
Multiple myeloma
For patient information click here
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Haytham Allaham, M.D. [2]; Shyam Patel [3]
Synonyms and keywords:Kahler disease; Kahler’s disease; MM; Myeloma; Myelomatosis; Medullary plasmacytoma; Plasmacytoma
Overview
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1] Associate Editor(s)-in-Chief: Haytham Allaham, M.D. [2]
Overview
Multiple myeloma (MM) is a mature B-cell neoplastic proliferative disease. Multiple myeloma is part of the broad group of diseases called hematological malignancies and is also known as plasma cell myeloma, myelomatosis, or Kahler disease.[1]There are no established causes for multiple myeloma. Multiple myeloma must be differentiated from monoclonal gammopathy of undetermined significance(MGUS), isolated plasmacytoma of the bone, and extramedullary plasmacytoma.[2] The most potent risk factor in the development of multiple myeloma is old age.[3][4][5] The prognosis of multiple myeloma is good with treatment, while without treatment, multiple myeloma will result in death with a median survival of 7 months.[6][7] Multiple myeloma is the second most common blood cancer after non-Hodgkin’s lymphoma & 14th most common cancer overall in United States.[8][9][10] There is insufficient evidence to recommend routine screening for multiple myeloma.[11][12] If left untreated, most of patients with multiple myeloma may progress to develop fatigue, bone pain, and pallor.[10] Multiple myeloma may be divided into three stages based on either the International Staging System or Durie-Salmon Staging System.[13] The most common symptoms of multiple myeloma include bone pain, pallor, and fatigue.[10][14][15] Patients with multiple usually appear fatigued and lethargic.[10][14] Laboratory findings consistent with the diagnosis of multiple myeloma include abnormal complete blood count, erythrocyte sedimentation rate (ESR), basic metabolic panel, electrophoresis and immunohistochemistry.[14][10] Pharmacological regimes for patients with active (symptomatic) multiple myeloma include steroid therapy, immune modulator therapy, and chemotherapy.[16][17] Whereas patients with smoldering (asymptomatic) multiple myeloma are managed by observation and undergoing follow up tests every 3 to 6 months.[16][17]
Pathophysiology
Multiple myeloma arises from post-germinal center B lymphocytes, that are normally involved in production of human immunoglobulins.[4][10][18][19] Development of multiple myeloma is the result of multiple genetic translocation between the immunoglobulin heavy chain gene and oncogenes which leads to dysregulated multiplication of plasma cells.[10][18] On microscopic histopathological analysis, abundant eosinophilic cytoplasm, eccentrically placed nucleus, and russell bodies bodies are characteristic findings of multiple myeloma.[7]
Causes
There are no established causes for multiple myeloma.
Differentiating Multiple Myeloma from other Diseases
Multiple myeloma must be differentiated from monoclonal gammopathy of undetermined significance(MGUS), isolated plasmacytoma of the bone, and extramedullary plasmacytoma.[20]
Epidemiology and Demographics
In 2012, the incidence of multiple myeloma was approximately 6.3 per 100,000 cases with a mortality rate of 3.3 per 100,000 cases in the United States.[21] The prevalence of multiple myeloma was estimated to be 89,658 cases in 2012 in the United States.[9][10] Multiple myeloma is the second most common blood cancer after non-Hodgkin’s lymphoma & 14th most common cancer overall in United States.[8][9][10] Male are more commonly affected with multiple myeloma than female. The male to female ratio is approximately 1.54 to 1.[10][4] Multiple myeloma usually affects individuals of the African American and Native Pacific Islanders race. Asian individuals are less likely to develop multiple myeloma.[10] The incidence of multiple myeloma increases with age; the median age at diagnosis is between 65 to 70 years years.[10]
Risk Factors
The most potent risk factor in the development of multiple myeloma is old age. Other risk factors include positive family history, positive history of monoclonal gammopathy of undetermined significance (MGUS), and occupational exposure to radiation and toxic chemicals.[10][4][22]
Screening
There is insufficient evidence to recommend routine screening for multiple myeloma.[23][24]
Natural History, Complications and Prognosis
If left untreated, most of patients with multiple myeloma may progress to develop fatigue, bone pain, and pallor.[10] Complications that can develop as a result of multiple myeloma are anemia, renal failure, skeletal complications, and neurological complications.[6] The prognosis of multiple myeloma is good with treatment, while without treatment, multiple myeloma will result in death with a median survival of 7 months.[6][7] Multiple myeloma is associated with a 10 year survival of 3%. The presence of plasma cell leukemia or soft tissue plasmacytomas is associated with a particularly poor prognosis among patients with multiple myeloma.[25] According to a report published by National Cancer Institute there is a 43.25% chance of 5 year survival.[6]
Diagnosis
Diagnostic Criteria
The International Myeloma Working Group (IMWG) proposed updated criteria for the diagnosis of multiple myeloma in November 2014. The diagnosis requires >10% clonal plasma cell proliferation in the bone marrow, or biopsy-proven plasmacytosis at an extramedullary site plus one of more of the multiple myeloma-defining CRAB features (hypercalcemia, renal failure, anaemia, and bone lesions) or one or more of the newly added biomarkers of malignancy (clonal bone marrow plasma cell percentage ≥60%, involved:uninvolved serum free light chain ratio ≥100, and >1 focal lesions on MRI studies).[26]
Staging
Multiple myeloma may be divided into three stages based on either the International Staging System or Durie-Salmon Staging System.[27] The International Staging System for multiple myeloma was published by International Myeloma Working Group in 2003 and is the most widely used staging system.[28][29] It is used for both guiding treatment as well as predicting prognosis. The Durie-Salmon staging system, first published in 1975, is a clinical staging system for multiple myeloma that correlates measured myeloma cell mass to the presenting clinical features, response to treatment, and survival.[30] Durie-Salmon Staging System is still in use, but has been largely superseded by the more practical ISS.[31]
History and Symptoms
The most common symptoms of multiple myeloma include bone pain, pallor, and fatigue.[10][14][15] However, the presenting symptoms of multiple myeloma may vary greatly due to involvement of many organ systems. The common symptoms of multiple myeloma can be remembered by the mnemonic CRAB – C = Calcium (elevated), R =Renal failure, A = Anemia, B = Bone lesions.[32][14][15]
Physical Examination
Patients with multiple usually appear fatigued and lethargic.[10][14] Physical examination of patients with multiple myeloma is usually remarkable for pallor, purpura, hepatosplenomegaly, carpal tunnel syndrome, and signs of cord compression.[10][14] Any of these physical findings may warrant further evaluation, and thus leads to an incidental diagnosis of multiple myeloma.
Laboratory Findings
Laboratory findings consistent with the diagnosis of multiple myeloma include abnormal complete blood count, erythrocyte sedimentation rate (ESR), basic metabolic panel, electrophoresis and immunohistochemistry. An elevated concentration of serum protein level without concomitant elevation of serum albumin level is very suggestive of multiple myeloma.[14][10]
X Ray
X-ray may be helpful in the diagnosis of multiple myeloma. Findings on X-ray suggestive of multiple myeloma include punched out bony lesions, generalized osteopenia, and hair on end appearance.[4]
CT
CT scan does not have a great role in the diagnosis of disseminated multiple myeloma.[4]
MRI
MRI may be diagnostic of multiple myeloma. Findings on MRI suggestive of multiple myeloma include infiltration and replacement of the bone marrow.[4]
Other Imaging Findings
Positron Emission Tomography (PET) scan may be diagnostic of multiple myeloma.[14][4][33][34] Findings on PET scan suggestive of multiple myeloma include uptake of the F18-FDG molecule by lesions of bone lysis seen on PET-CT scan.[4]
Other Diagnostic Studies
Biopsy and genetic testing may be helpful in the diagnosis of multiple myeloma.[14] On bone marrow biopsy, multiple myeloma is characterized by an increase in percentage of abnormal plasma cells.[14] On genetic testing, multiple myeloma is characterized by chromosome 13 deletion and chromosome 14 translocation.[14][10]
Treatment
Medical Therapy
Pharmacological regimes for patients with active (symptomatic) multiple myeloma include steroid therapy, immune modulator therapy, and chemotherapy.[16][17] Whereas patients with smoldering (asymptomatic) multiple myeloma are managed by observation and undergoing follow up tests every 3 to 6 months.[16][17] The optimal therapy for active multiple myeloma depends on whether or not a patient is eligible for bone marrow transplantation.[16][17] Pharmacologic medical therapy for active multiple myeloma patients who are eligible for a bone marrow transplant include either dexamethasone, lenalidomide, bortezomib, thalidomide, carfilzomib, cyclophosphamide, vincristine, or doxorubicin.[16][17] In addition to the aforementioned agents, pharmacological regimes used for treatment of active multiple myeloma patients who are not eligible for a bone marrow transplant include either melphalan or prednisone.[16][17] Alkylating agents are not recommended among transplant eligible patients, as the toxicity of such agents makes the harvest process of bone marrow stem cell difficult later in the course of the disease.[16][17]
Surgery
Surgery is not a main treatment for multiple myeloma. Emergency surgery may be needed to help support weight-bearing bones in the spine or legs to prevent bones from breaking.
References
- ↑ Sergentanis TN, Zagouri F, Tsilimidos G, Tsagianni A, Tseliou M, Dimopoulos MA, Psaltopoulou T (October 2015). “Risk Factors for Multiple Myeloma: A Systematic Review of Meta-Analyses”. Clin Lymphoma Myeloma Leuk. 15 (10): 563–77.e1–3. doi:10.1016/j.clml.2015.06.003. PMID 26294217.
- ↑ “Myeloma – SEER Stat Fact Sheets”. Retrieved 17 February 2014.
- ↑ Press Releases. Compugen (2015)http://www.cgen.com/media-center/press-releases/-314 Accessed on September, 20th 2015
- ↑ 4.0 4.1 4.2 4.3 4.4 4.5 4.6 4.7 4.8 Multiple myeloma. Radiopaedia (2015)http://radiopaedia.org/articles/multiple-myeloma-1 Accessed on September, 20th 2015
- ↑ Multiple myeloma. The American Cancer Society (2015) http://www.cancer.org/cancer/multiplemyeloma/detailedguide/multiple-myeloma-risk-factors Accessed on September, 20 2015
- ↑ 6.0 6.1 6.2 6.3 Multiple myeloma. National Cancer Institute(2015) www.cancer.gov/types/myeloma/hp/myeloma-treatment-pdq#link/_40_toc Accessed on September, 20th 2015
- ↑ 7.0 7.1 7.2 Multiple myeloma. Librepathology (2015)http://www.wikidoc.org/index.php?title=Multiple_myeloma_pathophysiology&action=edit§ion Accessed on September, 20th 2015=1
- ↑ 8.0 8.1 Collins, CD. (2005). “Problems monitoring response in multiple myeloma”. Cancer Imaging. 5 Spec No A: S119–26. doi:10.1102/1470-7330.2005.0033. PMID 16361127.
- ↑ 9.0 9.1 9.2 Seer stat fact sheet. National cancer institute (2015)http://seer.cancer.gov/statfacts/html/mulmy.html Accessed on September, 20th 2015
- ↑ 10.00 10.01 10.02 10.03 10.04 10.05 10.06 10.07 10.08 10.09 10.10 10.11 10.12 10.13 10.14 10.15 10.16 10.17 10.18 Multiple myeloma. Wikipedia (2015)https://en.wikipedia.org/wiki/Multiple_myeloma#Pathophysiology Accessed on September, 20th 2015
- ↑ Multiple Myeloma Prevention and Screening.(2015)http://www.mdanderson.org/patient-and-cancer-information/cancer-information/cancer-types/multiple-myeloma/prevention/index.html
- ↑ Can multiple myeloma be prevented?(2015)http://www.cancer.org/cancer/multiplemyeloma/detailedguide/multiple-myeloma-prevention
- ↑ About multiple myeloma. University of California San Francisco (2015)http://cancer.ucsf.edu/research/multiple-myeloma/ Accessed on September, 18 2015
- ↑ 14.00 14.01 14.02 14.03 14.04 14.05 14.06 14.07 14.08 14.09 14.10 14.11 Multiple myeloma. Canadian Cancer Society (2015) http://www.cancer.ca/en/cancer-information/cancer-type/multiple-myeloma/signs-and-symptoms/?region=mb Accessed on September 20th 2015
- ↑ 15.0 15.1 15.2 Multiple myeloma. Cancer. gov(2015) http://www.cancer.gov/types/myeloma Accessed on September, 20th 2015
- ↑ 16.0 16.1 16.2 16.3 16.4 16.5 16.6 16.7 Treatment guide active multiple myeloma. National comprehensive cancer network(2015) http://www.nccn.org/patients/guidelines/myeloma/#44/z Accessed on September, 20th 2015
- ↑ 17.0 17.1 17.2 17.3 17.4 17.5 17.6 17.7 Treatment guide smoldering multiple myeloma. National comprehensive cancer network(2015) http://www.nccn.org/patients/guidelines/myeloma/#44/z Accessed on September, 20th 2015
- ↑ 18.0 18.1 Multiple myeloma. Medlineplus (2015)https://www.nlm.nih.gov/medlineplus/multiplemyeloma.html Accessed on September, 20th 2015
- ↑ Multiple myeloma. National cancer institute (2015) Accessed on September, 20th 2015
- ↑ “Myeloma – SEER Stat Fact Sheets”. Retrieved 17 February 2014.
- ↑ Plasma cell neoplasm.National cancer institute (2015)http://www.cancer.gov/types/myeloma/hp/myeloma-treatment-pdq#cit/section_1.1
- ↑ Multiple myeloma. The American Cancer Society (2015) http://www.cancer.org/cancer/multiplemyeloma/detailedguide/multiple-myeloma-risk-factors Accessed on September, 20 2015
- ↑ Multiple Myeloma Prevention and Screening.(2015)http://www.mdanderson.org/patient-and-cancer-information/cancer-information/cancer-types/multiple-myeloma/prevention/index.html
- ↑ Can multiple myeloma be prevented?(2015)http://www.cancer.org/cancer/multiplemyeloma/detailedguide/multiple-myeloma-prevention
- ↑ Plasma cell neoplasm. Cancer.gov (2015)http://www.cancer.gov/types/myeloma/hp/myeloma-treatment-pdq#link/_40_toc Accessed on September, 20th 2015
- ↑ Rajkumar, S. Vincent, Meletios A. Dimopoulos, Antonio Palumbo, Joan Blade, Giampaolo Merlini, María-Victoria Mateos, Shaji Kumar et al. “International Myeloma Working Group updated criteria for the diagnosis of multiple myeloma.” The Lancet Oncology 15, no. 12 (2014): e538-e548
- ↑ About multiple myeloma. University of California San Francisco (2015)http://cancer.ucsf.edu/research/multiple-myeloma/ Accessed on September, 18 2015
- ↑ Greipp PR, San Miguel J, Fonseca R, Avet-Loiseau H, Jacobson JL, Rasmussen E, Crowley J, Durie BMG. Development of an international prognostic index (IPI) for myeloma: report of the international myeloma working group. Hematology Journal 2003;4:S42. NLM ID 100965523.
- ↑ About multiple myeloma. University of California San Francisco (2015)http://cancer.ucsf.edu/research/multiple-myeloma/ Accessed on September, 18 2015
- ↑ Durie BG, Salmon SE (1975). “A clinical staging system for multiple myeloma. Correlation of measured myeloma cell mass with presenting clinical features, response to treatment, and survival”. Cancer. 36 (3): 842–54. PMID 1182674.
