
Glioma
For patient information click here
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor-In-Chief: Cafer Zorkun, M.D., Ph.D. [2],Faizan Sheraz, M.D. [3],Shanshan Cen, M.D. [4],Sujit Routray, M.D. [5]
Synonyms and keywords:Gliomas; gliooma; gliome; gliom; glejak; glial tumor; glial neoplasm; neuroglial tumor; neuroglial neoplasm; neoplasm of the neuroglia; neoplasm of neuroglia; tumor of the glial cell; glial cell tumor; astrocytoma; brainstem glioma; optic nerve glioma; mixed gliomas; pilocytic astrocytoma; diffuse astrocytoma; anaplastic astrocytoma; glioblastoma multiforme; oligodendroglioma; anaplastic oligodendroglioma; oligoastrocytoma; anaplastic oligoastrocytoma; ependymoma; anaplastic ependymoma; gliosarcoma; brain tumor
Overview
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor-In-Chief: Swathi Venkatesan, M.B.B.S.[2]
Overview
A glioma is a type of primary central nervous system (CNS) tumor that arises from glial cells. The most common site of involvement of gliomas is the brain, but gliomas can also affect the spinal cord or any other part of the CNS, such as the optic nerve.[1] Gliomas were reported as early as the 1850s. Retinal gliomas were most commonly reported because they were easier to detect and sample in the absence of advanced imaging and surgical techniques. Glioma may be classified into several subtypes based on the type of cell, grade, and location.[2] The pathogenesis of cerebral glioma involves invasion of the tumor cells into the adjacent normal brain tissue. The gross and histopathological appearance of glioma varies with the tumor grade and type.[3][4][5][6][7] Glioma must be differentiated from primary CNS lymphoma, cerebral metastases, meningioma, brain abscess, cavernous malformation, stroke, acute disseminated encephalomyelitis, cavernous sinus syndrome, intracranial hemorrhage, gerstmann syndrome, spinal tuberculosis, hamartoma, germinoma, teratoma, piloid gliosis, and progressive multifocal leukoencephalopathy.[3][2] The incidence of glioma is estimated to be 4.9 cases per 100,000 individuals in the US.[8] Patients of all age groups may develop glioma. Males are more commonly affected with glioma than females. It usually affects individuals of the caucasian race. African american, latin american, and asian individuals are less likely to develop glioma. Common risk factors in the development of glioma are occupational factors, environmental factors, genetic factors, and viruses.[2][3][8][5][9] Common complications of glioma include brain herniation, coma, metastasis, and recurrence. The prognosis of glioma varies with the grade of tumor. The 1-year and 2-year survival rate of patients with malignant glioma is approximately 50% and 25%, respectively.[10] Common symptoms of glioma include morning headaches, nausea and vomiting, seizures, drowsiness, changes in speech, difficulty in swallowing, vision changes, abnormal eye movements, changes in personality, memory loss, loss of balance, difficulty in walking, weakness in extremities, numbness in extremities, pain in extremities, and loss of appetite.[2] The CT scan and MRI findings of glioma vary with the tumor grade and type.[2][4][3][5][10][6] The predominant therapy for glioma is surgical resection. Adjunctive chemotherapy and radiation may be required.[2]
Historical Perspective
- Gliomas were reported as early as the 1850s.
- The first recorded reports of gliomas were given in British scientific reports, by Berns in 1800 and in 1804 by Abernety
- With the first comprehensive histomorphological description being given in 1865 by Rudolf Virchow.
- In 1926 Percival Bailey and Harvey Cushing gave the base for the modern classification of gliomas.
- Between 1934 and 1941 the most prolific researcher in glioma research was Hans-Joachim Scherer, who postulated some of the clinico-morphological aspects of Glioblastoma multiforme.
- Retinal gliomas were most commonly reported because they were easier to detect and sample in the absence of advanced imaging and surgical techniques.
Classification
- The classification and grading of gliomas have evolved over time, beginning in 1926 with a system devised by Bailey and Cushing and later revised by Kernohan, Ringertz, and others.
- As of the 2016 edition of the WHO classification, gliomas are classified based not only on histopathologic appearance but also on well-established molecular parameters
- Glioma may be classified into several subtypes based on the type of cell (ependymoma, astrocytoma, oligodendroglioma, and mixed gliomas), grade (low-grade and high-grade gliomas), and location (infratentorial and supratentorial).[2]
- Astrocytomas are glial cell tumors
- Develop from connective tissue cells called astrocytes.
- The most common primary intra-axial brain tumor, accounting for nearly half of all primary brain tumors.
- They are most often found in the cerebrum (the large, outer part of the brain), but also in the cerebellum (located at the base of the brain).
- Astrocytomas can develop in adults or in children.
- Pilocytic astrocytomas are low-grade cerebellum gliomas commonly found in children. In adults, astrocytomas are more common in the cerebrum.
- High-grade astrocytomas, called glioblastoma multiforme, are the most malignant of all brain tumors.
- Brain stem gliomas
- Also called diffuse infiltrating brainstem gliomas, or DIPGs, are rare tumors found in the brain stem.
- Cannot be surgically removed because of their remote location, where they intertwine with normal brain tissue and affect the delicate and complex functions this area controls.
- These tumors occur most often in school-age children
- Responsible for the greatest number of childhood deaths from primary brain tumors.
Pathophysiology
The pathogenesis of cerebral glioma involves invasion of the tumor cells into the adjacent normal brain tissue. Although in certain areas the margin of the tumor may seem to be macroscopically well defined from the brain, there are always microscopic nests of tumor cells extending well out into the brain.[3] Genes involved in the pathogenesis of glioma include ERCC1, ERCC2, XRCC1, MGMT, IDH1, IDH2, p53, EGFR, TSC1, TSC2, RB1, APC, hMLH1, hMSH2, PMS2, PTEN, NF1, and NF2.[2][8] The gross and histopathological appearance of glioma varies with the tumor grade and type.[11][4][5][6][7]
Causes
There are no established causes for glioma.
Differentiating brain tumors from other diseases
Glioma must be differentiated from primary CNS lymphoma, cerebral metastases, meningioma, brain abscess, cavernous malformation, stroke, acute disseminated encephalomyelitis, cavernous sinus syndrome, intracranial hemorrhage, gerstmann syndrome, spinal tuberculosis, hamartoma, germinoma, teratoma, piloid gliosis, and progressive multifocal leukoencephalopathy.[2][3]
Epidemiology and Demographics
Glioma is the most common primary intracranial tumor. The incidence of glioma is estimated to be 4.9 cases per 100,000 individuals in the US.[8] Patients of all age groups may develop glioma. Males are more commonly affected with glioma than females. It usually affects individuals of the caucasian race. African american, latin american, and asian individuals are less likely to develop glioma.
Risk factors
Common risk factors in the development of glioma are occupational factors, environmental factors, genetic factors, and viruses.[2][3][8][5][9]
Screening
There is insufficient evidence to recommend routine screening for glioma.[12]
Natural History, Complications and Prognosis
Common complications of glioma include brain herniation, coma, metastasis, and recurrence. The prognosis of glioma varies with the grade of tumor. The 1-year and 2-year survival rate of patients with malignant glioma is approximately 50% and 25%, respectively.[10]
Staging
There is no established system for the staging of glioma.[10]
History and Symptoms
Common symptoms of glioma include morning headaches, nausea and vomiting, seizures, drowsiness, changes in speech, difficulty in swallowing, vision changes, abnormal eye movements, changes in personality, memory loss, loss of balance, difficulty in walking, weakness in extremities, numbness in extremities, pain in extremities, and loss of appetite.[2]
Physical examination
Common physical examination findings of glioma include aphasia, vision loss, strabismus, memory loss, sensory loss, paresis, abnormal gait, ataxia, papilledema, and focal neurological deficits.[2]
Laboratory Findings
There are no diagnostic lab findings associated with glioma.
X Ray
There are no x-ray findings associated with glioma.
CT
Head CT scan may be diagnostic of glioma. The CT scan findings of glioma vary with the tumor grade and type.[2][4][3][5][10][6]
MRI
Brain MRI may be diagnostic of glioma. The MRI findings of glioma vary with the tumor grade and type.[2][4][3][5][10][6]
Ultrasound
There are no ultrasound findings associated with glioma.
Other Imaging Findings
Other imaging studies for high-grade gliomas include PET scan, which demonstrates accumulation of [18F]-fluorodeoxyglucose (increased glucose metabolism).[2]
Other Diagnostic Studies
Other diagnostic studies for glioma include biopsy, which demonstrates astrocytes with or without atypia and mitoses, depending on the type of glioma.[2]
Medical Therapy
Treatment for glioma depends on the location and grade. The predominant therapy for glioma is surgical resection. Adjunctive chemotherapy and radiation may be required.[2]
Surgery
Surgery is the mainstay of treatment for glioma.[2]
References
- ↑ Mamelak A.N., and Jacoby, D.B. Targeted delivery of antitumoral therapy to glioma and other malignancies with synthetic chlorotoxin (TM-601) Expert Opin. Drug Drliv. (2007) 4(2):175-186.
- ↑ 2.00 2.01 2.02 2.03 2.04 2.05 2.06 2.07 2.08 2.09 2.10 2.11 2.12 2.13 2.14 2.15 2.16 2.17 Classification of glioma. Wikipedia. https://en.wikipedia.org/wiki/Glioma
- ↑ 3.0 3.1 3.2 3.3 3.4 3.5 3.6 3.7 3.8 Pathology of pilocytic astrocytoma. Libre Pathology. http://librepathology.org/wiki/index.php/Pilocytic_astrocytoma
- ↑ 4.0 4.1 4.2 4.3 4.4 Pathology of gliomas. Libre Pathology. http://librepathology.org/wiki/index.php/Oligodendroglioma
- ↑ 5.0 5.1 5.2 5.3 5.4 5.5 5.6 Pathology of anaplastic astrocytoma. Libre Pathology. http://librepathology.org/wiki/index.php?title=Neuropathology_tumours&redirect=no#Infiltrative_astrocytomas
- ↑ 6.0 6.1 6.2 6.3 6.4 Pathology of glioblastoma. Libre Pathology. http://librepathology.org/wiki/index.php/Glioblastoma
- ↑ 7.0 7.1 Pathology of ependymoma. Libre Pathology. http://librepathology.org/wiki/index.php/Ependymoma
- ↑ 8.0 8.1 8.2 8.3 8.4 Schwartzbaum JA, Fisher JL, Aldape KD, Wrensch M (2006). “Epidemiology and molecular pathology of glioma”. Nat Clin Pract Neurol. 2 (9): 494–503, quiz 1 p following 516. doi:10.1038/ncpneuro0289. PMID 16932614.
- ↑ 9.0 9.1 Ostrom, Quinn T.; Bauchet, Luc; Davis, Faith G.; Deltour, Isabelle; Fisher, James L.; Langer, Chelsea Eastman; Pekmezci, Melike; Schwartzbaum, Judith A.; Turner, Michelle C. (Jul 2014). “The epidemiology of glioma in adults: a “state of the science” review”. Neuro-Oncology. 16 (7): 896–913. doi:10.1093/neuonc/nou087. ISSN 1523-5866. PMC 4057143. PMID 24842956.
- ↑ 10.0 10.1 10.2 10.3 10.4 10.5 Prognostic factors of glioma. National Cancer Institute. http://www.cancer.gov/types/brain/patient/adult-brain-treatment-pdq
- ↑ Pathology of pilocytic astrocytoma. Libre Pathology. http://librepathology.org/wiki/index.php/Pilocytic_astrocytoma
- ↑ Early detection, diagnosis, and staging of glioma. American cancer society. http://www.cancer.org/cancer/braincnstumorsinadults/detailedguide/brain-and-spinal-cord-tumors-in-adults-detection
Historical Perspective
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1] Associate Editor(s)-in-Chief: Serge Korjian M.D.
Overview
Gliomas were reported as early as the 1850s. Retinal gliomas were most commonly reported because they were easier to detect and sample in the absence of advanced imaging and surgical techniques.
Historical Perspective
- The earliest mention of gliomas in the literature dates back to the late 19th century (1850-1860).
- Most reported cases involved retinal gliomas, which were more easily detected and sampled. [1]
- Publications from Virchow in Germany were the earliest to distinguish retinal neuroglia from other connective tissue. This allowed the classification of these tumors as gliomata rather than sarcomas. [2][3]
References
- ↑ Delafield F (1870). “Tumors of the Retina”. Trans Am Ophthalmol Soc. 1 (7): 73–84. PMC 1361440. PMID 16691695.
- ↑ Knapp H (1870). “A Case of Retinal Glioma, operated on at a very early period, and showing some New and Peculiar Anatomical Conditions”. Trans Am Ophthalmol Soc. 1 (7): 84–6. PMC 1361441. PMID 16691696.
- ↑ Virchow RL. Cellular Pathology As Based Upon Physiological and Pathological Histology. Nabu Press; 2010.
Classification
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor-In-Chief: Cafer Zorkun, M.D., Ph.D. [2], Sujit Routray, M.D. [3]
Overview
Glioma may be classified into several subtypes based on the type of cell (ependymoma, astrocytoma, oligodendroglioma, and mixed gliomas), grade (low-grade and high-grade gliomas), and location (infratentorial and supratentorial).[1]
Classification
Glioma may be classified into several subtypes based on the type of cell, grade, and location.[1]
1. Based on the type of cell
Glioma may be classified according to the type of cell into four subtypes:[1]
- Ependymomas — ependymal cells
- Astrocytomas — astrocytes
- Oligodendrogliomas — oligodendrocytes
- Mixed gliomas (oligoastrocytomas) — cells from different types of glia
2. Based on the grade
Glioma may be classified according to the grade into two subtypes:[1]
- Low-grade gliomas are well-differentiated tumors. These are benign tumors.
- High-grade gliomas are undifferentiated or anaplastic tumors. These are malignant tumors.
WHO grading system for astrocytomas
| Grade | Type of tumor |
|---|---|
|
WHO grade 1 |
|
|
WHO grade 2 |
|
|
WHO grade 3 |
|
|
WHO grade 4 |
3. Based on the location
Glioma may be classified according to the location into two subtypes:[1]
- Infratentorial: mostly in children (70%)
- Supratentorial: mostly in adults (70%)
References
Pathophysiology
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor-In-Chief: Cafer Zorkun, M.D., Ph.D. [2], Sujit Routray, M.D. [3]
Overview
The pathogenesis of cerebral glioma involves invasion of the tumor cells into the adjacent normal brain tissue. Although in certain areas the margin of the tumor may seem to be macroscopically well defined from the brain, there are always microscopic nests of tumor cells extending well out into the brain.[1] Genes involved in the pathogenesis of glioma include ERCC1, ERCC2, XRCC1, MGMT, IDH1, IDH2, p53, EGFR, TSC1, TSC2, RB1, APC, hMLH1, hMSH2, PMS2, PTEN, NF1, and NF2.[2][3] The gross and histopathological appearance of glioma varies with the tumor grade and type.[4][5][6][7][8]
Pathophysiology
Pathogenesis
- The pathogenesis of cerebral glioma involves invasion of the tumor cells into the adjacent normal brain tissue. Although in certain areas the margin of the tumor may seem to be macroscopically well defined from the brain, there are always microscopic nests of tumor cells extending well out into the brain.[1]
- Astrocytic projections interact with vessels and act as additional elements of the blood brain barrier (BBB). The tumors take advantage of the blood brain barrier to ensure survival and continuous growth.
