
Eosinophilic esophagitis
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1], Associate Editor(s)-in-Chief: Ajay Gade MD[2]]
Synonyms and keywords:: Eosinophilic oesophagitis
Overview
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1], Associate Editor(s)-in-Chief: Ajay Gade MD[2]]
Overview
Eosinophilic esophagitis (EoE) is an immunoallergic disorder resulting from the interaction between genetics and environmental triggers such as repeated exposure to food and aeroallergens. The documented cytokine expression profile in the esophageal tissue of EoE patients is that of a TH2 inflammatory response. IL-5 and IL-13 are produced by the type-2 helper T cells (Th2) in response to the antigenic proteins from the food or inhalation. Cytokines produced by TH-1 cells are tumor necrosis factor (TNF)-α, Interferon (IFN)-γ. CD34+ myeloid precursor cells in the bone marrow produce eosinophils and then the eosinophils develop granulation and migrate to vascular spaces. Eosinophils cause inflammation in the EoE patients by the following mechanisms angiogenic molecules from the eosinophils recruits the inflammatory cells and the increase the vascularity. Fibrogenic mediators such as TGF-β1 and matrix metalloproteinase 9 (MMP)-9 causes the airway remodeling. The esophageal mucosa in patients with a longstanding EoE is characterized by a loss of elasticity. On histologic examination of the subepithelial compartments of the esophagus show an increase in the fibrous tissue. There is no established system for the classification of Eosinophilic esophagitis (EoE). The causes of EoE include food and pollens. Eosinophilic esophagitis must be differentiated from other diseases that cause dysphagia such as reflux esophagitis, esophageal carcinoma, systemic sclerosis, esophageal spasm, pseudoachalasia, stroke, esophageal candidiasis and chagas disease. The incidence Eosinophilic esophagitis (EoE) is approximately 10 per 100,000 individuals worldwide. The prevalence of EoE is approximately 50-100 per 100,000 individuals worldwide. The risk factors of EoE are as follows bimodal age distribution, male gender, cold and dry climate. The history and symptoms of eosinophilic esophagitis (EoE), dysphagia, regurgitation, cough, chest pain, food impaction, upper abdominal pain, vomiting.The complications of the EoE includes Scarring of esophagus-leading to dysphagia, Esophageal stenosis, Tears or perforation during the endoscopy or retching leading to boerhaave syndrome.As relatively newly recognized disease, there is very limited data on the causes, natural history, prognosis, diagnosis and management of these patients. The long-term prognosis of the EoE is unclear but patients diagnosed with EoE have an unaffected lifespan. Patients who are untreated or have discontinued the treatment have progression of their symptoms. The EoE patients with a narrow esophageal lumen are resistant to the corticosteroid treatment and require many esophageal endoscopic procedures. There are no specific diagnostic markers to diagnose the EoE patients, however, an increased peripheral eosinophil count is also seen in majority patients. The barium swallow of the esophagus shows multiple rings associated with eosinophilic esophagitis, There are no MRI nor CT scan findings associated with EoE. however, an MRI or a CT scan may be helpful in the diagnosis of complications of EoE such as tears, perforation strictures etc. The optimal treatment of eosinophilic esophagitis remains uncertain. An eight-week course of therapy with topical corticosteroids (fluticasone or budesonide) may be used as the first-line pharmacologic therapy. Allergen elimination usually leads to improvement in dysphagia and reduction of eosinophil infiltration. Esophageal dilation of is generally reserved for refractory cases with esophageal stricture.
Historical Perspective
In 1981, Picus and Frank reported a case of a 16-year-old boy with progressive dysphagia for 1.5 years, endoscopic findings were suggestive of multiple 1-mm nodular filling defects in the esophagus in an area of stricture with dilatation above. The radiology showed a luminal narrowing, wall rigidity, and high circulating eosinophil count assumed to be a variant of eosinophilic gastroenteritis.
Classification
There is no established system for the classification of Eosinophilic esophagitis (EoE).
Pathophysiology
Eosinophilic esophagitis is an immunoallergic disorder resulting from the interaction between genetics and environmental triggers such as repeated exposure to food and aeroallergens. Patients presenting with EoE have a history of elevated serum IgE levels, response to interventions such as diet restriction, history of food hypersensitivity. Eosinophils originate from CD34+ myeloid precursor cells in the bone marrow, mature to a granulated state and migrate to vascular spaces. The eosinophils are absent in an otherwise normal esophagus, the presence of the eosinophils in the esophagus suggests GERD or EoE. They tend to be present in all layers of the esophagus in EoE, but predominate in the lamina propria and submucosal regions. The documented cytokine expression profile in the esophageal tissue of EoE patients is that of a TH2 inflammatory response. IL-5 and IL-13 are produced by the type-2 helper T cells (Th2) in response to the antigenic proteins from the food or inhalation. IL-13 further stimulates the epithelial cells of the esophagus to produce large proteins to induce a gene called eotaxin-3, which in turn recruits eosinophils from the peripheral blood into the tissue. IL-5 prolongs the survival of the eosinophils. The activated TH2 response leads to the recruitment and activation of Mast cells degranulate and cause tissue damage and repair. Cytokines produced by TH-1 cells are tumor necrosis factor (TNF)-α, Interferon (IFN)-γ, TNF-α is expressed by the epithelial cells of the esophagus whereas the INF-γ is upregulated by the peripheral T cells. Delayed or type- IV hypersensitivity is the mechanism is involved in the EoE rather than the non-IgE. It is postulated that the EoE-defining endoscopic and histologic manifestations are a culmination of the disease process which, may have debilitating long-term effects including strictures and food impactions in untreated or poorly managed cases of EoE. CD34+ myeloid precursor cells in the bone marrow produce eosinophils and then the eosinophils develop granulation and migrate to vascular spaces. Eosinophils although present in all the layers of the esophagus in patients with EoE, they are predominant in the lamina propria and submucosa of the esophagus. The preformed granule proteins of the eosinophils are ECP- Eosinophil Cationic Protein, MBP- Major Basic Protein, EPO- Eosinophil Peroxidase, EDN- Eosinophil Derived Neurotoxin. Upon the stimulation and the degranulation, the eosinophils release the granule proteins into the tissues. Eosinophils synthesize and release cytokines such as IL-5, IL-13, Transforming growth factor (TGF)-α and -β, Chemokines (eotaxins and RANTES), Lipid mediators such as platelet activating factor (PAF) and leukotriene C4. IL-5, IL-13, and granulocyte–macrophage colony stimulating factor (GM-CSF) can cause the maturation and migration of the eosinophils. Eosinophils cause inflammation in the EoE patients by the following mechanisms Angiogenic molecules from the eosinophils recruits the inflammatory cells and the increase the vascularity. Fibrogenic mediators such as TGF-β1 and matrix metalloproteinase 9 (MMP)-9 causes the airway remodeling. MBP and MMP-9 disrupt the integrity of the epithelial cells of the esophageal through their involvement in smooth muscles, fibroblasts, and cell-adhesion molecules. The above-mentioned processes lead to tissue remodeling eventually causing an overall esophageal dysfunction.
