
Congestive heart failure
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Lakshmi Gopalakrishnan, M.B.B.S. [2], Mitra Chitsazan, M.D.[3] Seyedmahdi Pahlavani, M.D. [4] Syed Hassan A. Kazmi BSc, MD [5] Edzel Lorraine Co, D.M.D., M.D. [6]
Synonyms and keywords: CHF; pump failure; left heart failure; chronic heart failure; acute heart failure; LV dysfunction; LV failure; impaired filling; reduced cardiac output; HFpEF; HFrEF; heart failure preserved ejection fraction; heart failure reduced ejection fraction; decompensated heart failure; acute decompensated heart failure; ADHF
Overview
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Syed Hassan A. Kazmi BSc, MD [2]
Overview
Heart failure is a complex syndrome whereby there is inadequate output of the heart to meet the metabolic demands of the body. Abnormal function of different anatomic parts of the heart cause heart failure including the pericardium, the myocardium, the endocardium, the heart valves and the great vessels. Symptoms of heart failure are due to a lack of both forward blood flow to the body, and backward flow into the lungs. Heart failure is a clinical syndrome characterized by symptoms of dyspnea, edema and fatigue and signs such as rales on physical examination. Heart failure may be classified based on ejection fraction into heart failure with preserved ejection fraction (HFpEF) and heart failure with reduced ejection fraction (HFrEF). LV remodeling is the basic concept for HFpEF pathophysiolgy. Two models are emerging in HFpEF pathophysiology, the traditional model discussed about ventricular diastolic dysfunction , LV hypertrophy, impaired relaxation, endothelial dysfunction, arterial and ventricular stiffness and their effect on cardiac function. The emerged model discussed role of systemic microvascular endothelial inflammation due to existing comorbidities such as, diabetes, hypertension, obesity, smoking and ischemia in cardiac remodeling and dysfunction. The pathogenesis of HFrEF is related largely to cellular proliferation and metabolism. Pathological processes that result in progression of HF and are common to both HFrEF and HFpEF are altered excitation-contraction coupling, epigenetic modifications, changes in sarcomeric coupling proteins, increased adrenergic drive, increased activity of renin-angiotensin aldosterone axis, nitric oxide insensitivity, adensoine triphosphate (ATP) depletion, reactive oxygen species production and an elevated cell death rate. The causes of heart failure can be broadly divided into cardiac and non-cardiac. Cardiac causes include aortic regurgitation, aortic stenosis, arrhythmias, arrhythmogenic right ventricular dysplasia, arteriovenous fistula, atrial fibrillation, atrial septal defect, cardiac amyloidosis, cardiac aneurysm, congenital heart disease, constrictive pericarditis, dilated cardiomyopathy, Eisenmenger syndrome, endocarditis, hypertension, hypertrophic cardiomyopathy, hypoplastic left heart syndrome, interferon gamma, ischemic heart disease, malignant hypertension, mitral regurgitation, mitral stenosis, myocardial infarction, oxaprozin, patent ductus arteriosus, pericardial effusion, pericardial tamponade, pericarditis, peripartum cardiomyopathy, pertuzumab, restrictive cardiomyopathy, rheumatic carditis, rupture of the papillary muscles, Takotsubo cardiomyopathy, tricuspid insufficiency, valvular heart disease, ventricular aneurysm, ventricular septal defect. Congestive heart failure should be distinguished from other conditions that cause dyspnea, fatigue and edema. Heart failure affects close to 5 million people in the the United States of America and each year close to 500,000 new cases are diagnosed. Congestive heart failure is responsible for a significant portion of the healthcare budget, and more than 50% of patients seek re-admission within 6 months after treatment and the average duration of hospital stay is 6 days. In 2005 the prevalence among adults aged 20 and older in the United States was 5,300,000 (about 2,650,000 males, and 2,650,000 females). Heart failure is associated with significantly reduced physical and mental health, resulting in a markedly decreased quality of life. Congestive heart failure is also associated with a poor prognosis. If left untreated, heart failure may result in death due to complications associated with the condition. Heart failure resulting from atherosclerotic coronary artery disease has been shown to be associated with higher incidence of fatal events compared to heart failure that results from other cardiac diseases. Heart failure is a progressive disease with a major impact on the patient’s quality of life. With the exception of heart failure caused by reversible conditions, the condition usually worsens with time. Although some people survive many years, progressive disease is associated with an overall annual mortality rate of 10%. In the Framingham experience, 80% of men and 70% of women with heart failure who were under 65 years of age had died within 8 years of the diagnosis. There are several diagnostic criteria / algorithms that are used to diagnose heart failure including an algorithm from the ESC, Framingham study, and Boston. The classic symptoms of heart failure include dyspnea, fatigue, and fluid retention. Patients with heart failure present in different ways. Some patients present with exercise intolerance but show little evidence of congestion or edema. Other patients present with mild symptoms of edema and pulmonary congestion. The ejection fraction is usually below 35% in patients who are symptomatic with systolic heart failure. BNP levels may be useful in the initial establishment of the diagnosis of heart failure in the patient with dyspnea of unclear etiology. Chest x-ray in a patient with heart failure shows cardiomegaly (cardiac enlargement and pulmonary congestion (Kerley B lines, and in some cases pleural effusion). CMR may be used for assessment of LV and RV size and morphology, systolic and diastolic function, and for characterizing myocardial tissue for the purpose of understanding the etiology of LV systolic or diastolic dysfunction. Echocardiography is commonly used to diagnose and monitor the progression of heart failure. This modality uses ultrasound to determine the stroke volume (SV, the amount of blood in the heart that exits the ventricles with each beat), the end-diastolic volume (EDV, the total amount of blood at the end of diastole), and the SV divided by the EDV, a value known as the ejection fraction (EF). In pediatrics, the shortening fraction is the preferred measure of systolic function. Coronary angiography is perfomred in patients with heart failure in whom there is a suspicion of underlying atherosclerosis as the basis for the heart failure. Patients who are troponin or CK-MB positive, who have dynamic EKG changes or other signs and symptoms of an acute coronary syndrome who are revascularization candidates should undergo coronary angiography. Acute heart failure can occur in the setting of a new onset heart failure or worsening of an existing chronic heart failure (also known as acute decompensated heart failure, flash pulmonary edema, ADHF). ADHF presents with acute shortness of breath due to the development of pulmonary edema (the rapid accumulation of fluid in the lung). Other signs and symptoms of ADHF include hypotension with impaired and organ perfusion manifested by worsening renal function, altered mentation and cold clammy extremities. ADHF associated with a poor prognosis if not treated aggressively. Like chronic heart failure therapy, the goal is to improve symptoms but unlike chronic therapy the other goals are to improve oxygenation and hemodynamic stability. The mainstays of the acute medical treatment in acute decompensated congestive heart failure include oxygen to improve hypoxia, diuresis to reduce both preload and intravascular volume and vasodilators to reduce afterload. Some of the mainstays of chronic heart failure therapy are not initiated acutely (ACE inhibtors,beta blockers and digoxin). End of life care in the patient with congestive heart failure is focused on making the patient comfortable. Invasive procedures should be minimized, and patients may elect to have their defibrillators inactivated. The growing number of patients with Stage IV heart failure (intractable symptoms of fatigue, shortness of breath or chest pain at rest despite optimal medical therapy) should be considered for palliative care or hospice.
Historical Perspective
Heart failure (HF) is known to be recognized as a disease since ancient times. Italian Egyptologist Ernesto Schiaparelli reported the first case of decompensated heart failure (HF) in the remains of a tomb in the Valley of the Queens over 3500 years ago the remains are now housed in the Egyptian museum in Turin, Italy. They belonged to an Egyptian dignitary named Nebiri who lived under the reign of the 18th dynasty Pharaoh Thutmose III (1479–24 BC). Various other features of HF such as cardiac hypertrophy and coronary atherosclerosis were also known to Egyptians. In China, ‘the Yellow Emperor’s Classic of Internal Medicine’ described edema as early as 2600 B.C. The medieval Arab scholar Ibn Sina, known to the West as Avicenna (980–1037), had a reputation as an authority on heart disease. His treatise entitled ‘Kitab al-Adviyt-al-Qalbiye’ or ‘The book on drugs for cardiac diseases’ discusses therapies for difficulty in breathing, palpitation, and syncope. Widely used in the West in a Latin translation in the 14th century, the treatise remains in the Galenic tradition of humours. In 1628 when William Harvey clearly described circulation and elucidated hemodynamic abnormalities occurring in HF. Röntgen discovered x-rays in 1895 and allowed a more thorough understanding of maladaptive changes occurring in HF patients.In the 1940s and 1960s the advent of cardiac catheterization and cardiac surgery furthered our understanding of HF. The 1960s was also the decade that saw the emergence of LV assist devices (LVADs), beginning in 1961 when Dennis and co-workers uses a roller pump to assist the left ventricle. From the mid-1970s, the availability of vasodilators provided a means to reduce afterload in order to increase cardiac efficiency and cardiac output in HF
Classification
Several classification schemes are used to characterize heart failure based on:
- The pathophysiology of heart failure (systolic vs diastolic; left vs right; low output vs high output)
- The chronicity of heart failure (acute vs chronic)
- The severity of heart failure (the NY Heart Association Class)
- The stage of congestive heart failure (AHA Class A,B,C,D)
- The most recent classification according to the left ventricular ejection fraction; heart failure with reduced ejection fraction(HFrEF) vs heart failure with preserved ejection fraction (HFpEF)[1]
Pathophysiology
Heart failure is a complex syndrome whereby there is inadequate output of the heart to meet the metabolic demands of the body. Heart failure is caused by abnormal function of different anatomic parts of the heart including the pericardium, the myocardium, the endocardium, the heart valves and the great vessels. Heart failure is characterized by decreased cardiac output but not necessarily decreased ejection fraction. Symptoms of heart failure are due to a lack of both forward blood flow to the body, and backward flow into the lungs. The body tries to compensate for the low cardiac output by mechanisms that increase the preload and afterload. These mechanisms lead to exacerbation of the cardiac malfunction and symptoms associated with heart failure. LV remodeling is the basic concept for HFpEF pathophysiolgy. Two models are emerging in HFpEF pathophysiology, the traditional model discussed about ventricular diastolic dysfunction , LV hypertrophy, impaired relaxation, endothelial dysfunction, arterial and ventricular stiffness and their effect on cardiac function. The emerged model discussed role of systemic microvascular endothelial inflammation due to existing comorbidities such as, diabetes, hypertension, obesity, smoking and ischemia in cardiac remodeling and dysfunction. The pathogenesis of HFrEF is related largely to cellular proliferation and metabolism. Pathological processes that result in progression of HF and are common to both HFrEF and HFpEF are altered excitation-contraction coupling, epigenetic modifications, changes in sarcomeric coupling proteins, increased adrenergic drive, increased activity of renin-angiotensin aldosterone axis, nitric oxide insensitivity, adensoine triphosphate (ATP) depletion, reactive oxygen species production and an elevated cell death rate.
Causes
The causes of heart failure can be broadly divided into cardiac and non-cardiac. Cardiac causes include aortic regurgitation, aortic stenosis, arrhythmias, arrhythmogenic right ventricular dysplasia, arteriovenous fistula, atrial fibrillation, atrial septal defect, cardiac amyloidosis, cardiac aneurysm, congenital heart disease, constrictive pericarditis, dilated cardiomyopathy, Eisenmenger syndrome, endocarditis, hypertension, hypertrophic cardiomyopathy, hypoplastic left heart syndrome, interferon gamma, ischemic heart disease, malignant hypertension, mitral regurgitation, mitral stenosis, myocardial infarction, oxaprozin, patent ductus arteriosus, pericardial effusion, pericardial tamponade, pericarditis, peripartum cardiomyopathy, pertuzumab, restrictive cardiomyopathy, rheumatic carditis, rupture of the papillary muscles, Takotsubo cardiomyopathy, tricuspid insufficiency, valvular heart disease, ventricular aneurysm, ventricular septal defect.
Differentiating Heart Failure From Other Diseases
Congestive heart failure should be distinguished from other conditions that cause dyspnea, fatigue and edema.
Epidemiology and Demographics
Heart failure affects close to 5 million people in the the United States of America and each year close to 500,000 new cases are diagnosed. Congestive heart failure is responsible for a significant portion of the healthcare budget, and more than 50% of patients seek re-admission within 6 months after treatment and the average duration of hospital stay is 6 days. In 2005 the prevalence among adults aged 20 and older in the United States was 5,300,000 (about 2,650,000 males, and 2,650,000 females).
Risk Factors
Several risk factors may predispose to heart failure. These risk factors can be demographic, genetic, associated with lifestyle or medications.
Screening
There is insufficient evidence to recommend routine screening for heart failure.
Natural History, Complications And Prognosis
Heart failure is associated with significantly reduced physical and mental health, resulting in a markedly decreased quality of life. Congestive heart failure is also associated with a poor prognosis. If left untreated, heart failure may result in death due to complications associated with the condition. Heart failure resulting from atherosclerotic coronary artery disease has been shown to be associated with higher incidence of fatal events compared to heart failure that results from other cardiac diseases. Heart failure is a progressive disease with a major impact on the patient’s quality of life. With the exception of heart failure caused by reversible conditions, the condition usually worsens with time. Although some people survive many years, progressive disease is associated with an overall annual mortality rate of 10%. In the Framingham experience, 80% of men and 70% of women with heart failure who were under 65 years of age had died within 8 years of the diagnosis.
Differential Diagnosis of Causes of Heart Failure Segregated by Left and Right Sided Heart Failure
Left Ventricular Failure
Most Common Causes:
Expanded List of Causes:
- Atrial fibrillation
- Alcoholism
- Anemia
- Angina
- Aortic regurgitation
- Aortic Stenosis
- Arteriovenous fistula
- Beriberi
- Cardiac aneurysm
- Cardiomyopathy
- Constrictive pericarditis
- Drugs, toxins
- Hypertension
- Hyperthyroidism
- Hypovolemia
- Hypoxia
- Mediastinal tumors
- Mitral Regurgitation
- Myocardial Infarction
- Paget’s Disease
- Pancoast’s Tumor
- Pericardial effusion
- Pericardial tamponade
- Perimyocarditis
- Protein deficiency
- Restrictive cardiomyopathy
- Rupture of the papillary muscles
- Sepsis
- Superior vena cava syndrome
Right Ventricular Failure
Most Common Causes:
- Cardiomyopathy
- Cor pulmonale
- Diffuse myocarditis
- Left heart failure
Other Causes:
- After left ventricular failure
- After pulmonary resection
- Allergic alveolitis
- Bronchial asthma
- Chronic bronchitis
- Honeycomb lung
- Hyperglobulia
- Emphysema
- Mitral Stenosis
- Right ventricular myocardial infarction
- Pickwickian Syndrome
- Pleural fibrosis
- Pneumoconiosis
- Pulmonary fibrosis
- Pulmonic regurgitation
- Pulmonic stenosis
- Sarcoidosis
- Severe relapsing pulmonary emboli
- Silicosis
- Tachycardia
- Tricuspid insufficiency
Others
- Ascorbic acid deficiency
- Cardiac amyloidosis
- Carnitine deficiency
- Cervical vein stasis of non-cardiac genesis
- Congenital heart disease
- Cyanosis of non-cardiac genesis
- Diabetes Mellitus
- Dyspnea of non-cardiac genesis
- Edema of non-cardiac genesis
- Hemochromatosis
- Pleural effusion of non-cardiac genesis
- Pulmonary edema of non-cardiac genesis
- Thiamine deficiency
- Thyroid disease
Diagnosis
Clinical assessment
There are several diagnostic criteria / algorithms that are used to diagnose heart failure including an algorithm from the ESC, Framingham study, and Boston.
History and symptoms
The classic symptoms of heart failure include dyspnea, fatigue, and fluid retention. Patients with heart failure present in different ways. Some patients present with exercise intolerance but show little evidence of congestion or edema. Other patients present with mild symptoms of edema and pulmonary congestion. The ejection fraction is usually below 35% in patients who are symptomatic with systolic heart failure.
Physical examination
Physical examination is of utmost important in the suspicion, diagnosis and follow up of heart failure. Focus should be targeted mainly on the evaluation of the fluid status, blood pressure and weight changes.
