
Pancreatic cancer
For patient information click here Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Sudarshana Datta, MD [2] Aravind Reddy Kothagadi M.B.B.S[3]
Synonyms and keywords: Carcinoma of pancreas
Overview
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Aravind Reddy Kothagadi M.B.B.S[2], Sudarshana Datta, MD [3]
Overview
Pancreatic cancer is a malignant tumour within the pancreatic gland. In 1679, Morgagni was the first to recognize cancer of the pancreas and described the pancreas of one of his patients as a dry white pancreas of a scirrhous nature with “pretty hard” distinct lobules. Pancreatic cancers can be classified based on the production of hormones into exocrine and endocrine cancers. About 95 percent of pancreatic tumors are adenocarcinomas, which are exocrine tumors. The remaining 5 percent include other tumors of the exocrine pancreas (e.g. serous cystadenomas), acinar cell cancers, and pancreatic neuroendocrine tumors (such as insulinomas). These tumors have a completely different diagnostic and therapeutic profile, and generally a more favorable prognosis. The progression and development of pancreatic cancer is influenced by complex interactions and crosstalk between several cellular signaling pathways that include inactivation of tumor suppressor genes, activation of oncogenes and deregulation of molecules in various signaling pathways. Pancreatic cancer must be differentiated from other pancreatic pathologies such as chronic pancreatitis, autoimmune pancreatitis, pancreatic pseudocyst, choledocholithiasis, and neuroendocrine tumors of the pancreas. Pathologies of the bile duct and duodenum such as choledocholithiasis, gallstones (cholelithiasis), choledochal cysts, cholangiocarcinoma, bile duct strictures and ampullary cancer should be differentiated from pancreatic cancer based on imaging and biopsy findings. The most potent risk factors for pancreatic cancer include smoking, alcoholism, increased BMI, diabetes mellitus, chronic pancreatitis and a family history of pancreatic cancer. The most common symptoms of pancreatic cancer include mid-epigastric pain, jaundice, sudden unexplained weight loss and dark urine and light-colored or greasy stools. CT scan is the preferred diagnostic modality and findings that may be suggestive of pancreatic cancer include morphological changes of the gland, destruction of the peripancreatic fat and loss of the sharp margins with surrounding structures, involvement of the regional lymph nodes and adjacent vasculature, pancreatic ductal dilatation, pancreatic atrophy and obstruction of the common bile duct. In patients with pancreatic cancer, surgery is the primary modality of treatment. Extrapancreatic disease, in contrast, requires palliative therapy and curative resection is not performed in such patients.
Historical prospective
Herophilus of Chalcedon (circa 300 B.C.), the father of scientific anatomy, was the first to describe the pancreas but he had no conception of its function. Rufus of Ephesus (circa 100 A.D) coined the term pancreas (from the Greek words pan which means all and kreas which means flesh). It literally means all flesh due to its homogeneous composition. In 1679, Morgagni was the first to recognize cancer of the pancreas and described the pancreas of one of his patients as a dry white pancreas of a scirrhous nature with “pretty hard” distinct lobules. By the late 1800s, the clinical symptoms, signs and histology of pancreatic cancer had been defined. Bard and Pit differentiated between duct, acinar cell and islet cell cancers. Trendelenburg was the first to successfully excise a solid tumor of the pancreas and Kappeler described the first cholecystojejunostomy performed as palliative therapy in a pancreatic cancer patient. In February 1955, Whipple performed a two stage operation for carcinoma of the ampulla, where a cholecystojejunostomy and total duodenectomy were performed. This was the first total duodenectomy to be recorded in a human subject. In 1940, Whipple and Nelson performed the first ever recorded one-stage pancreaticoduodenectomy followed by occlusion of the pancreas.Post 1940, the one-stage has been modified repeatedly by surgeons world wide. The treatment of pancreatic cancer continues to be a dilemma. However, the mortality rate for pancreatoduodenal resection has declined from 21 percent before 1970 to 0 percent after 1970.
Classification
Pancreatic cancers can be classified based on the production of hormones into exocrine and endocrine cancers. Pancreatic exocrine tumors include different types such as adenocarcinoma, acinar cell carcinoma, adenosquamous carcinoma and pancreatoblastomas. Pancreatic endocrine tumors include insulinomas, glucagonomas, VIPomas, somatostatinomas and Ppomas.
Pathophysiology
Pancreatic cancer is the result of activation or inactivation of multiple gene subsets. The progression and development of pancreatic cancer is influenced by complex interactions and crosstalk between several cellular signaling pathways that include inactivation of tumor suppressor genes, activation of oncogenes and deregulation of molecules in various signaling pathways. EGFR, Akt, NF-kB and Hedgehog pathways are most commonly involved in the pathogenesis of pancreatic cancer. Majority of ductal adenocarcinomas have varying degrees of mucin production and duct-like structures and present as moderate-poorly differentiated masses. The ductal adenocarcinomas are referred to as “desmoplastic” or “scirrhous” carcinomas due to their characteristic dense stromal fibrosis occurring due to alterations in transforming growth factor-beta (TGF–beta) signaling. Local extension of tumor cells may occur into adjacent structures such as superior mesenteric vessels, perineural invasion both inside and outside the pancreas (eg, the retroperitoneum), duodenum, portal vein and stomach. Lymph node spread can occur to the regional peripancreatic, mesenteric, perigastric, portahepatic and omental lymph nodes.
Causes
Pancreatic cancer may be caused by the inactivation of tumor suppressor genes, activation of oncogenes and the deregulation of molecules in various signaling pathways.
Differentiating Pancreatic Cancer from other Diseases
Pancreatic cancer must be differentiated from other pancreatic pathologies such as chronic pancreatitis, autoimmune pancreatitis, pancreatic pseudocyst, choledocholithiasis, and neuroendocrine tumors of the pancreas. Pathologies of the bile duct and duodenum such as choledocholithiasis, gallstones (cholelithiasis), choledochal Cysts, cholangiocarcinoma, bile duct strictures and ampullary cancer should be differentiated from pancreatic cancer based on imaging and biopsy findings. Metastasis from different sites and vascular causes such as abdominal aortic aneurysms may also mimic pancreatic cancer.
Epidemiology and Demographics
In the United States, the age-adjusted prevalence of invasive pancreatic cancer is 11.7 per 100,000 in 2011. Pancreatic cancer is more prevalent in males than females.
Risk Factors
Pancreatic cancer is associated with number of predisposing risk factors such as age, gender, ethnicity, and environmental exposures. The most potent risk factors for pancreatic cancer include smoking, alcoholism, increased BMI, diabetes mellitus, chronic pancreatitis and a family history of pancreatic cancer. Individuals with hereditary pancreatitis, familial pancreatic cancer, Peutz-Jeghers disease, familial atypical multiple mole melanoma syndrome (FAMMM), Von Hippel-Lindau syndrome, multiple endocrine neoplasia type 1, cystic fibrosis of the pancreas and familial cancer syndromes such as Lynch syndrome, familial adenomatous polyposis (FAP) and hereditary breast and ovarian cancer-BRCA1 and BRCA2 mutations are also at an increased risk of pancreatic cancer. Other medical conditions which pose as a risk factor for pancreatic cancer are inflammatory bowel disease, periodontal disease and peptic ulcer disease.
Screening
In asymptomatic adults who are at average risk, the USPSTF recommends against routine screening for pancreatic cancer due to the lack of mortality benefit. In high-risk individuals, with familial pancreatic cancer or in those with genetic syndromes predisposing to pancreatic cancer, screening is suggested. In high- risk groups, screening by endoscopic ultrasound (EUS), magnetic resonance imaging (MRI) and magnetic resonance cholangiopancreatography (MRCP) are recommended.
Natural History, Complications and Prognosis
The symptoms of pancreatic cancer usually develop in the sixth decade of life, and start with symptoms such as jaundice, light-colored stools, dark urine, pain in the upper or middle abdomen and back, unexplained weight loss, anorexia and fatigue.Symptoms typically develop about 20-30 years after exposure to risk factors such as smoking and alcohol. Genetic factors such as alterations in tumor suppressor genes, oncogenes and different signaling pathways are responsible. If left untreated, patients with pancreatic cancer may progress to develop exocrine pancreatic insufficiency arising from pancreatic duct obstruction leading to malabsorption, malnutrition and cachexia. Dudodenal obstruction and biliary obstruction may cause symptoms of bowel obstruction and jaundice. Common complications of pancreatic cancer may arise as a result of the disease or therapy (surgical or medical). Depending on the extent of the tumor at the time of diagnosis, the prognosis is generally regarded as poor, with complete remission extremely rare.
Diagnosis
Staging
The exocrine and endocrine tumors of the pancreas are staged with the help of a single pancreatic staging system. Staging of Pancreatic cancer aids in determining the extent of the disease and helps in arriving at the diagnosis. Staging plays a major role in planning effective treatment and assessing the prognosis. Staging of pancreatic adenocarcinoma is done with the TNM staging system based on the results of imaging modalities such as CT, MRI, PET, TUS, endoscopic studies such as EUS and biopsy with ERCP. The American Joint Committee on Cancer (AJCC) TNM system is most often used to stage cancers of the pancreas based on the information from three variables, namley the T, N, and M. T – Indicates the size of the primary tumor and the extent of it’s growth outside the pancreas and into nearby organs. N – Indicates the spread to the regional lymph nodes, where the cancers usually first spread. M – Indicates the metastasis (spread) of cancer to other parts (organs) of the body. The most common sites for the spread of pancreatic cancer are the liver, lungs, and the peritoneum.
History and Symptoms
A positive history of cigarette smoking, alcoholism, diabetes mellitus, chronic pancreatitis and family history of pancreatic cancer are considered as risk factors for developing pancreatic cancer. The most common symptoms of pancreatic cancer include mid-epigastric pain, jaundice, sudden unexplained weight loss and dark urine and light-colored or greasy stools.
Physical Examination
Patients with pancreatic cancer are usually in the sixth decade of life and appear cachectic, with signs of malnutrition. Patients mostly present with palpable abdominal mass, epigastric tenderness radiating to the back, hepatospleenomegaly and signs of metastasis in advanced stages. These signs of metastasis include left supraclavicular lymphadenopathy (Virchow’s node), palpable periumbilical mass (Sister Mary Joseph’s node), metastatic palpable mass in the rectal pouch (Blumer’s shelf) and the involvement of other nodes in the cervical area.
Laboratory Findings
Laboratory findings in pancreatic cancer patients are often non specific and include abnormal liver function tests such as elevated serum bilirubin levels (conjugated and total), elevated alkaline phosphatase and gamma-glutamyl transpeptidase levels. Patients may have evidence of malnutrition, mild normocytic normochromic anemia and elevated CA 19-9 levels.
Chest X-ray
There are no chest X-ray findings associated with Pancreatic cancer
CT
Findings on CT scan that may be suggestive of pancreatic cancer include morphological changes of the gland, destruction of the peripancreatic fat and loss of the sharp margins with surrounding structures, involvement of the regional lymph nodes and adjacent vasculature, pancreatic ductal dilatation, pancreatic atrophy and obstruction of the common bile duct . MDCT (Multi-detector row computed tomography) the imaging modality widely used in suspected pancreatic cancer patients as the pre-operative examination. MDCT is used as the primary imaging modality, and is used in conjunction with PET/CT. MDCT helps in local and distant disease assessment in a single scan. MDCT is useful in the evaluation of vascular involvement, which helps in predicting the tumor resectability.
MRI
MRI is considered when there is a diagnostic difficulty even after performing a CT scan. MRI is helpful in staging the extent and spread of pancreatic carcinoma rather than for detecting tumors or lesions less than 2 cm in size. MRI scan while determining pancreatic adenocarcinoma relies on the assessment of the size, shape, contour of the gland. MRI is helpful in characterizing cystic lesions of the pancreas and can aid in arriving at the diagnosis. MRI scan of the pancreas while assessing for pancreatic cancer presents as hypointense on T1-weighted images and hyperintense or isointense on T2-weighted images. During dynamic MR imaging, the tumor of pancreatic cancer in the early phase shows diminished enhancement and in the late phase shows gradual enhancement.
Ultrasound
Pancreatic cancer has a variable appearance on USG. The appearance relative to normal pancreatic tissue may be hypoechoic, isoechoic or hyperechoic. In majority of the cases, an ill defined hypoechoic mass is seen infiltrating into a bright pancreatic parenchyma. Pancreatic and biliary duct dilatation is seen in case of carcinoma of the head of pancreas (Double duct sign). The disadvantage of a transabdominal USG is its inability to clearly demarcate lymphadenopathy, tumor margins and the relation of the tumor to vessels around the pancreas. Endoscopic Ultrasound (EUS) has a high efficacy in the detection of tumors smaller than 2 cm, for local T and N staging, and prediction of vascular invasion. It has a higher resolution than transabdominal ultrasound, due to the small distance between the endoscope and pancreas through the wall of the duodenum. EUS plays an important role in the preoperative staging of pancreatic cancer particularly in cases where CT evaluation suggests equivocal findings. Moreover, EUS-guided fine needle aspiration biopsy (FNA) is the best modality for obtaining a tissue diagnosis.
Other imaging findings
ERCP and PTC are other imaging techniques that can be used to diagnose pancreatic cancer.
Other Diagnostic Studies
There are no other diagnostic studies associated with Pancreatic cancer.
