
Right ventricular outflow tract obstruction
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor-In-Chief: Cafer Zorkun, M.D., Ph.D. [2]; Keri Shafer, M.D. [3]
Overview
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editors-In-Chief: Cafer Zorkun, M.D., Ph.D. [2]; Keri Shafer, M.D. [3] Mohammed Salih, MD. [4]
Overview
Right ventricular outflow tract (RVOT) and/or pulmonary artery obstruction are present in some form in 25 % of all congenital heart defects. The right ventricular outflow tract obstruction includes stenosis or narrowing of the pulmonary valve, the tissue above the valve (supravalvar obstruction) and below it(subvalvar obstruction). Congenital subvalvar and supravalvar right ventricular outflow tract stenosis usually occurs with other congenital heart defects such as Ventricular Septal Defect (VSD) or Tetralogy of Fallot. The timing and type of surgery will vary from patient to patient depending upon the severity of the obstruction and the associated congenital defect.
If right ventricular outflow tract obstruction is present and the ventricular septum is intact, usually the right ventricle will adapt better given that no right to left shunting is present. This absence of shunting may result in sufficient pulmonary blood flow to allow the patient to remain asymptomatic longer.
Usually therapy is directed to increase pulmonary blood flow and decompressing the right ventricle (RV) and it will depend on the severity and location of the defect. According to the anatomic features of the pulmonary valve stenosis, the physician may use balloon dilatation (a minimally invasive transvenous procedure) to dilate the obstruction during cardiac catheterization, but if the pulmonary artery is the structure involved, stenting (insertion of a small tube) within the narrowed region can be done following balloon angioplasty. Standard treatment of right ventricular outflow tract or pulmonary artery obstruction involves open chest surgery. [1] [2][3] [4] [5]
References
- ↑ Scarlat A, Bodner G, Liron M (1986). “Massive haemoptysis as the presenting symptom in mitral stenosis”. Thorax. 41 (5): 413–4. PMC 1020641. PMID 3750250.
- ↑ Waller BF, Howard J, Fess S (1995). “Pathology of tricuspid valve stenosis and pure tricuspid regurgitation–Part I.” Clin Cardiol. 18 (2): 97–102. PMID 7720297.
- ↑ Maher ER, Pazianas M, Curtis JR (1987). “Calcific aortic stenosis: a complication of chronic uraemia”. Nephron. 47 (2): 119–22. PMID 3696315.
- ↑ Hull MC, Morris CG, Pepine CJ, Mendenhall NP (2003). “Valvular dysfunction and carotid, subclavian, and coronary artery disease in survivors of hodgkin lymphoma treated with radiation therapy”. JAMA. 290 (21): 2831–7. doi:10.1001/jama.290.21.2831. PMID 14657067.
- ↑ Dweck MR, Boon NA, Newby DE (2012). “Calcific aortic stenosis: a disease of the valve and the myocardium”. J Am Coll Cardiol. 60 (19): 1854–63. doi:10.1016/j.jacc.2012.02.093. PMID 23062541.
Anatomy of Pulmonary Valve
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1] Associate Editor(s)-in-Chief:
Synonyms and keywords: Pulmonic valve
Overview
The pulmonary valve is the semilunar valve of the heart that lies between the right ventricle and the pulmonary artery and has three cusps.
Similar to the aortic valve, the pulmonic valve opens in ventricular systole, when the pressure in the right ventricle rises above the pressure in the pulmonary artery. At the end of ventricular systole, when the pressure in the right ventricle falls rapidly, the pressure in the pulmonary artery will close the pulmonic valve.
The closure of the pulmonic valve contributes the P2 component of the second heart sound (S2).
The right heart is a low-pressure system, so the P2 component of the second heart sound is usually softer than the A2 component of the second heart sound. However, it is physiologically normal in some young people to hear both components separated during inhalation.
Normal Anatomy
- Pulmonary valve is located at the distal part of the right ventricular outflow tract at the junction of the pulmonary artery.
- It is located anterior and superior to the aortic valve at the level of the third intercostal space and separated from the tricuspid valve by the infundibulum of the right ventricle. [1]
- It is comprised of three equal sized, semilunar cusps or leaflets (right, left, anterior), nomenclature based on the corresponding aortic valve. [2] [2]
- The three cusps are joined by commissures and the cusps are thinner when compared to the aortic valve, due to a low pressure in the right ventricle.[2]
- The area of the valve is related to body surface area and men usually have greater valve area when compared with women.
- The normal orifice area is approximately around 3cm². [3]
- The pulmonary valve opens in the right ventricular systole allowing the deoxygenated blood to be delivered to the lungs. [2]
- During the right ventricular diastole the pulmonary valves close completely to prevent regurgitation of blood into the right ventricle.[2]
-
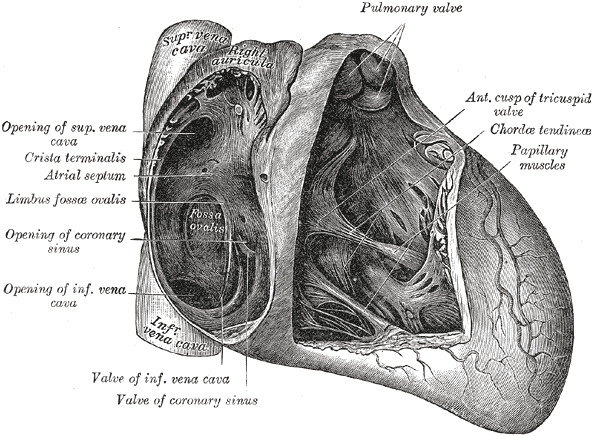 Interior of right side of heart.
Interior of right side of heart.

Congenital Abnormalities

Related Chapters
- ↑ Maganti K, Rigolin VH, Sarano ME, Bonow RO (2010). “Valvular heart disease: diagnosis and management”. Mayo Clin Proc. 85 (5): 483–500. doi:10.4065/mcp.2009.0706. PMC 2861980. PMID 20435842.