Laboratory findings
Once the diagnosis of heart failure is made, subsequent laboratory studies should be directed toward the identification of an underlying cause of heart failure. Laboratory tests used for diagnosis and monitor disease activity include renal function tests, thyroid function tests, serum BNP levels and serum CA-125 levels. BNP levels may be useful in the initial establishment of the diagnosis of heart failure in the patient with dyspnea of unclear etiology. In a meta-analysis, BNP was superior N-terminal pro-BNP (NTproBNP) and was associated with a sensitivity of 85% and specificity of 84% in the diagnosis of heart failure in the primary care setting. Once the diagnosis of heart failure is made, subsequent laboratory studies should be directed toward the identification of an underlying cause of heart failure. Renal function should be assessed as a rough guide to the patient’s intravascular volume status and renal perfusion. A urinalysis is helpful in the assessment of the patient’s volume status. Electrolyte assessment and the correction of electrolyte disturbances such as hypokalemia, hyperkalemia and hypomagnesemia is critical in those patients treated with diuretics. Hyponatremia (due to poor stimulation of the baroreceptors and appropriate ADH release and free water retention) is associated with a poor prognosis.
Electrocardiogram
Although there is no diagnostic criteria of congestive heart failure on the EKG, there may be signs of the underlying cardiac cause(s) of congestive heart failure. The EKG often shows low QRS voltage. Other changes associated with HF include ventricular hypertrophy, atrial enlargement, poor R wave progression, left bundle branch block.
Chest X-ray
Chest x-ray in a patient with heart failure shows cardiomegaly (cardiac enlargement and pulmonary congestion (Kerley B lines, and in some cases pleural effusion)
MRI
CMR may be used for assessment of LV and RV size and morphology, systolic and diastolic function, and for characterizing myocardial tissue for the purpose of understanding the etiology of LV systolic or diastolic dysfunction. The writing committee recognizes the potential capabilities of spectroscopic techniques for acquiring metabolic information of the heart when evaluating individuals with heart failure.
Echocardiography
Echocardiography is commonly used to diagnose and monitor the progression of heart failure. This modality uses ultrasound to determine the stroke volume (SV, the amount of blood in the heart that exits the ventricles with each beat), the end-diastolic volume (EDV, the total amount of blood at the end of diastole), and the SV divided by the EDV, a value known as the ejection fraction (EF). In pediatrics, the shortening fraction is the preferred measure of systolic function.
Exercise stress test
Exercise stress testing with an assessment of oxygen consumption is useful in assessing the functional capacity of the heart failure patient. Angiography can exclude the presence of an ischemic basis for the disease, and cardiac catheterization can evaluate the hemodynamic basis of heart failure and the response to drug. Myocardial viability studies can determine whether hypocontractile myocardium is viable but just hibernating, and could therefore benefit from revascularization.
Myocardial viability studies
Myocardial viability studies can determine whether hypocontractile myocardium is viable but just hibernating, and could therefore benefit from revascularization.
Cardiac catheterization
Coronary angiography is perfomred in patients with heart failure in whom there is a suspicion of underlying atherosclerosis as the basis for the heart failure. Patients who are troponin or CK-MB positive, who have dynamic EKG changes or other signs and symptoms of an acute coronary syndrome who are revascularization candidates should undergo coronary angiography.
Invasive hemodynamic monitoring
Based upon the results of the ESCAPE trial, there is no benefit in clinical outcomes associated with the routine use of a pulmonary artery line in patients with decompensated CHF.
Treatment
Acute Treatment
Acute heart failure can occur in the setting of a new onset heart failure or worsening of an existing chronic heart failure (also known as acute decompensated heart failure, flash pulmonary edema, ADHF). ADHF presents with acute shortness of breath due to the development of pulmonary edema (the rapid accumulation of fluid in the lung). Other signs and symptoms of ADHF include hypotension with impaired and organ perfusion manifested by worsening renal function, altered mentation and cold clammy extremities. ADHF associated with a poor prognosis if not treated aggressively. Like chronic heart failure therapy, the goal is to improve symptoms but unlike chronic therapy the other goals are to improve oxygenation and hemodynamic stability. The mainstays of the acute medical treatment in acute decompensated congestive heart failure include oxygen to improve hypoxia, diuresis to reduce both preload and intravascular volume and vasodilators to reduce afterload. Some of the mainstays of chronic heart failure therapy are not initiated acutely (ACE inhibtors,beta blockers and digoxin).
General Measures in the Management of Heart Failure
- Treat the underlying cause of heart failure such as ischemic heart disease, hypertension, and valvular heart disease.
- Treat other non cardiac diseases that might contribute to the symptoms of heart failure such as diabetes and hyperthyroidism[2].
- Treat with a low salt diet[3]
- Follow the patient’s weight to check for fluid overload
- Treat with vaccines for influenza and pneumococcus [4][5]
Diuresis: First Step in the Management of Heart Failure
The treatment of chronic heart failure often begins with the administration of diuretics, particularly if the patient has signs or symptoms of volume overload. While increased left ventricular volume increases contractility to a point, if the heart is filled beyond that point, its contractility diminishes (the patient “falls of the Staring curve“). Diuretics can reduce volume overload and reduce shortness of breath and edema. There are three kinds of diuretics, loop diuretics, thiazides and potassium-sparing diuretics. Diuretics rapidly improve the symptoms of heart failure (within hours to days). Diuretics reduce excess volume that accumulates with heart failure and decrease pulmonary edema that causes symptoms of dyspnea and orthopnea[6]. Lasix 20 to 40 mg PO daily is a conventional starting dose, but in some patients, torsemide may be a better choice due to its more predictable absorption. Once a day dosing of a given diuretic is preferred to twice a day dosing at a lower dose. A rise in BUN and Cr may reflect a reduction in renal perfusion, and further diuresis should only be undertaken with careful monitoring of renal function. The patient should weigh themselves each morning at the same time on the same scale, and the diuretic dosing should be adjusted to maintain a constant weight. Given the risk of hypokalemia or hyperkalemia, the blood level of electrolyes should be checked regularly.
ACE Inhibition and Angiotensin Receptor Blockade: Second Step in the Management of Heart Failure
After diuretics are started or at the same time they are started, an ACE inhibitor can be initiated [7]. This includes a large group of drugs, such as Enalapril (Vasotec/Renitec), Ramipril (Altace/Tritace/Ramace/Ramiwin), Quinapril (Accupril), Perindopril (Coversyl/Aceon), Lisinopril (Lisodur/Lopril/Novatec/Prinivil/Zestril) and Benazepril (Lotensin). They can improve symptoms and prognosis of heart failure in several ways including afterload reduction and favorable ventricular remodeling. Usual side effects include dry cough and angioedema. Patients with bilateral renal artery stenosis or severe renal impairment are not appropriate for angiotensin converting enzyme inhibitor (ACEI).
During or after the initiation of diuresis, one could start, for example, lisinopril 5 mg Q day. Every 1 – 2 weeks, the dose would be escalated to achieve a target dose of 15 to 20 mg Q day. An ACE inhibitor is initiated before a beta blocker because an ACE inhibitor achieves its hemodynamic effect more rapidly, and is less likely to cause a decline in hemodynamics. Although there is some data to suggest that aspirin blunts the hemodynamic effect of ACE inhibitors, there is no data to suggest that aspirin reduces the clinical efficacy of ACE inhibitors in heart failure patients. Aspirin should be administered to patients with ischemic heart disease, but not to patients without it.
If a patient cannot tolerate a an ACE inhibitor (develops a cough), then an Angiotensin II receptor blocker can be administered in its place. Angiotensin II receptor antagonists block the activation of angiotensin II AT1 receptors. Blockade of AT1 receptors directly causes vasodilation, reduces secretion of vasopressin, reduces production and secretion of aldosterone. Because angiotensin II receptor antagonists do not inhibit the breakdown of bradykinin or other kinins, and are thus only rarely associated with the persistent dry cough and/or angioedema that limit ACE inhibitor therapy. Commonly administered agents in the management of heart failure include Candesartan, Valsartan, Telmisartan, Losartan, Irbesartan, and Olmesartan. The effectiveness of switching to an ARB from and ACE inhibitor was demonstrated for candesartan in the CHARM Alternative trial [8].
In general, ARBs are as effective or slightly less effective than ACE inhibitors in the treatment of congestive heart failure.[9][10] It is a class 2a recommendation to substitute an ARB as an alternative to ACE inhibitors if the patient is already taking an ARB for another indication.[11]
The efficacy of adding an ARB to an ACE inhibitor was assessed in the CHARM Added trial[12]. While there was a reduction in the composite primary endpoint in the study, there was no reduction in mortality. Furthermore, the VALIANT trial demonstrated that an ARB should not be added to an ACE inhibitor in the post MI setting. These results for ARBs are in contrast to the results of the EMPHASIS HF trial showed that the addition of eplerenone (an aldosterone antagonist) to ACE inhibition improved clinical outcomes including mortality among patients with class II or III heart failure with a reduced LVEF.[13] Thus, based upon the mortality benefit observed in the EMPHASIS HF trial, an aldosterone antagonist rather than and ARB should be added to an ACE inhibitor in patients with NYHA class II heart failure and an LVEF < 30%, in the post-MI patient who has an LVEF < 40% who has heart failure symptoms or diabetes, and the patient with class III or IV heart failure who has an LVEF < 35%.
“Triple therapy”, the combined use of an ACE inhibitor, an ARB and an aldosterone antagonist is a relative contraindication.
Beta blockers: Third Step in the Management of Heart Failure
Beta blockers reduce the heart rate which lowers the myocardial energy expenditure. They also prolong diastolic filling and lengthen the period of coronary perfusion. Beta blockers can also decrease the toxicity of catecholamines on the myocardium.
Once you have achieved a stable dose of a diuretic and an ACE inhibitor, then one of the three beta blockers that have been associated with improved survival (carvedilol, metoprolol succinate or bisoprolol) can be added and the dose titrated based upon the patient’s tolerance. You should avoid beta-blockers with intrinsic sympathomimetic activity (pindolol or acebutolol). It should be noted that the 35% reduction in one year mortality observed in meta-analyses of beta-blockers in heart failure was when these drugs were added to ACE inhibitors[14]. There are no direct comparisons of the various beta-blockers, but some data does suggest that carvedilol may improve LVEF more than the others, but it may not be as well tolerated due to its vasodilatory properties. If the patient has been over diuresed, they may not tolerate the addition of a beta blocker.
- Relative contraindications to beta-blocker administration include the following:
- Asthma or bronchospasm
- Hypotension resulting in poor end organ perfusion or symptoms
- Bradycardia or heart block (first degree heart block with a PR interval > 0.24, second degree heart block, third degree heart block
- Peripheral arterial disease with limb ischemia at rest
- Moderate or greater peripheral edema
- Recent intravenous inotropic therapy
Given the potential for hemodynamic decompensation, the initiation of beta-blockers is best undertaken by an individual or center specializing in heart failure management. The patient should be aware of potential side effects, and should be aware that it may take one to three months for the beta-blockers to improve heart failure symptoms. Therapy is initiated with very low doses, and the dose of the beta-blocker should be doubled every two weeks until the target dose is achieved or symptoms prevent further dose escalation.
- Carvedilol: Initial dose 3.125 mg twice daily, target dose 25 to 50 mg twice daily
- Metoprolol succinate: Initial dose 12.5 mg daily, target dose 200 mg daily
- Bisoprolol: Initial dose 1.25 mg daily, target dose 5 to 10 mg daily
Weight gain or peripheral edema that is not responsive to diuresis may require a reduction in the dose of beta-blockers.
Aldosterone Antagonism: Fourth Step in the Management of Heart Failure
An aldosterone antagonist can be added to the regimen of ‘select’ patients. These selected patients include:
- Class II heart failure and a left ventricular ejection fraction (LVEF) < 30%
- Class III/IV heart failure and a LVEF <35%
- Post ST segment elevation MI and a LVEF < 40% who have either symptomatic heart failure or diabetes.
- The serum potassium must be under 5.0 meq/li and the glomerular filtration rate (GFR) should be > 30 cc per minute
A requirement for aldosterone antagonist is that the patient’s renal function and potassium can be carefully monitored. Eplerenone has fewer endocrine side effects (1%) than spironolactone (10%), but is more costly. A reasonable strategy is to initiate therapy with spironolactone at a dose of 25 to 50 mg daily, and then switch to eplerenone at a dose of 25 to 50 mg daily if endocrine side effects develop.
Risk Factors for the Development of Hyperkalemia on an Aldosterone Antagonist
- Triple therapy with an ACE inhibitor and angiotensin II receptor blocker makes this combination a contraindication
- Higher doses of either an ACE inhibitor or an angiotensin receptor blocker (ARB)
- Hyperkalemia prior to initiation of spironolactone
- Comorbidities such as diabetes and chronic renal insufficiency
- Higher NYHA heart failure class
- Concomitant administration of beta blockers, nonsteroidal anti-inflammatory drugs (NSAIDs) or potassium supplements
- A daily dose of Spironolactone greater than 50 mg
The Combination of Hydralazine and a Nitrate: Fifth step in the Management of Heart Failure
The combination of hydralazine and a nitrate (particularly among black patients) can be added if the patient continues to have symptoms on a diuretic, ACE inhibitor (or ARB in the intolerant patient) and a beta blocker. The initial dose is isosorbide dinitrate 20 mg three times a day along with hydralazine 25 mg three times a day. The dose(s) can be increased every 2 to 4 weeks to a target dose of isosorbide dinitrate 40 mg three times a day and hydralazine 75 mg three times a day.
Digoxin: Sixth step in the Management of Heart Failure
Digitalis can strengthen the contractility of the heart and can also be useful to achieve rate control in patients with heart failure who also have atrial fibrillation. In the DIG trial, digoxin reduced the rate of re-hospitalization but did not improve mortality among all patients enrolled in the trial.[15] However, in a retrospective analysis, mortality was reduced in male patients who had digoxin levels between 0.5 and 0.8 ng/mL and was increased in male patients with digoxin levels > 1.2 ng/ml.[16] A similar trend was observed among women patients: there was a trend towards lower mortality at digoxin concentrations between 0.5 to 0.9 ng/ml, but significantly higher mortality at digoxin concentrations > 1.2 ng/ml.[17]
Digoxin should not be used as primary therapy for congestive heart failure. The administration of digoxin is reasonable in patients with NYHA class II-IV heart failure symptoms who have an LVEF of < 40% despite treatment with diuretics, angiotensin-converting enzyme inhibitors, beta blockers, and an aldosterone antagonist. Small doses of 0.125 mg per day of digoxin are often effective in maintaining a serum digoxin level between 0.5 and 0.8 ng/ml.
Cardiac Resynchronization Therapy
Cardiac Resynchronization Therapy (CRT) is recommended in congestive heart failure patients with:
- Symptoms: NYHA Class II-IV
- QRS: A prolonged QRS interval > 0.12
- LVEF: A LVEF < 30% to 35%
Percutaneous Coronary Intervention (PCI):
Coronary artery disease (CAD) and impaired blood flow to the heart is one of the main causes of heart failure. Relieving the blockages in the coronary arteries can improve overall heart function, which may improve or resolve heart failure symptoms. The procedure is usually performed in a cardiac catherization laboratory. A catheter, a very small tube with a tiny deflated balloon on the end, is inserted through an incision in the groin area and then guided over a floppy wire to the section of the diseased artery. The balloon is then inflated to prop open the artery. The balloon is deflated and withdrawn once the artery has been fully opened. A stent may be placed during the procedure to keep the blood vessel open. Clinical trials have demonstrated that percutaneous coronary intervention (PCI) is a very effective and safe procedure to dilate blocked vessels and can improve a patient’s symptoms if ischemia or lack of blood flow is the problem.
Left Ventricular Assist Device (LVAD):
A left ventricular assist device (LVAD) is a mechanical pump-type device that can help maintain the pumping ability of a failing heart. One type of LVAD has tubing that pulls blood from the left ventricle into a pump. The pump then ejects blood into the aorta. LVADs are typically used for weeks to months as a “bridge” to more definitive therapy such as a heart transplant rather than as a final or “destination” therapy.
Intracardiac defibrillator
Fifty percent of patients with heart failure die of sudden cardiac death. ICDs are indicated for patients with previous myocardial infarction and an LVEF <30%, sustained ventricular tachycardia, inducible ventricular tachycardia. The morbidity and mortality benefit of ICD placement compared with anti-arrhythmic drug therapy is controversial.
Ultrafiltration
In the setting of congestive heart failure, ultrafiltration has been associated with a reduced incidence of hospitalization compared with diuretics in the UNLOAD trial, but no difference in mortality.
Heart Transplantation
A Heart transplant may be the only effective treatment option for patients with severe, progressive heart failure that can not be helped by medications, dietary and lifestyle changes. During a heart transplant procedure, the surgeons connect the patient to a heart-lung machine, which takes over the functions of the heart and lungs. Then the surgeons remove the diseased heart and replace it with the donor heart. Finally, the major blood vessels are reconnected and the new heart is ready to work. The outlook for people with heart transplants is good during the first few years after the transplant. Over 85 percent of patients are alive more than a year after their heart transplant.
