
Iron deficiency anemia
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor-In-Chief: Jogeet Singh Sekhon, M.D. [2] Cafer Zorkun, M.D., Ph.D. [3]
Synonyms and keywords: Fe deficiency anemia
For patient information, click here
Overview
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief:
Overview
Iron deficiency anemia occurs when body iron stores are inadequate to meet normal metabolic demands of the body. It is the most common cause of microcytic anemia.
Iron deficiency anemia occurs in the setting of blood loss, insufficient dietary intake or poor oral absorption of iron from food. Symptoms of iron deficiency anemia including fatigue, weakness, shortness of breath, lightheadedness, and pallor. Twenty percent of all women of childbearing age have iron deficiency anemia, compared with only 2% of adult men. The principal cause of iron deficiency anemia in premenopausal women is excessive blood loss during menses. In post menopausal women and men, the main cause of iron deficiency are digestive tract diseases.
Iron deficiency anemia is the final stage of iron deficiency. When the body has sufficient iron to meet its needs (functional iron), the remainder is stored for later use in the bone marrow, liver, and spleen. Iron deficiency ranges from iron depletion, which yields little physiological damage, to iron deficiency anemia, which can affect the function of numerous organ systems. Iron depletion causes the amount of stored iron to be reduced, but has no effect on the functional iron. However, a person with no stored iron has no reserves to use if the body requires more iron. In essence, the amount of iron absorbed by the body is not adequate for growth and development or to replace the amount lost.
Historical Perspective
Iron deficiency anemia was discovered in 1852 by Karl Vierordt and his student H. Welcher.
Classification
There is no established system for the classification of iron deficiency. However, based on the pathology, it can be divided into functional and absolute iron deficiency.
Pathophysiology
Iron homeostasis is maintained by a balance of iron absorption and iron loss. Iron absorption is a more active process and is mainly responsible for regulation of iron balance. The absorption of iron is highly regulated by hepcidin, a protein secreted by hepatocytes.
Iron is absorbed in ferrous form (Fe2+) in the small intestine via divalent metal transporter (DMT1). After absorption, depending on iron levels in the body, iron can be sequestered in ferritin or bound to transferrin by ferroportin. Once bound to transferrin, iron is transported to cells that require iron. Iron enters cells when transferrin binds to transferrin receptor (TfR).
Iron deficiency occurs in three stages. In the prelatent stage, ferritin is low but serum iron levels are normal. In the latent stage, transferrin saturation and serum iron are also low in addition to low ferritin. In the last stage, hemoglobin level is below normal along with depletion of iron stores and drop in serum iron and transferrin saturation.
Causes
In developed nations, the main cause of iron deficiency anemia is blood loss. Bleeding from any source can cause iron deficiency anemia. Obvious causes of blood loss like menorrhagia, hematemesis, melena, hematuria, multiple child births, frequent blood donations can be easily recognized with history alone. Occult blood loss from causes like GI bleeding, parasitic infestations etc may be overlooked.
Inadequate dietary iron is the most common cause of iron deficiency anemia in resource poor countries. It is also the most common cause of iron deficiency anemia in toddlers. In toddlers, poor nutritional practices like excessive cow milk intake or snacking contribute to iron deficiency.
Malabsorption due to celiac disease, atrophic gastritis, Helicobacter pylori infection, post-bariatric surgery can also cause iron deficiency.
Drugs which suppress gastric acid can also impair absorption of iron as iron requires an acidic medium for absorption. Certain antibiotics like quinolones, doxycyline, chrloramphenicol etc also diminish the absorption of iron.[1]
Chronic conditions like chronic heart failure, CKD, inflammatory bowel disease, malignancy, rheumatoid arthritis are also associated with iron deficiency anemia.
Other less common cause of iron deficiency include urinary and pulmonary hemosiderosis and genetic conditions like IRIDA due to TMPRSS6 mutations.
Differentiating Iron Deficiency Anemia from other Diseases
Iron deficiency anemia and Thalassemia Minor present with many of the same lab results. It is very important not to treat a patient with Thalassemia with an iron supplement as this can lead to hemochromatosis (accumulation of iron in the liver) A hemoglobin electrophoresis would provide useful evidence in distinguishing these two conditions, along with iron studies.
Epidemiology and Demographics
According to WHO’s Global Burden of Disease Project 2000 (GBD 2000), iron deficiency is responsible for 841,000 deaths worldwide with the major burden of mortality seen in Africa and parts of Asia.
In the US, iron deficiency is seen in 9% of toddlers between age 1 and 2 years. Compared to white toddlers, Hispanic toddlers are twice as likely to have iron deficiency.[2]
The prevalence in adolescent girls and women in reproductive age group is between 9% to 11%. It is most commonly seen in multiparous women from low income minority populations. In males, it is seen in around 1% of population with slightly high prevalence of 2 – 4% in middle aged and older men.
There is a positive correlation between obesity and the risk of developing iron deficiency.[3]
Risk Factors
Risk of iron deficiency anemia is more in those individuals who consume less iron in diet and who are at increased risk of bleeding.
Screening
Screening is recommended in women of reproductive age and toddlers.
Natural History, Complications, and Prognosis
Untreated iron deficiency anemia is associated with significant cognitive impairment and decreased work capacity and quality of life.
During pregnancy, untreated iron deficiency can affect fetal brain maturation and predispose the newborn to iron deficiency and low birth weight. Maternal adverse outcomes include depression, increase risk of sepsis and maternal mortality.
In patients undergoing cardiac or abdominal surgery, pre operative iron deficiency is associated with poor outcomes. In patients with heart failure, untreated iron deficiency can cause an increase in mortality.
If treated with iron supplementation, the prognosis is excellent.
Diagnosis
Diagnostic criteria
Iron deficiency anemia is diagnosed on the basis of results of CBC, peripheral blood film and iron studies. A normal hemoglobin does not rule out iron deficiency. Iron deficiency is diagnosed when serum ferritin is < 30ng/mL.
History and Symptoms
Majority of symptoms are non specific and include weakness, fatigue, dyspnea on exertion, irritability, poor concentration and decreased exercise capacity. These are attributable to low oxygen delivery to tissues and decreased activity of iron containing enzymes.
Pica occurs in approximately half of these patients and pagophagia (craving for ice) is quite specific for iron deficiency.[4]
Patients may have a history of dry mouth, hair loss, dysphagia, brittle fingernails and restless leg syndrome
Beeturia is a finding which is not specific for iron deficiency but is increased in these individuals. It is the result of a change in GI function due to severe Iron deficiency. The urine turns red following ingestion of beets.
Physical examination can be normal or show dry skin, atrophic glossitis, cheilosis, pallor and koilonychia(spoon shaped nails). Cardiac auscultation may reveal systolic murmur.
Physical Examination
Physical examination may reveal pallor, koilonychia (spoon shaped nails), cheilosis, atrophic glossitis, dry skin and systolic murmur on cardiac auscultation.
Laboratory Findings
The first step in diagnosis is ordering a CBC, peripheral smear and serum ferritin. Low serum ferritin is only seen in iron deficiency anemia but high ferritin can be seen in many chronic disorders. Absolute iron deficiency is diagnosed with a serum ferritin of < 30ng/mL. A normal hemoglobin does not exclude iron deficiency as hemoglobin does not become low till a significant percentage of body iron is depleted.
Uncomplicated iron deficiency can be diagnosed by assessing standard iron parameters, such as serum ferritin and transferrin saturation.
Serum iron varies during the day and is influenced by diet. A fasting sample should be obtained in the morning. Plasma iron is reduced as the iron in the body is exhausted. Total iron binding capacity (TIBC) is elevated in iron deficiency anemia.
Serum transferrin is raised in iron deficiency anemia. Transferrin saturation index (TSAT) is the ratio of serum iron to TIBC. It is one of the earliest biomarker of ID and is useful when serum ferritin is unequivocal. A decrease (< 20%) indicates ID, either absolute or functional.[5]
Soluble transferrin receptor (sTfR) is a fragment of membrane receptor for transferrin. It is elevated in iron deficiency because of upregulation of transferrin receptors. It can help differentiate between absolute(increased sTfR) and functional ID( normal sTfR).
sTfR–Ferritin index is the ratio of sTfR to serum ferritin. It is also considered a good indicator for evaluation of iron deficiency.
Other tests available for evaluating iron status include Zinc protoporphyrin/heme ratio and reticulocyte hemoglobin content.