Causes
The causes of EoE are the food and pollen react with the lining of the esophagus, these allergens cause the multiplication of eosinophils in the layers of the esophagus and produce a protein that causes inflammation. The inflammation further cause scarring, excessive fibrous tissue deposition over the lining of the esophagus eventually leading to dysphagia. The dysphagia can sometimes worsen to cause food impaction and additional symptoms such as chest pain.
Differentiating Eosinophilic esophagitis overview from Other Diseases
Eosinophilic esophagitis must be differentiated from other diseases that cause dysphagia such as reflux esophagitis, esophageal carcinoma, systemic sclerosis, esophageal spasm, pseudoachalasia, stroke, esophageal candidiasis and chagas disease.
Epidemiology and Demographics
The incidence Eosinophilic esophagitis (EoE) is approximately 10 per 100,000 individuals worldwide. The prevalence of EoE is approximately 50-100 per 100,000 individuals worldwide. Patients of all age groups may develop EoE. It usually affects individuals of the white race. Males are more commonly affected by EoE than females. EoE is a rare disease that tends to affect people with a history of European ancestry.
Risk Factors
The risk factors of EoE are as follows bimodal age distribution common in both children and adults, male gender, cold and dry climate, EoE is common in people with a history of European ancestry, summer and fall, positive family history of EoE, history of allergies such as asthma, industrial exposures, environmental allergies, chronic respiratory disease, food allergies and atopic dermatitis.
Screening
There is insufficient evidence to recommend routine screening for Eosinophilic esophagitis (EoE).
Natural History, Complications, and Prognosis
Natural History
The natural course of primary EoE is, in patients with EoE, symptoms persist over years raising suspicion that a chronic inflammatory process is an underlying event responsible for it. The inflammatory activity is proportional to the density of the eosinophilic infiltration in the esophageal tissue. Similar to asthma, EoE has chronic persistent eosinophilic inflammation and can eventually lead to irreversible structural changes of the esophagus which is called re-modeling of the esophagus. The esophageal mucosa in patients with a longstanding EoE is characterized by a loss of elasticity. On histologic examination of the subepithelial compartments of the esophagus show an increase in the fibrous tissue. In patients with EoE, the chronic eosinophilic inflammation leads to an increased deposition of the fibrous connective tissue which in turn causes the remodeling of the esophagus hindering the esophageal transport.
Complications
The complications of the EoE are as follows: Scarring of esophagus-leading to dysphagia, Esophageal stenosis, Tears or perforation during the endoscopy or retching leading to boerhaave syndrome.
Prognosis
The long-term prognosis of the EoE is unclear but patients diagnosed with EoE have an unaffected lifespan.
Diagnosis
Diagnostic Criteria
History and Symptoms
The history and symptoms of eosinophilic esophagitis (EoE), dysphagia, regurgitation, cough, chest pain, food impaction, upper abdominal pain, vomiting. Clinical features in children are follows abdominal pain, nausea, emesis, failure to thrive. Clinical features in the adolescents and adults are as follows dysphagia, heartburn, food impaction, strictures.
Physical Examination
The physical examination of the patients with EoE is usually normal.
Laboratory Findings
There are no specific diagnostic markers to diagnose the EoE patients. Although not specific, elevated serum IgE levels are identified in majority patients. An increased peripheral eosinophil count is also seen in majority patients. There are 3 main ways in which food allergies can be detected in EE are Skin prick testing, Blood allergy testing, Atopy patch testing.
Imaging Findings
The barium swallow of the esophagus shows multiple rings associated with eosinophilic esophagitis, There are no MRI or CT scan findings associated with EoE. however, an MRI or a CT scan may be helpful in the diagnosis of complications of EoE such as tears, perforation strictures etc
Other Diagnostic Studies
Treatment
Medical Therapy
The optimal treatment of eosinophilic esophagitis remains uncertain. An eight-week course of therapy with topical corticosteroids (fluticasone or budesonide) may be used as the first-line pharmacologic therapy. Allergen elimination usually leads to improvement in dysphagia and reduction of eosinophil infiltration. Esophageal dilation of is generally reserved for refractory cases with esophageal stricture.
Surgery
Surgical intervention is not recommended for the management of Eosinophilic esophagitis.
Prevention
There are no established measures for the primary prevention of Eosinophilic esophagitis (EoE).
References
Historical Perspective
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1], Associate Editor(s)-in-Chief: Ajay Gade MD[2]]
Overview
In 1981, Picus and Frank reported a case of a 16-year-old boy with progressive dysphagia for 1.5 years, endoscopic findings were suggestive of multiple 1-mm nodular filling defects in the esophagus in an area of stricture with dilatation above. The radiology showed a luminal narrowing, wall rigidity, and high circulating eosinophil count assumed to be a variant of eosinophilic gastroenteritis.
Historical Perspective
- The historical perspective of the EoE is as the following:[1][2][3][4][5][6][7][8][9][10]
- In 1978, Landres et al reported an isolated case of vigorous achalasia and concluded that this was a variant of eosinophilic gastroenteritis in a patient with marked hypertrophy and eosinophilic infiltration of esophagus.
- In 1981, Picus and Frank reported a case of a 16-year-old boy with progressive dysphagia for 1.5 years, endoscopic findings were suggestive of multiple 1-mm nodular filling defects in the esophagus in an area of stricture with dilatation above.
- The radiology showed a luminal narrowing, wall rigidity, and high circulating eosinophil count assumed to be a variant of eosinophilic gastroenteritis.
- In 1982, Münch et al and in 1983, Matzinger and Daneman both described isolated cases of esophageal eosinophilia with dysphagia in patients with assumed eosinophilic gastroenteritis.
- In 1985, Feczko et al reported 3 cases of eosinophilic infiltration of esophagus, with 2 of the patients showing eosinophilic gastroenteritis. Two out of the three patients developed esophageal stricture secondary to submucosal fibrosis.
- In 1985, eosinophilic infiltration was reported in esophageal mucosal biopsy of 11 patients with average age of 14.6 years. These patients had reflux symptoms and their eosinophil density was low. In retrospect, these were probably patients with gastroesophageal reflux disease (GERD).
- In 1989, Attwood et al described esophageal asthma, an episodic dysphagia with eosinophilic infiltrates.
- These investigators compared a group of 15 adults who presented with dysphagia without esophageal obstruction and normal pH monitoring to a group of 100 adults with GERD as defined by increased acid exposure in the distal esophagus.
