
Uremic pericarditis
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor-In-Chief: Varun Kumar, M.B.B.S.; Lakshmi Gopalakrishnan, M.B.B.S.Amandeep Singh M.D.[2]
Synonyms and keywords:Pericarditis fibrinosa, Uraemic pericarditis, Pericarditis due to uremia, Pericarditis due to uraemia
To go back to the main page on Pericarditis, click here.
Overview
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor-In-Chief: Varun Kumar, M.B.B.S.
Overview
Renal failure can be associated with the development of a pericardial effusion and pericarditis, a condition known as uremic pericarditis. The underlying pathophysiology is not entirely clear, but it is hypothesized that uremic pericarditis is due to a build up of metabolic toxins such as urea, creatinine, methylguanidine which cause inflammation of pericardium. With the introduction of dialysis, the incidence of uremic pericarditis has dropped[1].
Differentiating Uremic Pericarditis from other Diseases
Signs and symptoms of pericarditis may be similar to several other conditions including myocardial infarction, aortic dissection and pulmonary embolism which are life threatening and therefore it is important to differentiate them. Pain along the trapezius ridge, which is unresponsive to vasodilator therapy and varies with position, is a specific sign of pericarditis.
Diagnosis
Laboratory Findings
Non-specific markers of inflammation are generally elevated in pericarditis. These include the leukocyte count, C-reactive protein, and ESR. The cardiac troponin is elevated if there is an injury to the underlying myocardium, a condition termed as myopericarditis. Diagnostic pericardiocentesis and biopsy help in identifying an underlying infectious or malignant process.
Echocardiography
Echocardiogram may show presence of fluid surrounding the heart in pericardial effusion. Loculated effusions secondary to adhesions in pericardial cavity may also be visualized as shown in the video below. Swinging motion of the heart may be seen in patients with cardiac tamponade.
CT
On CT, pericardial fluid adds to the thickness of pericardium as both have the similar signal intensities. In pericarditis, pericardium can generate an intermediate signal intensity and may enhance after gadolinium administration. In pericardial effusion, hemorrhagic effusions can be differentiated from a transudate or an exudate based on signal characteristics (high signal on T1-weighted images) or density (high-density clot on CT). CT is superior to MRI in the visualization of pericardial calcification which is often seen in the patient with pericardial constriction. CT imaging also helps in detecting the presence of tumors and the extent of metastasis of the neoplasm.
MRI
On MRI, normal pericardium appears as a thin dark band that is bordered by a bright band on both sides on T1 weighted spin imaging. These surrounding bright bands are associated with the surrounding epicardial and pericardial fat. Following the administration of gadolinium, pericardium may appear thick and inflamed in the setting of pericarditis. Lower intensity signal is observed in constrictive pericarditis than in acute pericarditis. Comprehensive visualization of the LV endocardium and the physiologic consequences of abnormal pericardial thickening can also be obtained without exposure to ionizing radiation.[2]
Cardiac Catheterization
In presence Cardiac tamponade, there is equalization of pressures in all four chambers of heart. The right atrial pressure equals the right ventricular end diastolic pressure equals the pulmonary artery diastolic pressure.
References
- ↑ Bailey GL, Hampers CL, Hager EB, Merrill JP (1968). “Uremic pericarditis. Clinical features and management”. Circulation. 38 (3): 582–91. PMID 5673609.
- ↑ Hatle LK, Appleton CP, Popp RL (1989). “Differentiation of constrictive pericarditis and restrictive cardiomyopathy by Doppler echocardiography”. Circulation. 79 (2): 357–70. PMID 2914352.
Pathophysiology
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor-In-Chief: Varun Kumar, M.B.B.S.; Lakshmi Gopalakrishnan, M.B.B.S.
