
Tuberculous pericarditis
For patient information click, here.
To go back to the main page on Pericarditis, click here.
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editors-In-Chief: Fahimeh Shojaei, M.D., Varun Kumar, M.B.B.S.; Lakshmi Gopalakrishnan, M.B.B.S.
Synonyms and keywords: TB pericarditis
Overview
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor-In-Chief: Fahimeh Shojaei, M.D., Varun Kumar, M.B.B.S.; Lakshmi Gopalakrishnan, M.B.B.S.
Overview
Tuberculous pericarditis was first discovered by Rokitansky, an English scientist, in 1852. Tuberculous pericarditis is the result of hematogenous or lymphatic spread of mycobacterium tuberculosis to the pericardium. This causes acute inflammation of the pericardium and we may have polymorphonuclear (PMN) and leukocytes infiltration in the pericardium. This may lead to pericardial effusion and fibrinous changes of the pericardium. The visceral pericardium thickens with fibrin deposition (changes of constrictive pericarditis). There are four pathologic stages of involvement: stage 1 is presence of diffuse fibrin deposition, granulomas and abundant mycobacterium. Stage 2 is development of serous or serosanguineous pericardial effusion with a predominantly lymphocytic exudate with monocytes and foam cells. Stage 3 is absorption of the effusion with organization of granulomatous caseation and thickening of pericardium secondary to deposition of fibrin and collagen. Stage 4 is development of constrictive pericarditis. The pericardial space is obliterated by dense adhesions with marked thickening of parietal layer and replacement of granulomas by fibrous tissue. Conditions associated with tuberculous pericarditis include pulmonary TB, HIV, malignancy, chemotherapy, and diabetes mellitus. On gross pathology, thickened pericardium, shaggy hemorrhage, and exudate are characteristic findings of tuberculous pericarditis. On microscopic histopathological analysis, acid fast bacilli is characteristic findings of tuberculous pericarditis. The prevalence of tuberculous pericarditis is approximately 1-2% of patients with pulmonary tuberculosis. Patients of all age groups may develop tuberculous pericarditis. The incidence of tuberculous pericarditis increases with age. Tuberculous pericarditis commonly affects elderly. Tuberculous pericarditis usually affects individuals of the black race. Men are more commonly affected by tuberculous pericarditis than female. Since the prevalence of tuberculous pericarditis may follow tuberculosis prevalence, The majority of tuberculous pericarditis cases are reported in South Africa, Indonesia, Nigeria, Pakistan, India, and China. Patients with tuberculous pericarditis may have a positive history of pulmonary TB, HIV infection, any Immune system dysfunction, elderly, black race, male gender, and living/traveling to TB endemic areas. Common symptoms of tuberculous pericarditis include fever, weight loss, night sweat, cough, breathlessness, chest pain, malaise, and ankle edema. Patients with tuberculous pericarditis usually appear Cachectic. They may have fever, tachycardia, pulsus paradoxus, hypotension, tachypnea, JVP distension, kussmaul’s sign, lymphadenopathy, ankle edama, pleura dullness, decreased breath sounds, pericardial knock, pericardial rub, fine/coarse crackles upon auscultation of the lung, hepatomegaly, ascites, distant heart sounds, displaced point of maximal impulse (PMI) suggestive of cardiomegaly, friction rub, and S4. A 2 months course of isoniazid, pyrazinamide, rifampicin, and ethambutol followed by 4months course of isoniazid and rifampicin is shown to be effective for treatment of tuberculous pericarditis. Short course chemotherapy is beneficial in HIV infected patients. The mainstay of treatment for tuberculous pericarditis is medical therapy. Pericardiectomy is usually reserved for patients resistance constrictive pericarditis.
Historical Perspective
Tuberculous pericarditis was first discovered by Rokitansky, an English scientist, in 1852.
Classification
There is no established system for the classification of Tuberculous pericarditis.
Pathophysiology
Tuberculous pericarditis is the result of hematogenous or lymphatic spread of mycobacterium tuberculosis to the pericardium. This causes acute inflammation of the pericardium and we may have polymorphonuclear (PMN) and leukocytes infiltration in the pericardium. This may lead to pericardial effusion and fibrinous changes of the pericardium. The visceral pericardium thickens with fibrin deposition (changes of constrictive pericarditis). There are four pathologic stages of involvement: stage 1 is presence of diffuse fibrin deposition, granulomas and abundant mycobacterium. Stage 2 is development of serous or serosanguineous pericardial effusion with a predominantly lymphocytic exudate with monocytes and foam cells. Stage 3 is absorption of the effusion with organization of granulomatous caseation and thickening of pericardium secondary to deposition of fibrin and collagen. Stage 4 is development of constrictive pericarditis. The pericardial space is obliterated by dense adhesions with marked thickening of parietal layer and replacement of granulomas by fibrous tissue. Conditions associated with tuberculous pericarditis include pulmonary TB, HIV, malignancy, chemotherapy, and diabetes mellitus. On gross pathology, thickened pericardium, shaggy hemorrhage, and exudate are characteristic findings of tuberculous pericarditis. On microscopic histopathological analysis, acid fast bacilli is characteristic findings of tuberculous pericarditis. Pericardiocentesis is the gold standard test for the diagnosis of tuberculous pericarditis. Pericardial biopsy must be performed when we can’t find acid fast bacilli in sputum or pericardial fluid. Finding acid fast bacilli on pericardiocentesis is confirmatory for tuberculous pericarditis.