Treatment
Medical Therapy
The therapy for pancreatic cancer depends largely on the disease progression and the stage of cancer. There are five different types of treatment for patients with pancreatic cancer: surgery, radiation therapy, chemotherapy, chemoradiation therapy and targeted therapy. In patients with pancreatic cancer, surgery is the primary modality of treatment. Extrapancreatic disease, in contrast, requires palliative therapy and curative resection is not performed in such patients. Patients with unresectable disease may be treated with chemotherapy and/or radiation therapy as a part of adjuvant or neoadjuvant therapy. Chemotherapy may be administered when surgical intervention is not deemed appropriate. The National Comprehensive Cancer Network (NCCN) has recommended guidelines for treatment in patients based on their performance status, which is a major prognostic factor. Performance status assesses extent of metastatic disease, size of the tumor and degree of weight loss. In patients with locally advanced unresectable or metastatic disease with good performance status, a combination of Leucovorin,5-fuorouracil, Oxaliplatin and Irinotecan (FOLFIRINOX) is preferred. Radiotherapy may form part of neoadjuvant therapy to attempt to shrink a tumor to a resectable state, but its use on unresectable tumors remains controversial. Neoadjuvant therapy may be used as the toxic effects of chemotherapy can be tolerated more easily before surgery as compared to after resection. Moreover, shrinkage of the tumor with neoadjuvant therapy makes resection easier and improves patient prognosis.
Surgery
The mainstay of therapy for pancreatic cancer is surgery. Various methods of surgical resection may be employed and each of these has its own sets of risks and perioperative complications. The method of surgical resection depends on the locally invasive characteristics and size of the neoplasm. The different surgical techniques that may be used for resectable pancreatic cancer include pancreaticoduodenectomy (Whipple Procedure), pylorus sparing Whipple procedure, distal pancreatectomy and total pancreatectomy. The National Comprehensive Cancer Network (NCCN) has recommended certain guidelines on resectability of pancreatic neoplasms based on resection margins, probability of cure, age and comorbidities. Curative resection is not contraindicated in all patients with vascular invasion, especially in cases with venous invasion. Extrapancreatic disease requires palliative therapy and curative resection is not performed in such patients. CA19-9 levels are not used to dictate the initial strategy for treatment of pancreatic cancer. However, elevated levels of CA19-9 can help predict the likelihood of complete resection, the prognosis of patients with resectable disease and the presence of occult metastasis.
Primary Prevention
Primary prevention of pancreatic cancer involves the cessation of cigarette smoking, regular exercise and a healthy diet as per the American Cancer Society (ACS) guidelines. Cigarette smoking is considered to be the most significant modifiable risk factor for the development of pancreatic cancer. The risk of developing pancreatic cancer becomes almost equivalent to that of a nonsmoker after five years of smoking cessation. The American Cancer Society (ACS) has issued guidelines for diet and physical activity at both individual and community levels and advocates the intake of plenty of vegetables and fruits, protein from fowl and plant sources like whole grains and consumption of tuna, mackerel or salmon that are major sources of protein and long-chain omega-3 fatty acids.
Secondary Prevention
Secondary prevention of pancreatic cancer involves proper diet based on American Cancer Society (ACS) guidelines and palliative therapy for patients. Malabsorption may arise when pancreatic duct obstruction leads to exocrine pancreatic insufficiency. The diet proposed for pancreatic cancer patients is based on ACS guidelines and advocates administration of pancreatic enzyme replacement therapy, avoidance of high-protein/high-fat diets, individualized dietary prescriptions from a registered dietitian and dietary supplementation with omega-3 fatty acids. Palliative therapy is considered as an important part of secondary prevention and includes adequate analgesia, treatment of jaundice and duodenal obstruction, arising as complications of surgery.
References
Historical Perspective
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Sudarshana Datta, MD [2]
Overview
Herophilus of Chalcedon (circa 300 B.C.), the father of scientific anatomy, was the first to describe the pancreas but he had no conception of its function. Rufus of Ephesus (circa 100 A.D) coined the term pancreas (from the Greek words pan meaning all and kreas meaning flesh). It literally means all flesh due to its homogeneous composition. In 1679, Morgagni was the first to recognize cancer of the pancreas and described the pancreas of one of his patients as a dry white pancreas of a scirrhous nature with “pretty hard” distinct lobules. By the late 1800s, the clinical symptoms, signs and histology of pancreatic cancer had been defined. Bard and Pit differentiated between duct, acinar cell and islet cell cancers. Trendelenburg was the first to successfully excise a solid tumor of the pancreas and Kappeler described the first cholecystojejunostomy performed as palliative therapy in a pancreatic cancer patient. In February 1955, Whipple performed a two stage operation for carcinoma of the ampulla, where a cholecystojejunostomy and total duodenectomy were performed. This was the first total duodenectomy to be recorded in a human subject. Whipple and Nelson subsequently performed the first ever recorded one-stage pancreaticoduodenectomy followed by occlusion of the pancreas. Post 1940, the one-stage has been modified repeatedly by surgeons world wide. Even today, the treatment of pancreatic cancer continues to be a dilemma. However, the mortality rate for pancreatoduodenal resection has declined considerably after 1970.
Historical Perspective
History of the pancreas
The history of the pancreas is as follows:[1]
- Due to its hidden retroperitoneal location, the pancreas was initially termed as the hermit organ by 20th century surgeons and ignored both as an organ and as a seat of disease.
- The pancreas was first recognized as a discrete organ by the Greeks.
- Herophilus of Chalcedon (circa 300 B.C.), the father of scientific anatomy, was the first to describe the pancreas but he had no conception of its function.
- Rufus of Ephesus (circa 100 A.D) coined the term pancreas (from the Greek words pan: all and kreas: flesh).
- The pancreas, literally means all flesh due to its homogeneous composition.
16th century:
- Vesalius described the pancreas and the vessels running through it, but knew nothing of the ductal system or its function.
17th century:
- Johann George Wirsung achieved medical immortality when he described the main duct of the human pancreas which currently bears his name.
- Regnier de Graaf utilized cannulation and studies on pancreatic secretions to demonstrate the true significance of the pancreatic duct.
18th century:
- Albrecht Von Haller pointed out that the pancreatic and bile ducts entered the intestine jointly and the function of pancreatic juice was to dilute bile.
- In 1742, Santorini illustrated the accessory duct which currently bears his name.
19th century:
- Willy Kuhne discovered trypsin.
- In 1815, Alexander discovered pancreatic lipase and its role in digestion.
History of pancreatic cancer:
The history of the pancreatic cancer is as follows:[2][3][4][5][6]
- In 1679, Morgagni was the first to recognize cancer of the pancreas and described the pancreas of one of his patients as a dry white pancreas of a scirrhous nature with “pretty hard” distinct lobules.
- Morgagni also described a distended gall bladder which is now known as the Corvosier’s sign in patients of pancreatic cancer.
- By the late 1800s, the clinical symptoms, signs and histology of pancreatic cancer had been defined. Bard and Pit differentiated between duct, acinar cell and islet cell cancers.
- In 1882, Trendelenburg was the first to successfully excise a solid tumor of the pancreas.
- In 1887, Kappeler described the first cholecystojejunostomy performed as palliative therapy in a pancreatic cancer patient.
- In 1893, Nimier published a detailed review on surgical treatment of pancreatitis and pancreatic cancer.
- In 1898, Codivilla performed a block excision of a major part of the duodenum and head of the pancreas for pancreatic carcinoma.
- in 1912, Kausch carried out the first successful two stage partial pancreaticoduodectomy , where he implanted the stump of the resected pancreas into the distal stump of the resected duodenum.
- In February 1955, Whipple performed a two stage operation for carcinoma of the ampulla, where a cholecystojejunostomy and total duodenectomy were performed. This was the first total duodenectomy to be recorded in a human subject.
- In 1940, Whipple and Nelson performed the first ever recorded one-stage pancreaticoduodenectomy followed by occlusion of the pancreas.
- Post 1940, the one-stage has been modified repeatedly by surgeons world wide.
- Even today, only one tenth of the patients with pancreatic carcinoma undergo resection.
- The mortality rate for pancreaticoduodenectomy has declined from 21 percent before 1970 to 0 percent after 1970, but the five year survival rate is still in the range of 5 to 8 percent.
References
- ↑ Lamadrid Montemayor F, Rico Nieva P (1972). “[Analgesic and antiphlogistic action of benzidamine in obstetrics]”. Ginecol Obstet Mex (in Spanish; Castilian). 32 (190): 209–12. PMID 4560737.
- ↑ Busnardo AC, DiDio LJ, Tidrick RT, Thomford NR (1983). “History of the pancreas” (PDF). American Journal of Surgery. 146 (5): 539–50. doi:10.1016/0002-9610(83)90286-6. PMID 6356946.
- ↑ Are C, Dhir M, Ravipati L (June 2011). “History of pancreaticoduodenectomy: early misconceptions, initial milestones and the pioneers”. HPB : the official journal of the International Hepato Pancreato Biliary Association. 13 (6): 377–84. doi:10.1111/j.1477-2574.2011.00305.x. PMID 21609369.
- ↑ Cameron JL, Riall TS, Coleman J, Belcher KA (July 2006). “One thousand consecutive pancreaticoduodenectomies”. Annals of surgery. 244 (1): 10–5. doi:10.1097/01.sla.0000217673.04165.ea. PMID 16794383.
- ↑ Klimstra DS, Modlin IR, Coppola D, Lloyd RV, Suster S (2010). “The pathologic classification of neuroendocrine tumors: a review of nomenclature, grading, and staging systems”. Pancreas. 39 (6): 707–12. doi:10.1097/MPA.0b013e3181ec124e. PMID 20664470.
- ↑ Fernández-del Castillo C, Morales-Oyarvide V, McGrath D, Wargo JA, Ferrone CR, Thayer SP, Lillemoe KD, Warshaw AL (September 2012). “Evolution of the Whipple procedure at the Massachusetts General Hospital”. Surgery. 152 (3 Suppl 1): S56–63. doi:10.1016/j.surg.2012.05.022. PMC 3806095. PMID 22770961.
Classification
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Aravind Reddy Kothagadi M.B.B.S[2]
Overview
Pancreatic cancers can be classified based on the production of hormones into exocrine and endocrine cancers. Pancreatic exocrine tumors include different types such as Adenocarcinoma, acinar cell carcinoma, adenosquamous carcinoma and pancreatoblastomas. Pancreatic endocrine tumors include insulinomas, glucagonomas, VIPomas, somatostatinomas and Ppomas. Additionally, early-onset pancreatic cancer is defined as pancreatic cancer that occurs before the age of 50 years.
Classification
Pancreatic cancers can be classified based on the production of hormones into exocrine and endocrine cancers:
- Types of Pancreatic Cancers:[1]
| Types of Pancreatic Cancers | |
|---|---|
| Pancreatic Exocrine Cancers | Pancreatic Endocrine Cancers (Pancreatic Neuroendocrine Tumours) |
|
|
|
|
|
|
- Types of Pancreatic Intraepithelial Neoplasia (PanIN):[1]
| Types of Pancreatic Intraepithelial Neoplasia (PanIN) |
|---|
| PanIN 1 (low grade) |
|
|
| PanIN 2 (intermediate grade) |
|
| PanIN 3 (high grade/carcinoma in situ) |
|
|
- Functional Pancreatic Neuroendocrine Tumors and their Characteristics are mentioned in the following table:[2]
| Functional Pancreatic Neuroendocrine Tumors and their Characteristics | |||
|---|---|---|---|
| Tumor type and syndrome | Location in pancreas | Signs and symptoms | Circulating biomarkers |
| Insulinoma (Whipple’s triad) |
|
|
|
| Gastrinoma (Zollinger–Ellison) |
|
|
|
| VIPoma (Verner– Morrison syndrome, WDHA) |
|
| |
| Glucagonoma |
| ||
| Somatostatinoma |
|
|
|
| Ppoma |
|
|
|
**Key
CgA- Chromogranin A
CgB- Chromogranin B
PP- Pancreatic polypeptide
| TNM Classification for Pancreatic Cancer: | |
|---|---|
| Primary tumor | |
| TX | Primary tumor cannot be assessed |
| T0 | No evidence of primary tumor |
| Tis | Carcinoma in situ |
| T1 | Tumor limited to the pancreas, ≤2 cm in greatest dimension |
| T2 | Tumor limited to the pancreas, >2 cm in greatest dimension |
| T3 | Tumor extends beyond the pancreas but without involvement of the celiac axis or the superior mesenteric artery |
| T4 | Tumor involves the celiac axis or the superior mesenteric artery (unresectable primary tumor) |
| Regional lymph nodes | |
| NX | Regional lymph nodes cannot be assessed |
| N0 | No regional lymph node metastasis |
| N1 | Regional lymph node metastasis |
| Distant metastases | |
| MX | Distant metastasis cannot be assessed |
| M0 | No distant metastasis |
| M1 | Distant metastasis |
Refrences
- ↑ 1.0 1.1 1.2 Bond-Smith G, Banga N, Hammond TM, Imber CJ (2012). “Pancreatic adenocarcinoma”. BMJ. 344: e2476. doi:10.1136/bmj.e2476. PMID 22592847.
- ↑ Ryan DP, Hong TS, Bardeesy N (2014). “Pancreatic adenocarcinoma”. N Engl J Med. 371 (11): 1039–49. doi:10.1056/NEJMra1404198. PMID 25207767.
- ↑ Seufferlein T, Bachet JB, Van Cutsem E, Rougier P, ESMO Guidelines Working Group (2012). “Pancreatic adenocarcinoma: ESMO-ESDO Clinical Practice Guidelines for diagnosis, treatment and follow-up”. Ann Oncol. 23 Suppl 7: vii33–40. doi:10.1093/annonc/mds224. PMID 22997452.