Overview
The pathophysiology of uremic pericarditis is not fully understood. However, there is a correlation observed with levels of blood urea nitrogen(usually >60 mg/dL) and creatinine. In renal failure, the absence or inadequate dialysis can lead to accumulation of these toxins in the body which may cause inflammation of pericardium and development of adhesions between the two pericardial layers. This could lead to loculation of effusion in pericardial cavity. Patients undergoing dialysis may also develop pericarditis. In a series, 13% of patients undergoing hemodialysis developed pericarditis.
Pathophysiology
- The pathophysiology of uremic pericarditis is not fully understood. However, there is a correlation observed with levels of blood urea nitrogen(usually >60 mg/dL) and creatinine.
- In renal failure, the absence or inadequate dialysis can lead to accumulation of these toxins in the body which may cause inflammation of pericardium and development of adhesions between the two pericardial layers. This could lead to loculation of effusion in pericardial cavity.
- Patients undergoing dialysis may also develop pericarditis. In a series, 13% of patients undergoing hemodialysis developed pericarditis[1]
- Uremic pericarditis can occur as a serous or a hemorrhagic effusion with considerable overlapping. Hemorrhagic effusions are more common secondary to uremia induced platelet dysfunction and the use of anticoagulation during hemodialysis.
- Dialysis associated pericarditis may also be secondary to volume overload and bacterial or viral infections.[2]
- Presence of a large pericardial effusion that persists for >10 days after intensive dialysis has a high likelihood of development of cardiac tamponade.
