
Pericarditis in malignancy
For patient information click here
To go back to the main page on Pericarditis, click here.
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor-In-Chief: Varun Kumar, M.B.B.S.; Lakshmi Gopalakrishnan, M.B.B.S.
Synonyms and keywords: Neoplastic pericarditis; malignant pericarditis
Overview
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor-In-Chief: Varun Kumar, M.B.B.S.; Lakshmi Gopalakrishnan, M.B.B.S.
Overview
Many malignant neoplasms such as lung cancer, breast cancer, esophageal cancer, lymphomas, melanomas, kaposi’s sarcoma and leukemias may metastasize to pericardium causing pericarditis, effusion, cardiac tamponade and pericardial constriction. Malignant pericardial effusion is seen in approximately 50-60% of patients presenting with pericardial effusion who have a history of malignancy.[1][2] Among patients presenting with pericarditis or pericardial effusion with no history of malignancy, undiagnosed underlying malignancy was detected in 4-7%.[3][4][5]
Malignancy related pericardial disease can manifest as pericarditis, pericardial effusion, cardiac tamponade or pericardial constriction.
Pathophysiology
The pericardium may be involved by direct local spread from neoplasms such as breast and lung carcinomas or by metastatic spread via blood stream and lymphatics as in melanomas, lymphomas and leukemias.
Pericardial effusion in such situations may occur either secondary to pericardial inflammation or obstruction of lymphatic drainage by enlarged mediastinal nodes.[6][7][5]
References
- ↑ Gornik HL, Gerhard-Herman M, Beckman JA (2005). “Abnormal cytology predicts poor prognosis in cancer patients with pericardial effusion”. J Clin Oncol. 23 (22): 5211–6. doi:10.1200/JCO.2005.00.745. PMID 16051963.
- ↑ Porte HL, Janecki-Delebecq TJ, Finzi L, Métois DG, Millaire A, Wurtz AJ (1999). “Pericardoscopy for primary management of pericardial effusion in cancer patients”. Eur J Cardiothorac Surg. 16 (3): 287–91. PMID 10554845.
- ↑ Permanyer-Miralda G, Sagristá-Sauleda J, Soler-Soler J (1985). “Primary acute pericardial disease: a prospective series of 231 consecutive patients”. Am J Cardiol. 56 (10): 623–30. PMID 4050698.
- ↑ Imazio M, Cecchi E, Demichelis B, Ierna S, Demarie D, Ghisio A; et al. (2007). “Indicators of poor prognosis of acute pericarditis”. Circulation. 115 (21): 2739–44. doi:10.1161/CIRCULATIONAHA.106.662114. PMID 17502574.
- ↑ 5.0 5.1 Imazio M, Demichelis B, Parrini I, Favro E, Beqaraj F, Cecchi E; et al. (2005). “Relation of acute pericardial disease to malignancy”. Am J Cardiol. 95 (11): 1393–4. doi:10.1016/j.amjcard.2005.01.094. PMID 15904655.
- ↑ Maisch B, Seferović PM, Ristić AD, Erbel R, Rienmüller R, Adler Y; et al. (2004). “Guidelines on the diagnosis and management of pericardial diseases executive summary; The Task force on the diagnosis and management of pericardial diseases of the European society of cardiology”. Eur Heart J. 25 (7): 587–610. doi:10.1016/j.ehj.2004.02.002. PMID 15120056.
- ↑ Ben-Horin S, Bank I, Guetta V, Livneh A (2006). “Large symptomatic pericardial effusion as the presentation of unrecognized cancer: a study in 173 consecutive patients undergoing pericardiocentesis”. Medicine (Baltimore). 85 (1): 49–53. doi:10.1097/01.md.0000199556.69588.8e. PMID 16523053.
Pathophysiology
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor-In-Chief: Varun Kumar, M.B.B.S.; Lakshmi Gopalakrishnan, M.B.B.S.
Overview
The pericardium may be involved by direct local spread from neoplasms such as breast and lung carcinomas or by metastatic spread via blood stream and lymphatics as in melanomas, lymphomas and leukemias.