Causes
Common cause of tuberculous pericarditis is lymphatic or hematogenous spread of mycobacterium tuberculosis to the pericardium.
Differentiating Tuberculous pericarditisfrom Other Diseases
Epidemiology and Demographics
The prevalence of tuberculous pericarditis is approximately 1-2% of patients with pulmonary tuberculosis. Patients of all age groups may develop tuberculous pericarditis. The incidence of tuberculous pericarditis increases with age. Tuberculous pericarditis commonly affects elderly. Tuberculous pericarditis usually affects individuals of the black race. Men are more commonly affected by tuberculous pericarditis than female. Since the prevalence of tuberculous pericarditis may follow tuberculosis prevalence, The majority of tuberculous pericarditis cases are reported in South Africa, Indonesia, Nigeria, Pakistan, India, and China.
Risk Factors
Common risk factors in the development of tuberculous pericarditis include immunodeficiency (AIDS, malignancy, chemotherapy, diabetes and elderly), TB exposure, male gender, and African-American race.
Screening
There is insufficient evidence to recommend routine screening for tuberculous pericarditis.
Natural History, Complications, and Prognosis
Diagnosis
Diagnostic Study of Choice
Pericardiocentesis is the gold standard test for the diagnosis of tuberculous pericarditis. Pericardial biopsy must be performed when we can’t find acid fast bacilli in sputum or pericardial fluid. Finding acid fast bacilli on pericardiocentesis is confirmatory for tuberculous pericarditis.
History and Symptoms
Patients with tuberculous pericarditis may have a positive history of pulmonary TB, HIV infection, any Immune system dysfunction, elderly, black race, male gender, and living/traveling to TB endemic areas. Common symptoms of tuberculous pericarditis include fever, weight loss, night sweat, cough, breathlessness, chest pain, malaise, and ankle edema.
Physical Examination
Patients with tuberculous pericarditis usually appear Cachectic. They may have fever, tachycardia, pulsus paradoxus, hypotension, tachypnea, JVP distension, kussmaul’s sign, lymphadenopathy, ankle edama, pleura dullness, decreased breath sounds, pericardial knock, pericardial rub, fine/coarse crackles upon auscultation of the lung, hepatomegaly, ascites, distant heart sounds, displaced point of maximal impulse (PMI) suggestive of cardiomegaly, friction rub, and S4.
Laboratory Findings
Laboratory findings consistent with the diagnosis of tuberculous pericarditis include mild anemia, normal leukocyte count, exudate pericardial effusion, mycobacterium tuberculosis bacilli in pericardial effusion, and positive HIV test.
Electrocardiogram
An ECG may be helpful in the diagnosis of tuberculous pericarditis. Findings on an ECG suggestive of tuberculous pericarditis include low voltage QRS, absence of ST segment elevation which we usually see in acute pericarditis, inverted T wave, atrial fibrillation, and electrical alternans.
X-ray
An x-ray may be helpful in the diagnosis of tuberculous pericarditis. Findings on an x-ray suggestive of tuberculous pericarditis include pericardial calcification, pericardial thickening, pericardial effusion, and evidence of pulmonary TB.
Echocardiography and Ultrasound
Echocardiography/ultrasound may be helpful in the diagnosis of tuberculous pericarditis. Findings on an echocardiography/ultrasound suggestive of tuberculous pericarditis include pericardial effusion, , pericardial thickening, increased right ventricular dimensions, decreased left ventricular dimensions, abnormal septal motion, flattening of the left ventricular posterior wall during diastol, dilated inferior vena cava, and dilated atrium.
CT scan
CT scan may be helpful in the diagnosis of tuberculous pericarditis. Findings on CT scan suggestive of tuberculous pericarditis include calcification of the pericardium, thickened pericardium, pericardial effusion, and back flow of blood into the IVC and hepatic veins (in contrast CT scan).
MRI
MRI may be helpful in the diagnosis of tuberculous pericarditis. Findings on MRI suggestive of tuberculous pericarditis include pericardial effusion, pericardial thickening, mediastinal and tracheobronchial lymphadenopathy (with hilar sparing), and bowing of the interventricular septum toward the left ventricle during diastole.
Other Imaging Findings
There are no other imaging findings associated with tuberculous pericarditis.
Other Diagnostic Studies
Other diagnostic studies for tuberculous pericarditis include PPD skin test, interferon-gamma assay, smear and culture of pericardial, sputum, and gastric fluid, pericardial biopsy, and lymph node biopsy.
Treatment
Medical Therapy
A 2 months course of isoniazid, pyrazinamide, rifampicin, and ethambutol followed by 4months course of isoniazid and rifampicin is shown to be effective for treatment of tuberculous pericarditis. Short course chemotherapy is beneficial in HIV infected patients.
Surgery
The mainstay of treatment for tuberculous pericarditis is medical therapy. Pericardiectomy is usually reserved for patients resistance constrictive pericarditis.
Primary Prevention
There are no established measures for the primary prevention of tuberculous pericarditis.
Secondary Prevention
There are no established measures for the secondary prevention of tuberculous pericarditis.
References
Historical Perspective
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Fahimeh Shojaei, M.D.
Overview
Tuberculous pericarditis was first discovered by Rokitansky, an English scientist, in 1852.
