
Hepatocellular carcinoma
For patient information click here
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Dildar Hussain, MBBS [2], Mohamad Alkateb, MBBCh [3]
Synonyms and keywords: Hepatoma; Malignant hepatoma; Liver cancer; Malignant liver tumor; Primary liver cell carcinoma; Hepatic cancer
Overview
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1] Associate Editor(s)-in-Chief: Mohamad Alkateb, MBBCh [2]
Overview
Hepatocellular carcinoma (HCC, also called hepatoma) is a primary malignancy (cancer) of the liver. The majority of hepaticellular carcinoma cases are due to either a viral hepatitis infection (hepatitis B or C) or cirrhosis (alcoholism being the most common cause of hepatic cirrhosis). In countries where hepatitis is not endemic, most malignant cancers in the liver are not primary hepatocellular carcinoma and the majority of cases are metastasis from other part of the body, e.g. the colon. Treatment options of hepatocellular carcinoma and prognosis are dependent on many factors, especially on tumor size and staging.
In non-western countries, the usual outcome is poor, because only 10 – 20% of hepatocellular carcinomas can be removed completely using surgery. If the cancer cannot be completely removed, the disease is usually deadly within 3 to 6 months. This is partially due to late presentation with large tumours, but also due to the lack of medical expertise and facilities. This is a rare tumor in the United States.
Historical Perspective
Hepatocellular carcinoma was first noted to be associated with hepatitis B infection in 1970.
Pathophysiology
On microscopic histopathological analysis, large polygonal tumours cells with graunular eosinophilic cytoplasm or layered dense collagen bundles are characteristic findings of hepatocellular carcinoma.
Causes
Common causes of hepatocellular carcinoma include hepatitis B, hepatitis C, alcoholic liver cirrhosis, hemochromatosis, and hepatic porphyrias.
Differentiating Hepatocellular Carcinoma from other Diseases
Hepatocellular carcinoma must be differentiated from other diseases that cause abdominal pain, jaundice, and weight loss, such as hepatitis B, hepatitis C, liver cirrhosis, and pancreatitis.
Epidemiology and Demographics
Hepatocellular carcinoma is the 5th most common tumor worldwide. The epidemiology of hepatocellular carcinoma exhibits two main patterns, one in North America and Western Europe and another in non-Western countries, such as those in Sub-Saharan Africa, Central Asia and Southeast Asia, and the Amazon basin. Men are more affected than women and it is more common between the 3rd and 5th decades of life. Hepatocellular carcinoma causes 662,000 deaths worldwide per year.
Risk Factors
Common risk factors in the development of hepatocellular carcinoma are chronic hepatitis B, chronic hepatitis C, cirrhosis, and inherited metabolic diseases.
Screening
According to the American Association of Liver Diseases recommendations, screening for hepatocellular carcinoma by ultrasound (US) is recommended among patients with hepatitis B, hepatitis C, and cirrhosis. Screening is also recommended for Asian men over the age of 40, Asian women over the age of 50, and African American.
Natural History, Complications and Prognosis
The majority of hepatocellular carcinomas present with advanced disease because the symptoms tend to occur later in the course of the disease. Without treatment, the patient will develop symptoms of jaundice, ascites, right upper quadrant abdominal pain, nausea, and vomiting, which will eventually lead to death. There are a variety of complications associated with hepatocellular carcinoma such as jaundice, ascites, cachexia, and coagulopathy. Depending on the extent of the tumor at the time of diagnosis, the prognosis may vary. However, the prognosis is generally regarded as poor. If the cancer is inoperable, the disease is usually deadly within 3 to 6 months.
Diagnostic Studies
Staging
According to the TNM staging system, there are four stages of hepatocellular carcinoma based on the tumor size, lymph node involvement, and distant metastasis.
Diagnostic study of choice
Hepatocellular carcinoma is best diagnosed on a core biopsy of the liver. Core biopsy is done in a single visit at the hospital.
History and symptoms
The majority of patients with are asymptomatic hepatocellular carcinoma during the early stages of the disease. Symptoms of hepatocellular carcinoma include abdominal pain, nausea, vomiting, weakness, jaundice, pruritus, splenomegaly, fatigue, hematemesis, fever, and loss of appetite.
Physical examination
Patients with hepatocellular carcinoma usually appear cachectic. Physical examination of patients with hepatocellular carcinoma is usually remarkable for jaundice, pruritus, ascites, splenomegaly, esophageal varices, and cachexia.
Laboratory findings
An elevated concentration of serum alpha-fetoprotein (AFP) may be helpful in the diagnosis of hepatocellular carcinoma.
X-Ray
Performing chest x-ray might be helpful in detection of hepatocellular carcinoma metastasis to the lungs or to detect pleural effusion.
Abdominal CT
Abdominal CT scan with intravenous contrast agent is the best method to diagnose hepatocellular carcinoma.
Abdominal MRI
MRI may be helpful in the diagnosis of hepatocellular carcinoma.
Abdominal ultrasound
Ultrasound may be helpful in the diagnosis of hepatocellular carcinoma.
Other imaging studies
Hepatic angiography maybe helpful in the diagnosis of hepatocellular carcinoma. Hepatic angiography may show early opacification of the portal vein, filling defects in the hepatic venous system, and Portal vein tumor thrombus.
Other diagnostic studies
Other diagnostic studies for hepatocellular carcinoma include laparoscopy and biopsy.
Treatment
Medical therapy
Patients with hepatocellular carcinoma are treated with ethanol injections, transcatheter arterial chemoembolization (TACE), sealed source radiotherapy, radiofrequency ablation (RFA), intra-arterial iodine-131-lipiodol administration, high intensity focused ultrasound (HIFU), hormonal therapy, and chemotherapy.
Surgery
The feasibility of surgery depends on the stage of hepatocellular carcinoma at time of diagnosis.
Primary prevention
Hepatitis B vaccine is recommended for all children to prevent the development of hepatitis B, which is a major risk factor for hepatocellular carcinoma. Other primary pr evention strategies include abstinence from alcohol and screening for hemochromatosis.
References
Historical perspective
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1] Associate Editor(s)-in-Chief: Dildar Hussain, MBBS [2]
Overview
IN 1910 Eggel did a survey on literature from all over the world on hepatocellular carcinoma and demonstrated its gross anatomical classification. HCC was first noted to be associated with Hepatitis B infection in 1970. Kyoto University Japan, developed a technique to use the right lobe of the donor liver. Total of 48 adult HCC cases underwent transplant until April 2002 with good outcomes. The ongoing advancement in harvesting embryonic stem cells for tissue production strongly predicts that the liver transplantation may someday be replaced by stem cell therapy. A number of techniques have evolved for the use of in vitro and in vivo produced hepatocytes derived from stem cells for liver transplantation.
Historical Perspective
- In 1910 Eggel in Germany did a survey on literature from all over the world for hepatocellular carcinoma (HCC) autopsies out of which he discovered only 163 cases and demonstrated its gross anatomical classification. It was then speculated that the European numbers were far higher than those outside Europe.[1]
- In 1911, Yamagiwa suggested a new classification system based on the cell of origin and divided hepatobiliary cancers into hepatocellular cancer and cholangiocellular cancer, with the proposed terminology of hepatoma and cholangioma.[2][3]
- In 1951, Berman drew the world’s attention towards the extremely high incidence of HCC among young Mozambican males which was over 500 times more common in this population as among the northern European counterparts. Higginson followed up and studied the global epidemiology and confirmed Berman’s report.
- Edmondson with Peters and Simson, Steiner, Nakashima, unequivocally presented that there is a huge regional variation in pathology and that the HCC does not represent a single disease. Livers affected with HCC weighed more than 4 kg at autopsy among the South African blacks and less than 2 kg in the Japanese population.[4][5][6][7]
- Hepatocellular carcinoma was first noted to be associated with hepatitis B infection in 1970.[8]
- Okuda K, Fujimoto I, Hanai A and Urano Y published a study in Japan in 1987 describing the varying trends in the incidence of hepatocellular carcinoma in Japan stating the increase in HCC cases with chronic hepatitis C infection with cirrhosis were reported in majority compared to those with cirrhosis and hepatitis B infection.[9]
- In another study by Colombo et al published in 1991, it was noted that patients with liver cirrhosis belonging to western countries were at a substantial risk for hepatocellular carcinoma compared to the Asian population, with an annual incidence rate of 3 percent.[10]
- Data obtained from northern European countries was obtained, where the lancet used for smallpox vaccination was changed for every child in the distant past, it seemed that smallpox vaccination rather than intramuscular injection of vaccine was a significant iatrogenic factor for hepatitis C infection (HCV infection) and HCV-associated HCC in those countries where the same lancet was used repeatedly for vaccination.[3]
- In 1965 another study was done by the Japanese surgeons, pathologists, and radiologists recruiting patients from 829 participating institutes with more than 17,500 cases of primary liver malignancies. The data was compiled annually leading towards progress in the diagnosis and management of HCC. A broad clinical and pathologic study of small and early HCC was carried out by the Japanese hepatologists and radiologists and an early detection (screening) program was developed in which ultrasound and alpha-fetoprotein (AFP) measurement are carried out at regular intervals, which lead to an early detection international strategy for diagnosis and management of HCC.[11]
- Percutaneous ethanol injection (PEI) therapy and lipiodol-assisted chemoembolisation was adopted in Japan in 1983.
- Kyoto University Japan, developed a technique to use the right lobe of the donor liver. Total of 48 adult HCC cases underwent transplant until April 2002 with good outcomes.
- The ongoing advancement in harvesting embryonic stem cells for tissue production strongly predicts that the liver transplantation may someday be replaced by stem cell therapy. A number of techniques have evolved for the use of in vitro and in vivo produced hepatocytes derived from stem cells for liver transplantation.
References
- ↑ Eggel H, Ueber das prim&-e Carcinom der Leber. Beitr z path Ana z allg Path 1910;30:506-604
- ↑ Yamagiwa K. Zum Kenntniss des prim%ren parenchymatosen Leberkarzinoms (“Hepatoma”). Virchows Arch Path Anat 1911;203:75-131.
- ↑ 3.0 3.1 Okuda K (2002). “Hepatocellular carcinoma–history, current status and perspectives”. Dig Liver Dis. 34 (9): 613–6. PMID 12405244.
- ↑ Berman C. Primary carcinoma of the Liver. London: Higginson Lewis; 19.5 1.
- ↑ Okuda K, Peters RL, Simson IW. Gross anatomical features of hepatocellular carcinoma from three disparate geographic areas Proposal of new classification. Cancer 1984;54:2165-73.
- ↑ Steiner PE. Cancer of the liver and cirrhosis in trans-Saharan Africa and the United States of America. Cancer 1960;13:1085-166.
- ↑ Nakashima T, Okuda K, Kojiro M, Jimi A, Yamaguchi R, Sakamoto K, Ikari T (1983). “Pathology of hepatocellular carcinoma in Japan. 232 Consecutive cases autopsied in ten years”. Cancer. 51 (5): 863–77. PMID 6295617.
- ↑ Di Bisceglie AM (2009). “Hepatitis B and hepatocellular carcinoma”. Hepatology. 49 (5 Suppl): S56–60. doi:10.1002/hep.22962. PMC 3047495. PMID 19399807.
- ↑ Okuda K, Fujimoto I, Hanai A, Urano Y (1987). “Changing incidence of hepatocellular carcinoma in Japan”. Cancer Res. 47 (18): 4967–72. PMID 3040235.
- ↑ Colombo M, de Franchis R, Del Ninno E, Sangiovanni A, De Fazio C, Tommasini M, Donato MF, Piva A, Di Carlo V, Dioguardi N (1991). “Hepatocellular carcinoma in Italian patients with cirrhosis”. N. Engl. J. Med. 325 (10): 675–80. doi:10.1056/NEJM199109053251002. PMID 1651452.
- ↑ Okuda K, The Liver Cancer Study Group of Japan. Primary liver cancer in Japan. Cancer 1980;45:2663-9.
Classification
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Dildar Hussain, MBBS [2]
Overview
Hepatocellular carcinoma (HCC) may be classified into different histological subtypes based on the microscopic features. The TNM staging system is widely used for the staging of hepatocellular carcinoma, the Cancer of the Liver Italian Program (CLIP) system is used widely because it is adapted from the original Okuda classification system that takes cirrhosis into account.
