
Hyperparathyroidism
For patient information click here
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Anmol Pitliya, M.B.B.S. M.D.[2]
Synonyms and keywords: Hyperparathyroid; parathyroid hormone levels raised; parathyroid related hypercalcemia; overactive parathyroid glands
Overview
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1];Associate Editor(s)-in-Chief: Anmol Pitliya, M.B.B.S. M.D.[2]
Overview
Hyperparathyroidism is overactivity of the parathyroid glands resulting in excess production of parathyroid hormone (PTH). The parathyroid hormone monitors calcium and phosphorus levels and helps to maintain these levels. Overactivity of one or more of the parathyroid glands causes high calcium levels (hypercalcemia) and low levels of phosphorus in the blood. Hyperparathyroidism was first described and treated in the 1930s by Fuller Albright of Massachusetts General Hospital, working at the Mallinckrodt General Clinical Research Center.
Historical Perspective
In 1880, Ivar Sandström, a Swedish anatomist, described parathyroids in human following 50 autopsies. In 1924, James Bertram Collip, a Canadian biochemist, discovered and extracted parathyroid hormone and treated tetany with the help of parathyroid extract along with Douglous B Leitch. In 1925, Felix Mandl, a viennese surgeon performed first parathyroidectomy to treat a patient suffering from osteitis fibrosa cystica. In 1959, Howard Rasmussen and Lyman C. Craig at the Rockefeller Institute for Medical Research purified parathyroid hormone. They also isolated the active polypeptide (parathormone B) from bovine parathyroid gland and gave its tentative formula in 1961.
Classification
Hyperparathyroidism can be classified according to origin of defect into primary, secondary and tertiary. Primary hyperparathyroidism results from a hyperfunction of the parathyroid glands themselves. There is oversecretion of PTH due to adenoma, hyperplasia or, rarely, carcinoma of the parathyroid glands. Secondary hyperparathyroidism is due to increase in secretion of parathyroid hormone from a secondary process. Tertiary hyperparathyroidism is a state of excessive secretion of parathyroid hormone (PTH) after a long period of secondary hyperparathyroidism and resulting in hypercalcemia even after treatment of secondary hyperparathyroidism..
Pathophysiology
Hyperparathyroidism is an increase in serum parathyroid hormone. Normally, parathyroid hormone increases serum calcium and magnesium concentration, and decreases serum phosphate concentration. Secretion of parathyroid hormone from parathyroid gland is stimulated by low serum calcium. Parathyroid glands have calcium-sensing receptors responsible for sensing extracellular ionized calcium. Calcium and magnesium provides a negative feedback for secretion of parathyroid hormone. Primary hyperparathyroidism is due to increase in secretion of parathyroid hormone from a primary process in parathyroid gland.Majority of times, increase in secretion of parathyroid hormone is the result of parathyroid adenoma (85%). Calcium-sensing receptor expression is reduced in parathyroid adenoma resulting in an increase in calcium sensing set point. In minority of cases, development of primary hyperparathyroidism is the result of multiple genetic mutations. Genes involved in the pathogenesis of primary hyperparathyroidism include calcium-sensing receptor gene, HRPT2 gene (CDC73 gene), Cyclin D1 gene (CCND1)/PRAD1 gene, MEN1 gene, and RET gene. Secondary hyperparathyroidism is due to increase in secretion of parathyroid hormone from a secondary process, most commonly due chronic renal failure. Fibroblast growth factor 23 (FGF-23) concentration increases in chronic renal failure which plays a central role in regulation of phosphate, vitamin D homeostasis and pathogenesis of secondary hyperparathyroidism. Majority of times, tertiary hyperparathyroidism occurs in patients after renal transplantation.Patients with secondary hyperparathyroidism continues to have elevated parathyroid hormone even after renal transplantation. Classically, there is hyperplasia of all four of parathyroid gland. On gross pathology, parathyroid adenoma is a soft, tan nodule which is well-circumscribed by a delicate capsule. Typically, cut surface of parathyroid adenoma is smooth, soft, and reddish brown in color. It should be differentiated from normal parathyroid gland tissue which is yellow-brown color. Parathyroid hyperplasia usually involves multiple glands. Bones and kidney are also commonly involved in hyperparathyroidism. Hypercalcemia due to hyperparathyroidism may cause metastatic calcification in many organs including lungs, heart, blood vessels, stomach. Chief cells are predominant in parathyroid adenoma on microcopy. Adenoma is seperated from a rim of non-neoplastic tissue on the edge by a fibrous capsule. Endocrine atypia (cells with bizarre and pleomorphic nuclei) is often seen in parathyroid adenoma. It should not be mistaken as a sign of malignancy. Majority of times, hyperplasia of chief cells is observed in parathyroid hyperplasia. It may be diffuse or multinodular. Cytologic details are unreliable for diagnosis of parathyroid carcinoma.
Causes
Hyperparathyroidism is caused by an increase in concentration of parathyroid hormone in serum. There are three type of hyperparathyroidism including primary, secondary and tertiary hyperparathyroidism. There are an array of different causes for all types of hyperparathyroidism. Most common cause of primary hyperparathyroidism is parathyroid adenoma (85%) followed by parathyroid hyperplasia (15%), and parathyroid carcinoma (5%). Most common cause of secondary hyperparathyroidism is chronic renal failure and vitamin D deficiency. Most common cause of tertiary hyperparathyroidism is post renal transplantation.
Differentiating Hyperparathyroidism from Other Diseases
There are three types of hyperparathyroidism (primary, secondary, and tertiary) and should be differentiated between each other. Hyperparathyroidism should be differentiated from other causes of hypercalcemia. Causes of hypercalcemia other than hyperparathyroidism include familial hypocalciuric hypercalcemia, hypercalcemia related to malignancy, medication-induced hypercalcemia, hypercalcemia due to nutritional disorders, and hypercalcemia related to granulomatous diseases.
Epidemiology and Demographics
Primary hyperparathyroidism is the 3rd most common endocrine disorder. Highest incidence of primary hyperparathyroidism is in post-menopausal women.The incidence of primary hyperparathyroidism is approximately 0.4 to 21.6 per 100,000 person years. The prevalence of primary hyperparathyroidism is approximately .01 to .07 per 100,000 individuals. The incidence of primary hyperparathyroidism increases with age. Primary hyperparathyroidism usually affects individuals of African-American race. Women are more commonly affected by primary hyperparathyroidism than men. The women to men ratio is approximately 3 to 1. Difference in gender specific incidence of primary hyperparathyroidism becomes more pronounced with advancing age. There is insufficient data on epidemiology and demographics of secondary and tertiary hyperparathyroidism.
Risk Factors
Common risk factors in the development of primary hyperparathyroidism include postmenopausal women, age group 50-60 year, family history of hyperparathyroidism, and history of familial syndromes. Common risk factors in the development of secondary hyperparathyroidism in chronic renal failure include high serum phosphorus expression levels, low serum creatinine expression levels, low serum calcium expression levels, female gender, and hypertension. Common risk factors in the development of tertiary hyperparathyroidism post renal transplantation include elderly individuals and longer duration of dialysis.
Screening
There is insufficient evidence to recommend routine screening for hyperparathyroidism.
Natural History, Complications, and Prognosis
Primary hyperparathyroidism usually develops in the fifth decade of life, in post-menopausal women and starts as asymptomatic hypercalcemia in presence of increased parathyroid hormone. If left untreated, some of patients with primary hyperparathyroidism may commonly develop marked hypercalcemia, marked hypercalciuria, cortical bone demineralization and nephrolithiasis.
Secondary hyperparathyroidism arise in the early course of chronic renal failure. As renal failure progress, secondary hyperparathyroidism becomes more notable. If left untreated, secondary hyperparathyroidism carries an increased risk of vascular calcification with increasing age and duration of dialysis in patients.
Tertiary hyperparathyroidism usually develops in post renal transplant patients. If left untreated, tertiary hyperparathyroidism in post renal transplant patients may carry the risk of amyloid deposition, calciphylaxis, destructive or erosive spondyloarthropathy, osteonecrosis, and musculoskeletal infections.
Hyperparathyroidism leads to a variety of complications in various organ systems depending on the type of hyperparathyroidism.
Prognosis is all types hyperparathyroidism is generally good after proper treatment.
Diagnosis
History and Symptoms
The majority of patients with primary hyperparathyroidism are asymptomatic. Asymptomatic primary hyperparathyroidism patient is expected to develop signs and symptoms, but most of the patients does not becomes symptomatic with time. The hallmark of primary hyperparathyroidism is asymptomatic hypercalcemia. The classic signs and symptoms of primary hyperparathyroidism are present in a few individuals and are summarized by the mnemonic painful bones, kidney stones, abdominal groans, psychic moans, and fatigue overtones.The majority of patients with secondary hyperparathyroidism have a history of either chronic renal failure or long term vitamin D deficiency.The majority of patients with tertiary hyperparathyroidism have a history of renal transplantation.
Physical Examination
Physical examination of patients with hyperparathyroidism is usually unremarkable. Patients may have physical findings due to severe hypercalcemia and other complications of hyperparathyroidism.
Laboratory Findings
An elevated serum calcium on routine biochemical screening in a asymptomatic patient should raise the suspicion of primary hyperparathyroidism. An elevated concentration of serum calcium with elevated parathyroid hormone level is diagnostic of primary hyperparathyoidism. Most consistent laboratory findings associated with the diagnosis of secondary hyperparathyroidism include elevated serum parathyroid hormone level and low to normal serum calcium. An elevated concentration of serum calcium with elevated parathyroid hormone level in post renal transplant patients is diagnostic of tertiary hyperparathyoidism. Measurement of total serum calcium with automatic techniques has similar or even more reliability than serum ionized calcium measurement. Method of choice for measuring intact parathyroid hormone include Immunoradiometric assay (IMRA) or Immunochemiluminescent assay (ICMA). 24-Hour urinary calcium excretion is used to seperate the patients with familial hypocalciuric hypercalcemia and typical primary hyperparathyroidism. Serum 1,25-dihydroxy vitamin D (calcitriol) concentration are significantly lower in familial hypocalciuric hypercalcemia than primary hyperparathyroidism.
Electrocardiogram
There are no ECG findings associated with hyperparathyroidism. However, an ECG may be helpful in the diagnosis of cardiac complications of hyperparathyroidism.
X-ray
X-ray is helpful in diagnosis of hyperparathyroidism. Finding in primary hyperparathyroidism includes subperiosteal bone resorption, endoosteal bone resorption, subchondral resorption, subligamentous resorption, intracortical resorption, osteopenia, brown tumors, salt and pepper sign in the skull (pepper pot skull), and chondrocalcinosis. X-ray is the preferred imaging for diagnosis of secondary hyperparathyroidism as majority of findings are radiological. Findings in secondary and tertiary hyperparathyroidism are often associated with the osteosclerosis of renal osteodystrophy, and the osteomalacia of vitamin D deficiency and includes subperiosteal bone resorption, subchondral resorption, subligamentous resorption, severe osteopenia, osteosclerosis, brown tumor, amyloid deposition, soft tissue and vascular calcification, superior and inferior rib notching, and osteonecrosis.
CT scan
Good quality preoperative evaluation favors post operative results. 4-dimentional CT scan is an investigation for preoperative localizing of hyper-functioning parathyroid gland. 4D-CT is significantly more sensitive than Tc-99m sestamibi scintigraphy and ultrasound for precise (quadrant) localization of hyper-functioning parathyroid glands. 4D-CT is required to be performed with three phases including non-contrast, arterial, and delayed phase imaging. 4D-CT provides extremely detailed images of neck in multiple planes and enables the visualization of difference in hyper-functioning parathyroid gland compared with normal parathyroid glands and other structures in the neck on the basis on perfusion characteristics ( rapid uptake and washout). 4D-CT is particularly useful in cases of re-operation. The major disadvantage of 4D-CT is significant radiation exposure associated with scanning the patient multiple times.
MRI
MRI may be helpful in the post-operative evaluation of hyper functioning parathyroid glands, particularly in patients with recurrent or persistent hyperparathyroidism. MRI has similar sensitivity and positive predictive value as Tc-99m sestamibi scintigraphy for post-operative detection of hyper-functioning parathyroid glands. MRI with gadolinium and fat suppression is used for detection of ectopic parathyroid adenoma (particularly those located in mediastinum).
Ultrasound
Neck ultrasound is used for preoperative localization of hyper-functioning parathyroid gland. Neck ultrasound alone is not a sensitive investigation for this purpose. Neck ultrasound along with Tc-99m sestamibi scintigraphy is most common used diagnostic modality for preoperative localization of hyper-functioning parathyroid gland.
Other Imaging Findings
Imaging modalities may be helpful in preoperative localization of hyper-functioning parathyroid glands. This includes both non-invasive and invasive modalities. Non-invasive imaging modalities for preoperative localization of hyper-functioning parathyroid glands include Tc-99m sestamibi scintigraphy (sestamibi or MIBI), single photon emission computed tomography (SPECT), positron emission tomography (PET). Invasive modalities used for preoperative localization of hyper-functioning parathyroid glands include selective arteriography and angiography. Dual energy X-ray absorptiometry is helpful in detecting low bone mineral density (BMD) caused by hyperparathyroidism.
Other Diagnostic Studies
Other diagnostic study useful for preoperative localization of hyper-functioning parathyroid glands include super selective venous sampling. Another diagnostic study include measurement of intraoperative parathyroid hormone (IOPTH) by using a modified sensitive assay (immunoradiometric assay). IOPTH is beneficial for predicting long term surgical outcomes.
Treatment
Medical Therapy
Surgical therapy is preferred over medical therapy in hyperparathyroidism. However medical therapy is considered in a few circumstances. Patients with primary hyperparathyroidism who do not undergo parathyroidectomy should be monitored for the potential progression of disease. Monitoring includes serum calcium, skeletal monitoring, and renal monitoring. Medical management of primary hyperparathyroidism includes nutritional supplements and pharmacotherapy. Nutritional supplements includes elemental calcium supplements and vitamin D analogs. Pharmacotherapy includes bisphosphonates, calcimimetics, and estrogen receptor-targeted therapy. Medical management of secondary hyperparathyroidism includes calcimimetics, vitamin D analogues, and phosphate binders/phosphate restriction. Medical management of tertiary hyperparathyroidism includes calcimimetics.