- Glioma cells migrate to different regions of the brain guided by the extension of blood vessels, colonizing the healthy adjacent tissue.
- Uncontrolled and fast growth also leads to the disruption of the chimeric and fragile vessels in the tumor mass resulting in peritumoral edema.[9]
Genetics
Genes involved in the pathogenesis of glioma include:[2][3]
Associated Conditions
Gliomas may be associated with:[3][10]
- Neurofibromatosis type 1
- Neurofibromatosis type 2
- Tuberous sclerosis
- Li-Fraumeni syndrome
- Turcot syndrome
- Maffucci syndrome
- Von Hippel-Lindau disease
- Retinoblastoma
Gross Pathology
The gross pathological appearance of glioma varies with the tumor grade and type. Common findings are listed below:[4][5][6][7][8]
| Type of glioma | Gross pathological features |
|---|---|
| |
| |
| |
| |
| |
|
Gallery
-
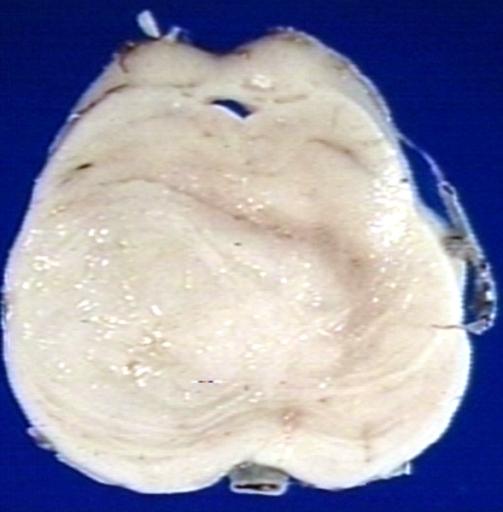
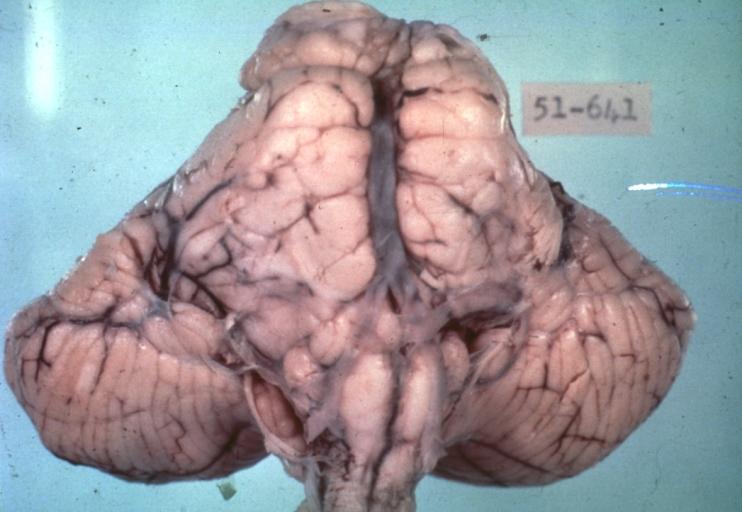 Brain: Pontine Glioma: Gross; fixed tissue, anterior view of brain stem and cerebellum with bosselated tumor adjacent to basilar artery
Brain: Pontine Glioma: Gross; fixed tissue, anterior view of brain stem and cerebellum with bosselated tumor adjacent to basilar artery -
 Brain: Pontine Glioma: Gross; fixed tissue, sagittal section brain stem and cerebellum
Brain: Pontine Glioma: Gross; fixed tissue, sagittal section brain stem and cerebellum -
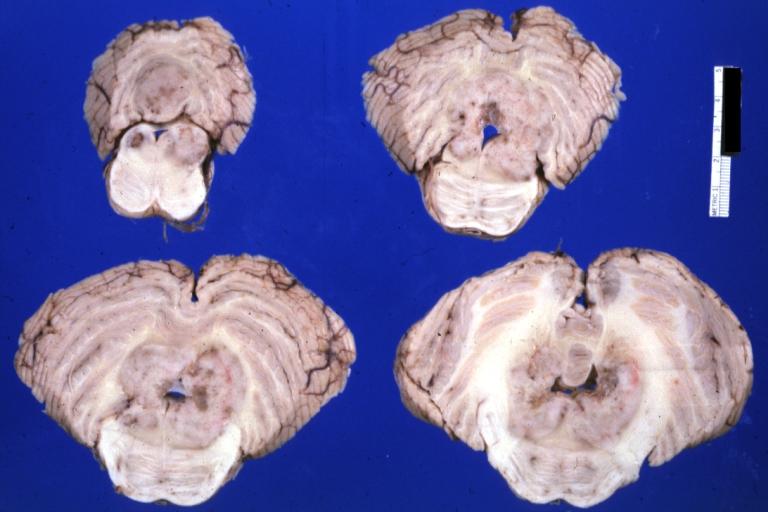
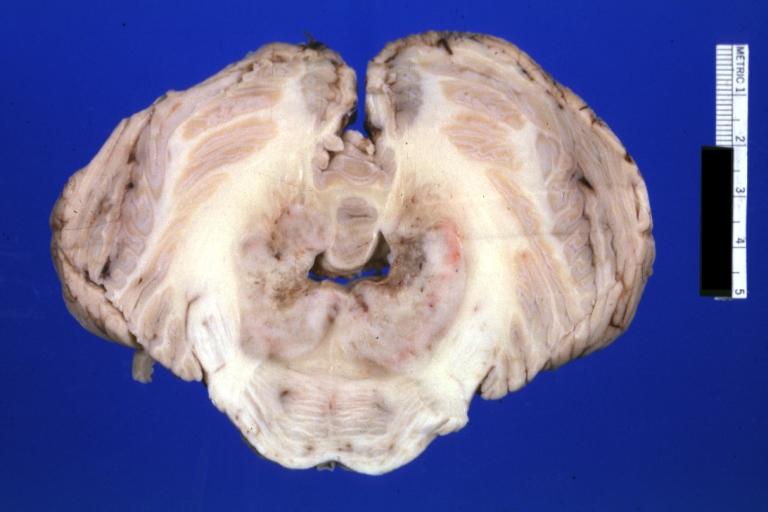
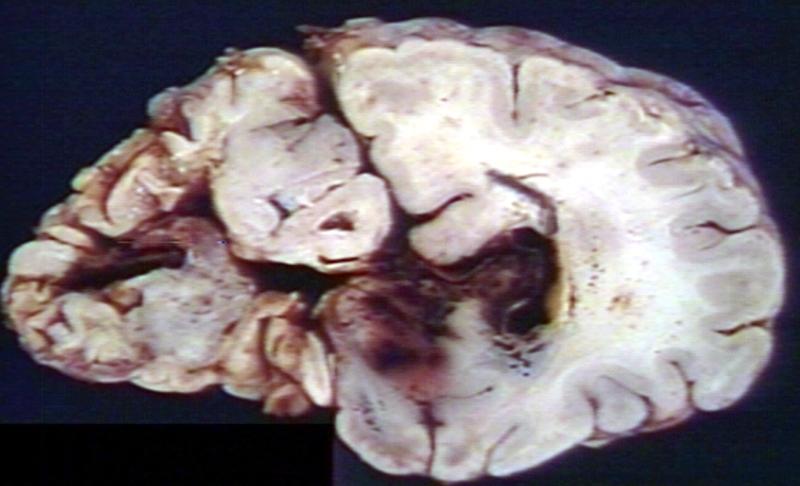
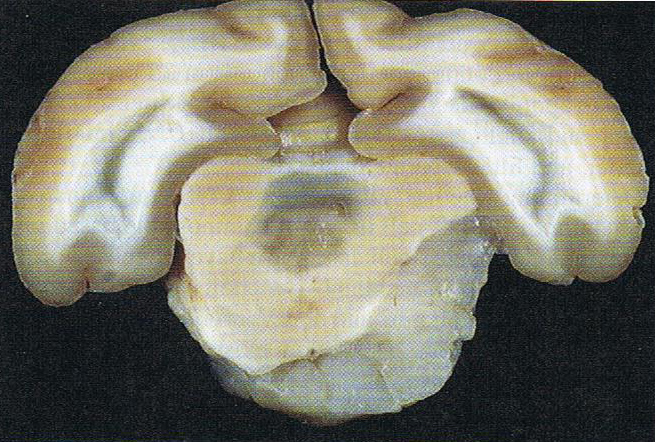
 Brain: Glioma: Gross; fixed tissue, horizontal section brain stem and cerebellum with obvious gelatinous appearing neoplasm a pontine glioma
Brain: Glioma: Gross; fixed tissue, horizontal section brain stem and cerebellum with obvious gelatinous appearing neoplasm a pontine glioma -
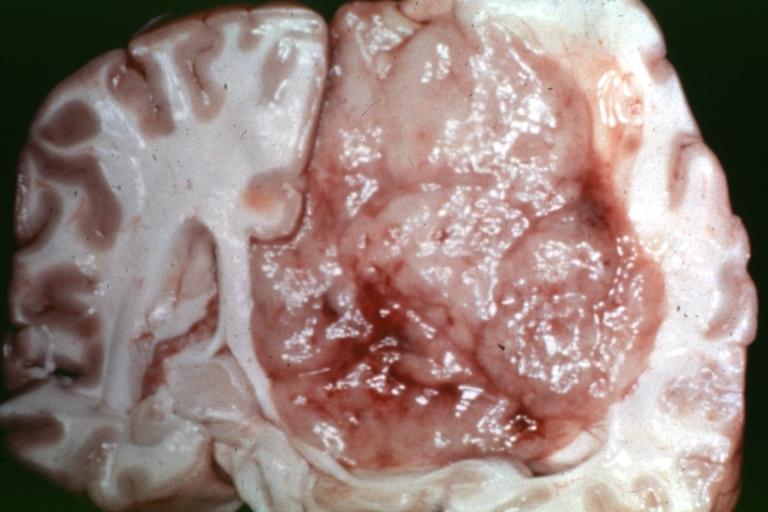
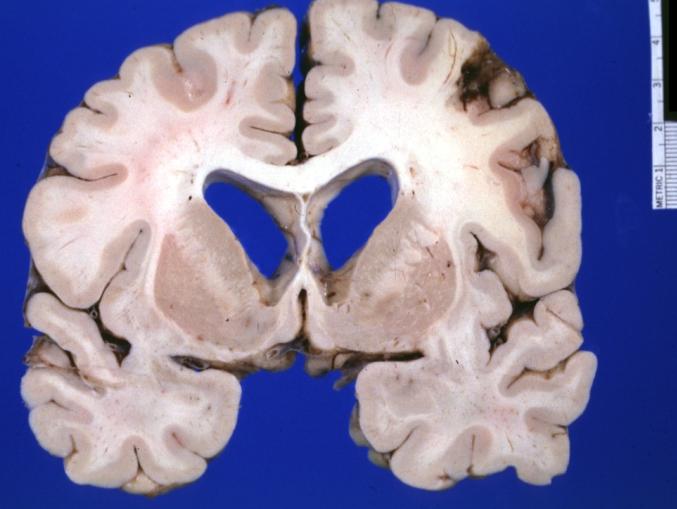
 Brain: Oligodendroglioma: Gross; natural color, large, well circumscribed lesion in left frontal lobe
Brain: Oligodendroglioma: Gross; natural color, large, well circumscribed lesion in left frontal lobe -
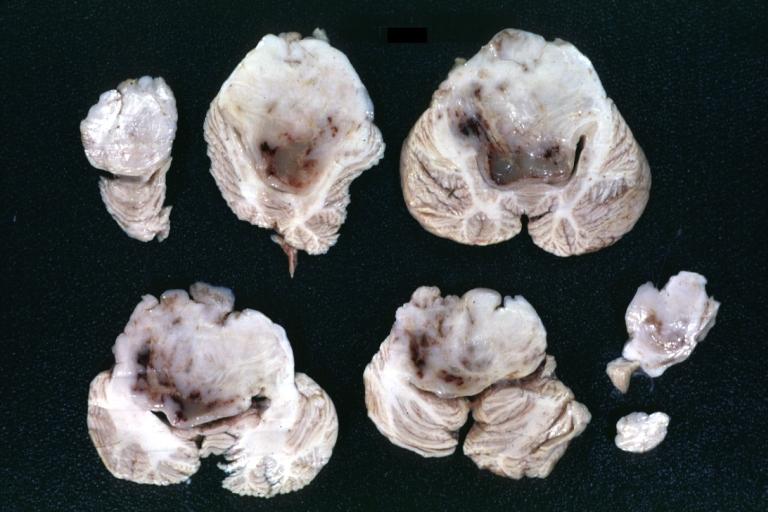 Brain: Glioma: Gross; fixed tissue, horizontal sections brain stem and cerebellum showing large pontine glioma
Brain: Glioma: Gross; fixed tissue, horizontal sections brain stem and cerebellum showing large pontine glioma -
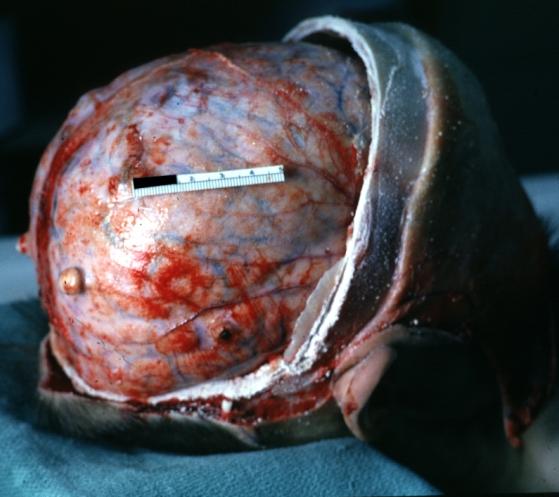
 Brain: Pontine Glioma and Diffuse Meningeal Gliomatosis: Gross; fixed tissue, view of cerebral hemispheres from inferior with brain stem and cerebellum removed. Pontine asymmetry is easily seen due to low grade astrocytoma and meningeal gliomatosis is easily seen over frontal lobes
Brain: Pontine Glioma and Diffuse Meningeal Gliomatosis: Gross; fixed tissue, view of cerebral hemispheres from inferior with brain stem and cerebellum removed. Pontine asymmetry is easily seen due to low grade astrocytoma and meningeal gliomatosis is easily seen over frontal lobes -
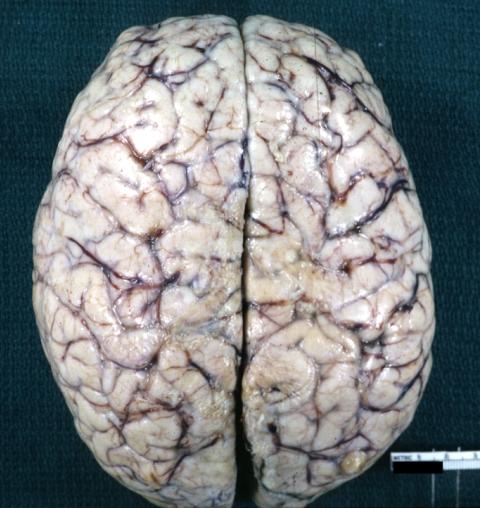 Brain: Pontine Glioma and Diffuse Meningeal Gliomatosis in 7 yo boy: Gross; fixed tissue, view of cerebral hemispheres from vertex meningeal gliomatosis.