Gross Pathology
-
 Pericarditis in uremia
Pericarditis in uremia -
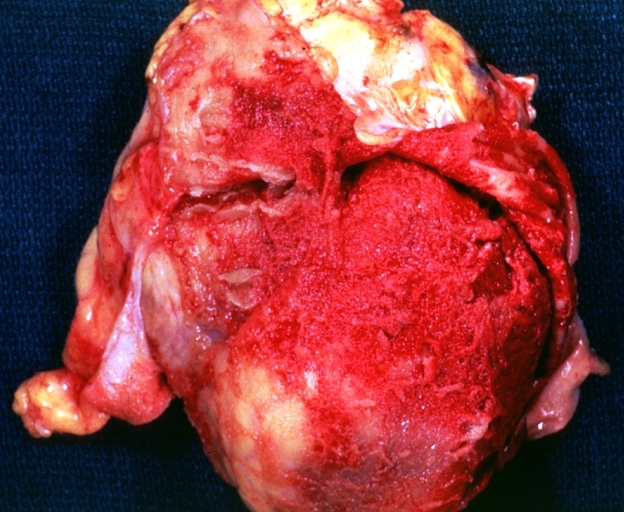
 Fibrinous pericarditis: Gross, natural color, an excellent example of bread and butter appearance. Uremia, chronic glomerulonephritis and sepsis.
Fibrinous pericarditis: Gross, natural color, an excellent example of bread and butter appearance. Uremia, chronic glomerulonephritis and sepsis. -
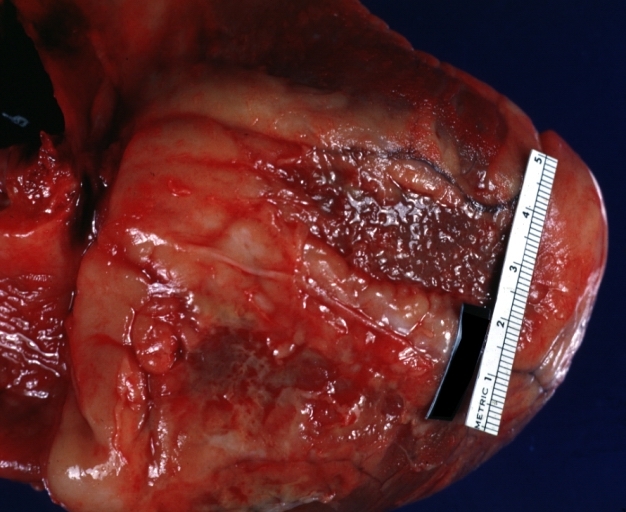 Fibrinous pericarditis: Gross, natural color, close-up view of minimal fibrinous exudate on epicardial surface due to terminal renal failure
Fibrinous pericarditis: Gross, natural color, close-up view of minimal fibrinous exudate on epicardial surface due to terminal renal failure -
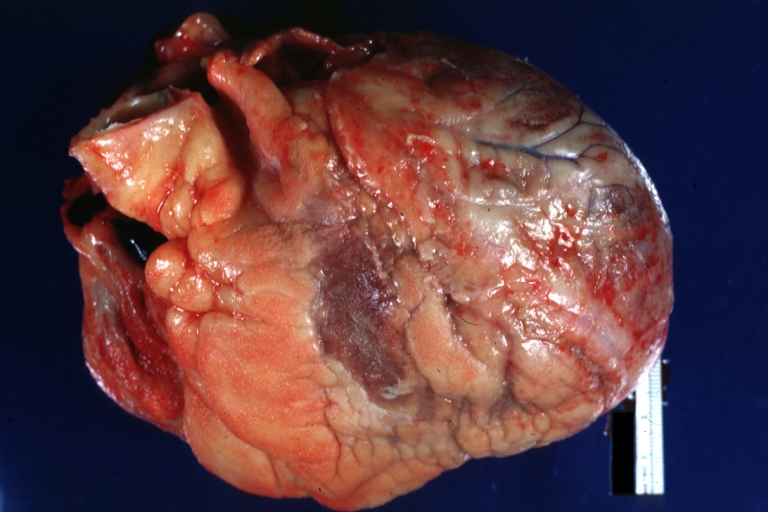 Fibrinous pericarditis: Gross, natural color, anterior view of heart with mild fibrinous exudate over epicardium due to terminal renal failure
Fibrinous pericarditis: Gross, natural color, anterior view of heart with mild fibrinous exudate over epicardium due to terminal renal failure




Microscopic Pathology
-
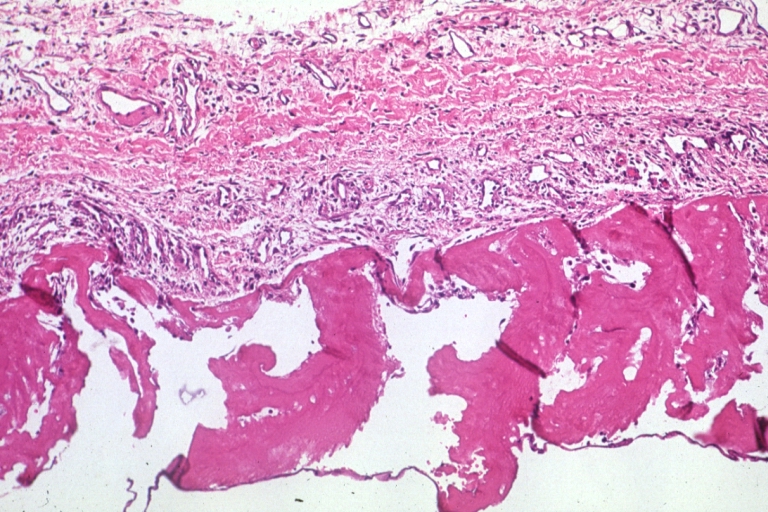 Uremic pericarditis: Micro med mag, H&E. A good example.
Uremic pericarditis: Micro med mag, H&E. A good example.

References
- ↑ Rutsky EA, Rostand SG (1987). “Treatment of uremic pericarditis and pericardial effusion”. Am J Kidney Dis. 10 (1): 2–8. PMID 3605080.
- ↑ Gunukula SR, Spodick DH (2001). “Pericardial disease in renal patients”. Semin Nephrol. 21 (1): 52–6. PMID 11172559.
Causes
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor-In-Chief: Varun Kumar, M.B.B.S.; Lakshmi Gopalakrishnan, M.B.B.S.