Surgery
Surgery is the mainstay of treatment for hyperparathyroidism. Symptomatic hyperparathyroidism is an indication for surgery. However, there are guidelines for surgery in asymptomatic primary hyperparathyroidism. Surgery for hyperparathyroidism is parathyroidectomy which includes bilateral neck exploration and minimally invasive parathyroidectomy. Most commonly done surgery for hyperparathyroidism is minimally invasive parathyroidectomy (MIP). There are various types of MIP. MIP provides excellent postoperative cure rates comparable to bilateral neck exploration (BNE) with less complications than BNE. This is due to precise preoperative localization of hyper-functioning parathyroid gland and use of intraoperative parathyroid hormone (IOPTH) monitoring for predicting post-surgical success (postoperative normocalcemia).
Primary Prevention
Effective measures for the primary prevention of secondary hyperparathyroidism in chronic kidney disease include aggressive management of hyperphosphatemia in early stages of chronic kidney disease and prevention and treatment of vitamin D deficiency in stage 3 & 4 chronic kidney disease. There are no established measures for the primary prevention of primary hyperparathyroidism and tertiary hyperparathyroidism.
Secondary Prevention
Secondary prevention of primary hyperparathyroidism includes monitoring for potential progression of disease in patients who do not undergo parathyroidectomy. There are guidelines for monitoring of patients with asymptomatic hyperparathyroidism not undergoing parathyroidectomy. Effective measures for secondary prevention of secondary hyperparathyroidism include maintain adequate nutrition, proper intake of vitamin D and/or sufficient sunlight exposure, and adequate physical activity. Effective measures for secondary prevention of tertiary hyperparathyroidism include early detection and treatment of hyperparathyroidism by either calcimimetics or parathyroidectomy.
References
Historical Perspective
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Anmol Pitliya, M.B.B.S. M.D.[2]
Overview
In 1880, Ivar Sandström, a Swedish anatomist, described parathyroids in human following 50 autopsies. In 1924, James Bertram Collip, a Canadian biochemist, discovered and extracted parathormone and treated tetany with the help of parathyroid extract along with Douglous B Leitch. In 1925, Felix Mandl, a viennese surgeon performed first parathyroidectomy to treat a patient suffering from suffering from osteitis fibrosa cystica. In 1959, Howard Rasmussen and Lyman C. Craig at the Rockefeller Institute for Medical Research purified parathyroid hormone. They also isolated the active polypeptide (parathormone B) from bovine parathyroid gland and gave its tentative formula in 1961.
Historical Perspective
Discovery
- The oldest known case of hyperparathyroidism was found in a cadaver from a Early Neolithic cemetery in southwest Germany.[1]
- In 1852, Sir Richard Owen, Hunterian Professor and Conservator of the Museum in the Royal College of Surgeons of England, described parathyroids in rhinoceros.[2]
- In 1880, Ivar Sandström, a Swedish anatomist, described parathyroids in human following 50 autopsies. He found two parathyroid glands bilaterally in 43 out of 50 autopsies.[3]
- In 1891, Friedrich van Rechlinghausen, a German pathologist described ‘osteitis fibrosa cystica‘ (the parathyroid cystic bone disease).[3]
- In 1909, William George MacCallum and Carl Voegtlin, demonstrated association between parathyroid gland, calcium, and tetany.[4]
- In 1924, James Bertram Collip, a Canadian biochemist, discovered and extracted parathormone.[5]
- In 1932, L. I. Pugsley and Hans Selye, described the histological changes in the bone due to parathyroid hormone action and calcium metabolism in rat experiments. [6]
- In 1948, Nigel Ashworth Barnicot, an English anthropologist described the association between parathyroid hormone and bone resorption.[7]
- In the same year, Iftakhar Jahan and Robert F. Pitts described effect of parathyroid hormone in decreasing calcium and magnesium excretion.[8]
- In 1959, Howard Rasmussen and Lyman C. Craig at the Rockefeller Institute for Medical Research purified parathyroid hormone.[9] They also isolated the active polypeptide (parathormone B) from bovine parathyroid gland and gave its tentative formula in 1961.[10]
Landmark Events in the Development of Treatment Strategies
- In 1925, James Bertram Collip along with Douglous B Leitch, was the first who treated tetany with the help of parathyroid extract. They names the extract as parathyrin.[11]
- In 1925, Felix Mandl, a viennese surgeon, was the first who performed parathyroidectomy to treat a patient suffering from osteitis fibrosa cystica.[12]
Famous Cases
- Garry Shandling, a famous comedian suffered from hyperparathyroidism.[13]
References
- ↑ Zink AR, Panzer S, Fesq-Martin M, Burger-Heinrich E, Wahl J, Nerlich AG (2005). “Evidence for a 7000-year-old case of primary hyperparathyroidism”. JAMA. 293 (1): 40–2. doi:10.1001/jama.293.1.40-c. PMID 15632333.
- ↑ Modarai B, Sawyer A, Ellis H (2004). “The glands of Owen”. J R Soc Med. 97 (10): 494–5. doi:10.1258/jrsm.97.10.494. PMC 1079622. PMID 15459265.
- ↑ 3.0 3.1 Johansson H (2015). “The Uppsala anatomist Ivar Sandström and the parathyroid gland”. Ups. J. Med. Sci. 120 (2): 72–7. doi:10.3109/03009734.2015.1027426. PMC 4463479. PMID 25913489.
- ↑ Maccallum WG, Voegtlin C (1909). “ON THE RELATION OF TETANY TO THE PARATHYROID GLANDS AND TO CALCIUM METABOLISM”. J. Exp. Med. 11 (1): 118–51. PMC 2124703. PMID 19867238.
- ↑ Collip, J. B. (1925). “THE EXTRACTION OF A PARATHYROID HORMONE WHICH WILL PREVENT OR CONTROL PARATHYROID TETANY AND WHICH REGULATES THE LEVEL OF BLOOD CALCIUM”. Journal of Biological Chemistry. 63 (2): 395–438.
- ↑ PUGSLEY, L. I.; SELYE, HANS (July 28, 1933). “THE HISTOLOGICAL CHANGES IN THE BONE RESPONSIBLE FOR THE ACTION OF PARATHYROID HORMONE ON THE CALCIUM METABOLISM OF THE RAT”. The Journal of Physiology. 79 (1): 113–117.
- ↑ BARNICOT NA (1948). “The local action of the parathyroid and other tissues on bone in intracerebral grafts”. J. Anat. 82 (Pt. 4): 233–48. PMID 18113751.
- ↑ JAHAN I, PITTS RF (1948). “Effect of parathyroid on renal tubular reabsorption of phosphate and calcium”. Am. J. Physiol. 155 (1): 42–9. PMID 18102666.
- ↑ Rasmussen, Howard; Craig, Lyman C. (1959). “PURIFICATION OF PARATHYROID HORMONE BY USE OF COUNTERCURRENT DISTRIBUTION”. Journal of the American Chemical Society. 81 (18): 5003–5003. doi:10.1021/ja01527a066. ISSN 0002-7863.
- ↑ Rasmussen, Howard; Craig, Lyman C. (1961). “Isolation of a Parathyroid Polypeptide from Acetic Acid Extracts of Bovine Parathyroid Glands”. {Journal of Biological Chemistry. 236 (4): 1083–1086.
- ↑ Collip JB, Leitch DB (1925). “A Case of Tetany treated with Parathyrin”. Can Med Assoc J. 15 (1): 59–60. PMC 1707993. PMID 20315252.
- ↑ Thompson, Scott M.; Thompson, Geoffrey B. (April 8, 2015). Felix Mandl. Surgical Endocrinopathies. p. 153-156. ISBN 978-3-319-13661-5.
- ↑ “Garry Shandling and the Disease You Didn’t Know About – The Atlantic”.
Classification
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Anmol Pitliya, M.B.B.S. M.D.[2]
Overview
Hyperparathyroidism can be classified according to origin of defect into primary, secondary and tertiary.
Classification
Hyperparathyroidism can be classified according to origin of defect into primary, secondary and tertiary.
Primary hyperparathyroidism
- Primary hyperparathyroidism is due to over activity of the parathyroid glands themselves. The most important causes of oversecretion of parathyroid hormone include:
- Adenoma
- Hyperplasia
- Carcinoma of the parathyroid glands
Secondary hyperparathyroidism
Secondary hyperparathyroidism is due to increase in secretion of parathyroid hormone from a secondary process.
Tertiary hyperparathyroidism
Tertiary hyperparathyroidism is a state of excessive secretion of parathyroid hormone (PTH) after a long period of secondary hyperparathyroidism and resulting in hypercalcemia even after treatment of secondary hyperparathyroidism.
| Hyperparathyroidism | |||||||||||||||||||||||||||||||||||||
| Primary hyperparathyroidism | Secondary hyperparathyroidism | Tertiary hyperparathyroidosm | |||||||||||||||||||||||||||||||||||
| •Parathyroid adenoma •Parathyroid hyperplasia •Parathyroid carcinoma | •Chronic renal failure •Vitamin D deficiency | •Post-renal transplantation | |||||||||||||||||||||||||||||||||||
References
Pathophysiology
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1];Associate Editor(s)-in-Chief: Anmol Pitliya, M.B.B.S. M.D.[2]
Overview
Hyperparathyroidism is an increase in serum parathyroid hormone. Normally, parathyroid hormone increases serum calcium and magnesium concentration, and decreases serum phosphate concentration. Secretion of parathyroid hormone from parathyroid gland is stimulated by low serum calcium. Parathyroid glands have calcium-sensing receptors responsible for sensing extracellular ionized calcium. Calcium and magnesium provides a negative feedback for secretion of parathyroid hormone. Primary hyperparathyroidism is due to increase in secretion of parathyroid hormone from a primary process in parathyroid gland. Majority of times, increase in secretion of parathyroid hormone is the result of parathyroid adenoma (85%). Calcium-sensing receptor expression in reduced in parathyroid adenoma resulting in an increase in calcium sensing set point. In minority of cases, development of primary hyperparathyroidism is the result of multiple genetic mutations. Genes involved in the pathogenesis of primary hyperparathyroidism include calcium-sensing receptor gene, HRPT2 gene (CDC73 gene), Cyclin D1 gene (CCND1)/PRAD1 gene, MEN1 gene, and RET gene. Secondary hyperparathyroidism is due to increase in secretion of parathyroid hormone from a secondary process, most commonly due chronic renal failure. Fibroblast growth factor 23 (FGF-23) concentration increases in chronic renal failure which plays a central role in regulation of phosphate vitamin D homeostasis and pathogenesis of secondary hyperparathyroidism. Majority of times, tertiary hyperparathyroidism occurs in patients after renal transplantation.Patients with secondary hyperparathyroidism continues to have elevated parathyroid hormone even after renal transplantation. Classically, there is hyperplasia of all four of parathyroid gland. On gross pathology, parathyroid adenoma is a soft, tan nodule which is well-circumscribed by a delicate capsule. Typically, cut surface of parathyroid adenoma is smooth, soft, and reddish brown in color. It should be differentiated from normal parathyroid gland tissue which is yellow-brown color. Parathyroid hyperplasia usually involves multiple glands. Bones and kidney are also commonly involved in hyperparathyroidism. Hypercalcemia due to hyperparathyroidism may cause metastatic calcification in many organs including lungs, heart, blood vessels, stomach. Chief cells are predominant in parathyroid adenoma on microcopy. Adenoma is seperated from a rim of non-neoplastic tissue on the edge by a fibrous capsule. Endocrine atypia (cells with bizarre and pleomorphic nuclei) is often seen in parathyroid adenoma. It should not be mistaken as a sign of malignancy. Majority of times, hyperplasia of chief cells is observed in parathyroid hyperplasia. It may be diffuse or multinodular. Cytologic details are unreliable for diagnosis of parathyroid carcinoma.
Pathophysiology
Parathyroid, Vitamin D, and Mineral Homeostasis
The effect of parathyroid hormone on mineral metabolism is as follows:[1][2]
- Effect of parathyroid hormone on inorganic phosphate metabolism:
- Increases excretion of inorganic phosphate from kidney resulting in decreased serum concentration of phosphate.
- Effect on parathyroid hormone on calcium metabolism:
- Direct effect:
- Increased resorption of bones.
- Decreases excretion from kidney.
- Indirect effect:
- Increases conversion of inactive 25-hydroxy vitamin D to the active 1,25-dihydroxy vitamin D which increases absorption of calcium from gut. Decreased phosphate concentration also increases this conversion process. Vitamin D shows synergism with parathyroid hormone action on bone.
- Decreased serum inorganic phosphate concentration prevents precipitation of calcium phosphate in bones.
- Both these direct and indirect mechanism results in an increased serum calcium concentration.
- Direct effect:
- Effect of parathyroid hormone on magnesium concentration:
Effect of minerals and vitamin D on parathyroid hormone:
- Decrease in serum calcium concentration stimulates parathyroid hormone.
- Calcium provides negative feedback on parathyroid hormone.
- Magnesium provides negative feedback on parathyroid hormone.
- Vitamin D decreases the concentration of parathyroid hormone.
| Parathyroid hormone | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Kidney | Bone | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Decreased excretion of magnesium | Increasead conversion of inactive 25-hydroxy vitamin D to the active 1,25-dihydroxy vitamin D | Increase excretion of inorganic phosphate | Decrease excretion of calcium | Increased resorption of bone | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Increased serum concentration of magnesium | Increased absorption of calcium from gut | Decreased serum concentration of inorganic phosphate | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Prevents precipitation of calcium phosphate in bones | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Increased serum concentration of calcium | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Calcium-sensing receptors
- Calcium-sensing receptors are present on parathyroid glands. They are a type of 7-transmembrane receptors in G-protein coupled receptors superfamily of receptors.[3]
- Calcium-sensing receptors sense change in extracellular concentration of ionized calcium.[4]
- Calcium-sensing receptor expression in reduced in primary hyperparathyroidism (parathyroid adenoma) and secondary hyperparathyroidism.[5]
- This reduced expression of receptor causes an increases in calcium sensing set point.[6]
- This in turn leads to increase in secretion of parathyroid hormone in presence on normal serum concentration of extracellular ionized calcium.
Pathogenesis of primary hyperparathyroidism
- Primary hyperparathyroidism is due to increase in secretion of parathyroid hormone from a primary process in parathyroid gland.
- Majority of times, increase in secretion of parathyroid hormone is the result of parathyroid adenoma (85%). Other causes of increase in secretion of parathyroid hormone includes parathyroid hyperplasia (15%) and parathyroid carcinoma (5%).[7]
- Calcium-sensing receptor expression in reduced in parathyroid adenoma resulting in an increase in calcium sensing set point.[5][6]
- In parathyroid hyperplasia, an increase in cell number causes increased secretion of parathyroid hormone.