Brain: Pontine Glioma and Diffuse Meningeal Gliomatosis in 7 yo boy: Gross; fixed tissue, view of cerebral hemispheres from vertex meningeal gliomatosis. -
 Brain: Pontine Glioma and Diffuse Meningeal Gliomatosis: Gross; in situ dural nodule
Brain: Pontine Glioma and Diffuse Meningeal Gliomatosis: Gross; in situ dural nodule -
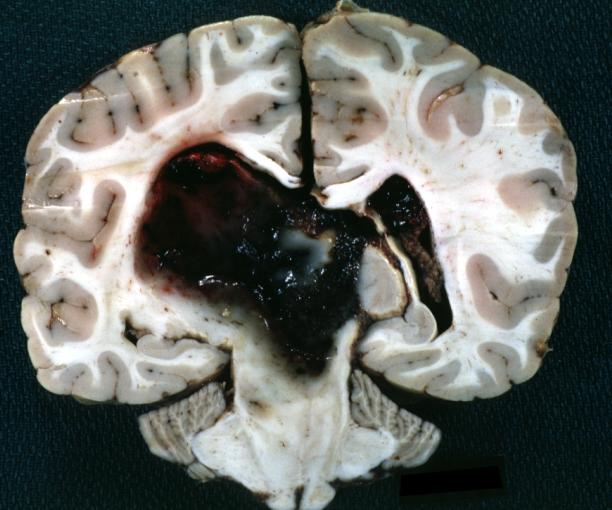
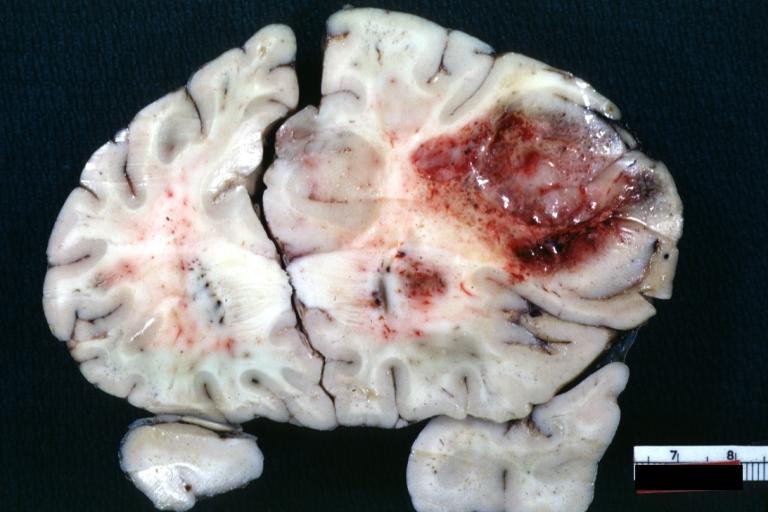
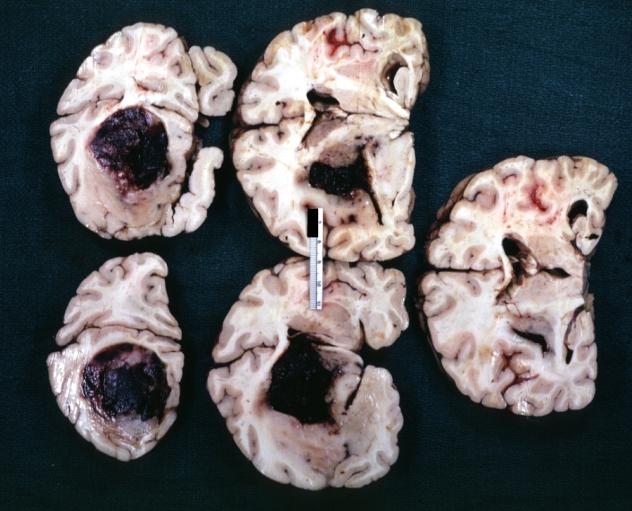 Brain: Oligodendroglioma: Gross; fixed tissue, multiple coronal sections, cerebral hemispheres with large tumor and hemorrhage into tumor
Brain: Oligodendroglioma: Gross; fixed tissue, multiple coronal sections, cerebral hemispheres with large tumor and hemorrhage into tumor -
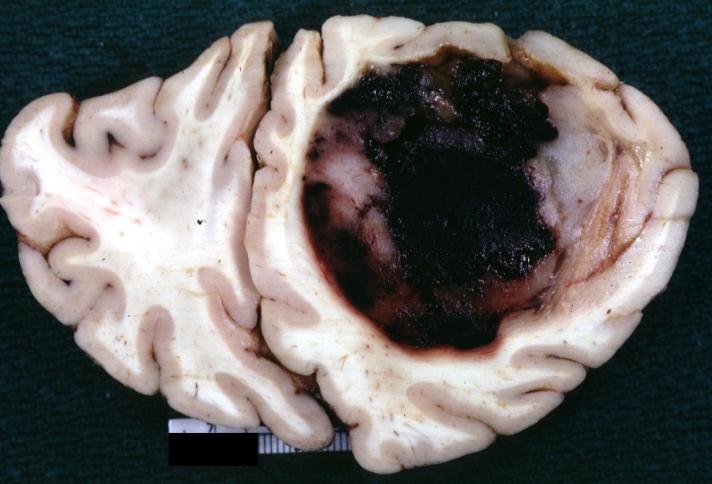
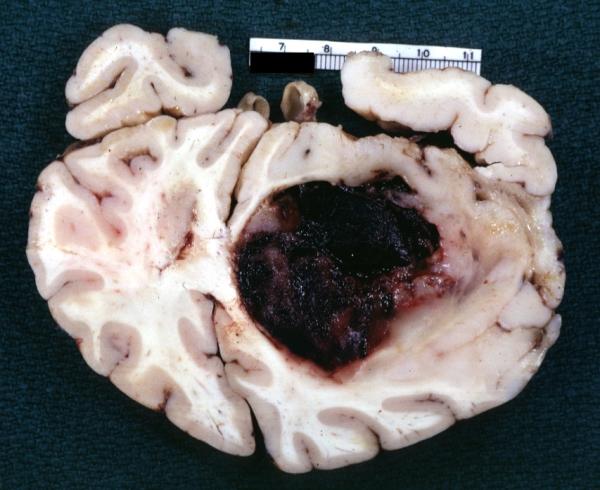 Brain: Oligodendroglioma: Gross; fixed tissue, coronal section, cerebral hemispheres, large hemorrhagic lesion in one hemisphere
Brain: Oligodendroglioma: Gross; fixed tissue, coronal section, cerebral hemispheres, large hemorrhagic lesion in one hemisphere -
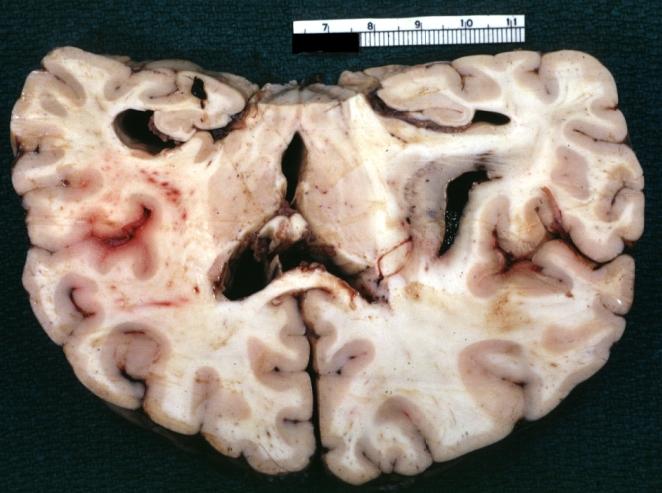 Brain: Oligodendroglioma: Gross; fixed tissue, ischemic tissue, anterior to tumor mass
Brain: Oligodendroglioma: Gross; fixed tissue, ischemic tissue, anterior to tumor mass -
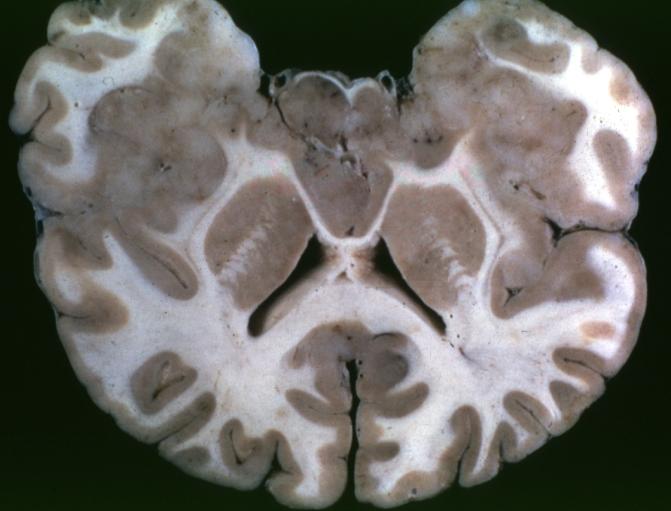
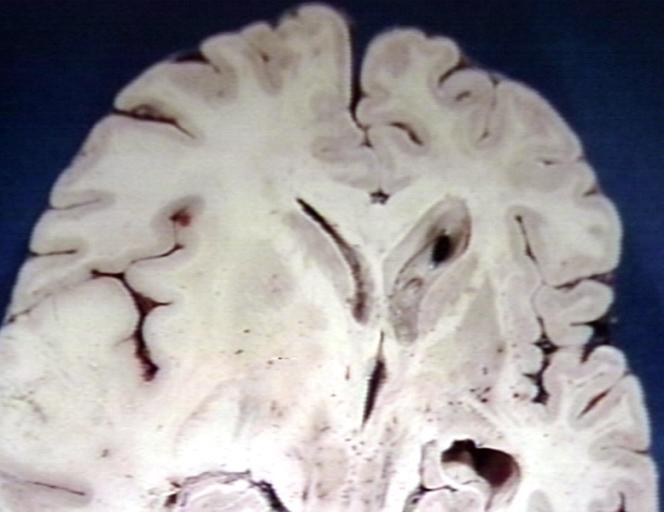
 Brain: Oligodendroglioma: Gross; natural color, coronal section, cerebral hemispheres, large lesion, left parieto occipital white matter
Brain: Oligodendroglioma: Gross; natural color, coronal section, cerebral hemispheres, large lesion, left parieto occipital white matter -
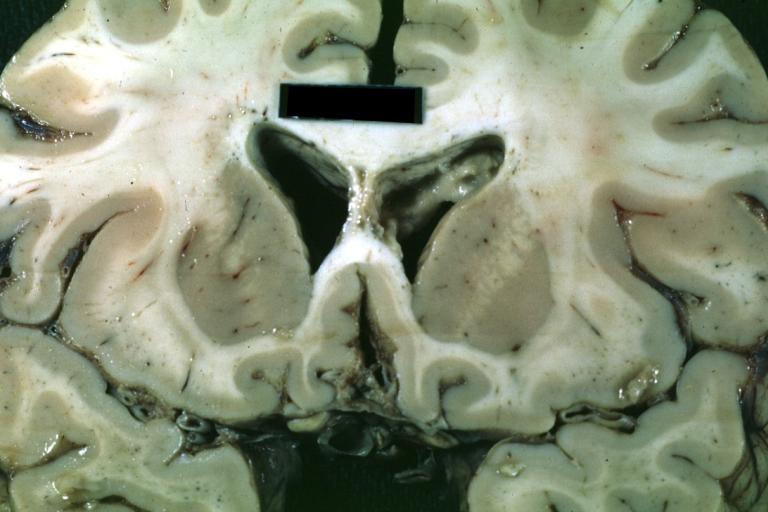
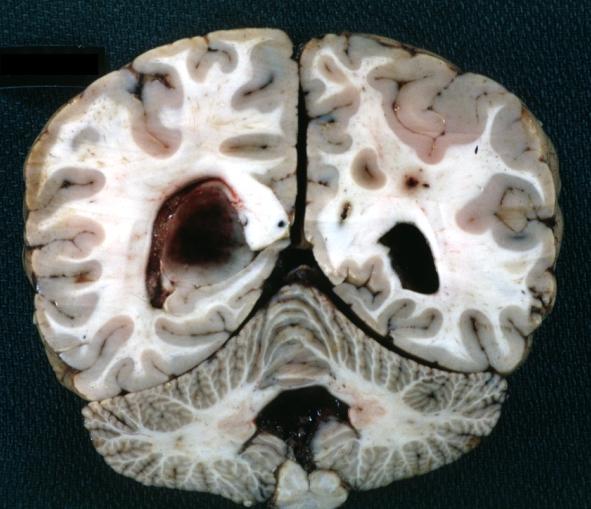
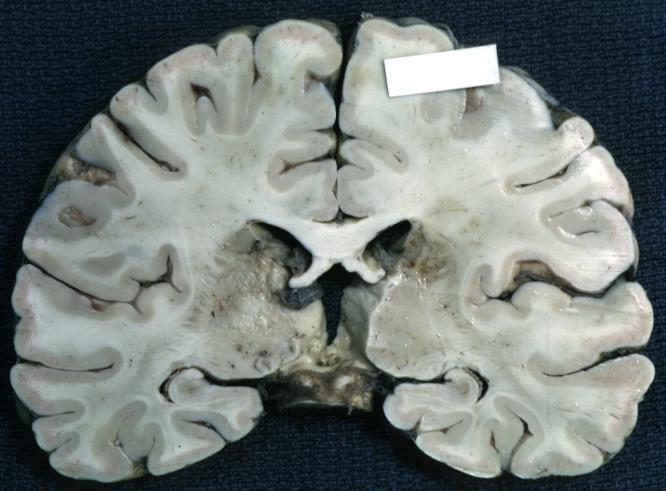
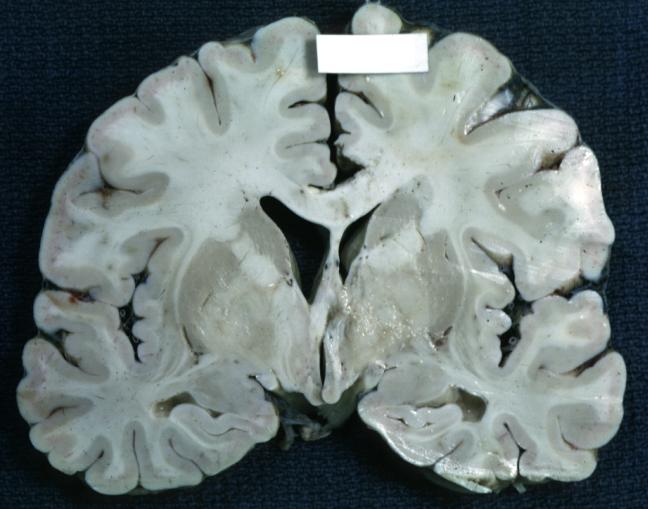
 Brain: Gliomatosis Cerebri: Gross; fixed tissue, coronal sections, cerebral hemispheres, lesion is in temporal lobes and hypothalamus
Brain: Gliomatosis Cerebri: Gross; fixed tissue, coronal sections, cerebral hemispheres, lesion is in temporal lobes and hypothalamus -
 Brain: Ventriculitis: Gross; fixed tissue, case of glioma with meningitis, a nice view of ventriculitis in one lateral ventricle
Brain: Ventriculitis: Gross; fixed tissue, case of glioma with meningitis, a nice view of ventriculitis in one lateral ventricle -
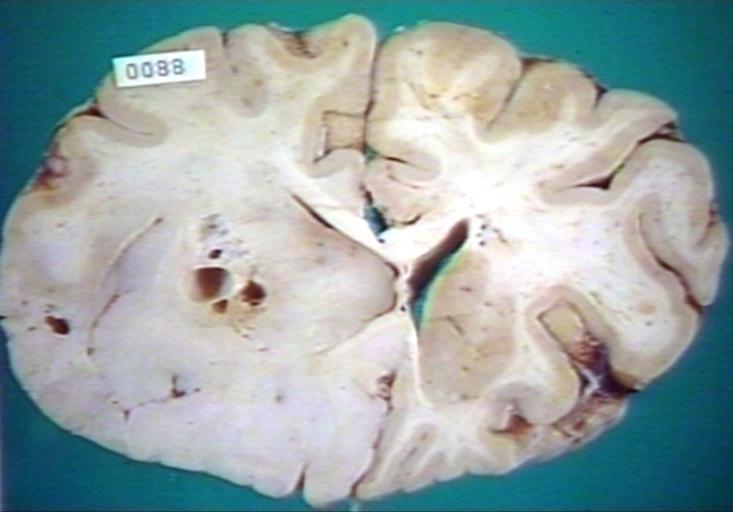
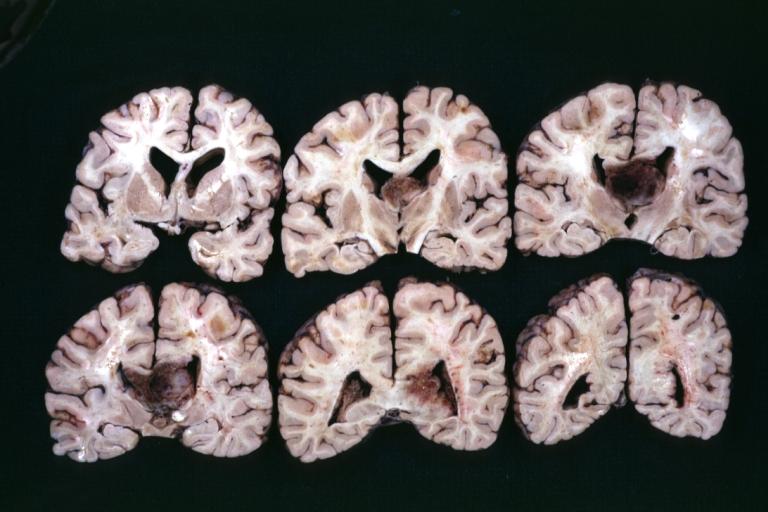
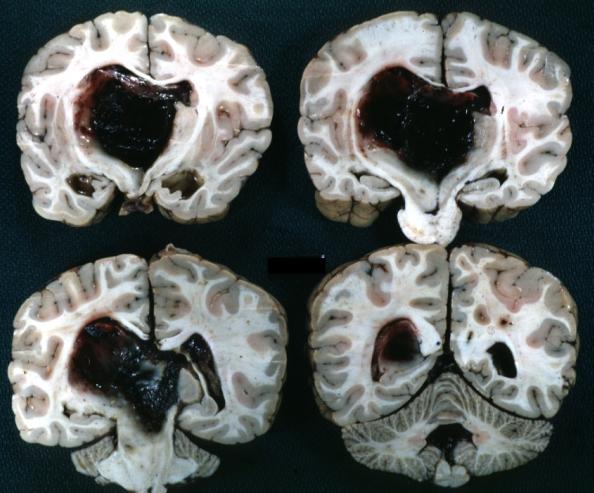 Brain: Glioma Thalamic Grade Ii-Iii: Gross; fixed tissue, four coronal sections, cerebral hemispheres, very large hemorrhagic lesion
Brain: Glioma Thalamic Grade Ii-Iii: Gross; fixed tissue, four coronal sections, cerebral hemispheres, very large hemorrhagic lesion -
 Brain: Glioma Thalamic Grade Ii-Iii: Gross; fixed tissue, coronal section, cerebral hemispheres with large hemorrhagic lesion
Brain: Glioma Thalamic Grade Ii-Iii: Gross; fixed tissue, coronal section, cerebral hemispheres with large hemorrhagic lesion -
 Brain: Glioma Thalamic Grade Ii-Iii: Gross fixed tissue coronal section cerebral hemispheres lesions appears to be in choroid plexus of lateral ventricle in this picture. There is blood in fourth ventricle
Brain: Glioma Thalamic Grade Ii-Iii: Gross fixed tissue coronal section cerebral hemispheres lesions appears to be in choroid plexus of lateral ventricle in this picture. There is blood in fourth ventricle -
 Brain: Cerebral Sarcoma or Microglioma: Gross; fixed tissue, coronal section, cerebral hemispheres (58 yo man)
Brain: Cerebral Sarcoma or Microglioma: Gross; fixed tissue, coronal section, cerebral hemispheres (58 yo man) -
 Brain: Cerebral Sarcoma or Microglioma: Gross; fixed tissue, coronal section, cerebral hemispheres
Brain: Cerebral Sarcoma or Microglioma: Gross; fixed tissue, coronal section, cerebral hemispheres -
 Brain: Cerebral Sarcoma or Microglioma: Gross; fixed tissue, coronal section, cerebral hemispheres
Brain: Cerebral Sarcoma or Microglioma: Gross; fixed tissue, coronal section, cerebral hemispheres -
