
Ependymoma
For patient information, click here
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1] Associate Editor(s)-in-Chief: Ahmad Al Maradni, M.D. [2]
Synonyms and keywords: Cellular ependymoma; Clear cell ependymoma; Ependymal tumor; Papillary ependymoma; Tanycytic ependymoma; Ependymal cell tumor; Ependymal neoplasm
Overview
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1] Associate Editor(s)-in-Chief: Ahmad Al Maradni, M.D. [2]
Overview
Ependymoma is the third most common neuroepithelial tumor of the central nervous system (CNS) in childhood. It arises for ependymal cells of the central nervous system and is dominated by intracranial mass. The World Health Organization (WHO) classification of CNS tumors defines several histopathological variants of ependymoma (grade I, II, III). On gross pathology, a well-encapsulated tumor arises from the floor of the fourth ventricle, situated in the lower back portion of the brain is a characteristic finding of ependymoma. On microscopic histopathological analysis, perivascular pseudorosettes are characteristic findings of ependymoma. Development of ependymoma is the result of multiple genetic mutations (ERBB2, ERBB4, MMP2, MMP14, NOTCH1, and MEN1). There are no established causes for ependymomas. Ependymoma must be differentiated from medulloblastoma, choroid plexus papilloma, and glioblastoma. Common risk factors in the development of ependymoma are children with certain hereditary diseases (neurofibromatosis type II and Turcot syndrome), ERBB2, ERBB4, and human telomerase reverse transcriptase TERT gene expression, over-expression of kinetochore proteins, and down-regulation of metallothioneins.Symptoms of ependymoma include headache, nausea, vomiting, blurry or double vision, drowsiness (after several hours of the above symptoms), irritability, ataxia, neck pain, cranial nerve palsies, seizures, focal neurologic deficits, back pain, lower extremity weakness, bowel and bladder dysfunction. MRI may be diagnostic of ependymoma. Finding on brain MRI suggestive of ependymoma include large mixed cystic/solid lesion with haemorrhage and fluid which may indicate areas of necrosis. The predominant therapy for ependymoma is surgical resection. Adjunctive chemoradiation may be required.
Classification
Ependymoma may be classified into several subtypes based on WHO classification (grade I, II, III) and the site of origin.
Pathology
On gross pathology, a well-encapsulated tumor arises from the floor of the fourth ventricle, situated in the lower back portion of the brain is a characteristic finding of ependymoma. On microscopic histopathological analysis, perivascular pseudorosettes are characteristic findings of ependymoma. Development of ependymoma is the result of multiple genetic mutations (ERBB2, ERBB4, MMP2, MMP14, NOTCH1, and MEN1).
Causes
There are no established causes for ependymomas.
Epidemiology and Demographics
The incidence of ependymoma is approximately 0.05 to 0.08 per 100,000 individuals in the United States.[1]The posterior fossa tumours tend to present more commonly in the paediatric age group (mean age at diagnosis is 6 years of age). Men and women are affected equally by ependymomal tumors.
Risk Factors
Common risk factors in the development of ependymoma are children with certain hereditary diseases (neurofibromatosis type II and Turcot syndrome), over-expression of kinetochore proteins, and down-regulation of metallothioneins.
Differentiating Ependymoma from other Diseases
Ependymoma must be differentiated from medulloblastoma, choroid plexus papilloma, and glioblastoma.
Natural History, Complication and Prognosis
If left untreated, patients with ependymoma may progress to develop nausea, vomiting, headache, and irritability. Common complications of ependymoma include seizure, hydrocephalus, muscle paralysis, and speech problems.
Diagnosis
History and Symptoms
Symptoms of ependymoma include headache, nausea, and irritability.
Physical Examination
Patients with ependymoma usually appear well. Physical examination of patients with ependymoma is usually remarkable for altered mental status, spasticity, and muscle weakness.
Staging
There is no established system for the staging of ependymoma.
Laboratory Findings
There are no diagnostic lab findings associated with ependymoma.
CT
Head CT scan may be diagnostic of ependymoma. Findings on CT scan suggestive of ependymoma include heterogeneous mass with coarse calcification, solid component, and cystic component.
MRI
Brain MRI may be diagnostic of ependymoma. Finding on brain MRI suggestive of ependymoma include large mixed cystic/solid lesion with haemorrhage and fluid which may indicate areas of necrosis.
Ultrasound
Intraoperative ultrasound is used in intradural spinal ependymomas.
Other Diagnostic Studies
Other diagnostic studies for ependymoma include EEG, which demonstrates various abnormalities, and cerebrospinal fluid analysis, which demonstrates positive cytology.
Treatment
Medical Therapy
The predominant therapy for ependymoma is surgical resection. Adjunctive chemoradiation may be required.
Surgery
Surgery is the main stay of treatment for myxopapillary ependymoma (WHO grade 1), subependymoma (WHO grade 1), ependymoma (WHO grade I), and anaplastic ependymoma (WHO grade III).
Primary Prevention
There are no primary preventive measures available for ependymoma.
Secondary Prevention
Secondary prevention strategies following ependymoma include regular clinical assessment and neuroimaging.
References
- ↑ National Cancer Institute. Physician Data Query Database 2015. http://www.cancer.gov/publications/pdq
Historical Perspective
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief:
Overview
Historical Perspective
Discovery
- There is limited information about the historical perspective of [disease name].
OR
- [Disease name] was first discovered by [name of scientist], a [nationality + occupation], in [year]/during/following [event].
- The association between [important risk factor/cause] and [disease name] was made in/during [year/event].
- In [year], [scientist] was the first to discover the association between [risk factor] and the development of [disease name].
- In [year], [gene] mutations were first implicated in the pathogenesis of [disease name].
Landmark Events in the Development of Treatment Strategies
Impact on Cultural History
Famous Cases
The following are a few famous cases of [disease name]:
References
Classification
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]Associate Editor(s)-in-Chief: Ahmad Al Maradni, M.D. [2]
Overview
Ependymoma may be classified into several subtypes based on WHO classification (grade I, II, III) and the site of origin.