Pathogenesis of secondary hyperparathyroidism
- Secondary hyperparathyroidism is due to increase in secretion of parathyroid hormone from a secondary process, most commonly due chronic renal failure. Other causes include vitamin D deficiency, severe calcium deficiency.[8]
- Chronic renal failure leads to high serum inorganic phosphate and low serum calcium and deficiency of active form of vitamin D (1,25-dihydroxy vitamin D/calcitriol)
- This leads to continuous stimulation of parathyroid glands resulting down-regulation of parathyroid vitamin D receptors and calcium-sensing receptors.
- Fibroblast growth factor 23 (FGF-23) concentration increases in chronic renal failure which plays a central role in regulation of phosphate vitamin D homeostasis.
- Elevated FGF-23 expression down-regulates remaining 25(OH)-1-hydroxylase enzyme. 25(OH)-1-hydroxylase enzyme is responsible for conversion of inactive 25-hydroxy vitamin D into active 1,25-dihydroxy vitamin D (calcitriol). This aggravates the deficiency of active vitamin D.
- These all factors leads to hyperplasia of parathyroid gland.
| Chronic renal failure | |||||||||||||||||||||||||||||||||||||||
| Elevated serum inorganic phosphate concentration | |||||||||||||||||||||||||||||||||||||||
| Elevated FGF-23 | |||||||||||||||||||||||||||||||||||||||
| Decreased calcitriol | |||||||||||||||||||||||||||||||||||||||
| Decreaed serum calcium concentration | |||||||||||||||||||||||||||||||||||||||
| Continuous stimulation of parathyroid gland | |||||||||||||||||||||||||||||||||||||||
| Downregulation of parathyroid vitamin D receptors and calcium-sensing receptors | |||||||||||||||||||||||||||||||||||||||
| Parathyroid hyperplasia | |||||||||||||||||||||||||||||||||||||||
| Increased secretion of parathyroid hormone | |||||||||||||||||||||||||||||||||||||||
Mechanism of fibroblast growth factor 23 (FGF-23)
The mechanism of fibroblast growth factor 23 (FGF-23) in chronic renal disease and development of secondary hyperparathyroidism is as follows:[8]
- FGF-23 is a hormone produced in the osteocytes and osteoblasts.
- Its production is increased due to high serum phosphate and high calcitriol.
- FGF-23 binds and activates a receptor called fibroblast growth factor receptor 1 (FGFR1).
- FGFR1 is functional when co-expressed with the Klotho transmembrane protein, as a Klotho-FGF receptor complex.
- FGF-23 reduces the expression of type II sodium phosphate co-transporters (NaPi-2a and NaPi-2c) decreasing phosphate reabsorption in proximal tubules.
- In chronic renal failure, as a result, phosphate absorption is increased in proximal tubules due to effect of FGF-23 as well as increased parathyroid hormone. This is responsible for normal serum phosphate levels in majority of patients until the glomerular filtration rate (GFR) falls below 20 ml/min.
- As chronic renal failure progresses, these negative feedback loops are impaired leading to deranged phosphate homeostasis.
- FGF-23 have direct and indirect effect on parathyroid hormone.
- Direct effect: In normal parathyroid gland, FGF-23 decreases synthesis of parathyroid hormone through the mitogen-activated protein kinase (MAPK) pathway.[9] FGF-23 increases expression of the parathyroid calcium-sensing receptor and the vitamin D receptor, and reduces cellular proliferation.[10]
- Indirect effect: Increased synthesis of parathyroid hormone by decreasing synthesis of calcitriol.
- FGF-23 fails to activate mitogen-activated protein kinase pathway in hyperplastic parathyroid gland secondary to chronic renal failure.[10]
Pathogenesis of tertiary hyperparathyroidism
- Majority of times, tertiary hyperparathyroidism occurs in patients after renal transplantation.[11]
- Patients with secondary hyperparathyroidism continues to have elevated parathyroid hormone even after renal transplantation.
- Patients with secondary hyperparathyroidism and long term hypocalcemia tends to have hyperplasia of chief cells of parathyroid gland and increased secretion of parathyroid hormone.
- The primary disorder in secondary hyperparathyroidism is chronic renal failure in majority of patients. After correction of chronic renal failure by renal transplant, the hyperplastic parathyroid gland fails to resolve and continues to secrete excess amount of parathyroid hormone.
- Clasically, there is hyperplasia of all four of parathyroid gland.
Genetics
The development of primary hyperparathyroidism is the result of multiple genetic mutations in minority of cases. Genes involved in the pathogenesis of primary hyperparathyroidism include calcium-sensing receptor gene, HRPT2 gene (CDC73 gene), Cyclin D1 gene (CCND1)/PRAD1 gene, MEN1 gene, and RET gene.
- Calcium-sensing receptor gene mutation:[12]
- Calcium-sensing receptor (CSR) gene is present on chromosome 3q.
- Few individuals carries an inherited mutation in the extracellular calcium-sensing receptor gene.
- The first identified mutation in CSR gene is a point mutation in which phenylalanine is replaced with leucine at codon 881 of CSR gene.[13]
- This mutation reduces the activity of calcium-sensing receptor.
- This mutation can be heterozygous or homozygous.
- Individuals carrying heterozygous mutation have familial hypocalciuric hypercalcemia (FHH) or familial benign hypercalcemia. FHH is characterized by parathyroid dependent hypercalcemia and decreased responsiveness of parathyroid and kidney to hypercalcemia.
- Individuals carrying homozygous mutation have neonatal severe hyperparathyroidism. Neonatal severe hyperparathyroidism is characterized by marked parathyroid hyperplasia.
- Familial hypocalciuric hypercalcemia (FHH) and neonatal severe hyperparathyroidism are transmitted in autosomal dominant pattern.
- HRPT2 gene(CDC73 gene) mutations:[14]
- HRPT2 gene code for parafibromin protein.
- HRPT2 gene mutations are found in a type of familial hyperparathyroidism, hyperparathyroidism-jaw tumor (HPT-JT) syndrome.
- HRTP2 gene mutations increases risk of parathyroid carcinoma.
- Cyclin D1 gene (CCND1)/PRAD1 gene:[15][16]
- PRAD1 (parathyroid adenoma 1) is a protooncogene located on chromosome 11q13.
- Cyclin D1 gene translocation and oncogene action observed in 8% of adenomas.
- Cyclin D1 gene overexpression is observed in 20% to 40% of parathyroid adenomas.
- MEN1 gene:[15][17]
- MEN 1 ics a tumor supressor gene on chromosome 11q13.
- Somatic loss of single MEN1 allele is observed in 25% to 40% of sporadic parathyroid adenomas.
- RET gene:[18]
- RET gene is a proto-oncogene.
- RET proto-oncogene is associated with multiple endocrine neoplasia type 2 (MEN 2).
- MEN2A caries increased risk of parathyroid adenoma and/or parathyroid hyperplasia.
- CDNK1B gene:[19]
- CDNK1B mutation causes Multiple endocrine neoplasia type 4 (MEN 4).
- Parathyroid tumors are found along with anterior pituitary, gonadal, adrenal, and renal tumors in MEN 4 syndrome.
- CDNK1B encodes for the cyclin-dependent kinase inhibitor p27kip1.
Associated Conditions
The conditions associated with hyperparathyroidism include:[20][21][22][12][14][17][23][24][25][26][27][28]
- Brown tumor
- Chronic renal failure
- Depression
- Familial hypocalciuric hypercalcemia
- Hyperparathyroid-jaw tumor syndrome
- Hypertension
- Multiple endocrine neoplasia type 1
- Multiple endocrine neoplasia type 2A
- Multiple endocrine neoplasia type 4
- Neonatal severe hyperparathyroidism
- Osteitis fibrosa cystica
- Osteoporosis
- Osteomalacia
- Osteoarthritis
- Pancreatitis
Gross Pathology
Parathyroid glands
Parathyroid adenoma
- On gross pathology, parathyroid adenoma is a soft, tan nodule which is well-circumscribed by a delicate capsule.[29]
- Most commonly, parathyroid adenoma is present in single gland. Some times multiple glands are involved.
- If single gland is involved, the other glands may shrink due to negative feedback.
- Majority of times, parathyroid adenoma weight ranges between 0.5 gram to 5 gram.
- Typically, cut surface of parathyroid adenoma is smooth, soft, and reddish brown in color. It should be differentiated from normal parathyroid gland tissue which is yellow-brown color.[30]
- The tissue of parathyroid gland that is not involved in parathyroid adenoma is typically atrophied and compressed. Fat component of normal parathyroid tissue is also observed.
- On rare occasion, parathyroid adenoma may be cystic.
 |
 |
 |
Parathyroid hyperplasia
- Parathyroid hyperplasia usually involves multiple glands.[29]
- The combine weight of all hyperplastic gland is usually less than 1 gram.
Parathyroid carcinoma
- On gross pathology, parathyroid carcinoma may range from a well circumscribed lesion to invasive neoplasm.[29]
- Sometimes, it may be difficult to differentiate from parathyroid adenoma.
- One parathyroid gland enlarges in parathyroid carcinoma, consisting gery-white and irregular mass.
- Sometimes, mass of single parathyroid carcinoma becomes more than 10 gram in weight.
Other organs
Bones
- There is erosion of bone martix and bone resorption due to increase in osteoclastic activity.[29][31]
- Most common site is metaphysis of long tubular bones.
- There is increased osteoblastic activity along with bone resorption leading to formation of new bone trabeculae.
- As severity increases, there is gross thinning of cortex and increase in amount of fibrous tissue in marrow along with multiple foci of hemorrhage and cysts. The condition is called osteitis fibrosa cystica.
- Sometimes there is development of masses due to aggregation of osteoclasts, reactive giant cells and hemorrhagic debris. This may be confused with neoplasm. This is called brown tumor of hyperparathyroidism.
Kidneys
| |
 |
 |
Other organs
- Hypercalcemia due to hyperparathyroidism may cause metastatic calcification in many organs including lungs, heart, blood vessels, stomach.[29][33]
Microscopic Pathology
Parathyroid adenoma
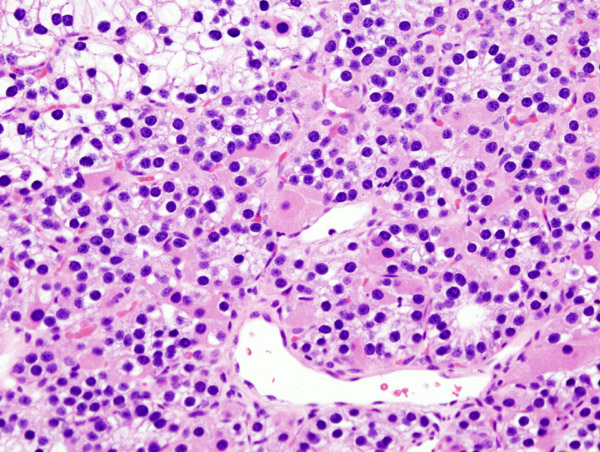
- Chief cells are predominant in parathyroid adenoma on microcopy.
- In majority of cases, a few nests of larger oxyphil cells are also present.
- Adenoma is seperated from a rim of non-neoplastic tissue on the edge by a fibrous capsule.
- Chief cells present in adenoma larger than normal chief cells and shows greater variability on nuclear size.
- Endocrine atypia (cells with bizarre and pleomorphic nuclei) is often seen in parathyroid adenoma. It should not be mistaken as a sign of malignancy.
- Mitotic figures are rarely present.
- Parathyroid adenoma has incospicuous adipose tissue when compared with normal parathyroid gland.