 Brain: Infarct Subcortical: Gross; fixed tissue, close-up view of old small subcortical infarct, a case of microglioma
Brain: Infarct Subcortical: Gross; fixed tissue, close-up view of old small subcortical infarct, a case of microglioma -
 Brain: Microglioma: Gross; fixed tissue; cerebellum and fourth ventricle with periventricular tumor invasion
Brain: Microglioma: Gross; fixed tissue; cerebellum and fourth ventricle with periventricular tumor invasion -
 Brain: Microglioma: Gross fixed tissue horizontal sections cerebellum and brain stem with periventricular neoplastic infiltrate
Brain: Microglioma: Gross fixed tissue horizontal sections cerebellum and brain stem with periventricular neoplastic infiltrate -
 Brain: Microglioma: Gross fixed tissue horizontal section midbrain and cerebellum at mid pons level periventricular tumor infiltration
Brain: Microglioma: Gross fixed tissue horizontal section midbrain and cerebellum at mid pons level periventricular tumor infiltration -
 Brain: Microglioma: Gross fixed tissue horizontal section rostral pons and cerebellum
Brain: Microglioma: Gross fixed tissue horizontal section rostral pons and cerebellum -
 Brain: Microglioma: Gross fixed tissue horizontal section rostral pons and cerebellum periventricular tumor invasion
Brain: Microglioma: Gross fixed tissue horizontal section rostral pons and cerebellum periventricular tumor invasion -
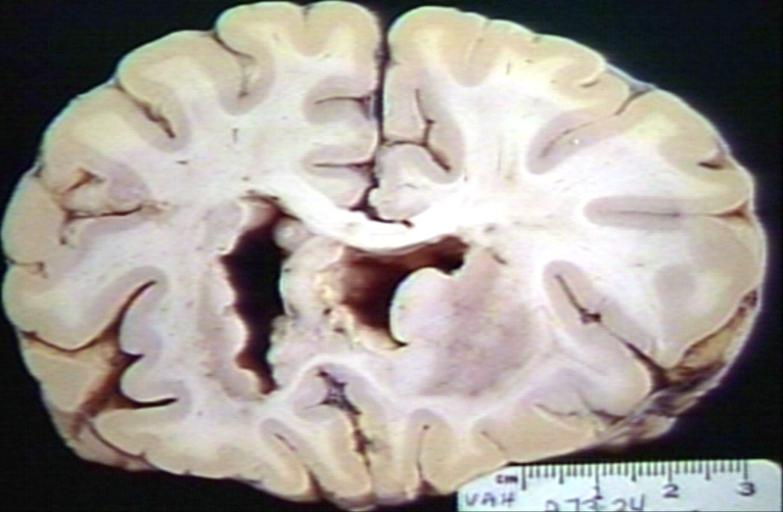
 Brain: Microglioma: Gross fixed tissue coronal section cerebral hemispheres with mild ventricular dilation
Brain: Microglioma: Gross fixed tissue coronal section cerebral hemispheres with mild ventricular dilation -
 Glioma: Optic Nerve
Glioma: Optic Nerve -
 Brain: Oligodendroglioma, Frontal Lobe
Brain: Oligodendroglioma, Frontal Lobe -
 Brain: Oligodendroglioma, Mixed Astrocytoma & Oligodendroglioma
Brain: Oligodendroglioma, Mixed Astrocytoma & Oligodendroglioma -
 Brain: Oligodendroglioma
Brain: Oligodendroglioma -
 Brain: Oligodendroglioma
Brain: Oligodendroglioma -
 Brain: Glioma, Grade II Anaplastic
Brain: Glioma, Grade II Anaplastic -
 Brain: Glioma, Brain stem, Low Grade
Brain: Glioma, Brain stem, Low Grade -
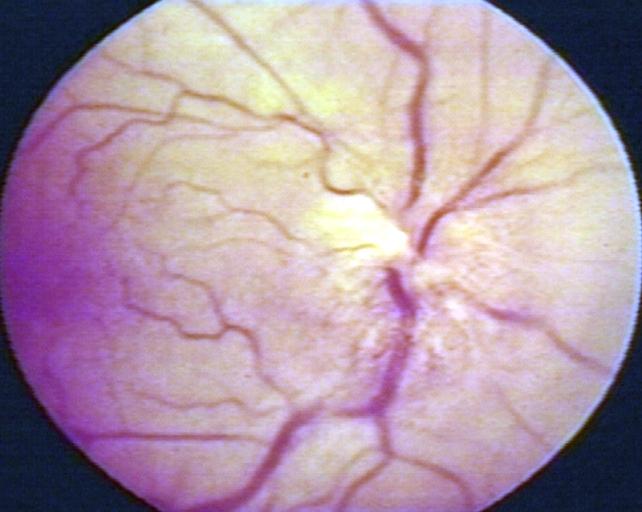 Fundoscopy: Eye; Optic Nerve Glioma, Optic Nerve
Fundoscopy: Eye; Optic Nerve Glioma, Optic Nerve -
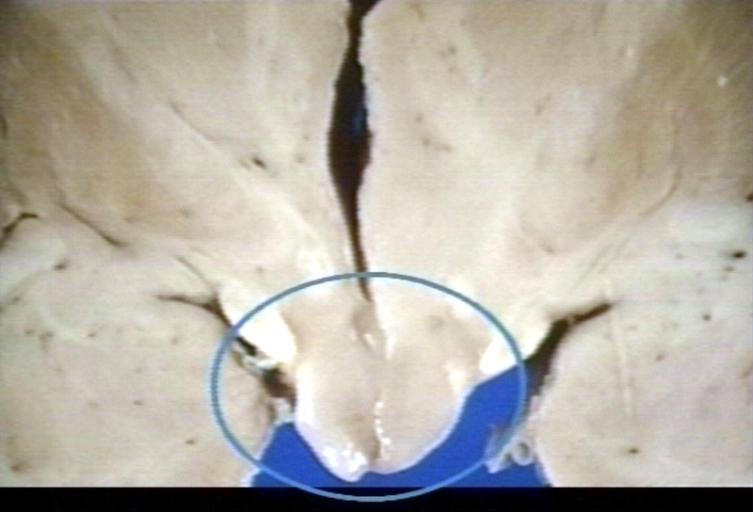 Brain: Glioma, Hypothalamic, Circle Around Region of Tumor
Brain: Glioma, Hypothalamic, Circle Around Region of Tumor -
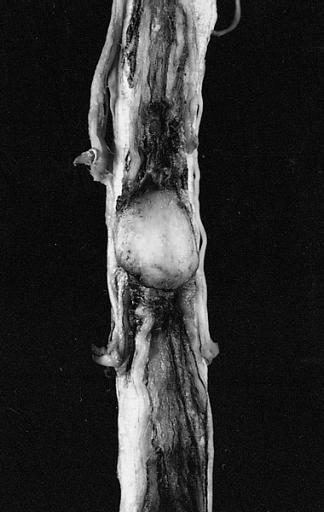
 CNS: Pilocytic Astrocytoma of the Spinal Cord. The fusiform expansion of the spinal cord produced by this pilocytic astrocytoma is not, on external examination alone, distinguishable from that produced by a nonresectable diffuse glioma.
CNS: Pilocytic Astrocytoma of the Spinal Cord. The fusiform expansion of the spinal cord produced by this pilocytic astrocytoma is not, on external examination alone, distinguishable from that produced by a nonresectable diffuse glioma. -
 Brain: Glioma, Pontine
Brain: Glioma, Pontine -
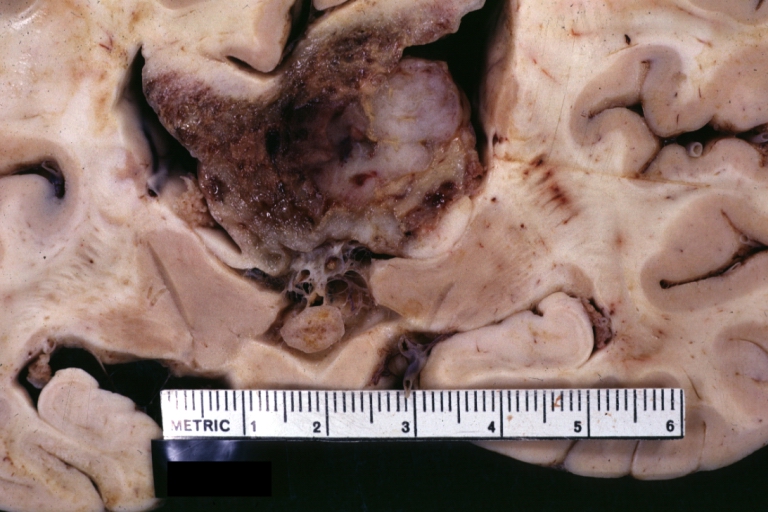 Brain: Glioblastoma Multiforme: Gross fixed tissue close-up large necrotic tumor mass in septum pellucidum
Brain: Glioblastoma Multiforme: Gross fixed tissue close-up large necrotic tumor mass in septum pellucidum -
 Brain: Glioblastoma Multiforme: Gross fixed tissue coronal section of the brain with a large necrotic tumor mass in septum pellucidum diagnosed as astrocytoma grade III
Brain: Glioblastoma Multiforme: Gross fixed tissue coronal section of the brain with a large necrotic tumor mass in septum pellucidum diagnosed as astrocytoma grade III -
 Brain: Glioblastoma Multiforme: Gross natural color large hemorrhagic lesion in right centrum semiovale
Brain: Glioblastoma Multiforme: Gross natural color large hemorrhagic lesion in right centrum semiovale -
 CNS: Malignant pilocytic astrocytoma: A 29-year-old woman died 2 years after a diagnosis of “atypical pilocytic astrocytoma” of the pineal region. At autopsy, multiple tumor implants were present in the craniospinal subarachnoid spaces.