Overview
Disease name] may be caused by Chronic renal failure
OR
Common causes of [disease] include [cause1], [cause2], and [cause3].
OR
The most common cause of [disease name] is [cause 1]. Less common causes of [disease name] include [cause 2], [cause 3], and [cause 4].
OR
The cause of [disease name] has not been identified. To review risk factors for the development of [disease name], click here.
Causes
Life-threatening Causes
- Life-threatening causes include conditions which may result in death or permanent disability within 24 hours if left untreated. There are no life-threatening causes of disease name, however complications resulting from untreated disease name is common.
- Life-threatening causes of [symptom/manifestation] include [cause1], [cause2], and [cause3].
- [Cause] is a life-threatening cause of [disease].
Common Causes
Common causes of uremic pericarditis include:
- Chronic renal failure
- The causes of chronic renal failure include:
Less Common Causes
Less common causes of uremic pericarditis include less common causes of chronic renal failure that includes:
Causes by Organ System
| Cardiovascular | No underlying causes |
| Chemical/Poisoning | No underlying causes |
| Dental | No underlying causes |
| Dermatologic | No underlying causes |
| Drug Side Effect | No underlying causes |
| Ear Nose Throat | No underlying causes |
| Endocrine | No underlying causes |
| Environmental | No underlying causes |
| Gastroenterologic | No underlying causes |
| Genetic | No underlying causes |
| Hematologic | No underlying causes |
| Iatrogenic | No underlying causes |
| Infectious Disease | No underlying causes |
| Musculoskeletal/Orthopedic | No underlying causes |
| Neurologic | No underlying causes |
| Nutritional/Metabolic | No underlying causes |
| Obstetric/Gynecologic | No underlying causes |
| Oncologic | No underlying causes |
| Ophthalmologic | No underlying causes |
| Overdose/Toxicity | No underlying causes |
| Psychiatric | No underlying causes |
| Pulmonary | No underlying causes |
| Renal/Electrolyte | No underlying causes |
| Rheumatology/Immunology/Allergy | No underlying causes |
| Sexual | No underlying causes |
| Trauma | No underlying causes |
| Urologic | No underlying causes |
| Miscellaneous | No underlying causes |
Causes in Alphabetical Order
List the causes of the disease in alphabetical order:
- Cause 1
- Cause 2
- Cause 3
- Cause 4
- Cause 5
- Cause 6
- Cause 7
- Cause 8
- Cause 9
- Cause 10
References
Causes
- Absence of dialysis in renal failure
- Inadequate dialysis in renal failure
- Volume overload during dialysis
- Infections
References
Differentiating Uremic Pericarditis from other Diseases
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [2]; Associate Editor(s)-in-Chief: Syed Hassan A. Kazmi BSc, MD [3] Homa Najafi, M.D.[4]
Overview
Pericarditis must be differentiated from diseases presenting with chest pain, shortness of breath and tachypnea which include myocardial infarction, pulmonary embolism, congestive heart failure, pneumonia, vasculitis, and chronic obstructive pulmonary disease (COPD). Manifestation of the pericarditis can help in differentiation from myocardial infarction. Moreover, other differential diagnosis include aortic stenosis, coronary artery vasospasm, esophageal rupture, esophageal spasm, esophagitis,acute gastritis, gastroesophageal reflux disease, and peptic ulcer disease should be considered.
Differentiating Pericarditis from other Diseases
- Pericarditis must be differentiated from diseases presenting with chest pain, shortness of breath and tachypnea.
