
Abdominal aortic aneurysm
For patient information click here
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor-In-Chief: Cafer Zorkun, M.D., Ph.D. [2] Ramyar Ghandriz MD[3]
Synonyms and keywords: Abdominal aneurysm, aortic; aortic aneurysm, abdominal; AAA; triple A
Overview
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor-In-Chief: Cafer Zorkun, M.D., Ph.D. [2]
Synonyms and keywords: Abdominal aneurysm, aortic; aortic aneurysm, abdominal; AAA; triple A
Overview
An abdominal aortic aneurysm is a localized dilatation of the abdominal aorta, that exceeds the normal diameter of the abdominal aorta by more than 50%. The normal diameter of an aorta depends on the patient’s age, sex, height, weight, race, body surface area, and baseline blood pressure. On average, the normal diameter of the infrarenal aorta is 2 cm, and therefore a true AAA measures 3.0 cm or more. Aortic ectasia is a mild generalized dilatation (<50% of the normal diameter of ≤ 2.9 cm) that is due to age-related degenerative changes in the vessel walls.
Historical Perspective
The etymology of the word aneurysm comes from the Greek word for “dilatation”. Abdominal aortic aneurysm as a medical condition has been recognized since ancient times, but was not been successfully treated until the early part of the 20th century. In 1923, Rudolph Matas (who also proposed the concept of endoaneurysmorrhaphy), performed the first successful aortic ligation on a human. In 1949, Albert Einstein was operated on by Rudolf Nissen by wrapping the aorta with polyethene cellophane, which induced fibrosis and restricted the growth of the aneurysm. In 1951, Charles Dubost performed the first AAA repair using a homograft. In 1953, Blakemore and Voorhees repaired a ruptured AAA using a Vinyon-N graft (nylon). In 1962, Javid and Creech reported the technique of endoaneurysmorrhaphy. In 1980, Parodi et al described an endovascular repair.
Definition
The normal diameter of one’s aorta depends on the patient’s age, sex, height, weight, race, body surface area, and baseline blood pressure. On average, the normal diameter of the infrarenal aorta (where abdominal aortic aneurysms are located) is 2 cm. Therefore an abdominal aortic aneurysm is defined as a dilation of 3.0 cm or more.
An abdominal aortic aneurysm is to be distinguished from aortic ectasia which is defined as a mild generalized dilatation (<50% of the normal diameter of ≤ 2.9 cm) that is due to age-related degenerative changes in vessel wall.
Anatomy

