
Incidentaloma
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Mohamed Riad, M.D.[2] Mohammed Abdelwahed M.D[3]
For patient information, click here
Synonyms and keywords: Adrenal incidentaloma
Overview
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Mohammed Abdelwahed M.D[2]
Overview
Adrenal incidentaloma is an asymptomatic adrenal mass detected on imaging not performed for a suspected adrenal disease. Malignancy is an uncommon cause of adrenal incidentaloma. In most cases, adrenal incidentalomas are nonfunctioning adrenocortical adenomas, although, they may secrete cortisol, catecholamines or aldosterone. Common causes of incidentaloma include adenoma, carcinoma, pheochromocytoma, congenital adrenal hyperplasia, myelolipoma, and hemangioma. If left untreated, patients with adrenal incidentaloma may progress to develop Dyslipidemia, Osteoporosis, Hyperglycemia, Malignant hypertension, Intracranial hemorrhage, Acute coronary syndrome, Aortic dissection, malignant transformation, and metastasis. Prevalence of adrenal incidentaloma is 2% in autopsy studies and 3% in radiological studies. It may present with symptoms that are mainly subclinical such as subclinical Cushing’s syndrome which includes diabetes, and a high incidence of vertebral fractures, dyslipidemia, impaired glucose tolerance or type 2 diabetes mellitus, and evidence of atherosclerosis. Pheochromocytoma symptoms and signs are paroxysmal attacks of hypertension, palpitations, diaphoresis, headache, pallor, and tremor. Primary hyperaldosteronism patients show hypertension and hypokalemia. Abdominal CT scan may be helpful in the diagnosis of adrenal incidentaloma to the differentiation between benign and malignant incidentaloma. Malignancy is suggested on CT by a large diameter more than 6 cm, irregular border, inhomogeneity, a “washout” of contrast after 15 min of less than 40%, and calcifications. MRI has advantages in certain clinical situations. The advantages of MRI over CT are its lack of radiation exposure, lack of iodine-based contrast media and its superior tissue contrast resolution. Surgery is the mainstay of treatment for incidentalomas. Adrenalectomy for patients with hyperaldosteronism, pheochromocytoma, cortisol-secreting tumors, and adrenal incidentalomas is safe and effective.
Historical Perspective
In 1979, incidentaloma was first described by Korobkin et al. In 1989, a large study at the Mayo Clinic found the prevalence of adrenal incidentaloma to be 3400 per 100,000 persons.
Classification
Adrenal incidentaloma may be classified as functioning (secreting) or non-functioning incidentaloma. Adrenal incidentaloma may also be classified by the nature into benign masses or malignant masses.
Pathophysiology
The pathophysiology of adrenal incidentaloma depends on nature and function of the mass. Incidentalomas are mostly adrenal tumors that are often discovered as an incidental finding. Malignancy is an uncommon cause of adrenal incidentaloma in patients without a known diagnosis of cancer. An adrenal incidentaloma may secrete cortisol. Cushing’s syndrome is linked to hypercortisolism which can develop by excess ACTH secretion or excess cortisol secretion by adrenal glands. An adrenal incidentaloma may secrete catecholamines and in such a case it is considered a pheochromocytoma. It may be sporadic, but some occur as a component of hereditary cancer syndromes such as Li-Fraumeni syndrome, Beckwith-Wiedemann syndrome, and Multiple endocrine neoplasia type 1. Genetic base of sporadic incidentaloma is mutations in TP53 gene, located on chromosome 17p13. A role of the TP53 tumor suppressor gene in sporadic adrenocortical carcinoma has also been studied. On gross pathology, adrenocortical adenoma is a yellow, well circumscribed tumor in the adrenal cortex, which is usually 2–5 cm in diameter. The color of the tumor, as with adrenal cortex as a whole, is due to the stored lipid (mainly cholesterol), from which the cortical hormones are synthesized.
Causes
Common causes of incidentaloma include adenoma, carcinoma, pheochromocytoma, congenital adrenal hyperplasia, massive macronodular adrenal disease, and nodular variant of Cushing’s disease. Less Common Causes include myelolipoma, neuroblastoma, ganglioneuroma, hemangioma.
Differentiating adrenal incidentaloma from Other Diseases
Adrenal incidentaloma must be differentiated from other diseases that cause adrenal masses such as adrenal adenoma, adrenocortical carcinoma, Cushing’s syndrome, pheochromocytoma, and metastasis.
Epidemiology and Demographics
Prevalence of adrenal masses which are not apparent clinically is around 2% in autopsy studies. Radiological studies report a frequency of around 3%. The prevalence of adrenal incidentalomas increases with age. The prevalence of adrenal incidentaloma is higher in older patients 10%. There is no racial or gender predilection to incidentaloma.
Risk Factors
Most adrenocortical carcinomas are sporadic, but some occur as a component of hereditary cancer syndromes such as Li-Fraumeni syndrome, Beckwith-Wiedemann syndrome, and multiple endocrine neoplasia type 1(MEN1). Genetic basis of sporadic incidentaloma include TP53 gene. A role for the TP53 tumor suppressor gene in sporadic ACCs is suggested by the frequent finding of loss of heterozygosity (LOH) at the 17p13 locus in sporadic ACCs. Another chromosomal locus that is strongly implicated in the pathogenesis of ACC is 11p, the area of abnormality in Beckwith-Wiedemann syndrome and the site of the insulin-like growth factor-2 (IGF-2) gene.
Screening
According to the European Society of Endocrinology Clinical Practice Guideline, screening for adrenal incidentaloma includes: family screening for patients with bilateral macro-nodular hyperplasia, patients with asymptomatic vertebral fractures, patients with possible autonomous cortisol secretion, and patients with a hereditary syndrome leading to adrenal tumors. Screening test include 24-hour urine fractionated metanephrines for pheochromocytoma, 24-hour urinary free cortisol for patients with symptoms of Cushing’s syndrome, and plasma aldosterone concentration, plasma renin activity for patients with primary aldosteronism.
Natural History, Complications, and Prognosis
If left untreated, patients with adrenal incidentaloma may progress to develop dyslipidemia, osteoporosis, hyperglycemia, malignant hypertension, intracranial hemorrhage, acute coronary syndrome, aortic dissection, malignant transformation, and metastasis. Prognosis is usually good in benign adrenal incidentalomas, death is not directly related to the adrenal mass, but to cardiovascular accidents, malignancy, and chronic disorders, as observed in the general population. Adrenocortical carcinoma (ACC) carries a poor prognosis and is unlike most tumors of the adrenal cortex, which are benign (adenomas) and only occasionally cause Cushing’s syndrome.
Diagnosis
Diagnostic Criteria
There are no definitive diagnostic criteria for adrenal incidentaloma management but there are guidelines to diagnose and treat the mass according to Endocrine Society. Radiological evaluation including non-contrast CT attenuation value expressed in Hounsfield unit (HU) is the best tool to differentiate between benign and malignant adrenal masses. All patients should undergo hormonal evaluation for subclinical Cushing’s syndrome and pheochromocytoma, and those with hypertension should also be evaluated for primary hyperaldosteronism.
History and Symptoms
Sub-clinical Cushing’s syndrome which includes diabetes, and a high incidence of vertebral fractures, dyslipidemia, impaired glucose tolerance or type 2 diabetes mellitus, and evidence of atherosclerosis. Pheochromocytoma: Paroxysmal attacks of hypertension, palpitations, diaphoresis, headache, pallor, and tremor. Primary hyperaldosteronism patients show hypertension and hypokalemia. Approximately 60 percent of adrenocortical carcinomas (ACC) are sufficiently secretory to present clinical syndrome of hormone excess. The family history of Li-Fraumeni syndrome, Beckwith-Wiedemann syndrome, and multiple endocrine neoplasia type 1 (MEN1).
Physical Examination
Most of patients will not show any special signs as the definition of adrenal incidentaloma means incidentaly discovered mass during imaging for ant other reasons. Some cases shows signs of subclinical Cushing’s syndrome, pheochromocytoma, or hyperaldosteronism. Common physical examination findings of include patients may appear quite well if the disease is asymptomatic. Patients may appear tired, weak, diaphoretic and anxious. Tachypnea if malignant secondaries are found in the lung with a rapid strong equal pulse and high blood pressure. Jaundice, hyperpigmentation, Telangiectasia, thinning of the skin and easy bruising may be found. A palpable abdominal mass in the lower abdominal quadrant may be found. Hyporeflexia due to low potassium level in aldosternonma, Proximal muscle weakness bilaterally, and bilateral tremors may be found.
Laboratory Findings.
Laboratory findings consistent with the diagnosis of incidentaloma include an abnormal 1 mg over night dexamethasone for sub-clinical Cushing’s syndrome that should be confirmed with 24-hour urinary free cortisol, serum ACTH concentration, and dehydroepiandrosterone sulfate (DHEAS). In patients with adrenal masses that have a probability for pheochromocytoma, routine measurement of 24-hour urinary fractionated metanephrines and catecholamines should be done. All patients with hypertension and an adrenal incidentaloma should be evaluated by measurements of plasma aldosterone concentration and plasma renin activity.
Electrocardiogram
On EKG, catecholamines secreting incidentaloma is characterized by the presence of sinus tachycardia and supraventricular tachycardia.
X-ray
There are no x-ray findings associated with adrenal incidentaloma.