- For a full discussion of the differential diagnosis of chest pain click here
- For an expert algorithm that aids in the diagnosis of the cause of chest pain click here
- Pericarditis must be differentiated from myocardial infarction as an important cause of chest pain.The differentiating features include:[1]
| Characteristic/Parameter | Pericarditis | Myocardial infarction |
|---|---|---|
| Pain description | Sharp, pleuritic, retro-sternal (under the sternum) or left precordial (left chest) pain. | Crushing, pressure-like, heavy pain. Described as “elephant on the chest“. |
| Radiation | Pain radiates to the trapezius ridge (to the lowest portion of the scapula on the back) or no radiation. | Pain radiates to the jaw, or the left or arm, or does not radiate. |
| Exertion | Does not change the pain | Can increase the pain |
| Position | Pain is worse supine or upon inspiration (breathing in) | Not positional |
| Onset/duration | Sudden pain, that lasts for hours or sometimes days before a patient comes to the ER | Sudden or chronically worsening pain that can come and go in paroxysms or it can last for hours before the patient decides to come to the ER |
Differentiating pericarditis from other diseases on the basis of chest pain, shortness of breath, and tachypnea
The differentials include the following:[2][3][4][5][6][7][8][9][10][11][12][13][14][15][16][17][18][19][20][21]
| Diseases | Diagnostic tests | Physical Examination | Symptoms | Past medical history | Other Findings | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| CT scan and MRI | EKG | Chest X-ray | Tachypnea | Tachycardia | Fever | Chest Pain | Hemoptysis | Dyspnea on Exertion | Wheezing | Chest Tenderness | Nasalopharyngeal Ulceration | Carotid Bruit | |||
| Pulmonary embolism |
|
|
|
✔ | ✔ | ✔ (Low grade) | ✔ | ✔ (In case of massive PE) | ✔ | – | – | – | – |
|
|
| Congestive heart failure |
|
✔ | ✔ | ✔ | – | – | ✔ | – | – | – | – |
|
| ||
| Percarditis |
|
|
|
✔ | ✔ | ✔ (Low grade) | ✔ (Relieved by sitting up and leaning forward) | – | ✔ | – | – | – | – |
|
|
| Pneumonia |
|
|
|
✔ | ✔ | ✔ | ✔ | – | ✔ | ✔ | – | – | – |
|
|
| Vasculitis |
|
|
✔ | ✔ | ✔ | ✔ | ✔ | ✔ | – | ✔ | ✔ | ✔ |
|
||
| Chronic obstructive pulmonary disease (COPD) |
|
|
✔ | ✔ | – | – | – | ✔ | ✔ | – | – | – |
|
| |
Other differentials
Pericarditis also resembles the following disorders and needs to be differentiated from them:
- Angina pectoris
- Aortic stenosis
- Coronary artery vasospasm
- Esophageal rupture
- Esophageal spasm
- Esophagitis
- Gastritis, acute
- Gastroesophageal reflux disease
- Peptic ulcer disease
References
- ↑ American College of Physicians (ACP). Medical Knowledge Self-Assessment Program (MKSAP-15): Cardiovascular Medicine. “Pericardial disease.” p. 64. ISBN 978-934465-28-8 [1]
- ↑ Brenes-Salazar JA (2014). “Westermark’s and Palla’s signs in acute and chronic pulmonary embolism: Still valid in the current computed tomography era”. J Emerg Trauma Shock. 7 (1): 57–8. doi:10.4103/0974-2700.125645. PMC 3912657. PMID 24550636.
- ↑ “CT Angiography of Pulmonary Embolism: Diagnostic Criteria and Causes of Misdiagnosis | RadioGraphics”.
- ↑ Bĕlohlávek J, Dytrych V, Linhart A (2013). “Pulmonary embolism, part I: Epidemiology, risk factors and risk stratification, pathophysiology, clinical presentation, diagnosis and nonthrombotic pulmonary embolism”. Exp Clin Cardiol. 18 (2): 129–38. PMC 3718593. PMID 23940438.
- ↑ “Pulmonary Embolism: Symptoms – National Library of Medicine – PubMed Health”.
- ↑ Ramani GV, Uber PA, Mehra MR (2010). “Chronic heart failure: contemporary diagnosis and management”. Mayo Clin. Proc. 85 (2): 180–95. doi:10.4065/mcp.2009.0494. PMC 2813829. PMID 20118395.