The aorta below the renal arteries, also known as the infrarenal aorta, is the location of 90% of abdominal aortic aneurysms. Other possible locations are suprarenal and pararenal. The aneurysm can extend to include one or both of the iliac arteries.
Classification
Aneurysms are usually classified by their shape:
Fusiform Aneurysms
Most common type seen in the infrarenal aorta and are diffuse and circumferential.
Saccular Aneurysms
Involve only a portion of the circumference, with a characteristic outpouching of the vessel wall.
Pathophysiology
The underlying pathophysiology of abdominal aortic aneurysm involves genetic influences, smoking, hypertension, hemodynamic influences and underlying atherosclerosis. In rare instances infection, arteritis, and connective tissue disorders may play a role.
Causes
The most common cause of an AAA is atherosclerosis.
Differentiating Abdominal Aortic Aneurysm from other Diseases
An abdominal aortic aneurysm should be differentiated from other causes of abdominal pain such as acute cholecystitis, gastrointestinal bleeding, perforated peptic ulcer, ischemic bowel, nephrolithiasis, pyelonephritis, appendicitis, cholelithiasis, large bowel obstruction, small bowel obstruction, pancreatitis, musculoskeletal pain, myocardial infarction, and urinary tract infection.
Epidemiology and Demographics
Abdominal aortic aneurysm is the 13th leading cause of death in the US. Abdominal aortic aneurysms are more common in developed countries. Elderly, caucasian males who are smokers are at higher risk for developing an abdominal aortic aneurysm.
Risk Factors
Initial Development
Smoking
The most significant modifiable risk factor for the development of an abdominal aortic aneurysm is smoking which increases the risk of aneurysm development 8 fold.
Age
Advanced age and family history are the strongest non-modifiable risk factors for the development of an abdominal aortic aneurysm.
Hypercholesterolemia
Hypercholesterolemia and hypertension are risk factors as well.
Caucasian Race
Caucasian race is associated with a higher incidence of AAA when compared to non Caucasian race.
Expansion
An increased rate of expansion of abdominal aortic aneurysm is related to systolic hypertension, wide pulse pressure, and ongoing smoking.
Rupture
The risk of abdominal aortic aneurysm rupture is proportional to the size and rate of growth of the aneurysm. Abdominal aortic aneurysms greater than 5 cm diameter or those that grow faster than 1 cm per year have a significantly increased risk of rupture and are indications for elective operative repair. Advanced age, female gender, hypertension, active smoking, outpouchings, and mural thrombus are also risk factors for abdominal aortic aneurysm rupture.
Screening
Approximately 16% of large abdominal aortic aneurysms (diameter > 5.5 cm) rupture, causing 9,000 AAA-related deaths in the United States per year[1]. Several studies have shown that screening can drastically reduce the aneurysm rupture rate by 45-49% for men older than 60, and reduce AAA-related mortality by 21-68%. In a landmark study randomizing 67,800 men, (The Multicenter Aneurysm Screening Study) aneurysm-related mortality was 53% lower in the screening group as compared with control patients[2][3]. The United States Preventive Services Task Force (USPSTF) recommends one-time screening for abdominal aortic aneurysm (AAA) by ultrasonography in any man aged 65 to 75 who has ever smoked. The USPSTF makes no recommendation for or against screening for AAA in men aged 65 to 75 who have never smoked. The USPSTF recommends against routine screening for AAA in women.
Natural History, Complications and Prognosis
Abdominal aortic aneurysms expand slowly over time. An aortic aneurysm can progress to a ruptured abdominal aortic aneurysm, which is a medical emergency associated with an extremely high mortality. Serious complications can also occur as a result of an aortic dissection, such as myocardial infarction, shock, stroke, kidney failure, and arterial emboli. A ruptured AAA carries an overall mortality rate approaching 75%, which is much higher than the mortality rate of 2-6% in those patients who underwent elective surgical repair. Approximately 16% of large AAAs (diameter >5.5 cm) rupture, causing 9,000 AAA-related deaths in the United States per year[1]. Several studies have shown that screening can drastically reduce the aneurysm rupture rate by 45-49% for men older than 60, and reduce AAA-related mortality by 21-68%. The outcome is usually good if an experienced surgeon repairs the aneurysm before it ruptures. Rupture of an abdominal aortic aneurysm is associated with a 60% to 90% mortality before the patient reaches a hospital. It is associated with a 30% to 80% operative mortality among those patients who survive long enough to undergo surgery.
History and Symptoms
Given that smoking increases the risk of abdominal aortic aneurysm development, a smoking history should be obtained in elderly men. If a male over the age of 65 has a history of smoking, they should undergo ultrasonography to screen for an abdominal aortic aneurysm. Abdominal aortic aneurysms are usually asymptomatic until they expand or rupture. Spontaneous abdominal pain in a patient with a pulsatile epigastric mass or a known AAA may signal rupture into the retroperitoneum or leakage within the aneurysm wall. If a patient does develop symptoms, the risk of rupture is quite high, which is why symptoms are considered an indication for surgery. Pain is the most common symptomatic manifestation of AAA.
Physical Examination
Physical examination has a low sensitivity in the detection of small abdominal aortic aneurysms (29-61% for abdominal aortic aneurysms 3.0-3.9 cm in diameter) but has a sensitivity of 76-82% to detect those abdominal aortic aneurysms that are 5.0 cm or larger that may warrant repair. It is easier to detect a pulsatile mass in thin patients and those who do not have tense abdomens. Contrary to popular belief, gentle palpation of abdominal aortic aneurysms is safe, and does not precipitate rupture.
Abdominal X Ray
Plain abdominal radiographs are obtained in patients with abdominal complaints before the diagnosis of AAA has been made. It is very difficult to evaluate patients with AAA using plain radiographs, because aortic wall calcification is seen in less than half of the cases with AAA. However, plain radiographs may be helpful when an aneurysmal aorta appears normal on angiogram, due to thrombus within the sac.
Abdominal Ultrasound
Abdominal ultrasound is the standard imaging modality to detect and follow the progression of an abdominal aortic aneurysm. When performed by an expert, it has a sensitivity and specificity close to 100% and 96%, respectively. Abdominal ultrasound can also detect mural thrombus, iliac artery aneurysms, and free peritoneal blood. Patients should fast before examination to optimize image quality.
Computed Tomography (CT)
Although CT scanning provides detailed anatomic information and is valuable in planning abdominal aortic aneurysm repair, it is not used as a screening tool given the potential nephrotoxicity associated with the dye load, the cost, and the exposure to radiation.
Magnetic Resonance Imaging (MRI)
MRI might be a better soft tissue visualizer than ultrasonography and CT, but its limitations limit its usage as a screening tool and as a diagnostic tool during emergencies like ruptured AAA. However its advantages makes it a good alternative in AAA patients with poor renal function and in elective preoperative evaluation of unruptured AAA[4].
Other Imaging Findings
Angiography is an alternative less often used imaging method for visualization of an abdominal aortic aneurysm. Angiography is helpful in determining anatomy of aorta precisely. It can be used preoperatively in case of suspected suprarenal or thoracic aortic aneurysm, femoral or popliteal aneurysm, renal artery stenosis, unexplained renal insufficiency, occlusive ilio-femoral disease, or visceral ischemia.
Medical Therapy
Risk factor modification, such as smoking cessation, management of hypertension, and lipid lowering are essential in reducing the risk of development and the rate of progression of abdominal aortic aneurysms.
Surgery
Indications for operative repair of an abdominal aortic aneurysm include the presence of symptoms such as back pain, the presence of a rupture or contained rupture, an abdominal aortic aneurysm diameter greater than 5.5 cm, a rate of expansion of greater than 1 cm in one year, and an inflammatory or infectious etiology. Open surgical repair is favored in young patients as an elective procedure, the presence of an expanding aneurysm, symptomatic aneurysm, or ruptured aneurysm. An endovascular repair (EVAR) is favored in older patients and high risk patients or those unfit for open repair. Risk factors for postoperative morbidity and mortality include extensive atheromatous disease, mural calcification, thrombosis, juxtarenal extension of the aneurysm and the presence of inflammatory changes.
Prevention
Smoking cessation and blood pressure management are two strategies to reverse modifiable risk factors for the development, progression, and rupture of an abdominal aortic aneurysm.
References
- ↑ 1.0 1.1 Gillum RF (1995). “Epidemiology of aortic aneurysm in the United States”. Journal of Clinical Epidemiology. 48 (11): 1289–98. PMID 7490591. Retrieved 2012-10-27. Unknown parameter
|month=ignored (help) - ↑ Ashton HA, Buxton MJ, Day NE, Kim LG, Marteau TM, Scott RA, Thompson SG, Walker NM (2002). “The Multicentre Aneurysm Screening Study (MASS) into the effect of abdominal aortic aneurysm screening on mortality in men: a randomised controlled trial”. Lancet. 360 (9345): 1531–9. PMID 12443589. Retrieved 2012-10-27. Unknown parameter
|month=ignored (help) - ↑ “Multicentre aneurysm screening study (MASS): cost effectiveness analysis of screening for abdominal aortic aneurysms based on four year results from randomised controlled trial”. BMJ (Clinical Research Ed.). 325 (7373): 1135. 2002. PMC 133450. PMID 12433761. Retrieved 2012-10-27. Unknown parameter
|month=ignored (help) - ↑ Thurnher, SA.; Dorffner, R.; Thurnher, MM.; Winkelbauer, FW.; Kretschmer, G.; Polterauer, P.; Lammer, J. (1997). “Evaluation of abdominal aortic aneurysm for stent-graft placement: comparison of gadolinium-enhanced MR angiography versus helical CT angiography and digital subtraction angiography”. Radiology. 205 (2): 341–52. PMID 9356613. Unknown parameter
|month=ignored (help)
Historical Perspective
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Hardik Patel, M.D. Ramyar Ghandriz MD[2]
Overview
The etymology of the word aneurysm comes from the Greek word for “dilatation”. Abdominal aortic aneurysm as a medical condition has been recognized since ancient times, but was not been successfully treated until the early part of the 20th century. In 1923, Rudolph Matas (who also proposed the concept of endoaneurysmorrhaphy), performed the first successful aortic ligation on a human. In 1949, Albert Einstein was operated on by Rudolf Nissen by wrapping the aorta with polyethene cellophane, which induced fibrosis and restricted the growth of the aneurysm. In 1951, Charles Dubost performed the first AAA repair using a homograft. In 1953, Blakemore and Voorhees repaired a ruptured AAA using a Vinyon-N graft (nylon). In 1962, Javid and Creech reported the technique of endoaneurysmorrhaphy. In 1980, Parodi et al described an endovascular repair.
Historical Perspective
2nd Century AD
- The first historical accounts regarding abdominal aortic aneurysm date from Ancient Rome, more precisely from the 2nd century AD, when Greek surgeon Antyllus tried to treat an abdominal aortic aneurysm with proximal and distal ligature, along with central incision and evacuation of thrombotic material from the aneurysm.[1]
1923
- However, attempts to treat the AAA surgically were unsuccessful until 1923. In that year, Rudolph Matas (who also proposed the concept of endoaneurysmorrhaphy), performed the first successful aortic ligation on a human.[2]
1949
- Other methods that were successful in treating an AAA included wrapping the aorta with polyethene cellophane, which induced fibrosis and restricted the growth of the aneurysm. Albert Einstein was operated on by Rudolf Nissen with use of this technique in 1949, and survived five years after the operation.[3]
1951
1953
- Blakemore and Voorhees repaired a ruptured AAA using a Vinyon-N graft (nylon). [5]
- Later, they were replaced by Dacron and polytetrafluoroethylene (PTFE).
- Silk sutures were banned because of degeneration, in favor of braided Dacron, polyethylene, and PTFE sutures, all of which retain tensile strength.
1962
- Javid and Creech reported the technique of endoaneurysmorrhaphy, which dramatically reduced mortality.[6]
1980
- Parodi et al described an endovascular repair using a large Palmaz stent and unilateral aortofemoral and femorofemoral crossover Dacron grafts.[7]
References
- ↑ Bobadilla, Joseph L. (2013). “From Ebers to EVARs: A Historical Perspective on Aortic Surgery”. AORTA. 1 (2): 89–95. doi:10.12945/j.aorta.2013.13-004. ISSN 2325-4637.
- ↑ Livesay JJ et al. Milestones in Treatment of Aortic Aneurysm. Tex Heart Inst J 2005; 32: 130–134. PMCID 1163455
- ↑ Famous Patients, Famous Operations, 2002 – Part 3: The Case of the Scientist with a Pulsating Mass from Medscape Surgery
- ↑ Cervantes, Jorge (2003). “Reflections on the 50th Anniversary of the First Abdominal Aortic Aneurysm Resection”. World Journal of Surgery. 27 (2): 246–248. doi:10.1007/s00268-002-6413-6. ISSN 0364-2313.
- ↑ Norton, Jeffrey A.; Barie, Philip S.; Bollinger, R. Randal; Chang, Alfred E.; Lowry, Stephen F.; Mulvihill, Sean J.; Pass, Harvey I.; Thompson, Robert W. (2008). doi:10.1007/978-0-387-68113-9. Missing or empty
|title=(help) - ↑ Paty, Philip S.K.; Darling, R.Clement; Chang, Benjamin B.; Shah, Dhiraj M.; Leather, Robert P. (1997). “A prospective randomized study comparing exclusion technique and endoaneurysmorrhaphy for treatment of infrarenal aortic aneurysm”. Journal of Vascular Surgery. 25 (3): 442–445. doi:10.1016/S0741-5214(97)70253-2. ISSN 0741-5214.
- ↑ Parodi JC, Palmaz JC, Barone HD (1991). “Transfemoral intraluminal graft implantation for abdominal aortic aneurysms”. Ann Vasc Surg. 5 (6): 491–9. PMID 1837729.
Classification
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1] ;Associate Editor(s)-in-Chief: Ramyar Ghandriz MD[2]
Overview
Aneurysms are usually classified by their shape. Abdominal aorta aneurysm is classified by their location as suprarenal or infrarenal. size of the aneurysm is another important criteria that may indicate the need for surgery, so they may be classified by their size in many textbooks.
Classification
Fusiform Aneurysms
- They are the most common type of aneurysm seen in the infrarenal aorta.
- They are diffuse and circumferential.[1]
Saccular Aneurysms
- Involve only a portion of the circumference, with a characteristic outpouching of the vessel wall.[2].
Size based classification
- Determined by ultrasonography, where as it manifest the best maintenance method[3]:
- Small aneurysm (<5.5 cm) needs close follow ups.
- If during follow ups, an aneurysm growth in size was rapid, surgery is required.
- Pronounced aneurysm (>5.5 cm) needs surgical repair via graft placement or endovascular stent placement.
References
- ↑ Wang, Linda J.; Prabhakar, Anand M.; Kwolek, Christopher J. (2018). “Current status of the treatment of infrarenal abdominal aortic aneurysms”. Cardiovascular Diagnosis and Therapy. 8 (S1): S191–S199. doi:10.21037/cdt.2017.10.01. ISSN 2223-3652.
- ↑ Cronenwett, Jack (2014). Rutherford’s vascular surgery. Philadelphia, PA: Saunders/Elsevier. ISBN 978-1-4557-5304-8.
- ↑ Kontopodis, Nikolaos; Lioudaki, Stella; Pantidis, Dimitrios; Papadopoulos, George; Georgakarakos, Efstratios; Ioannou, Christos V (2016). “Advances in determining abdominal aortic aneurysm size and growth”. World Journal of Radiology. 8 (2): 148. doi:10.4329/wjr.v8.i2.148. ISSN 1949-8470.
Pathophysiology
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor-In-Chief: Cafer Zorkun, M.D., Ph.D. [2] Ramyar Ghandriz MD[3]
Overview
The underlying pathophysiology of abdominal aortic aneurysm involves genetic influences, smoking, hypertension, hemodynamic influences and underlying atherosclerosis. In rare instances infection, arteritis, and connective tissue disorders may play a role.
Pathophysiology
Pathology
- The most striking histopathological changes of aneurysmatic aorta are seen in tunica media and intima. [1]
- Changes indicated include an accumulation of lipids in foam cells( a kind of macrophage), extracellular free cholesterol crystals, calcifications, ulcerations, ruptures of the layers, and thrombosis.[2]
- There is an adventitial inflammatory infiltrate.
- The degradation of tunica media in proteolytic manners,is the basic process of abdominal aortic aneurysm initial phase. [3]
- Matrix metalloproteinases role in Abdominal aortic aneurysm has been shown by some researchers.[4]
- This leads to elimination of elastin from the media, rendering the aortic wall more susceptible to the influence of the blood pressure.
- Inflammation is another condition which plays a role in abdominal aortic aneurysm development.[5]
- The aortic wall has a specific arrangement of structural proteins that give it both strength and elasticity.
- The composition of the extracellular matrix protein in the media may change with age or in response to other conditions, therefore resulting in subsequent destruction of the elastic lamella, rendering the aorta less able to withstand the force of systolic pressure.
- The infra-renal aorta is more prone to develop aneurysms than other segments for the following reasons:[6]
- It is the segment that must expand the most during systole and contract the most during diastole.
- It has a thinner wall, and has fewer vasa vasora than the thoracic aorta.
- It is more prone to atherosclerosis, a proposed nidus for aneurysmal dilatation.
- Patients with abdominal aortic aneurysms (AAA) also have atherosclerosis in the aorta and other arteries, suggesting that aneurysmal disease may be part of a larger spectrum of vascular disease, and that atherosclerosis actually promotes AAA formation.
- In atherosclerotic AAA, inflammatory cells infiltrate into the vessel wall and may secrete specific matrix metalloproteinases (MMPs).[7]
- The different types of MMPs play diverse roles via complex interactions that eventually lead to degradation of the structural media proteins, and subsequently to aneurysmal dilatation.
- There are significantly fewer smooth muscle cells in human AAA tissues than in normal or atherosclerotic nonaneurysmal aortic tissue.
- This decrease in smooth muscle cells in suspected to be secondary to apoptosis, therefore suggesting a role for focal cell apoptosis in the pathogenesis of AAA.
Genetics
- There is likely a genetic component to the development of an abdominal aortic aneurysm. A familial pattern of inheritance is most notable in males.[8]
- It has been postulated that a variant of alpha 1-antitrypsin deficiency may play a small role.
- It has also been postulated that there is a pattern of X-linked mutation, which would explain the lower incidence in heterozygous females.
Associated Conditions
- Smoking appears to be a critical environmental influence on the development of an abdominal aortic aneurysm.[9]
Hemodynamic Influences
- Abdominal aortic aneurysm is a focal degenerative process with a predilection for the infrarenal aorta.
- More than 90 % of abdominal aortic aneurysms occur in the infrarenal location.
- The higher incidence of abdominal aortic aneurysms in the infrarenal region may be due to differences between the infrarenal and the thoracic aorta with respect to histologic and mechanical characteristics. [10]
- The diameter progressively decreases from the root to the bifurcation, and the wall of the abdominal aorta also contains a smaller proportion of elastin.
- The mechanical tension in the abdominal aortic wall is therefore higher than in the thoracic aortic wall.
- The elasticity and distensibility also decline with age, which can result in gradual dilatation of the segment.
- Higher intraluminal pressure in patients with arterial hypertension markedly contributes to the progression of the pathological process.[11]
Atherosclerosis
- Although abdominal aortic aneurysms are frequently involved with atherosclerosis, the exact role of atherosclerosis in the pathophysiology of abdominal aortic aneurysms remains unclear at this time.
Other
Other causes of the development of abdominal aortic aneurysm include:
- Arteritis
- Connective tissue disorders (e.g. Marfan syndrome, Ehlers-Danlos syndrome)
- Cystic medial necrosis
- Infection
- Trauma
Associated Diseases
Abdominal aortic aneurysms are associated with a high prevalence of systemic atherosclerosis:
- 23%-86% have coronary artery disease
- 3%-20% have cerebrovascular disease
- 12%-42% have peripheral arterial disease
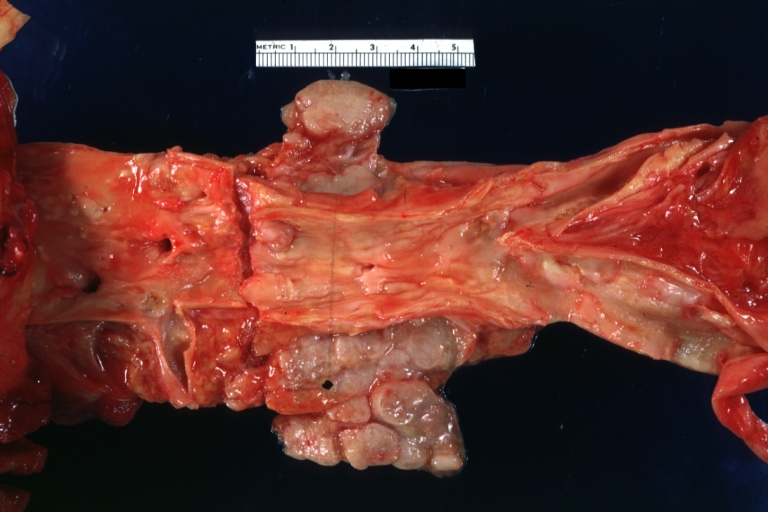
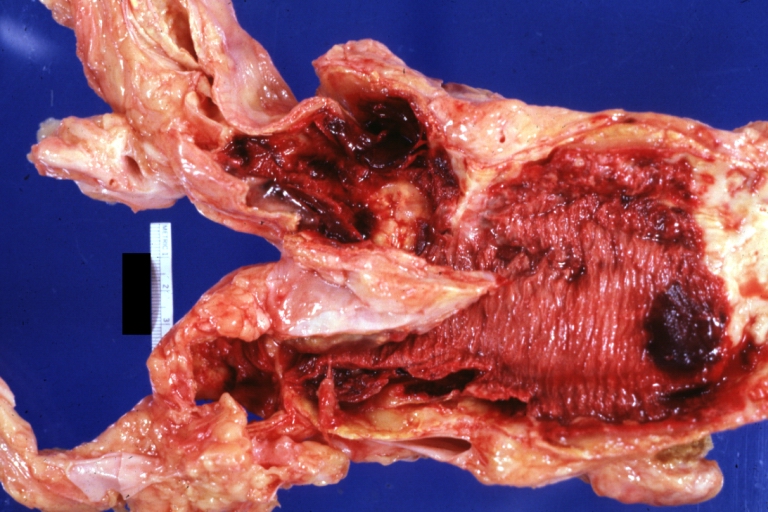
Gross Pathology
-
 Dissecting Aneurysm: Gross very good example dissected channel has been opened
Dissecting Aneurysm: Gross very good example dissected channel has been opened -
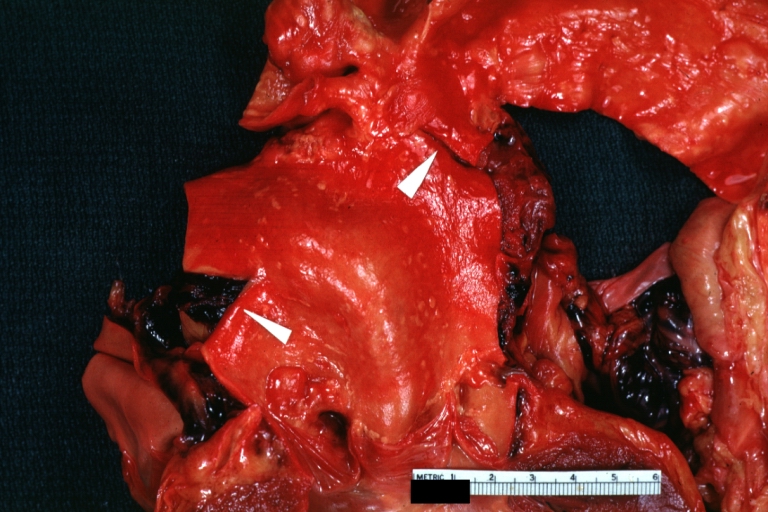
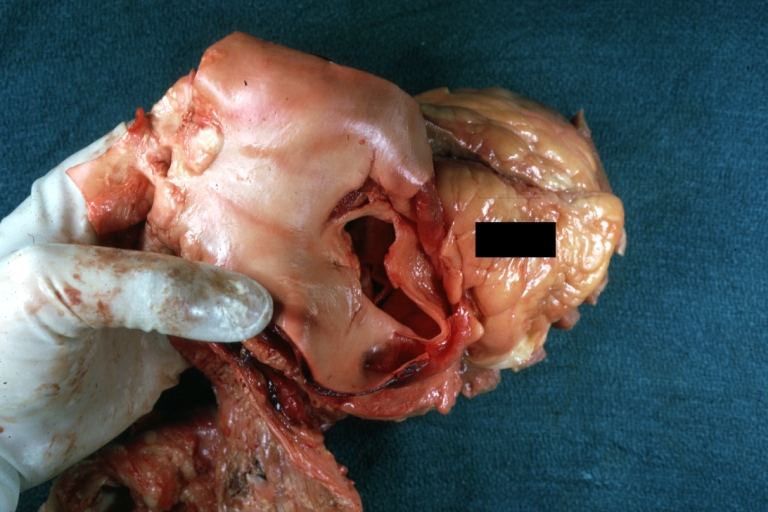
 Dissecting Aneurysm: Gross external view good appearance from adventitia
Dissecting Aneurysm: Gross external view good appearance from adventitia -
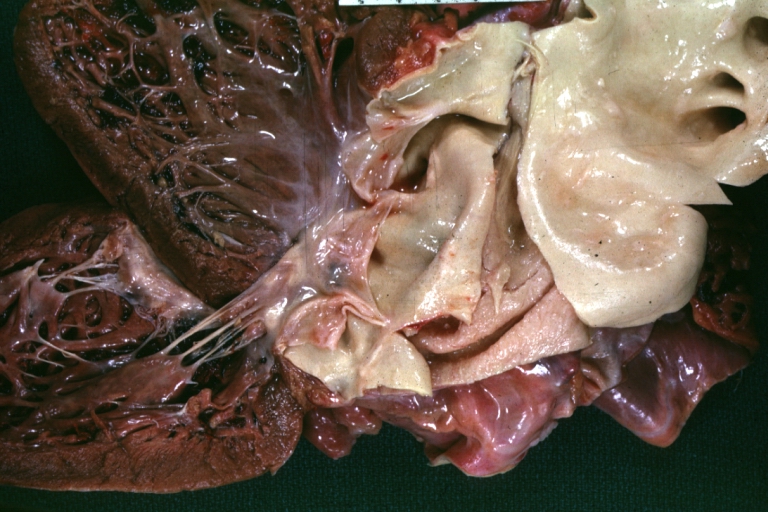
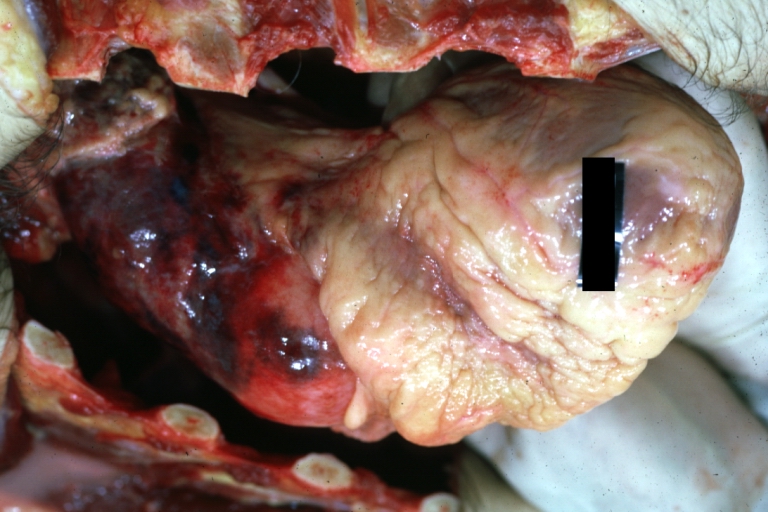
 Dissecting Aneurysm: Gross opened false channel
Dissecting Aneurysm: Gross opened false channel



-
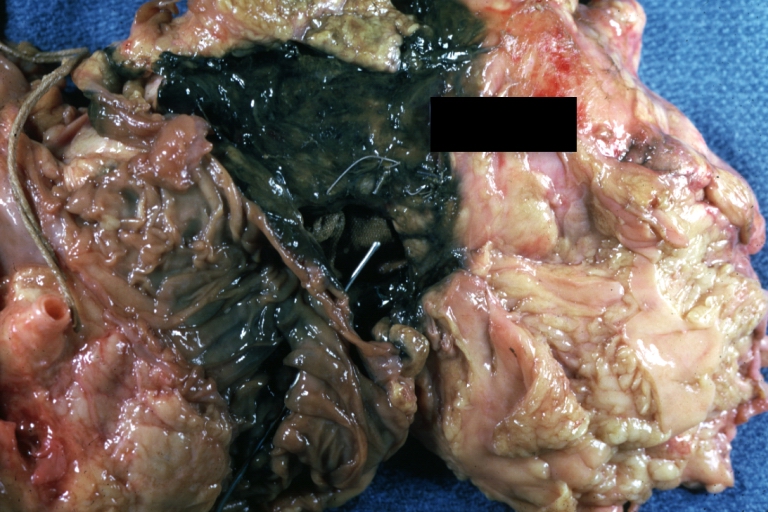
 Dissecting Aneurysm: Gross good example dissection beginning at third portion aortic arch
Dissecting Aneurysm: Gross good example dissection beginning at third portion aortic arch -
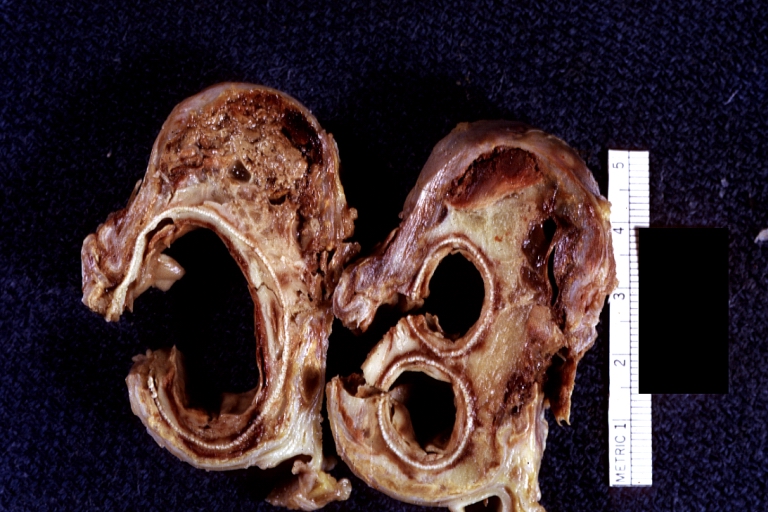
 Dissecting Aneurysm: Gross cross sections showing thrombus in false lumen true lumen has been opened longitudinally
Dissecting Aneurysm: Gross cross sections showing thrombus in false lumen true lumen has been opened longitudinally -
 Dissecting Aneurysm: Gross shows origin just above aortic valve false channel shown in descending thoracic aorta (very good example)
Dissecting Aneurysm: Gross shows origin just above aortic valve false channel shown in descending thoracic aorta (very good example)



