
Uveitis
For patient information click here Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Tarek Nafee, M.D. [2], Mohamed Moubarak, M.D. [3]
Synonyms and keywords: Iritis; pars planitis; choroiditis; retinitis; chorioretinitis; anterior uveitis; posterior uveitis; sarcoid uveitis; Behcet’s uveitis; infectious uveitis; JIA uveitis; lupus uveitis; Multiple sclerosis uveitis; HLA-B27 uveitis; TINU syndrome; TINU; relapsing uveitis; chronic uveitis; acute anterior uveitis
Overview
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Tarek Nafee, M.D. [2] Basir Gill, M.B.B.S, M.D.[3]
Overview
Uveitis specifically refers to inflammation of the middle layer of the eye, termed the “uvea“. In common usage, it may refer to an inflammatory process involving the interior of the eye. The uvea consists of the iris, ciliary body, and choroid; it provides most of the blood supply to the retina. Uveitis may occur unilaterally or bilaterally, affect the anterior, intermediate, or posterior segment of the eye, may be infectious or non infectious, and granulomatous or non-granulomatous. The exact pathogenesis of uveitis is not fully understood. It is thought that uveitis is mediated by a genetic predisposition and an acquired cross immunity to infectious agents, or cross immunity to self-antigens due to underlying autoimmune diseases. Common causes of uveitis include seronegative spondyloarthropathy, sarcoidosis, juvenile idiopathic arthritis, systemic lupus erythematosus, Behçet syndrome, multiple sclerosis, AIDS, syphilis, and tuberculosis. Uveitis must be differentiated from other diseases such as conjunctivitis, endophthalmitis, or scleritis. A history of cigarette smoking is associated with all etiologies and subtypes of uveitis. Uveitis is estimated to be responsible for approximately 10% of the blindness in the United States. If left untreated uveitis can progress to permanent vision loss or result in complications such as cataracts, glaucoma, and retinal detachment. A history of an underlying associated condition along with symptoms of eye pain, redness, photophobia, floaters, and blurry vision is strongly suggestive of uveitis. There are no specific laboratory or physical examination findings associated with uveitis. Imaging modalities may assist in diagnosing an underlying condition, though have no diagnostic utility for uveitis itself. Slit lamp test is the diagnostic modality of choice. Other ophthalmologic studies may assist in further characterizing the disease. Mainstay medical therapy is by high dose corticosteroids. Targeted antimicrobials may be required to treat an underlying infection. Surgical intervention is reserved for managing complications of uveitis such as cataract surgery or glaucoma surgery. The only indicated guideline for screening is in patients suspected of or diagnosed with juvenile idiopathic arthritis. Prompt treatment of a potential underlying infection may help prevent development of uveitis.
Historical Perspective
Uveitis was first discovered by Hippocrates, a Greek physician, and was a well known to other major medical physicians, such as Galen and Aëtius of Amida. In 1952, corticosteroids were used to treat uveitis for the first time.[1]
Classification
Uveitis is best described using various, concurrent classification systems. Uveitis may be classified according to anatomical location into 4 subtypes, depending on which part of the uvea is primarily affected: anterior, intermediate, posterior, and panuveitis. Based on the duration of symptoms it may be further sub-classified as acute or chronic. Upon further investigation, uveitis may be classified according to histological features of the inflammation such as granulomatous or non-granulomatous. Additionally, uveitis may be described by the laterality of the condition (unilateral or bilateral). Finally, uveitis may be classified by general underlying systemic causes such as infectious, autoimmune, drug-induced, or idiopathic.[2][3][4][5][6]
Pathophysiology
The healthy eye maintains immune privilege, limiting responses to self and foreign antigens through the blood–retina barrier, regulatory T cells, and anti-inflammatory cytokines such as TGF-β and IL-10.[7][8] Noninfectious uveitis results from loss of immune tolerance to retinal proteins, causing aberrant T-cell activation.[7][8] Infectious uveitis arises when pathogens breach the blood–retina barrier and may amplify inflammation via antigenic mimicry.[8] In both forms, MHC class II–mediated antigen presentation activates CD4+ T cells, which differentiate into Th1 and Th17 cells that infiltrate ocular tissues and secrete IFN-γ, IL-2, and IL-17, driving recruitment of inflammatory cells and resulting in chorioretinitis, vasculitis, and edema. [7][8][9][10]
Causes
Common causes of uveitis include seronegative spondyloarthropathy, sarcoidosis, juvenile idiopathic arthritis, systemic lupus erythematosus, Behçet syndrome, multiple sclerosis AIDS, syphilis, and tuberculosis.[6][11]
Differentiating Uveitis from Other Diseases
Uveitis must be differentiated from other diseases that cause conjunctival injection, eye pain, photophobia, or visual disturbance. Masquerade syndromes, which are ophthalmic disorders that clinically present as either an anterior or posterior uveitis but are not primarily inflammatory, must be differentiated from uveitis. As uveitis manifests in a variety of clinical etiologies, differentiation must also be established in accordance with the particular subtype.[12][6][13][14]
Epidemiology and Demographics
Worldwide, the prevalence of uveitis ranges from 38 to 714 per 100,000 persons. The prevalence among different subtypes of uveitis varies greatly. Anterior, chronic, non-granulomatous and non-infectious subtypes are more commonly seen than others. The worldwide incidence of uveitis ranges from 17 to 52 per 100,000 persons per year. The age, sex, and race distribution is also dictated by the prevalence of the underlying cause within those demographic groups. Uveitis is associated with 3% to 10% of vision impairment in the US and Europe, and up to one-fourth of blindness in low- and middle-income countries.[5][6][11][15]
Risk Factors
A history of cigarette smoking is associated with all etiologies and subtypes of uveitis.[16] Some underlying causes have specific potent risk factors for developing uveitis such as seronegative spondyloarthropathies, immunosuppression, sarcoidosis, and juvenile idiopathic arthritis.[13] Geographic variation in etiology and presentation is driven by differences in infection burden, air pollution, tobacco smoking, and genetic background. [17][18]
Screening
There is insufficient evidence to recommend routine screening for uveitis for the general population. For patients diagnosed with or suspected of having juvenile idiopathic arthritis (JIA), screening guidelines have been recommended by the American Academy of Pediatrics (AAP) and the British Society of Paediatrics and Rheumatology (BSPAR).[19][20]
Natural History, Complications and Prognosis
If left untreated, uveitis can progress to permanent vision loss. Complications of uveitis include cataracts, glaucoma, macular edema, and retinal detachment. With appropriate treatment, most attacks of anterior uveitis resolve within days to weeks, however, relapses are common. Inflammation related to posterior uveitis may last from months to years and may cause permanent vision damage, even with treatment. [21][22][4][23][24]
Diagnosis
History and Symptoms
Obtaining a complete history is an important aspect of making a diagnosis of uveitis. It provides insight into cause, precipitating factors, and associated underlying conditions. Uveitis can present unilaterally or bilaterally. Symptoms may develop acutely or insidiously, and may vary depending on the underlying etiology of the uveitis. Acute uveitis attacks are more commonly symptomatic and affect the anterior chamber. Symptoms of anterior uveitis include eye pain, eye redness, and photophobia. Intermediate, posterior, and panuveitis commonly present with floaters, blurry vision, and impaired vision. Chronic uveitis usually has an indolent courses and may not present with eye pain or redness.[6]
Physical Examination
A complete medical history and comprehensive eye examination must be performed by an optometrist or ophthalmologist to properly diagnosis uveitis. Eye examination of patients with uveitis is usually remarkable for eye redness and increased or decreased intraocular pressure. Depending on the affected anatomy of the uvea, “snowbanking” or optic disc edema may be seen on dilated fundus exam, and mutton fat keratic precipitates on slit lamp test may also be appreciated.[25][26] A complete physical examination can provide insight into the cause, and associated underlying conditions.
Laboratory Findings
There is no single international consensus diagnostic algorithm, and the investigations are tailored to, Regional infection prevalence, comorbidities and immunosuppression, and clinical presentation.[15] The presence of certain non-specific laboratory findings, in the presence of uveitis, may be suggestive of certain underlying causes. Examples of tests that may demonstrate abnormal findings include CBC, ESR, CRP, complete metabolic panel, iron studies, and serology titers.[27][28][29][30][31] Immunocompromised patients, particularly those with HIV, require comprehensive infectious screening including for CMV, Candida and other opportunistic pathogens.[32][33][34][35]
X Ray
There are no diagnostic x ray findings associated with uveitis. Positive x ray findings may be found in underlying conditions such as sarcoidosis[36], tuberculosis[37], and seronegative spondyloarthropathies[38][39].
CT
There are no diagnostic CT scan findings associated with uveitis. The presence of certain CT findings, in the presence of uveitis, may be suggestive of specific underlying causes such as inflammatory bowel disease[40][41][42], sarcoidosis[43][44], and Behcet’s disease[45][46].
MRI
There are no diagnostic MRI findings associated with uveitis. The presence of certain MRI findings, in the presence of uveitis, may be suggestive of specific underlying causes such as sarcoidosis, multiple sclerosis, Behcet’s disease, syphilis, and joint abnormalities in seronegative spondyloarthropathies.[47][48][49][50][39]
Ultrasound
There are no diagnostic ultrasound findings associated with uveitis.
Other Imaging Findings
There are no other diagnostic imaging findings associated with uveitis.