- ↑ Blinderman CD, Homel P, Billings JA, Portenoy RK, Tennstedt SL (2008). “Symptom distress and quality of life in patients with advanced congestive heart failure”. J Pain Symptom Manage. 35 (6): 594–603. doi:10.1016/j.jpainsymman.2007.06.007. PMC 2662445. PMID 18215495.
- ↑ Hawkins NM, Petrie MC, Jhund PS, Chalmers GW, Dunn FG, McMurray JJ (2009). “Heart failure and chronic obstructive pulmonary disease: diagnostic pitfalls and epidemiology”. Eur. J. Heart Fail. 11 (2): 130–9. doi:10.1093/eurjhf/hfn013. PMC 2639415. PMID 19168510.
- ↑ Takasugi JE, Godwin JD (1998). “Radiology of chronic obstructive pulmonary disease”. Radiol. Clin. North Am. 36 (1): 29–55. PMID 9465867.
- ↑ Wedzicha JA, Donaldson GC (2003). “Exacerbations of chronic obstructive pulmonary disease”. Respir Care. 48 (12): 1204–13, discussion 1213–5. PMID 14651761.
- ↑ Nakawah MO, Hawkins C, Barbandi F (2013). “Asthma, chronic obstructive pulmonary disease (COPD), and the overlap syndrome”. J Am Board Fam Med. 26 (4): 470–7. doi:10.3122/jabfm.2013.04.120256. PMID 23833163.
- ↑ Khandaker MH, Espinosa RE, Nishimura RA, Sinak LJ, Hayes SN, Melduni RM, Oh JK (2010). “Pericardial disease: diagnosis and management”. Mayo Clin. Proc. 85 (6): 572–93. doi:10.4065/mcp.2010.0046. PMC 2878263. PMID 20511488.
- ↑ Bogaert J, Francone M (2013). “Pericardial disease: value of CT and MR imaging”. Radiology. 267 (2): 340–56. doi:10.1148/radiol.13121059. PMID 23610095.
- ↑ Gharib AM, Stern EJ (2001). “Radiology of pneumonia”. Med. Clin. North Am. 85 (6): 1461–91, x. PMID 11680112.
- ↑ Schmidt WA (2013). “Imaging in vasculitis”. Best Pract Res Clin Rheumatol. 27 (1): 107–18. doi:10.1016/j.berh.2013.01.001. PMID 23507061.
- ↑ Suresh E (2006). “Diagnostic approach to patients with suspected vasculitis”. Postgrad Med J. 82 (970): 483–8. doi:10.1136/pgmj.2005.042648. PMC 2585712. PMID 16891436.
- ↑ Stein PD, Dalen JE, McIntyre KM, Sasahara AA, Wenger NK, Willis PW (1975). “The electrocardiogram in acute pulmonary embolism”. Prog Cardiovasc Dis. 17 (4): 247–57. PMID 123074.
- ↑ Warnier MJ, Rutten FH, Numans ME, Kors JA, Tan HL, de Boer A, Hoes AW, De Bruin ML (2013). “Electrocardiographic characteristics of patients with chronic obstructive pulmonary disease”. COPD. 10 (1): 62–71. doi:10.3109/15412555.2012.727918. PMID 23413894.
- ↑ Stein PD, Matta F, Ekkah M, Saleh T, Janjua M, Patel YR, Khadra H (2012). “Electrocardiogram in pneumonia”. Am. J. Cardiol. 110 (12): 1836–40. doi:10.1016/j.amjcard.2012.08.019. PMID 23000104.
- ↑ Hazebroek MR, Kemna MJ, Schalla S, Sanders-van Wijk S, Gerretsen SC, Dennert R, Merken J, Kuznetsova T, Staessen JA, Brunner-La Rocca HP, van Paassen P, Cohen Tervaert JW, Heymans S (2015). “Prevalence and prognostic relevance of cardiac involvement in ANCA-associated vasculitis: eosinophilic granulomatosis with polyangiitis and granulomatosis with polyangiitis”. Int. J. Cardiol. 199: 170–9. doi:10.1016/j.ijcard.2015.06.087. PMID 26209947.