Classification
- In the most recent World Health Organization (WHO) classification of brain tumors, ependymal tumors are classified into the following four main subtypes:[1][2]
- Subependymoma (WHO grade I): a subependymoma is a slow-growing neoplasm, usually attached to the ventricle wall and is composed of glial tumor cell clusters ingrained in a fibrillary matrix.[3]
- Myxopapillary ependymoma (WHO grade I): a myxopapillary ependymoma arises almost exclusively in the location of the conus medullaris, cauda equina, and filum terminale of the spinal cord and is characterized histologically by tumor cells arranged in a papillary manner around vascularized myxoid stromal cores.[4]
- Ependymoma (WHO grade II): the ependymoma, which is considered a grade II neoplasm originating from the walls of the ventricles or from the spinal canal, is composed of neoplastic ependymal cells. Ependymomas are subdivided, based on histological findings, into the following four subtypes[5]:
- Cellular ependymoma: the most common subtype, this subtype usually demonstrates significant cellularity without an increase in mitotic activity[6].
- Papillary ependymoma: forms linear, epithelial-like surfaces along cerebrospinal fluid.
- Clear cell ependymoma: displays an oligodendroglial-like appearance with perinuclear halos, this variant is preferentially located in the supratentorial compartment of the brain[7].
- Tanycytic ependymoma: the rarest form of grade II ependymoma, this subtype is most commonly found in the spinal cord; tumor cells are arranged in fascicles of variable width and cell density and are poorly intertwined[8].
- Anaplastic ependymoma (WHO grade III): also known as malignant ependymoma. An anaplastic ependymoma is considered a malignant glioma of ependymal differentiation and, compared with the grade II ependymomas, shows increased cellularity and increased mitotic activity. It is often associated with microvascular proliferation and necrosis[9].
- Supratentorial ependymomas[11]
- Infratentorial ependymomas[12]
- Spinal cord ependymomas[13]
References
- ↑ Louis DN, Ohgaki H, Wiestler OD, et al., eds.: WHO Classification of Tumours of the Central Nervous System. 4th ed. Lyon, France: IARC Press, 2007.
- ↑ 2.0 2.1 Eoendymoma. http://www.cancer.gov/types/brain/hp/child-ependymoma-treatment-pdq#section/_35 URL Accessed on 10 6 2015.
- ↑ Huang Y (2015). “Subependymoma with extensive microcystic transformation: a case report”. Int J Clin Exp Pathol. 8 (2): 2191–4. PMC 4396238. PMID 25973126.
- ↑ Weber DC, Wang Y, Miller R, Villà S, Zaucha R, Pica A; et al. (2015). “Long-term outcome of patients with spinal myxopapillary ependymoma: treatment results from the MD Anderson Cancer Center and institutions from the Rare Cancer Network”. Neuro Oncol. 17 (4): 588–95. doi:10.1093/neuonc/nou293. PMC 4483075. PMID 25301811.
- ↑ Grier JT, Batchelor T (2006). “Low-grade gliomas in adults”. Oncologist. 11 (6): 681–93. doi:10.1634/theoncologist.11-6-681. PMID 16794247.
- ↑ Wu J, Armstrong TS, Gilbert MR (2016). “Biology and management of ependymomas”. Neuro Oncol. 18 (7): 902–13. doi:10.1093/neuonc/now016. PMC 4896548. PMID 27022130.
- ↑ Lee BH, Kwon JT, Park YS (2011). “Supratentorial clear cell ependymoma mimicking oligodendroglioma : case report and review of the literature”. J Korean Neurosurg Soc. 50 (3): 240–3. doi:10.3340/jkns.2011.50.3.240. PMC 3218185. PMID 22102956.
- ↑ Tomek M, Jayajothi A, Brandner S, Jaunmuktane Z, Lee CH, Davagnanam I (2016). “Imaging features of spinal tanycytic ependymoma”. Neuroradiol J. 29 (1): 61–5. doi:10.1177/1971400915621322. PMC 4978340. PMID 26755489.
- ↑ Sarıkafa Ş, Çelik SE, Yarikkaya E, Sayılgan A (2015). “Malignant Transformation of Grade II Ependymoma in a 2-Year-Old Child: Case Report”. J Neurol Surg Rep. 76 (1): e151–5. doi:10.1055/s-0035-1549311. PMC 4520988. PMID 26251794.
- ↑ Andreiuolo F, Puget S, Peyre M, Dantas-Barbosa C, Boddaert N, Philippe C; et al. (2010). “Neuronal differentiation distinguishes supratentorial and infratentorial childhood ependymomas”. Neuro Oncol. 12 (11): 1126–34. doi:10.1093/neuonc/noq074. PMC 3098029. PMID 20615923.
- ↑ Mangalore S, Aryan S, Prasad C, Santosh V (2015). “Imaging characteristics of supratentorial ependymomas: Study on a large single institutional cohort with histopathological correlation”. Asian J Neurosurg. 10 (4): 276–81. doi:10.4103/1793-5482.162702. PMC 4558802. PMID 26425155.
- ↑ Mandera M, Makarska J, Sobol G, Musioł K (2015). “Infratentorial ependymomas–a study of the centre in Katowice”. Childs Nerv Syst. 31 (7): 1089–96. doi:10.1007/s00381-015-2683-9. PMC 4493855. PMID 25822933.
- ↑ Armstrong TS, Vera-Bolanos E, Bekele BN, Aldape K, Gilbert MR (2010). “Adult ependymal tumors: prognosis and the M. D. Anderson Cancer Center experience”. Neuro Oncol. 12 (8): 862–70. doi:10.1093/neuonc/noq009. PMC 2940672. PMID 20511182.
Pathophysiology
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [2] Associate Editor(s)-in-Chief: Ahmad Al Maradni, M.D. [3]
Overview
On gross pathology, a well-encapsulated tumor which arises from the floor of the fourth ventricle, situated in the lower back portion of the brain is a characteristic finding of ependymoma. On microscopic histopathological analysis, perivascular pseudorosettes are characteristic findings of ependymoma. Development of ependymoma is the result of multiple genetic mutations (ERBB2, ERBB4, MMP2, MMP14, NOTCH1, and MEN1).[1]
Genetics
- One expression-defined group occurs primarily in young children and is characterized by a largely balanced genomic profile with an increased occurrence of chromosome 1q and proteins such as tenascin C and epidermal growth factor receptor.[2][3][4][5][6][7][8]
- The second expression-defined group occurs primarily in older children and adults and is characterized by a numerous cytogenetic abnormalities involving the whole chromosome or chromosomal arms.[9]
- Genes involved in ependymoma formation and progression are:[10]
- ERBB2
- ERBB4
- Human telomerase reverse transcriptase TERT
- KIT receptor tyrosine kinase and phospho-KIT receptor expression is associated with tumor progression
- MMP2 and MMP14 mutations appear to also play a role in tumor growth and progression in intracranial cases.
- NOTCH1 mutations have been found in approximately 8% of pediatric ependymomas
- MEN1 mutations are occasionally found in pediatric ependymomas.