-
 Atherosclerotic Aneurysm: Gross, a good example of typical abdominal aorta aneurysm with mural thrombus
Atherosclerotic Aneurysm: Gross, a good example of typical abdominal aorta aneurysm with mural thrombus -
 Dissecting Aneurysm: Gross, a very good example of dissection beginning just above aortic ring
Dissecting Aneurysm: Gross, a very good example of dissection beginning just above aortic ring -
 Atherosclerotic Aneurysm: Gross, (rather) good example of abdominal aortic aneurysm
Atherosclerotic Aneurysm: Gross, (rather) good example of abdominal aortic aneurysm



-
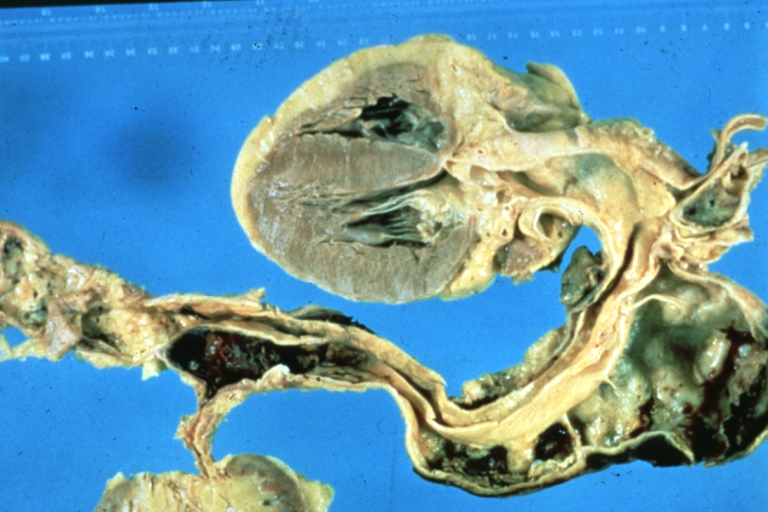
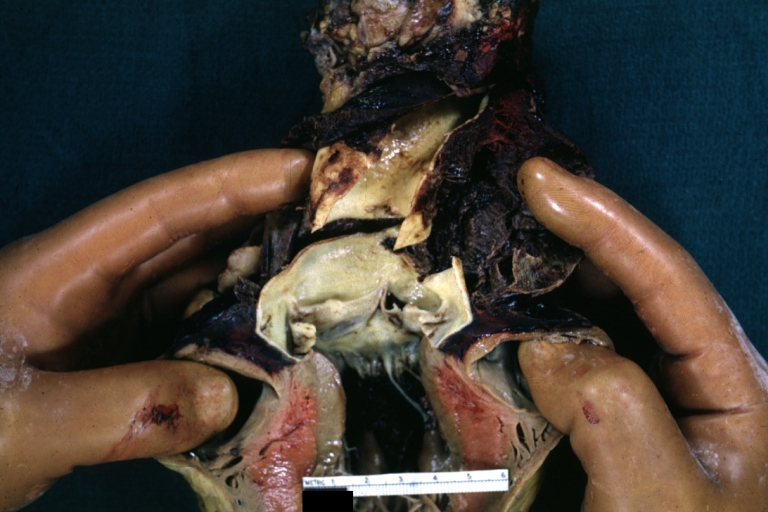
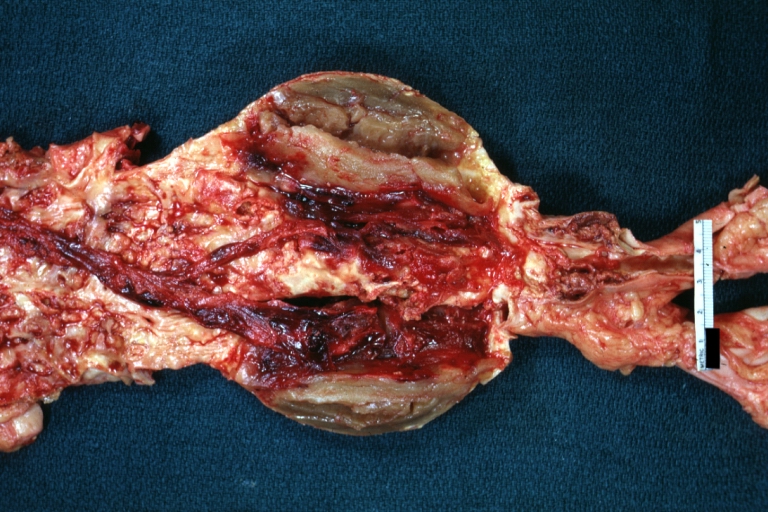
 Dissecting Aneurysm: Gross, an excellent example, starting just above the aortic valve with reflection of aorta to show the dissection tract and some thrombus
Dissecting Aneurysm: Gross, an excellent example, starting just above the aortic valve with reflection of aorta to show the dissection tract and some thrombus -
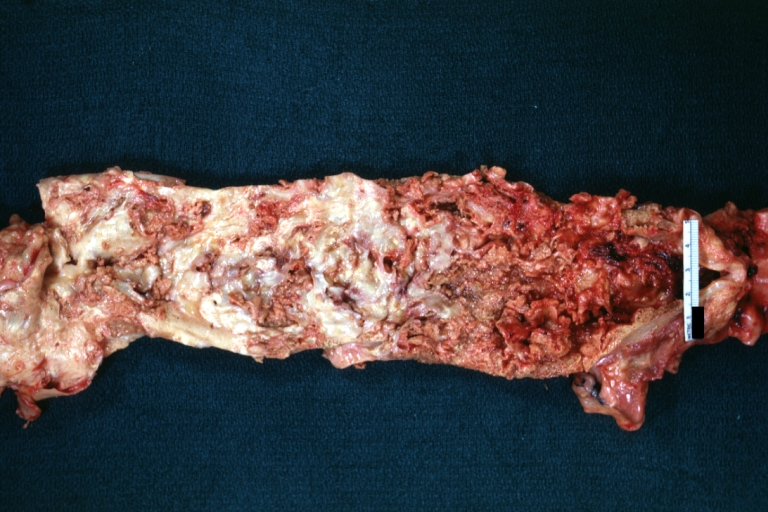
 Dissecting Aneurysm: Gross shows dilated aorta with extensive atherosclerosis dissection is seen, a small abdominal aorta atherosclerotic aneurysm is present good for association of dilation with dissection
Dissecting Aneurysm: Gross shows dilated aorta with extensive atherosclerosis dissection is seen, a small abdominal aorta atherosclerotic aneurysm is present good for association of dilation with dissection -
 Dissecting Aneurysm: Gross arrow points to start of dissection in first portion aortic arch good but not the best example shows dilation
Dissecting Aneurysm: Gross arrow points to start of dissection in first portion aortic arch good but not the best example shows dilation



-
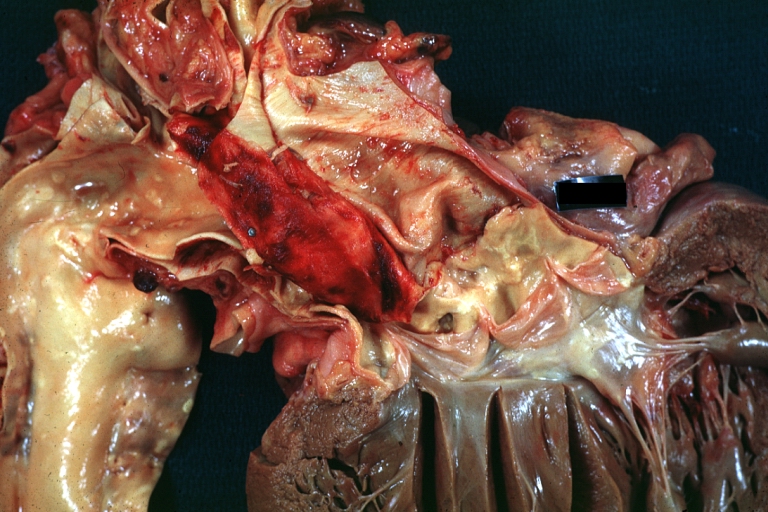
 Dissecting Aneurysm: Gross, very good to show start of dissection above aortic valve and blood in false channel
Dissecting Aneurysm: Gross, very good to show start of dissection above aortic valve and blood in false channel -
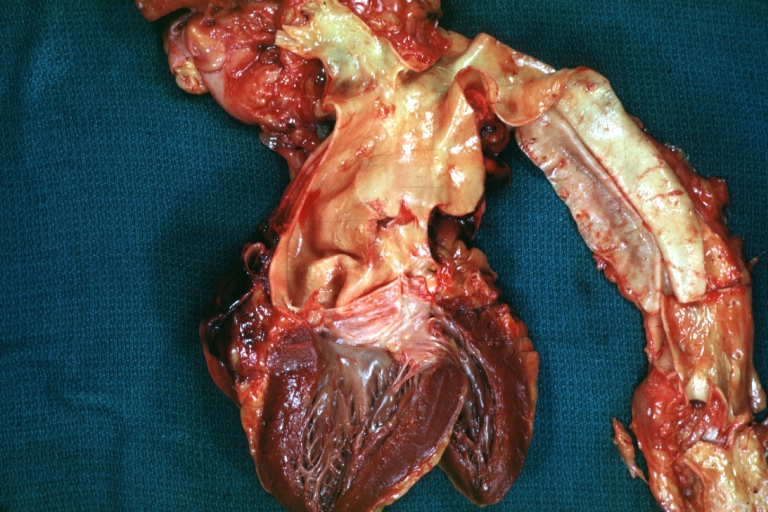
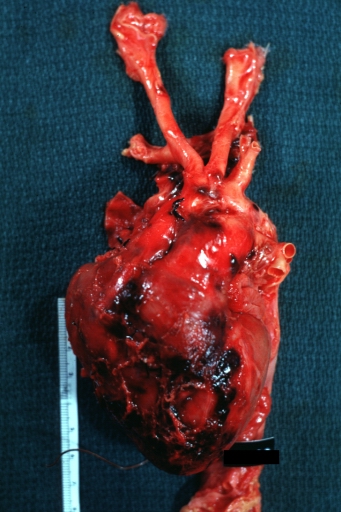
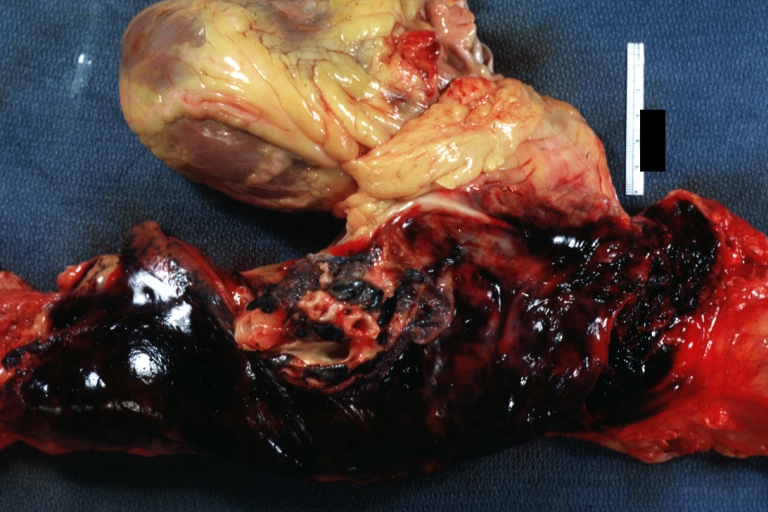
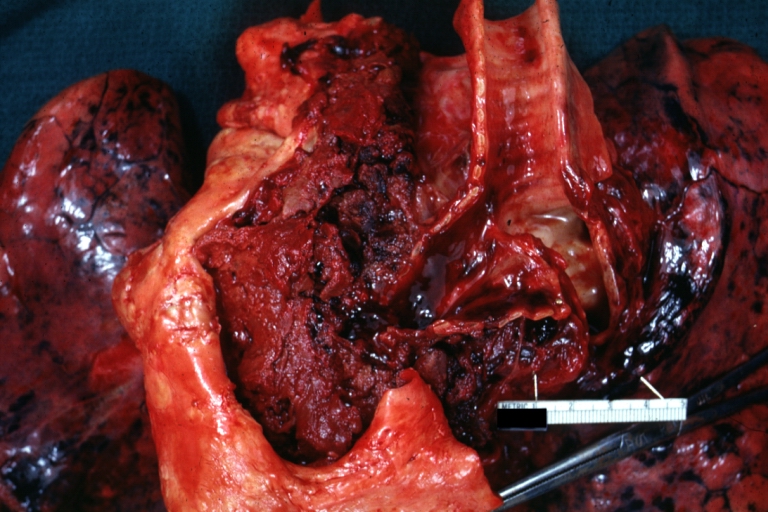
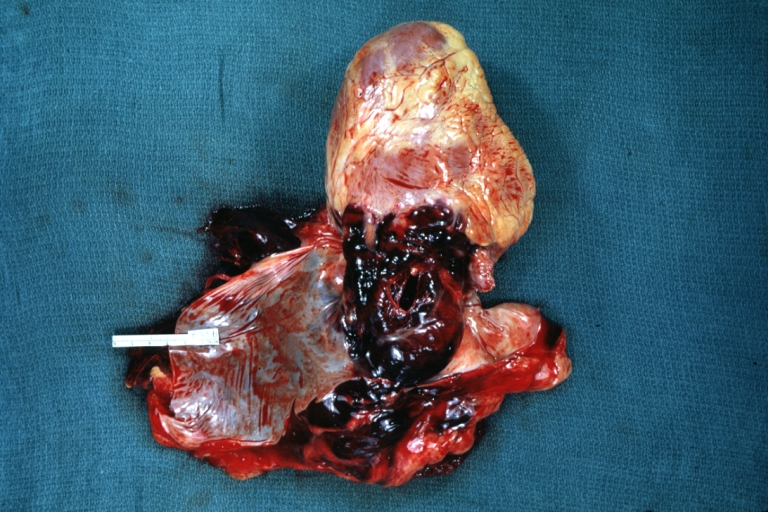 Dissecting Aneurysm: Gross, heart with root of aorta to show hemorrhage into pericardium (a very good example)
Dissecting Aneurysm: Gross, heart with root of aorta to show hemorrhage into pericardium (a very good example) -
 Dissecting Aneurysm: Gross, of heart and aorta with dissection and large false channel (a good example)
Dissecting Aneurysm: Gross, of heart and aorta with dissection and large false channel (a good example)