End-of-life considerations
End of life care in the patient with congestive heart failure is focused on making the patient comfortable. Invasive procedures should be minimized, and patients may elect to have their defibrillators inactivated. The growing number of patients with Stage IV heart failure (intractable symptoms of fatigue, shortness of breath or chest pain at rest despite optimal medical therapy) should be considered for palliative care or hospice, according to American College of Cardiology/American Heart Association guidelines listed below. Some have argued that any patient with NYHA class III CHF should have a palliative care referral. Palliative care can not only provide symptom management, but also assist with advanced care planning, goals of care in the case of a significant decline, and making sure the patient has a medical power of attorney and discussed his or her wishes with this individual.
Treatment of special populations
There is unfortunately insufficient data in subgroups of patients to mandate a change to guidelines recommendations regarding the management of heart failure. Dosages should be altered as needed in the elderly or in those with altered metabolism. African american patients may respond to the addition of hydralazineand nitrates to the standard of care in the treatment of heart failure.
References
- ↑ Yancy CW, Jessup M, Bozkurt B, Masoudi FA, Butler J, McBride PE; et al. (2013). “2013 ACCF/AHA Guideline for the Management of Heart Failure: A Report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines”. J Am Coll Cardiol. doi:10.1016/j.jacc.2013.05.019. PMID 23747642.
- ↑ DeGroot WJ, Leonard JJ (1970). “Hyperthyroidism as a high cardiac output state”. Am Heart J. 79 (2): 265–75. PMID 4903771.
- ↑ Evangelista LS, Shinnick MA (2008). “What do we know about adherence and self-care?”. J Cardiovasc Nurs. 23 (3): 250–7. doi:10.1097/01.JCN.0000317428.98844.4d. PMC 2880251. PMID 18437067.
- ↑ Martins Wde A, Ribeiro MD, Oliveira LB, Barros Lda S, Jorge AC, Santos CM; et al. (2011). “Influenza and pneumococcal vaccination in heart failure: a little applied recommendation”. Arq Bras Cardiol. 96 (3): 240–5. PMID 21271169.
- ↑ Pfeffer MA, McMurray JJ, Velazquez EJ, Rouleau JL, Køber L, Maggioni AP, Solomon SD, Swedberg K, Van de Werf F, White H, Leimberger JD, Henis M, Edwards S, Zelenkofske S, Sellers MA, Califf RM (2003). “Valsartan, captopril, or both in myocardial infarction complicated by heart failure, left ventricular dysfunction, or both”. The New England Journal of Medicine. 349 (20): 1893–906. doi:10.1056/NEJMoa032292. PMID 14610160. Retrieved 2013-04-29. Unknown parameter
|month=ignored (help) - ↑ Michael Felker G (2010). “Diuretic management in heart failure”. Congest Heart Fail. 16 Suppl 1: S68–72. doi:10.1111/j.1751-7133.2010.00172.x. PMID 20653715.
- ↑ Shiokawa Y (1975). “Proceedings: Streptococcus surveys in Ryukyu Islands, Japan”. Jpn Circ J. 39 (2): 168–71. PMID 1117548.
- ↑ Granger CB, McMurray JJ, Yusuf S, Held P, Michelson EL, Olofsson B, Ostergren J, Pfeffer MA, Swedberg K (2003). “Effects of candesartan in patients with chronic heart failure and reduced left-ventricular systolic function intolerant to angiotensin-converting-enzyme inhibitors: the CHARM-Alternative trial”. Lancet. 362 (9386): 772–6. doi:10.1016/S0140-6736(03)14284-5. PMID 13678870. Retrieved 2013-04-29. Unknown parameter
|month=ignored (help) - ↑ Jong P, Demers C, McKelvie RS, Liu PP (2002). “Angiotensin receptor blockers in heart failure: meta-analysis of randomized controlled trials”. Journal of the American College of Cardiology. 39 (3): 463–70. PMID 11823085. Retrieved 2013-04-29. Unknown parameter
|month=ignored (help) - ↑ Pitt B, Poole-Wilson PA, Segal R, Martinez FA, Dickstein K, Camm AJ, Konstam MA, Riegger G, Klinger GH, Neaton J, Sharma D, Thiyagarajan B (2000). “Effect of losartan compared with captopril on mortality in patients with symptomatic heart failure: randomised trial–the Losartan Heart Failure Survival Study ELITE II”. Lancet. 355 (9215): 1582–7. PMID 10821361. Retrieved 2013-04-29. Unknown parameter
|month=ignored (help) - ↑ Hunt SA, Abraham WT, Chin MH, Feldman AM, Francis GS, Ganiats TG, Jessup M, Konstam MA, Mancini DM, Michl K, Oates JA, Rahko PS, Silver MA, Stevenson LW, Yancy CW (2009). “2009 focused update incorporated into the ACC/AHA 2005 Guidelines for the Diagnosis and Management of Heart Failure in Adults: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines: developed in collaboration with the International Society for Heart and Lung Transplantation”. Circulation. 119 (14): e391–479. doi:10.1161/CIRCULATIONAHA.109.192065. PMID 19324966. Retrieved 2013-04-29. Unknown parameter
|month=ignored (help) - ↑ McMurray JJ, Ostergren J, Swedberg K, Granger CB, Held P, Michelson EL, Olofsson B, Yusuf S, Pfeffer MA (2003). “Effects of candesartan in patients with chronic heart failure and reduced left-ventricular systolic function taking angiotensin-converting-enzyme inhibitors: the CHARM-Added trial”. Lancet. 362 (9386): 767–71. doi:10.1016/S0140-6736(03)14283-3. PMID 13678869. Retrieved 2013-04-29. Unknown parameter
|month=ignored (help) - ↑ Zannad F, McMurray JJ, Krum H, van Veldhuisen DJ, Swedberg K, Shi H, Vincent J, Pocock SJ, Pitt B (2011). “Eplerenone in patients with systolic heart failure and mild symptoms”. The New England Journal of Medicine. 364 (1): 11–21. doi:10.1056/NEJMoa1009492. PMID 21073363. Retrieved 2013-04-29. Unknown parameter
|month=ignored (help) - ↑ Brophy JM, Joseph L, Rouleau JL (2001). “Beta-blockers in congestive heart failure. A Bayesian meta-analysis”. Annals of Internal Medicine. 134 (7): 550–60. PMID 11281737. Retrieved 2013-04-28. Unknown parameter
|month=ignored (help) - ↑ “The effect of digoxin on mortality and morbidity in patients with heart failure. The Digitalis Investigation Group”. The New England Journal of Medicine. 336 (8): 525–33. 1997. doi:10.1056/NEJM199702203360801. PMID 9036306. Retrieved 2013-04-29. Unknown parameter
|month=ignored (help) - ↑ Rathore SS, Curtis JP, Wang Y, Bristow MR, Krumholz HM (2003). “Association of serum digoxin concentration and outcomes in patients with heart failure”. JAMA : the Journal of the American Medical Association. 289 (7): 871–8. PMID 12588271. Retrieved 2013-04-29. Unknown parameter
|month=ignored (help) - ↑ Adams KF, Patterson JH, Gattis WA, O’Connor CM, Lee CR, Schwartz TA, Gheorghiade M (2005). “Relationship of serum digoxin concentration to mortality and morbidity in women in the digitalis investigation group trial: a retrospective analysis”. Journal of the American College of Cardiology. 46 (3): 497–504. doi:10.1016/j.jacc.2005.02.091. PMID 16053964. Retrieved 2013-04-29. Unknown parameter
|month=ignored (help)
Classification
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1];Associate Editor(s)-in-Chief: Mitra Chitsazan, M.D.[2], Sara Zand, M.D.[3] Jair Basantes de la Calle, M.D.
Overview
LVEF has an important role in the classification of patients with HF because of differing prognosis and response to treatments. In the guideline of 2022 AHA, HFrEF is defined as LVEF ≤40% . HF with preserved EF (HFpEF) including approximately 50% of the population with HF with increased prevalence. HFpEF is defined as LVEF ≥50%. Heaet failure improved EF is considered when follow-up LVEF reaches more than 40%.
Classification
Several classification systems are used to characterize heart failure according to the: [1] [2]
- The pathophysiology of heart failure:
- Systolic vs diastolic heart failure
- Left-sided, right-sided or biventricular heart failure
- Low output vs high output heart failure
- The underlying physiology based on left ventricular ejection fraction:
- Heart failure with reduced ejection fraction (HFrEF), heart failure with mid-range ejection fraction (HFmrEF), heart failure with preserved ejection fraction (HFpEF)
- The chronicity of heart failure:
- acute or chronic
- The severity of symptoms of heart failure:
- New York Heart Association Class (NYHA class)
- Killip class (severity of the symptoms in the acute setting after myocardial infarction)
- The stage (progression of the disease) of congestive heart failure:
- The American College of Cardiology Foundation/American Heart Association (ACCF/AHA) classification: A, B, C, D.
1. Systolic versus Diastolic Heart Failure
- Systolic Dysfunction: The left ventricular ejection fraction is reduced in systolic dysfunction and there is depressed contractility of the heart.
- Diastolic Dysfunction: The left ventricular ejection fraction is preserved in diastolic dysfunction and there is an abnormality in myocardial relaxation or excessive myocardial stiffness. Systolic and diastolic dysfunction commonly occur in conjunction with each other.
2. Left-, Right- and Biventricular Failure
Another common method of classifying heart failure is based upon the ventricle involved.
- Left-ventricular Heart Failure: There is impaired left ventricular function with the reduced flow into the aorta.
- Right-ventricular Heart Failure: There is impaired right ventricular function with the reduced flow into the pulmonary artery and lungs.
- Biventricular Failure: The most common cause of right heart failure is left heart failure, and mixed presentations are common, especially when the cardiac septum is involved.
3. High output versus Low output Heart Failure
- Low Output Failure: The cardiac output is reduced, and the systemic vascular resistance (SVR) is high. In low output failure, there is an inadequate supply of blood flow to meet normal metabolic demands.
- High Output Failure: The cardiac output is increased, and the systemic vascular resistance (SVR) is low. Rather than an inadequate supply of blood flow to meet normal metabolic demands as occurs in low output failure, in high output failure there is an excess requirement for oxygen and nutrients and the demand outstrips what the heart can provide.[3] Causes of high output heart failure include severe anemia, Gram negative septicaemia, beriberi (vitamin B1/thiamine deficiency), thyrotoxicosis, Paget’s disease, arteriovenous fistulae, or arteriovenous malformations.
4. Classification of Heart Failure Based on the Ejection Fraction (EF)
- HFrEF is defined as LVEF <_40% or significant reduction in LV systolic function.
- HFmrEF is defined when LVEF is between 41% and 49% or there is mildly reduced LV systolic function.
- HF p EF is defined as LVEF >_50%, with symptoms and signs of heart failure , with evidence of structural and/or functional cardiac abnormalities and/or high level of natriuretic peptides (NPs).
Abbreviations: HF: Heart failure; HFmrEF: Heart failure with mildly reduced ejection fraction; HFpEF: Heart failure with preserved ejection fraction ; HFrEF: Heart failure with reduced ejection fraction; LV: Left ventricle; LVEF: Left ventricular ejection fraction;
| HFrEF | HFmrEF | HFpEF |
|---|---|---|
| Symptoms± Signs, LVEF ≤ 40% | Symptoms± Signs, LVEF ≥ 41%-49% | Symptoms± Signs, LVEF≥ 50%, cardiac structure and function abnormalities,
LV diastolic dysfunction, high LV filling pressures, high natriuretic peptides |
| The above table adopted from 2021 ESC Guideline |
|---|
| Classification of heart failure by LVEF | |
| Type of heart failure according to LVEF | Criteria |
| HFrEF (heart failure with reduced EF) | LVEF ≤ 40% |
| HFimpEF ( heart failure with improved EF) | |
| HFmrEF (heart failure with mildly reduced EF) |
|
| HFpEF (heart failure with preserved EF) |
|
| The above table adopted from 2022 AHA Guideline |
|---|
5. Chronicity of Heart Failure
- Acute or Decompensated: Acute or decompensated heart failure is a term used to describe exacerbated or decompensated heart failure, and refers to an episode in which a patient sustains a change in heart failure signs and symptoms that necessitates urgent therapy or hospitalization.[6]
- Chronic: There is stable symptomatology in chronic heart failure.
6. The Severity of Heart Failure
The NYHA functional classification is used to describe the severity of symptoms and exercise intolerance in patients with congestive heart failure.
| The New York Heart Association Criteria (NYHA) | |
| NYHA Class | Definition |
| NYHA I | No symptoms with ordinary activity |
| NYHA II |
Slight limitation of physical activity. Comfortable at rest, but ordinary physical activity results in fatigue, palpitation, dyspnea, or angina. |
| NYHA III |
Marked limitation of physical activity. Comfortable at rest, but less than ordinary physical activity results in fatigue, palpitation, dyspnea, or anginal pain. |
| NYHA IV | Unable to carry out any physical activity without discomfort. Symptoms are present at rest. |
7. The Stages of heart failure
The ACC/AHA classification system was introduced to emphasize the natural history of the heart failure syndrome and to identify opportunities to intervene earlier and prevent disease progression.
| 2022 AHA/ACC/HFSA Guideline for the Management of Heart Failure: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Stages of Heart Failure | |||
| Stages | Definition | Example | Corresponding NYHA class |
| A |
|
|
None |
| B | Patients without current or previous sings/ symptoms of HF but evidence of the following: |
|
NYHA class I |
| C | Patient with past or current symptoms/ signs of HF | The trajectory of Stage C HF:
|
NYHA classes I, II, III, and IV |
| D | Profound HF symptoms. | Patients have symptoms that interfere with daily life activities. They may also have recurrent hospitalizations despite attempts to optimize guideline-directed medical therapy. | NYHA class IV |
References
- ↑ Aurigemma GP (2006). “heart failure–a common and lethal condition by any name”. N Engl J Med. 355 (3): 308–10. doi:10.1056/NEJMe068128. PMID 16855273.
- ↑ Yancy CW, Jessup M, Bozkurt B, Masoudi FA, Butler J, McBride PE; et al. (2013). “2013 ACCF/AHA Guideline for the Management of Heart Failure: A Report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines”. J Am Coll Cardiol. doi:10.1016/j.jacc.2013.05.019. PMID 23747642.
- ↑ Template:DorlandsDict
- ↑ McDonagh TA, Metra M, Adamo M, Gardner RS, Baumbach A, Böhm M, Burri H, Butler J, Čelutkienė J, Chioncel O, Cleland J, Coats A, Crespo-Leiro MG, Farmakis D, Gilard M, Heymans S, Hoes AW, Jaarsma T, Jankowska EA, Lainscak M, Lam C, Lyon AR, McMurray J, Mebazaa A, Mindham R, Muneretto C, Francesco Piepoli M, Price S, Rosano G, Ruschitzka F, Kathrine Skibelund A (September 2021). “2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure”. Eur Heart J. 42 (36): 3599–3726. doi:10.1093/eurheartj/ehab368. PMID 34447992 Check
|pmid=value (help). Vancouver style error: initials (help) - ↑ 5.0 5.1 Heidenreich PA, Bozkurt B, Aguilar D, Allen LA, Byun JJ, Colvin MM; et al. (2022). “2022 AHA/ACC/HFSA Guideline for the Management of Heart Failure: Executive Summary: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines”. Circulation. 145 (18): e876–e894. doi:10.1161/CIR.0000000000001062. PMID 35363500 Check
|pmid=value (help). - ↑ Jessup. M, et al. 2009 Focused Update: ACCF/AHA Guidelines for the Diagnosis and Management of Heart Failure in Adults. Circulation. 2009 Apr 14;119(14):1977-2016. PMID 19324967
Pathophysiology
Systolic dysfunction | Diastolic dysfunction | HFpEF | HFrEF
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Cafer Zorkun, M.D., Ph.D. [2]; Saleh El Dassouki, M.D [3]; Atif Mohammad, MD
Overview
Heart failure is a complex syndrome whereby there is inadequate output of the heart to meet the metabolic demands of the body. Heart failure is caused by abnormal function of different anatomic parts of the heart including the pericardium, the myocardium, the endocardium, the heart valves and the great vessels. Heart failure is characterized by decreased cardiac output but not necessarily decreased ejection fraction. Symptoms of heart failure are due to a lack of both forward blood flow to the body, and backward flow into the lungs. The body tries to compensate for the low cardiac output by mechanisms that increase the preload and afterload. These mechanisms lead to exacerbation of the cardiac malfunction and symptoms associated with heart failure.