CNS: Malignant pilocytic astrocytoma: A 29-year-old woman died 2 years after a diagnosis of “atypical pilocytic astrocytoma” of the pineal region. At autopsy, multiple tumor implants were present in the craniospinal subarachnoid spaces. -
 Brain: Oligodendroglioma; Ventricular Cobblestone Effect
Brain: Oligodendroglioma; Ventricular Cobblestone Effect











































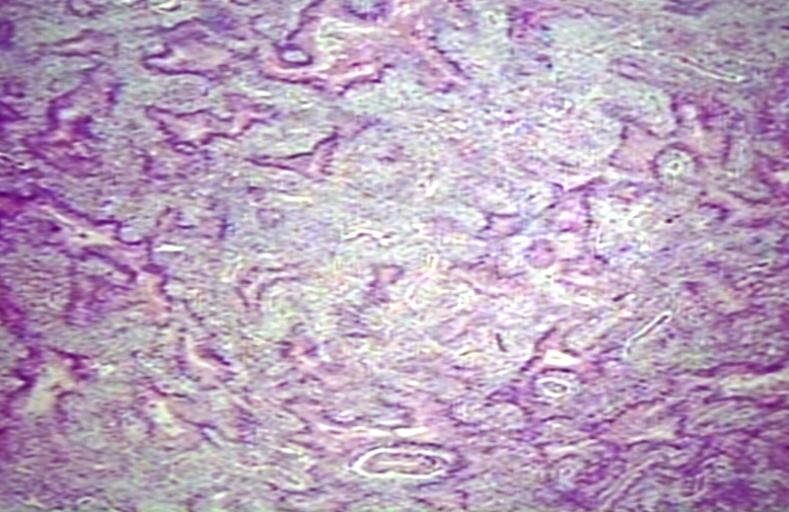
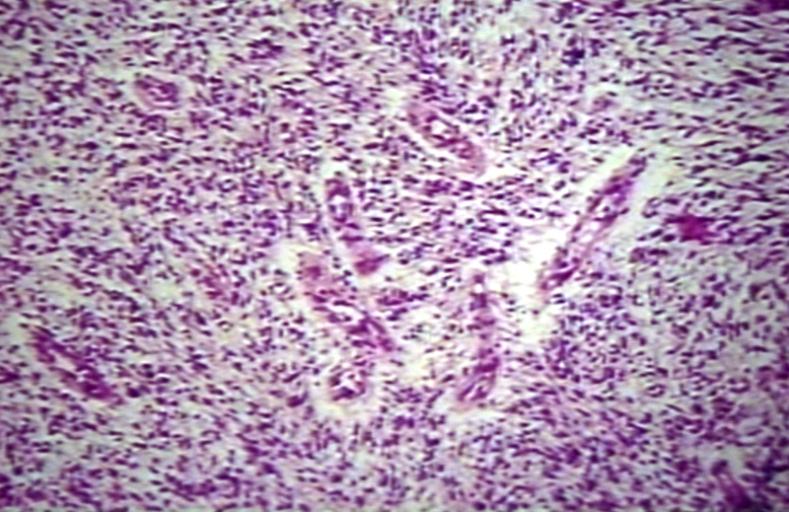
Microscopic Pathology
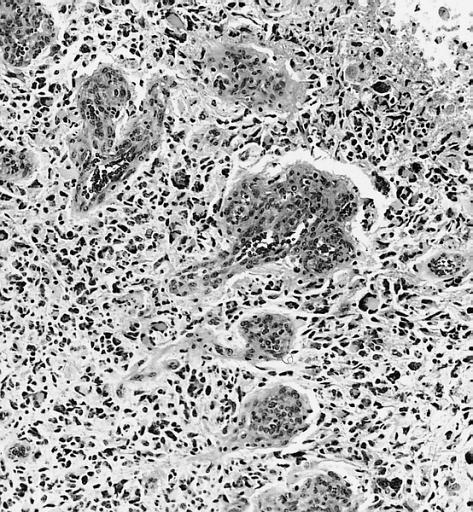
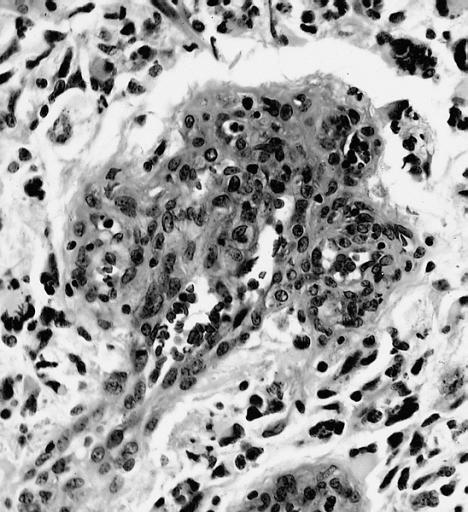
The histopathological appearance of glioma varies with the tumor grade and type, with increasing cellular atypia, mitoses, endothelial cell proliferation, and necrosis. Common findings are listed below:[4][5][6][7][8]
| Type of glioma | Histopathological features |
|---|---|
| |
| |
| |
| |
|
Gallery
-
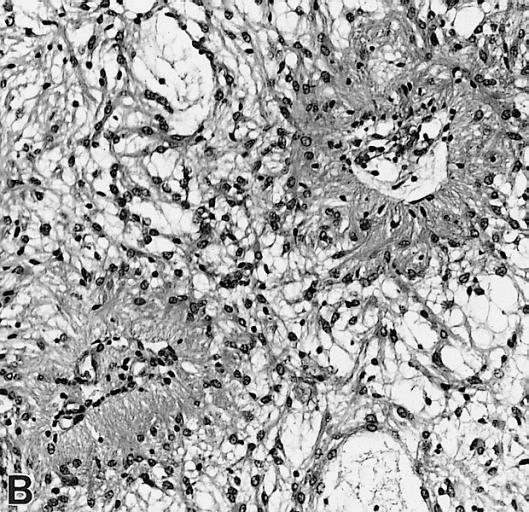
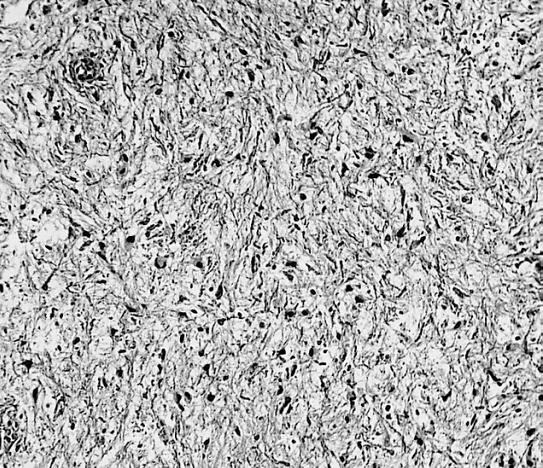
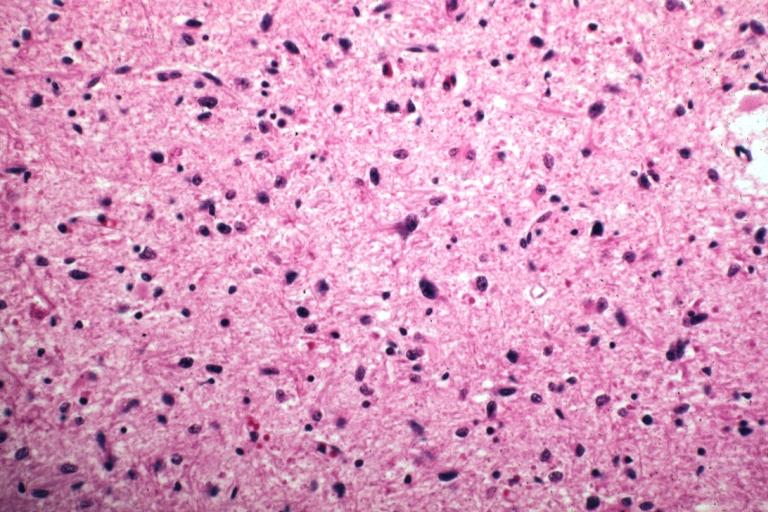
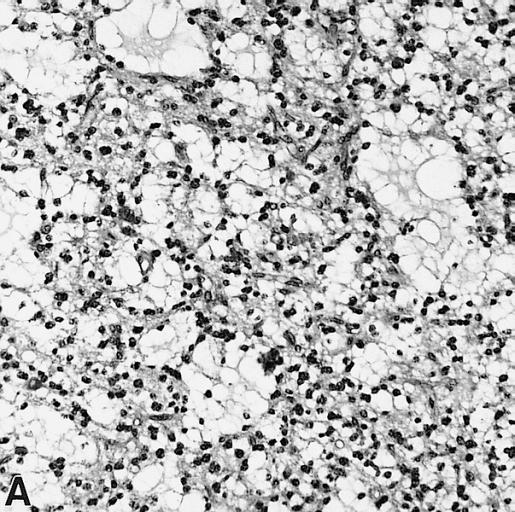 CNS: Pilocytic astrocytoma: variations in histologic appearance. As illustrated, many lesions are composed largely of spongy tissue rich in microcysts. Characteristic of pilocytic astrocytomas in general, the lesion is largely a solid mass of neoplastic cells without an obvious background of infiltrated brain.
CNS: Pilocytic astrocytoma: variations in histologic appearance. As illustrated, many lesions are composed largely of spongy tissue rich in microcysts. Characteristic of pilocytic astrocytomas in general, the lesion is largely a solid mass of neoplastic cells without an obvious background of infiltrated brain. -
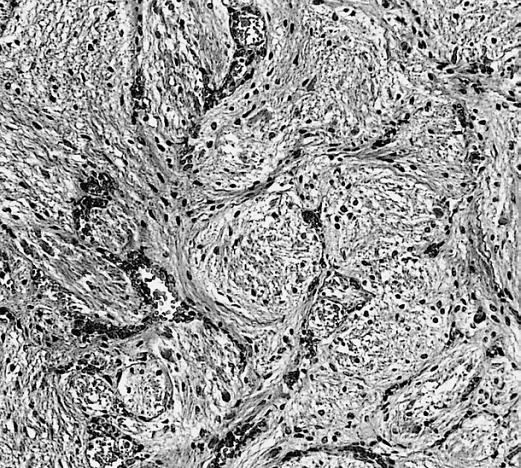
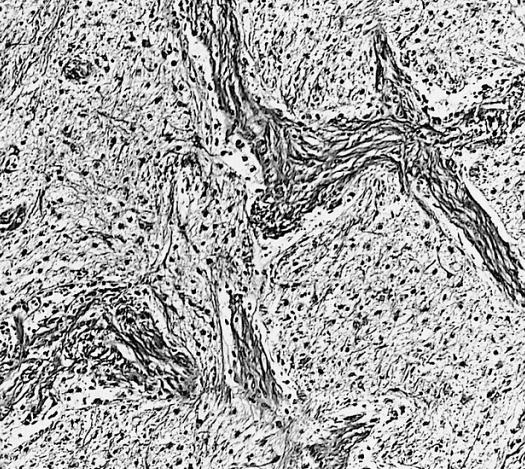
 CNS: Pilocytic astrocytoma: variations in histologic appearance. The perivascular radiating processes in some lesions can create a likeness to an ependymoma. Note the spongy background unusual for ependymomas.
CNS: Pilocytic astrocytoma: variations in histologic appearance. The perivascular radiating processes in some lesions can create a likeness to an ependymoma. Note the spongy background unusual for ependymomas. -
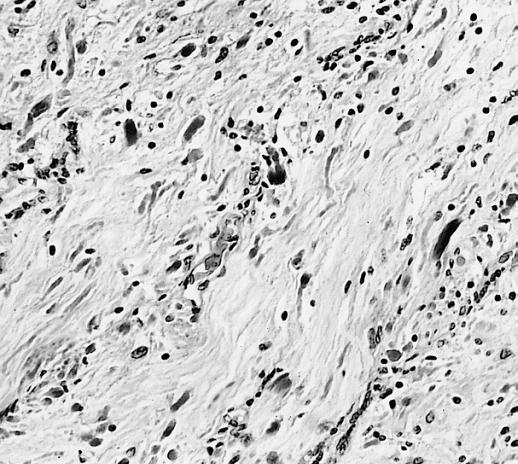
 CNS: Pilocytic astrocytoma: variations in histologic appearance. Other pilocytic astrocytomas are solid, rather than microcystic, and may be lobular.
CNS: Pilocytic astrocytoma: variations in histologic appearance. Other pilocytic astrocytomas are solid, rather than microcystic, and may be lobular. -
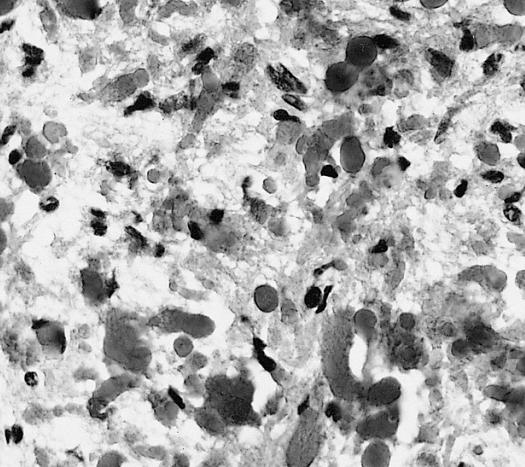
 CNS: Pilocytic astrocytoma: variations in histologic appearance. Rosenthal fibers, usually confined to the solid rather than spongy regions are found in many pilocytic astrocytomas, but are not requisite for the diagnosis.
CNS: Pilocytic astrocytoma: variations in histologic appearance. Rosenthal fibers, usually confined to the solid rather than spongy regions are found in many pilocytic astrocytomas, but are not requisite for the diagnosis. -
 CNS: Pilocytic astrocytoma: variations in histologic appearance. Rosenthal fibers are extremely abundant in some lesions. Particularly in the cerebellum, it can be difficult to distinguish such solid, paucicellular, highly fibrillar pilocytic astrocytomas from reactive gliosis with abundant Rosenthal fiber formation.