Historical Perspective
Discovery
- Tuberculous pericarditis was first discovered by Rokitansky, an English scientist, in 1852.
- Different scientists and doctors have described multiple cases of tuberculous pericarditis:
- Quinquad and Lejard in 1872
- Osler in 1893
- Reisman in 1901
- Clarke in 1929
- Roubier and Dubois in 1300
- Thompson in 1933
- Bellet, McMillan, and Gouley in 1934
References
Classification
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Fahimeh Shojaei, M.D.
Overview
There is no established system for the classification of Tuberculous pericarditis.
Classification
There is no established system for the classification of Tuberculous pericarditis.
References
Pathophysiology
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor-In-Chief: Fahimeh Shojaei, M.D., Varun Kumar, M.B.B.S.; Lakshmi Gopalakrishnan, M.B.B.S.
Overview
Tuberculous pericarditis is the result of hematogenous or lymphatic spread of mycobacterium tuberculosis to the pericardium. This causes acute inflammation of the pericardium and we may have polymorphonuclear (PMN) and leukocytes infiltration in the pericardium. This may lead to pericardial effusion and fibrinous changes of the pericardium. The visceral pericardium thickens with fibrin deposition (changes of constrictive pericarditis). There are four pathologic stages of involvement: stage 1 is presence of diffuse fibrin deposition, granulomas and abundant mycobacterium. Stage 2 is development of serous or serosanguineous pericardial effusion with a predominantly lymphocytic exudate with monocytes and foam cells. Stage 3 is absorption of the effusion with organization of granulomatous caseation and thickening of pericardium secondary to deposition of fibrin and collagen. Stage 4 is development of constrictive pericarditis. The pericardial space is obliterated by dense adhesions with marked thickening of parietal layer and replacement of granulomas by fibrous tissue. Conditions associated with tuberculous pericarditis include pulmonary TB, HIV, malignancy, chemotherapy, and diabetes mellitus. On gross pathology, thickened pericardium, shaggy hemorrhage, and exudate are characteristic findings of tuberculous pericarditis. On microscopic histopathological analysis, acid fast bacilli is characteristic findings of tuberculous pericarditis.
Pathophysiology
Pathogenesis
- Tuberculous pericarditis is the result of hematogenous or lymphatic spread of mycobacterium tuberculosis to the pericardium.[1][2][3][4]
- This causes acute inflammation of the pericardium.
- We may have polymorphonuclear (PMN) and leukocytes infiltration in the pericardium.
- Pericardial vascularization may happen as well.
- This may lead to pericardial effusion and fibrinous changes of the pericardium.
- Effusive constrictive pericarditis may be seen in some patients.
- The visceral pericardium thickens with fibrin deposition (changes of constrictive pericarditis).
- There are four pathologic stages of involvement:
- Stage 1: Presence of diffuse fibrin deposition, granulomas and abundant mycobacterium
- Stage 2: Development of serous or serosanguineous pericardial effusion with a predominantly lymphocytic exudate with monocytes and foam cells
- Stage 3: Absorption of the effusion with organization of granulomatous caseation and thickening of pericardium secondary to deposition of fibrin and collagen.
- Stage 4: Development of constrictive pericarditis. The pericardial space is obliterated by dense adhesions with marked thickening of parietal layer and replacement of granulomas by fibrous tissue.
Genetics
The development of tuberculous pericarditis is not the result of any genetic mutation.
Associated Conditions
Conditions associated with tuberculous pericarditis include:
- Pulmonary TB
- HIV
- Malignancy
- Chemotherapy
- Diabetes mellitus
Gross Pathology Images
On gross pathology, thickened pericardium, shaggy hemorrhage, and exudate are characteristic findings of tuberculous pericarditis.

Microscopic Pathology Images
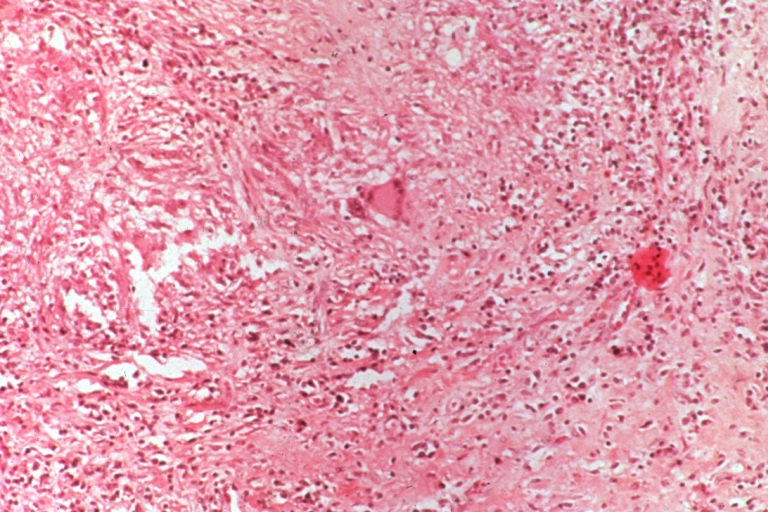
On microscopic histopathological analysis, acid fast bacilli is characteristic findings of tuberculous pericarditis.
