
Thoracic aortic aneurysm
For patient information, click here
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Mohammed Salih, MD. [2] Associate Editor(s)-in-Chief: Aarti Narayan, M.B.B.S [3]
Synonyms and keywords: TAA, thoracic aneurysm, ascending aorta aneurysm, arch aneurysm
Overview
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1] Associate Editor(s)-In-Chief: Maheep Singh Sangha, M.B.B.S. Associate Editor(s)-in-Chief: Mohammed Salih, MD. [2]
Overview
A thoracic aortic aneurysm (TAA) is defined as an expansion or dilation of the aorta greater than 4.5 cm. Thoracic aortic aneurysms (TAAs) encompass all aneurysms the aorta between the aortic root and the crura of the diaphragm. The aortic root and the ascending thoracic aorta are the most common sites of TAAs (60%), followed by the descending thoracic aorta (40%). Involvement of the aortic arch and/or extension of a TAA into the abdominal aorta (AA) (so called thoracoabdominal aneurysms) are relatively uncommon subsets (each encountered in 10% of cases or less).
Pathophysiology
An aneurysm occurs when a part or entire circumference of the vessel is pathologically dilated. A true aneurysm involves all three layers of the vessel, whereas pseudoaneurysm is characterized by disruption of the intima and media, and the dilated segment of the aorta is lined by adventitia alone.
Causes
Two of the most common causes of thoracic aorta aneurysm are marfan’s syndrome and atherosclerosis. In some centers, a prior history of dissection with aneurysmal dilation is the most common cause of surgical repair.
Differentiation of Thoracic Aortic Aneurysm from Other Disorders
Thoracic aortic aneurysms are often asymptomatic and as a result can be easily missed. If chest pain is present, it is critical to differentiate a thoracic aortic aneurysm with dissection from other potential life-threatening diseases.
Epidemiology and Demographics
Thoracic aortic aneurysms are relatively uncommon (6 to 10 new ones per 100,000 person years) and are less prevalent than abdominal aortic aneurysm. Thoracic aortic aneurysms are generally diagnosed after the sixth and seventh decades of life. Although men are affected 2 to 4 times as often as women, women are at higher risk of rupture by a factor 6.8.
Risk Factors
Hypertension and cigarette smoking are the most important risk factors, though the importance of genetic factors in the development of thoracic aortic aneurysm (such as familial thoracic aortic aneurysm; familial aortic dissection) has been increasingly recognized. Approximately 10% of patients may have other family members who have aortic aneurysms. It is also important to note that individuals with a history of aneurysms in other parts of the body have a higher chance of developing a thoracic aortic aneurysm.[1]
Natural History, Complications and Prognosis
Thoracic aneurysms enlarge at a more rapid rate than abdominal aneurysms (0.42 vs. 0.28 cm/yr), with aneurysms of the aortic arch growing at ~ 0.56 cm/yr. Aneurysms that are 5-6 cm in diameter have a faster rate of growth and a greater tendency to rupture than smaller ones. Aortic dissection and aortic rupture are the two most feared complications of an aortic aneurysm. The five-year survival of patients with a thoracic aortic aneurysm is 56%. The following are associated with a poorer prognosis: the presence of diastolic dysfunction; trauma as a cause of the aneurysm; the presence of coronary artery disease and the presence of carotid artery disease.
Screening
Screening for TAA is not recommended in the general population. However, certain population substrates, such as those with history of marfan’s syndrome, turner’s syndrome, ehlers-danlos type IV syndrome, familial thoracic aortic disease syndromes, bicuspid aortic valve, takayasu arteritis, giant cell arteritis, loeys-dietz syndrome or a confirmed genetic mutation known to predispose to aortic aneurysms and aortic dissections (TGFBR1, TGFBR2, FBN1, ACTA2, or MYH11) should have imaging study to screen for TAAs. First-degree relatives of people with thoracic aortic aneurysm or dissection should have aortic imaging to identify asymptomatic disease. Patients with high risk syndromes such as marfan’s syndrome and loeys-dietz syndrome should undergo complete aortic imaging at initial diagnosis and 6 months thereafter to establish if enlargement is occurring.
Natural History, Complications and Prognosis
Thoracic aortic aneurysms typically expand slowly at a rate of approximately 0.1-0.2 cm/year. Aortic dissection and aortic rupture are the two most feared complications of an aortic aneurysm. The five-year survival of patients with a thoracic aortic aneurysm is 56%. The following are associated with a poorer prognosis: the presence of diastolic dysfunction; trauma as a cause of the aneurysm; the presence of coronary artery disease and the presence of carotid artery disease.
Diagnosis
History and Symptoms
Most thoracic aortic aneurysms are asymptomatic and diagnosed incidentally on imaging studies. The development of symptoms can indicate that the thoracic aortic aneurysm is expanding. When symptoms are present, they are generally due to compression of adjacent structures. These compressive symptoms include dysphagia (compression of the esophagus), dyspnea and chronic cough (compression of the airway), or hoarseness (compression of the recurrent laryngeal nerve).
Physical Examination
A large thoracic aortic aneurysm may be associated with findings on physical examination secondary to aortic insufficiency (wide pulse pressure, diastolic murmur, heart failure) and compression of adjacent structures such as the recurrent laryngeal nerve (hoarseness), superior vena cava obstruction (selling of the face and neck), and the airway (stridor and wheezing).
General Approach to Imaging in the Patient with a Thoracic Aortic Aneurysm
The diagnosis of a thoracic aortic aneurysm is often made as an incidental finding on either chest x-ray (widening of the mediastinum), on transthoracic echocardiography (dilated aortic root) or on trans esophageal echocardiography (enlarged ascending aorta or aortic arch). The definitive diagnosis is made using CT angiography but MRA is also an excellent test. Once diagnosed, serial CTA (or MRA) are recommended every 6-12 months. The frequency of surveillance imaging should be increased if the aneurysm is larger at baseline, if there is a recent history of accelerating expansion, if the patient is pregnant, and if the patient has marfan syndrome, loeys-dietz syndrome or a confirmed genetic mutation known to predispose to aortic aneurysms and aortic dissections (TGFBR1, TGFBR2, FBN1, ACTA2, or MYH11). Indeed in these high risk syndromes, the patient should undergo complete aortic imaging at the time of the initial diagnosis and then every 6 months to determine if enlargement is occurring. Bicuspid aortic valve, coarctation of the aorta, and/or dilatation of the ascending thoracic aorta should be excluded in a patient with turner’s syndrome. Follow-up imaging should be obtained every 5 to 10 years in the patient with turner’s syndrome if the initial imaging is normal, and yearly if any abnormalities are present. Patients with bicuspid aortic valve disease and first-degree relatives of patients with bicuspid aortic valve disease should undergo imaging to rule out the presence of the thoracic aortic aneurysm.
Chest X-Ray
Thoracic aortic aneurysm is associated with a abnormality on chest x-ray in 80 to 90% of patients. Smaller aneurysms (saccular aneurysms) may not be apparent on a chest x ray.
MRI
The definitive diagnosis of thoracic aortic aneurysm can be made using magnetic resonance angiography (MRA). Once the diagnosis is made, serial MRAs (or CT) are recommended every 6-12 months.
CT
Computed tomography is the most effective method for measuring and monitoring the maximum outer diameter of a thoracic aortic aneurysm over long periods of time.
Echocardiography or Ultrasound
The diagnosis of a thoracic aortic aneurysm is often made as an incidental finding on transthoracic echocardiography (dilated aortic root) or on trans esophageal echocardiography (enlarged ascending aorta or aortic arch). The definitive diagnosis is made using CT angiography but MRA is also an excellent test. Once diagonosed, serial CTA (or MRA) are recommended every 6-12 months.