Pathophysiology
Decreased Cardiac Output
- Heart failure is defined as the inability of the heart to pump enough blood to meet the demands of the body.
- Therefore, heart failure is characterized by a reduced stroke volume as a result of a failure of systole, diastole or both:
- Systolic heart failure: Increased end systolic volume is usually caused by reduced contractility.
- Diastolic heart failure: Decreased end diastolic volume results from impaired ventricular filling, as occurs when the compliance of the ventricle falls (i.e. when the walls stiffen in diastolic dysfunction).
- Heart failure was once thought to be secondary to a depressed left ventricular ejection fraction. However, studies have shown that approximately 50% of patients who are diagnosed with heart failure have a normal ejection fraction (diastolic dysfunction). Patients may be broadly classified as having heart failure with depressed left ventricular ejection fraction (systolic dysfunction) or normal/preserved ejection fraction (diastolic dysfunction). Systolic and diastolic dysfunction commonly occur in conjunction with each other.
- Normally, blood flows from the lungs, into the pulmonary veins, into the left atrium, through the mitral valve, and finally into the left ventricle. When the left ventricle cannot be normally filled during diastole in both diastolic and systolic heart failure, blood will back up into the left atrium and, eventually, into the lungs. The result is a higher than normal pressure of blood within the vessels of the lung. As a result of hydrostatic forces, this high pressure leads to leaking of fluid (i.e. transudate) from the lung’s vasculature into the air-spaces (alveoli) of the lungs. The result is pulmonary edema, a condition characterized by difficulty breathing, inadequate oxygenation of blood, and, if severe and untreated, death.
Underlying Cardiac Abnormalities Leading to Heart Failure
Heart failure may result from an abnormality or dysfunction of any one of the anatomical structures of the heart:
- Pericardium
- It can be damaged by infiltration of inflammatory cells (e.g. pericarditis) or fluid (pericardial effusion).
- Myocardium
- It can be damaged by ischemic injury (e.g. acute MI), toxins (e.g. chemotherapy), infiltration by inflammatory cells (e.g. myocarditis), pressure overload (e.g. hypertension or aortic stenosis), metabolic derangements, or volume overload (aortic insufficiency or mitral insufficiency).
- Endocardium
- It can be damaged by infiltration
- Valvular heart disease
- Valves can be damaged or dysfunctional from birth (bicuspid aortic valve) or can be acquired (e.g. endocarditis or rheumatic heart disease).
- Disorders of the great vessels
- Great vessels can be stiffened by atherosclerosis (e.g. hypertension) or can be chronically constricted (e.g. pulmonary hypertension)
Systolic versus Diastolic Dysfunction
Systolic Dysfunction
- Heart failure caused by systolic dysfunction is more readily recognized. It can be simplistically described as failure of the pump function of the heart.
- It is characterized by a decreased ejection fraction (less than 40%-45%). The strength of ventricular contraction is attenuated and inadequate for creating an adequate stroke volume, resulting in inadequate cardiac output. In general, this is caused by dysfunction or destruction of cardiac myocytes or their molecular components.
- In congenital diseases such as Duchenne muscular dystrophy, the molecular structure of individual myocytes is affected.
- Myocytes and their components can be damaged by inflammation (such as in myocarditis) or by infiltration (such as in amyloidosis).
- Toxins and pharmacological agents (such as ethanol, cocaine, and amphetamines) cause intracellular damage and oxidative stress.
- The most common mechanism of damage is ischemia causing infarction and scar formation.
- After myocardial infarction, dead myocytes are replaced by scar tissue, deleteriously affecting the function of the myocardium. On echocardiogram, this is manifest by abnormal or absent wall motion.
- Because the ventricle is inadequately emptied, ventricular end-diastolic pressure and volumes increase. This is transmitted to the atrium. On the left side of the heart, the increased pressure is transmitted to the pulmonary vasculature, and the resultant hydrostatic pressure favors extravasation of fluid into the lung parenchyma, causing pulmonary edema. On the right side of the heart, the increased pressure is transmitted to the systemic venous circulation and systemic capillary beds, favoring extravasation of fluid into the tissues of peripheral organs and extremities, resulting in dependent peripheral edema.
- Shown below is an image summarizing the pathophysiology of systolic heart failure.

Diastolic Dysfunction
- Heart failure caused by diastolic dysfunction is generally described as the failure of the ventricular chambers to adequately relax and results from stiffening of the ventricular walls. The consequence is reduced filling of chambers of the heart.
- The failure of ventricular relaxation also results in elevated end-diastolic pressures, and the end result is identical to the case of systolic dysfunction (pulmonary edema in left heart failure, peripheral edema in right heart failure.)
- Diastolic dysfunction can be caused by processes similar to those that cause systolic dysfunction, particularly causes that affect cardiac remodeling.
- Diastolic dysfunction typically becomes symptomatic in physiological conditions under which a high cardiac demand is required. Therefore, patients suffering from diastolic dysfunction are sensitive to increases in heart rate, and sudden bouts of tachycardia (which can be caused simply by physiological responses to exertion, fever, or dehydration, or by pathological tachyarrhythmias such as atrial fibrillation with rapid ventricular response) which may result in flash pulmonary edema.
- Adequate rate control (usually with a pharmacological agent that slows down atrioventricular node conduction such as a calcium channel blocker or a beta-blocker) is therefore key to preventing decompensation.
- Left ventricular diastolic function can be determined through echocardiography by measurement of various parameters such as the E/A ratio (early-to-atrial left ventricular filling ratio), the E (early left ventricular filling) deceleration time, and the isovolumetric relaxation time.
Manifestations of Heart Failure
Pulmonary Edema
- The reduction in forward cardiac output leads to a rise in the pulmonary capillary wedge pressure. Rales usually develop if the pulmonary capillary wedge pressure is >25 mm Hg. Rales may not be present in the patient with chronic heart failure. Rales may develop at even lower pressures if left ventricular function deteriorates suddenly.
- Dyspnea and orthopnea occur due to interstitial edema within the lungs at lower pressures.
Hypotension
- Heart failure is characterized by decreased cardiac output and hence it causes low blood pressure.
Hypoperfusion
The reduction in forward cardiac output leads to hypoperfusion at rest which manifests as:
- Cool extremities
- Confusion and altered mentation
- Impaired renal perfusion and declining renal function (increased blood urea nitrogen [BUN] and serum creatinine [Cr] ; mostly leading to pre-renal failure [BUN:Cr > 20])
- Reduced perfusion of skeletal muscle causes atrophy of the muscle fibres. This can result in weakness, increased fatigue and decreased peak strength, all contributing to exercise intolerance and claudication.[1]
- In severe heart failure, the effects of decreased cardiac output and poor perfusion become more apparent, and patients will manifest symptoms of systemic hypoperfusion including generalized weakness, dizziness, and syncope.
Impaired Cardiac Reserve
As the heart works harder to meet normal metabolic demands, the amount cardiac output can increase in times of increased oxygen demand (e.g. exercise) is reduced. This contributes to the exercise intolerance commonly seen in heart failure. This translates to the loss of one’s cardiac reserve. The cardiac reserve refers to the ability of the heart to work harder during exercise or strenuous activity. Since the heart has to work harder to meet the normal metabolic demands, it is incapable of meeting the metabolic demands of the body during exercise.
Compensatory Mechanisms and Their Associated Complications
- Shown below is an image summarizing the compensatory mechanisms of the heart along with their associated complications.

- Left ventricular systolic dysfunction is associated with a reduction in stroke volume, the amount of blood the heart ejects with each heart beat.
- The reduction in stroke volume leads to a reduction in cardiac output which is the stroke volume multiplied by the heart rate.
- There are several mechanisms to preserve forward cardiac output (the product of stroke volume and heart rate):
- Dilation of the left ventricle to increase the stroke volume and
- Increase in heart rate
Dilatation of the Left Ventricle:
- Dilation of the left ventricle increases volume and increases contractility up to a point (see Frank-Starling law of the heart). As further LV dilation occurs, however, contractility drops. This is due to reduced ability to cross-link actin and myosin filaments in over-stretched heart muscle.[2].
- As further dilation occurs, functional mitral regurgitation (MR) may develop despite an anatomically normal mitral valve.
- Left ventricular enlargement and lack of forward cardiac output can lead to left atrial enlargement. Left atrial dilation may lead to atrial fibrillation which occurs in 20% of patients with congestive heart failure. Atrial fibrillation diminishes left ventricular filling through the loss of the atrial kick (the atrial contraction) and due to an increase in the heart rate which reduces the time available for the left ventricle to fill.
Hypertrophy of the Myocardium:
- Hypertrophy (an increase in physical size) of the myocardium can develop, which is caused by the terminally differentiated heart muscle fibers increasing in size in an attempt to improve contractility. This may contribute to the increased stiffness and decreased ability to relax during diastole.
Activation of the Sympathetic Nervous System:
- Arterial blood pressure falls. This destimulates baroreceptors in the carotid sinus and aortic arch which link to the nucleus tractus solitarius. This center in the brain increases sympathetic activity, releasing catecholamines into the blood stream. Binding to alpha-1 receptors results in systemic arterial vasoconstriction. This helps restore blood pressure but also increases the total peripheral resistance, increasing the workload of the heart. Binding to beta-1 receptors in the myocardium increases the heart rate and make contractions more forceful, in an attempt to increase cardiac output. This also, however, increases the amount of work the heart has to perform.
- The increased heart rate, stimulated by increased sympathetic activity[3] maintains cardiac output. Initially, this helps compensate for heart failure by maintaining blood pressure and perfusion, but places further strain on the myocardium, increasing coronary perfusion requirements, which can lead to worsening of ischemic heart disease. Sympathetic activity may also cause potentially fatal arrhythmias.
- Increased sympathetic stimulation also causes the hypothalamus to secrete vasopressin (also known as antidiuretic hormone or ADH), which causes free water retention in the kidneys leading to hyponatremia. This free water retention increases total body blood volume and blood pressure.
Stimulation of the Renal / Adrenal / Sympathetic Axis:
- Reduced perfusion (blood flow) to the kidneys stimulates the release of renin – an enzyme which catalyses the production of the potent vasopressor angiotensin. Angiotensin and its metabolites cause further vasocontriction, and stimulate increased secretion of the steroid aldosterone from the adrenal glands. This promotes salt and fluid retention at the kidneys, also increasing the blood volume.
- The chronically high levels of circulating neuroendocrine hormones such as catecholamines, renin, angiotensin, and aldosterone affects the myocardium directly, causing structural remodelling of the heart over the long term. Many of these remodelling effects seem to be mediated by transforming growth factor beta (TGF-beta), which is a common downstream target of the signal transduction cascade initiated by catecholamines[4] and angiotensin II,[5] and also by epidermal growth factor (EGF), which is a target of the signaling pathway activated by aldosterone[6]
- The increased peripheral resistance and greater blood volume place further strain on the heart and accelerates the process of damage to the myocardium. Vasoconstriction and fluid retention produce an increased hydrostatic pressure in the capillaries. This shifts the balance of forces in favour of interstitial fluid formation as the increased pressure forces additional fluid out of the blood, into the tissue. This results in edema (fluid build-up) in the tissues. In right-sided heart failure this commonly starts in the ankles where venous pressure is high due to the effects of gravity (although if the patient is bed-ridden, fluid accumulation may begin in the sacral region.) It may also occur in the abdominal cavity, where the fluid build-up is called ascites. In left-sided heart failure edema can occur in the lungs – this is called cardiogenic pulmonary edema. This reduces spare capacity for ventilation, causes stiffening of the lungs and reduces the efficiency of gas exchange by increasing the distance between the air and the blood. The consequences of this are shortness of breath, orthopnea and paroxysmal nocturnal dyspnea.
Right Heart Failure as a Result of Left Heart Failure
- The hypoxia caused by pulmonary edema causes vasoconstriction in the pulmonary circulation, which results in pulmonary hypertension. Since the right ventricle generates far lower pressures than the left ventricle (approximately 20 mmHg versus around 120 mmHg, respectively, in the healthy individual) but nonetheless generates cardiac output exactly equal to the left ventricle, this means that a small increase in pulmonary vascular resistance causes a large increase in amount of work the right ventricle must perform.
- Other mechanisms of right heart failure are mediated by neurohormonal activation.[7]
- Mechanical effects may also contribute. As the left ventricle distends, the intraventricular septum bows into the right ventricle, decreasing the filling capacity of the right ventricle.