-
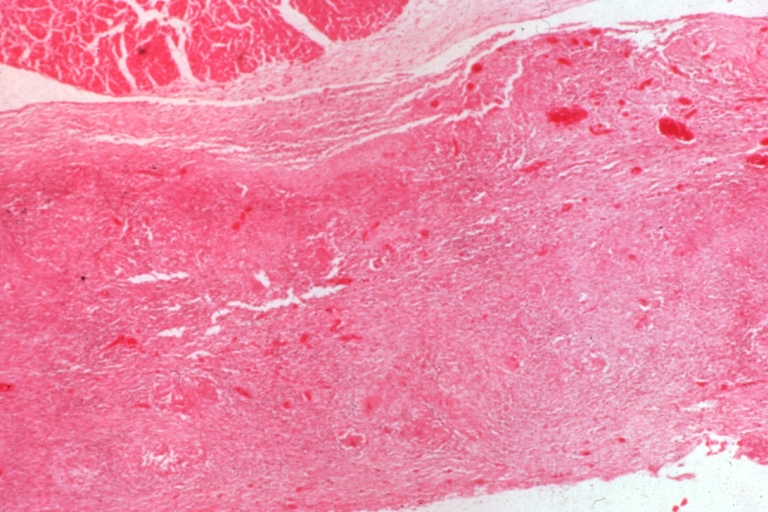 Tuberculous pericarditis.
Tuberculous pericarditis. -
 Tuberculous pericarditis.
Tuberculous pericarditis. -
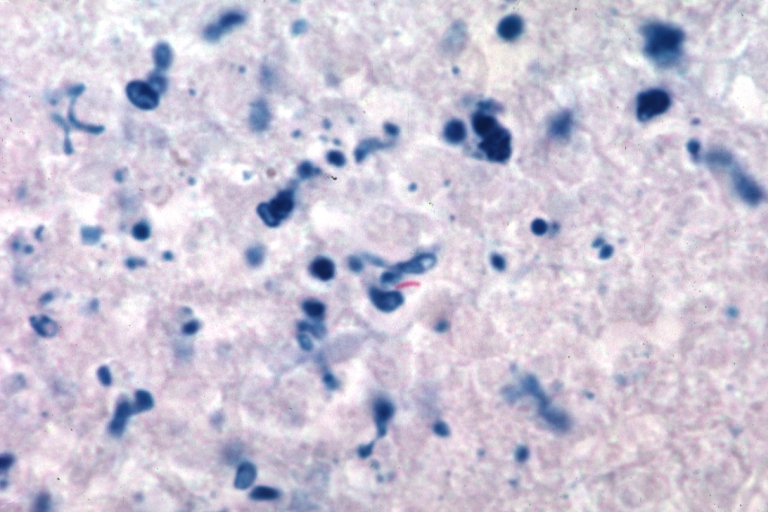 Tuberculous pericarditis: Micro oil acid fast stain. The organism easily seen.
Tuberculous pericarditis: Micro oil acid fast stain. The organism easily seen.



-
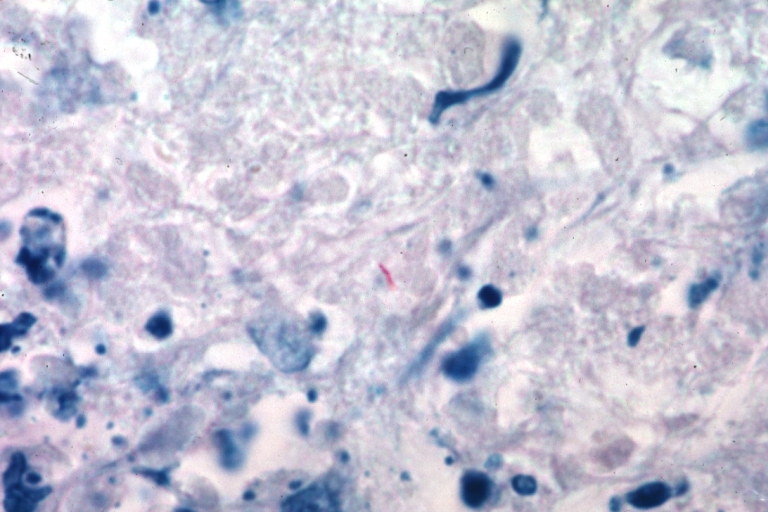 Tuberculous pericarditis: Micro oil acid fast stain. The organism easily seen.
Tuberculous pericarditis: Micro oil acid fast stain. The organism easily seen. -
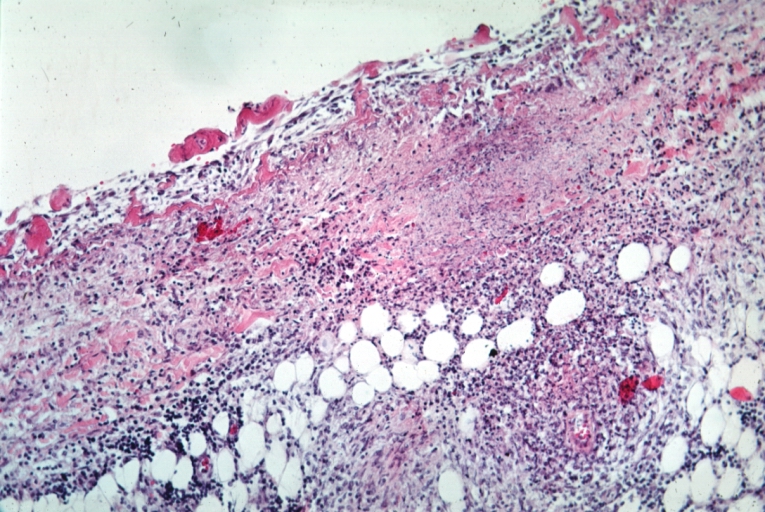 Tuberculous pericarditis: Micro med mag, H&E, a typical lesion.