- ↑ 2.0 2.1 2.2 2.3 2.4 Schmoldt A, Benthe HF, Haberland G, Felt V, Nedvídková J, Hynie S, Mosinger B, Vavrinková M, Järvisalo J, Saris NE (September 1975). “Digitoxin metabolism by rat liver microsomes”. Biochem. Pharmacol. 24 (17): 1639–41. doi:10.1016/0006-2952(75)90009-x. PMC 5922622. PMID 10.
- ↑ Carabello BA (2005). “Modern management of mitral stenosis”. Circulation. 112 (3): 432–7. doi:10.1161/CIRCULATIONAHA.104.532498. PMID 16027271.
Classification
Classification
Pulmonary valve stenosis | Pulmonary subvalvular stenosis | Pulmonary supravalvular stenosis | Pulmonary valve atresia
Pathophysiology
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief:
Overview
pulmonic stenosis is most commonly secondary to acute rheumatic fever. Generally, the initial valvulitis is associated with valvular regurgitation but over a period of 2 or more years, the commissures fuse and the valves thicken and calcify. The chordal supporting structure also calcifies and retracts. The result is the typical “fish mouth deformity”. 70% of the time; the mitral valve is involved in isolation, and 25% of the time; the aortic valve is involved as well. The tricuspid and pulmonic valves are involved less commonly. Patients develop symptoms when the mitral vavle area is 2 to 2.5 cm2.
Pathophysiology
Almost all cases of pulmonic stenosis are due to disease in the heart secondary to rheumatic fever and the consequent rheumatic heart disease (a condition that may develop after strep throat or scarlet fever). Around 90% of cases of rheumatic heart disease are associated with pulmonic stenosis. Pulmonic stenosis is a progressive valvular disease which progression depends mainly on the degree of the narrowing of the pulmonic valve as well as on the maladaptive ventricular wall response. [1] [2][3] [4] [5] [5] [6] [4] [7] [8] [9] [10] [11] [5] [5][5] [12] [12] [13] [12]
Genetics
[Disease name] is transmitted in [mode of genetic transmission] pattern.
OR
Genes involved in the pathogenesis of [disease name] include:
- [Gene1]
- [Gene2]
- [Gene3]
OR
The development of [disease name] is the result of multiple genetic mutations such as:
- [Mutation 1]
- [Mutation 2]
- [Mutation 3]
Associated Conditions
Conditions associated with [disease name] include:
- [Condition 1]
- [Condition 2]
- [Condition 3]
Gross Pathology
On gross pathology, [feature1], [feature2], and [feature3] are characteristic findings of [disease name].
Microscopic Pathology
On microscopic histopathological analysis, [feature1], [feature2], and [feature3] are characteristic findings of [disease name].
References
- ↑ Scarlat A, Bodner G, Liron M (1986). “Massive haemoptysis as the presenting symptom in mitral stenosis”. Thorax. 41 (5): 413–4. PMC 1020641. PMID 3750250.
- ↑ Waller BF, Howard J, Fess S (1995). “Pathology of tricuspid valve stenosis and pure tricuspid regurgitation–Part I.” Clin Cardiol. 18 (2): 97–102. PMID 7720297.
- ↑ Maher ER, Pazianas M, Curtis JR (1987). “Calcific aortic stenosis: a complication of chronic uraemia”. Nephron. 47 (2): 119–22. PMID 3696315.
- ↑ 4.0 4.1 Hull MC, Morris CG, Pepine CJ, Mendenhall NP (2003). “Valvular dysfunction and carotid, subclavian, and coronary artery disease in survivors of hodgkin lymphoma treated with radiation therapy”. JAMA. 290 (21): 2831–7. doi:10.1001/jama.290.21.2831. PMID 14657067.
- ↑ 5.0 5.1 5.2 5.3 5.4 Dweck MR, Boon NA, Newby DE (2012). “Calcific aortic stenosis: a disease of the valve and the myocardium”. J Am Coll Cardiol. 60 (19): 1854–63. doi:10.1016/j.jacc.2012.02.093. PMID 23062541.
- ↑ Tamura T, Horiuchi H, Imai M, Tada T, Shiomi H, Kuroda M; et al. (2015). “Unexpectedly High Prevalence of Acquired von Willebrand Syndrome in Patients with Severe Aortic Stenosis as Evaluated with a Novel Large Multimer Index”. J Atheroscler Thromb. 22 (11): 1115–23. doi:10.5551/jat.30809. PMID 26269004.
- ↑ Cleland JG, Swedberg K, Follath F, Komajda M, Cohen-Solal A, Aguilar JC, Dietz R, Gavazzi A, Hobbs R, Korewicki J, Madeira HC, Moiseyev VS, Preda I, van Gilst WH, Widimsky J, Freemantle N, Eastaugh J, Mason J (2003). “The EuroHeart Failure survey programme– a survey on the quality of care among patients with heart failure in Europe. Part 1: patient characteristics and diagnosis”. European Heart Journal. 24 (5): 442–63. PMID 12633546. Retrieved 2012-04-11. Unknown parameter
|month=ignored (help) - ↑ Stewart BF, Siscovick D, Lind BK, Gardin JM, Gottdiener JS, Smith VE, Kitzman DW, Otto CM (1997). “Clinical factors associated with calcific aortic valve disease. Cardiovascular Health Study”. Journal of the American College of Cardiology. 29 (3): 630–4. PMID 9060903. Retrieved 2012-04-11. Unknown parameter
|month=ignored (help) - ↑ Galli D, Manuguerra R, Monaco R, Manotti L, Goldoni M, Becchi G; et al. (2016). “Understanding the structural features of symptomatic calcific aortic valve stenosis: A broad-spectrum clinicopathologic study in 236 consecutive surgical cases”. Int J Cardiol. 228: 364–374. doi:10.1016/j.ijcard.2016.11.180. PMID 27866029.
- ↑ Joseph J, Naqvi SY, Giri J, Goldberg S (2016). “Aortic stenosis: pathophysiology, diagnosis and therapy”. Am J Med. doi:10.1016/j.amjmed.2016.10.005. PMID 27810479.