Pathophysiology
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Sudarshana Datta, MD [2]
Overview
The development of pancreatic cancer is influenced by complex interactions between several cellular signaling pathways that include inactivation of tumor suppressor genes, activation of oncogenes and deregulation of molecules in various signaling pathways. Some of the important tumor suppressor genes involved are p53, p16, p27CIP1, DPC4 and BRCA2. These tumor suppressor genes are commonly inactivated by deletion, hypermethylation or mutation. The oncogenes involved in the pathogenesis of pancreatic cancer include Ras, Cox-2, Akt-2, Notch, Cyclin- D1 genes. Signal transduction pathways such as EGFR, Akt, NF-kB and Hedgehog pathways undergo genomic alterations and crosstalk between these pathways plays an important role in pancreatic tumorigenesis.
Pathophysiology
Pathogenesis and Genetics
- The pathogenesis of pancreatic cancer involves the activation or inactivation of multiple gene subsets.[1][2][3][4][5][6][7]
- The progression and development of pancreatic cancer is influenced by complex interactions and crosstalk between several cellular signaling pathways: [8][9][10][11][12][13][14][15][8][16][17][18]
- Inactivation of tumor suppressor genes
- Activation of oncogenes
- Deregulation of molecules in various signaling pathways
Inactivation of tumor suppressor genes:
- Tumor suppressor genes may be inactivated by:
- p53[19]
- Deletion or mutation of p53 causes its inactivation in at least half of the pancreatic cancers. p53 is a tumor suppressor gene that is involved in cell cycle control and induction of apoptosis.
- p53 stimulates the production of p21WAF1, which inhibits the complex of cyclin D1 and CDK2, causing cell cycle arrest at the G1 phase and inhibition of cell growth.
- p53 inactivation causes uncontrolled cell growth and proliferation.
- The established association of Kras mutations with p53 inactivation is suggestive of crosstalk between different signaling pathways involved in pancreatic carcinogenesis.
- Loss of p53 can also determine a patient’s response to chemotherapy as its inactivation can increase resistance to certain agents of chemotherapy.
- p16 [1][20][21][22][23][24][25][26]
- p16 participates in the aggressiveness of pancreatic cancer by inhibiting cyclin D and CDK4/6 mediated phosphorylation of Rb in the G1/S transition of the cell cycle.
- Phosphorylation of Rb activates genes in the cell cycle required for DNA synthesis and lack of phosphorylation inhibits cell growth.
- 95% of the patients with pancreatic cancer have inactivated p16 with:
- 40% deletion
- 15% hypermethylation
- 40% mutation
- P16 mutation causes increased Rb phosphorylation, leading to uncontrolled cellular proliferation and increased carcinogenesis. Survival time is lesser and tumor is larger in size in patients with p16 mutation.
- p27CIP1
- p27CIP1 mutations have been implicated in pancreatic cancer by altering cellular progression in the G1 to S phase.
- DPC4
- DPC4 has been found to be deleted in approximately half of all pancreatic cancers.
- The inactivation of DPC4 causes impaired function of a gene that plays an important role in the inhibition of cell growth and angiogenesis.
- DPC4 inactivation causes increased angiogenesis and proliferation of cancer cells, with increase in the incidence of poorly differentiated tumors, thereby worsening prognosis in patients.
- BRCA2[23][27][28][29][30]
- BRCA2, a gene that participates in DNA damage repair has also been implicated in the pathogenesis of pancreatic cancer by altering the G1 to S cell cycle transition.
Activation of oncogenes:
- Oncogenes may be activated by:
- Ras oncogene[31][32][33][34][35][36]
- Ras oncogene activation is found in over ninety percent of pancreatic cancers. This oncogene is involved in mediating cell proliferation, migration and signal transduction.
- Point mutation or amplification of K-ras in the early phase of carcinogenesis leads to the formation of a constitutively activated Ras that binds to GTP and propagates uncontrolled cellular replication via downstream signaling pathways.
- Cox-2 activation[37][38][39][40][41]
- COX-2 is an inducible isoform of the COX enzyme and its synthesis is stimulated in pancreatic carcinogenic and inflammatory processes.
- Activated Ras present in ninety percent of pancreatic cancers increases COX-2 mRNA stability, hence contributing to pancreatic carcinogenesis.
- Akt-2 gene amplification
- Akt-2 gene amplification occurs in 10–15% of pancreatic cancers leading to its activation.
- Activation of Akt-2 gene stimulates cell growth, thereby accelerating progression to pancreatic cancer.
- Notch gene[42][43][44][45][46][47]
- Notch protein activation causes translocation of Notch into the nucleus. The Notch protein is bound to transcriptional factors and plays a vital role in the development of organs and pancreatic carcinogenesis by regulating the expression of target genes.
- Notch also contributes to pancreatic cancer by inhibition of apoptosis of cells.
- Up-regulation of cyclin D1
- Cyclin D1 overexpression promotes tumor cell growth and confers resistance to cisplatin, proving the effect of cyclin D1 on the pathogenesis of pancreatic cancer.[48][49]
Deregulation of EGFR signalling:[50]
- Genomic alterations of EGFR include the following:
- EGFR consists of an intracellular tyrosine kinase domain and its activation causes mobilization of molecules in different cell signaling pathways by transphosphorylation of tyrosine residues.
- Alterations of EGFR stimulate receptor tyrosine kinases and promote the development and progression of pancreatic cancer by influencing:[51][52][53][54]
- Cell cycle progression and division
- Apoptosis
- Angiogenesis
- Motility
- Invasion
- Resistance to chemotherapy
- Metastasis
Deregulation of NF-κB signalling: [55][56][57][58][59][60][61][62]
- Under normal conditions, NF-κB is sequestered in the cytoplasm under tight association with its inhibitors: p100 proteins and IκB.
- NF-κB is activated by phosphorylation of IκB and p100, resulting in the translocation of active NF-κB into the nucleus, thereby up-regulating gene transcription.
- The constitutive activation of NF-κB in pancreatic cancer causes increased expression of many genes eg. uPA , survivin, VEGF, MMP-9, involved in: [63][64][65]
- Apoptosis
- Cell growth
- Inflammation
- Stress response
- Cell differentiation
- Angiogenesis
- Invasion
- Cell survival
- Metastasis
- Pancreatic cancer cells display over expression of urokinase-type plasminogen activator (uPA), directly involved in the regulation of angiogenesis, tumor invasion and metastasis.
Deregulation of Akt signaling:
- Deregulation of Akt signaling is found in about seventy percent of the cases of pancreatic cancer and is associated with high tumor grade and prognosis.
- EGF binding leads to PI3K pathway activation.
- Activated PI3K phosphorylates phosphatidylinositides (PIP3) and this, in turn causes phosphorylation and activation of Akt.
- Phosphorylation of Akt (p-Akt) activates NF-κB and inhibits apoptosis, thereby promoting cell survival.
- Akt also regulates the NF-κB pathway via phosphorylation and activation, causing upregulation of gene transcription.
Deregulation of Hedgehog signaling:[12][66][67][68][69]
- In case of pancreatic development in the embryo, Hedgehog (Hh) signaling is an essential pathway.
- Hedgehog signaling plays an essential role in:
- Tissue morphogenesis
- Organ formation of developing gastrointestinal tract
- Deregulation of the Hh pathway leading to overexpression of Shh is known to contribute to pancreatic tumorigenesis.
- Sonic hedgehog signaling is aberrantly expressed in seventy percent of pancreas specimens from carcinoma patients, implicating its role in pancreatic tumorigenesis.
Early-Onset Pancreatic Cancer
- Approximately 30% of patients with early-onset pancreatic cancer harbor germline variants in DNA damage repair genes (e.g., BRCA1/2, PALB2), compared with approximately 15% in later-onset pancreatic cancer.[70]
Gross Pathology
The gross pathology of pancreatic adenocarcinoma, which accounts for three-fourths of all pancreatic malignancies is as follows:[71]
- Grossly, ductal adenocarcinomas of the pancreas tend to be gritty, hard, gray-white poorly defined masses that cause obstruction of the main pancreatic duct and the distal common bile duct.
- Chronic pancreatitis of the obstructed pancreatic segment arises due to obstruction of the main pancreatic duct.
- Patients do not present with malabsorption or steatorrhea as the accessory duct of Santorini can still allow bypass of the main pancreatic duct.
- The head of the pancreas is most commonly involved.
- Head lesions make up 75% of all lesions, while the rest are body/tail lesions.
- Ductal adenocarcinomas do not always originate in the main pancreatic or major branch ducts and may arise in small ducts within the peripheral acinar tissue. Hence, the term “ductal” is based on histology and not the origin.
- Early onset pancreatic cancer is associated with larger tumor size compared to later onset pancreatic cancer[72] as well as poorly differentiated histology and advanced stage presentation (stage III 62%, stage IV 55%).[73]
Microscopic Pathology
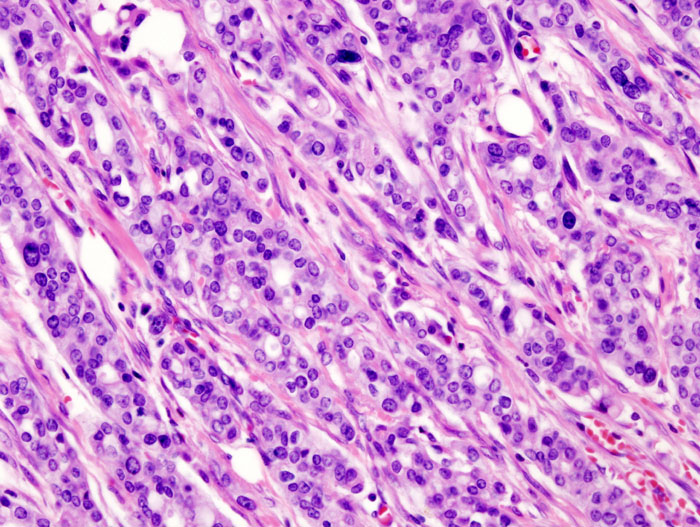
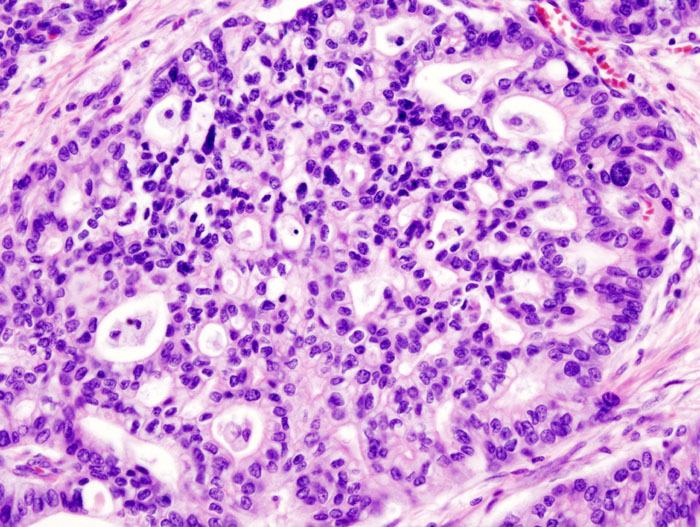
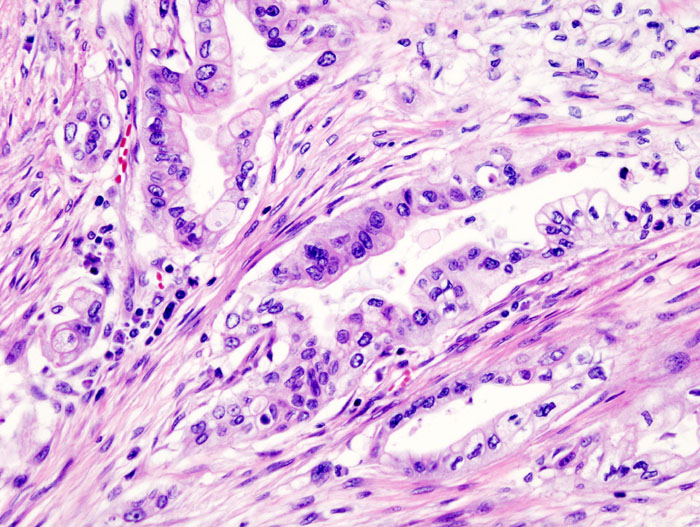
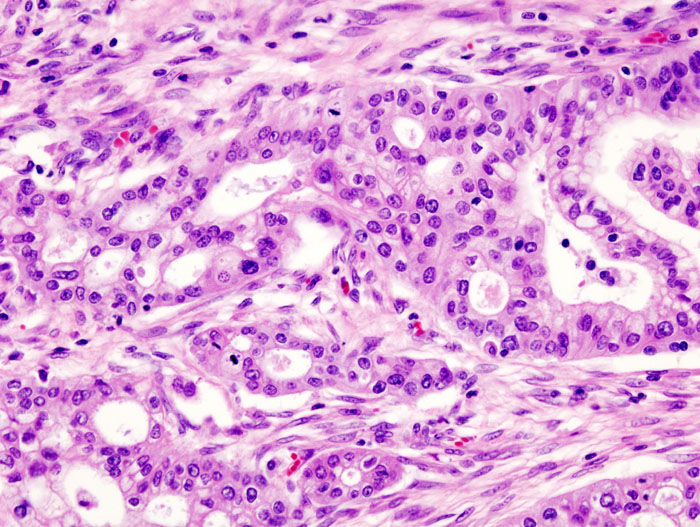
On microscopic histopathological analysis, the following features are noted:[74]
- Majority of ductal adenocarcinomas have varying degrees of mucin production and duct-like structures and present as moderate-poorly differentiated masses.
- The ductal adenocarcinomas are referred to as “desmoplastic” or “scirrhous” carcinomas due to their characteristic dense stromal fibrosis occurring due to alterations in transforming growth factor-beta (TGF-beta) signaling.