Treatment
Medical Therapy
Medical therapy for patients with a thoracic aortic aneurysm includes aggressive blood pressure control, smoking cessation, and aggressive lipid management.
Surgery
Indications for surgical repair of a thoracic aortic aneurysm include rupture; symptoms such as pain consistent with impending rupture; aortic regurgitation; growth ≥ 0.5 – 1 cm/year; bicuspid aortic valve; asymptomatic patients with degenerative thoracic aneurysm, chronic aortic dissection, intramural hematoma, penetrating atherosclerotic ulcer, mycotic aneurysm, or pseudoaneurysm, who are otherwise suitable candidates once a TAA reaches a pre-specified size (>5 cm in the ascending aorta, >6 cm in the descending segment) referral for surgical or endovascular repair sholuld be initiated. Most patients undergo repair once they reach >5.5 cm diameter in the ascending aorta and > 6.5 cm in the descending thoracic aorta, respectively. Patients with marfan syndrome or other genetically mediated disorders (vascular ehlers-danlos syndrome, turner syndrome, bicuspid aortic valve, or familial thoracic aortic aneurysm and dissection) should undergo elective operation at smaller diameters (4.0 to 5.0 cm depending on the condition. To avoid acute dissection or rupture, adult patients with loeys-dietz syndrome should undergo surgery for an aortic diameter of >4.4 to 4.6 cm. If a marfan syndrome patient is contemplating pregnancy, they should undergo aortic root replacement if the diameter is greater than 4 cm, and patients undergoing aortic valve repair or replacement and who have an ascending aorta or aortic root of greater than 4.5 cm should be considered for concomitant repair of the aortic root or replacement of the ascending aorta. A woven dacron tube graft is most commonly used in the repair of thoracic aortic aneurysms.
References
- ↑ Thoracic Aortic Disease – Northwestern Memorial Hospital. Thoracic Aortic Aneurysm
Pathophysiology
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Aarti Narayan, M.B.B.S [2] Mohammed Salih, MD. [3]
Overview
An aneurysm occurs when a part or entire circumference of the vessel is pathologically dilated. A true aneurysm involves all three layers of the vessel, whereas pseudoaneurysm is characterized by disruption of the intima and media, and the dilated segment of the aorta is lined by adventitia alone. Thoracic aortic aneurysm (TAA) is a clinically silent and potentially fatal disease whose pathophysiology is poorly understood. Application of data derived from animal models and human tissue analysis of abdominal aortic aneurysms may prove misleading given current evidence of structural and biochemical aortic heterogeneity above and below the diaphragm. Genetic predisposition is more common in TAA and includes multi-faceted syndromes such as Marfan, Loeys-Dietz, and type IV Ehlers-Danlos as well as autosomal-dominant familial patterns of inheritance. Investigation into the consequences of these known mutations has provided insight into the cell signaling cascades leading to degenerative remodeling of the aortic medial extracellular matrix (ECM) with TGF-β playing a major role. Targeted research into modifying the upstream regulation or downstream effects of the TGF-β1 pathway may provide opportunities for intervention to attenuate TAA progression.
Pathophysiology
- The clinical manifestations of thoracic aortic aneurysms depends on hemo-dynamic factors as well as factors intrinsic to individual arterial components.
- Cystic medial necrosis is the most common pathology associated with ascending aortic aneurysms, whereas atherosclerosis is most frequently involved in the arch and descending aorta.
- The aortic aneurysms associated with marfan syndrome grow at a faster rate and are more prone to rupture.
- Most thoracic aneurysms are asymptomatic. However, the enlarging aorta can compress adjacent organs and cause symptoms like chest pain, dyspnea, hoarseness of voice, cough and dysphagia. Also symptoms of congestive heart failure can occur from severe aortic regurgitation and congestion of head, neck and upper extremities from superior vena cava compression.[1][2]
Elastin and Collagen
- Increased activity of certain enzymes causes degradation of elastin and collagen in the arteries. This leads to loss of elasticity, weakens the aortic wall and causes it to dilate.[3]
- Moreover, the part of aorta below the origin of renal arteries has less amount of elastin compared to collagen, accounting for increased frequency of aneurysms in this area[4].
- In patients with marfan’s syndrome there is a defect on chromosome 15 that is associated with impaired fibrillin synthesis, which is the core protein of microfibrils. Frequently among patients with marfan’s syndrome there is cystic medial degeneration[5].
Hemodynamic Factors
- The aorta being a low resistance circuit, repeated trauma from a reflected wave results in dilatation[6].
- Systemic hypertension accelerates the process of dilatation of aorta and contributes to the formation of aneurysms[7][8][9].
Genetics
- FBN1: This is one of the genes involved in marfan’s syndrome[10][11][12].
- TGFBR1: This is one of the genes involved in loeys-dietz syndrome[13].
- TGFBR2: This is one of the genes involved in loeys-dietz syndrome[14].
- COL3A1: This is one of the genes involved in ehlers danlos syndrome[15].
- ACTA2: This is one of the genes involved in familial thoracic aortic aneurysm and dissection (FTAAD)[16].
Pathogenesis
- During embryologic development, the ascending and arch aorta to the ligamentum arteriosum formed by cells from the neural crest, and the media[17].
- It grows by assembling sequential lamellar units to reach a total of 55-60 by adulthood[18].
- It always maintaining a constant ratio of aortic diameter to medial thickness[19].
- Interestingly, that ratio remains consistent during abdominal aortic growth as well, but in that region the precursor cells originate in the mesoderm and the number of lamellar units remains constant while the thickness of each unit is expanded during maturation[20].
- This disparity in aortic cellular origin and segmental growth patterns contributes to differences in and extracellular matrix (ECM) microfibril density and VSMC reactivity to vasoactive growth factors , with downstream effects on susceptibility to aneurysmal degeneration[21].
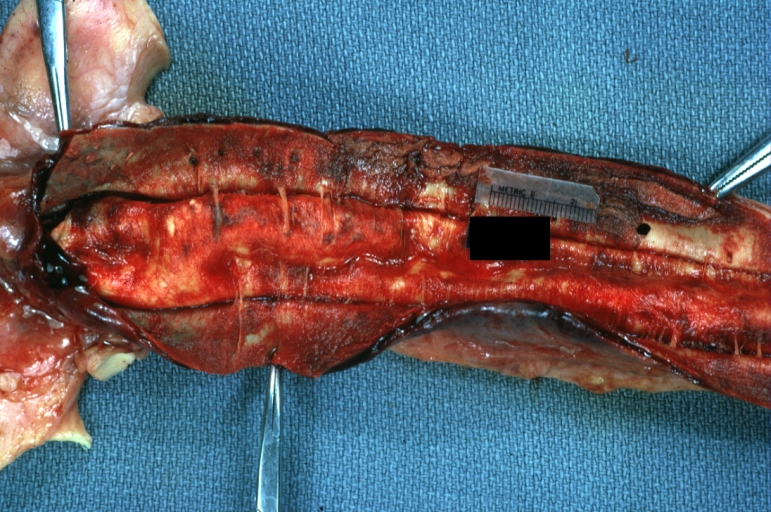
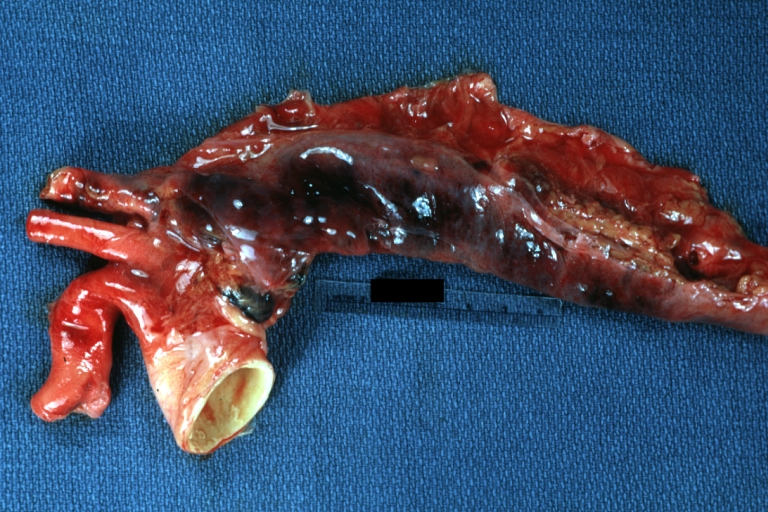
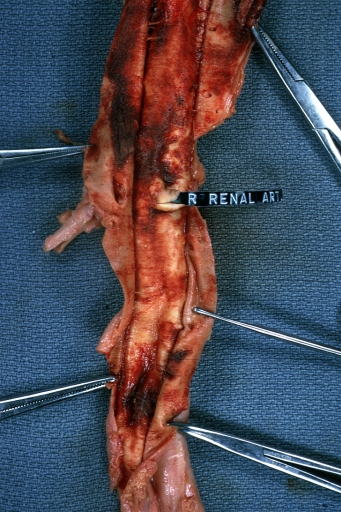
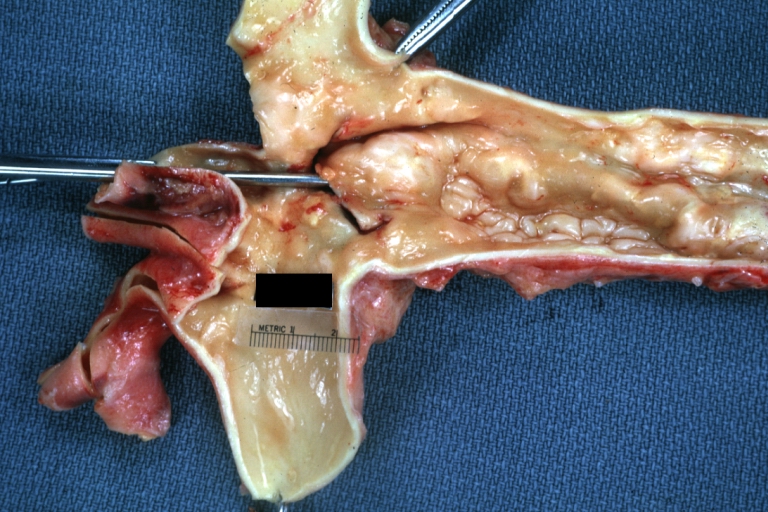
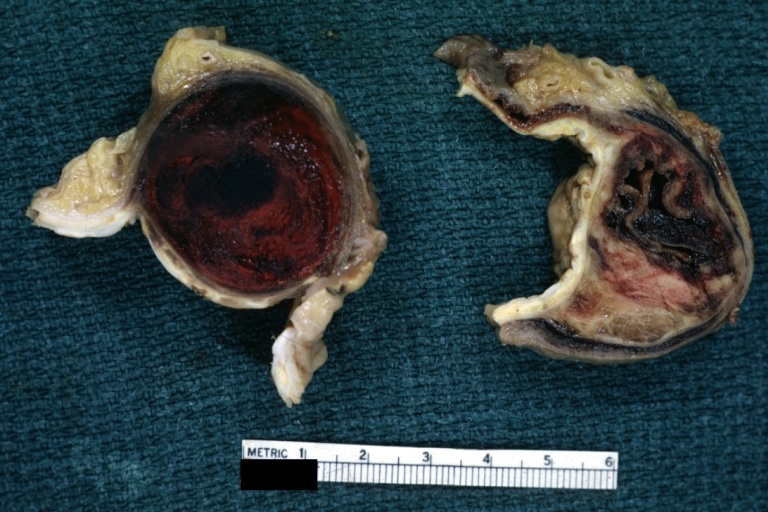
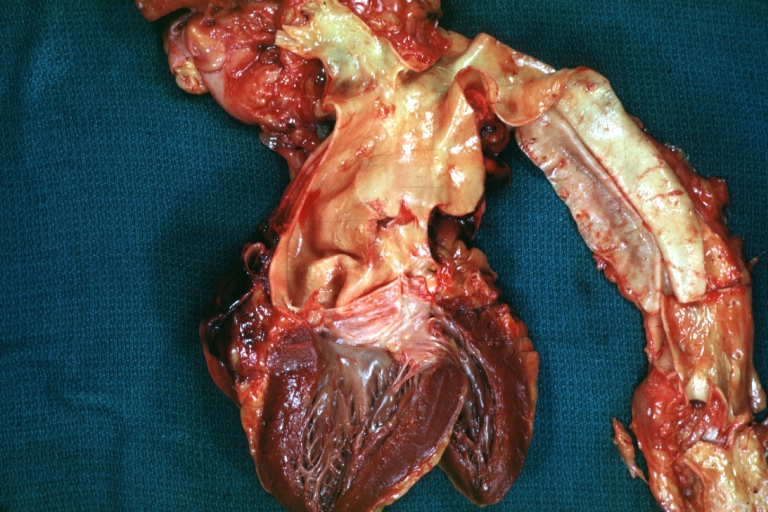
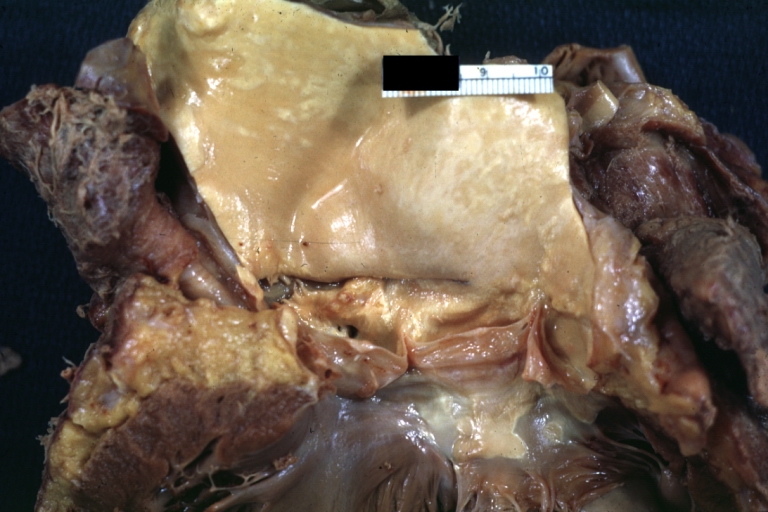
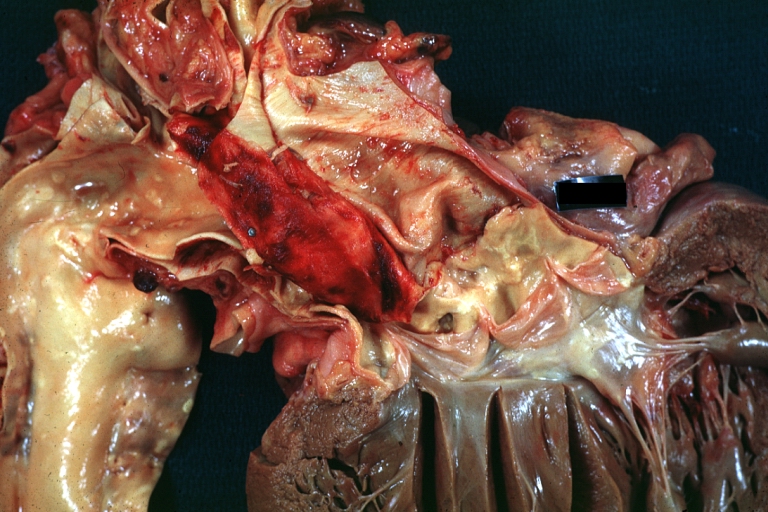
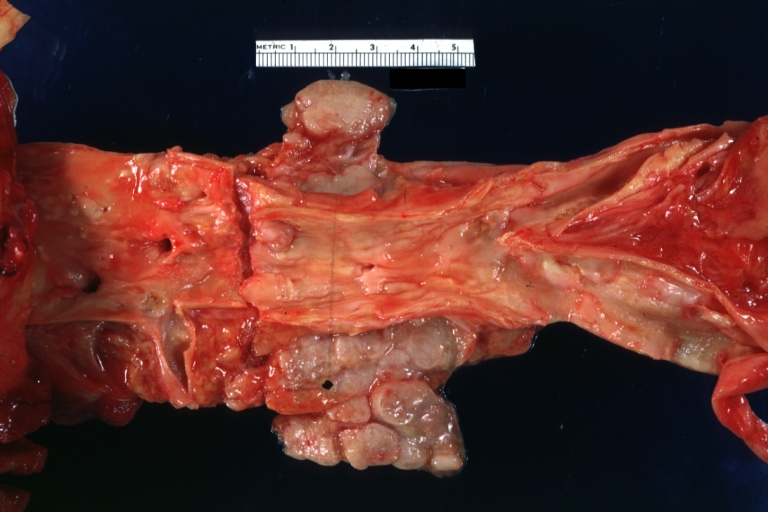
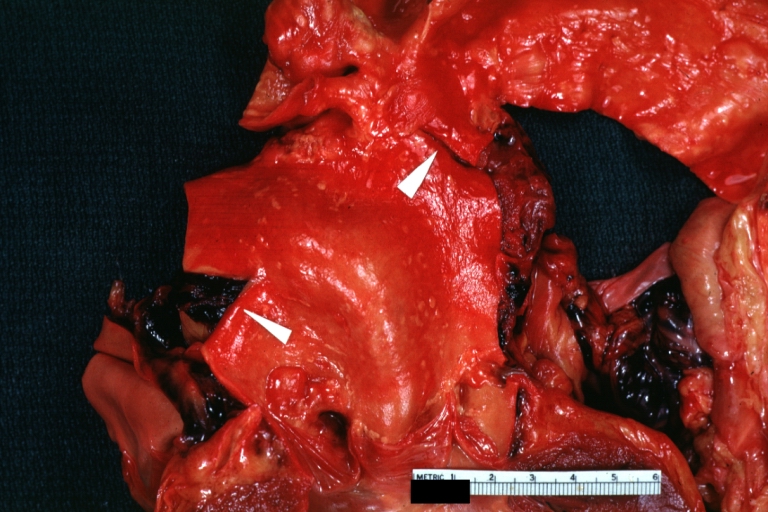
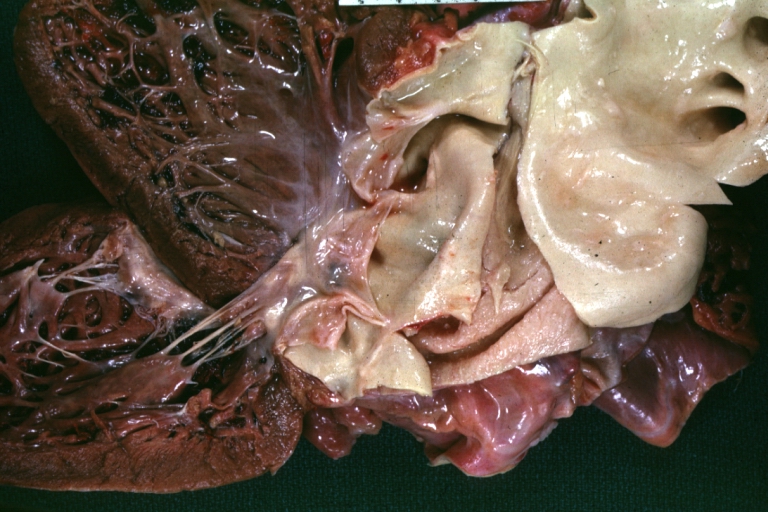
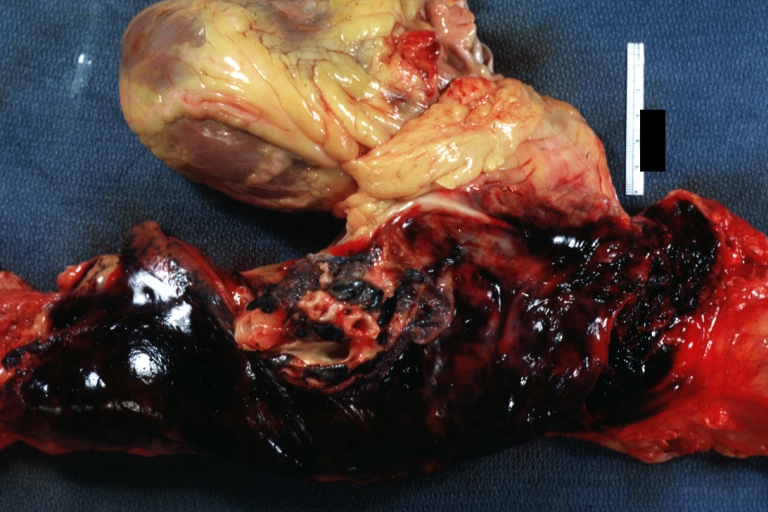
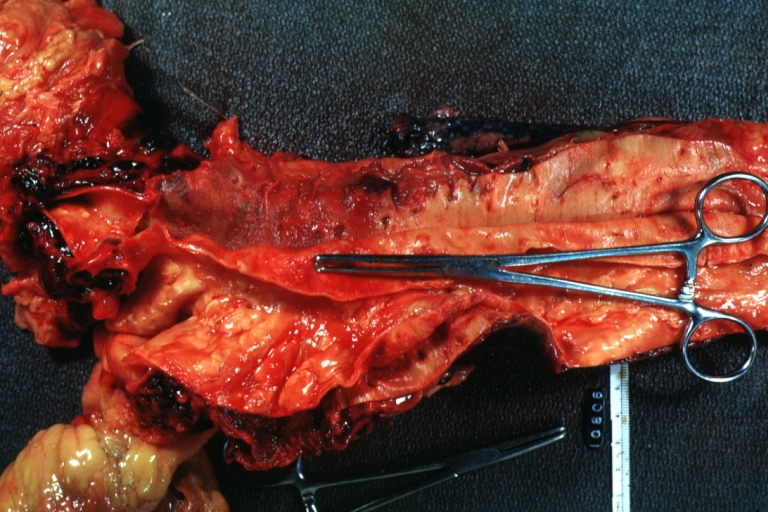
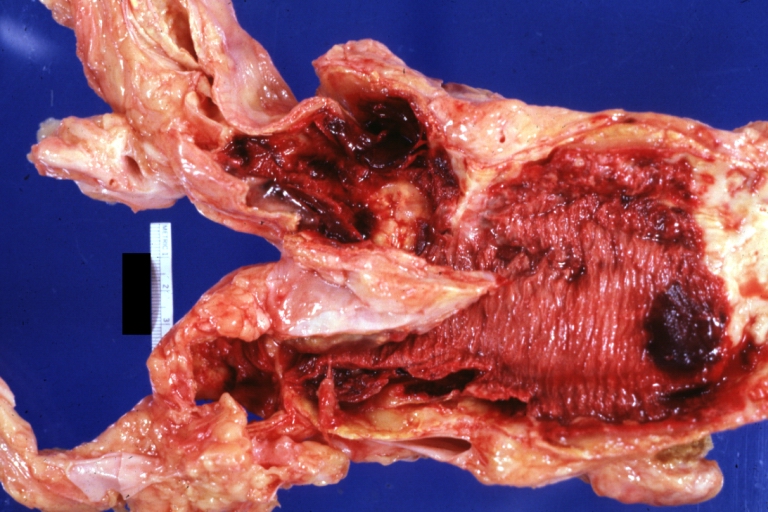
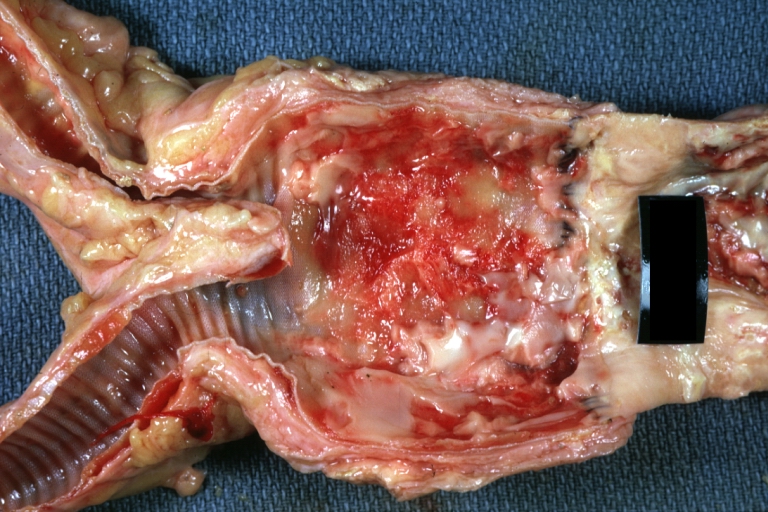
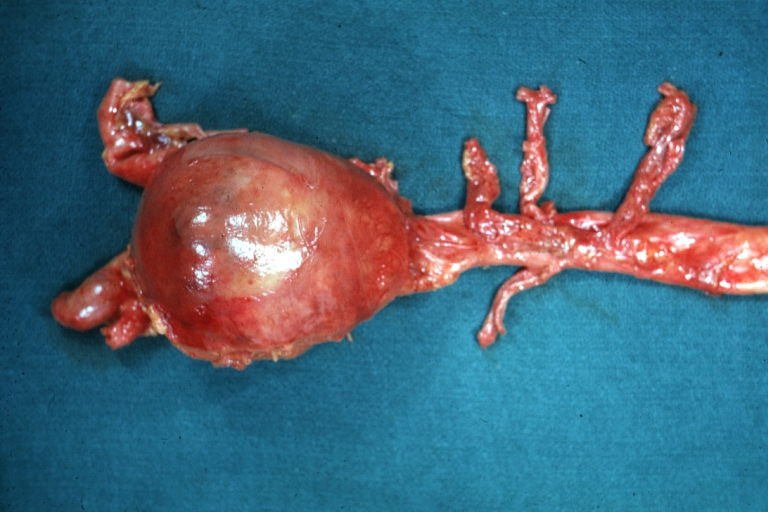
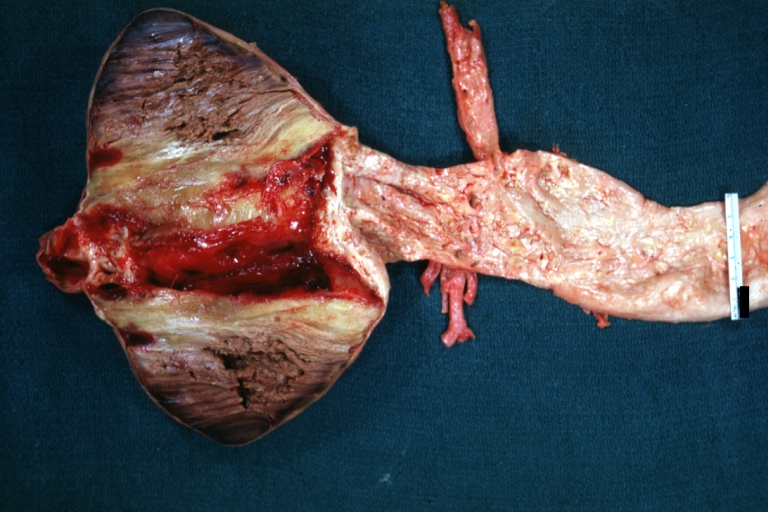
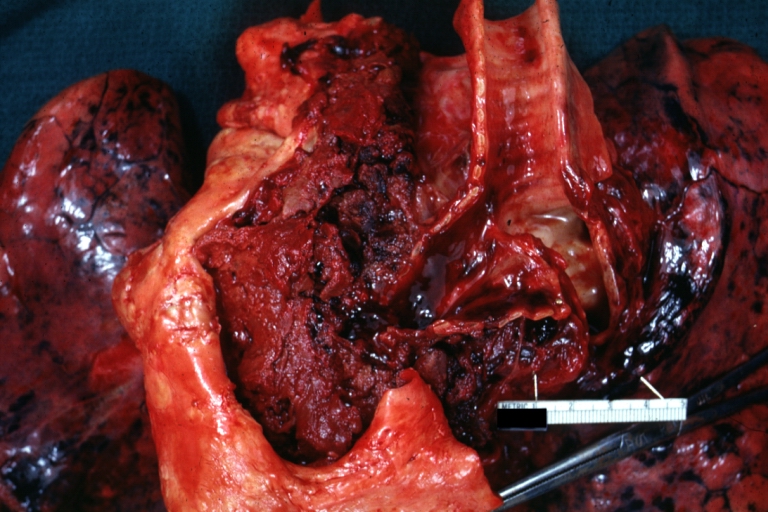
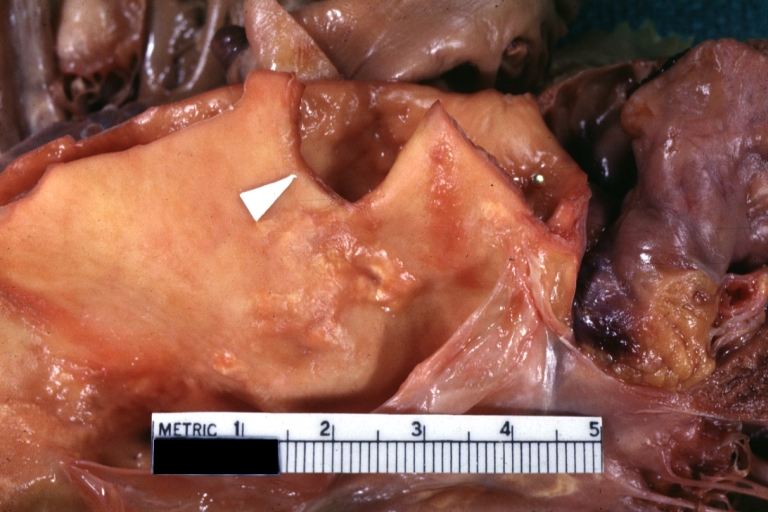
Gross Pathology
Microscopic Pathology
On microscopic histopathological analysis, [feature1], [feature2], and [feature3] are characteristic findings of [disease name].
-
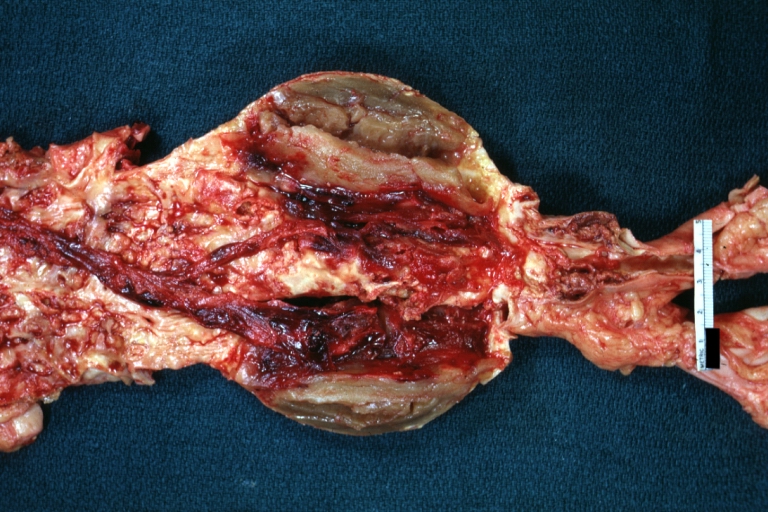
 Dissecting Aneurysm: Gross very good example dissected channel has been opened
Dissecting Aneurysm: Gross very good example dissected channel has been opened -
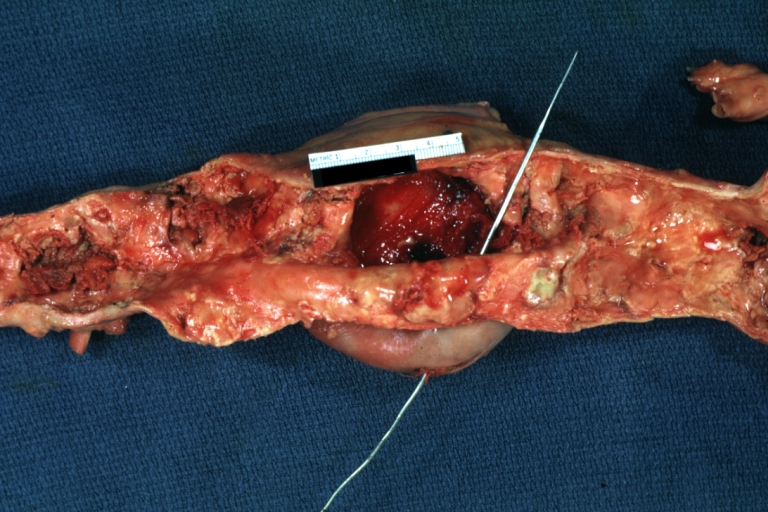
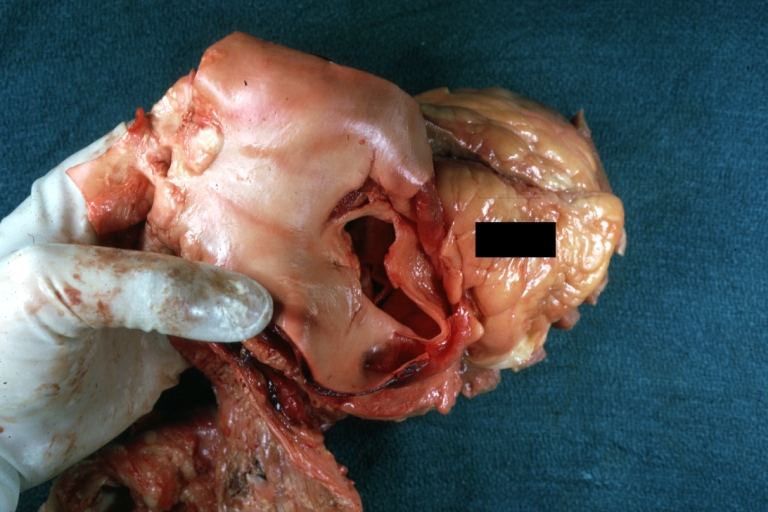
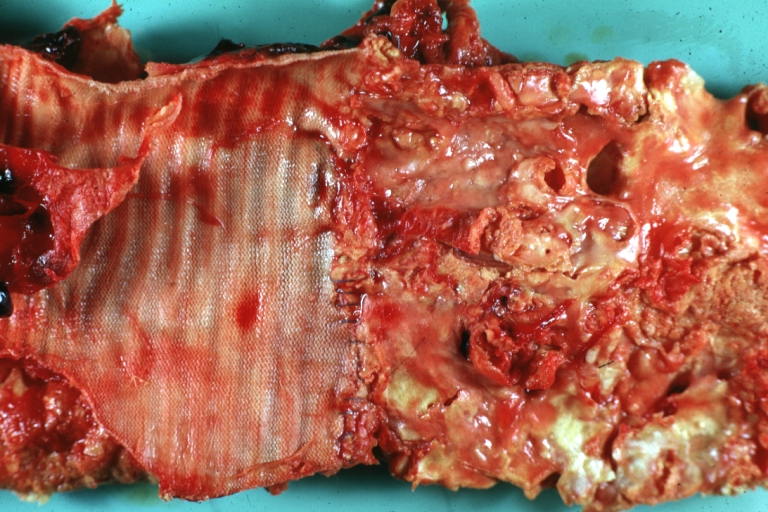
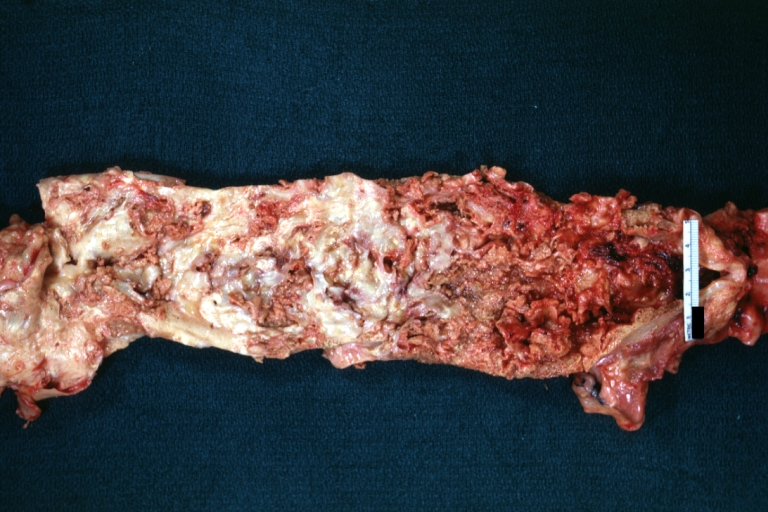
 Dissecting Aneurysm: Gross external view good appearance from adventitia
Dissecting Aneurysm: Gross external view good appearance from adventitia -
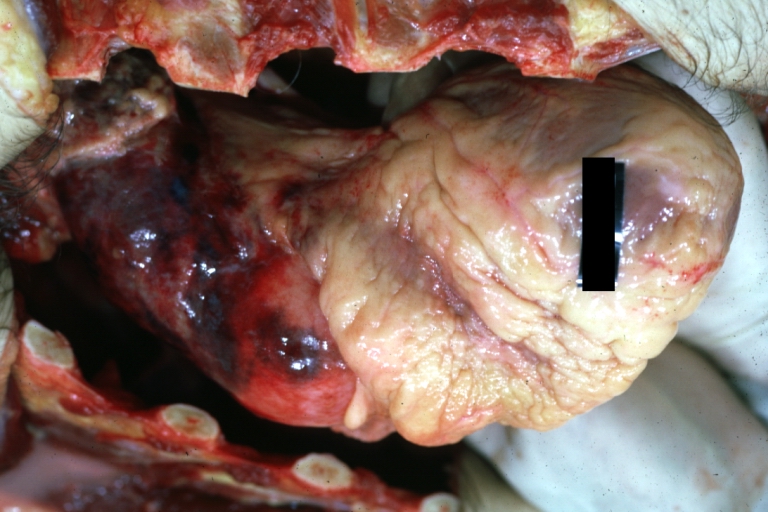
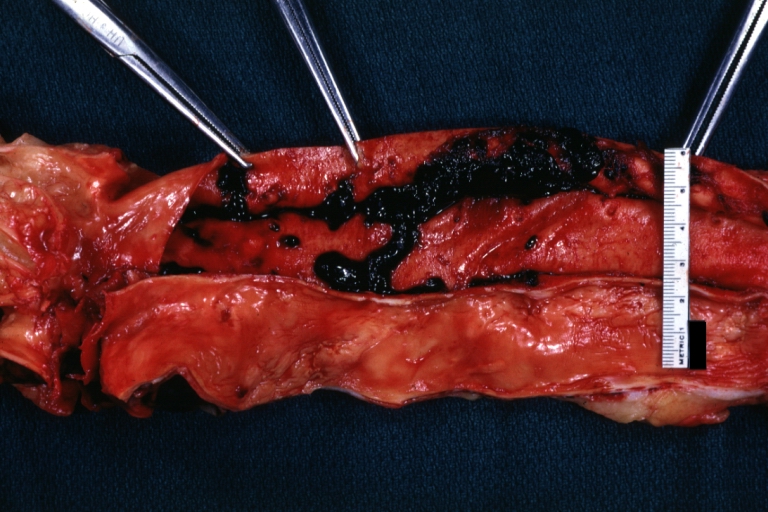
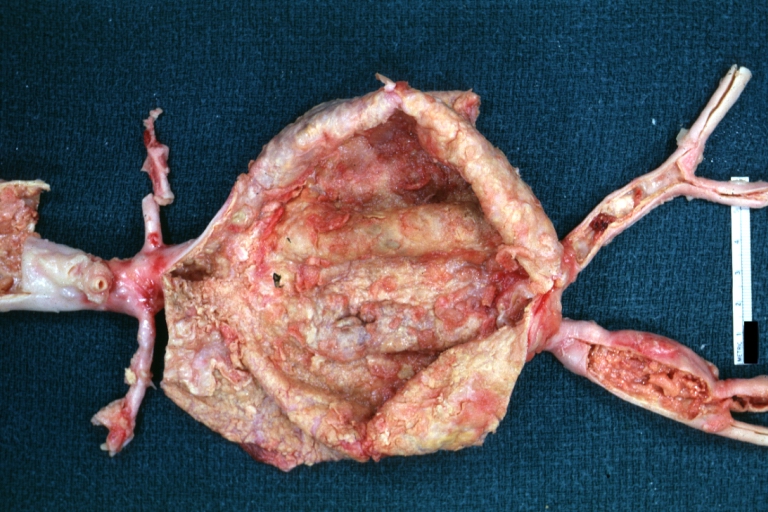
 Dissecting Aneurysm: Gross opened false channel
Dissecting Aneurysm: Gross opened false channel