- ↑ Otto CM, Prendergast B (2014). “Aortic-valve stenosis–from patients at risk to severe valve obstruction”. N Engl J Med. 371 (8): 744–56. doi:10.1056/NEJMra1313875. PMID 25140960.
- ↑ 12.0 12.1 12.2 Nishimura RA, Otto CM, Bonow RO, Carabello BA, Erwin JP, Guyton RA; et al. (2014). “2014 AHA/ACC guideline for the management of patients with valvular heart disease: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines”. J Am Coll Cardiol. 63 (22): e57–185. doi:10.1016/j.jacc.2014.02.536. PMID 24603191.
- ↑ Enriquez-Sarano M, Tajik AJ (2004). “Clinical practice. Aortic regurgitation”. N Engl J Med. 351 (15): 1539–46. doi:10.1056/NEJMcp030912. PMID 15470217.
Common Causes
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor-In-Chief: Varun Kumar, M.B.B.S.
Overview
Causes
Congenital
Common Causes
- Rheumatic heart disease [1] [2] [3] [4] [1][5]
- Sometimes described are intravenous leiomyomatosis, ventriculoatrial shunts causing TS.[6]
- Carcinoid syndrome[1] [7] [8] [9] [1] </ref> [6]
- Benign tumors like atrial myxomas can cause functional TS[10]. [11]
Causes by Organ System
| Cardiovascular | Congenital heart disease, cardiac tumor, saphenous vein bypass graft aneurysm,[12] Ebstein’s anomaly, endomyocardial fibrosis, infective endocarditis, myxoma, rheumatic heart disease |
| Chemical/Poisoning | No underlying causes |
| Dental | No underlying causes |
| Dermatologic | No underlying causes |
| Drug Side Effect | Methysergide |
| Ear Nose Throat | No underlying causes |
| Endocrine | Carcinoid syndrome |
| Environmental | No underlying causes |
| Gastroenterologic | No underlying causes |
| Genetic | No underlying causes |
| Hematologic | No underlying causes |
| Iatrogenic | Pacemaker infection, pacemaker leads[13], device closure of right coronary arteriovenous fistula.[14] |
| Infectious Disease | Infective endocarditis |
| Musculoskeletal/Orthopedic | No underlying causes |
| Neurologic | No underlying causes |
| Nutritional/Metabolic | Fabry disease, Whipple’s disease |
| Obstetric/Gynecologic | No underlying causes |
| Oncologic | Carcinoid syndrome, cardiac tumor, intravenous leiomyomatous tumor,[4] metastatic tumor, myxoma |
| Ophthalmologic | No underlying causes |
| Overdose/Toxicity | No underlying causes |
| Psychiatric | No underlying causes |
| Pulmonary | No underlying causes |
| Renal/Electrolyte | No underlying causes |
| Rheumatology/Immunology/Allergy | Amyloidosis,[15] systemic lupus erythematosus |
| Sexual | No underlying causes |
| Trauma | No underlying causes |
| Urologic | No underlying causes |
| Miscellaneous | Giant blood cyst |
- Tetralogy of fallot [16] Chronic turbulent flow through a deformed valve appears to cause these changes and as a result the valve looses it’s normal morphology.[17] [18] [19]
- Noonan syndrome
- Leopard syndrome
- William’s syndrome
- Alagille syndrome
- Congenital rubella syndrome
Acquired
- Carcinoid syndrome [20]
- Rheumatic fever [21]
- Homograft dysfunction[22]
- Pulmonary hypertension [23] [24]
Overview
Disease name] may be caused by [cause1], [cause2], or [cause3].
OR
Common causes of [disease] include [cause1], [cause2], and [cause3].
OR
The most common cause of [disease name] is [cause 1]. Less common causes of [disease name] include [cause 2], [cause 3], and [cause 4].
OR
The cause of [disease name] has not been identified. To review risk factors for the development of [disease name], click here.
Causes
Life-threatening Causes
- Life-threatening causes include conditions which may result in death or permanent disability within 24 hours if left untreated. There are no life-threatening causes of disease name, however complications resulting from untreated disease name is common.
- Life-threatening causes of [symptom/manifestation] include [cause1], [cause2], and [cause3].
- [Cause] is a life-threatening cause of [disease].
Common Causes
Common causes of [disease name] may include:
- [Cause1]
- [Cause2]
- [Cause3]
OR
- [Disease name] is caused by an infection with [pathogen name].
- [Pathogen name] is caused by [pathogen name].
Less Common Causes
Less common causes of [disease name] include:
- [Cause1]
- [Cause2]
- [Cause3]
Genetic Causes
- [Disease name] is caused by a mutation in the [gene name] gene.
Causes by Organ System
| Cardiovascular | No underlying causes |
| Chemical/Poisoning | No underlying causes |
| Dental | No underlying causes |
| Dermatologic | No underlying causes |
| Drug Side Effect | No underlying causes |
| Ear Nose Throat | No underlying causes |
| Endocrine | No underlying causes |
| Environmental | No underlying causes |
| Gastroenterologic | No underlying causes |
| Genetic | No underlying causes |
| Hematologic | No underlying causes |
| Iatrogenic | No underlying causes |
| Infectious Disease | No underlying causes |
| Musculoskeletal/Orthopedic | No underlying causes |
| Neurologic | No underlying causes |
| Nutritional/Metabolic | No underlying causes |
| Obstetric/Gynecologic | No underlying causes |
| Oncologic | No underlying causes |
| Ophthalmologic | No underlying causes |
| Overdose/Toxicity | No underlying causes |
| Psychiatric | No underlying causes |
| Pulmonary | No underlying causes |
| Renal/Electrolyte | No underlying causes |
| Rheumatology/Immunology/Allergy | No underlying causes |
| Sexual | No underlying causes |
| Trauma | No underlying causes |
| Urologic | No underlying causes |
| Miscellaneous | No underlying causes |
Causes in Alphabetical Order
List the causes of the disease in alphabetical order:
- Cause 1
- Cause 2
- Cause 3
- Cause 4
- Cause 5
- Cause 6
- Cause 7
- Cause 8
- Cause 9
- Cause 10
References
- ↑ 1.0 1.1 1.2 1.3 Waller BF, Howard J, Fess S (1995). “Pathology of tricuspid valve stenosis and pure tricuspid regurgitation–Part I.” Clin Cardiol. 18 (2): 97–102. PMID 7720297.