-
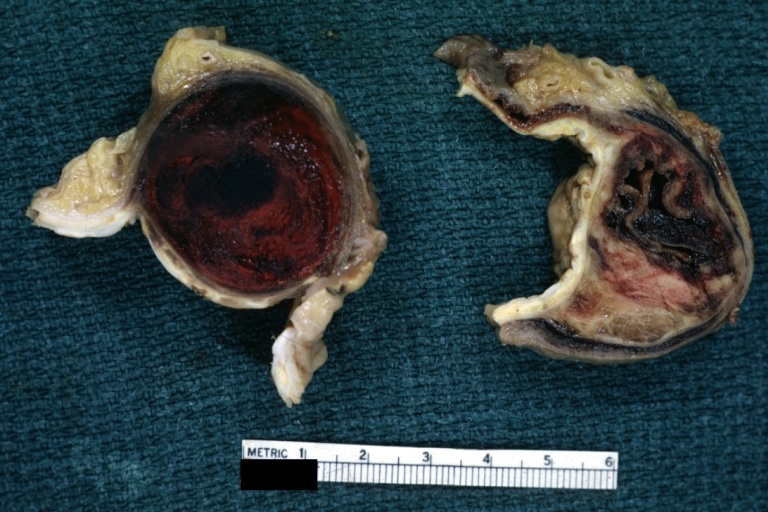
 Dissecting Aneurysm: Gross cross section of aorta with two channels (a good example)
Dissecting Aneurysm: Gross cross section of aorta with two channels (a good example) -
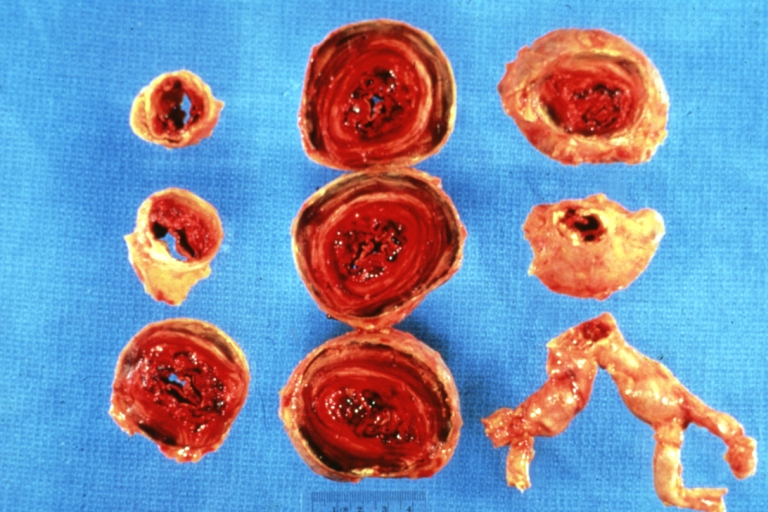 Atherosclerotic Aneurysm: Gross, a nice view of cross section of abdominal aorta aneurysm
Atherosclerotic Aneurysm: Gross, a nice view of cross section of abdominal aorta aneurysm -
 Dissecting Aneurysm: Gross good example of typical angular tear above aortic valve
Dissecting Aneurysm: Gross good example of typical angular tear above aortic valve



-
 Dissecting Aneurysm: Gross good example angular tear above aortic valve
Dissecting Aneurysm: Gross good example angular tear above aortic valve -
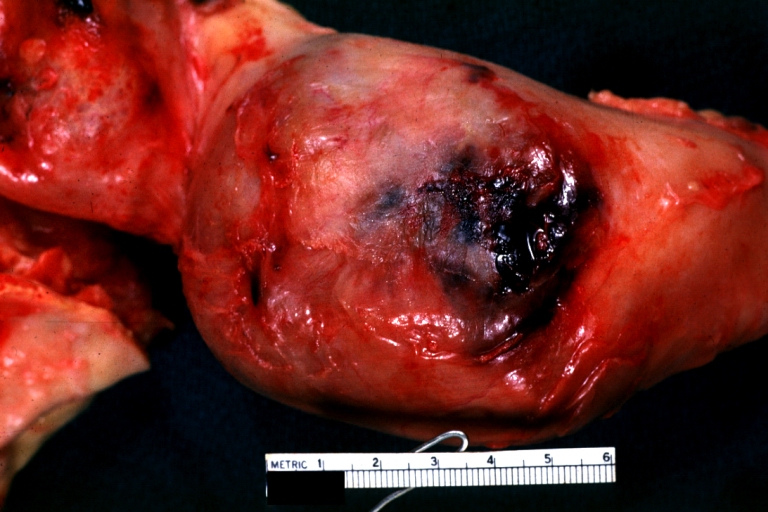 Atherosclerotic Aneurysm: Gross, external natural color very good example of an atherosclerotic thoracic aorta aneurysm with focal rupture
Atherosclerotic Aneurysm: Gross, external natural color very good example of an atherosclerotic thoracic aorta aneurysm with focal rupture -
 Atherosclerotic Aneurysm: Gross, excellent color, opened thoracic segment of aorta with two saccular atherosclerotic ruptured aneurysms
Atherosclerotic Aneurysm: Gross, excellent color, opened thoracic segment of aorta with two saccular atherosclerotic ruptured aneurysms



-
 Atherosclerotic Aneurysm: Gross, an excellent example, natural color, external view of typical thoracic aortic aneurysms
Atherosclerotic Aneurysm: Gross, an excellent example, natural color, external view of typical thoracic aortic aneurysms -
 Atherosclerotic Aneurysm: Gross unopened lesion natural color
Atherosclerotic Aneurysm: Gross unopened lesion natural color -
 Dissecting Aneurysm: Gross dissection first portion of arch fixed specimen (a good example)
Dissecting Aneurysm: Gross dissection first portion of arch fixed specimen (a good example)



-
 Dissecting Aneurysm: Gross, rather well shown dissection in first portion of the aortic arch
Dissecting Aneurysm: Gross, rather well shown dissection in first portion of the aortic arch -
 Dissecting Aneurysm: Gross, rather well shown dissection in first portion of the aortic arch
Dissecting Aneurysm: Gross, rather well shown dissection in first portion of the aortic arch -
 Dissecting Aneurysm: Gross, an excellent example of type I lesion
Dissecting Aneurysm: Gross, an excellent example of type I lesion



-
 Dissecting Aneurysm: Gross, external view, an excellent example
Dissecting Aneurysm: Gross, external view, an excellent example -
 Dissecting Aneurysm: Gross, Type I shows false channel
Dissecting Aneurysm: Gross, Type I shows false channel -
 Dissecting Aneurysm: Gross, opened to show false channel (good example)
Dissecting Aneurysm: Gross, opened to show false channel (good example)



-
 Atherosclerotic Aneurysm: Gross, very good example of ruptured thoracic segment
Atherosclerotic Aneurysm: Gross, very good example of ruptured thoracic segment -
 Dissecting Aneurysm: Gross, coagulum of blood in false channel
Dissecting Aneurysm: Gross, coagulum of blood in false channel -
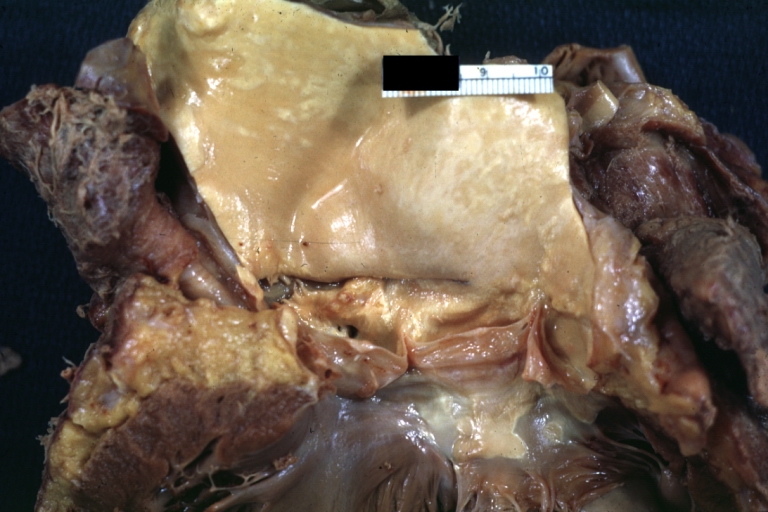
 Dissecting Aneurysm: Gross, aortic valve area dissection (well shown, typical lesion)
Dissecting Aneurysm: Gross, aortic valve area dissection (well shown, typical lesion)



-
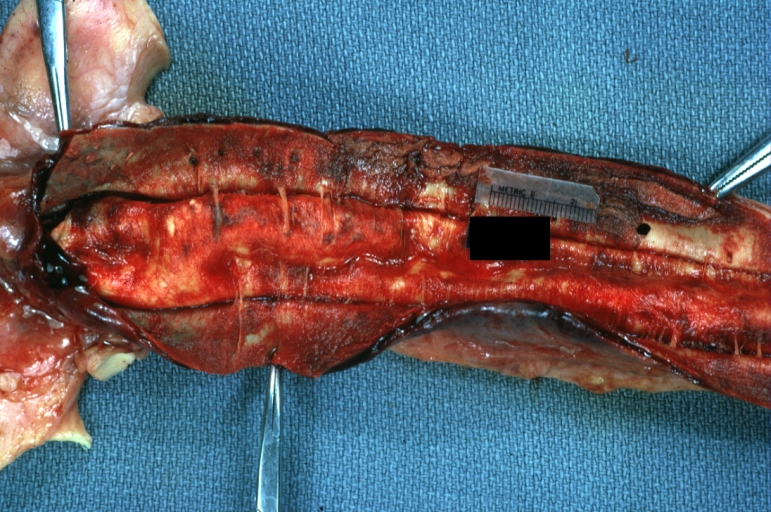
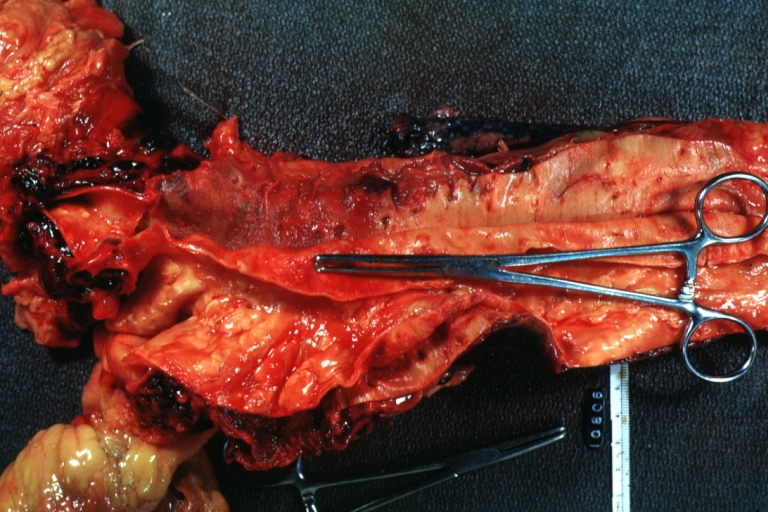
 Abdominal Aneurysm Ruptured: Gross (good example) opened kidneys in marked place, atherosclerosis in lower thoracic aorta
Abdominal Aneurysm Ruptured: Gross (good example) opened kidneys in marked place, atherosclerosis in lower thoracic aorta -
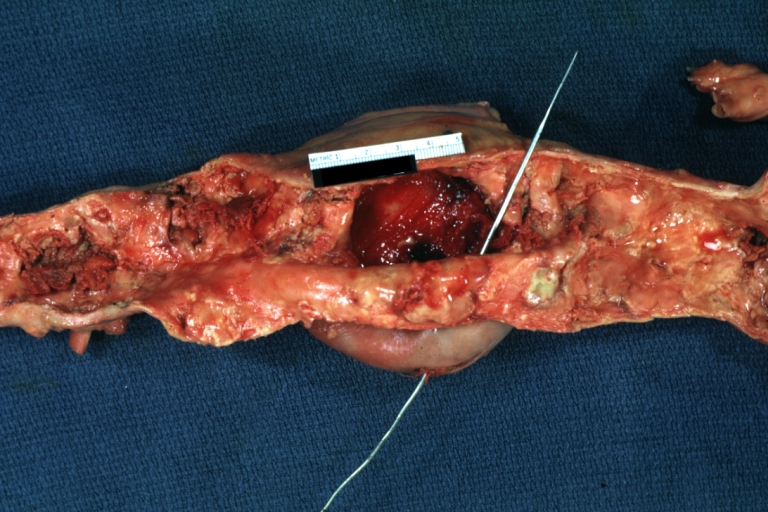
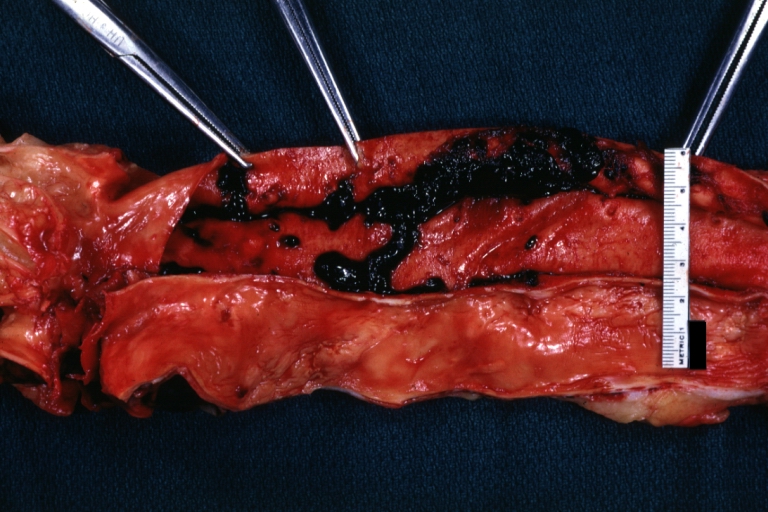
 Abdominal Aneurysm: Gross, (very good example) opened lesion with mural thrombus
Abdominal Aneurysm: Gross, (very good example) opened lesion with mural thrombus -
 Dissecting Aneurysm: Gross, large tear in first portion of aortic arch, annuloaortic ectasis
Dissecting Aneurysm: Gross, large tear in first portion of aortic arch, annuloaortic ectasis