-
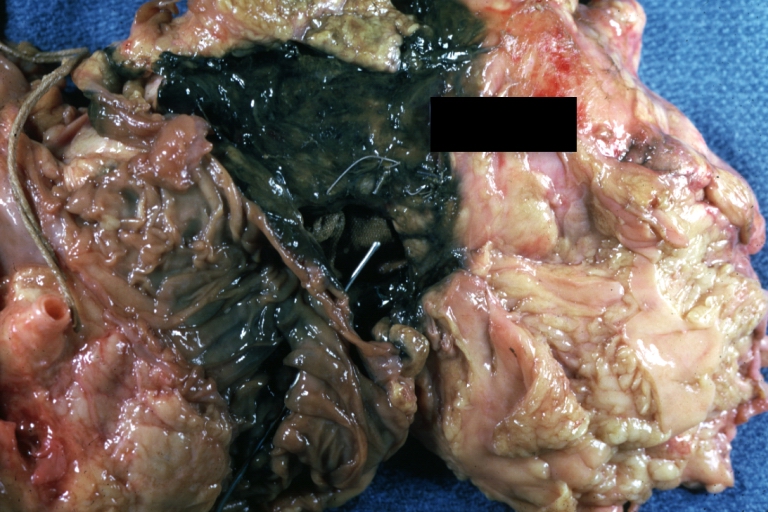
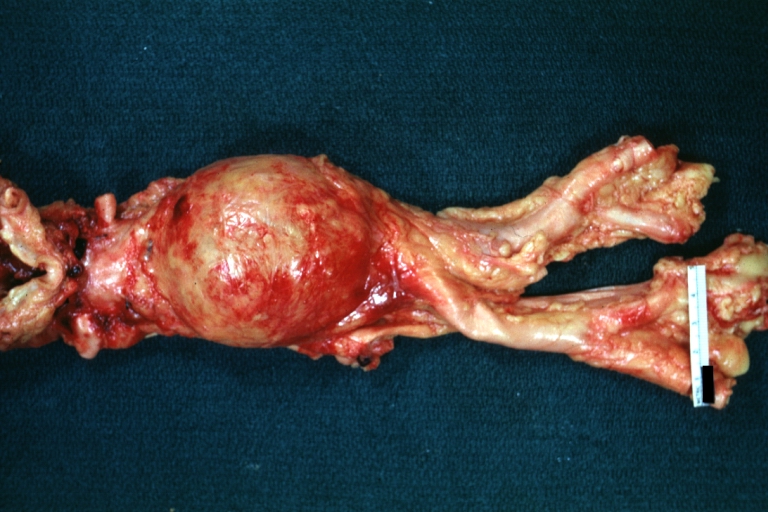
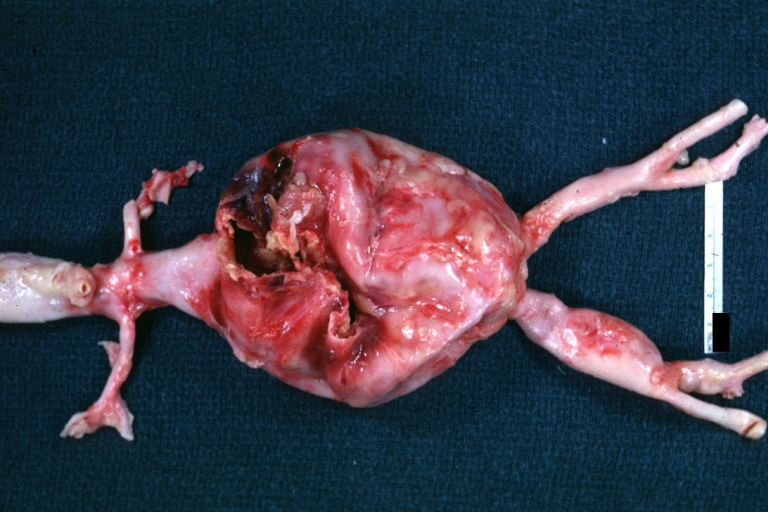
 Dissecting Aneurysm: Gross good example dissection beginning at third portion aortic arch
Dissecting Aneurysm: Gross good example dissection beginning at third portion aortic arch -
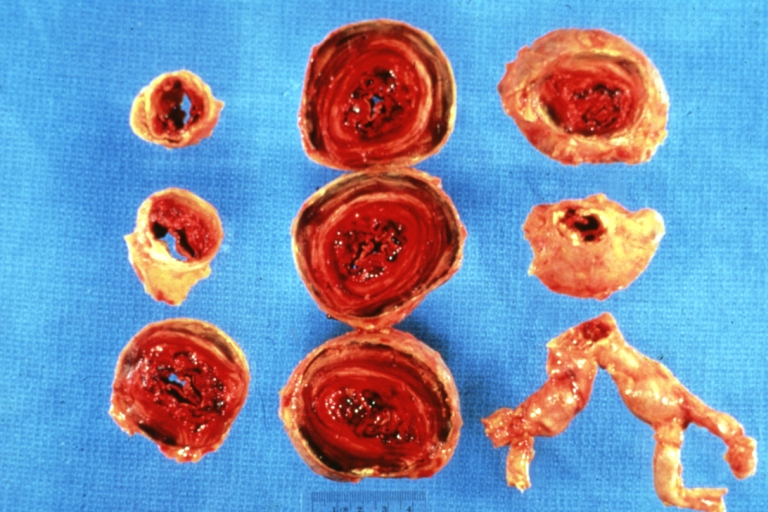
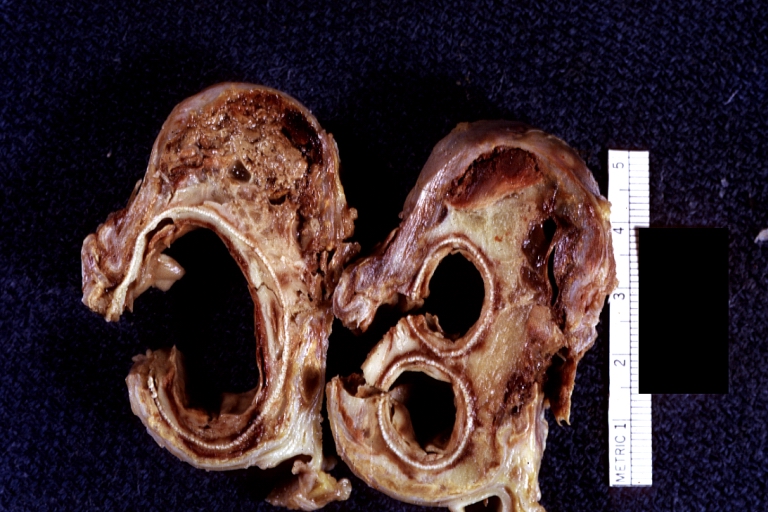
 Dissecting Aneurysm: Gross cross sections showing thrombus in false lumen true lumen has been opened longitudinally
Dissecting Aneurysm: Gross cross sections showing thrombus in false lumen true lumen has been opened longitudinally -
 Dissecting Aneurysm: Gross shows origin just above aortic valve false channel shown in descending thoracic aorta (very good example)
Dissecting Aneurysm: Gross shows origin just above aortic valve false channel shown in descending thoracic aorta (very good example)