- TPR and CHIBBY mutations have been identified in pediatric ependymomas.
- S100A6 and S100A4 on chromosome 1q have also been found to correspond to supratentorial tumor development and tumors occurring before the age of 3 years.
Associated Conditions
- The subependymal giant-cell astrocytoma, also called giant-cell glioma, is typically associated with tuberous sclerosis but can occur independently.
Pathology
- Ependymomas represent a relatively broad group of glial tumors which share common origin from differentiated ependymal cells lining the ventricles of the brain or the central canal of the spinal cord. They account for 5% of all neuroepithelial neoplasms.
- Ependymomas can occur anywhere, but certain location are typical. Common locations include:
- Floor of the fourth ventricle (common location in children)
- Spinal cord ependymoma
- Myxopapillary ependymoma (conus medullaris)
- Supratentorial ependymoma
- The subependymomas, variant of the ependymoma, arise in the fourth ventricle but may occur in the septum pellucidum and the cervical spinal cord.
Gross Pathology
- Ependymomas are well-encapsulated tumors which usually arise from the floor of the fourth ventricle.
-
![Fourth ventricle ependymomas frequently extend out of the ventricle into the subarachnoid space.[11]](https://www.wikidoc.org/images/0/0f/Epyndemomas_gross.jpg) Fourth ventricle ependymomas frequently extend out of the ventricle into the subarachnoid space.[11]
Fourth ventricle ependymomas frequently extend out of the ventricle into the subarachnoid space.[11]
![Fourth ventricle ependymomas frequently extend out of the ventricle into the subarachnoid space.[11]](https://www.wikidoc.org/index.php/File%3AEpyndemomas_gross.jpg)
Microscopic Pathology
- Ependymomas are composed of cells with regular, round to oval nuclei. There is a variably dense fibrillary background.
- Tumor cells may form gland-like round or elongated structures that resemble the embryologic ependymal canal, with long, delicate processes extending into the lumen; more frequently present are perivascular pseudorosettes in which tumor cells are arranged around vessels with an intervening zone consisting of thin ependymal processes directed toward the wall of the vessel.[1]
- Ependymal rosettes are rare but pathognomonic feature.
-
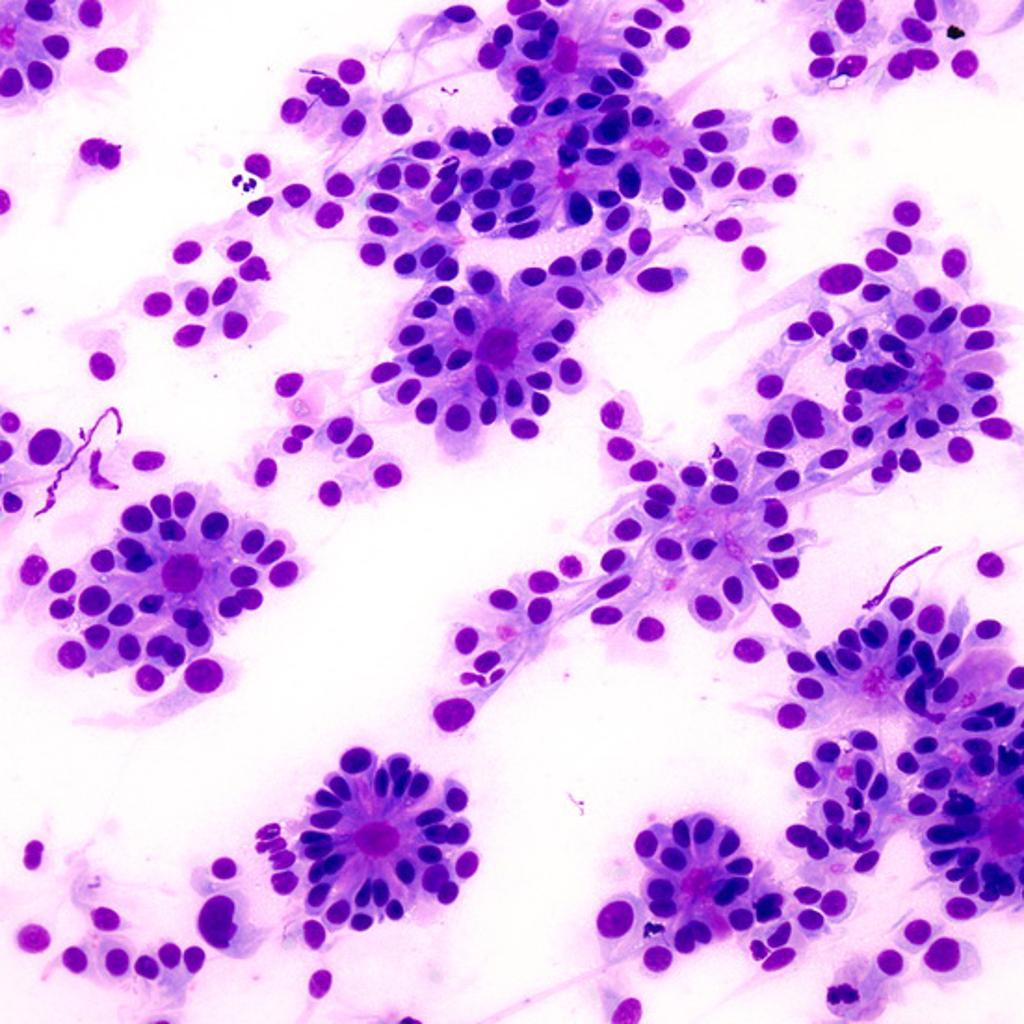
![Micrograph of an ependymoma. H&E stain show pseudoressettes pattern of ependymal cells.[12]](https://www.wikidoc.org/images/0/0a/532px-Ependymoma_low_intermed_mag.jpg) Micrograph of an ependymoma. H&E stain show pseudoressettes pattern of ependymal cells.[12]
Micrograph of an ependymoma. H&E stain show pseudoressettes pattern of ependymal cells.[12] -
 True ependymal rosette consisting of tumor cells arranged around well-defined lumens forming gland-like structures.<ref name=radiopaedia> Image courtesy of Dr Dharam RamnaniRadiopaedia (original file
True ependymal rosette consisting of tumor cells arranged around well-defined lumens forming gland-like structures.<ref name=radiopaedia> Image courtesy of Dr Dharam RamnaniRadiopaedia (original file -
![Higher magnification of one of the true ependymal rosettes showing a collar of cells around a central lumen forming a gland-like structure.[13]](https://www.wikidoc.org/images/b/b6/Ependymoma-true-ependymal-rosettes123.jpg) Higher magnification of one of the true ependymal rosettes showing a collar of cells around a central lumen forming a gland-like structure.[13]
Higher magnification of one of the true ependymal rosettes showing a collar of cells around a central lumen forming a gland-like structure.[13]
![Micrograph of an ependymoma. H&E stain show pseudoressettes pattern of ependymal cells.[12]](https://www.wikidoc.org/index.php/File%3A532px-Ependymoma_low_intermed_mag.jpg)

![Higher magnification of one of the true ependymal rosettes showing a collar of cells around a central lumen forming a gland-like structure.[13]](https://www.wikidoc.org/index.php/File%3AEpendymoma-true-ependymal-rosettes123.jpg)
References
- ↑ 1.0 1.1 Kumar, et al. (2005). The Central Nervous System. Pathologic Basis of Disease. 7th Edition. Philadelphia: Elsevier Saunders.