Other Diagnostic Studies
Other diagnostic studies associated with uveitis include slit lamp test and ocular tonometry. The slit lamp test is considered a gold standard modality in diagnosing uveitis. While intraocular pressure may increase or decrease depending on the anatomical location and severity of the inflammation, slit lamp test findings are relatively more consistent. Common slit lamp test findings include presence of inflammatory cells in the anterior chamber, keratic precipitates, and mutton fat precipitates. Slit lamp test findings associated with anatomical location include snowbanking in intermediate uveitis (e.g., pars planitis), snowballing in vitritis, and retinal edema in posterior uveitis.[6][51]
Treatment
Medical Therapy
Noninfectious anterior uveitis is treated first-line with topical prednisolone acetate 1% with intensive dosing and taper [5], with rimexolone showing comparable efficacy [52]; periocular or intravitreal corticosteroids are second-line when topical therapy is inadequate and systemic therapy is undesirable.[53][54][55] Moderate-to-severe intermediate, posterior uveitis, and panuveitis require systemic and/or intravitreal corticosteroids with immunosuppression [15], typically oral prednisone or IV methylprednisolone for severe disease, achieving rapid remission in many patients. [56][57]
DMARDs are first-line steroid-sparing systemic therapy for noninfectious posterior uveitis, and adalimumab is second line for refractory disease. [58][59][60][61][62][63][64] Corticosteroid treatment carries significant risk of cataract, glaucoma, and ocular hypertension [5][54][65][66]. Infectious uveitis requires pathogen-directed antimicrobial therapy first, with corticosteroids used only as adjuncts and never alone; gram-positive organisms predominate in endophthalmitis[67][68][69][70][71][72][73][74][75][76][77][78][79][80][81][82][83][84][85][86]
Surgery
There is no indication for surgical intervention in uveitis. Surgical management of uveitis is most commonly reserved for management of complications of uveitis or, rarely, for diagnostic purposes. Common complications of uveitis requiring surgery include cataract surgery, glaucoma surgery, or band keratopathy. Common indications for the diagnostic utility of surgery in uveitis include vitreous tap, vitreous biopsy, and posterior uveal biopsy.[87]
Primary Prevention
Appropriate treatment of an underlying disorder may help to prevent uveitis in persons with a systemic infection or inflammatory disease.
Secondary Prevention
There are no secondary prevention methods associated with uveitis.
References
- ↑ Foster CS, Vitale AT. Diagnosis & Treatment of Uveitis. JP Medical Ltd; 2013. https://books.google.com/books?id=vZxqM6cuQI4C&pg=PA192&lpg=PA192&dq=hippocrates+uveitis&source=bl&ots=xx1OQjRvqA&sig=pMnw0pkRrVrfVJICFWWJT1c_XLQ&hl=en&sa=X&ved=0ahUKEwjt–2LtYrPAhXBFR4KHa8XDXMQ6AEIJzAB#v=onepage&q=hippocrates%20uveitis&f=false Accessed on September 12, 2016
- ↑ Deschenes J, Murray PI, Rao NA, Nussenblatt RB, International Uveitis Study Group (2008). “International Uveitis Study Group (IUSG): clinical classification of uveitis”. Ocul Immunol Inflamm. 16 (1): 1–2. doi:10.1080/09273940801899822. PMID 18379933.
- ↑ Jabs DA, Nussenblatt RB, Rosenbaum JT, Standardization of Uveitis Nomenclature (SUN) Working Group (2005). “Standardization of uveitis nomenclature for reporting clinical data. Results of the First International Workshop”. Am J Ophthalmol. 140 (3): 509–16. PMID 16196117.
- ↑ 4.0 4.1 McCluskey PJ, Towler HM, Lightman S (2000). “Management of chronic uveitis”. BMJ. 320 (7234): 555–8. PMC 1117601. PMID 10688564.
- ↑ 5.0 5.1 5.2 5.3 Gutteridge IF, Hall AJ (2007). “Acute anterior uveitis in primary care”. Clin Exp Optom. 90 (2): 70–82. doi:10.1111/j.1444-0938.2006.00128.x. PMID 17311570.
- ↑ 6.0 6.1 6.2 6.3 6.4 6.5 Guly CM, Forrester JV (2010). “Investigation and management of uveitis”. BMJ. 341: c4976. doi:10.1136/bmj.c4976. PMID 20943722.
- ↑ 7.0 7.1 7.2 Lee RW, Dick AD (January 2012). “Current concepts and future directions in the pathogenesis and treatment of non-infectious intraocular inflammation”. Eye (Lond). 26 (1): 17–28. doi:10.1038/eye.2011.255. PMC 3259588. PMID 21960067.
- ↑ 8.0 8.1 8.2 8.3 Egwuagu CE, Alhakeem SA, Mbanefo EC (2021). “Uveitis: Molecular Pathogenesis and Emerging Therapies”. Front Immunol. 12: 623725. doi:10.3389/fimmu.2021.623725. PMC 8119754 Check
|pmc=value (help). PMID 33995347 Check|pmid=value (help). - ↑ Saari KM, Päivönsalo-Hietanen T, Vaahtoranta-Lehtonen H, Tuominen J, Sillanpää M (August 1995). “Epidemiology of endogenous uveitis in south-western Finland”. Acta Ophthalmol Scand. 73 (4): 345–9. doi:10.1111/j.1600-0420.1995.tb00040.x. PMID 8646582.
- ↑ Thorne JE, Suhler E, Skup M, Tari S, Macaulay D, Chao J, Ganguli A (November 2016). “Prevalence of Noninfectious Uveitis in the United States: A Claims-Based Analysis”. JAMA Ophthalmol. 134 (11): 1237–1245. doi:10.1001/jamaophthalmol.2016.3229. PMID 27608193.
- ↑ 11.0 11.1 Rodriguez A, Calonge M, Pedroza-Seres M, Akova YA, Messmer EM, D’Amico DJ; et al. (1996). “Referral patterns of uveitis in a tertiary eye care center”. Arch Ophthalmol. 114 (5): 593–9. PMID 8619771.
- ↑ Prior-Español Á, Martínez-Morillo M, Holgado-Pérez S, Juega FJ (2016). “Differential diagnosis of acute bilateral uveitis in the rheumatologist’s office”. Reumatol Clin. 12 (3): 174–175. doi:10.1016/j.reuma.2015.05.012. PMID 26187650.
- ↑ 13.0 13.1 American Academy of Ophthalmology EyeWiki (2015)http://eyewiki.aao.org/Category:Uveitis
- ↑ Rothova A, Ooijman F, Kerkhoff F, Van Der Lelij A, Lokhorst HM (2001). “Uveitis masquerade syndromes”. Ophthalmology. 108 (2): 386–99. PMID 11158819.
- ↑ 15.0 15.1 15.2 “Review on the Worldwide Epidemiology of Uveitis – Elisabetta Miserocchi, Giovanni Fogliato, Giulio Modorati, Francesco Bandello, 2013”.
- ↑ Lin P, Loh AR, Margolis TP, Acharya NR (2010). “Cigarette smoking as a risk factor for uveitis”. Ophthalmology. 117 (3): 585–90. doi:10.1016/j.ophtha.2009.08.011. PMC 2830339. PMID 20036011.
- ↑ Guo X, Chen Z, Xing Y (2021). “Immune-Mediated Uveitis and Lifestyle Factors: A Review”. Ophthalmic Res. 64 (5): 687–695. doi:10.1159/000518496. PMID 34348329 Check
|pmid=value (help). - ↑ Bai YC, Wang CY, Lin CL, Lai JN, Wei JC (2021). “Association Between Air Pollution and the Risk of Uveitis: A Nationwide, Population-Based Cohort Study”. Front Immunol. 12: 613893. doi:10.3389/fimmu.2021.613893. PMC 8013994 Check
|pmc=value (help). PMID 33815370 Check|pmid=value (help). - ↑ Sen ES, Dick AD, Ramanan AV (2015). “Uveitis associated with juvenile idiopathic arthritis”. Nat Rev Rheumatol. 11 (6): 338–48. doi:10.1038/nrrheum.2015.20. PMID 25825278.
- ↑ Cassidy J, Kivlin J, Lindsley C, Nocton J, Section on Rheumatology. Section on Ophthalmology (2006). “Ophthalmologic examinations in children with juvenile rheumatoid arthritis”. Pediatrics. 117 (5): 1843–5. doi:10.1542/peds.2006-0421. PMID 16651348.
- ↑ MedlinePlus Medical Encyclopedia Uveitis(2014)https://medlineplus.gov/ency/article/001005.htm
- ↑ Patient Trusted Medical Information and Support (2016)http://patient.info/health/uveitis-leaflet
- ↑ Rothova A, Suttorp-van Schulten MS, Frits Treffers W, Kijlstra A (1996). “Causes and frequency of blindness in patients with intraocular inflammatory disease”. Br J Ophthalmol. 80 (4): 332–6. PMC 505460. PMID 8703885.
- ↑ Nussenblatt RB (1990). “The natural history of uveitis”. Int Ophthalmol. 14 (5–6): 303–8. PMID 2249907.
- ↑ Patient Trusted Medical Information and Support (2016)http://patient.info/health/uveitis-leaflet
- ↑ Wyngaarden, James B.; Smith Jr., Lloyd H. (1988), Cecil Textbook Of Medicine, Philadelphia, PA: W.B. Saunders Company, pp. 2293–2294, ISBN 0-7216-1850-2
- ↑ Majumder PD, Sudharshan S, Biswas J (2013). “Laboratory support in the diagnosis of uveitis”. Indian J Ophthalmol. 61 (6): 269–76. doi:10.4103/0301-4738.114095. PMC 3744779. PMID 23803478.
- ↑ Agrawal RV, Murthy S, Sangwan V, Biswas J (2010). “Current approach in diagnosis and management of anterior uveitis”. Indian J Ophthalmol. 58 (1): 11–9. doi:10.4103/0301-4738.58468. PMC 2841369. PMID 20029142.
- ↑ Rathinam SR, Babu M (2013). “Algorithmic approach in the diagnosis of uveitis”. Indian J Ophthalmol. 61 (6): 255–62. doi:10.4103/0301-4738.114092. PMC 3744777. PMID 23803476.
- ↑ Herbort CP (2009). “Appraisal, work-up and diagnosis of anterior uveitis: a practical approach”. Middle East Afr J Ophthalmol. 16 (4): 159–67. doi:10.4103/0974-9233.58416. PMC 2855658. PMID 20404984.
- ↑ Kijlstra A (1990). “The value of laboratory testing in uveitis”. Eye (Lond). 4 ( Pt 5): 732–6. doi:10.1038/eye.1990.104. PMID 2178095.
- ↑ Tyagi M, Das AV, Kaza H, Basu S, Pappuru RR, Pathengay A, Murthy S, Agrawal H (April 2022). “LV Prasad Eye Institute EyeSmart electronic medical record-based analytics of big data: LEAD-Uveitis Report 1: Demographics and clinical features of uveitis in a multi-tier hospital based network in Southern India”. Indian J Ophthalmol. 70 (4): 1260–1267. doi:10.4103/ijo.IJO_1122_21. PMC 9240530 Check
|pmc=value (help). PMID 35326028 Check|pmid=value (help). - ↑ “Uveitis in HIV-Infected Patients – J-C.K. Mwanza, D.L. Kayembe, 2001”.