-
 Atherosclerotic Aneurysm: Gross, a good example of typical abdominal aorta aneurysm with mural thrombus
Atherosclerotic Aneurysm: Gross, a good example of typical abdominal aorta aneurysm with mural thrombus -
 Dissecting Aneurysm: Gross, a very good example of dissection beginning just above aortic ring
Dissecting Aneurysm: Gross, a very good example of dissection beginning just above aortic ring -
 Atherosclerotic Aneurysm: Gross, (rather) good example of abdominal aortic aneurysm
Atherosclerotic Aneurysm: Gross, (rather) good example of abdominal aortic aneurysm



-
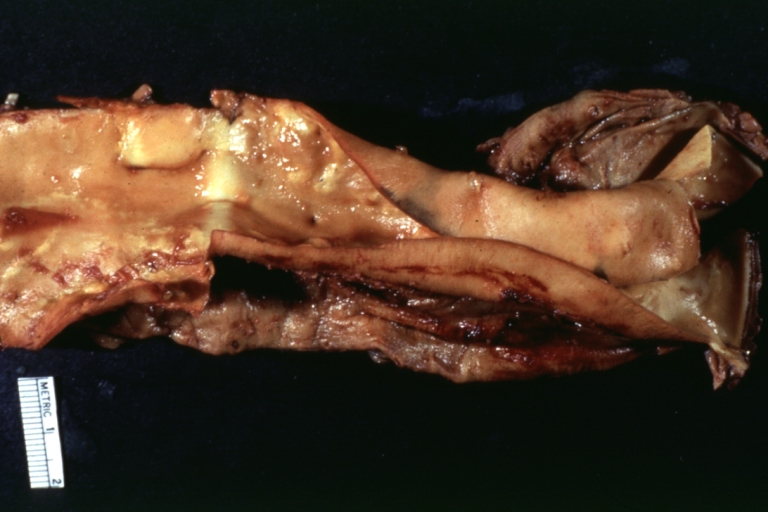
 Dissecting Aneurysm: Gross, an excellent example, starting just above the aortic valve with reflection of aorta to show the dissection tract and some thrombus
Dissecting Aneurysm: Gross, an excellent example, starting just above the aortic valve with reflection of aorta to show the dissection tract and some thrombus -
 Dissecting Aneurysm: Gross shows dilated aorta with extensive atherosclerosis dissection is seen, a small abdominal aorta atherosclerotic aneurysm is present good for association of dilation with dissection
Dissecting Aneurysm: Gross shows dilated aorta with extensive atherosclerosis dissection is seen, a small abdominal aorta atherosclerotic aneurysm is present good for association of dilation with dissection -
 Dissecting Aneurysm: Gross arrow points to start of dissection in first portion aortic arch good but not the best example shows dilation
Dissecting Aneurysm: Gross arrow points to start of dissection in first portion aortic arch good but not the best example shows dilation



-
 Dissecting Aneurysm: Gross, very good to show start of dissection above aortic valve and blood in false channel
Dissecting Aneurysm: Gross, very good to show start of dissection above aortic valve and blood in false channel -
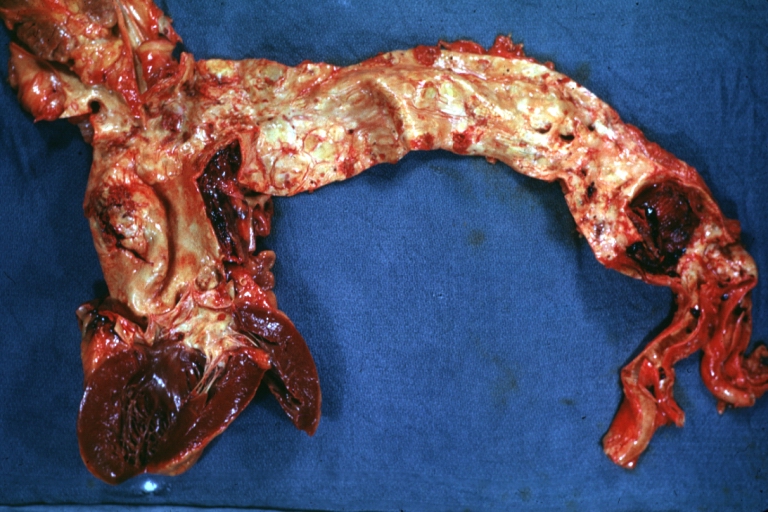
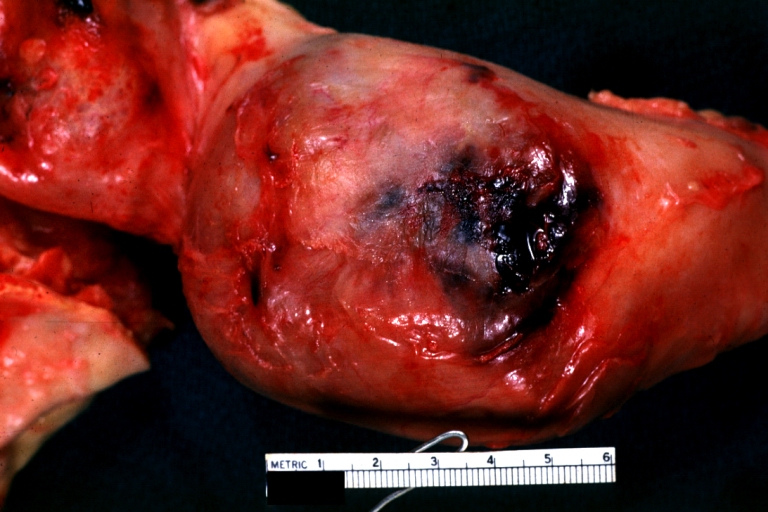
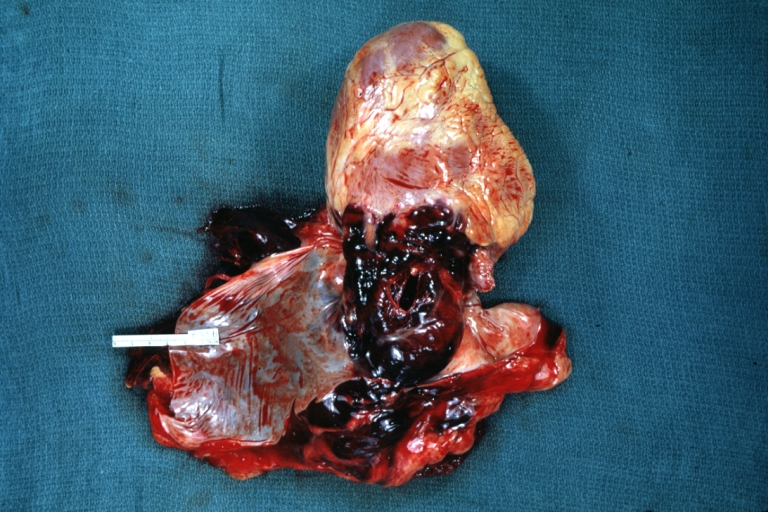 Dissecting Aneurysm: Gross, heart with root of aorta to show hemorrhage into pericardium (a very good example)
Dissecting Aneurysm: Gross, heart with root of aorta to show hemorrhage into pericardium (a very good example) -
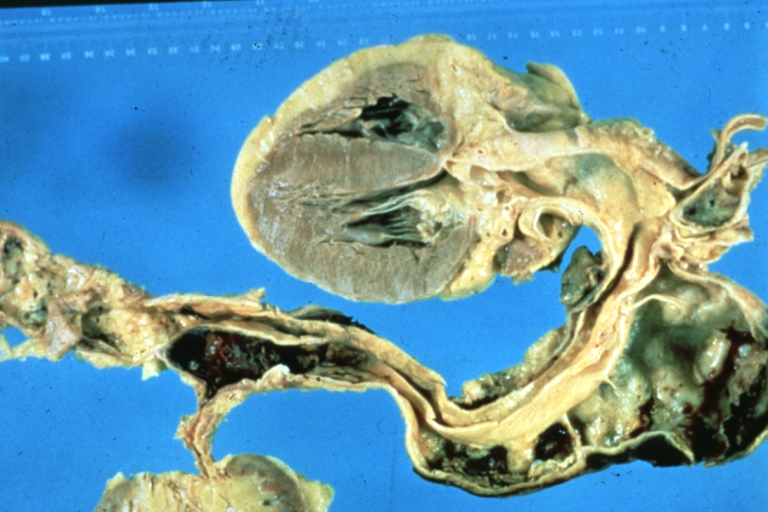 Dissecting Aneurysm: Gross, of heart and aorta with dissection and large false channel (a good example)
Dissecting Aneurysm: Gross, of heart and aorta with dissection and large false channel (a good example)



-
 Dissecting Aneurysm: Gross cross section of aorta with two channels (a good example)
Dissecting Aneurysm: Gross cross section of aorta with two channels (a good example) -
 Atherosclerotic Aneurysm: Gross, a nice view of cross section of abdominal aorta aneurysm
Atherosclerotic Aneurysm: Gross, a nice view of cross section of abdominal aorta aneurysm -
 Dissecting Aneurysm: Gross good example of typical angular tear above aortic valve
Dissecting Aneurysm: Gross good example of typical angular tear above aortic valve



-
 Dissecting Aneurysm: Gross good example angular tear above aortic valve
Dissecting Aneurysm: Gross good example angular tear above aortic valve -
 Atherosclerotic Aneurysm: Gross, external natural color very good example of an atherosclerotic thoracic aorta aneurysm with focal rupture
Atherosclerotic Aneurysm: Gross, external natural color very good example of an atherosclerotic thoracic aorta aneurysm with focal rupture -
 Atherosclerotic Aneurysm: Gross, excellent color, opened thoracic segment of aorta with two saccular atherosclerotic ruptured aneurysms
Atherosclerotic Aneurysm: Gross, excellent color, opened thoracic segment of aorta with two saccular atherosclerotic ruptured aneurysms



-
 Atherosclerotic Aneurysm: Gross, an excellent example, natural color, external view of typical thoracic aortic aneurysms
Atherosclerotic Aneurysm: Gross, an excellent example, natural color, external view of typical thoracic aortic aneurysms -
 Atherosclerotic Aneurysm: Gross unopened lesion natural color
Atherosclerotic Aneurysm: Gross unopened lesion natural color -
 Dissecting Aneurysm: Gross dissection first portion of arch fixed specimen (a good example)
Dissecting Aneurysm: Gross dissection first portion of arch fixed specimen (a good example)