-
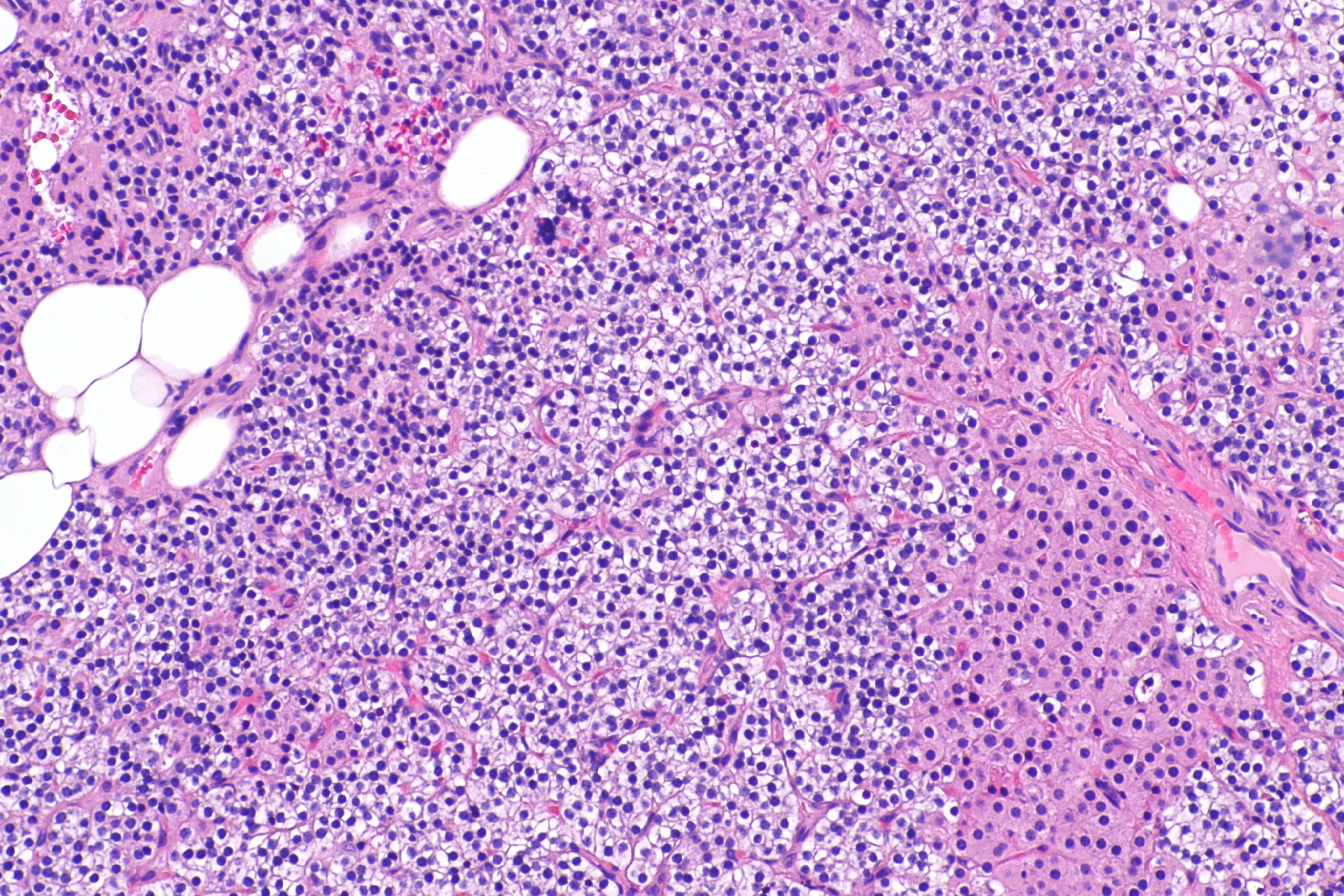
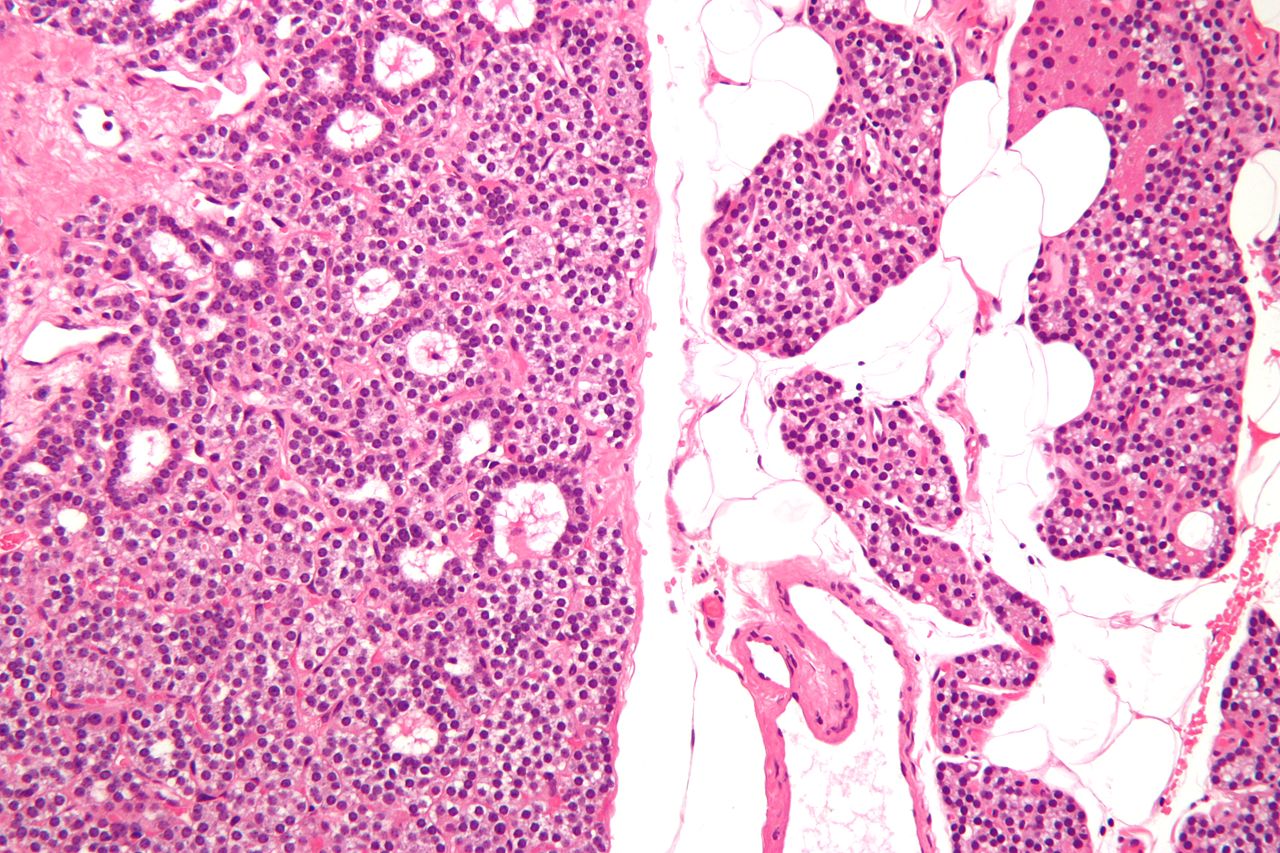 Intermediate/Low magnification micrograph of parathyroid adenoma. H&E stain. Features: Single cell population forming a single mass. Thin capsule. No adipose tissue. +/-Glandular architecture (which may lead to confusion with thyroid tissue). Normal parathyroid gland with prominent adipose tissue is seen on the right of the image. – Source: Wikipedia
Intermediate/Low magnification micrograph of parathyroid adenoma. H&E stain. Features: Single cell population forming a single mass. Thin capsule. No adipose tissue. +/-Glandular architecture (which may lead to confusion with thyroid tissue). Normal parathyroid gland with prominent adipose tissue is seen on the right of the image. – Source: Wikipedia -
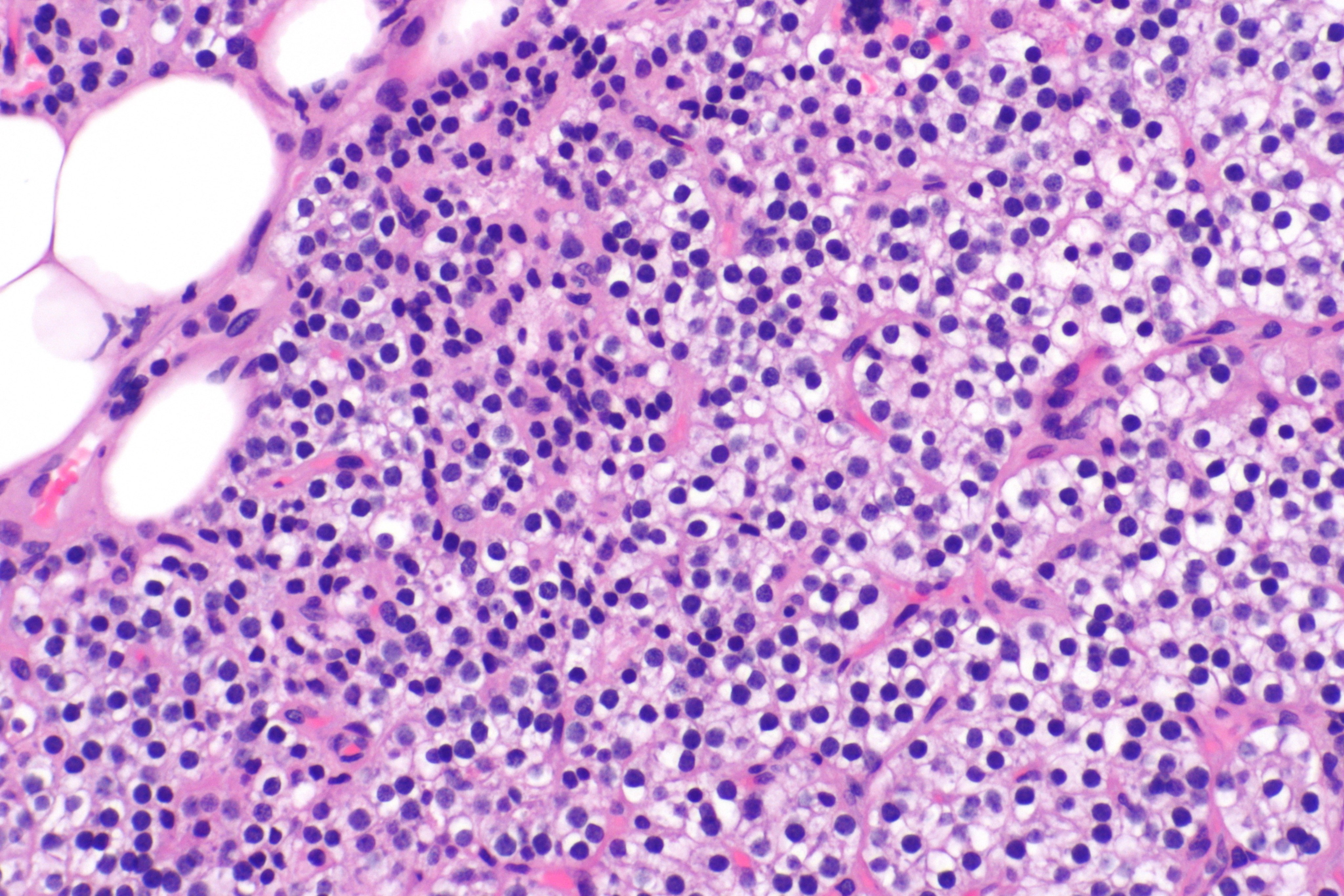
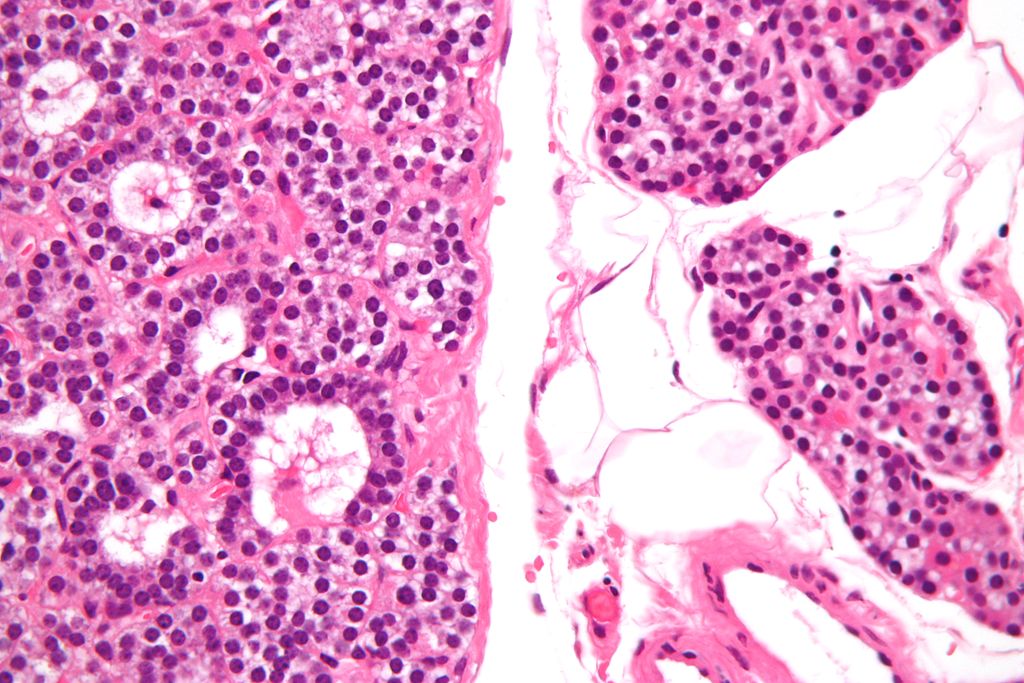 High magnification micrograph of a parathyroid adenoma. H&E stain. Features: Single cell population forming a single mass. Thin capsule. No adipose tissue. +/-Glandular architecture (which may lead to confusion with thyroid tissue). Normal parathyroid gland with prominent adipose tissue is seen on the right of the image. – Source:wikipeida
High magnification micrograph of a parathyroid adenoma. H&E stain. Features: Single cell population forming a single mass. Thin capsule. No adipose tissue. +/-Glandular architecture (which may lead to confusion with thyroid tissue). Normal parathyroid gland with prominent adipose tissue is seen on the right of the image. – Source:wikipeida -
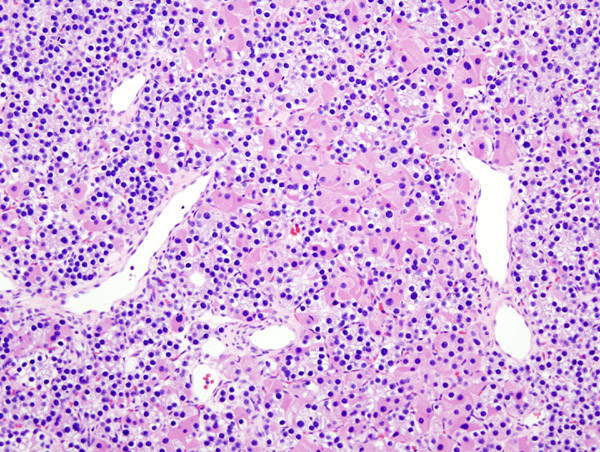 Histopatholgical image of parathyroid adenoma in a patient with primary hyperparathyroidism. Hematoxylin and eosin stain. – Source: Wikipedia
Histopatholgical image of parathyroid adenoma in a patient with primary hyperparathyroidism. Hematoxylin and eosin stain. – Source: Wikipedia -
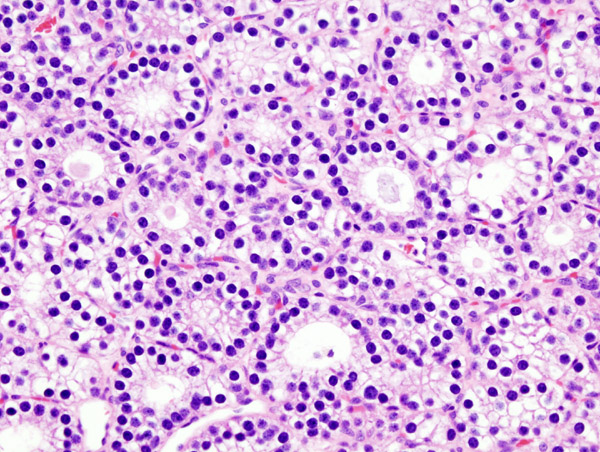 Histopatholgical image of parathyroid adenoma in a patient with primary hyperparathyroidism. Hematoxylin and eosin stain. – Source: Wikipedia
Histopatholgical image of parathyroid adenoma in a patient with primary hyperparathyroidism. Hematoxylin and eosin stain. – Source: Wikipedia -
 Histopatholgical image of parathyroid adenoma in a patient with primary hyperparathyroidism. – Source: Wikipedia
Histopatholgical image of parathyroid adenoma in a patient with primary hyperparathyroidism. – Source: Wikipedia





Parathyroid hyperplasia
- Majority of times, hyperplasia of chief cells is observed. It may be diffuse or multinodular.