- ↑ About multiple myeloma. University of California San Francisco (2015)http://cancer.ucsf.edu/research/multiple-myeloma/ Accessed on September, 18 2015
- ↑ International Myeloma Working Group. Criteria for the classification of monoclonal gammopathies, multiple myeloma and related disorders: a report of the International Myeloma Working Group. Br J Haematol 2003;121:749-57. PMID 12780789.
- ↑ Shortt CP, Gleeson TG, Breen KA, McHugh J, O’Connell MJ, O’Gorman PJ; et al. (2009). “Whole-Body MRI versus PET in assessment of multiple myeloma disease activity”. AJR Am J Roentgenol. 192 (4): 980–6. doi:10.2214/AJR.08.1633. PMID 19304704.
- ↑ Agarwal A, Chirindel A, Shah BA, Subramaniam RM (2013). “Evolving role of FDG PET/CT in multiple myeloma imaging and management”. AJR Am J Roentgenol. 200 (4): 884–90. doi:10.2214/AJR.12.9653. PMID 23521465.
Historical Perspective
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1] Associate Editor(s)-in-Chief: Haytham Allaham, M.D. [2] Shyam Patel [3]
Overview
Multiple myeloma was first discovered by Dr. Samuel Solly, a surgeon working in St.Thomas hospital in London in 1844.[1]The Bence Jones protein was first discovered by Dr. Henry Bence Jones and found to be associated with multiple myeloma in 1850; And the term “Bence Jones protein” was first used by Fleischer in 1880.[2]
Historical Perspective
- In 1844, Dr. Samuel Solly reported the first case of multiple myeloma. He was a a surgeon working in St. Thomas Hospital at London.[3][4] Dr. Solly treated patients with rhubard and orange peel.
- In 1845, abnormal urinary proteins were found to be associated with multiple myeloma. These were eventually coined as Bence Jones proteins. Dr. T. Watson treated patients with steel and quinine.
- In 1856, Dr. Heller described precipitation of urinary protein above a temperature of 50 degrees Celcius. This was eventually found to be the Bence Jones protein.
- In 1850, Dr. Henry Bence Jones first described the Bence Jones protein and found it to be associated with multiple myeloma.[5]
- In 1895, plasma cells were first described. It was later found that plasma cell proliferation was the cellular basis for multiple myeloma.[4]
- In 1928, Copeland and Geschickter reported the first large case series of multiple myeloma patients. They described 412 patients from 1848 to 1928 and noted that these patients had pathologic fractures, Bence Jones protein in the urine, renal dysfunction, and anemia.[4][4]
- In 1939, the monoclonal protein spike (M-spike) was described on protein electrophoresis. The M-spike was noted to be the gamma-globulin region.[4]
- In 1947, Dr. N. Alwall treated multiple myeloma patients with urethane.
- In 1956, light chains were recognized to be a component of multiple myeloma.[4]
- In the 1960s, the chemotherapy agent melphalan was shown to improve overall survival in multiple myeloma.[6]
- In 1958, Dr. N. Blokhin first used melphalan as a chemotherapy agent to treat multiple myeloma.[4]
- In 1961, the use of thalidomide was prohibited since it was found to be associated with birth defects.[6]
- In 1962, Gally and Edelman recognized that Bence Jones urinary protein and the serum immunoglobulin light chain had the same amino acid composition. The In the same year, R.E. Maas demonstrated that corticosteroids could be used to treat multiple myeloma.[4]
- In 1975, the Durie-Salmon staging system was developed.[4]
- In 1983, T.J. McElwain and R.L. Powles showed that autologous stem cell transplant could be used to treat multiple myeloma.[4]
- In the 1990s, it was shown that high-dose therapy with autologous stem cell rescue led to improved patient outcomes.[6]
- In 1999, Singhal and colleagues showed that thalidomide had a 32% response rate in a phase II clinical trial of relapsed/refractory multiple myeloma.
- In 2003, the proteasome inhibitor bortezomib was approved by the U.S. Food and Drug Administration for the treatment of multiple myeloma.
- In 2005, the International Staging System (ISS) was developed and cytogenetic classification was described.
- In 2014, the International Myeloma Working Group (IMWG) revised the diagnostic criteria for active multiple myeloma to include bone marrow [[plasma cell burden of 60% or greater, serum free light chain ratio of involved-to-uninvolved light chain of 100 or greater, and greater than 1 bony lesion on MRI measuring at least 5mm. The advent of the 2014 diagnostic criteria increased the proportion of patients diagnosed with active multiple myeloma.
References
- ↑ Moehler T, Goldschmidt H. Multiple Myeloma. Springer Science & Business Media; 2011. https://books.google.com/books?isbn=3540857729
- ↑ Ribatti D (March 2018). “A historical perspective on milestones in multiple myeloma research”. Eur. J. Haematol. 100 (3): 221–228. doi:10.1111/ejh.13003. PMID 29194778.
- ↑ Moehler T, Goldschmidt H. Multiple Myeloma. Springer Science & Business Media; 2011. https://books.google.com/books?isbn=3540857729
- ↑ 4.00 4.01 4.02 4.03 4.04 4.05 4.06 4.07 4.08 4.09 Kyle RA, Rajkumar SV (2008). “Multiple myeloma”. Blood. 111 (6): 2962–72. doi:10.1182/blood-2007-10-078022. PMC 2265446. PMID 18332230.
- ↑ Kyle RA, Steensma DP (2011). “History of multiple myeloma”. Recent Results Cancer Res. 183: 3–23. doi:10.1007/978-3-540-85772-3_1. PMID 21509678.
- ↑ 6.0 6.1 6.2 Hong J, Lee JH (2016). “Recent advances in multiple myeloma: a Korean perspective”. Korean J Intern Med. 31 (5): 820–34. doi:10.3904/kjim.2015.408. PMC 5016289. PMID 27604794.
Classification
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1] Associate Editor(s)-in-Chief: Haytham Allaham, M.D. [2] Shyam Patel [3]
Overview
Multiple myeloma can be classified into several subtypes based on the extent of organ involvement (medullary or extramedullary) and the disease clinical presentation (active symptomatic or smoldering asymptomatic).[1]
Classification
Plasma cell disorders such as multiple myeloma and its related diseases are classified according to disease burden and the extent of organ involvement, as follows:
| Disease | Diagnostic Criteria | Management Approach |
|---|---|---|
plus
plus
|
||
plus
|
Monitoring of complete blood count every 6-12 months | |
plus
|
| |
plus
|
(Please see Therapy section for details |
Multiple myeloma can be classified according to risk status. The risk stratification for multiple myeloma consists of three groups, as follows:[3][4]
| Risk group | Chromosomal Abnormalities | Frequency |
|---|---|---|
|
Standard risk |
|
75% |
|
Intermediate Risk |
|
10% |
|
High risk |
|
15%|- |
References
- ↑ Alexiou C, Kau RJ, Dietzfelbinger H, Kremer M, Spiess JC, Schratzenstaller B; et al. (1999). “Extramedullary plasmacytoma: tumor occurrence and therapeutic concepts”. Cancer. 85 (11): 2305–14. PMID 10357398.
- ↑ 2.0 2.1 2.2 Caers J, Paiva B, Zamagni E, Leleu X, Bladé J, Kristinsson SY; et al. (2018). “Diagnosis, treatment, and response assessment in solitary plasmacytoma: updated recommendations from a European Expert Panel”. J Hematol Oncol. 11 (1): 10. doi:10.1186/s13045-017-0549-1. PMC 5771205. PMID 29338789.
- ↑ Rajkumar SV (2016). “Multiple myeloma: 2016 update on diagnosis, risk-stratification, and management”. Am J Hematol. 91 (7): 719–34. doi:10.1002/ajh.24402. PMC 5291298. PMID 27291302.
- ↑ Sonneveld P, Avet-Loiseau H, Lonial S, Usmani S, Siegel D, Anderson KC; et al. (2016). “Treatment of multiple myeloma with high-risk cytogenetics: a consensus of the International Myeloma Working Group”. Blood. 127 (24): 2955–62. doi:10.1182/blood-2016-01-631200. PMC 4920674. PMID 27002115.
Pathophysiology
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1] Associate Editor(s)-in-Chief: Hannan Javed, M.D.[2]; Haytham Allaham, M.D. [3]; Shyam Patel [4]
Overview
Multiple myeloma, a disorder of clonal late B-cells, arises from post-germinal center plasma cells that are normally involved in production of human immunoglobulins.[1][2][3] Although the exact pathogenesis and the stage at which myeloma cells arise from post-germinal B-cells remain unclear, a variety of factors have been implicated in pathogenesis of multiple myeloma. Of these, chromosomal abnormalities are thought to be the most important. It has been suggested that all cases of multiple myeloma pass through MGUS. Renal involvement by multiple myeloma is catergorized into three entities: light chain cast nephropathy, monoclonal immunoglobulin deposition disease, and amyloidosis. Osseous involvement by multiple myeloma is based on cytokine and cellular interactions that lead to bone breakdown. On microscopic histopathological analysis, abundant eosinophilic cytoplasm, eccentrically placed nucleus, and Russell bodies are characteristic findings of multiple myeloma.[4]
Pathophysiology
Normal physiology and development of plasma cells
- Plasma cells are terminally differentiated B-cells which function to produce immunoglobulins. plasma cells arise from B lymphocytes through a series of events. These events take place in bone marrow and secondary lymphoid tissues.
- These events include immunoglobulin heavy-chain (IgH) VDJ gene rearrangement, migration into lymphoid tissues, somatic hypermutation (SMH) in the IgH and light-chain genes, antigen selection, switch in Ig class from IgM to IgG, IgA, IgD, or IgE, migration back to bone marrow and terminal differentiation into plasma cells.[5] [6][7]
Stem cells → Pre-B cells → Immature B-cells → Mature B-cells (naïve) → Activated B-cells → Memory B-cells and Plasmablasts → Plasma cells
- During these events, B cells express variety of surface markers which may be used to denote their developmental stage such as CD19, CD20, CD27, CD38, CD10, CD138. These markers and IgH chain gene sequences are important to define the nature of myeloma cells.[5][6][7]
- Plasma cells secrete antibodies which function in humoral immunity.[5][6] [7]
- Plasma cells are typically polyclonal and can respond to a variety of antigens, which helps combat infections. Under normal circumstances, there is no monoclonality amongst the plasma cell population in a person. These plasma cells are functionally intact in their ability to contribute to humoral immunity.[5][6][7]
- Transcription factors such as interferon regulatory factor 4 (IRF4), BCL6, B-lymphocyte-induced maturation protein 1 (BLIMP1, also known as PRDM1), paired box gene 5 (PAX5) and X box binding protein 1 (XBP1) play an important role in differentiation and survival of plasma cells.[8][9][10]
Interferon regulatory factor 4 (IRF4) → Down-regulation of BCL6 → Up-regulation of B-lymphocyte-induced maturation protein 1 (BLIMP1) → Down-regulation of paired box gene 5 (PAX5) and Up-regulation of X box binding protein 1 (XBP1).[11][12][13]
For more information on plasma cells, click here.
Normal physiology and development of Immunoglobulins
- Immunoglobulins (also known as Antibodies) are proteins that are found in blood or other bodily fluids of vertebrates, and are used by the immune system to identify and neutralize foreign objects, such as bacteria and viruses.
- They are made of a few basic structural units called chains; each antibody has two large heavy chains H and two small light chains L. There are several different types of antibody heavy chains, and several different kinds of antibodies, which are grouped into different isotypes based on which heavy chain they possess.[14][15]
- Five different antibody isotypes are known in mammals, which perform different roles, and help direct the appropriate immune response for each different type of foreign object they encounter.[14][15]
- Class switch recombination (CSR), a region specific deletion recombination process, generates different immunoglobulin (Ig) isotypes by replacing one switch region with another. This process leads to enhanced functionality of immunoglobulins.[16][17]
- Class switch recombination (CSR), just like somatic hypermutation (SMH), requires the expression of activation-induced deaminase (AID) and both are dependent on creation of double-stranded DNA breaks (DSB) in the Ig loci.[18][19][20]
For more information on immunoglobulins, click here.
Pathogenesis
The pathogenesis of multiple myeloma is complex and probably is a result of multiple and multi-step oncogenic events such as hyperdiploidy and deregulation of cyclin D1, and interaction of myeloma cells with marrow environment. Recently it has been suggested that all cases of multiple myeloma pass through an MGUS phase. The events surrounding the progression of MGUS into multiple myeloma are not well-defined but environmental and genetic factors have been proposed to have an association. A brief description of events thought to play a role in pathogenesis of multiple myeloma is given here.
Biology of myeloma cells
- Myeloma cells are malignant plasma cells which exhibit the morphology of mature plasma cells or plasmablasts. Majority of these cells seem to be mature, differentiated and quiescent, appearing to be without long-term proliferative potential.[21][22]
- Cells with similar morphology to mature B-cells but with immunoglobulin gene sequences and idiotype similar to myeloma cells have also been found in myeloma patients, both in bone marrow and the peripheral blood.[23][22]
- Current hypothesis is the presence of functional heterogeneity in myeloma cells with only a minor group of specialized myeloma cells exhibiting clonogenic growth potential. Although studies have shown the presence of myeloma cells sub-populations with distinct phenotypes and functionality in multiple myeloma such as presence of CD138+ and CD138− sub-populations, the phenotype of these so-called clonogenic cells is yet to be determined. [23][22][24]
- Myeloma cells express surface markers associated with plasma cells such as CD138, natural killer (NK) cells such as CD56/NCAM, T cells such as CD28, and sometimes the pan-B-cell marker CD20. Presence of CD19 and CD20 on sub-population of myeloma cells may suggest either early-lineage precursor for myeloma cells or possible de-differentiation of myeloma cells.[5][22][25][26][27]
- Myeloma cells show complex chromosomal abnormalities and mutations. Studies have demonstrated the presence of translocations in up to 75% of the myeloma cases.[5]
Environmental and hereditary factors
- The Key environmental and hereditary factors thought to confer a greater risk of developing multiple myeloma or play a part in pathogenesis are summarized in the table below.[8][28][29][30][31][32][33][34][35][36][37]
| Environmental and hereditary risk factors |
|---|
|
| * Likely influenced by environmental and behavioral confounding factors. |
Chromosomal aberrations
- Two major sets of chromosomal abnormalities seen in multiple myeloma are translocations with extensive IgH rearrangements and numerical aberrations, either trisomy or monosomy.[8][5]
Translocations
- Majority of translocations in multiple myeloma take place through class switch recombination (CSR). But few may occur through DH–JH recombination, possibly in early stages of B-cell development such as pre-B cell stage.[8][38]
- Majority of these translocations put oncogenes such as cyclin D1 (CCND1), CCND3, fibroblast growth factor receptor 3 (FGFR3), multiple myeloma SET domain (MMSET; also known as WHSC1), MAF and MAFB under the influence of enhancers present at Ig loci. .[5][8][39][40]
- These translocations cause over-expression of these oncogenes that in turn leads to dysregulation of cell-cycle such as increased cell survival, growth, progression and DNA repair. One of the key abnormality being the increased G1/S transition during the cell-cycle.[8][41]
- Many other translocations may occur in later phases of multiple myeloma. One important example is translocation of MYC, an oncogene that encodes transcription factors.[8][42][43]
Hyperdiploidy
- Gain of the odd numbered chromosomes including 3, 5, 7, 9, 11, 15, 19 and 21 is the other major abnormality observed in multiple myeloma.[5] [8]
- The mechanism of this gain phenomena is not well understood, one hypothesis being the gain of chromosome during single mitosis.[8]
| Chromosomal aberrations in multiple myeloma (MM) | ||
|---|---|---|
| Chromosomal Abnormality | Chromosome(s)/Protein(s) affected | Consequence |
| Trisomies | Odd-numbered chromosomes with the exception of chromosomes 1, 13, and 21 | |
| t(11;14)(q13;q32)
t(6;14q)(p21;32) t(12;14)(p13;q32) |
Cyclin D1
Cyclin D3 Cyclin D2 |
Over-expression; cell cycle dysregulation |
| t(4;14)(p16;q32) | FGFR3 or MMSET | Over-expression and activation; multiple myeloma cell proliferation/apoptosis prevention MMSET probably linked to crucial transforming event |
| t(14;16)(q32;q23)
t(14;20)(q32;q11) t(8;14)(q24;q32) |
c-MAF | Over-expression; involvement in IL-4 regulation |
| del 17p13 | p53 | Cell-cycle dysregulation/apoptosis |
| Monosomy 14 | Chromosome 14 | |
| Chromosome 13 deletion and monosomy | Chromosome 13 | |
| Gain(1q21) | Chromosome 1 | |
| Abbreviations used: FGFR3:fibroblast growth factor receptor 3; MMSET:multiple myeloma SET domain; MAF:musculoaponeurotic fibrosarcoma oncogene homolog. | ||
Mutations in myeloma
- Studies have demonstrated the presence of approximately 35 mutations per sample in multiple myeloma. These mutations cause loss of tumor suppressors and NFKB alterations.[8]
Tumor suppressors
- These mutations result in cell-cycle dysregulation with an increase in G1/S transition. Some of these mutations are mentioned in the table below.[8][44][45][46]
- The loss of tumor suppressors allows the cells to survive and grow without check points.