- In 1993, Attwood et al reported 12 adults with dysphagia, normal pH monitoring, and dense esophageal eosinophilia. Seven patients had food hypersensitivity, and all required advanced intervention (dilatation and/or steroids in 1 case) for resolution of symptoms.
- In 1994, Straumann et al described a series of 10 patients with acute recurrent dysphagia seen over a 4-year period. These patients showed discrete endoscopic changes, and high concentrations of epithelial esophageal eosinophils. They improved following systemic steroid and antihistamine treatment.
- In 1995 the first publication in children was reported by Kelly et al. They identified 10 children who were diagnosed on clinical and histological grounds to have EoE.
- Six out of those ten had been subject to antireflux therapy without any symptomatic improvement. Two of these patients had already received fundoplication, and all responded well to amino acid formulas, suggesting an allergic etiology.
- The characteristics in pediatric EoE appeared to reflect greater amounts of regurgitation and failure to thrive, while the typical presentation in adults with EoE was dysphagia and food impaction.
- In 2003 the chronic nature of the natural history of EoE was described by Straumann et after the follow-up of 30 adults with EoE.
References
- ↑ Landres RT, Kuster GG, Strum WB (1978). “Eosinophilic esophagitis in a patient with vigorous achalasia”. Gastroenterology. 74 (6): 1298–1301. PMID 648822.
- ↑ Picus D, Frank PH (1981). “Eosinophilic esophagitis”. AJR Am J Roentgenol. 136 (5): 1001–3. doi:10.2214/ajr.136.5.1001. PMID 6784497.
- ↑ Matzinger MA, Daneman A (1983). “Esophageal involvement in eosinophilic gastroenteritis”. Pediatr Radiol. 13 (1): 35–8. PMID 6844053.
- ↑ Feczko PJ, Halpert RD, Zonca M (1985). “Radiographic abnormalities in eosinophilic esophagitis”. Gastrointest Radiol. 10 (4): 321–4. PMID 4054495.
- ↑ Lee RG (1985). “Marked eosinophilia in esophageal mucosal biopsies”. Am. J. Surg. Pathol. 9 (7): 475–9. PMID 4091182.
- ↑ Attwood SE, Smyrk TC, Demeester TR, Jones JB (1993). “Esophageal eosinophilia with dysphagia. A distinct clinicopathologic syndrome”. Dig. Dis. Sci. 38 (1): 109–16. PMID 8420741.
- ↑ Straumann A, Spichtin HP, Bernoulli R, Loosli J, Vögtlin J (1994). “[Idiopathic eosinophilic esophagitis: a frequently overlooked disease with typical clinical aspects and discrete endoscopic findings]”. Schweiz Med Wochenschr (in German). 124 (33): 1419–29. PMID 7939509.
- ↑ Kelly KJ, Lazenby AJ, Rowe PC, Yardley JH, Perman JA, Sampson HA (1995). “Eosinophilic esophagitis attributed to gastroesophageal reflux: improvement with an amino acid-based formula”. Gastroenterology. 109 (5): 1503–12. PMID 7557132.
- ↑ Straumann A, Spichtin HP, Grize L, Bucher KA, Beglinger C, Simon HU (2003). “Natural history of primary eosinophilic esophagitis: a follow-up of 30 adult patients for up to 11.5 years”. Gastroenterology. 125 (6): 1660–9. PMID 14724818.
- ↑ Straumann A, Spichtin HP, Grize L, Bucher KA, Beglinger C, Simon HU (2003). “Natural history of primary eosinophilic esophagitis: a follow-up of 30 adult patients for up to 11.5 years”. Gastroenterology. 125 (6): 1660–9. PMID 14724818.
Classification
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1];Associate Editor(s)-in-Chief: Ajay Gade MD[2]]
Overview
There is no established system for the classification of Eosinophilic esophagitis (EoE).
Classification
There is no established system for the classification of Eosinophilic esophagitis (EoE).
References
Pathophysiology
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1];Associate Editor(s)-in-Chief: Ajay Gade MD[2]]
Overview
Eosinophilic esophagitis is an immunoallergic disorder resulting from the interaction between genetics and environmental triggers such as repeated exposure to food and aeroallergens. Patients presenting with EoE have a history of elevated serum IgE levels, response to interventions such as diet restriction, history of food hypersensitivity. Eosinophils originate from CD34+ myeloid precursor cells in the bone marrow, mature to a granulated state and migrate to vascular spaces. The eosinophils are absent in an otherwise normal esophagus, the presence of the eosinophils in the esophagus suggests GERD or EoE. They tend to be present in all layers of the esophagus in EoE, but predominate in the lamina propria and submucosal regions. The documented cytokine expression profile in the esophageal tissue of EoE patients is that of a TH2 inflammatory response. IL-5 and IL-13 are produced by the type-2 helper T cells (Th2) in response to the antigenic proteins from the food or inhalation. IL-13 further stimulates the epithelial cells of the esophagus to produce large proteins to induce a gene called eotaxin-3, which in turn recruits eosinophils from the peripheral blood into the tissue. IL-5 prolongs the survival of the eosinophils. The activated TH2 response leads to the recruitment and activation of Mast cells degranulate and cause tissue damage and repair. Cytokines produced by TH-1 cells are tumor necrosis factor (TNF)-α, Interferon (IFN)-γ, TNF-α is expressed by the epithelial cells of the esophagus whereas the INF-γ is upregulated by the peripheral T cells. Delayed or type- IV hypersensitivity is the mechanism is involved in the EoE rather than the non-IgE. It is postulated that the EoE-defining endoscopic and histologic manifestations are a culmination of the disease process which, may have debilitating long-term effects including strictures and food impactions in untreated or poorly managed cases of EoE. CD34+ myeloid precursor cells in the bone marrow produce eosinophils and then the eosinophils develop granulation and migrate to vascular spaces. Eosinophils although present in all the layers of the esophagus in patients with EoE, they are predominant in the lamina propria and submucosa of the esophagus. The preformed granule proteins of the eosinophils are ECP- Eosinophil Cationic Protein, MBP- Major Basic Protein, EPO- Eosinophil Peroxidase, EDN- Eosinophil Derived Neurotoxin. Upon the stimulation and the degranulation, the eosinophils release the granule proteins into the tissues. Eosinophils synthesize and release cytokines such as IL-5, IL-13, Transforming growth factor (TGF)-α and -β, Chemokines (eotaxins and RANTES), Lipid mediators such as platelet activating factor (PAF) and leukotriene C4. IL-5, IL-13, and granulocyte–macrophage colony stimulating factor (GM-CSF) can cause the maturation and migration of the eosinophils. Eosinophils cause inflammation in the EoE patients by the following mechanisms Angiogenic molecules from the eosinophils recruits the inflammatory cells and the increase the vascularity. Fibrogenic mediators such as TGF-β1 and matrix metalloproteinase 9 (MMP)-9 causes the airway remodeling. MBP and MMP-9 disrupt the integrity of the epithelial cells of the esophageal through their involvement in smooth muscles, fibroblasts, and cell-adhesion molecules. The above-mentioned processes lead to tissue remodeling eventually causing an overall esophageal dysfunction. TGF-β and eosinophilic granule proteins MBP and EPO are the key eosinophil effector proteins. The importance of eosinophils in mediating tissue fibrosis is supported by evidence in both murine and human models. These findings not only highlight the importance of targeting fibrosis reversal in treatment of EoE, but also underline the importance of eosinophils in tissue remodeling.