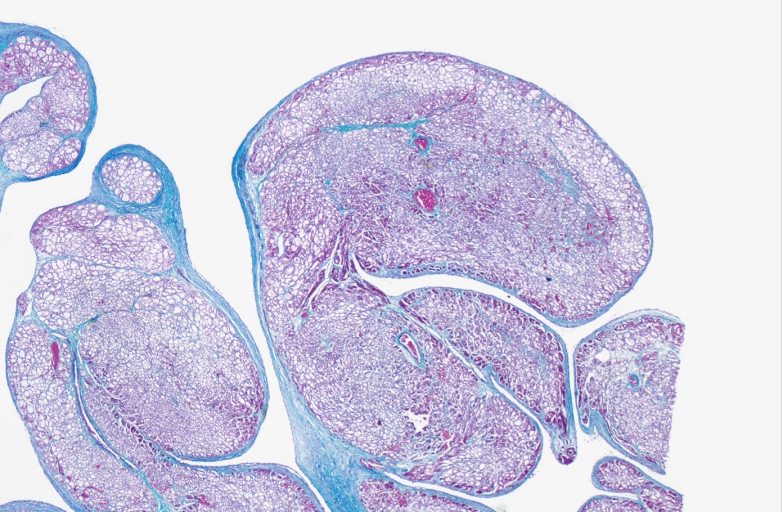
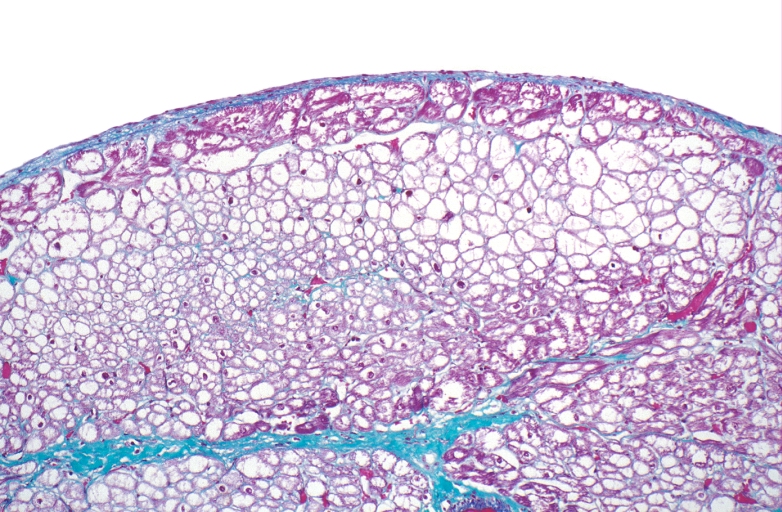
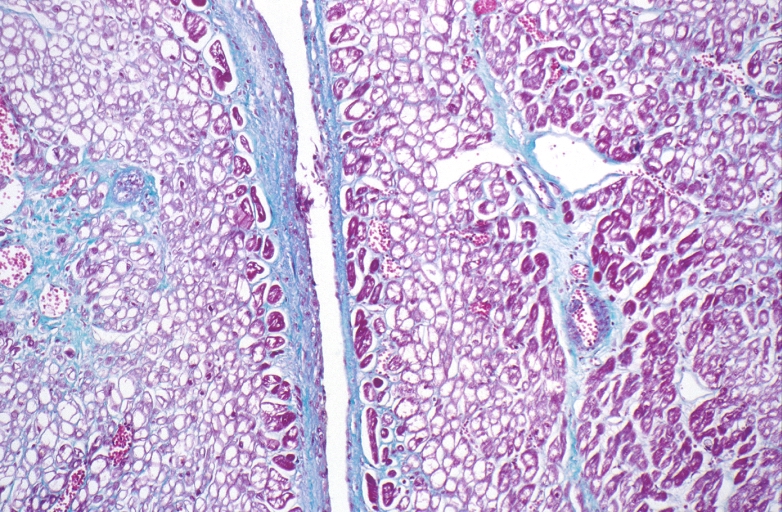
Microscopic Pathology
-
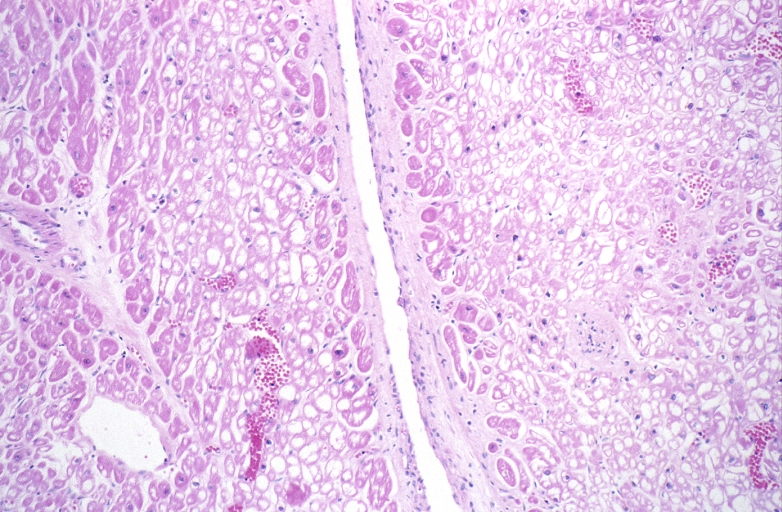
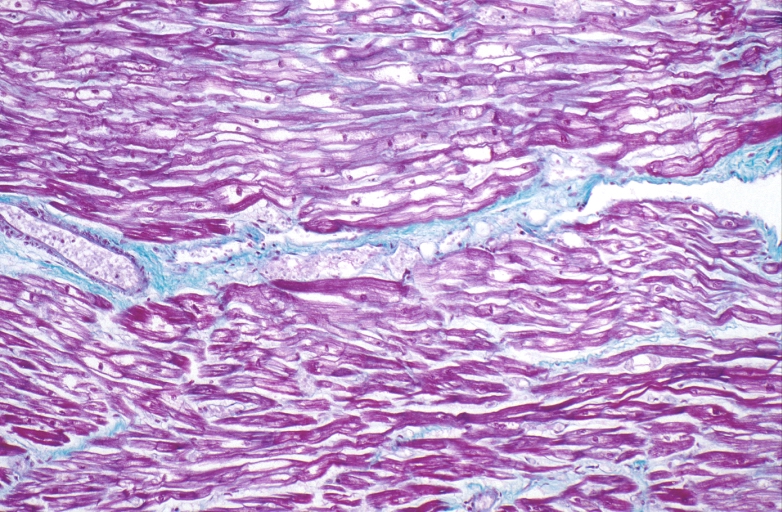
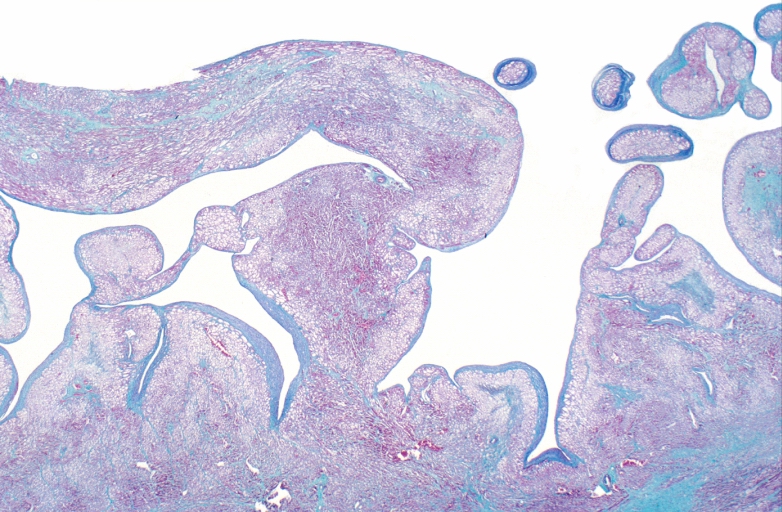 HEART: Congestive heart failure, hydropic change
HEART: Congestive heart failure, hydropic change -
 HEART: Congestive heart failure, hydropic change
HEART: Congestive heart failure, hydropic change -
 HEART: Congestive heart failure, hydropic change
HEART: Congestive heart failure, hydropic change



-
 HEART: Congestive heart failure, hydropic change
HEART: Congestive heart failure, hydropic change -
 HEART: Congestive heart failure, hydropic change
HEART: Congestive heart failure, hydropic change -
 HEART: Congestive heart failure, hydropic change
HEART: Congestive heart failure, hydropic change



-
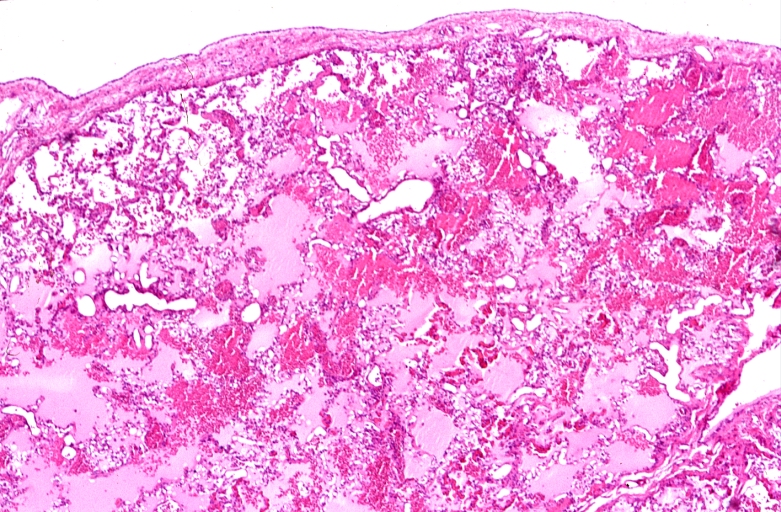
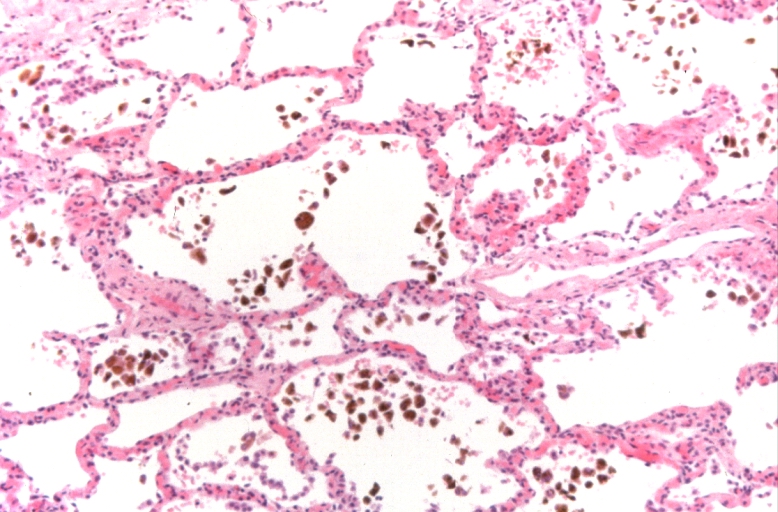 Lung, congestion, heart failure cells (hemosiderin laden macrophages)
Lung, congestion, heart failure cells (hemosiderin laden macrophages) -
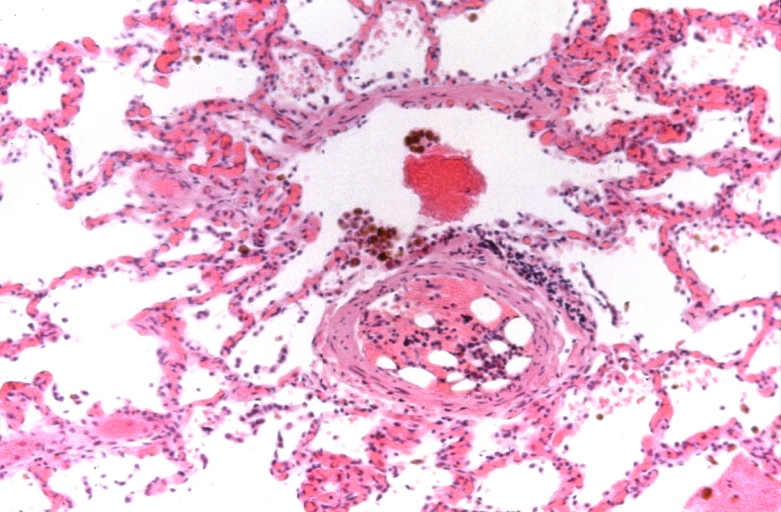 Lung, Congestive Heart Failure, bone marrow embolus
Lung, Congestive Heart Failure, bone marrow embolus -
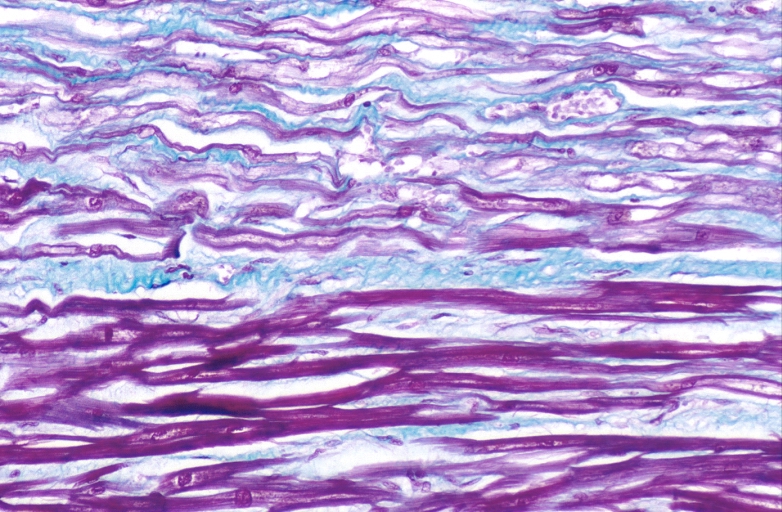
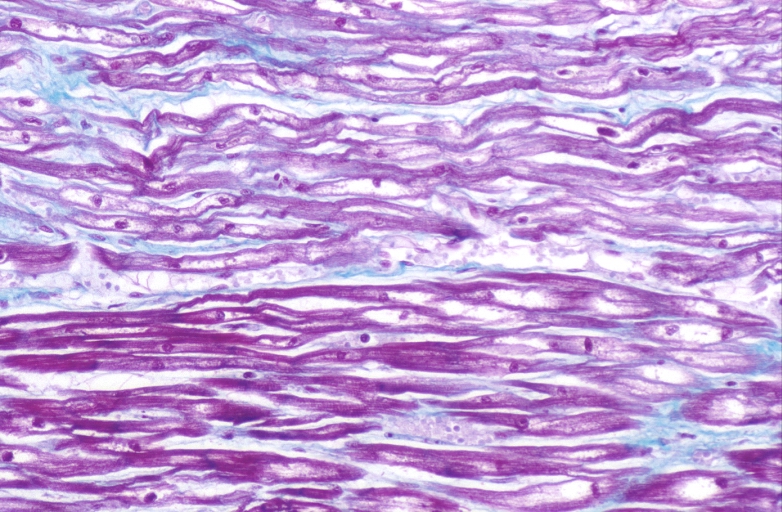
 Lung, pulmonary edema in patient with congestive heart failure due to heart transplant rejection
Lung, pulmonary edema in patient with congestive heart failure due to heart transplant rejection



-
 HEART: Congestive heart failure, hydropic change
HEART: Congestive heart failure, hydropic change -
 HEART Congestive heart failure, hydropic change
HEART Congestive heart failure, hydropic change -
 Spleen, congestion, congestive heart failure
Spleen, congestion, congestive heart failure



References
- ↑ Template:GPnotebook
- ↑ Boron and Boulpaep 2005 Medical Physiology Updated Edition p533 ISBN 0-7216-3256-4
- ↑ Rang HP (2003). Pharmacology. Edinburgh: Churchill Livingstone. p. 127. ISBN 0-443-07145-4.
- ↑ Shigeyama J, Yasumura Y, Sakamoto A; et al. (2005). “Increased gene expression of collagen Types I and III is inhibited by beta-receptor blockade in patients with dilated cardiomyopathy”. Eur. Heart J. 26 (24): 2698–705. doi:10.1093/eurheartj/ehi492. PMID 16204268. Unknown parameter
|month=ignored (help) - ↑ Tsutsui H, Matsushima S, Kinugawa S; et al. (2007). “Angiotensin II type 1 receptor blocker attenuates myocardial remodeling and preserves diastolic function in diabetic heart” (– Scholar search). Hypertens. Res. 30 (5): 439–49. doi:10.1291/hypres.30.439. PMID 17587756. Unknown parameter
|month=ignored (help) - ↑ Krug AW, Grossmann C, Schuster C; et al. (2003). “Aldosterone stimulates epidermal growth factor receptor expression”. J. Biol. Chem. 278 (44): 43060–6. doi:10.1074/jbc.M308134200. PMID 12939263. Unknown parameter
|month=ignored (help) - ↑ Hunter JG, Boon NA, Davidson S, Colledge NR, Walker B (2006). Davidson’s principles & practice of medicine. Elsevier/Churchill Livingstone. p. 544. ISBN 0-443-10057-8.
Causes
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]
Overview
There are several classification schemes used to characterize the pathophysiology of heart failure as either systolic vs diastolic; left vs right; or low output vs high output. The anatomic structure underlying the disease process is often characterized as well. The causes of heart failure are also often characterized by their chronicity (acute/decompensated or chronic).
Causes
Life Threatening Causes
Life-threatening causes include conditions which may result in death or permanent disability within 24 hours if left untreated. Congestive heart failure is life threatening and should be treated as such irrespective of the underlying cause.
Common Causes
- Arrhythmias
- Cardiomyopathies
- Cardiotoxins (e.g., alcohol, cocaine, aprotinin)
- Congenital heart disease
- Hypertension
- Ischemic heart disease
- Pericarditis
- Pulmonary embolism
- Valvular heart disease
- Viral myocarditis
Causes by Organ System
Causes in Alphabetical Order
- Ado-trastuzumab emtansine
- Alcoholism
- Anemia
- Aortic insufficiency
- Aortic stenosis
- Arrhythmias
- Arrhythmogenic right ventricular dysplasia
- Arteriovenous fistula
- Ascorbic acid deficiency
- Atenolol
- Atrial fibrillation
- Atrial septal defect
- Beriberi
- Bicalutamide
- Bicisate dihydrochloride
- Cardiac amyloidosis
- Cardiac aneurysm
- Carfilzomib
- Carnitine deficiency
- Certolizumab pegol
- Cidofovir
- Cinacalcet
- Coalworker’s pneumoconiosis
- Congenital heart disease
- Constrictive pericarditis
- Cor pulmonale
- Cyclophosphamide
- Dexamethasone
- Diabetes mellitus
- Diclofenac (patch)
- Dilated cardiomyopathy
- Disulfiram
- Dornase alfa
- Doxorubicin Hydrochloride
- Dronedarone
- Eisenmenger syndrome
- Endocarditis
- Epirubicin
- Epoetin alfa
- Ethylene glycol
- Felbamate
- Ferumoxytol
- Flurbiprofen
- Friedreich’s ataxia
- Glycogen storage disease
- Goserelin
- Hemochromatosis
- Human immunodeficiency virus
- Hydroxyethyl starch
- Hypertension
- Hyperthyroidism
- Hypertrophic cardiomyopathy
- Hypoplastic left heart syndrome
- Hypothyroidism
- Hypoxia
- Idarubicin hydrochloride
- Ibuprofen lysine
- Idursulfase
- Imatinib mesylate
- Interferon gamma
- Ischemic heart disease
- Ixabepilone
- Levothyroxine
- Lyme disease
- Malignant hypertension
- Marfan’s syndrome
- Mefenamic acid
- Meloxicam
- Meropenem
- Metabolic acidosis
- Methoxy polyethylene glycol-epoetin beta
- Methylprednisolone
- Metoclopramide
- Mitomycin
- Mitoxantrone
- Mitral regurgitation
- Mitral stenosis
- Mulibrey nanism syndrome
- Muromonab-CD3
- Muscular dystrophy
- Myocardial infarction
- Nilutamide
- Nitroglycerin
- Noonan syndrome
- Oprelvekin
- Oxaprozin
- Paget’s disease
- Pancoast’s tumor
- Patent ductus arteriosus
- Peginterferon Beta-1a
- Pergolide
- Pericardial effusion
- Pericardial tamponade
- Pericarditis
- Peripartum cardiomyopathy
- Phenylbutazone
- Pickwickian syndrome
- Piroxicam
- Ponatinib hydrochloride
- Pneumococcal Vaccine 13-Valent (Prevnar 13)
- Pramipexole
- Propranolol
- Prednisone
- Prednisolone
- Pulmonary artery stenosis
- Pulmonary embolism
- Pulmonary fibrosis
- Pulmonary hypertension
- Pulmonary valve stenosis
- Pulmonary vein stenosis
- Pulmonic regurgitation
- Restrictive cardiomyopathy
- Rheumatic carditis
- Rheumatic fever
- Rubidium Rb 82
- Rupture of the papillary muscles
- Sarcoidosis
- Sepsis
- Silicosis
- Sorafenib
- Sulindac
- Sunitinib malate
- Systemic lupus erythematosus
- Takotsubo cardiomyopathy
- Thyrotoxicosis
- Tolmetin
- Trastuzumab
- Tricuspid insufficiency
- Valdecoxib
- Vandetanib
- Valvular heart disease
- Ventricular aneurysm
- Ventricular septal defect
- Verapamil
- Viral myocarditis
- Whipple’s disease
References
Differentiating Chronic Heart Failure from other Diseases
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1];Associate Editor(s)-in-Chief: Seyedmahdi Pahlavani, M.D. [2]Syed Hassan A. Kazmi BSc, MD [3]
Overview
Congestive heart failure should be distinguished from other conditions that cause dyspnea, fatigue and edema.