Pericardial effusion in such situations may occur either secondary to pericardial inflammation or obstruction of lymphatic drainage by enlarged mediastinal nodes.[1][2][3]
Pathophysiology
Gross Pathology
-
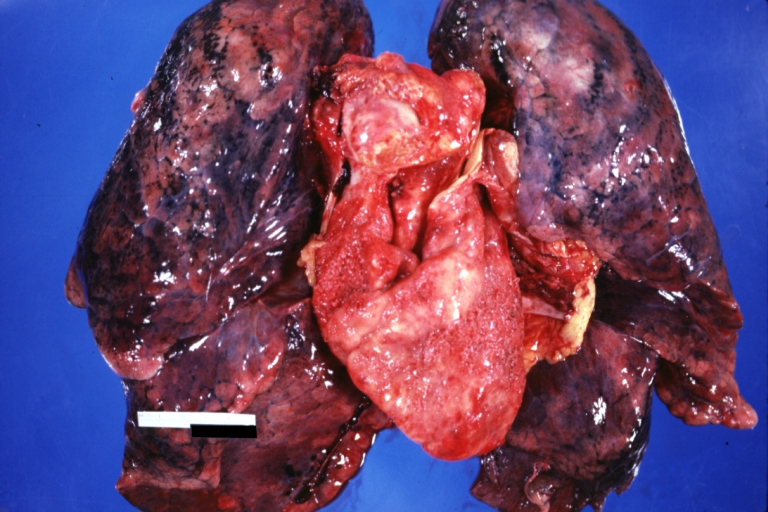 Neoplastic pericarditis: Gross, natural color, shaggy pericarditis. Primer is adenocarcinoma of the lung.
Neoplastic pericarditis: Gross, natural color, shaggy pericarditis. Primer is adenocarcinoma of the lung.

Microscopic Pathology
-
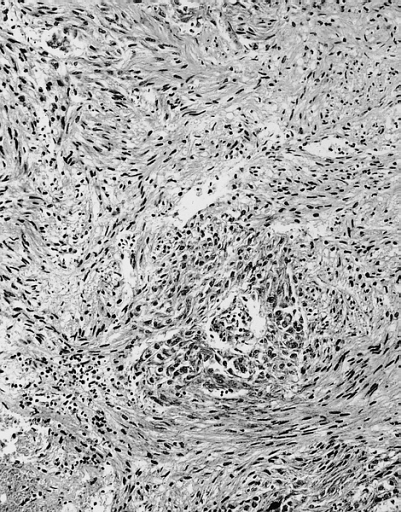 Malignant Mesothelioma, Biphasic Type: Pericardium: This tumor has epithelioid cells (lower half) surrounded by spindled cells. The patient was a 46-year-old woman with constrictive pericarditis; the pericardium was studded with coalescing tumor nodules.
Malignant Mesothelioma, Biphasic Type: Pericardium: This tumor has epithelioid cells (lower half) surrounded by spindled cells. The patient was a 46-year-old woman with constrictive pericarditis; the pericardium was studded with coalescing tumor nodules.

References
- ↑ Maisch B, Seferović PM, Ristić AD, Erbel R, Rienmüller R, Adler Y; et al. (2004). “Guidelines on the diagnosis and management of pericardial diseases executive summary; The Task force on the diagnosis and management of pericardial diseases of the European society of cardiology”. Eur Heart J. 25 (7): 587–610. doi:10.1016/j.ehj.2004.02.002. PMID 15120056.
- ↑ Ben-Horin S, Bank I, Guetta V, Livneh A (2006). “Large symptomatic pericardial effusion as the presentation of unrecognized cancer: a study in 173 consecutive patients undergoing pericardiocentesis”. Medicine (Baltimore). 85 (1): 49–53. doi:10.1097/01.md.0000199556.69588.8e. PMID 16523053.
- ↑ Imazio M, Demichelis B, Parrini I, Favro E, Beqaraj F, Cecchi E; et al. (2005). “Relation of acute pericardial disease to malignancy”. Am J Cardiol. 95 (11): 1393–4. doi:10.1016/j.amjcard.2005.01.094. PMID 15904655.