-
 Dissecting Aneurysm: Gross, rather well shown dissection in first portion of the aortic arch
Dissecting Aneurysm: Gross, rather well shown dissection in first portion of the aortic arch -
 Dissecting Aneurysm: Gross, rather well shown dissection in first portion of the aortic arch
Dissecting Aneurysm: Gross, rather well shown dissection in first portion of the aortic arch -
 Dissecting Aneurysm: Gross, an excellent example of type I lesion
Dissecting Aneurysm: Gross, an excellent example of type I lesion



-
 Dissecting Aneurysm: Gross, external view, an excellent example
Dissecting Aneurysm: Gross, external view, an excellent example -
 Dissecting Aneurysm: Gross, Type I shows false channel
Dissecting Aneurysm: Gross, Type I shows false channel -
 Dissecting Aneurysm: Gross, opened to show false channel (good example)
Dissecting Aneurysm: Gross, opened to show false channel (good example)



-
 Atherosclerotic Aneurysm: Gross, very good example of ruptured thoracic segment
Atherosclerotic Aneurysm: Gross, very good example of ruptured thoracic segment -
 Dissecting Aneurysm: Gross, coagulum of blood in false channel
Dissecting Aneurysm: Gross, coagulum of blood in false channel -
 Dissecting Aneurysm: Gross, aortic valve area dissection (well shown, typical lesion)
Dissecting Aneurysm: Gross, aortic valve area dissection (well shown, typical lesion)



-
 Abdominal Aneurysm Ruptured: Gross (good example) opened kidneys in marked place, atherosclerosis in lower thoracic aorta
Abdominal Aneurysm Ruptured: Gross (good example) opened kidneys in marked place, atherosclerosis in lower thoracic aorta -
 Abdominal Aneurysm: Gross, (very good example) opened lesion with mural thrombus
Abdominal Aneurysm: Gross, (very good example) opened lesion with mural thrombus -
 Dissecting Aneurysm: Gross, large tear in first portion of aortic arch, annuloaortic ectasis
Dissecting Aneurysm: Gross, large tear in first portion of aortic arch, annuloaortic ectasis



-
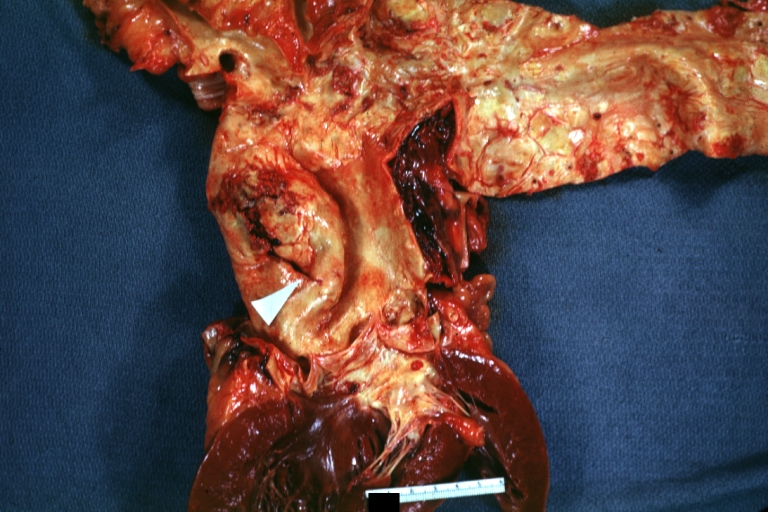
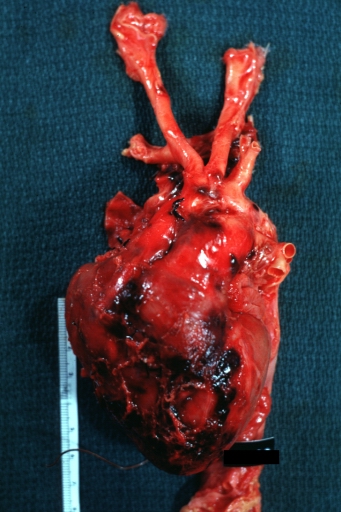
 Dissecting Aneurysm: Gross, external view of heart and first portion of aortic arch, annuloaortic ectasia, hemorrhage beneath adventitia is evidence of dissection
Dissecting Aneurysm: Gross, external view of heart and first portion of aortic arch, annuloaortic ectasia, hemorrhage beneath adventitia is evidence of dissection -
 Atherosclerotic Aneurysm Infected: Gross, infected abdominal aneurysm at superior suture line with rupture into duodenum
Atherosclerotic Aneurysm Infected: Gross, infected abdominal aneurysm at superior suture line with rupture into duodenum -
 Atherosclerotic Aneurysm: Gross, cross sections of repaired aneurysm showing Dacron graft and old mural thrombus. A nice example of fibrin layer in graft
Atherosclerotic Aneurysm: Gross, cross sections of repaired aneurysm showing Dacron graft and old mural thrombus. A nice example of fibrin layer in graft



-
 Ruptured Syphilitic Aneurysm
Ruptured Syphilitic Aneurysm -
 Dissecting Aneurysm in a patient with Marfan’s syndrome
Dissecting Aneurysm in a patient with Marfan’s syndrome -
 Traumatic Aneurysm
Traumatic Aneurysm



-
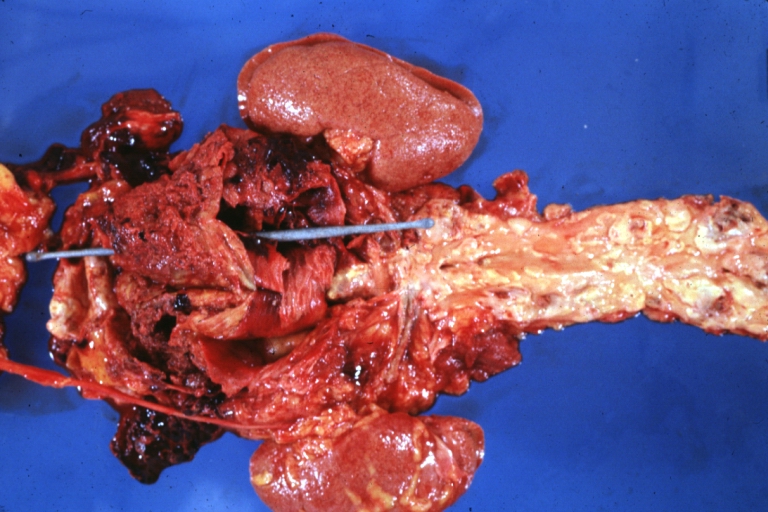
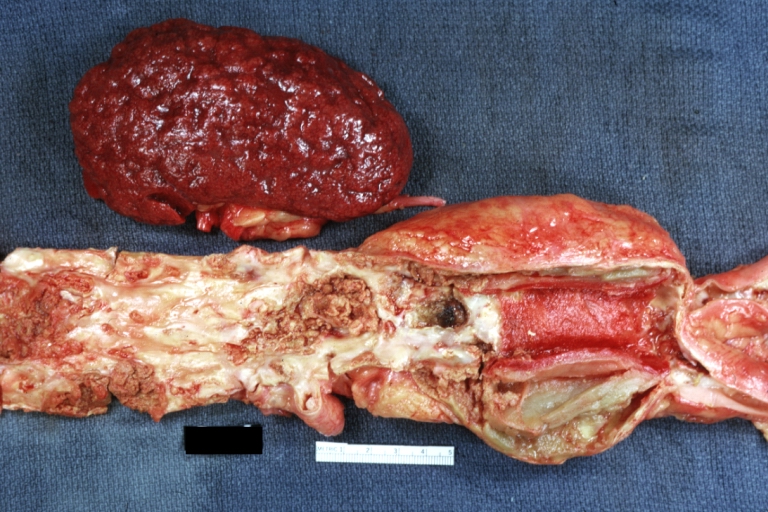 Kidney: Arteriosclerosis: Gross aorta with well shown renal artery containing large plaque and kidney with multiple cortical scars and atrophy also abdominal aorta aneurysm with mural thrombus (excellent example for renovascular hypertension)
Kidney: Arteriosclerosis: Gross aorta with well shown renal artery containing large plaque and kidney with multiple cortical scars and atrophy also abdominal aorta aneurysm with mural thrombus (excellent example for renovascular hypertension) -
 Dissecting Aneurysm: Gross, fixed tissue, descending thoracic segment dissection opened to show the false channel. The true surface is also visible
Dissecting Aneurysm: Gross, fixed tissue, descending thoracic segment dissection opened to show the false channel. The true surface is also visible -
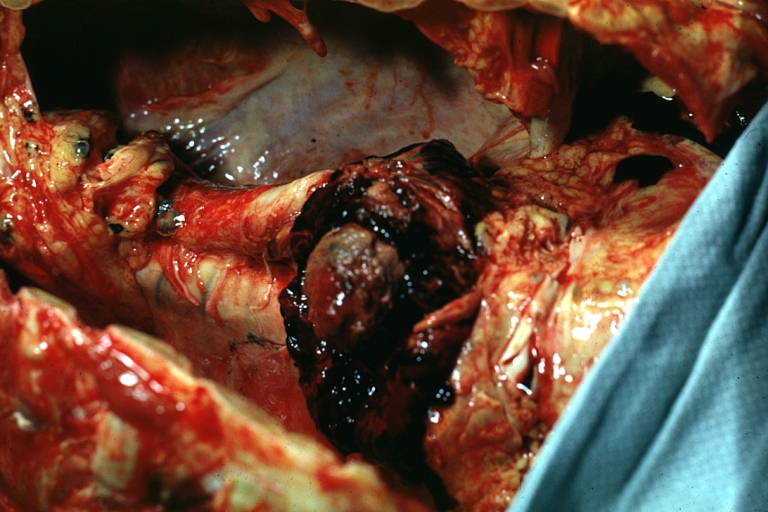 Aneurysm: Gross, ruptured thoracic aorta aneurysm, in situ lower thoracic portion (probably due to atherosclerosis)
Aneurysm: Gross, ruptured thoracic aorta aneurysm, in situ lower thoracic portion (probably due to atherosclerosis)



-
 Abdominal Aneurysm Graft Repair: Gross, natural color, close-up view, an excellent example of Dacron graft that has been in place for years with pseudointima and atherosclerosis
Abdominal Aneurysm Graft Repair: Gross, natural color, close-up view, an excellent example of Dacron graft that has been in place for years with pseudointima and atherosclerosis -
 Dacron Graft: Gross, close-up Dacron graft to repair aneurysm. Aorta completely covered with a calcified and ulcerated plaque with small mural thrombi (an excellent depiction of proximal suture line)
Dacron Graft: Gross, close-up Dacron graft to repair aneurysm. Aorta completely covered with a calcified and ulcerated plaque with small mural thrombi (an excellent depiction of proximal suture line) -
 Dissecting Aneurysm: Gross natural color descending aorta opened into false channel
Dissecting Aneurysm: Gross natural color descending aorta opened into false channel



-
 Abdominal Aneurysm: Gross, natural color, unopened specimen with about a six centimeter aneurysm between renals and bifurcation (a very good example of opened aneurysm)
Abdominal Aneurysm: Gross, natural color, unopened specimen with about a six centimeter aneurysm between renals and bifurcation (a very good example of opened aneurysm) -
 Abdominal Aneurysm: Gross, natural color, an opened aneurysm showing quite well laminated thrombus
Abdominal Aneurysm: Gross, natural color, an opened aneurysm showing quite well laminated thrombus -
 Atherosclerosis with Mural Thrombi: Gross, natural color, a nice photo of descending thoracic aorta with extensive ulcerated plaques and mural thrombi in distal portion. The case also has an abdominal aneurysm
Atherosclerosis with Mural Thrombi: Gross, natural color, a nice photo of descending thoracic aorta with extensive ulcerated plaques and mural thrombi in distal portion. The case also has an abdominal aneurysm



-
 Pseudoaneurysm Ruptured Into Duodenum: Gross natural color aorta and duodenum with arrow pointing to rupture point of aortobifemoral bypass pseudoaneurysm rupture and another in duodenum a very good demonstration of this very well known complication of aortic prostheses
Pseudoaneurysm Ruptured Into Duodenum: Gross natural color aorta and duodenum with arrow pointing to rupture point of aortobifemoral bypass pseudoaneurysm rupture and another in duodenum a very good demonstration of this very well known complication of aortic prostheses -
 Abdominal Aneurysm: Gross, natural color, large aneurysm opened showing sessile calcified plaques with no mural thrombus. Lesion extends from renal arteries to the bifurcation (the same lesion seen externally with focus of rupture)
Abdominal Aneurysm: Gross, natural color, large aneurysm opened showing sessile calcified plaques with no mural thrombus. Lesion extends from renal arteries to the bifurcation (the same lesion seen externally with focus of rupture) -
 Abdominal Aneurysm Ruptured: Gross, natural color, external view with large area of apparent rupture. Aorta is opened to show this aneurysm)
Abdominal Aneurysm Ruptured: Gross, natural color, external view with large area of apparent rupture. Aorta is opened to show this aneurysm)



-
 Abdominal Aneurysm: Gross, natural color, unopened large and quite typical aneurysm extending from below renal arteries to bifurcation
Abdominal Aneurysm: Gross, natural color, unopened large and quite typical aneurysm extending from below renal arteries to bifurcation -
 Abdominal Aneurysm: Gross, natural color, opened aneurysm with well shown and typical laminated thrombus (external view)
Abdominal Aneurysm: Gross, natural color, opened aneurysm with well shown and typical laminated thrombus (external view) -
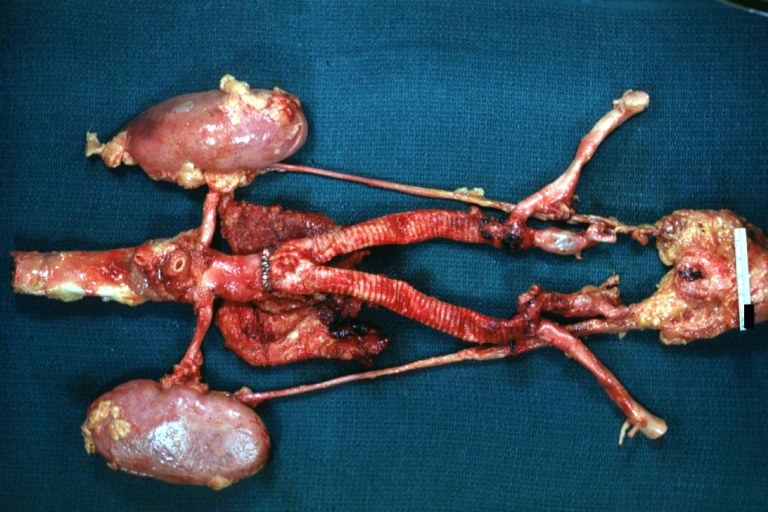 Aortobifemoral Prosthesis: Gross, natural color, nice dissection showing Dacron prosthesis replacing abdominal segment of aorta with portion of atherosclerotic aneurysm with renal arteries and kidneys
Aortobifemoral Prosthesis: Gross, natural color, nice dissection showing Dacron prosthesis replacing abdominal segment of aorta with portion of atherosclerotic aneurysm with renal arteries and kidneys