- There is typically considerable desmoplasia or formation of a dense fibrous stroma or structural tissue consisting of a range of cell types (including myofibroblasts, macrophages, lymphocytes and mast cells) and deposited material (such as type I collagen and hyaluronic acid).
- Local extension of tumor cells may occur into adjacent structures such as:[75]
- Superior mesenteric vessels
- Perineural invasion: both inside and outside the pancreas (eg, the retroperitoneum)
- Duodenum
- Portal vein
- Stomach
- Vertebral column
- Adrenal glands
- Spleen
- Transverse colon
- Lymph node spread can occur to the following sites:[76][77]
- Regional peripancreatic lymph nodes
- Mesenteric
- Perigastric
- Portahepatic
- Omental
- Microscopic study reveals the following:
- Mostly glandular appearance, may present as a solid occasionally.
- Nuclei shows the following features:
- Pleomorphism may be observed minimally.
- Nuclei is often small
- Coffee-bean appearance may be observed sometimes
- Cytoplasm shows the following features:
- Granular and abundant.
- Quasi endocrine look is observed, which may stain positive for endocrine markers
- Other features:
- May or may not present with Necrosis.
- May or may not show myxoid degeneration.
- May or may not present with cells around vessels.
-
 CC BY-SA 3.0, https://commons.wikimedia.org/w/index.php?curid=552900
CC BY-SA 3.0, https://commons.wikimedia.org/w/index.php?curid=552900 -
 CC BY-SA 3.0, https://commons.wikimedia.org/w/index.php?curid=552901
CC BY-SA 3.0, https://commons.wikimedia.org/w/index.php?curid=552901 -
 CC BY-SA 3.0, https://commons.wikimedia.org/w/index.php?curid=552904
CC BY-SA 3.0, https://commons.wikimedia.org/w/index.php?curid=552904 -
 CC BY-SA 3.0, https://commons.wikimedia.org/w/index.php?curid=552903
CC BY-SA 3.0, https://commons.wikimedia.org/w/index.php?curid=552903




References
- ↑ 1.0 1.1 Cowgill SM, Muscarella P (2003). “The genetics of pancreatic cancer”. Am. J. Surg. 186 (3): 279–86. PMID 12946833.
- ↑ Hruban RH, Petersen GM, Goggins M, Tersmette AC, Offerhaus GJ, Falatko F, Yeo CJ, Kern SE (1999). “Familial pancreatic cancer”. Ann. Oncol. 10 Suppl 4: 69–73. PMID 10436789.
- ↑ Greer JB, Whitcomb DC, Brand RE (2007). “Genetic predisposition to pancreatic cancer: a brief review”. Am. J. Gastroenterol. 102 (11): 2564–9. doi:10.1111/j.1572-0241.2007.01475.x. PMID 17958761.
- ↑ Soto JL, Barbera VM, Saceda M, Carrato A (2006). “Molecular biology of exocrine pancreatic cancer”. Clin Transl Oncol. 8 (5): 306–12. PMID 16760004.
- ↑ Shi C, Daniels JA, Hruban RH (2008). “Molecular characterization of pancreatic neoplasms”. Adv Anat Pathol. 15 (4): 185–95. doi:10.1097/PAP.0b013e31817bf57d. PMID 18580095.
- ↑ Blansfield JA, Choyke L, Morita SY, Choyke PL, Pingpank JF, Alexander HR, Seidel G, Shutack Y, Yuldasheva N, Eugeni M, Bartlett DL, Glenn GM, Middelton L, Linehan WM, Libutti SK (2007). “Clinical, genetic and radiographic analysis of 108 patients with von Hippel-Lindau disease (VHL) manifested by pancreatic neuroendocrine neoplasms (PNETs)”. Surgery. 142 (6): 814–8, discussion 818.e1–2. doi:10.1016/j.surg.2007.09.012. PMID 18063061.
- ↑ Kouvaraki MA, Shapiro SE, Cote GJ, Lee JE, Yao JC, Waguespack SG, Gagel RF, Evans DB, Perrier ND (2006). “Management of pancreatic endocrine tumors in multiple endocrine neoplasia type 1”. World J Surg. 30 (5): 643–53. doi:10.1007/s00268-006-0360-y. PMID 16680581.
- ↑ 8.0 8.1 Maitra A, Kern SE, Hruban RH (2006). “Molecular pathogenesis of pancreatic cancer”. Best Pract Res Clin Gastroenterol. 20 (2): 211–26. doi:10.1016/j.bpg.2005.10.002. PMID 16549325.
- ↑ Mimeault M, Brand RE, Sasson AA, Batra SK (2005). “Recent advances on the molecular mechanisms involved in pancreatic cancer progression and therapies”. Pancreas. 31 (4): 301–16. PMID 16258363.
- ↑ Talar-Wojnarowska R, Malecka-Panas E (2006). “Molecular pathogenesis of pancreatic adenocarcinoma: potential clinical implications”. Med. Sci. Monit. 12 (9): RA186–93. PMID 16940943.
- ↑ Neuman WL, Wasylyshyn ML, Jacoby R, Erroi F, Angriman I, Montag A, Brasitus T, Michelassi F, Westbrook CA (1991). “Evidence for a common molecular pathogenesis in colorectal, gastric, and pancreatic cancer”. Genes Chromosomes Cancer. 3 (6): 468–73. PMID 1663781.
- ↑ 12.0 12.1 Matthaios D, Zarogoulidis P, Balgouranidou I, Chatzaki E, Kakolyris S (2011). “Molecular pathogenesis of pancreatic cancer and clinical perspectives”. Oncology. 81 (3–4): 259–72. doi:10.1159/000334449. PMID 22116519.
- ↑ Konner J, O’Reilly E (2002). “Pancreatic cancer: epidemiology, genetics, and approaches to screening”. Oncology (Williston Park, N.Y.). 16 (12): 1615–22, 1631–2, discussion 1632–3, 1637–8. PMID 12520639.
- ↑ Hilgers W, Rosty C, Hahn SA (2002). “Molecular pathogenesis of pancreatic cancer”. Hematol. Oncol. Clin. North Am. 16 (1): 17–35, v. PMID 12063826.
- ↑ Hruban RH, Iacobuzio-Donahue C, Wilentz RE, Goggins M, Kern SE (2001). “Molecular pathology of pancreatic cancer”. Cancer J. 7 (4): 251–8. PMID 11561601.
- ↑ Singh S, Chitkara D, Kumar V, Behrman SW, Mahato RI (2013). “miRNA profiling in pancreatic cancer and restoration of chemosensitivity”. Cancer Lett. 334 (2): 211–20. doi:10.1016/j.canlet.2012.10.008. PMID 23073476.
- ↑ Yan L, McFaul C, Howes N, Leslie J, Lancaster G, Wong T, Threadgold J, Evans J, Gilmore I, Smart H, Lombard M, Neoptolemos J, Greenhalf W (2005). “Molecular analysis to detect pancreatic ductal adenocarcinoma in high-risk groups”. Gastroenterology. 128 (7): 2124–30. PMID 15940643.
- ↑ Jones S, Zhang X, Parsons DW, Lin JC, Leary RJ, Angenendt P, Mankoo P, Carter H, Kamiyama H, Jimeno A, Hong SM, Fu B, Lin MT, Calhoun ES, Kamiyama M, Walter K, Nikolskaya T, Nikolsky Y, Hartigan J, Smith DR, Hidalgo M, Leach SD, Klein AP, Jaffee EM, Goggins M, Maitra A, Iacobuzio-Donahue C, Eshleman JR, Kern SE, Hruban RH, Karchin R, Papadopoulos N, Parmigiani G, Vogelstein B, Velculescu VE, Kinzler KW (2008). “Core signaling pathways in human pancreatic cancers revealed by global genomic analyses”. Science. 321 (5897): 1801–6. doi:10.1126/science.1164368. PMC 2848990. PMID 18772397.
- ↑ Li Y, Bhuiyan M, Vaitkevicius VK, Sarkar FH (1998). “Molecular analysis of the p53 gene in pancreatic adenocarcinoma”. Diagn. Mol. Pathol. 7 (1): 4–9. PMID 9646028.
- ↑ Garcea G, Neal CP, Pattenden CJ, Steward WP, Berry DP (2005). “Molecular prognostic markers in pancreatic cancer: a systematic review”. Eur. J. Cancer. 41 (15): 2213–36. doi:10.1016/j.ejca.2005.04.044. PMID 16146690.
- ↑ Schutte M, Hruban RH, Geradts J, Maynard R, Hilgers W, Rabindran SK, Moskaluk CA, Hahn SA, Schwarte-Waldhoff I, Schmiegel W, Baylin SB, Kern SE, Herman JG (1997). “Abrogation of the Rb/p16 tumor-suppressive pathway in virtually all pancreatic carcinomas”. Cancer Res. 57 (15): 3126–30. PMID 9242437.
- ↑ Goggins M, Kern SE, Offerhaus JA, Hruban RH (1999). “Progress in cancer genetics: lessons from pancreatic cancer”. Ann. Oncol. 10 Suppl 4: 4–8. PMID 10436774.
- ↑ 23.0 23.1 Klein AP, Hruban RH, Brune KA, Petersen GM, Goggins M (2001). “Familial pancreatic cancer”. Cancer J. 7 (4): 266–73. PMID 11561603.
- ↑ Mangray S, King TC (1998). “Molecular pathobiology of pancreatic adenocarcinoma”. Front. Biosci. 3: D1148–60. PMID 9820739.
- ↑ Wang C, Lu X (2000). “[Alterations of the p16 gene for the carcinogenesis in pancreas]”. Zhongguo Yi Xue Ke Xue Yuan Xue Bao (in Chinese). 22 (5): 491–3. PMID 12903437.
- ↑ Gerdes B, Bartsch DK, Ramaswamy A, Kersting M, Wild A, Schuermann M, Frey M, Rothmund M (2000). “Multiple primary tumors as an indicator for p16INK4a germline mutations in pancreatic cancer patients?”. Pancreas. 21 (4): 369–75. PMID 11075991.
- ↑ Goggins M, Schutte M, Lu J, Moskaluk CA, Weinstein CL, Petersen GM, Yeo CJ, Jackson CE, Lynch HT, Hruban RH, Kern SE (1996). “Germline BRCA2 gene mutations in patients with apparently sporadic pancreatic carcinomas”. Cancer Res. 56 (23): 5360–4. PMID 8968085.
- ↑ Hahn SA, Greenhalf B, Ellis I, Sina-Frey M, Rieder H, Korte B, Gerdes B, Kress R, Ziegler A, Raeburn JA, Campra D, Grützmann R, Rehder H, Rothmund M, Schmiegel W, Neoptolemos JP, Bartsch DK (2003). “BRCA2 germline mutations in familial pancreatic carcinoma”. J. Natl. Cancer Inst. 95 (3): 214–21. PMID 12569143.
- ↑ Murphy KM, Brune KA, Griffin C, Sollenberger JE, Petersen GM, Bansal R, Hruban RH, Kern SE (2002). “Evaluation of candidate genes MAP2K4, MADH4, ACVR1B, and BRCA2 in familial pancreatic cancer: deleterious BRCA2 mutations in 17%”. Cancer Res. 62 (13): 3789–93. PMID 12097290.
- ↑ Hruban RH, Petersen GM, Ha PK, Kern SE (1998). “Genetics of pancreatic cancer. From genes to families”. Surg. Oncol. Clin. N. Am. 7 (1): 1–23. PMID 9443984.
- ↑ Kojima K, Vickers SM, Adsay NV, Jhala NC, Kim HG, Schoeb TR, Grizzle WE, Klug CA (2007). “Inactivation of Smad4 accelerates Kras(G12D)-mediated pancreatic neoplasia”. Cancer Res. 67 (17): 8121–30. doi:10.1158/0008-5472.CAN-06-4167. PMID 17804724.
- ↑ Almoguera C, Shibata D, Forrester K, Martin J, Arnheim N, Perucho M (1988). “Most human carcinomas of the exocrine pancreas contain mutant c-K-ras genes”. Cell. 53 (4): 549–54. PMID 2453289.
- ↑ Laghi L, Orbetegli O, Bianchi P, Zerbi A, Di Carlo V, Boland CR, Malesci A (2002). “Common occurrence of multiple K-RAS mutations in pancreatic cancers with associated precursor lesions and in biliary cancers”. Oncogene. 21 (27): 4301–6. doi:10.1038/sj.onc.1205533. PMID 12082617.
- ↑ Cheng RF, Wang J, Zhang JY, Sun L, Zhao YR, Qiu ZQ, Sun BC, Sun Y (2016). “MicroRNA-506 is up-regulated in the development of pancreatic ductal adenocarcinoma and is associated with attenuated disease progression”. Chin J Cancer. 35 (1): 64. doi:10.1186/s40880-016-0128-9. PMC 4930606. PMID 27371108.
- ↑ Hayashi N, Egami H, Ogawa M (2002). “[Genetics of pancreatic cancer: recent advances in molecular diagnosis]”. Nihon Geka Gakkai Zasshi (in Japanese). 103 (6): 476–81. PMID 12094699.
- ↑ Howe JR, Conlon KC (1997). “The molecular genetics of pancreatic cancer”. Surg Oncol. 6 (1): 1–18. PMID 9364657.
- ↑ El-Rayes BF, Ali S, Sarkar FH, Philip PA (2004). “Cyclooxygenase-2-dependent and -independent effects of celecoxib in pancreatic cancer cell lines”. Mol. Cancer Ther. 3 (11): 1421–6. PMID 15542781.