| Tumor suppressor genes commonly affected in myeloma |
|---|
| FAM46C (family with sequence similarity 46, member C) |
| DIS3 (Exosome complex exonuclease RRP44) |
| CYLD (Cylindromatosis) |
| Baculoviral IAP repeat containing protein 2 (BIRC2; also known as cIAP1) |
| BIRC3 (Baculoviral IAP repeat containing protein 3) |
| tumor necrosis factor receptor associated factor 3 (TRAF3) |
| CDKN2C |
| CDKN2A |
| TP53 |
NFKB alterations
- NF-κB (nuclear factor kappa-light-chain-enhancer of activated B cells) is a protein complex which regulates DNA transcription, production of cytokine and cell survival. NF-κB plays a key role in generating cellular responses to stimuli such as stress, free radicals, heavy metals, ultraviolet radiations, and foreign antigens. NF-κB is also crucial in response of the immune system towards infections.[47][48][23]
- Deregulated NF-κB system leads to increased growth factors and cytokines such as IL-6 which promote growth and survival in myeloma cells.[23]
- Mutations in multiple genes can cause activation of NF-κB system which in turn plays a role in pathogenesis of multiple myeloma. Some of these mutations, that have been documented in genes regulating NF-κB pathway, are mentioned below.[49][50]
| Genes mutated associated with canonical signaling | Genes mutated associated with non-canonical signaling |
|---|---|
| TLR4
TNFRSF1A IKBKB IKBIP |
MAP3K14 |
Epigenetic changes in multiple myeloma
- Epigenetic events such as methylation of DNA and histones play an important role in pathogenesis of multiple myeloma.
- Of these events, the most notable is the global hypomethylation and gene-specific hypermethylation that takes place during progression of MGUS to myeloma.[8]
- A subset of patients with t(4;14) translocation show prominent DNA methylation changes that lead to MMSET overexpression.[8][39]
- Other dysregulations related to epigenetics in multiple myeloma may effect KDM6A (UTX), a histone demethylase, mixed lineage leukemia (MLL) protein, lysine demethylase 6B (KDM6B) and homeobox A9 (HOXA9).[8][51]
Bone marrow microenvironment and multiple myeloma
- Bone marrow microenvironment comprises of bone marrow stromal cells (BMSCs), extracellular matrix (ECM) proteins such as collagen, fibronectin and laminin, and the extracellular fluid containing cytokines and growth factors. This microenvironment is conducive to normal hematopoiesis but this also helps myeloma cells to have increased replication activity and anti-apoptotic resistance.[5][8][52]
- One of the key processes is the interaction and adherence of myeloma cells with bone marrow stromal cells (BMSCs) and extracellular matrix proteins through cellular adhesion molecules (CAMs) such as CD44 (H-CAM), CD56 (N-CAM), members of the CD49 integrin family (including very-late antigen VLA-4 and VLA-5), lymphocyte function-associated antigen-1, syndecan-1, and selectin.[5][8][53]
- This interaction leads to activation of p42/44 mitogen-activated protein kinase, and nuclear factor κB (NF-κB) which cause increased adhesion molecules, both on myeloma cells and bone marrow stromal cells. These events ultimately lead to increased production of cytokines. Of these cytokines IL-6, TNFα, BAFF, IGF and HGF are of particular importance.[5][8][54][55][56]
- These events cause localization of tumor cells in bone marrow, increased proliferation and survival, and resistance to apoptosis and chemotherapy. Bone marrow niche thus plays a crucial role in pathogenesis of multiple myeloma.[5][8][54][55][56]
- Decreased cellular adhesion molecules such as CD56 and chemokine receptors such as CXCR4 on myeloma cells lead to decreased adhesion to bone marrow stromal cells and immune evasion, allowing the myeloma cells to spread outside the bone marrow.[57][58]
Cytokines in multiple myeloma pathogenesis
- A variety of cytokines have been implicated in pathogenesis of multiple myeloma. Some of the relevant cytokines, their mechanisms and effects on tumor cells have been summarized in the table below.[5][59][60][60][61][62][63][64][65][66][67][68]
| Cytokines | Mechanism | Effects on tumor cells and pathogenesis |
|---|---|---|
| Interleukin 6 | Activates signal transduction pathways |
|
| Tumor necrosis factor α
TNF-α |
Activation of NF-κB
Activation of the MAPK pathways |
|
| B-cell activating factor
(BAFF) |
Activation of NF-κB |
|
| Insulin-like growth factor-1
(IGF-1) |
Activation of PI3K/Akt |
|
| Vascular endothelial growth factor
(VEGF) |
VEGF Receptor activation |
|
| Interleukin 17
(IL-17) |
Interleukin 17 receptors activation |
Pathophysiology of renal involvement
Abnormal antibody fragments are produced in multiple myeloma and are deposited in various organs, such as the kidneys. There are three major forms of renal damage in patients with multiple myeloma.
- Cast nephropathy: End-organ damage to the kidneys is typically due to light chain cast nephropathy. The pathophysiology of this type of renal involvement is based on light chain deposition in the renal tubules, which results in obstruction. Free light chains are readily filtered at the glomerulus and are reabsorbed in the proximal tubule of the nephron. This reabsorption occurs via the megalin-cubulin transport system.[69] In patients with multiple myeloma, there is excess production of free light chains, and the ability of the nephron to resorb light chains in the proximal tubule cannot meet the demands of the freely filtered light chains. This results in excess secretion of free light chains in the urine (known as Bence-Jones protein). Eosinophilic proteinaceous casts and crystalline structures can be seen. Cast formation occurs in the tubules due to excess abundance of free light chains that interact with Tamm-Horsfall proteins in the thick ascending loop of Henle.[69] Tubular obstruction ensues, triggering local inflammation which results in interstitial nephritis and fibrosis.[69] The onset of cast nephropathy can be very quick, requiring prompt treatment. Risk factors for development of cast nephropathy include monoclonal immunoglobulin secretion of >10 g/day, sepsis, and volume depletion.[70] Patients can also develop Fanconi syndrome, resulting in dysfunctional reabsorption ability by the proximal tubule, and type II renal tubular acidosis.
- Monoclonal immunoglobulin deposition disease (MIDD): In this subtype of renal involvement by multiple myeloma, the initial pathophysiological process is filtration of monoclonal immunoglobulins and subsequent deposition of immunoglobulins along the tubular or glomerular basement membrane.[70] Deposits of immunoglobulin can have a similar appearance as Kimmelstein-Wilson lesions (seen in diabetes). The immunoglobulins can appear fibroblast-like.
- Light chain amyloidosis: The pathophysiology of renal involvement by light chain amyloidosis begins with beta-pleated sheet formation in the tubules or glomeruli. Beta-pleated sheets form as a result of electrostatic interactions between heparan sulfate proteoglycan and amyloid proteins. Amyloid fibrils usually consist of immunoglobulin light chains (usually lambda light chain) and deposit in the basement membrane. The size of the fibrils vary from 7 to 10 nanometers. A diagnosis of this type of renal involvement is made by the visualization of apple green birefringence upon Congo red staining of the renal specimen.[70] It is frequently associated with nephrotic range proteinuria, in which greater than 3 grams of protein is excreted daily.
Pathophysiology of osseous involvement
Bone disease characterized by progressive osteolytic bone lesions leading to bone resorption is hallmark of multiple myeloma. Abnormal bone remodeling is thought to be the cause. It has been reported that up to 80% of the patients have characteristic osteolytic bone lesions at presentation and 60% of the patients with multiple myeloma will develop at least one pathological fracture at some stage.The pathophysiology of bony involvement in multiple myeloma is complex and is briefly described here..[71][72][73]
Increased osteoclastic activity
Osteoclasts are large, multinucleated cells of monocyte–macrophage lineage and play a crucial role in bone remodeling. Myeloma cells, in addition to their direct interaction with other cells, produce and release a number of factors which promote osteoclast differentiation and activation. Some of these factors and interactions have been described below in the tables.[71][74][75]
| Cell-cell interactions | Consequences |
|---|---|
| Myeloma cells to bone marrow stromal cells |
|
| Alpha4-beta1 integrin to vascular cell adhesion molecule 1 (VCAM-1) interaction |
|
| Myeloma cells to osteoblasts | Decreased production of OPG |
| Myeloma cells to osteoclasts | Direct adherence of myeloma cells to osteoclasts may result in
|
| Myeloma cells to immune cells | Increased production of cytokines, chemokines and factors associated with growth,
survival and migration. |
.
| Molecular pathways and factors associated with increased osteoclastic activity | Association with multiple myeloma |
|---|---|
| RANK/RANKL pathway
Binding of RANKL to RANK → fusion of osteoclast precursors into multinucleated cells → mature osteoclasts → ↑ bone resorption Osteoprotegerin (OPG) is a soluble decoy receptor for RANKL → ↓ binding of RANKL to RANK → ↓ bone resorption
|
Myeloma cells lead to increased RANKL and decreased OPG causing bone resorption and destruction. RANKL/OPG ratio is an idependent
prognostic factor in multiple myeloma
|
| Notch pathway
Binding of Notch receptors to its ligands → ↑ RANKL production → ↑ bone resorption
|
Myeloma cells express Notch 1,2,3 and their ligands Jagged 1,2 and Delta-like 1,3,4. This pathway, in addition to bone resorption, may also be involved in metastasis of myeloma cells by increasing expression of adhesion molecules, migratory chemokines, and angiogenetic factors, and disruption of the immune surveillance.
|
CCL-3 (MIP-1α)/CCL-20
|
|
| Activin A
Binds to type II transmembrane serine/threonine kinase receptor (ActRIIA/B) → recruitment and phosphorylation the type I receptor (ActRI, also called activin receptor-like kinase 4 (ALK4) receptor) → heterodimer formation → activation of the Smad signaling cascade → translocation of Smad2/3/4 complex in the nucleus → action as transcriptional factor → RANK expression and activation of NF-κB pathway → increased osteoclast differentiation |
|
Osteopontin
|
|
Interleukin 3 (IL-3)
|
|
Vascular endothelial growth factor (VEGF)
|
|
Interleukin 6 (IL-6)
|
|
Interleukin 17 (IL-17)
|
|
| B cell-activating factor (BAFF)
Binding to its receptor → activation of NF-κB → ↑ MM cell survival
|
|
| Bruton’s tyrosine kinase (BTK)
Osteoclast precursors with CXC chemokine receptor type 4 (CXCR4) and Bruton’s tyrosine kinase (BTK) expression → migration towards stromal cell-derived factor-1α (SDF-1α) → ↑ activation of Bruton’s tyrosine kinase (BTK) in myeloma cells.
|
|
| Stromal cell-derived factor-1α (SDF-1α)
Osteoclast precursors with CXC chemokine receptor type 4 (CXCR4) and Bruton’s tyrosine kinase (BTK) expression → migration towards stromal cell-derived factor-1α (SDF-1α) → ↑ activation of Bruton’s tyrosine kinase (BTK) in myeloma cells.