- ↑ Agrawal R, Gunasekeran DV, Agarwal A, Carreño E, Aggarwal K, Gupta B, Raje D, Murthy SI, Westcott M, Chee SP, McCluskey P, Ling HS, Teoh S, Cimino L, Biswas J, Narain S, Agarwal M, Mahendradas P, Khairallah M, Jones N, Tugal-Tutkun I, Babu K, Basu S, Lee R, Al-Dhibi H, Bodaghi B, Invernizzi A, Goldstein DA, Herbort CP, Barisani-Asenbauer T, González-López JJ, Androudi S, Bansal R, Moharana B, Mahajan S, Esposti S, Tasiopoulou A, Nadarajah S, Agarwal M, Abraham S, Vala R, Lord J, Singh R, Sharma A, Sharma K, Zierhut M, Kon OM, Kempen J, Cunningham ET, Rousselot A, Nguyen QD, Pavesio C, Gupta V (September 2020). “The Collaborative Ocular Tuberculosis Study (COTS)-1: A Multinational Description of the Spectrum of Choroidal Involvement in 245 Patients with Tubercular Uveitis”. Ocul Immunol Inflamm. 28 (sup1): 38–48. doi:10.1080/09273948.2018.1489061. PMID 30156979.
- ↑ Alli HD, Ally N, Mayet I, Dangor Z, Madhi SA (2022). “Global prevalence and clinical outcomes of tubercular uveitis: a systematic review and meta-analysis”. Surv Ophthalmol. 67 (3): 770–792. doi:10.1016/j.survophthal.2021.10.001. PMID 34626620 Check
|pmid=value (help). - ↑ Miller BH, Rosado-de-Christenson ML, McAdams HP, Fishback NF (1995). “Thoracic sarcoidosis: radiologic-pathologic correlation”. Radiographics. 15 (2): 421–37. doi:10.1148/radiographics.15.2.7761646. PMID 7761646.
- ↑ Jeong YJ, Lee KS (2008). “Pulmonary tuberculosis: up-to-date imaging and management”. AJR Am J Roentgenol. 191 (3): 834–44. doi:10.2214/AJR.07.3896. PMID 18716117.
- ↑ Riley MJ, Ansell BM, Bywaters EG (1971). “Radiological manifestations of ankylosing spondylitis according to age at onset”. Ann Rheum Dis. 30 (2): 138–48. PMC 1005741. PMID 5569434.
- ↑ 39.0 39.1 Jacobson JA, Girish G, Jiang Y, Resnick D (2008). “Radiographic evaluation of arthritis: inflammatory conditions”. Radiology. 248 (2): 378–89. doi:10.1148/radiol.2482062110. PMID 18641245.
- ↑ Gore RM, Balthazar EJ, Ghahremani GG, Miller FH (1996). “CT features of ulcerative colitis and Crohn’s disease”. AJR Am J Roentgenol. 167 (1): 3–15. doi:10.2214/ajr.167.1.8659415. PMID 8659415.
- ↑ Furukawa A, Saotome T, Yamasaki M, Maeda K, Nitta N, Takahashi M; et al. (2004). “Cross-sectional imaging in Crohn disease”. Radiographics. 24 (3): 689–702. doi:10.1148/rg.243035120. PMID 15143222.
- ↑ Roggeveen MJ, Tismenetsky M, Shapiro R (2006). “Best cases from the AFIP: Ulcerative colitis”. Radiographics. 26 (3): 947–51. doi:10.1148/rg.263055149. PMID 16702465.
- ↑ Warshauer DM, Lee JK (2004). “Imaging manifestations of abdominal sarcoidosis”. AJR Am J Roentgenol. 182 (1): 15–28. doi:10.2214/ajr.182.1.1820015. PMID 14684507.
- ↑ Nakatsu M, Hatabu H, Morikawa K, Uematsu H, Ohno Y, Nishimura K; et al. (2002). “Large coalescent parenchymal nodules in pulmonary sarcoidosis: “sarcoid galaxy” sign”. AJR Am J Roentgenol. 178 (6): 1389–93. doi:10.2214/ajr.178.6.1781389. PMID 12034602.
- ↑ Ahn JM, Im JG, Ryoo JW, Kim SJ, Do YS, Choi YW; et al. (1995). “Thoracic manifestations of Behçet syndrome: radiographic and CT findings in nine patients”. Radiology. 194 (1): 199–203. doi:10.1148/radiology.194.1.7997553. PMID 7997553.
- ↑ Emad Y, Abdel-Razek N, Gheita T, el-Wakd M, el-Gohary T, Samadoni A (2007). “Multislice CT pulmonary findings in Behçet’s disease (report of 16 cases)”. Clin Rheumatol. 26 (6): 879–84. doi:10.1007/s10067-006-0408-x. PMID 17024317.
- ↑ Smith JK, Matheus MG, Castillo M (2004). “Imaging manifestations of neurosarcoidosis”. AJR Am J Roentgenol. 182 (2): 289–95. doi:10.2214/ajr.182.2.1820289. PMID 14736648.
- ↑ Lövblad KO, Anzalone N, Dörfler A, Essig M, Hurwitz B, Kappos L; et al. (2010). “MR imaging in multiple sclerosis: review and recommendations for current practice”. AJNR Am J Neuroradiol. 31 (6): 983–9. doi:10.3174/ajnr.A1906. PMID 20019103.
- ↑ Hegde AN, Mohan S, Lath N, Lim CC (2011). “Differential diagnosis for bilateral abnormalities of the basal ganglia and thalamus”. Radiographics. 31 (1): 5–30. doi:10.1148/rg.311105041. PMID 21257930.
- ↑ Pandey S (2011). “Magnetic resonance imaging of the spinal cord in a man with tabes dorsalis”. J Spinal Cord Med. 34 (6): 609–11. doi:10.1179/2045772311Y.0000000041. PMC 3237288. PMID 22330117.
- ↑ National Eye Institute (2016) https://nei.nih.gov/health/uveitis/uveitis
- ↑ Biswas J, Ganeshbabu TM, Raghavendran SR, Raizada S, Mondkar SV, Madhavan HN (May 2004). “Efficacy and safety of 1% rimexolone versus 1% prednisolone acetate in the treatment of anterior uveitis–a randomized triple masked study”. Int Ophthalmol. 25 (3): 147–53. doi:10.1007/s10792-004-5195-2. PMID 15847313.
- ↑ Takase H, Acharya NR, Babu K, Bodaghi B, Khairallah M, McCluskey PJ, Tesavibul N, Thorne JE, Tugal-Tutkun I, Yamamoto JH, Rao NA, Smith JR, Mochizuki M (November 2021). “Recommendations for the management of ocular sarcoidosis from the International Workshop on Ocular Sarcoidosis”. Br J Ophthalmol. 105 (11): 1515–1519. doi:10.1136/bjophthalmol-2020-317354. PMID 32933934 Check
|pmid=value (help). - ↑ 54.0 54.1 Thorne JE, Sugar EA, Holbrook JT, Burke AE, Altaweel MM, Vitale AT, Acharya NR, Kempen JH, Jabs DA (February 2019). “Periocular Triamcinolone vs. Intravitreal Triamcinolone vs. Intravitreal Dexamethasone Implant for the Treatment of Uveitic Macular Edema: The PeriOcular vs. INTravitreal corticosteroids for uveitic macular edema (POINT) Trial”. Ophthalmology. 126 (2): 283–295. doi:10.1016/j.ophtha.2018.08.021. PMC 6348060. PMID 30269924.
- ↑ Yeh S, Khurana RN, Shah M, Henry CR, Wang RC, Kissner JM, Ciulla TA, Noronha G (July 2020). “Efficacy and Safety of Suprachoroidal CLS-TA for Macular Edema Secondary to Noninfectious Uveitis: Phase 3 Randomized Trial”. Ophthalmology. 127 (7): 948–955. doi:10.1016/j.ophtha.2020.01.006. PMID 32173113 Check
|pmid=value (help). - ↑ Jabs DA, Rosenbaum JT, Foster CS, Holland GN, Jaffe GJ, Louie JS, Nussenblatt RB, Stiehm ER, Tessler H, Van Gelder RN, Whitcup SM, Yocum D (October 2000). “Guidelines for the use of immunosuppressive drugs in patients with ocular inflammatory disorders: recommendations of an expert panel”. Am J Ophthalmol. 130 (4): 492–513. doi:10.1016/s0002-9394(00)00659-0. PMID 11024423.
- ↑ Charkoudian LD, Ying GS, Pujari SS, Gangaputra S, Thorne JE, Foster CS, Jabs DA, Levy-Clarke GA, Nussenblatt RB, Rosenbaum JT, Suhler EB, Kempen JH (April 2012). “High-dose intravenous corticosteroids for ocular inflammatory diseases”. Ocul Immunol Inflamm. 20 (2): 91–9. doi:10.3109/09273948.2011.646382. PMC 3306126. PMID 22409561.
- ↑ “1 Recommendations | Adalimumab and dexamethasone for treating non-infectious uveitis | Guidance | NICE”.
- ↑ Dick AD, Rosenbaum JT, Al-Dhibi HA, Belfort R, Brézin AP, Chee SP, Davis JL, Ramanan AV, Sonoda KH, Carreño E, Nascimento H, Salah S, Salek S, Siak J, Steeples L (May 2018). “Guidance on Noncorticosteroid Systemic Immunomodulatory Therapy in Noninfectious Uveitis: Fundamentals Of Care for UveitiS (FOCUS) Initiative”. Ophthalmology. 125 (5): 757–773. doi:10.1016/j.ophtha.2017.11.017. PMID 29310963.
- ↑ Gangaputra S, Newcomb CW, Liesegang TL, Kaçmaz RO, Jabs DA, Levy-Clarke GA, Nussenblatt RB, Rosenbaum JT, Suhler EB, Thorne JE, Foster CS, Kempen JH (November 2009). “Methotrexate for ocular inflammatory diseases”. Ophthalmology. 116 (11): 2188–98.e1. doi:10.1016/j.ophtha.2009.04.020. PMC 3785935. PMID 19748676.
- ↑ Daniel E, Thorne JE, Newcomb CW, Pujari SS, Kaçmaz RO, Levy-Clarke GA, Nussenblatt RB, Rosenbaum JT, Suhler EB, Foster CS, Jabs DA, Kempen JH (March 2010). “Mycophenolate mofetil for ocular inflammation”. Am J Ophthalmol. 149 (3): 423–32.e1–2. doi:10.1016/j.ajo.2009.09.026. PMC 2826576. PMID 20042178.