Causes
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor-In-Chief: Varun Kumar, M.B.B.S.; Lakshmi Gopalakrishnan, M.B.B.S.
Causes
In Alphabetical Orrder
- Adenocarcinoma
- Angiosarcoma
- Burkitt lymphoma
- Fibrosarcoma
- Ganglioneuroblastoma
- High-grade sarcomas
- Hodgkin lymphoma
- Intrapericardial teratoma in the fetus and neonate
- Kaposi sarcoma and primary cardiac lymphoma in association with human immunodeficiency virus (HIV) infection
- Leiomyosarcomas
- Liposarcoma
- Liposarcomas
- Lymphoma
- Malignant pericardial teratoma
- Neuroblastoma
- Non-Hodgkin lymphoma
- Pericardial mesothelioma
- Pheochromocytoma
- Pheochromocytoma
- Primary mediastinal (thymic) B-cell lymphoma
- Rhabdomyosarcoma with tuberous sclerosis
- Sarcomas
- Wilms tumor
References
Differentiating Pericarditis in malignancy from other Diseases
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [2]; Associate Editor(s)-in-Chief: Syed Hassan A. Kazmi BSc, MD [3] Homa Najafi, M.D.[4]
Overview
Pericarditis must be differentiated from diseases presenting with chest pain, shortness of breath and tachypnea which include myocardial infarction, pulmonary embolism, congestive heart failure, pneumonia, vasculitis, and chronic obstructive pulmonary disease (COPD). Manifestation of the pericarditis can help in differentiation from myocardial infarction. Moreover, other differential diagnosis include aortic stenosis, coronary artery vasospasm, esophageal rupture, esophageal spasm, esophagitis,acute gastritis, gastroesophageal reflux disease, and peptic ulcer disease should be considered.
Differentiating Pericarditis from other Diseases
- Pericarditis must be differentiated from diseases presenting with chest pain, shortness of breath and tachypnea.
- For a full discussion of the differential diagnosis of chest pain click here
- For an expert algorithm that aids in the diagnosis of the cause of chest pain click here
- Pericarditis must be differentiated from myocardial infarction as an important cause of chest pain.The differentiating features include:[1]
| Characteristic/Parameter | Pericarditis | Myocardial infarction |
|---|---|---|
| Pain description | Sharp, pleuritic, retro-sternal (under the sternum) or left precordial (left chest) pain. | Crushing, pressure-like, heavy pain. Described as “elephant on the chest“. |
| Radiation | Pain radiates to the trapezius ridge (to the lowest portion of the scapula on the back) or no radiation. | Pain radiates to the jaw, or the left or arm, or does not radiate. |
| Exertion | Does not change the pain | Can increase the pain |
| Position | Pain is worse supine or upon inspiration (breathing in) | Not positional |
| Onset/duration | Sudden pain, that lasts for hours or sometimes days before a patient comes to the ER | Sudden or chronically worsening pain that can come and go in paroxysms or it can last for hours before the patient decides to come to the ER |
Differentiating pericarditis from other diseases on the basis of chest pain, shortness of breath, and tachypnea
The differentials include the following:[2][3][4][5][6][7][8][9][10][11][12][13][14][15][16][17][18][19][20][21]
| Diseases | Diagnostic tests | Physical Examination | Symptoms | Past medical history | Other Findings | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| CT scan and MRI | EKG | Chest X-ray | Tachypnea | Tachycardia | Fever | Chest Pain | Hemoptysis | Dyspnea on Exertion | Wheezing | Chest Tenderness | Nasalopharyngeal Ulceration | Carotid Bruit | |||