CT scan
Abdominal CT scan may be helpful in the diagnosis of adrenal incidentaloma. Differentiation between benign and malignant incidentaloma is important. Malignancy is suggested on CT by a large diameter more than 6 cm, irregular border, inhomogeneity, a “washout” of contrast after 15 min of less than 40%, and calcifications. Contrast-enhanced washout CT utilizes the unique perfusion pattern of adenomas. Adenomas take up intravenous CT contrast rapidly, but also have a rapid loss of contrast – a phenomenon termed ‘contrast enhancement washout’. It is assumed that malignant adrenal lesions usually enhance rapidly but demonstrate a slower washout of contrast medium.
MRI
Adrenal MRI may be helpful in the diagnosis of incidentaloma. Findings on MRI suggestive of incidentaloma include mild enhancement and a rapid washout of contrast, while malignant lesions show rapid and marked enhancement and a slower washout pattern. MRI has advantages in certain clinical situations. The advantages of MRI over CT are its lack of radiation exposure, lack of iodine-based contrast media and its superior tissue contrast resolution.
Other Imaging Findings
Findings on a Positron Emission Tomography (PET-CT) scan suggestive of/diagnostic of incidentaloma. Cancer cells have an increased requirement for glucose and take up more glucose and deoxyglucose than normal cells. standard uptake value (SUV) values have been utilized to differentiate between benign and malignant adrenal lesions. It may be helpful in the diagnosis of incidentaloma in selected patients; those with a history of malignancy or those in which CT densitometry or washout analysis is inconclusive or suspicious for malignancy because of their high sensitivity for detecting malignancy.
Other Diagnostic Studies
Fine-needle aspiration biopsy may be helpful in the diagnosis of incidentaloma. It can distinguish between an adrenal tumor and a metastatic tumor. In a patient with a known primary malignancy, performing a diagnostic CT-guided FNA biopsy may be indicated. The FNA biopsy of a pheochromocytoma may result in hemorrhage and hypertensive crisis. So, excluding pheochromocytoma with biochemical testing is necessary before any procedure.
Treatment
Medical Therapy
The mainstay of treatment for adrenal incidentaloma is surgery but preoperative medical management is needed for functional masses. Perioperative medical management of patients with subclinical Cushing’s syndrome includes glucocorticoid therapy during surgery. Such patients can safely undergo surgical resection of their tumor and have their cortisol levels measured postoperatively. Preoperative medical management of patients with pheochromocytoma includes preoperative treatment to control hypertension during surgery and hypotension after it. Three medical regimens for preoperative management of pheochromocytoma: Combined alpha and beta-adrenergic blockers, calcium channel blockers, and Metyrosine. Preoperative medical management of patients with aldosteronoma include medical therapy with mineralocorticoid receptor antagonists should be reserved for those who are unable or unwilling to undergo surgery.
Surgery
Surgery is the mainstay of treatment for adrenal incidentaloma. Adrenalectomy for patients with hyperaldosteronism, pheochromocytoma, cortisol-secreting tumors, and adrenal incidentalomas is safe and effective. A reasonable strategy may be to consider adrenalectomy for younger patients and those with new onset or a worsening of underlying comorbidities such as diabetes mellitus, hypertension, obesity, or osteoporosis. All patients with documented pheochromocytoma and adrenocortical cancer should undergo prompt surgical intervention. Risk factors for complications during surgery include high plasma norepinephrine concentration and larger tumor size.
Primary Prevention
There is no established method for primary prevention of incidentaloma.
Secondary Prevention
Effective measures for the secondary prevention of adrenal incidentaloma include annual biochemical follow-up for up to 5 years, no routine follow-up of adrenal incidentalomas with a non-contrast attenuation value no greater than 10 HU. Patients with adrenal masses less than 4 cm in size and a non-contrast attenuation value more than 10 HU should have a repeat CT study in 3–6 months and then yearly for 2 years.
References
Historical Perspective
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Mohammed Abdelwahed M.D[2]
Overview
In 1979, incidentaloma was first described by Korobkin et al. In 1989, a large study at the Mayo Clinic found the prevalence of adrenal incidentaloma to be 3400 per 100,000 persons.
Historical Perspective
- In 1979, incidentaloma was first described by Korobkin et al. They reported 15 patients studied on a CT for other indications who had an adrenal mass.[1]
- From 1985 through 1989, the prevalence of adrenal incidentaloma was found to be 3400 per 100,000 persons.[2]
- With widespread use of CT and magnetic resonance imaging (MRI), unexpected adrenal masses with a diameter of more than 1 cm are increasingly found and multiple methods of management have been established.
References
- ↑ Korobkin M, White EA, Kressel HY, Moss AA, Montagne JP (1979). “Computed tomography in the diagnosis of adrenal disease”. AJR Am J Roentgenol. 132 (2): 231–8. doi:10.2214/ajr.132.2.231. PMID 105590.
- ↑ Herrera MF, Grant CS, van Heerden JA, Sheedy PF, Ilstrup DM (1991). “Incidentally discovered adrenal tumors: an institutional perspective”. Surgery. 110 (6): 1014–21. PMID 1745970.
Classification
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Mohammed Abdelwahed M.D[2]
Overview
Adrenal incidentaloma may be classified as functioning (secreting) or nonfunctioning incidentaloma. Adrenal incidentaloma may also be classified by the nature into benign masses or malignant masses.
Classification
Adrenal incidentaloma may be classified by its function into:[1][2][3][4][5]
- Functioning (hormone secreting):
- Adenomas and carcinomas can secrete any type of adrenal hormone.
- Most of the adrenal incientalomas secrete excess cortisol with minimal signs of Cushing’s syndrome that may not be noticed.
- Pheochromocytomas secrete catecholamines.
- Aldosterone secreting masses may present with hypertension and hypokalemia.
- Nonfunctioning (nonhormonal secreting):
Adrenal incidentaloma may be classified on the basis of the nature, into:
References
- ↑ Grumbach MM, Biller BM, Braunstein GD, Campbell KK, Carney JA, Godley PA; et al. (2003). “Management of the clinically inapparent adrenal mass (“incidentaloma”)”. Ann Intern Med. 138 (5): 424–9. PMID 12614096.
- ↑ Young WF (2000). “Management approaches to adrenal incidentalomas. A view from Rochester, Minnesota”. Endocrinol Metab Clin North Am. 29 (1): 159–85, x. PMID 10732270.
- ↑ Sidhu S, Sywak M, Robinson B, Delbridge L (2004). “Adrenocortical cancer: recent clinical and molecular advances”. Curr Opin Oncol. 16 (1): 13–8. PMID 14685087.
- ↑ Lacroix A, Feelders RA, Stratakis CA, Nieman LK (2015). “Cushing’s syndrome”. Lancet. 386 (9996): 913–27. doi:10.1016/S0140-6736(14)61375-1. PMID 26004339.
- ↑ Raff H, Carroll T (2015). “Cushing’s syndrome: from physiological principles to diagnosis and clinical care”. J Physiol. 593 (3): 493–506. doi:10.1113/jphysiol.2014.282871. PMC 4324701. PMID 25480800.
Pathophysiology
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Mohammed Abdelwahed M.D[2]
Overview
The pathophysiology of adrenal incidentaloma depends on nature of the mass and its function. Incidentalomas are adrenal tumors that often discovered as an incidental finding. Malignancy is an uncommon cause of adrenal incidentaloma in patients without a known diagnosis of cancer. Incidentalomas may secrete cortisol. Cushing’s syndrome is linked to hypercortisolism which can develop by excess ACTH secretion or excess cortisol secretion by adrenal glands. Incidentalomas also may secrete catecholamines and in this case it is considered pheochromocytoma. Pheochromocytoma arises from chromaffin cells of the adrenal medulla and sympathetic ganglia. Malignant and benign pheochromocytomas share the same biochemical and histological features, the only difference is to have a distant spread or be locally invasive. It may be sporadic, but some occur as a component of hereditary cancer syndromes such as Li-Fraumeni syndrome, Beckwith-Wiedemann syndrome, and Multiple endocrine neoplasia type 1. Genetic base of sporadic incidentaloma is mutations in TP53 gene, located on chromosome 17p13. A role for the TP53 tumor suppressor gene in sporadic adrenocortical carcinoma. On gross pathology, adrenocortical adenoma is a yellow, well circumscribed tumor in the adrenal cortex, which is usually 2–5 cm in diameter. The color of tumor, as with adrenal cortex as a whole, is due to the stored lipid (mainly cholesterol), from which the cortical hormones are synthesized.
Pathophysiology
Incidentalomas are adrenal tumors that are often discovered as an incidental finding.[1][2][3]
- Most incidentalomas are nonfunctional, 9% are found to secrete low levels of cortisol, 4% are pheochromocytomas, and 1.5% are aldosteronomas.
- Malignancy is an uncommon cause of adrenal incidentaloma in patients without a known diagnosis of cancer.
- Frequency of primary adrenal carcinoma is approximately 2 to 5 percent; and 0.7 to 2.5% have non-adrenal metastases to the adrenal gland.
- Most adrenocortical carcinomas are sporadic, but some occur as a component of hereditary cancer syndromes.
Subclinical Cushing’s syndrome pathogenesis
The pathophysiology of Cushing’s syndrome is linked to hypercortisolism which can develop by excess ACTH secretion or excess cortisol secretion by adrenal glands. The underlying mechanisms are usually genetic mutations or overexpression of proteins:[4]
- Benign adrenocortical adenoma: Common defects leading to adrenocortical adenoma are mutations or activation of the cAMP-dependent or β-catenin signaling pathways and aberrant expression and function of various G-protein-coupled receptors (GPCR).[5]
- Adrenal cortical carcinoma: It is associated with germline TP53 mutations and MEN syndrome.[6]
- Bilateral adrenal hyperplasia: It is associated with MEN1, familial adenomatous polyposis, and fumarate hydratase gene mutations. Several inactivating mutations of armadillo repeat containing 5 genes are also identified.