- In minority of cases, there is accumulation of glycogen in cytoplasm resulting in abundant clear cytoplasm. This condition is called “water-clear cell hyperplasia”.
- Adipose tissue is in incospicuous in hyperplastic foci, same as adenoma.
-
 Micrograph showing a parathyroid hyperplasia (H&E stain) on intermediate magnification.Parathyroid adenoma is a clinicopathologic diagnosis. The histology is nonspecific. –Source: Wikimedia commons
Micrograph showing a parathyroid hyperplasia (H&E stain) on intermediate magnification.Parathyroid adenoma is a clinicopathologic diagnosis. The histology is nonspecific. –Source: Wikimedia commons -
 Micrograph showing a parathyroid hyperplasia (H&E stain) on high magnification.Parathyroid adenoma is a clinicopathologic diagnosis. The histology is nonspecific. – Source: Wikimedia commons
Micrograph showing a parathyroid hyperplasia (H&E stain) on high magnification.Parathyroid adenoma is a clinicopathologic diagnosis. The histology is nonspecific. – Source: Wikimedia commons -
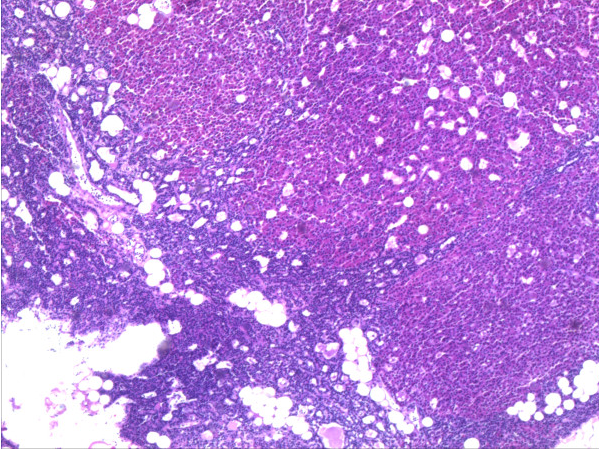 Hyperplasia of parathyroid gland HE-staining, 20× magnification. Source: Wikipedia. Biomedcentral For original file click here.Creative Commons lisence
Hyperplasia of parathyroid gland HE-staining, 20× magnification. Source: Wikipedia. Biomedcentral For original file click here.Creative Commons lisence



Parathyroid carcinoma
- Cytologic details are unreliable for diagnosis of parathyroid carcinoma.
- Definitive diagnostic criteria include invasion of surrounding tissue and metastasis.
- About one third of cases have local recurrence and another one third have distant metastasis.
References
- ↑ HARRISON MT (1964). “INTERRELATIONSHIPS OF VITAMIN D AND PARATHYROID HORMONE IN CALCIUM HOMEOSTASIS”. Postgrad Med J. 40: 497–505. PMC 2482768. PMID 14184232.
- ↑ Nussey, Stephen (2001). Endocrinology : an integrated approach. Oxford, UK Bethesda, Md: Bios NCBI. ISBN 1-85996-252-1.
- ↑ Brown EM, Gamba G, Riccardi D, Lombardi M, Butters R, Kifor O; et al. (1993). “Cloning and characterization of an extracellular Ca(2+)-sensing receptor from bovine parathyroid”. Nature. 366 (6455): 575–80. doi:10.1038/366575a0. PMID 8255296.
- ↑ Brown EM, Pollak M, Seidman CE, Seidman JG, Chou YH, Riccardi D; et al. (1995). “Calcium-ion-sensing cell-surface receptors”. N Engl J Med. 333 (4): 234–40. doi:10.1056/NEJM199507273330407. PMID 7791841.
- ↑ 5.0 5.1 Gogusev J, Duchambon P, Hory B, Giovannini M, Goureau Y, Sarfati E; et al. (1997). “Depressed expression of calcium receptor in parathyroid gland tissue of patients with hyperparathyroidism”. Kidney Int. 51 (1): 328–36. PMID 8995751.
- ↑ 6.0 6.1 Kifor O, Moore FD, Wang P, Goldstein M, Vassilev P, Kifor I; et al. (1996). “Reduced immunostaining for the extracellular Ca2+-sensing receptor in primary and uremic secondary hyperparathyroidism”. J Clin Endocrinol Metab. 81 (4): 1598–606. doi:10.1210/jcem.81.4.8636374. PMID 8636374.
- ↑ Wieneke JA, Smith A (2008). “Parathyroid adenoma”. Head Neck Pathol. 2 (4): 305–8. doi:10.1007/s12105-008-0088-8. PMC 2807581. PMID 20614300.
- ↑ 8.0 8.1 Cunningham J, Locatelli F, Rodriguez M (2011). “Secondary hyperparathyroidism: pathogenesis, disease progression, and therapeutic options”. Clin J Am Soc Nephrol. 6 (4): 913–21. doi:10.2215/CJN.06040710. PMID 21454719.
- ↑ Ben-Dov IZ, Galitzer H, Lavi-Moshayoff V, Goetz R, Kuro-o M, Mohammadi M, Sirkis R, Naveh-Many T, Silver J (2007). “The parathyroid is a target organ for FGF23 in rats”. J. Clin. Invest. 117 (12): 4003–8. doi:10.1172/JCI32409. PMC 2066196. PMID 17992255.
- ↑ 10.0 10.1 Canalejo R, Canalejo A, Martinez-Moreno JM, Rodriguez-Ortiz ME, Estepa JC, Mendoza FJ, Munoz-Castaneda JR, Shalhoub V, Almaden Y, Rodriguez M (2010). “FGF23 fails to inhibit uremic parathyroid glands”. J. Am. Soc. Nephrol. 21 (7): 1125–35. doi:10.1681/ASN.2009040427. PMC 3152229. PMID 20431039.
- ↑ Pitt SC, Sippel RS, Chen H (2009). “Secondary and tertiary hyperparathyroidism, state of the art surgical management”. Surg. Clin. North Am. 89 (5): 1227–39. doi:10.1016/j.suc.2009.06.011. PMC 2905047. PMID 19836494.
- ↑ 12.0 12.1 Hosokawa Y, Pollak MR, Brown EM, Arnold A (1995). “Mutational analysis of the extracellular Ca(2+)-sensing receptor gene in human parathyroid tumors”. J. Clin. Endocrinol. Metab. 80 (11): 3107–10. doi:10.1210/jcem.80.11.7593409. PMID 7593409.
- ↑ Carling T, Szabo E, Bai M, Ridefelt P, Westin G, Gustavsson P, Trivedi S, Hellman P, Brown EM, Dahl N, Rastad J (2000). “Familial hypercalcemia and hypercalciuria caused by a novel mutation in the cytoplasmic tail of the calcium receptor”. J. Clin. Endocrinol. Metab. 85 (5): 2042–7. doi:10.1210/jcem.85.5.6477. PMID 10843194.
- ↑ 14.0 14.1 Shattuck TM, Välimäki S, Obara T, Gaz RD, Clark OH, Shoback D; et al. (2003). “Somatic and germ-line mutations of the HRPT2 gene in sporadic parathyroid carcinoma”. N Engl J Med. 349 (18): 1722–9. doi:10.1056/NEJMoa031237. PMID 14585940.
- ↑ 15.0 15.1 Westin G, Björklund P, Akerström G (2009). “Molecular genetics of parathyroid disease”. World J Surg. 33 (11): 2224–33. doi:10.1007/s00268-009-0022-6. PMID 19373510.
- ↑ Hsi ED, Zukerberg LR, Yang WI, Arnold A (1996). “Cyclin D1/PRAD1 expression in parathyroid adenomas: an immunohistochemical study”. J Clin Endocrinol Metab. 81 (5): 1736–9. doi:10.1210/jcem.81.5.8626826. PMID 8626826.
- ↑ 17.0 17.1 Agarwal SK, Kester MB, Debelenko LV, Heppner C, Emmert-Buck MR, Skarulis MC; et al. (1997). “Germline mutations of the MEN1 gene in familial multiple endocrine neoplasia type 1 and related states”. Hum Mol Genet. 6 (7): 1169–75. PMID 9215689.
- ↑ Marquard, Jessica; Eng, Charis (September 27, 1999). “Multiple Endocrine Neoplasia Type 2”. GeneReviews® [Internet].
- ↑ Bilezikian JP (January 15, 2017). De Groot LJ, Chrousos G, Dungan K, et al., eds. Primary Hyperparathyroidism. Endotext [Internet]: South Dartmouth (MA): MDText.com, Inc.
- ↑ Bandeira F, Cusano NE, Silva BC, Cassibba S, Almeida CB, Machado VC, Bilezikian JP (2014). “Bone disease in primary hyperparathyroidism”. Arq Bras Endocrinol Metabol. 58 (5): 553–61. PMC 4315357. PMID 25166047.
- ↑ Rodriguez M, Nemeth E, Martin D (2005). “The calcium-sensing receptor: a key factor in the pathogenesis of secondary hyperparathyroidism”. Am J Physiol Renal Physiol. 288 (2): F253–64. doi:10.1152/ajprenal.00302.2004. PMID 15507543.
- ↑ Espiritu RP, Kearns AE, Vickers KS, Grant C, Ryu E, Wermers RA (2011). “Depression in primary hyperparathyroidism: prevalence and benefit of surgery”. J. Clin. Endocrinol. Metab. 96 (11): E1737–45. doi:10.1210/jc.2011-1486. PMID 21917870.
- ↑ Marquard, Jessica; Eng, Charis (September 27, 1999). “Multiple Endocrine Neoplasia Type 2”. GeneReviews® [Internet].
- ↑ Bilezikian JP (January 15, 2017). De Groot LJ, Chrousos G, Dungan K, et al., eds. Primary Hyperparathyroidism. Endotext [Internet]: South Dartmouth (MA): MDText.com, Inc.
- ↑ Mazzuoli GF, D’Erasmo E, Pisani D (1998). “Primary hyperparathyroidism and osteoporosis”. Aging (Milano). 10 (3): 225–31. PMID 9801732.
- ↑ Lips P (2001). “Vitamin D deficiency and secondary hyperparathyroidism in the elderly: consequences for bone loss and fractures and therapeutic implications”. Endocr Rev. 22 (4): 477–501. doi:10.1210/edrv.22.4.0437. PMID 11493580.
- ↑ Michael JW, Schlüter-Brust KU, Eysel P (2010). “The epidemiology, etiology, diagnosis, and treatment of osteoarthritis of the knee”. Dtsch Arztebl Int. 107 (9): 152–62. doi:10.3238/arztebl.2010.0152. PMC 2841860. PMID 20305774.
- ↑ Bai HX, Giefer M, Patel M, Orabi AI, Husain SZ (2012). “The association of primary hyperparathyroidism with pancreatitis”. J. Clin. Gastroenterol. 46 (8): 656–61. doi:10.1097/MCG.0b013e31825c446c. PMC 4428665. PMID 22874807.
- ↑ 29.0 29.1 29.2 29.3 29.4 Kumar, Vinay (2013). Robbins basic pathology. Philadelphia, PA: Elsevier/Saunders. p. 736-737. ISBN 9781437717815.
- ↑ Wieneke JA, Smith A (2008). “Parathyroid adenoma”. Head Neck Pathol. 2 (4): 305–8. doi:10.1007/s12105-008-0088-8. PMC 2807581. PMID 20614300.
- ↑ Goeddel DV, Yansura DG, Caruthers MH (1977). “Binding of synthetic lactose operator DNAs to lactose represessors”. Proc. Natl. Acad. Sci. U.S.A. 74 (8): 3292–6. PMC 431535. PMID 333432.
- ↑ Lila AR, Sarathi V, Jagtap V, Bandgar T, Menon PS, Shah NS (2012). “Renal manifestations of primary hyperparathyroidism”. Indian J Endocrinol Metab. 16 (2): 258–62. doi:10.4103/2230-8210.93745. PMC 3313745. PMID 22470864.
- ↑ Gui X, Miao L, Cai H, Xiao Y, Zhang D, Wang J, Meng F (2014). “[Primary hyperparathyroidism with metastatic pulmonary calcification: a case report and review of literature]”. Zhonghua Jie He He Hu Xi Za Zhi (in Chinese). 37 (5): 343–6. PMID 25011508.
Causes
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Anmol Pitliya, M.B.B.S. M.D.[2]
Overview
Hyperparathyroidism is caused by an increase in concentration of parathyroid hormone in serum. There are three type of hyperparathyroidism including primary, secondary and tertiary hyperparathyroidism. There are an array of different causes for all types of hyperparathyroidism. Most common cause of primary hyperparathyroidism is parathyroid adenoma (85%) followed by parathyroid hyperplasia (15%), and parathyroid carcinoma (5%). Most common cause of secondary hyperparathyroidism is chronic renal failure and vitamin D deficiency. Most common cause of tertiary hyperparathyroidism is post renal transplantation.
Hyperparathyroidism causes
Hyperparathyroidism causes can be divided based on the hyperthyroidism category.
Causes of Primary hyperparathyroidism
Causes of primary hyperparathyroidism are as follows:
Life Threatening causes
Life threatening causes include conditions which may result in death or permanent disability within 24 hours if left untreated. There are no life threatening causes of primary hyperparathyroidism.