-
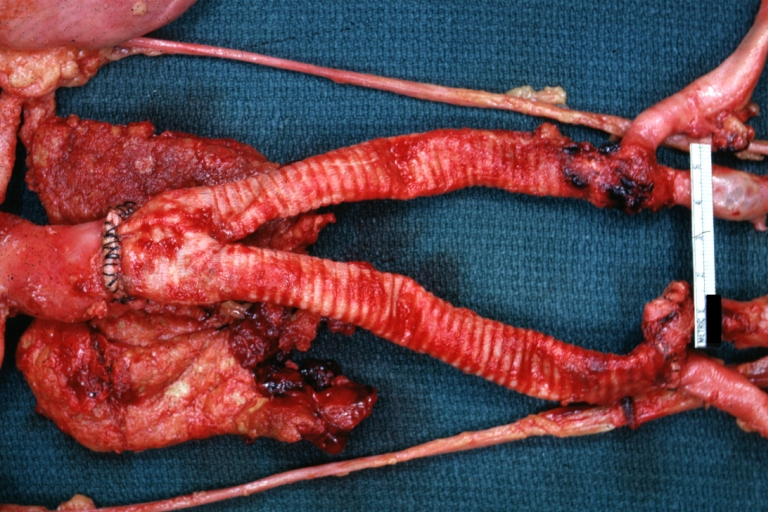 Aortobifemoral Prosthesis: Gross natural color close-up view of nicely dissected prosthesis extending from below renals to common iliac arteries portion of atherosclerotic aneurysm behind prosthesis
Aortobifemoral Prosthesis: Gross natural color close-up view of nicely dissected prosthesis extending from below renals to common iliac arteries portion of atherosclerotic aneurysm behind prosthesis -
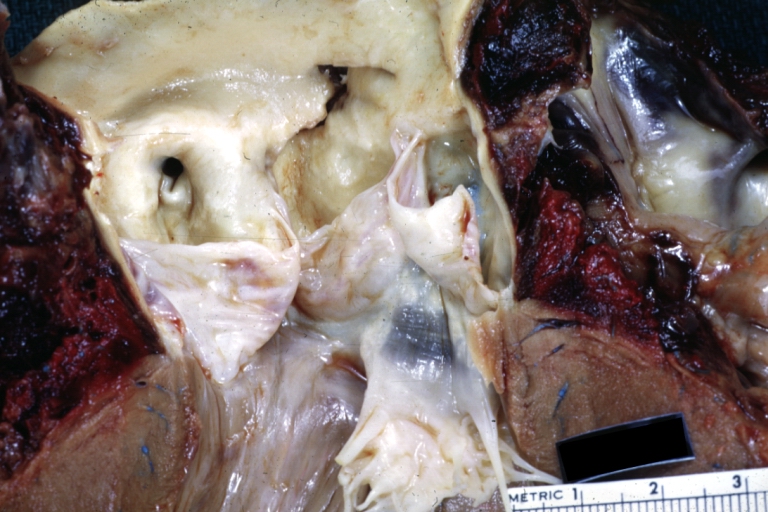
 Dissecting Aneurysm: Gross natural color close-up view of aortic valve and proximal aortic arch with ruptured intima rather good illustration of this lesion
Dissecting Aneurysm: Gross natural color close-up view of aortic valve and proximal aortic arch with ruptured intima rather good illustration of this lesion -
 Syphilitic Aneurysm: Gross natural color rather a close-up view and outstanding photo of aneurysm ruptured into the left main stem bronchus
Syphilitic Aneurysm: Gross natural color rather a close-up view and outstanding photo of aneurysm ruptured into the left main stem bronchus



-
 Syphilitic Aneurysm: Gross natural color typical tree barking in aorta aneurysm opening is seen in which is a thrombus aneurysm ruptured into left main stem bronchus (shown very well)
Syphilitic Aneurysm: Gross natural color typical tree barking in aorta aneurysm opening is seen in which is a thrombus aneurysm ruptured into left main stem bronchus (shown very well) -
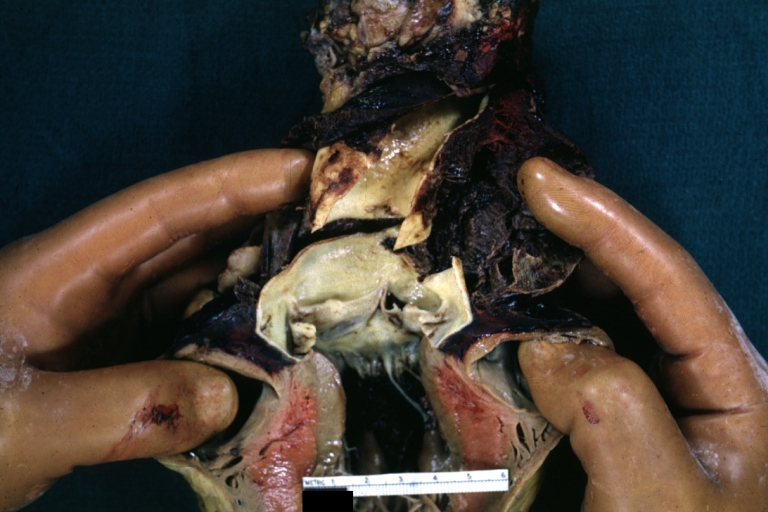
 Dissecting Aneurysm Chronic: Gross natural color first portion of aortic arch with intimal rent well shown with healed margins and view into false channel that shows a surface looking like atherosclerosis which is known to develop in a chronic dissection
Dissecting Aneurysm Chronic: Gross natural color first portion of aortic arch with intimal rent well shown with healed margins and view into false channel that shows a surface looking like atherosclerosis which is known to develop in a chronic dissection -
 Dissecting Aneurysm Chronic: Gross, natural color, closer view of the previous one (a very good example)
Dissecting Aneurysm Chronic: Gross, natural color, closer view of the previous one (a very good example)