- ↑ Deuter CM, Engelmann K, Heiligenhaus A, Lanzl I, Mackensen F, Ness T, Pleyer U, Stuebiger N, Wilhelm B, Luedtke H, Zierhut M, Doycheva D (May 2018). “Enteric-coated mycophenolate sodium in the treatment of non-infectious intermediate uveitis: results of a prospective, controlled, randomised, open-label, early terminated multicentre trial”. Br J Ophthalmol. 102 (5): 647–653. doi:10.1136/bjophthalmol-2017-310156. PMID 28903965.
- ↑ Jaffe GJ, Dick AD, Brézin AP, Nguyen QD, Thorne JE, Kestelyn P, Barisani-Asenbauer T, Franco P, Heiligenhaus A, Scales D, Chu DS, Camez A, Kwatra NV, Song AP, Kron M, Tari S, Suhler EB (September 2016). “Adalimumab in Patients with Active Noninfectious Uveitis”. N Engl J Med. 375 (10): 932–43. doi:10.1056/NEJMoa1509852. PMID 27602665.
- ↑ Nguyen QD, Merrill PT, Jaffe GJ, Dick AD, Kurup SK, Sheppard J, Schlaen A, Pavesio C, Cimino L, Van Calster J, Camez AA, Kwatra NV, Song AP, Kron M, Tari S, Brézin AP (September 2016). “Adalimumab for prevention of uveitic flare in patients with inactive non-infectious uveitis controlled by corticosteroids (VISUAL II): a multicentre, double-masked, randomised, placebo-controlled phase 3 trial”. Lancet. 388 (10050): 1183–92. doi:10.1016/S0140-6736(16)31339-3. PMID 27542302.
- ↑ “Corticosteroid-induced cataracts – Survey of Ophthalmology”.
- ↑ Prieto-Del-Cura M, González-Guijarro JJ (November 2020). “Risk factors for ocular complications in adult patients with uveitis”. Eur J Ophthalmol. 30 (6): 1381–1389. doi:10.1177/1120672119899379. PMID 31902244.
- ↑ Takakura A, Tessler HH, Goldstein DA, Guex-Crosier Y, Chan CC, Brown DM, Thorne JE, Wang R, Cunningham ET (June 2014). “Viral retinitis following intraocular or periocular corticosteroid administration: a case series and comprehensive review of the literature”. Ocul Immunol Inflamm. 22 (3): 175–82. doi:10.3109/09273948.2013.866256. PMC 4154532. PMID 24655372.
- ↑ Benz MS, Scott IU, Flynn HW, Unonius N, Miller D (January 2004). “Endophthalmitis isolates and antibiotic sensitivities: a 6-year review of culture-proven cases”. Am J Ophthalmol. 137 (1): 38–42. doi:10.1016/s0002-9394(03)00896-1. PMID 14700642.
- ↑ Agrawal R, Testi I, Mahajan S, Yuen YS, Agarwal A, Kon OM, Barisani-Asenbauer T, Kempen JH, Gupta A, Jabs DA, Smith JR, Nguyen QD, Pavesio C, Gupta V (February 2021). “Collaborative Ocular Tuberculosis Study Consensus Guidelines on the Management of Tubercular Uveitis-Report 1: Guidelines for Initiating Antitubercular Therapy in Tubercular Choroiditis”. Ophthalmology. 128 (2): 266–276. doi:10.1016/j.ophtha.2020.01.008. PMID 32115264 Check
|pmid=value (help). - ↑ Betzler BK, Putera I, Testi I, La Distia Nora R, Kempen J, Kon OM, Pavesio C, Gupta V, Agrawal R (2023). “Anti-tubercular therapy in the treatment of tubercular uveitis: A systematic review and meta-analysis”. Surv Ophthalmol. 68 (2): 241–256. doi:10.1016/j.survophthal.2022.10.001. PMID 36272559 Check
|pmid=value (help). - ↑ Workowski KA, Bachmann LH, Chan PA, Johnston CM, Muzny CA, Park I, Reno H, Zenilman JM, Bolan GA (July 2021). “Sexually Transmitted Infections Treatment Guidelines, 2021”. MMWR Recomm Rep. 70 (4): 1–187. doi:10.15585/mmwr.rr7004a1. PMC 8344968 Check
|pmc=value (help). PMID 34292926 Check|pmid=value (help). - ↑ Zhang T, Zhu Y, Xu G (2017). “Clinical Features and Treatments of Syphilitic Uveitis: A Systematic Review and Meta-Analysis”. J Ophthalmol. 2017: 6594849. doi:10.1155/2017/6594849. PMC 5511639. PMID 28751982.
- ↑ Thng ZX, Putera I, Testi I, Chan K, Westcott M, Chee SP, Dick AD, Kempen JH, Bodaghi B, Thorne JE, Barisani-Asenbauer T, de Smet MD, Smith JR, McCluskey P, La Distia Nora R, Jabs DA, de Boer JH, Sen HN, Goldstein DA, Khairallah M, Davis JL, Rosenbaum JT, Jones NP, Nguyen QD, Pavesio C, Agrawal R, Gupta V (January 2024). “The Infectious Uveitis Treatment Algorithm Network (TITAN) Report 1-global current practice patterns for the management of Herpes Simplex Virus and Varicella Zoster Virus anterior uveitis”. Eye (Lond). 38 (1): 61–67. doi:10.1038/s41433-023-02630-9. PMC 10764303 Check
|pmc=value (help). PMID 37419957 Check|pmid=value (help). - ↑ Thng ZX, Putera I, Testi I, Chan K, Westcott M, Chee SP, Dick AD, Kempen JH, Bodaghi B, Thorne JE, Barisani-Asenbauer T, de Smet MD, Smith JR, McCluskey P, La Distia Nora R, Jabs DA, de Boer JH, Sen HN, Goldstein DA, Khairallah M, Davis JL, Rosenbaum JT, Jones NP, Nguyen QD, Pavesio C, Agrawal R, Gupta V (January 2024). “The Infectious Uveitis Treatment Algorithm Network (TITAN) Report 2-global current practice patterns for the management of Cytomegalovirus anterior uveitis”. Eye (Lond). 38 (1): 68–75. doi:10.1038/s41433-023-02631-8. PMC 10764804 Check
|pmc=value (help). PMID 37419958 Check|pmid=value (help). - ↑ Zandi S, Bodaghi B, Garweg JG (2018). “Review for Disease of the Year: Treatment of Viral Anterior Uveitis: A Perspective”. Ocul Immunol Inflamm. 26 (7): 1135–1142. doi:10.1080/09273948.2018.1498109. PMID 30096015.
- ↑ Brodie JT, Thotathil AZ, Jordan CA, Sims J, Niederer RL (November 2024). “Risk of Recurrence in Acute Anterior Uveitis”. Ophthalmology. 131 (11): 1281–1289. doi:10.1016/j.ophtha.2024.06.003. PMID 38852922 Check
|pmid=value (help). - ↑ La Distia Nora R, Putera I, Mayasari YD, Hikmahwati W, Pertiwi AM, Ridwan AS, Sitompul R, Westcott M, Chee SP, Pavesio C, Thng ZX, Gupta V, Agrawal R (2022). “Clinical characteristics and treatment outcomes of cytomegalovirus anterior uveitis and endotheliitis: A systematic review and meta-analysis”. Surv Ophthalmol. 67 (4): 1014–1030. doi:10.1016/j.survophthal.2021.12.006. PMID 34954093 Check
|pmid=value (help). - ↑ Ude IN, Yeh S, Shantha JG (March 2022). “Cytomegalovirus retinitis in the highly active anti-retroviral therapy era”. Ann Eye Sci. 7. doi:10.21037/aes-21-18. PMC 9053080 Check
|pmc=value (help). PMID 35498636 Check|pmid=value (help). - ↑ Chiang WY, Lin CP, Cho WH, Yang CH, Chen SN, Hwang YS, Hsu SM, Hwang DK, Chen SC, Kuo HK, Sheu SJ (August 2023). “Cytomegalovirus Uveitis: Taiwan expert consensus”. J Formos Med Assoc. 122 (8): 668–674. doi:10.1016/j.jfma.2023.03.014. PMID 37003913 Check
|pmid=value (help). - ↑ Khan FA, Slain D, Khakoo RA (December 2007). “Candida endophthalmitis: focus on current and future antifungal treatment options”. Pharmacotherapy. 27 (12): 1711–21. doi:10.1592/phco.27.12.1711. PMID 18041891.
- ↑ Rex JH, Bennett JE, Sugar AM, Pappas PG, van der Horst CM, Edwards JE, Washburn RG, Scheld WM, Karchmer AW, Dine AP (November 1994). “A randomized trial comparing fluconazole with amphotericin B for the treatment of candidemia in patients without neutropenia. Candidemia Study Group and the National Institute”. N Engl J Med. 331 (20): 1325–30. doi:10.1056/NEJM199411173312001. PMID 7935701.
- ↑ Pappas PG, Kauffman CA, Andes DR, Clancy CJ, Marr KA, Ostrosky-Zeichner L, Reboli AC, Schuster MG, Vazquez JA, Walsh TJ, Zaoutis TE, Sobel JD (February 2016). “Clinical Practice Guideline for the Management of Candidiasis: 2016 Update by the Infectious Diseases Society of America”. Clin Infect Dis. 62 (4): e1–50. doi:10.1093/cid/civ933. PMC 4725385. PMID 26679628.
- ↑ Patterson TF, Thompson GR, Denning DW, Fishman JA, Hadley S, Herbrecht R, Kontoyiannis DP, Marr KA, Morrison VA, Nguyen MH, Segal BH, Steinbach WJ, Stevens DA, Walsh TJ, Wingard JR, Young JA, Bennett JE (August 2016). “Practice Guidelines for the Diagnosis and Management of Aspergillosis: 2016 Update by the Infectious Diseases Society of America”. Clin Infect Dis. 63 (4): e1–e60. doi:10.1093/cid/ciw326. PMC 4967602. PMID 27365388.