- ↑ Korshunov A, Golanov A, Timirgaz V (2000). “Immunohistochemical markers for intracranial ependymoma recurrence. An analysis of 88 cases”. J Neurol Sci. 177 (1): 72–82. PMID 10967185.
- ↑ Mendrzyk F, Korshunov A, Benner A, Toedt G, Pfister S, Radlwimmer B; et al. (2006). “Identification of gains on 1q and epidermal growth factor receptor overexpression as independent prognostic markers in intracranial ependymoma”. Clin Cancer Res. 12 (7 Pt 1): 2070–9. doi:10.1158/1078-0432.CCR-05-2363. PMID 16609018.
- ↑ Mohankumar KM, Currle DS, White E, Boulos N, Dapper J, Eden C; et al. (2015). “An in vivo screen identifies ependymoma oncogenes and tumor-suppressor genes”. Nat Genet. 47 (8): 878–87. doi:10.1038/ng.3323. PMC 4520751. PMID 26075792.
- ↑ Abedalthagafi MS, Wu MP, Merrill PH, Du Z, Woo T, Sheu SH; et al. (2016). “Decreased FOXJ1 expression and its ciliogenesis programme in aggressive ependymoma and choroid plexus tumours”. J Pathol. 238 (4): 584–97. doi:10.1002/path.4682. PMC 5364032. PMID 26690880.
- ↑ Georgescu MM, Yell P, Mobley BC, Shang P, Georgescu T, Wang SH; et al. (2015). “NHERF1/EBP50 is an organizer of polarity structures and a diagnostic marker in ependymoma”. Acta Neuropathol Commun. 3: 11. doi:10.1186/s40478-015-0197-z. PMC 4352254. PMID 25775275.
- ↑ Andreiuolo F, Le Teuff G, Bayar MA, Kilday JP, Pietsch T, von Bueren AO; et al. (2017). “Integrating Tenascin-C protein expression and 1q25 copy number status in pediatric intracranial ependymoma prognostication: A new model for risk stratification”. PLoS One. 12 (6): e0178351. doi:10.1371/journal.pone.0178351. PMC 5472261. PMID 28617804.
- ↑ Araki A, Chocholous M, Gojo J, Dorfer C, Czech T, Heinzl H; et al. (2016). “Chromosome 1q gain and tenascin-C expression are candidate markers to define different risk groups in pediatric posterior fossa ependymoma”. Acta Neuropathol Commun. 4 (1): 88. doi:10.1186/s40478-016-0349-9. PMC 4994287. PMID 27550150.
- ↑ Wani K, Armstrong TS, Vera-Bolanos E, Raghunathan A, Ellison D, Gilbertson R; et al. (2012). “A prognostic gene expression signature in infratentorial ependymoma”. Acta Neuropathol. 123 (5): 727–38. doi:10.1007/s00401-012-0941-4. PMC 4013829. PMID 22322993.
- ↑ Zakrzewska M, Fendler W, Zakrzewski K, Sikorska B, Grajkowska W, Dembowska-Bagińska B; et al. (2016). “Altered MicroRNA Expression Is Associated with Tumor Grade, Molecular Background and Outcome in Childhood Infratentorial Ependymoma”. PLoS One. 11 (7): e0158464. doi:10.1371/journal.pone.0158464. PMC 4938415. PMID 27390862.
- ↑ EPENDYMOMA. http://librepathology.org/wiki/index.php/File:AFIP405713G-EPENDYMOMA.jpg 2015. URL Accessed on 10 6, 2015
- ↑ Ependymoma. https://en.wikipedia.org/wiki/Ependymoma#/media/File:Ependymoma_low_intermed_mag.jpg. URL Accessed on 10 6, 2015
- ↑ Image courtesy of Dr Dharam RamnaniRadiopaedia (original filehere). [1] CreativeCommons BY-SANC
Causes
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1] Associate Editor(s)-in-Chief: Ahmad Al Maradni, M.D. [2]
Overview
There are no established causes for ependymomas.
Causes
There are no established causes for ependymomas.
References
Epidemiology and Demographics
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1] Associate Editor(s)-in-Chief: Ahmad Al Maradni, M.D. [2]
Overview
The incidence of ependymoma is approximately 0.05 to 0.08 per 100,000 individuals in the United States.[1] The posterior fossa tumours tend to present more commonly in the paediatric age group (mean age at diagnosis is 6 years of age). Male and female are affected equally by ependymomal tumors.
Epidemiology and Demographics
Incidence
- The incidence of ependymoma is approximately 0.05 to 0.08 per 100,000 individuals in the United States.[1]
Age
- The posterior fossa tumors tend to present more commonly among the paediatric age group (mean age at diagnosis is 6 years of age).
- Subependymoma usually affects people older than 40 years of age.
Gender
- Males and females are affected equally by ependymomal tumors.
- Subependymoma more often affects men than women.
References
- ↑ 1.0 1.1 National Cancer Institute. Physician Data Query Database 2015. http://www.cancer.gov/publications/pdq
Risk Factors
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1] Associate Editor(s)-in-Chief: Ahmad Al Maradni, M.D. [2]
Overview
The incidence of ependymoma is approximately 0.05 to 0.08 per 100,000 individuals in the United States.[1] The posterior fossa tumours tend to present more commonly in the paediatric age group (mean age at diagnosis is 6 years of age). Male and female are affected equally by ependymomal tumors.
Epidemiology and Demographics
Incidence
- The incidence of ependymoma is approximately 0.05 to 0.08 per 100,000 individuals in the United States.[1]
Age
- The posterior fossa tumors tend to present more commonly among the paediatric age group (mean age at diagnosis is 6 years of age).