Classification
Classification based on histological features
- Hepatocellular carcinoma may be classified into different histological subtypes based on the microscopic features:[1][2][3]
- Fibrolamellar carcinoma
- Sarcomatoid HCC
- Undifferentiated carcinoma
- Combined HCC-cholangiocarcinoma (HCC-CC)
- Lymphoepithelioma
- Scirrhous hepatocellular carcinoma (scirrhous HCC)
- Trabecular hepatocellular carcinoma
- Pseudoglandular hepatocellular carcinoma
- Acinar hepatocellular carcinoma
- Compact hepatocellular carcinoma
| Hepatocellular carcinoma | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Fibrolamellar carcinoma | Undifferentiated carcinoma | Sarcomatoid HCC | Combined HCC-CC* | Lymphoepithelioma | Scirrhous HCC | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Abbreviations: Combined HCC-cholangiocarcinoma (HCC-CC)*
Classification based on TNM staging
According to the TNM staging system, there are four stages of hepatocellular carcinoma based on the tumor size, lymph node involvement, and distant metastasis. Although the TNM staging system is widely used for the staging of hepatocellular carcinoma, the Cancer of the Liver Italian Program (CLIP) system is preferable because it is adopted from the original Okuda classification system that takes cirrhosis into account.
TNM staging system
According to the TNM staging system, there are four stages of hepatocellular carcinoma based on the tumor size, lymph node involvement, and distant metastasis.[4]
Primary tumor
| Primary tumor | Interpretation |
| TX | Primary tumor cannot be assessed |
| T0 | No evidence of primary tumor |
| T1 | A single tumor with no invasion into the blood vessels of the liver |
| T2 | A single tumor with invasion into the blood vessels or multiple tumors, none more than 5 cm in size |
| T3a | Multiple tumors, with any tumor larger than 5 cm |
| T3b | The tumor has grown into either the portal or hepatic vein |
| T4 | The tumor has grown into nearby organs (other than the gallbladder) or the tumor has grown into the layer of tissue that covers the organs in the abdomen (visceral peritoneum) |
Regional lymph node
| Lymph node involvement | Interpretation |
| NX | Regional lymph nodes cannot be assessed |
| N0 | No regional lymph node metastasis |
| N1 | Regional lymph node metastasis |
Distant metastasis
| M0 | No distant metastasis |
| M1 | Distant metastasis |
Clip and Okuda staging systems for hepatocellular carcinoma
Cancer of the Liver Italian Program (CLIP) system is used widely because it is adopted from the original Okuda classification system that takes cirrhosis into account.
CLIP Classification
| Variable | Points | ||
|---|---|---|---|
| 0 | 1 | 2 | |
| i.Tumor number (%) | Single | Multiple | – |
| Hepatic replacement by tumor | <50 | <50 | >50 |
| ii. Child-Pugh score | A | B | C |
| iii. α fetoprotein level (ng/mL) | <400 | ≥400 | – |
| iv.Portal vein thrombosis (CT) | No | Yes | – |
| CLIP stages (score = sum of points): CLIP 0, 0 points; CLIP 1, 1 point; CLIP 2, 2 points; CLIP 3, more than 3
points. | |||
OKUDA Classification
| OKUDA Classification | |||||||
| Tumor extenta | Bilirubin (mg/dL) | Albumin (g/L) | Ascites | ||||
| ≥50% | <50 | ≥ 3 | <3 | ≤3 | >3 | + | – |
| (+) | (−) | (+) | (−) | (+) | (−) | (+) | (−) |
| Okuda stages: stage 1, all (−); stage 2, 1 or 2 (+); stage 3, 3 or 4 (+) | |||||||
a. Liver span occupied by the tumor.
Adopted from Harrison’s Textbook of Medicine*
References
- ↑ Shafizadeh N, Kakar S (2013). “Hepatocellular Carcinoma: Histologic Subtypes”. Surg Pathol Clin. 6 (2): 367–84. doi:10.1016/j.path.2013.03.007. PMID 26838979.
- ↑ Matsuura S, Aishima S, Taguchi K, Asayama Y, Terashi T, Honda H, Tsuneyoshi M (2005). “‘Scirrhous’ type hepatocellular carcinomas: a special reference to expression of cytokeratin 7 and hepatocyte paraffin 1″. Histopathology. 47 (4): 382–90. doi:10.1111/j.1365-2559.2005.02230.x. PMID 16178893.
- ↑ Drebber, U.; Dienes, H. P. (2006). “Diagnose und Differenzialdiagnose des hepatozellulären Karzinoms”. Der Pathologe. 27 (4): 294–299. doi:10.1007/s00292-006-0842-1. ISSN 0172-8113.
- ↑ Canadian Cancer Society.http://www.cancer.ca/en/cancer-information/cancer-type/liver/staging/?region=ab
Pathophysiology
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]Associate Editor(s)-in-Chief: Dildar Hussain, MBBS [2]
Overview
The exact pathogenesis of hepatocellular carcinoma (HCC) is not fully understood. It is thought that HCC is mediated by either HBV infection, HCV infection, underlying cirrhotic liver disease, inflammation, necrosis, and fibrosis. On microscopic histopathological analysis, large polygonal tumor cells with granular eosinophilic cytoplasm or layered dense collagen bundles are characteristic findings of hepatocellular carcinoma.
Pathophysiology
Pathogenesis
- The exact pathogenesis of hepatocellular carcinoma is not fully understood. HCC arises from precancerous lesions and well-differentiated HCC further progresses to a less differentiated form. There is still an enormous demand for the explanation of objective morphological, phenotypic and genetic markers for the progression of HCC.
- It is thought that hepatocellular carcinoma is mediated by:[1][2]
- Chronic exposure of liver insult due to HBV infection, HCV infection, aflatoxin, nonalcoholic steatohepatitis (NASH) causes damage to the hepatocytes induces a vicious circle of destruction and regeneration of hepatocytes which finally causes the activation of stellate cells and hepatocyte senescence which contributes in the development of cirrhosis.
- As a result of the genomic instability the initiation of HCC occurs, step wise multiplication of different genetic events that lead to tumor progression and metastases include the following:
- Gene rearrangements
- Somatic mutations
- Copy number alterations
- Epigenetic changes
- Growth factor pathway alterations
- Molecular pathway alterations
- The major molecular events that occur in the pathogenesis of hepatocellular carcinoma include the following:[3][4][5][6][7][8][9][10][11][12][13][14][15][16][17][18][19][20][21][22][23][24][25][26][27][28][29][30][31][32][33][34][35][36][37][38][39][40][41][42][43][44][45][46][47][48][49][50][51][52][53][54]
| Major molecular events in the pathogenesis of HCC | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Genomic alterations | Epigenetic modifications | Growthfactor pathway alterations | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Gene Mutations | Gene Amplification | DNA methylation micro RNA | Micro RNA | LNC RNA | Major Signaling pathways | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| •TERT promoter •TP53 •CTNNB1 •AXIN1 •AXIN2 •ATM •RPS6KA3 •JAK1 •IL6R •IL6ST •ARID1 •ARID2 | •CCND1 •FGF19 •CDKNA2A •CDKNA2B •AXIN1 •IRF2 •MET | GSTP1 •E-cadherin •CDKNA2 •RASSF1A •SOCS3 •MIGMT | •MiR-155 •MiR-122 •MiR-224 •MiR-21 | •HULC •HEIH •Dreh •MVIH •HOTAIR •MDIG •LINE1 | •Wnt/β–catenin •Tyrosine kinase pathways EGF HGF/c-MET FGF VEGF •IGF •HIF1 •HIF2 •TGF β •Hedgehog | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
To review the pathogenesis of HBV infection, click here.
To review the pathogenesis of HCV infection click here.
To review the pathogenesis of hepatic cirrhosis, click here.
Genetics
- As of now there is no significant manifestation of an ordered cycle of genomic events leading to hepato-carcinogenesis. The pattern of genomic transformations exhibit huge variations often between two different HCCs from a single patient.
- Hepatocellular carcinoma is most commonly implicated with underlying chronic hepatitis and cirrhosis, however different genes have been associated with the pathogenesis of the HCC, which are further divided into four major groups:[2][24]
- Genes regulating DNA damage response
- Genes involved in cell cycle control
- Genes involved in growth inhibition and apoptosis
- Genes responsible for cell to cell interaction and signal transduction
- Genes involved in the pathogenesis of hepatocellular carcinoma include:
Associated Conditions
The associated conditions with hepatocellular carcinoma are
- HBV infection
- HCV infection
- Underlying cirrhotic liver disease
- Inflammation
- Necrosis and fibrosis of the liver
Microscopic Pathology
- On microscopic histopathological analysis, large polygonal tumor cells with granular eosinophilic cytoplasm or layered dense collagen bundles are characteristic findings of hepatocellular carcinoma.
Gross Pathology
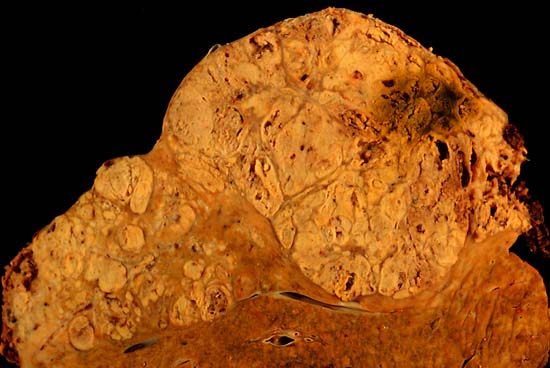
On gross pathology, hepatocellular carcinoma has the following characteristic findings:[55]
- Nodular or diffusely infiltrative.
- The nodular type may be unifocal (large mass) or multifocal (when developed as a complication of cirrhosis). Tumor nodules are round to oval, grey or green (if the tumor produces bile), well circumscribed but not encapsulated.
- In about fifty percent of the cases, the tumors are multifocal where as some authors have suggested it to be around 75 percent.
- The portal vein is infiltrated by the poorly circumcised diffused type and the hepatic veins are rarely infiltrated.
- Pale in relation to surrounding liver or green (due to bile secretion)
-
 Hepatocelluler carcinoma. The image shows a longitudinal slice taken through the full length of the liver.
Hepatocelluler carcinoma. The image shows a longitudinal slice taken through the full length of the liver.
(Courtesy of Ed Uthman, MD) -
 The tumor is at the top, cirrhotic liver at the bottom, and a fibrous reaction in between. Hepatocellular carcinomas can have a variety of gross patterns, including multinodular / multifocal, such as this one.
The tumor is at the top, cirrhotic liver at the bottom, and a fibrous reaction in between. Hepatocellular carcinomas can have a variety of gross patterns, including multinodular / multifocal, such as this one.
(Courtesy of Ed Uthman, MD)


Microscopic Pathology
On microscopic histopathological analysis, hepatocellular carcinoma has the following characteristic findings:
- Large polygonal tumor cells with:
- Granular eosinophilic cytoplasm
- Low NC ratio
- Layered dense collagen bundles [56]
Videos
{{#ev:youtube|qsR92joabBg}}
References
- ↑ Röcken C, Carl-McGrath S (2001). “Pathology and pathogenesis of hepatocellular carcinoma”. Dig Dis. 19 (4): 269–78. doi:10.1159/000050693. PMID 11935086.
- ↑ 2.0 2.1 Dhanasekaran R, Bandoh S, Roberts LR (2016). “Molecular pathogenesis of hepatocellular carcinoma and impact of therapeutic advances”. F1000Res. 5. doi:10.12688/f1000research.6946.1. PMC 4870992. PMID 27239288.