- ↑ Dennert RM, van Paassen P, Schalla S, Kuznetsova T, Alzand BS, Staessen JA, Velthuis S, Crijns HJ, Tervaert JW, Heymans S (2010). “Cardiac involvement in Churg-Strauss syndrome”. Arthritis Rheum. 62 (2): 627–34. doi:10.1002/art.27263. PMID 20112390.
Epidemiology and Demographics
Please help WikiDoc by adding more content here. It’s easy! Click here to learn about editing.
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor-In-Chief: Varun Kumar, M.B.B.S.; Lakshmi Gopalakrishnan, M.B.B.S.
Epidemiology and Demographics
Pericarditis in renal failure occurs in approximately in 13 percent of patients who are on maintenance hemodialysis[1]. Hyperurcemia due to inadequate dialysis or fluid overload may be the reason for pericarditis[2].
Uremic pericarditis can occur as a serous or a hemorrhagic effusion with considerable overlapping. Hemorrhagic effusions are more common secondary to uremia induced platelet dysfunction and the use of anticoagulation during hemodialysis.
Dialysis associated pericarditis may also be secondary to bacterial or viral infections[3].
References
- ↑ Rutsky EA, Rostand SG (1987). “Treatment of uremic pericarditis and pericardial effusion”. Am J Kidney Dis. 10 (1): 2–8. PMID 3605080.
- ↑ Lundin, AP. Recurrent uremic pericarditis: A marker of inadequate dialysis. Semin Dial 1990; 3:5.
- ↑ Gunukula SR, Spodick DH (2001). “Pericardial disease in renal patients”. Semin Nephrol. 21 (1): 52–6. PMID 11172559.
Natural History, Complications and Prognosis
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor-In-Chief: Varun Kumar, M.B.B.S.; Lakshmi Gopalakrishnan, M.B.B.S.
Overview
If left untreated, [#]% of patients with [disease name] may progress to develop [manifestation 1], [manifestation 2], and [manifestation 3].
OR
Common complications of [disease name] include [complication 1], [complication 2], and [complication 3].
OR
Prognosis is generally excellent/good/poor, and the 1/5/10-year mortality/survival rate of patients with [disease name] is approximately [#]%.
Natural History, Complications, and Prognosis
Natural History
- The symptoms of (disease name) usually develop in the first/ second/ third decade of life, and start with symptoms such as ___.
- The symptoms of (disease name) typically develop ___ years after exposure to ___.
- If left untreated, [#]% of patients with [disease name] may progress to develop [manifestation 1], [manifestation 2], and [manifestation 3].
Complications
Click on the blue links below to read more about specific complications of uremic pericarditis:
Uremic pericarditis often can be complicated by significant fluid buildup around the heart, a condition known as a pericardial effusion.
If the fluid accumulates too rapidly or is too large, then cardiac tamponade, a condition in which the heart is compressed by the fluid and cannot pump enough blood forward may occur. Cardiac tamponade may require urgent intervention including pericardiocentesis. This complication is more common in patients with specific underlying etiologies such as malignancy, tuberculosis[1], or purulent pericarditis and rarely occurs in idiopathic pericarditis.
If scarring of the sac around the heart (the pericardium) occurs, then this is called constrictive pericarditis which may require surgical stripping of the scar (pericardiectomy).
Uremic pericarditis may lead to hemorrhagic pericarditis and is associated with significant morbidity and poor prognosis[2].
Prognosis
- Prognosis is generally excellent/good/poor, and the 1/5/10-year mortality/survival rate of patients with [disease name] is approximately [–]%.
- Depending on the extent of the [tumor/disease progression] at the time of diagnosis, the prognosis may vary. However, the prognosis is generally regarded as poor/good/excellent.