- ↑ Hull MC, Morris CG, Pepine CJ, Mendenhall NP (2003). “Valvular dysfunction and carotid, subclavian, and coronary artery disease in survivors of hodgkin lymphoma treated with radiation therapy”. JAMA. 290 (21): 2831–7. doi:10.1001/jama.290.21.2831. PMID 14657067.
- ↑ Gotoh T, Kuroda T, Yamasawa M, Nishinaga M, Mitsuhashi T, Seino Y; et al. (1995). “Correlation between lipoprotein(a) and aortic valve sclerosis assessed by echocardiography (the JMS Cardiac Echo and Cohort Study)”. Am J Cardiol. 76 (12): 928–32. PMID 7484833.
- ↑ 4.0 4.1 Nili M, Liban E, Levy MJ (June 1982). “Tricuspid stenosis due to intravenous leiomyomatosis–a call for caution: case report and review of the literature”. Tex Heart Inst J. 9 (2): 231–5. PMC 351617. PMID 15226964.
- ↑ Khatib N, Blumenfeld Z, Bronshtein M (November 2012). “Early prenatal diagnosis of tricuspid stenosis”. Am. J. Obstet. Gynecol. 207 (5): e6–8. doi:10.1016/j.ajog.2012.08.030. PMID 22964066.
- ↑ 6.0 6.1 Akram Q, Saravanan D, Levy R (April 2011). “Valvuloplasty for tricuspid stenosis caused by a ventriculoatrial shunt”. Catheter Cardiovasc Interv. 77 (5): 722–5. doi:10.1002/ccd.22745. PMID 20824751.
- ↑ Toy, Eugene, et al. Case Files: Internal Medicine. McGraw-Hill Companies, Inc. 2007. Page 43. ISBN 0071463038.
- ↑ Roberts WC, Ko JM (July 2008). “Some observations on mitral and aortic valve disease”. Proc (Bayl Univ Med Cent). 21 (3): 282–99. doi:10.1080/08998280.2008.11928412. PMC 2446420. PMID 18628928.
- ↑ Baumgartner H, Hung J, Bermejo J, Chambers JB, Evangelista A, Griffin BP; et al. (2009). “Echocardiographic assessment of valve stenosis: EAE/ASE recommendations for clinical practice”. Eur J Echocardiogr. 10 (1): 1–25. doi:10.1093/ejechocard/jen303. PMID 19065003.
- ↑ Şaşkın H, Düzyol Ç, Özcan KS, Aksoy R (August 2015). “Right atrial myxoma mimicking tricuspid stenosis”. BMJ Case Rep. 2015. doi:10.1136/bcr-2015-210818. PMC 4550937. PMID 26272962.
- ↑ Muraru D, Badano LP, Sarais C, Soldà E, Iliceto S (June 2011). “Evaluation of tricuspid valve morphology and function by transthoracic three-dimensional echocardiography”. Curr Cardiol Rep. 13 (3): 242–9. doi:10.1007/s11886-011-0176-3. PMID 21365261.
- ↑ Jellis CL, Navia JL, Flamm SD, Rodriguez LL (2016). “Severe Functional Tricuspid Stenosis Secondary to a Giant Saphenous Vein Bypass Graft Aneurysm”. Circulation. 133 (21): 2099–102. doi:10.1161/CIRCULATIONAHA.115.014772. PMID 27217436 PMID: 27217436 Check
|pmid=value (help). - ↑ Taira K, Suzuki A, Fujino A, Watanabe T, Ogyu A, Ashikawa K (2006). “Tricuspid valve stenosis related to subvalvular adhesion of pacemaker lead: a case report”. J Cardiol. 47 (6): 301–6. PMID 16800373.
- ↑ Changchien C, Lin MT, Wang CC, Liu HM, Wang CC, Chiu SN; et al. (2015). “Neonatal tricuspid stenosis caused by device closure of a large coronary fistula”. EuroIntervention. 11 (7): e1. doi:10.4244/EIJV11I7A162. PMID 26603866 PMID: 26603866 Check
|pmid=value (help). - ↑ Kim KH, Park CH, Park HS, Kim YR, Choi EY (2014). “Amyloidosis-induced tricuspid stenosis mimicking rheumatic heart disease”. Eur Heart J Cardiovasc Imaging. 15 (10): 1167. doi:10.1093/ehjci/jeu075. PMID 24797117.
- ↑ Horstkotte D, Niehues R, Strauer BE (1991). “Pathomorphological aspects, aetiology and natural history of acquired mitral valve stenosis”. Eur Heart J. 12 Suppl B: 55–60. PMID 1936027.
- ↑ Marcus RH, Sareli P, Pocock WA, Barlow JB (1994). “The spectrum of severe rheumatic mitral valve disease in a developing country. Correlations among clinical presentation, surgical pathologic findings, and hemodynamic sequelae”. Ann Intern Med. 120 (3): 177–83. PMID 8043061.
- ↑ Carabello BA (2005). “Modern management of mitral stenosis”. Circulation. 112 (3): 432–7. doi:10.1161/CIRCULATIONAHA.104.532498. PMID 16027271.
- ↑ Maganti K, Rigolin VH, Sarano ME, Bonow RO (2010). “Valvular heart disease: diagnosis and management”. Mayo Clin Proc. 85 (5): 483–500. doi:10.4065/mcp.2009.0706. PMC 2861980. PMID 20435842.
- ↑ Mohamed AL, Zain MM (2004). “Hoarseness of Voice in a Patient with Mitral Stenosis and Ortner’s Syndrome”. Malays J Med Sci. 11 (2): 65–8. PMC 3433978. PMID 22973129.