Mechanism of cortisol secretion
The secretion of cortisol is controlled by hypothalamic-pituitary axis by the following mechanism:[7]
- Paraventricular nuclei in the hypothalamus release corticotropin releasing hormone (CRH).
- CRH is transferred to anterior pituitary via the portal veins.
- CRH stimulates the activity of corticotrophs; cells that produce proopiomelanocortin (POMC) in the anterior pituitary.
- Corticotrophs produce adrenocorticotropic hormone (ACTH) by the post-translational modification of POMC.
- ACTH is drained into systemic circulation via the pituitary capillaries and stimulates the adrenal cortex (zona fasciculata) to produce cortisol.
- Cortisol acts on hypothalamus and pituitary through a feedback mechanism to regulate the secretion of CRH and ACTH.
Pathogenesis of pheochromocytoma
Pheochromocytoma arises from chromaffin cells of the adrenal medulla and sympathetic ganglia. Malignant and benign pheochromocytomas share the same biochemical and histological features, the only difference is to have a distant spread or be locally invasive.
Basic physiology of catecholamines
Catecholamines act on nearly all body tissues. Its actions vary by tissue type and tissue expression of adrenergic receptors.[8]
- Epinephrine is a non-selective agonist of all adrenergic receptors, including the major sub-types α1, α2, β1, β2, and β3:
- Binding to α1 receptors causes vasoconstriction. Blood vessels with α1-adrenergic receptors are present in the skin, the sphincters of the gastrointestinal system, kidney (renal artery) and brain. During the fight-or-flight response vasoconstriction results in decreased blood flow to these organs.
- Binding to α2 receptors inhibits insulin secretion by the pancreas, stimulates glycogenolysis in the liver and muscle, and stimulates glycolysis and inhibits insulin-mediated glycogenesis in muscle. It suppresses the release of norepinephrine by negative feedback.
- Binding to β2 receptors causes smooth muscle relaxation in the uterus, GI tract, urinary detrusor muscle of bladder wall, and bronchi. It also causes dilatation of smaller coronary arteries, hepatic artery, skeletal muscle arteries.
- Binding to β1 receptors causes renin release from juxtaglomerular cells and lipolysis in adipose tissue. It Increases cardiac output via below mechanisms:
- Increase in heart rate in sinoatrial node.
- Increase in atrial cardiac muscle contractility.
- Increases in contractility and automaticity of ventricular cardiac muscle.
- Increases in conduction and automaticity of atrioventricular node.
Genetics
Sporadic cases genetics
- TP53 gene, located on chromosome 17p13, is the most frequently mutated gene in human cancers. A role for the TP53 tumor suppressor gene in sporadic ACCs is suggested by the frequent finding of loss of heterozygosity (LOH) at the 17p13 locus in sporadic ACCs.[9]
- Although loss of heterozygosity at 17p13 is common, only approximately one-third of these tumors have a mutation of TP53. This suggests that another as yet unidentified suppressor gene is present in this locus.[10]
- Another chromosomal locus that is strongly implicated in the pathogenesis of ACC is 11p, the area of abnormality in Beckwith-Wiedemann syndrome and the site of the insulin-like growth factor-2 (IGF-2) gene. LOH at the 11p15 locus and overexpression of IGF-2 have been associated with the malignant phenotype in sporadic ACCs.[11] However, other growth-related tumor suppressor genes at this locus may also be involved.[12]
Most adrenocortical tumors are monoclonal, suggesting that they result from accumulated genetic abnormalities, such as activation of proto-oncogenes and inactivation of tumor suppressor genes.
- Beta-catenin mutations (CTNNB1):
- Constitutive activation of beta-catenin in the Wnt signaling pathway has been identified as a frequent alteration in benign and malignant adrenocortical tumors[13].
- The increased occurrence of adrenal tumors in patients with mutations of adenomatous polyposis coli (APC) suggested that the Wnt/beta-catenin pathway could be involved in adrenal tumorigenesis.[14]
- This pathway is essential for embryonic development of the adrenal, and its ectopic constitutive activation is associated with cancer development in a number of tissues.[15]
- Aberrant receptors:
- Somatic mutations of protein kinase A (PKA) catalytic subunit (PRKACA) were identified in patients with overt Cushing’s syndrome but not in adenomas secreting less cortisol.[16]
- In additional reports, the same mutation was found in over 50 percent of patients with Cushing’s syndrome due to adrenal adenomas.[17]
- The most frequent hotspot p.Leu206Arg mutation is located in the active cleft of the catalytic subunit, inactivating the site where the regulatory subunit RII-beta usually binds, thus causing a constitutive PKA activation.
Mutations in aldosterone-producing adenomas
- The most frequent causes of primary aldosteronism include bilateral idiopathic hyperplasia and unilateral aldosterone-producing adenoma.[18]
- Somatic mutations in KCNJ5 have been identified in patients with primary aldosteronism due to APAs.
- These mutations are more common in women than men; APAs with KCNJ5 mutations are larger than those without mutations.
- Somatic mutations in other important genes implicated in regulation of aldosterone synthesis (ATP1A1, ATP2B3, CACNA1D, CTNNB1, ARMC5) have also been identified.
Associated Conditions
- Most adrenocortical carcinomas are sporadic, but some occur as a component of hereditary cancer syndromes.[19][20]
- Hereditary cancer syndromes:
- Li-Fraumeni syndrome (associated with inactivating mutations of the TP53 tumor suppressor gene on chromosome 17p):
- Breast cancer
- Soft tissue and bone sarcoma
- Brain tumors
- Beckwith-Wiedemann syndrome (associated with abnormalities in 11p15):
- Multiple endocrine neoplasia type 1 (MEN1) (associated with inactivating mutations of the MEN1 gene on chromosome 11q):
- Li-Fraumeni syndrome (associated with inactivating mutations of the TP53 tumor suppressor gene on chromosome 17p):
Gross Pathology
- On gross pathology, adrenocortical adenoma is a solitary unilateral well-circumscribed mass.
- Size usually varies from 2–5 cm in diameter.
- The color of tumor is yellow due to the stored lipid (cholesterol) from which the cortical hormones are synthesized.
- Weight usually < 50 grams.
- Functional ACA may result in atrophy of ipsilateral or contralateral adrenal cortex.
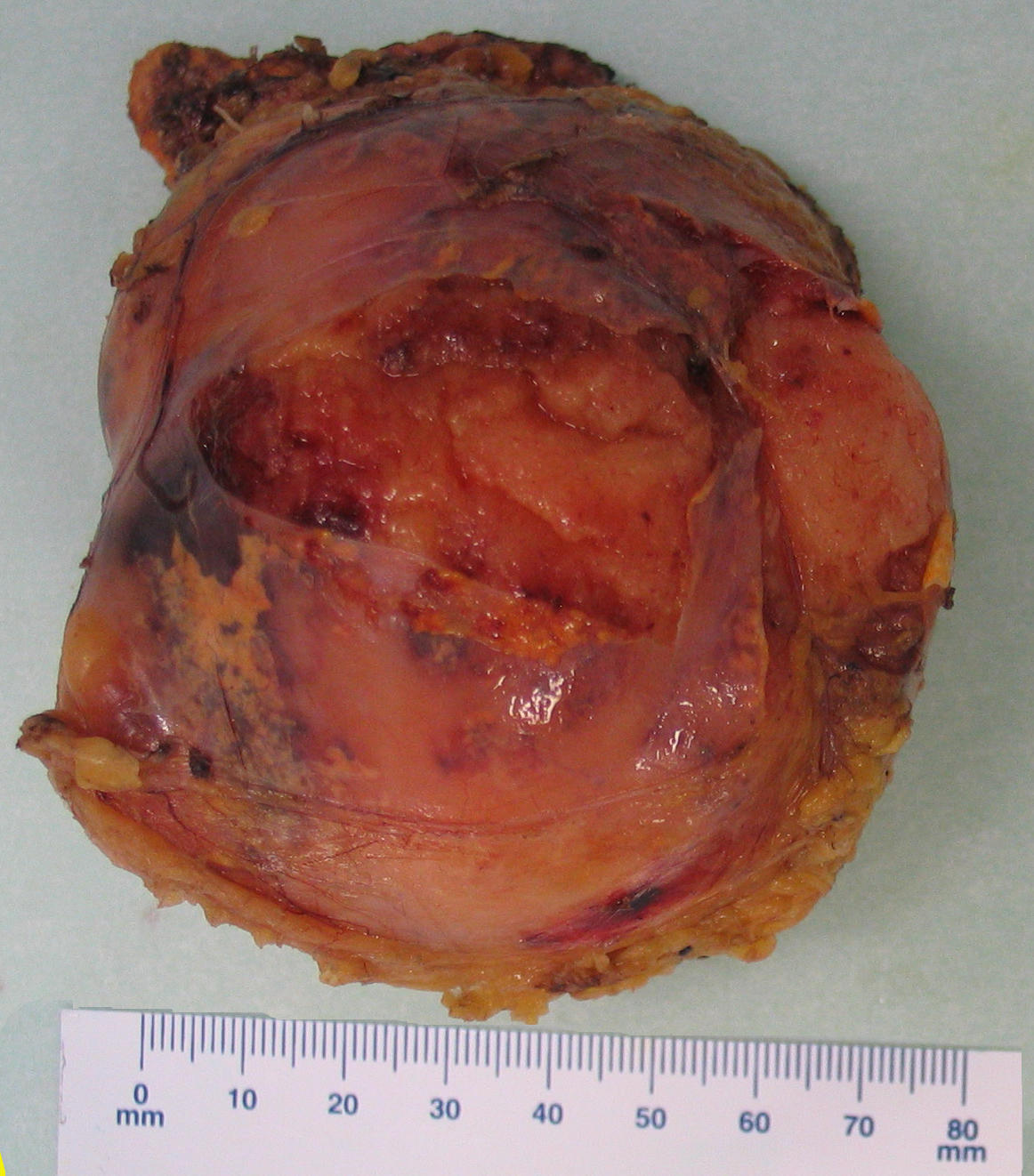
- On gross pathology, adrenocortical carcinomas are often large ( > 5 cm in largest diameter).