Treatment
Medical Therapy
Iron supplementation is available in oral and IV forms. Oral iron is readily available, inexpensive, effective, safe, and convenient. Some of the available formulations include ferrous sulfate, ferrous fumarate, and ferrous gluconate. GI side effects are seen in up to 70% of the patients taking oral iron, leading to noncompliance with treatment. GI symptoms can be minimized by the use of chelated forms of iron. Enteric-coated tablets lead to poor absorption and should not be used.[6]
Intravenous iron is available in many forms, such as ferric carboxymaltose, ferric gluconate, ferric/iron sucrose, ferumoxytol, and low-molecular-weight iron dextran. Response to IV iron should be checked to establish the need for further supplementation six to eight weeks after initial iron replacement.[7]
There is a very low risk of allergic reactions with all IV iron formulations. Premedication with antihistamines does not prevent infusion reactions and should not be given. Patients with a history of asthma or drug allergies should receive steroids prior to infusion.
In pregnancy, oral iron is given during the first trimester as the safety of IV iron in the first trimester has not been established.
Generally, oral iron is given to pregnant women if it can be tolerated. Exceptions include women with severe anemia, women with IBD, and those who have undergone bariatric surgery. In these patients, IV iron is preferred. All IV forms have equal efficacy and safety except for some formulations of ferric gluconate which contain benzyl alcohol as a preservative. These are avoided because of the possibility of harm to the fetus.
Prevention
In developing countries, patients should be advised to consume iron rich foods and fruits and vegetables high in Vitamin C. In babies born to iron deficient mothers, delayed umbilical cord clamping can be helpful in preventing iron deficiency in newborns.[8]
In infants, iron should be supplemented after 6 months of breastfeeding. Iron fortified cereal and formula should be given. Anti helminthic drugs should be given to children with parasitic infections. In areas where prevalence of iron deficiency is high, women of reproductive age group should take daily iron supplements.
References
- ↑ Muñoz, Manuel. “Disorders of Iron Metabolism. Part II: Iron Deficiency and Iron Overload”.
- ↑ Brotanek , Gosz, Weitzman, Flores, Jane M, Jacqueline, Michael, Glenn. “Iron Deficiency in Early Childhood in the United States: Risk Factors and racial/ethnic Disparities”.
- ↑ “Obesity and Iron Deficiency: A Quantitative Meta-Analysis”.
- ↑ “Pica: Its Frequency and Significance in Patients With Iron-Deficiency Anemia Due to Chronic Gastrointestinal Blood Loss”.
- ↑ “Guidelines on the Diagnosis and Treatment of Iron Deficiency Across Indications: A Systematic Review”.
- ↑ “Current Misconceptions in Diagnosis and Management of Iron Deficiency”.
- ↑ “Guidelines on the Diagnosis and Treatment of Iron Deficiency Across Indications: A Systematic Review”.
- ↑ “Iron Deficiency Anemia: A Common and Curable Disease”.
Historical Perspective
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1] Shyam Patel [2]; Associate Editor(s)-in-Chief: Jogeet Singh Sekhon, M.D. [3]
Overview
Iron deficiency anemia was discovered in 1852 by Karl Vierordt and his student H. Welcher. Over the next century, the details of iron regulation were elucidated.
Historical Perspective
Discovery
- In 1852, Karl Vierordt and his student H. Welcher discovered iron deficiency anemia.
- In 1949, Finch and colleagues showed that reticulocytes (precursors of red blood cells) can incorporate iron from the plasma to make hemoglobin.[1]
- In 1969, Evan Morgan and colleagues showed internalization of transferrin (the carrier of iron) by cells.[1] This was one of the first demonstrations that the internalization of a membrane protein was important for iron regulation.
- In 1979, Bothwell published a monograph about early iron homeostasis. By this time, iron regulation was well understood.[1]
- In 1990, Donnall Thomas received the Nobel Prize for his discoveries about bone marrow transplantation.[1]
- Between 1990 and 2010, the prevalence of anemia worldwide decreased from 40.2% to 32.9%.[2]
- In 2000, Breton-Gorius and Bessis showed via electron micrography that there were erythroblastic islands (locations of red blood cell production) in the bone marrow, and they showed that iron (in the form of ferritin) could be transferred between the erythroblasts and surrounding cells.[1]
References
- ↑ 1.0 1.1 1.2 1.3 1.4 Sheftel AD, Mason AB, Ponka P (2012). “The long history of iron in the Universe and in health and disease”. Biochim Biophys Acta. 1820 (3): 161–87. doi:10.1016/j.bbagen.2011.08.002. PMC 3258305. PMID 21856378.
- ↑ Muñoz M, Gómez-Ramírez S, Besser M, Pavía J, Gomollón F, Liumbruno GM; et al. (2017). “Current misconceptions in diagnosis and management of iron deficiency”. Blood Transfus. 15 (5): 422–437. doi:10.2450/2017.0113-17. PMC 5589705. PMID 28880842.
Classification
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1] Shyam Patel [2]; Associate Editor(s)-in-Chief: Jogeet Singh Sekhon, M.D. [3]
Overview
There is no established system for the classification of iron deficiency anemia. However, based on the pathology it can be divided into 2 types on the basis of cause of iron deficiency into absolute iron deficiency and functional iron deficiency.
Classification
Iron deficiency anemia can be classified into[1].
- Absolute iron deficiency arising due to the lowered or exhausted level of total body iron stores.
- Functional iron deficiency wherein the total body iron stores are normal or increased, with the insufficient iron supply to the bone marrow. Functional iron deficiency is present in many acute and chronic inflammatory states. In this case, the problem lies within utilization of iron stores.
References
- ↑ Camaschella C (2015). “Iron deficiency: new insights into diagnosis and treatment”. Hematology Am Soc Hematol Educ Program. 2015: 8–13. doi:10.1182/asheducation-2015.1.8. PMID 26637694.
Pathophysiology
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1] Shyam Patel [2]
Overview
Iron is needed for haemoglobin synthesis which is essential for oxygen transport in the body. Iron is stored as ferritin in the body and transported as transferrin. The source of iron is diet and recycling iron from reticuloendothelial cells. The absorption of iron is highly regulated by hepcidin. Loss of iron from the body, inadequate intake or increased hepcidin can lead to iron deficiency anemia.
Pathophysiology
Physiology
- Iron is needed for the synthesis of haemoglobin and new DNA. It is a major component of oxidation and reduction enzymes (cytochromes)[1]
- In the human body, iron mainly exists as bound to protein (hemoprotein), as heme compounds (hemoglobin or myoglobin), heme enzymes, or nonheme compounds (flavin-iron enzymes, transferrin, and ferritin).[2]
- The body requires iron for the synthesis of its oxygen transport proteins, (hemoglobin and myoglobin), and for the formation of heme enzymes and other iron-containing enzymes involved in electron transfer and oxidation-reductions.
- Human iron metabolism is controlled by various factors.
- 60% of the body iron is found in the hemoglobin present in circulating erythrocytes, 25% is contained in transferrin and ferritin, and the remaining 15% is bound to myoglobin in muscle tissue and in a variety of enzymes involved in the oxidative metabolism and many other cell functions.[3]
- Iron is bound and transported in the body via transferrin and stored in ferritin molecules.
- Iron is delivered to tissues by circulating transferrin, a transporter that captures iron released into the plasma from intestinal enterocytes or reticuloendothelial macrophages.[4]
- The binding of transferrin to the cell-surface transferrin receptor (TfR) 1 results in endocytosis and uptake of iron.
- Internalized iron is transported to mitochondria for the synthesis of heme or other iron containing enzymes.
- Excess iron is stored in cytosolic ferritin.
Absorption of iron
- Iron absorption occurs by the enterocytes in the duodenum and upper jejunum.[5][6][7]
- Dietary iron occurs in two forms: heme and non-heme. The primary sources of heme iron are hemoglobin and myoglobin from consumption of meat, poultry, and fish, whereas non-heme iron is obtained from cereals, pulses, legumes, fruits, and vegetables.[8]
- In the blood, it is transported by transferrin to the cells or the bone marrow for erythropoiesis.[9]
- Iron absorption is controlled by ferroportin on the basolateral surface of the cell. Ferroportin allows or does not allow iron from the mucosal cell into the plasma.
- Iron is absorbed in Fe+2 (ferric) state.
- The iron is consumed in Fe+3 (ferrous) state and is reduced to Fe+2 state by the acidic gastric pH by enzyme ferric reductase.[10]
- Fe+2 is absorbed by the enterocytes and exported across the basolateral membrane into the bloodstream via Fe+2 transporter ferroportin.
- The ferroportin-mediated efflux of Fe+2 is coupled by its reoxidation to Fe+3, catalyzed by ferroxidase hephaestin that interacts with ferroportin.[11]
- The total iron content of transferrin is dynamic and undergoes changes to sustain erythropoiesis.
- Senescent RBCs are cleared by reticuloendothelial macrophages, which metabolize hemoglobin and heme and release iron into the bloodstream.