- The presence of [characteristic of disease] is associated with a particularly [good/poor] prognosis among patients with [disease/malignancy].
- [Subtype of disease/malignancy] is associated with the most favorable prognosis.
- The prognosis varies with the [characteristic] of tumor; [subtype of disease/malignancy] have the most favorable prognosis.
References
- ↑ Mayosi BM, Burgess LJ, Doubell AF (2005). “Tuberculous pericarditis”. Circulation. 112 (23): 3608–16. doi:10.1161/CIRCULATIONAHA.105.543066. PMID 16330703.
- ↑ Nicholls, AJ. Heart and Circulation. In: Handbook of Dialysis, Daugirdas, JT, Ing, TS (Eds), Little, Brown and Co., New York 1994. p.149.
Diagnosis
Diagnosis
History and Symptoms | Physical Examination | Laboratory Findings | Electrocardiogram | Chest X ray | Echocardiography | CT | MRI | Cardiac Catheterization
Treatment
Treatment
Overview | Medical Therapy | Pericardiocentesis | Pericardial Window | Pericardiectomy Template:WH Template:WS
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor-In-Chief: Varun Kumar, M.B.B.S.; Lakshmi Gopalakrishnan, M.B.B.S.
Treatment
- Patient with uremic pericarditis should be treated with intensive hemodialysis which would most often results in resolution of pericardial effusion and chest pain[1][2]within 1-2 weeks. Pericardiocentesis can be done to drain effusion if it is causing hemodynamic compromise such as in cardiac tamponade. Use of heparin free hemodialysis is adviced to prevent development of hemopericardium.
- Hypokalemia and hypophosphatemia should be prevented by supplementing the dialysis solution when appropriate[3].
- NSAIDs may be used in treatment of chest pain secondary to pericarditis. In case of recurrent pericardial effusion, pericardiotomy where a pericardial window for drainage of effusion may be made. In large refractory effusion, intra pericardial instillation of non-absorbable corticosteroids may be considered[4][5].
- Pericardiectomy should be done in refractory and severely symptomatic patients.
- Appropriate antivirals or antibiotics should be used in treatment of infective pericarditis which may occur in immunocompromised states resulting after renal transplantation[6].
References
- ↑ Maisch B, Seferović PM, Ristić AD, Erbel R, Rienmüller R, Adler Y; et al. (2004). “Guidelines on the diagnosis and management of pericardial diseases executive summary; The Task force on the diagnosis and management of pericardial diseases of the European society of cardiology”. Eur Heart J. 25 (7): 587–610. doi:10.1016/j.ehj.2004.02.002. PMID 15120056.
- ↑ Maisch B, Ristić AD (2003). “Practical aspects of the management of pericardial disease”. Heart. 89 (9): 1096–103. PMC 1767862. PMID 12923044.
- ↑ Emelife-Obi C, Chow MT, Qamar-Rohail H, Leehey DJ, Gandhi VC, Ing TS (1998). “Use of a phosphorus-enriched hemodialysate to prevent hypophosphatemia in a patient with renal failure-related pericarditis”. Clin Nephrol. 50 (2): 131–3. PMID 9725787.
- ↑ Wood JE, Mahnensmith RL (2001). “Pericarditis associated with renal failure: evolution and management”. Semin Dial. 14 (1): 61–6. PMID 11208042.
- ↑ Rutsky EA, Rostand SG (1987). “Treatment of uremic pericarditis and pericardial effusion”. Am J Kidney Dis. 10 (1): 2–8. PMID 3605080.
- ↑ Sever MS, Steinmuller DR, Hayes JM, Streem SB, Novick AC (1991). “Pericarditis following renal transplantation”. Transplantation. 51 (6): 1229–32. PMID 1646505.
[[Category:Up-To-Date cardiology]
Looking for the patient version?
© 2026 MyEClinic – IFTM Institut für Telematik in der Medizin GmbH