- Cut surface is full of areas of hemorrhage and necrosis.
- ACC color ranges from brown to orange depending on the lipid content of their cells.
- ACC is unencapsulated, often soft and friable.
- On gross pathology, pheochromocytoma varies from small to large and usually associated with hemorrhage and necrosis.[21]
- Pheochromocytoma are usually lobulated and small tumors have compressed adrenal gland.
- Familial tumors are bilateral.
- It may be associated with hyperplasia in the adjacent medulla.
- Chromaffin reaction: Fresh tumor cut section turns dark brown if add potassium dichromate at pH 5-6.
- On gross pathology, myelolipoma usually occurs unilateral (one adrenal gland).
- Myelolipoma diameter ranges from small (few millimeters) to large (34 centimeters).
- The cut surface has colors varying from yellow to red to brown, depending on the distribution of fat and blood.
-
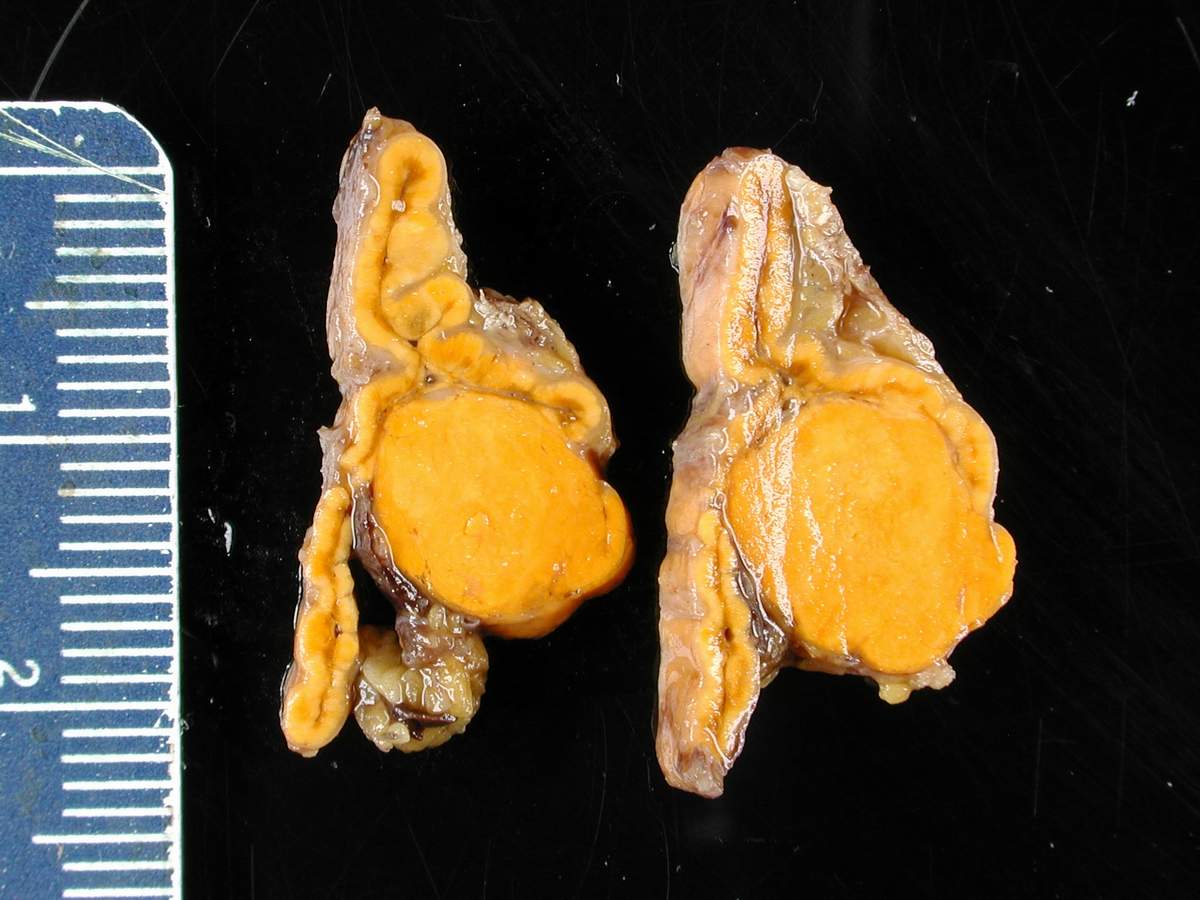 Adrenocortical adenoma gross pathology, source: By Nephron – Own work, CC BY-SA 3.0, https://commons.wikimedia.org/w/index.php?curid=5938524
Adrenocortical adenoma gross pathology, source: By Nephron – Own work, CC BY-SA 3.0, https://commons.wikimedia.org/w/index.php?curid=5938524 -
![Adrenocortical carcinoma gross pathology, source: By AFIP Atlas of Tumor Pathology - [1], Public Domain, https://commons.wikimedia.org/w/index.php?curid=6719487](https://www.wikidoc.org/images/1/18/Adrenal_cortical_carcinoma.JPG) Adrenocortical carcinoma gross pathology, source: By AFIP Atlas of Tumor Pathology – [1], Public Domain, https://commons.wikimedia.org/w/index.php?curid=6719487
Adrenocortical carcinoma gross pathology, source: By AFIP Atlas of Tumor Pathology – [1], Public Domain, https://commons.wikimedia.org/w/index.php?curid=6719487 -
 Myelolipoma gross pathology,source: By Mattopaedia – Own work, CC BY-SA 3.0, https://commons.wikimedia.org/w/index.php?curid=5668284
Myelolipoma gross pathology,source: By Mattopaedia – Own work, CC BY-SA 3.0, https://commons.wikimedia.org/w/index.php?curid=5668284 -
![Bilateral pheochromocytoma in MEN2. Gross image, source: By AFIP Atlas of Tumor Pathology - [1], Public Domain, https://commons.wikimedia.org/w/index.php?curid=4288117](https://www.wikidoc.org/images/5/5f/Bilateral_pheo_MEN2.jpg) Bilateral pheochromocytoma in MEN2. Gross image, source: By AFIP Atlas of Tumor Pathology – [1], Public Domain, https://commons.wikimedia.org/w/index.php?curid=4288117
Bilateral pheochromocytoma in MEN2. Gross image, source: By AFIP Atlas of Tumor Pathology – [1], Public Domain, https://commons.wikimedia.org/w/index.php?curid=4288117

![Adrenocortical carcinoma gross pathology, source: By AFIP Atlas of Tumor Pathology - [1], Public Domain, https://commons.wikimedia.org/w/index.php?curid=6719487](https://www.wikidoc.org/index.php/File%3AAdrenal_cortical_carcinoma.JPG)

![Bilateral pheochromocytoma in MEN2. Gross image, source: By AFIP Atlas of Tumor Pathology - [1], Public Domain, https://commons.wikimedia.org/w/index.php?curid=4288117](https://www.wikidoc.org/index.php/File%3ABilateral_pheo_MEN2.jpg)
Microscopic Pathology
Adrenal adenoma and carcinoma
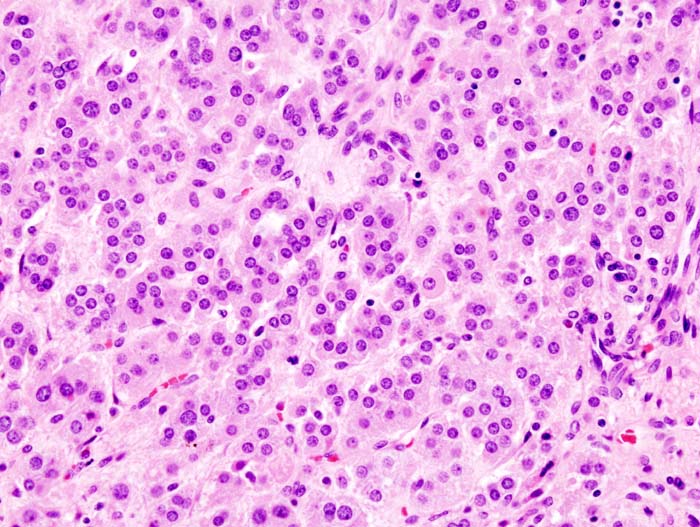
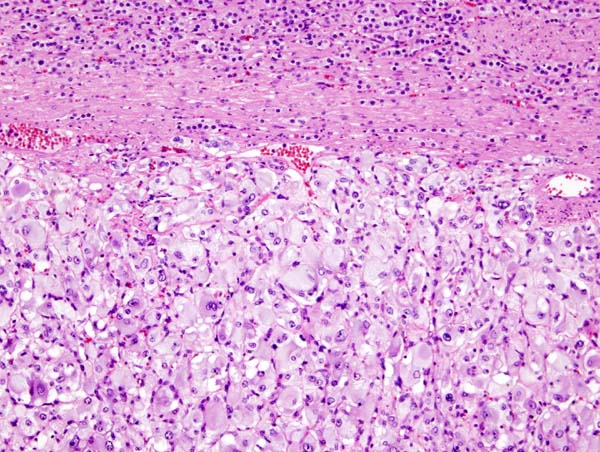
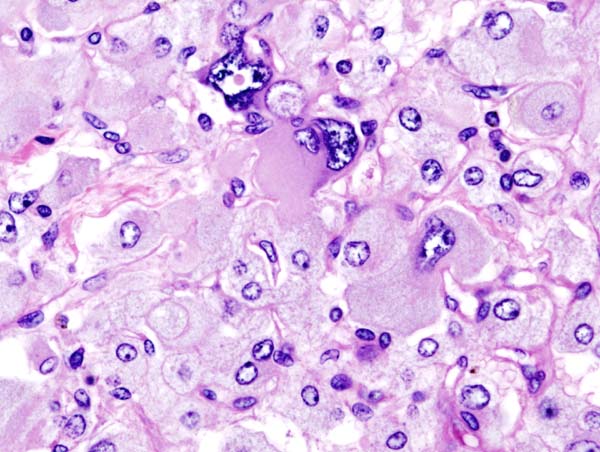
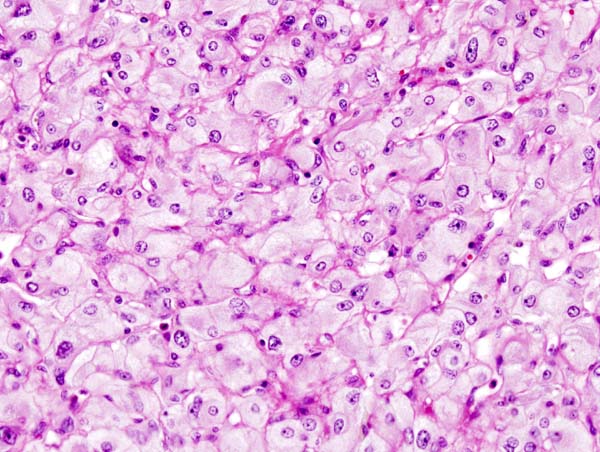
- On microscopic examination, the tumor usually displays sheets of atypical cells with some resemblance to the cells of the normal adrenal cortex. The presence of invasion and mitotic activity help differentiate small cancers from adrenocortical adenomas.[5][22]
- In comparison to surrounding adrenal gland, Adrenal cortical adenoma cells are larger, different cytoplasm, increased variation in nuclear size
- Distinct cell borders, cells have abundant foamy cytoplasm reminiscent of zona fasciculata
- Balloon cells: clusters of cells with enlarged lipid-rich cytoplasm
Pheochromocytoma
On microscopic pathology, pheochromocytoma typically demonstrates a nesting (Zellballen) pattern on microscopy. This pattern is composed of well-defined clusters of tumor cells containing eosinophilic cytoplasm separated by fibrovascular stroma.[23][24]
Myelolipoma
- Islands of hematopoietic cells and mature fat.