Differentiating Congestive Heart Failure from other Diseases
Heart failure is a clinical syndrome of dyspnea, fatigue and edema. There are several disorders that cause heart failure and should not be confused with the syndrome of heart failure.
- Cardiac arrest and asystole refer to situations in which there is no cardiac output at all. Without urgent treatment these result in sudden death.
- Myocardial infarction (“Heart attack”) refers to heart muscle damage due to an insufficient blood supply to the heart, usually as a result of a blocked coronary artery.
- Cardiomyopathy refers specifically to problems within the heart muscle, and these problems can result in heart failure. Ischemic cardiomyopathy implies that the cause of muscle damage is coronary artery disease. Dilated cardiomyopathy implies that the muscle damage has resulted in enlargement of the heart. Hypertrophic cardiomyopathy involves enlargement and thickening of the heart muscle.
- There are non-cardiac causes of edema that primarily involve the lung or respiratory system. These conditions are distinguished from heart failure in so far as they do not cause peripheral edema, and they are not be associated with an elevation in BNP.
| Organ System | Disease | Symptoms | Signs | Laboratory findings | Diagnostic modality | Management |
|---|---|---|---|---|---|---|
| Cardiac | HFpEF (Heart Failure with preserved Ejection Fraction | Exertional dyspnea, reduced exercise tolerance, orthopnea, paroxysmal nocturnal dyspnea, edema | Elevated JVP, fine crackles, edema | Increased BNP | Echocardiography (EF ≥ 50 %) | Control of volume overload and hypertension,
treatment of underlying condition (obesity, AF, coronary artery disease, anemia) |
| HFrEF (Heart Failure with reduced Ejection Fraction) | Exertional dyspnea, reduced exercise tolerance, orthopnea, paroxysmal nocturnal dyspnea, edema | Elevated JVP, fine crackles, edema | Increased BNP | Echocardiography (EF ≤ 40 %) | Diuretics, ACE inhibitors, ARBs, beta blockers, nitrates | |
| Pericardial disease | Exercise intolerance, dyspnea, fatigue | Elevated JVP, pericardial knock, kussmaul’s sign, pulsus paradoxus | – | Echocardiography, ECG | Diuretics, pericardiectomy | |
| Hypertrophic cardiomyopathy | Dyspnea, chest pain, palpitation, lightheadedness | Systolic murmur | – | Echocardiography, ECG | Beta blockers, verapamil | |
| Valvular disease (MR, TR) | Edema, fatigue, exercise intolerance, dyspnea, lightheadedness | Cardiac murmur | – | Echocardiography, ECG | Valve repair or replacement, diuretics, beta blockers | |
| Arrhythmia | Palpitation, lightheadedness, chest tightness | Tachycardia, abnormal pulse | – | Echocardiography, ECG, holter monitoring | Pharmacological cardioversion (anti arrhythmics), electrical cardioversion, ablation | |
| Pulmonary | Chronic airway disease | Cough, dyspnea, chest pain, exercise intolerance | Tachypnea, respiratory distress, cyanosis, edema, rhonchi and crackles | Hypoxemia, hypercapnea, polycythemia, | PFT, chest imaging | Bronchodilators, corticosteroids, anticholinergics |
| Interstitial lung diseaee | Exercise intolerance, cough | Crackles, clubbing, cyanosis | Hypoxemia | PFT, Chest imaging, lung biopsy | Corticosteroids, bronchodilators | |
| Pulmonary hypertension | Dyspnea, fatigue, chest pain, syncope, palpitation | Edema, clubbing, elevated JVP, TR murmur | Elevated BNP, elevated d-dimer | Echocardiography, cardiac cathaterization | Diuretics, calcium channel blockers, endothelin receptor antagonist, phosphodiesterase 5 inhibitor | |
| Sleep apnea | Snoring, somnolence, headache, fatigue, irritability | tachypnea, hypertension, tachycardia | Hypoxemia, polycythemia | Polysomnography | Weight reduction, CPAP | |
| High output status | Anemia | Palpitation, lightheadedness, fatigue | Cheilosis, delayed capillary refill | Decreased Hb and HCT | CBC, Iron study, bone marrow aspiration and biopsy | Iron replacement, nutritional support |
| Thyrotoxicosis | Palpitation, sweating, weight loss | Proptosis, tachycardia | Decreased TSH, increased T3,T4 | Thyroid function test | Thyrostatics, beta blockers, ablation | |
| Others | Liver disease | Fatigue, edema, jaundice | Ascites, palmar erythema, gynecomastia | Increased AST and ALT, decreased albumin, increased Br | Liver function test, Liver biopsy | Diuretics, treatment of underlying disease |
| Chronic kidney disease | Fatigue, anorexia, nausea, edema, decreased exercise tolerance | Edema, hypertension, crackles | Increased BUN and Cr | BUN, Cr | Control of blood pressure, anemia, dialysis, kidney transplant |
Other Causes of Dyspnea
CHF should be differentiated from other diseases presenting with shortness of breath and tachypnea. The differentials include the following:[1][2][3][4][5][6][7][8][9][10][11][12][13][14][15][16][17][18][19][20]
| Diseases | Diagnostic tests | Physical Examination | Symptoms | Past medical history | Other Findings | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| CT scan and MRI | EKG | Chest X-ray | Tachypnea | Tachycardia | Fever | Chest Pain | Hemoptysis | Dyspnea on Exertion | Wheezing | Chest Tenderness | Nasalopharyngeal Ulceration | Carotid Bruit | |||
| Pulmonary embolism |
|
|
|
✔ | ✔ | ✔ (Low grade) | ✔ | ✔ (In case of massive PE) | ✔ | – | – | – | – |
|
|
| Congestive heart failure |
|
✔ | ✔ | ✔ | – | – | ✔ | – | – | – | – |
|
| ||
| Percarditis |
|
|
|
✔ | ✔ | ✔ (Low grade) | ✔ (Relieved by sitting up and leaning forward) | – | ✔ | – | – | – | – |
|
|
| Pneumonia |
|
|
|
✔ | ✔ | ✔ | ✔ | – | ✔ | ✔ | – | – | – |
|
|
| Vasculitis |
|
|
✔ | ✔ | ✔ | ✔ | ✔ | ✔ | – | ✔ | ✔ | ✔ |
|
||
| Chronic obstructive pulmonary disease (COPD) |
|
|
✔ | ✔ | – | – | – | ✔ | ✔ | – | – | – |
|
| |
| COVID-19-associated heart failure |
|
|
|
✔ | ✔ | – | – | ✔ | ✔ | – | – | – | – | – | |
Other Conditions that Cause Dyspnea that are Emergencies
The following emergency conditions should be excluded when diagnosing a patient with heart failure:
Non Cardiac Causes of Dyspnea
- Abdominal masses
- Acute bronchitis
- Acute Chest Syndrome
- Acute myeloid leukemia
- Acute promyelocytic leukemia
- Acute tracheobronchitis
- AIDS
- Air pollution
- Air-conditioner lung
- Allergy
- Alpha 1-antitrypsin deficiency
- Altitude sickness
- Amniotic fluid embolism
- Amphotericin B
- Amyl nitrite
- Amyotrophic Lateral Sclerosis (ALS)
- Anaphylactoid reactions
- Anaphylaxis
- Anemia
- Anthrax
- Anxiety
- Asbestosis
- Aspergillus clavatus
- Aspiration
- Asthma
- Atelectasis
- Atypical pneumonia
- Barium
- Beta-blockers
- Betazole
- Bird breeder’s lung
- Bird fancier’s lung
- Bland-White-Garland Syndrome
- Bleomycin in ABVD
- Blood transfusion
- Brain stem infarction
- Bronchial asthma
- Bronchial tumors
- Bronchiolitis
- Bronchiolitis obliterans
- Bronchiolitis obliterans organizing pneumonia
- Bronchitis
- Bronchogenic carcinoma
- Bronchoscopy
- Cardiovascular syphilis
- Caspofungin
- Cheese worker’s lung
- Chemical worker’s lung
- Chest trauma
- Chest tube
- Cholesterol pericarditis
- Chronic bronchitis
- Chronic fatigue syndrome
- Chronic Obstructive Pulmonary Disease (COPD)
- Chylothorax
- Cirrhosis
- Cladosporium
- CMV Pneumonitis
- Community-acquired pneumonia
- Croup
- Cystic Fibrosis
- Daptomycin
- Decompression sickness
- Decreased thoracic or diaphragmatic excursion
- Diabetic coma
- Diffuse panbronchiolitis
- Diverticulosis
- Drugs
- Ehrlichiosis (canine)
- Empty nose syndrome
- Empyema, pleural
- Encephalitis
- Eosinophilic pneumonia
- Ephedrine
- Epidemic dropsy
- Erdheim-Chester disease
- Esophageal cancer
- Esophageal diseases with tracheal compression
- Exercise-induced asthma
- Extrinsic allergic alveolitis
- Fat embolism
- Fibrosing alveolitis, cryptogenic
- Gamma-Hydroxybutyric acid
- Gastroesophageal reflux
- Gemeprost
- Glatiramer acetate
- Glottal edema
- Goiter
- Goodpasture syndrome
- Grain handler’s lung
- Gram-negative sepsis
- Guillain-Barre Syndrome
- Hemochlyothorax
- Hemothorax
- Histiocytosis X
- Hoose (disease)
- Humidifier lung
- Hydrochlyothorax
- Hypersensitivity Pneumonitis
- Hyperthyroidism
- Hypoxia
- Hysteria
- Idiopathic pulmonary fibrosis
- Iloprost
- Interstitial lung disease
- Intoxication (carbon monoxide, cyanide)
- Intrapulmonary receptor stimulation
- Intussusception (medical disorder)
- Iron deficiency anemia
- Irregular Heart Rhythms
- Ketorolac
- Kyphoscoliosis
- Laryngeal/bronchospasm
- Leukemia
- Lung cancer
- Lymphangitic metastases
- Lymphocytic interstitial pneumonia
- Lymphoma
- Malignant Mesothelioma
- Malt worker’s lung
- Mediastinal tumors
- Megaloblastic Anemias
- Mercury (element)
- Metabolic acidosis
- Methyl isocyanate
- Micropolyspora faeni
- Miliary tuberculosis
- Mollusk shell hypersensitivity
- Mucor stolonifer
- Multiple rib fractures
- Myasthenia Gravis
- Myxoma
- Neuromuscular disease
- Obesity
- Phrenic nerve paralysis
- Pleural callosity
- Pneumoconiosis
- Pneumonia
- Pneumochlyothorax
- Pneumothorax
- Pleural Effusion
- Pleural fibrosis
- Polyradiculitis
- Pulmonary arteriovenous malformation
- Pulmonary Emphysema
- Pulmonary fibrosis
- Quincke’s Edema
- Radiation pneumonitis
- Respiratory tract infection
- Sarcoidosis
- Shock
- Shock lung
- Sleep Apnea Syndrome
- Trauma
- Tracheal stenosis
- Tracheal tumors
- Tracheomalacia
- Tracheobronchial collapse
- Uremia
Other Causes of Fatigue
There are numerous non-cardiac causes of fatigue. Again, these non-cardiac causes are not associated with dyspnea and edema.
Other Causes of Edema
Other non cardiac causes of pedal edema are listed below. Obviously, the majority of these disorders do not also cause dyspnea and fatigue, and that distinguishes them form heart failure.
- ACE inhibitor
- Aceon
- Acquired C1-esterase inhibitor deficiency
- Actos
- Acute glomerulonephritis
- Addison’s Disease
- Aldomet
- Amlodipine
- Amniotic band
- Angioneurotic edema
- Angiotensin converting enzyme inhibitor
- Anemia
- Anorexia Nervosa
- AV fistula
- Avandia
- Bartter’s Syndrome
- Beta blockers
- Boils
- Bruise
- Bulimia Nervosa
- Burn
- Cachexia
- Carbuncle
- Cardura
- Cellulitis
- Chemotherapy
- Cisplatin
- Cold (physical stimuli)
- Contact dermatitis
- Contusion
- Cushing’s Syndrome
- Diltiazem
- Drugs
- Docetax
- Erysipelas
- Exudative enteropathy
- Filariasis
- Fracture
- Frostbite
- Gas gangrene
- Glitazones
- Gout
- Hyperthyroidism
- Hypoalbuminemia
- Hypoplasia
- Hypothyroidism
- Ibuprophen
- Idiopathic edema
- Insect bite
- Irritant
- Ligamentous sprain
- Liver failure
- Lymph node mass
- Malabsorption
- Malnutrition
- Mediastinal cancer
- Milroy’s Disease
- Minipress
- Motrin
- Musculoskeletal trauma
- Neoplasm
- Nephrotic Syndrome
- Nifedipine
- Norvasc
- Osteomyelitis
- Peripheral nerve lesion
- Premenstrual edema
- Scleroderma
- Sepsis syndrome
- Snakebites
- Starvation edema
- Sunburn
- Surgical excision
- Tendonous strain
- Thrombophlebitis
- Thrombosis
- Tight clothing
- Trentinion
- Trichinosis
- Tumors
- Univasc
- Valproic acid
- Varicose veins
- Vesinoid
- vytorin
References
- ↑ Brenes-Salazar JA (2014). “Westermark’s and Palla’s signs in acute and chronic pulmonary embolism: Still valid in the current computed tomography era”. J Emerg Trauma Shock. 7 (1): 57–8. doi:10.4103/0974-2700.125645. PMC 3912657. PMID 24550636.
- ↑ “CT Angiography of Pulmonary Embolism: Diagnostic Criteria and Causes of Misdiagnosis | RadioGraphics”.
- ↑ Bĕlohlávek J, Dytrych V, Linhart A (2013). “Pulmonary embolism, part I: Epidemiology, risk factors and risk stratification, pathophysiology, clinical presentation, diagnosis and nonthrombotic pulmonary embolism”. Exp Clin Cardiol. 18 (2): 129–38. PMC 3718593. PMID 23940438.
- ↑ “Pulmonary Embolism: Symptoms – National Library of Medicine – PubMed Health”.
- ↑ Ramani GV, Uber PA, Mehra MR (2010). “Chronic heart failure: contemporary diagnosis and management”. Mayo Clin. Proc. 85 (2): 180–95. doi:10.4065/mcp.2009.0494. PMC 2813829. PMID 20118395.
- ↑ Blinderman CD, Homel P, Billings JA, Portenoy RK, Tennstedt SL (2008). “Symptom distress and quality of life in patients with advanced congestive heart failure”. J Pain Symptom Manage. 35 (6): 594–603. doi:10.1016/j.jpainsymman.2007.06.007. PMC 2662445. PMID 18215495.
- ↑ Hawkins NM, Petrie MC, Jhund PS, Chalmers GW, Dunn FG, McMurray JJ (2009). “Heart failure and chronic obstructive pulmonary disease: diagnostic pitfalls and epidemiology”. Eur. J. Heart Fail. 11 (2): 130–9. doi:10.1093/eurjhf/hfn013. PMC 2639415. PMID 19168510.
- ↑ Takasugi JE, Godwin JD (1998). “Radiology of chronic obstructive pulmonary disease”. Radiol. Clin. North Am. 36 (1): 29–55. PMID 9465867.
- ↑ Wedzicha JA, Donaldson GC (2003). “Exacerbations of chronic obstructive pulmonary disease”. Respir Care. 48 (12): 1204–13, discussion 1213–5. PMID 14651761.