- The transferrin iron pool is replenished by iron recycled from RBCs and by newly absorbed dietary iron.
- Macrophages export Fe+2 from their plasma membrane via ferroportin, in a process coupled by reoxidation of Fe+2 to Fe+3 by ceruloplasmin and followed by the loading of Fe+3 to transferrin.
Regulation of iron homeostasis
- Iron balance is mainly regulated at the point of absorption.[12]
- Hepcidin is a circulating peptide hormone secreted by the liver that plays a central role in the regulation of iron homeostasis. Inflammatory conditions lead to increased IL-6 production, which stimulates hepcidin production.
- This hormone is produced by hepatocytes and is a negative regulator of iron entry into plasma. Hepcidin acts by binding to ferroportin.[13][14][15]
- Binding of hepcidin induces ferroportin degradation.
- The loss of ferroportin from the cell surface prevents iron entry into plasma and decreased iron levels in the body.[16]
- Decreased expression of hepcidin leads to increased cell surface ferroportin and increased iron absorption.
- Plasma hepcidin levels are regulated by cytokines, plasma iron, anemia, and hypoxia.
- Overexpression of hepcidin leads to the anemia of chronic disease, while low hepcidin production results in hereditary hemochromatosis (HFE).
Storage
- Ferritin concentration together with that of hemosiderin reflects the body iron stores.[17][18][19][20][21][21]
- They store iron in an insoluble form and are present primarily in the liver, spleen, and bone marrow.
- Serum ferritin is the most convenient laboratory test to estimate iron stores.
Factors effecting iron absorption
- Factors that enhance iron uptake are:
- Factors inhibiting iron absorption are:
- Phytate (myo-inositol hexakisphosphate) is the main inhibitor of iron absorption[24][25][26].
- Calcium
- Animal proteins such as milk proteins, egg proteins, and albumin, have been shown to inhibit iron absorption.
- Proteins from soybean also decrease iron absorption.
- Suppresion of gastric acid such as use of antacids suprress iron absorption.
- Lead competes with iron for the absorption and blocks its absorption by competetive inhibition.
Iron requirement
| Age | Male | Female | Pregnancy | Lactation |
|---|---|---|---|---|
| Birth to 6 months | 0.27 mg* | 0.27 mg* | ||
| 7–12 months | 11 mg | 11 mg | ||
| 1–3 years | 7 mg | 7 mg | ||
| 4–8 years | 10 mg | 10 mg | ||
| 9–13 years | 8 mg | 8 mg | ||
| 14–18 years | 11 mg | 15 mg | 27 mg | 10 mg |
| 19–50 years | 8 mg | 18 mg | 27 mg | 9 mg |
| 51+ years | 8 mg | 8 mg |
Pathogenesis
- Iron deficiency anemia occurs when there is[27][28]:
- Low dietary intake
- Increased demands of iron
- Impaired absorption of iron
- Excessive loss of iron (blood loss)
- Increased hepcidin (chronic inflammation)
- Low dietary intake:
- Iron is obtained from foods such as:
- meat, such as lamb, pork, chicken, and beef
- beans
- pumpkin and squash seeds
- leafy greens, such as spinach
- raisins and other dried fruit
- eggs
- seafood, such as clams, sardines, shrimp, and oysters
- Iron-fortified dry and instant cereals Foods high in vitamin C include:
- Fruits such as oranges, grapefruits, strawberries, kiwis, guavas, papayas, pineapples, melons, and mangoes
- Red and green bell peppers
- Brussels sprouts
- Cauliflower
- Tomatoes
- Leafy greens
- Increased demands of iron
- Growth, the requirement of iron increases during the developmental period from infancy to adolescence and during adolescence.
- Pregnancy, during pregnancy the demand for iron is increased.
- Impaired absorption of iron:
- Malabsorption
- Deficiency of vitamin C in diet
- Excessive loss of iron (blood loss)
- The only means of excretion for iron is through blood loss
- Any source of external and internal bleeding can cause iron deficiency depending on the blood loss
- Increased hepcidin
- In chonric inflammatory conditions, the levels of hepcidin increase
- Increased hepcidin causes ferriportin degeneration and impaired iron absorption
- Iron is obtained from foods such as:
- Iron is required for haemoglobin synthesis, so deficiency of iron leads to depletion of haemoglobin
- Decrease in haemoglobin leads to anemia
- Due to low haemoglobin, oxygen is not tranported effectively to cells and results in hypoxia
| Population | Hb Diagnostic of anaemia (g/dL) |
|---|---|
| Children aged 6 months to 6 years old | <11.0 |
| Children aged 6-14 years old | <12.0 |
| Adult men | <13.0 |
| Adult non-pregnant women | <12.0 |
| Adult pregnant women | <11.0 |
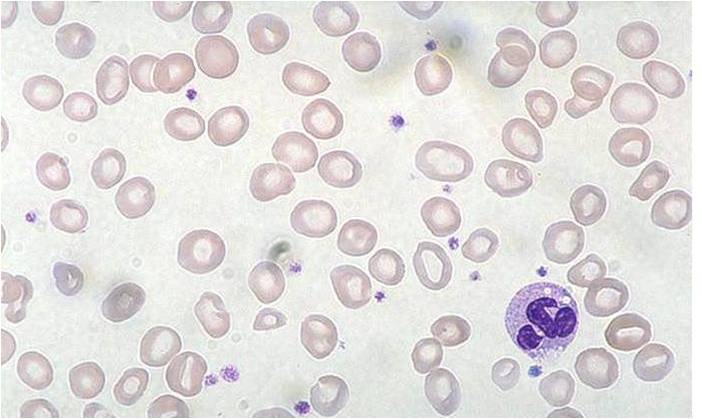
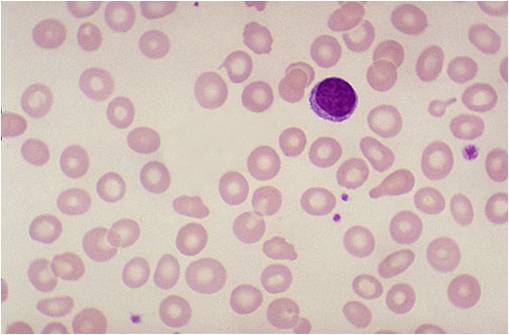
Histology
(Images shown below are courtesy of Melih Aktan MD, Istanbul Medical Faculty – Turkey)
-
 Iron deficiency anemia
Iron deficiency anemia -
 Iron deficiency anemia
Iron deficiency anemia -
 Iron deficiency anemia
Iron deficiency anemia



Video
{{#ev:youtube|7uDbu7esZik}}
External Link
Center for disease control and prevention
References
- ↑ Brissot P, Troadec MB, Loréal O, Brissot E (2018). “Pathophysiology and classification of iron overload diseases; update 2018”. Transfus Clin Biol. doi:10.1016/j.tracli.2018.08.006. PMID 30173950.
- ↑ Murray-Kolb LE (2018). “Examining Consequence of Brain Iron Deficiency in the Absence of Anemia”. J Nutr. doi:10.1093/jn/nxy186. PMID 30169646.
- ↑ Ghaffari S, Pourafkari L (2018). “Koilonychia in Iron-Deficiency Anemia”. N Engl J Med. 379 (9): e13. doi:10.1056/NEJMicm1802104. PMID 30157401.
- ↑ Kassebaum NJ, Jasrasaria R, Naghavi M, Wulf SK, Johns N, Lozano R; et al. (2014). “A systematic analysis of global anemia burden from 1990 to 2010”. Blood. 123 (5): 615–24. doi:10.1182/blood-2013-06-508325. PMC 3907750. PMID 24297872.
- ↑ Price EA, Mehra R, Holmes TH, Schrier SL (2011). “Anemia in older persons: etiology and evaluation”. Blood Cells Mol Dis. 46 (2): 159–65. doi:10.1016/j.bcmd.2010.11.004. PMID 21208814.
- ↑ Mast AE, Bialkowski W, Bryant BJ, Wright DJ, Birch R, Kiss JE; et al. (2016). “A randomized, blinded, placebo-controlled trial of education and iron supplementation for mitigation of iron deficiency in regular blood donors”. Transfusion. 56 (6 Pt 2): 1588–97. doi:10.1111/trf.13469. PMC 4905782. PMID 26813849.
- ↑ Shams S, Asheri H, Kianmehr A, Ziaee V, Koochakzadeh L, Monajemzadeh M; et al. (2010). “The prevalence of iron deficiency anaemia in female medical students in Tehran”. Singapore Med J. 51 (2): 116–9. PMID 20358149.
- ↑ Fonseca C, Marques F, Robalo Nunes A, Belo A, Brilhante D, Cortez J (2016). “Prevalence of anaemia and iron deficiency in Portugal: the EMPIRE study”. Intern Med J. 46 (4): 470–8. doi:10.1111/imj.13020. PMID 26841337.