CNS: Pilocytic astrocytoma: variations in histologic appearance. Rosenthal fibers are extremely abundant in some lesions. Particularly in the cerebellum, it can be difficult to distinguish such solid, paucicellular, highly fibrillar pilocytic astrocytomas from reactive gliosis with abundant Rosenthal fiber formation. -
 CNS: Pilocytic astrocytoma: variations in histologic appearance. A loose array of polar cells creates an additional variant of pilocytic astrocytoma.
CNS: Pilocytic astrocytoma: variations in histologic appearance. A loose array of polar cells creates an additional variant of pilocytic astrocytoma. -
 CNS: Pilocytic astrocytoma: variations in histologic appearance. Some pilocytic astrocytomas are traversed by prominent collagenous septa.
CNS: Pilocytic astrocytoma: variations in histologic appearance. Some pilocytic astrocytomas are traversed by prominent collagenous septa. -
 CNS: Pilocytic astrocytoma: variations in histologic appearance. Unusual pilocytic astrocytomas have an extensive mucinous background without microcysts.
CNS: Pilocytic astrocytoma: variations in histologic appearance. Unusual pilocytic astrocytomas have an extensive mucinous background without microcysts. -
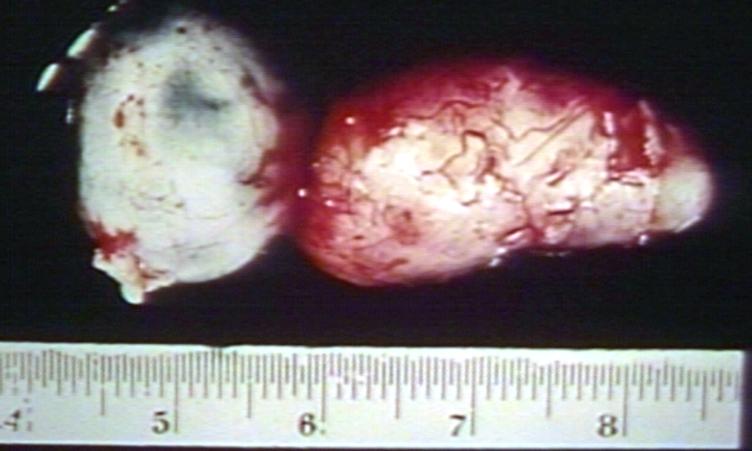
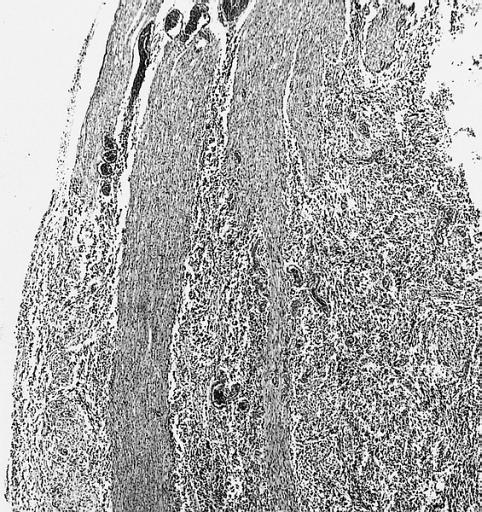
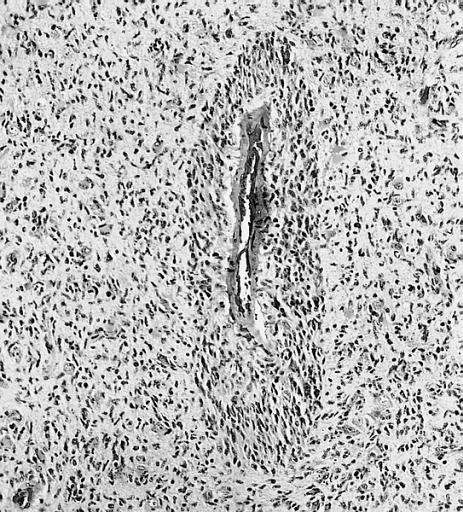
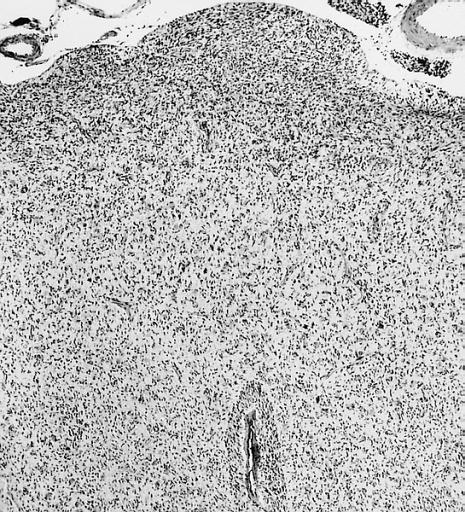
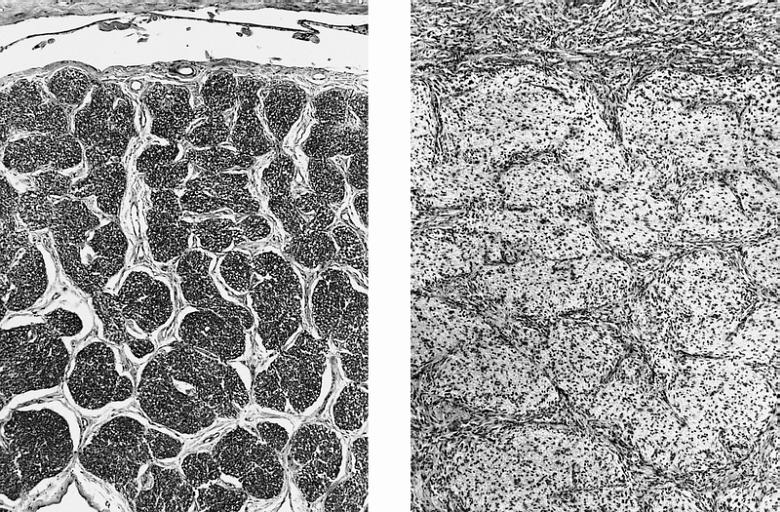 CNS: Comparison of normal optic nerve and pilocytic astrocytoma of the optic nerve. These two figures compare, at the same magnification, the normal optic nerve (left) with one containing a pilocytic astrocytoma (right). The neoplasm enlarges the compartments of the nerve and extends in collar-like fashion into the subarachnoid space.
CNS: Comparison of normal optic nerve and pilocytic astrocytoma of the optic nerve. These two figures compare, at the same magnification, the normal optic nerve (left) with one containing a pilocytic astrocytoma (right). The neoplasm enlarges the compartments of the nerve and extends in collar-like fashion into the subarachnoid space. -
 CNS: Pilocytic astrocytoma; The “hair cells” for which this lesion is named are readily seen.
CNS: Pilocytic astrocytoma; The “hair cells” for which this lesion is named are readily seen. -
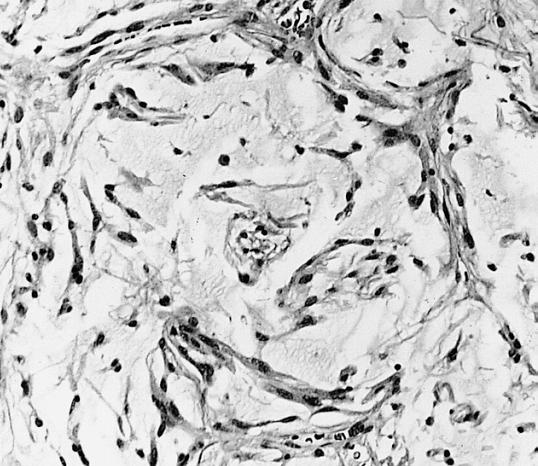
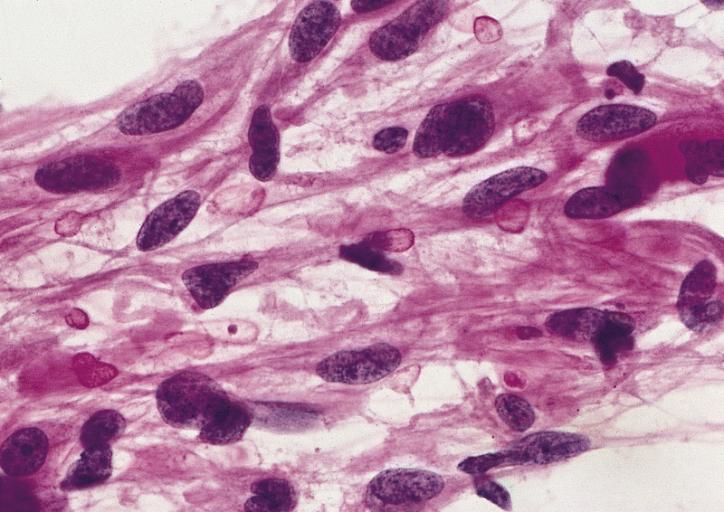
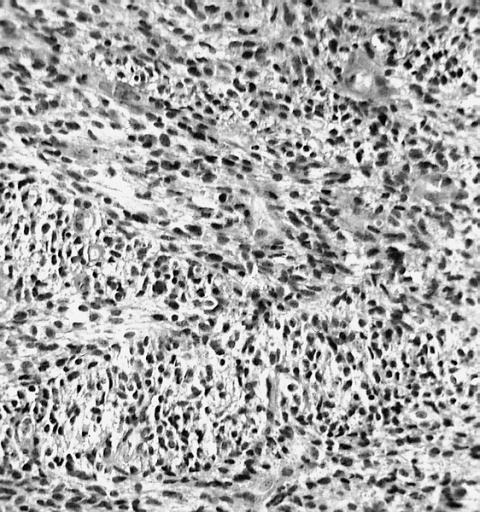
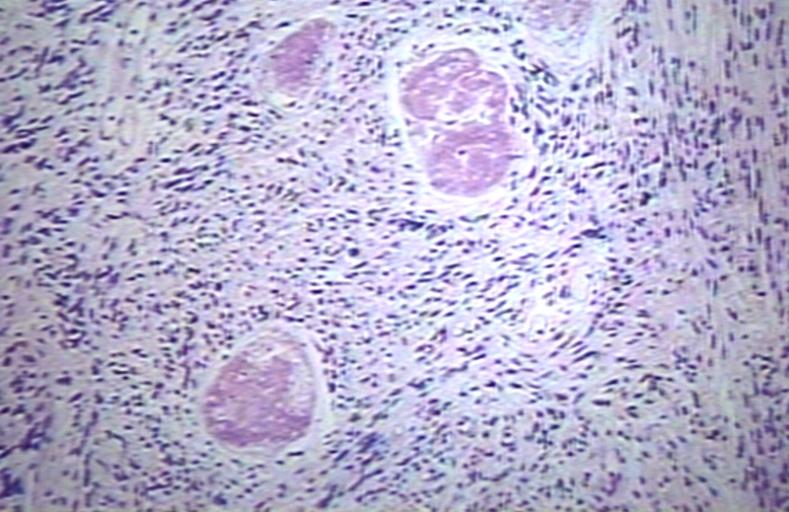
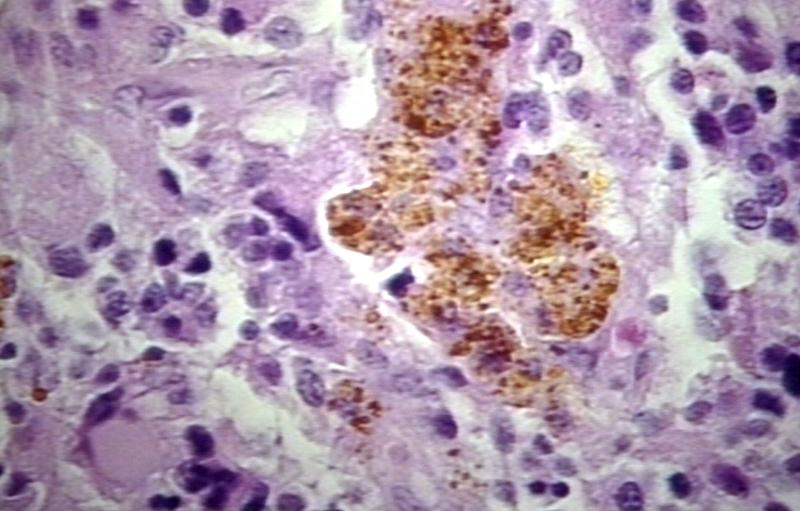
 CNS: Pilocytic astrocytoma; Nuclear hyperchromasia and pleomorphism are common. Note the typical cellular elongation, and, at the center of the illustration, the eosinophilic granular body that populates pilocytic astrocytomas and certain other slowly growing gliomas.
CNS: Pilocytic astrocytoma; Nuclear hyperchromasia and pleomorphism are common. Note the typical cellular elongation, and, at the center of the illustration, the eosinophilic granular body that populates pilocytic astrocytomas and certain other slowly growing gliomas. -
 CNS: Pilocytic astrocytoma; Intracytoplasmic Rosenthal fibers are prominent in some pilocytic neoplasms.
CNS: Pilocytic astrocytoma; Intracytoplasmic Rosenthal fibers are prominent in some pilocytic neoplasms. -
 Brain: Malignant ependymoma: Micro med mag H&E tumor cells.
Brain: Malignant ependymoma: Micro med mag H&E tumor cells. -
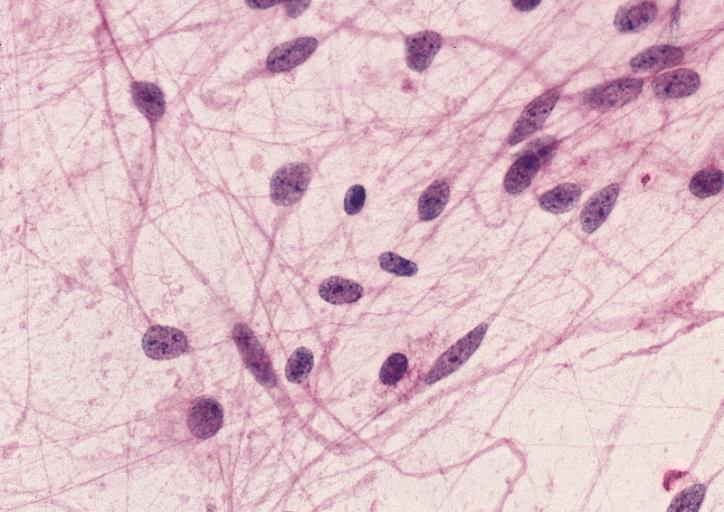
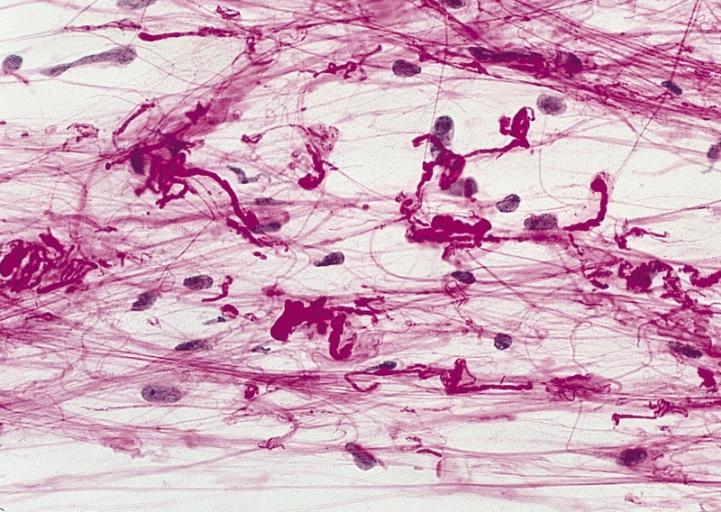
 CNS: Oligodendroglioma; Occasional oligodendrogliomas contain cells with minute, refractile eosinophilic bodies representing miniature Rosenthal fibers.