- ↑ Hussain T, Gupta S, Adhami VM, Mukhtar H (2005). “Green tea constituent epigallocatechin-3-gallate selectively inhibits COX-2 without affecting COX-1 expression in human prostate carcinoma cells”. Int. J. Cancer. 113 (4): 660–9. doi:10.1002/ijc.20629. PMID 15455372.
- ↑ Wei D, Wang L, He Y, Xiong HQ, Abbruzzese JL, Xie K (2004). “Celecoxib inhibits vascular endothelial growth factor expression in and reduces angiogenesis and metastasis of human pancreatic cancer via suppression of Sp1 transcription factor activity”. Cancer Res. 64 (6): 2030–8. PMID 15026340.
- ↑ Okami J, Yamamoto H, Fujiwara Y, Tsujie M, Kondo M, Noura S, Oshima S, Nagano H, Dono K, Umeshita K, Ishikawa O, Sakon M, Matsuura N, Nakamori S, Monden M (1999). “Overexpression of cyclooxygenase-2 in carcinoma of the pancreas”. Clin. Cancer Res. 5 (8): 2018–24. PMID 10473081.
- ↑ Inoue S, Tezel E, Nakao A (2001). “Molecular diagnosis of pancreatic cancer”. Hepatogastroenterology. 48 (40): 933–8. PMID 11490843.
- ↑ Wang Z, Banerjee S, Li Y, Rahman KM, Zhang Y, Sarkar FH (2006). “Down-regulation of notch-1 inhibits invasion by inactivation of nuclear factor-kappaB, vascular endothelial growth factor, and matrix metalloproteinase-9 in pancreatic cancer cells”. Cancer Res. 66 (5): 2778–84. doi:10.1158/0008-5472.CAN-05-4281. PMID 16510599.
- ↑ Büchler P, Gazdhar A, Schubert M, Giese N, Reber HA, Hines OJ, Giese T, Ceyhan GO, Müller M, Büchler MW, Friess H (2005). “The Notch signaling pathway is related to neurovascular progression of pancreatic cancer”. Ann. Surg. 242 (6): 791–800, discussion 800–1. PMC 1409885. PMID 16327489.
- ↑ Miyamoto Y, Maitra A, Ghosh B, Zechner U, Argani P, Iacobuzio-Donahue CA, Sriuranpong V, Iso T, Meszoely IM, Wolfe MS, Hruban RH, Ball DW, Schmid RM, Leach SD (2003). “Notch mediates TGF alpha-induced changes in epithelial differentiation during pancreatic tumorigenesis”. Cancer Cell. 3 (6): 565–76. PMID 12842085.
- ↑ Wang Z, Zhang Y, Banerjee S, Li Y, Sarkar FH (2006). “Inhibition of nuclear factor kappab activity by genistein is mediated via Notch-1 signaling pathway in pancreatic cancer cells”. Int. J. Cancer. 118 (8): 1930–6. doi:10.1002/ijc.21589. PMID 16284950.
- ↑ Wang Z, Zhang Y, Banerjee S, Li Y, Sarkar FH (2006). “Notch-1 down-regulation by curcumin is associated with the inhibition of cell growth and the induction of apoptosis in pancreatic cancer cells”. Cancer. 106 (11): 2503–13. doi:10.1002/cncr.21904. PMID 16628653.
- ↑ Wang Z, Zhang Y, Li Y, Banerjee S, Liao J, Sarkar FH (2006). “Down-regulation of Notch-1 contributes to cell growth inhibition and apoptosis in pancreatic cancer cells”. Mol. Cancer Ther. 5 (3): 483–93. doi:10.1158/1535-7163.MCT-05-0299. PMID 16546962.
- ↑ Biliran H, Wang Y, Banerjee S, Xu H, Heng H, Thakur A, Bollig A, Sarkar FH, Liao JD (2005). “Overexpression of cyclin D1 promotes tumor cell growth and confers resistance to cisplatin-mediated apoptosis in an elastase-myc transgene-expressing pancreatic tumor cell line”. Clin. Cancer Res. 11 (16): 6075–86. doi:10.1158/1078-0432.CCR-04-2419. PMID 16115953.
- ↑ Kornmann M, Arber N, Korc M (1998). “Inhibition of basal and mitogen-stimulated pancreatic cancer cell growth by cyclin D1 antisense is associated with loss of tumorigenicity and potentiation of cytotoxicity to cisplatinum”. J. Clin. Invest. 101 (2): 344–52. doi:10.1172/JCI1323. PMC 508573. PMID 9435306.
- ↑ Bruns CJ, Harbison MT, Davis DW, Portera CA, Tsan R, McConkey DJ, Evans DB, Abbruzzese JL, Hicklin DJ, Radinsky R (2000). “Epidermal growth factor receptor blockade with C225 plus gemcitabine results in regression of human pancreatic carcinoma growing orthotopically in nude mice by antiangiogenic mechanisms”. Clin. Cancer Res. 6 (5): 1936–48. PMID 10815919.
- ↑ Marshall J (2006). “Clinical implications of the mechanism of epidermal growth factor receptor inhibitors”. Cancer. 107 (6): 1207–18. doi:10.1002/cncr.22133. PMID 16909423.
- ↑ Wang Z, Sengupta R, Banerjee S, Li Y, Zhang Y, Rahman KM, Aboukameel A, Mohammad R, Majumdar AP, Abbruzzese JL, Sarkar FH (2006). “Epidermal growth factor receptor-related protein inhibits cell growth and invasion in pancreatic cancer”. Cancer Res. 66 (15): 7653–60. doi:10.1158/0008-5472.CAN-06-1019. PMID 16885366.
- ↑ Zhang Y, Banerjee S, Wang Z, Xu H, Zhang L, Mohammad R, Aboukameel A, Adsay NV, Che M, Abbruzzese JL, Majumdar AP, Sarkar FH (2006). “Antitumor activity of epidermal growth factor receptor-related protein is mediated by inactivation of ErbB receptors and nuclear factor-kappaB in pancreatic cancer”. Cancer Res. 66 (2): 1025–32. doi:10.1158/0008-5472.CAN-05-2968. PMID 16424038.
- ↑ Zhang Y, Banerjee S, Wang ZW, Marciniak DJ, Majumdar AP, Sarkar FH (2005). “Epidermal growth factor receptor-related protein inhibits cell growth and induces apoptosis of BxPC3 pancreatic cancer cells”. Cancer Res. 65 (9): 3877–82. doi:10.1158/0008-5472.CAN-04-3654. PMID 15867387.
- ↑ Wang W, Abbruzzese JL, Evans DB, Chiao PJ (1999). “Overexpression of urokinase-type plasminogen activator in pancreatic adenocarcinoma is regulated by constitutively activated RelA”. Oncogene. 18 (32): 4554–63. doi:10.1038/sj.onc.1202833. PMID 10467400.
- ↑ Bava SV, Puliappadamba VT, Deepti A, Nair A, Karunagaran D, Anto RJ (2005). “Sensitization of taxol-induced apoptosis by curcumin involves down-regulation of nuclear factor-kappaB and the serine/threonine kinase Akt and is independent of tubulin polymerization”. J. Biol. Chem. 280 (8): 6301–8. doi:10.1074/jbc.M410647200. PMID 15590651.
- ↑ Fahy BN, Schlieman MG, Virudachalam S, Bold RJ (2004). “Inhibition of AKT abrogates chemotherapy-induced NF-kappaB survival mechanisms: implications for therapy in pancreatic cancer”. J. Am. Coll. Surg. 198 (4): 591–9. doi:10.1016/j.jamcollsurg.2003.12.005. PMID 15051014.
- ↑ Fujioka S, Sclabas GM, Schmidt C, Frederick WA, Dong QG, Abbruzzese JL, Evans DB, Baker C, Chiao PJ (2003). “Function of nuclear factor kappaB in pancreatic cancer metastasis”. Clin. Cancer Res. 9 (1): 346–54. PMID 12538487.
- ↑ Karin M (2006). “Nuclear factor-kappaB in cancer development and progression”. Nature. 441 (7092): 431–6. doi:10.1038/nature04870. PMID 16724054.
- ↑ Li L, Aggarwal BB, Shishodia S, Abbruzzese J, Kurzrock R (2004). “Nuclear factor-kappaB and IkappaB kinase are constitutively active in human pancreatic cells, and their down-regulation by curcumin (diferuloylmethane) is associated with the suppression of proliferation and the induction of apoptosis”. Cancer. 101 (10): 2351–62. doi:10.1002/cncr.20605. PMID 15476283.
- ↑ Li Y, Ahmed F, Ali S, Philip PA, Kucuk O, Sarkar FH (2005). “Inactivation of nuclear factor kappaB by soy isoflavone genistein contributes to increased apoptosis induced by chemotherapeutic agents in human cancer cells”. Cancer Res. 65 (15): 6934–42. doi:10.1158/0008-5472.CAN-04-4604. PMID 16061678.
- ↑ Li Y, Chinni SR, Sarkar FH (2005). “Selective growth regulatory and pro-apoptotic effects of DIM is mediated by AKT and NF-kappaB pathways in prostate cancer cells”. Front. Biosci. 10: 236–43. PMID 15574364.
- ↑ Liptay S, Weber CK, Ludwig L, Wagner M, Adler G, Schmid RM (2003). “Mitogenic and antiapoptotic role of constitutive NF-kappaB/Rel activity in pancreatic cancer”. Int. J. Cancer. 105 (6): 735–46. doi:10.1002/ijc.11081. PMID 12767057.
- ↑ {{cite journal |vauthors=Rahman KW, Sarkar FH |title=Inhibition of nuclear translocation of nuclear factor-{kappa}B contributes to 3,3′-diindolylmethane-induced apoptosis in breast cancer cells |journal=Cancer Res. |volume=65 |issue=1 |pages=364–71 |year=2005 |pmid=15665315 |doi= |url=}}
- ↑ Zhang H, Morisaki T, Nakahara C, Matsunaga H, Sato N, Nagumo F, Tadano J, Katano M (2003). “PSK-mediated NF-kappaB inhibition augments docetaxel-induced apoptosis in human pancreatic cancer cells NOR-P1”. Oncogene. 22 (14): 2088–96. doi:10.1038/sj.onc.1206310. PMID 12687011.
- ↑ Nakashima H, Nakamura M, Yamaguchi H, Yamanaka N, Akiyoshi T, Koga K, Yamaguchi K, Tsuneyoshi M, Tanaka M, Katano M (2006). “Nuclear factor-kappaB contributes to hedgehog signaling pathway activation through sonic hedgehog induction in pancreatic cancer”. Cancer Res. 66 (14): 7041–9. doi:10.1158/0008-5472.CAN-05-4588. PMID 16849549.
- ↑ Thayer SP, di Magliano MP, Heiser PW, Nielsen CM, Roberts DJ, Lauwers GY, Qi YP, Gysin S, Fernández-del Castillo C, Yajnik V, Antoniu B, McMahon M, Warshaw AL, Hebrok M (2003). “Hedgehog is an early and late mediator of pancreatic cancer tumorigenesis”. Nature. 425 (6960): 851–6. doi:10.1038/nature02009. PMC 3688051. PMID 14520413.
- ↑ Berman DM, Karhadkar SS, Maitra A, Montes De Oca R, Gerstenblith MR, Briggs K, Parker AR, Shimada Y, Eshleman JR, Watkins DN, Beachy PA (2003). “Widespread requirement for Hedgehog ligand stimulation in growth of digestive tract tumours”. Nature. 425 (6960): 846–51. doi:10.1038/nature01972. PMID 14520411.
- ↑ Mathew E, Zhang Y, Holtz AM, Kane KT, Song JY, Allen BL, Pasca di Magliano M (2014). “Dosage-dependent regulation of pancreatic cancer growth and angiogenesis by hedgehog signaling”. Cell Rep. 9 (2): 484–94. doi:10.1016/j.celrep.2014.09.010. PMC 4362534. PMID 25310976.
- ↑ Castet F, Fabregat-Franco C, Castillo G, et al. Clinical and genomic characterisation of early-onset pancreatic cancer. Eur J Cancer. 2023;194:113338. doi:10.1016/j.ejca.2023.113338
- ↑ Esposito I, Konukiewitz B, Schlitter AM, Klöppel G (2014). “Pathology of pancreatic ductal adenocarcinoma: facts, challenges, and future developments”. World J. Gastroenterol. 20 (38): 13833–41. doi:10.3748/wjg.v20.i38.13833. PMC 4194566. PMID 25320520.
- ↑ Zironda A, Zhang C, Day C, et al. Early vs conventional onset pancreatic ductal adenocarcinoma: analysis of surgical and oncologic outcomes in patients undergoing curative intent resection. HPB (Oxford). 2024;26(1):145-153. doi:10. 1016/j.hpb.2023.09.010
- ↑ Ordonez JE, Hester CA, Zhu H, et al. Clinicopathologic features and outcomes of early-onset pancreatic adenocarcinoma in the United States. Ann Surg Oncol. 2020;27(6):1997- 2006. doi:10.1245/s10434-019-08096-y
- ↑ Rossi ML, Rehman AA, Gondi CS (2014). “Therapeutic options for the management of pancreatic cancer”. World J. Gastroenterol. 20 (32): 11142–59. doi:10.3748/wjg.v20.i32.11142. PMC 4145755. PMID 25170201.
- ↑ Oda Y, Aishima S, Morimatsu K, Shindo K, Fujino M, Mizuuchi Y, Hattori M, Miyazaki T, Tanaka M, Oda Y (2014). “Pancreatic intraepithelial neoplasia in the background of invasive ductal carcinoma of the pancreas as a prognostic factor”. Histopathology. 65 (3): 389–97. doi:10.1111/his.12397. PMID 24931343.