Common causes
- Parathyroid adenoma[1]
- Usually single gland affected
- Sometimes multiple gland affected
Less common causes
- Parathyroid hyperplasia
- Parathyroid carcinoma
- Familial isloated hyperparathyroidism
- Radiation exposure (due to development of parathyroid adenoma or parathyroid hyperplasia)[2][3][4]
- Celiac disease[5][6]
Genetic causes
- Calcium-sensing receptor gene mutation[7]
- HRPT2 gene mutations (hyperparathyroidism-jaw tumor (HPT-JT) syndrome) [8]
- Cyclin D1 gene (CCND1)/PRAD1 gene translocation or overexression (parathyroid adenoma)[9][10]
- MEN1 gene (Multiple endocrine neoplasia type 1)[9][11]
- RET gene mutations (multiple endocrine neoplasia type 2A)[12]
Causes of secondary hyperparathyroidism
Causes of secondary hyperparathyroidism are as follows:
Common causes
- Chronic renal failure (leading to parathyroid hyperplasia)[13]
- Vitamin D deficiency[14]
Less common causes
- Severe calcium deficiency[15]
- Gastric bypass surgery, particularly roux-en-Y gastric bypass (RYGBP)[16]
- Malabsorption syndrome[17]
Causes of tertiary hyperparathyroidism
Causes of tertiary hyperparathyroidism are as follows:
Common causes
- Chronic renal failure (leading to parathyroid hyperplasia)
- Renal transplant patients[18]
Less common cause
- Long standing celiac disease[5]
- Long standing hypocalcemia[19]
Causes by Organ System
| Cardiovascular | No underlying causes |
| Chemical/Poisoning | No underlying causes |
| Dental | Hyperparathyroidism-jaw tumor syndrome |
| Dermatologic | No underlying causes |
| Drug Side Effect | No underlying causes |
| Ear Nose Throat | No underlying causes |
| Endocrine | Parathyroid adenoma, parathyroid hyperplasia, parathyroid carcinoma, neonatal severe primary hyperparathyroidism, familial isolated hyperparathyroidism, Familial hypocalciuric hypercalcemia |
| Environmental | No underlying causes |
| Gastroenterologic | Celiac disease, gastric bypass surgery, malabsorption syndrome |
| Genetic | Familial hypocalciuric hypercalcemia, neonatal severe primary hyperparathyroidism |
| Hematologic | No underlying causes |
| Iatrogenic | Gastric bypass surgery, radiation exposure |
| Infectious Disease | No underlying causes |
| Musculoskeletal/Orthopedic | No underlying causes |
| Neurologic | No underlying causes |
| Nutritional/Metabolic | Vitamin D deficiency, severe calcium deficiency |
| Obstetric/Gynecologic | No underlying causes |
| Oncologic | Hyperparathyroidism-jaw tumor syndrome, parathyroid adenoma,parathyroid carcinoma, multiple endocrine neoplasia type 1 (MEN 1), multiple endocrine neoplasia type 2A (MEN 2A), multiple endocrine neoplasia type 4 (MEN 4) |
| Ophthalmologic | No underlying causes |
| Overdose/Toxicity | No underlying causes |
| Psychiatric | No underlying causes |
| Pulmonary | No underlying causes |
| Renal/Electrolyte | Chronic renal failure, renal transplant, severe calcium deficiency |
| Rheumatology/Immunology/Allergy | Celiac disease |
| Sexual | No underlying causes |
| Trauma | No underlying causes |
| Urologic | No underlying causes |
| Miscellaneous | No underlying causes |
Causes in Alphabetical Order
- Celiac disease
- Chronic renal failure
- Chronic dialysis
- Familial hypocalciuric hypercalcemia
- Familial isolated hyperparathyroidism
- Gastric bypass surgery
- Hyperparathyroidism-jaw tumor syndrome
- Malabsorption syndrome
- Multiple endocrine neoplasia type 1(MEN 1)
- Neonatal severe primary hyperparathyroidism
- Parathyroid adenoma
- Parathyroid carcinoma
- Parathyroid hyperplasia
- Radiation exposure
- Renal transplant patients
- Severe calcium deficiency
- Vitamin D deficiency
References
- ↑ Wieneke JA, Smith A (2008). “Parathyroid adenoma”. Head Neck Pathol. 2 (4): 305–8. doi:10.1007/s12105-008-0088-8. PMC 2807581. PMID 20614300.
- ↑ Boehm BO, Rosinger S, Belyi D, Dietrich JW (2011). “The parathyroid as a target for radiation damage”. N Engl J Med. 365 (7): 676–8. doi:10.1056/NEJMc1104982. PMID 21848480.
- ↑ McMullen T, Bodie G, Gill A, Ihre-Lundgren C, Shun A, Bergin M; et al. (2009). “Hyperparathyroidism after irradiation for childhood malignancy”. Int J Radiat Oncol Biol Phys. 73 (4): 1164–8. doi:10.1016/j.ijrobp.2008.06.1487. PMID 18774659.
- ↑ Tisell LE, Hansson G, Lindberg S, Ragnhult I (1977). “Hyperparathyroidism in persons treated with X-rays for tuberculous cervical adenitis”. Cancer. 40 (2): 846–54. PMID 890665.
- ↑ 5.0 5.1 Maida MJ, Praveen E, Crimmins SR, Swift GL (2006). “Coeliac disease and primary hyperparathyroidism: an association?”. Postgrad Med J. 82 (974): 833–5. doi:10.1136/pgmj.2006.045500. PMC 2653933. PMID 17148709.
- ↑ Ludvigsson JF, Kämpe O, Lebwohl B, Green PH, Silverberg SJ, Ekbom A (2012). “Primary hyperparathyroidism and celiac disease: a population-based cohort study”. J. Clin. Endocrinol. Metab. 97 (3): 897–904. doi:10.1210/jc.2011-2639. PMC 3319223. PMID 22238405.
- ↑ Hosokawa Y, Pollak MR, Brown EM, Arnold A (1995). “Mutational analysis of the extracellular Ca(2+)-sensing receptor gene in human parathyroid tumors”. J. Clin. Endocrinol. Metab. 80 (11): 3107–10. doi:10.1210/jcem.80.11.7593409. PMID 7593409.
- ↑ Shattuck TM, Välimäki S, Obara T, Gaz RD, Clark OH, Shoback D; et al. (2003). “Somatic and germ-line mutations of the HRPT2 gene in sporadic parathyroid carcinoma”. N Engl J Med. 349 (18): 1722–9. doi:10.1056/NEJMoa031237. PMID 14585940.
- ↑ 9.0 9.1 Westin G, Björklund P, Akerström G (2009). “Molecular genetics of parathyroid disease”. World J Surg. 33 (11): 2224–33. doi:10.1007/s00268-009-0022-6. PMID 19373510.
- ↑ Hsi ED, Zukerberg LR, Yang WI, Arnold A (1996). “Cyclin D1/PRAD1 expression in parathyroid adenomas: an immunohistochemical study”. J Clin Endocrinol Metab. 81 (5): 1736–9. doi:10.1210/jcem.81.5.8626826. PMID 8626826.
- ↑ Agarwal SK, Kester MB, Debelenko LV, Heppner C, Emmert-Buck MR, Skarulis MC; et al. (1997). “Germline mutations of the MEN1 gene in familial multiple endocrine neoplasia type 1 and related states”. Hum Mol Genet. 6 (7): 1169–75. PMID 9215689.
- ↑ Marquard, Jessica; Eng, Charis (September 27, 1999). “Multiple Endocrine Neoplasia Type 2”. GeneReviews® [Internet].
- ↑ Rodriguez M, Nemeth E, Martin D (2005). “The calcium-sensing receptor: a key factor in the pathogenesis of secondary hyperparathyroidism”. Am J Physiol Renal Physiol. 288 (2): F253–64. doi:10.1152/ajprenal.00302.2004. PMID 15507543.
- ↑ Lips P (2001). “Vitamin D deficiency and secondary hyperparathyroidism in the elderly: consequences for bone loss and fractures and therapeutic implications”. Endocr Rev. 22 (4): 477–501. doi:10.1210/edrv.22.4.0437. PMID 11493580.
- ↑ Mehrotra M, Gupta SK, Kumar K, Awasthi PK, Dubey M, Pandey CM; et al. (2006). “Calcium deficiency-induced secondary hyperparathyroidism and osteopenia are rapidly reversible with calcium supplementation in growing rabbit pups”. Br J Nutr. 95 (3): 582–90. PMID 16512945.
- ↑ Johnson JM, Maher JW, DeMaria EJ, Downs RW, Wolfe LG, Kellum JM (2006). “The long-term effects of gastric bypass on vitamin D metabolism”. Ann. Surg. 243 (5): 701–4, discussion 704–5. doi:10.1097/01.sla.0000216773.47825.c1. PMC 1570540. PMID 16633006.
- ↑ Pitt SC, Sippel RS, Chen H (2009). “Secondary and tertiary hyperparathyroidism, state of the art surgical management”. Surg. Clin. North Am. 89 (5): 1227–39. doi:10.1016/j.suc.2009.06.011. PMC 2905047. PMID 19836494.
- ↑ Kilgo MS, Pirsch JD, Warner TF, Starling JR (1998). “Tertiary hyperparathyroidism after renal transplantation: surgical strategy”. Surgery. 124 (4): 677–83, discussion 683–4. doi:10.1067/msy.1998.91483. PMID 9780988.
- ↑ Pitt SC, Sippel RS, Chen H (2009). “Secondary and tertiary hyperparathyroidism, state of the art surgical management”. Surg. Clin. North Am. 89 (5): 1227–39. doi:10.1016/j.suc.2009.06.011. PMC 2905047. PMID 19836494.
Differentiating Hyperparathyroidism from other Diseases
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1];Associate Editor(s)-in-Chief: Anmol Pitliya, M.B.B.S. M.D.[2]
Overview
There are three types of hyperparathyroidism (primary, secondary, and tertiary) and should be differentiated between each other. Hyperparathyroidism should be differentiated from other causes of hypercalcemia. Causes of hypercalcemia other than hyperparathyroidism include familial hypocalciuric hypercalcemia, hypercalcemia related to malignancy, medication-induced hypercalcemia, hypercalcemia due to nutritional disorders, and hypercalcemia related to granulomatous diseases.
Differentiating hyperparathyroidism from other diseases
There are three types of hyperparathyroidism (primary, secondary, and tertiary) and should be differentiated between each other. Hyperparathyroidism should be differentiated from other causes of hypercalcemia. Causes of hypercalcemia include:
- Parathyroid related
- Hyperparathyroidism
- Primary hyperparathyroidism
- Secondary hyperparathyroidism
- Tertiary hyperparathyroidism
- Familial hypocalciuric hypercalcemia
- Hyperparathyroidism
- Non-parathyroid related
- Malignancy
- Humoral hypercalcemia of malignancy
- Osteolytic tumors
- Production of calcitriol by tumors
- Ectopic parathyroid hormone production
- Medication-induced
- Nutritional
- Granulomatous disease
- Surgical
- Immobization
- Malignancy
| Differential diagnosis of hyperparathyroidism on the basis of hypercalcemia | ||||||||
|---|---|---|---|---|---|---|---|---|
| Disorder | Mechanism of hypercalcemia | Clinical features | Laboratory findings | Imaging & diagnostic modalities | ||||
| PTH | Calcium | Phosphate | Other findings | |||||
| Hyperparathyroidism | Primary hyperparathyroidism | Increase in secretion of parathyroid hormone (PTH) from a primary process in parathyroid gland. Parathyroid hormone causes increase in serum calcium. |
|
↑ | ↑ | ↓/Normal | Normal/↑ calcitriol | Findings of bone resorption:
Preoperative localization of hyperfunctioning parathyroid gland:
Predicting post-operative success:
|
| Secondary hyperparathyroidism | Increase in secretion of parathyroid hormone (PTH) from a secondary process. Parathyroid hormone causes increase in serum calcium after long periods. |
|
↑ | ↓/Normal | ↑ | — | ||
| Tertiary hyperparathyroidism | Continuous elevation of parathyroid hormone (PTH) even after successful treatment of the secondary cause of elevated parathyroid hormone. Parathyroid hormone causes increase in serum calcium. |
|
↑ | ↑ | ↑ | — | ||
| Familial hypocalciuric hypercalcemia | This is a genetic disorder caused my mutation in calcium-sensing receptor gene. |
|
Normal/↑ | Normal/↑ | — | — |
| |
| Malignancy[1][2] | Humoral hypercalcemia of malignancy[3][4][5][6] | Tumor cells secretes parathyroid hormone-related protein (PTHrP) which has similar action as parathyroid hormone. |
|
— | ↑ | ↓/Normal | ↑ PTHrP
Normal/↑ calcitriol |
|
| Osteolytic tumors[7][8] | Multiple myeloma produces osteolysis of bones causing hypercalcemia. Osteolytic metasteses can cause bone resorption causing hypercalcemia. |
|
↓ | ↑ | — | — | ||
| Production of calcitirol[9] | Some tumors has ectopic activity of 1-alpha-hydroxylase leading to increased production of calcitriol. Calcitriol is active form of vitamin D and causes hypercalcemia. |
|
— | ↑ | — | ↑ Calcitriol | ||
| Ectopic parathyroid hormone[10] | Some tumors leads to ectopic production of parathyroid hormone. |
|
↑ | ↑ | ↓/Normal | Normal/↑ calcitriol | ||
| Medication induced | Lithium[11] | Lithium lowers urinary calcium and causes hypercalcemia. Lithium has been reported to cause an increase in parathyroid hormone and enlargement if parathyroid gland after weeks to months of therapy. |
|
↑ | ↑ | — | — |
|
| Thiazide diuretics[12] | Thiazide diuretics lowers urinary calcium excretion and causes hypercalcemia. |
|
— | ↑ | — | — | — | |
| Nutritional | Milk-alkali syndrome | Hypercalcemia is be caused by high intake of calcium carbonate. |
|
— | ↑ | — | ↓ calcitriol | |
| Vitamin D toxicity[13][14][15] | Excess vitamin D causes increased absorption of calcium from intestine causing hypercalcemia. |
|
— | ↑ | — | ↑ Vitamin D (calcidiol and/or calcitriol) | — | |
| Granulomatous disease | Sarcoidosis[18] | Hypercalcemia is causes by endogeous production of calcitriol by disease-activated macrophages. |
|
— | ↑ | — | ↑ Calcitriol
↑ ACE levels |
|
DIfferentiating Hyperparathyroidism from other diseases
| Disease | Gene | Chromosome | Differentiating Features | Components of MEN | Diagnosis | ||
|---|---|---|---|---|---|---|---|
| Parathyroid | Pitutary | Pancreas | |||||
| von Hippel-Lindau syndrome | Von Hippel–Lindau tumor suppressor | 3p25.3 |
|
– | – | + |
|
| Carney complex | PRKAR1A | 17q23-q24 |
|
– | – | – |
|
| Neurofibromatosis type 1 | RAS | 17 | – | – | – | Prenatal
Postnatal Cardinal Clinical Features” are required for positive diagnosis.
| |
| Li-Fraumeni syndrome | TP53 | 17 | Early onset of diverse amount of cancers such as | – | – | – |
Criteria
|
| Gardner’s syndrome | APC | 5q21 |
|
– | – | – |
|
| Multiple endocrine neoplasia type 2 | RET | – |
|
+ | – | – |
Criteria Two or more specific endocrine tumors
|
| Cowden syndrome | PTEN | – | Hamartomas | – | – | – |
|
| Acromegaly/gigantism | – | – |
|
– | + | – |
|
| Pituitary adenoma | – | – |
|
– | + | – |
|
| Hyperparathyroidism | – | – | – | + | – | – |
|
| Pheochromocytoma/paraganglioma |
VHL RET NF1 SDHB SDHD |
– | Characterized by | – | – | – |
|
| Adrenocortical carcinoma |
|
17p, 13q |
|
– | – | – |
|
| Adapted from Toledo SP, Lourenço DM, Toledo RA. A differential diagnosis of inherited endocrine tumors and their tumor counterparts, journal=Clinics (Sao Paulo), volume= 68, issue= 7, 07/24/2013[19] | |||||||
References
- ↑ Mirrakhimov AE (2015). “Hypercalcemia of Malignancy: An Update on Pathogenesis and Management”. N Am J Med Sci. 7 (11): 483–93. doi:10.4103/1947-2714.170600. PMC 4683803. PMID 26713296.