- Subependymoma usually affects people older than 40 years of age.
Gender
- Males and females are affected equally by ependymomal tumors.
- Subependymoma more often affects men than women.
References
- ↑ 1.0 1.1 National Cancer Institute. Physician Data Query Database 2015. http://www.cancer.gov/publications/pdq
Differentiating Ependymoma from other Diseases
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Fahimeh Shojaei, M.D.
Overview
On the basis of seizure, visual disturbance, and constitutional symptoms, ependymoma must be differentiated from oligodendroglioma, meningioma, hemangioblastoma, pituitary adenoma, schwannoma, primary CNS lymphoma, medulloblastoma, astrocytoma, craniopharyngioma, pinealoma, AV malformation, brain aneurysm, bacterial brain abscess, tuberculosis, toxoplasmosis, hydatid cyst, CNS cryptococcosis, CNS aspergillosis, and brain metastasis.
Differentiating ependymoma from other Diseases
Differentiating ependymoma from other diseases on the basis of seizure, visual disturbance, and constitutional symptoms
On the basis of seizure, visual disturbance, and constitutional symptoms, ependymoma must be differentiated from oligodendroglioma, meningioma, hemangioblastoma, pituitary adenoma, schwannoma, primary CNS lymphoma, medulloblastoma, astrocytoma, craniopharyngioma, pinealoma, AV malformation, brain aneurysm, bacterial brain abscess, tuberculosis, toxoplasmosis, hydatid cyst, CNS cryptococcosis, CNS aspergillosis, and brain metastasis.
| Diseases | Clinical manifestations | Para-clinical findings | Gold standard |
Additional findings | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Symptoms | Physical examination | |||||||||
| Lab Findings | MRI | Immunohistopathology | ||||||||
| Head- ache |
Seizure | Visual disturbance | Constitutional | Focal neurological deficit | ||||||
| Childhood primary brain tumors | ||||||||||
| Ependymoma [1][2] |
+ | +/− | +/− | − | + | − |
|
|
| |
| Pilocytic astrocytoma [3][4][5] |
+ | +/− | +/− | − | + | − |
|
|
| |
| Medulloblastoma [6][7][8] |
+ | +/− | +/− | − | + | − |
|
|
| |
| Craniopharyngioma [9][10][11][2] |
+ | +/− | + Bitemporal hemianopia | − | + |
|
|
|
| |
| Pinealoma [12][13][14] |
+ | +/− | +/− | − | + vertical gaze palsy |
|
|
|
| |
| Adult primary brain tumors | ||||||||||
| Glioblastoma multiforme [15][16][2] |
+ | +/− | +/− | − | + | − |
|
|
| |
| Oligodendroglioma [17][18][19] |
+ | + | +/− | − | + | − |
|
|
| |
| Meningioma [20][21][22] |
+ | +/− | +/− | − | + | − |
|
|
| |
| Hemangioblastoma [23][24][25][26] |
+ | +/− | +/− | − | + | − |
|
| ||
| Pituitary adenoma [27][28][2] |
− | − | + Bitemporal hemianopia | − | − |
|
|
|
| |
| Schwannoma [29][30][31][32] |
− | − | − | − | + | − |
|
|
| |
| Primary CNS lymphoma [33][34] |
+ | +/− | +/− | − | + | − |
|
|
| |
| Vascular | ||||||||||
| AV malformation [35][36][2] |
+ | + | +/− | − | +/− | − |
|
| ||
| Brain aneurysm [37][38][39][40][41] |
+ | +/− | +/− | − | +/− | − |
|
|
|
|
| Infectious | ||||||||||
| Bacterial brain abscess [42][43] |
+ | +/− | +/− | + | + |
|
|
|
|
|
| Tuberculosis [44][2][45] |
+ | +/− | +/− | + | + |
|
|
|
|
|
| Toxoplasmosis [46][47] |
+ | +/− | +/− | − | + |
|
|
|
|
|
| Hydatid cyst [48][2] |
+ | +/− | +/− | +/− | + |
|
|
|
|
|
| CNS cryptococcosis [49] |
+ | +/− | +/− | + | + |
|
|
|
|
|
| CNS aspergillosis [50] |
+ | +/− | +/− | + | + |
|
|
|
|
|
| Other | ||||||||||
| Brain metastasis [51][2] |
+ | +/− | +/− | + | + | − |
|
|
|
|
ABBREVIATIONS
CNS=Central nervous system, AV=Arteriovenous, CSF=Cerebrospinal fluid, NF-2=Neurofibromatosis type 2, MEN-1=Multiple endocrine neoplasia, GFAP=Glial fibrillary acidic protein, HIV=Human immunodeficiency virus, BhCG=Human chorionic gonadotropin, ESR=Erythrocyte sedimentation rate, AFB=Acid fast bacilli, MRA=Magnetic resonance angiography, CTA=CT angiography
References
- ↑ Yuh, E. L.; Barkovich, A. J.; Gupta, N. (2009). “Imaging of ependymomas: MRI and CT”. Child’s Nervous System. 25 (10): 1203–1213. doi:10.1007/s00381-009-0878-7. ISSN 0256-7040.
- ↑ 2.0 2.1 2.2 2.3 2.4 2.5 2.6 2.7 Mattle, Heinrich (2017). Fundamentals of neurology : an illustrated guide. Stuttgart New York: Thieme. ISBN 9783131364524.
- ↑ Sathornsumetee S, Rich JN, Reardon DA (November 2007). “Diagnosis and treatment of high-grade astrocytoma”. Neurol Clin. 25 (4): 1111–39, x. doi:10.1016/j.ncl.2007.07.004. PMID 17964028.
- ↑ Pedersen CL, Romner B (January 2013). “Current treatment of low grade astrocytoma: a review”. Clin Neurol Neurosurg. 115 (1): 1–8. doi:10.1016/j.clineuro.2012.07.002. PMID 22819718.
- ↑ Mattle, Heinrich (2017). Fundamentals of neurology : an illustrated guide. Stuttgart New York: Thieme. ISBN 9783131364524.
- ↑ Dorwart, R H; Wara, W M; Norman, D; Levin, V A (1981). “Complete myelographic evaluation of spinal metastases from medulloblastoma”. Radiology. 139 (2): 403–408. doi:10.1148/radiology.139.2.7220886. ISSN 0033-8419.