- ↑ Cook JD, Skikne BS (1989). “Iron deficiency: definition and diagnosis”. J Intern Med. 226 (5): 349–55. PMID 2681511.
- ↑ Annibale B, Capurso G, Chistolini A, D’Ambra G, DiGiulio E, Monarca B; et al. (2001). “Gastrointestinal causes of refractory iron deficiency anemia in patients without gastrointestinal symptoms”. Am J Med. 111 (6): 439–45. PMID 11690568.
- ↑ Lopez A, Cacoub P, Macdougall IC, Peyrin-Biroulet L (2016). “Iron deficiency anaemia”. Lancet. 387 (10021): 907–16. doi:10.1016/S0140-6736(15)60865-0. PMID 26314490.
- ↑ Khadem G, Scott IA, Klein K (2012). “Evaluation of iron deficiency anaemia in tertiary hospital settings: room for improvement?”. Intern Med J. 42 (6): 658–64. doi:10.1111/j.1445-5994.2012.02724.x. PMID 22288902.
- ↑ Ioannou GN, Rockey DC, Bryson CL, Weiss NS (2002). “Iron deficiency and gastrointestinal malignancy: a population-based cohort study”. Am J Med. 113 (4): 276–80. PMID 12361812. Review in: ACP J Club. 2003 May-Jun;138(3):80
- ↑ Unsworth DJ, Lock FJ, Harvey RF (1999). “Iron-deficiency anaemia in premenopausal women”. Lancet. 353 (9158): 1100. PMID 10199377.
- ↑ Corazza GR, Valentini RA, Andreani ML, D’Anchino M, Leva MT, Ginaldi L; et al. (1995). “Subclinical coeliac disease is a frequent cause of iron-deficiency anaemia”. Scand J Gastroenterol. 30 (2): 153–6. PMID 7732338.
- ↑ Unsworth DJ, Lock RJ, Harvey RF (2000). “Improving the diagnosis of coeliac disease in anaemic women”. Br J Haematol. 111 (3): 898–901. PMID 11122153.
- ↑ Camaschella C (2015). “Iron deficiency: new insights into diagnosis and treatment”. Hematology Am Soc Hematol Educ Program. 2015: 8–13. doi:10.1182/asheducation-2015.1.8. PMID 26637694.
- ↑ Hershko C, Hoffbrand AV, Keret D, Souroujon M, Maschler I, Monselise Y; et al. (2005). “Role of autoimmune gastritis, Helicobacter pylori and celiac disease in refractory or unexplained iron deficiency anemia”. Haematologica. 90 (5): 585–95. PMID 15921373.
- ↑ Kalantar-Zadeh K, Höffken B, Wünsch H, Fink H, Kleiner M, Luft FC (1995). “Diagnosis of iron deficiency anemia in renal failure patients during the post-erythropoietin era”. Am J Kidney Dis. 26 (2): 292–9. PMID 7645533.
- ↑ Eschbach JW, Cook JD, Scribner BH, Finch CA (1977). “Iron balance in hemodialysis patients”. Ann Intern Med. 87 (6): 710–3. PMID 931207.
- ↑ 21.0 21.1 Hershko C, Camaschella C (2014). “How I treat unexplained refractory iron deficiency anemia”. Blood. 123 (3): 326–33. doi:10.1182/blood-2013-10-512624. PMID 24215034.
- ↑ Iolascon A, d’Apolito M, Servedio V, Cimmino F, Piga A, Camaschella C (2006). “Microcytic anemia and hepatic iron overload in a child with compound heterozygous mutations in DMT1 (SCL11A2)”. Blood. 107 (1): 349–54. doi:10.1182/blood-2005-06-2477. PMID 16160008.
- ↑ Coates A, Mountjoy M, Burr J (2017). “Incidence of Iron Deficiency and Iron Deficient Anemia in Elite Runners and Triathletes”. Clin J Sport Med. 27 (5): 493–498. doi:10.1097/JSM.0000000000000390. PMID 27606953.
- ↑ Thomas DW, Hinchliffe RF, Briggs C, Macdougall IC, Littlewood T, Cavill I; et al. (2013). “Guideline for the laboratory diagnosis of functional iron deficiency”. Br J Haematol. 161 (5): 639–48. doi:10.1111/bjh.12311. PMID 23573815.
- ↑ Simpson E, Mull JD, Longley E, East J (2000). “Pica during pregnancy in low-income women born in Mexico”. West J Med. 173 (1): 20–4, discussion 25. PMC 1070964. PMID 10903283.
- ↑ Rector WG (1989). “Pica: its frequency and significance in patients with iron-deficiency anemia due to chronic gastrointestinal blood loss”. J Gen Intern Med. 4 (6): 512–3. PMID 2585159.
- ↑ Reynolds RD, Binder HJ, Miller MB, Chang WW, Horan S (1968). “Pagophagia and iron deficiency anemia”. Ann Intern Med. 69 (3): 435–40. PMID 5244572.
- ↑ Trost LB, Bergfeld WF, Calogeras E (2006). “The diagnosis and treatment of iron deficiency and its potential relationship to hair loss”. J Am Acad Dermatol. 54 (5): 824–44. doi:10.1016/j.jaad.2005.11.1104. PMID 16635664.
Causes
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief:
Please help WikiDoc by adding content here. It’s easy! Click here to learn about editing.
Overview
Iron deficiency anemia causes can be broadly divided into physiological causes as that seen during growth and pregnancy and due to pathological process. The pathological process could be further divided based on blood loss and inadequate iron absorption.
Causes
Life threatening causes
- Severe blood loss such as traumatic haemorrhage, haemetemesis, haemoptysis or uncontrolled bleeding from any body part can result in death from hypovolemic shock[1][2][3][4]
[5][6][7][8][9][10][11][12][13] .
Most common causes
- Growth
- Pregnancy
- Malnutrition
- Malabsorption
- Blood loss
- Chronic Kidney disease
- Anemia of chronic disease
- Myeloproliferative disorders
Less common causes
- Erythrpoetin/eryhtropoetin stimulating drugs
- Leflunomide
- Pramipexole
- Trientine
Genetic cause
- IRIDA- iron referactory iron deficiency anemia due to TMPRSS6 mutation
- SLC11A-2 mutation
- Iron-refractory iron deficiency anaemia •
- Divalent metal transporter deficiency anaemia, •
- Fanconianaemia
- Pyruvate kinase deficiency
Pathological
Blood Loss
- Menstruation
- Gastrointestinal tract (Bleeding from the gastrointestinal tract (ulcers, hemorrhoids, Esophageal varices, The use of aspirin, ibuprofen, or arthritis medicines for a long time, Cancer in the esophagus, stomach, or colon)
- Food sensitivity
- Hookworms
- Genitourinary tract
- Respiratory tract (Rarely laryngological bleeding or from the respiratory tract)
- Blood donation
Inadequate Iron Absorption
- Dietary deficiency
- Impaired absorption (Celiac disease, Crohn’s disease)
- Intestinal malabsorption
- Gastric surgery
- Hypochorhydria
- Taking too many antacids that contain calcium
Causes by Organ System
| Cardiovascular | No underlying causes | ||||||||||||||||||
| Chemical/Poisoning | No underlying causes | ||||||||||||||||||
| Dental | Gum bleeding | ||||||||||||||||||
| Dermatologic | No underlying causes | ||||||||||||||||||
| Drug Side Effect | Leflunomide, Pramipexole, trientine, antacids | ||||||||||||||||||
| Ear Nose Throat | Epistaxis | ||||||||||||||||||
| Endocrine | Erythropoetin deficiency | ||||||||||||||||||
| Environmental | No underlying causes | ||||||||||||||||||
| Gastroenterologic | Haemetemesis, Celiac disease, bariatric surgery, Gatsritis, esophageal varices, Tropical sprue, Whipple’s disease, Small intestinal bacterial overgrowth syndrome, Giardia, Malabsorption
| ||||||||||||||||||
| Genetic | SLC11A2 mutation, IRIDA | ||||||||||||||||||
| Hematologic | Myeloproliferative disorder | ||||||||||||||||||
| Iatrogenic | Erythrpoetin administartion | ||||||||||||||||||
| Infectious Disease | H.pylori, Giardia, Hookworms, Entamoeba histolytica | ||||||||||||||||||
| Musculoskeletal/Orthopedic | No underlying causes | ||||||||||||||||||
| Neurologic | No underlying causes | ||||||||||||||||||
| Nutritional/Metabolic | No underlying causes | ||||||||||||||||||
| Obstetric/Gynecologic | Mennorhagia, Fibroids, Post partum bleeding, Pregnancy, Endometriosis | ||||||||||||||||||
| Oncologic | Colon cancer, esophageal cancer, gastric cancer, pancreatic cancer, lung cancer | ||||||||||||||||||
| Ophthalmologic | No underlying causes | ||||||||||||||||||
| Overdose/Toxicity | No underlying causes | ||||||||||||||||||
| Psychiatric | No underlying causes | ||||||||||||||||||
| Pulmonary | Haemoptysis | ||||||||||||||||||
| Renal/Electrolyte | Chronic kidney disease, haemodialysis | ||||||||||||||||||
| Rheumatology/Immunology/Allergy | Anemia of chronic disease | ||||||||||||||||||
| Sexual | No underlying causes | ||||||||||||||||||
| Trauma | Bleeding | ||||||||||||||||||
| Urologic | Haematuria | ||||||||||||||||||
| Miscellaneous | Decreased iron intake, increased body requirements | ||||||||||||||||||
Causes in alphabetical order
- Anemia of chronic disease
- Antacids
- Bariatric surgery
- Blood donation
- Blood loss
- Carcinoid syndrome
- Celiac disease
- Chronic kidney disease
- Crohn’s disease
- Colon cancer
- Decreased iron intake
- Diverticulosis
- Endometriosis
- Entamoeba histolytica
- Epistaxis
- Erythropoetin deficiency
- Esophageal cancer
- Esophageal varices
- Fibroids
- Gastritis
- GI fistula
- Gastric cancer
- Giardia
- H. Pylori
- Hookworm
- Haemoptysis
- Haemetemesis
- Haematuria
- Haemorrhoids
- Myeloproliferative disorders
- Malnutrition
- Malabsorption
- Peptic ulcer disease
- Pregnancy
- Post partum bleeding
- Pancreatic cancer
- Stricture
- Tropical sprue
- Ulcerative colitis
- Whipple disease
- Zollinger Ellison syndrome
Center for disease control and prevention
References
- ↑ “Recommendations to Prevent and Control Iron Deficiency in the United States”. Retrieved 2012-09-18.
