In 1937, Karl Lisch published an article on the irishamartomas and their association with neurofibromatosis 1, now known as “Lisch nodules”, while at the University Eye Clinic in Munich.
Neurofibromatosis (NF), a disease described in 1882 by Friedrich Daniel Von Recklinghausen. [1]
NF is a neuroectodermal abnormality constituted by a set of clinical symptoms that compromise the skin, nervous system, bones, eyes and other sites.
Lisch Nodules were named after the infamous Austrian ophthalmologist Karl Lisch (1907-1999). [2]
Lisch was a well known ophthalmologist; his patients came from all parts of Austria, Germany, and Italy. In the region of North Tyrol he was called “Ophthalmological Pope”.
Besides general ophthalmology, Lisch was interested in scientific research. He published more than 120 scientific papers in German science journals.
In 1937, Karl Lisch published an article on the iris hamartomas and their association with neurofibromatosis 1, now known as “Lisch nodules”, while at the University Eye Clinic in Munich.
Lisch’a article described his observations in 3 patients with neurofibromatosis
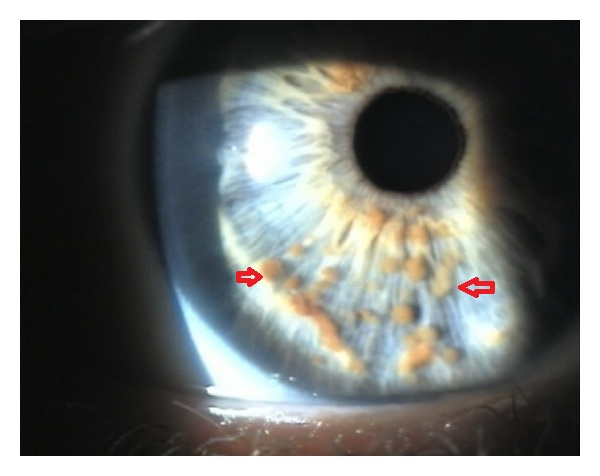
Patient 1: a 39 year old male who had been affected with several nodules and pigmented lesions on the skin, typical of neurofibromatosis, since the age of 15 years. His mother and his sisters had a similar disorder. Lisch observed several brown nodules on the surface of the iris. The nodules could be seen even without the slit lamp due to the greyish-blue color of the iris.
Patient 2: 27 year old patient with similar cutaneous and iris lesions could be detected along with a family history of neurofibromatosis. In comparison to the first patient the iris nodules were much more pigmented.
Patient 3: a 44 year old male suffered form bilateral optic nerve gliomas with chiasmal involvement. The slit lamp examination revealed tiny iris nodules in both eyes.
A hamartoma is defined as a benign tumor or nodular growth that is composed of proliferating mature histologically normal cells that normally reside at the affected tissue
In ophthalmic jargon, iris hamartomas traditionally refer to Lisch nodules which are encountered in patients with neurofibromatosis type 1 (NF1).
NF1 is due to mutations in the NF1 gene, located at chromosome 17q11.2
Neurofibromin, the protein product encoded by the gene, is expressed in many tissues, including brain, kidney, spleen, and thymus
Mutations in the NF1 gene result in loss of production or reduced function of protein; this causes a wide spectrum of clinical findings, including NF1-associated tumors
Histopathologically, Lisch nodules are composed of melanocytes and spindle cells, usually concentrated on the superficial layers of the iris stroma. [1]
The spindle cells are larger than the normal iris melanocytes.
Immunohistochemical studies show positive reaction against vimentin, smooth muscle actin and neuron specific enolase.
References
↑Kiratli, H (2011). “Head and Neck: Iris Hamartomas”. Atlas of Genetics and Cytogenetics in Oncology and Haematology (1). doi:10.4267/2042/44673. ISSN1768-3262.
Lisch Nodules commonly associated with neurofibromatosis and is caused by genetic defects or mutations that either are passed on by a parent or occur spontaneously at conception.
Please help WikiDoc by adding content here. It’s easy! Click here to learn about editing.
The differential diagnosis of Lisch nodules must include:[1]
Iris mamillations
Irido-corneo-endothelial syndrome
Rieger’s anomaly or syndrome
Iris nevi
Melanoma
Inflammatory conditions
Sarcoidosis
Lepra
Tuberculosis
Syphilis
References
↑Kiratli, H (2011). “Head and Neck: Iris Hamartomas”. Atlas of Genetics and Cytogenetics in Oncology and Haematology (1). doi:10.4267/2042/44673. ISSN1768-3262.
NF1 is an autosomal dominant genetic disorder with an incidence of approximately 1 in 2600 to 3000 individuals.
Approximately one-half of the cases are familial (inherited)
The remainder are the result of de novo (sporadic) mutations.
The de novo mutations occur primarily in paternally derived chromosomes, and the likelihood of de novo NF1 increases with advanced paternal age
Lisch nodules are predominantly visible in children usually after the age of six years.[1]
Lisch Nodule incidence in NF1 increases with age and their prevalence raises by about 10% per year of life, up to age 9.
Lisch nodules are found in 93% of adults with NF-1 but have not been described in NF-2.[2]
Lisch Nodules may be found in a very limited number of individuals without NF.[3]
Multiple Lisch nodules appear to be found only in patients with peripheral neurofibromatosis (neurofibromatosis type 1, or von Recklinghausen’s disease), an autosomal disorder with a prevalence of 1 in 3500.