- ↑ Kalogeropoulos D, Sakkas H, Mohammed B, Vartholomatos G, Malamos K, Sreekantam S, Kanavaros P, Kalogeropoulos C (January 2022). “Ocular toxoplasmosis: a review of the current diagnostic and therapeutic approaches”. Int Ophthalmol. 42 (1): 295–321. doi:10.1007/s10792-021-01994-9. PMC 8351587 Check
|pmc=value (help). PMID 34370174 Check|pmid=value (help). - ↑ Pradhan E, Bhandari S, Gilbert RE, Stanford M (May 2016). “Antibiotics versus no treatment for toxoplasma retinochoroiditis”. Cochrane Database Syst Rev. 2016 (5): CD002218. doi:10.1002/14651858.CD002218.pub2. PMC 7100541 Check
|pmc=value (help). PMID 27198629. - ↑ Feliciano-Alfonso JE, Muñoz-Ortiz J, Marín-Noriega MA, Vargas-Villanueva A, Triviño-Blanco L, Carvajal-Saiz N, de-la-Torre A (July 2021). “Safety and efficacy of different antibiotic regimens in patients with ocular toxoplasmosis: systematic review and meta-analysis”. Syst Rev. 10 (1): 206. doi:10.1186/s13643-021-01758-7. PMC 8287816 Check
|pmc=value (help). PMID 34275483 Check|pmid=value (help). - ↑ Katzav S, Shapiro J, Segal S, yM (1986). bmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=3744781 “General nesthesia during excision of a mouse tumor accelerates postsurgical growth of metastases by suppression of natural killer cell activity” Check
|url=value (help). Isr J Med Sci. 22 (5): 339–45. PMID PMC3744781 : PMC3744781 Check|pmid=value (help).
Historical Perspective
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Tarek Nafee, M.D. [2]
Overview
Uveitis was first discovered by Hippocrates, a Greek physician, and was well known to other major medical physicians, such as Galen and Aëtius of Amida. In 1952, corticosteroids were used to treat uveitis for the first time.[1]
Historical Perspective
- Uveitis is an ancient disease.
- Uveitis was first discovered by Hippocrates, a Greek physician, and was well known to other major medical physicians, such as Galen and Aëtius of Amida.[1]
- In 1806, Antonio Scarpa, an Italian anatomist, described a uveitis case study and the treatment of the disease for the first time in modern literature.[2]
- In 1830, William Mackenzie, a Scottish physician, described uveitis for the first time in English medical literature.[1][3]
- In 1952, corticosteroids were used to treat uveitis for the first time.[1]
References
- ↑ 1.0 1.1 1.2 1.3 Foster CS, Vitale AT. Diagnosis & Treatment of Uveitis. JP Medical Ltd; 2013. https://books.google.com/books?id=vZxqM6cuQI4C&pg=PA192&lpg=PA192&dq=hippocrates+uveitis&source=bl&ots=xx1OQjRvqA&sig=pMnw0pkRrVrfVJICFWWJT1c_XLQ&hl=en&sa=X&ved=0ahUKEwjt–2LtYrPAhXBFR4KHa8XDXMQ6AEIJzAB#v=onepage&q=hippocrates%20uveitis&f=false Accessed on September 12, 2016
- ↑ Scarpa A. Practical Observations on the Principal Diseases of the Eye https://books.google.com/books?id=ueFHAQAAMAAJ&pg=PA455&lpg=PA455&dq=practical+observations+on+the+principal+diseases+of+the+eye&source=bl&ots=Xx1CrOTLYc&sig=VX3jr4qS_RZ9GupOaVubHBQ1kFY&hl=en&sa=X&ved=0ahUKEwjp4NTot4rPAhUE8x4KHbheAYgQ6AEIPTAH#v=onepage&q=practical%20observations%20on%20the%20principal%20diseases%20of%20the%20eye&f=false Accessed on September 12, 2016
- ↑ Mackenzie W. Practical Treatise of the Diseases of the Eye https://archive.org/details/practical00mack Accessed on September 12, 2016
Classification
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Tarek Nafee, M.D. [2]
Overview
Uveitis is best described using various, concurrent classification systems. Uveitis may be classified according to anatomical location into 4 subtypes, depending on which part of the uvea is primarily affected: anterior, intermediate, posterior, and panuveitis. Based on the duration of symptoms it may be further sub-classified as acute or chronic. Upon further investigation, uveitis may be classified according to histological features of the inflammation such as granulomatous or non-granulomatous. Additionally, uveitis may be described by the laterality of the condition (unilateral or bilateral). Finally, uveitis may be classified by general underlying systemic causes such as infectious, autoimmune, drug-induced, or idiopathic.[1][2][3][4][5]
Classification
Uveitis can be described according to the following classifications:[1][2][5]
- Classification by Anatomical Location
- Anterior uveitis: Iritis, cyclitis or iridocyclitis (inflammation affecting the iris, the ciliary body, or both)
- Intermediate uveitis: Viritis or pars planitis (inflammation of the the vitreous humor or the pars plana)
- Posterior uveitis: Choroiditis, retinitis, or chorioretinitis (inflammation of the choroid, the retina, or both)
- Panuveitis: Inflammation of the entire uvea
- Classification by Duration of Symptoms[3]
- Classification by type of inflammation[4]
- Granulomatous: showing granulomatous inflammation on slit lamp test
- Non-granulomatous showing no granulomatous inflammation on slit lamp test
- Classification by Laterality
- Unilateral: Single eye involvement
- Bilateral: Both eyes involvement
- Classification by Etiology[1][2]
- Idiopathic: No known cause
- Infectious: Bacterial, viral, fungal, or parasitic cause
- Autoimmune/Inflammatory: Caused by a systemic non-infectious inflammatory condition commonly associated with uveitis
- Drug-Induced: Iatrogenic cause by medications that are associated with incidence of uveitis
As uveitis manifests in a variety of clinical etiologies, differentiation must be established in accordance with the classification system for particular subtypes. Etiologies of acute anterior unilateral infectious uveitis must be differentiated from other subtypes that cause conjuctival injection, eye pain, and photophobia such as acute anterior bilateral non-infectious uveitis or chronic anterior uveitis. Diversely, posterior infectious uveitis must be differentiated from other subtypes that cause visual changes such as intermediate non-infectious uveitis and infectious panuveitis. Using the above model, the following is a classification of uveitis, which includes the most common subtypes:
Anterior Uveitis
Anterior uveitis can be classified according to the following presentation:[5][6][7]
- Acute (>3 months of active symptoms)[3]
- Unilateral
- Infectious: Cytomegalovirus, Herpes simplex, Varicella zoster, syphilis
- Non-infectious: Seronegative spondyloarthropathy, relapsing polychondritis, systemic lupus erythematosus (SLE), Kawasaki disease
- Bilateral
- Infectious: Tuberculosis, syphilis
- Non-infectious: tubulointerstitial nephritis with uveitis (TINU syndrome)
- Unilateral
- Chronic (>3 months of active symptoms)[3]
- Infectious: Tuberculosis
- Non-infectious: juvenile idiopathic arthritis, Sjorgen’s Syndrome, sarcoidosis
Intermediate Uveitis
Intermediate may present with unilateral or bilateral involvement. It can be classified according to the following etiologies[5][6][7]
- Infectious: Lyme disease, Whipple’s disease
- Non-infectious: multiple sclerosis, sarcoidosis, tubulointerstitial nephritis with uveitis (TINU syndrome), lymphoma
Posterior Uveitis
Posterior uveitis may present with unilateral or bilateral involvement. It can be classified according to the following most common etiologies:[5][6][7]
- Infectious: Toxoplasmosis, Cytomegalovirus, Tuberculosis, Syphilis, Toxocariasis, Herpes simplex, Varicella zoster, cat scratch disease
- Non-infectious:Vogt-Koyanagi-Harada syndrome, systemic lupus erythematosus, granulomatosis with polyangitis, Behcet’s disease, birdshot chorioretinopathy, lymphoma
Panuveitis
Panuveitis may present with unilateral or bilateral involvement. It can be classified according to the following most common etiologies:[5][6][7]
- Infectious: Tuberculosis, syphilis
- Non-infectious: Juvenile idiopathic arthritis, Behcet’s disease, sarcoidosis, Vogt-Koyanagi-Harada syndrome, Sjorgen’s Syndrome
References
- ↑ 1.0 1.1 1.2 Deschenes J, Murray PI, Rao NA, Nussenblatt RB, International Uveitis Study Group (2008). “International Uveitis Study Group (IUSG): clinical classification of uveitis”. Ocul Immunol Inflamm. 16 (1): 1–2. doi:10.1080/09273940801899822. PMID 18379933.
- ↑ 2.0 2.1 2.2 Jabs DA, Nussenblatt RB, Rosenbaum JT, Standardization of Uveitis Nomenclature (SUN) Working Group (2005). “Standardization of uveitis nomenclature for reporting clinical data. Results of the First International Workshop”. Am J Ophthalmol. 140 (3): 509–16. PMID 16196117.
- ↑ 3.0 3.1 3.2 3.3 McCluskey PJ, Towler HM, Lightman S (2000). “Management of chronic uveitis”. BMJ. 320 (7234): 555–8. PMC 1117601. PMID 10688564.
- ↑ 4.0 4.1 Gutteridge IF, Hall AJ (2007). “Acute anterior uveitis in primary care”. Clin Exp Optom. 90 (2): 70–82. doi:10.1111/j.1444-0938.2006.00128.x. PMID 17311570.
- ↑ 5.0 5.1 5.2 5.3 5.4 5.5 Guly CM, Forrester JV (2010). “Investigation and management of uveitis”. BMJ. 341: c4976. doi:10.1136/bmj.c4976. PMID 20943722.
- ↑ 6.0 6.1 6.2 6.3 American Academy of Ophthalmology EyeWiki (2015)http://eyewiki.aao.org/Category:Uveitis
- ↑ 7.0 7.1 7.2 7.3 Prior-Español Á, Martínez-Morillo M, Holgado-Pérez S, Juega FJ (2016). “Differential diagnosis of acute bilateral uveitis in the rheumatologist’s office”. Reumatol Clin. 12 (3): 174–175. doi:10.1016/j.reuma.2015.05.012. PMID 26187650.