Tuberculous pericarditis: Micro med mag, H&E, a typical lesion.


References
- ↑ Peel AA (1948). “TUBERCULOUS PERICARDITIS”. Br Heart J. 10 (3): 195–207. PMC 481044. PMID 18610109.
- ↑ Permanyer-Miralda G, Sagristá-Sauleda J, Soler-Soler J (1985). “Primary acute pericardial disease: a prospective series of 231 consecutive patients”. Am J Cardiol. 56 (10): 623–30. PMID 4050698.
- ↑ Mayosi BM, Burgess LJ, Doubell AF (2005). “Tuberculous pericarditis”. Circulation. 112 (23): 3608–16. doi:10.1161/CIRCULATIONAHA.105.543066. PMID 16330703.
- ↑ Sagristà-Sauleda J, Angel J, Sánchez A, Permanyer-Miralda G, Soler-Soler J (2004). “Effusive-constrictive pericarditis”. N Engl J Med. 350 (5): 469–75. doi:10.1056/NEJMoa035630. PMID 14749455.
Causes
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Fahimeh Shojaei, M.D.
Overview
Common cause of tuberculous pericarditis is lymphatic or hematogenous spread of mycobacterium tuberculosis to the pericardium.
causes
Common cause of tuberculous pericarditis is:
- Lymphatic or hematogenous spread of mycobacterium tuberculosis to the pericardium.
References
Differentiating Tuberculous Pericarditis from other Diseases
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [2]; Associate Editor(s)-in-Chief: Syed Hassan A. Kazmi BSc, MD [3] Homa Najafi, M.D.[4]
Overview
Pericarditis must be differentiated from diseases presenting with chest pain, shortness of breath and tachypnea which include myocardial infarction, pulmonary embolism, congestive heart failure, pneumonia, vasculitis, and chronic obstructive pulmonary disease (COPD). Manifestation of the pericarditis can help in differentiation from myocardial infarction. Moreover, other differential diagnosis include aortic stenosis, coronary artery vasospasm, esophageal rupture, esophageal spasm, esophagitis,acute gastritis, gastroesophageal reflux disease, and peptic ulcer disease should be considered.
Differentiating Pericarditis from other Diseases
- Pericarditis must be differentiated from diseases presenting with chest pain, shortness of breath and tachypnea.
- For a full discussion of the differential diagnosis of chest pain click here
- For an expert algorithm that aids in the diagnosis of the cause of chest pain click here
- Pericarditis must be differentiated from myocardial infarction as an important cause of chest pain.The differentiating features include:[1]
| Characteristic/Parameter | Pericarditis | Myocardial infarction |
|---|---|---|
| Pain description | Sharp, pleuritic, retro-sternal (under the sternum) or left precordial (left chest) pain. | Crushing, pressure-like, heavy pain. Described as “elephant on the chest“. |
| Radiation | Pain radiates to the trapezius ridge (to the lowest portion of the scapula on the back) or no radiation. | Pain radiates to the jaw, or the left or arm, or does not radiate. |
| Exertion | Does not change the pain | Can increase the pain |
| Position | Pain is worse supine or upon inspiration (breathing in) | Not positional |
| Onset/duration | Sudden pain, that lasts for hours or sometimes days before a patient comes to the ER | Sudden or chronically worsening pain that can come and go in paroxysms or it can last for hours before the patient decides to come to the ER |
Differentiating pericarditis from other diseases on the basis of chest pain, shortness of breath, and tachypnea
The differentials include the following:[2][3][4][5][6][7][8][9][10][11][12][13][14][15][16][17][18][19][20][21]
| Diseases | Diagnostic tests | Physical Examination | Symptoms | Past medical history | Other Findings | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| CT scan and MRI | EKG | Chest X-ray | Tachypnea | Tachycardia | Fever | Chest Pain | Hemoptysis | Dyspnea on Exertion | Wheezing | Chest Tenderness | Nasalopharyngeal Ulceration | Carotid Bruit | |||
| Pulmonary embolism |
|
|
|
✔ | ✔ | ✔ (Low grade) | ✔ | ✔ (In case of massive PE) | ✔ | – | – | – | – |
|
|
| Congestive heart failure |
|
✔ | ✔ | ✔ | – | – | ✔ | – | – | – | – |
|
| ||
| Percarditis |
|
|
|
✔ | ✔ | ✔ (Low grade) | ✔ (Relieved by sitting up and leaning forward) | – | ✔ | – | – | – | – |
|
|
| Pneumonia |
|
|
|
✔ | ✔ | ✔ | ✔ | – | ✔ | ✔ | – | – | – |
|
|
| Vasculitis |
|
|
✔ | ✔ | ✔ | ✔ | ✔ | ✔ | – | ✔ | ✔ | ✔ |
|
||
| Chronic obstructive pulmonary disease (COPD) |
|
|
✔ | ✔ | – | – | – | ✔ | ✔ | – | – | – |
|
| |
Other differentials
Pericarditis also resembles the following disorders and needs to be differentiated from them:
- Angina pectoris
- Aortic stenosis
- Coronary artery vasospasm
- Esophageal rupture
- Esophageal spasm
- Esophagitis
- Gastritis, acute
- Gastroesophageal reflux disease
- Peptic ulcer disease
References
- ↑ American College of Physicians (ACP). Medical Knowledge Self-Assessment Program (MKSAP-15): Cardiovascular Medicine. “Pericardial disease.” p. 64. ISBN 978-934465-28-8 [1]
- ↑ Brenes-Salazar JA (2014). “Westermark’s and Palla’s signs in acute and chronic pulmonary embolism: Still valid in the current computed tomography era”. J Emerg Trauma Shock. 7 (1): 57–8. doi:10.4103/0974-2700.125645. PMC 3912657. PMID 24550636.