- ↑ Fruehwald-Pallamar, Julia; Puchner, Stefan B.; Rossi, Andrea; Garre, Maria L.; Cama, Armando; Koelblinger, Claus; Osborn, Anne G.; Thurnher, Majda M. (2011). “Magnetic resonance imaging spectrum of medulloblastoma”. Neuroradiology. 53 (6): 387–396. doi:10.1007/s00234-010-0829-8. ISSN 0028-3940.
- ↑ Burger, P. C.; Grahmann, F. C.; Bliestle, A.; Kleihues, P. (1987). “Differentiation in the medulloblastoma”. Acta Neuropathologica. 73 (2): 115–123. doi:10.1007/BF00693776. ISSN 0001-6322.
- ↑ Brunel H, Raybaud C, Peretti-Viton P, Lena G, Girard N, Paz-Paredes A, Levrier O, Farnarier P, Manera L, Choux M (September 2002). “[Craniopharyngioma in children: MRI study of 43 cases]”. Neurochirurgie (in French). 48 (4): 309–18. PMID 12407316.
- ↑ Prabhu, Vikram C.; Brown, Henry G. (2005). “The pathogenesis of craniopharyngiomas”. Child’s Nervous System. 21 (8–9): 622–627. doi:10.1007/s00381-005-1190-9. ISSN 0256-7040.
- ↑ Kennedy HB, Smith RJ (December 1975). “Eye signs in craniopharyngioma”. Br J Ophthalmol. 59 (12): 689–95. PMC 1017436. PMID 766825.
- ↑ Ahmed SR, Shalet SM, Price DA, Pearson D (September 1983). “Human chorionic gonadotrophin secreting pineal germinoma and precocious puberty”. Arch. Dis. Child. 58 (9): 743–5. PMID 6625640.
- ↑ Sano, Keiji (1976). “Pinealoma in Children”. Pediatric Neurosurgery. 2 (1): 67–72. doi:10.1159/000119602. ISSN 1016-2291.
- ↑ Baggenstoss, Archie H. (1939). “PINEALOMAS”. Archives of Neurology And Psychiatry. 41 (6): 1187. doi:10.1001/archneurpsyc.1939.02270180115011. ISSN 0096-6754.
- ↑ Sathornsumetee S, Rich JN, Reardon DA (November 2007). “Diagnosis and treatment of high-grade astrocytoma”. Neurol Clin. 25 (4): 1111–39, x. doi:10.1016/j.ncl.2007.07.004. PMID 17964028.
- ↑ Pedersen CL, Romner B (January 2013). “Current treatment of low grade astrocytoma: a review”. Clin Neurol Neurosurg. 115 (1): 1–8. doi:10.1016/j.clineuro.2012.07.002. PMID 22819718.
- ↑ Smits M (2016). “Imaging of oligodendroglioma”. Br J Radiol. 89 (1060): 20150857. doi:10.1259/bjr.20150857. PMC 4846213. PMID 26849038.
- ↑ Wesseling P, van den Bent M, Perry A (June 2015). “Oligodendroglioma: pathology, molecular mechanisms and markers”. Acta Neuropathol. 129 (6): 809–27. doi:10.1007/s00401-015-1424-1. PMC 4436696. PMID 25943885.
- ↑ Kerkhof M, Benit C, Duran-Pena A, Vecht CJ (2015). “Seizures in oligodendroglial tumors”. CNS Oncol. 4 (5): 347–56. doi:10.2217/cns.15.29. PMC 6082346. PMID 26478444.
- ↑ Zee CS, Chin T, Segall HD, Destian S, Ahmadi J (June 1992). “Magnetic resonance imaging of meningiomas”. Semin. Ultrasound CT MR. 13 (3): 154–69. PMID 1642904.
- ↑ Shibuya M (2015). “Pathology and molecular genetics of meningioma: recent advances”. Neurol. Med. Chir. (Tokyo). 55 (1): 14–27. doi:10.2176/nmc.ra.2014-0233. PMID 25744347.
- ↑ Begnami MD, Palau M, Rushing EJ, Santi M, Quezado M (September 2007). “Evaluation of NF2 gene deletion in sporadic schwannomas, meningiomas, and ependymomas by chromogenic in situ hybridization”. Hum. Pathol. 38 (9): 1345–50. doi:10.1016/j.humpath.2007.01.027. PMC 2094208. PMID 17509660.
- ↑ Lonser RR, Butman JA, Huntoon K, Asthagiri AR, Wu T, Bakhtian KD, Chew EY, Zhuang Z, Linehan WM, Oldfield EH (May 2014). “Prospective natural history study of central nervous system hemangioblastomas in von Hippel-Lindau disease”. J. Neurosurg. 120 (5): 1055–62. doi:10.3171/2014.1.JNS131431. PMC 4762041. PMID 24579662.
- ↑ Hussein MR (October 2007). “Central nervous system capillary haemangioblastoma: the pathologist’s viewpoint”. Int J Exp Pathol. 88 (5): 311–24. doi:10.1111/j.1365-2613.2007.00535.x. PMC 2517334. PMID 17877533.
- ↑ Lee SR, Sanches J, Mark AS, Dillon WP, Norman D, Newton TH (May 1989). “Posterior fossa hemangioblastomas: MR imaging”. Radiology. 171 (2): 463–8. doi:10.1148/radiology.171.2.2704812. PMID 2704812.
- ↑ Perks WH, Cross JN, Sivapragasam S, Johnson P (March 1976). “Supratentorial haemangioblastoma with polycythaemia”. J. Neurol. Neurosurg. Psychiatry. 39 (3): 218–20. PMID 945331.
- ↑ Kucharczyk W, Davis DO, Kelly WM, Sze G, Norman D, Newton TH (December 1986). “Pituitary adenomas: high-resolution MR imaging at 1.5 T”. Radiology. 161 (3): 761–5. doi:10.1148/radiology.161.3.3786729. PMID 3786729.
- ↑ Syro LV, Scheithauer BW, Kovacs K, Toledo RA, Londoño FJ, Ortiz LD, Rotondo F, Horvath E, Uribe H (2012). “Pituitary tumors in patients with MEN1 syndrome”. Clinics (Sao Paulo). 67 Suppl 1: 43–8. PMC 3328811. PMID 22584705.
- ↑ Donnelly, Martin J.; Daly, Carmel A.; Briggs, Robert J. S. (2007). “MR imaging features of an intracochlear acoustic schwannoma”. The Journal of Laryngology & Otology. 108 (12). doi:10.1017/S0022215100129056. ISSN 0022-2151.
- ↑ Feany MB, Anthony DC, Fletcher CD (May 1998). “Nerve sheath tumours with hybrid features of neurofibroma and schwannoma: a conceptual challenge”. Histopathology. 32 (5): 405–10. PMID 9639114.