Pathophysiology
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Tarek Nafee, M.D. [2]
Overview
The healthy eye possesses immune privilege, which suppresses immune responses to both endogenous retinal antigens (such as S-antigen) and exogenous antigens. This immune privilege is maintained by the blood–retina barrier, cellular mechanisms including regulatory T cells, and cytokine-mediated mechanisms involving transforming growth factor beta and interleukin-10.[1][2]
Uveitis is mediated by a genetic predisposition and an acquired cross immunity to infectious agents, or cross immunity to self-antigens due to underlying autoimmune diseases. It is estimated that 35% to 50% of cases of uveitis are idiopathic.[3][4] Development of uveitis is hypothesized to be the result of a genetic predisposition for acquiring the disease; contributions of several human leukocyte antigen (HLA) alleles are most commonly implicated.[4][5]This includes HLA-B27 in seronegative spondyloarthropathies, HLA-A29 in birdshot chorioretinopathy, HLA-B51 in Behcet syndrome and multiple sclerosis, HLA-B8, HLA-DR15, and HLA-DR2.[4][5]
Pathogenesis
Initiation of Uveitis
Noninfectious uveitis is hypothesized to result from reduced immune tolerance to retinal proteins, leading to inappropriate immune activation within the eye. In infectious uveitis, pathogenic organisms breach the blood–retina barrier and initiate inflammation; pathogen-derived antigens may resemble retinal proteins, a process known as antigenic mimicry, which can exacerbate the inflammatory response.[1][2] Infectious uveitis is hypothesized to be secondary to a T-cell mediated hypersensitivity reaction resulting in immunoactivating cytokine production by proliferating Tн17 and Tн1 cells.[5][6] A similar mechanism is hypothesized for autoimmune etiologies of uveitis with the exception of an unknown source of the triggering antigen.[7][8][9][10]
Antigen Presentation and T-Cell Activation
The prevailing mechanism in both infectious and noninfectious uveitis involves antigen presentation via major histocompatibility complex class II molecules, leading to activation of naïve CD4⁺ T cells. In infectious uveitis, antigen presentation is initiated by pathogen-derived antigens, whereas in noninfectious uveitis it is initiated by ocular autoantigens.[1][2]
Effector T-Cell Response
Upon activation, naïve CD4⁺ T cells differentiate predominantly into Th1 and Th17 subsets, which migrate to the retina and uveal tissues. These effector T cells play a central role in sustaining intraocular inflammation.[1][2]
Cytokine Cascade and Innate Immune Recruitment
Activated Th1 and Th17 cells release proinflammatory cytokines, including interferon-gamma, interleukin-2, and interleukin-17, triggering a cytokine cascade that recruits innate immune cells such as macrophages and neutrophils into ocular tissues.[2]
Inflammatory Tissue Injury
The accumulation of inflammatory cells and sustained cytokine signaling result in tissue damage, manifesting as chorioretinitis, retinal vasculitis, and edema, which contribute directly to visual dysfunction in uveitis.[2]

The retina’s immune privilege relies on the blood-retina barrier, which shields
ocular tissue proteins from the systemic immune system. This protective
mechanism can be compromised, leading to autoimmune reactions. Within the
retina, Tregs marked by CD4+, CD25+, and FoxP3+ identifiers contribute to
immune tolerance by emitting neuropeptides and anti-inflammatory cytokines.
These Tregs can suppress other T cells that have escaped elimination in the
thymus during development and have the potential to react against
self-antigens, producing cytokines, TGFβ, and IL-35 to reduce inflammation.
Furthermore, retinal pigment epithelium and retinal cells express certain
proteins on their surfaces that deactivate lymphocytes, thereby regulating
ocular inflammation. Disease is typically associated with major
histocompatibility complex class II molecule–mediated presentation of
autoantigens or cross-reactive foreign peptides to naive T cells. Activated CD4+
T cells differentiate into CD4+ TH1 and TH17 cells that migrate to the affected
tissue, recruiting inflammatory cells and producing tissue damage. T cells
differentiate into CD4+ TH1 and TH17 cells, producing IFNγ and IL-17,
respectively. These facilitate the recruitment and activation of downstream
cytokine release and innate inflammatory response, such as IL-6, TNF, and
granzyme B (a protease involved in programmed cell death), which in turn can
lead to vasculitis and edema.21,22
IFNγ indicates interferon gamma; TGFβ, transforming growth factor beta.
TNF, tumor necrosis factor; Treg, regulatory T cell.[11]
Associated Conditions
The following conditions are associated with uveitis:[3][4][12]
- Seronegative spondyloarthropathy
- Sarcoidosis
- Multiple sclerosis
- Inflammatory bowel disease
- Systemic lupus erythematosus (SLE)
- Behçet’s syndrome
- Birdshot retinochoroidopathy
- Juvenile idiopathic arthritis (JIA)
- Vogt-Koyanagi-Harada syndrome
- Fuch’s heterochromic iridocyclitis
- Lymphoma
- Lyme Disease
- Acquired immunodeficiency syndrome (AIDS)
- Herpes simplex
- Varicella Zoster
- Cytomegalovirus
- Syphilis
- Toxoplasmosis
- Toxocariasis
- Tuberculosis
- Rubella
- Cat scratch disease (Bartonella spp.)
Gross Pathology
On gross pathology, redness of the eye and dilated cilliary vessels are common yet non-specific findings in uveitis. The following are images of the gross pathology of uveitis:[13][14]
-
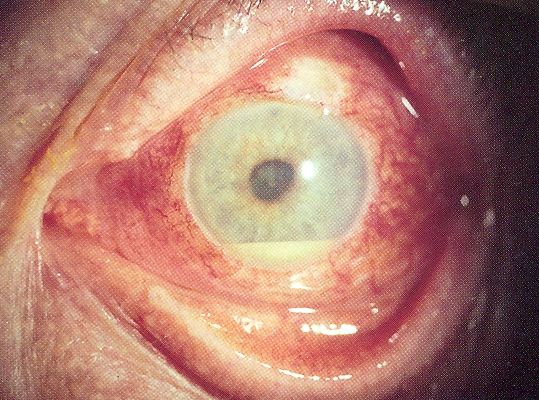 Uveitis with pus in the anterior chamber
Uveitis with pus in the anterior chamber -
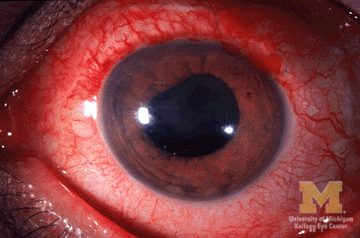 Anterior Uveitis
Anterior Uveitis


Microscopic Pathology
On microscopic histopathological analysis, lymphocytic infiltration, monocytic infiltration, epitheloid cells, and granulomatous inflammation of the uveal structures are characteristic findings of uveitis. The following are images of the microscopic pathology of uveitis:[15]
-
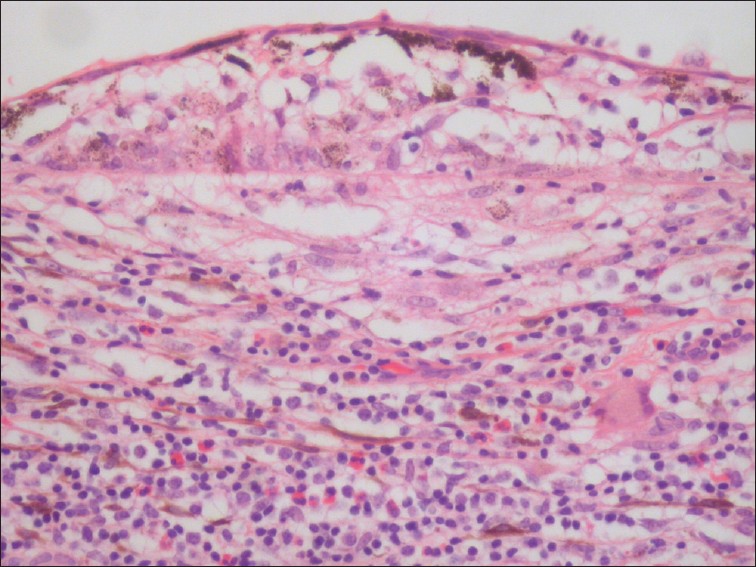 Uveitis with infiltration of lymphocytes
Uveitis with infiltration of lymphocytes -
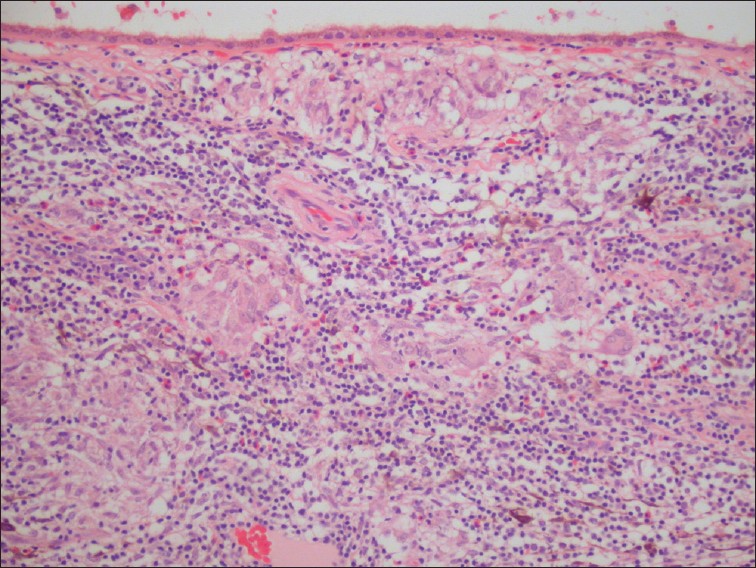 Uveitis with granulomatous inflammation and infiltration of the choroid by lymphocytes and macrophages
Uveitis with granulomatous inflammation and infiltration of the choroid by lymphocytes and macrophages


References
- ↑ 1.0 1.1 1.2 1.3 Lee, R. W. J., & Dick, A. D. (2012). Current concepts and future directions in the pathogenesis and treatment of non-infectious intraocular inflammation. Eye (London, England), 26(1), 17–28. https://doi.org/10.1038/eye.2011.255
- ↑ 2.0 2.1 2.2 2.3 2.4 2.5 Egwuagu, C. E., Alhakeem, S. A., & Mbanefo, E. C. (2021). Uveitis: Molecular pathogenesis and emerging therapies. Frontiers in Immunology, 12, 623725. https://doi.org/10.3389/fimmu.2021.623725
- ↑ 3.0 3.1 Rodriguez A, Calonge M, Pedroza-Seres M, Akova YA, Messmer EM, D’Amico DJ; et al. (1996). “Referral patterns of uveitis in a tertiary eye care center”. Arch Ophthalmol. 114 (5): 593–9. PMID 8619771.