References
- ↑ Coady MA, Rizzo JA, Elefteriades JA (November 1999). “Developing surgical intervention criteria for thoracic aortic aneurysms”. Cardiol Clin. 17 (4): 827–39. doi:10.1016/s0733-8651(05)70118-1. PMID 10589349.
- ↑ Ruddy JM, Jones JA, Spinale FG, Ikonomidis JS (November 2008). “Regional heterogeneity within the aorta: relevance to aneurysm disease”. J. Thorac. Cardiovasc. Surg. 136 (5): 1123–30. doi:10.1016/j.jtcvs.2008.06.027. PMC 2679174. PMID 19026791.
- ↑ Castellano JM, Kovacic JC, Sanz J, Fuster V (April 2012). “Are we ignoring the dilated thoracic aorta?”. Ann. N. Y. Acad. Sci. 1254: 164–74. doi:10.1111/j.1749-6632.2012.06493.x. PMID 22548582.
- ↑ Wolinsky H (October 1970). “Comparison of medial growth of human thoracic and abdominal aortas”. Circ. Res. 27 (4): 531–8. doi:10.1161/01.res.27.4.531. PMID 5507030.
- ↑ Halloran BG, Davis VA, McManus BM, Lynch TG, Baxter BT (July 1995). “Localization of aortic disease is associated with intrinsic differences in aortic structure”. J. Surg. Res. 59 (1): 17–22. doi:10.1006/jsre.1995.1126. PMID 7630123.
- ↑ Steed MM, Tyagi SC (October 2011). “Mechanisms of cardiovascular remodeling in hyperhomocysteinemia”. Antioxid. Redox Signal. 15 (7): 1927–43. doi:10.1089/ars.2010.3721. PMC 3159179. PMID 21126196.
- ↑ Zhou J, Austin RC (2009). “Contributions of hyperhomocysteinemia to atherosclerosis: Causal relationship and potential mechanisms”. Biofactors. 35 (2): 120–9. doi:10.1002/biof.17. PMID 19449439.
- ↑ Steed MM, Tyagi N, Sen U, Schuschke DA, Joshua IG, Tyagi SC (September 2010). “Functional consequences of the collagen/elastin switch in vascular remodeling in hyperhomocysteinemic wild-type, eNOS-/-, and iNOS-/- mice”. Am. J. Physiol. Lung Cell Mol. Physiol. 299 (3): L301–11. doi:10.1152/ajplung.00065.2010. PMC 2951073. PMID 20581102.
- ↑ Dalton ML, Gadson PF, Wrenn RW, Rosenquist TH (July 1997). “Homocysteine signal cascade: production of phospholipids, activation of protein kinase C, and the induction of c-fos and c-myb in smooth muscle cells”. FASEB J. 11 (8): 703–11. doi:10.1096/fasebj.11.8.9240971. PMID 9240971.
- ↑ Jones JA, Barbour JR, Lowry AS, Bouges S, Beck C, McClister DM, Mukherjee R, Ikonomidis JS (December 2006). “Spatiotemporal expression and localization of matrix metalloproteinas-9 in a murine model of thoracic aortic aneurysm”. J. Vasc. Surg. 44 (6): 1314–21. doi:10.1016/j.jvs.2006.07.042. PMC 1761919. PMID 17145436.
- ↑ Rateri DL, Howatt DA, Moorleghen JJ, Charnigo R, Cassis LA, Daugherty A (September 2011). “Prolonged infusion of angiotensin II in apoE(-/-) mice promotes macrophage recruitment with continued expansion of abdominal aortic aneurysm”. Am. J. Pathol. 179 (3): 1542–8. doi:10.1016/j.ajpath.2011.05.049. PMC 3157213. PMID 21763672.
- ↑ Beck L, D’Amore PA (April 1997). “Vascular development: cellular and molecular regulation”. FASEB J. 11 (5): 365–73. PMID 9141503.
- ↑ Gadson PF, Dalton ML, Patterson E, Svoboda DD, Hutchinson L, Schram D, Rosenquist TH (February 1997). “Differential response of mesoderm- and neural crest-derived smooth muscle to TGF-beta1: regulation of c-myb and alpha1 (I) procollagen genes”. Exp. Cell Res. 230 (2): 169–80. doi:10.1006/excr.1996.3398. PMID 9024776.
- ↑ El-Hamamsy I, Yacoub MH (December 2009). “Cellular and molecular mechanisms of thoracic aortic aneurysms”. Nat Rev Cardiol. 6 (12): 771–86. doi:10.1038/nrcardio.2009.191. PMID 19884902.
- ↑ {{cite journal |vauthors=Wrana JL, Attisano L, Wieser R, Ventura F, Massagué J |title=Mechanism of activation of the TGF-beta receptor |journal=Nature |volume=370 |issue=6488 |pages=341–7 |date=August 1994 |pmid=8047140 |doi=10.1038/370341a0 |url=} }
- ↑ Leivonen SK, Chantry A, Hakkinen L, Han J, Kahari VM (November 2002). “Smad3 mediates transforming growth factor-beta-induced collagenase-3 (matrix metalloproteinase-13) expression in human gingival fibroblasts. Evidence for cross-talk between Smad3 and p38 signaling pathways”. J. Biol. Chem. 277 (48): 46338–46. doi:10.1074/jbc.M206535200. PMID 12270924.
- ↑ Kucich U, Rosenbloom JC, Abrams WR, Rosenbloom J (February 2002). “Transforming growth factor-beta stabilizes elastin mRNA by a pathway requiring active Smads, protein kinase C-delta, and p38”. Am. J. Respir. Cell Mol. Biol. 26 (2): 183–8. doi:10.1165/ajrcmb.26.2.4666. PMID 11804868.
- ↑ Kwak HJ, Park MJ, Cho H, Park CM, Moon SI, Lee HC, Park IC, Kim MS, Rhee CH, Hong SI (March 2006). “Transforming growth factor-beta1 induces tissue inhibitor of metalloproteinase-1 expression via activation of extracellular signal-regulated kinase and Sp1 in human fibrosarcoma cells”. Mol. Cancer Res. 4 (3): 209–20. doi:10.1158/1541-7786.MCR-05-0140. PMID 16547158.
- ↑ Kim ES, Kim MS, Moon A (November 2004). “TGF-beta-induced upregulation of MMP-2 and MMP-9 depends on p38 MAPK, but not ERK signaling in MCF10A human breast epithelial cells”. Int. J. Oncol. 25 (5): 1375–82. PMID 15492828.
- ↑ Holm TM, Habashi JP, Doyle JJ, Bedja D, Chen Y, van Erp C, Lindsay ME, Kim D, Schoenhoff F, Cohn RD, Loeys BL, Thomas CJ, Patnaik S, Marugan JJ, Judge DP, Dietz HC (April 2011). “Noncanonical TGFβ signaling contributes to aortic aneurysm progression in Marfan syndrome mice”. Science. 332 (6027): 358–61. doi:10.1126/science.1192149. PMC 3111087. PMID 21493862.
- ↑ Barbour JR, Spinale FG, Ikonomidis JS (May 2007). “Proteinase systems and thoracic aortic aneurysm progression”. J. Surg. Res. 139 (2): 292–307. doi:10.1016/j.jss.2006.09.020. PMID 17292415.
Causes
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Aarti Narayan, M.B.B.S [2] Mohammed Salih, MD. [3]
Overview
Two of the most common causes of thoracic aorta aneurysm are Marfan’s syndrome and atherosclerosis. In some centers, a prior history of dissection with aneurysmal dilation is the most common cause of surgical repair.
Causes
Life Threatening Causes
Life-threatening causes include conditions which may result in death or permanent disability within 24 hours if left untreated.
Common Causes
Causes by Organ System
| Cardiovascular | Aortic dissection, aortic stenosis, aortic valve replacement, aortitis, atherosclerosis, bacterial endocarditis, bicuspid aortic valve, systemic hypertension |
| Chemical / poisoning | No underlying causes |
| Dermatologic | No underlying causes |
| Drug Side Effect | No underlying causes |
| Ear Nose Throat | No underlying causes |
| Endocrine | No underlying causes |
| Environmental | No underlying causes |
| Gastroenterologic | No underlying causes |
| Genetic | Arterial tortuosity syndrome, bicuspid aortic valve, Ehlers-Danlos syndrome, familial thoracic aortic aneurysms and dissections, Loeys-Dietz syndrome, Marfan syndrome, Turner syndrome |
| Hematologic | No underlying causes |
| Iatrogenic | Previous surgery on the aorta |
| Infectious Disease | Aortitis, quaternary syphilis, septic embolism |
| Musculoskeletal / Ortho | No underlying causes |
| Neurologic | No underlying causes |
| Nutritional / Metabolic | No underlying causes |
| Obstetric/Gynecologic | No underlying causes |
| Oncologic | No underlying causes |
| Opthalmologic | No underlying causes |
| Overdose / Toxicity | No underlying causes |
| Psychiatric | No underlying causes |
| Pulmonary | Wegener’s granulomatosis |
| Renal / Electrolyte | No underlying causes |
| Rheum / Immune / Allergy | Ankylosing spondylitis, aortitis, Behcet’s disease, giant cell arteritis, reactive arthritis, rheumatoid arthritis, rheumatoid vasculitis, Takayasu’s arteritis, Wegener’s granulomatosis |
| Sexual | No underlying causes |
| Trauma | Sudden deceleration |
| Urologic | No underlying causes |
| Miscellaneous | No underlying causes |
Causes in Alphabetical Order
- Ankylosing spondylitis
- Aortic dissection
- Aortic stenosis
- Aortitis
- Aortic valve replacement
- Arterial tortuosity syndrome
- Atherosclerosis
- Bacterial infection, often following valvular endocarditis
- Behcet’s disease
- Bicuspid aortic valve
- Ehlers-Danlos syndrome
- Familial thoracic aortic aneurysms and dissections
- Giant cell arteritis
- Loeys-Dietz syndrome
- Marfan’s syndrome
- Quaternary syphilis
- Reactive arthritis
- Rheumatoid arthritis
- Rheumatoid vasculitis
- Septic embolism
- Systemic hypertension
- Takayasu’s arteritis
- Temporal arteritis
- Traumatic – Sudden deceleration
- Turner’s syndrome
- Wegener’s granulomatosis
Causes Based Upon Inherited versus Sporadic versus Syndromic Basis
Sporadic Causes
- Ankylosing spondylitis
- Atherosclerosis
- Bacterial infection, often following valvular endocarditis
- Behcet’s disease[4]
- Giant cell arteritis[5]
- Previous injury to the aorta such as an aortic dissection
- Syphilis[6]
- Takayasu’s arteritis[7]
- Traumatic – sudden deceleration
Familial Causes
- Familial thoracic aortic aneurysms and dissections[8]
- Bicuspid aortic valve with post-stenotic dilation due to turbulence[9]
Syndromic Causes
- Marfan’s syndrome: Aortic root dilation with or without associated aortic regurgitation occurs in 75%-80% of marfan’s patients[10].
- Loeys-Dietz syndrome[11]
- Ehlers-Danlos syndrome
- Turner’s syndrome[12]
References
- ↑ Cheung K, Boodhwani M, Chan KL, Beauchesne L, Dick A, Coutinho T (February 2017). “Thoracic Aortic Aneurysm Growth: Role of Sex and Aneurysm Etiology”. J Am Heart Assoc. 6 (2). doi:10.1161/JAHA.116.003792. PMC 5523737. PMID 28159818.
- ↑ Naidu DP, Quinones JA, Lutschg KW, Balaguru D (August 2017). “Healthy Adolescent with a Mycotic Aortic Aneurysm from Community-Acquired Methicillin-Resistant Staphylococcus aureus”. Tex Heart Inst J. 44 (4): 279–282. doi:10.14503/THIJ-16-5932. PMC 5577956. PMID 28878584.
- ↑ Im KS, Choi MK, Jeon YK, Lee JM (July 2016). “Dissecting thoracic aortic aneurysm associated with tuberculous pleural effusion”. J Thorac Dis. 8 (7): E520–2. doi:10.21037/jtd.2016.05.68. PMC 4958844. PMID 27499987.
- ↑ Zhang SH, Zhang FX (September 2017). “Behcet’s disease with recurrent thoracic aortic aneurysm combined with femoral artery aneurysm: a case report and literature review”. J Cardiothorac Surg. 12 (1): 79. doi:10.1186/s13019-017-0644-y. PMC 5585960. PMID 28874203.
- ↑ Kermani TA, Warrington KJ, Crowson CS, Ytterberg SR, Hunder GG, Gabriel SE, Matteson EL (December 2013). “Large-vessel involvement in giant cell arteritis: a population-based cohort study of the incidence-trends and prognosis”. Ann. Rheum. Dis. 72 (12): 1989–94. doi:10.1136/annrheumdis-2012-202408. PMC 4112513. PMID 23253927.
- ↑ Li W, Yin XJ, Liu HY, Yang R (2016). “Syphilitic aortic aneurysm with a pulmonary lesion: a case report and literature view”. Springerplus. 5 (1): 1725. doi:10.1186/s40064-016-3397-5. PMC 5053956. PMID 27777861.
- ↑ Pan L, Du J, Chen D, Zhao Y, Guo X, Qi G, Wang T, Du J (October 2019). “Takayasu Arteritis with Dyslipidemia Increases Risk of Aneurysm”. Sci Rep. 9 (1): 14083. doi:10.1038/s41598-019-50527-z. PMC 6773689 Check
|pmc=value (help). PMID 31575993. - ↑ Isselbacher EM, Lino Cardenas CL, Lindsay ME (June 2016). “Hereditary Influence in Thoracic Aortic Aneurysm and Dissection”. Circulation. 133 (24): 2516–28. doi:10.1161/CIRCULATIONAHA.116.009762. PMC 5031368. PMID 27297344.
- ↑ Norton E, Yang B (2017). “Managing Thoracic Aortic Aneurysm in Patients with Bicuspid Aortic Valve Based on Aortic Root-Involvement”. Front Physiol. 8: 397. doi:10.3389/fphys.2017.00397. PMC 5469203. PMID 28659818.
- ↑ Pepe G, Giusti B, Sticchi E, Abbate R, Gensini GF, Nistri S (2016). “Marfan syndrome: current perspectives”. Appl Clin Genet. 9: 55–65. doi:10.2147/TACG.S96233. PMC 4869846. PMID 27274304.
- ↑ MacFarlane EG, Parker SJ, Shin JY, Kang BE, Ziegler SG, Creamer TJ, Bagirzadeh R, Bedja D, Chen Y, Calderon JF, Weissler K, Frischmeyer-Guerrerio PA, Lindsay ME, Habashi JP, Dietz HC (February 2019). “Lineage-specific events underlie aortic root aneurysm pathogenesis in Loeys-Dietz syndrome”. J. Clin. Invest. 129 (2): 659–675. doi:10.1172/JCI123547. PMC 6355234. PMID 30614814.
- ↑ Corbitt H, Morris SA, Gravholt CH, Mortensen KH, Tippner-Hedges R, Silberbach M, Maslen CL (October 2018). “TIMP3 and TIMP1 are risk genes for bicuspid aortic valve and aortopathy in Turner syndrome”. PLoS Genet. 14 (10): e1007692. doi:10.1371/journal.pgen.1007692. PMC 6188895. PMID 30281655.
Differentiating Thoracic aortic aneurysm from other Diseases
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Aarti Narayan, M.B.B.S [2] Associate Editor(s)-in-Chief: Mohammed Salih, MD. [3]
Overview
Thoracic aortic aneurysms are often asymptomatic and as a result can be easily missed. If chest pain is present, it is critical to differentiate a thoracic aortic aneurysm with dissection from other potential life-threatening diseases.
Differentiating Thoracic Aortic Aneurysm from other Disorders
- Abdominal aortic aneurysms [1]
- Acute myocardial infarction [2]
- Congestive heart failure
- Aortic regurgitation
- Blunt chest trauma
- Hypertensive emergency
- Hemothorax
- Pneumothorax
- Pericarditis
- Pulmonary embolism
- Cardiac tamponade
- Superior vena cava syndrome
Thoracic aortic aneurysm should be differentiated from other diseases presenting with chest pain, shortness of breath and tachypnea. The differentials include the following:[3][4][5][6][7][8][9][10][11][12][13][14][15][16][17][18][19][20][21][22]
| Diseases | Diagnostic tests | Physical Examination | Symptoms | Past medical history | Other Findings | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| CT scan and MRI | EKG | Chest X-ray | Tachypnea | Tachycardia | Fever | Chest Pain | Hemoptysis | Dyspnea on Exertion | Wheezing | Chest Tenderness | Nasalopharyngeal Ulceration | Carotid Bruit | |||
| Pulmonary embolism |
|
|
|
✔ | ✔ | ✔ (Low grade) | ✔ | ✔ (In case of massive PE) | ✔ | – | – | – | – |
|
|
| Congestive heart failure |
|
✔ | ✔ | ✔ | – | – | ✔ | – | – | – | – |
|
| ||
| Percarditis |
|
|
|
✔ | ✔ | ✔ (Low grade) | ✔ (Relieved by sitting up and leaning forward) | – | ✔ | – | – | – | – |
|
|
| Pneumonia |
|
|
|
✔ | ✔ | ✔ | ✔ | – | ✔ | ✔ | – | – | – |
|
|
| Vasculitis |
|
|
✔ | ✔ | ✔ | ✔ | ✔ | ✔ | – | ✔ | ✔ | ✔ |
|
||
| Chronic obstructive pulmonary disease (COPD) |
|
|
✔ | ✔ | – | – | – | ✔ | ✔ | – | – | – |
|
| |
References
- ↑ Larsson E, Vishnevskaya L, Kalin B, Granath F, Swedenborg J, Hultgren R (2011). “High frequency of thoracic aneurysms in patients with abdominal aortic aneurysms”. Annals of Surgery. 253 (1): 180–4. doi:10.1097/SLA.0b013e3181d96498. PMID 20571364. Unknown parameter
|month=ignored (help) - ↑ Schubert H (2003). “Thoracic aortic dissection: distinguishing it from acute myocardial infarction”. Canadian Family Physician Médecin De Famille Canadien. 49: 583–5. PMC 2214223. PMID 12790268. Unknown parameter
|month=ignored (help) - ↑ Brenes-Salazar JA (2014). “Westermark’s and Palla’s signs in acute and chronic pulmonary embolism: Still valid in the current computed tomography era”. J Emerg Trauma Shock. 7 (1): 57–8. doi:10.4103/0974-2700.125645. PMC 3912657. PMID 24550636.
- ↑ “CT Angiography of Pulmonary Embolism: Diagnostic Criteria and Causes of Misdiagnosis | RadioGraphics”.
- ↑ Bĕlohlávek J, Dytrych V, Linhart A (2013). “Pulmonary embolism, part I: Epidemiology, risk factors and risk stratification, pathophysiology, clinical presentation, diagnosis and nonthrombotic pulmonary embolism”. Exp Clin Cardiol. 18 (2): 129–38. PMC 3718593. PMID 23940438.
- ↑ “Pulmonary Embolism: Symptoms – National Library of Medicine – PubMed Health”.
- ↑ Ramani GV, Uber PA, Mehra MR (2010). “Chronic heart failure: contemporary diagnosis and management”. Mayo Clin. Proc. 85 (2): 180–95. doi:10.4065/mcp.2009.0494. PMC 2813829. PMID 20118395.
- ↑ Blinderman CD, Homel P, Billings JA, Portenoy RK, Tennstedt SL (2008). “Symptom distress and quality of life in patients with advanced congestive heart failure”. J Pain Symptom Manage. 35 (6): 594–603. doi:10.1016/j.jpainsymman.2007.06.007. PMC 2662445. PMID 18215495.
- ↑ Hawkins NM, Petrie MC, Jhund PS, Chalmers GW, Dunn FG, McMurray JJ (2009). “Heart failure and chronic obstructive pulmonary disease: diagnostic pitfalls and epidemiology”. Eur. J. Heart Fail. 11 (2): 130–9. doi:10.1093/eurjhf/hfn013. PMC 2639415. PMID 19168510.
- ↑ Takasugi JE, Godwin JD (1998). “Radiology of chronic obstructive pulmonary disease”. Radiol. Clin. North Am. 36 (1): 29–55. PMID 9465867.
- ↑ Wedzicha JA, Donaldson GC (2003). “Exacerbations of chronic obstructive pulmonary disease”. Respir Care. 48 (12): 1204–13, discussion 1213–5. PMID 14651761.
- ↑ Nakawah MO, Hawkins C, Barbandi F (2013). “Asthma, chronic obstructive pulmonary disease (COPD), and the overlap syndrome”. J Am Board Fam Med. 26 (4): 470–7. doi:10.3122/jabfm.2013.04.120256. PMID 23833163.
- ↑ Khandaker MH, Espinosa RE, Nishimura RA, Sinak LJ, Hayes SN, Melduni RM, Oh JK (2010). “Pericardial disease: diagnosis and management”. Mayo Clin. Proc. 85 (6): 572–93. doi:10.4065/mcp.2010.0046. PMC 2878263. PMID 20511488.
- ↑ Bogaert J, Francone M (2013). “Pericardial disease: value of CT and MR imaging”. Radiology. 267 (2): 340–56. doi:10.1148/radiol.13121059. PMID 23610095.
- ↑ Gharib AM, Stern EJ (2001). “Radiology of pneumonia”. Med. Clin. North Am. 85 (6): 1461–91, x. PMID 11680112.
- ↑ Schmidt WA (2013). “Imaging in vasculitis”. Best Pract Res Clin Rheumatol. 27 (1): 107–18. doi:10.1016/j.berh.2013.01.001. PMID 23507061.
- ↑ Suresh E (2006). “Diagnostic approach to patients with suspected vasculitis”. Postgrad Med J. 82 (970): 483–8. doi:10.1136/pgmj.2005.042648. PMC 2585712. PMID 16891436.
- ↑ Stein PD, Dalen JE, McIntyre KM, Sasahara AA, Wenger NK, Willis PW (1975). “The electrocardiogram in acute pulmonary embolism”. Prog Cardiovasc Dis. 17 (4): 247–57. PMID 123074.
- ↑ Warnier MJ, Rutten FH, Numans ME, Kors JA, Tan HL, de Boer A, Hoes AW, De Bruin ML (2013). “Electrocardiographic characteristics of patients with chronic obstructive pulmonary disease”. COPD. 10 (1): 62–71. doi:10.3109/15412555.2012.727918. PMID 23413894.
- ↑ Stein PD, Matta F, Ekkah M, Saleh T, Janjua M, Patel YR, Khadra H (2012). “Electrocardiogram in pneumonia”. Am. J. Cardiol. 110 (12): 1836–40. doi:10.1016/j.amjcard.2012.08.019. PMID 23000104.
- ↑ Hazebroek MR, Kemna MJ, Schalla S, Sanders-van Wijk S, Gerretsen SC, Dennert R, Merken J, Kuznetsova T, Staessen JA, Brunner-La Rocca HP, van Paassen P, Cohen Tervaert JW, Heymans S (2015). “Prevalence and prognostic relevance of cardiac involvement in ANCA-associated vasculitis: eosinophilic granulomatosis with polyangiitis and granulomatosis with polyangiitis”. Int. J. Cardiol. 199: 170–9. doi:10.1016/j.ijcard.2015.06.087. PMID 26209947.
- ↑ Dennert RM, van Paassen P, Schalla S, Kuznetsova T, Alzand BS, Staessen JA, Velthuis S, Crijns HJ, Tervaert JW, Heymans S (2010). “Cardiac involvement in Churg-Strauss syndrome”. Arthritis Rheum. 62 (2): 627–34. doi:10.1002/art.27263. PMID 20112390.
Epidemiology and Demographics
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Aarti Narayan, M.B.B.S [2] Mohammed Salih, MD. [3]
Overview
Thoracic aortic aneurysms are relatively uncommon (6 to 10 new ones per 100,000 person years) and are less prevalent than abdominal aortic aneurysm. Thoracic aortic aneurysms are generally diagnosed after the sixth and seventh decades of life. Although men are affected 2 to 4 times as often as women, women are at higher risk of rupture by a factor 6.8.
Epidemiology and Demographics
- TAAs are relatively uncommon with an estimated incidence between 6 and 10 new aneurysms per 100,000 person-years. According to a study by Beckerstaff et al.,[1] the incidence of thoracic aortic aneurysms was reported to be 5.3 per 100,000 per year. Another study done by Clouse et al. showed the incidence to be 10.4 per 100,000 per year.[2]
- However, the incidence and prevalence of TAD has been increasing in the past years. The annual number of surgeries performed on the aorta have increased, along with improved post- surgical and long term survival.[3][2]
Age
- TAAs are usually diagnosed after the sixth and seventh decade of life.
Gender
- Males are affected approximately two to four times more often than females.
Race
- Thoracic aortic aneurysm is more common in caucasians.
References
- ↑ Bickerstaff LK, Pairolero PC, Hollier LH; et al. (1982). “Thoracic aortic aneurysms: a population-based study”. Surgery. 92 (6): 1103–8. PMID 7147188. Unknown parameter
|month=ignored (help) - ↑ 2.0 2.1 Clouse WD, Hallett JW, Schaff HV, Gayari MM, Ilstrup DM, Melton LJ (1998). “Improved prognosis of thoracic aortic aneurysms: a population-based study”. JAMA : the Journal of the American Medical Association. 280 (22): 1926–9. PMID 9851478. Unknown parameter
|month=ignored (help) - ↑ Olsson C, Thelin S, Ståhle E, Ekbom A, Granath F (2006). “Thoracic aortic aneurysm and dissection: increasing prevalence and improved outcomes reported in a nationwide population-based study of more than 14,000 cases from 1987 to 2002”. Circulation. 114 (24): 2611–8. doi:10.1161/CIRCULATIONAHA.106.630400. PMID 17145990. Unknown parameter
|month=ignored (help)
Risk Factors
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1] Associate Editor(s)-in-Chief: Mohammed Salih, MD. [2]
Overview
Hypertension and cigarette smoking are the most important risk factors, though the importance of genetic factors in the development of thoracic aortic aneurysm (such as familial thoracic aortic aneurysm; familial aortic dissection) has been increasingly recognized. Approximately 10% of patients may have other family members who have aortic aneurysms. It is also important to note that individuals with a history of aneurysms in other parts of the body have a higher chance of developing a thoracic aortic aneurysm.
Risk Factors
Thoracic aortic aneurysm risk factors include:[1][2][3][4][5][6][7][8]
- Smoking or chewing tobacco
- High blood pressure
- Bicuspid aortic valves
- Atherosclerosis (buildup of plaque in the arteries that can damage the lining)
- Gender: Aortic aneurysms are three times more prevalent in males versus females.
- Race: Aortic aneurysms are more frequent in Caucasian individuals versus other races.
- Individuals who have a family history of aortic aneurysms have a much higher risk of rupture and tend to develop aneurysms at a younger age.
- Chronic obstructive pulmonary disease
- Previous repair of a thoracic aorta aneurysm[9]
- Turners syndrome[10]
References
- ↑ Isselbacher EM (February 2005). “Thoracic and abdominal aortic aneurysms”. Circulation. 111 (6): 816–28. doi:10.1161/01.CIR.0000154569.08857.7A. PMID 15710776.
- ↑ Reed D, Reed C, Stemmermann G, Hayashi T (January 1992). “Are aortic aneurysms caused by atherosclerosis?”. Circulation. 85 (1): 205–11. doi:10.1161/01.cir.85.1.205. PMID 1728451.
- ↑ Tilson MD (January 1992). “Aortic aneurysms and atherosclerosis”. Circulation. 85 (1): 378–9. doi:10.1161/01.cir.85.1.378. PMID 1728475.
- ↑ Bickerstaff LK, Pairolero PC, Hollier LH, Melton LJ, Van Peenen HJ, Cherry KJ, Joyce JW, Lie JT (December 1982). “Thoracic aortic aneurysms: a population-based study”. Surgery. 92 (6): 1103–8. PMID 7147188.
- ↑ Clouse WD, Hallett JW, Schaff HV, Gayari MM, Ilstrup DM, Melton LJ (December 1998). “Improved prognosis of thoracic aortic aneurysms: a population-based study”. JAMA. 280 (22): 1926–9. doi:10.1001/jama.280.22.1926. PMID 9851478.
- ↑ Palmieri V, Bella JN, Arnett DK, Roman MJ, Oberman A, Kitzman DW, Hopkins PN, Paranicas M, Rao DC, Devereux RB (May 2001). “Aortic root dilatation at sinuses of valsalva and aortic regurgitation in hypertensive and normotensive subjects: The Hypertension Genetic Epidemiology Network Study”. Hypertension. 37 (5): 1229–35. doi:10.1161/01.hyp.37.5.1229. PMID 11358933.
- ↑ Prakash SK, Pedroza C, Khalil YA, Milewicz DM (April 2012). “Diabetes and reduced risk for thoracic aortic aneurysms and dissections: a nationwide case-control study”. J Am Heart Assoc. 1 (2). doi:10.1161/JAHA.111.000323. PMC 3487378. PMID 23130125.
- ↑ Thoracic Aortic Disease – Northwestern Memorial Hospital. Thoracic Aortic Aneurysm
- ↑ Lee JJ, Dimick JB, Williams DM, Henke PK, Deeb GM, Eagle KA, Stanley JC, Upchurch GR (October 2003). “Existence of abdominal aortic aneurysms in patients with thoracic aortic dissections”. J. Vasc. Surg. 38 (4): 671–5. doi:10.1016/s0741-5214(03)00727-4. PMID 14560211.
- ↑ Gøtzsche CO, Krag-Olsen B, Nielsen J, Sørensen KE, Kristensen BO (November 1994). “Prevalence of cardiovascular malformations and association with karyotypes in Turner’s syndrome”. Arch. Dis. Child. 71 (5): 433–6. doi:10.1136/adc.71.5.433. PMC 1030059. PMID 7826114.
Screening
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Aarti Narayan, M.B.B.S [2]; Raviteja Guddeti, M.B.B.S. [3] Mohammed Salih, MD. [4]
Overview
Screening for TAA is not recommended in the general population. However, certain population substrates, such as those with history of marfan’s syndrome, turner’s syndrome, ehlers-danlos type IV syndrome, familial thoracic aortic disease syndromes, bicuspid aortic valve, takayasu arteritis, giant cell arteritis, loeys-dietz syndrome or a confirmed genetic mutation known to predispose to aortic aneurysms and aortic dissections (TGFBR1, TGFBR2, FBN1, ACTA2, or MYH11) should have imaging study to screen for TAAs. First-degree relatives of people with thoracic aortic aneurysm or dissection should have aortic imaging to identify asymptomatic disease. Patients with high risk syndromes such as marfan’s syndrome and loeys-dietz syndrome should undergo complete aortic imaging at initial diagnosis and 6 months thereafter to establish if enlargement is occurring.
Screening
Marfan’s Syndrome
People diagnosed with marfan syndrome should immediately have an echocardiogram to measure the aorta, and followed up 6 months later to check for aortic enlargement.[1] Annual imaging is recommended for patients with marfan syndrome if stability of the aortic diameter is documented. If the maximal aortic diameter is 4.5 cm or greater, or if the aortic diameter shows significant growth from baseline, more frequent imaging should be considered (Level of Evidence: C).
Loeys-Dietz Syndrome
Patients with loeys-dietz syndrome or a confirmed genetic mutation known to predispose to aortic aneurysms and aortic dissections (TGFBR1, TGFBR2, FBN1, ACTA2, or MYH11) should undergo complete aortic imaging at initial diagnosis and 6 months thereafter to establish if enlargement is occurring.
Turner’s Syndrome
Patients with turner syndrome should undergo imaging of the heart and aorta for evidence of bicuspid aortic valve, coarctation of the aorta, or dilatation of the ascending thoracic aorta. If initial imaging is normal and there are no risk factors for aortic dissection, repeat imaging should be performed every 5 to 10 years or if otherwise clinically indicated. If abnormalities exist, annual imaging or follow-up imaging should be done.
2010 ACCF/AHA/AATS/ACR/ASA/SCA/SCAI/SIR/STS/SVM Guidelines for the Diagnosis and Management of Patients With Thoracic Aortic Disease (DO NOT EDIT)[2]
Genetic Syndromes (DO NOT EDIT)[2]
| Class I |
| “1. An echocardiogram is recommended at the time of diagnosis of Marfan syndrome to determine the aortic root and ascending aortic diameters and 6 months thereafter to determine the rate of enlargement of the aorta. (Level of Evidence: C)” |
| “2. Annual imaging is recommended for patients with Marfan syndrome if stability of the aortic diameter is documented. If the maximal aortic diameter is 4.5 cm or greater, or if the aortic diameter shows significant growth from baseline, more frequent imaging should be considered. (Level of Evidence: C)” |
| “3. Patients with Loeys-Dietz syndrome or a confirmed genetic mutation known to predispose to aortic aneurysms and aortic dissections (TGFBR1, TGFBR2, FBN1, ACTA2, or MYH11) should undergo complete aortic imaging at initial diagnosis and 6 months thereafter to establish if enlargement is occurring.[3][4][5][6] (Level of Evidence: C)” |
| “4. Patients with Loeys-Dietz syndrome should have yearly magnetic resonance imaging from the cerebrovascular circulation to the pelvis.[7][8][9] (Level of Evidence:B)” |
| “5. Patients with Turner syndrome should undergo imaging of the heart and aorta for evidence of bicuspid aortic valve, coarctation of the aorta, or dilatation of the ascending thoracic aorta.[10] If initial imaging is normal and there are no risk factors for aortic dissection, repeat imaging should be performed every 5 to 10 years or if otherwise clinically indicated. If abnormalities exist, annual imaging or follow-up imaging should be done. (Level of Evidence:C)” |
Genetic Syndromes of Familial Thoracic Aortic Aneurysms and Dissections (DO NOT EDIT)[2]
| Class IIa |
| “1. Sequencing of the ACTA2 gene is reasonable in patients with a family history of thoracic aortic aneurysms and/or dissections to determine if ACTA2 mutations are responsible for the inherited predisposition. (Level of Evidence: B)” |
| Class IIb |
| “1. Sequencing of other genes known to cause familial thoracic aortic aneurysms and/or dissection (TGFBR1, TGFBR2, MYH11) may be considered in patients with a family history and clinical features associated with mutations in these genes. (Level of Evidence: B)” |
| “2. If one or more first-degree relatives of a patient with known thoracic aortic aneurysm and/or dissection are found to have thoracic aortic dilatation, aneurysm, or dissection, then referral to a geneticist may be considered. (Level of Evidence: C)” |
References
- ↑ Hiratzka LF, Bakris GL, Beckman JA; et al. (2010). “2010 ACCF/AHA/AATS/ACR/ASA/SCA/SCAI/SIR/STS/SVM Guidelines for the diagnosis and management of patients with thoracic aortic disease. A Report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines, American Association for Thoracic Surgery, American College of Radiology,American Stroke Association, Society of Cardiovascular Anesthesiologists, Society for Cardiovascular Angiography and Interventions, Society of Interventional Radiology, Society of Thoracic Surgeons,and Society for Vascular Medicine”. J. Am. Coll. Cardiol. 55 (14): e27–e129. doi:10.1016/j.jacc.2010.02.015. PMID 20359588. Unknown parameter
|month=ignored (help) - ↑ 2.0 2.1 2.2 Hiratzka LF, Bakris GL, Beckman JA; et al. (2010). “2010 ACCF/AHA/AATS/ACR/ASA/SCA/SCAI/SIR/STS/SVM guidelines for the diagnosis and management of patients with Thoracic Aortic Disease: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines, American Association for Thoracic Surgery, American College of Radiology, American Stroke Association, Society of Cardiovascular Anesthesiologists, Society for Cardiovascular Angiography and Interventions, Society of Interventional Radiology, Society of Thoracic Surgeons, and Society for Vascular Medicine”. Circulation. 121 (13): e266–369. doi:10.1161/CIR.0b013e3181d4739e. PMID 20233780. Unknown parameter
|month=ignored (help) - ↑ Pearson GD, Devereux R, Loeys B, Maslen C, Milewicz D, Pyeritz R; et al. (2008). “Report of the National Heart, Lung, and Blood Institute and National Marfan Foundation Working Group on research in Marfan syndrome and related disorders”. Circulation. 118 (7): 785–91. doi:10.1161/CIRCULATIONAHA.108.783753. PMC 2909440. PMID 18695204.
- ↑ Svensson LG, Crawford ES, Coselli JS, Safi HJ, Hess KR (1989). “Impact of cardiovascular operation on survival in the Marfan patient”. Circulation. 80 (3 Pt 1): I233–42. PMID 2766531.
- ↑ Svensson LG, Blackstone EH, Feng J, de Oliveira D, Gillinov AM, Thamilarasan M; et al. (2007). “Are Marfan syndrome and marfanoid patients distinguishable on long-term follow-up?”. Ann Thorac Surg. 83 (3): 1067–74. doi:10.1016/j.athoracsur.2006.10.062. PMID 17307461.
- ↑ Zhu L, Vranckx R, Khau Van Kien P, Lalande A, Boisset N, Mathieu F; et al. (2006). “Mutations in myosin heavy chain 11 cause a syndrome associating thoracic aortic aneurysm/aortic dissection and patent ductus arteriosus”. Nat Genet. 38 (3): 343–9. doi:10.1038/ng1721. PMID 16444274.
- ↑ LeMaire SA, Pannu H, Tran-Fadulu V, Carter SA, Coselli JS, Milewicz DM (2007). “Severe aortic and arterial aneurysms associated with a TGFBR2 mutation”. Nat Clin Pract Cardiovasc Med. 4 (3): 167–71. doi:10.1038/ncpcardio0797. PMC 2561071. PMID 17330129.
- ↑ Loeys BL, Schwarze U, Holm T, Callewaert BL, Thomas GH, Pannu H; et al. (2006). “Aneurysm syndromes caused by mutations in the TGF-beta receptor”. N Engl J Med. 355 (8): 788–98. doi:10.1056/NEJMoa055695. PMID 16928994.
- ↑ Williams JA, Loeys BL, Nwakanma LU, Dietz HC, Spevak PJ, Patel ND; et al. (2007). “Early surgical experience with Loeys-Dietz: a new syndrome of aggressive thoracic aortic aneurysm disease”. Ann Thorac Surg. 83 (2): S757–63, discussion S785-90. doi:10.1016/j.athoracsur.2006.10.091. PMID 17257922.
- ↑ Bondy CA, Turner Syndrome Study Group (2007). “Care of girls and women with Turner syndrome: a guideline of the Turner Syndrome Study Group”. J Clin Endocrinol Metab. 92 (1): 10–25. doi:10.1210/jc.2006-1374. PMID 17047017.
Natural History, Complications and Prognosis
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Aarti Narayan, M.B.B.S [2] Mohammed Salih, MD. [3]
Overview
Thoracic aortic aneurysms typically expand slowly at a rate of approximately 0.1-0.2 cm/year. Aortic dissection and aortic rupture are the two most feared complications of an aortic aneurysm. The five-year survival of patients with a thoracic aortic aneurysm is 56%. The following are associated with a poorer prognosis: the presence of diastolic dysfunction; trauma as a cause of the aneurysm; the presence of coronary artery disease and the presence of carotid artery disease.
Natural History
Thoracic aneurysms enlarge at a more rapid rate than abdominal aneurysms (0.42 vs 0.28 cm/yr), with aneurysms of the aortic arch growing at ~ 0.56 cm/yr. Aneurysms that are 5-6 cm in diameter have a faster rate of growth and a greater tendency to rupture than smaller ones.[1]
Complications
Dissection
- Aortic dissection and aortic rupture are the two most feared complications of an aortic aneurysm. Patients who have a prior dissection as a cause of an aneurysm are at increased risk of rapid expansion and re-dissection of the aneurysm.[2][3][4][5][6][7]
- Aortic regurgitation
- Congestive heart failure
Shown below is the annual risk of thoracic aortic rupture, dissection or death for different diameters of thoracic aortic aneurysms. This draft forms the basis for performing surgery when the aorta is 5.0 to 6 cm in diameter depending upon whether the patient has Marfan syndrome or not.