CNS: Oligodendroglioma; Occasional oligodendrogliomas contain cells with minute, refractile eosinophilic bodies representing miniature Rosenthal fibers. -
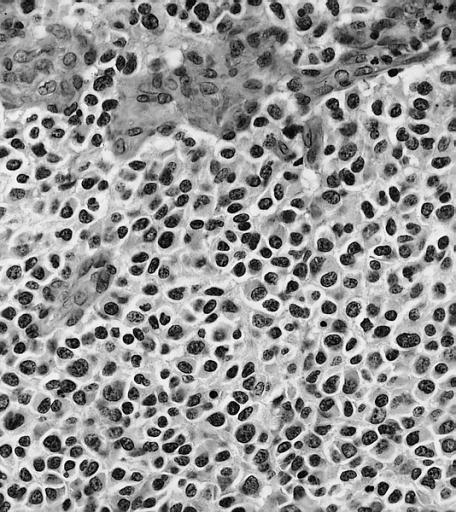
 CNS: Oligodendroglioma; The cells of some oligodendrogliomas acquire sufficient cytoplasm and process formation to become decidedly astrocytic, but their nuclei retain the roundness, uniformity, and chromatin distribution typical of oligodendroglioma.
CNS: Oligodendroglioma; The cells of some oligodendrogliomas acquire sufficient cytoplasm and process formation to become decidedly astrocytic, but their nuclei retain the roundness, uniformity, and chromatin distribution typical of oligodendroglioma. -
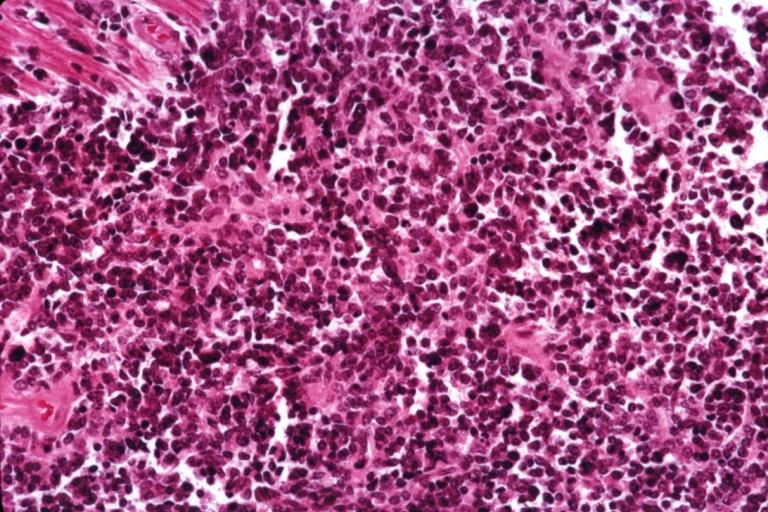
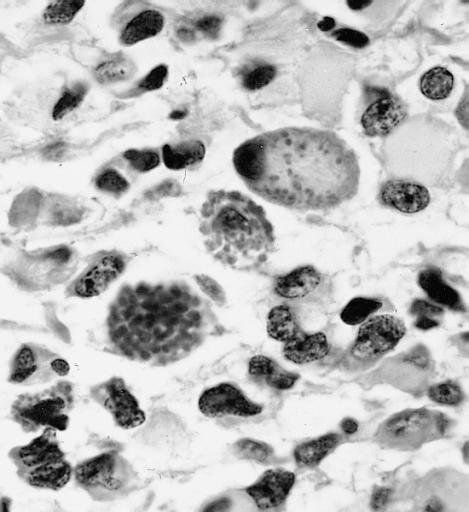
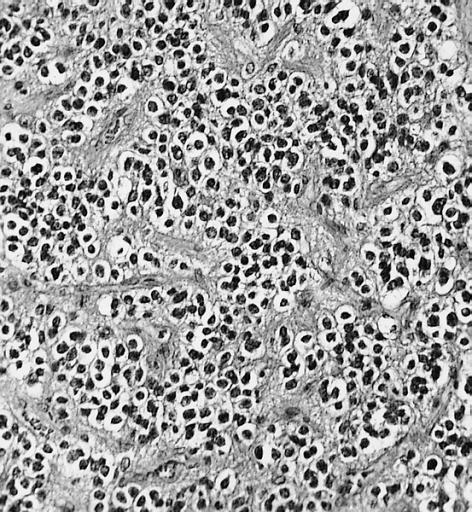
 Anaplastic oligodendroglioma: Anaplastic oligodendrogliomas are highly cellular and associated with vascular proliferation.
Anaplastic oligodendroglioma: Anaplastic oligodendrogliomas are highly cellular and associated with vascular proliferation. -
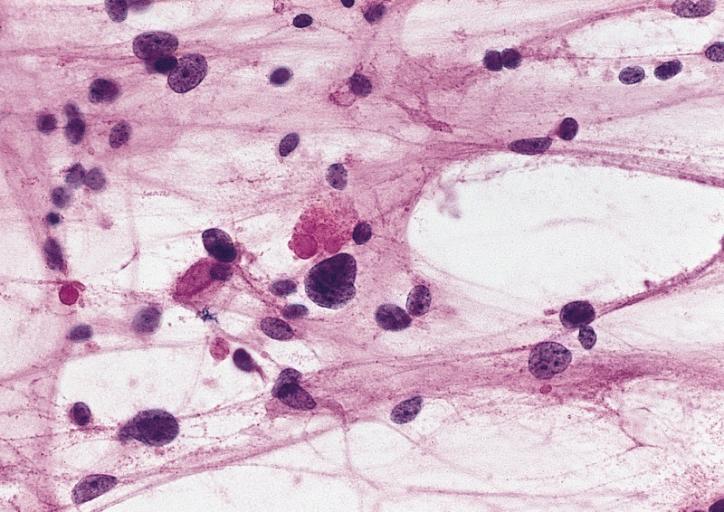
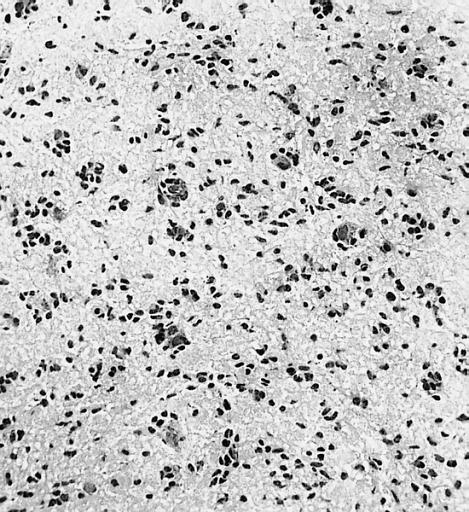 CNS: Oligodendroglioma (frozen section); Oligodendrogliomas in frozen sections lack the distinctive halos so often seen in permanent sections. Cellular monomorphism and infiltration of cerebral cortex with perineuronal satellitosis suggest the correct diagnosis.
CNS: Oligodendroglioma (frozen section); Oligodendrogliomas in frozen sections lack the distinctive halos so often seen in permanent sections. Cellular monomorphism and infiltration of cerebral cortex with perineuronal satellitosis suggest the correct diagnosis. -
 CNS: Clear cell ependymoma; Perinuclear clearing similar to that seen in oligodendrogliomas is a prominent feature of the clear cell variant. Note the vague perivascular pseudorosettes. The lesion was a discrete occipital intraventricular mass.
CNS: Clear cell ependymoma; Perinuclear clearing similar to that seen in oligodendrogliomas is a prominent feature of the clear cell variant. Note the vague perivascular pseudorosettes. The lesion was a discrete occipital intraventricular mass. -
 CNS: Glioblastoma multiforme; Brain: Glioblastoma multiforme. Grade I-Ii: Micro med mag with H&E, tumor well shown
CNS: Glioblastoma multiforme; Brain: Glioblastoma multiforme. Grade I-Ii: Micro med mag with H&E, tumor well shown -
 CNS: Glioblastoma multiforme arising in an astrocytoma. At higher magnification, gemistocytic astrocytoma with microcystic change is apparent at the bottom of the illustration and cellular nodules of glioblastoma multiforme are seen at the top. The 6-year history of symptoms attested to the initially low-grade nature of this astrocytic tumor.
CNS: Glioblastoma multiforme arising in an astrocytoma. At higher magnification, gemistocytic astrocytoma with microcystic change is apparent at the bottom of the illustration and cellular nodules of glioblastoma multiforme are seen at the top. The 6-year history of symptoms attested to the initially low-grade nature of this astrocytic tumor. -
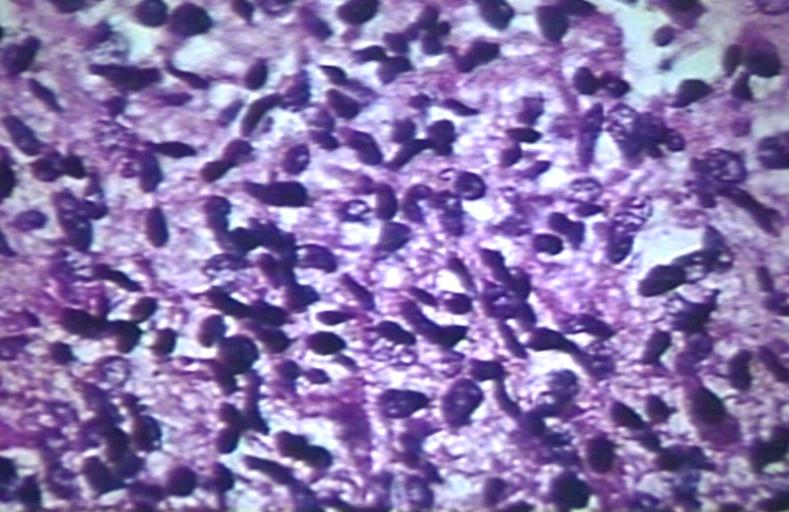
 CNS: Glioblastoma multiforme; Characteristic of most glioblastomas are small cells with elongated nuclei and bipolar processes. As here, the chromatin is generally not markedly dense nor are nucleoli usually prominent.
CNS: Glioblastoma multiforme; Characteristic of most glioblastomas are small cells with elongated nuclei and bipolar processes. As here, the chromatin is generally not markedly dense nor are nucleoli usually prominent. -
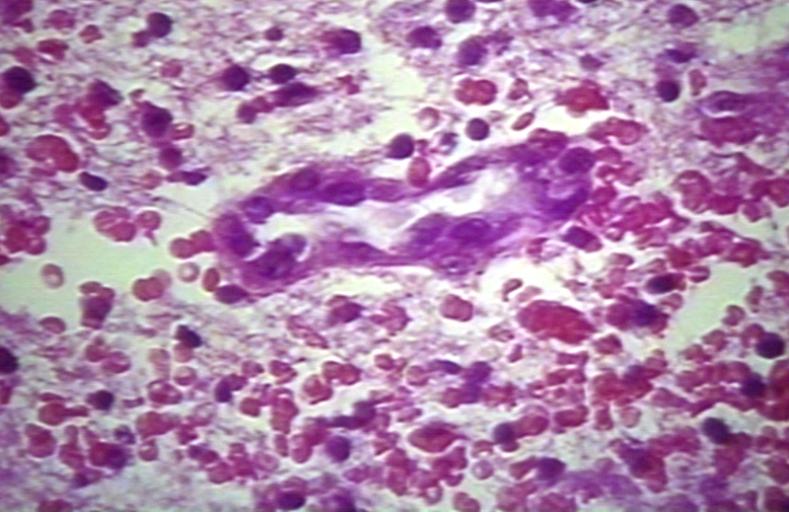
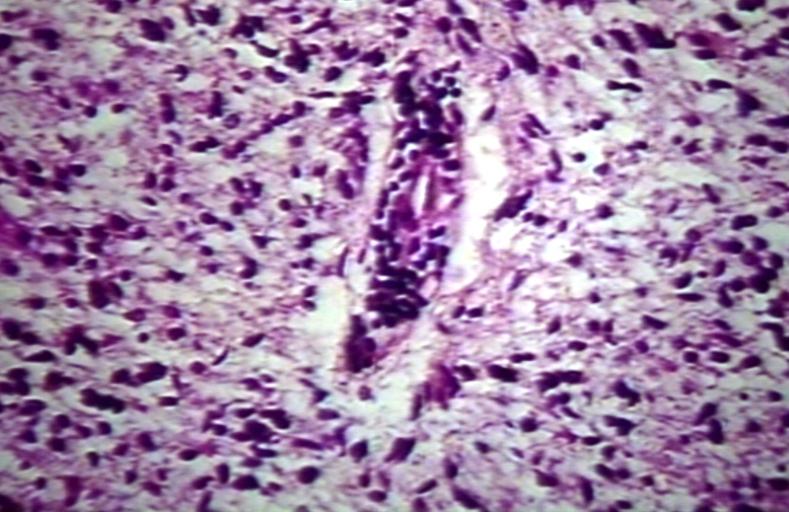
 CNS: Glioblastoma multiforme; Vascular proliferation, a common feature of glioblastoma, produces tufts which often grow directionally. Here, as is often the case, they are oriented toward a focus of necrosis (top right).
CNS: Glioblastoma multiforme; Vascular proliferation, a common feature of glioblastoma, produces tufts which often grow directionally. Here, as is often the case, they are oriented toward a focus of necrosis (top right). -
 CNS: Glioblastoma multiforme; At high magnification, the neovascular tuft is a mass which, as can be confirmed by immunohistochemistry, is formed of both endothelial cells and smooth muscle cells (pericytes).
CNS: Glioblastoma multiforme; At high magnification, the neovascular tuft is a mass which, as can be confirmed by immunohistochemistry, is formed of both endothelial cells and smooth muscle cells (pericytes). -
 CNS: Glioblastoma multiforme; In many instances, necrosis is surrounded by a distinctive collar of cells, which are often smaller than those in surrounding neoplastic tissue. The phenomenon is referred to as pseudopalisading.