- ↑ 4.0 4.1 4.2 4.3 Guly CM, Forrester JV (2010). “Investigation and management of uveitis”. BMJ. 341: c4976. doi:10.1136/bmj.c4976. PMID 20943722.
- ↑ 5.0 5.1 5.2 Przeździecka-Dołyk J, Węgrzyn A, Turno-Kręcicka A, Misiuk-Hojło M (2016). “Immunopathogenic Background of Pars Planitis”. Arch Immunol Ther Exp (Warsz). 64 (2): 127–37. doi:10.1007/s00005-015-0361-y. PMC 4805694. PMID 26438050.
- ↑ Urban B, Bakunowicz-Łazarczyk A, Michalczuk M (2014). “Immune recovery uveitis: pathogenesis, clinical symptoms, and treatment”. Mediators Inflamm. 2014: 971417. doi:10.1155/2014/971417. PMC 4096001. PMID 25089078.
- ↑ Sun D, Liang D, Kaplan HJ, Shao H (2015). “The role of Th17-associated cytokines in the pathogenesis of experimental autoimmune uveitis (EAU)”. Cytokine. 74 (1): 76–80. doi:10.1016/j.cyto.2014.12.017. PMC 4457592. PMID 25742774.
- ↑ Bi HS, Liu ZF, Cui Y (2015). “Pathogenesis of innate immunity and adaptive immunity in the mouse model of experimental autoimmune uveitis”. J Chin Med Assoc. 78 (5): 276–82. doi:10.1016/j.jcma.2015.01.002. PMID 25769932.
- ↑ Horai R, Caspi RR (2011). “Cytokines in autoimmune uveitis”. J Interferon Cytokine Res. 31 (10): 733–44. doi:10.1089/jir.2011.0042. PMC 3189550. PMID 21787221.
- ↑ Ke Y, Liu K, Huang GQ, Cui Y, Kaplan HJ, Shao H; et al. (2009). “Anti-inflammatory role of IL-17 in experimental autoimmune uveitis”. J Immunol. 182 (5): 3183–90. doi:10.4049/jimmunol.0802487. PMC 3275433. PMID 19234216.
- ↑ Maghsoudlou, P., Epps, S. J., Guly, C. M., & Dick, A. D. (2025). Uveitis in adults: A review: A review. The Journal of the American Medical Association, 334(5), 419–434. https://doi.org/10.1001/jama.2025.4358
- ↑ American Academy of Ophthalmology EyeWiki(2015)http://eyewiki.aao.org/Category:Uveitis
- ↑ Wikipedia Uveitis(2006)https://en.wikipedia.org/wiki/Uveitis#/media/File:Hypopyon.jpg
- ↑ University of Michigan Eyes Have It(2009)http://kellogg.umich.edu/theeyeshaveit/red-eye/anterior-uveitis.html
- ↑ Arevalo JF, Garcia RA, Al-Dhibi HA, Sanchez JG, Suarez-Tata L (2012). “Update on sympathetic ophthalmia”. Middle East Afr J Ophthalmol. 19 (1): 13–21. doi:10.4103/0974-9233.92111. PMC 3277011. PMID 22346110.
Causes
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Tarek Nafee, M.D. [2]
Overview
Common causes of uveitis include seronegative spondyloarthropathy, sarcoidosis, juvenile idiopathic arthritis, systemic lupus erythematosus, Behçet syndrome, multiple sclerosis, AIDS, syphilis, and tuberculosis.[1][2]
Causes
Uveitis may be caused by either systemic inflammatory diseases, localized infectious diseases, or isolated syndromes confined to the eye. No specific diagnosis is made in approximately one-half of cases. However, uveitis is often associated with human leukocyte antigen (HLA) alleles such as HLA-B27, HLA-A29, HLA-B51, HLA-B8, HLA-DR15, HLA-DR2.[1][2][3]
Systemic inflammatory disorders causing uveitis
Systemic autoimmune disorders that can cause uveitis include:[1][2][4]
- Ankylosing spondylitis
- Behçet’s disease
- Inflammatory bowel disease
- Juvenile rheumatoid arthritis
- Kawasaki disease
- Multiple sclerosis
- Psoriatic arthritis
- Reiter’s syndrome
- Sarcoidosis
- Systemic lupus erythematosus
- Whipple disease
Infectious disease causes of uveitis
Infectious diseases that can cause uveitis include:[1][2][5]
- Toxocariasis
- Toxoplasmosis
- Tuberculosis
- Syphilis
- Leptospirosis
- Brucellosis
- Herpes simplex
- Varicella zoster
- Presumed ocular histoplasmosis syndrome
- Lyme disease
- Cytomegalovirus
- Rubella
- Cat scratch disease (Batronela spp.)
Isolated eye disorders causing uveitis
Isolated eye disorders that can cause uveitis include:[1][2][6]
- Vogt-Koyanagi-Harada syndrome
- Acute posterior multifocal placoid pigment epitheliopathy
- Birdshot retinochoroidopathy
Cause by Anatomical Location
The cause of uveitis may vary depending on the anatomical location affected:[1][2]
- Anterior uveitis may be associated with autoimmune diseases, but most cases occur in healthy people for unapparent reasons. The disorder may affect only one eye. It is most common in young and middle-aged people.
- Intermediate uveitis usually occurs in young men and is generally not associated with any other disease. In most cases, the cause is unknown.[7] However, some evidence suggests it may be linked to Crohn’s disease and possibly multiple sclerosis.[8]
- Posterior uveitis may develop in people who have an autoimmune disease or who have had a systemic (body-wide) infection. The most common cause of posterior uveitis is infections resulting from toxoplasmosis.[9]
Causes by Organ System
Causes in Alphabetical Order
References
- ↑ 1.0 1.1 1.2 1.3 1.4 1.5 Guly CM, Forrester JV (2010). “Investigation and management of uveitis”. BMJ. 341: c4976. doi:10.1136/bmj.c4976. PMID 20943722.
- ↑ 2.0 2.1 2.2 2.3 2.4 2.5 Rodriguez A, Calonge M, Pedroza-Seres M, Akova YA, Messmer EM, D’Amico DJ; et al. (1996). “Referral patterns of uveitis in a tertiary eye care center”. Arch Ophthalmol. 114 (5): 593–9. PMID 8619771.
- ↑ Przeździecka-Dołyk J, Węgrzyn A, Turno-Kręcicka A, Misiuk-Hojło M (2016). “Immunopathogenic Background of Pars Planitis”. Arch Immunol Ther Exp (Warsz). 64 (2): 127–37. doi:10.1007/s00005-015-0361-y. PMC 4805694. PMID 26438050.
- ↑ White G.“Uveitis.” AllAboutVision.com. Retrieved August 20, 2006.
- ↑ White G.“Uveitis.” AllAboutVision.com. Retrieved August 20, 2006.
- ↑ White G.“Uveitis.” AllAboutVision.com. Retrieved August 20, 2006.
- ↑ http://www.preventblindness.org/uveitis/what/types.html
- ↑ http://www.nlm.nih.gov/medlineplus/ency/article/001005.htm
- ↑ http://www.preventblindness.org/uveitis/what/types.html
Differentiating Uveitis from other Diseases
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Tarek Nafee, M.D. [2]
Overview
Uveitis must be differentiated from other diseases that cause conjunctival injection, eye pain, photophobia, or visual disturbance. Masquerade syndromes, which are ophthalmic disorders that clinically present as either an anterior or posterior uveitis but are not primarily inflammatory, must be differentiated from uveitis. As uveitis manifests in a variety of clinical etiologies, differentiation must also be established in accordance with the particular subtype.[1][2][3][4]
Differential Diagnosis
Uveitis must be differentiated from other diseases that cause conjunctival injection, eye pain, photophobia, or visual disturbance. Masquerade syndromes, which are ophthalmic disorders that clinically present as either an anterior or posterior uveitis but are not primarily inflammatory, must be differentiated from uveitis. As uveitis manifests in a variety of clinical etiologies, differentiation must also be established in accordance with the particular subtype.[1][2][3][4]
Differentiating Uveitis from Other Diseases
Uveitis must be differentiated from other diseases that cause conjunctival injection, eye pain, photophobia, or visual disturbance, and include:[5][6][7]
- Corneal ulceration
- Conjunctivitis
- Closed angle glaucoma
- Corneal abrasion
- Ulcerative keratitis
- Herpes keratitis
- Intraocular foreign body
- Episcleritis or scleritis
- Endophthalmitis
- Radiation-induced keratitis
Masquerade syndromes
Masquerade syndromes are ophthalmic disorders that clinically present as either an anterior or posterior uveitis, but are not primarily inflammatory. The following are some of the most common:[4]
- Anterior segment
- Posterior segment
References
- ↑ 1.0 1.1 Prior-Español Á, Martínez-Morillo M, Holgado-Pérez S, Juega FJ (2016). “Differential diagnosis of acute bilateral uveitis in the rheumatologist’s office”. Reumatol Clin. 12 (3): 174–175. doi:10.1016/j.reuma.2015.05.012. PMID 26187650.
- ↑ 2.0 2.1 Guly CM, Forrester JV (2010). “Investigation and management of uveitis”. BMJ. 341: c4976. doi:10.1136/bmj.c4976. PMID 20943722.
- ↑ 3.0 3.1 American Academy of Ophthalmology EyeWiki (2015)http://eyewiki.aao.org/Category:Uveitis
- ↑ 4.0 4.1 4.2 Rothova A, Ooijman F, Kerkhoff F, Van Der Lelij A, Lokhorst HM (2001). “Uveitis masquerade syndromes”. Ophthalmology. 108 (2): 386–99. PMID 11158819.
- ↑ Dart JK (1986). “Eye disease at a community health centre”. Br Med J (Clin Res Ed). 293 (6560): 1477–80. PMC 1342247. PMID 3099921.
- ↑ Leibowitz HM (2000). “The red eye”. N Engl J Med. 343 (5): 345–51. doi:10.1056/NEJM200008033430507. PMID 10922425.
- ↑ University of Michigan Eyes Have it (2009)http://kellogg.umich.edu/theeyeshaveit/red-eye/
Epidemiology and Demographics
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Tarek Nafee, M.D. [2]; M Chadi Alraies M.D., MPH [3]
Overview
Worldwide, the prevalence of uveitis ranges from 69 to 204 per 100,000 persons. The prevalence among different subtypes of uveitis varies greatly. Anterior, chronic, non-granulomatous and non-infectious subtypes are more commonly seen than others. The worldwide incidence of uveitis ranges from 17 to 52 per 100,000 persons per year. The age, sex, and race distribution is also dictated by the prevalence of the underlying cause within those demographic groups.[1][2][3]
Epidemiology
Worldwide incidence and prevalence of uveitis has been well studied. The epidemiologic data varies greatly by underlying etiology or classification of uveitis.