- ↑ Linefsky JP, O’Brien KD, Katz R, de Boer IH, Barasch E, Jenny NS; et al. (2011). “Association of serum phosphate levels with aortic valve sclerosis and annular calcification: the cardiovascular health study”. J Am Coll Cardiol. 58 (3): 291–7. doi:10.1016/j.jacc.2010.11.073. PMC 3147295. PMID 21737022.
- ↑ Inglessis I, Landzberg MJ (2007). “Interventional catheterization in adult congenital heart disease”. Circulation. 115 (12): 1622–33. doi:10.1161/CIRCULATIONAHA.105.592428. PMID 17389281.
- ↑ Roberts WC (1973). “Valvular, subvalvular and supravalvular aortic stenosis: morphologic features”. Cardiovasc Clin. 5 (1): 97–126. PMID 4272665.
- ↑ Lucena CM, Santos RP (2015). “Association between Aortic Valve Sclerosis and Adverse Cardiovascular Events”. Arq Bras Cardiol. 105 (1): 99. doi:10.5935/abc.20150081. PMC 4523295. PMID 26270071.
Differentiating Right ventricular outflow tract obstruction from other Diseases
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor-In-Chief: Cafer Zorkun, M.D., Ph.D. [2]; Keri Shafer, M.D. [3]
Overview
Right ventricular outflow tract obstruction must be distinguished from an ASD, a small VSD, aortic stenosis, and acyanotic or pink tetralogy of Fallot.
Differentiating Right ventricular outflow tract obstruction from other Diseases
Right ventricular outflow tract obstruction must be distinguished from several other conditions. [1]
1. Atrial septal defect: Also has a systolic ejection murmur, wide fixed split S2, EKG showing RVH. In ASD the split of the S2 is fixed, there is no ejection click. [2]
2. Small Ventricular septal defect: Amyl nitrate increases venous return and increases the murmur of pulmonary stenosis, in VSD the murmur becomes softer.
3. Mild left-sided outflow obstruction: With valsalva maneuver the murmur of aortic stenosis becomes softer after about 5 beats, with pulmonary stenosis it becomes softer within 3 beats.
4. Acyanotic or pink tetralogy of Fallot: with amyl nitrate and increased venous return the murmur of PS increases, and the murmur of tetralogy decreases because of peripheraldilation and an increase in right to left shunting. [3]
The differential diagnosis of aortic regurgitation includes other valvular abnormalities:[4][5][6][7][8][9]
- Aortic stenosis: The murmur of aortic stenosis is harsh and best heard at the right second intercostal space.
- Mitral regurgitation: The murmur of mitral regurgitation is blowing, soft and best heard at the apex.
- Mitral stenosis: The murmur of mitral stenosis is mid-diastolic, rumbling, and best heard after the opening snap.
- Tricuspid regurgitation: The murmur of tricuspid regurgitation is blowing, holosystolic, and best heard over the fourth intercostal area at the left sternal border.
- Tricuspid stenosis: The murmur of tricuspid stenosis is characterized by a mid diastolic murmur best heard over the left sternal border with rumbling character and tricuspid opening snap with wide splitting of S1.
Aortic regurgitation should also be differentiated from other diseases that might cause similar clinical presentation, such as:[10][11][12][13]
- Acute coronary syndrome
- Anemia
- Heart failure
- Infective endocarditis
- Patent ductus arteriosus
- Pregnancy
- Thyrotoxicosis
- Volume depletion
- Wet beriberi
Following are the cardiac conditions having similar presentation as Aortic regurgitation:[14][15][16][17][18][19][20][21][22][23][24][25][26][27][28][29][30][31][32][33][34][35][36]
| Diseases | History | Symptoms | Physical Examination | Murmur | Diagnosis | Other Findings | |||
|---|---|---|---|---|---|---|---|---|---|
| ECG | CXR | Echocardiogram | Cardiac Catheterization | ||||||
| Mitral Stenosis |
|
|
|
|
|
|
|
Right heart catheterization:
Left heart catheterization:
|
|
| Mitral Regurgitation |
|
|
Palpation
Auscultation
|
|
|
Acute MR
Chronic MR
|
|
|
|
| Atrial septal defect |
|
|
Inspection
Palpation
Auscultation
|
|
|
|
|
|
|
| Left Atrial Myxoma |
|
|
Skin
Auscultation:
|
|
|
Rare findings:
|
|
|
|
| Prosthetic Valve Obstruction |
|
|
Ausculation
Muffling of murmur |
|
|
Causes:
| |||
| Cor Triatriatum |
|
|
Auscultation
Other findings
|
|
Non specific but may have
|
|
|
|
Types
|
| Congenital Mitral Stenosis |
|
Infants:
Older patients:
|
Auscultation
Other findings
|
Mild-Moderate
Severe
|
|
|
|
Very rare condition | |
| Supravalvular Ring Mitral Stenosis |
|
|
Auscultation:
Lungs: Fine, crepitant rales and rhonchi or wheezes may be present Heart: Murmur |
|
|
Supramitral ring:
Intramitral ring:
(Difficult to visualize membrane <1mm in size) |
|
Types
It is attached between the opening of the atrial appendage and the mitral annulus which helps in differentiating with Cor triatriatum sinister.
| |
References
- ↑ Waller BF, Howard J, Fess S (February 1995). “Pathology of tricuspid valve stenosis and pure tricuspid regurgitation–Part I”. Clin Cardiol. 18 (2): 97–102. doi:10.1002/clc.4960180212. PMID 7720297.
- ↑ REID JM, STEVENSON JG, BARCLAY RS, WELSH TM (1962). “Combined aortic and mitral stenosis”. Br Heart J. 24: 509–15. PMC 1017912. PMID 14491175.
- ↑ Shinoda H, Stern PH (1992). “Diurnal rhythms in Ca transfer into bone, Ca release from bone, and bone resorbing activity in serum of rats”. Am J Physiol. 262 (2 Pt 2): R235–40. PMID 1539731.
- ↑ Nishimura RA, Otto CM, Bonow RO, Carabello BA, Erwin JP, Guyton RA; et al. (2014). “2014 AHA/ACC guideline for the management of patients with valvular heart disease: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines”. J Am Coll Cardiol. 63 (22): e57–185. doi:10.1016/j.jacc.2014.02.536. PMID 24603191.