Prognosis
The five-year survival of patients with a thoracic aortic aneurysm is 56%. The principal causes of death due to thoracic aneurysmal disease are dissection and rupture. Women face a 6.8 fold higher risk of aortic rupture. Once rupture occurs, the mortality rate is 50–80%. Most deaths in patients with the Marfan syndrome are the result of aortic disease. It is estimated that up to 47,000 people die each year from all types of aortic disease (thoracic and abdominal aortic aneurysms combined)[8][9].
Factors associated with a worse prognosis are:
- Diastolic dysfunction
- Traumatic aneurysm
- Associated coronary artery disease
- Carotid artery disease
References
- ↑ Gillum RF (November 1995). “Epidemiology of aortic aneurysm in the United States”. J Clin Epidemiol. 48 (11): 1289–98. doi:10.1016/0895-4356(95)00045-3. PMID 7490591.
- ↑ Clouse WD, Hallett JW, Schaff HV, Gayari MM, Ilstrup DM, Melton LJ (December 1998). “Improved prognosis of thoracic aortic aneurysms: a population-based study”. JAMA. 280 (22): 1926–9. doi:10.1001/jama.280.22.1926. PMID 9851478.
- ↑ Juvonen T, Ergin MA, Galla JD, Lansman SL, Nguyen KH, McCullough JN, Levy D, de Asla RA, Bodian CA, Griepp RB (June 1997). “Prospective study of the natural history of thoracic aortic aneurysms”. Ann. Thorac. Surg. 63 (6): 1533–45. doi:10.1016/s0003-4975(97)00414-1. PMID 9205145.
- ↑ Coady MA, Rizzo JA, Hammond GL, Kopf GS, Elefteriades JA (June 1999). “Surgical intervention criteria for thoracic aortic aneurysms: a study of growth rates and complications”. Ann. Thorac. Surg. 67 (6): 1922–6, discussion 1953–8. doi:10.1016/s0003-4975(99)00431-2. PMID 10391339.
- ↑ Kim JB, Kim K, Lindsay ME, MacGillivray T, Isselbacher EM, Cambria RP, Sundt TM (October 2015). “Risk of rupture or dissection in descending thoracic aortic aneurysm”. Circulation. 132 (17): 1620–9. doi:10.1161/CIRCULATIONAHA.114.015177. PMID 26338955.
- ↑ Yiu RS, Cheng SW (May 2016). “Natural history and risk factors for rupture of thoracic aortic arch aneurysms”. J. Vasc. Surg. 63 (5): 1189–94. doi:10.1016/j.jvs.2015.12.043. PMID 26926929.
- ↑ Geisbüsch S, Stefanovic A, Schray D, Oyfe I, Lin HM, Di Luozzo G, Griepp RB (January 2014). “A prospective study of growth and rupture risk of small-to-moderate size ascending aortic aneurysms”. J. Thorac. Cardiovasc. Surg. 147 (1): 68–74. doi:10.1016/j.jtcvs.2013.06.030. PMID 23953716.
- ↑ Davies RR, Goldstein LJ, Coady MA, Tittle SL, Rizzo JA, Kopf GS, Elefteriades JA (January 2002). “Yearly rupture or dissection rates for thoracic aortic aneurysms: simple prediction based on size”. Ann. Thorac. Surg. 73 (1): 17–27, discussion 27–8. doi:10.1016/s0003-4975(01)03236-2. PMID 11834007.
- ↑ Knipp BS, Deeb GM, Prager RL, Williams CY, Upchurch GR, Patel HJ (October 2007). “A contemporary analysis of outcomes for operative repair of type A aortic dissection in the United States”. Surgery. 142 (4): 524–8, discussion 528.e1. doi:10.1016/j.surg.2007.07.012. PMID 17950344.
Diagnosis
Diagnosis
History and Symptoms | Physical Examination | General Approach to Imaging in Thoracic Aortic Aneurysm | Chest X Ray | MRI | CT | Echocardiography
Treatment
Treatment
Medical Therapy | Surgery | Endovascular Stent Grafting | Secondary Prevention | Lifestyle Changes
Looking for the patient version?
© 2026 MyEClinic – IFTM Institut für Telematik in der Medizin GmbH