- ↑ Nakawah MO, Hawkins C, Barbandi F (2013). “Asthma, chronic obstructive pulmonary disease (COPD), and the overlap syndrome”. J Am Board Fam Med. 26 (4): 470–7. doi:10.3122/jabfm.2013.04.120256. PMID 23833163.
- ↑ Khandaker MH, Espinosa RE, Nishimura RA, Sinak LJ, Hayes SN, Melduni RM, Oh JK (2010). “Pericardial disease: diagnosis and management”. Mayo Clin. Proc. 85 (6): 572–93. doi:10.4065/mcp.2010.0046. PMC 2878263. PMID 20511488.
- ↑ Bogaert J, Francone M (2013). “Pericardial disease: value of CT and MR imaging”. Radiology. 267 (2): 340–56. doi:10.1148/radiol.13121059. PMID 23610095.
- ↑ Gharib AM, Stern EJ (2001). “Radiology of pneumonia”. Med. Clin. North Am. 85 (6): 1461–91, x. PMID 11680112.
- ↑ Schmidt WA (2013). “Imaging in vasculitis”. Best Pract Res Clin Rheumatol. 27 (1): 107–18. doi:10.1016/j.berh.2013.01.001. PMID 23507061.
- ↑ Suresh E (2006). “Diagnostic approach to patients with suspected vasculitis”. Postgrad Med J. 82 (970): 483–8. doi:10.1136/pgmj.2005.042648. PMC 2585712. PMID 16891436.
- ↑ Stein PD, Dalen JE, McIntyre KM, Sasahara AA, Wenger NK, Willis PW (1975). “The electrocardiogram in acute pulmonary embolism”. Prog Cardiovasc Dis. 17 (4): 247–57. PMID 123074.
- ↑ Warnier MJ, Rutten FH, Numans ME, Kors JA, Tan HL, de Boer A, Hoes AW, De Bruin ML (2013). “Electrocardiographic characteristics of patients with chronic obstructive pulmonary disease”. COPD. 10 (1): 62–71. doi:10.3109/15412555.2012.727918. PMID 23413894.
- ↑ Stein PD, Matta F, Ekkah M, Saleh T, Janjua M, Patel YR, Khadra H (2012). “Electrocardiogram in pneumonia”. Am. J. Cardiol. 110 (12): 1836–40. doi:10.1016/j.amjcard.2012.08.019. PMID 23000104.
- ↑ Hazebroek MR, Kemna MJ, Schalla S, Sanders-van Wijk S, Gerretsen SC, Dennert R, Merken J, Kuznetsova T, Staessen JA, Brunner-La Rocca HP, van Paassen P, Cohen Tervaert JW, Heymans S (2015). “Prevalence and prognostic relevance of cardiac involvement in ANCA-associated vasculitis: eosinophilic granulomatosis with polyangiitis and granulomatosis with polyangiitis”. Int. J. Cardiol. 199: 170–9. doi:10.1016/j.ijcard.2015.06.087. PMID 26209947.
- ↑ Dennert RM, van Paassen P, Schalla S, Kuznetsova T, Alzand BS, Staessen JA, Velthuis S, Crijns HJ, Tervaert JW, Heymans S (2010). “Cardiac involvement in Churg-Strauss syndrome”. Arthritis Rheum. 62 (2): 627–34. doi:10.1002/art.27263. PMID 20112390.
Epidemiology and Demographics
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Cafer Zorkun, M.D., Ph.D. [2]; Saleh El Dassouki, M.D [3]; Atif Mohammad, M.D. ;Seyedmahdi Pahlavani, M.D. [4]; Edzel Lorraine Co, D.M.D., M.D. [5]
Overview
Heart failure affects close to 5 million people in the United States of America and each year close to 500,000 new cases are diagnosed. Congestive heart failure is responsible for a significant portion of the healthcare budget, and more than 50% of patients seek re-admission within 6 months after treatment and the average duration of hospital stay is 6 days. In 2001, nearly 53,000 patients died of heart failure as a primary cause.
Epidemiology and Demographics
Prevalence
It is estimated that about 5.7 million adults in the United States have heart failure (about 2,650,000 males, and 2,650,000 females).
It is estimated that the prevalence of HF will increase 46% from 2012 to 2030, resulting in >8 million people ≥18 years of age with HF in the United States.[1]

Prevalence of heart failure by sex and age (Source: National Center for Health Statistics and National Heart, Lung, and Blood Institute).
Incidence
- Approximately, there are 915 000 new HF cases annually.[1]
- Data from the NHLBI’s Framingham Heart Study indicate that;[2][3]
- Heart failure (HF) incidence approaches 10 per 1,000 population after age 65.
- 75% of heart failure cases have antecedent hypertension. About 22% of male and 46% of female myocardial infarction (MI) victims will be disabled with heart failure within 6 years of the index event.
- At age 40, the lifetime risk of developing heart failure for both men and women is 1 in 5.
- At age 40, the lifetime risk of heart failure occurring without antecedent myocardial infarction is 1 in 9 for men and 1 in 6 for women.
- The lifetime risk doubles for people with blood pressure >160/90 mm Hg compared to those with blood pressure <140/90 mm Hg.
- A study conducted in Olmsted County, Minnesota, showed that the incidence of heart failure (ICD9/428) has not declined during two decades, but survival after onset has increased overall, with less improvement among women and elderly persons. [4][5]
- An increase of 26% in the number of hospitalizations due to heart failure in 2017. [6]
Age
Heart failure is the leading cause of hospitalization in people older than 65.[7] In developed countries, the mean age of patients with heart failure is 75 years old. In developing countries, two to three percent of the population suffers from heart failure, but in those 70 to 80 years old, it occurs in 20—30 percent. The incidence of heart failure approaches 10 per 1000 population after age 65 years, and approximately 80% of patients hospitalized are more than 65 years old.[8]
Gender
Men have a higher incidence of heart failure, but the overall prevalence rate is similar in both sexes, since women survive longer after the onset of heart failure.[9] Women tend to be older when diagnosed with heart failure (after menopause), they are more likely than men to have diastolic dysfunction, and seem to experience a lower overall quality of life than men after diagnosis.[9]
Race
New information suggests that elements of heart failure in African Americans and Caucasians may be different[10] and therapy for heart failure has different efficacies depending on racial, ethnic, and genetic backgrounds. Blacks have the highest risk for HF. In the Atherosclerosis Risk In Communities (ARIC) study, black men were found to have the highest risk, while white women were found to have the lowest risk.[8]
Country Specific Causes
In tropical countries, the most common cause of HF is valvular heart disease or some type of cardiomyopathy. Moreover as underdeveloped countries become more affluent, there has also been an increase in diabetes, hypertension and obesity which has resulted in heart failure.
In USA, HF is much higher in African Americans, Hispanics, Native Americans and recent immigrants from the eastern bloc countries like Russia. This high prevalence in these ethnic populations has been linked to high incidence of diabetes and hypertension. In many new immigrants to the USA the high prevalence of heart failure has largely been attributed to lack of preventive health care or substandard treatment.[11]
Costs
In the United States, HF costs exceed $40 billion, taking into consideration the cost of medications, healthcare services and lack of productivity. It’s noteworthy that HF is respsonsible for 1 in 9 deaths in the United States.[8]

Hospital discharges for heart failure by sex which include people discharged alive, dead, and status unknown. Source: National Hospital Discharge Survey/National Center for Health Statistics and National Heart, Lung, and Blood Institute.
References
- ↑ 1.0 1.1 Mozaffarian D, Benjamin EJ, Go AS, Arnett DK, Blaha MJ, Cushman M, Das SR, de Ferranti S, Després JP, Fullerton HJ, Howard VJ, Huffman MD, Isasi CR, Jiménez MC, Judd SE, Kissela BM, Lichtman JH, Lisabeth LD, Liu S, Mackey RH, Magid DJ, McGuire DK, Mohler ER, Moy CS, Muntner P, Mussolino ME, Nasir K, Neumar RW, Nichol G, Palaniappan L, Pandey DK, Reeves MJ, Rodriguez CJ, Rosamond W, Sorlie PD, Stein J, Towfighi A, Turan TN, Virani SS, Woo D, Yeh RW, Turner MB (2016). “Heart Disease and Stroke Statistics-2016 Update: A Report From the American Heart Association”. Circulation. 133 (4): e38–360. doi:10.1161/CIR.0000000000000350. PMID 26673558.
- ↑ Disease and Stroke Statistics – 2008 Update, American Heart Association. Accessed on 09 March 2008
- ↑ Lloyd-Jones DM, Larson MG, Leip EP, Beiser A, D’Agostino RB, Kannel WB, Murabito JM, Vasan RS, Benjamin EJ, Levy D; Lifetime Risk for Developing Congestive Heart Failure. Framingham Heart Study. Circulation. 2002; 106: 3068–72 PMID 12473553
- ↑ Véronique L. Roger, Susan A. Weston, Margaret M. Redfield, Jens P. Hellermann-Homan, Jill Killian, Barbara P. Yawn, Steven J. Jacobsen Trends in Heart Failure Incidence and Survival in a Community-Based Population JAMA. 2004; 292: 344-50 PMID 15265849
- ↑ Thomas S, Rich MW (2007) Epidemiology, pathophysiology, and prognosis of heart failure in the elderly. Heart Fail Clin 3 (4):381-7. DOI:10.1016/j.hfc.2007.07.004 PMID: 17905375
- ↑ Agarwal MA, Fonarow GC, Ziaeian B (2021). “National Trends in Heart Failure Hospitalizations and Readmissions From 2010 to 2017”. JAMA Cardiol. 6 (8): 952–956. doi:10.1001/jamacardio.2020.7472. PMC 7876620 Check
|pmc=value (help). PMID 33566058 Check|pmid=value (help). - ↑ Krumholz HM, Chen YT, Wang Y, Vaccarino V, Radford MJ, Horwitz RI (2000). “Predictors of readmission among elderly survivors of admission with heart failure”. Am. Heart J. 139 (1 Pt 1): 72–7. doi:10.1016/S0002-8703(00)90311-9. PMID 10618565.
- ↑ 8.0 8.1 8.2 Yancy CW, Jessup M, Bozkurt B, Masoudi FA, Butler J, McBride PE; et al. (2013). “2013 ACCF/AHA Guideline for the Management of Heart Failure: A Report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines”. J Am Coll Cardiol. doi:10.1016/j.jacc.2013.05.019. PMID 23747642.
- ↑ 9.0 9.1 Strömberg A, Mårtensson J. (2003). “Gender differences in patients with heart failure”. Eur. J. Cardiovasc. Nurs. 2 (1): 7–18. doi:10.1016/S1474-5151(03)00002-1. PMID 14622644. Unknown parameter
|month=ignored (help) - ↑ Aronow, WS (1999). “Comparison of incidence of congestive heart failure in older African-Americans, Hispanics, and Caucasians”. Am J of Cardiol. 84 (5): 611–2. doi:10.1016/S0002-9149(99)00392-6. PMID 10482169. Unknown parameter
|coauthors=ignored (help) - ↑ Heart Failure Information, Retrieved on 2010-01-21.
Risk Factors
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Cafer Zorkun, M.D., Ph.D. [2]; Saleh El Dassouki, M.D. [3]; Atif Mohammad, M.D.
Overview
Several risk factors may predispose to heart failure. These risk factors can be demographic, genetic, associated with lifestyle or medications.
Risk Factors
Common risk factors associated with heart failure include:
| Risk factors for heart failure | Prevention strategies |
|---|---|
| Sedentary habit | Regular physical activity |
| Cigarette smoking | Cigarette smoking cessation |
| Obesity | Physical activity and healthy diet |
| Excessive alcohol intake | General population: no/light alcohol
intake is beneficial, avoiding alcohol in Patients with alcohol-induced CMP |
| Influenza | Influenza vaccination |
| Microbes (Trypanosoma cruzi, Streptococci) | Early diagnosis, antimicrobial therapy |
| Cardiotoxic drugs (anthracyclines) | Cardiac function and side effect monitoring, dose adaptation, change of chemotherapy |
| Chest radiation | Cardiac function and side effect monitoring, dose adaptation |
| Hypertension | Life style modification, antihypertensive drugs |
| Hyperlipidemia | Healthy diet, statins |
| Diabetes mellitus | Physical activities, healthy diet, SGLT2 inhibitors |
| Coronary artery disease | Life style modification, statins |
| The above table adopted from 2021 ESC Guideline |
|---|
References
- ↑ McDonagh TA, Metra M, Adamo M, Gardner RS, Baumbach A, Böhm M, Burri H, Butler J, Čelutkienė J, Chioncel O, Cleland J, Coats A, Crespo-Leiro MG, Farmakis D, Gilard M, Heymans S, Hoes AW, Jaarsma T, Jankowska EA, Lainscak M, Lam C, Lyon AR, McMurray J, Mebazaa A, Mindham R, Muneretto C, Francesco Piepoli M, Price S, Rosano G, Ruschitzka F, Kathrine Skibelund A (September 2021). “2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure”. Eur Heart J. 42 (36): 3599–3726. doi:10.1093/eurheartj/ehab368. PMID 34447992 Check
|pmid=value (help). Vancouver style error: initials (help)
Natural History, Complications and Prognosis
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Cafer Zorkun, M.D., Ph.D. [2]; Saleh El Dassouki, M.D. [3]; Atif Mohammad, M.D.
Overview
Heart failure is associated with significantly reduced physical and mental health, resulting in a markedly decreased quality of life. Congestive heart failure is also associated with a poor prognosis. If left untreated, heart failure may result in death due to complications associated with the condition. Heart failure resulting from atherosclerotic coronary artery disease has been shown to be associated with higher incidence of fatal events compared to heart failure that results from other cardiac diseases. Heart failure is a progressive disease with a major impact on the patient’s quality of life. With the exception of heart failure caused by reversible conditions, the condition usually worsens with time. Although some people survive many years, progressive disease is associated with an overall annual mortality rate of 10%. In the Framingham experience, 80% of men and 70% of women with heart failure who were under 65 years of age had died within 8 years of the diagnosis.
Natural History
- If left untreated, heart failure may result in death due to complications associated with the condition. Heart failure is a progressive disease with a major impact on the patient’s quality of life.
- Heart failure resulting from atherosclerotic coronary artery disease has been shown to be associated with higher incidence of fatal events compared to heart failure that results from other cardiac diseases
- Initiation of therapy for heart failure may lead to stabilization of the patient’s clinical condition which is referred to as the stability phase.[1]
- Months to years following the stability phase, the patient functional status may decline resulting in multiple hospitalizations and eventually the condition may become refractory to treatment whn ventricular remodeling sets in.[2]
- Once refractory, heart failure may be managed titration of pharmacological therapy and by the use to left ventricular assist devices and cardiac transplantation.
- Common Triggers for referral to heart failure specialist are:[3]
- New-onset HF (regardless of EF): Refer for evaluation of etiology, therapies base on the guideline, evaluation by advanced imaging, endomyocardial biopsy, or genetic testing
- Chronic HF with high-risk features, such as development or persistence of one or more of the following risk factors:
- Need for chronic intravenous inotropes
- Persistent NYHA functional class III–IV symptoms of congestion or profound fatigue
- Systolic blood pressure ≤90 mm Hg or symptomatic hypotension
- Creatinine ≥1.8 mg/dL or BUN ≥43 mg/dL
- Initiation of atrial fibrillation, ventricular arrhythmias, or repetitive ICD shocks
- Two or more emergency department visits or hospitalizations for worsening HF in the prior 12 months
- Inability to tolerate optimally dosed beta-blockers and/or ACEI/ARB/ARNI and/or aldosterone antagonists
- Clinical deterioration, by worsening edema, increase biomarkers (BNP, NT-proBNP, others), worsened exercise testing, decompensated hemodynamics, or evidence of progressive remodeling on imaging
- High mortality risk using a validated risk model such as the Seattle Heart Failure Model
- Persistently reduced LVEF ≤ 35% despite GDMT for ≥3 months: refer for device therapy in those patients without prior placement of ICD or CRT, unless device therapy is contraindicated or inconsistent with overall goals of care
- Second opinion needed regarding etiology of HF, for example:
- Coronary ischemia and possibility of the need for revascularization
- Valvular heart disease and possibility of the need for valve repair
- Suspected myocarditis
- Suspected specific cardiomyopathies ( hypertrophic cardiomyopathy, arrhythmogenic right ventricular dysplasia, Chagas disease, restrictive cardiomyopathy, cardiac sarcoidosis, amyloid, aortic stenosis)
- Annual review needed for patients with established advanced HF
- Assessment of patient for participation in a clinical trial
Complications
1. Cardiac Arrhythmias:
- Ventricular tachycardia and ventricular fibrillation can occur as serious complications of heart failure when its pump function is severely impaired. This further worsens the cardiac output and even possible death.