- ↑ Yachida S, Jones S, Bozic I, Antal T, Leary R, Fu B, Kamiyama M, Hruban RH, Eshleman JR, Nowak MA, Velculescu VE, Kinzler KW, Vogelstein B, Iacobuzio-Donahue CA (2010). “Distant metastasis occurs late during the genetic evolution of pancreatic cancer”. Nature. 467 (7319): 1114–7. doi:10.1038/nature09515. PMC 3148940. PMID 20981102.
- ↑ Campbell PJ, Yachida S, Mudie LJ, Stephens PJ, Pleasance ED, Stebbings LA, Morsberger LA, Latimer C, McLaren S, Lin ML, McBride DJ, Varela I, Nik-Zainal SA, Leroy C, Jia M, Menzies A, Butler AP, Teague JW, Griffin CA, Burton J, Swerdlow H, Quail MA, Stratton MR, Iacobuzio-Donahue C, Futreal PA (2010). “The patterns and dynamics of genomic instability in metastatic pancreatic cancer”. Nature. 467 (7319): 1109–13. doi:10.1038/nature09460. PMC 3137369. PMID 20981101.
Causes
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Aravind Reddy Kothagadi M.B.B.S[2]
Overview
Pancreatic cancer may be caused by the inactivation of tumor suppressor genes such as p53, p16, p27CIP1 and BRCA2. Oncogenes such as Ras , Cox-2, Akt-2, Notch and Cyclin D1 may undergo activation and lead to the development of pancreatic cancer. Deregulation and crosstalk between different signal transduction pathways due to genomic alterations also have a proven role in the causation of pancreatic cancer.
Causes
- Pancreatic cancer may be caused by the following:[1][2][3]
- Inactivation of tumor suppressor genes
- Activation of oncogenes
- Deregulation of molecules in various signaling pathways
- Inactivation of tumor suppressor genes:
- Tumor suppressor genes may be inactivated by:
- Tumor suppressor genes:
- Deregulation of molecules in various signaling pathways:
References
- ↑ Yabar CS, Winter JM (2016). “Pancreatic Cancer: A Review”. Gastroenterol Clin North Am. 45 (3): 429–45. doi:10.1016/j.gtc.2016.04.003. PMID 27546841.
- ↑ Ryan DP, Hong TS, Bardeesy N (2014). “Pancreatic adenocarcinoma”. N Engl J Med. 371 (11): 1039–49. doi:10.1056/NEJMra1404198. PMID 25207767.
- ↑ Goral V (2015). “Pancreatic Cancer: Pathogenesis and Diagnosis”. Asian Pac J Cancer Prev. 16 (14): 5619–24. PMID 26320426.
Differentiating Pancreatic Cancer from other Disorders
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Sudarshana Datta, MD [2]
Overview
Pancreatic cancer must be distinguished from other pancreatobiliary pathologies that cause abdominal pain and jaundice such as acute suppurative cholangitis, acute cholecystitis, cholelithiasis, chronic pancreatitis, primary biliary cirrhosis and primary sclerosing cholangitis. Pancreatic cancer must also be differentiated from other pancreatic pathologies such as autoimmune pancreatitis, pancreatic pseudocyst, and neuroendocrine tumors of the pancreas. Pathologies of the bile duct and duodenum such as Choledocholithiasis, gallstones (cholelithiasis), choledochal cysts, Cholangiocarcinoma, Bile duct strictures and ampullary cancer should be differentiated from pancreatic cancer based on imaging and biopsy findings. Metastasis from different sites and vascular causes such as abdominal aortic aneurysms may also mimic pancreatic cancer.
Differentiating Pancreatic Cancer from other Diseases
Pancreatic cancer may also be distinguished from other causes of abdominal pain and jaundice as depicted in the table below:
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Differentials based on weight loss, nausea, vomiting, diarrhea, fatigue and abdominal pain
Pancreatic carcinoma should be differentiated from other diseases presenting with weight loss, nausea, vomiting, diarrhea, fatigue and abdominal pain. The differentials include the following:
| Disease | Clinical manifestations | Diagnosis | Comments | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Symptoms | Signs | |||||||||||||||
| Abdominal Pain | Fever | Rigors and chills | Nausea or vomiting | Jaundice | Constipation | Diarrhea | Weight loss | GI bleeding | Hypo-
tension |
Guarding | Rebound Tenderness | Bowel sounds | Lab Findings | Imaging | ||
| Chronic pancreatitis | Epigastric | − | − | ± | ± | − | + | + | − | − | − | − | N | CT scan
|
| |
| Pancreatic carcinoma | Epigastric | − | − | + | + | − | + | + | − | − | − | − | N |
Skin manifestations may include: | ||
| Dumping syndrome | Lower and then diffuse | − | − | + | − | − | + | + | − | + | − | − | Hyperactive |
|
|
|
Abbreviations:
RUQ= Right upper quadrant of the abdomen, LUQ= Left upper quadrant, LLQ= Left lower quadrant, RLQ= Right lower quadrant, LFT= Liver function test, SIRS= Systemic inflammatory response syndrome, ERCP= Endoscopic retrograde cholangiopancreatography, IV= Intravenous, N= Normal, AMA= Anti mitochondrial antibodies, LDH= Lactate dehydrogenase, GI= Gastrointestinal, CXR= Chest X ray, IgA= Immunoglobulin A, IgG= Immunoglobulin G, IgM= Immunoglobulin M, CT= Computed tomography, PMN= Polymorphonuclear cells, ESR= Erythrocyte sedimentation rate, CRP= C-reactive protein, TS= Transferrin saturation, SF= Serum Ferritin, SMA= Superior mesenteric artery, SMV= Superior mesenteric vein, ECG= Electrocardiogram
To review a comprehensive differential diagnosis of diseases presenting with abdominal pain, click here.
Differentiating Pancreatic Carcinoma on the basis of involved Organ
The differentials for pancreatic cancer mainly involve pathologies of the pancreas, bile duct, duodenum, lymphovascular tissue or metastasis from other sites. It is difficult to differentiate pancreatic cancer from other neoplasms as they all present with non specific constitutional symptoms. Hence, differentiation is primarily based on anatomic location:[1][2][3][4][5][6][7][8][9][10][11][12][13][14][15][16][17][18][19][20][21][22][23][24][25][26][27][28]
| Origin | Disease | Diagnostic study of choice |
|---|---|---|
| Pancreas |
| |
| Bile duct | ||
| Duodenum |
|
|
| Lymphovascular
tissue |
| |
| Metastasis |
References
- ↑ He XK, Ding Y, Sun LM (2017). “Contrast-enhanced endoscopic ultrasound for differential diagnosis of pancreatic cancer: an updated meta-analysis”. Oncotarget. 8 (39): 66392–66401. doi:10.18632/oncotarget.18915. PMC 5630421. PMID 29029521.
- ↑ Steinman J, Zaheer A, Kluger MD, Remotti H, Hecht EM (2017). “Rare pancreatic tumors”. Abdom Radiol (NY). doi:10.1007/s00261-017-1342-x. PMID 29022085.
- ↑ Ran L, Zhao W, Zhao Y, Bu H (2017). “Value of contrast-enhanced ultrasound in differential diagnosis of solid lesions of pancreas (SLP): A systematic review and a meta-analysis”. Medicine (Baltimore). 96 (28): e7463. doi:10.1097/MD.0000000000007463. PMC 5515757. PMID 28700485.
- ↑ Kołodziejczyk E, Wejnarska K, Oracz G (2016). “Autoimmune pancreatitis in the paediatric population – review of the literature and own experience”. Dev Period Med. 20 (4): 279–286. PMID 28216481.
- ↑ Zhu L, Xue HD, Liu W, Wang X, Sui X, Wang Q, Zhang D, Li P, Jin ZY (2017). “Enhancing pancreatic mass with normal serum CA19-9: key MDCT features to characterize pancreatic neuroendocrine tumours from its mimics”. Radiol Med. 122 (5): 337–344. doi:10.1007/s11547-017-0734-x. PMID 28197876.
- ↑ Sano I, Katanuma A, Yane K, Kin T, Nagai K, Yamazaki H, Koga H, Kitagawa K, Yokoyama K, Ikarashi S, Takahashi K, Maguchi H, Omori Y, Shinohara T (2017). “Pancreatic Metastasis from Rectal Cancer that was Diagnosed by Endoscopic Ultrasonography-guided Fine Needle Aspiration (EUS-FNA)”. Intern. Med. 56 (3): 301–305. doi:10.2169/internalmedicine.56.7213. PMC 5348454. PMID 28154274.
- ↑ Salaria SN, Shi C (2016). “Pancreatic Neuroendocrine Tumors”. Surg Pathol Clin. 9 (4): 595–617. doi:10.1016/j.path.2016.05.006. PMID 27926362.
- ↑ Kawasaki K, Kawaguchi Y, Suzuki Y, Tanaka N (2016). “Renal neuroendocrine tumour and synchronous pancreas metastasis: histopathological diagnosis using prostatic acid phosphatase”. BMJ Case Rep. 2016. doi:10.1136/bcr-2016-214759. PMID 27803081.
- ↑ Nassour I, Choti MA (2016). “Diagnosis and Treatment of Pancreatic Cystic Neoplasms”. JAMA. 316 (12): 1326. doi:10.1001/jama.2016.9130. PMID 27673319.
- ↑ Javadi S, Menias CO, Korivi BR, Shaaban AM, Patnana M, Alhalabi K, Elsayes KM (2017). “Pancreatic Calcifications and Calcified Pancreatic Masses: Pattern Recognition Approach on CT”. AJR Am J Roentgenol. 209 (1): 77–87. doi:10.2214/AJR.17.17862. PMID 28418702.
- ↑ Bergmann F (2016). “[Pancreatic acinar neoplasms : Comparative molecular characterization]”. Pathologe (in German). 37 (Suppl 2): 191–195. doi:10.1007/s00292-016-0235-z. PMID 27807633.
- ↑ Cheng SK, Chuah KL (2016). “Metastatic Renal Cell Carcinoma to the Pancreas: A Review”. Arch. Pathol. Lab. Med. 140 (6): 598–602. doi:10.5858/arpa.2015-0135-RS. PMID 27232353.
- ↑ Haage P, Schwartz CA, Scharwächter C (2016). “[Ductal adenocarcinoma and unusual differential diagnosis]”. Radiologe (in German). 56 (4): 325–37. doi:10.1007/s00117-016-0090-1. PMID 27000276.
- ↑ Scialpi M, Reginelli A, D’Andrea A, Gravante S, Falcone G, Baccari P, Manganaro L, Palumbo B, Cappabianca S (2016). “Pancreatic tumors imaging: An update”. Int J Surg. 28 Suppl 1: S142–55. doi:10.1016/j.ijsu.2015.12.053. PMID 26777740.
- ↑ Senosiain Lalastra C, Foruny Olcina JR (2015). “[Autoimmune pancreatitis]”. Gastroenterol Hepatol (in Spanish; Castilian). 38 (9): 549–55. doi:10.1016/j.gastrohep.2015.01.006. PMID 25799073.
- ↑ Barbier L, Delpero JR (2014). “[Pancreatic tumours]”. Rev Prat (in French). 64 (9): 1307–12. PMID 25638877.
- ↑ Díte P, Uvírová M, Bojková M, Novotný I, Dvorácková J, Kianicka B, Nechutová H, Dovrtelová L, Floreánová K, Martínek A (2014). “Differentiating autoimmune pancreatitis from pancreatic cancer”. Minerva Gastroenterol Dietol. 60 (4): 247–53. PMID 25288201.
- ↑ Lalwani N, Mannelli L, Ganeshan DM, Shanbhogue AK, Dighe MK, Tiwari HA, Maximin S, Monti S, Ragucci M, Prasad SR (2015). “Uncommon pancreatic tumors and pseudotumors”. Abdom Imaging. 40 (1): 167–80. doi:10.1007/s00261-014-0189-7. PMID 25063236.
- ↑ Dite P, Nechutova H, Uvirova M, Dvorackova J, Kianicka B, Martinek A (2014). “Autoimmune pancreatitis”. Biomed Pap Med Fac Univ Palacky Olomouc Czech Repub. 158 (1): 17–22. doi:10.5507/bp.2013.094. PMID 24572485.
- ↑ Mastoraki A, Tzortzopoulou A, Tsela S, Danias N, Sakorafas G, Smyrniotis V, Arkadopoulos N (2014). “Hereditary pancreatitis: dilemmas in differential diagnosis and therapeutic approach”. J Gastrointest Cancer. 45 (1): 22–6. doi:10.1007/s12029-013-9559-6. PMID 24242859.
- ↑ Beyer G, Menzel J, Krüger PC, Ribback S, Lerch MM, Mayerle J (2013). “[Autoimmune pancreatitis]”. Dtsch. Med. Wochenschr. (in German). 138 (46): 2359–70, quiz 2371–4. doi:10.1055/s-0033-1349475. PMID 24193862.
- ↑ Al-Hawary MM, Kaza RK, Azar SF, Ruma JA, Francis IR (2013). “Mimics of pancreatic ductal adenocarcinoma”. Cancer Imaging. 13 (3): 342–9. doi:10.1102/1470-7330.2013.9012. PMC 3800430. PMID 24060833.
- ↑ Bednar F, Scheiman JM, McKenna BJ, Simeone DM (2013). “Breast cancer metastases to the pancreas”. J. Gastrointest. Surg. 17 (10): 1826–31. doi:10.1007/s11605-013-2291-5. PMID 23918083.
- ↑ DiMagno MJ, DiMagno EP (2013). “Chronic pancreatitis”. Curr. Opin. Gastroenterol. 29 (5): 531–6. doi:10.1097/MOG.0b013e3283639370. PMC 4387887. PMID 23852141.