- ↑ Killela PJ, Reitman ZJ, Jiao Y, Bettegowda C, Agrawal N, Diaz LA, Friedman AH, Friedman H, Gallia GL, Giovanella BC, Grollman AP, He TC, He Y, Hruban RH, Jallo GI, Mandahl N, Meeker AK, Mertens F, Netto GJ, Rasheed BA, Riggins GJ, Rosenquist TA, Schiffman M, Shih I, Theodorescu D, Torbenson MS, Velculescu VE, Wang TL, Wentzensen N, Wood LD, Zhang M, McLendon RE, Bigner DD, Kinzler KW, Vogelstein B, Papadopoulos N, Yan H (2013). “TERT promoter mutations occur frequently in gliomas and a subset of tumors derived from cells with low rates of self-renewal”. Proc. Natl. Acad. Sci. U.S.A. 110 (15): 6021–6. doi:10.1073/pnas.1303607110. PMC 3625331. PMID 23530248. Vancouver style error: initials (help)
- ↑ Nault JC, Mallet M, Pilati C, Calderaro J, Bioulac-Sage P, Laurent C, Laurent A, Cherqui D, Balabaud C, Zucman-Rossi J, Zucman Rossi J (2013). “High frequency of telomerase reverse-transcriptase promoter somatic mutations in hepatocellular carcinoma and preneoplastic lesions”. Nat Commun. 4: 2218. doi:10.1038/ncomms3218. PMC 3731665. PMID 23887712.
- ↑ Chen YL, Jeng YM, Chang CN, Lee HJ, Hsu HC, Lai PL, Yuan RH (2014). “TERT promoter mutation in resectable hepatocellular carcinomas: a strong association with hepatitis C infection and absence of hepatitis B infection”. Int J Surg. 12 (7): 659–65. doi:10.1016/j.ijsu.2014.05.066. PMID 24866078.
- ↑ Schulze K, Imbeaud S, Letouzé E, Alexandrov LB, Calderaro J, Rebouissou S, Couchy G, Meiller C, Shinde J, Soysouvanh F, Calatayud AL, Pinyol R, Pelletier L, Balabaud C, Laurent A, Blanc JF, Mazzaferro V, Calvo F, Villanueva A, Nault JC, Bioulac-Sage P, Stratton MR, Llovet JM, Zucman-Rossi J (2015). “Exome sequencing of hepatocellular carcinomas identifies new mutational signatures and potential therapeutic targets”. Nat. Genet. 47 (5): 505–511. doi:10.1038/ng.3252. PMC 4587544. PMID 25822088.
- ↑ Totoki Y, Tatsuno K, Covington KR, Ueda H, Creighton CJ, Kato M, Tsuji S, Donehower LA, Slagle BL, Nakamura H, Yamamoto S, Shinbrot E, Hama N, Lehmkuhl M, Hosoda F, Arai Y, Walker K, Dahdouli M, Gotoh K, Nagae G, Gingras MC, Muzny DM, Ojima H, Shimada K, Midorikawa Y, Goss JA, Cotton R, Hayashi A, Shibahara J, Ishikawa S, Guiteau J, Tanaka M, Urushidate T, Ohashi S, Okada N, Doddapaneni H, Wang M, Zhu Y, Dinh H, Okusaka T, Kokudo N, Kosuge T, Takayama T, Fukayama M, Gibbs RA, Wheeler DA, Aburatani H, Shibata T (2014). “Trans-ancestry mutational landscape of hepatocellular carcinoma genomes”. Nat. Genet. 46 (12): 1267–73. doi:10.1038/ng.3126. PMID 25362482.
- ↑ Cleary SP, Jeck WR, Zhao X, Chen K, Selitsky SR, Savich GL, Tan TX, Wu MC, Getz G, Lawrence MS, Parker JS, Li J, Powers S, Kim H, Fischer S, Guindi M, Ghanekar A, Chiang DY (2013). “Identification of driver genes in hepatocellular carcinoma by exome sequencing”. Hepatology. 58 (5): 1693–702. doi:10.1002/hep.26540. PMC 3830584. PMID 23728943.
- ↑ Hussain SP, Schwank J, Staib F, Wang XW, Harris CC (2007). “TP53 mutations and hepatocellular carcinoma: insights into the etiology and pathogenesis of liver cancer”. Oncogene. 26 (15): 2166–76. doi:10.1038/sj.onc.1210279. PMID 17401425.
- ↑ Guichard C, Amaddeo G, Imbeaud S, Ladeiro Y, Pelletier L, Maad IB, Calderaro J, Bioulac-Sage P, Letexier M, Degos F, Clément B, Balabaud C, Chevet E, Laurent A, Couchy G, Letouzé E, Calvo F, Zucman-Rossi J (2012). “Integrated analysis of somatic mutations and focal copy-number changes identifies key genes and pathways in hepatocellular carcinoma”. Nat. Genet. 44 (6): 694–8. doi:10.1038/ng.2256. PMC 3819251. PMID 22561517.
- ↑ Kan Z, Zheng H, Liu X, Li S, Barber TD, Gong Z, Gao H, Hao K, Willard MD, Xu J, Hauptschein R, Rejto PA, Fernandez J, Wang G, Zhang Q, Wang B, Chen R, Wang J, Lee NP, Zhou W, Lin Z, Peng Z, Yi K, Chen S, Li L, Fan X, Yang J, Ye R, Ju J, Wang K, Estrella H, Deng S, Wei P, Qiu M, Wulur IH, Liu J, Ehsani ME, Zhang C, Loboda A, Sung WK, Aggarwal A, Poon RT, Fan ST, Wang J, Hardwick J, Reinhard C, Dai H, Li Y, Luk JM, Mao M (2013). “Whole-genome sequencing identifies recurrent mutations in hepatocellular carcinoma”. Genome Res. 23 (9): 1422–33. doi:10.1101/gr.154492.113. PMC 3759719. PMID 23788652.
- ↑ Ozturk M (1991). “p53 mutation in hepatocellular carcinoma after aflatoxin exposure”. Lancet. 338 (8779): 1356–9. PMID 1682737.
- ↑ Madden CR, Finegold MJ, Slagle BL (2002). “Altered DNA mutation spectrum in aflatoxin b1-treated transgenic mice that express the hepatitis B virus x protein”. J. Virol. 76 (22): 11770–4. PMC 136763. PMID 12388740.
- ↑ Villanueva A, Llovet JM (2014). “Liver cancer in 2013: Mutational landscape of HCC–the end of the beginning”. Nat Rev Clin Oncol. 11 (2): 73–4. doi:10.1038/nrclinonc.2013.243. PMID 24395088.
- ↑ Wang K, Lim HY, Shi S, Lee J, Deng S, Xie T, Zhu Z, Wang Y, Pocalyko D, Yang WJ, Rejto PA, Mao M, Park CK, Xu J (2013). “Genomic landscape of copy number aberrations enables the identification of oncogenic drivers in hepatocellular carcinoma”. Hepatology. 58 (2): 706–17. doi:10.1002/hep.26402. PMID 23505090.
- ↑ Su PF, Lee TC, Lin PJ, Lee PH, Jeng YM, Chen CH, Liang JD, Chiou LL, Huang GT, Lee HS (2007). “Differential DNA methylation associated with hepatitis B virus infection in hepatocellular carcinoma”. Int. J. Cancer. 121 (6): 1257–64. doi:10.1002/ijc.22849. PMID 17534893.
- ↑ Wong IH, Lo YM, Zhang J, Liew CT, Ng MH, Wong N, Lai PB, Lau WY, Hjelm NM, Johnson PJ (1999). “Detection of aberrant p16 methylation in the plasma and serum of liver cancer patients”. Cancer Res. 59 (1): 71–3. PMID 9892188.
- ↑ Zhang YJ, Ahsan H, Chen Y, Lunn RM, Wang LY, Chen SY, Lee PH, Chen CJ, Santella RM (2002). “High frequency of promoter hypermethylation of RASSF1A and p16 and its relationship to aflatoxin B1-DNA adduct levels in human hepatocellular carcinoma”. Mol. Carcinog. 35 (2): 85–92. doi:10.1002/mc.10076. PMID 12325038.
- ↑ Zhong S, Tang MW, Yeo W, Liu C, Lo YM, Johnson PJ (2002). “Silencing of GSTP1 gene by CpG island DNA hypermethylation in HBV-associated hepatocellular carcinomas”. Clin. Cancer Res. 8 (4): 1087–92. PMID 11948118.
- ↑ Bakker J, Lin X, Nelson WG (2002). “Methyl-CpG binding domain protein 2 represses transcription from hypermethylated pi-class glutathione S-transferase gene promoters in hepatocellular carcinoma cells”. J. Biol. Chem. 277 (25): 22573–80. doi:10.1074/jbc.M203009200. PMID 11960994.
- ↑ Niwa Y, Kanda H, Shikauchi Y, Saiura A, Matsubara K, Kitagawa T, Yamamoto J, Kubo T, Yoshikawa H (2005). “Methylation silencing of SOCS-3 promotes cell growth and migration by enhancing JAK/STAT and FAK signalings in human hepatocellular carcinoma”. Oncogene. 24 (42): 6406–17. doi:10.1038/sj.onc.1208788. PMID 16007195.
- ↑ Zhang YJ, Chen Y, Ahsan H, Lunn RM, Lee PH, Chen CJ, Santella RM (2003). “Inactivation of the DNA repair gene O6-methylguanine-DNA methyltransferase by promoter hypermethylation and its relationship to aflatoxin B1-DNA adducts and p53 mutation in hepatocellular carcinoma”. Int. J. Cancer. 103 (4): 440–4. doi:10.1002/ijc.10852. PMID 12478658.
- ↑ Fujimoto A, Totoki Y, Abe T, Boroevich KA, Hosoda F, Nguyen HH, Aoki M, Hosono N, Kubo M, Miya F, Arai Y, Takahashi H, Shirakihara T, Nagasaki M, Shibuya T, Nakano K, Watanabe-Makino K, Tanaka H, Nakamura H, Kusuda J, Ojima H, Shimada K, Okusaka T, Ueno M, Shigekawa Y, Kawakami Y, Arihiro K, Ohdan H, Gotoh K, Ishikawa O, Ariizumi S, Yamamoto M, Yamada T, Chayama K, Kosuge T, Yamaue H, Kamatani N, Miyano S, Nakagama H, Nakamura Y, Tsunoda T, Shibata T, Nakagawa H (2012). “Whole-genome sequencing of liver cancers identifies etiological influences on mutation patterns and recurrent mutations in chromatin regulators”. Nat. Genet. 44 (7): 760–4. doi:10.1038/ng.2291. PMID 22634756.
- ↑ 24.0 24.1 Li M, Zhao H, Zhang X, Wood LD, Anders RA, Choti MA, Pawlik TM, Daniel HD, Kannangai R, Offerhaus GJ, Velculescu VE, Wang L, Zhou S, Vogelstein B, Hruban RH, Papadopoulos N, Cai J, Torbenson MS, Kinzler KW (2011). “Inactivating mutations of the chromatin remodeling gene ARID2 in hepatocellular carcinoma”. Nat. Genet. 43 (9): 828–9. doi:10.1038/ng.903. PMC 3163746. PMID 21822264.
- ↑ Xu J, Zhu X, Wu L, Yang R, Yang Z, Wang Q, Wu F (2012). “MicroRNA-122 suppresses cell proliferation and induces cell apoptosis in hepatocellular carcinoma by directly targeting Wnt/β-catenin pathway”. Liver Int. 32 (5): 752–60. doi:10.1111/j.1478-3231.2011.02750.x. PMID 22276989.
- ↑ Tsai WC, Hsu PW, Lai TC, Chau GY, Lin CW, Chen CM, Lin CD, Liao YL, Wang JL, Chau YP, Hsu MT, Hsiao M, Huang HD, Tsou AP (2009). “MicroRNA-122, a tumor suppressor microRNA that regulates intrahepatic metastasis of hepatocellular carcinoma”. Hepatology. 49 (5): 1571–82. doi:10.1002/hep.22806. PMID 19296470.
- ↑ Fornari F, Gramantieri L, Giovannini C, Veronese A, Ferracin M, Sabbioni S, Calin GA, Grazi GL, Croce CM, Tavolari S, Chieco P, Negrini M, Bolondi L (2009). “MiR-122/cyclin G1 interaction modulates p53 activity and affects doxorubicin sensitivity of human hepatocarcinoma cells”. Cancer Res. 69 (14): 5761–7. doi:10.1158/0008-5472.CAN-08-4797. PMID 19584283.
- ↑ Wang Y, Lee CG (2011). “Role of miR-224 in hepatocellular carcinoma: a tool for possible therapeutic intervention?”. Epigenomics. 3 (2): 235–43. doi:10.2217/epi.11.5. PMID 22122284.
- ↑ Wang Y, Ren J, Gao Y, Ma JZ, Toh HC, Chow P, Chung AY, Ooi LL, Lee CG (2013). “MicroRNA-224 targets SMAD family member 4 to promote cell proliferation and negatively influence patient survival”. PLoS ONE. 8 (7): e68744. doi:10.1371/journal.pone.0068744. PMC 3726696. PMID 23922662.