- ↑ Stewart AF (2005). “Clinical practice. Hypercalcemia associated with cancer”. N Engl J Med. 352 (4): 373–9. doi:10.1056/NEJMcp042806. PMID 15673803.
- ↑ Ratcliffe WA, Hutchesson AC, Bundred NJ, Ratcliffe JG (1992). “Role of assays for parathyroid-hormone-related protein in investigation of hypercalcaemia”. Lancet. 339 (8786): 164–7. doi:10.1016/0140-6736(92)90220-W. PMID 1346019.
- ↑ Ikeda K, Ohno H, Hane M, Yokoi H, Okada M, Honma T, Yamada A, Tatsumi Y, Tanaka T, Saitoh T (1994). “Development of a sensitive two-site immunoradiometric assay for parathyroid hormone-related peptide: evidence for elevated levels in plasma from patients with adult T-cell leukemia/lymphoma and B-cell lymphoma”. J. Clin. Endocrinol. Metab. 79 (5): 1322–7. doi:10.1210/jcem.79.5.7962324. PMID 7962324.
- ↑ Horwitz MJ, Tedesco MB, Sereika SM, Hollis BW, Garcia-Ocaña A, Stewart AF (2003). “Direct comparison of sustained infusion of human parathyroid hormone-related protein-(1-36) [hPTHrP-(1-36)] versus hPTH-(1-34) on serum calcium, plasma 1,25-dihydroxyvitamin D concentrations, and fractional calcium excretion in healthy human volunteers”. J. Clin. Endocrinol. Metab. 88 (4): 1603–9. doi:10.1210/jc.2002-020773. PMID 12679445.
- ↑ Stewart AF, Vignery A, Silverglate A, Ravin ND, LiVolsi V, Broadus AE; et al. (1982). “Quantitative bone histomorphometry in humoral hypercalcemia of malignancy: uncoupling of bone cell activity”. J Clin Endocrinol Metab. 55 (2): 219–27. doi:10.1210/jcem-55-2-219. PMID 7085851.
- ↑ Roodman GD (2004). “Mechanisms of bone metastasis”. N Engl J Med. 350 (16): 1655–64. doi:10.1056/NEJMra030831. PMID 15084698.
- ↑ Guise TA, Yin JJ, Taylor SD, Kumagai Y, Dallas M, Boyce BF; et al. (1996). “Evidence for a causal role of parathyroid hormone-related protein in the pathogenesis of human breast cancer-mediated osteolysis”. J Clin Invest. 98 (7): 1544–9. doi:10.1172/JCI118947. PMC 507586. PMID 8833902.
- ↑ Seymour JF, Gagel RF, Hagemeister FB, Dimopoulos MA, Cabanillas F (1994). “Calcitriol production in hypercalcemic and normocalcemic patients with non-Hodgkin lymphoma”. Ann Intern Med. 121 (9): 633–40. PMID 7944070.
- ↑ VanHouten JN, Yu N, Rimm D, Dotto J, Arnold A, Wysolmerski JJ, Udelsman R (2006). “Hypercalcemia of malignancy due to ectopic transactivation of the parathyroid hormone gene”. J. Clin. Endocrinol. Metab. 91 (2): 580–3. doi:10.1210/jc.2005-2095. PMID 16263810.
- ↑ Mallette LE, Khouri K, Zengotita H, Hollis BW, Malini S (1989). “Lithium treatment increases intact and midregion parathyroid hormone and parathyroid volume”. J. Clin. Endocrinol. Metab. 68 (3): 654–60. doi:10.1210/jcem-68-3-654. PMID 2918061.
- ↑ Griebeler ML, Kearns AE, Ryu E, Thapa P, Hathcock MA, Melton LJ; et al. (2016). “Thiazide-Associated Hypercalcemia: Incidence and Association With Primary Hyperparathyroidism Over Two Decades”. J Clin Endocrinol Metab. 101 (3): 1166–73. doi:10.1210/jc.2015-3964. PMC 4803175. PMID 26751196.
- ↑ Hoeck HC, Laurberg G, Laurberg P (1994). “Hypercalcaemic crisis after excessive topical use of a vitamin D derivative”. J. Intern. Med. 235 (3): 281–2. PMID 8120527.
- ↑ Jacobus CH, Holick MF, Shao Q, Chen TC, Holm IA, Kolodny JM, Fuleihan GE, Seely EW (1992). “Hypervitaminosis D associated with drinking milk”. N. Engl. J. Med. 326 (18): 1173–7. doi:10.1056/NEJM199204303261801. PMID 1313547.
- ↑ Sharma OP (1996). “Vitamin D, calcium, and sarcoidosis”. Chest. 109 (2): 535–9. PMID 8620732.
- ↑ Jacobus CH, Holick MF, Shao Q, Chen TC, Holm IA, Kolodny JM, Fuleihan GE, Seely EW (1992). “Hypervitaminosis D associated with drinking milk”. N. Engl. J. Med. 326 (18): 1173–7. doi:10.1056/NEJM199204303261801. PMID 1313547.
- ↑ Hoeck HC, Laurberg G, Laurberg P (1994). “Hypercalcaemic crisis after excessive topical use of a vitamin D derivative”. J. Intern. Med. 235 (3): 281–2. PMID 8120527.
- ↑ Dusso AS, Kamimura S, Gallieni M, Zhong M, Negrea L, Shapiro S, Slatopolsky E (1997). “gamma-Interferon-induced resistance to 1,25-(OH)2 D3 in human monocytes and macrophages: a mechanism for the hypercalcemia of various granulomatoses”. J. Clin. Endocrinol. Metab. 82 (7): 2222–32. doi:10.1210/jcem.82.7.4074. PMID 9215298.
- ↑ Toledo SP, Lourenço DM, Toledo RA (2013). “A differential diagnosis of inherited endocrine tumors and their tumor counterparts”. Clinics (Sao Paulo). 68 (7): 1039–56. doi:10.6061/clinics/2013(07)24. PMC 3715026. PMID 23917672.
Epidemiology and Demographics
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Anmol Pitliya, M.B.B.S. M.D.[2]
Overview
Primary hyperparathyroidism is the 3rd most common endocrine disorder. Highest incidence of primary hyperparathyroidism is in post-menopausal women.The incidence of primary hyperparathyroidism is approximately 0.4 to 21.6 per 100,000 person years. The prevalence of primary hyperparathyroidism is approximately .01 to .07 per 100,000 individuals. The incidence of primary hyperparathyroidism increases with age. Primary hyperparathyroidism usually affects individuals of African-American race. Women are more commonly affected by primary hyperparathyroidism than men. The women to men ratio is approximately 3 to 1. Difference in gender specific incidence of primary hyperparathyroidism becomes more pronounced with advancing age. There is insufficient data on epidemiology and demographics of secondary and tertiary hyperparathyroidism.
Epidemiology and Demographics
Primary hyperparathyroidism
Primary hyperparathyroidism is the 3rd most common endocrine disorder. Highest incidence of primary hyperparathyroidism is in post-menopausal women.[1] Epidemiology and demographics of primary hyperparathyroidism is as follows:[2]
Incidence
- The incidence of primary hyperparathyroidism is approximately 0.4 to 21.6 per 100,000 person years.
Prevalence
- The prevalence of primary hyperparathyroidism is approximately .01 to .07 per 100,000 individuals.
Age
- The incidence of primary hyperparathyroidism increases with age.
- In individuals age < 50 years, the incidence of primary hyperparathyroidism ranges from a low of 12 per 100,000 person years to a high of 24 per 100,000 per person years.
Race
- Primary hyperparathyroidism usually affects individuals of African-American race.
- The incidence of primary hyperparathyroidism according to race is as follows:
| Incidence of Primary hyperparathyroidism according to race | ||
|---|---|---|
| Race | Gender (incidence per 100,000 person years) | |
| Women | Men | |
| African-American | 92 | 46 |
| White | 81 | 29 |
| Asian | 52 | 28 |
| Hispanic | 49 | 17 |
| Other race | 25 | 6 |
Gender
- Women are more commonly affected by primary hyperparathyroidism than men. The women to men ratio is approximately 3 to 1.
- In women, the incidence of primary hyperparathyroidism ranges from a low of 34 per 100,000 person years to a high of 120 per 100,000 person years with an average incidence of 66 per 100,000 person years.
- In men, the incidence of primary hyperparathyroidism ranges from a low of 13 per 100,000 person years to a high of 36 per 100,000 person years with an average incidence of 24 per 100,000 person years.
- Difference in gender specific incidence of primary hyperparathyroidism becomes more pronounced with advancing age.
| Incidence of primary hyperparathyroidism in different age group | ||
|---|---|---|
| Age group | Gender (incidence per 100,000 person years) | |
| Women | Men | |
| Age < 50 years | 12-24 | 12-24 |
| Age 50 – 59 years | 80 | 36 |
| Age 70-79 years | 196 | 95 |
Secondary and Tertiary Hyperparathyroidism
There is insufficient data on epidemiology and demographics of secondary and tertiary hyperparathyroidism.
References
- ↑ Fraser WD (2009). “Hyperparathyroidism”. Lancet. 374 (9684): 145–58. doi:10.1016/S0140-6736(09)60507-9. PMID 19595349.
- ↑ Yeh MW, Ituarte PH, Zhou HC, Nishimoto S, Liu IL, Harari A, Haigh PI, Adams AL (2013). “Incidence and prevalence of primary hyperparathyroidism in a racially mixed population”. J. Clin. Endocrinol. Metab. 98 (3): 1122–9. doi:10.1210/jc.2012-4022. PMC 3590475. PMID 23418315.
Risk Factors
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Anmol Pitliya, M.B.B.S. M.D.[2]
Overview
Common risk factors in the development of primary hyperparathyroidism include postmenopausal women, age group 50-60 year, family history of hyperparathyroidism, and history of familial syndromes. Common risk factors in the development of secondary hyperparathyroidism in chronic renal failure include high serum phosphorus expression levels, low serum creatinine expression levels, low serum calcium expression levels, female gender, and hypertension. Common risk factors in the development of tertiary hyperparathyroidism post renal transplantation include elderly individuals and longer duration of dialysis.
Risk Factors
Common risk factors in the development of primary hyperparathyroidism include postmenopausal women, age group 50-60 year, family history of hyperparathyroidism, and history of familial syndromes.
Common risk factors in the development of secondary hyperparathyroidism in chronic renal failure include high serum phosphorus expression levels, low serum creatinine expression levels, low serum calcium expression levels, female gender, and hypertension.
Common risk factors in the development of tertiary hyperparathyroidism post renal transplantation include elderly individuals and longer duration of dialysis.
Common Risk Factors
Common risk factors in the development of primary hyperparathyroidism include:
- Postmenopausal women
- Age group 50-60 years
- Family history of hyperparathyroidism
- History of familial syndromes such as multiple endocrine neoplasia type 1, type 2A or type 4; familial hypocalciuric hypercalcemia, hyperparathyroid-jaw tumor syndrome
Common risk factors in the development of secondary hyperparathyroidism in chronic renal failure include:[1]
- High serum phosphorus expression levels
- Low serum creatinine expression levels
- Low serum calcium expression levels
- Female gender
- Hypertension
Common risk factors in the development of tertiary hyperparathyroidism post renal transplantation include:[2]
- Elderly individuals
- Longer duration of dialysis
Less Common Risk Factors
Less common risk factors in the development of primary hyperparathyroidism include:
Less common risk factors in the development of secondary hyperparathyroidism in chronic renal failure include:[1]
References
- ↑ 1.0 1.1 Wei Y, Lin J, Yang F, Li X, Hou Y, Lu R, Shi X, Liu Z, Du Y (2016). “Risk factors associated with secondary hyperparathyroidism in patients with chronic kidney disease”. Exp Ther Med. 12 (2): 1206–1212. doi:10.3892/etm.2016.3438. PMC 4950648. PMID 27446345.
- ↑ Hamidian Jahromi A, Roozbeh J, Raiss-Jalali GA, Dabaghmanesh A, Jalaeian H, Bahador A, Nikeghbalian S, Salehipour M, Salahi H, Malek-Hosseini A (2009). “Risk factors of post renal transplant hyperparathyroidism”. Saudi J Kidney Dis Transpl. 20 (4): 573–6. PMID 19587496.
- ↑ Szalat, Auryan; Mazeh, Haggi; Freund, Herbert R (2009). “Lithium-associated hyperparathyroidism: report of four cases and review of the literature” (PDF). European Journal of Endocrinology. 160: 317–323.
Screening
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Anmol Pitliya, M.B.B.S. M.D.[2]
Overview
There is insufficient evidence to recommend routine screening for hyperparathyroidism.
Screening
There is insufficient evidence to recommend routine screening for hyperparathyroidism.
References
Natural History, Complications and Prognosis
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Anmol Pitliya, M.B.B.S. M.D.[2]
Overview
Primary hyperparathyroidism usually develops in the fifth decade of life, in post-menopausal women and starts as asymptomatic hypercalcemia in presence of increased parathyroid hormone. If left untreated, some of patients with primary hyperparathyroidism may commonly develop marked hypercalcemia, marked hypercalciuria, cortical bone demineralization and nephrolithiasis.
Secondary hyperparathyroidism arise in the early course of chronic renal failure. As renal failure progress, secondary hyperparathyroidism becomes more notable. If left untreated, secondary hyperparathyroidism carries an increased risk of vascular calcification with increasing age and duration of dialysis in patients.