| Pulmonary embolism |
|
|
|
✔ | ✔ | ✔ (Low grade) | ✔ | ✔ (In case of massive PE) | ✔ | – | – | – | – |
|
|
| Congestive heart failure |
|
✔ | ✔ | ✔ | – | – | ✔ | – | – | – | – |
|
| ||
| Percarditis |
|
|
|
✔ | ✔ | ✔ (Low grade) | ✔ (Relieved by sitting up and leaning forward) | – | ✔ | – | – | – | – |
|
|
| Pneumonia |
|
|
|
✔ | ✔ | ✔ | ✔ | – | ✔ | ✔ | – | – | – |
|
|
| Vasculitis |
|
|
✔ | ✔ | ✔ | ✔ | ✔ | ✔ | – | ✔ | ✔ | ✔ |
|
||
| Chronic obstructive pulmonary disease (COPD) |
|
|
✔ | ✔ | – | – | – | ✔ | ✔ | – | – | – |
|
| |
Other differentials
Pericarditis also resembles the following disorders and needs to be differentiated from them:
- Angina pectoris
- Aortic stenosis
- Coronary artery vasospasm
- Esophageal rupture
- Esophageal spasm
- Esophagitis
- Gastritis, acute
- Gastroesophageal reflux disease
- Peptic ulcer disease
References
- ↑ American College of Physicians (ACP). Medical Knowledge Self-Assessment Program (MKSAP-15): Cardiovascular Medicine. “Pericardial disease.” p. 64. ISBN 978-934465-28-8 [1]
- ↑ Brenes-Salazar JA (2014). “Westermark’s and Palla’s signs in acute and chronic pulmonary embolism: Still valid in the current computed tomography era”. J Emerg Trauma Shock. 7 (1): 57–8. doi:10.4103/0974-2700.125645. PMC 3912657. PMID 24550636.
- ↑ “CT Angiography of Pulmonary Embolism: Diagnostic Criteria and Causes of Misdiagnosis | RadioGraphics”.
- ↑ Bĕlohlávek J, Dytrych V, Linhart A (2013). “Pulmonary embolism, part I: Epidemiology, risk factors and risk stratification, pathophysiology, clinical presentation, diagnosis and nonthrombotic pulmonary embolism”. Exp Clin Cardiol. 18 (2): 129–38. PMC 3718593. PMID 23940438.
- ↑ “Pulmonary Embolism: Symptoms – National Library of Medicine – PubMed Health”.
- ↑ Ramani GV, Uber PA, Mehra MR (2010). “Chronic heart failure: contemporary diagnosis and management”. Mayo Clin. Proc. 85 (2): 180–95. doi:10.4065/mcp.2009.0494. PMC 2813829. PMID 20118395.
- ↑ Blinderman CD, Homel P, Billings JA, Portenoy RK, Tennstedt SL (2008). “Symptom distress and quality of life in patients with advanced congestive heart failure”. J Pain Symptom Manage. 35 (6): 594–603. doi:10.1016/j.jpainsymman.2007.06.007. PMC 2662445. PMID 18215495.
- ↑ Hawkins NM, Petrie MC, Jhund PS, Chalmers GW, Dunn FG, McMurray JJ (2009). “Heart failure and chronic obstructive pulmonary disease: diagnostic pitfalls and epidemiology”. Eur. J. Heart Fail. 11 (2): 130–9. doi:10.1093/eurjhf/hfn013. PMC 2639415. PMID 19168510.
- ↑ Takasugi JE, Godwin JD (1998). “Radiology of chronic obstructive pulmonary disease”. Radiol. Clin. North Am. 36 (1): 29–55. PMID 9465867.
- ↑ Wedzicha JA, Donaldson GC (2003). “Exacerbations of chronic obstructive pulmonary disease”. Respir Care. 48 (12): 1204–13, discussion 1213–5. PMID 14651761.
- ↑ Nakawah MO, Hawkins C, Barbandi F (2013). “Asthma, chronic obstructive pulmonary disease (COPD), and the overlap syndrome”. J Am Board Fam Med. 26 (4): 470–7. doi:10.3122/jabfm.2013.04.120256. PMID 23833163.
- ↑ Khandaker MH, Espinosa RE, Nishimura RA, Sinak LJ, Hayes SN, Melduni RM, Oh JK (2010). “Pericardial disease: diagnosis and management”. Mayo Clin. Proc. 85 (6): 572–93. doi:10.4065/mcp.2010.0046. PMC 2878263. PMID 20511488.