- ↑ “CT Angiography of Pulmonary Embolism: Diagnostic Criteria and Causes of Misdiagnosis | RadioGraphics”.
- ↑ Bĕlohlávek J, Dytrych V, Linhart A (2013). “Pulmonary embolism, part I: Epidemiology, risk factors and risk stratification, pathophysiology, clinical presentation, diagnosis and nonthrombotic pulmonary embolism”. Exp Clin Cardiol. 18 (2): 129–38. PMC 3718593. PMID 23940438.
- ↑ “Pulmonary Embolism: Symptoms – National Library of Medicine – PubMed Health”.
- ↑ Ramani GV, Uber PA, Mehra MR (2010). “Chronic heart failure: contemporary diagnosis and management”. Mayo Clin. Proc. 85 (2): 180–95. doi:10.4065/mcp.2009.0494. PMC 2813829. PMID 20118395.
- ↑ Blinderman CD, Homel P, Billings JA, Portenoy RK, Tennstedt SL (2008). “Symptom distress and quality of life in patients with advanced congestive heart failure”. J Pain Symptom Manage. 35 (6): 594–603. doi:10.1016/j.jpainsymman.2007.06.007. PMC 2662445. PMID 18215495.
- ↑ Hawkins NM, Petrie MC, Jhund PS, Chalmers GW, Dunn FG, McMurray JJ (2009). “Heart failure and chronic obstructive pulmonary disease: diagnostic pitfalls and epidemiology”. Eur. J. Heart Fail. 11 (2): 130–9. doi:10.1093/eurjhf/hfn013. PMC 2639415. PMID 19168510.
- ↑ Takasugi JE, Godwin JD (1998). “Radiology of chronic obstructive pulmonary disease”. Radiol. Clin. North Am. 36 (1): 29–55. PMID 9465867.
- ↑ Wedzicha JA, Donaldson GC (2003). “Exacerbations of chronic obstructive pulmonary disease”. Respir Care. 48 (12): 1204–13, discussion 1213–5. PMID 14651761.
- ↑ Nakawah MO, Hawkins C, Barbandi F (2013). “Asthma, chronic obstructive pulmonary disease (COPD), and the overlap syndrome”. J Am Board Fam Med. 26 (4): 470–7. doi:10.3122/jabfm.2013.04.120256. PMID 23833163.
- ↑ Khandaker MH, Espinosa RE, Nishimura RA, Sinak LJ, Hayes SN, Melduni RM, Oh JK (2010). “Pericardial disease: diagnosis and management”. Mayo Clin. Proc. 85 (6): 572–93. doi:10.4065/mcp.2010.0046. PMC 2878263. PMID 20511488.
- ↑ Bogaert J, Francone M (2013). “Pericardial disease: value of CT and MR imaging”. Radiology. 267 (2): 340–56. doi:10.1148/radiol.13121059. PMID 23610095.
- ↑ Gharib AM, Stern EJ (2001). “Radiology of pneumonia”. Med. Clin. North Am. 85 (6): 1461–91, x. PMID 11680112.
- ↑ Schmidt WA (2013). “Imaging in vasculitis”. Best Pract Res Clin Rheumatol. 27 (1): 107–18. doi:10.1016/j.berh.2013.01.001. PMID 23507061.
- ↑ Suresh E (2006). “Diagnostic approach to patients with suspected vasculitis”. Postgrad Med J. 82 (970): 483–8. doi:10.1136/pgmj.2005.042648. PMC 2585712. PMID 16891436.
- ↑ Stein PD, Dalen JE, McIntyre KM, Sasahara AA, Wenger NK, Willis PW (1975). “The electrocardiogram in acute pulmonary embolism”. Prog Cardiovasc Dis. 17 (4): 247–57. PMID 123074.
- ↑ Warnier MJ, Rutten FH, Numans ME, Kors JA, Tan HL, de Boer A, Hoes AW, De Bruin ML (2013). “Electrocardiographic characteristics of patients with chronic obstructive pulmonary disease”. COPD. 10 (1): 62–71. doi:10.3109/15412555.2012.727918. PMID 23413894.
- ↑ Stein PD, Matta F, Ekkah M, Saleh T, Janjua M, Patel YR, Khadra H (2012). “Electrocardiogram in pneumonia”. Am. J. Cardiol. 110 (12): 1836–40. doi:10.1016/j.amjcard.2012.08.019. PMID 23000104.