References
↑Maharaj, A; Singh,, VRS; Lalchan, SA (2014). “Lisch and the Importance of His Nodules”. West Indian Medical Journal. doi:10.7727/wimj.2013.323. ISSN0043-3144.
↑Greene, Carol L; Male, Wendy S; Coleman, Shelley H; Ohrliok, Martin E; Gordon, Robert A (1987). “LISCH NODULES IN AN UNSELECTED POPULATION: PREVALENCE AND USEFULNESS AS INDICATION OF NEUROFIBROMATOSIS”. Pediatric Research. 21 (4): 227A–227A. doi:10.1203/00006450-198704010-00368. ISSN0031-3998.
The biggest risk factor for neurofibromatosis is a family history of the disorder. [1]
NF1 and NF2 are both autosomal dominant disorders, which means that any child of a parent with the disorder has a 50 percent chance of inheriting the genetic mutation.
About half of people with NF1 and NF2 inherited the disease from the affected parent.
People with NF1 and NF2 that don’t have affected relatives likely have a new gene mutation.
Neurofibromatosis is caused by genetic defects (mutations) that either are passed on by a parent or occur spontaneously at conception.
The NF1 gene is located on chromosome 17. This gene produces a protein called neurofibromin that helps regulate cell growth. The mutated gene causes a loss of neurofibromin, which allows cells to grow uncontrolled.
The NF2 gene is located on chromosome 22, and produces a protein called merlin (also called schwannomin), which suppresses tumors. The mutated gene causes a loss of merlin, leading to uncontrolled cell growth.
Two genes are known to cause schwannomatosis. Mutations of the genes SMARCB1 and LZTR1, which suppress tumors, are associated with this type of neurofibromatosis.
Lisch Nodules are not regularly screened, they’re usually detected when other signs and symptoms of neurofibromatosis appear. [1]
However, Lisch nodules are seen in 95% of children with NF1 by age 20
They can often be seen with no magnification, especially in adults, who usually have multiple, bilateral nodules
A slit-lamp examination, however, is required to distinguish them from nevi on the iris, which are flat or minimally elevated, densely pigmented lesions with blurred margins.
References
↑Ferner, R. E; Huson, S. M; Thomas, N.; Moss, C.; Willshaw, H.; Evans, D G.; Upadhyaya, M.; Towers, R.; Gleeson, M.; Steiger, C.; Kirby, A. (2006). “Guidelines for the diagnosis and management of individuals with neurofibromatosis 1”. Journal of Medical Genetics. 44 (2): 81–88. doi:10.1136/jmg.2006.045906. ISSN1468-6244.
The diagnosis is primarily based on clinical assessment and two or more of the features are required to confirm the diagnosis.
Physical Examination
Physical Examination
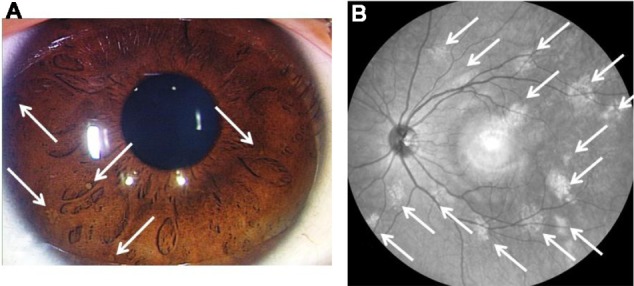
Lisch nodules and near-infrared reflectance image (case 4). At least five Lisch nodules were detected and were classified as scale III (A). Note that 14 bright, patchy lesions were detected by near-infrared reflectance (B). The hyper-reflective point at the center of the image is an optical artifact. Case courtesy by Shinji Makino et al[38]Lisch nodules occur in 90% of adults with neurofibromatosis 1.[39][40][41][42][43][44]
↑Lubs, Marie-Louise E.; Bauer, Mislen S.; Formas, Maria E.; Djokic, Borivoje (1991). “Lisch Nodules in Neurofibromatosis Type 1”. New England Journal of Medicine. 324 (18): 1264–1266. doi:10.1056/NEJM199105023241807. ISSN0028-4793.
↑Dimitrova, Valentina (2009). “A CASE OF NEUROFIBROMATOSIS TYPE 1”. Journal of IMAB – Annual Proceeding (Scientific Papers). 14, 1 (2008): 63–67. doi:10.5272/jimab.14-1-2010.63. ISSN1312-773X.
↑Richetta, A; Giustini, S; Recupero, SM; Pezza, M; Carlomagno, V; Amoruso, G; Calvieri, S (2004). “Lisch nodules of the iris in neurofibromatosis type 1”. Journal of the European Academy of Dermatology and Venereology. 18 (3): 342–344. doi:10.1111/j.1468-3083.2004.00915.x. ISSN0926-9959.
↑Lubs, Marie-Louise E.; Bauer, Mislen S.; Formas, Maria E.; Djokic, Borivoje (1991). “Lisch Nodules in Neurofibromatosis Type 1”. New England Journal of Medicine. 324 (18): 1264–1266. doi:10.1056/NEJM199105023241807. ISSN0028-4793.
↑Lubs, Marie-Louise E.; Bauer, Mislen S.; Formas, Maria E.; Djokic, Borivoje (1991). “Lisch Nodules in Neurofibromatosis Type 1”. New England Journal of Medicine. 324 (18): 1264–1266. doi:10.1056/NEJM199105023241807. ISSN0028-4793.