Pathophysiology
- The pathophysiology of the EoE is as follows:[1][2][3][4][5][6][7][8][9][10]
- Eosinophilic esophagitis is an immunoallergic disorder resulting from the interaction between genetics and environmental triggers such as repeated exposure to food and aeroallergens.
- Patients presenting with EoE have a history of:
- Elevated serum IgE levels
- Response to interventions such as diet restriction
- History of food hypersensitivity
- Eosinophils originate from CD34+ myeloid precursor cells in the bone marrow, mature to a granulated state and migrate to the vascular spaces.
- The eosinophils are absent in an otherwise normal esophagus, the presence of the eosinophils in the esophagus suggests GERD or EoE.
- They tend to be present in all layers of the esophagus in EoE, but predominate in the lamina propria and submucosal regions.
- The documented cytokine expression profile in the esophageal tissue of patients is that of a TH2 inflammatory response.
- IL-5 and IL-13 are produced by the type-2 helper T cells (Th2) in response to the antigenic proteins from the food or inhalation.
- IL-13 further stimulates the epithelial cells of the esophagus to produce large proteins to induce a gene called eotaxin-3, which in turn recruits eosinophils from the peripheral blood into the tissue.
- IL-5 prolongs the survival of the eosinophils.
- The activated TH2 response leads to the recruitment and activation of
- Mast cells degranulate and cause tissue damage and repair.
- Cytokines produced by TH-1 cells are
- TNF-α is expressed by the epithelial cells of the esophagus whereas INF-γ is upregulated by the peripheral T cells.
- Delayed or type- IV hypersensitivity is the mechanism is involved in the EoE.
- It is postulated that the EoE-defining endoscopic and histologic manifestations are a culmination of the disease process which, may have debilitating long-term effects including strictures and food impactions in untreated or poorly managed cases of EoE.
- The preformed granule proteins of the eosinophils are
- ECP– Eosinophil Cationic Protein
- MBP– Major Basic Protein
- EPO– Eosinophil Peroxidase
- EDN– Eosinophil Derived Neurotoxin
- Upon the stimulation and the degranulation, the eosinophils release the granule proteins into the tissues.
- Eosinophils synthesize and release cytokines such as
- IL-5
- IL-13
- Transforming growth factor (TGF)-α and -β
- Chemokines (eotaxins and RANTES)
- Lipid mediators such as platelet activating factor (PAF) and leukotriene C4
- IL-5, IL-13, and granulocyte–macrophage colony stimulating factor (GM-CSF) can cause the maturation and migration of the eosinophils.
- Eosinophils cause inflammation in the EoE patients by the following mechanisms
- Angiogenic molecules from the eosinophils recruits the inflammatory cells and increase the vascularity.
- Fibrogenic mediators such as TGF-β1 and matrix metalloproteinase 9 (MMP)-9 causes the airway remodeling.
- MBP and MMP-9 disrupt the integrity of the epithelial cells of the esophagus through their involvement in the smooth muscles, fibroblasts, and cell-adhesion molecules.
- The above-mentioned processes lead to tissue remodeling eventually, causing an overall esophageal dysfunction.
- TGF-β and eosinophilic granule proteins MBP and EPO are the key eosinophil effector proteins. The importance of eosinophils in mediating tissue fibrosis is supported by evidence in both murine and human models.
- These findings not only highlight the importance of targeting fibrosis reversal in the treatment of EoE, but also underline the importance of eosinophils in tissue remodeling.
Gross Pathology
- Mucosal biopsies of the esophagus should be obtained in all patients in whom EoE is a clinical possibility regardless of the endoscopic appearance.
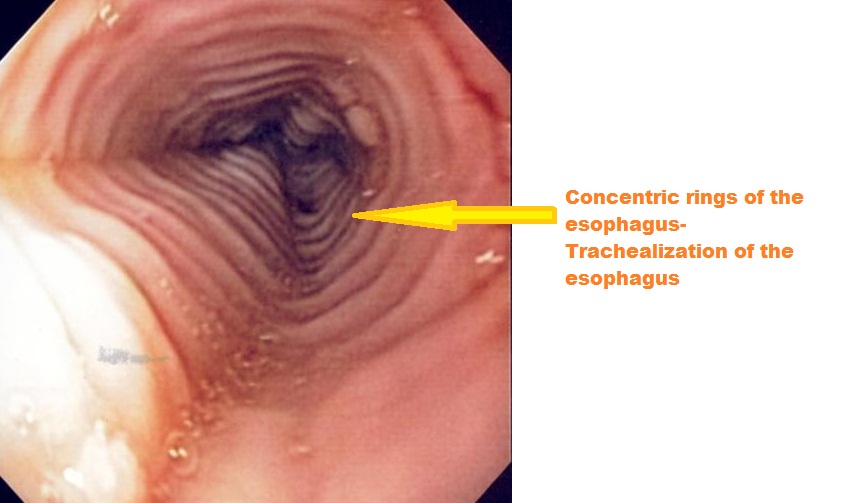
- Endoscopic abnormalities in patients with EoE are as follows:[11][12][13][14][15]
- Fixed esophageal ring which is corrugated
- White exudate
- Longitudinal furrows
- Mucosal pallor
- Diffuse esophageal narrowing
- Mucosal fragility leading to esophageal lacerations during the endoscopy
- However, because these endoscopic features have been described in other esophageal disorders, none can be considered pathognomonic for EoE.
-
 Endoscopy of the esophagus: Eosinophilic esophagitis
Endoscopy of the esophagus: Eosinophilic esophagitis
Source: Wikimedia

Histopathology
- Characteristic features are as follows:
- > 20 eosinophils/0.24 mm2.
- Papillae are elongated
- Papillae reach into the top 1/3 of the epithelial layer
- Basal cell hyperplasia; > 3 cells thick or >15% of epithelial thickness

References
- ↑ Malhotra N, Levine J (2014). “Eosinophilic esophagitis: an autoimmune esophageal disorder”. Curr Probl Pediatr Adolesc Health Care. 44 (11): 335–40. doi:10.1016/j.cppeds.2014.10.004. PMID 25499460.