- ↑ Chen H, Xue L, Wang H, Wang Z, Wu H (July 2017). “Differential NF2 Gene Status in Sporadic Vestibular Schwannomas and its Prognostic Impact on Tumour Growth Patterns”. Sci Rep. 7 (1): 5470. doi:10.1038/s41598-017-05769-0. PMID 28710469.
- ↑ Hardell, Lennart; Hansson Mild, Kjell; Sandström, Monica; Carlberg, Michael; Hallquist, Arne; Påhlson, Anneli (2003). “Vestibular Schwannoma, Tinnitus and Cellular Telephones”. Neuroepidemiology. 22 (2): 124–129. doi:10.1159/000068745. ISSN 0251-5350.
- ↑ Chinn RJ, Wilkinson ID, Hall-Craggs MA, Paley MN, Miller RF, Kendall BE, Newman SP, Harrison MJ (December 1995). “Toxoplasmosis and primary central nervous system lymphoma in HIV infection: diagnosis with MR spectroscopy”. Radiology. 197 (3): 649–54. doi:10.1148/radiology.197.3.7480733. PMID 7480733.
- ↑ Paulus, Werner (1999). “Classification, Pathogenesis and Molecular Pathology of Primary CNS Lymphomas”. Journal of Neuro-Oncology. 43 (3): 203–208. doi:10.1023/A:1006242116122. ISSN 0167-594X.
- ↑ Kucharczyk, W; Lemme-Pleghos, L; Uske, A; Brant-Zawadzki, M; Dooms, G; Norman, D (1985). “Intracranial vascular malformations: MR and CT imaging”. Radiology. 156 (2): 383–389. doi:10.1148/radiology.156.2.4011900. ISSN 0033-8419.
- ↑ Fleetwood, Ian G; Steinberg, Gary K (2002). “Arteriovenous malformations”. The Lancet. 359 (9309): 863–873. doi:10.1016/S0140-6736(02)07946-1. ISSN 0140-6736.
- ↑ Chapman, Arlene B.; Rubinstein, David; Hughes, Richard; Stears, John C.; Earnest, Michael P.; Johnson, Ann M.; Gabow, Patricia A.; Kaehny, William D. (1992). “Intracranial Aneurysms in Autosomal Dominant Polycystic Kidney Disease”. New England Journal of Medicine. 327 (13): 916–920. doi:10.1056/NEJM199209243271303. ISSN 0028-4793.
- ↑ Castori M, Voermans NC (October 2014). “Neurological manifestations of Ehlers-Danlos syndrome(s): A review”. Iran J Neurol. 13 (4): 190–208. PMC 4300794. PMID 25632331.
- ↑ Schievink, W. I.; Raissi, S. S.; Maya, M. M.; Velebir, A. (2010). “Screening for intracranial aneurysms in patients with bicuspid aortic valve”. Neurology. 74 (18): 1430–1433. doi:10.1212/WNL.0b013e3181dc1acf. ISSN 0028-3878.
- ↑ Germain DP (May 2017). “Pseudoxanthoma elasticum”. Orphanet J Rare Dis. 12 (1): 85. doi:10.1186/s13023-017-0639-8. PMC 5424392. PMID 28486967.
- ↑ Farahmand M, Farahangiz S, Yadollahi M (October 2013). “Diagnostic Accuracy of Magnetic Resonance Angiography for Detection of Intracranial Aneurysms in Patients with Acute Subarachnoid Hemorrhage; A Comparison to Digital Subtraction Angiography”. Bull Emerg Trauma. 1 (4): 147–51. PMC 4789449. PMID 27162847.
- ↑ Haimes, AB; Zimmerman, RD; Morgello, S; Weingarten, K; Becker, RD; Jennis, R; Deck, MD (1989). “MR imaging of brain abscesses”. American Journal of Roentgenology. 152 (5): 1073–1085. doi:10.2214/ajr.152.5.1073. ISSN 0361-803X.
- ↑ Brouwer, Matthijs C.; Tunkel, Allan R.; McKhann, Guy M.; van de Beek, Diederik (2014). “Brain Abscess”. New England Journal of Medicine. 371 (5): 447–456. doi:10.1056/NEJMra1301635. ISSN 0028-4793.
- ↑ Morgado, Carlos; Ruivo, Nuno (2005). “Imaging meningo-encephalic tuberculosis”. European Journal of Radiology. 55 (2): 188–192. doi:10.1016/j.ejrad.2005.04.017. ISSN 0720-048X.
- ↑ Be NA, Kim KS, Bishai WR, Jain SK (March 2009). “Pathogenesis of central nervous system tuberculosis”. Curr. Mol. Med. 9 (2): 94–9. PMC 4486069. PMID 19275620.
- ↑ Chinn RJ, Wilkinson ID, Hall-Craggs MA, Paley MN, Miller RF, Kendall BE, Newman SP, Harrison MJ (December 1995). “Toxoplasmosis and primary central nervous system lymphoma in HIV infection: diagnosis with MR spectroscopy”. Radiology. 197 (3): 649–54. doi:10.1148/radiology.197.3.7480733. PMID 7480733.
- ↑ Helton KJ, Maron G, Mamcarz E, Leventaki V, Patay Z, Sadighi Z (November 2016). “Unusual magnetic resonance imaging presentation of post-BMT cerebral toxoplasmosis masquerading as meningoencephalitis and ventriculitis”. Bone Marrow Transplant. 51 (11): 1533–1536. doi:10.1038/bmt.2016.168. PMID 27348541.
- ↑ Taslakian B, Darwish H (September 2016). “Intracranial hydatid cyst: imaging findings of a rare disease”. BMJ Case Rep. 2016. doi:10.1136/bcr-2016-216570. PMC 5030532. PMID 27620198.
- ↑ McCarthy M, Rosengart A, Schuetz AN, Kontoyiannis DP, Walsh TJ (July 2014). “Mold infections of the central nervous system”. N. Engl. J. Med. 371 (2): 150–60. doi:10.1056/NEJMra1216008. PMC 4840461. PMID 25006721.
- ↑ McCarthy M, Rosengart A, Schuetz AN, Kontoyiannis DP, Walsh TJ (July 2014). “Mold infections of the central nervous system”. N. Engl. J. Med. 371 (2): 150–60. doi:10.1056/NEJMra1216008. PMC 4840461. PMID 25006721.
- ↑ Pope WB (2018). “Brain metastases: neuroimaging”. Handb Clin Neurol. 149: 89–112. doi:10.1016/B978-0-12-811161-1.00007-4. PMC 6118134. PMID 29307364.