- ↑ Sun J, Lu H, Wang X, Jin H (2013). “MicroRNAs in hepatocellular carcinoma: regulation, function, and clinical implications”. ScientificWorldJournal. 2013: 924206. doi:10.1155/2013/924206. PMC 3575633. PMID 23431261.
- ↑ Du Y, Kong G, You X, Zhang S, Zhang T, Gao Y, Ye L, Zhang X (2012). “Elevation of highly up-regulated in liver cancer (HULC) by hepatitis B virus X protein promotes hepatoma cell proliferation via down-regulating p18”. J. Biol. Chem. 287 (31): 26302–11. doi:10.1074/jbc.M112.342113. PMC 3406714. PMID 22685290.
- ↑ Xie H, Ma H, Zhou D (2013). “Plasma HULC as a promising novel biomarker for the detection of hepatocellular carcinoma”. Biomed Res Int. 2013: 136106. doi:10.1155/2013/136106. PMC 3674644. PMID 23762823.
- ↑ Yang F, Zhang L, Huo XS, Yuan JH, Xu D, Yuan SX, Zhu N, Zhou WP, Yang GS, Wang YZ, Shang JL, Gao CF, Zhang FR, Wang F, Sun SH (2011). “Long noncoding RNA high expression in hepatocellular carcinoma facilitates tumor growth through enhancer of zeste homolog 2 in humans”. Hepatology. 54 (5): 1679–89. doi:10.1002/hep.24563. PMID 21769904.
- ↑ Huang JF, Guo YJ, Zhao CX, Yuan SX, Wang Y, Tang GN, Zhou WP, Sun SH (2013). “Hepatitis B virus X protein (HBx)-related long noncoding RNA (lncRNA) down-regulated expression by HBx (Dreh) inhibits hepatocellular carcinoma metastasis by targeting the intermediate filament protein vimentin”. Hepatology. 57 (5): 1882–92. doi:10.1002/hep.26195. PMID 23239537.
- ↑ Yuan SX, Yang F, Yang Y, Tao QF, Zhang J, Huang G, Yang Y, Wang RY, Yang S, Huo XS, Zhang L, Wang F, Sun SH, Zhou WP (2012). “Long noncoding RNA associated with microvascular invasion in hepatocellular carcinoma promotes angiogenesis and serves as a predictor for hepatocellular carcinoma patients’ poor recurrence-free survival after hepatectomy”. Hepatology. 56 (6): 2231–41. doi:10.1002/hep.25895. PMID 22706893.
- ↑ Lay AJ, Jiang XM, Kisker O, Flynn E, Underwood A, Condron R, Hogg PJ (2000). “Phosphoglycerate kinase acts in tumour angiogenesis as a disulphide reductase”. Nature. 408 (6814): 869–73. doi:10.1038/35048596. PMID 11130727.
- ↑ Yang Z, Zhou L, Wu LM, Lai MC, Xie HY, Zhang F, Zheng SS (2011). “Overexpression of long non-coding RNA HOTAIR predicts tumor recurrence in hepatocellular carcinoma patients following liver transplantation”. Ann. Surg. Oncol. 18 (5): 1243–50. doi:10.1245/s10434-011-1581-y. PMID 21327457.
- ↑ Geng YJ, Xie SL, Li Q, Ma J, Wang GY (2011). “Large intervening non-coding RNA HOTAIR is associated with hepatocellular carcinoma progression”. J. Int. Med. Res. 39 (6): 2119–28. doi:10.1177/147323001103900608. PMID 22289527.
- ↑ Li G, Zhang H, Wan X, Yang X, Zhu C, Wang A, He L, Miao R, Chen S, Zhao H (2014). “Long noncoding RNA plays a key role in metastasis and prognosis of hepatocellular carcinoma”. Biomed Res Int. 2014: 780521. doi:10.1155/2014/780521. PMC 3976793. PMID 24757675.
- ↑ Lau CC, Sun T, Ching AK, He M, Li JW, Wong AM, Co NN, Chan AW, Li PS, Lung RW, Tong JH, Lai PB, Chan HL, To KF, Chan TF, Wong N (2014). “Viral-human chimeric transcript predisposes risk to liver cancer development and progression”. Cancer Cell. 25 (3): 335–49. doi:10.1016/j.ccr.2014.01.030. PMID 24582836.
- ↑ Thompson MD, Monga SP (2007). “WNT/beta-catenin signaling in liver health and disease”. Hepatology. 45 (5): 1298–305. doi:10.1002/hep.21651. PMID 17464972.
- ↑ Hoshida Y, Nijman SM, Kobayashi M, Chan JA, Brunet JP, Chiang DY, Villanueva A, Newell P, Ikeda K, Hashimoto M, Watanabe G, Gabriel S, Friedman SL, Kumada H, Llovet JM, Golub TR (2009). “Integrative transcriptome analysis reveals common molecular subclasses of human hepatocellular carcinoma”. Cancer Res. 69 (18): 7385–92. doi:10.1158/0008-5472.CAN-09-1089. PMC 3549578. PMID 19723656.
- ↑ Tanabe KK, Lemoine A, Finkelstein DM, Kawasaki H, Fujii T, Chung RT, Lauwers GY, Kulu Y, Muzikansky A, Kuruppu D, Lanuti M, Goodwin JM, Azoulay D, Fuchs BC (2008). “Epidermal growth factor gene functional polymorphism and the risk of hepatocellular carcinoma in patients with cirrhosis”. JAMA. 299 (1): 53–60. doi:10.1001/jama.2007.65. PMID 18167406.
- ↑ Kaposi-Novak P, Lee JS, Gòmez-Quiroz L, Coulouarn C, Factor VM, Thorgeirsson SS (2006). “Met-regulated expression signature defines a subset of human hepatocellular carcinomas with poor prognosis and aggressive phenotype”. J. Clin. Invest. 116 (6): 1582–95. doi:10.1172/JCI27236. PMC 1462944. PMID 16710476.
- ↑ Llovet JM, Peña CE, Lathia CD, Shan M, Meinhardt G, Bruix J (2012). “Plasma biomarkers as predictors of outcome in patients with advanced hepatocellular carcinoma”. Clin. Cancer Res. 18 (8): 2290–300. doi:10.1158/1078-0432.CCR-11-2175. PMID 22374331.
- ↑ French DM, Lin BC, Wang M, Adams C, Shek T, Hötzel K, Bolon B, Ferrando R, Blackmore C, Schroeder K, Rodriguez LA, Hristopoulos M, Venook R, Ashkenazi A, Desnoyers LR (2012). “Targeting FGFR4 inhibits hepatocellular carcinoma in preclinical mouse models”. PLoS ONE. 7 (5): e36713. doi:10.1371/journal.pone.0036713. PMC 3352934. PMID 22615798.
- ↑ Desnoyers LR, Pai R, Ferrando RE, Hötzel K, Le T, Ross J, Carano R, D’Souza A, Qing J, Mohtashemi I, Ashkenazi A, French DM (2008). “Targeting FGF19 inhibits tumor growth in colon cancer xenograft and FGF19 transgenic hepatocellular carcinoma models”. Oncogene. 27 (1): 85–97. doi:10.1038/sj.onc.1210623. PMID 17599042.
- ↑ Yoshiji H, Kuriyama S, Noguchi R, Yoshii J, Ikenaka Y, Yanase K, Namisaki T, Kitade M, Uemura M, Masaki T, Fukui H (2005). “Angiopoietin 2 displays a vascular endothelial growth factor dependent synergistic effect in hepatocellular carcinoma development in mice”. Gut. 54 (12): 1768–75. doi:10.1136/gut.2005.067900. PMC 1774778. PMID 16033879.
- ↑ Park YN, Kim YB, Yang KM, Park C (2000). “Increased expression of vascular endothelial growth factor and angiogenesis in the early stage of multistep hepatocarcinogenesis”. Arch. Pathol. Lab. Med. 124 (7): 1061–5. doi:10.1043/0003-9985(2000)124<1061:IEOVEG>2.0.CO;2. PMID 10888784.
- ↑ Kim KW, Bae SK, Lee OH, Bae MH, Lee MJ, Park BC (1998). “Insulin-like growth factor II induced by hypoxia may contribute to angiogenesis of human hepatocellular carcinoma”. Cancer Res. 58 (2): 348–51. PMID 9443416.
- ↑ Cannito S, Turato C, Paternostro C, Biasiolo A, Colombatto S, Cambieri I, Quarta S, Novo E, Morello E, Villano G, Fasolato S, Musso T, David E, Tusa I, Rovida E, Autelli R, Smedile A, Cillo U, Pontisso P, Parola M (2015). “Hypoxia up-regulates SERPINB3 through HIF-2α in human liver cancer cells”. Oncotarget. 6 (4): 2206–21. doi:10.18632/oncotarget.2943. PMC 4385846. PMID 25544768.
- ↑ Luo D, Wang Z, Wu J, Jiang C, Wu J (2014). “The role of hypoxia inducible factor-1 in hepatocellular carcinoma”. Biomed Res Int. 2014: 409272. doi:10.1155/2014/409272. PMC 4101982. PMID 25101278.
- ↑ Coulouarn C, Factor VM, Thorgeirsson SS (2008). “Transforming growth factor-beta gene expression signature in mouse hepatocytes predicts clinical outcome in human cancer”. Hepatology. 47 (6): 2059–67. doi:10.1002/hep.22283. PMC 2762280. PMID 18506891.
- ↑ Giannelli G, Bergamini C, Fransvea E, Sgarra C, Antonaci S (2005). “Laminin-5 with transforming growth factor-beta1 induces epithelial to mesenchymal transition in hepatocellular carcinoma”. Gastroenterology. 129 (5): 1375–83. doi:10.1053/j.gastro.2005.09.055. PMID 16285938.
- ↑ Reynolds AR, Furlan A, Fetzer DT, Sasatomi E, Borhani AA, Heller MT, Tublin ME (2015). “Infiltrative hepatocellular carcinoma: what radiologists need to know”. Radiographics. 35 (2): 371–86. doi:10.1148/rg.352140114. PMID 25763723.
- ↑ “Hepatocellular carcinoma”.
Causes
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1] Associate Editor(s)-in-Chief: Dildar Hussain, MBBS [2] Mohamad Alkateb, MBBCh [3]
Overview
Common causes of hepatocellular carcinoma include hepatitis B, hepatitis C, alcoholic liver cirrhosis, hemochromatosis, and hepatic porphyrias. Other causes include non alcholic fatty liver disease, non-alchoholic steatohepatitis, and metabolic disorders as diabetes mellitus type two and obesity.
Common Causes
Common causes of hepatocellular carcinoma include the following:[1][2][3][4][5][6][7]
- Hepatitis B
- Hepatitis C
- Liver cirrhosis
- Aflatoxins
- Hemochromatosis
- Hepatic porphyrias (acute intermittent porphyria, porphyria cutanea tarda, hereditary coproporphyria, and variegate porphyria)
- Tyrosinemia type 1
Less common causes
Less common causes of hepatocellular carcinoma include the following:[8][9][10]
- Non alcholic fatty liver disease(NAFLD)
- Non alchoholic steatohepatitis(NASH)
- Metabolic disorders:
- Gut microbiota[11]
Drugs
The carcinogenic drugs for hepatocellular carcinoma are:
References
- ↑ Jiang, Kun; Centeno, Barbara A. (2018). “Primary Liver Cancers, Part 2”. Cancer Control. 25 (1): 107327481774465. doi:10.1177/1073274817744658. ISSN 1073-2748.
- ↑ Said, Adnan; Ghufran, Aiman (2017). “Epidemic of non-alcoholic fatty liver disease and hepatocellular carcinoma”. World Journal of Clinical Oncology. 8 (6): 429–436. doi:10.5306/wjco.v8.i6.429. ISSN 2218-4333.
- ↑ Erkekoglu P, Oral D, Chao MW, Kocer-Gumusel B (2017). “Hepatocellular Carcinoma and Possible Chemical and Biological Causes: A Review”. J. Environ. Pathol. Toxicol. Oncol. 36 (2): 171–190. doi:10.1615/JEnvironPatholToxicolOncol.2017020927. PMID 29199597.