- Usually show normal trilineage hematopoiesis, but often with markedly increased megakaryocytes.
- Larger tumors may have hemorrhage, necrosis, calcification and cysts.
- Rarely may have areas of fibromyxoid degeneration resembling low grade fibromyxoid sarcoma.
-
 Adrenal adenoma microscopic picture, source: By Michael Feldman, MD, PhDUniversity of Pennsylvania School of Medicine – CC BY-SA 3.0, https://commons.wikimedia.org/w/index.php?curid=535950
Adrenal adenoma microscopic picture, source: By Michael Feldman, MD, PhDUniversity of Pennsylvania School of Medicine – CC BY-SA 3.0, https://commons.wikimedia.org/w/index.php?curid=535950 -
![Adrenocortical carcinoma microscopic picture, source: By AFIP Atlas of Tumor Pathology - [1], Public Domain, https://commons.wikimedia.org/w/index.php?curid=6719510](https://www.wikidoc.org/images/a/a0/Adrenal_cortical_carcinoma_%281%29.jpg) Adrenocortical carcinoma microscopic picture, source: By AFIP Atlas of Tumor Pathology – [1], Public Domain, https://commons.wikimedia.org/w/index.php?curid=6719510
Adrenocortical carcinoma microscopic picture, source: By AFIP Atlas of Tumor Pathology – [1], Public Domain, https://commons.wikimedia.org/w/index.php?curid=6719510 -
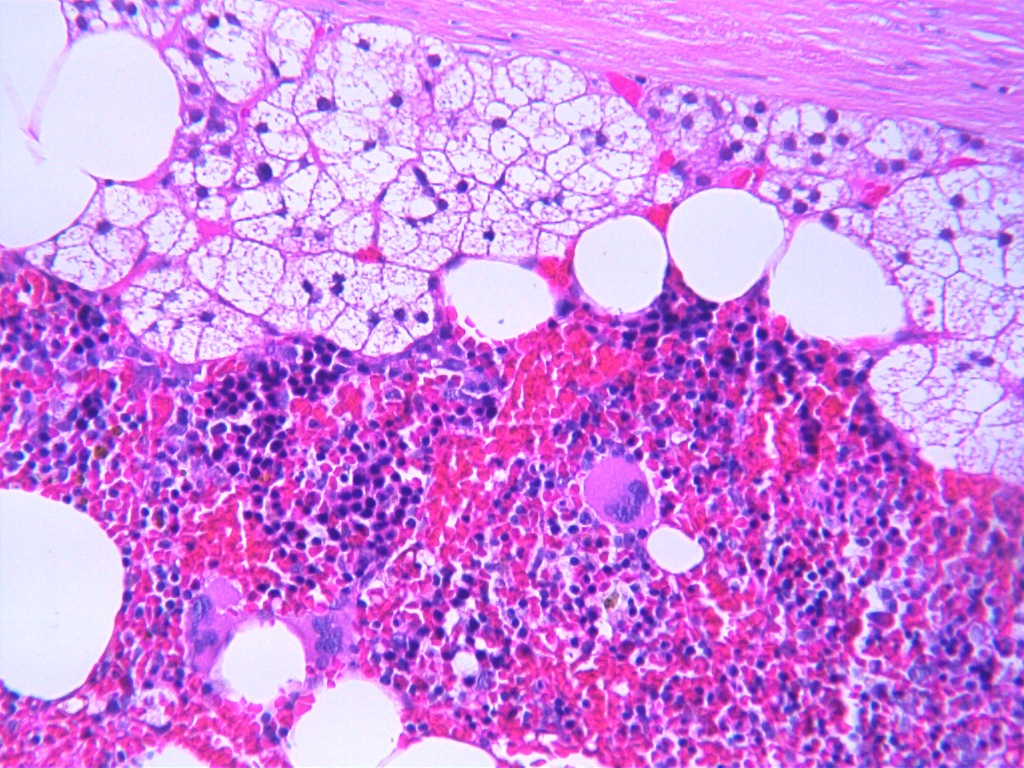 Myelolipoma microscopic picture, source: By Mattopaedia – Own work, CC BY-SA 3.0, https://commons.wikimedia.org/w/index.php?curid=5688142
Myelolipoma microscopic picture, source: By Mattopaedia – Own work, CC BY-SA 3.0, https://commons.wikimedia.org/w/index.php?curid=5688142 -
 Micrograph of pheochromocytoma, source: By Nephron – Own work, CC BY-SA 3.0, https://commons.wikimedia.org/w/index.php?curid=5938524
Micrograph of pheochromocytoma, source: By Nephron – Own work, CC BY-SA 3.0, https://commons.wikimedia.org/w/index.php?curid=5938524 -
 Histopathology of adrenal pheochromocytoma. Adrenectomy specimen, source: Wikipedia
Histopathology of adrenal pheochromocytoma. Adrenectomy specimen, source: Wikipedia -
 Micrograph of pheochromocytoma, source: Wikipedia
Micrograph of pheochromocytoma, source: Wikipedia -
Micrograph of pheochromocytoma, source: Wikipedia

![Adrenocortical carcinoma microscopic picture, source: By AFIP Atlas of Tumor Pathology - [1], Public Domain, https://commons.wikimedia.org/w/index.php?curid=6719510](https://www.wikidoc.org/index.php/File%3AAdrenal_cortical_carcinoma_%281%29.jpg)




References
- ↑ Grumbach MM, Biller BM, Braunstein GD, Campbell KK, Carney JA, Godley PA; et al. (2003). “Management of the clinically inapparent adrenal mass (“incidentaloma”)”. Ann Intern Med. 138 (5): 424–9. PMID 12614096.
- ↑ Young WF (2000). “Management approaches to adrenal incidentalomas. A view from Rochester, Minnesota”. Endocrinol Metab Clin North Am. 29 (1): 159–85, x. PMID 10732270.
- ↑ Sidhu S, Sywak M, Robinson B, Delbridge L (2004). “Adrenocortical cancer: recent clinical and molecular advances”. Curr Opin Oncol. 16 (1): 13–8. PMID 14685087.
- ↑ Lacroix A, Feelders RA, Stratakis CA, Nieman LK (2015). “Cushing’s syndrome”. Lancet. 386 (9996): 913–27. doi:10.1016/S0140-6736(14)61375-1. PMID 26004339.
- ↑ Raff H, Carroll T (2015). “Cushing’s syndrome: from physiological principles to diagnosis and clinical care”. J Physiol. 593 (3): 493–506. doi:10.1113/jphysiol.2014.282871. PMC 4324701. PMID 25480800.
- ↑ Else T, Kim AC, Sabolch A, Raymond VM, Kandathil A, Caoili EM; et al. (2014). “Adrenocortical carcinoma”. Endocr Rev. 35 (2): 282–326. doi:10.1210/er.2013-1029. PMC 3963263. PMID 24423978.