- ↑ Hazebroek MR, Kemna MJ, Schalla S, Sanders-van Wijk S, Gerretsen SC, Dennert R, Merken J, Kuznetsova T, Staessen JA, Brunner-La Rocca HP, van Paassen P, Cohen Tervaert JW, Heymans S (2015). “Prevalence and prognostic relevance of cardiac involvement in ANCA-associated vasculitis: eosinophilic granulomatosis with polyangiitis and granulomatosis with polyangiitis”. Int. J. Cardiol. 199: 170–9. doi:10.1016/j.ijcard.2015.06.087. PMID 26209947.
- ↑ Dennert RM, van Paassen P, Schalla S, Kuznetsova T, Alzand BS, Staessen JA, Velthuis S, Crijns HJ, Tervaert JW, Heymans S (2010). “Cardiac involvement in Churg-Strauss syndrome”. Arthritis Rheum. 62 (2): 627–34. doi:10.1002/art.27263. PMID 20112390.
Epidemiology and Demographics
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor-In-Chief: Fahimeh Shojaei, M.D., Varun Kumar, M.B.B.S.; Lakshmi Gopalakrishnan, M.B.B.S.
Overview
The prevalence of tuberculous pericarditis is approximately 1-2% of patients with pulmonary tuberculosis. Patients of all age groups may develop tuberculous pericarditis. The incidence of tuberculous pericarditis increases with age. Tuberculous pericarditis commonly affects elderly. Tuberculous pericarditis usually affects individuals of the black race. Men are more commonly affected by tuberculous pericarditis than female. Since the prevalence of tuberculous pericarditis may follow tuberculosis prevalence, The majority of tuberculous pericarditis cases are reported in South Africa, Indonesia, Nigeria, Pakistan, India, and China.
Epidemiology and Demographics
Prevalence
- The prevalence of tuberculous pericarditis is approximately 1-2% of patients with pulmonary tuberculosis.[1][2]
Age
- Patients of all age groups may develop tuberculous pericarditis.
- The incidence of tuberculous pericarditis increases with age.
- Tuberculous pericarditis commonly affects elderly.
Race
Gender
Region
- Since the prevalence of tuberculous pericarditis may follow tuberculosis prevalence, The majority of tuberculous pericarditis cases are reported in:[5]
- South Africa
- The incidence of tuberculosis in South Africa is 834 per 100,000 of the overall population.
- The mortality of tuberculosis (excluding HIV–TB coinfection) in South Africa is 46 per 100,000 of the overall population.
- Indonesia
- The incidence of tuberculosis in Indonesia is 395 per 100,000 of the overall population.
- The mortality of tuberculosis (excluding HIV–TB coinfection) in Indonesia is 40 per 100,000 of the overall population.
- Nigeria
- The incidence of tuberculosis in Nigeria is 322 per 100,000 of the overall population.
- The mortality of tuberculosis (excluding HIV–TB coinfection) in Nigeria is 99 per 100,000 of the overall population.
- Pakistan
- The incidence of tuberculosis in Pakistan is 270 per 100,000 of the overall population.
- The mortality of tuberculosis (excluding HIV–TB coinfection) in Pakistan is 23 per 100,000 of the overall population.
- India
- The incidence of tuberculosis in India is 217 per 100,000 of the overall population.
- The mortality of tuberculosis (excluding HIV–TB coinfection) in India is 36 per 100,000 of the overall population.
- China
- The incidence of tuberculosis in China is 67 per 100,000 of the overall population.
- The mortality of tuberculosis (excluding HIV–TB coinfection) in China is 2.6 per 100,000 of the overall population.
- South Africa
Developed Countries
- After the resurgence of TB in the mid-1980s, the number of case counts steadily increased, peaking in 1992.[5]
- Since the 1992 TB resurgence peak in the United States, the number of TB cases reported has decreased annually.
- The year 2014 marked the twenty-second year of decline in the total number of TB cases reported in the United States since the peak of the resurgence.
- In 2014, a total of 9,421 cases were reported from the 50 states and the District of Columbia (DC).
- This represented a decline of 1.5% from 2013.
- The number of cases per 100,000 in 2013 and 2014 has been stable at a rate of 3.0.


References
- ↑ Fowler NO (1991). “Tuberculous pericarditis”. JAMA. 266 (1): 99–103. PMID 2046135.
- ↑ Larrieu AJ, Tyers GF, Williams EH, Derrick JR (1980). “Recent experience with tuberculous pericarditis”. Ann Thorac Surg. 29 (5): 464–8. PMID 7377888.
- ↑ HAGEMAN JH, D ESOPO ND, GLENN WW (February 1964). “TUBERCULOSIS OF THE PERICARDIUM. A LONG-TERM ANALYSIS OF FORTY-FOUR PROVED CASES”. N. Engl. J. Med. 270: 327–32. doi:10.1056/NEJM196402132700702. PMID 14082261.
- ↑ Rooney JJ, Crocco JA, Lyons HA (January 1970). “Tuberculous pericarditis”. Ann. Intern. Med. 72 (1): 73–81. doi:10.7326/0003-4819-72-1-73. PMID 5410398.
- ↑ 5.0 5.1 5.2 5.3 “WHO 2016 TB Report” (PDF).
Risk Factors
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Fahimeh Shojaei, M.D.
Overview
Common risk factors in the development of tuberculous pericarditis include immunodeficiency (AIDS, malignancy, chemotherapy, diabetes and elderly), TB exposure, male gender, and African-American race.