- ↑ Price EA, Mehra R, Holmes TH, Schrier SL (2011). “Anemia in older persons: etiology and evaluation”. Blood Cells Mol Dis. 46 (2): 159–65. doi:10.1016/j.bcmd.2010.11.004. PMID 21208814.
- ↑ Mast AE, Bialkowski W, Bryant BJ, Wright DJ, Birch R, Kiss JE; et al. (2016). “A randomized, blinded, placebo-controlled trial of education and iron supplementation for mitigation of iron deficiency in regular blood donors”. Transfusion. 56 (6 Pt 2): 1588–97. doi:10.1111/trf.13469. PMC 4905782. PMID 26813849.
- ↑ Cook JD, Skikne BS (1989). “Iron deficiency: definition and diagnosis”. J Intern Med. 226 (5): 349–55. PMID 2681511.
- ↑ Annibale B, Capurso G, Chistolini A, D’Ambra G, DiGiulio E, Monarca B; et al. (2001). “Gastrointestinal causes of refractory iron deficiency anemia in patients without gastrointestinal symptoms”. Am J Med. 111 (6): 439–45. PMID 11690568.
- ↑ Lopez A, Cacoub P, Macdougall IC, Peyrin-Biroulet L (2016). “Iron deficiency anaemia”. Lancet. 387 (10021): 907–16. doi:10.1016/S0140-6736(15)60865-0. PMID 26314490.
- ↑ Khadem G, Scott IA, Klein K (2012). “Evaluation of iron deficiency anaemia in tertiary hospital settings: room for improvement?”. Intern Med J. 42 (6): 658–64. doi:10.1111/j.1445-5994.2012.02724.x. PMID 22288902.
- ↑ Ioannou GN, Rockey DC, Bryson CL, Weiss NS (2002). “Iron deficiency and gastrointestinal malignancy: a population-based cohort study”. Am J Med. 113 (4): 276–80. PMID 12361812. Review in: ACP J Club. 2003 May-Jun;138(3):80
- ↑ Camaschella C (2015). “Iron deficiency: new insights into diagnosis and treatment”. Hematology Am Soc Hematol Educ Program. 2015: 8–13. doi:10.1182/asheducation-2015.1.8. PMID 26637694.
- ↑ Corazza GR, Valentini RA, Andreani ML, D’Anchino M, Leva MT, Ginaldi L; et al. (1995). “Subclinical coeliac disease is a frequent cause of iron-deficiency anaemia”. Scand J Gastroenterol. 30 (2): 153–6. PMID 7732338.
- ↑ Unsworth DJ, Lock RJ, Harvey RF (2000). “Improving the diagnosis of coeliac disease in anaemic women”. Br J Haematol. 111 (3): 898–901. PMID 11122153.
- ↑ Hershko C, Hoffbrand AV, Keret D, Souroujon M, Maschler I, Monselise Y; et al. (2005). “Role of autoimmune gastritis, Helicobacter pylori and celiac disease in refractory or unexplained iron deficiency anemia”. Haematologica. 90 (5): 585–95. PMID 15921373.
- ↑ Eschbach JW, Cook JD, Scribner BH, Finch CA (1977). “Iron balance in hemodialysis patients”. Ann Intern Med. 87 (6): 710–3. PMID 931207.
Differentiating Iron Deficiency Anemia from other Diseases
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-In-Chief: Associate Editor(s)-in-Chief: Sargun Singh Walia M.B.B.S.[2],Vamsikrishna Gunnam M.B.B.S [3]
Please help WikiDoc by adding content here. It’s easy! Click here to learn about editing.
Overview
Iron deficiency anemia and Thalassemia Minor present with many of the same lab results. It is very important not to treat a patient with Thalassemia with an iron supplement as this can lead to hemochromatosis (accumulation of iron in the liver) A hemoglobin electrophoresis would provide useful evidence in distinguishing these two conditions, along with iron studies.
Differential Diagnosis
| Disease | Genetics | Clinical manifestation | Lab findings | |||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| History | Symptoms | Signs | Hemolysis | Intrinsic/
Extrinsic |
Hb concentration | MCV | RDW | Reticulocytosis | Haptoglobin levels | Hepcidin | Iron studies | Specific finding on blood smear | ||||||
| Serum iron | Serum Tfr level | Transferrin or TIBC | Ferritin | Transferrin saturation | ||||||||||||||
| Iron deficiency anemia[1] | − |
|
− | − | Hypochromic | Microcytic | ↑ | Nl or ↓ | Nl | Nl | ↓ | ↑ | ↑ | ↓ | ↓↓↓ |
| ||
| Iron deficiency anemia (early phase)[2] | − |
|
− | − | Normochromic | Normocytic | ↑ | ↓ | Nl | Nl | ↓ | ↑ | ↑ | ↓ | ↓ |
| ||
| Lead poisoning[3] | − |
|
|
|
− | − | Hypochromic | Microcytic | Nl | Nl or ↓ | Nl | Nl | Nl to ↓ | Nl | Nl | Nl to ↓ | − | |
| Sideroblastic anemia[4] |
|
|
|
|
− | − | Hypochromic | Microcytic | Nl | Nl or ↓ | Nl | Nl | ↑ | Nl | Nl to ↓ | ↑ | − |
|
| Disease | Genetics | History | Symptoms | Signs | Hemolysis | Intrinsic/
Extrinsic |
Hb concentration | MCV | RDW | Reticulocytosis | Haptoglobin levels | Hepcidin | Serum iron | Serum Tfr level | IBC | Ferritin | Transferrin saturation | Specific finding on blood smear |
| Anemia of chronic disease[5] | − | − | − | − | Hypochromic | Microcytic | Nl | Nl or ↓ | Nl | ↑ | ↓ | Nl | ↓ | ↑ | − | NA | ||
| Thalassemia[6] | α-thalassemia
|
|
α-thalassemia
|
− | − | Hypochromic | Microcytic | Nl |
|
Nl | Nl | Nl to ↑ | Nl | Nl | ↑ | Nl to ↑ |
| |
| G6PD deficiency[7] |
|
+ | Intrinsic | Normochromic | Normocytic | ↑ | ↑ but usually causes resolution within 4-7 days | ↓ | ↓ | Nl to ↑ | Nl | ↑ | ↑ | ↑ |
| |||
| Pyruvate kinase deficiency[8] |
|
|
|
+ | Intrinsic | Normochromic | Normocytic | ↑ | ↑ | ↓ | Nl | ↑ | Nl | Nl | ↑ | − |
| |
| Disease | Genetics | History | Symptoms | Signs | Hemolysis | Intrinsic/
Extrinsic |
Hb concentration | MCV | RDW | Reticulocytosis | Haptoglobin levels | Hepcidin | Serum iron | Serum Tfr level | IBC | Ferritin | Transferrin saturation | Specific finding on blood smear |
| Sickle cell anemia[9] |
|
|
+ | Intrinsic | Normochromic | Normocytic | ↑ | ↑ | ↓ | Nl or moderately ↑ | Nl | Nl | Nl or moderately ↑ | ↓ | Nl |
| ||
| HbC disease[10] |
|
|
+ | Intrinsic | Normochromic | Normocytic | ↑ | ↑ | ↓ | Nl | Nl | Nl | Nl | ↓ | − |
| ||
| Paroxysmal nocturnal hemoglobinuria[11][12] |
|
|
|
|
+ | Intrinsic | Normochromic | Normocytic | ↑ | ↑ | ↓ | Nl | ↓ | Nl | ↑ | ↓ | − | NA |