- ↑ Martin LJ, Franciosi JP, Collins MH, Abonia JP, Lee JJ, Hommel KA, Varni JW, Grotjan JT, Eby M, He H, Marsolo K, Putnam PE, Garza JM, Kaul A, Wen T, Rothenberg ME (2015). “Pediatric Eosinophilic Esophagitis Symptom Scores (PEESS v2.0) identify histologic and molecular correlates of the key clinical features of disease”. J. Allergy Clin. Immunol. 135 (6): 1519–28.e8. doi:10.1016/j.jaci.2015.03.004. PMC 4460579. PMID 26051952.
- ↑ Lucendo AJ, Arias A, Tenias JM (2014). “Relation between eosinophilic esophagitis and oral immunotherapy for food allergy: a systematic review with meta-analysis”. Ann. Allergy Asthma Immunol. 113 (6): 624–9. doi:10.1016/j.anai.2014.08.004. PMID 25216976.
- ↑ López-Colombo A (2012). “[Eosinophilic esophagitis]”. Rev Gastroenterol Mex (in Spanish; Castilian). 77 Suppl 1: 1–3. doi:10.1016/j.rgmx.2012.07.002. PMID 22939463.
- ↑ Chehade M, Lucendo AJ, Achem SR, Souza RF (2013). “Causes, evaluation, and consequences of eosinophilic esophagitis”. Ann. N. Y. Acad. Sci. 1300: 110–8. doi:10.1111/nyas.12243. PMID 24117638.
- ↑ Straumann A (2013). “Eosinophilic esophagitis: a bulk of mysteries”. Dig Dis. 31 (1): 6–9. doi:10.1159/000347095. PMID 23797116.
- ↑ Straumann A (2012). “Eosinophilic esophagitis: rapidly emerging disorder”. Swiss Med Wkly. 142: w13513. doi:10.4414/smw.2012.13513. PMID 22307811.
- ↑ Schoepfer AM, Simon D, Straumann A (2011). “Eosinophilic oesophagitis: latest intelligence”. Clin. Exp. Allergy. 41 (5): 630–9. doi:10.1111/j.1365-2222.2011.03739.x. PMID 21429051.
- ↑ Godat S, Moradpour D, Schoepfer A (2011). “[Eosinophilic esophagitis: update 2011]”. Rev Med Suisse (in French). 7 (307): 1678–80, 1682. PMID 21987875.
- ↑ Potter JW, Saeian K, Staff D, Massey BT, Komorowski RA, Shaker R, Hogan WJ (2004). “Eosinophilic esophagitis in adults: an emerging problem with unique esophageal features”. Gastrointest. Endosc. 59 (3): 355–61. PMID 14997131.
- ↑ 44</a>)”>“Table 3: Proposed classification and grading system for the endoscopic assessment of the esophageal features of eosinophilic esophagitis (<a id=ref-link-section-1 title=”” href=/articles/#ref44>44</a>)”.
- ↑ “Vertical lines in distal esophageal mucosa (VLEM): a true endoscopic manifestation of esophagitis in children? – PubMed – NCBI”.
- ↑ “Fragility of the esophageal mucosa: a pathognomonic endoscopic sign of primary eosinophilic esophagitis? – PubMed – NCBI”.
- ↑ “Eosinophilic esophagitis: red on microscopy, white on endoscopy. – PubMed – NCBI”.
- ↑ “The prevalence and diagnostic utility of endoscopic features of eosinophilic esophagitis: a meta-analysis. – PubMed – NCBI”.
Causes
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1];Associate Editor(s)-in-Chief: Ajay Gade MD[2]]
Overview
The causes of EoE are the food and pollen react with the lining of the esophagus, these allergens cause the multiplication of eosinophils in the layers of the esophagus and produce a protein that causes inflammation. The inflammation further cause scarring, excessive fibrous tissue deposition over the lining of the esophagus eventually leading to dysphagia. The dysphagia can sometimes worsen to cause food impaction and additional symptoms such as chest pain.
Causes
- The causes of EoE are as follows:[1][2][3][4][5][6][7]
- The food and pollen react with the lining of the esophagus, these allergens cause the multiplication of eosinophils in the layers of the esophagus and produce a protein that causes inflammation.
- The inflammation further cause scarring, excessive fibrous tissue deposition over the lining of the esophagus eventually leading to dysphagia.
- The dysphagia can sometimes worsen to cause food impaction and additional symptoms such as chest pain.
EoE contributes to or causes GERD
- Various hypotheses have been proposed that EoE contributes to the development of GERD.
- Mucosal barrier– Eosinophils secrete inflammatory mediators such as VIP (Vasoactive intestinal peptide), PAF (platelet-activating factor), IL-6 which damages the integrity of the mucosal barrier and the smooth muscles of the esophagus.
- Peristalsis– VIP and PAF predisposes a patient to reflux by inducing relaxation of the LES, whereas the IL-6 affects the peristalsis and clearance of the acid, the alterations in esophageal function contribute to increased acid exposure due to impaired clearance of reflux contents
- Cytotoxic effect– Eosinophil cationic protein, Major basic protein, and Eosinophil peroxidase secreted by eosinophils have a direct cytotoxic effect on the mucosa, rendering the esophageal epithelium more susceptible to caustic injury by reflux gastric contents.
- Epithelial cells and nerves– the above-mentioned events exposes the epithelial cells and nerves to further acid injury.
- Remodeling– fibrosis and increased thickness of the esophageal wall, eventually leads to an increase in esophageal mural stiffness causing esophageal remodeling.
GERD contributes to or causes EoE
- There is a possibility that GERD may cause EoE.
- The pathognomic histological feature of the GERD is dilation of inter-cellular spaces of the esophageal squamous epithelium.
- Increased mucosal permeability in GERD due to a breach of the mucosal integrity of the esophagus leads to the penetration of allergens that may have been swallowed into the sub-epithelial space, which may then be accessed by antigen-presenting cells.
- The initial step of allergic sensitization involves antigen presentation by dendritic cells to naive T cells which are transformed to antigen-specific type 2 T helper (TH2) cells.
- The thymic stromal lymphopoietin (TSLP) production from the esophageal epithelium primes esophageal mucosal basophils to secrete IL-4, which promotes the allergic sensitization process.
References
- ↑ Makar AB, McMartin KE, Palese M, Tephly TR, Kia L, Hirano I (1975). “Formate assay in body fluids: application in methanol poisoning”. Biochem Med. 13 (2): 117–26. doi:10.1038/nrgastro.2015.75. PMC 4948861. PMID 1.
- ↑ Savarino EV, Tolone S, Bartolo O, de Cassan C, Caccaro R, Galeazzi F, Nicoletti L, Salvador R, Martinato M, Costantini M, Savarino V (2016). “The GerdQ questionnaire and high resolution manometry support the hypothesis that proton pump inhibitor-responsive oesophageal eosinophilia is a GERD-related phenomenon”. Aliment. Pharmacol. Ther. 44 (5): 522–30. doi:10.1111/apt.13718. PMID 27373195.