- ↑ Lindman BR, Clavel MA, Mathieu P, Iung B, Lancellotti P, Otto CM; et al. (2016). “Calcific aortic stenosis”. Nat Rev Dis Primers. 2: 16006. doi:10.1038/nrdp.2016.6. PMC 5127286. PMID 27188578.
- ↑ Chandrashekhar Y, Westaby S, Narula J (2009). “Mitral stenosis”. Lancet. 374 (9697): 1271–83. doi:10.1016/S0140-6736(09)60994-6. PMID 19747723.
- ↑ Chockalingam A, Gnanavelu G, Elangovan S, Chockalingam V (2003). “Clinical spectrum of chronic rheumatic heart disease in India”. J Heart Valve Dis. 12 (5): 577–81. PMID 14565709.
- ↑ Zoghbi WA, Enriquez-Sarano M, Foster E, Grayburn PA, Kraft CD, Levine RA; et al. (2003). “Recommendations for evaluation of the severity of native valvular regurgitation with two-dimensional and Doppler echocardiography”. J Am Soc Echocardiogr. 16 (7): 777–802. doi:10.1016/S0894-7317(03)00335-3. PMID 12835667.
- ↑ Roguin A, Rinkevich D, Milo S, Markiewicz W, Reisner SA (1998). “Long-term follow-up of patients with severe rheumatic tricuspid stenosis”. Am Heart J. 136 (1): 103–8. PMID 9665226.
- ↑ Choudhry NK, Etchells EE (1999). “The rational clinical examination. Does this patient have aortic regurgitation?”. JAMA. 281 (23): 2231–8. PMID 10376577.
- ↑ Elkayam U, Goland S, Pieper PG, Silverside CK (2016). “High-Risk Cardiac Disease in Pregnancy: Part I.” J Am Coll Cardiol. 68 (4): 396–410. doi:10.1016/j.jacc.2016.05.048. PMID 27443437.
- ↑ Lozano HF, Sharma CN (2004). “Reversible pulmonary hypertension, tricuspid regurgitation and right-sided heart failure associated with hyperthyroidism: case report and review of the literature”. Cardiol Rev. 12 (6): 299–305. doi:10.1097/01.crd.0000137259.83169.e3. PMID 15476566.
- ↑ Anand IS (2016). “High-Output Heart Failure Revisited”. J Am Coll Cardiol. 68 (5): 483–6. doi:10.1016/j.jacc.2016.05.036. PMID 27470456.
- ↑ Nassar PN, Hamdan RH (2011). “Cor Triatriatum Sinistrum: Classification and Imaging Modalities”. Eur J Cardiovasc Med. 1 (3): 84–87. doi:10.5083/ejcm.20424884.21. PMC 3286827. PMID 22379596.
- ↑ Roudaut R, Serri K, Lafitte S (2007). “Thrombosis of prosthetic heart valves: diagnosis and therapeutic considerations”. Heart. 93 (1): 137–42. doi:10.1136/hrt.2005.071183. PMC 1861363. PMID 17170355.
- ↑ Apostolakis EE, Baikoussis NG (2009). “Methods of estimation of mitral valve regurgitation for the cardiac surgeon”. J Cardiothorac Surg. 4: 34. doi:10.1186/1749-8090-4-34. PMC 2723095. PMID 19604402.
- ↑ Alboliras ET, Edwards WD, Driscoll DJ, Seward JB (1987). “Cor triatriatum dexter: two-dimensional echocardiographic diagnosis”. J Am Coll Cardiol. 9 (2): 334–7. PMID 3805524.
- ↑ Gibson DG, Honey M, Lennox SC (1974). “Cor triatriatum. Diagnosis by echocardiography”. Br Heart J. 36 (8): 835–8. PMC 458901. PMID 4412638.
- ↑ Cor triatrium https://radiopaedia.org/articles/cor-triatriatum (2016) Accessed on November 29, 2016
- ↑ Sosland RP, Vacek JL, Gorton ME (2007). “Congenital mitral stenosis: a rare presentation and novel approach to management”. J Thorac Cardiovasc Surg. 133 (2): 572–3. doi:10.1016/j.jtcvs.2006.10.025. PMID 17258606.
- ↑ Driscoll DJ, Gutgesell HP, McNamara DG (1978). “Echocardiographic features of congenital mitral stenosis”. Am J Cardiol. 42 (2): 259–66. PMID 685838.
- ↑ Bonou M, Lampropoulos K, Barbetseas J (2012). “Prosthetic heart valve obstruction: thrombolysis or surgical treatment?”. Eur Heart J Acute Cardiovasc Care. 1 (2): 122–7. doi:10.1177/2048872612451169. PMC 3760527. PMID 24062899.
- ↑ Maganti K, Rigolin VH, Sarano ME, Bonow RO (2010). “Valvular heart disease: diagnosis and management”. Mayo Clin Proc. 85 (5): 483–500. doi:10.4065/mcp.2009.0706. PMC 2861980. PMID 20435842.
- ↑ DEXTER L (1956). “Atrial septal defect”. Br Heart J. 18 (2): 209–25. PMC 479579. PMID 13315850.
- ↑ Webb G, Gatzoulis MA (2006). “Atrial septal defects in the adult: recent progress and overview”. Circulation. 114 (15): 1645–53. doi:10.1161/CIRCULATIONAHA.105.592055. PMID 17030704.
- ↑ Geva T, Martins JD, Wald RM (2014). “Atrial septal defects”. Lancet. 383 (9932): 1921–32. doi:10.1016/S0140-6736(13)62145-5. PMID 24725467.
- ↑ Demir M, Akpinar O, Acarturk E (2005). “Atrial myxoma: an unusual cause of myocardial infarction”. Tex Heart Inst J. 32 (3): 445–7. PMC 1336732. PMID 16392241.
- ↑ MacGowan SW, Sidhu P, Aherne T, Luke D, Wood AE, Neligan MC; et al. (1993). “Atrial myxoma: national incidence, diagnosis and surgical management”. Ir J Med Sci. 162 (6): 223–6. PMID 8407260.