| Hereditary spherocytosis[13] |
|
|
+ | Intrinsic | Normochromic | Normocytic | ↑ | ↑ | ↓ | Nl | ↓ | Nl | ↑ | Nl | − |
| ||
| Disease | Genetics | History | Symptoms | Signs | Hemolysis | Intrinsic/
Extrinsic |
Hb concentration | MCV | RDW | Reticulocytosis | Haptoglobin levels | Hepcidin | Serum iron | Serum Tfr level | IBC | Ferritin | Transferrin saturation | Specific finding on blood smear |
| Microangiopathic hemolytic anemia[14][15] | − | Associated with |
|
+ | Extrinsic | Normochromic | Normocytic | ↑ | ↑ | ↓ | Nl | ↓ | Nl | − | ↑ | − |
| |
| Macroangiopathic hemolytic anemia[16] | Associated with | + | Extrinsic | Normochromic | Normocytic | ↑ | ↑ | ↓ | Nl | ↓ | Nl | − | − | − | ||||
| Autoimmune hemolytic anemia[17] | − | Associated with: |
|
|
+ | Extrinsic | Normochromic | Normocytic | ↑ | ↑ | ↓ | Nl | ↓ | Nl | − | − | − |
|
| Aplastic anemia[18] |
|
|
|
− | − | Normochromic | Normocytic | ↑ | ↓ | Nl | Nl | ↓ | ↓ | Nl | ↑ | ↓ |
| |
| Disease | Genetics | History | Symptoms | Signs | Hemolysis | Intrinsic/
Extrinsic |
Hb concentration | MCV | RDW | Reticulocytosis | Haptoglobin levels | Hepcidin | Serum iron | Serum Tfr level | IBC | Ferritin | Transferrin saturation | Specific finding on blood smear |
| Folate deficiency[19] |
|
|
|
|
− | − | Anisochromic | Macrocytic | ↑ | ↓ | Nl | Nl | ↑ | ↑ | ↓ | ↑ | ↑ |
|
| Vitamin B12 deficiency[20] |
|
|
|
− | − | Anisochromic | Macrocytic | ↑ | ↓ | Nl | Nl | ↑ | ↑ | ↓ | ↑ | ↑ | ||
| Orotic aciduria[21] |
|
|
|
|
− | − | Anisochromic | Macrocytic | ↑ | ↓ | Nl | Nl | ↑ | ↑ | ↓ | ↑ | ↑ | NA |
| Fanconi anemia[22] |
|
|
|
− | − | Anisochromic | Macrocytic | ↑ | ↓ | Nl | Nl | ↑ | ↑ | ↓ | ↑ | ↑ | ||
| Disease | Genetics | History | Symptoms | Signs | Hemolysis | Intrinsic/
Extrinsic |
Hb concentration | MCV | RDW | Reticulocytosis | Haptoglobin levels | Hepcidin | Serum iron | Serum Tfr level | IBC | Ferritin | Transferrin saturation | Specific finding on blood smear |
| Diamond-Blackfan anemia[23] | Mutations in:
|
|
|
|
− | − | Anisochromic | Macrocytic | Nl | ↓ | Nl | Nl | ↑ | ↑ | ↓ | ↑ | ↑ | NA |
| Infections[24] | − | Associated with | + | Extrinsic | Normochromic | Normocytic | ↑ | ↑ | ↓ | Nl | Nl | Nl | − | − | − |
| ||
| Chronic kidney disease[25] | − | − | − | Normochromic | Normocytic | ↑ | Nl/↑ | Nl | ↑ | ↓ | − | ↓ | ↑ | ↓ | Nl | |||
| Liver disease[26] | − |
|
|
− | − | Anisochromic | Macrocytic | ↑ | ↑ | Nl | Nl | ↑ | ↑ | ↓ | ↑ | ↑ | ||
| Alcoholism[27] | − |
|
− | − | Anisochromic | Macrocytic | ↑ | ↑ | Nl | Nl | ↑ | ↑ | ↓ | ↑ | ↑ | |||
| Disease | Genetics | History | Symptoms | Signs | Hemolysis | Intrinsic/
Extrinsic |
Hb concentration | MCV | RDW | Reticulocytosis | Haptoglobin levels | Hepcidin | Serum iron | Serum Tfr level | IBC | Ferritin | Transferrin saturation | Specific finding on blood smear |
References
- ↑ Camaschella C (May 2015). “Iron-deficiency anemia”. N. Engl. J. Med. 372 (19): 1832–43. doi:10.1056/NEJMra1401038. PMID 25946282.
- ↑ De Andrade Cairo RC, Rodrigues Silva L, Carneiro Bustani N, Ferreira Marques CD (June 2014). “Iron deficiency anemia in adolescents; a literature review”. Nutr Hosp. 29 (6): 1240–9. doi:10.3305/nh.2014.29.6.7245. PMID 24972460.
- ↑ Bain BJ (December 2014). “Lead poisoning”. Am. J. Hematol. 89 (12): 1141. doi:10.1002/ajh.23852. PMID 25220013.
- ↑ Bottomley SS, Fleming MD (August 2014). “Sideroblastic anemia: diagnosis and management”. Hematol. Oncol. Clin. North Am. 28 (4): 653–70, v. doi:10.1016/j.hoc.2014.04.008. PMID 25064706.
- ↑ Roy CN (2010). “Anemia of inflammation”. Hematology Am Soc Hematol Educ Program. 2010: 276–80. doi:10.1182/asheducation-2010.1.276. PMID 21239806.
- ↑ Zainal NZ, Alauddin H, Ahmad S, Hussin NH (December 2014). “α-Thalassemia with Haemoglobin Adana mutation: prenatal diagnosis”. Malays J Pathol. 36 (3): 207–11. PMID 25500521.
- ↑ Luzzatto L, Seneca E (February 2014). “G6PD deficiency: a classic example of pharmacogenetics with on-going clinical implications”. Br. J. Haematol. 164 (4): 469–80. doi:10.1111/bjh.12665. PMC 4153881. PMID 24372186.
- ↑ Grace RF, Zanella A, Neufeld EJ, Morton DH, Eber S, Yaish H, Glader B (September 2015). “Erythrocyte pyruvate kinase deficiency: 2015 status report”. Am. J. Hematol. 90 (9): 825–30. doi:10.1002/ajh.24088. PMC 5053227. PMID 26087744.
- ↑ Singh PC, Ballas SK (March 2015). “Emerging drugs for sickle cell anemia”. Expert Opin Emerg Drugs. 20 (1): 47–61. doi:10.1517/14728214.2015.985587. PMID 25431087.
- ↑ Lemonne N, Billaud M, Waltz X, Romana M, Hierso R, Etienne-Julan M, Connes P (2016). “Rheology of red blood cells in patients with HbC disease”. Clin. Hemorheol. Microcirc. 61 (4): 571–7. doi:10.3233/CH-141906. PMID 25335812.
- ↑ Bunyaratvej A, Butthep P (January 1992). “Cytometric analysis of paroxysmal nocturnal hemoglobinuria erythrocytes”. J Med Assoc Thai. 75 Suppl 1: 237–42. PMID 1402472.
- ↑ Kahng J, Kim Y, Kim JO, Koh K, Lee JW, Han K (January 2015). “A novel marker for screening paroxysmal nocturnal hemoglobinuria using routine complete blood count and cell population data”. Ann Lab Med. 35 (1): 35–40. doi:10.3343/alm.2015.35.1.35. PMC 4272963. PMID 25553278.
- ↑ Da Costa L, Galimand J, Fenneteau O, Mohandas N (July 2013). “Hereditary spherocytosis, elliptocytosis, and other red cell membrane disorders”. Blood Rev. 27 (4): 167–78. doi:10.1016/j.blre.2013.04.003. PMID 23664421.
- ↑ Morishita E (July 2015). “[Diagnosis and treatment of microangiopathic hemolytic anemia]”. Rinsho Ketsueki (in Japanese). 56 (7): 795–806. doi:10.11406/rinketsu.56.795. PMID 26251142.