- ↑ Raff H, Carroll T (2015). “Cushing’s syndrome: from physiological principles to diagnosis and clinical care”. J Physiol. 593 (3): 493–506. doi:10.1113/jphysiol.2014.282871. PMC 4324701. PMID 25480800.
- ↑ Arnall DA, Marker JC, Conlee RK, Winder WW (1986). “Effect of infusing epinephrine on liver and muscle glycogenolysis during exercise in rats”. Am J Physiol. 250 (6 Pt 1): E641–9. PMID 3521311.
- ↑ Gicquel C, Bertagna X, Gaston V, Coste J, Louvel A, Baudin E; et al. (2001). “Molecular markers and long-term recurrences in a large cohort of patients with sporadic adrenocortical tumors”. Cancer Res. 61 (18): 6762–7. PMID 11559548.
- ↑ Libè R, Groussin L, Tissier F, Elie C, René-Corail F, Fratticci A; et al. (2007). “Somatic TP53 mutations are relatively rare among adrenocortical cancers with the frequent 17p13 loss of heterozygosity”. Clin Cancer Res. 13 (3): 844–50. doi:10.1158/1078-0432.CCR-06-2085. PMID 17289876.
- ↑ Gicquel C, Raffin-Sanson ML, Gaston V, Bertagna X, Plouin PF, Schlumberger M; et al. (1997). “Structural and functional abnormalities at 11p15 are associated with the malignant phenotype in sporadic adrenocortical tumors: study on a series of 82 tumors”. J Clin Endocrinol Metab. 82 (8): 2559–65. doi:10.1210/jcem.82.8.4170. PMID 9253334.
- ↑ Bourcigaux N, Gaston V, Logié A, Bertagna X, Le Bouc Y, Gicquel C (2000). “High expression of cyclin E and G1 CDK and loss of function of p57KIP2 are involved in proliferation of malignant sporadic adrenocortical tumors”. J Clin Endocrinol Metab. 85 (1): 322–30. doi:10.1210/jcem.85.1.6303. PMID 10634406.
- ↑ Mazzuco TL, Durand J, Chapman A, Crespigio J, Bourdeau I (2012). “Genetic aspects of adrenocortical tumours and hyperplasias”. Clin Endocrinol (Oxf). 77 (1): 1–10. doi:10.1111/j.1365-2265.2012.04403.x. PMID 22471738.
- ↑ Smith TG, Clark SK, Katz DE, Reznek RH, Phillips RK (2000). “Adrenal masses are associated with familial adenomatous polyposis”. Dis Colon Rectum. 43 (12): 1739–42. PMID 11156460.
- ↑ Kikuchi A (2003). “Tumor formation by genetic mutations in the components of the Wnt signaling pathway”. Cancer Sci. 94 (3): 225–9. PMID 12824913.
- ↑ Beuschlein F, Fassnacht M, Assié G, Calebiro D, Stratakis CA, Osswald A; et al. (2014). “Constitutive activation of PKA catalytic subunit in adrenal Cushing’s syndrome”. N Engl J Med. 370 (11): 1019–28. doi:10.1056/NEJMoa1310359. PMC 4727447. PMID 24571724.
- ↑ Ronchi CL, Di Dalmazi G, Faillot S, Sbiera S, Assié G, Weigand I; et al. (2016). “Genetic Landscape of Sporadic Unilateral Adrenocortical Adenomas Without PRKACA p.Leu206Arg Mutation”. J Clin Endocrinol Metab. 101 (9): 3526–38. doi:10.1210/jc.2016-1586. PMID 27389594.
- ↑ Monticone S, Castellano I, Versace K, Lucatello B, Veglio F, Gomez-Sanchez CE; et al. (2015). “Immunohistochemical, genetic and clinical characterization of sporadic aldosterone-producing adenomas”. Mol Cell Endocrinol. 411: 146–54. doi:10.1016/j.mce.2015.04.022. PMC 4474471. PMID 25958045.
- ↑ Koch CA, Pacak K, Chrousos GP (2002). “The molecular pathogenesis of hereditary and sporadic adrenocortical and adrenomedullary tumors”. J Clin Endocrinol Metab. 87 (12): 5367–84. doi:10.1210/jc.2002-021069. PMID 12466322.
- ↑ Lynch HT, Radford B, Lynch JF (1990). “SBLA syndrome revisited”. Oncology. 47 (1): 75–9. PMID 2300390.
- ↑ Sajjanar AB, Athanikar VS, Dinesh US, Nanjappa B, Patil PB (2015). “Non Functional Unilateral Adrenal Myelolipoma, A Case Report”. J Clin Diagn Res. 9 (6): ED03–4. doi:10.7860/JCDR/2015/13209.6070. PMC 4525519. PMID 26266130.
- ↑ Mondal SK, Dasgupta S, Jain P, Mandal PK, Sinha SK (2013). “Histopathological study of adrenocortical carcinoma with special reference to the Weiss system and TNM staging and the role of immunohistochemistry to differentiate it from renal cell carcinoma”. J Cancer Res Ther. 9 (3): 436–41. doi:10.4103/0973-1482.119329. PMID 24125979.
- ↑ Bezuglova TV (2003). “Criteria for predicting the outcome of pheochromocytoma by the immunohistochemical and electron microscopic findings”. Bull Exp Biol Med. 136 (4): 408–10. PMID 14714096.
- ↑ Sporny S, Musiał J (2005). “[Markers of malignancy in pheochromocytomas]”. Endokrynol Pol. 56 (6): 946–51. PMID 16821216.
Causes
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Mohammed Abdelwahed M.D[2]
Overview
Common causes of incidentaloma include adenoma, carcinoma, pheochromocytoma, congenital adrenal hyperplasia, massive macronodular adrenal disease, and nodular variant of Cushing’s disease. Less Common Causes include myelolipoma, neuroblastoma, ganglioneuroma, hemangioma.
Causes
Common Causes
The common causes of incidentaloma include:[1][2]
- Adenoma (nonfunctioning, cortisol-secreting, aldosterone-secreting, and pheochromocytoma)
- Carcinoma (any adrenal hormone)
- Pheochromocytoma
- Congenital adrenal hyperplasia
- Massive macro-nodular adrenal disease
- Nodular variant of Cushing’s disease
Less Common Causes
The less common causes of incidentaloma include:[3][4][5][6][7]
- Infiltrative diseases
- Myelolipoma
- Neuroblastoma
- Ganglioneuroma
- Hemangioma
- Carcinoma
- Metastasis
- Cyst
- Hemorrhage
- Granuloma
- Amyloidosis
References
- ↑ Nieman LK (2010). “Approach to the patient with an adrenal incidentaloma”. J Clin Endocrinol Metab. 95 (9): 4106–13. doi:10.1210/jc.2010-0457. PMC 2936073. PMID 20823463.
- ↑ Barzon L, Sonino N, Fallo F, Palu G, Boscaro M (2003). “Prevalence and natural history of adrenal incidentalomas”. Eur J Endocrinol. 149 (4): 273–85. PMID 14514341.
- ↑ Young WF (2007). “Clinical practice. The incidentally discovered adrenal mass”. N Engl J Med. 356 (6): 601–10. doi:10.1056/NEJMcp065470. PMID 17287480.
- ↑ “NIH state-of-the-science statement on management of the clinically inapparent adrenal mass (“incidentaloma”)”. NIH Consens State Sci Statements. 19 (2): 1–25. 2002. PMID 14768652.
- ↑ Mantero F, Terzolo M, Arnaldi G, Osella G, Masini AM, Alì A; et al. (2000). “A survey on adrenal incidentaloma in Italy. Study Group on Adrenal Tumors of the Italian Society of Endocrinology”. J Clin Endocrinol Metab. 85 (2): 637–44. doi:10.1210/jcem.85.2.6372. PMID 10690869.
- ↑ Bernini G, Moretti A, Argenio G, Salvetti A (2002). “Primary aldosteronism in normokalemic patients with adrenal incidentalomas”. Eur J Endocrinol. 146 (4): 523–9. PMID 11916621.
- ↑ Mansmann G, Lau J, Balk E, Rothberg M, Miyachi Y, Bornstein SR (2004). “The clinically inapparent adrenal mass: update in diagnosis and management”. Endocr Rev. 25 (2): 309–40. doi:10.1210/er.2002-0031. PMID 15082524.
Differentiating Incidentaloma from other Diseases
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Mohammed Abdelwahed M.D[2]
Overview
Adrenal incidentaloma must be differentiated from other diseases that cause adrenal masses such as adrenal adenoma, adrenocortical carcinoma, Cushing’s syndrome, pheochromocytoma, metastasis, and other causes of bilateral adrenal masses.
Differentiating different causese of Incidentaloma
- The cause of adrenal incidentaloma commonly include adrenal adenoma, sub-clinical Cushing’s syndrome, pheochromocytoma, and adrenocortical carcinoma. These causes can be differentiated from each other as follows:
| Differential Diagnosis | Clinical picture | Imagings | Laboratory tests | |
|---|---|---|---|---|
| Adrenal adenoma |
|
|
| |
| Adrenocortical carcinoma |
|
|
| |
| Cushing’s syndrome |
|
|
| |
| Pheochromocytoma |
|
|
| |
| Adrenal metastasis |
|
|
Differential diagnosis of Cushing’s disease from other diseases
The table below summarizes the findings that differentiate Cushing’s disease from other conditions that may cause hypertension, hyperandrogenism, and obesity. Facial plethora, skin changes, osteoporosis, nephrolithiasis and neuropsychiatric conditions should raise the concern for Cushing’s syndrome.[1][2][3][4]
Differentiating pheochromocytoma from other diseasesPheochromocytoma must be differentiated from other causes of paroxysmal hypertension. The differentials include:
References
|
Epidemiology and Demographics
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Mohammed Abdelwahed M.D[2]
Overview
The Prevalence of clinically inapparent adrenal masses (≥1 cm in diameter) in adults was estimated to be between 1 and 6%. The vast majority of adrenal incidentalomas are nonfunctioning benign tumors. The prevalence of adrenal incidentalomas increases with age especially in obese, diabetic, and hypertensive patients. There is no racial or gender predilection to adrenal incidentaloma.