Tertiary hyperparathyroidism usually develops in post renal transplant patients. If left untreated, tertiary hyperparathyroidism in post renal transplant patients may carry the risk of amyloid deposition, calciphylaxis, destructive or erosive spondyloarthropathy, osteonecrosis, and musculoskeletal infections.
Hyperparathyroidism leads to a variety of complications in various organ systems depending on the type of hyperparathyroidism.
Prognosis is all types hyperparathyroidism is generally good after proper treatment.
Natural History
Primary hyperparathyroidism
- Primary hyperparathyroidism usually develops in the fifth decade of life, in post-menopausal women and starts as asymptomatic hypercalcemia in presence of increased parathyroid hormone.
- If left untreated, some of the patients with primary hyperparathyroidism may develop marked hypercalcemia, hypercalciuria, cortical bone demineralization and nephrolithiasis.[1][2]
Secondary hyperparathyroidism
- Secondary hyperparathyroidism arise in the early course of chronic renal failure. As renal failure progress, secondary hyperparathyroidism becomes more notable.[3]
- Secondary hyperparathyroidism leads to vascular calcification due to elevated calcium and phosphorus levels. This is strongly associated with increase in morbidity and mortality.[4]
- If left untreated, secondary hyperparathyroidism carries an increased risk of vascular calcification with increasing age and duration of dialysis in patients.
Tertiary hyperparathyroidism
- Tertiary hyperparathyroidism usually develops in post renal transplant patients.
- If left untreated, tertiary hyperparathyroidism in post renal transplant patients may carry the risk of amyloid deposition, calciphylaxis, destructive or erosive spondyloarthropathy, osteonecrosis, and musculoskeletal infections.[5]
Complications
| Complications involving Organ system | Complications of hyperparathyroidism | ||
|---|---|---|---|
| Primary hyperparathyroidism | Secondary hyperparathyroidism | Tertiary hyperparathyroidism | |
| Cardiaovascular complications |
|
|
— |
| Endocrine complications[8] | — | — | |
| Gastrointestinal complications[9] | — | — | |
| Hematologic complications[10] | — |
|
|
| Metabolic complications |
|
||
| Musculo-skeletal complications | |||
| Neurologic complications | — |
|
— |
| Neuromuscular complications |
|
|
|
| Pregnancy related complications[26] |
|
— | — |
| Psychiatric complications |
|
— | — |
| Renal complications |
|
|
|
| Rheumatologic complications | — |
| |
| System non-specific complications | — |
|
|
Prognosis
Primary hyperparathyroidism
- Prognosis of primary hyperparathyroidism is generally excellent after parathyroidectomy.
- The complications of primary hyperparathyroidism resolves after the treatment.
- Untreated complication of primary hyperparathyroidism may be fatal.[9]
Secondary hyperparathyroidism
- Effective treatment can reduce morbidity and mortality associated with uncontrolled secondary hyperparathyroidism.[4]
- Hyperphosphatemia and metastatic calcification results due elevated product of serum calcium and serum phosphorus. Both conditions are present in patients with secondary hyperparathyroidism in presence of end stage renal disease. This leads to a significant increase in morbidity and mortality. Aggressive control of hyperphosphatemia may improve prognosis[37]
Tertiary hyperparathyroidism
- Prognosis of tertiary hyperparathyroidism is generally good after resection of abnormal hyperplastic gland.[38]
References
- ↑ 1.0 1.1 Peacock M (2002). “Primary hyperparathyroidism and the kidney: biochemical and clinical spectrum”. J. Bone Miner. Res. 17 Suppl 2: N87–94. PMID 12412783.
- ↑ Silverberg SJ, Shane E, de la Cruz L, Dempster DW, Feldman F, Seldin D, Jacobs TP, Siris ES, Cafferty M, Parisien MV (1989). “Skeletal disease in primary hyperparathyroidism”. J. Bone Miner. Res. 4 (3): 283–91. doi:10.1002/jbmr.5650040302. PMID 2763869.
- ↑ Nikodimopoulou M, Liakos S (2011). “Secondary hyperparathyroidism and target organs in chronic kidney disease”. Hippokratia. 15 (Suppl 1): 33–8. PMC 3139677. PMID 21897756.
- ↑ 4.0 4.1 Cunningham J, Locatelli F, Rodriguez M (2011). “Secondary hyperparathyroidism: pathogenesis, disease progression, and therapeutic options”. Clin J Am Soc Nephrol. 6 (4): 913–21. doi:10.2215/CJN.06040710. PMID 21454719.
- ↑ 5.0 5.1 5.2 Jevtic V (2003). “Imaging of renal osteodystrophy”. Eur J Radiol. 46 (2): 85–95. doi:10.1016/S0720-048X(03)00072-X. PMID 12714225.
- ↑ Stefenelli T, Abela C, Frank H, Koller-Strametz J, Globits S, Bergler-Klein J, Niederle B (1997). “Cardiac abnormalities in patients with primary hyperparathyroidism: implications for follow-up”. J. Clin. Endocrinol. Metab. 82 (1): 106–12. doi:10.1210/jcem.82.1.3666. PMID 8989242.
- ↑ Strózecki P, Adamowicz A, Nartowicz E, Odrowaz-Sypniewska G, Włodarczyk Z, Manitius J (2001). “Parathormon, calcium, phosphorus, and left ventricular structure and function in normotensive hemodialysis patients”. Ren Fail. 23 (1): 115–26. PMID 11256521.
- ↑ Bai HX, Giefer M, Patel M, Orabi AI, Husain SZ (2012). “The association of primary hyperparathyroidism with pancreatitis”. J. Clin. Gastroenterol. 46 (8): 656–61. doi:10.1097/MCG.0b013e31825c446c. PMC 4428665. PMID 22874807.
- ↑ 9.0 9.1 9.2 Corlew DS, Bryda SL, Bradley EL, DiGirolamo M (1985). “Observations on the course of untreated primary hyperparathyroidism”. Surgery. 98 (6): 1064–71. PMID 3878002.
- ↑ Remuzzi G, Benigni A, Dodesini P, Schieppati A, Livio M, Poletti E, Mecca G, de Gaetano G (1981). “Parathyroid hormone inhibits human platelet function”. Lancet. 2 (8259): 1321–3. doi:10.1016/S0140-6736(81)91343-X. PMID 6118720.
- ↑ Fitzpatrick LA, Bilezikian JP (1987). “Acute primary hyperparathyroidism”. Am. J. Med. 82 (2): 275–82. PMID 3812520.
- ↑ Ahmad S, Kuraganti G, Steenkamp D (2015). “Hypercalcemic crisis: a clinical review”. Am. J. Med. 128 (3): 239–45. doi:10.1016/j.amjmed.2014.09.030. PMID 25447624.
- ↑ Lips P (2001). “Vitamin D deficiency and secondary hyperparathyroidism in the elderly: consequences for bone loss and fractures and therapeutic implications”. Endocr Rev. 22 (4): 477–501. doi:10.1210/edrv.22.4.0437. PMID 11493580.
- ↑ Saab G, Whaley-Connell A, Bombeck A, Kurella Tamura M, Li S, Chen SC, McFarlane SI, Sowers JR, Norris K, Bakris GL, McCullough PA (2011). “The Association between Parathyroid Hormone Levels and the Cardiorenal Metabolic Syndrome in Non-Diabetic Chronic Kidney Disease”. Cardiorenal Med. 1 (2): 123–130. doi:10.1159/000327149. PMC 3101512. PMID 22258399.
- ↑ Hjelmesæth, Jøran; Hofsø, Dag; Aasheim, Erlend T; Jenssen, Trond; Moan, Johan; Hager, Helle; Røislien, Jo; Bollerslev, Jens (2009). “Parathyroid hormone, but not vitamin D, is associated with the metabolic syndrome in morbidly obese women and men: a cross-sectional study”. Cardiovascular Diabetology. 8 (1): 7. doi:10.1186/1475-2840-8-7. ISSN 1475-2840.
- ↑ Barbur MA, Kurjak M, Becker K (1997). “[Systematic calciphylaxis in chronic renal failure: fulminant course after kidney transplantation]”. Pathologe (in German). 18 (6): 453–8. PMID 9451734.
- ↑ Bandeira F, Cusano NE, Silva BC, Cassibba S, Almeida CB, Machado VC, Bilezikian JP (2014). “Bone disease in primary hyperparathyroidism”. Arq Bras Endocrinol Metabol. 58 (5): 553–61. PMC 4315357. PMID 25166047.
- ↑ Mazzuoli GF, D’Erasmo E, Pisani D (1998). “Primary hyperparathyroidism and osteoporosis”. Aging (Milano). 10 (3): 225–31. PMID 9801732.
- ↑ Spaulding CM, Young G (1997). “Osteitis fibrosa cystica and chronic renal failure”. J Am Podiatr Med Assoc. 87 (5): 238–40. doi:10.7547/87507315-87-5-238. PMID 9158318.
- ↑ Eastwood JB (1977). “Renal osteodystrophy–a radiological review”. CRC Crit Rev Diagn Imaging. 9 (1): 77–104. PMID 328228.
- ↑ Adams JE (1999). “Renal bone disease: radiological investigation”. Kidney Int. Suppl. 73: S38–41. PMID 10633462.
- ↑ Goldstein DA, Feinstein EI, Chui LA, Pattabhiraman R, Massry SG (1980). “The relationship between the abnormalities in electroencephalogram and blood levels of parathyroid hormone in dialysis patients”. J. Clin. Endocrinol. Metab. 51 (1): 130–4. doi:10.1210/jcem-51-1-130. PMID 6892917.
- ↑ Avram MM, Feinfeld DA, Huatuco AH (1978). “Search for the uremic toxin. Decreased motor-nerve conduction velocity and elevated parathyroid hormone in uremia”. N. Engl. J. Med. 298 (18): 1000–3. doi:10.1056/NEJM197805042981805. PMID 205786.
- ↑ Mallette LE, Patten BM, Engel WK (1975). “Neuromuscular disease in secondary hyperparathyroidism”. Ann. Intern. Med. 82 (4): 474–83. PMID 47234.
- ↑ Gerhardt RE, Zeitlin EL (1978). “Neuromuscular disease in tertiary hyperparathyroidism”. Arch. Intern. Med. 138 (6): 1013–5. PMID 646555.
- ↑ Poomthavorn P, Ongphiphadhanakul B, Mahachoklertwattana P (2008). “Transient neonatal hypoparathyroidism in two siblings unmasking maternal normocalcemic hyperparathyroidism”. Eur. J. Pediatr. 167 (4): 431–4. doi:10.1007/s00431-007-0528-6. PMID 17569990.
- ↑ Walker MD, McMahon DJ, Inabnet WB, Lazar RM, Brown I, Vardy S, Cosman F, Silverberg SJ (2009). “Neuropsychological features in primary hyperparathyroidism: a prospective study”. J. Clin. Endocrinol. Metab. 94 (6): 1951–8. doi:10.1210/jc.2008-2574. PMC 2690425. PMID 19336505.
- ↑ Espiritu RP, Kearns AE, Vickers KS, Grant C, Ryu E, Wermers RA (2011). “Depression in primary hyperparathyroidism: prevalence and benefit of surgery”. J. Clin. Endocrinol. Metab. 96 (11): E1737–45. doi:10.1210/jc.2011-1486. PMID 21917870.
- ↑ McAllion SJ, Paterson CR (1989). “Psychiatric morbidity in primary hyperparathyroidism”. Postgrad Med J. 65 (767): 628–31. PMC 2429194. PMID 2608590.
- ↑ Lila AR, Sarathi V, Jagtap V, Bandgar T, Menon PS, Shah NS (2012). “Renal manifestations of primary hyperparathyroidism”. Indian J Endocrinol Metab. 16 (2): 258–62. doi:10.4103/2230-8210.93745. PMC 3313745. PMID 22470864.
- ↑ Tassone F, Gianotti L, Emmolo I, Ghio M, Borretta G (2009). “Glomerular filtration rate and parathyroid hormone secretion in primary hyperparathyroidism”. J. Clin. Endocrinol. Metab. 94 (11): 4458–61. doi:10.1210/jc.2009-0587. PMID 19808852.
- ↑ Kim H, Cheigh JS, Ham HW (2001). “Urinary stones following renal transplantation”. Korean J. Intern. Med. 16 (2): 118–22. PMC 4531707. PMID 11590898.
- ↑ Michael JW, Schlüter-Brust KU, Eysel P (2010). “The epidemiology, etiology, diagnosis, and treatment of osteoarthritis of the knee”. Dtsch Arztebl Int. 107 (9): 152–62. doi:10.3238/arztebl.2010.0152. PMC 2841860. PMID 20305774.
- ↑ Hochberg, Marc (2015). “204. Primary hyperparathyroidism: rheumatologic manifestations and bone disease”. Rheumatology. Philadelphia, PA: Mosby/Elsevier. p. 1668. ISBN 9780323091381.
- ↑ Rubin MR, Silverberg SJ (2002). “Rheumatic manifestations of primary hyperparathyroidism and parathyroid hormone therapy”. Curr Rheumatol Rep. 4 (2): 179–85. PMID 11890884.
- ↑ Adler JS, Cameron DC (1989). “Erosive spondylo-arthropathy and tertiary hyperparathyroidism”. Australas Radiol. 33 (1): 90–2. PMID 2712794.
- ↑ 37.0 37.1 Block GA, Hulbert-Shearon TE, Levin NW, Port FK (1998). “Association of serum phosphorus and calcium x phosphate product with mortality risk in chronic hemodialysis patients: a national study”. Am. J. Kidney Dis. 31 (4): 607–17. PMID 9531176.
- ↑ Nichol PF, Starling JR, Mack E, Klovning JJ, Becker BN, Chen H (2002). “Long-term follow-up of patients with tertiary hyperparathyroidism treated by resection of a single or double adenoma”. Ann. Surg. 235 (5): 673–8, discussion 678–80. PMC 1422493. PMID 11981213.
Diagnosis
Diagnosis
History and Symptoms | Physical Examination | Laboratory Findings | EKG | X ray | CT | MRI | Ultrasound | Other Imaging Findings | Other Diagnostic Studies
Treatment
Treatment
Medical Therapy | Surgery | Primary Prevention | Secondary Prevention | Cost-Effectiveness of Therapy | Future or Investigational Therapies
Looking for the patient version?
© 2026 MyEClinic – IFTM Institut für Telematik in der Medizin GmbH