- ↑ Straumann A (2013). “Eosinophilic esophagitis: a bulk of mysteries”. Dig Dis. 31 (1): 6–9. doi:10.1159/000347095. PMID 23797116.
- ↑ Straumann A (2012). “Eosinophilic esophagitis: rapidly emerging disorder”. Swiss Med Wkly. 142: w13513. doi:10.4414/smw.2012.13513. PMID 22307811.
- ↑ Schoepfer AM, Simon D, Straumann A (2011). “Eosinophilic oesophagitis: latest intelligence”. Clin. Exp. Allergy. 41 (5): 630–9. doi:10.1111/j.1365-2222.2011.03739.x. PMID 21429051.
- ↑ Godat S, Moradpour D, Schoepfer A (2011). “[Eosinophilic esophagitis: update 2011]”. Rev Med Suisse (in French). 7 (307): 1678–80, 1682. PMID 21987875.
- ↑ Potter JW, Saeian K, Staff D, Massey BT, Komorowski RA, Shaker R, Hogan WJ (2004). “Eosinophilic esophagitis in adults: an emerging problem with unique esophageal features”. Gastrointest. Endosc. 59 (3): 355–61. PMID 14997131.
Differentiating Eosinophilic Esophagitis from other Diseases
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1];Associate Editor(s)-in-Chief: Ajay Gade MD[2]]
Overview
Eosinophilic esophagitis must be differentiated from other diseases that cause dysphagia such as reflux esophagitis, esophageal carcinoma, systemic sclerosis.
Differential Diagnosis
| Dysphagia | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Oropharyngeal dysphagia | Esophageal dysphagia | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Solids only | Solids and Liquids | Solids only | Solids and Liquids | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| •Zenker’s diverticulum •Neoplasm •Webs | Neurogenic | Myogenic | Pain | •Achalasia •Scleroderma •DES | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| •Myasthenia gravis •Connective tissue disorder •Myotonic dystrophy | No | Yes | Heart burn | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Barium swallow | Mental status | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| •Pill esophagitis •Caustic injury •Chemotherapy | Yes | No | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Impaired | Normal | Non progressive | Progressive | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Sac | Webs | Mass | Scleroderma | •Achalasia •DES | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Stroke | •ALS •Parkinsonism | •Rings •Webs | •Strictures •Cancer | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Zenker’s diverticulum | Plummer-Vinson syndrome | Carcinoma | Chest pain and manometry | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Barium swallow | Weight loss | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Increase LES pressure | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Rings | Webs | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Yes | No | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Rapid | Slow | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Achalasia | DES | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Cancer | Strictures/GERD | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Eosinophilic esophagitis must be differentiated from other diseases that cause dysphagia such as reflux esophagitis, esophageal carcinoma, and systemic sclerosis.[1][2][3][4][5][6][7][8][9][10][11]
| Disease | Signs and Symptoms | Barium esophagogram | Endoscopy | Other imaging and laboratory findings | Gold Standard | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Onset | Dysphagia | Weight loss | Heartburn | Other findings | Mental status | |||||||
| Solids | Liquids | Type | ||||||||||
| Plummer-Vinson syndrome |
|
+ | – | Non progressive | +/- | – | Normal |
|
|
|
Triad of | |
| Esophageal stricture |
|
+ | – | Progressive | +/- | +/- | Normal |
|
|
|
||
| Diffuse esophageal spasm |
|
+ | + | Non progressive | + | + | Normal |
|
|
|
||
| Achalasia |
|
+ | + | Non progressive | +/- | – |
|
Normal |
|
|||
| Systemic sclerosis |
|
+ | + | Progressive | +/- | + |
|
Normal |
|
|
Positive serology for | |
| Zenker’s diverticulum |
|
+ | – | +/- | – |
|
Normal |
|
|
| ||
| Esophageal carcinoma |
|
+ | + | Progressive | + | +/- | Normal |
|
|
|||
| Stroke |
|
+ | + | Progressive | + | +/- |
|
Impaired |
|
|
||
| Motor disorders |
|
+ | + | Progressive | +/- | Normal |
|
|
|
| ||
| GERD |
|
+ | – | Progressive | +/- | + | Normal |
|
|
| ||
| Esophageal web |
|
+ | +/- | Progressive | – | +/- |
|
Normal |
|
|
|
|
| Eosinophilic esophagitis | Gradual | + | Progressive | +/- | +/- |
|
Normal | |||||
References
- ↑ Ferri, Fred (2015). Ferri’s clinical advisor 2015 : 5 books in 1. Philadelphia, PA: Elsevier/Mosby. ISBN 978-0323083751.
- ↑ Boeckxstaens GE, Zaninotto G, Richter JE (2013). “Achalasia”. Lancet. doi:10.1016/S0140-6736(13)60651-0. PMID 23871090.
- ↑ Badillo R, Francis D (2014). “Diagnosis and treatment of gastroesophageal reflux disease”. World J Gastrointest Pharmacol Ther. 5 (3): 105–12. doi:10.4292/wjgpt.v5.i3.105. PMC 4133436. PMID 25133039.
- ↑ Napier KJ, Scheerer M, Misra S (2014). “Esophageal cancer: A Review of epidemiology, pathogenesis, staging workup and treatment modalities”. World J Gastrointest Oncol. 6 (5): 112–20. doi:10.4251/wjgo.v6.i5.112. PMC 4021327. PMID 24834141.
- ↑ Matsuura H (2017). “Diffuse Esophageal Spasm: Corkscrew Esophagus”. Am. J. Med. doi:10.1016/j.amjmed.2017.08.041. PMID 28943381.
- ↑ Lassen JF, Jensen TM (1992). “[Corkscrew esophagus]”. Ugeskr. Laeg. (in Danish). 154 (5): 277–80. PMID 1736462.
- ↑ Ruigómez A, García Rodríguez LA, Wallander MA, Johansson S, Eklund S (2006). “Esophageal stricture: incidence, treatment patterns, and recurrence rate”. Am. J. Gastroenterol. 101 (12): 2685–92. doi:10.1111/j.1572-0241.2006.00828.x. PMID 17227515.
- ↑ Shami VM (2014). “Endoscopic management of esophageal strictures”. Gastroenterol Hepatol (N Y). 10 (6): 389–91. PMC 4080876. PMID 25013392.
- ↑ López Rodríguez MJ, Robledo Andrés P, Amarilla Jiménez A, Roncero Maíllo M, López Lafuente A, Arroyo Carrera I (2002). “Sideropenic dysphagia in an adolescent”. J. Pediatr. Gastroenterol. Nutr. 34 (1): 87–90. PMID 11753173.