|
|
Annexin II (Annexin A2)
|
|
PU.1
|
Decreased osteoblast activity
Inhibition of osteoblasts leading to decreased bone formation is now considered to be a critical event in bone disease in multiple myeloma. This inhibition leads to bone loss as well as inability to repair the osteoytic lesions caused by increased osteoclastic activity. Several pathways and factors have been associated with suppressed osteoblastic activity. Some of them are mentioned below in the table.[71][74][75]
| Molecular pathways and factors associated with osteoblastic activity | Association with multiple myeloma |
|---|---|
Wingless and integration-1 (Wnt) signaling
Activation of Wnt pathway → binding of Wnt ligands to Wnt co-receptors LRP5/6 and one trans-membrane receptor of the FDZ family → formation of DVL–Axin–FRAT1–GSK-3β complex → translocation of β-catenin from cytoplasm to nucleus → activation of T cell factor/lymphoid enhancer factor (TCF/LEF) transcription factors → ↑ bone formation and ↓ bone resorption Formation of WNT ligand–receptor tyrosine kinase-like orphan receptor 2 (ROR2) or the receptor-like tyrosine kinase (RYK)–FZD–DVL complex → activation of one of these 3 pathways: 1) Disheveled-associated activator of morphogenesis 1 (DAAM1)–RHO–RHO-associated kinase (ROCK) pathway; 2) RAC–Jun kinase (JNK)–RUNX2 pathway; WNT–Ca2+ pathway
|
Dickkopf 1 (Dkk-1)
Secreted frizzled related protein-2 (sFRP-2)
Runt-related transcription factor 2 (Runx2)/corebinding factor runt domain alpha subunit 1 (CBFA1)
|
| EphrinB2/EphB4 signaling pathway
Binding of ligands called ephrins (Eph receptor-interacting proteins) → activation of two cascades: 1) the forward signaling → ↑ osteoblast differentiation by downregulating RhoA; 2) the reverse signaling → ↓ osteoclast differentiation by ↓ Fos and Nfatc1 transcription
|
Multiple myeloma patients have decreased expression of both EphrinB2 and EphB4 in bone marrow stromal cells. |
Transforming growth factor-β (TGF-β)
|
Inhibition of Transforming Growth Factor-β have been shown to prevent myeloma cells to block osteoblastic differentiation. |
| Bone morphogenetic proteins (BMPs) | Myeloma cells express negative regulators of bone morphogenetic proteins that result in decreased activity of these proteins which in turn causes decreased osteoblastogenesis. |
Hepatocyte growth factor (HGF)
|
|
Interleukin 3 (IL-3)
|
Elevated levels had been demonstrated in bone marrow of myeloma patients. |
Interleukin 7 (IL-7)
|
|
Growth factor independence-1 (GFI1)
|
Bone marrow stromal cells (BMSCs) in myeloma patients have been shown to over-express growth factor independence-1 (GFI1). |
Tissue necrosis factor-α (TNF-α)
|
Tissue necrosis factor-α (TNF-α) levels are increased in multiple myeloma and it is thought to play a complex role in pathogenesis of multiple myeloma. |
| Adiponectin
adipocyte-derived hormone thought to act on osteoblasts and osteoclasts |
Increased adiponectin secretion through pharmacologic interventions have shown to decrease osteolytic lesions in myeloma. |
Renal involvement in multiple myeloma
Renal involvement is common in multiple myeloma as up to 50% of the patients go on to develop kidney disease at some point during the disease course. Half of these patients recover kidney function while the rest of them develop chronic kidney dysfunction. The causes of renal involvement in multiple myeloma are multiple and diverse. They can broadly be classified into Ig dependent and Ig independent mechanisms. Some of them have been discussed below in the table and then described briefly.[76][77][70]
| Ig-dependent renal injury | Ig-independent renal injury | ||
|---|---|---|---|
| Cause | Notes | Cause | Notes |
| Cast nephropathy (myeloma kidney) | Risk factors
|
Volume depletion | May cause
|
| Monoclonal Ig deposition disease | Sepsis | May cause
| |
| Light chain amyloidosis (AL) |
|
Hypercalcemia | May result in acute kidney injury directly or contribute to cast nephropathy |
| Glomerulonephritis | Following types have been demonstrated
|
Tumor lysis syndrome | Caused by uric acid or phosphate nephropathy |
| Tubulointerstitial nephritis | May be caused be either Ig-dependent or Ig-independent mechanisms | Direct parenchymal invasion by plasma cells | Rare cause. Association with advanced or aggressive multiple myeloma |
| Minimal change disease | Often with albuminuria and light chain proteinuria | Pyelonephritis | Rare cause. Pathogenesis is typically multifactorial and may include:
|
| Hyperviscosity syndrome | Seen primarily in cases of IgA, IgG3, or IgM myeloma | Medication toxicity | Following drugs may cause kidney injury:
|
| Henoch–Scholein purpura/IgA nephropathy | Associated with IgA myeloma | ||
| Immunotactoid glomerulopathy (and possibly fibrillary GN) | Rare conditions. The association between fibrillary disease and paraproteins is is not understood at this point. | ||
| Thrombotic microangiopathy (TMA) | Endothelial injury caused by paraprotein leads to thrombotic microangiopathy. | ||
| Membranous glomerulopathy | |||
Cast nephropathy (myeloma kidney)
- Normally circulating monoclonal free light chains are relatively freely filtered through the glomerulus and a receptor-mediated process leads to their endocytosis in proximal tubule cells. They bind to the tandem scavenger receptor system cubilin/megalin, followed by endocytosis through the clathrin-dependent endosomal/lysosomal pathway. They are then degraded within lysosomes.
- In multiple myeloma, myeloma cells produce excess of monoclonal free light chains that overwhelms the capacity of the proximal tubule cells to absorb and catabolize them. This leads to large amounts of monoclonal free light chains reaching distal renal tubules.
- In distal renal tubules, they interact with Tamm-Horsfall protein (uromodulin), a glycoprotein produced in the medullary thick ascending limb of the loop of Henle in kidneys. This interaction leads to formation of myeloma casts.
- These casts block the glomerular flow, compromising renal function and may lead to proximal tubular atrophy. This may also contribute to interstitial fibrosis.
- This blockage leads to increased luminal pressure, resulting in decreased blood flow and causing further renal injury.
- The excessive amounts of monoclonal free light chains being absorbed in proximal renal tubules leads to induction of apoptosis and DNA damage in proximal renal tubules.
- Free light chains also leads to increased pro-inflammatory cytokines such as IL-6, macrophage chemoattractant protein-1 (MCP-1), and tumor necrosis factor α (TNFα) through transcription factors nuclear factor kappa B (NFκB) and mitogen-activated protein kinases.
- All these events leads to kidney injury and inability of renal cells to repair the injury. On histopathological studies, chronic tubulointerstitial nephropathy with marked tubular atrophy, laminated casts in the tubules, and interstitial fibrosis may be observed.
| Factors associated with increased risk
of AKI or CKD in multiple myeloma |
Mechanism of injury |
|---|---|
| Volume depletion | Increased FLC concentration
Decreased GFR Pre-renal azotemia |
| Hypercalcemia | Renal vasoconstriction
Decreased GFR |
| Iodinated contrast media | Nephrotoxicity |
| Nonsteroidal anti-inflammatory drugs | Renal vasoconstriction
Decreased GFR |
| Diuretics | Increased sodium chloride concentration
Increased cast formation |
| Aminoglycosides | Renal vasoconstriction
Decreased GFR |
| Hyperuricemia | |
| Comorbidities such as chronic kidney disease, diabetes, aging, hypertension, and cardiovascular disease. | |
Hypercalcemia
- Hypercalcemia in multiple myeloma primarily results from increased osteoclastic bone resorption. It is the second most common cause of renal injury in myeloma patients.
- Hypercalcemia leads to intra-tubular calcium deposition and vasoconstriction in renal vasculature. The resultant decrease in GFR not only causes renal injury by itself but also favors cast formation.
- By impairing renal concentrating ability through resistance to anti-diuretic hormone, it may also cause nephrogenic diabetes insipidus. Polyuria may develop, leading to hypovolemia. Net effect is decreased GFR, concentrated urine, reduced urine flow, and pre-renal azotemia.
Light-chain glomerulopathy
- Deposition of immunoglobulins either in the form of amyloid or non-amyloid, typically resulting in non-selective proteinuria.
- Amyloid deposits are fibrillar structures, consist of variable region fragments of the light chain, and are seen primarily within the glomeruli.
- Some patients may have predominant vascular amyloid deposits rather than glomerular deposits and present with renal failure instead of nephrotic syndrome.
Light chain deposition disease (LCDD)
- Non-fibrillar, granular deposits are topically observed in mesangial area along with thickening of basement membrane which resembles type II membranoproliferative glomerulonephritis or diabetic glomerulopathy. The light chain deposits may also be observed in renal vasculature in addition to mesangial area.
- Typical clinical picture is that of nephrotic syndrome but renal impairment is more severe with almost all patients developing renal failure.
Immune dysfunction in multiple myeloma
- Immunodeficiency is an important characteristic of multiple myeloma and is thought to associated with increased risk for infections, and affects disease progression and response to treatment.[5][78]
- The typical clinical picture is that of global immunosuppression. The interaction between myeloma cells and bone marrow stromal cells and cytokines produced as a result of this interaction are thought to play a key role.[5][78][79][80]
- Following abnormalities have been demonstrated in myeloma patients:[79][81][80]
- Decreased numbers of natural killer cells, B-cells, and memory T cells
- Decreased non-myeloma immunoglobulins
- Decreased expression of cell-surface markers on CD4+ and CD8+ T cells such as CD28 and CD152. These markers are associated with cell-signaling.
- Abnormal signal transduction in T-cells
- Abnormalities in cytokine production
- Abnormalities in antibodies response and production
- Aberrations in B-cells maturation
- Defects in natural killer cells and antigen presenting cells
Gross Pathology
-
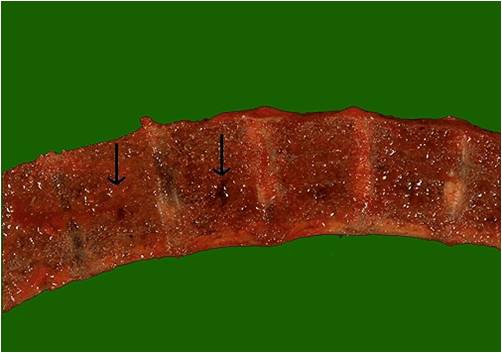 Vertebrae in multiple myeloma
Vertebrae in multiple myeloma
(Image courtesy of Melih Aktan M.D.) -
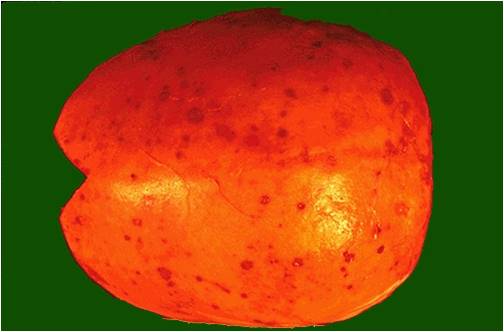 Calvarium in multiple myeloma.
Calvarium in multiple myeloma.
(Image courtesy of Melih Aktan M.D.)


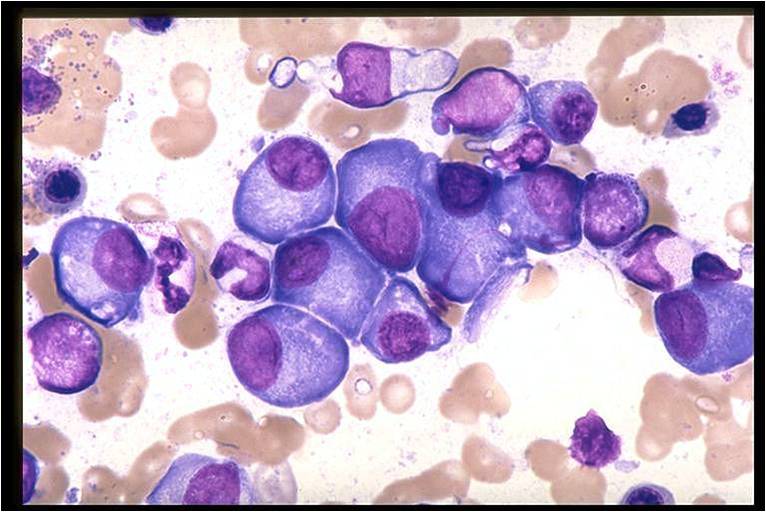
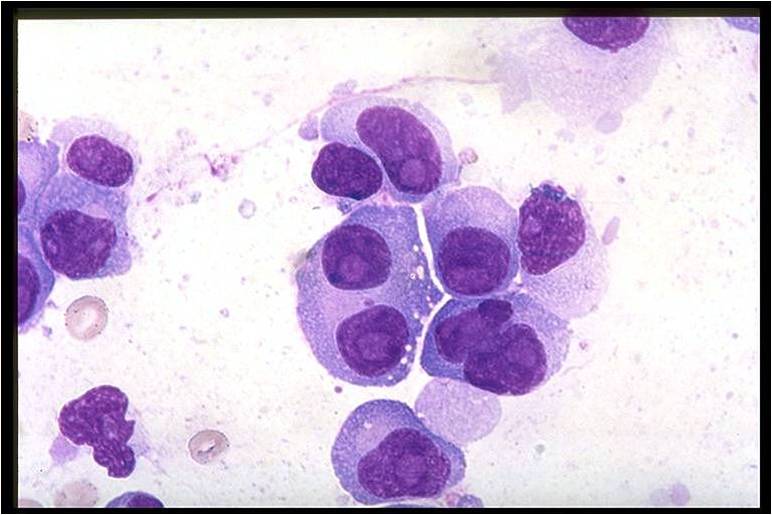
Microscopic Pathology
On microscopic histopathological analysis, multiple myeloma is characterized by the following:[4]
- Abundant eosinophilic cytoplasm
- Eccentrically placed nucleus
- Clock face morphology of the nucleus due to chromatin clumps around the edges
- Russell bodies which are eosinophilic, large (10-15 micrometres), homogenous immunoglobulin-containing inclusions
- Dutcher bodies which are PAS stain +ve intranuclear crystalline rods
- Shown below is a series of microscopic images seen in multiple myeloma:
-
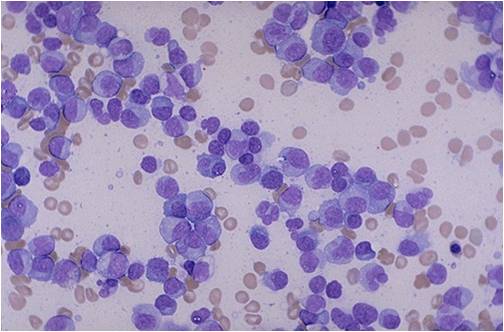 Bone marrow aspiration in multiple myeloma.
Bone marrow aspiration in multiple myeloma.
(Image courtesy of Melih Aktan M.D.) -
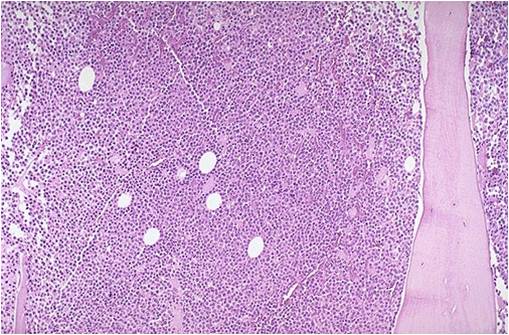 Bone marrow biopsy in multiple myeloma.
Bone marrow biopsy in multiple myeloma.
(Image courtesy of Melih Aktan M.D.) -
 Bone marrow in multiple myeloma.
Bone marrow in multiple myeloma.
(Image courtesy of Melih Aktan M.D.) -
 Bone marrow in multiple myeloma.
Bone marrow in multiple myeloma.
(Image courtesy of Melih Aktan M.D.) -
![Multiple myeloma slide with intermediate magnification[4]](https://www.wikidoc.org/images/4/40/Multiple_myeloma_intermed_mag.jpg) Multiple myeloma slide with intermediate magnification[4]
Multiple myeloma slide with intermediate magnification[4] -
![Multiple myeloma slide with high magnification[4]](https://www.wikidoc.org/images/d/d5/Multiple_myeloma.jpg) Multiple myeloma slide with high magnification[4]
Multiple myeloma slide with high magnification[4] -
![Multiple myeloma slide with russell bodies[4]](https://www.wikidoc.org/images/a/ad/Russell_bodies.jpg) Multiple myeloma slide with russell bodies[4]
Multiple myeloma slide with russell bodies[4]




![Multiple myeloma slide with intermediate magnification[4]](https://www.wikidoc.org/index.php/File%3AMultiple_myeloma_intermed_mag.jpg)
![Multiple myeloma slide with high magnification[4]](https://www.wikidoc.org/index.php/File%3AMultiple_myeloma.jpg)
![Multiple myeloma slide with russell bodies[4]](https://www.wikidoc.org/index.php/File%3ARussell_bodies.jpg)
References
- ↑ Multiple myeloma. Radiopaedia (2015)http://radiopaedia.org/articles/multiple-myeloma-1 Accessed on September, 20th 2015
- ↑ Multiple myeloma. Wikipedia (2015)https://en.wikipedia.org/wiki/Multiple_myeloma#Pathophysiology Accessed on September, 20th 2015
- ↑ Multiple myeloma. Medlineplus (2015)https://www.nlm.nih.gov/medlineplus/multiplemyeloma.html Accessed on September, 20th 2015
- ↑ 4.0 4.1 4.2 4.3 4.4 Multiple myeloma. Librepathology (2015)http://www.wikidoc.org/index.php?title=Multiple_myeloma_pathophysiology&action=edit§ion=1 Accessed on September, 20th 2015
- ↑ 5.00 5.01 5.02 5.03 5.04 5.05 5.06 5.07 5.08 5.09 5.10 5.11 5.12 5.13 5.14 5.15 Borrello I (November 2012). “Can we change the disease biology of multiple myeloma?”. Leuk. Res. 36 Suppl 1: S3–12. doi:10.1016/S0145-2126(12)70003-6. PMC 3698609. PMID 23176722.