- Atrial fibrillation which is rapid beating of atrium without optimal forward pumping of blood is another complication of heart failure which occurs as a result of resistance to blood flow from atrium to ventricles. These patients are at increased risk of stroke.
- Left bundle branch block is an abnormality in electrical conduction in the heart.
2. Pulmonary Congestion:
- Pulmonary congestion which occur in left ventricular failure can cause pulmonary edema.
- Venous stasis and pedal edema can occur as a complication of right heart failure. These conditions predispose patients to venous ulcers, infections and cellulites.
- Cardiac cirrhosis occurs as a result of hepatic venous congestion. This can lead to coma and even death [4].
3. Angina and myocardial infarction: Cardiac ischemia and infarction can also occur when heart failure patients undergo exertion. With LV dilation, LV wall stress increases, and this increases the risk of angina. Autopsy studies demonstrate that plaque rupture and coronary thrombosis is a common mode of death in patients with congestive heart failure.
4. Renal failure: Renal impairment can occur secondary to decreased renal perfusion. This further worsens heart failure by fluid retention.
5. Cardiac cachexia: Unintentional rapid weight loss (a loss of at least 7.5% of normal weight within 6 months) can occur in chronic heart failure[5]. This is a bad prognostic factor.
Prognosis
Risk Stratification Tools
The prognosis in patients with heart failure can be assessed using a variety of risk stratification tools and cardiopulmonary exercise testing. Clinical prediction rules use a composite of clinical factors such as lab tests and blood pressure to estimate prognosis. Among several clinical prediction rules for assessing the prognosis in acute heart failure, the ‘EFFECT rule’ slightly outperformed other rules in stratifying patients and identifying those at low risk of death during hospitalization or within 30 days.[6] Other simpler methods for identifying low risk patients include the:
- ADHERE Tree rule which indicates that patients with blood urea nitrogen < 43 mg/dl and systolic blood pressure at least 115 mm Hg have less than 10% chance of inpatient death or complications.
- BWH rule indicates that patients with systolic blood pressure over 90 mm Hg, respiratory rate of 30 or less breaths per minute, serum sodium over 135 mmol/L, no new ST-T wave changes have less than 10% chance of inpatient death or complications.
A very important method for assessing prognosis in advanced heart failure patients is cardiopulmonary exercise testing (CPX testing). CPX testing is usually required prior to heart transplantation as an indicator of prognosis. Cardiopulmonary exercise testing involves measurement of exhaled oxygen and carbon dioxide during exercise. The peak oxygen consumption (VO2 max) is used as an indicator of prognosis. As a general rule, a VO2 max less than 12-14 cc/kg/min indicates a poor survival and suggests that the patient may be a candidate for a heart transplant. Patients with a VO2 max<10 cc/kg/min have clearly poorer prognosis. The most recent International Society for Heart and Lung Transplantation (ISHLT) guidelines[7] also suggest two other parameters that can be used for evaluation of prognosis in advanced heart failure, the heart failure survival score and the use of a criterion of VE/VCO2 slope > 35 from the CPX test. The heart failure survival score is a score calculated using a combination of clinical predictors and the VO2 max from the cardiopulmonary exercise test.
Mortality Associated with Heart Failure
Based on the 44-year follow-up of the NHLBI’s Framingham Heart Study:
- 80% of men and 70% of women under age 65 who have heart failure will die within following 8 years.
- In people diagnosed with heart failure, sudden cardiac death occurs at 6 to 9 times the rate of the general population.
- One in eight deaths has heart failure mentioned on the death certificate.
References
- ↑ Chaudhry SP, Stewart GC (July 2016). “Advanced Heart Failure: Prevalence, Natural History, and Prognosis”. Heart Fail Clin. 12 (3): 323–33. doi:10.1016/j.hfc.2016.03.001. PMID 27371510.
- ↑ Allen LA, Stevenson LW, Grady KL, Goldstein NE, Matlock DD, Arnold RM, Cook NR, Felker GM, Francis GS, Hauptman PJ, Havranek EP, Krumholz HM, Mancini D, Riegel B, Spertus JA (April 2012). “Decision making in advanced heart failure: a scientific statement from the American Heart Association”. Circulation. 125 (15): 1928–52. doi:10.1161/CIR.0b013e31824f2173. PMC 3893703. PMID 22392529.
- ↑ Bozkurt B, Hershberger RE, Butler J, Grady KL, Heidenreich PA, Isler ML, Kirklin JK, Weintraub WS (April 2021). “2021 ACC/AHA Key Data Elements and Definitions for Heart Failure: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Data Standards (Writing Committee to Develop Clinical Data Standards for Heart Failure)”. Circ Cardiovasc Qual Outcomes. 14 (4): e000102. doi:10.1161/HCQ.0000000000000102. PMC 8059763 Check
|pmc=value (help). PMID 33755495 Check|pmid=value (help). - ↑ Moussavian SN, Dincsoy HP, Goodman S, Helm RA, Bozian RC (1982). “Severe hyperbilirubinemia and coma in chronic congestive heart failure”. Digestive Diseases and Sciences. 27 (2): 175–80. PMID 7075414. Unknown parameter
|month=ignored (help);|access-date=requires|url=(help) - ↑ Freeman LM (2009). “The pathophysiology of cardiac cachexia”. Current Opinion in Supportive and Palliative Care. 3 (4): 276–81. doi:10.1097/SPC.0b013e32833237f1. PMID 19797959. Retrieved 2011-04-30. Unknown parameter
|month=ignored (help) - ↑ Auble TE, Hsieh M, McCausland JB, Yealy DM (2007). “Comparison of four clinical prediction rules for estimating risk in heart failure”. Annals of emergency medicine. 50 (2): 127–35, 135.e1–2. doi:10.1016/j.annemergmed.2007.02.017. PMID 17449141.
- ↑ Mandeep R. Mehra; et al. “Evaluation of listing criteria for cardiac transplantation”. Journal of Heart and Lung Transplantation. Retrieved 8 April 2010.
Diagnosis
Diagnosis
Clinical Assessment | History and Symptoms | Physical Examination | Laboratory Findings | Electrocardiogram | Chest X Ray | Echocardiography | Cardiac MRI | Exercise Stress Test | Myocardial Viability Studies | Cardiac Catheterization | Invasive hemodynamic monitoring
Treatment
Treatment
Treatment of Heart failure with reduced ejection fraction
- In all patients: Angiotensin-converting enzyme inhibitors | Beta Blockers | Aldosterone Antagonists | Angiotensin Receptor-Neprilysin Inhibitor | Sodium-glucose co-transporter 2 inhibitors
- In selected patients: Diuretics | Angiotensin receptor blockers | If-channel inhibitor | Combination of hydralazine and isosorbide dinitrate | Digoxin | Iron
Guideline-recommended medical therapy (GDMT) for heart failure with reduced ejection fraction (HFrEF) can be suggested by the Heart Failure Educational Decision Aid medication optimization algorithm[1].
- Cardiac rhythm management for patients with heart failure with reduced ejection fraction: Antiarrhythmic drugs | Implantable cardioverter defibrillator | Cardiac resynchronization therapy
- Nutritional supplements and hormonal therapies
- Exercise training
- Drugs to avoid
- Drug interactions
- Treatment of underlying causes
- Treatment of associated conditions
Ultrafiltration | Mechanical circulatory support | Heart transplantation
ACC/AHA Guideline Recommendations
ACC/AHA Guideline Recommendations
Treatment of Hypertension | Treatment of Diabetes Mellitus | Management of Metabolic Syndrome | Management of Atherosclerotic Disease | Control of Conditions That May Cause Heart Failure | ACC/AHA Guideline Recommendations
Implementation of Practice Guidelines
End-Of-Life Considerations
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1] Associate Editor(s)-in-Chief: Edzel Lorraine Co, D.M.D., M.D. [2]
Overview
End of life care in the patient with congestive heart failure is focused on making the patient comfortable. Invasive procedures should be minimized, and patients may elect to have their defibrillators inactivated. The growing number of patients with Stage IV heart failure (intractable symptoms of fatigue, shortness of breath or chest pain at rest despite optimal medical therapy) should be considered for palliative care or hospice, according to American College of Cardiology/American Heart Association guidelines listed below.
Some have argued that any patient with NYHA class III CHF should have a palliative care referral. Palliative care can not only provide symptom management, but also assist with advanced care planning, goals of care in the case of a significant decline, and making sure the patient has a medical power of attorney and discussed his or her wishes with this individual.
2022 AHA/ACC/HFSA Guideline/ 2013 ACCF/AHA Guideline/2009 ACC/AHA Focused Update and 2005 Guidelines for the Diagnosis and Management of Heart Failure in the Adult (DO NOT EDIT) [1] [2][3]
| Class I |
| “1.For all patients with HF, palliative and supportive care- including high-quality communication, conveyance of prognosis, clarifying goals of care, shared decision-making, symptom management, and caregiver support- should be provided to improve QOL and relieve suffering. [4](Level of Evidence: C-LD) ” |
| “2. For patients with HF being considered for, or treated with, life-extending therapies, the option for discontinuation should be anticipated and discussed through the continuum of care, including at the time of initiation, and reassessed with changing medical conditions and shifting goals of care.[5][6] (Level of Evidence: C-LD) ” |
| Class IIa |
| “3. For patients with HF– particularly stage D HF patients being evaluated for advanced therapies, patients requiring inotropic support or temporary mechanical support, patients experiencing uncontrolled symptoms, major medical decisions, or multimorbidity, frailty, and cognitive impairment – specialist palliative care consultation can be useful to improve QOL and relieve suffering. [7][8][9](Level of Evidence: B-R) ” |
| “4. For patients with HF, execution of advance care directives can be useful to improve documentation of treatment preferences, delivery of patient-centered care, and dying in preferred place.[10](Level of Evidence: C-LD) ” |
| “5. In patients with advanced HF with expected survival <6 months, timely referral to hospice can be useful to improve QOL. [11](Level of Evidence: C-LD) ” |
Vote on and Suggest Revisions to the Current Guidelines
External Links
- 2022 AHA/ACC/HFSA Guideline for the Management of Heart Failure: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines[12]
- 2009 focused update: ACCF/AHA Guidelines for the Diagnosis and Management of Heart Failure in Adults: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines: developed in collaboration with the International Society for Heart and Lung Transplantation [3]
- The ACC/AHA 2005 Guideline Update for the Diagnosis and Management of Chronic Heart Failure in the Adult [13]
References
- ↑ 1.0 1.1 Heidenreich PA, Bozkurt B, Aguilar D, Allen LA, Byun JJ, Colvin MM; et al. (2022). “2022 AHA/ACC/HFSA Guideline for the Management of Heart Failure: Executive Summary: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines”. Circulation. 145 (18): e876–e894. doi:10.1161/CIR.0000000000001062. PMID 35363500 Check
|pmid=value (help). - ↑ 2.0 2.1 2.2 Yancy CW, Jessup M, Bozkurt B, Masoudi FA, Butler J, McBride PE; et al. (2013). “2013 ACCF/AHA Guideline for the Management of Heart Failure: A Report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines”. J Am Coll Cardiol. doi:10.1016/j.jacc.2013.05.019. PMID 23747642.
- ↑ 3.0 3.1 3.2 Jessup M, Abraham WT, Casey DE, Feldman AM, Francis GS, Ganiats TG et al. (2009) 2009 focused update: ACCF/AHA Guidelines for the Diagnosis and Management of Heart Failure in Adults: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines: developed in collaboration with the International Society for Heart and Lung Transplantation. Circulation 119 (14):1977-2016.DOI:10.1161/CIRCULATIONAHA.109.192064 PMID:19324967
- ↑ Datla S, Verberkt CA, Hoye A, Janssen DJA, Johnson MJ (2019). “Multi-disciplinary palliative care is effective in people with symptomatic heart failure: A systematic review and narrative synthesis”. Palliat Med. 33 (8): 1003–1016. doi:10.1177/0269216319859148. PMID 31307276.
- ↑ Goldstein N, Carlson M, Livote E, Kutner JS (2010). “Brief communication: Management of implantable cardioverter-defibrillators in hospice: A nationwide survey”. Ann Intern Med. 152 (5): 296–9. doi:10.7326/0003-4819-152-5-201003020-00007. PMC 2832227. PMID 20194235.
- ↑ McIlvennan CK, Jones J, Allen LA, Swetz KM, Nowels C, Matlock DD (2016). “Bereaved Caregiver Perspectives on the End-of-Life Experience of Patients With a Left Ventricular Assist Device”. JAMA Intern Med. 176 (4): 534–9. doi:10.1001/jamainternmed.2015.8528. PMID 26998594.
- ↑ Rogers JG, Patel CB, Mentz RJ, Granger BB, Steinhauser KE, Fiuzat M; et al. (2017). “Palliative Care in Heart Failure: The PAL-HF Randomized, Controlled Clinical Trial”. J Am Coll Cardiol. 70 (3): 331–341. doi:10.1016/j.jacc.2017.05.030. PMC 5664956. PMID 28705314.
- ↑ Bekelman DB, Allen LA, McBryde CF, Hattler B, Fairclough DL, Havranek EP; et al. (2018). “Effect of a Collaborative Care Intervention vs Usual Care on Health Status of Patients With Chronic Heart Failure: The CASA Randomized Clinical Trial”. JAMA Intern Med. 178 (4): 511–519. doi:10.1001/jamainternmed.2017.8667. PMC 5876807. PMID 29482218.
- ↑ O’Donnell AE, Schaefer KG, Stevenson LW, DeVoe K, Walsh K, Mehra MR; et al. (2018). “Social Worker-Aided Palliative Care Intervention in High-risk Patients With Heart Failure (SWAP-HF): A Pilot Randomized Clinical Trial”. JAMA Cardiol. 3 (6): 516–519. doi:10.1001/jamacardio.2018.0589. PMC 6128511. PMID 29641819.
- ↑ Schichtel M, Wee B, Perera R, Onakpoya I (2020). “The Effect of Advance Care Planning on Heart Failure: a Systematic Review and Meta-analysis”. J Gen Intern Med. 35 (3): 874–884. doi:10.1007/s11606-019-05482-w. PMC 7080664 Check
|pmc=value (help). PMID 31720968. - ↑ Candy B, Holman A, Leurent B, Davis S, Jones L (2011). “Hospice care delivered at home, in nursing homes and in dedicated hospice facilities: A systematic review of quantitative and qualitative evidence”. Int J Nurs Stud. 48 (1): 121–33. doi:10.1016/j.ijnurstu.2010.08.003. PMID 20846650.
- ↑ Heidenreich PA, Bozkurt B, Aguilar D, Allen LA, Byun JJ, Colvin MM, Deswal A, Drazner MH, Dunlay SM, Evers LR, Fang JC, Fedson SE, Fonarow GC, Hayek SS, Hernandez AF, Khazanie P, Kittleson MM, Lee CS, Link MS, Milano CA, Nnacheta LC, Sandhu AT, Stevenson LW, Vardeny O, Vest AR, Yancy CW (May 2022). “2022 AHA/ACC/HFSA Guideline for the Management of Heart Failure: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines”. Circulation. 145 (18): e895–e1032. doi:10.1161/CIR.0000000000001063. PMID 35363499 Check
|pmid=value (help). - ↑ Hunt SA, Abraham WT, Chin MH, Feldman AM, Francis GS, Ganiats TG et al. (2005) ACC/AHA 2005 Guideline Update for the Diagnosis and Management of Chronic Heart Failure in the Adult: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Update the 2001 Guidelines for the Evaluation and Management of Heart Failure): developed in collaboration with the American College of Chest Physicians and the International Society for Heart and Lung Transplantation: endorsed by the Heart Rhythm Society. Circulation 112 (12):e154-235. DOI:10.1161/CIRCULATIONAHA.105.167586 PMID: 16160202
Specific Groups
Specific Groups
Special Populations | Patients who have concomitant disorders | Obstructive Sleep Apnea in the Patient with CHF
References
References
- ↑ Dorsch, Michael P.; Sifuentes, Aaron; Cordwin, David J.; Kuo, Rachel; Rowell, Brigid E.; Arzac, Juan J.; DeBacker, Ken; Guidi, Jessica L.; Hummel, Scott L.; Koelling, Todd M. (April 2023). “A Computable Algorithm for Medication Optimization in Heart Failure With Reduced Ejection Fraction”. JACC: Advances: 100289. doi:10.1016/j.jacadv.2023.100289. ISSN 2772-963X.
Looking for the patient version?
© 2026 MyEClinic – IFTM Institut für Telematik in der Medizin GmbH