- ↑ Fu, Jing; Wang, Hongyang (2018). “Precision diagnosis and treatment of liver cancer in China”. Cancer Letters. 412: 283–288. doi:10.1016/j.canlet.2017.10.008. ISSN 0304-3835.
- ↑ Fujiwara N, Friedman SL, Goossens N, Hoshida Y (2017). “Risk factors and prevention of hepatocellular carcinoma in the era of precision medicine”. J. Hepatol. doi:10.1016/j.jhep.2017.09.016. PMID 28989095.
- ↑ Parkin, Donald Maxwell (2006). “The global health burden of infection-associated cancers in the year 2002”. International Journal of Cancer. 118 (12): 3030–3044. doi:10.1002/ijc.21731. ISSN 0020-7136.
- ↑ Shi, J; Zhu, L; Liu, S; Xie, W-f (2005). “A meta-analysis of case–control studies on the combined effect of hepatitis B and C virus infections in causing hepatocellular carcinoma in China”. British Journal of Cancer. 92 (3): 607–612. doi:10.1038/sj.bjc.6602333. ISSN 0007-0920.
- ↑ Agosti, Pasquale; Sabbà, Carlo; Mazzocca, Antonio (2018). “Emerging metabolic risk factors in hepatocellular carcinoma and their influence on the liver microenvironment”. Biochimica et Biophysica Acta (BBA) – Molecular Basis of Disease. 1864 (2): 607–617. doi:10.1016/j.bbadis.2017.11.026. ISSN 0925-4439.
- ↑ Gerbes A, Zoulim F, Tilg H, Dufour JF, Bruix J, Paradis V, Salem R, Peck-Radosavljevic M, Galle PR, Greten TF, Nault JC, Avila MA (2018). “Gut roundtable meeting paper: selected recent advances in hepatocellular carcinoma”. Gut. 67 (2): 380–388. doi:10.1136/gutjnl-2017-315068. PMID 29150490.
- ↑ Didi-Kouko Coulibaly J, Yeboua M, Kouassi Mbengue A, Kouadio EA, Anzouan-Kacou Kissi H, Binan AY, Lohoues Kouacou MJ, Attia A, N’Drin DY, Toutou T, Adoubi I, Pineau P (2017). “Evolution of hepatocellular carcinoma epidemiology in Côte d’Ivoire”. Bull Cancer. 104 (11): 937–945. doi:10.1016/j.bulcan.2017.09.010. PMID 29128083.
- ↑ Sanduzzi Zamparelli M, Rocco A, Compare D, Nardone G (2017). “The gut microbiota: A new potential driving force in liver cirrhosis and hepatocellular carcinoma”. United European Gastroenterol J. 5 (7): 944–953. doi:10.1177/2050640617705576. PMC 5676553. PMID 29163959.
Differentiating Hepatocellular carcinoma from other Diseases
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1] Associate Editor(s)-in-Chief: Dildar Hussain, MBBS [2]
Overview
Hepatocellular carcinoma must be differentiated from other diseases that cause abdominal pain, jaundice, and weight loss, such as liver cirrhosis and pancreatitis.
Differentiating Hepatocellular Carcinoma from other Diseases
Hepatocellular carcinoma must be differentiated from the following diseases:[1][2][3][4][5][6][7][8][9][10]
- Angiomyolipoma[11][12][13]
- Adenoma
- Borderline (high-grade dysplastic) nodule
- Cholangiocarcinoma[14][15][16][17]
- Confluent fibrosis[18][19][20][21][22][23][24]
- Focal nodular hyperplasia[25][26][27][28]
- Focal fat sparing and deposit on liver[29][30][[#cite_note-NicolauBr�2004-31|[31]]][32][33]
- Gallbladder cancer
- Hereditary hemorrhagic telangiectasia[34][35][36][37][38]
- Inflammatory pseudotumors[39][40][41][42]
- Liver hemangioma[43][44][45][46][47][48][49][49][50][51][52][53]
- Hepatoblastoma in children
- Inflammatory lesions[54][55][46][56][57]
- Mesenchymal hamartoma in children[58][59]
- Multiacinar regenerative nodule
- Macroregenerative nodule (low-grade dysplastic nodule)[60]
- Nontumorous arterioportal shunts
- Pseudomass in chronic portal vein thrombosis
- Pyogenic liver abscesses
- Pancreatic cancer
- Stomach cancer
Abbreviations: RUQ= Right upper quadrant of the abdomen, LUQ= Left upper quadrant, LLQ= Left lower quadrant, RLQ= Right lower quadrant, LFT= Liver function test, SIRS= Systemic inflammatory response syndrome, ERCP= Endoscopic retrograde cholangiopancreatography, IV= Intravenous, N= Normal, AMA= Anti mitochondrial antibodies, LDH= Lactate dehydrogenase, GI= Gastrointestinal, CXR= Chest X ray, IgA= Immunoglobulin A, IgG= Immunoglobulin G, IgM= Immunoglobulin M, CT= Computed tomography, PMN= Polymorphonuclear cells, ESR= Erythrocyte sedimentation rate, CRP= C-reactive protein, TS= Transferrin saturation, SF= Serum Ferritin, SMA= Superior mesenteric artery, SMV= Superior mesenteric vein, ECG= Electrocardiogram
| Disease | Clinical manifestations | Diagnosis | Comments | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Symptoms | Signs | |||||||||||||||
| Abdominal Pain | Fever | Rigors and chills | Nausea or vomiting | Jaundice | Constipation | Diarrhea | Weight loss | GI bleeding | Hypo-
tension |
Guarding | Rebound Tenderness | Bowel sounds | Lab Findings | Imaging | ||
| Hepatocellular carcinoma/Metastasis | RUQ | + | − | + | + | + | + | + | + | + | − | + |
|
|
Other symptoms: | |
| Cholangiocarcinoma | RUQ | + | − | + | + | − | − | + | − | − | − | + | Normal |
|
| |
| Pancreatic carcinoma | MidEpigastric | − | − | + | + | + | − | + | − | − | − | + | Normal |
Skin manifestations may include: | ||
| Focal nodular hyperplasia | Diffuse | ± | − | − | ± | − | − | + | + | − | − | − | Normal |
|
|
|
| Disease | Abdominal Pain | Fever | Rigors and chills | Nausea or vomiting | Jaundice | Constipation | Diarrhea | Weight loss | GI bleeding | Hypo-
tension |
Guarding | Rebound Tenderness | Bowel sounds | Lab Findings | Imaging | Comments |
| Gallbladder cancer | Midepigastric | − | − | + | + | − | + | + | − | − | − | − | Normal |
|
||
| Liver hemangioma | Intermittent RUQ | − | − | + | + | − | − | − | − | − | − | − | Normal |
|
| |
| Liver abscess | RUQ | + | − | + | + | − | − | + | − | − | − | − | Normal |
|
|
|
| Cirrhosis | RUQ+Bloating | + | − | + | + | − | − | + | − | − | − | − | Normal |
|
US
|
|
| Inflammatory lesions | RUQ | ± | − | + | + | − | − | − | − | − | − | − | Normal |
|
US
|
|
References
- ↑ Kim TK, Lee E, Jang HJ (2015). “Imaging findings of mimickers of hepatocellular carcinoma”. Clin Mol Hepatol. 21 (4): 326–43. doi:10.3350/cmh.2015.21.4.326. PMC 4712159. PMID 26770920.
- ↑ Ferrell, Linda (2000). “Liver Pathology: Cirrhosis, Hepatitis and Primary Liver Tumors. Update and Diagnostic Problems”. Modern Pathology. 13 (6): 679–704. doi:10.1038/modpathol.3880119. ISSN 0893-3952.
- ↑ Kim, Tae Kyoung; Lee, Eunchae; Jang, Hyun-Jung (2015). “Imaging findings of mimickers of hepatocellular carcinoma”. Clinical and Molecular Hepatology. 21 (4): 326. doi:10.3350/cmh.2015.21.4.326. ISSN 2287-2728.
- ↑ Doo, Kyung Won; Lee, Chang Hee; Choi, Jae Woong; Lee, Jongmee; Kim, Kyeong Ah; Park, Cheol Min (2009). ““Pseudo Washout” Sign in High-Flow Hepatic Hemangioma on Gadoxetic Acid Contrast-Enhanced MRI Mimicking Hypervascular Tumor”. American Journal of Roentgenology. 193 (6): W490–W496. doi:10.2214/AJR.08.1732. ISSN 0361-803X.
- ↑ Zech CJ, Herrmann KA, Reiser MF, Schoenberg SO (2007). “MR imaging in patients with suspected liver metastases: value of liver-specific contrast agent Gd-EOB-DTPA”. Magn Reson Med Sci. 6 (1): 43–52. PMID 17510541.
- ↑ Cheng, H C; Tsai, S H; Chiang, J H; Chang, C Y (1995). “Hyalinized liver hemangioma mimicking malignant tumor at MR imaging”. American Journal of Roentgenology. 165 (4): 1016–1017. doi:10.2214/ajr.165.4.7676959. ISSN 0361-803X.
- ↑ Haratake J, Horie A, Nagafuchi Y (1992). “Hyalinized hemangioma of the liver”. Am. J. Gastroenterol. 87 (2): 234–6. PMID 1370873.
- ↑ Takayasu, K; Moriyama, N; Shima, Y; Muramatsu, Y; Yamada, T; Makuuchi, M; Yamasaki, S; Hirohashi, S (1986). “Atypical radiographic findings in hepatic cavernous hemangioma: correlation with histologic features”. American Journal of Roentgenology. 146 (6): 1149–1153. doi:10.2214/ajr.146.6.1149. ISSN 0361-803X.
- ↑ Yamashita Y, Shimada M, Taguchi K, Gion T, Hasegawa H, Utsunomiya T, Hamatsu T, Matsumata T, Sugimachi K (2000). “Hepatic sclerosing hemangioma mimicking a metastatic liver tumor: report of a case”. Surg. Today. 30 (9): 849–52. PMID 11039718.
- ↑ Kim, Tae Kyoung; Lee, Eunchae; Jang, Hyun-Jung (2015). “Imaging findings of mimickers of hepatocellular carcinoma”. Clinical and Molecular Hepatology. 21 (4): 326. doi:10.3350/cmh.2015.21.4.326. ISSN 2287-2728.
- ↑ Lee, So Jung; Kim, So Yeon; Kim, Kyoung Won; Shin, Yong Moon; Kim, Hyoung Jung; Lee, Jong Seok; Kim, Sun A (2012). “Hepatic angiomyolipoma with minimal fat, mimicking hepatocellular carcinoma”. Clinical and Molecular Hepatology. 18 (3): 330. doi:10.3350/cmh.2012.18.3.330. ISSN 2287-2728.
- ↑ Kim R, Lee JM, Joo I, Lee DH, Woo S, Han JK, Choi BI (2015). “Differentiation of lipid poor angiomyolipoma from hepatocellular carcinoma on gadoxetic acid-enhanced liver MR imaging”. Abdom Imaging. 40 (3): 531–41. doi:10.1007/s00261-014-0244-4. PMID 25231411.
- ↑ Jeon TY, Kim SH, Lim HK, Lee WJ (2010). “Assessment of triple-phase CT findings for the differentiation of fat-deficient hepatic angiomyolipoma from hepatocellular carcinoma in non-cirrhotic liver”. Eur J Radiol. 73 (3): 601–6. doi:10.1016/j.ejrad.2009.01.010. PMID 19200676.
- ↑ Kim, T K; Choi, B I; Han, J K; Jang, H J; Cho, S G; Han, M C (1997). “Peripheral cholangiocarcinoma of the liver: two-phase spiral CT findings”. Radiology. 204 (2): 539–543. doi:10.1148/radiology.204.2.9240550. ISSN 0033-8419.
- ↑ Choi BI, Kim TK, Han JK (1998). “MRI of clonorchiasis and cholangiocarcinoma”. J Magn Reson Imaging. 8 (2): 359–66. PMID 9562062.
- ↑ Guo, Le-Hang; Xu, Hui-Xiong (2015). “Contrast-Enhanced Ultrasound in the Diagnosis of Hepatocellular Carcinoma and Intrahepatic Cholangiocarcinoma: Controversy over the ASSLD Guideline”. BioMed Research International. 2015: 1–5. doi:10.1155/2015/349172. ISSN 2314-6133.