- ↑ George JN, Charania RS (March 2013). “Evaluation of patients with microangiopathic hemolytic anemia and thrombocytopenia”. Semin. Thromb. Hemost. 39 (2): 153–60. doi:10.1055/s-0032-1333538. PMID 23390027.
- ↑ Westphal RG, Azen EA (May 1971). “Macroangiopathic hemolytic anemia due to congenital cardiovascular anomalies”. JAMA. 216 (9): 1477–8. PMID 5108522.
- ↑ Hill QA (October 2015). “Autoimmune hemolytic anemia”. Hematology. 20 (9): 553–4. doi:10.1179/1024533215Z.000000000401. PMID 26447931.
- ↑ Dolberg OJ, Levy Y (2014). “Idiopathic aplastic anemia: diagnosis and classification”. Autoimmun Rev. 13 (4–5): 569–73. doi:10.1016/j.autrev.2014.01.014. PMID 24424170.
- ↑ Koike H, Takahashi M, Ohyama K, Hashimoto R, Kawagashira Y, Iijima M, Katsuno M, Doi H, Tanaka F, Sobue G (March 2015). “Clinicopathologic features of folate-deficiency neuropathy”. Neurology. 84 (10): 1026–33. doi:10.1212/WNL.0000000000001343. PMID 25663227.
- ↑ Hunt A, Harrington D, Robinson S (September 2014). “Vitamin B12 deficiency”. BMJ. 349: g5226. PMID 25189324.
- ↑ Grohmann K, Lauffer H, Lauenstein P, Hoffmann GF, Seidlitz G (April 2015). “Hereditary orotic aciduria with epilepsy and without megaloblastic anemia”. Neuropediatrics. 46 (2): 123–5. doi:10.1055/s-0035-1547341. PMID 25757096.
- ↑ Alter BP (2014). “Fanconi anemia and the development of leukemia”. Best Pract Res Clin Haematol. 27 (3–4): 214–21. doi:10.1016/j.beha.2014.10.002. PMC 4254647. PMID 25455269.
- ↑ Vlachos A, Blanc L, Lipton JM (June 2014). “Diamond Blackfan anemia: a model for the translational approach to understanding human disease”. Expert Rev Hematol. 7 (3): 359–72. doi:10.1586/17474086.2014.897923. PMID 24665981.
- ↑ Bustinduy AL, Parraga IM, Thomas CL, Mungai PL, Mutuku F, Muchiri EM, Kitron U, King CH (March 2013). “Impact of polyparasitic infections on anemia and undernutrition among Kenyan children living in a Schistosoma haematobium-endemic area”. Am. J. Trop. Med. Hyg. 88 (3): 433–40. doi:10.4269/ajtmh.12-0552. PMC 3592521. PMID 23324217.
- ↑ Drawz P, Rahman M (June 2015). “Chronic kidney disease”. Ann. Intern. Med. 162 (11): ITC1–16. doi:10.7326/AITC201506020. PMID 26030647.
- ↑ Marks PW (July 2013). “Hematologic manifestations of liver disease”. Semin. Hematol. 50 (3): 216–21. doi:10.1053/j.seminhematol.2013.06.003. PMID 23953338.
- ↑ Yokoyama A, Yokoyama T, Brooks PJ, Mizukami T, Matsui T, Kimura M, Matsushita S, Higuchi S, Maruyama K (May 2014). “Macrocytosis, macrocytic anemia, and genetic polymorphisms of alcohol dehydrogenase-1B and aldehyde dehydrogenase-2 in Japanese alcoholic men”. Alcohol. Clin. Exp. Res. 38 (5): 1237–46. doi:10.1111/acer.12372. PMID 24588059.
Epidemiology and Demographics
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Jogeet Singh Sekhon, M.D. [2]
Overview
Iron deficiency anemia can occur in any age group, region, gender but there are some factors that predispose individuals of some groups to develop iron deficiency.
Epidemiology and Demographics
Incidence
- The incidence/prevalence of iron deficicency anemia is approximately 720-1360 per 100,000 individuals worldwide.[1]
Age
- Patients of all age groups may develop iron deficiency anemia[2][3][4][5].
- Older individuals are more commonly affected.
- Children aged 6 months to 24 months are also at risk.
Race
- African Americans have more risk of developing iron deficiency anemia.
Gender
- Iron deficiency anemia develops more commonly in females than males.
Region
- Iron deficiency anemia is more common in regions where meat is consumed in small quantities.
Developed Countries
Developing Countries
External Link
Center for disease control and prevention
References
- ↑ “Recommendations to Prevent and Control Iron Deficiency in the United States”. Retrieved 2012-09-18.
- ↑ Camaschella C (2015). “Iron-deficiency anemia”. N Engl J Med. 372 (19): 1832–43. doi:10.1056/NEJMra1401038. PMID 25946282.
- ↑ Lopez A, Cacoub P, Macdougall IC, Peyrin-Biroulet L (2016). “Iron deficiency anaemia”. Lancet. 387 (10021): 907–16. doi:10.1016/S0140-6736(15)60865-0. PMID 26314490.
- ↑ Khadem G, Scott IA, Klein K (2012). “Evaluation of iron deficiency anaemia in tertiary hospital settings: room for improvement?”. Intern Med J. 42 (6): 658–64. doi:10.1111/j.1445-5994.2012.02724.x. PMID 22288902.
- ↑ Camaschella C (2015). “Iron deficiency: new insights into diagnosis and treatment”. Hematology Am Soc Hematol Educ Program. 2015: 8–13. doi:10.1182/asheducation-2015.1.8. PMID 26637694.
Risk Factors
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Jogeet Singh Sekhon, M.D. [2]
Overview
Risk of iron deficiency anemia is more in those individuals who consume less iron in diet and who are at increased risk of bleeding.
Risk Factors
- Women of childbearing age.
- Pregnant women.
- People with poor diets.
- People who donate blood frequently.
- Infants and children, especially those born prematurely or experiencing a growth spurt.
- Vegetarians who don’t replace meat with another iron-rich food.
- Infants who drink cow’s milk rather than breast milk or iron-fortified formula.
References
- ↑ Camaschella C (2015). “Iron deficiency: new insights into diagnosis and treatment”. Hematology Am Soc Hematol Educ Program. 2015: 8–13. doi:10.1182/asheducation-2015.1.8. PMID 26637694.
- ↑ Lopez A, Cacoub P, Macdougall IC, Peyrin-Biroulet L (2016). “Iron deficiency anaemia”. Lancet. 387 (10021): 907–16. doi:10.1016/S0140-6736(15)60865-0. PMID 26314490.
Screening
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Jogeet Singh Sekhon, M.D. [2]
Please help WikiDoc by adding content here. It’s easy! Click here to learn about editing.
Overview
Screening is recommended in pregnant women and new borns.
Screening
- CBC is the initial test.
- If microcytic hypochromic anemia is seen, then iron studies are done.
References
- ↑ Lopez A, Cacoub P, Macdougall IC, Peyrin-Biroulet L (2016). “Iron deficiency anaemia”. Lancet. 387 (10021): 907–16. doi:10.1016/S0140-6736(15)60865-0. PMID 26314490.
- ↑ Cook JD, Skikne BS (1989). “Iron deficiency: definition and diagnosis”. J Intern Med. 226 (5): 349–55. PMID 2681511.
Natural History, Complications and Prognosis
- Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Jogeet Singh Sekhon, M.D. [2]
Please help WikiDoc by adding content here. It’s easy! Click here to learn about editing.
Overview
The symptoms of iron deficiency are similar as in any other case of anemia. Iron deficiency anemia has age specific presentations. Iron deficiency anemia can lead to severe complications if not treated. The prognosis of iron deficiency anemia is good if iron supplementation is started.
Natural History
- .The stage of anemia develops when there is chronic deficiency of iron and all the iron stores of body are used up.
- Initially in iron defiicency, no symptoms develop as body has sufficient store of iron in the form of ferritin.
- Normal ferittin levels are 20 to 300 ng/mL. This level denotes suffiicient iron levels in the body.
- Ferittin levels between 20-40 ng/ml denotes iron deficiency without anemia.
- Ferittin levels <20 ng/ml denotes iron deficency with anemia and signs and symptoms of anemia develop at this stage.
- Iron deficiency anemia has age specific presentations:
- Infants (age 0-12 months) and Preschool Children (age 1-5 years)
- Iron-deficiency anemia is defined as a Hb concentration of less than or equal to 10.0 g/dL .
- Developmental delays.
- Behavioral disturbances (e.g., decreased motor activity, social interaction, and attention to tasks)
- Iron-deficiency anemia also contributes to lead poisoning in children by increasing the gastrointestinal tract’s ability to absorb heavy metals, including lead.