-
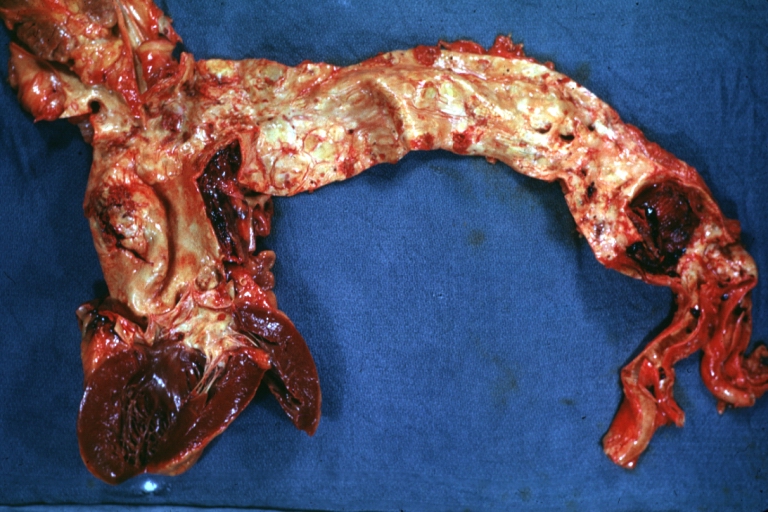
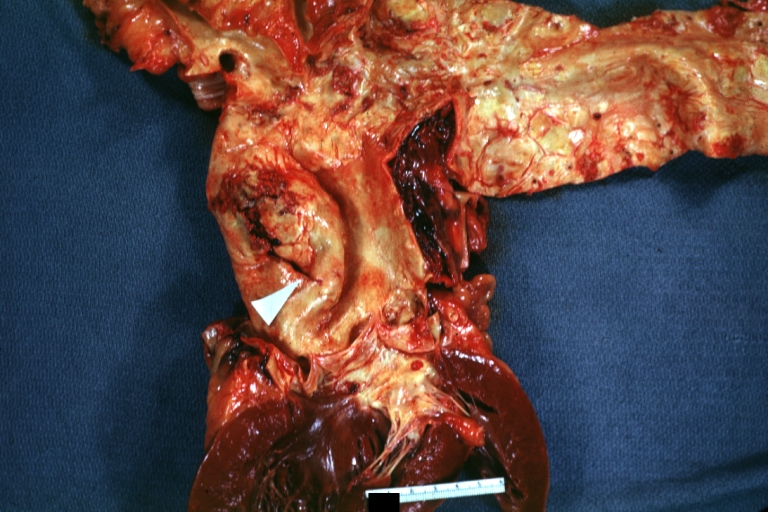
 Dissecting Aneurysm: Gross, external view of heart and first portion of aortic arch, annuloaortic ectasia, hemorrhage beneath adventitia is evidence of dissection
Dissecting Aneurysm: Gross, external view of heart and first portion of aortic arch, annuloaortic ectasia, hemorrhage beneath adventitia is evidence of dissection -
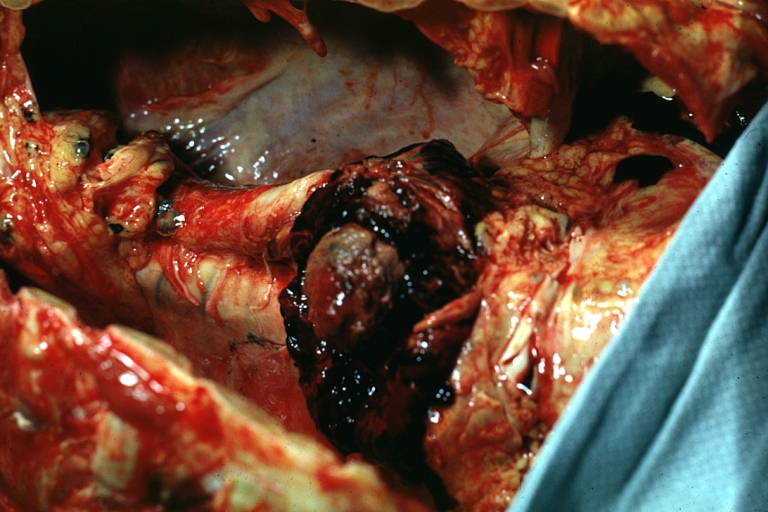
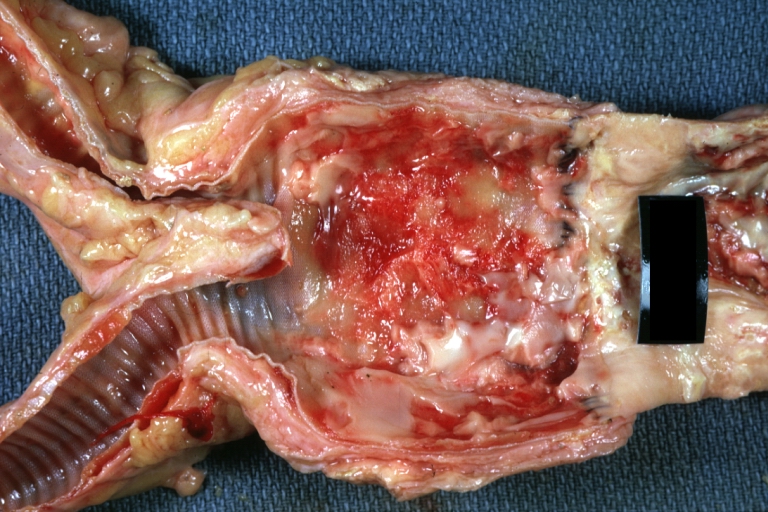
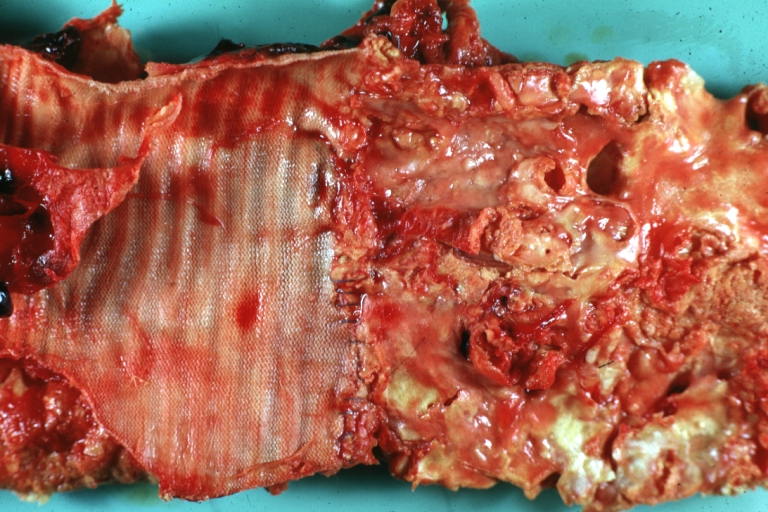
 Atherosclerotic Aneurysm Infected: Gross, infected abdominal aneurysm at superior suture line with rupture into duodenum
Atherosclerotic Aneurysm Infected: Gross, infected abdominal aneurysm at superior suture line with rupture into duodenum -
 Atherosclerotic Aneurysm: Gross, cross sections of repaired aneurysm showing Dacron graft and old mural thrombus. A nice example of fibrin layer in graft
Atherosclerotic Aneurysm: Gross, cross sections of repaired aneurysm showing Dacron graft and old mural thrombus. A nice example of fibrin layer in graft



-
 Ruptured Syphilitic Aneurysm
Ruptured Syphilitic Aneurysm -
 Dissecting Aneurysm in a patient with Marfan’s syndrome
Dissecting Aneurysm in a patient with Marfan’s syndrome -
 Traumatic Aneurysm
Traumatic Aneurysm



-
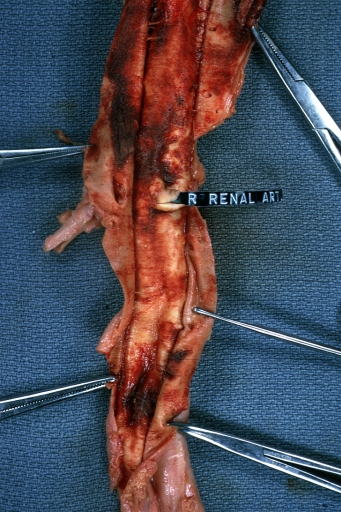
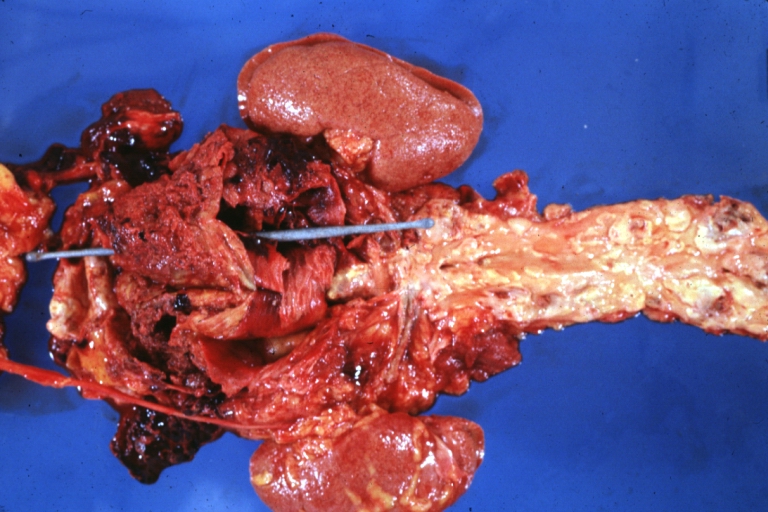
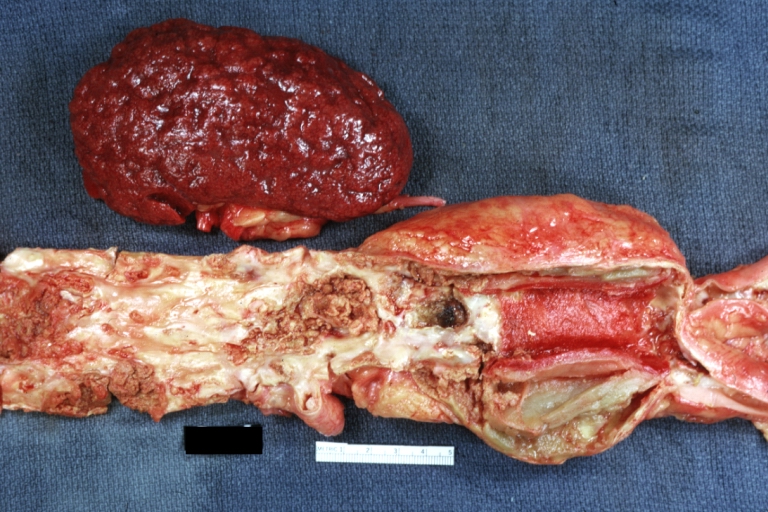 Kidney: Arteriosclerosis: Gross aorta with well shown renal artery containing large plaque and kidney with multiple cortical scars and atrophy also abdominal aorta aneurysm with mural thrombus (excellent example for renovascular hypertension)
Kidney: Arteriosclerosis: Gross aorta with well shown renal artery containing large plaque and kidney with multiple cortical scars and atrophy also abdominal aorta aneurysm with mural thrombus (excellent example for renovascular hypertension) -
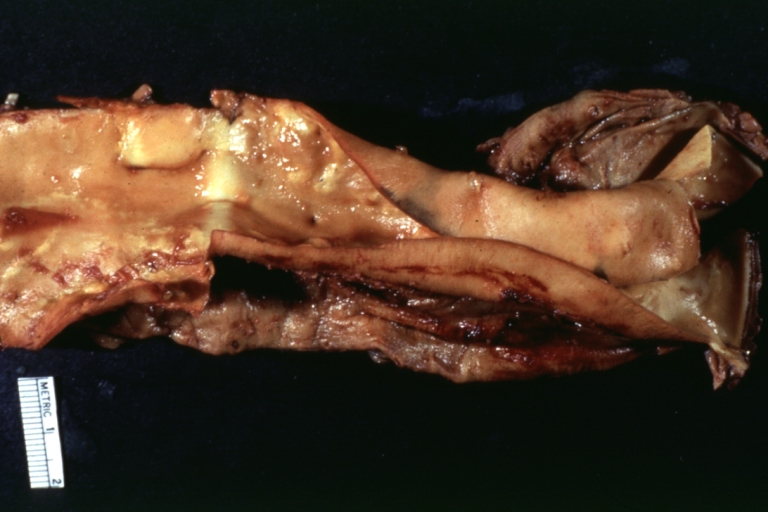
 Dissecting Aneurysm: Gross, fixed tissue, descending thoracic segment dissection opened to show the false channel. The true surface is also visible
Dissecting Aneurysm: Gross, fixed tissue, descending thoracic segment dissection opened to show the false channel. The true surface is also visible -
 Aneurysm: Gross, ruptured thoracic aorta aneurysm, in situ lower thoracic portion (probably due to atherosclerosis)
Aneurysm: Gross, ruptured thoracic aorta aneurysm, in situ lower thoracic portion (probably due to atherosclerosis)



-
 Abdominal Aneurysm Graft Repair: Gross, natural color, close-up view, an excellent example of Dacron graft that has been in place for years with pseudointima and atherosclerosis
Abdominal Aneurysm Graft Repair: Gross, natural color, close-up view, an excellent example of Dacron graft that has been in place for years with pseudointima and atherosclerosis -
 Dacron Graft: Gross, close-up Dacron graft to repair aneurysm. Aorta completely covered with a calcified and ulcerated plaque with small mural thrombi (an excellent depiction of proximal suture line)
Dacron Graft: Gross, close-up Dacron graft to repair aneurysm. Aorta completely covered with a calcified and ulcerated plaque with small mural thrombi (an excellent depiction of proximal suture line) -
 Dissecting Aneurysm: Gross natural color descending aorta opened into false channel
Dissecting Aneurysm: Gross natural color descending aorta opened into false channel



-
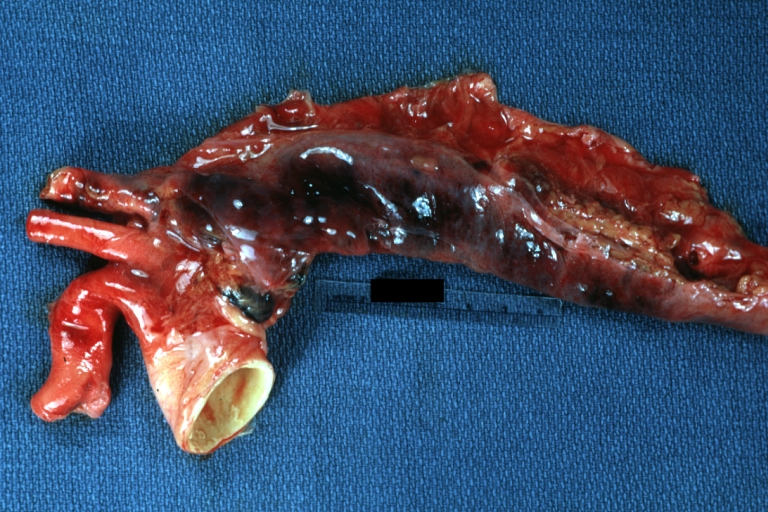
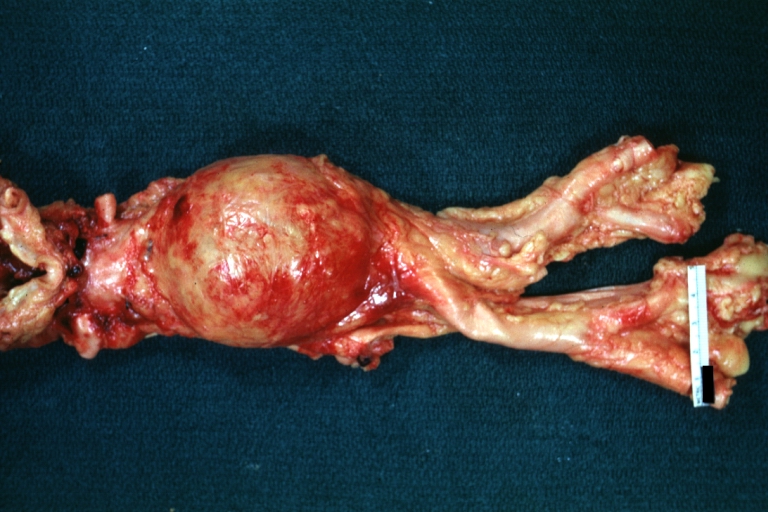 Abdominal Aneurysm: Gross, natural color, unopened specimen with about a six centimeter aneurysm between renals and bifurcation (a very good example of opened aneurysm)
Abdominal Aneurysm: Gross, natural color, unopened specimen with about a six centimeter aneurysm between renals and bifurcation (a very good example of opened aneurysm) -
 Abdominal Aneurysm: Gross, natural color, an opened aneurysm showing quite well laminated thrombus
Abdominal Aneurysm: Gross, natural color, an opened aneurysm showing quite well laminated thrombus -
 Atherosclerosis with Mural Thrombi: Gross, natural color, a nice photo of descending thoracic aorta with extensive ulcerated plaques and mural thrombi in distal portion. The case also has an abdominal aneurysm
Atherosclerosis with Mural Thrombi: Gross, natural color, a nice photo of descending thoracic aorta with extensive ulcerated plaques and mural thrombi in distal portion. The case also has an abdominal aneurysm