- ↑ Wilson, Stephanie R.; Kim, Tae Kyoung; Jang, Hyun-Jung; Burns, Peter N. (2007). “Enhancement Patterns of Focal Liver Masses: Discordance Between Contrast-Enhanced Sonography and Contrast-Enhanced CT and MRI”. American Journal of Roentgenology. 189 (1): W7–W12. doi:10.2214/AJR.06.1060. ISSN 0361-803X.
- ↑ Ohtomo K, Baron RL, Dodd GD, Federle MP, Miller WJ, Campbell WL, Confer SR, Weber KM (1993). “Confluent hepatic fibrosis in advanced cirrhosis: appearance at CT”. Radiology. 188 (1): 31–5. doi:10.1148/radiology.188.1.8511316. PMID 8511316.
- ↑ Hussain, Hero K.; Syed, Ibrahim; Nghiem, Hanh V.; Johnson, Timothy D.; Carlos, Ruth C.; Weadock, William J.; Francis, Isaac R. (2004). “T2-weighted MR Imaging in the Assessment of Cirrhotic Liver”. Radiology. 230 (3): 637–644. doi:10.1148/radiol.2303020921. ISSN 0033-8419.
- ↑ Ohtomo K, Baron RL, Dodd GD, Federle MP, Ohtomo Y, Confer SR (1993). “Confluent hepatic fibrosis in advanced cirrhosis: evaluation with MR imaging”. Radiology. 189 (3): 871–4. doi:10.1148/radiology.189.3.8234718. PMID 8234718.
- ↑ Brancatelli G, Baron RL, Federle MP, Sparacia G, Pealer K (2009). “Focal confluent fibrosis in cirrhotic liver: natural history studied with serial CT”. AJR Am J Roentgenol. 192 (5): 1341–7. doi:10.2214/AJR.07.2782. PMID 19380559.
- ↑ Kelekis NL, Makri E, Vassiou A, Patsiaoura K, Spiridakis M, Dalekos GN (2004). “Confluent hepatic fibrosis as the presenting imaging sign in nonadvanced alcoholic cirrhosis”. Clin Imaging. 28 (2): 124–7. doi:10.1016/S0899-7071(03)00243-2. PMID 15050225.
- ↑ Ooi CG, Chan KL, Peh WC, Saing H, Ngan H (1999). “Confluent hepatic fibrosis in monozygotic twins”. Pediatr Radiol. 29 (1): 53–5. doi:10.1007/s002470050534. PMID 9880618.
- ↑ Park YS, Lee CH, Kim BH, Lee J, Choi JW, Kim KA, Ahn JH, Park CM (2013). “Using Gd-EOB-DTPA-enhanced 3-T MRI for the differentiation of infiltrative hepatocellular carcinoma and focal confluent fibrosis in liver cirrhosis”. Magn Reson Imaging. 31 (7): 1137–42. doi:10.1016/j.mri.2013.01.011. PMID 23688409.
- ↑ Brancatelli G, Federle MP, Grazioli L, Golfieri R, Lencioni R (2002). “Large regenerative nodules in Budd-Chiari syndrome and other vascular disorders of the liver: CT and MR imaging findings with clinicopathologic correlation”. AJR Am J Roentgenol. 178 (4): 877–83. doi:10.2214/ajr.178.4.1780877. PMID 11906867.
- ↑ Brancatelli G, Federle MP, Grazioli L, Golfieri R, Lencioni R (2002). “Benign regenerative nodules in Budd-Chiari syndrome and other vascular disorders of the liver: radiologic-pathologic and clinical correlation”. Radiographics. 22 (4): 847–62. doi:10.1148/radiographics.22.4.g02jl17847. PMID 12110714.
- ↑ Newerla, Caroline; Schaeffer, Fabienne; Terracciano, Luigi; Hohmann, Joachim (2012). “Multiple FNH-Like Lesions in a Patient with Chronic Budd-Chiari Syndrome: Gd-EOB-Enhanced MRI and BR1 CEUS Findings”. Case Reports in Radiology. 2012: 1–5. doi:10.1155/2012/685486. ISSN 2090-6862.
- ↑ Yoneda N, Matsui O, Kitao A, Kita R, Kozaka K, Koda W, Kobayashi S, Gabata T, Ikeda H, Sato Y, Nakanuma Y (2012). “Hepatocyte transporter expression in FNH and FNH-like nodule: correlation with signal intensity on gadoxetic acid enhanced magnetic resonance images”. Jpn J Radiol. 30 (6): 499–508. doi:10.1007/s11604-012-0085-4. PMID 22618456.
- ↑ Matsui, O; Kadoya, M; Takahashi, S; Yoshikawa, J; Gabata, T; Takashima, T; Kitagawa, K (1995). “Focal sparing of segment IV in fatty livers shown by sonography and CT: correlation with aberrant gastric venous drainage”. American Journal of Roentgenology. 164 (5): 1137–1140. doi:10.2214/ajr.164.5.7717220. ISSN 0361-803X.
- ↑ Itai Y, Matsui O (1999). “‘Nonportal’ splanchnic venous supply to the liver: abnormal findings on CT, US and MRI”. Eur Radiol. 9 (2): 237–43. doi:10.1007/s003300050661. PMID 10101644.
- [[#cite_ref-NicolauBr�2004_31-0|↑]] Nicolau, C.; Br�, C. (2004). “Focal liver lesions: evaluation with contrast-enhanced ultrasonography”. Abdominal Imaging. 29 (3). doi:10.1007/s00261-003-0117-8. ISSN 0942-8925. replacement character in
|last2=at position 3 (help) - ↑ Hamer OW, Aguirre DA, Casola G, Lavine JE, Woenckhaus M, Sirlin CB (2006). “Fatty liver: imaging patterns and pitfalls”. Radiographics. 26 (6): 1637–53. doi:10.1148/rg.266065004. PMID 17102041.
- ↑ Hamer OW, Aguirre DA, Casola G, Sirlin CB (2005). “Imaging features of perivascular fatty infiltration of the liver: initial observations”. Radiology. 237 (1): 159–69. doi:10.1148/radiol.2371041580. PMID 16100085.
- ↑ Memeo, M.; Stabile Ianora, A. A.; Scardapane, A.; Buonamico, P.; Sabbà, C.; Angelelli, G. (2004). “Hepatic involvement in hereditary hemorrhagic telangiectasia:”. Abdominal Imaging. 29 (2): 211–220. doi:10.1007/s00261-003-0101-3. ISSN 0942-8925.
- ↑ Siddiki H, Doherty MG, Fletcher JG, Stanson AW, Vrtiska TJ, Hough DM, Fidler JL, McCollough CH, Swanson KL (2008). “Abdominal findings in hereditary hemorrhagic telangiectasia: pictorial essay on 2D and 3D findings with isotropic multiphase CT”. Radiographics. 28 (1): 171–84. doi:10.1148/rg.281075037. PMID 18203937.
- ↑ Oliver JH, Baron RL (1996). “Helical biphasic contrast-enhanced CT of the liver: technique, indications, interpretation, and pitfalls”. Radiology. 201 (1): 1–14. doi:10.1148/radiology.201.1.8816509. PMID 8816509.
- ↑ Yu JS, Kim KW, Sung KB, Lee JT, Yoo HS (1997). “Small arterial-portal venous shunts: a cause of pseudolesions at hepatic imaging”. Radiology. 203 (3): 737–42. doi:10.1148/radiology.203.3.9169697. PMID 9169697.
- ↑ Wu, Jim S.; Saluja, Sanjay; Garcia-Tsao, Guadalupe; Chong, Alice; Henderson, Katherine J.; White, Robert I. (2006). “Liver Involvement in Hereditary Hemorrhagic Telangiectasia: CT and Clinical Findings Do Not Correlate in Symptomatic Patients”. American Journal of Roentgenology. 187 (4): W399–W405. doi:10.2214/AJR.05.1068. ISSN 0361-803X.
- ↑ Itai, Y; Matsui, O (1997). “Blood flow and liver imaging”. Radiology. 202 (2): 306–314. doi:10.1148/radiology.202.2.9015047. ISSN 0033-8419.
- ↑ {{cite
- ↑ Mathieu D, Vasile N, Dibie C, Grenier P (1985). “Portal cavernoma: dynamic CT features and transient differences in hepatic attenuation”. Radiology. 154 (3): 743–8. doi:10.1148/radiology.154.3.3881794. PMID 3881794.
- ↑ Itai Y, Murata S, Saida Y, Minami M. Central zone and peripheral zone of the liver based on portal and hepatic arterial blood supply: imaging approach to deformity of cirrhotic liver. Jpn J Clin Radiol. 1994;39:1553–1559
- ↑ Kim, Tae Kyoung; Lee, Kyoung Ho; Jang, Hyun–Jung; Haider, Masoom A.; Jacks, Lindsay M.; Menezes, Ravi J.; Park, Seong Ho; Yazdi, Leyla; Sherman, Morris; Khalili, Korosh (2011). “Analysis of Gadobenate Dimeglumine–enhanced MR Findings for Characterizing Small (1–2-cm) Hepatic Nodules in Patients at High Risk for Hepatocellular Carcinoma”. Radiology. 259 (3): 730–738. doi:10.1148/radiol.11101549. ISSN 0033-8419.
- ↑ Kim JH, Kim TK, Kim BS, Eun HW, Kim PN, Lee MG, Ha HK (2002). “Enhancement of hepatic hemangiomas with levovist on coded harmonic angiographic ultrasonography”. J Ultrasound Med. 21 (2): 141–8. PMID 11833870.
- ↑ Brannigan, Margot; Burns, Peter N.; Wilson, Stephanie R. (2004). “Blood Flow Patterns in Focal Liver Lesions at Microbubble-enhanced US”. RadioGraphics. 24 (4): 921–935. doi:10.1148/rg.244035158. ISSN 0271-5333.
- ↑ 46.0 46.1 Kim TK, Jang HJ, Wilson SR (2006). “Benign liver masses: imaging with microbubble contrast agents”. Ultrasound Q. 22 (1): 31–9. PMID 16641791.
- ↑ Jang, Hyun-Jung; Kim, Tae Kyoung; Lim, Hyo Keun; Park, Sang Jae; Sim, Jung Suk; Kim, Hyae Young; Lee, Joo-Hyuk (2003). “Hepatic Hemangioma: Atypical Appearances on CT, MR Imaging, and Sonography”. American Journal of Roentgenology. 180 (1): 135–141. doi:10.2214/ajr.180.1.1800135. ISSN 0361-803X.
- ↑ . doi:10.1102/1470-7330.2009.0015. Missing or empty
|title=(help) - ↑ 49.0 49.1 Jang, Hyun-Jung; Yu, Hojun; Kim, Tae Kyoung (2009). “Imaging of Focal Liver Lesions”. Seminars in Roentgenology. 44 (4): 266–282. doi:10.1053/j.ro.2009.05.008. ISSN 0037-198X.
- ↑ Bhayana, Deepak; Kim, Tae Kyoung; Jang, Hyun-Jung; Burns, Peter N.; Wilson, Stephanie R. (2010). “Hypervascular Liver Masses on Contrast-Enhanced Ultrasound: The Importance of Washout”. American Journal of Roentgenology. 194 (4): 977–983. doi:10.2214/AJR.09.3375. ISSN 0361-803X.
- ↑ Tamada T, Ito K, Yamamoto A, Sone T, Kanki A, Tanaka F, Higashi H (2011). “Hepatic hemangiomas: evaluation of enhancement patterns at dynamic MRI with gadoxetate disodium”. AJR Am J Roentgenol. 196 (4): 824–30. doi:10.2214/AJR.10.5113. PMID 21427331.
- ↑ Heiken, Jay P. (2007). “Distinguishing benign from malignant liver tumours”. Cancer Imaging. 7 (Special Issue A): S1–S14. doi:10.1102/1470-7330.2007.9084. ISSN 1470-7330.
- ↑ Alturkistany, Samira; Jang, Hyun-Jung; Yu, Hojun; Lee, Kyoung Ho; Kim, Tae Kyoung (2011). “Fading hepatic hemangiomas on multiphasic CT”. Abdominal Radiology. 37 (5): 775–780. doi:10.1007/s00261-011-9826-6. ISSN 2366-004X.