Natural History, Complications and Prognosis
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1] Associate Editor(s)-in-Chief: Ahmad Al Maradni, M.D. [2]
Overview
If left untreated, patients with ependymoma may progress to develop nausea, vomiting, headache, and irritability. Common complications of ependymoma include seizure, hydrocephalus, muscle paralysis, and speech problems.
Complication
Common complications associated with ependymomas are:
Prognosis
Unfavorable factors affecting outcome include the following:[1]
- Gain of chromosome 1q25 is present in approximately 20% of pediatric intracranial ependymoma cases and has been reported as a negative prognostic factor by multiple research groups.[2][3]
- Gene expression profile[4]
- Other factors that have been reported to be associated with poor prognosis for pediatric ependymoma include expression of the enzymatic subunit of telomerase (hTERT) and expression of the neural stem cell marker Nestin.[5][6]
- Tumor location. Cranial variants of ependymoma have a less favorable outcome than primary spinal cord ependymomas. Location within the spinal cord may also affect outcome, with tumors in the lower portion of the spinal cord having a worse prognosis.[7]
- Younger age at diagnosis.[8]
- Anaplastic histology[9]
- Subtotal resection[10]
- Lower doses of radiation[11]
- Immunohistochemical testing has identified increased expression of markers of proliferation (e.g., Ki-67 and MIB-1) and increased expression of EZH2, a polycomb complex protein involved in epigenetic regulation of gene expression, as prognostic factors for greater risk of treatment failure.[12][13][14]
References
- ↑ Eoendymoma. http://www.cancer.gov/types/brain/hp/child-ependymoma-treatment-pdq#section/_35 URL Accessed on 10 6 2015.
- ↑ Godfraind C, Kaczmarska JM, Kocak M, Dalton J, Wright KD, Sanford RA; et al. (2012). “Distinct disease-risk groups in pediatric supratentorial and posterior fossa ependymomas”. Acta Neuropathol. 124 (2): 247–57. doi:10.1007/s00401-012-0981-9. PMC 3554251. PMID 22526017.
- ↑ Mendrzyk F, Korshunov A, Benner A, Toedt G, Pfister S, Radlwimmer B; et al. (2006). “Identification of gains on 1q and epidermal growth factor receptor overexpression as independent prognostic markers in intracranial ependymoma”. Clin Cancer Res. 12 (7 Pt 1): 2070–9. doi:10.1158/1078-0432.CCR-05-2363. PMID 16609018.
- ↑ Wani K, Armstrong TS, Vera-Bolanos E, Raghunathan A, Ellison D, Gilbertson R; et al. (2012). “A prognostic gene expression signature in infratentorial ependymoma”. Acta Neuropathol. 123 (5): 727–38. doi:10.1007/s00401-012-0941-4. PMC 4013829. PMID 22322993.
- ↑ Tabori U, Ma J, Carter M, Zielenska M, Rutka J, Bouffet E; et al. (2006). “Human telomere reverse transcriptase expression predicts progression and survival in pediatric intracranial ependymoma”. J Clin Oncol. 24 (10): 1522–8. doi:10.1200/JCO.2005.04.2127. PMID 16575002.
- ↑ Modena P, Buttarelli FR, Miceli R, Piccinin E, Baldi C, Antonelli M; et al. (2012). “Predictors of outcome in an AIEOP series of childhood ependymomas: a multifactorial analysis”. Neuro Oncol. 14 (11): 1346–56. doi:10.1093/neuonc/nos245. PMC 3480268. PMID 23076205.
- ↑ Oh MC, Sayegh ET, Safaee M, Sun MZ, Kaur G, Kim JM; et al. (2013). “Prognosis by tumor location for pediatric spinal cord ependymomas”. J Neurosurg Pediatr. 11 (3): 282–8. doi:10.3171/2012.11.PEDS12292. PMID 23259510.
- ↑ Tamburrini G, D’Ercole M, Pettorini BL, Caldarelli M, Massimi L, Di Rocco C (2009). “Survival following treatment for intracranial ependymoma: a review”. Childs Nerv Syst. 25 (10): 1303–12. doi:10.1007/s00381-009-0874-y. PMID 19387655.
- ↑ Korshunov A, Golanov A, Sycheva R, Timirgaz V (2004). “The histologic grade is a main prognostic factor for patients with intracranial ependymomas treated in the microneurosurgical era: an analysis of 258 patients”. Cancer. 100 (6): 1230–7. doi:10.1002/cncr.20075. PMID 15022291.
- ↑ White F (1975). “Epidemiology and infection control”. Dimens Health Serv. 52 (12): 34, 37, 39. PMID 1303-12 Check
|pmid=value (help). - ↑ Vaidya K, Smee R, Williams JR (2012). “Prognostic factors and treatment options for paediatric ependymomas”. J Clin Neurosci. 19 (9): 1228–35. doi:10.1016/j.jocn.2012.02.006. PMID 22840355.
- ↑ Li AM, Dunham C, Tabori U, Carret AS, McNeely PD, Johnston D; et al. (2015). “EZH2 expression is a prognostic factor in childhood intracranial ependymoma: a Canadian Pediatric Brain Tumor Consortium study”. Cancer. 121 (9): 1499–507. doi:10.1002/cncr.29198. PMID 25586788.
- ↑ Wolfsberger S, Fischer I, Höftberger R, Birner P, Slavc I, Dieckmann K; et al. (2004). “Ki-67 immunolabeling index is an accurate predictor of outcome in patients with intracranial ependymoma”. Am J Surg Pathol. 28 (7): 914–20. PMID 15223962.
- ↑ Kurt E, Zheng PP, Hop WC, van der Weiden M, Bol M, van den Bent MJ; et al. (2006). “Identification of relevant prognostic histopathologic features in 69 intracranial ependymomas, excluding myxopapillary ependymomas and subependymomas”. Cancer. 106 (2): 388–95. doi:10.1002/cncr.21608. PMID 16342252.
Diagnosis
Diagnosis
History and Symptoms | Physical Examination | Staging | Laboratory Findings | CT | MRI | Ultrasound | Other Imaging Findings | Other Diagnostic Studies
Treatment
Treatment
Medical Therapy | Surgery | Primary Prevention | Secondary Prevention | Cost-Effectiveness of Therapy | Future or Investigational Therapies
External Links
External Links
Images and technical information
Survivor stories
Looking for the patient version?
© 2026 MyEClinic – IFTM Institut für Telematik in der Medizin GmbH