- ↑ Circulation http://circ.ahajournals.org/content/119/7/1034 (2016) Accessed on December 7, 2016
- ↑ Alphonso N, Nørgaard MA, Newcomb A, d’Udekem Y, Brizard CP, Cochrane A (2005). “Cor triatriatum: presentation, diagnosis and long-term surgical results”. Ann Thorac Surg. 80 (5): 1666–71. doi:10.1016/j.athoracsur.2005.04.055. PMID 16242436.
- ↑ circulation http://circ.ahajournals.org/content/36/1/101 (1967) Accessed on 7 December, 2016
- ↑ Moore P, Adatia I, Spevak PJ, Keane JF, Perry SB, Castaneda AR; et al. (1994). “Severe congenital mitral stenosis in infants”. Circulation. 89 (5): 2099–106. PMID 8181134.
- ↑ Uva MS, Galletti L, Gayet FL, Piot D, Serraf A, Bruniaux J; et al. (1995). “Surgery for congenital mitral valve disease in the first year of life”. J Thorac Cardiovasc Surg. 109 (1): 164–74, discussion 174-6. doi:10.1016/S0022-5223(95)70432-9. PMID 7815793.
- ↑ Banerjee A, Kohl T, Silverman NH (1995). “Echocardiographic evaluation of congenital mitral valve anomalies in children”. Am J Cardiol. 76 (17): 1284–91. PMID 7503011.
- ↑ Sullivan ID, Robinson PJ, de Leval M, Graham TP (1986). “Membranous supravalvular mitral stenosis: a treatable form of congenital heart disease”. J Am Coll Cardiol. 8 (1): 159–64. PMID 3711511.
- ↑ Subramaniam V, Herle A, Mohammed N, Thahir M (2011). “Ortner’s syndrome: case series and literature review”. Braz J Otorhinolaryngol. 77 (5): 559–62. PMID 22030961.
Epidemiology and Demographics
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor-In-Chief: Varun Kumar, M.B.B.S.
Overview
Isolated pulmonic valvular stenosis with intact ventricular septum is the second most common congenital cardiac defect.
Epidemiology and Demographics
Right ventricular outflow tract obstruction represents 8-12% of all congenital heart defects in children[1][2] and 15% of all congenital heart defects in adults[3][4][5]. Isolated pulmonic valvular stenosis with intact ventricular septum is the second most common congenital cardiac defect. [6] [7]
Right ventricular outflow tract obstruction secondary to rheumatic fever is rare and it seldom causes serious pulmonic valvular deformity. It usually may occur in association with the pulmonary hypertension that occurs at high altitudes. The prevalence of rheumatic disease in developed nations is steadily declining. Developing countries, in contrast, have higher rates of rheumatic fever and subsequent mitral stenosis with a prevalence of more than 10 cases per 1,000 in India and 4-10 cases per 1,000 in China, Russia, Africa and Australia. [8] [9] [10].
Age
Right ventricular outflow tract obstruction usually occurs in newborn. However, the age at presentation depends on the severity of the obstruction with many patients with mild obstruction presenting at adolescence or adulthood. [9] [11]
Race
Prevalence of pulmonary stenosis does not differ significantly with race.[12] [8]
Gender
Prevalence of right ventricular outflow tract is equal among males and females.[3] [7]
References
- ↑ Keith JD, Rowe RD, Vlad P. Heart Disease in Infancy and Childhood. 3rd ed. New York, NY: Macmillan Co; 1978:4-6, 761-88
- ↑ Nadas A. Pulmonary stenosis. In: Fyler DC, ed. Nadas’ Pediatric Cardiology. Hanley & Belfus;1992:459-470.
- ↑ 3.0 3.1 Johnson LW, Grossman W, Dalen JE, Dexter L (1972). “Pulmonic stenosis in the adult. Long-term follow-up results”. N Engl J Med. 287 (23): 1159–63. doi:10.1056/NEJM197212072872301. PMID 5082217.
- ↑ CAMPBELL M (1954). “Simple pulmonary stenosis; pulmonary valvular stenosis with a closed ventricular septum”. Br Heart J. 16 (3): 273–300. PMC 479528. PMID 13182146.
- ↑ ABRAHAMS DG, WOOD P (1951). “Pulmonary stenosis with normal aortic root”. Br Heart J. 13 (4): 519–48. PMC 503699. PMID 14886471.
- ↑ Frantz C, Stewart KM, Weaver VM (2010). “The extracellular matrix at a glance”. J Cell Sci. 123 (Pt 24): 4195–200. doi:10.1242/jcs.023820. PMC 2995612. PMID 21123617.
- ↑ 7.0 7.1 Bonow RO, Carabello BA, Chatterjee K, de Leon AC, Faxon DP, Freed MD; et al. (2008). “2008 Focused update incorporated into the ACC/AHA 2006 guidelines for the management of patients with valvular heart disease: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Revise the 1998 Guidelines for the Management of Patients With Valvular Heart Disease): endorsed by the Society of Cardiovascular Anesthesiologists, Society for Cardiovascular Angiography and Interventions, and Society of Thoracic Surgeons”. Circulation. 118 (15): e523–661. doi:10.1161/CIRCULATIONAHA.108.190748. PMID 18820172.
- ↑ 8.0 8.1 Seckeler MD, Hoke TR (2011). “The worldwide epidemiology of acute rheumatic fever and rheumatic heart disease”. Clin Epidemiol. 3: 67–84. doi:10.2147/CLEP.S12977. PMC 3046187. PMID 21386976.
- ↑ 9.0 9.1 Dweck MR, Boon NA, Newby DE (2012). “Calcific aortic stenosis: a disease of the valve and the myocardium”. J Am Coll Cardiol. 60 (19): 1854–63. doi:10.1016/j.jacc.2012.02.093. PMID 23062541.