-
 Pseudoaneurysm Ruptured Into Duodenum: Gross natural color aorta and duodenum with arrow pointing to rupture point of aortobifemoral bypass pseudoaneurysm rupture and another in duodenum a very good demonstration of this very well known complication of aortic prostheses
Pseudoaneurysm Ruptured Into Duodenum: Gross natural color aorta and duodenum with arrow pointing to rupture point of aortobifemoral bypass pseudoaneurysm rupture and another in duodenum a very good demonstration of this very well known complication of aortic prostheses -
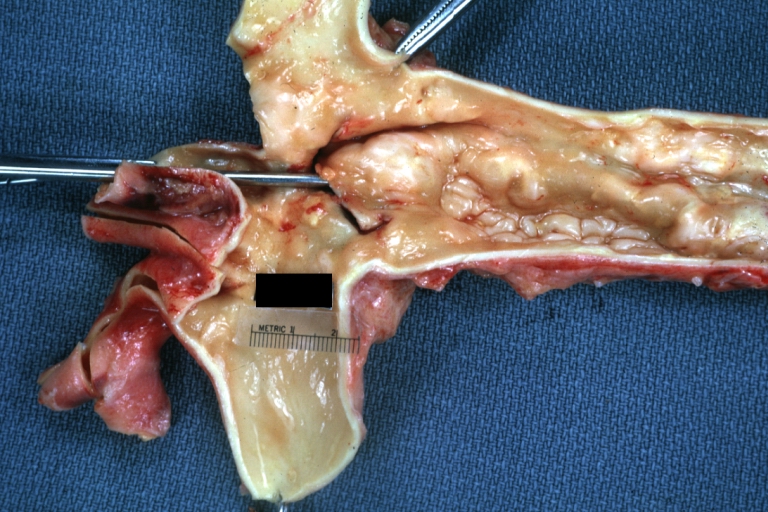
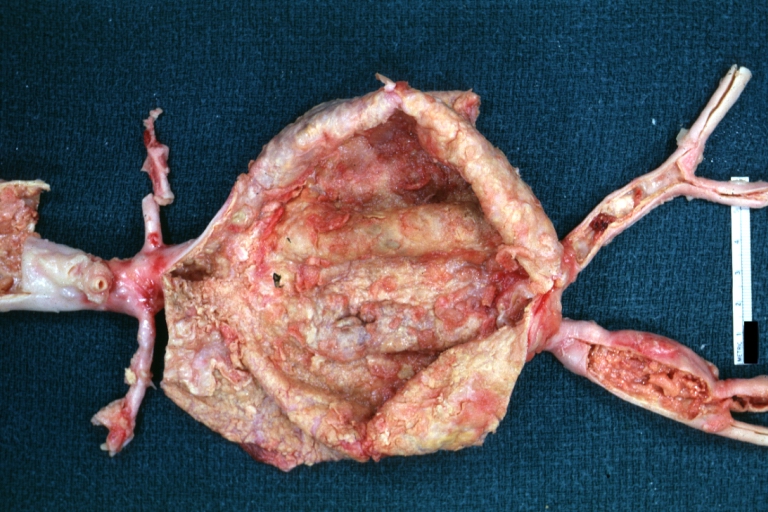 Abdominal Aneurysm: Gross, natural color, large aneurysm opened showing sessile calcified plaques with no mural thrombus. Lesion extends from renal arteries to the bifurcation (the same lesion seen externally with focus of rupture)
Abdominal Aneurysm: Gross, natural color, large aneurysm opened showing sessile calcified plaques with no mural thrombus. Lesion extends from renal arteries to the bifurcation (the same lesion seen externally with focus of rupture) -
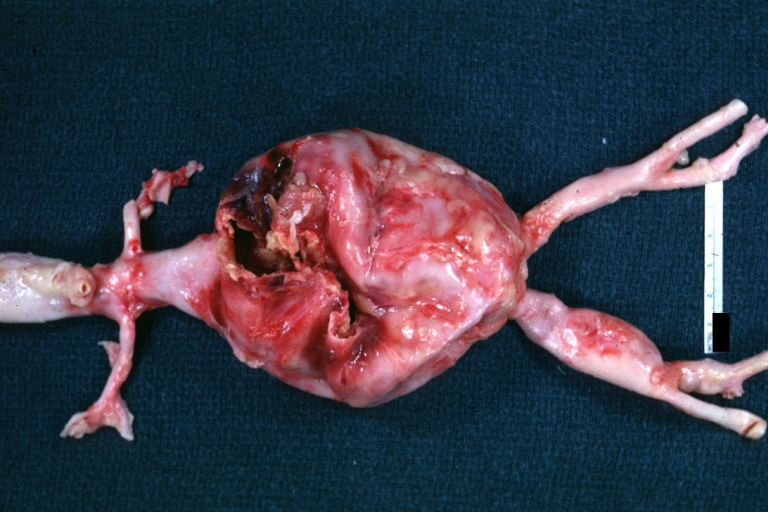 Abdominal Aneurysm Ruptured: Gross, natural color, external view with large area of apparent rupture. Aorta is opened to show this aneurysm)
Abdominal Aneurysm Ruptured: Gross, natural color, external view with large area of apparent rupture. Aorta is opened to show this aneurysm)



-
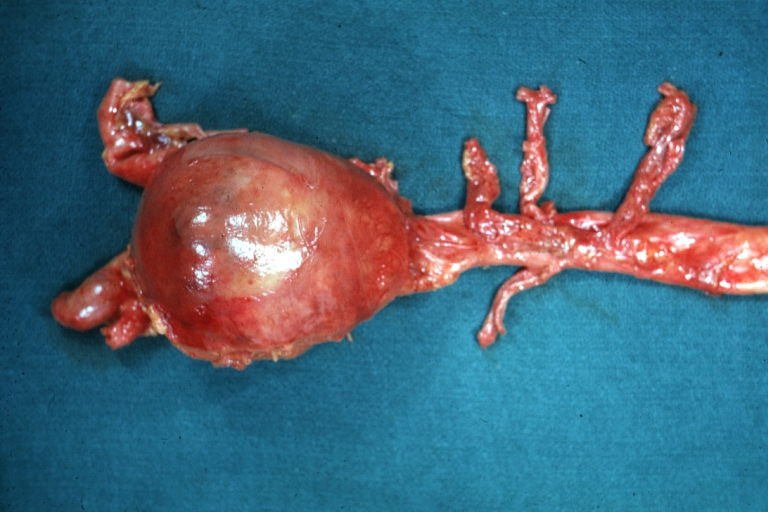 Abdominal Aneurysm: Gross, natural color, unopened large and quite typical aneurysm extending from below renal arteries to bifurcation
Abdominal Aneurysm: Gross, natural color, unopened large and quite typical aneurysm extending from below renal arteries to bifurcation -
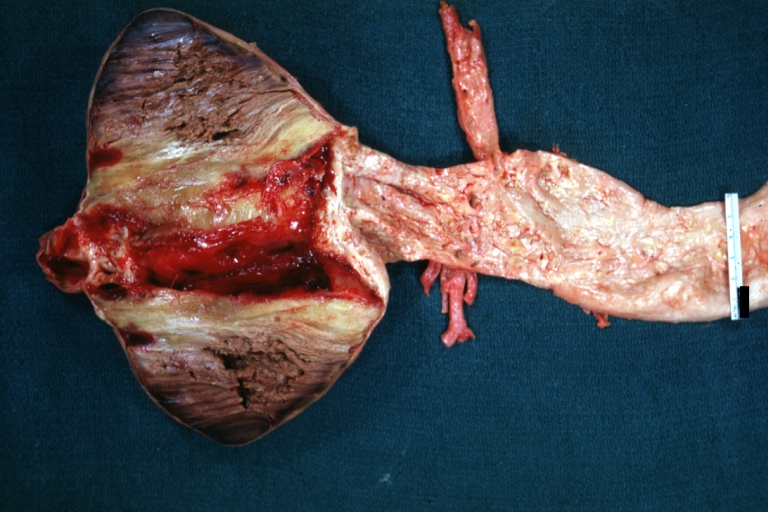 Abdominal Aneurysm: Gross, natural color, opened aneurysm with well shown and typical laminated thrombus (external view)
Abdominal Aneurysm: Gross, natural color, opened aneurysm with well shown and typical laminated thrombus (external view) -
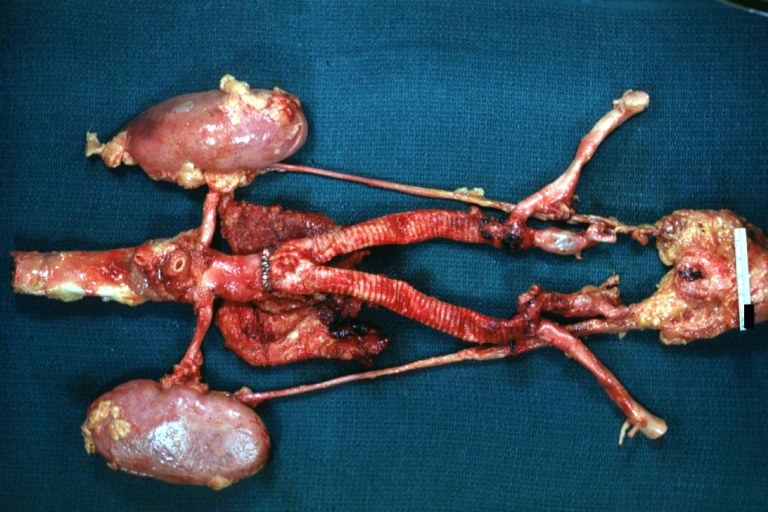 Aortobifemoral Prosthesis: Gross, natural color, nice dissection showing Dacron prosthesis replacing abdominal segment of aorta with portion of atherosclerotic aneurysm with renal arteries and kidneys
Aortobifemoral Prosthesis: Gross, natural color, nice dissection showing Dacron prosthesis replacing abdominal segment of aorta with portion of atherosclerotic aneurysm with renal arteries and kidneys



-
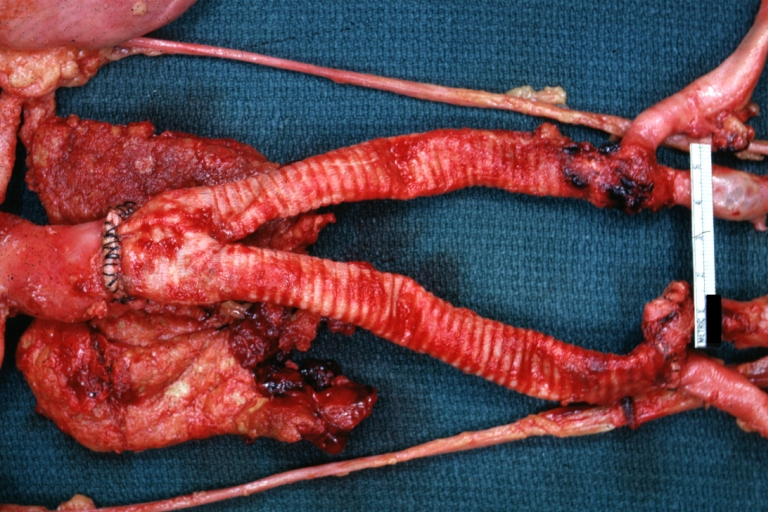 Aortobifemoral Prosthesis: Gross natural color close-up view of nicely dissected prosthesis extending from below renals to common iliac arteries portion of atherosclerotic aneurysm behind prosthesis
Aortobifemoral Prosthesis: Gross natural color close-up view of nicely dissected prosthesis extending from below renals to common iliac arteries portion of atherosclerotic aneurysm behind prosthesis -
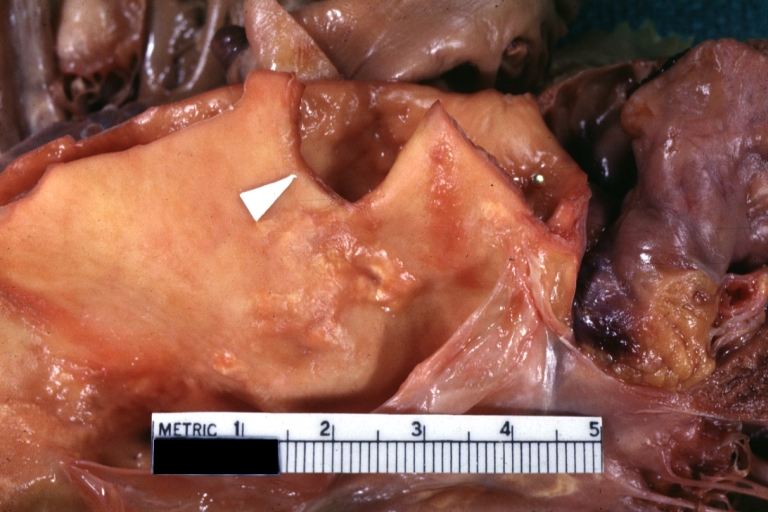
 Dissecting Aneurysm: Gross natural color close-up view of aortic valve and proximal aortic arch with ruptured intima rather good illustration of this lesion
Dissecting Aneurysm: Gross natural color close-up view of aortic valve and proximal aortic arch with ruptured intima rather good illustration of this lesion -
 Syphilitic Aneurysm: Gross natural color rather a close-up view and outstanding photo of aneurysm ruptured into the left main stem bronchus
Syphilitic Aneurysm: Gross natural color rather a close-up view and outstanding photo of aneurysm ruptured into the left main stem bronchus



-
 Syphilitic Aneurysm: Gross natural color typical tree barking in aorta aneurysm opening is seen in which is a thrombus aneurysm ruptured into left main stem bronchus (shown very well)
Syphilitic Aneurysm: Gross natural color typical tree barking in aorta aneurysm opening is seen in which is a thrombus aneurysm ruptured into left main stem bronchus (shown very well) -
 Dissecting Aneurysm Chronic: Gross natural color first portion of aortic arch with intimal rent well shown with healed margins and view into false channel that shows a surface looking like atherosclerosis which is known to develop in a chronic dissection
Dissecting Aneurysm Chronic: Gross natural color first portion of aortic arch with intimal rent well shown with healed margins and view into false channel that shows a surface looking like atherosclerosis which is known to develop in a chronic dissection -
 Dissecting Aneurysm Chronic: Gross, natural color, closer view of the previous one (a very good example)
Dissecting Aneurysm Chronic: Gross, natural color, closer view of the previous one (a very good example)