- ↑ Liu GJ, Lu MD, Xie XY, Xu HX, Xu ZF, Zheng YL, Liang JY, Wang W (2008). “Real-time contrast-enhanced ultrasound imaging of infected focal liver lesions”. J Ultrasound Med. 27 (4): 657–66. PMID 18359914.
- ↑ Kim, Kyoung Won; Choi, Byung Ihn; Park, Seong Ho; Kim, Ah Young; Koh, Young Hwan; Lee, Hyun Ju; Han, Joon Koo (2004). “Pyogenic hepatic abscesses: distinctive features from hypovascular hepatic malignancies on contrast-enhanced ultrasound with SH U 508A; early experience”. Ultrasound in Medicine & Biology. 30 (6): 725–733. doi:10.1016/j.ultrasmedbio.2004.03.006. ISSN 0301-5629.
- ↑ Syed MA, Kim TK, Jang HJ (2007). “Portal and hepatic vein thrombosis in liver abscess: CT findings”. Eur J Radiol. 61 (3): 513–9. doi:10.1016/j.ejrad.2006.11.022. PMID 17161932.
- ↑ Menias, Christine O.; Surabhi, Venkateswar R.; Prasad, Srinivasa R.; Wang, Hanlin L.; Narra, Vamsi R.; Chintapalli, Kedar N. (2008). “Mimics of Cholangiocarcinoma: Spectrum of Disease”. RadioGraphics. 28 (4): 1115–1129. doi:10.1148/rg.284075148. ISSN 0271-5333.
- ↑ Gollapudi P, Chejfec G, Zarling EJ (1992). “Spontaneous regression of hepatic pseudotumor”. Am. J. Gastroenterol. 87 (2): 214–7. PMID 1734701.
- ↑ Yoon KH, Ha HK, Lee JS, Suh JH, Kim MH, Kim PN, Lee MG, Yun KJ, Choi SC, Nah YH, Kim CG, Won JJ, Auh YH (1999). “Inflammatory pseudotumor of the liver in patients with recurrent pyogenic cholangitis: CT-histopathologic correlation”. Radiology. 211 (2): 373–9. doi:10.1148/radiology.211.2.r99ma36373. PMID 10228516.
- ↑ CHEDID, Marcio F.; KRUEL, Cleber R. P.; PINTO, Marcelo A.; GREZZANA-FILHO, Tomaz J. M.; LEIPNITZ, Ian; KRUEL, Cleber D. P.; SCAFFARO, Leandro A.; CHEDID, Aljamir D. (2017). “HEPATOCELLULAR CARCINOMA: DIAGNOSIS AND OPERATIVE MANAGEMENT”. ABCD. Arquivos Brasileiros de Cirurgia Digestiva (São Paulo). 30 (4): 272–278. doi:10.1590/0102-6720201700040011. ISSN 2317-6326.
Epidemiology & Demographics
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1] Associate Editor(s)-in-Chief: Dildar Hussain, MBBS [2] Mohamad Alkateb, MBBCh [3]
Overview
Hepatocellular carcinoma is the 5th most common tumor worldwide. The epidemiology of hepatocellular carcinoma exhibits two main patterns, one in North America and Western Europe and the other in non-Western countries, such as those in Sub-Saharan Africa, Central Asia, Southeast Asia, and the Amazon basin. Men are affected more than women and it is more common between the 4th and 5th decades of life. Hepatocellular carcinoma causes 662,000 deaths worldwide annually.
Epidemiology and Demographics
The epidemiology of hepatocellular carcinoma exhibits two main patterns, one in North America and Western Europe and the other in non-Western countries, such as those in Sub-Saharan Africa, Central Asia and Southeast Asia, and the Amazon basin. Although the incidence of hepatocellular carcinoma is increasing worldwide due to its association with viral infections; it still remains relatively uncommon in the United States and Western Europe. HCC is the fastest-growing cause of cancer-related deaths and the second most common cause of mortality among women.[1][2][3][4]
Incidence
In almost 90% of the cases Hepatocellular carcinoma patients have underlying liver cirrhosis.[5][6]
- The incidence of Hepatocellular carcinoma is described below:[5][7][8]
- In 1975-77, the incidence of Hepatocellular carcinoma in the United States was 1.4 per 100,000 which increased to 4.8 per 100,000 in 2005-2007.[9]
- In 2007, the incidence of Hepatocellular carcinoma was estimated to be over 20 cases per 100,000 persons in sub-Saharan Africa, and Eastern Asia.
- In 2007, the incidence of Hepatocellular carcinoma was estimated to be 10-20 per 100,000 persons in Mediterranean countries such as Italy, Spain, and Greece.
- In 2007, the incidence of Hepatocellular carcinoma was estimated to be <5 per 100,000 persons in North and South America.
- In 2010, the incidence of Hepatocellular carcinoma was estimated to be 6 per 100,000 persons in the USA.[10]
- In 2012, the incidence of Hepatocellular carcinoma was estimated to be 10.6 per 100,000 persons among Latinos in Texas.[11]
- in 2014, the incidence of Hepatocellular carcinoma was estimated to be over 20 per 100,000 persons in sub-Saharan Africa and Eastern Asia.[12]
Prevalence
Case-fatality rate/Mortality rate
- It is estimated that that 28,920 deaths (19,610 men and 9,310 women) will occur due to hepatocellular carcinoma in the United States.[14]
Age
Hepatocellular carcinoma is more common between the 4th and 5th decades of life.[10]
Race
- Hepatocellular carcinoma is reported highest among the Asians and Pacific Islanders followed by Hispanics, Blacks, American Indians/Alaska Natives, and Whites race.[15]
Gender
Males are three times more affected than females.[16]
Region
- The majority of hepatocellular carcinoma cases are reported in Asia.[17]
Developed Countries
Hepatocellular carcinoma is generally a rare tumor in the West. Metastasis from other parts of the body is the main cause for developing hepatocellular carcinoma in the western countries. Due to the advancement in the health care system in the western countries, hepatocellular carcinoma is usually discovered at early stages in comparison to the developing countries such as Sub-Saharan Africa.
Developing Countries
In some parts of the world, such as Sub-Saharan Africa and Southeast Asia, hepatocellular carcinoma is the most common cancer. It affects men more than women and the age of onset is between late teens and early 30s. This variation is due to the different methods of hepatitis B transmission in different populations. For example, infection at or around birth predisposes to earlier cancers than if people are infected later. The time to develop hepatocellular carcinoma after hepatitis B infection can vary from years to decades. The average survival time from the time of hepatocellular carcinoma diagnosis to death is about 5.9 months and about 3 months (median survival time) in Sub-Saharan Africa according to Manson’s textbook of tropical diseases. Hepatocellular carcinoma is one of the deadliest cancers in China.
References
- ↑ Papadopoulos N, Argiana V, Deutsch M (2018). “Hepatitis C infection in patients with hereditary bleeding disorders: epidemiology, natural history, and management”. Ann Gastroenterol. 31 (1): 35–41. doi:10.20524/aog.2017.0204. PMID 29333065.
- ↑ Didi-Kouko Coulibaly, Judith; Yeboua, Mireille; Kouassi Mbengue, Alphonsine; Kouadio, Emile Allah; Anzouan-Kacou Kissi, Henriette; Binan, Allah Yves-Omer; Lohoues Kouacou, Marie-Jeanne; Attia, Alain; N’Drin, Dominique Yao; Toutou, Toussaint; Adoubi, Innocent; Pineau, Pascal (2017). “Evolution of hepatocellular carcinoma epidemiology in Côte d’Ivoire”. Bulletin du Cancer. 104 (11): 937–945. doi:10.1016/j.bulcan.2017.09.010. ISSN 0007-4551.
- ↑ “Cancer”. World Health Organization. February 2006. Retrieved 2007-05-24.
- ↑ Budny A, Kozłowski P, Kamińska M, Jankiewicz M, Kolak A, Budny B, Budny W, Niemunis-Sawicka J, Szczypiór G, Kurniawka B, Burdan F (2017). “[Epidemiology and risk factors of hepatocellular carcinoma]”. Pol. Merkur. Lekarski (in Polish). 43 (255): 133–139. PMID 28987047.
- ↑ 5.0 5.1 Colombo, Massimo; de Franchis, Roberto; Del Ninno, Ersilio; Sangiovanni, Angelo; De Fazio, Cristina; Tommasini, Maurizio; Donato, M. Francesca; Piva, Anna; Di Carlo, Valerio; Dioguardi, Nicola (1991). “Hepatocellular Carcinoma in Italian Patients with Cirrhosis”. New England Journal of Medicine. 325 (10): 675–680. doi:10.1056/NEJM199109053251002. ISSN 0028-4793.
- ↑ 6.0 6.1 Rowe, JulieH; Ghouri, YezazAhmed; Mian, Idrees (2017). “Review of hepatocellular carcinoma: Epidemiology, etiology, and carcinogenesis”. Journal of Carcinogenesis. 16 (1): 1. doi:10.4103/jcar.JCar_9_16. ISSN 1477-3163.
- ↑ Mittal S, El-Serag HB (2013). “Epidemiology of hepatocellular carcinoma: consider the population”. J. Clin. Gastroenterol. 47 Suppl: S2–6. doi:10.1097/MCG.0b013e3182872f29. PMC 3683119. PMID 23632345.
- ↑ El-Serag HB, Lau M, Eschbach K, Davila J, Goodwin J (2007). “Epidemiology of hepatocellular carcinoma in Hispanics in the United States”. Arch. Intern. Med. 167 (18): 1983–9. doi:10.1001/archinte.167.18.1983. PMID 17923599.
- ↑ Davila JA, El-Serag HB. The Rising Incidence of Hepatocellular Carcinoma in the United States: an Update. Gastroenterology. 2012;142(suppl 1):S914–S914.
- ↑ 10.0 10.1 El-Serag, Hashem B.; Kanwal, Fasiha (2014). “Epidemiology of hepatocellular carcinoma in the United States: Where are we? Where do we go?”. Hepatology. 60 (5): 1767–1775. doi:10.1002/hep.27222. ISSN 0270-9139.
- ↑ Lee, Jung Eun; Ramirez, Amelie G.; Weiss, Nancy S.; Holden, Alan E. C.; Suarez, Lucina; Cooper, Sharon P.; Munoz, Edgar; Naylor, Susan L. (2012). “Incidence and Risk Factors for Hepatocellular Carcinoma in Texas Latinos: Implications for Prevention Research”. PLoS ONE. 7 (4): e35573. doi:10.1371/journal.pone.0035573. ISSN 1932-6203.
- ↑ Mittal, Sahil; El-Serag, Hashem B. (2013). “Epidemiology of Hepatocellular Carcinoma”. Journal of Clinical Gastroenterology. 47: S2–S6. doi:10.1097/MCG.0b013e3182872f29. ISSN 0192-0790.
- ↑ World Health Organization, I.A.f.R.o.C. Estimated Cancer Incidence, Mortality and Prevalence Worldwide in 2012. Available from: http://www.globocan.iarc.fr/Pages/fact_sheets_population.aspx
- ↑ “Liver Cancer: Statistics | Cancer.Net”.
- ↑ Altekruse, Sean F.; McGlynn, Katherine A.; Reichman, Marsha E. (2009). “Hepatocellular Carcinoma Incidence, Mortality, and Survival Trends in the United States From 1975 to 2005”. Journal of Clinical Oncology. 27 (9): 1485–1491. doi:10.1200/JCO.2008.20.7753. ISSN 0732-183X.
- ↑ El-Serag, Hashem B.; Kanwal, Fasiha (2014). “Epidemiology of hepatocellular carcinoma in the United States: Where are we? Where do we go?”. Hepatology. 60 (5): 1767–1775. doi:10.1002/hep.27222. ISSN 0270-9139.
- ↑ El-Serag, Hashem B.; Kanwal, Fasiha (2014). “Epidemiology of hepatocellular carcinoma in the United States: Where are we? Where do we go?”. Hepatology. 60 (5): 1767–1775. doi:10.1002/hep.27222. ISSN 0270-9139.
Risk factors
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1] Associate Editor(s)-in-Chief: Dildar Hussain, MBBS [2] Mohamad Alkateb, MBBCh [3]
Overview
Common risk factors in the development of hepatocellular carcinoma are chronic hepatitis B infection, chronic hepatitis C infection, cirrhosis, inherited metabolic diseases and aflaoxins.