- ↑ Berger AW, Seufferlein T, Kleger A (2017). “[Cystic pancreatic tumors: diagnostics and new biomarkers]”. Chirurg (in German). 88 (11): 905–912. doi:10.1007/s00104-017-0493-1. PMID 28831506.
- ↑ Nougaret S, Mannelli L, Pierredon MA, Schembri V, Guiu B (2016). “Cystic pancreatic lesions: From increased diagnosis rate to new dilemmas”. Diagn Interv Imaging. 97 (12): 1275–1285. doi:10.1016/j.diii.2016.08.017. PMID 27840080.
- ↑ Xu MM, Yin S, Siddiqui AA, Salem RR, Schrope B, Sethi A, Poneros JM, Gress FG, Genkinger JM, Do C, Brooks CA, Chabot JA, Kluger MD, Kowalski T, Loren DE, Aslanian H, Farrell JJ, Gonda TA (2017). “Comparison of the diagnostic accuracy of three current guidelines for the evaluation of asymptomatic pancreatic cystic neoplasms”. Medicine (Baltimore). 96 (35): e7900. doi:10.1097/MD.0000000000007900. PMC 5585501. PMID 28858107.
- ↑ Dong J, Cong L, Zhang TP, Zhao YP (2016). “Pancreatic metastasis of renal cell carcinoma”. HBPD INT. 15 (1): 30–8. PMID 26818541.
Epidemiology and Demographics
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief:
Overview
In the United States, the age-adjusted prevalence of invasive pancreatic cancer is 11.7 per 100,000 in 2011. Pancreatic cancer is more prevalent in males than females.
Epidemiology and Demographics
Prevalence
- In the United States, the age-adjusted prevalence of invasive pancreatic cancer is 11.7 per 100,000 in 2011.[1]
Mortality rate
- As per the GLOBOCAN 2012 estimates, pancreatic cancer leads to more than 331,000 deaths per year (accounting for 4.0% of all deaths), making it as the seventh leading cause of cancer death in both males and females. [2]
- In 2012, about 338,000 suffered from pancreatic cancer, making it the 11th most common cancer.[2] [3]
Incidence
- Estimated new cases and deaths from pancreatic cancer in the United States in 2015:
- New cases: 48,960
- Deaths: 40,560
- The incidence of carcinoma of the pancreas has markedly increased over the past several decades and ranks as the fourth leading cause of cancer death in the United States.
- Incidence rates for pancreatic cancer in 2012 were: [2]
- In United States, the highest incidence rate of 7.4 per 100,000 people
- In Western Europe, 7.3 per 100,000 people
- In Europe and Australia/New Zealand, equally about 6.5 per 100,000 people
- In Middle Africa and South-Central Asia, the lowest incidence rate of 1.0 per 100,000 people
- In Pakistan, 0.5 per 100,000 people
- The delay-adjusted incidence of invasive pancreatic cancer in 2011 was estimated to be 12.63 per 100,000 persons in the United States[1]
- In 2011, the age-adjusted incidence of invasive pancreatic cancer was 12.30 per 100,000 persons in the United States[1]
Age
- While the overall age-adjusted incidence of invasive pancreatic cancer in the United States between 2007 and 2011 is 12.3 per 100,000, the age-adjusted incidence of invasive pancreatic cancer by age category is:[1]
- Under 65 years: 4 per 100,000
- 65 and over: 69.4 per 100,000
Gender
- In the United States, the age-adjusted prevalence of invasive pancreatic cancer by gender in 2011 is:[1]
- In males: 12.3 per 100,000
- In females: 11.2 per 100,000
- In the United States, the delay-adjusted incidence of invasive pancreatic cancer by gender in 2011 is:[1]
- In males: 14.75 per 100,000 persons
- In females: 10.93 per 100,000 persons
- In the United States, the age-adjusted incidence of invasive pancreatic cancer by gender on 2011 is:[1]
- In males: 14.38 per 100,000 persons
- In females: 10.62 per 100,000 persons
Shown below is an image depicting the delay-adjusted incidence and observed incidence of invasive pancreatic cancer by gender and race in the United States between 1975 and 2011. These graphs are adapted from SEER: The Surveillance, Epidemiology, and End Results Program of the National Cancer Institute.[1]
<figure-inline class=”mw-default-size”><figure-inline><figure-inline><figure-inline> </figure-inline></figure-inline></figure-inline></figure-inline>
</figure-inline></figure-inline></figure-inline></figure-inline>
Race
- Shown below is a table depicting the age-adjusted prevalence of invasive pancreatic cancer by race in 2011 in the United States.[1]
| All Races | White | Black | Asian/Pacific Islander | Hispanic | |
| Age-adjusted prevalence | 11.7 per 100,000 | 11.7 per 100,000 | 13 per 100,000 | 10.4 per 100,000 | 9.6 per 100,000 |
Shown below is an image depicting the incidence of invasive pancreatic cancer by race in the United States between 1975 and 2011.[1]
<figure-inline class=”mw-default-size”><figure-inline><figure-inline><figure-inline> </figure-inline></figure-inline></figure-inline></figure-inline>
</figure-inline></figure-inline></figure-inline></figure-inline>
API: Asian/Pacific Islander; AI/AN: American Indian/ Alaska Native
Percent Distribution of Invasive Pancreatic Cancer by Histology
Among patients with histologically confirmed cases of invasive pancreatic cancer, the percent distribution of the types of the disease in the United States are:[1]
- Carcinoma: 97.9%
- Epidermoid carcinoma: 0.2%
- Adenocarcinoma: 86%
- Adenocarcinoma not otherwise specified: 69.9%
- Papillary adenocarcinoma: 0.1%
- Mucinous adenocarcinoma: 2.6%
- Mucin- producing adenocarcinoma: 1.1%
- Inflitrating duct carcinoma: 9.8%
- Other adenocarcinoma: 2.6%
- Other specific carcinoma: 6.5%
- Carcinoma not otherwise specified: 5.2%
- Sarcoma and other soft tissue tumors: 0.1%
- Other specific types: 0.1%
- Unspecified: 1.9%
Developed Countries
- Developed countries have the highest incidence and mortality rates of pancreatic cancer. [2]
Developing Countries
- Pancreatic cancer incidence and mortality varies across different countries. The incidence is considerably lower in developing countries. [2]
Early-Onset Pancreatic Cancer
Early-Onset Pancreatic Cancer is defined as pancreatic cancer with the onset at age less than 50 years.
Incidence
- Incidence of early-onset pancreatic cancer increased 1.1 to 1.4 per 100,000 from 2013 to 2022 in the US[4] and globally from 2001 to 2018.[5]
- 1324 incident cases of early-onset pancreatic cancer were reported in 2022 representing 5.2% of all pancreatic cancers reported.[4]
Gender
- From 2013 to 2022, early onset pancreatic cancer in the US increased predominantly among women (from 1.0 to 1.4 per 100,00) compared with men (from 1.3 to 1.4 per 100,000).[4]
Race
- Higher number of cases among non-hispanic black individuals (1.7 per 100,000) compared to hispanic and non-hispanic white individuals (1.4 per 100,000).[4]
- The largest increase in incidence rates occurred among Hispanic individuals and non-hispanic white individuals compared to non-hispanic black individuals.[4]
Cancer Type
- Pancreatic ductal adenocarcinoma accounts for most pancreatic cancers (90%).
- Pancreatic neuroendocrine tumors account approx 5% and incidence of early-onset pancreatic neuroendocrine tumors is increasing in the US.[6]
Awareness
- November is pancreatic cancer awareness month.
- Purple is the traditional color chosen to represent pancreatic cancer awareness.
- The National Cancer Institute’s cancer research budget was $4.824 billion in 2004, an estimated $52.7 million of which was devoted to pancreatic cancer.[7]
- Research spending per pancreatic cancer patient is $1145, the lowest of any leading cancer.[8]
- The Pancreatic Cancer Action Network (PanCAN) was created as an advocacy group for pancreatic cancer.
- The National Charity pancreatic cancer UK works to raise awareness in the UK.
References
- ↑ 1.00 1.01 1.02 1.03 1.04 1.05 1.06 1.07 1.08 1.09 1.10 Howlader N, Noone AM, Krapcho M, Garshell J, Miller D, Altekruse SF, Kosary CL, Yu M, Ruhl J, Tatalovich Z,Mariotto A, Lewis DR, Chen HS, Feuer EJ, Cronin KA (eds). SEER Cancer Statistics Review, 1975-2011, National Cancer Institute. Bethesda, MD, http://seer.cancer.gov/csr/1975_2011/, based on November 2013 SEER data submission, posted to the SEER web site, April 2014.
- ↑ 2.0 2.1 2.2 2.3 2.4 Ilic M, Ilic I (2016). “Epidemiology of pancreatic cancer”. World J Gastroenterol. 22 (44): 9694–9705. doi:10.3748/wjg.v22.i44.9694. PMC 5124974. PMID 27956793.
- ↑ Ferlay J, Soerjomataram I, Dikshit R, Eser S, Mathers C, Rebelo M; et al. (2015). “Cancer incidence and mortality worldwide: sources, methods and major patterns in GLOBOCAN 2012”. Int J Cancer. 136 (5): E359–86. doi:10.1002/ijc.29210. PMID 25220842.
- ↑ 4.0 4.1 4.2 4.3 4.4 Surveillance, Epidemiology, and End Results Program. SEER*Explorer: an interactive website for SEER cancer statistics. Surveillance Research Program, National Cancer Institute; April 16, 2025. Accessed May 19, 2025. https://seer.cancer.gov/ statistics-network/explorer/
- ↑ Huang J, Lok V, Ngai CH, et al. Worldwide burden of, risk factors for, and trends in pancreatic cancer. Gastroenterology. 2021;160(3):744-754. doi:10.1053/j.gastro.2020.10.007
- ↑ Hackeng WM, Hruban RH, Offerhaus GJ, Brosens LA. Surgical and molecular pathology of pancreatic neoplasms. Diagn Pathol. 2016;11(1):47. doi:10.1186/s13000-016-0497-z
- ↑ http://pancan.org/About/pancreaticCancerStats.html
- ↑ http://pancan.org/About/pancreaticCancerStats.html
Risk Factors
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Aravind Reddy Kothagadi M.B.B.S[2]
Overview
Pancreatic cancer is associated with number of predisposing risk factors such as age, gender, ethnicity, and environmental exposures. The most potent risk factors for pancreatic cancer include smoking, alcoholism, increased BMI, diabetes mellitus, chronic pancreatitis and a family history of pancreatic cancer. Individuals with hereditary pancreatitis, familial pancreatic cancer, Peutz-Jeghers disease, familial atypical multiple mole melanoma syndrome (FAMMM), von Hippel-Lindau syndrome, multiple endocrine neoplasia type 1, cystic fibrosis of the pancreas and familial cancer syndromes such as lynch syndrome, familial adenomatous polyposis (FAP) and hereditary breast and ovarian cancer–BRCA1 and BRCA2 mutations are also at an increased risk of pancreatic cancer. Other medical conditions which pose as a risk factor for pancreatic cancer are inflammatory bowel disease, periodontal disease and peptic ulcer disease.
Risk Factors
- The most potent risk factors for pancreatic cancer include smoking, alcoholism, increased BMI, diabetes mellitus, chronic pancreatitis and a family history of pancreatic cancer.
- Individuals with the following conditions are also at an increased risk of pancreatic cancer:[1][2][3]
- Hereditary pancreatitis
- Familial pancreatic cancer
- Peutz-Jeghers disease
- Familial atypical mole melanoma syndrome (FAMMM)
- Cystic fibrosis of pancreas
- Familial cancer syndromes such as:
- Lynch syndrome
- Familial adenomatous polyposis (FAP)
- Von Hippel-Lindau syndrome
- Multiple endocrine neoplasia type 1
- Hereditary breast and ovarian cancer–BRCA1 and BRCA2 mutations
- Risk factors for Pancreatic cancer are illustrated in the following tables:
- Risk factors for Pancreatic Cancers:[4]
| Risk factors for Pancreatic Cancer |
|---|
| Risk factors |
|
|
| Familial Cancer Syndromes |
|
| Other medical conditions |
|
- Risk Factors and Inherited Syndromes associated with Pancreatic Cancer:[5]
| Risk Factors and Inherited Syndromes associated with Pancreatic Cancer | |||
|---|---|---|---|
| Risk Factor | Approximate Risk | ||
| Smoking | 2-3 % | ||
| Long-standing Diabetes mellitus | 2 % | ||
| Nonhereditary and chronic pancreatitis | 2-6 % | ||
| Obesity, Inactivity or both | 2 % | ||
| Non O Blood Group | 1-2 % | ||
| Genetic Syndrome and Associated Gene or Genes | |||
| Hereditary pancreatitis (PRSS1, SPINK1) | 50 % | ||
| Familial atypical multiple mole and melanoma syndrome (p16) | 10-20 % | ||
| Hereditary breast and ovarian cancer syndromes (BRCA1, BRCA2, PALB2) | 1-2 % | ||
| Peutz-Jeghers syndrome (STK11 [LKB1]) | 30-40 % | ||
| Hereditary nonpolyposis colorectal cancer (Lynch syndrome) (MLH1, MSH2, MSH6) | 4 % | ||
| Ataxia-telangiectasia (ATM) | Unknown | ||
| Li-Fraumeni syndrome (P53) | Unknown | ||
Early-Onset Pancreatic Cancer
Early-Onset Pancreatic Cancer is defined as pancreatic cancer at age of onset less than 50 years.
| Risk Factors for Early-Onset Pancreatic Cancer |
|---|
| Alcohol* |
| Metabolic dysfunction with associated Steatotic Liver Disease |
| Obesity |
| Sedentary lifestyle |
| Smoking |
*Alcohol consumption of more than 26g/day compared to less than 26g/day was associated with early-onset pancreatic cancer, particularly among individuals younger than 45 years.[6]
Following risk factors were more strongly associated with early-onset pancreatic cancer than with later-onset pancreatic cancer[7]:
- Diabetes
- Non-O Blood Group
- Non-O Blood Group was more strongly associated with pancreatic risk among participants aged 70 years or younger vs those older than 70 years.