- ↑ Salem A, Abdelgawad A, Elshemy A (August 2018). “Early and Midterm Outcomes of Rheumatic Mitral Valve Repair”. Heart Surg Forum. 21 (5): E352–E358. doi:10.1532/hsf.1978. PMID 30311884. Vancouver style error: initials (help)
- ↑ Nassar PN, Hamdan RH (2011). “Cor Triatriatum Sinistrum: Classification and Imaging Modalities”. Eur J Cardiovasc Med. 1 (3): 84–87. doi:10.5083/ejcm.20424884.21. PMC 3286827. PMID 22379596.
- ↑ Rao PS. Demographic features of tricuspid atresia. In: Rao PS, ed. Tricuspid Atresia. 2nd ed. Mt. Kisco, NY: Futura; 1992:23-37.
Risk Factors
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]
Overview
The most common risk factor for the development of pulominic stenosis is the presence of a congenital bicuspid pulmonic valve. Risk factors that may speed up the progression of pulmonic stenosis include the same risk factors as atherosclerosis. [1]
Overview
There are no established risk factors for [disease name].
OR
The most potent risk factor in the development of [disease name] is [risk factor 1]. Other risk factors include [risk factor 2], [risk factor 3], and [risk factor 4].
OR
Common risk factors in the development of [disease name] include [risk factor 1], [risk factor 2], [risk factor 3], and [risk factor 4].
OR
Common risk factors in the development of [disease name] may be occupational, environmental, genetic, and viral.
Risk Factors
There are no established risk factors for [disease name]. [2]
OR
The most potent risk factor in the development of [disease name] is [risk factor 1]. Other risk factors include [risk factor 2], [risk factor 3], and [risk factor 4].
OR
Common risk factors in the development of [disease name] include [risk factor 1], [risk factor 2], [risk factor 3], and [risk factor 4].
Common Risk Factors
- Common risk factors in the development of [disease name] may be occupational, environmental, genetic, and viral. [3]
- Common risk factors in the development of [disease name] include:
- [Risk factor 1]
- [Risk factor 2]
- [Risk factor 3]
Less Common Risk Factors
- Less common risk factors in the development of [disease name] include:
- [Risk factor 1]
- [Risk factor 2]
- [Risk factor 3]
References
- ↑ Roberts WC (1973). “Valvular, subvalvular and supravalvular aortic stenosis: morphologic features”. Cardiovasc Clin. 5 (1): 97–126. PMID 4272665.
- ↑ Rajamannan NM, Nealis TB, Subramaniam M, Pandya S, Stock SR, Ignatiev CI; et al. (2005). “Calcified rheumatic valve neoangiogenesis is associated with vascular endothelial growth factor expression and osteoblast-like bone formation”. Circulation. 111 (24): 3296–301. doi:10.1161/CIRCULATIONAHA.104.473165. PMID 15956138.
- ↑ Waller BF, Howard J, Fess S (March 1995). “Pathology of tricuspid valve stenosis and pure tricuspid regurgitation–Part II”. Clin Cardiol. 18 (3): 167–74. doi:10.1002/clc.4960180312. PMID 7743689.
Template:WH Template:WS [[Category: (name of the system)]
Natural History, Complications and Prognosis
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]
Overview
If left untreated, [#]% of patients with [disease name] may progress to develop [manifestation 1], [manifestation 2], and [manifestation 3].
OR
Common complications of [disease name] include [complication 1], [complication 2], and [complication 3].
OR
Prognosis is generally excellent/good/poor, and the 1/5/10-year mortality/survival rate of patients with [disease name] is approximately [#]%.
Natural History, Complications, and Prognosis
Natural History
Patients with congenital pulmonary stenosis manifest clinical features few hours after birth, in childhood or in adulthood. Manifestation of symptoms, symptom severity and the outcomes are dependent on the severity of stenosis.[1] Patients with mild pulmonic stenosis have a benign course and do not progress and patients with moderate and severe stenosis have dyspnea with exertion and syncope.[2]
Complications
If left untreated, patients with moderate to severe stenosis progress to develop tricuspid regurgitation and right ventricular dysfunction leading to right ventricular failure and arrhythmias.[3]
Prognosis
Patients with moderate to severe pulmonic valve stenosis are managed well with surgery or balloon valvuloplasty and have very good prognosis. [4]
References
- ↑ Hayes CJ, Gersony WM, Driscoll DJ, Keane JF, Kidd L, O’Fallon WM; et al. (1993). “Second natural history study of congenital heart defects. Results of treatment of patients with pulmonary valvar stenosis”. Circulation. 87 (2 Suppl): I28–37. PMID 8425320.
- ↑ Mody MR (1975). “The natural history of uncomplicated valvular pulmonic stenosis”. Am Heart J. 90 (3): 317–21. PMID 1163423.
- ↑ Wolfe RR, Driscoll DJ, Gersony WM, Hayes CJ, Keane JF, Kidd L; et al. (1993). “Arrhythmias in patients with valvar aortic stenosis, valvar pulmonary stenosis, and ventricular septal defect. Results of 24-hour ECG monitoring”. Circulation. 87 (2 Suppl): I89–101. PMID 8425327.
- ↑ Bonow RO, Carabello BA, Chatterjee K, de Leon AC, Faxon DP, Freed MD; et al. (2008). “2008 Focused update incorporated into the ACC/AHA 2006 guidelines for the management of patients with valvular heart disease: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Revise the 1998 Guidelines for the Management of Patients With Valvular Heart Disease): endorsed by the Society of Cardiovascular Anesthesiologists, Society for Cardiovascular Angiography and Interventions, and Society of Thoracic Surgeons”. Circulation. 118 (15): e523–661. doi:10.1161/CIRCULATIONAHA.108.190748. PMID 18820172.
Diagnosis
Diagnosis
History and Symptoms | Physical Examination | Electrocardiogram | Chest X Ray | Echocardiography | Cardiac Catheterization | Pulmonary Angiography
Treatment
Treatment
Indications For Surgery | Surgery | Pre-Operative A/P | Post-Operative A/P | Cost-Effectiveness of Therapy | Future or Investigational Therapies
Special Scenario
Special Scenario
Looking for the patient version?
© 2026 MyEClinic – IFTM Institut für Telematik in der Medizin GmbH