- ↑ Bogaert J, Francone M (2013). “Pericardial disease: value of CT and MR imaging”. Radiology. 267 (2): 340–56. doi:10.1148/radiol.13121059. PMID 23610095.
- ↑ Gharib AM, Stern EJ (2001). “Radiology of pneumonia”. Med. Clin. North Am. 85 (6): 1461–91, x. PMID 11680112.
- ↑ Schmidt WA (2013). “Imaging in vasculitis”. Best Pract Res Clin Rheumatol. 27 (1): 107–18. doi:10.1016/j.berh.2013.01.001. PMID 23507061.
- ↑ Suresh E (2006). “Diagnostic approach to patients with suspected vasculitis”. Postgrad Med J. 82 (970): 483–8. doi:10.1136/pgmj.2005.042648. PMC 2585712. PMID 16891436.
- ↑ Stein PD, Dalen JE, McIntyre KM, Sasahara AA, Wenger NK, Willis PW (1975). “The electrocardiogram in acute pulmonary embolism”. Prog Cardiovasc Dis. 17 (4): 247–57. PMID 123074.
- ↑ Warnier MJ, Rutten FH, Numans ME, Kors JA, Tan HL, de Boer A, Hoes AW, De Bruin ML (2013). “Electrocardiographic characteristics of patients with chronic obstructive pulmonary disease”. COPD. 10 (1): 62–71. doi:10.3109/15412555.2012.727918. PMID 23413894.
- ↑ Stein PD, Matta F, Ekkah M, Saleh T, Janjua M, Patel YR, Khadra H (2012). “Electrocardiogram in pneumonia”. Am. J. Cardiol. 110 (12): 1836–40. doi:10.1016/j.amjcard.2012.08.019. PMID 23000104.
- ↑ Hazebroek MR, Kemna MJ, Schalla S, Sanders-van Wijk S, Gerretsen SC, Dennert R, Merken J, Kuznetsova T, Staessen JA, Brunner-La Rocca HP, van Paassen P, Cohen Tervaert JW, Heymans S (2015). “Prevalence and prognostic relevance of cardiac involvement in ANCA-associated vasculitis: eosinophilic granulomatosis with polyangiitis and granulomatosis with polyangiitis”. Int. J. Cardiol. 199: 170–9. doi:10.1016/j.ijcard.2015.06.087. PMID 26209947.
- ↑ Dennert RM, van Paassen P, Schalla S, Kuznetsova T, Alzand BS, Staessen JA, Velthuis S, Crijns HJ, Tervaert JW, Heymans S (2010). “Cardiac involvement in Churg-Strauss syndrome”. Arthritis Rheum. 62 (2): 627–34. doi:10.1002/art.27263. PMID 20112390.
Epidemiology and Demographics
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor-In-Chief: Varun Kumar, M.B.B.S.; Lakshmi Gopalakrishnan, M.B.B.S.
Epidemiology and Demographics
In developed countries malignancy is the leading cause of cardiac tamponade secondary to pericardial effusion. Malignant pericardial effusion is seen in approximately 50-60% of patients presenting with pericardial effusion who have history of malignancy.[1][2] Among patients presenting with pericarditis or pericardial effusion with no history of malignancy, undiagnosed underlying malignancy was detected in 4-7%.[3][4][5]
Carcinoma of the lung is the most common cause for pericardial effusion in malignancy accounting for approximately 40%. Another 40% of cases could be due to breast carcinoma and lymphomas. Carcinoma of GI tract, melanoma, sarcomas, and other neoplastic diseases are less common.
Kaposi sarcoma and lymphomas associated with HIV were other neoplastic causes of pericardial effusion which accounted for 5% and 7% respectively[6] in one study and 15% together[7] in another series. However, with the use of antiretroviral agents, the incidence of Kaposi carcinoma and subsequent pericardial effusion has considerably decreased.