References
- ↑ Jain D, Dietz HC, Oswald GL, Maleszewski JJ, Halushka MK (2011). “Causes and histopathology of ascending aortic disease in children and young adults”. Cardiovasc Pathol. 20 (1): 15–25. doi:10.1016/j.carpath.2009.09.008. PMC 3046386. PMID 19926309.
- ↑ Grebe, Alena; Latz, Eicke (2013). “Cholesterol Crystals and Inflammation”. Current Rheumatology Reports. 15 (3). doi:10.1007/s11926-012-0313-z. ISSN 1523-3774.
- ↑ Yetkin, Ertan; Ozturk, Selcuk (2018). “Dilating Vascular Diseases: Pathophysiology and Clinical Aspects”. International Journal of Vascular Medicine. 2018: 1–9. doi:10.1155/2018/9024278. ISSN 2090-2824.
- ↑ Maguire, Eithne M.; Pearce, Stuart W. A.; Xiao, Rui; Oo, Aung Y.; Xiao, Qingzhong (2019). “Matrix Metalloproteinase in Abdominal Aortic Aneurysm and Aortic Dissection”. Pharmaceuticals. 12 (3): 118. doi:10.3390/ph12030118. ISSN 1424-8247.
- ↑ Li, Hanrong; Bai, Shuling; Ao, Qiang; Wang, Xiaohong; Tian, Xiaohong; Li, Xiang; Tong, Hao; Hou, Weijian; Fan, Jun (2018). “Modulation of Immune-Inflammatory Responses in Abdominal Aortic Aneurysm: Emerging Molecular Targets”. Journal of Immunology Research. 2018: 1–15. doi:10.1155/2018/7213760. ISSN 2314-8861.
- ↑ Aggarwal S, Qamar A, Sharma V, Sharma A (2011). “Abdominal aortic aneurysm: A comprehensive review”. Exp Clin Cardiol. 16 (1): 11–5. PMC 3076160. PMID 21523201.
- ↑ Ramella M, Boccafoschi F, Bellofatto K, Follenzi A, Fusaro L, Boldorini R; et al. (2017). “Endothelial MMP-9 drives the inflammatory response in abdominal aortic aneurysm (AAA)”. Am J Transl Res. 9 (12): 5485–5495. PMC 5752898. PMID 29312500.
- ↑ Clifton, MA: Familial abdominal aortic aneurysms. Br. J. Surg., 64, 1977, p. 765-766
- ↑ Norman, Paul E.; Curci, John A. (2013). “Understanding the Effects of Tobacco Smoke on the Pathogenesis of Aortic Aneurysm”. Arteriosclerosis, Thrombosis, and Vascular Biology. 33 (7): 1473–1477. doi:10.1161/ATVBAHA.112.300158. ISSN 1079-5642.
- ↑ Wang, Linda J.; Prabhakar, Anand M.; Kwolek, Christopher J. (2018). “Current status of the treatment of infrarenal abdominal aortic aneurysms”. Cardiovascular Diagnosis and Therapy. 8 (S1): S191–S199. doi:10.21037/cdt.2017.10.01. ISSN 2223-3652.
- ↑ Fitridge R, Thompson M (2011). “Mechanisms of Vascular Disease: A Reference Book for Vascular Specialists”. PMID 30485032.
Causes
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Vendhan Ramanujam M.B.B.S [2] Ramyar Ghandriz MD[3]
Overview
The most common cause of abdominal aortic aneurysm is atherosclerosis.
Causes
Life Threatening Causes
Life-threatening causes include conditions which may result in death or permanent disability within 24 hours if left untreated.[1]
Common Causes
Causes by Organ System
Causes in Alphabetical Order
References
- ↑ 1.0 1.1 Porter, Robert (2011). The Merck manual of diagnosis and therapy. Whitehouse Station, N.J: Merck Sharp & Dohme Corp. ISBN 9780911910193.
- ↑ Santosa, F.; Schrader, S.; Nowak, T.; Luther, B.; Kröger, K.; Bufe, A. (2013). “Thoracal, abdominal and thoracoabdominal aortic aneurysm”. Int Angiol. 32 (5): 501–5. PMID 23903309. Unknown parameter
|month=ignored (help) - ↑ Singh, K.; Bønaa, KH.; Jacobsen, BK.; Bjørk, L.; Solberg, S. (2001). “Prevalence of and risk factors for abdominal aortic aneurysms in a population-based study : The Tromsø Study”. Am J Epidemiol. 154 (3): 236–44. PMID 11479188. Unknown parameter
|month=ignored (help)
Differentiating Abdominal Aortic Aneurysm from other Diseases
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor-In-Chief: Cafer Zorkun, M.D., Ph.D. [2]; Hardik Patel, M.D. Ramyar Ghandriz MD[3]
Overview
An abdominal aortic aneurysm should be differentiated from other causes of abdominal pain such as acute cholecystitis, gastrointestinal bleeding, perforated peptic ulcer, ischemic bowel, nephrolithiasis, pyelonephritis, appendicitis, cholelithiasis, large bowel obstruction, small bowel obstruction, pancreatitis, musculoskeletal pain, myocardial infarction, and urinary tract infection.
Differentiating Abdominal Aortic Aneurysm from other Diseases
- A patient becomes symptomatically after abdominal aortic rupture, so the differentiation is according to the rupture which causes acute abdomen signs and symptoms.
- Non-symptomatic AAA is diagnosed through abdominal ultrasound with no other differentials.
- In a patient with a suspected abdominal aortic aneurysm, the following conditions also need to be considered:[1]
- Acute cholecystitis
- Gastritis and peptic ulcer disease
- Gastrointestinal bleeding
- Ischemic bowel
- Diverticulitis
- Nephrolithiasis
- Pyelonephritis
- Appendicitis
- Cholelithiasis
- Large bowel obstruction
- Small bowel obstruction
- Pancreatitis
- Musculoskeletal pain
- Myocardial infarction
- Urinary tract infection in women
References
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Epidemiology and Demographics
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor-In-Chief: Cafer Zorkun, M.D., Ph.D. [2]; Aarti Narayan, M.B.B.S [3]
Overview
Abdominal aortic aneurysm is the 13th leading cause of death in the US. Abdominal aortic aneurysms are more common in developed countries. Elderly, caucasian males who are smokers are at a higher risk for developing an abdominal aortic aneurysm.
Epidemiology and Demographics
Incidence
- The incidence of abdominal aortic aneurysms increases after age 60 and peaks in the seventh and eighth decades of life.[1]
Prevalence
- The prevalence among males over 60 years is 2000-6000/100,000.[2]
Age
- Abdominal aortic aneurysms (AAA) is a disease of the elderly, and is the 10th leading cause of death in older men in the United States.[3]
- An individual’s risk of AAA increases by 6% per decade of life
- Rupture of the AAA occurs in 1-3% of men aged 65 or more with an associated mortality rate of 70-95%.[4]
- AAA tends to cluster in families, therefore affecting younger members of families in the absence of traditional acquired risk factors.
Gender
- Abdominal aortic aneurysm is 5 times more common in men than women.[5]
Race
- The disease tends to affect older Caucasian males and is 3.5 times more common in Caucasian men than in African-American men.[6]
Developed Countries
- In the US, the incidence of abdominal aortic aneurysm is 2-4% in the adult population.[7]
Developing Countries
- Abdominal aortic aneurysm is uncommon in individuals of African, African American, Asian and Hispanic heritage.[8]
Other
References
- ↑ Zommorodi, Sayid; Leander, Karin; Roy, Joy; Steuer, Johnny; Hultgren, Rebecka (2018). “Understanding abdominal aortic aneurysm epidemiology: socioeconomic position affects outcome”. Journal of Epidemiology and Community Health. 72 (10): 904–910. doi:10.1136/jech-2018-210644. ISSN 0143-005X.
- ↑ Anderson, Oliver; Shiralkar, Sandy (2008). “Prevalence of Abdominal Aortic Aneurysms in Over 65-Year-Old Men with Inguinal Hernias”. The Annals of The Royal College of Surgeons of England. 90 (5): 386–388. doi:10.1308/003588408X285937. ISSN 0035-8843.
- ↑ Umebayashi, Ryoko; Uchida, Haruhito A.; Wada, Jun (2018). “Abdominal aortic aneurysm in aged population”. Aging. 10 (12): 3650–3651. doi:10.18632/aging.101702. ISSN 1945-4589.
- ↑ Lindholt JS, Juul S, Fasting H, Henneberg EW (2005). “Screening for abdominal aortic aneurysms: single centre randomised controlled trial”. BMJ. 330 (7494): 750. doi:10.1136/bmj.38369.620162.82. PMC 555873. PMID 15757960. Review in: ACP J Club. 2005 Sep-Oct;143(2):39
- ↑ Hannawa KK, Eliason JL, Upchurch GR (2009). “Gender differences in abdominal aortic aneurysms”. Vascular. 17 Suppl 1: S30–9. doi:10.2310/6670.2008.00092. PMC 2913052. PMID 19426607.
- ↑ Lackland, Daniel T. (2014). “Racial Differences in Hypertension: Implications for High Blood Pressure Management”. The American Journal of the Medical Sciences. 348 (2): 135–138. doi:10.1097/MAJ.0000000000000308. ISSN 0002-9629.
- ↑ Folli, Franco; Li, Xi; Zhao, Ge; Zhang, Jian; Duan, Zhiquan; Xin, Shijie (2013). “Prevalence and Trends of the Abdominal Aortic Aneurysms Epidemic in General Population – A Meta-Analysis”. PLoS ONE. 8 (12): e81260. doi:10.1371/journal.pone.0081260. ISSN 1932-6203.
- ↑ “StatPearls”. 2019. PMID 29262134.
- ↑ Aune, Dagfinn; Schlesinger, Sabrina; Norat, Teresa; Riboli, Elio (2018). “Tobacco smoking and the risk of abdominal aortic aneurysm: a systematic review and meta-analysis of prospective studies”. Scientific Reports. 8 (1). doi:10.1038/s41598-018-32100-2. ISSN 2045-2322.
Risk Factors
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Cafer Zorkun, M.D., Ph.D. [2]; Vishnu Vardhan Serla M.B.B.S. [3] Ramyar Ghandriz MD[4]
Overview
The most significant modifiable risk factor for the development of an abdominal aortic aneurysm is smoking which increases the risk of aneurysm development 8 fold. Advanced age and family history are the strongest non-modifiable risk factors for the development of an abdominal aortic aneurysm. Hypercholesterolemia and hypertension are risk factors as well. Both diabetes mellitus and being of African American descent appear to be associated with a lower incidence of abdominal aortic aneurysm. Caucasians report a higher incidence of AAA when compared to the non Caucasians. An increased rate of expansion of abdominal aortic aneurysm is related to systolic hypertension, wide pulse pressure, and ongoing smoking. The risk of abdominal aortic aneurysm rupture is proportional to the size and rate of growth of the aneurysm. Abdominal aortic aneurysms greater than 5 cm diameter or those that grow faster than 1 cm per year have a significantly increased risk of rupture and are indications for elective operative repair. Advanced age, female gender, hypertension, active smoking, outpouchings, and mural thrombus are also risk factors for abdominal aortic aneurysm rupture.
Risk Factors
Risk Factors for Abdominal Aortic Aneurysm Development
- The strongest independent acquired risk factor for AAA is smoking. In a study by Wilmink et. al, it is shown that current smokers are 7.6 times more likely to manifest an abdominal aortic aneurysm than non smokers. Risk of developing abdominal aortic aneurysm increases related to increase in smoking duration, but amount of cigarettes smoked per day did not provide any further information.[1][2]
- Most important non-reversible risk factors are advanced age and family history. There is an increased risk of developing abdominal aortic aneurysm by 2 to 5 folds with family history,compared to normal society[3][4][5].
- The prevalence of abdominal aortic aneurysms among first-degree relatives diagnosed with abdominal aortic aneurysms increases to 15-29%, compared with 2% among relatives of controls.[6]
- Male sex
- Caucasian race
- Genetic factors like genetic polymorphism and presence of HLA-DRB 1 alleles B1*0404 and HLA-DRB1 alleles B1*15[7]
- Hypertension
- Known atherosclerotic disease – coronary artery disease, cerebrovascular disease, peripheral artery disease
- Hypercholesterolemia
- Chronic obstructive pulmonary disease
Cardiovascular risk factors tend to cluster in certain patients:
- Men who smoke and are hypertensive have an incidence of abdominal aortic aneurysm that is 2-5 times than those of the general population.
- Similarly, women over the age of 60 with cardiovascular risk factors are 2-3 times more likely to develop aneurysmal disease.
- Both diabetes mellitus and being of African American descent appear to be associated with a lower incidence of abdominal aortic aneurysm.
Risk Factors for Rapid Abdominal Aortic Aneurysm Expansion
- In small abdominal aortic aneurysm (3-5.4 cm), the expansion rate appears to be proportional to the initial diameter.[8]
- Independent of the initial diameter of the aneurysm, other factors related to rapid expansion of an abdominal aortic aneurysm are:
- Systolic hypertension
- Wide pulse pressure
- Ongoing smoking
Factors not Associated with more Rapid Expansion of Abdominal Aortic Aneurysm
C-reactive protein levels have also been found to be elevated in larger aneurysms, however they do not appear to be linked to rapid expansion.[9]
Risk Factors for Abdominal Aortic Aneurysm Rupture
The risk of rupture is proportional to the size and rate of growth of the aneurysm. Aneurysms greater than 5 cm diameter or those that grow faster than 1 cm per year have a significantly increased risk of rupture and are indications for elective operative repair.[10][11] In the UK small aneurysm trial, important independent variables were identified with abdominal aortic aneurysm rupture:
- Female sex
- Increased diameter of the abdominal aortic aneurysm
- Current smoker
- Mean blood pressure
- Increased age
- Forced expiratory volume in 1 second
- Size at diagnosis is one of the best predictors of rupture.
- The risk increases substantially when the diameter exceeds 6 cm in men and 5 cm in women.
- Small aneurysms can rupture as well, and are threefold more likely to rupture in women.
- Localized outpouchings seems to increase the aneurysm’s vulnerability for rupture.
- It has been suggested that the aneurysm growth and rupture correlate with the growth of the aneurysm’s mural thrombus: the part of the aneurysm wall that is covered with thrombus has been shown to be thinner and showed focal anoxia, inflammation, apoptosis of the smooth muscle cells, and a more degraded extracellular matrix than wall segments not covered by the thrombus.
Management of Patients With Peripheral Artery Disease
Atherosclerotic Risk Factors
- (Compilation of 2005 and 2011 ACCF/AHA Guideline Recommendations) : A Report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines[12]
| Class I |
| “1.In patients with AAAs, blood pressure and fasting serum lipid values should be monitored and controlled as recommended for patients with atherosclerotic disease. (Level of Evidence: C)” |
| “2.Patients with aneurysms or a family history of aneurysms should be advised to stop smoking and be offered smoking cessation interventions, including behavior modification, nicotine replacement, or bupropion(Level of Evidence: B) ” |
References
- ↑ Wilmink TB, Quick CR, Day NE (1999). “The association between cigarette smoking and abdominal aortic aneurysms”. Journal of Vascular Surgery. 30 (6): 1099–105. PMID 10587395. Unknown parameter
|month=ignored (help) - ↑ Kent, KC.; Zwolak, RM.; Egorova, NN.; Riles, TS.; Manganaro, A.; Moskowitz, AJ.; Gelijns, AC.; Greco, G. (2010). “Analysis of risk factors for abdominal aortic aneurysm in a cohort of more than 3 million individuals”. J Vasc Surg. 52 (3): 539–48. doi:10.1016/j.jvs.2010.05.090. PMID 20630687. Unknown parameter
|month=ignored (help) - ↑ Larsson, E.; Granath, F.; Swedenborg, J.; Hultgren, R. (2009). “A population-based case-control study of the familial risk of abdominal aortic aneurysm”. J Vasc Surg. 49 (1): 47–50, discussion 51. doi:10.1016/j.jvs.2008.08.012. PMID 19028058. Unknown parameter
|month=ignored (help) - ↑ Salo, JA.; Soisalon-Soininen, S.; Bondestam, S.; Mattila, PS. (1999). “Familial occurrence of abdominal aortic aneurysm”. Ann Intern Med. 130 (8): 637–42. PMID 10215559. Unknown parameter
|month=ignored (help) - ↑ Lederle, FA.; Johnson, GR.; Wilson, SE.; Chute, EP.; Hye, RJ.; Makaroun, MS.; Barone, GW.; Bandyk, D.; Moneta, GL. (2000). “The aneurysm detection and management study screening program: validation cohort and final results. Aneurysm Detection and Management Veterans Affairs Cooperative Study Investigators”. Arch Intern Med. 160 (10): 1425–30. PMID 10826454. Unknown parameter
|month=ignored (help) - ↑ Aggarwal S, Qamar A, Sharma V, Sharma A (2011). “Abdominal aortic aneurysm: A comprehensive review”. Exp Clin Cardiol. 16 (1): 11–5. PMC 3076160. PMID 21523201.
- ↑ Rasmussen, Todd E; Hallett, John W.; Mathieu Metzger, Renate L.; Richardson, Darcy M.; Harmsen, William S.; Goronzy, Jorg J.; Weyand, Cornelia M. (1997). “Genetic risk factors in inflammatory abdominal aortic aneurysms: Polymorphic residue 70 in the HLA-DR B1 gene as a key genetic element”. Journal of Vascular Surgery. 25 (2): 356–364. doi:10.1016/S0741-5214(97)70358-6. ISSN 0741-5214.
- ↑ Devaraj, S; Dodds, SR (2008). “Ultrasound Surveillance of Ectatic Abdominal Aortas”. The Annals of The Royal College of Surgeons of England. 90 (6): 477–482. doi:10.1308/003588408X301064. ISSN 0035-8843.
- ↑ Norman, Paul; Spencer, Carole A.; Lawrence-Brown, Michael M.; Jamrozik, Konrad (2004). “C-Reactive Protein Levels and the Expansion of Screen-Detected Abdominal Aortic Aneurysms in Men”. Circulation. 110 (7): 862–866. doi:10.1161/01.CIR.0000138746.14425.00. ISSN 0009-7322.
- ↑ Dahnert W. Radiology Review Manual, 5th edition. Lippincott, Williams and Wilkins 2003
- ↑ Rakita D, Newatia A, Hines JJ, Siegel DN, Friedman B (2007). “Spectrum of CT findings in rupture and impending rupture of abdominal aortic aneurysms”. Radiographics. 27 (2): 497–507. doi:10.1148/rg.272065026. PMID 17374865.