- ↑ 6.0 6.1 6.2 6.3 Chng WJ, Glebov O, Bergsagel PL, Kuehl WM (December 2007). “Genetic events in the pathogenesis of multiple myeloma”. Best Pract Res Clin Haematol. 20 (4): 571–96. doi:10.1016/j.beha.2007.08.004. PMC 2198931. PMID 18070707.
- ↑ 7.0 7.1 7.2 7.3 Hengeveld PJ, Kersten MJ (February 2015). “B-cell activating factor in the pathophysiology of multiple myeloma: a target for therapy?”. Blood Cancer J. 5: e282. doi:10.1038/bcj.2015.3. PMC 4349256. PMID 25723853.
- ↑ 8.00 8.01 8.02 8.03 8.04 8.05 8.06 8.07 8.08 8.09 8.10 8.11 8.12 8.13 8.14 8.15 8.16 8.17 Boyle EM, Davies FE, Leleu X, Morgan GJ (April 2014). “Understanding the multiple biological aspects leading to myeloma”. Haematologica. 99 (4): 605–12. doi:10.3324/haematol.2013.097907. PMC 3971069. PMID 24688108.
- ↑ Reimold AM, Iwakoshi NN, Manis J, Vallabhajosyula P, Szomolanyi-Tsuda E, Gravallese EM, Friend D, Grusby MJ, Alt F, Glimcher LH (July 2001). “Plasma cell differentiation requires the transcription factor XBP-1”. Nature. 412 (6844): 300–7. doi:10.1038/35085509. PMID 11460154.
- ↑ Nutt SL, Taubenheim N, Hasbold J, Corcoran LM, Hodgkin PD (October 2011). “The genetic network controlling plasma cell differentiation”. Semin. Immunol. 23 (5): 341–9. doi:10.1016/j.smim.2011.08.010. PMID 21924923.
- ↑ Boyle EM, Davies FE, Leleu X, Morgan GJ (April 2014). “Understanding the multiple biological aspects leading to myeloma”. Haematologica. 99 (4): 605–12. doi:10.3324/haematol.2013.097907. PMC 3971069. PMID 24688108.
- ↑ Reimold AM, Iwakoshi NN, Manis J, Vallabhajosyula P, Szomolanyi-Tsuda E, Gravallese EM, Friend D, Grusby MJ, Alt F, Glimcher LH (July 2001). “Plasma cell differentiation requires the transcription factor XBP-1”. Nature. 412 (6844): 300–7. doi:10.1038/35085509. PMID 11460154.
- ↑ Nutt SL, Taubenheim N, Hasbold J, Corcoran LM, Hodgkin PD (October 2011). “The genetic network controlling plasma cell differentiation”. Semin. Immunol. 23 (5): 341–9. doi:10.1016/j.smim.2011.08.010. PMID 21924923.
- ↑ 14.0 14.1 Eleonora Market, F. Nina Papavasiliou (2003) V(D)J Recombination and the Evolution of the Adaptive Immune System PLoS Biology1(1): e16.
- ↑ 15.0 15.1 Litman GW, Rast JP, Shamblott MJ; et al. (1993). “Phylogenetic diversification of immunoglobulin genes and the antibody repertoire”. Mol. Biol. Evol. 10 (1): 60–72. PMID 8450761.
- ↑ Boyle EM, Davies FE, Leleu X, Morgan GJ (April 2014). “Understanding the multiple biological aspects leading to myeloma”. Haematologica. 99 (4): 605–12. doi:10.3324/haematol.2013.097907. PMC 3971069. PMID 24688108.
- ↑ Nutt SL, Taubenheim N, Hasbold J, Corcoran LM, Hodgkin PD (October 2011). “The genetic network controlling plasma cell differentiation”. Semin. Immunol. 23 (5): 341–9. doi:10.1016/j.smim.2011.08.010. PMID 21924923.
- ↑ Boyle EM, Davies FE, Leleu X, Morgan GJ (April 2014). “Understanding the multiple biological aspects leading to myeloma”. Haematologica. 99 (4): 605–12. doi:10.3324/haematol.2013.097907. PMC 3971069. PMID 24688108.
- ↑ Keim C, Kazadi D, Rothschild G, Basu U (January 2013). “Regulation of AID, the B-cell genome mutator”. Genes Dev. 27 (1): 1–17. doi:10.1101/gad.200014.112. PMC 3553278. PMID 23307864.
- ↑ González D, van der Burg M, García-Sanz R, Fenton JA, Langerak AW, González M, van Dongen JJ, San Miguel JF, Morgan GJ (November 2007). “Immunoglobulin gene rearrangements and the pathogenesis of multiple myeloma”. Blood. 110 (9): 3112–21. doi:10.1182/blood-2007-02-069625. PMID 17634408.
- ↑ Invalid
<ref>tag; no text was provided for refs namedpmid231767222 - ↑ 22.0 22.1 22.2 22.3 Matsui W, Huff CA, Wang Q, Malehorn MT, Barber J, Tanhehco Y, Smith BD, Civin CI, Jones RJ (March 2004). “Characterization of clonogenic multiple myeloma cells”. Blood. 103 (6): 2332–6. doi:10.1182/blood-2003-09-3064. PMC 3311914. PMID 14630803.
- ↑ 23.0 23.1 23.2 23.3 Tian B, Brasier AR (2003). “Identification of a nuclear factor kappa B-dependent gene network”. Recent Prog. Horm. Res. 58: 95–130. PMID 12795416.
- ↑ Huff CA, Matsui W (June 2008). “Multiple myeloma cancer stem cells”. J. Clin. Oncol. 26 (17): 2895–900. doi:10.1200/JCO.2007.15.8428. PMC 2610256. PMID 18539970.
- ↑ Bataille R, Jégo G, Robillard N, Barillé-Nion S, Harousseau JL, Moreau P, Amiot M, Pellat-Deceunynck C (September 2006). “The phenotype of normal, reactive and malignant plasma cells. Identification of “many and multiple myelomas” and of new targets for myeloma therapy”. Haematologica. 91 (9): 1234–40. PMID 16956823.
- ↑ Grogan TM, Durie BG, Lomen C, Spier C, Wirt DP, Nagle R, Wilson GS, Richter L, Vela E, Maxey V (October 1987). “Delineation of a novel pre-B cell component in plasma cell myeloma: immunochemical, immunophenotypic, genotypic, cytologic, cell culture, and kinetic features”. Blood. 70 (4): 932–42. PMID 3115338.
- ↑ Kiel K, Cremer FW, Rottenburger C, Kallmeyer C, Ehrbrecht E, Atzberger A, Hegenbart U, Goldschmidt H, Moos M (May 1999). “Analysis of circulating tumor cells in patients with multiple myeloma during the course of high-dose therapy with peripheral blood stem cell transplantation”. Bone Marrow Transplant. 23 (10): 1019–27. doi:10.1038/sj.bmt.1701767. PMID 10373068.
- ↑ Morgan GJ, Davies FE, Linet M (July 2002). “Myeloma aetiology and epidemiology”. Biomed. Pharmacother. 56 (5): 223–34. PMID 12199621.
- ↑ Wadhera RK, Rajkumar SV (October 2010). “Prevalence of monoclonal gammopathy of undetermined significance: a systematic review”. Mayo Clin. Proc. 85 (10): 933–42. doi:10.4065/mcp.2010.0337. PMC 2947966. PMID 20713974.
- ↑ Landgren O, Kyle RA, Pfeiffer RM, Katzmann JA, Caporaso NE, Hayes RB, Dispenzieri A, Kumar S, Clark RJ, Baris D, Hoover R, Rajkumar SV (May 2009). “Monoclonal gammopathy of undetermined significance (MGUS) consistently precedes multiple myeloma: a prospective study”. Blood. 113 (22): 5412–7. doi:10.1182/blood-2008-12-194241. PMC 2689042. PMID 19179464.
- ↑ Wang SS, Voutsinas J, Chang ET, Clarke CA, Lu Y, Ma H, West D, Lacey JV, Bernstein L (July 2013). “Anthropometric, behavioral, and female reproductive factors and risk of multiple myeloma: a pooled analysis”. Cancer Causes Control. 24 (7): 1279–89. doi:10.1007/s10552-013-0206-0. PMC 3684420. PMID 23568533.
- ↑ Grulich AE, van Leeuwen MT, Falster MO, Vajdic CM (July 2007). “Incidence of cancers in people with HIV/AIDS compared with immunosuppressed transplant recipients: a meta-analysis”. Lancet. 370 (9581): 59–67. doi:10.1016/S0140-6736(07)61050-2. PMID 17617273.
- ↑ Kachuri L, Demers PA, Blair A, Spinelli JJ, Pahwa M, McLaughlin JR, Pahwa P, Dosman JA, Harris SA (October 2013). “Multiple pesticide exposures and the risk of multiple myeloma in Canadian men”. Int. J. Cancer. 133 (8): 1846–58. doi:10.1002/ijc.28191. PMID 23564249.
- ↑ Singh J, Dudley AW, Kulig KA (December 1990). “Increased incidence of monoclonal gammopathy of undetermined significance in blacks and its age-related differences with whites on the basis of a study of 397 men and one woman in a hospital setting”. J. Lab. Clin. Med. 116 (6): 785–9. PMID 2246554.
- ↑ Kristinsson SY, Björkholm M, Goldin LR, Blimark C, Mellqvist UH, Wahlin A, Turesson I, Landgren O (November 2009). “Patterns of hematologic malignancies and solid tumors among 37,838 first-degree relatives of 13,896 patients with multiple myeloma in Sweden”. Int. J. Cancer. 125 (9): 2147–50. doi:10.1002/ijc.24514. PMC 2737604. PMID 19582882.
- ↑ Broderick P, Chubb D, Johnson DC, Weinhold N, Försti A, Lloyd A, Olver B, Ma Y, Dobbins SE, Walker BA, Davies FE, Gregory WA, Childs JA, Ross FM, Jackson GH, Neben K, Jauch A, Hoffmann P, Mühleisen TW, Nöthen MM, Moebus S, Tomlinson IP, Goldschmidt H, Hemminki K, Morgan GJ, Houlston RS (November 2011). “Common variation at 3p22.1 and 7p15.3 influences multiple myeloma risk”. Nat. Genet. 44 (1): 58–61. doi:10.1038/ng.993. PMC 5108406. PMID 22120009.
- ↑ Chubb D, Weinhold N, Broderick P, Chen B, Johnson DC, Försti A, Vijayakrishnan J, Migliorini G, Dobbins SE, Holroyd A, Hose D, Walker BA, Davies FE, Gregory WA, Jackson GH, Irving JA, Pratt G, Fegan C, Fenton JA, Neben K, Hoffmann P, Nöthen MM, Mühleisen TW, Eisele L, Ross FM, Straka C, Einsele H, Langer C, Dörner E, Allan JM, Jauch A, Morgan GJ, Hemminki K, Houlston RS, Goldschmidt H (October 2013). “Common variation at 3q26.2, 6p21.33, 17p11.2 and 22q13.1 influences multiple myeloma risk”. Nat. Genet. 45 (10): 1221–1225. doi:10.1038/ng.2733. PMC 5053356. PMID 23955597.
- ↑ Walker BA, Wardell CP, Johnson DC, Kaiser MF, Begum DB, Dahir NB, Ross FM, Davies FE, Gonzalez D, Morgan GJ (April 2013). “Characterization of IGH locus breakpoints in multiple myeloma indicates a subset of translocations appear to occur in pregerminal center B cells”. Blood. 121 (17): 3413–9. doi:10.1182/blood-2012-12-471888. PMID 23435460.
- ↑ 39.0 39.1 Chesi M, Nardini E, Brents LA, Schröck E, Ried T, Kuehl WM, Bergsagel PL (July 1997). “Frequent translocation t(4;14)(p16.3;q32.3) in multiple myeloma is associated with increased expression and activating mutations of fibroblast growth factor receptor 3”. Nat. Genet. 16 (3): 260–4. doi:10.1038/ng0797-260. PMC 3901950. PMID 9207791.
- ↑ Fonseca R, Bergsagel PL, Drach J, Shaughnessy J, Gutierrez N, Stewart AK, Morgan G, Van Ness B, Chesi M, Minvielle S, Neri A, Barlogie B, Kuehl WM, Liebisch P, Davies F, Chen-Kiang S, Durie BG, Carrasco R, Sezer O, Reiman T, Pilarski L, Avet-Loiseau H (December 2009). “International Myeloma Working Group molecular classification of multiple myeloma: spotlight review”. Leukemia. 23 (12): 2210–21. doi:10.1038/leu.2009.174. PMC 2964268. PMID 19798094.
- ↑ Brito JL, Walker B, Jenner M, Dickens NJ, Brown NJ, Ross FM, Avramidou A, Irving JA, Gonzalez D, Davies FE, Morgan GJ (January 2009). “MMSET deregulation affects cell cycle progression and adhesion regulons in t(4;14) myeloma plasma cells”. Haematologica. 94 (1): 78–86. doi:10.3324/haematol.13426. PMC 2625417. PMID 19059936.
- ↑ Shou Y, Martelli ML, Gabrea A, Qi Y, Brents LA, Roschke A, Dewald G, Kirsch IR, Bergsagel PL, Kuehl WM (January 2000). “Diverse karyotypic abnormalities of the c-myc locus associated with c-myc dysregulation and tumor progression in multiple myeloma”. Proc. Natl. Acad. Sci. U.S.A. 97 (1): 228–33. PMC 26645. PMID 10618400.
- ↑ Nobuyoshi M, Kawano M, Tanaka H, Ishikawa H, Tanabe O, Iwato K, Asaoku H, Sakai A, Kuramoto A (April 1991). “Increased expression of the c-myc gene may be related to the aggressive transformation of human myeloma cells”. Br. J. Haematol. 77 (4): 523–8. PMID 2025578.
- ↑ Walker BA, Leone PE, Chiecchio L, Dickens NJ, Jenner MW, Boyd KD, Johnson DC, Gonzalez D, Dagrada GP, Protheroe RK, Konn ZJ, Stockley DM, Gregory WM, Davies FE, Ross FM, Morgan GJ (October 2010). “A compendium of myeloma-associated chromosomal copy number abnormalities and their prognostic value”. Blood. 116 (15): e56–65. doi:10.1182/blood-2010-04-279596. PMID 20616218.
- ↑ Gonzalez-Paz N, Chng WJ, McClure RF, Blood E, Oken MM, Van Ness B, James CD, Kurtin PJ, Henderson K, Ahmann GJ, Gertz M, Lacy M, Dispenzieri A, Greipp PR, Fonseca R (February 2007). “Tumor suppressor p16 methylation in multiple myeloma: biological and clinical implications”. Blood. 109 (3): 1228–32. doi:10.1182/blood-2006-05-024661. PMID 16840723.
- ↑ Seemann S, Maurici D, Olivier M, Caron de Fromentel C, Hainaut P (2004). “The tumor suppressor gene TP53: implications for cancer management and therapy”. Crit Rev Clin Lab Sci. 41 (5–6): 551–83. doi:10.1080/10408360490504952. PMID 15603511.