In regions where tuberculosis is not highly prevalent, malignancy may be the most common cause of a hemorrhagic effusion.[8][9]
Sex
Higher incidence of the pericardial effusion related to malignancy is observed among males with ratio of 7:3 as reported in a series.[10]
References
- ↑ Gornik HL, Gerhard-Herman M, Beckman JA (2005). “Abnormal cytology predicts poor prognosis in cancer patients with pericardial effusion”. J Clin Oncol. 23 (22): 5211–6. doi:10.1200/JCO.2005.00.745. PMID 16051963.
- ↑ Porte HL, Janecki-Delebecq TJ, Finzi L, Métois DG, Millaire A, Wurtz AJ (1999). “Pericardoscopy for primary management of pericardial effusion in cancer patients”. Eur J Cardiothorac Surg. 16 (3): 287–91. PMID 10554845.
- ↑ Permanyer-Miralda G, Sagristá-Sauleda J, Soler-Soler J (1985). “Primary acute pericardial disease: a prospective series of 231 consecutive patients”. Am J Cardiol. 56 (10): 623–30. PMID 4050698.
- ↑ Imazio M, Cecchi E, Demichelis B, Ierna S, Demarie D, Ghisio A; et al. (2007). “Indicators of poor prognosis of acute pericarditis”. Circulation. 115 (21): 2739–44. doi:10.1161/CIRCULATIONAHA.106.662114. PMID 17502574.
- ↑ Imazio M, Demichelis B, Parrini I, Favro E, Beqaraj F, Cecchi E; et al. (2005). “Relation of acute pericardial disease to malignancy”. Am J Cardiol. 95 (11): 1393–4. doi:10.1016/j.amjcard.2005.01.094. PMID 15904655.
- ↑ Chen Y, Brennessel D, Walters J, Johnson M, Rosner F, Raza M (1999). “Human immunodeficiency virus-associated pericardial effusion: report of 40 cases and review of the literature”. Am Heart J. 137 (3): 516–21. PMID 10047635.
- ↑ Gowda RM, Khan IA, Mehta NJ, Gowda MR, Sacchi TJ, Vasavada BC (2003). “Cardiac tamponade in patients with human immunodeficiency virus disease”. Angiology. 54 (4): 469–74. PMID 12934767.
- ↑ Maisch B, Ristic A, Pankuweit S (2010). “Evaluation and management of pericardial effusion in patients with neoplastic disease”. Prog Cardiovasc Dis. 53 (2): 157–63. doi:10.1016/j.pcad.2010.06.003. PMID 20728703.
- ↑ Atar S, Chiu J, Forrester JS, Siegel RJ (1999). “Bloody pericardial effusion in patients with cardiac tamponade: is the cause cancerous, tuberculous, or iatrogenic in the 1990s?”. Chest. 116 (6): 1564–9. PMID 10593777.
- ↑ Medary I, Steinherz LJ, Aronson DC, La Quaglia MP (1996). “Cardiac tamponade in the pediatric oncology population: treatment by percutaneous catheter drainage”. J Pediatr Surg. 31 (1): 197–9, discussion 199-200. PMID 8632279.
Natural History, Complications and Prognosis
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor-In-Chief: Varun Kumar, M.B.B.S.; Lakshmi Gopalakrishnan, M.B.B.S.
Please help WikiDoc by adding more content here. It’s easy! Click here to learn about editing.
Prognosis
Guarded prognosis associated with malignancies is worsened by pericardial effusion and cardiac tamponade. Children may have poor prognosis and thus, prompt detection and treatment of cardiac tamponade improves survival.[1][2]
Patients rarely present with cardiac tamponade as their first presentation. Superior vena cava syndrome may occur in some patients secondary to either a coexisting tumor or rapid accumulation of pericardial effusion.[3]
Prognosis of symptomatic malignant pericardial disease is grave with a short life expectancy of 2-4 months.[4][5][6][7] While the patients with hematologic[8] or breast cancer,[9] or those in whom malignant cells are not present in the pericardium[10] have a better prognosis in comparison to those with solid tumors, lung cancer,[11] etc.