- ↑ Chisholm M (1974). “The association between webs, iron and post-cricoid carcinoma”. Postgrad Med J. 50 (582): 215–9. PMC 2495558. PMID 4449772.
- ↑ Larsson LG, Sandström A, Westling P (1975). “Relationship of Plummer-Vinson disease to cancer of the upper alimentary tract in Sweden”. Cancer Res. 35 (11 Pt. 2): 3308–16. PMID 1192404.
Epidemiology and Demographics
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1];Associate Editor(s)-in-Chief: Ajay Gade MD[2]]
Overview
The incidence of Eosinophilic esophagitis (EoE) is approximately 10 per 100,000 individuals worldwide. The prevalence of EoE is approximately 50-100 per 100,000 individuals worldwide. Patients of all age groups may develop EoE. It usually affects individuals of the white race. Males are more commonly affected by EoE than females. EoE is a rare disease that tends to affect people with a history of European ancestry.
Epidemiology and Demographics
The Epidemiology and Demographics of the EoE are as follows:[1][2][3][4][5][6]
Incidence
- The incidence of EoE is approximately 10 per 100,000 individuals worldwide.
Prevalence
- The prevalence of EoE is approximately 50-100 per 100,000 individuals worldwide.
Among patients with symptoms[7]:
- Dysphagia: 10.5%
- Heartburn: 6.6%
Age
- Patients of all age groups may develop EoE.
Race
- EoE usually affects individuals of the white race.
Gender
- Males are more commonly affected by EoE than females.
Region
- EoE is a rare disease that tends to affect people with a history of European ancestry.
References
- ↑ Dellon ES (2014). “Epidemiology of eosinophilic esophagitis”. Gastroenterol. Clin. North Am. 43 (2): 201–18. doi:10.1016/j.gtc.2014.02.002. PMC 4019938. PMID 24813510.
- ↑ Soon IS, Butzner JD, Kaplan GG, deBruyn JC (2013). “Incidence and prevalence of eosinophilic esophagitis in children”. J. Pediatr. Gastroenterol. Nutr. 57 (1): 72–80. doi:10.1097/MPG.0b013e318291fee2. PMID 23539047.
- ↑ Sperry SL, Crockett SD, Miller CB, Shaheen NJ, Dellon ES (2011). “Esophageal foreign-body impactions: epidemiology, time trends, and the impact of the increasing prevalence of eosinophilic esophagitis”. Gastrointest. Endosc. 74 (5): 985–91. doi:10.1016/j.gie.2011.06.029. PMC 3951006. PMID 21889135.
- ↑ Cianferoni A, Spergel JM (2015). “Eosinophilic Esophagitis and Gastroenteritis”. Curr Allergy Asthma Rep. 15 (9): 58. doi:10.1007/s11882-015-0558-5. PMID 26233430.
- ↑ Furuta GT, Katzka DA (2015). “Eosinophilic Esophagitis”. N. Engl. J. Med. 373 (17): 1640–8. doi:10.1056/NEJMra1502863. PMC 4905697. PMID 26488694.
- ↑ Kocsis D, Tulassay Z, Juhász M (2015). “[Dietary and pharmacological aspects of eosinophilic esophagitis]”. Orv Hetil (in Hungarian). 156 (23): 927–32. doi:10.1556/650.2015.30164. PMID 26027600.
- ↑ Veerappan GR, Perry JL, Duncan TJ, Baker TP, Maydonovitch C, Lake JM; et al. (2009). “Prevalence of eosinophilic esophagitis in an adult population undergoing upper endoscopy: a prospective study”. Clin Gastroenterol Hepatol. 7 (4): 420–6, 426.e1–2. doi:10.1016/j.cgh.2008.10.009. PMID 19162236.
Risk Factors
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1];Associate Editor(s)-in-Chief: Ajay Gade MD[2]]
Overview
The risk factors of EoE are as follows bimodal age distribution common in both children and adults, male gender, cold and dry climate, EoE is common in people with a history of European ancestry, summer and fall, positive family history of EoE, history of allergies such as asthma, industrial exposures, environmental allergies, chronic respiratory disease, food allergies and atopic dermatitis.
Risk Factors
The risk factors of EoE are as follows:[1][2][3][4][5]
- Age– EoE has a bimodal age distribution common in both children and adults.
- Sex– Males are more prone to EoE than the females.
- Weather– Cold and dry climate trigger EoE.
- Location– EoE is common in people with a history of European ancestry.
- Season– Summer and fall, this is because people stay outdoors during this time and the higher levels of the pollen and the other allergens during these seasons.
- Family history– EoE runs in the family and it is more common in people with a positive family history of the EoE.
- History of allergies– EoE is very common in patient with a history of allergies such as asthma, industrial exposures, environmental allergies, chronic respiratory disease, food allergies and atopic dermatitis.
References
- ↑ “Genetic dissection of eosinophilic esophagitis provides insight into disease pathogenesis and treatment strategies. – PubMed – NCBI”.
- ↑ “www.ncbi.nlm.nih.gov” (PDF).
- ↑ “Genetics of Eosinophilic Esophagitis – FullText – Digestive Diseases 2014, Vol. 32, No. 1-2 – Karger Publishers”.
- ↑ Furuta GT, Katzka DA (2015). “Eosinophilic Esophagitis”. N. Engl. J. Med. 373 (17): 1640–8. doi:10.1056/NEJMra1502863. PMC 4905697. PMID 26488694.
- ↑ Kocsis D, Tulassay Z, Juhász M (2015). “[Dietary and pharmacological aspects of eosinophilic esophagitis]”. Orv Hetil (in Hungarian). 156 (23): 927–32. doi:10.1556/650.2015.30164. PMID 26027600.
Screening
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1];Associate Editor(s)-in-Chief: Ajay Gade MD[2]]
Overview
There is insufficient evidence to recommend routine screening for Eosinophilic esophagitis (EoE).
Screening
There is insufficient evidence to recommend routine screening for Eosinophilic esophagitis (EoE).