- Obesity
- Smoking
- Tall Height
- Those with early-onset pancreatic cancer were more likely to have a family history of pancreatic cancer were more likely to have a family history of pancreatic cancer in a first degree relative.[6]
References
- ↑ Goral V (2015). “Pancreatic Cancer: Pathogenesis and Diagnosis”. Asian Pac J Cancer Prev. 16 (14): 5619–24. PMID 26320426.
- ↑ Pandol, Stephen; Gukovskaya, Anna; Edderkoui, Mouad; Dawson, David; Eibl, Guido; Lugea, Aurelia (2012). “Epidemiology, risk factors, and the promotion of pancreatic cancer: Role of the stellate cell”. Journal of Gastroenterology and Hepatology. 27: 127–134. doi:10.1111/j.1440-1746.2011.07013.x. ISSN 0815-9319.
- ↑ Lowenfels, Albert B.; Maisonneuve, Patrick (2005). “Risk factors for pancreatic cancer”. Journal of Cellular Biochemistry. 95 (4): 649–656. doi:10.1002/jcb.20461. ISSN 0730-2312.
- ↑ Bond-Smith G, Banga N, Hammond TM, Imber CJ (2012). “Pancreatic adenocarcinoma”. BMJ. 344: e2476. doi:10.1136/bmj.e2476. PMID 22592847.
- ↑ Ryan DP, Hong TS, Bardeesy N (2014). “Pancreatic adenocarcinoma”. N Engl J Med. 371 (11): 1039–49. doi:10.1056/NEJMra1404198. PMID 25207767.
- ↑ 6.0 6.1 McWilliams RR, Maisonneuve P, Bamlet WR, et al. Risk factors for early-onset and very-early-onset pancreatic adenocarcinoma: a Pancreatic Cancer Case-Control Consortium (PanC4) analysis. Pancreas. 2016;45(2):311-316. doi:10.1097/MPA.0000000000000392
- ↑ Yuan C, Kim J, Wang QL, et al; PanScan/PanC4 I-III Consortium. The age-dependent association of risk factors with pancreatic cancer. Ann Oncol. 2022;33(7):693-701. doi:10.1016/j.annonc.2022.03. 276
Screening
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]Associate Editor(s)-in-Chief: Aravind Reddy Kothagadi M.B.B.S[2]
Overview
In asymptomatic adults who are at average risk, the U.S.P.S.T.F recommends against routine screening for pancreatic cancer due to the lack of mortality benefit. In high-risk individuals, with familial pancreatic cancer or in those with genetic syndromes predisposing to pancreatic cancer, screening is suggested. In high- risk groups, screening by endoscopic ultrasound (EUS), magnetic resonance imaging (MRI) and magnetic resonance cholangiopancreatography (MRCP) are recommended.
Screening
- In asymptomatic adults who are at average risk, the U.S.P.S.T.F recommends against routine screening for pancreatic cancer due to the lack of mortality benefit.
- In high-risk individuals, with familial pancreatic cancer or in those with genetic syndromes predisposing to pancreatic cancer, screening is suggested. In high- risk groups, screening by endoscopic ultrasound (EUS), magnetic resonance imaging (MRI) and magnetic resonance cholangiopancreatography (MRCP) are recommended.[1][2]
- Screening is recommended in individuals with the following conditions who are at an increased risk of pancreatic cancer:[3]
- Hereditary pancreatitis
- Familial pancreatic cancer
- Peutz-Jeghers disease
- Familial atypical mole melanoma syndrome (FAMMM)
- Cystic fibrosis of pancreas
- Familial cancer syndromes such as:
References
- ↑ Poruk KE, Firpo MA, Adler DG, Mulvihill SJ (2013). “Screening for pancreatic cancer: why, how, and who?”. Ann Surg. 257 (1): 17–26. doi:10.1097/SLA.0b013e31825ffbfb. PMC 4113008. PMID 22895395.
- ↑ Greer JB, Brand RE (2007). “Screening for pancreatic cancer: current evidence and future directions”. Gastroenterol Hepatol (N Y). 3 (12): 929–38. PMC 3104195. PMID 21960811.
- ↑ Goral V (2015). “Pancreatic Cancer: Pathogenesis and Diagnosis”. Asian Pac J Cancer Prev. 16 (14): 5619–24. PMID 26320426.
Natural History, Complications and Prognosis
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Aravind Reddy Kothagadi M.B.B.S[2] Sudarshana Datta, MD [3]
Overview
Patients with pancreatic cancer present with symptoms such as jaundice, light-colored stools, dark urine, and epigastric pain in the sixth decade of life. If left untreated, patients with pancreatic cancer may progress to develop exocrine pancreatic insufficiency arising from pancreatic duct obstruction leading to malabsorption, malnutrition and cachexia. Common complications of pancreatic cancer include intractable pain and obstructive jaundice that develop as a result of surgical intervention. Depending on the extent of the tumor at the time of diagnosis, the prognosis is generally regarded as poor, with complete remission being extremely rare.
Natural History
The natural history of pancreatic cancer is as follows:[1][2][3]
- The symptoms of pancreatic cancer usually develop in the sixth decade of life, and start with symptoms such as jaundice, light-colored stools, dark urine, pain in the upper or middle abdomen and back, unexplained weight loss, anorexia and fatigue.
- The symptoms of pancreatic cancer typically develop about 20-30 years after exposure to risk factors such as smoking and alcohol. Genetic factors such as alterations in tumor suppressor genes, oncogenes and different signaling pathways may also be responsible.
- If left untreated, patients with pancreatic cancer may progress to develop exocrine pancreatic insufficiency arising from pancreatic duct obstruction leading to malabsorption, malnutrition and cachexia. Dudodenal obstruction and biliary obstruction may cause symptoms of bowel obstruction and jaundice. Metastasis may occur to different sites.
Complications
Common complications of pancreatic cancer may arise as a result of the disease or therapy:[4][5][6][7][8][9][10]
- Malabsorption
- Exocrine pancreatic insufficiency due to pancreatic duct obstruction by the tumor may lead to malabsorption. Malabsorption in patients presents with anorexia, weight loss, and diarrhea.
- Intractable pain
- Patients with advanced pancreatic cancer may develop intractable pain requiring narcotic analgesics and surgical intervention such as neurolysis of celiac ganglia.[4][11]
- Jaundice
- Obstructive jaundice can present with features of cholangitis:
- Fever and chills
- Nausea, vomiting
- Clay-colored stools
- Dark urine
- Yellowish discoloration of skin
- Pruritus
- Right upper quadrant pain
- Anorexia
- Obstructive jaundice can present with features of cholangitis:
- Patients may require Endoscopic decompression with stent placement in patients due to biliary obstruction.
- Duodenal obstruction
- Patients may develop duodenal obstruction as a result of complications of surgery.
- Duodenal obstruction may be treated with endoscopic stenting or gastrojejunostomy.
Prognosis
- The primary factors that influence prognosis are:
- Whether the tumor is localized and can be completely resected
- Whether the tumor has spread to lymph nodes or elsewhere
Staging and TNM (tumour, lymph node, metastasis) classification related to incidence, treatment, and prognosis:[12]
| Staging and TNM Classification related to Incidence, Treatment, and Prognosis | ||||
|---|---|---|---|---|
| Stage | TNM Classification | Clinical Classification | Incidence at diagnosis (%) | 5-year survival rate (%) |
| 0 | Tis, N0, M0 | Resectable | 7.5 | 15 |
| IA | T1, N0, M0 | — | — | 14 |
| IB | T2, N0, M0 | — | — | 12 |
| IIA | T3, N0, M0 | — | — | 7 |
| IIB | T1-3, N1, M0 | Locally advanced | 29.3 | 5 |
| III | T4, any N, M0 | — | — | 3 |
| IV | Any T, any N, M1 | Metastatic | 47.2 | 1 |
Five year survival rate
- The percentage of people who live for a minimum of five years after diagnosis is called the 5- year survival rate.
- Survival rates for exocrine pancreatic cancer:
- Lifespan is found to be longer in patients treated with surgery, as opposed to other patients.
- The 5-year survival rate for people at various stages of pancreatic cancer are as follows based on the most recent statistics of the American Cancer Society are as follows:[13][14]
- Stage IA: 14%
- Stage IB: 12%
- Stage IIA 7%
- Stage IIB 5%
- Stage III 3%
- Stage IV 1%
- Survival rates for neuroendocrine pancreatic tumors (treated with surgery) are as follows:
- Stage I pancreatic NETs 61%
- Stage II pancreatic NETs 52%
- Stage III pancreatic NETs 41%
- Stage IV pancreatic NETs 16%
- Five year survival rate of tumors not removed by surgery is 16%
References
- ↑ Chang SC, Yang WV (2016). “Hyperglycemia, tumorigenesis, and chronic inflammation”. Crit. Rev. Oncol. Hematol. 108: 146–153. doi:10.1016/j.critrevonc.2016.11.003. PMID 27931833.
- ↑ Sohal DP, Mangu PB, Khorana AA, Shah MA, Philip PA, O’Reilly EM, Uronis HE, Ramanathan RK, Crane CH, Engebretson A, Ruggiero JT, Copur MS, Lau M, Urba S, Laheru D (2016). “Metastatic Pancreatic Cancer: American Society of Clinical Oncology Clinical Practice Guideline”. J. Clin. Oncol. 34 (23): 2784–96. doi:10.1200/JCO.2016.67.1412. PMC 5019760. PMID 27247222.
- ↑ Frič P, Škrha J, Šedo A, Bušek P, Kmochová K, Laclav M, Solař S, Bunganič B, Zavoral M (2016). “Early pancreatic carcinogenesis – risk factors, early symptoms, and the impact of antidiabetic drugs”. Eur J Gastroenterol Hepatol. 28 (7): e19–25. doi:10.1097/MEG.0000000000000646. PMID 27120389.
- ↑ 4.0 4.1 Koulouris AI, Banim P, Hart AR (2017). “Pain in Patients with Pancreatic Cancer: Prevalence, Mechanisms, Management and Future Developments”. Dig. Dis. Sci. 62 (4): 861–870. doi:10.1007/s10620-017-4488-z. PMID 28229252.
- ↑ Ramsey ML, Conwell DL, Hart PA (2017). “Complications of Chronic Pancreatitis”. Dig. Dis. Sci. 62 (7): 1745–1750. doi:10.1007/s10620-017-4518-x. PMC 5667546. PMID 28281169.
- ↑ Vujasinovic M, Valente R, Del Chiaro M, Permert J, Löhr JM (2017). “Pancreatic Exocrine Insufficiency in Pancreatic Cancer”. Nutrients. 9 (3). doi:10.3390/nu9030183. PMC 5372846. PMID 28241470.
- ↑ Poruk KE, Wolfgang CL (2016). “Palliative Management of Unresectable Pancreas Cancer”. Surg. Oncol. Clin. N. Am. 25 (2): 327–37. doi:10.1016/j.soc.2015.11.005. PMID 27013367.
- ↑ Kapoor VK (2016). “Complications of pancreato-duodenectomy”. Rozhl Chir. 95 (2): 53–9. PMID 27008166.
- ↑ Hucl T (2016). “[Malignant biliary obstruction]”. Cas. Lek. Cesk. (in Czech). 155 (1): 30–7. PMID 26898789.
- ↑ Dong J, Cong L, Zhang TP, Zhao YP (2016). “Pancreatic metastasis of renal cell carcinoma”. HBPD INT. 15 (1): 30–8. PMID 26818541.
- ↑ Dobosz Ł, Kaczor M, Stefaniak TJ (2016). “Pain in pancreatic cancer: review of medical and surgical remedies”. ANZ J Surg. 86 (10): 756–761. doi:10.1111/ans.13609. PMID 27111447.
- ↑ Bond-Smith G, Banga N, Hammond TM, Imber CJ (2012). “Pancreatic adenocarcinoma”. BMJ. 344: e2476. doi:10.1136/bmj.e2476. PMID 22592847.
- ↑ “Pancreatic Cancer Survival Rates, by Stage”.
- ↑ Carrato, A.; Falcone, A.; Ducreux, M.; Valle, J. W.; Parnaby, A.; Djazouli, K.; Alnwick-Allu, K.; Hutchings, A.; Palaska, C.; Parthenaki, I. (2015). “A Systematic Review of the Burden of Pancreatic Cancer in Europe: Real-World Impact on Survival, Quality of Life and Costs”. Journal of Gastrointestinal Cancer. 46 (3): 201–211. doi:10.1007/s12029-015-9724-1. ISSN 1941-6628.
Diagnosis
Diagnosis
Staging | History and Symptoms | Physical Examination | Laboratory Findings | Chest X Ray | CT | MRI | Ultrasound | Other Imaging Findings | Other Diagnostic Studies
Treatment
Treatment
Medical Therapy | Surgery | Treatment by Stage | Primary Prevention | Secondary Prevention | Cost-Effectiveness of Therapy | Future or Investigational Therapies
Looking for the patient version?
© 2026 MyEClinic – IFTM Institut für Telematik in der Medizin GmbH