- Psychiatric illnesses such as unipolar disorder, bipolar disorder and autism spectrum disorder in adolescense.
- Adults (persons aged greater than or equal to 18 years)
- Decreased functional capacity
- Signs of hypoxia due to low oxygen delivery to the tissues.
- Pregnant Female
- Increased chances of pre term labor
- Low birth weight baby
- Infants (age 0-12 months) and Preschool Children (age 1-5 years)
Complications
- Iron deficiency anemia can lead to severe complications if not treated[8][9][10][11][12][13][14][15].
- Severe iron deficiency (ferittin <10 ng/mL (<10 mcg/L; <22.5 picoM/L) can lead to severe complications.
- Exercise:
- Fatigue
- Low stamina
- Muscle atrophy
- Decreased aerobic capacity
- Decreased endurance ability
- Heart
- Irregular heart beat
- Cardiac failure
- Dilated cardiomyopathy
- Systolic flow murmur
- Myocardial ischemia
- Angina pectoris
- Haemodynamic instability
- Lungs
- Development delay in children
- Mental retardation
- Behavioral differences
- Psychiatric illness
- Shortened attention span
- Neurocognitive delay
- Pregnancy
- Preterm labor
- Low birth weight baby
- Postpartum depression
- Restless leg syndrome
- Atrophic glossitis
- Alopecia
- Immune system weakness
- Syncope
- Plummer Vinson syndrome
Prognosis
- The prognosis of iron deficiency anemia is good if iron supplementation is started.
- Serum iron levels improve within 2 months of starting treatment.
- Severe iron defiicency is present when ferritin <10 ng/mL and Hb <7mg/dl. At this stage severe complications may start developing.
- The severity of iron deficiency anemia depends on:
- Level of severity.
- Age of onset.
- Presence of chronic disease.
- Speed of onset.
- Cause of iron deficiency.
- In cases like chronic diseases, restoring iron stores will not treat the anemia unless the disease is treated as cause of anemia is not decreased iron deficiency but iron trapped in its storage form.
- Reversible causes like bleeding can be managed with blood transfusion and have a good prognosis if blood can be restored in sufficient time .
- Iron supplementation improves learning, memory, and cognitive test performance in adolescents who have low levels of iron. Iron supplementation also improves the performance of athletes with anemia and iron deficiency.
Finding the cause of iron deficiency
The gastrointestinal tract may be the cause, even in the absence of signs of gastrointestinal bleeding[16]. The prevalence of gastrointestinal lesions among asymptomatic patients with iron deficiency were[16]:
- Occult blood positive: 67%
- Occult blood negative: 41%
Gastrointestinal evaluation is underused[17][18][19].
References
- ↑ Price EA, Mehra R, Holmes TH, Schrier SL (2011). “Anemia in older persons: etiology and evaluation”. Blood Cells Mol Dis. 46 (2): 159–65. doi:10.1016/j.bcmd.2010.11.004. PMID 21208814.
- ↑ Mast AE, Bialkowski W, Bryant BJ, Wright DJ, Birch R, Kiss JE; et al. (2016). “A randomized, blinded, placebo-controlled trial of education and iron supplementation for mitigation of iron deficiency in regular blood donors”. Transfusion. 56 (6 Pt 2): 1588–97. doi:10.1111/trf.13469. PMC 4905782. PMID 26813849.
- ↑ Cook JD, Skikne BS (1989). “Iron deficiency: definition and diagnosis”. J Intern Med. 226 (5): 349–55. PMID 2681511.
- ↑ Annibale B, Capurso G, Chistolini A, D’Ambra G, DiGiulio E, Monarca B; et al. (2001). “Gastrointestinal causes of refractory iron deficiency anemia in patients without gastrointestinal symptoms”. Am J Med. 111 (6): 439–45. PMID 11690568.
- ↑ Lopez A, Cacoub P, Macdougall IC, Peyrin-Biroulet L (2016). “Iron deficiency anaemia”. Lancet. 387 (10021): 907–16. doi:10.1016/S0140-6736(15)60865-0. PMID 26314490.
- ↑ Khadem G, Scott IA, Klein K (2012). “Evaluation of iron deficiency anaemia in tertiary hospital settings: room for improvement?”. Intern Med J. 42 (6): 658–64. doi:10.1111/j.1445-5994.2012.02724.x. PMID 22288902.
- ↑ Ioannou GN, Rockey DC, Bryson CL, Weiss NS (2002). “Iron deficiency and gastrointestinal malignancy: a population-based cohort study”. Am J Med. 113 (4): 276–80. PMID 12361812. Review in: ACP J Club. 2003 May-Jun;138(3):80
- ↑ Corazza GR, Valentini RA, Andreani ML, D’Anchino M, Leva MT, Ginaldi L; et al. (1995). “Subclinical coeliac disease is a frequent cause of iron-deficiency anaemia”. Scand J Gastroenterol. 30 (2): 153–6. PMID 7732338.
- ↑ Unsworth DJ, Lock RJ, Harvey RF (2000). “Improving the diagnosis of coeliac disease in anaemic women”. Br J Haematol. 111 (3): 898–901. PMID 11122153.
- ↑ Hershko C, Hoffbrand AV, Keret D, Souroujon M, Maschler I, Monselise Y; et al. (2005). “Role of autoimmune gastritis, Helicobacter pylori and celiac disease in refractory or unexplained iron deficiency anemia”. Haematologica. 90 (5): 585–95. PMID 15921373.
- ↑ Eschbach JW, Cook JD, Scribner BH, Finch CA (1977). “Iron balance in hemodialysis patients”. Ann Intern Med. 87 (6): 710–3. PMID 931207.
- ↑ Hershko C, Camaschella C (2014). “How I treat unexplained refractory iron deficiency anemia”. Blood. 123 (3): 326–33. doi:10.1182/blood-2013-10-512624. PMID 24215034.
- ↑ Iolascon A, d’Apolito M, Servedio V, Cimmino F, Piga A, Camaschella C (2006). “Microcytic anemia and hepatic iron overload in a child with compound heterozygous mutations in DMT1 (SCL11A2)”. Blood. 107 (1): 349–54. doi:10.1182/blood-2005-06-2477. PMID 16160008.
- ↑ Simpson E, Mull JD, Longley E, East J (2000). “Pica during pregnancy in low-income women born in Mexico”. West J Med. 173 (1): 20–4, discussion 25. PMC 1070964. PMID 10903283.
- ↑ Rector WG (1989). “Pica: its frequency and significance in patients with iron-deficiency anemia due to chronic gastrointestinal blood loss”. J Gen Intern Med. 4 (6): 512–3. PMID 2585159.
- ↑ 16.0 16.1 Rockey DC, Cello JP (1993). “Evaluation of the gastrointestinal tract in patients with iron-deficiency anemia”. N Engl J Med. 329 (23): 1691–5. doi:10.1056/NEJM199312023292303. PMID 8179652.
- ↑ Singh H, Daci K, Petersen LA, Collins C, Petersen NJ, Shethia A; et al. (2009). “Missed opportunities to initiate endoscopic evaluation for colorectal cancer diagnosis”. Am J Gastroenterol. 104 (10): 2543–54. doi:10.1038/ajg.2009.324. PMC 2758321. PMID 19550418.
- ↑ Read AJ, Waljee AK, Chen CS, Holleman R, Kumbier KE, Saini SD (2021). “Prevalence of Appropriate Testing for Incident Anemia in the US Department of Veterans Affairs”. JAMA Netw Open. 4 (1): e2034406. doi:10.1001/jamanetworkopen.2020.34406. PMC 7838922 Check
|pmc=value (help). PMID 33496793 Check|pmid=value (help). - ↑ Read AJ, Waljee AK, Sussman JB, Singh H, Chen GY, Vijan S; et al. (2021). “Testing Practices, Interpretation, and Diagnostic Evaluation of Iron Deficiency Anemia by US Primary Care Physicians”. JAMA Netw Open. 4 (10): e2127827. doi:10.1001/jamanetworkopen.2021.27827. PMC 8486982 Check
|pmc=value (help). PMID 34596670 Check|pmid=value (help).
Diagnosis
Diagnosis
Diagnostic Study of Choice | History and Symptoms | Physical Examination | Laboratory Findings | Electrocardiogram | X Ray | CT | MRI | Echocardiography or Ultrasound | Other Imaging Findings | Other Diagnostic Studies
Treatment
Treatment
Medical Therapy | Surgery | Primary Prevention | Secondary Prevention | Cost-Effectiveness of Therapy | Future or Investigational Therapies
References
References
Looking for the patient version?
© 2026 MyEClinic – IFTM Institut für Telematik in der Medizin GmbH