CNS: Glioblastoma multiforme; In many instances, necrosis is surrounded by a distinctive collar of cells, which are often smaller than those in surrounding neoplastic tissue. The phenomenon is referred to as pseudopalisading. -
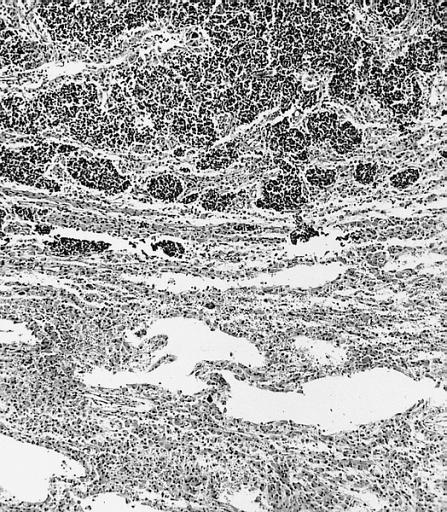
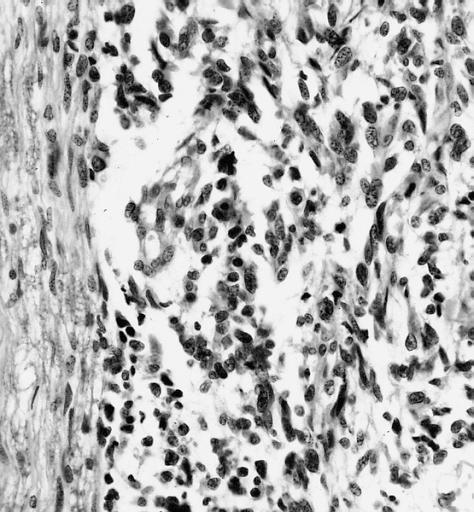
 CNS: Cerebrospinal dissemination of glioblastoma multiforme; As seen at low (left) and high (right) magnification, the small undifferentiated-appearing cells of this glioblastoma are drop metastases colonizing the nerve roots of the cauda equina.
CNS: Cerebrospinal dissemination of glioblastoma multiforme; As seen at low (left) and high (right) magnification, the small undifferentiated-appearing cells of this glioblastoma are drop metastases colonizing the nerve roots of the cauda equina. -
 CNS: Cerebrospinal dissemination of glioblastoma multiforme; As seen at low (left) and high (right) magnification, the small undifferentiated-appearing cells of this glioblastoma are drop metastases colonizing the nerve roots of the cauda equina.
CNS: Cerebrospinal dissemination of glioblastoma multiforme; As seen at low (left) and high (right) magnification, the small undifferentiated-appearing cells of this glioblastoma are drop metastases colonizing the nerve roots of the cauda equina. -
 CNS: Glioblastoma multiforme; Higher magnification reveals the small cell nature of such tumors.
CNS: Glioblastoma multiforme; Higher magnification reveals the small cell nature of such tumors. -
 CNS: Glioblastoma multiforme; Some glioblastomas are especially infiltrative of the cerebral cortex where subpial, perivascular, and perineuronal accumulations are prominent.
CNS: Glioblastoma multiforme; Some glioblastomas are especially infiltrative of the cerebral cortex where subpial, perivascular, and perineuronal accumulations are prominent. -
 CNS: Glioblastoma multiforme; Although this densely cellular and largely undifferentiated lesion technically merits a diagnosis of anaplastic astrocytoma, it is, for practical purposes, a glioblastoma.
CNS: Glioblastoma multiforme; Although this densely cellular and largely undifferentiated lesion technically merits a diagnosis of anaplastic astrocytoma, it is, for practical purposes, a glioblastoma. -
-
 Brain: Glioblastoma multiforme; pallisading
Brain: Glioblastoma multiforme; pallisading -
 Brain: Glioblastoma multiforme; vascular proliferation
Brain: Glioblastoma multiforme; vascular proliferation -
 Brain: Glioblastoma multiforme; Plump and juicy endothelial cells, extravasated blood
Brain: Glioblastoma multiforme; Plump and juicy endothelial cells, extravasated blood -
 Brain: Glioblastoma multiforme; perivascular lymphocytes
Brain: Glioblastoma multiforme; perivascular lymphocytes -
 Brain: Glioblastoma multiforme; thrombosed vessel
Brain: Glioblastoma multiforme; thrombosed vessel -
 Brain: Glioblastoma multiforme; Hemosiderin in glioblastoma
Brain: Glioblastoma multiforme; Hemosiderin in glioblastoma




































References
- ↑ 1.0 1.1 Pathology of glioma. http://www.surgwiki.com/wiki/Intracranial_tumours,_infection_and_aneurysms
- ↑ 2.0 2.1 Pathology of glioma. Wikipedia. https://en.wikipedia.org/wiki/Glioma
- ↑ 3.0 3.1 3.2 Schwartzbaum JA, Fisher JL, Aldape KD, Wrensch M (2006). “Epidemiology and molecular pathology of glioma”. Nat Clin Pract Neurol. 2 (9): 494–503, quiz 1 p following 516. doi:10.1038/ncpneuro0289. PMID 16932614.
- ↑ 4.0 4.1 4.2 Pathology of pilocytic astrocytoma. Libre Pathology. http://librepathology.org/wiki/index.php/Pilocytic_astrocytoma
- ↑ 5.0 5.1 5.2 Pathology of gliomas. Libre Pathology. http://librepathology.org/wiki/index.php/Oligodendroglioma
- ↑ 6.0 6.1 6.2 Pathology of anaplastic astrocytoma. Libre Pathology. http://librepathology.org/wiki/index.php?title=Neuropathology_tumours&redirect=no#Infiltrative_astrocytomas
- ↑ 7.0 7.1 7.2 Pathology of glioblastoma. Libre Pathology. http://librepathology.org/wiki/index.php/Glioblastoma
- ↑ 8.0 8.1 8.2 Pathology of ependymoma. Libre Pathology. http://librepathology.org/wiki/index.php/Ependymoma
- ↑ Dubois LG, Campanati L, Righy C, D’Andrea-Meira I, Spohr TC, Porto-Carreiro I; et al. (2014). “Gliomas and the vascular fragility of the blood brain barrier”. Front Cell Neurosci. 8: 418. doi:10.3389/fncel.2014.00418. PMC 4264502. PMID 25565956.
- ↑ Reuss, D; von Deimling, A (2009). “Hereditary tumor syndromes and gliomas”. Recent results in cancer research. Fortschritte der Krebsforschung. Progres dans les recherches sur le cancer. 171: 83–102. doi:10.1007/978-3-540-31206-2_5. PMID 19322539.
Causes
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]Associate Editor(s)-in-Chief: Sujit Routray, M.D. [2]
Overview
Common causes of glioma include genetic mutations (ERCC1, ERCC2, XRCC1, MGMT, IDH1, IDH2, p53, EGFR, TSC1, TSC2, RB1, APC, hMLH1, hMSH2, PMS2, PTEN, NF1, and NF2).[1][2]
Causes
References
- ↑ 1.0 1.1 Pathology of glioma. Wikipedia. https://en.wikipedia.org/wiki/Glioma
- ↑ 2.0 2.1 Schwartzbaum JA, Fisher JL, Aldape KD, Wrensch M (2006). “Epidemiology and molecular pathology of glioma”. Nat Clin Pract Neurol. 2 (9): 494–503, quiz 1 p following 516. doi:10.1038/ncpneuro0289. PMID 16932614.
Differentiating Glioma from other Diseases
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]Associate Editor(s)-in-Chief: Sujit Routray, M.D. [2]
Overview
Glioma must be differentiated from primary CNS lymphoma, cerebral metastases, meningioma, brain abscess, cavernous malformation, stroke, acute disseminated encephalomyelitis, cavernous sinus syndrome, intracranial hemorrhage, gerstmann syndrome, spinal tuberculosis, hamartoma, germinoma, teratoma, piloid gliosis, and progressive multifocal leukoencephalopathy.[1][2]
Differential diagnosis
Glioma must be differentiated from:[1][2]
- Primary CNS lymphoma
- Cerebral metastases
- Meningioma
- Brain abscess
- Cavernous malformation
- Stroke
- Acute disseminated encephalomyelitis
- Cavernous sinus syndrome
- Intracranial hemorrhage
- Gerstmann syndrome
- Spinal tuberculosis
- Hamartoma
- Germinoma
- Teratoma
- Piloid gliosis
- Progressive multifocal leukoencephalopathy
References
- ↑ 1.0 1.1 DDx of gliomas. Libre Pathology. http://librepathology.org/wiki/index.php/Oligodendroglioma
- ↑ 2.0 2.1 Differential diagnosis of glioblastoma multiforme. Dr Dylan Kurda and Dr Frank Gaillard et al. Radiopaedia 2015. http://radiopaedia.org/articles/Glioblastoma
Epidemiology and Demographics
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]Associate Editor(s)-in-Chief: Sujit Routray, M.D. [2]
Overview
Glioma is the most common primary intracranial tumor. The incidence of glioma is estimated to be 4.9 cases per 100,000 individuals in the US.[1] Patients of all age groups may develop glioma. Males are more commonly affected with glioma than females. It usually affects individuals of the caucasian race. African american, latin american, and asian individuals are less likely to develop glioma.
Epidemiology and demographics
Incidence
- Glioma is the most common primary intracranial tumor.
- The incidence of glioma is estimated to be 4.9 cases per 100,000 individuals in the US.[1]
Age
- Patients of all age groups may develop glioma.
- Pilocytic astrocytoma is a common disease that tends to affect children and adolescents. The median age at diagnosis is 17 years.
- Glioblastoma multiforme is a common disease that tends to affect the elderly population. The median age at diagnosis is 62 years.
Gender
- Males are more commonly affected with glioma than females.[1]
Race
- Glioma usually affects individuals of the caucasian race. African american, latin american, and asian individuals are less likely to develop glioma.
References
- ↑ 1.0 1.1 1.2 Schwartzbaum JA, Fisher JL, Aldape KD, Wrensch M (2006). “Epidemiology and molecular pathology of glioma”. Nat Clin Pract Neurol. 2 (9): 494–503, quiz 1 p following 516. doi:10.1038/ncpneuro0289. PMID 16932614.
Risk Factors
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]Associate Editor(s)-in-Chief: Sujit Routray, M.D. [2]
Overview
Common risk factors in the development of glioma may be occupational, environmental, genetic, and viral.[1][2][3][4][5]
Risk factors
Common risk factors in the development of glioma may be occupational, environmental, genetic, and viral.[1][2][3][4][5]
| Category | Risk factors |
|---|---|
|
Occupational factors |
|
|
Environmental factors |
|
|
Genetic factors |
|
|
Viruses |
References
- ↑ 1.0 1.1 Efird, Jimmy T.; Davies, Stephen W.; O’Neal, Wesley T.; Anderson, Ethan J. (2014). “Animal viruses, bacteria, and cancer: a brief commentary”. Frontiers in Public Health. 2: 14. doi:10.3389/fpubh.2014.00014. ISSN 2296-2565. PMC 3923154. PMID 24592380.
- ↑ 2.0 2.1 Ruder, Avima M.; Carreón, Tania; Butler, Mary Ann; Calvert, Geoffrey M.; Davis-King, Karen E.; Waters, Martha A.; Schulte, Paul A.; Mandel, Jack S.; Morton, Roscoe F. (Jun 15, 2009). “Exposure to farm crops, livestock, and farm tasks and risk of glioma: the Upper Midwest Health Study”. American Journal of Epidemiology. 169 (12): 1479–1491. doi:10.1093/aje/kwp075. ISSN 1476-6256. PMID 19403843.
- ↑ 3.0 3.1 Ostrom, Quinn T.; Bauchet, Luc; Davis, Faith G.; Deltour, Isabelle; Fisher, James L.; Langer, Chelsea Eastman; Pekmezci, Melike; Schwartzbaum, Judith A.; Turner, Michelle C. (Jul 2014). “The epidemiology of glioma in adults: a “state of the science” review”. Neuro-Oncology. 16 (7): 896–913. doi:10.1093/neuonc/nou087. ISSN 1523-5866. PMC 4057143. PMID 24842956.
- ↑ 4.0 4.1 Reuss, D; von Deimling, A (2009). “Hereditary tumor syndromes and gliomas”. Recent results in cancer research. Fortschritte der Krebsforschung. Progres dans les recherches sur le cancer. 171: 83–102. doi:10.1007/978-3-540-31206-2_5. PMID 19322539.
- ↑ 5.0 5.1 Schwartzbaum JA, Fisher JL, Aldape KD, Wrensch M (2006). “Epidemiology and molecular pathology of glioma”. Nat Clin Pract Neurol. 2 (9): 494–503, quiz 1 p following 516. doi:10.1038/ncpneuro0289. PMID 16932614.
Screening
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]Associate Editor(s)-in-Chief: Sujit Routray, M.D. [2]
Overview
There is insufficient evidence to recommend routine screening for glioma.[1]
Screening
There is insufficient evidence to recommend routine screening for glioma.[1]
References
- ↑ 1.0 1.1 Early detection, diagnosis, and staging of glioma. American cancer society. http://www.cancer.org/cancer/braincnstumorsinadults/detailedguide/brain-and-spinal-cord-tumors-in-adults-detection
Natural History, Complications and Prognosis
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]Associate Editor(s)-in-Chief: Sujit Routray, M.D. [2]
Overview
Common complications of glioma include brain herniation, hydrocephalus, coma, metastasis, recurrence, side effects of chemotherapy, and side effects of radiation therapy. The prognosis of glioma varies with the grade of tumor. The 1-year and 2-year survival rate of patients with malignant glioma is approximately 50% and 25%, respectively.[1]
Complications
Common complications of glioma include:
- Brain herniation
- Hydrocephalus
- Coma
- Metastasis
- Recurrence
- Side effects of chemotherapy
- Side effects of radiation therapy
Prognosis
- The prognosis of glioma varies with the grade of tumor: WHO grade 1 and WHO grade 4 have the most favorable and worst prognosis, respectively.
- The 1-year and 2-year survival rate of patients with malignant glioma is approximately 50% and 25%, respectively.
- Post-operative radiation therapy is often used as an adjunct to surgery in the treatment of high-grade gliomas as it has shown to double the median survival for high-grade gliomas to 37 weeks (versus 17 weeks with surgery alone).
- The prognosis of glioma may depend on other factors which include:[1]
- Location of the tumor (brain or spinal cord)
- Resectability
- Primary diagnosis vs. recurrence
- Specific mutations:
- DNA methylation of the O6-methylguanine-DNA methyltransferase (MGMT) gene promoter
- Mutation of isocitrate dehydrogenase: IDH1 or IDH2 genes
- Codeletion of chromosomes 1p and 19q
References
- ↑ 1.0 1.1 Prognostic factors of glioma. National Cancer Institute. http://www.cancer.gov/types/brain/patient/adult-brain-treatment-pdq
Diagnosis
Diagnosis
Staging | History and Symptoms | Physical Examination | Laboratory Findings | X Ray | CT | MRI | Ultrasound | Other Imaging Findings | Other Diagnostic Studies
Treatment
Treatment
Medical Therapy | Surgery | Cost-Effectiveness of Therapy | Future or Investigational Therapies
Looking for the patient version?
© 2026 MyEClinic – IFTM Institut für Telematik in der Medizin GmbH