Common Risk Factors
Common risk factors that may increase the risk of developing hepatocellular carcinoma are:[1][2][3][4][5][6][7][8][9][10]
- Chronic hepatitis B
- Chronic hepatitis C
- Cirrhosis with hemochromatosis
- Nonalcoholic steatohepatitis
- Food contaminated with Aspergillus flavus (especially peanuts and corns stored during prolonged wet seasons), which produces aflatoxins.
Less Common Risk Factors
Less common risk factors that may increase the risk of developing hepatocellular carcinoma are:[11][12][13][14]
- Anabolic steroids
- Alpha1-antitrypsin deficiency
- Arsenic
- Alcohol
- Obesity
- Diabetes Mellitus
- Food infected with Aspergillus flavus (especially peanuts and corns stored during prolonged wet seasons), which produces aflatoxin.
- Glycogen storage diseases
- Hemochromatosis
- Inherited metabolic diseases such as:
- Smoking
- Tyrosinemia
- Vinyl chloride and thorium dioxide
- Wilson disease
References
- ↑ National Cancer Institute. Physician Data Query Database 2015.http://www.cancer.gov/types/liver/hp/adult-liver-treatment-pdq
- ↑ Trichopoulos D, Bamia C, Lagiou P, Fedirko V, Trepo E, Jenab M, Pischon T, Nöthlings U, Overved K, Tjønneland A, Outzen M, Clavel-Chapelon F, Kaaks R, Lukanova A, Boeing H, Aleksandrova K, Benetou V, Zylis D, Palli D, Pala V, Panico S, Tumino R, Sacerdote C, Bueno-De-Mesquita HB, Van Kranen HJ, Peeters PH, Lund E, Quirós JR, González CA, Sanchez Perez MJ, Navarro C, Dorronsoro M, Barricarte A, Lindkvist B, Regnér S, Werner M, Hallmans G, Khaw KT, Wareham N, Key T, Romieu I, Chuang SC, Murphy N, Boffetta P, Trichopoulou A, Riboli E (2011). “Hepatocellular carcinoma risk factors and disease burden in a European cohort: a nested case-control study”. J. Natl. Cancer Inst. 103 (22): 1686–95. doi:10.1093/jnci/djr395. PMC 3216968. PMID 22021666.
- ↑ Cecil, Russell L., James B. Wyngaarden, and Lloyd H. Smith. Textbook of . Philadelphia: Saunders, 1988. Print.
- ↑ “Redirecting”.
- ↑ CHEDID, Marcio F.; KRUEL, Cleber R. P.; PINTO, Marcelo A.; GREZZANA-FILHO, Tomaz J. M.; LEIPNITZ, Ian; KRUEL, Cleber D. P.; SCAFFARO, Leandro A.; CHEDID, Aljamir D. (2017). “HEPATOCELLULAR CARCINOMA: DIAGNOSIS AND OPERATIVE MANAGEMENT”. ABCD. Arquivos Brasileiros de Cirurgia Digestiva (São Paulo). 30 (4): 272–278. doi:10.1590/0102-6720201700040011. ISSN 2317-6326.
- ↑ Fujiwara N, Friedman SL, Goossens N, Hoshida Y (2017). “Risk factors and prevention of hepatocellular carcinoma in the era of precision medicine”. J. Hepatol. doi:10.1016/j.jhep.2017.09.016. PMID 28989095.
- ↑ Trad, Dorra; Bibani, Norsaf; Sabbah, Meriam; Elloumi, Hela; Gargouri, Dalila; Ouakaa, Asma; Kharrat, Jamel (2017). “Known, new and emerging risk factors of hepatocellular carcinoma (review)”. La Presse Médicale. 46 (11): 1000–1007. doi:10.1016/j.lpm.2017.09.025. ISSN 0755-4982.
- ↑ Budny A, Kozłowski P, Kamińska M, Jankiewicz M, Kolak A, Budny B, Budny W, Niemunis-Sawicka J, Szczypiór G, Kurniawka B, Burdan F (2017). “[Epidemiology and risk factors of hepatocellular carcinoma]”. Pol. Merkur. Lekarski (in Polish). 43 (255): 133–139. PMID 28987047.
- ↑ Parkin, Donald Maxwell (2006). “The global health burden of infection-associated cancers in the year 2002”. International Journal of Cancer. 118 (12): 3030–3044. doi:10.1002/ijc.21731. ISSN 0020-7136.
- ↑ Shi, J; Zhu, L; Liu, S; Xie, W-f (2005). “A meta-analysis of case–control studies on the combined effect of hepatitis B and C virus infections in causing hepatocellular carcinoma in China”. British Journal of Cancer. 92 (3): 607–612. doi:10.1038/sj.bjc.6602333. ISSN 0007-0920.
- ↑ Trad, Dorra; Bibani, Norsaf; Sabbah, Meriam; Elloumi, Hela; Gargouri, Dalila; Ouakaa, Asma; Kharrat, Jamel (2017). “Known, new and emerging risk factors of hepatocellular carcinoma (review)”. La Presse Médicale. 46 (11): 1000–1007. doi:10.1016/j.lpm.2017.09.025. ISSN 0755-4982.
- ↑ Clavière C, Bronowicki JP, Hudziak H, Bigard MA, Gaucher P (1998). “[Role of sex steroids and their receptors in the pathophysiology of hepatocellular carcinoma]”. Gastroenterol. Clin. Biol. (in French). 22 (1): 73–86. PMID 9762169.
- ↑ “Studies of Cancer in Humans – Tobacco Smoke and Involuntary Smoking – NCBI Bookshelf”.
- ↑ “Tobacco smoke and involuntary smoking”. IARC Monogr Eval Carcinog Risks Hum. 83: 1–1438. 2004. PMC 4781536. PMID 15285078.
Screening
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1] Associate Editor(s)-in-Chief: Mohamad Alkateb, MBBCh [2]
Overview
According to the American Association of Liver Diseases, screening for hepatocellular carcinoma by ultrasound (US) is recommended among patients with hepatitis B, hepatitis C, and cirrhosis. Screening is also recommended for Asian men over the age of 40, Asian women over the age of 50, and African American.
Screening
Screening for hepatocellular carcinoma by abdominal ultrasound and serum levels of alpha-fetoprotein is recommended for the following populations:[1][2]
- Patients with hepatitis B
- Patients with hepatitis C
- Patietns with cirrhosis
- Asian men over the age of 40
- Asian women over the age of 50
- African American
References
- ↑ Trad, Dorra; Bibani, Norsaf; Sabbah, Meriam; Elloumi, Hela; Gargouri, Dalila; Ouakaa, Asma; Kharrat, Jamel (2017). “Known, new and emerging risk factors of hepatocellular carcinoma (review)”. La Presse Médicale. 46 (11): 1000–1007. doi:10.1016/j.lpm.2017.09.025. ISSN 0755-4982.
- ↑ Sirlin CB, Kielar AZ, Tang A, Bashir MR (2018). “LI-RADS: a glimpse into the future”. Abdom Radiol (NY). 43 (1): 231–236. doi:10.1007/s00261-017-1448-1. PMID 29318354.
Natural History, Complications & Prognosis
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1] Associate Editor(s)-in-Chief: Dildar Hussain, MBBS [2] Mohamad Alkateb, MBBCh [3]
Overview
Depending on the extent of the tumor at the time of diagnosis, the prognosis may vary. However, the prognosis is generally regarded as poor. If the cancer is inoperable, the disease is usually deadly within 3 to 6 months. The survival rate of hepatocellular carcinoma is less than 50 percent.
Natural History
Without treatment, the patient will develop symptoms of jaundice, ascites, cachexia, right upper quadrant abdominal pain, nausea, and vomiting, which will eventually lead to death.
Complications
Complications directly related to cancer
Complications that can develop as a result of hepatocellular carcinoma include the following:
- Jaundice
- Ascites
- Cachexia
- Coagulopathy
- Erythrocytosis
- Hypercalcemia
- Hypertension
- Watery diarrhea
- Hypoglycemia
- Hypercholesterolemia
Complications related to transarterial embolization/chemoembolization (TAE/TACE) therapy
The following complications may result from TAE/TACE therapy of the tumour:[1][2][3][4]
- Liver rupture
- Liver abscess
- Femoral artery pseudoaneurysm
- Cholecystitis
- Biloma
- Pulmonary embolism
- Partial intestinal obstruction
Complications related to radiofrequency ablation
Common complications of radiofrequency ablation therapy include the following:[5]
- Sepsis
- Hepatic failure
- Intraperitoneal bleeding
- Liver abscess
- Bile duct injury
- Grounding pad burns
Prognosis
Due to its late presentation, the prognosis of hepatocellular carcinoma is poor even with treatment. Without treatment, hepatocellular carcinoma will result in early death. The prognosis depends on the following:[6]
- Operable vs inoperable cancer
- Cancer staging: Size and metastasis play a major role in prognosis
- Patient’s general health
- Time of cancer diagnosis
The survival rate of Hepatocellular carcinoma is less than 50 percent.
Independent predictors of prognosis
- The following parameters are known to be independent predictors of prognosis for hepatocellular carcinoma:[7]
- Alpha fetoprotein (AFP)
- Alkaline phosphatase
- International normalized ratio
- Creatinine
- MELD score > 10
- Number of nodules
- Maximum tumor diameter
- Portal vein thrombosis
- Extra-hepatic metastasis
- Performance status
Prognosis based on staging systems
- The Barcelona Clinic Liver Cancer (BCLC) staging system has the best independent predictive power for survival when compared with the other 6 prognostic systems.[7]
References
- ↑ Tu J, Jia Z, Ying X, Zhang D, Li S, Tian F, Jiang G (2016). “The incidence and outcome of major complication following conventional TAE/TACE for hepatocellular carcinoma”. Medicine (Baltimore). 95 (49): e5606. doi:10.1097/MD.0000000000005606. PMC 5266057. PMID 27930585.
- ↑ Jia Z, Tian F, Jiang G (2013). “Ruptured hepatic carcinoma after transcatheter arterial chemoembolization”. Curr Ther Res Clin Exp. 74: 41–3. doi:10.1016/j.curtheres.2012.12.006. PMC 3862201. PMID 24384870.
- ↑ Chung JW, Park JH, Im JG, Han JK, Han MC (1993). “Pulmonary oil embolism after transcatheter oily chemoembolization of hepatocellular carcinoma”. Radiology. 187 (3): 689–93. doi:10.1148/radiology.187.3.8388567. PMID 8388567.
- ↑ Chung JW, Park JH, Han JK, Choi BI, Han MC, Lee HS, Kim CY (1996). “Hepatic tumors: predisposing factors for complications of transcatheter oily chemoembolization”. Radiology. 198 (1): 33–40. doi:10.1148/radiology.198.1.8539401. PMID 8539401.
- ↑ Rhim H (2005). “Complications of radiofrequency ablation in hepatocellular carcinoma”. Abdom Imaging. 30 (4): 409–18. doi:10.1007/s00261-004-0255-7. PMID 15688113.
- ↑ Altekruse, Sean F.; McGlynn, Katherine A.; Reichman, Marsha E. (2009). “Hepatocellular Carcinoma Incidence, Mortality, and Survival Trends in the United States From 1975 to 2005”. Journal of Clinical Oncology. 27 (9): 1485–1491. doi:10.1200/JCO.2008.20.7753. ISSN 0732-183X.
- ↑ 7.0 7.1 Marrero JA, Fontana RJ, Barrat A, Askari F, Conjeevaram HS, Su GL, Lok AS (2005). “Prognosis of hepatocellular carcinoma: comparison of 7 staging systems in an American cohort”. Hepatology. 41 (4): 707–16. doi:10.1002/hep.20636. PMID 15795889.
Diagnosis
Diagnosis
Staging | Diagnostic Study of Choice | History and Symptoms | Physical Examination | Lab Studies | Electrocardiogram | Chest X Ray | MRI | CT | Echocardiography or Ultrasound | Other imaging findings | Other diagnostic studies
Treatment
Treatment
Medical Therapy | Surgery | Primary prevention | Secondary prevention | Cost-Effectiveness of Therapy | Future or Investigational Therapies
Looking for the patient version?
© 2026 MyEClinic – IFTM Institut für Telematik in der Medizin GmbH