References
- ↑ Ben-Horin S, Bank I, Guetta V, Livneh A (2006). “Large symptomatic pericardial effusion as the presentation of unrecognized cancer: a study in 173 consecutive patients undergoing pericardiocentesis”. Medicine (Baltimore). 85 (1): 49–53. doi:10.1097/01.md.0000199556.69588.8e. PMID 16523053.
- ↑ Bień E, Stefanowicz J, Aleszewicz-Baranowska J, Połczyńska K, Szołkiewicz A, Stachowicz-Stencel T; et al. (2005). “[Cardio-vascular disorders at the time of diagnosis of malignant solid tumours in children–own experiences]”. Med Wieku Rozwoj. 9 (3 Pt 2): 551–9. PMID 16719168.
- ↑ Tsai MH, Yang CP, Chung HT, Shih LY (2009). “Acute myeloid leukemia in a young girl presenting with mediastinal granulocytic sarcoma invading pericardium and causing superior vena cava syndrome”. J Pediatr Hematol Oncol. 31 (12): 980–2. doi:10.1097/MPH.0b013e3181b86ff3. PMID 19956024.
- ↑ Tsang TS, Seward JB, Barnes ME, Bailey KR, Sinak LJ, Urban LH; et al. (2000). “Outcomes of primary and secondary treatment of pericardial effusion in patients with malignancy”. Mayo Clin Proc. 75 (3): 248–53. PMID 10725950.
- ↑ Gross JL, Younes RN, Deheinzelin D, Diniz AL, Silva RA, Haddad FJ (2006). “Surgical management of symptomatic pericardial effusion in patients with solid malignancies”. Ann Surg Oncol. 13 (12): 1732–8. doi:10.1245/s10434-006-9073-1. PMID 17028771.
- ↑ Cullinane CA, Paz IB, Smith D, Carter N, Grannis FW (2004). “Prognostic factors in the surgical management of pericardial effusion in the patient with concurrent malignancy”. Chest. 125 (4): 1328–34. PMID 15078742.
- ↑ Dequanter D, Lothaire P, Berghmans T, Sculier JP (2008). “Severe pericardial effusion in patients with concurrent malignancy: a retrospective analysis of prognostic factors influencing survival”. Ann Surg Oncol. 15 (11): 3268–71. doi:10.1245/s10434-008-0059-z. PMID 18648881.
- ↑ Dosios T, Theakos N, Angouras D, Asimacopoulos P (2003). “Risk factors affecting the survival of patients with pericardial effusion submitted to subxiphoid pericardiostomy”. Chest. 124 (1): 242–6. PMID 12853529.
- ↑ Girardi LN, Ginsberg RJ, Burt ME (1997). “Pericardiocentesis and intrapericardial sclerosis: effective therapy for malignant pericardial effusions”. Ann Thorac Surg. 64 (5): 1422–7, discussion 1427-8. doi:10.1016/S0003-4975(97)00992-2. PMID 9386714.
- ↑ Neragi-Miandoab S, Linden PA, Ducko CT, Bueno R, Richards WG, Sugarbaker DJ; et al. (2008). “VATS pericardiotomy for patients with known malignancy and pericardial effusion: survival and prognosis of positive cytology and metastatic involvement of the pericardium: a case control study”. Int J Surg. 6 (2): 110–4. doi:10.1016/j.ijsu.2007.12.005. PMID 18329349.
- ↑ García-Riego A, Cuiñas C, Vilanova JJ (2001). “Malignant pericardial effusion”. Acta Cytol. 45 (4): 561–6. PMID 11480719.
Diagnosis
Diagnosis
History and Symptoms | Physical Examination | Laboratory Findings | Electrocardiogram | Chest X Ray | CT | MRI | Echocardiography | Cardiac Catheterization
Treatment
Treatment
Approach to Treatment | Medical Therapy | Pericardiocentesis | Pericardial Window | Pericardial Stripping
Looking for the patient version?
© 2026 MyEClinic – IFTM Institut für Telematik in der Medizin GmbH