Risk Factors
Common Risk Factors
- Common risk factors in the development of tuberculous pericarditis include:[1][2][3]
- Immunodeficiency
- TB exposure
- Male gender
- African american race
Less Common Risk Factors
- Less common risk factors in the development of tuberculous pericarditis include:[4][5]
- IV drug use
- Malnutrition
- chronic hemodialysis
References
- ↑ Wragg, A (2000). “Tuberculous pericarditis and HIV infection”. Heart. 84 (2): 127–128. doi:10.1136/heart.84.2.127. ISSN 0007-0769.
- ↑ Subhash, H S; Ashwin, I; Mukundan, U; Danda, D; John, G; Cherian, A M; Thomas, K (2016). “Drug Resistant Tuberculosis in Diabetes Mellitus: A Retrospective Study from South India”. Tropical Doctor. 33 (3): 154–156. doi:10.1177/004947550303300311. ISSN 0049-4755.
- ↑ Rooney JJ, Crocco JA, Lyons HA (January 1970). “Tuberculous pericarditis”. Ann. Intern. Med. 72 (1): 73–81. doi:10.7326/0003-4819-72-1-73. PMID 5410398.
- ↑ Amedia C, Oettinger CW (August 1977). “Unusual presentation of tuberculosis in chronic hemodialysis patients”. Clin. Nephrol. 8 (2): 363–6. PMID 891049.
- ↑ Zachariah, R.; Spielmann, M.P.; Harries, A.D.; Salaniponi, F.M.L. (2002). “Moderate to severe malnutrition in patients with tuberculosis is a risk factor associated with early death”. Transactions of the Royal Society of Tropical Medicine and Hygiene. 96 (3): 291–294. doi:10.1016/S0035-9203(02)90103-3. ISSN 0035-9203.
Screening
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Fahimeh Shojaei, M.D.
Overview
There is insufficient evidence to recommend routine screening for tuberculous pericarditis.
Screening
There is insufficient evidence to recommend routine screening for tuberculous pericarditis.
References
Natural History, Complications and Prognosis
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor-In-Chief: Varun Kumar, M.B.B.S.; Lakshmi Gopalakrishnan, M.B.B.S.
Natural History, Complications and Prognosis
Tuberculous pericarditis often has a complicated course and poor clinical outcomes. It can lead to pericardial effusion and subsequently, cardiac tamponade which may require urgent intervention including pericardiocentesis. The mortality rate of tuberculous pericarditis in the preantibiotic era was 80-90%[1]. The mortality rate in the modern era is currently 8-17%[2][3] and is 17-34% if the TB is associated with HIV[4].
Tuberculous pericarditis can also cause heart failure as observed in Eastern Cape and Zimbabwe where it is a common cause, but less common than rheumatic heart disease. In this region, TB pericarditis is a more common cause of heart failure than hypertensive heart disease and cardiomyopathy[5][6]
Constrictive pericarditis is another complication of tuberculous pericarditis occurring in 30-60% of patients despite prompt antituberculosis treatment and the use of corticosteroids[7][8]
References
- ↑ Harvey AM, Whitehill MR. Tuberculous pericarditis. Medicine. 1937; 16: 45–94
- ↑ Desai HN (1979). “Tuberculous pericarditis. A review of 100 cases”. S Afr Med J. 55 (22): 877–80. PMID 472922.
- ↑ Bhan GL (1980). “Tuberculous pericarditis”. J Infect. 2 (4): 360–4. PMID 7185934.
- ↑ Hakim JG, Ternouth I, Mushangi E, Siziya S, Robertson V, Malin A (2000). “Double blind randomised placebo controlled trial of adjunctive prednisolone in the treatment of effusive tuberculous pericarditis in HIV seropositive patients”. Heart. 84 (2): 183–8. PMC 1760932. PMID 10908256.
- ↑ Strang JI (1984). “Tuberculous pericarditis in Transkei”. Clin Cardiol. 7 (12): 667–70. PMID 6509811.
- ↑ Hakim JG, Manyemba J (1998). “Cardiac disease distribution among patients referred for echocardiography in Harare, Zimbabwe”. Cent Afr J Med. 44 (6): 140–4. PMID 9810393.
- ↑ SCHRIRE V (1959). “Experience with pericarditis at Groote Schuur Hospital, Cape Town: an analysis of one hundred and sixty cases studied over a six-year period”. S Afr Med J. 33: 810–7. PMID 14443596.
- ↑ Sagristà-Sauleda J, Permanyer-Miralda G, Soler-Soler J (1988). “Tuberculous pericarditis: ten year experience with a prospective protocol for diagnosis and treatment”. J Am Coll Cardiol. 11 (4): 724–8. PMID 3351140.
Diagnosis
Diagnosis
Diagnostic study of choice | History and Symptoms | Physical Examination | Laboratory Findings | Electrocardiogram | X-Ray Findings | Echocardiography and Ultrasound | CT-Scan Findings | MRI Findings | Other Imaging Findings | Other Diagnostic Studies
Treatment
Treatment
Medical Therapy | Interventions | Surgery | Primary Prevention | Secondary Prevention | Cost-Effectiveness of Therapy | Future or Investigational Therapies
Looking for the patient version?
© 2026 MyEClinic – IFTM Institut für Telematik in der Medizin GmbH