- ↑ Gilmore TD (October 2006). “Introduction to NF-kappaB: players, pathways, perspectives”. Oncogene. 25 (51): 6680–4. doi:10.1038/sj.onc.1209954. PMID 17072321.
- ↑ Perkins ND (January 2007). “Integrating cell-signalling pathways with NF-kappaB and IKK function”. Nat. Rev. Mol. Cell Biol. 8 (1): 49–62. doi:10.1038/nrm2083. PMID 17183360.
- ↑ Roy P, Sarkar UA, Basak S (May 2018). “The NF-κB Activating Pathways in Multiple Myeloma”. Biomedicines. 6 (2). doi:10.3390/biomedicines6020059. PMC 6027071. PMID 29772694.
- ↑ Chapman MA, Lawrence MS, Keats JJ, Cibulskis K, Sougnez C, Schinzel AC, Harview CL, Brunet JP, Ahmann GJ, Adli M, Anderson KC, Ardlie KG, Auclair D, Baker A, Bergsagel PL, Bernstein BE, Drier Y, Fonseca R, Gabriel SB, Hofmeister CC, Jagannath S, Jakubowiak AJ, Krishnan A, Levy J, Liefeld T, Lonial S, Mahan S, Mfuko B, Monti S, Perkins LM, Onofrio R, Pugh TJ, Rajkumar SV, Ramos AH, Siegel DS, Sivachenko A, Stewart AK, Trudel S, Vij R, Voet D, Winckler W, Zimmerman T, Carpten J, Trent J, Hahn WC, Garraway LA, Meyerson M, Lander ES, Getz G, Golub TR (March 2011). “Initial genome sequencing and analysis of multiple myeloma”. Nature. 471 (7339): 467–72. doi:10.1038/nature09837. PMC 3560292. PMID 21430775.
- ↑ van Haaften G, Dalgliesh GL, Davies H, Chen L, Bignell G, Greenman C, Edkins S, Hardy C, O’Meara S, Teague J, Butler A, Hinton J, Latimer C, Andrews J, Barthorpe S, Beare D, Buck G, Campbell PJ, Cole J, Forbes S, Jia M, Jones D, Kok CY, Leroy C, Lin ML, McBride DJ, Maddison M, Maquire S, McLay K, Menzies A, Mironenko T, Mulderrig L, Mudie L, Pleasance E, Shepherd R, Smith R, Stebbings L, Stephens P, Tang G, Tarpey PS, Turner R, Turrell K, Varian J, West S, Widaa S, Wray P, Collins VP, Ichimura K, Law S, Wong J, Yuen ST, Leung SY, Tonon G, DePinho RA, Tai YT, Anderson KC, Kahnoski RJ, Massie A, Khoo SK, Teh BT, Stratton MR, Futreal PA (May 2009). “Somatic mutations of the histone H3K27 demethylase gene UTX in human cancer”. Nat. Genet. 41 (5): 521–3. doi:10.1038/ng.349. PMC 2873835. PMID 19330029.
- ↑ Mitsiades CS, Mitsiades NS, Munshi NC, Richardson PG, Anderson KC (July 2006). “The role of the bone microenvironment in the pathophysiology and therapeutic management of multiple myeloma: interplay of growth factors, their receptors and stromal interactions”. Eur. J. Cancer. 42 (11): 1564–73. doi:10.1016/j.ejca.2005.12.025. PMID 16765041.
- ↑ Teoh G, Anderson KC (February 1997). “Interaction of tumor and host cells with adhesion and extracellular matrix molecules in the development of multiple myeloma”. Hematol. Oncol. Clin. North Am. 11 (1): 27–42. PMID 9081202.
- ↑ 54.0 54.1 Chauhan D, Uchiyama H, Akbarali Y, Urashima M, Yamamoto K, Libermann TA, Anderson KC (February 1996). “Multiple myeloma cell adhesion-induced interleukin-6 expression in bone marrow stromal cells involves activation of NF-kappa B”. Blood. 87 (3): 1104–12. PMID 8562936.
- ↑ 55.0 55.1 Moreaux J, Legouffe E, Jourdan E, Quittet P, Rème T, Lugagne C, Moine P, Rossi JF, Klein B, Tarte K (April 2004). “BAFF and APRIL protect myeloma cells from apoptosis induced by interleukin 6 deprivation and dexamethasone”. Blood. 103 (8): 3148–57. doi:10.1182/blood-2003-06-1984. PMC 2387243. PMID 15070697.
- ↑ 56.0 56.1 Derksen PW, Keehnen RM, Evers LM, van Oers MH, Spaargaren M, Pals ST (February 2002). “Cell surface proteoglycan syndecan-1 mediates hepatocyte growth factor binding and promotes Met signaling in multiple myeloma”. Blood. 99 (4): 1405–10. PMID 11830493.
- ↑ Pellat-Deceunynck C, Barillé S, Jego G, Puthier D, Robillard N, Pineau D, Rapp MJ, Harousseau JL, Amiot M, Bataille R (December 1998). “The absence of CD56 (NCAM) on malignant plasma cells is a hallmark of plasma cell leukemia and of a special subset of multiple myeloma”. Leukemia. 12 (12): 1977–82. PMID 9844928.
- ↑ Barker HF, Hamilton MS, Ball J, Drew M, Franklin IM (July 1992). “Expression of adhesion molecules LFA-3 and N-CAM on normal and malignant human plasma cells”. Br. J. Haematol. 81 (3): 331–5. PMID 1382543.
- ↑ Seidl S, Kaufmann H, Drach J (September 2003). “New insights into the pathophysiology of multiple myeloma”. Lancet Oncol. 4 (9): 557–64. PMID 12965277.
- ↑ 60.0 60.1 Gupta D, Treon SP, Shima Y, Hideshima T, Podar K, Tai YT, Lin B, Lentzsch S, Davies FE, Chauhan D, Schlossman RL, Richardson P, Ralph P, Wu L, Payvandi F, Muller G, Stirling DI, Anderson KC (December 2001). “Adherence of multiple myeloma cells to bone marrow stromal cells upregulates vascular endothelial growth factor secretion: therapeutic applications”. Leukemia. 15 (12): 1950–61. PMID 11753617.
- ↑ Chauhan D, Kharbanda S, Ogata A, Urashima M, Teoh G, Robertson M, Kufe DW, Anderson KC (January 1997). “Interleukin-6 inhibits Fas-induced apoptosis and stress-activated protein kinase activation in multiple myeloma cells”. Blood. 89 (1): 227–34. PMID 8978296.
- ↑ Hideshima T, Chauhan D, Schlossman R, Richardson P, Anderson KC (July 2001). “The role of tumor necrosis factor alpha in the pathophysiology of human multiple myeloma: therapeutic applications”. Oncogene. 20 (33): 4519–27. doi:10.1038/sj.onc.1204623. PMID 11494147.
- ↑ Jourdan M, Tarte K, Legouffe E, Brochier J, Rossi JF, Klein B (March 1999). “Tumor necrosis factor is a survival and proliferation factor for human myeloma cells”. Eur. Cytokine Netw. 10 (1): 65–70. PMC 2025696. PMID 10210775.
- ↑ Tai YT, Li XF, Breitkreutz I, Song W, Neri P, Catley L, Podar K, Hideshima T, Chauhan D, Raje N, Schlossman R, Richardson P, Munshi NC, Anderson KC (July 2006). “Role of B-cell-activating factor in adhesion and growth of human multiple myeloma cells in the bone marrow microenvironment”. Cancer Res. 66 (13): 6675–82. doi:10.1158/0008-5472.CAN-06-0190. PMID 16818641.
- ↑ Georgii-Hemming P, Wiklund HJ, Ljunggren O, Nilsson K (September 1996). “Insulin-like growth factor I is a growth and survival factor in human multiple myeloma cell lines”. Blood. 88 (6): 2250–8. PMID 8822946.
- ↑ Dankbar B, Padró T, Leo R, Feldmann B, Kropff M, Mesters RM, Serve H, Berdel WE, Kienast J (April 2000). “Vascular endothelial growth factor and interleukin-6 in paracrine tumor-stromal cell interactions in multiple myeloma”. Blood. 95 (8): 2630–6. PMID 10753844.
- ↑ Prabhala RH, Pelluru D, Fulciniti M, Prabhala HK, Nanjappa P, Song W, Pai C, Amin S, Tai YT, Richardson PG, Ghobrial IM, Treon SP, Daley JF, Anderson KC, Kutok JL, Munshi NC (July 2010). “Elevated IL-17 produced by TH17 cells promotes myeloma cell growth and inhibits immune function in multiple myeloma”. Blood. 115 (26): 5385–92. doi:10.1182/blood-2009-10-246660. PMC 2902136. PMID 20395418.
- ↑ Noonan K, Marchionni L, Anderson J, Pardoll D, Roodman GD, Borrello I (November 2010). “A novel role of IL-17-producing lymphocytes in mediating lytic bone disease in multiple myeloma”. Blood. 116 (18): 3554–63. doi:10.1182/blood-2010-05-283895. PMC 4017298. PMID 20664052.
- ↑ 69.0 69.1 69.2 Finkel KW, Cohen EP, Shirali A, Abudayyeh A, American Society of Nephrology Onco-Nephrology Forum (2016). “Paraprotein-Related Kidney Disease: Evaluation and Treatment of Myeloma Cast Nephropathy”. Clin J Am Soc Nephrol. 11 (12): 2273–2279. doi:10.2215/CJN.01640216. PMC 5142056. PMID 27526708.
- ↑ 70.0 70.1 70.2 70.3 Heher EC, Rennke HG, Laubach JP, Richardson PG (2013). “Kidney disease and multiple myeloma”. Clin J Am Soc Nephrol. 8 (11): 2007–17. doi:10.2215/CJN.12231212. PMC 3817918. PMID 23868898.
- ↑ 71.0 71.1 71.2 Terpos E, Ntanasis-Stathopoulos I, Gavriatopoulou M, Dimopoulos MA (January 2018). “Pathogenesis of bone disease in multiple myeloma: from bench to bedside”. Blood Cancer J. 8 (1): 7. doi:10.1038/s41408-017-0037-4. PMC 5802524. PMID 29330358.
- ↑ Terpos E, Morgan G, Dimopoulos MA, Drake MT, Lentzsch S, Raje N, Sezer O, García-Sanz R, Shimizu K, Turesson I, Reiman T, Jurczyszyn A, Merlini G, Spencer A, Leleu X, Cavo M, Munshi N, Rajkumar SV, Durie BG, Roodman GD (June 2013). “International Myeloma Working Group recommendations for the treatment of multiple myeloma-related bone disease”. J. Clin. Oncol. 31 (18): 2347–57. doi:10.1200/JCO.2012.47.7901. PMC 4878084. PMID 23690408.
- ↑ Terpos E, Berenson J, Cook RJ, Lipton A, Coleman RE (May 2010). “Prognostic variables for survival and skeletal complications in patients with multiple myeloma osteolytic bone disease”. Leukemia. 24 (5): 1043–9. doi:10.1038/leu.2010.62. PMID 20376081.
- ↑ 74.0 74.1 Edwards CM, Zhuang J, Mundy GR (June 2008). “The pathogenesis of the bone disease of multiple myeloma”. Bone. 42 (6): 1007–13. doi:10.1016/j.bone.2008.01.027. PMC 2474770. PMID 18406675.
- ↑ 75.0 75.1 Hameed A, Brady JJ, Dowling P, Clynes M, O’Gorman P (2014). “Bone disease in multiple myeloma: pathophysiology and management”. Cancer Growth Metastasis. 7: 33–42. doi:10.4137/CGM.S16817. PMC 4133035. PMID 25187738.
- ↑ Dimopoulos MA, Kastritis E, Rosinol L, Bladé J, Ludwig H (August 2008). “Pathogenesis and treatment of renal failure in multiple myeloma”. Leukemia. 22 (8): 1485–93. doi:10.1038/leu.2008.131. PMID 18528426.
- ↑ Mussap M, Merlini G (2014). “Pathogenesis of renal failure in multiple myeloma: any role of contrast media?”. Biomed Res Int. 2014: 167125. doi:10.1155/2014/167125. PMC 4022292. PMID 24877060.
- ↑ 78.0 78.1 Cook G, Campbell JD (September 1999). “Immune regulation in multiple myeloma: the host-tumour conflict”. Blood Rev. 13 (3): 151–62. doi:10.1054/blre.1999.0111.
- ↑ 79.0 79.1 Schütt P, Brandhorst D, Stellberg W, Poser M, Ebeling P, Müller S, Buttkereit U, Opalka B, Lindemann M, Grosse-Wilde H, Seeber S, Moritz T, Nowrousian MR (August 2006). “Immune parameters in multiple myeloma patients: influence of treatment and correlation with opportunistic infections”. Leuk. Lymphoma. 47 (8): 1570–82. doi:10.1080/10428190500472503. PMID 16966269.
- ↑ 80.0 80.1 Urashima M, Ogata A, Chauhan D, Hatziyanni M, Vidriales MB, Dedera DA, Schlossman RL, Anderson KC (March 1996). “Transforming growth factor-beta1: differential effects on multiple myeloma versus normal B cells”. Blood. 87 (5): 1928–38. PMID 8634441.
- ↑ Mozaffari F, Hansson L, Kiaii S, Ju X, Rossmann ED, Rabbani H, Mellstedt H, Osterborg A (February 2004). “Signalling molecules and cytokine production in T cells of multiple myeloma-increased abnormalities with advancing stage”. Br. J. Haematol. 124 (3): 315–24. PMID 14717778.
Causes
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1] Associate Editor(s)-in-Chief: Haytham Allaham, M.D. [2] Shyam Patel [3]
Overview
The causes of multiple myeloma include sporadic mutations, such as TP53 mutation, and inherited predisposition.
Causes
Common causes
The causes of multiple myeloma include:
- Mutations in the tumor suppressor TP53 (most common)
- Sporadic mutations and genetic predisposition
- Mutations in tumor suppressors or oncogenes
- Chromosomal aberrations such as translocations can trigger the onset of malignancy and allow for uncontrolled plasma cell proliferation.[1]
Less common causes
- Familial causes are less contributory to the development of multiple myeloma compared to sporadic causes.[1]
Causes by Organ System
| Cardiovascular | No underlying causes |
| Chemical/Poisoning | No underlying causes |
| Dental | No underlying causes |
| Dermatologic | No underlying causes |
| Drug Side Effect | No underlying causes |
| Ear Nose Throat | No underlying causes |
| Endocrine | No underlying causes |
| Environmental | No underlying causes |
| Gastroenterologic | No underlying causes |
| Genetic | Mutations in the tumor suppressor TP53, sporadic mutations and genetic predisposition, mutations in tumor suppressors or oncogenes, chromosomal aberrations such as translocations, familial inheritance |
| Hematologic | No underlying causes |
| Iatrogenic | No underlying causes |
| Infectious Disease | No underlying causes |
| Musculoskeletal/Orthopedic | No underlying causes |
| Neurologic | No underlying causes |
| Nutritional/Metabolic | No underlying causes |
| Obstetric/Gynecologic | No underlying causes |
| Oncologic | No underlying causes |
| Ophthalmologic | No underlying causes |
| Overdose/Toxicity | No underlying causes |
| Psychiatric | No underlying causes |
| Pulmonary | No underlying causes |
| Renal/Electrolyte | No underlying causes |
| Rheumatology/Immunology/Allergy | No underlying causes |
| Sexual | No underlying causes |
| Trauma | No underlying causes |
| Urologic | No underlying causes |
| Miscellaneous | No underlying causes |
Causes in Alphabetical Order
List the causes of the multiple myeloma in alphabetical order:
- Chromosomal aberrations
- Familial inheritance
- Mutations in oncogenes
- Mutations in the tumor suppressor TP53
- Mutations in tumor suppressors
- Translocations
References
- ↑ 1.0 1.1 Rajkumar SV (2016). “Multiple myeloma: 2016 update on diagnosis, risk-stratification, and management”. Am J Hematol. 91 (7): 719–34. doi:10.1002/ajh.24402. PMC 5291298. PMID 27291302.