Epidemiology and Demographics
Incidence and Prevalence
- The incidence and prevalence of adrenal incidentaloma can only be assessed from imaging or autopsy studies.
- The prevalence of adrenal incidentaloma in adults was estimated to be between 1 and 6%, with a peak prevalence of (≤7%) reported in the 5th to 7th decades. .[1][2]
- The recent development in imaging and diagnostic modalities has been associated with an increase in the prevalence of adrenal incidentaloma.
- The vast majority of adrenal incidentalomas are nonfunctioning benign tumors; of which the nonfunctioning cortical adenomas are constituting about 75%.[3][4][5]
- The functional tumors represent about 14% of adrenal incidentalomas which may release cortisol, aldosterone, or both in rare occasions.
- Prevalence of pheochromocytoma is 4–7% of incidentalomas.[6]
- Prevalence of hyperaldosteronism is 1.1 to 10%.[7]
- The incidence of primary adrenal carcinoma or metastases in patients with adrenal incidentaloma is approximately 4%.[8]
- The risk of malignancy over time for masses defined as benign at diagnosis is estimated at about 1/1000, even though 5-25% of masses increase in size during follow-up.[9]
- Hyperfunction develops in about 1.7% of cases and the risk is higher in patients with lesions larger than 3 cm.[9]
- The prevalence is higher in obese, diabetic, and hypertensive patients.[10]
Age
- The prevalence of adrenal incidentalomas increases with age. It is less than 1% in patients younger than 30 yr of age and up to 7% in patients over age 70.[10][11]
- In childhood, adrenal incidentalomas are extremely rare.
- Adrenal incidentaloma is more common in older patients.
Race
- There is no racial predilection to adrenal incidentaloma.
Gender
- There is no gender predilection to adrenal incidentaloma.
References
- ↑ Dietrich CF, Correas JM, Dong Y, Nolsoe C, Westerway SC, Jenssen C (2020). “WFUMB position paper on the management incidental findings: adrenal incidentaloma”. Ultrasonography. 39 (1): 11–21. doi:10.14366/usg.19029. PMC 6920619 Check
|pmc=value (help). PMID 31786909. - ↑ Sherlock M, Scarsbrook A, Abbas A, Fraser S, Limumpornpetch P, Dineen R; et al. (2020). “Adrenal Incidentaloma”. Endocr Rev. 41 (6). doi:10.1210/endrev/bnaa008. PMC 7431180 Check
|pmc=value (help). PMID 32266384 Check|pmid=value (help). - ↑ Barzon L, Sonino N, Fallo F, Palu G, Boscaro M (2003). “Prevalence and natural history of adrenal incidentalomas”. Eur J Endocrinol. 149 (4): 273–85. doi:10.1530/eje.0.1490273. PMID 14514341.
- ↑ Mantero F, Terzolo M, Arnaldi G, Osella G, Masini AM, Alì A; et al. (2000). “A survey on adrenal incidentaloma in Italy. Study Group on Adrenal Tumors of the Italian Society of Endocrinology”. J Clin Endocrinol Metab. 85 (2): 637–44. doi:10.1210/jcem.85.2.6372. PMID 10690869.
- ↑ Lam KY, Lo CY (2002). “Metastatic tumours of the adrenal glands: a 30-year experience in a teaching hospital”. Clin Endocrinol (Oxf). 56 (1): 95–101. doi:10.1046/j.0300-0664.2001.01435.x. PMID 11849252.
- ↑ Mantero F, Masini AM, Opocher G, Giovagnetti M, Arnaldi G (1997). “Adrenal incidentaloma: an overview of hormonal data from the National Italian Study Group”. Horm Res. 47 (4–6): 284–9. PMID 9167966.
- ↑ Funder JW, Carey RM, Mantero F, Murad MH, Reincke M, Shibata H; et al. (2016). “The Management of Primary Aldosteronism: Case Detection, Diagnosis, and Treatment: An Endocrine Society Clinical Practice Guideline”. J Clin Endocrinol Metab. 101 (5): 1889–916. doi:10.1210/jc.2015-4061. PMID 26934393.
- ↑ Fassnacht M, Arlt W, Bancos I, Dralle H, Newell-Price J, Sahdev A; et al. (2016). “Management of adrenal incidentalomas: European Society of Endocrinology Clinical Practice Guideline in collaboration with the European Network for the Study of Adrenal Tumors”. Eur J Endocrinol. 175 (2): G1–G34. doi:10.1530/EJE-16-0467. PMID 27390021.
- ↑ 9.0 9.1 Barzon L, Sonino N, Fallo F, Palu G, Boscaro M (2003). “Prevalence and natural history of adrenal incidentalomas”. Eur J Endocrinol. 149 (4): 273–85. PMID 14514341.
- ↑ 10.0 10.1 Grumbach MM, Biller BM, Braunstein GD, Campbell KK, Carney JA, Godley PA; et al. (2003). “Management of the clinically inapparent adrenal mass (“incidentaloma”)”. Ann Intern Med. 138 (5): 424–9. PMID 12614096.
- ↑ Mansmann G, Lau J, Balk E, Rothberg M, Miyachi Y, Bornstein SR (2004). “The clinically inapparent adrenal mass: update in diagnosis and management”. Endocr Rev. 25 (2): 309–40. doi:10.1210/er.2002-0031. PMID 15082524.
Risk Factors
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Mohammed Abdelwahed M.D[2]
Overview
Most adrenocortical carcinomas are sporadic, but some occur as a component of hereditary cancer syndromes such as Li-Fraumeni syndrome, Beckwith-Wiedemann syndrome, and Multiple endocrine neoplasia type 1(MEN1).
Risk Factors
Most adrenocortical carcinomas are sporadic, but some occur as a component of hereditary cancer syndromes.[1][2]
- Hereditary cancer syndromes:
- Li-Fraumeni syndrome (associated with inactivating mutations of the TP53 tumor suppressor gene on chromosome 17p):
- Breast cancer
- Soft tissue and bone sarcoma
- Brain tumors
- Beckwith-Wiedemann syndrome (associated with abnormalities in 11p15):
- Multiple endocrine neoplasia type 1 (MEN1) (associated with inactivating mutations of the MEN1 gene on chromosome 11q):
- Li-Fraumeni syndrome (associated with inactivating mutations of the TP53 tumor suppressor gene on chromosome 17p):
References
- ↑ Sidhu S, Sywak M, Robinson B, Delbridge L (2004). “Adrenocortical cancer: recent clinical and molecular advances”. Curr Opin Oncol. 16 (1): 13–8. PMID 14685087.
- ↑ Lynch HT, Radford B, Lynch JF (1990). “SBLA syndrome revisited”. Oncology. 47 (1): 75–9. PMID 2300390.
Screening
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Mohammed Abdelwahed M.D[2]
Overview
According to the European Society of Endocrinology Clinical Practice Guideline, screening for adrenal incidentaloma includes: family screening for patients with bilateral macronodular hyperplasia, patients with asymptomatic vertebral fractures, patients with possible autonomous cortisol secretion, and patients with a hereditary syndrome leading to adrenal tumors. Screening test include 24-hour urine fractionated metanephrines for pheochromocytoma, 24-hour urinary free cortisol for patients with symptoms of Cushing’s syndrome, and Plasma aldosterone concentration, plasma renin activity for patients with Primary aldosteronism.
Screening
According to the European Society of Endocrinology Clinical Practice Guideline, screening for adrenal incidentaloma includes:[1]
Indications for adrenal incidentaloma screening
- Patients with possible autonomous cortisol secretion for hypertension and type 2 diabetes mellitus.
- Patients with asymptomatic vertebral fractures.
- Screening imaging in patients with a hereditary syndrome leading to adrenal tumors.
- Family screening with 1 mg dexamethasone test can be considered in cases of bilateral macronodular hyperplasia, especially in younger patients.
Screening measures
| Disease | Laboratory tests |
|---|---|
| Pheochromocytoma[2] | 24-hour urine:
Blood: |
| Cushing’s syndrome[3] | For patients with symptoms of Cushing’s syndrome:
For patients lacking symptoms of Cushing’s syndrome:
|
| Primary aldosteronism[4] | Plasma aldosterone concentration, plasma renin activity |
Biochemical Evaluation in Patients with Adrenal Incidentaloma
Mild Autonomous Cortisol Excess
- It refers to an abnormal increase in cortisol secretion that is independent of normal hypothalamic–pituitary control without the clinical picture of of Cushing’s syndrome, also known as subclinical Cushing’s syndrome.
- It is the most common functional disorder in patients with adrenal incidentaloma with a prevalence of 10%.[5][6]
- It is frequently associated with coexisting conditions such as obesity, insulin resistance or type 2 diabetes mellitus, dyslipidemia, hypertension, and osteoporosis than in nonfunctioning adrenal tumors.[7]
- Screening test: Overnight dexamethasone (1 mg) suppression test; an abnormal result is a serum cortisol level >1.8 μg per deciliter (50 nmol per liter) with confirmation of serum dexamethasone level (to ensure adherence); a higher serum cortisol cutoff level (e.g., 3–5 μg per deciliter) can be used to reduce the risk of a false positive.