References
Natural History, Complications and Prognosis
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1];Associate Editor(s)-in-Chief: Ajay Gade MD[2]]
Overview
In patients with EoE, symptoms persist over years raising suspicion that a chronic inflammatory process is an underlying event responsible for it. The inflammatory activity is proportional to the density of the eosinophilic infiltration in the esophageal tissue. Similar to asthma, EoE has chronic persistent eosinophilic inflammation and can eventually lead to irreversible structural changes of the esophagus which is called re-modeling of the esophagus. The esophageal mucosa in patients with a longstanding EoE is characterized by a loss of elasticity. On histologic examination of the subepithelial compartments of the esophagus show an increase in the fibrous tissue. The endosonographic studies of the esophagus in patients with EoE shows following findings: Thickening of the mucosa, Thickening of the submucosal, and muscularis propria layers. In patients with EoE, the chronic eosinophilic inflammation leads to an increased deposition of the fibrous connective tissue which in turn causes the remodeling of the esophagus hindering the esophageal transport. The complications of the EoE are as follows Scarring of esophagus-leading to dysphagia, Esophageal stenosis– causing food stuck. Tears or perforation during the endoscopy or retching leading to boerhaave syndrome. The prognosis of the EoE is as follows: EoE is a relatively newly recognized disease, there is very limited data on the causes, natural history, prognosis, diagnosis and management of these patients. The long-term prognosis of the EoE is unclear but patients diagnosed with EoE have an unaffected lifespan. Patients should be counseled that although it is a chronic disease, it is a benign condition. Patients who are untreated or have discontinued the treatment have progression of their symptoms. The EoE patients with a narrow esophageal lumen are resistant to the corticosteroid treatment and require many esophageal endoscopic procedures. The dysphagia is common in patients with increased eosinophil count in the blood. The EoE is restricted only to the esophagus sparing the stomach and the duodenum. A common concern by patient and their families is what is the chance of that EoE may progress to a malignancy if untreated, EoE does not progress into metaplasia or dysplasia or esophageal cancer.
Natural History
- The natural course of primary EoE is as follows:[1][2][3]
- In patients with EoE, symptoms persist over years raising suspicion that a chronic inflammatory process is an underlying event responsible for it.
- The inflammatory activity is proportional to the density of the eosinophilic infiltration in the esophageal tissue.
- Similar to asthma, EoE has chronic persistent eosinophilic inflammation and can eventually lead to irreversible structural changes of the esophagus which is called remodeling of the esophagus.
- The esophageal mucosa in patients with a longstanding EoE is characterized by loss of elasticity.
- Histologic examination of the subepithelial compartments of the esophagus shows an increase in the fibrous tissue.
- The endosonographic studies of the esophagus in patients with EoE shows following findings:
- Thickening of the mucosa
- Thickening of the submucosal, and muscularis propria layers
- In patients with EoE, the chronic eosinophilic inflammation leads to an increased deposition of the fibrous connective tissue which in turn causes the remodeling of the esophagus hindering the esophageal transport.
Complications
- The complications of the EoE are as follows:[4][5][6]
- Scarring of esophagus leading to dysphagia
- Esophageal stenosis
- Tears or perforation during the endoscopy or retching leading to boerhaave syndrome.
Prognosis
- The prognosis of the EoE is as follows:[7][8][9][10][11]
- EoE is a relatively newly recognized disease, there is very limited data on the causes, natural history, prognosis, diagnosis and management of these patients.
- The long-term prognosis of EoE is unclear but patients diagnosed with EoE have an unaffected lifespan.
- Patients should be counseled that although it is a chronic disease, it is a benign condition.
- Patients who are untreated or have discontinued the treatment have progression of their symptoms.
- EoE patients with a narrow esophageal lumen are resistant to the corticosteroid treatment and require many esophageal endoscopic procedures..
- dysphagia is common in patients with increased eosinophil count in the blood.
- EoE is restricted only to the esophagus sparing the stomach and the duodenum.
- EoE does not progress into metaplasia or dysplasia or esophageal cancer.
References
- ↑ Attwood SE, Furuta GT (2014). “Eosinophilic esophagitis: historical perspective on an evolving disease”. Gastroenterol. Clin. North Am. 43 (2): 185–99. doi:10.1016/j.gtc.2014.02.010. PMC 4035232. PMID 24813509.
- ↑ Dellon ES, Hirano I (2017). “Epidemiology and Natural History of Eosinophilic Esophagitis”. Gastroenterology. doi:10.1053/j.gastro.2017.06.067. PMID 28774845.
- ↑ Falk GW (2014). “Clinical presentation of eosinophilic esophagitis in adults”. Gastroenterol. Clin. North Am. 43 (2): 231–42. doi:10.1016/j.gtc.2014.02.009. PMID 24813512.
- ↑ Straumann A (2011). “The natural history and complications of eosinophilic esophagitis”. Thorac Surg Clin. 21 (4): 575–87. doi:10.1016/j.thorsurg.2011.09.004. PMID 22040638.
- ↑ Chehade M, Lucendo AJ, Achem SR, Souza RF (2013). “Causes, evaluation, and consequences of eosinophilic esophagitis”. Ann. N. Y. Acad. Sci. 1300: 110–8. doi:10.1111/nyas.12243. PMID 24117638.
- ↑ Saillen E, Cellier C, Naneix AL, Canioni D, Bruneval P, Pouchot J, Georgin-Lavialle S (2014). “[Eosinophilic esophagitis]”. Presse Med (in French). 43 (1): 34–8. doi:10.1016/j.lpm.2013.03.012. PMID 23891531.
- ↑ Dellon ES, Gonsalves N, Hirano I, Furuta GT, Liacouras CA, Katzka DA (2013). “ACG clinical guideline: Evidence-based approach to the diagnosis and management of esophageal eosinophilia and eosinophilic esophagitis (EoE)”. Am. J. Gastroenterol. 108 (5): 679–92, quiz 693. doi:10.1038/ajg.2013.71. PMID 23567357.
- ↑ Lipka S, Keshishian J, Boyce HW, Estores D, Richter JE (2014). “The natural history of steroid-naïve eosinophilic esophagitis in adults treated with endoscopic dilation and proton pump inhibitor therapy over a mean duration of nearly 14 years”. Gastrointest. Endosc. 80 (4): 592–8. doi:10.1016/j.gie.2014.02.012. PMID 24703087.
- ↑ Eluri S, Runge TM, Cotton CC, Burk CM, Wolf WA, Woosley JT, Shaheen NJ, Dellon ES (2016). “The extremely narrow-caliber esophagus is a treatment-resistant subphenotype of eosinophilic esophagitis”. Gastrointest. Endosc. 83 (6): 1142–8. doi:10.1016/j.gie.2015.11.019. PMID 26608127.
- ↑ Straumann A, Spichtin HP, Grize L, Bucher KA, Beglinger C, Simon HU (2003). “Natural history of primary eosinophilic esophagitis: a follow-up of 30 adult patients for up to 11.5 years”. Gastroenterology. 125 (6): 1660–9. PMID 14724818.
- ↑ Spergel JM, Brown-Whitehorn TF, Beausoleil JL, Franciosi J, Shuker M, Verma R, Liacouras CA (2009). “14 years of eosinophilic esophagitis: clinical features and prognosis”. J. Pediatr. Gastroenterol. Nutr. 48 (1): 30–6. doi:10.1097/MPG.0b013e3181788282. PMID 19172120.
Diagnosis
Diagnosis
History and Symptoms | Physical Examination | Laboratory Findings | X Ray | CT | MRI | Other Imaging Findings | Other Diagnostic Studies
Looking for the patient version?
© 2026 MyEClinic – IFTM Institut für Telematik in der Medizin GmbH