Differentiating Multiple Myeloma from other Diseases
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1] Associate Editor(s)-in-Chief: Hannan Javed, M.D.[2] Haytham Allaham, M.D. [3] Shyam Patel [4]
Overview
Multiple myeloma must be differentiated from other causes of bone lesions such as osteoporosis, osteomalacia, scurvy, osteogenesis imperfecta, and homocystinuria. Each condition has unique causes, features, and treatment.
Differentiating Multiple Myeloma from other Diseases
- The table below summarizes how to differentiate multiple myeloma from other conditions that have a similar presentation:[1][2][3][4][5][6][7]
References
- ↑ “Myeloma – SEER Stat Fact Sheets”. Retrieved 17 February 2014.
- ↑ Zuo QY, Wang H, Li W, Niu XH, Huang YH, Chen J; et al. (2017). “Treatment and outcomes of tumor-induced osteomalacia associated with phosphaturic mesenchymal tumors: retrospective review of 12 patients”. BMC Musculoskelet Disord. 18 (1): 403. doi:10.1186/s12891-017-1756-1. PMC 5609032. PMID 28934935.
- ↑ Shaker JL, Albert C, Fritz J, Harris G (2015). “Recent developments in osteogenesis imperfecta”. F1000Res. 4 (F1000 Faculty Rev): 681. doi:10.12688/f1000research.6398.1. PMC 4566283. PMID 26401268.
- ↑ Kumar A, Palfrey HA, Pathak R, Kadowitz PJ, Gettys TW, Murthy SN (2017). “The metabolism and significance of homocysteine in nutrition and health”. Nutr Metab (Lond). 14: 78. doi:10.1186/s12986-017-0233-z. PMC 5741875. PMID 29299040.
- ↑ Soh KT, Tario JD, Wallace PK (December 2017). “Diagnosis of Plasma Cell Dyscrasias and Monitoring of Minimal Residual Disease by Multiparametric Flow Cytometry”. Clin. Lab. Med. 37 (4): 821–853. doi:10.1016/j.cll.2017.08.001. PMC 5804349. PMID 29128071.
- ↑ Kyle RA, Rajkumar SV (January 2009). “Criteria for diagnosis, staging, risk stratification and response assessment of multiple myeloma”. Leukemia. 23 (1): 3–9. doi:10.1038/leu.2008.291. PMC 2627786. PMID 18971951.
- ↑ Rajkumar SV, Landgren O, Mateos MV (May 2015). “Smoldering multiple myeloma”. Blood. 125 (20): 3069–75. doi:10.1182/blood-2014-09-568899. PMC 4432003. PMID 25838344.
Epidemiology and Demographics
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1] Associate Editor(s)-in-Chief: Hannan Javed, M.D.[2]; Haytham Allaham, M.D. [3]; Shyam Patel [4]
Overview
In 2012, the incidence of multiple myeloma was approximately 6.3 per 100,000 cases with a mortality rate of 3.3 per 100,000 cases in the United States. The prevalence of multiple myeloma was estimated to be 89,658 cases in 2012 in the United States. Multiple myeloma is the second most common blood cancer after non-Hodgkin’s lymphoma and 14th most common cancer overall in United States. Males are more commonly affected with multiple myeloma than females; the male to female ratio is approximately 1.54 to 1. Multiple myeloma usually affects individuals of the African American race. Asian individuals are less likely to develop multiple myeloma. The incidence of multiple myeloma increases with age.
Epidemiology and Demographics
Incidence
- The age-standardized incidence rate of multiple myeloma worldwide is 1.5 per 100,000 persons per year.[1][2]
- According to age-adjusted rates based in 2011-2015, the incidence of multiple myeloma was approximately 6.7 per 100,000 individuals with a case-fatality rate of 3.3 per 100,000 in the United States.[3][2]
- In 2018, multiple myeloma will constitute approximately 1.8% of the estimated new cancer cases.[4][2]
- In 2018, the estimated deaths caused by multiple myeloma will constitute 2.1% of all cancer mortality cases.[5][2]
- In 2018, approximately 30,770 people will be diagnosed with multiple myeloma.[6]
- In 2018, approximately 12,770 people die from multiple myeloma.[2]
- According to 2013-2015 data, approximately 0.8% of all people will have a diagnosis of multiple myeloma at some point during their lifetime in US.[2]
- According to an estimation in 2015, there were 124,733 people with myeloma living in the United States.[2]
- Multiple myeloma is the second most common hematologic malignancy, after non-Hodgkin lymphoma.[1]
- Since 1975, the overall multiple myeloma incidence has increased nearly 1 percent annually.[4]
- Solitary plasmacytoma accounts for approximately 5% of plasma cell neoplasms.[7]
| Multiple Myeloma Epidemiology | |
|---|---|
| Estimated New Cases in 2018 | 30,770 |
| % of All New Cancer Cases | 1.8% |
| Estimated Deaths in 2018 | 12,770 |
| % of All Cancer Deaths | 2.1% |
| 5 Years Survival Rate (2008-2014) | 50.7% |
| Adopted from National Cancer Institute[2] | |
Prevalence
- Myeloma is the 14th leading cause of cancer death in the United States.[5]
- According to an estimation in 2015, there were 124,733 people with myeloma living in the United States.[2]
Age
- The incidence of multiple myeloma increases with age, and the median age at diagnosis is 69 years.[2]
| Percent of New Cases by Age Group | |
|---|---|
| Age | Percent of New cases |
| <20 | |
| 20-34 | 0.5% |
| 35-44 | 2.8% |
| 45-54 | 10.9% |
| 55-64 | 23.2% |
| 65-74 | 29.8% |
| 75-84 | 23.7% |
| >84 | 9.0% |
| Adopted from National Cancer Institute[2] | |
Gender
- Males are more commonly affected with multiple myeloma than females. The male to female ratio is approximately 1.54 to 1.[8]
Race
- Among African Americans, multiple myeloma is one of the top 10 leading causes of cancer deaths.[5]
- The incidence of multiple myeloma in the African American population is more than the European American population.
- African Americans have a 2-fold higher age-standardized incidence rate of multiple myeloma than Caucasians. The incidence of multiple myeloma in African Americans is 9.6 per 100,000 persons. The incidence of Caucasians is 4.1 per 100,000 persons.[1]
| New Cases per 100,000 Persons by Race/Ethnicity & Sex | ||
|---|---|---|
| Race | Female | Male |
| All Races | 5.3 | 8.4 |
| White | 4.7 | 7.9 |
| Black | 11.6 | 15.9 |
| Asian/Pacific Islander | 3.1 | 4.9 |
| American Indian/Alaska Native | 5.5 | 6.2 |
| Hispanic | 5.0 | 7.6 |
| Non-Hispanic | 5.4 | 8.5 |
| Adopted from National Cancer Institute[2] | ||
Gallery










References
- ↑ 1.0 1.1 1.2 Hong J, Lee JH (2016). “Recent advances in multiple myeloma: a Korean perspective”. Korean J Intern Med. 31 (5): 820–34. doi:10.3904/kjim.2015.408. PMC 5016289. PMID 27604794.
- ↑ 2.00 2.01 2.02 2.03 2.04 2.05 2.06 2.07 2.08 2.09 2.10 2.11 “Myeloma – Cancer Stat Facts”.
- ↑ Plasma cell neoplasm.National cancer institute (2015)http://www.cancer.gov/types/myeloma/hp/myeloma-treatment-pdq#cit/section_1.1 Accessed on September, 20th 2015
- ↑ 4.0 4.1 A snapshot of myeloma. National cancer institute(2014)http://www.cancer.gov/research/progress/snapshots/myeloma Accessed on September, 20th 2015
- ↑ 5.00 5.01 5.02 5.03 5.04 5.05 5.06 5.07 5.08 5.09 5.10 Seer stat fact sheet. National cancer institute (2015)http://seer.cancer.gov/statfacts/html/mulmy.html Accessed on September, 20th 2015
- ↑ “Myeloma – Cancer Stat Facts”.
- ↑ Jia R, Xue L, Liang H, Gao K, Li J, Zhang Z (2015). “Surgery combined with radiotherapy for the treatment of solitary plasmacytoma of the rib: a case report and review of the literature”. J Cardiothorac Surg. 10: 125. doi:10.1186/s13019-015-0335-5. PMC 4605096. PMID 26464186.
- ↑ Multiple myeloma. Radiopaedia (2015)http://radiopaedia.org/articles/multiple-myeloma-1 Accessed on September, 20th 2015
Risk Factors
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1] Associate Editor(s)-in-Chief: Haytham Allaham, M.D. [2]; Shyam Patel [3]
Overview
Risk factors for multiple myeloma include advanced age, African American race, male gender, obesity, exposure to chemicals and radiation, the presence of family history of hematologic conditions.
Risk Factors
The table below lists the risk factors for multiple myeloma:
| Risk Factor | Description |
|---|---|
| Age | The chance of developing multiple myeloma increases with age, as somatic mutations in plasma cells accumulate with aging. The median age of diagnosis of multiple myeloma is 61. Only 1% of multiple myeloma cases are diagnosed in patients younger than 35 years.[1][2][3] |
| Race | African Americans and Native Pacific Islanders are at higher risk of developing multiple myeloma compared to Caucasians.[4][3][5] |
| Gender | Males are more commonly affected by multiple myeloma than females.[2][3] |
| Presence of other plasma cell disorders | Patients with other plasma cell disorders such as monoclonal gammopathy of undetermined significance (MGUS) or smoldering multiple myeloma are at increased risk for development of active multiple myeloma.[6][3] The risk for progression to active multiple myeloma depends on the plasma cell burden, free light chain ratio, and subtype of paraprotein. |
| Family history | A familial predisposition to myeloma exists due to hyperphosphorylation of specific proteins that may contribute to a higher rates of multiple myeloma in certain groups.[7][4][8][3] Patients with germline mutations in tumor suppressors such as TP53 may be at increased risk for multiple myeloma. |
| Obesity | Obesity increases a person’s risk of developing multiple myeloma, as is true for other types of malignancies.[6][3] The pathophysiologic basis for the link between obesity and multiple myeloma is not well described. |
| Workplace exposures | Petroleum workers and farmers tend to have higher incidence of multiple myeloma relative to other occupations.[9][6][3] Agent Orange exposure may also be linked to the development of multiple myeloma. Agent Orange exposure is common among U.S. veterans. |
| Presence of other diseases | There is a slight increase in the risk for developing multiple myeloma among patients with type 2 diabetes mellitus. There is a weak association between systemic lupus erythematosus (SLE) and multiple myeloma, especially in the United States and Canada. Other autoimmune conditions such as pernicious anemia and ankylosing spondylitis are associated with significantly increased risk for developing multiple myeloma.[10] |
| Radiation | People who were exposed to radiation (atomic bombs or nuclear accidents) have a higher risk for developing multiple myeloma.[6][3] Ionizing radiation is more likely to cause multiple myeloma compared to other types of radiation, as ionizing radiation induces DNA damage. |
References
- ↑ Press Releases. Compugen (2015)http://www.cgen.com/media-center/press-releases/-314 Accessed on September, 20th 2015
- ↑ 2.0 2.1 Multiple myeloma. Radiopaedia (2015)http://radiopaedia.org/articles/multiple-myeloma-1 Accessed on September, 20th 2015
- ↑ 3.0 3.1 3.2 3.3 3.4 3.5 3.6 3.7 Multiple myeloma. The American Cancer Society (2015) http://www.cancer.org/cancer/multiplemyeloma/detailedguide/multiple-myeloma-risk-factors Accessed on September, 20 2015
- ↑ 4.0 4.1 Multiple myeloma. Wikipedia (2015)https://en.wikipedia.org/wiki/Multiple_myeloma#Pathophysiology Accessed on September, 20th 2015
- ↑ Seer stat fact sheet. National cancer institute (2015)http://seer.cancer.gov/statfacts/html/mulmy.html Accessed on September, 20th 2015
- ↑ 6.0 6.1 6.2 6.3 Multiple myeloma. MedlinePlus (2015)http://www.wikidoc.org/index.php?title=Multiple_myeloma_risk_factors&action=edit§ion=2 Accessed on Septmeber, 20th 2015
- ↑ Bourguet, CC.; Grufferman, S.; Delzell, E.; DeLong, ER.; Cohen, HJ. (1985). “Multiple myeloma and family history of cancer. A case-control study”. Cancer. 56 (8): 2133–9. PMID 4027940. Unknown parameter
|month=ignored (help) - ↑ Koura DT, Langston AA (2013). “Inherited predisposition to multiple myeloma”. Ther Adv Hematol. 4 (4): 291–7. doi:10.1177/2040620713485375. PMC 3734900. PMID 23926460.
- ↑ Gallagher, RP.; Spinelli, JJ.; Elwood, JM.; Skippen, DH. (1983). “Allergies and agricultural exposure as risk factors for multiple myeloma”. Br J Cancer. 48 (6): 853–7. PMID 6652026. Unknown parameter
|month=ignored (help) - ↑ Sergentanis TN, Zagouri F, Tsilimidos G, Tsagianni A, Tseliou M, Dimopoulos MA, Psaltopoulou T (October 2015). “Risk Factors for Multiple Myeloma: A Systematic Review of Meta-Analyses”. Clin Lymphoma Myeloma Leuk. 15 (10): 563–77.e1–3. doi:10.1016/j.clml.2015.06.003. PMID 26294217.
Screening
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1] Associate Editor(s)-in-Chief: Haytham Allaham, M.D. [2]; Shyam Patel [3]
Overview
Risk factors for multiple myeloma include advanced age, African American race, male gender, obesity, exposure to chemicals and radiation, the presence of family history of hematologic conditions.