- Confirmatory test: Measurement of levels of morning serum corticotropin and cortisol levels, 24-hr urinary cortisol, late-night salivary cortisol, midnight serum cortisol, and DHEAS.
- False positives may occur in patients receiving medications that accelerate hepatic metabolism of dexamethasone and with nonadherence to dexamethasone.
- Consider a pseudo-Cushing’s syndrome state due to diabetes, obesity, pregnancy, alcoholism, psychiatric disorders.
Pheochromocytoma
- Measurement of levels of plasma-free metanephrines or 24-hr urinary fractionated metanephrines.
- False positives may occur in patients with stress and illness warranting hospitalization; with medications that increase levels of endogenous catecholamines; with excessive caffeine; and with recreational drug use (e.g., amphetamines).
- Biochemical testing may not be necessary if the adrenal mass has CT attenuation of ≤10 Hounsfield units; genetic testing for inherited syndrome should be performed, regardless of family history, if screening test is positive.
Primary hyperaldosteronism
- Screening test: Measurement of mid-morning plasma aldosterone concentration and plasma renin activity; a ratio of plasma aldosterone concentration to plasma renin activity >20 confirms diagnosis.
- Confirmatory test: If the ratio of plasma aldosterone concentration to plasma renin activity <20, confirmatory testing includes 24-hr urinary aldosterone excretion test with patient receiving high-sodium diet, aldosterone suppression test, and testing with saline infusion while patient is sitting.
- False positives can be caused by beta-blockers, methyldopa, clonidine, nonsteroidal anti-inflammatory drugs, and oral contraceptives and estrogen; false negatives can be caused by angiotensin-converting–enzyme inhibitors, angiotensin II receptor blockers, and potassium-sparing diuretics (e.g., spironolactone, eplerenone, and amiloride).
- If patient is a candidate for adrenalectomy and >35 yr of age, adrenal venous sampling is recommended to confirm lateralization of aldosterone to the side of the adrenal mass (some patients have bilateral aldosterone hypersecretion, or the contralateral adrenal gland may be the source of excess aldosterone and the tumor detected is nonfunctioning)
References
- ↑ Fassnacht M, Arlt W, Bancos I, Dralle H, Newell-Price J, Sahdev A; et al. (2016). “Management of adrenal incidentalomas: European Society of Endocrinology Clinical Practice Guideline in collaboration with the European Network for the Study of Adrenal Tumors”. Eur J Endocrinol. 175 (2): G1–G34. doi:10.1530/EJE-16-0467. PMID 27390021.
- ↑ Grumbach MM, Biller BM, Braunstein GD, Campbell KK, Carney JA, Godley PA; et al. (2003). “Management of the clinically inapparent adrenal mass (“incidentaloma”)”. Ann Intern Med. 138 (5): 424–9. PMID 12614096.
- ↑ Valli N, Catargi B, Ronci N, Vergnot V, Leccia F, Ferriere JM; et al. (2001). “Biochemical screening for subclinical cortisol-secreting adenomas amongst adrenal incidentalomas”. Eur J Endocrinol. 144 (4): 401–8. PMID 11275951.
- ↑ Young WF (2007). “Clinical practice. The incidentally discovered adrenal mass”. N Engl J Med. 356 (6): 601–10. doi:10.1056/NEJMcp065470. PMID 17287480.
- ↑ Barzon L, Sonino N, Fallo F, Palu G, Boscaro M (2003). “Prevalence and natural history of adrenal incidentalomas”. Eur J Endocrinol. 149 (4): 273–85. doi:10.1530/eje.0.1490273. PMID 14514341.
- ↑ Mantero F, Terzolo M, Arnaldi G, Osella G, Masini AM, Alì A; et al. (2000). “A survey on adrenal incidentaloma in Italy. Study Group on Adrenal Tumors of the Italian Society of Endocrinology”. J Clin Endocrinol Metab. 85 (2): 637–44. doi:10.1210/jcem.85.2.6372. PMID 10690869.
- ↑ Sbardella E, Minnetti M, D’Aluisio D, Rizza L, Di Giorgio MR, Vinci F; et al. (2018). “Cardiovascular features of possible autonomous cortisol secretion in patients with adrenal incidentalomas”. Eur J Endocrinol. 178 (5): 501–511. doi:10.1530/EJE-17-0986. PMID 29510982.
Natural History, Complications and Prognosis
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Mohammed Abdelwahed M.D[2]
Overview
If left untreated, patients with adrenal incidentaloma may progress to develop dyslipidemia, osteoporosis, hyperglycemia, malignant hypertension, intracranial hemorrhage, acute coronary syndrome, aortic dissection, malignant transformation, and metastasis. Prognosis is usually good in benign adrenal incidentalomas, death is not directly related to the adrenal mass, but to cardiovascular accidents, malignancy, and chronic disorders, as observed in the general population. Adrenocortical carcinoma (ACC) carries a poor prognosis and is unlike most tumors of the adrenal cortex, which are benign (adenomas) and only occasionally cause Cushing’s syndrome.
Natural History, Complications, and Prognosis
Natural History
- The symptoms of adrenal incidentaloma usually develop in the fifth decade of life, and start with symptoms such as weight loss, anorexia, diabetes, high incidence of vertebral fractures, dyslipidemia, impaired glucose tolerance or type 2 diabetes mellitus, and evidence of atherosclerosis, paroxysmal attacks of hypertension, palpitation, diaphoresis, headache, pallor, and tremor, hypertension and hypokalemia.
- If left untreated, patients with adrenal incidentaloma may progress to develop dyslipidemia, osteoporosis, hyperglycemia, malignant hypertension, intracranial hemorrhage, acute coronary syndrome, aortic dissection, malignant transformation, and metastasis.
- It seems that the majority of masses remain hormonally and morphologically unchanged. Some cases develop mass enlargement or adrenal hyperfunction.[1][2]
- Nine precents of cases showed appearance of another mass in the contralateral adrenal gland. Mass enlargement was generally limited to 1–2 cm increase in diameter over a period of 1–3 years.[3]
- Reduction or even disappearance of the adrenal mass have been reported in up to 40% of adrenal incidentalomas, most often in the case of cystic lesions, hematomas, or adrenal pseudotumors.
Complications
- Common complications of adrenal incidentaloma include:[4]
- Hypertension
- Glucose intolerance
- Diabetes mellitus
- Obesity
- Dyslipidemia
- Osteoporosis
- Hyperglycemia (due to opposition of insulin effect by high doses of adrenaline secreted by the tumor)
- Malignant hypertension that may cause cerebrovascular accidents such as:
- Metastasis to:
Prognosis
Adrenocortical carcinoma (ACC) carries a poor prognosis and is unlike most tumors of the adrenal cortex, which are benign (adenomas) and only occasionally cause Cushing’s syndrome. Adrenal mass size is important because the smaller the adrenocortical carcinoma is at the time of diagnosis, the better the overall prognosis.[5]
- In the vast majority of patients with apparently benign adrenal incidentalomas, death is not directly related to the adrenal mass, but to cardiovascular accidents, malignancy, and chronic disorders, as observed in the general population.
- The most common causes of death are related to cardiovascular diseases (acute myocardial infarction, ventricular arrhythmia, cardiac failure, multi-infarct dementia, and acute cerebrovascular infarct).
- Mean age at death is 72.8 years.
- Five-year disease-free survival after a complete resection of a stage I–III ACC is 30%.
- The most important prognostic factors are:
- Age of the patient
- Stage of the tumor
- Mitotic activity
- Venous invasion, has worse prognosis.
- Weight of more than 50g, has worse prognosis.
- Diameter of 6.5 cm, has worse prognosis.
References
- ↑ Herrera MF, Grant CS, van Heerden JA, Sheedy PF, Ilstrup DM (1991). “Incidentally discovered adrenal tumors: an institutional perspective”. Surgery. 110 (6): 1014–21. PMID 1745970.
- ↑ Barzon L, Fallo F, Sonino N, Boscaro M (2002). “Development of overt Cushing’s syndrome in patients with adrenal incidentaloma”. Eur J Endocrinol. 146 (1): 61–6. PMID 11751069.
- ↑ Bondanelli M, Campo M, Trasforini G, Ambrosio MR, Zatelli MC, Franceschetti P; et al. (1997). “Evaluation of hormonal function in a series of incidentally discovered adrenal masses”. Metabolism. 46 (1): 107–13. PMID 9005978.
- ↑ Dekkers OM, Horváth-Puhó E, Jørgensen JO, Cannegieter SC, Ehrenstein V, Vandenbroucke JP; et al. (2013). “Multisystem morbidity and mortality in Cushing’s syndrome: a cohort study”. J Clin Endocrinol Metab. 98 (6): 2277–84. doi:10.1210/jc.2012-3582. PMID 23533241.
- ↑ Barry MK, van Heerden JA, Farley DR, Grant CS, Thompson GB, Ilstrup DM (1998). “Can adrenal incidentalomas be safely observed?”. World J Surg. 22 (6): 599–603, discussion 603-4. PMID 9597935.
Diagnosis
Diagnosis
History and Symptoms | Physical Examination | Electrocardiogram | Laboratory Findings | X-Ray Findings | Echocardiography and Ultrasound | CT-Scan Findings | MRI Findings | Other Diagnostic Studies | Other Imaging Findings
Treatment
Treatment
Medical Therapy | Surgery | Primary Prevention | Secondary Prevention | Cost-Effectiveness of Therapy | Future or Investigational Therapies
Looking for the patient version?
© 2026 MyEClinic – IFTM Institut für Telematik in der Medizin GmbH