: ACCF/AHA Guidelines for the Diagnosis and Management of Heart Failure in Adults: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines: developed in collaboration with the International Society for Heart and Lung Transplantation [6]
References
References
- ↑ Heidenreich PA, Bozkurt B, Aguilar D, Allen LA, Byun JJ, Colvin MM; et al. (2022). “2022 AHA/ACC/HFSA Guideline for the Management of Heart Failure: Executive Summary: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines”. Circulation. 145 (18): e876–e894. doi:10.1161/CIR.0000000000001062. PMID 35363500 Check
|pmid=value (help). - ↑ Badgett RG, Mulrow CD, Otto PM, Ramírez G (1996). “How well can the chest radiograph diagnose left ventricular dysfunction?”. J Gen Intern Med. 11 (10): 625–34. doi:10.1007/BF02599031. PMID 8945695.
- ↑ Knudsen CW, Omland T, Clopton P, Westheim A, Abraham WT, Storrow AB; et al. (2004). “Diagnostic value of B-Type natriuretic peptide and chest radiographic findings in patients with acute dyspnea”. Am J Med. 116 (6): 363–8. doi:10.1016/j.amjmed.2003.10.028. PMID 15006584. Review in: ACP J Club. 2004 Sep-Oct;141(2):48
- ↑ Heidenreich PA, Bozkurt B, Aguilar D, Allen LA, Byun JJ, Colvin MM, Deswal A, Drazner MH, Dunlay SM, Evers LR, Fang JC, Fedson SE, Fonarow GC, Hayek SS, Hernandez AF, Khazanie P, Kittleson MM, Lee CS, Link MS, Milano CA, Nnacheta LC, Sandhu AT, Stevenson LW, Vardeny O, Vest AR, Yancy CW (May 2022). “2022 AHA/ACC/HFSA Guideline for the Management of Heart Failure: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines”. Circulation. 145 (18): e895–e1032. doi:10.1161/CIR.0000000000001063. PMID 35363499 Check
|pmid=value (help). - ↑ Hunt SA, Abraham WT, Chin MH, Feldman AM, Francis GS, Ganiats TG, Jessup M, Konstam MA, Mancini DM, Michl K, Oates JA, Rahko PS, Silver MA, Stevenson LW, Yancy CW, Antman EM, Smith SC Jr, Adams CD, Anderson JL, Faxon DP, Fuster V, Halperin JL, Hiratzka LF, Jacobs AK, Nishimura R, Ornato JP, Page RL, Riegel B; American College of Cardiology; American Heart Association Task Force on Practice Guidelines; American College of Chest Physicians; International Society for Heart and Lung Transplantation; Heart Rhythm Society. ACC/AHA 2005 Guideline Update for the Diagnosis and Management of Chronic Heart Failure in the Adult: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Update the 2001 Guidelines for the Evaluation and Management of Heart Failure): developed in collaboration with the American College of Chest Physicians and the International Society for Heart and Lung Transplantation: endorsed by the Heart Rhythm Society. Circulation. 2005 Sep 20; 112(12): e154-235. Epub 2005 Sep 13. PMID 16160202
- ↑ Jessup M, Abraham WT, Casey DE, Feldman AM, Francis GS, Ganiats TG et al. (2009) 2009 focused update: ACCF/AHA Guidelines for the Diagnosis and Management of Heart Failure in Adults: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines: developed in collaboration with the International Society for Heart and Lung Transplantation. Circulation 119 (14):1977-2016. DOI:10.1161/CIRCULATIONAHA.109.192064 PMID: 19324967
Looking for the patient version?
© 2026 MyEClinic – IFTM Institut für Telematik in der Medizin GmbH