Risk Factors
The table below lists the risk factors for multiple myeloma:
| Risk Factor | Description |
|---|---|
| Age | The chance of developing multiple myeloma increases with age, as somatic mutations in plasma cells accumulate with aging. The median age of diagnosis of multiple myeloma is 61. Only 1% of multiple myeloma cases are diagnosed in patients younger than 35 years.[1][2][3] |
| Race | African Americans and Native Pacific Islanders are at higher risk of developing multiple myeloma compared to Caucasians.[4][3][5] |
| Gender | Males are more commonly affected by multiple myeloma than females.[2][3] |
| Presence of other plasma cell disorders | Patients with other plasma cell disorders such as monoclonal gammopathy of undetermined significance (MGUS) or smoldering multiple myeloma are at increased risk for development of active multiple myeloma.[6][3] The risk for progression to active multiple myeloma depends on the plasma cell burden, free light chain ratio, and subtype of paraprotein. |
| Family history | A familial predisposition to myeloma exists due to hyperphosphorylation of specific proteins that may contribute to a higher rates of multiple myeloma in certain groups.[7][4][8][3] Patients with germline mutations in tumor suppressors such as TP53 may be at increased risk for multiple myeloma. |
| Obesity | Obesity increases a person’s risk of developing multiple myeloma, as is true for other types of malignancies.[6][3] The pathophysiologic basis for the link between obesity and multiple myeloma is not well described. |
| Workplace exposures | Petroleum workers and farmers tend to have higher incidence of multiple myeloma relative to other occupations.[9][6][3] Agent Orange exposure may also be linked to the development of multiple myeloma. Agent Orange exposure is common among U.S. veterans. |
| Presence of other diseases | There is a slight increase in the risk for developing multiple myeloma among patients with type 2 diabetes mellitus. There is a weak association between systemic lupus erythematosus (SLE) and multiple myeloma, especially in the United States and Canada. Other autoimmune conditions such as pernicious anemia and ankylosing spondylitis are associated with significantly increased risk for developing multiple myeloma.[10] |
| Radiation | People who were exposed to radiation (atomic bombs or nuclear accidents) have a higher risk for developing multiple myeloma.[6][3] Ionizing radiation is more likely to cause multiple myeloma compared to other types of radiation, as ionizing radiation induces DNA damage. |
References
- ↑ Press Releases. Compugen (2015)http://www.cgen.com/media-center/press-releases/-314 Accessed on September, 20th 2015
- ↑ 2.0 2.1 Multiple myeloma. Radiopaedia (2015)http://radiopaedia.org/articles/multiple-myeloma-1 Accessed on September, 20th 2015
- ↑ 3.0 3.1 3.2 3.3 3.4 3.5 3.6 3.7 Multiple myeloma. The American Cancer Society (2015) http://www.cancer.org/cancer/multiplemyeloma/detailedguide/multiple-myeloma-risk-factors Accessed on September, 20 2015
- ↑ 4.0 4.1 Multiple myeloma. Wikipedia (2015)https://en.wikipedia.org/wiki/Multiple_myeloma#Pathophysiology Accessed on September, 20th 2015
- ↑ Seer stat fact sheet. National cancer institute (2015)http://seer.cancer.gov/statfacts/html/mulmy.html Accessed on September, 20th 2015
- ↑ 6.0 6.1 6.2 6.3 Multiple myeloma. MedlinePlus (2015)http://www.wikidoc.org/index.php?title=Multiple_myeloma_risk_factors&action=edit§ion=2 Accessed on Septmeber, 20th 2015
- ↑ Bourguet, CC.; Grufferman, S.; Delzell, E.; DeLong, ER.; Cohen, HJ. (1985). “Multiple myeloma and family history of cancer. A case-control study”. Cancer. 56 (8): 2133–9. PMID 4027940. Unknown parameter
|month=ignored (help) - ↑ Koura DT, Langston AA (2013). “Inherited predisposition to multiple myeloma”. Ther Adv Hematol. 4 (4): 291–7. doi:10.1177/2040620713485375. PMC 3734900. PMID 23926460.
- ↑ Gallagher, RP.; Spinelli, JJ.; Elwood, JM.; Skippen, DH. (1983). “Allergies and agricultural exposure as risk factors for multiple myeloma”. Br J Cancer. 48 (6): 853–7. PMID 6652026. Unknown parameter
|month=ignored (help) - ↑ Sergentanis TN, Zagouri F, Tsilimidos G, Tsagianni A, Tseliou M, Dimopoulos MA, Psaltopoulou T (October 2015). “Risk Factors for Multiple Myeloma: A Systematic Review of Meta-Analyses”. Clin Lymphoma Myeloma Leuk. 15 (10): 563–77.e1–3. doi:10.1016/j.clml.2015.06.003. PMID 26294217.
Natural History, Complications and Prognosis
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1] Associate Editor(s)-in-Chief: Haytham Allaham, M.D. [2] Shyam Patel [3]
Overview
The natural history of multiple myeloma begins with an asymptomatic phase, then progresses to symptomatic involvement and organ involvement. Outcomes are generally good if treatment is begun at an appropriate time. Complications of multiple myeloma include hematologic complications, such as cytopenias, and skeletal complications, such as pathologic fractures. The prognosis of multiple myeloma is based on chromosome changes, stage of disease, kidney function, labelling index, age, performance status, and various laboratory values.
Natural History
- Multiple myeloma: The natural history of multiple myeloma usually begins with an asymptomatic phase. Monoclonal paraprotein or free light chains can be elevated in the absence of symptoms and are frequently detected on laboratory testing. If left untreated, most of the patients with multiple myeloma will gradually develop fatigue, bone pain, and pallor. In as many as 30-40% cases the diagnosis may be incidental and is often diagnosed on routine blood screening. Additional laboratory workup can reveal signs of end-organ damage, such as anemia, renal dysfunction, or elevated calcium. Bony pain can ensue if left untreated. Upon recognition of a possible diagnosis of multiple myeloma, a bone marrow biopsy is usually performed for definitive diagnosis. Once treatment with induction therapy is underway, patient typically experience improvement in laboratory measures, such as reduction in monoclonal paraprotein, reduction in free light chain levels, reduction in calcium, increase in hemoglobin, and improvement in glomerular filtration rate (GFR). The improvement in laboratory parameters is typically seen within 1-3 months after starting induction chemotherapy. After 6-8 cycles of induction chemotherapy, patients will typically proceed to autologous stem cell transplant. If transplant is not performed, the natural history of the disease is characterized by relapse, in which the malignant plasma cell clone is resistant to the initial induction chemotherapy regimen.
- Plasmacytoma: The natural history of plasmacytoma begins with a symptomatic phase, which typically presents as a solid mass. The first diagnostic step is typically a tissue biopsy, which reveals the presence of clonal plasma cells. Once the diagnosis is made, further workup includes assessment for systemic involvement. In most cases, a diagnosis of plasmacytoma is not concurrent with a diagnosis of multiple myeloma. However, the natural history of plasmacytoma is such that there is a risk of progression to active multiple myeloma after many years. After a median follow-up of 58 months, 67% of patients will develop progression to multiple myeloma. Approximately 20% of patients will die from progression of disease.[1]
Complications
Complications that can develop as a result of multiple myeloma are divided into hematologic complications and systemic complications:[2][3]
Hematologic complications
Hematologic complications of multiple myeloma are due to the accumulation of excess numbers of abnormal plasma cells, which impairs normal hematopoiesis. This is referred to as myelophthisis, or the replacement of normal bone marrow by infiltrating tumor cells. This can result in complications such as anemia, thrombocytopenia, and leukopenia.
- Anemia: Impaired erythroid progenitor formation leads to decreased red blood cell production, which results in anemia. The anemia is usually normocytic (mean corpuscular volume of 80-100 femtoliters). Patients can experience signs and symptoms including fatigue, mucosal and conjunctival pallor, shortness of breath, and decreased exercise tolerance. Severe anemia can occur in patients who have concurrent renal dysfunction from multiple myeloma, as erythropoietin production is impaired in patients with renal complications. Patients may require red blood cell transfusion if the hemoglobin level is less than 7 g/dl or if severe symptomatic anemia develops. Complications from transfusion include HIV infection, hepatitis B infection, hepatitis C infection, pulmonary edema from volume overload, alloimmunization to red blood cell products, and hemosiderosis (iron overload state).
- Thrombocytopenia: Impaired megakaryocyte formation leads to decreased platelet production, which results in thrombocytopenia. Patients can experience signs and symptoms including mucosal bleeding, upper and lower gastrointestinal bleeding, bruising, petechiae, and ecchymoses. In rare cases, fatal hemorrhage can occur. Patients may require platelet transfusion if the platelet count is less than 10,000 cells per microliter, or less than 50,000 cells per microliter in the setting of bleeding diathesis.
- Leukopenia: Impaired granulocyte and lymphocyte progenitor formation leads to decreased mature white blood cell production, which results in leukopenia. Patients can experience signs and symptoms including localized infections (pneumonia, urinary tract infections, cellulitis, dental infections), fevers, chills, and sepsis. In rare cases, infection can be very severe and lead to severe sepsis. Patients may require treatment with antibiotics. Of note, although the plasma cell burden is increased in multiple myeloma, these plasma cells do not function in a normal manner, and the abnormal paraprotein production in multiple myeloma does not confer adequate humoral immunity. Thus, patient can have normal plasma cell counts but can be functionally immunosuppressed.
Systemic complications
Systemic complications of multiple myeloma are due to the effects of plasma cells on various non-hematologic organs, such as the kidneys, bones, and nervous system.
- Skeletal complications: Skeletal-related events are diverse and include asymptomatic lytic lesions, symptomatic lytic lesions, and pathologic fractures. Pathologic fractures in the appendicular skeleton (long bones) can result in functional impairment and impaired mobility. Pathologic fractures in the axial skeleton (vertebral column) can result in more serious complications. Spinal cord compression occurs if pathologic fractures occur in the vertebral column with impingement of bony fragments on the spinal cord. Symptoms include back pain, numbness, dysthesias, decreased deep tendon reflexes, and loss of bowel or bladder control. Spinal cord compression is an oncologic emergency and requires urgent neurosurgical decompression, radiation therapy, and administration of dexamethasone 10mg IV followed by 4 mg PO every 6 hours to prevent further cord compromise.
- Hypercalcemia: In patients with multiple myeloma, calcium is frequently greater than 11 mg/dl. Hypercalcemia can result in signs and symptoms include nephrolithiasis (kidney stones), psychiatric disturbance, bony pain, and constipation. Treatment of hypercalcemia includes calcitonin, bisphosphonates, denosumab, furosemide, and corticosteroids.
- Renal failure: Multiple myeloma is associated with both acute renal failure and chronic renal failure. The mechanism of renal failure is usually due to abnormal deposition of immunoglobulin light chains in renal tubules, a process known as cast nephropathy. Signs and symptoms of renal failure include decreased urine output, volume overload, nausea, pruritic, metallic taste, and normocytic anemia due to erythropoietin deficiency.
- Neurologic complications: The effects of abnormal plasma cells on the nervous system can result in neurologic impairment. Multiple myeloma can cause neurologic complications via various mechanisms, including plasma cell infiltration of tissues of the central nervous system, plasma cell infiltration of tissues of the peripheral nerves (resulting in carpel tunnel syndrome), osseous destruction in areas abutting nerve roots (resulting in radiculopathy), or osseous destruction in areas abutting the spinal cord (result in spinal cord compression).
Prognosis
The prognosis of multiple myeloma depends of a variety of factors. The most important factor that determines disease biology and prognosis is cytogenetics. Overall, prognosis is generally good with appropriate treatment. Without treatment, multiple myeloma will result in death with a median survival of 7 months. The median overall survival for newly diagnosed multiple myeloma ranges from 2 to 10 years. The 5-year overall survival rate of multiple myeloma is approximately 46%. However, the prognosis is far better in the current era since multiple new therapeutic interventions have been introduced. The table below lists common prognostic factors for multiple myeloma.[4][5][6][7][8]
| Prognostic Factor | Description |
|---|---|
| Chromosome changes | Cytogenetic analysis of multiple myeloma cells has prognostic value, with deletion of chromosome 13, non-hyperdiploidy, and the balanced translocations t(4;14), t(14;16), and t(14;20) conferring a poorer prognosis. Gain of chromosome 1q21 is associated with a somewhat poor prognosis. The 11q13 and 6p21 cytogenetic abnormalities are associated with a better prognosis. |
| Stage | Advanced stage of multiple myeloma, such as Durie-Salmon or International Staging System (ISS) stage III, are associated with poor prognosis. |
| Kidney function | An elevated level of creatinine is associated with poor prognosis. |
| Labelling index | The labeling index indicates how fast the cancer cells are growing. A high plasma cell labeling index (PCLI) or proliferation (reproduction) rate (Ki-67) is associated with poor prognosis. |
| Age | Older patients have worse prognosis than younger patients. |
| Associated plasma cell disorder | The presence of plasma cell leukemia or soft tissue plasmacytoma is associated with a particularly poor prognosis among patients with multiple myeloma. |
| Performance status | Performance status is ranked on a 0–5 scale per the Eastern Cooperative Oncology Group (ECOG) classification. The lower the number, the healthier and more active the person is, and the better the prognosis. Performance status is important in multiple myeloma because people who are healthier can withstand more intensive treatment. |
| Beta-2-microglobulin | A higher level of beta-2-microglobulin is associated with poor prognosis. This laboratory value is incorporated into the International Staging System (ISS). |
| Albumin level | A lower albumin level is associated with poor prognosis. This laboratory value is incorporated into the International Staging System (ISS). |
| Lactate dehydrogenase level | A higher level of lactate dehydrogenase (LDH) is associated with poor prognosis. This laboratory value is incorporated into the Revised International Staging System (R-ISS). |
| Response to treatment | Patients whose cancer responds to treatment and enters complete remission have a better prognosis than people whose cancer does not respond to the initial treatment. |
The prognosis for solitary plasmacytoma is generally very good. The median survival is 10 years. The 5-year survival rate is 72% and the 20-year survival rate is 37%.[1]
References
- ↑ 1.0 1.1 Jia R, Xue L, Liang H, Gao K, Li J, Zhang Z (2015). “Surgery combined with radiotherapy for the treatment of solitary plasmacytoma of the rib: a case report and review of the literature”. J Cardiothorac Surg. 10: 125. doi:10.1186/s13019-015-0335-5. PMC 4605096. PMID 26464186.
- ↑ Bladé, J.; Rosiñol, L. (2007). “Complications of multiple myeloma”. Hematol Oncol Clin North Am. 21 (6): 1231–46, xi. doi:10.1016/j.hoc.2007.08.006. PMID 17996596. Unknown parameter
|month=ignored (help) - ↑ Eslick R, Talaulikar D (October 2013). “Multiple myeloma: from diagnosis to treatment”. Aust Fam Physician. 42 (10): 684–8. PMID 24130968.
- ↑ Multiple myeloma. Canadian cancer society (2015)http://www.cancer.ca/en/cancer-information/cancer-type/multiple-myeloma/prognosis-and-survival/?region=mb Accessed on September, 20th 2015
- ↑ Multiple myeloma. Wikipedia (2015)https://en.wikipedia.org/wiki/Multiple_myeloma#Prognosis Accessed on September, 20th 2015
- ↑ Plasma cell neoplasm. Cancer.gov (2015)http://www.cancer.gov/types/myeloma/hp/myeloma-treatment-pdq#link/_40_toc
- ↑ Multiple myeloma. National Cancer Institute(2015) www.cancer.gov/types/myeloma/hp/myeloma-treatment-pdq#link/_40_toc Accessed on September, 20th 2015
- ↑ Sonneveld P, Avet-Loiseau H, Lonial S, Usmani S, Siegel D, Anderson KC; et al. (2016). “Treatment of multiple myeloma with high-risk cytogenetics: a consensus of the International Myeloma Working Group”. Blood. 127 (24): 2955–62. doi:10.1182/blood-2016-01-631200. PMC 4920674. PMID 27002115.
Diagnosis
Diagnosis
Diagnostic Criteria | Staging | History and Symptoms | Physical Examination | Laboratory Findings | X Ray | CT | MRI | Other Imaging Findings | Other Diagnostic Studies
Treatment
Treatment
Medical Therapy | Surgery | Primary Prevention | Secondary Prevention | Future or Investigational Therapies
Looking for the patient version?
© 2026 MyEClinic – IFTM Institut für Telematik in der Medizin GmbH