- ↑ Rooke TW, Hirsch AT, Misra S, Sidawy AN, Beckman JA, Findeiss L; et al. (2013). “Management of patients with peripheral artery disease (compilation of 2005 and 2011 ACCF/AHA Guideline Recommendations): a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines”. J Am Coll Cardiol. 61 (14): 1555–70. doi:10.1016/j.jacc.2013.01.004. PMC 4492473. PMID 23473760.
Screening
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Caitlin J. Harrigan [2]; Vishnu Vardhan Serla M.B.B.S. [3] Ramyar Ghandriz MD[4]
Overview
Approximately 16% of large abdominal aortic aneurysms (diameter > 5.5 cm) rupture, causing 9,000 AAA-related deaths in the United States per year. Several studies have shown that screening can drastically reduce the aneurysm rupture rate by 45-49% for men older than 60, and reduce AAA-related mortality by 21-68%. In a landmark study randomizing 67,800 men, (The Multicenter Aneurysm Screening Study) aneurysm-related mortality was 53% lower in the screening group as compared with control patients. The United States Preventive Services Task Force (USPSTF) recommends one-time screening for abdominal aortic aneurysm (AAA) by ultrasonography in any man, aged 65 to 75 who has ever smoked. The USPSTF makes no recommendation for or against screening for AAA in men aged 65 to 75 who have never smoked. The USPSTF recommends against routine screening for AAA in women.
Screening
- Patients with abdominal aortic aneurysms (AAAs) are often asymptomatic, with the first clinical event often being fatal or life-threatening.[1]
- Due to this apparent “detection gap,” between the asymptomatic disease and clinically apparent disease screening may be of benefit.[2]
- AAAs are usually asymptomatic during this “detection gap”, with the possibility of as many as one in three rupturing if left untreated.[3]
- A ruptured AAA carries an overall mortality rate approaching 75%, with a mortality rate of 2-6% in those patients who underwent elective surgical repair.[4]
- Approximately 16% of large AAAs (diameter >5.5 cm) rupture, causing 9,000 AAA-related deaths in the United States per year.
- Several studies have shown that screening can drastically reduce the aneurysm rupture rate by 45-49% for men older than 60, and reduce AAA-related mortality by 21-68%.
Landmark Trial in AAA Screening
- In the largest population-based screening study to date, the Multi center Aneurysm Screening Study (MASS) randomized 67,800 men (age 65-74) equally to either a group that received an ultrasound screening for AAA or a control group. [3][2]
- In the screening group, men with an abdominal aorta larger than 3 cm in diameter were followed with serial ultrasounds for a mean duration of 4.1 years.
- When the aneurysm reached 5.5 cm, grew more than 1 cm/year or became symptomatic, it was repaired surgically.
- The aneurysm-related mortality was 53% lower in the screening group.
- However, despite the relative risk reduction in the MASS trial, there were 65 AAA-related deaths in the intervention group (absolute risk of 0.19%), and 113 AAA-related deaths in the control group (absolute risk 0.33%).
Screening
Cost-Effectiveness
It is estimated that abdominal aortic aneurysm screening is as cost-effective as mammography for breast cancer detection as well as therapeutic interventions such as coronary artery bypass graft surgery with a cost of $11,285 per quality adjusted life year saved.[5]
Safety
- Physical examinations may detect large AAAs, but is not specific or sensitive enough to detect smaller ones.[6]
- The cornerstone of AAA screening is ultrasonography. It is available in almost every medical center and many physician offices.
- Abdominal aortic ultrasonography is fast, inexpensive, safe and well-tolerated by most patients
- It is highly accurate with 95% sensitivity and 100% specificity for AAAs.[7]
- The most important limitations of ultrasonography are:
- Computed tomography (CT) and magnetic resonance angiography are accurate for diagnosing AAA, but are less often used as a first-degree screening modality because of the lack of availability, and the risks and side-effects of iodinated contrasts for CT.
Ethics
- Screening using ultrasonography causes no serious side effects, and is therefore ethically acceptable.[8]
- Several studies have shown that screening for AAAs and diagnosing asymptomatic small aneurysms in clinical practice were not associated with long-term emotional or psychological stress to patients.[9]
- A simple screening ultrasound test costs approximately $500, for which Medicare usually reimburses $160.
- Lack of insurance coverage raises the ethical dilemma of AAA screening being available only to the elite who can afford it.
Identification as a Trigger to Screen for Polyvascular Disease
- Small, asymptomatic AAAs (3-5.5 cm) may serve as a marker for vascular disease elsewhere, thus finding one provides good reason to aggressively start to modify risk factors.
Follow-Up Intervals
- Periodic ultrasonographic surveillance is recommended for aneurysms smaller than the repair cutoff.
- If an abdominal aortic aneurysm is 4 to 5.4 cm then surveillance ultrasounds can be obtained every 6 to 12 months.
- If an abdominal aortic aneurysm is 3 to 4 cm then surveillance ultrasounds can be obtained every 2 to 3 years.
- However, definite and unified parameters for appropriate surveillance intervals have not yet been determined because clinical trials have enrolled heterogeneous populations and used different standards for diagnosis and management.
- In general, older men may need more frequent follow-up scans, as men older than 70 years have three times the rate of progression than younger men.
- Aneurysm diameters determined by ultrasound may vary up to 0.5 cm, which should be considered when recommending optimal times for rescanning and repair.
Recommendations by The United States Preventive Service Task Force
Clinical practice guidelines[10] and systematic review[11] by the United States Preventive Service Task Force in 2014 stated:
- “The USPSTF recommends 1-time screening screening for AAA with ultrasonography in men aged 65 to 75 years who have ever smoked.”
- “The USPSTF recommends that clinicians selectively offer screening for AAA in men aged 65 to 75 years who have never smoked”
- “The USPSTF concludes that the current evidence is insufficient to assess the balance of benefits and harms of screening for AAA in women aged 65 to 75 years who have ever smoked”
- “The USPSTF recommends against routine screening for AAA in women who have never smoked.”
The projected benefit of screening is:[12]
- Number needed to invite to prevent one death is 175 – 225.
Management of Patients With Peripheral Artery Disease (Compilation of 2005 and 2011 ACCF/AHA Guideline Recommendations) : A Report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines
Screening High-Risk Populations[13]
| Class I |
| “1.Men 60 years of age or older who are either the siblings or offspring of patients with AAAs should undergo physical examination and ultrasound screening for detection of aortic aneurysms. (Level of Evidence: B)” |
| Class IIa |
| “1.Men who are 65 to 75 years of age who have ever smoked should undergo a physical examination and 1-time ultrasound screening for detection of AAAs. (Level of Evidence: B)” |
Sources
http://www.uspreventiveservicestaskforce.org/uspstf/uspsaneu.htm
References
- ↑ Gillum RF (1995). “Epidemiology of aortic aneurysm in the United States”. Journal of Clinical Epidemiology. 48 (11): 1289–98. PMID 7490591. Retrieved 2012-10-27. Unknown parameter
|month=ignored (help) - ↑ 2.0 2.1 “Multicentre aneurysm screening study (MASS): cost effectiveness analysis of screening for abdominal aortic aneurysms based on four year results from randomised controlled trial”. BMJ (Clinical Research Ed.). 325 (7373): 1135. 2002. PMC 133450. PMID 12433761. Retrieved 2012-10-27. Unknown parameter
|month=ignored (help) - ↑ 3.0 3.1 Ashton HA, Buxton MJ, Day NE, Kim LG, Marteau TM, Scott RA, Thompson SG, Walker NM (2002). “The Multicentre Aneurysm Screening Study (MASS) into the effect of abdominal aortic aneurysm screening on mortality in men: a randomised controlled trial”. Lancet. 360 (9345): 1531–9. PMID 12443589. Retrieved 2012-10-27. Unknown parameter
|month=ignored (help) - ↑ Pasternak RC, Abrams J, Greenland P, Smaha LA, Wilson PW, Houston-Miller N (2003). “34th Bethesda Conference: Task force #1–Identification of coronary heart disease risk: is there a detection gap?”. Journal of the American College of Cardiology. 41 (11): 1863–74. PMID 12798553. Retrieved 2012-10-27. Unknown parameter
|month=ignored (help) - ↑ Kent KC, Zwolak RM, Jaff MR, Hollenbeck ST, Thompson RW, Schermerhorn ML, Sicard GA, Riles TS, Cronenwett JL (2004). “Screening for abdominal aortic aneurysm: a consensus statement”. Journal of Vascular Surgery. 39 (1): 267–9. doi:10.1016/j.jvs.2003.08.019. PMID 14718853. Retrieved 2012-10-27. Unknown parameter
|month=ignored (help) - ↑ Fink, Howard A.; Lederle, Frank A.; Roth, Craig S.; Bowles, Carolyn A.; Nelson, David B.; Haas, Michele A. (2000). “The Accuracy of Physical Examination to Detect Abdominal Aortic Aneurysm”. Archives of Internal Medicine. 160 (6): 833. doi:10.1001/archinte.160.6.833. ISSN 0003-9926.
- ↑ Rubano, Elizabeth; Mehta, Ninfa; Caputo, William; Paladino, Lorenzo; Sinert, Richard; Carpenter, Christopher (2013). “Systematic Review: Emergency Department Bedside Ultrasonography for Diagnosing Suspected Abdominal Aortic Aneurysm”. Academic Emergency Medicine. 20 (2): 128–138. doi:10.1111/acem.12080. ISSN 1069-6563.
- ↑ Haar, Gail ter (2011). “Ultrasonic imaging: safety considerations”. Interface Focus. 1 (4): 686–697. doi:10.1098/rsfs.2011.0029. ISSN 2042-8898.
- ↑ Vammen S, Lindholt JS, Ostergaard L, Fasting H, Henneberg EW (2001). “Randomized double-blind controlled trial of roxithromycin for prevention of abdominal aortic aneurysm expansion”. The British Journal of Surgery. 88 (8): 1066–72. doi:10.1046/j.0007-1323.2001.01845.x. PMID 11488791. Retrieved 2012-10-27. Unknown parameter
|month=ignored (help) - ↑ LeFevre ML (2014). “Screening for Abdominal Aortic Aneurysm: U.S. Preventive Services Task Force Recommendation Statement”. Ann Intern Med. doi:10.7326/M14-1204. PMID 24957320.
- ↑ Guirguis-Blake JM, Beil TL, Senger CA, Whitlock EP (2014). “Ultrasonography screening for abdominal aortic aneurysms: a systematic evidence review for the U.S. Preventive Services Task Force”. Ann Intern Med. 160 (5): 321–9. doi:10.7326/M13-1844. PMID 24473919. Review in: Ann Intern Med. 2014 May 20;160(10):JC6
- ↑ Burden AC (2014). “ACP Journal Club. Review: ultrasonography screening reduces long-term abdominal aortic aneurysm-related mortality”. Ann Intern Med. 160 (10): JC6. doi:10.7326/0003-4819-160-10-201405200-02006. PMID 24842440.
- ↑ Rooke TW, Hirsch AT, Misra S, Sidawy AN, Beckman JA, Findeiss L; et al. (2013). “Management of patients with peripheral artery disease (compilation of 2005 and 2011 ACCF/AHA Guideline Recommendations): a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines”. J Am Coll Cardiol. 61 (14): 1555–70. doi:10.1016/j.jacc.2013.01.004. PMC 4492473. PMID 23473760.
Natural History, Complications and Prognosis
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]
Overview
An aortic aneurysm can progress to a ruptured abdominal aortic aneurysm, which is a medical emergency associated with an extremely high mortality. Serious complications can also occur as a result of an aortic dissection, such as myocardial infarction, shock, stroke, kidney failure, and arterial emboli. A ruptured AAA carries an overall mortality rate approaching 75%, which is much higher than the mortality rate of 2-6% in those patients who underwent elective surgical repair. Approximately 16% of large AAAs (diameter >5.5 cm) rupture, causing 9,000 AAA-related deaths in the United States per year. Several studies have shown that screening can drastically reduce the aneurysm rupture rate by 45-49% for men older than 60, and reduce AAA-related mortality by 21-68%.
Natural History
Abdominal aortic aneurysms expand slowly over time. It is for this reason that ultrasound surveillance is recommended. The risk for rupture of an aneurysm depends on several factors[1]:
- Size of an aneurysm
- Risk of rupture increases greatly once the size of aneurysm reaches 5.5 cm.
- Rate of expansion
- If the rate of expansion exceeds 1 cm per year, this is an indication for surgery.
- Growth tends to be more rapid in smokers than non-smokers.
- Gender
- The risk of rupture is higher in women than in men.[2]
Management of Patients With Peripheral Artery Disease (Compilation of 2005 and 2011 ACCF/AHA Guideline Recommendations) : A Report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines
Aortic Aneurysm Rupture[3]
| Class I |
| “1. Patients with infrarenal or juxtarenal AAAs measuring 5.5 cm or larger should undergo repair to eliminate the risk of rupture. (Level of Evidence: B)” |
| “2.Patients with infrarenal or juxtarenal AAAs measuring 4.0 to 5.4 cm in diameter should be monitored by ultrasound or computed tomographic scans every 6 to 12 months to detect expansion. (Level of Evidence: A) ” |
| Class IIa |
| “1.Repair can be beneficial in patients with infrarenal or juxtarenal AAAs 5.0 to 5.4 cm in diameter. (Level of Evidence: B)” |
| “2.Repair is probably indicated in patients with suprarenal or type IV thoracoabdominal aortic aneurysms larger than 5.5 to 6.0 cm. (Level of Evidence: B)” |
| “3.In patients with AAAs smaller than 4.0 cm in diameter, monitoring by ultrasound examination every 2 to 3 years is reasonable. (Level of Evidence: B)” |
| Class III |
| “1.Intervention is not recommended for asymptomatic infrarenal or juxtarenal AAAs if they measure less than 5.0 cm in diameter in men or less than 4.5 cm in diameter in women(Level of Evidence: A)” |
Complications
When an abdominal aortic aneurysm ruptures, it is a true medical emergency. Aortic dissection occurs when the innermost lining of the artery tears and blood leaks into the wall of the artery. This most commonly occurs in the aorta within the chest. Complications include:
- Aortic rupture: Once an aneurysm has ruptured, it presents with a classic pain–hypotension-mass triad. The pain is classically reported in the abdomen, back or flank. It is usually acute, severe and constant, and may radiate through the abdomen to the back. The diagnosis of an abdominal aortic aneurysm can be confirmed at the bedside by the use of ultrasound. Rupture is indicated by the presence of free fluid in potential abdominal spaces, such as Morrison’s pouch, the splenorenal space, subdiaphragmatic spaces and peri-vesical spaces. A contrast-enhanced abdominal CT scan is needed for confirmation. Only 10-25% of patients survive a rupture due to large pre and post-operative mortality. Annual mortality from ruptured abdominal aneurysms in the United States alone is about 15,000.
- Acute aortic occlusion
- Aortocaval or aortoduodenal fistulae
- Arterial embolism
- Disseminated intravascular coagulation
- Heart attack
- Hypovolemic shock
- Kidney failure
- Stroke
Prognosis
Elective Surgery in the Absence of Abdominal Aortic Aneurysm Rupture
The outcome is usually good if an experienced surgeon repairs the aneurysm before it ruptures.
Emergency Surgery in the Setting of Abdominal Aortic Aneurysm Rupture
Rupture of an abdominal aortic aneurysm is associated with a 60% to 90% mortality before the patient reaches a hospital. It is associated with a 30% to 80% operative mortality among those patients who survive long enough to undergo surgery.
References
- ↑ Gillum RF (1995). “Epidemiology of aortic aneurysm in the United States”. Journal of Clinical Epidemiology. 48 (11): 1289–98. PMID 7490591. Retrieved 2012-10-27. Unknown parameter
|month=ignored (help) - ↑ Norman PE, Powell JT (2007). “Abdominal aortic aneurysm: the prognosis in women is worse than in men”. Circulation. 115 (22): 2865–9. doi:10.1161/CIRCULATIONAHA.106.671859. PMID 17548742. Unknown parameter
|month=ignored (help) - ↑ Rooke TW, Hirsch AT, Misra S, Sidawy AN, Beckman JA, Findeiss L; et al. (2013). “Management of patients with peripheral artery disease (compilation of 2005 and 2011 ACCF/AHA Guideline Recommendations): a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines”. J Am Coll Cardiol. 61 (14): 1555–70. doi:10.1016/j.jacc.2013.01.004. PMC 4492473. PMID 23473760.
Diagnosis
Diagnosis
History and Symptoms | Physical Examination | Abdominal X Ray | Ultrasound | CT | MRI | Other Imaging Findings
Looking for the patient version?
© 2026 MyEClinic – IFTM Institut für Telematik in der Medizin GmbH