Prevalence
The reported global prevalence of uveitis ranges widely from 38 to 714 per 100,000 people, reflecting substantial geographic and methodological variability. Uveitis is responsible for 3%–10% of visual impairment in the United States and Europe and has been associated with up to one-quarter of blindness in low- and middle-income countries.[4]
Prevalence by Subtype
Several studies have reported prevalence data among a large group of uveitis patients, as follows:
- By anatomy In the United States and Europe, [5][6][7][8][9]
- Anterior uveitis is the most common subtype (41%–60%)
- Posterior uveitis (17%–23%)
- Intermediate uveitis (9%–15%)
- Panuveitis (7%–32%)
- By Etiology In high-income countries, 52%–79% of uveitis cases are noninfectious, while 11%–21% are infectious; in contrast, infectious causes account for up to 50% of cases in low- and middle-income countries.[4][10] In high-income settings, the most common infectious causes include toxoplasmosis (5%–7%) and herpes-related uveitis (5%–15%), whereas tuberculosis-related (8%–13%) and HIV-related (10%–14%) uveitis are more prevalent in low- and middle-income countries.[6][11][12][13][14][15][16] Despite comprehensive evaluation, 27%–51% of uveitis cases remain idiopathic.[5][7][17][8][18] In the United States and Europe, 37%–49% of uveitis cases are associated with systemic inflammatory diseases, most commonly axial spondyloarthritis.[5][6][7][17][19][20][21]
- By Laterality Laterality varies by anatomic subtype: anterior uveitis is more often unilateral (≈53%), whereas intermediate uveitis (79%), posterior uveitis (57%), and panuveitis (75%) are more commonly bilateral.[22]
- Geographic Contrast The epidemiology of uveitis varies substantially by geography and ethnicity, reflecting differences in genetic susceptibility, environmental exposures, and regional infection prevalence.[23][24] In regions with a lower prevalence of HLA-B27, such as Japan, panuveitis predominates (≈46%), followed by anterior (38%), posterior (13%), and intermediate uveitis (3%).[25] Sarcoidosis-associated uveitis is more frequent in Europe and the United States (≈8%–10%), Behçet disease accounts for approximately 30% of uveitis cases in Turkey, and Vogt–Koyanagi–Harada disease is more prevalent in East Asian populations.[9][26][27][28][29]
- By Prognosis In a large US insurance-based cohort, approximately 5% of patients with noninfectious intermediate, posterior, or panuveitis developed blindness or low vision within 5 years.[30]
Incidence
Worldwide, the incidence of uveitis ranges from 17 to 52 per 100,000 per year.[1][2][3]
Demographics
The age, sex, and race distribution of uveitis is dictated by the prevalence of the underlying cause within those demographic groups.
Age
Uveitis can occur at any age but presents most frequently in young and middle-aged adults (20–50 years), who account for approximately 60%–80% of cases.[4][17][31]The prevalence among age groups varies greatly depending on the underlying etiology. The following is an example of age distribution by underlying etiology:[3][32][33][34][35]
- Children: Juvenile rheumatoid arthritis, toxocariasis
- Young adults: Behçet’s disease, HLA-B27 antigen associated uveitis, Fuch’s uveitis
- Older adults: Vogt-Koyanagi-Harada syndrome, herpes zoster ophthalmicus, and tuberculosis
Gender
Overall, uveitis is more common in women, with approximately 57% of cases occurring in females.[36] Female predominance is particularly pronounced in uveitis associated with multiple sclerosis (≈75% female), juvenile idiopathic arthritis (50%–80% female), and sarcoidosis (55%–64% female), whereas HLA-B27–associated uveitis shows a male predominance (male-to-female ratio ≈1.5:1).[37] The prevalence of uveitis among one of the sexes depends on the gender distribution of the underlying disorder.[3]
Race
The prevalence of different etiologies of uveitis vary by race. Caucasians are more affected by HLA-B27 related conditions making HLA-related uveitis highly prevalent in this race group. Alternatively, middle eastern people are more likely affected with Behcet’s disease, making them more likely to have uveitis related to this disease. African Americans are more commonly affected by sarcoidosis, thus sarcoid related uveitis is more common in this group.[32][33][34][35]
References
- ↑ 1.0 1.1 Guly CM, Forrester JV (2010). “Investigation and management of uveitis”. BMJ. 341: c4976. doi:10.1136/bmj.c4976. PMID 20943722.
- ↑ 2.0 2.1 Gutteridge IF, Hall AJ (2007). “Acute anterior uveitis in primary care”. Clin Exp Optom. 90 (2): 70–82. doi:10.1111/j.1444-0938.2006.00128.x. PMID 17311570.
- ↑ 3.0 3.1 3.2 3.3 Rodriguez A, Calonge M, Pedroza-Seres M, Akova YA, Messmer EM, D’Amico DJ; et al. (1996). “Referral patterns of uveitis in a tertiary eye care center”. Arch Ophthalmol. 114 (5): 593–9. PMID 8619771.
- ↑ 4.0 4.1 4.2 Miserocchi, E., Fogliato, G., Modorati, G., & Bandello, F. (2013). Review on the worldwide epidemiology of uveitis. European Journal of Ophthalmology, 23(5), 705–717. https://doi.org/10.5301/ejo.5000278
- ↑ 5.0 5.1 5.2 Bertrand, P.-J., Jamilloux, Y., Ecochard, R., Richard-Colmant, G., Gerfaud-Valentin, M., Guillaud, M., Denis, P., Kodjikian, L., & Sève, P. (2019). Uveitis: Autoimmunity… and beyond. Autoimmunity Reviews, 18(9), 102351. https://doi.org/10.1016/j.autrev.2019.102351
- ↑ 6.0 6.1 6.2 Bajwa, A., Osmanzada, D., Osmanzada, S., Khan, I., Patrie, J., Xin, W., & Reddy, A. K. (2015). Epidemiology of uveitis in the mid-Atlantic United States. Clinical Ophthalmology (Auckland, N.Z.), 9, 889–901. https://doi.org/10.2147/OPTH.S80972
- ↑ 7.0 7.1 7.2 Barisani-Asenbauer, T., Maca, S. M., Mejdoubi, L., Emminger, W., Machold, K., & Auer, H. (2012). Uveitis- a rare disease often associated with systemic diseases and infections- a systematic review of 2619 patients. Orphanet Journal of Rare Diseases, 7(1), 57. https://doi.org/10.1186/1750-1172-7-57
- ↑ 8.0 8.1 Jabs, D. A., & Busingye, J. (2013). Approach to the diagnosis of the uveitides. American Journal of Ophthalmology, 156(2), 228–236. https://doi.org/10.1016/j.ajo.2013.03.027
- ↑ 9.0 9.1 Jones, N. P., Pockar, S., & Steeples, L. R. (2023). Changing trends in uveitis in the United Kingdom: 5000 consecutive referrals to a tertiary referral centre. Ocular Immunology and Inflammation, 31(5), 921–926. https://doi.org/10.1080/09273948.2022.2067067
- ↑ Tsirouki, T., Dastiridou, A., Symeonidis, C., Tounakaki, O., Brazitikou, I., Kalogeropoulos, C., & Androudi, S. (2018). A focus on the epidemiology of uveitis. Ocular Immunology and Inflammation, 26(1), 2–16. https://doi.org/10.1080/09273948.2016.1196713
- ↑ Cimino, L., Aldigeri, R., Salvarani, C., Zotti, C. A., Boiardi, L., Parmeggiani, M., Casali, B., & Cappuccini, L. (2010). The causes of uveitis in a referral centre of Northern Italy. International Ophthalmology, 30(5), 521–529. https://doi.org/10.1007/s10792-010-9359-y
- ↑ Hermann, L., Falcão-Reis, F., & Figueira, L. (2021). Epidemiology of Uveitis in a tertiary care centre in Portugal. Seminars in Ophthalmology, 36(1–2), 51–57. https://doi.org/10.1080/08820538.2021.1885721
- ↑ Tyagi, M., Das, A. V., Kaza, H., Basu, S., Pappuru, R. R., Pathengay, A., Murthy, S., & Agrawal, H. (2022). LV Prasad Eye Institute EyeSmart electronic medical record-based analytics of big data: LEAD-Uveitis Report 1: Demographics and clinical features of uveitis in a multi-tier hospital based network in Southern India. Indian Journal of Ophthalmology, 70(4), 1260–1267. https://doi.org/10.4103/ijo.IJO_1122_21
- ↑ Mwanza, J. C., & Kayembe, D. L. (2001). Uveitis in HIV-infected patients. European Journal of Ophthalmology, 11(1), 53–56. https://doi.org/10.1177/112067210101100110
- ↑ Agrawal, R., Gunasekeran, D. V., Agarwal, A., Carreño, E., Aggarwal, K., Gupta, B., Raje, D., Murthy, S. I., Westcott, M., Chee, S. P., McCluskey, P., Ling, H. S., Teoh, S., Cimino, L., Biswas, J., Narain, S., Agarwal, M., Mahendradas, P., Khairallah, M., … Gupta, V. (2020). The collaborative ocular tuberculosis study (COTS)-1: A multinational description of the spectrum of choroidal involvement in 245 patients with tubercular uveitis. Ocular Immunology and Inflammation, 28(sup1), 38–48. https://doi.org/10.1080/09273948.2018.1489061
- ↑ Alli, H. D., Ally, N., Mayet, I., Dangor, Z., & Madhi, S. A. (2022). Global prevalence and clinical outcomes of tubercular uveitis: a systematic review and meta-analysis. Survey of Ophthalmology, 67(3), 770–792. https://doi.org/10.1016/j.survophthal.2021.10.001
- ↑ 17.0 17.1 17.2 Rothova, A., Buitenhuis, H. J., Meenken, C., Brinkman, C. J., Linssen, A., Alberts, C., Luyendijk, L., & Kijlstra, A. (1992). Uveitis and systemic disease. The British Journal of Ophthalmology, 76(3), 137–141. https://doi.org/10.1136/bjo.76.3.137
- ↑ Chang, J. H.-M., & Wakefield, D. (2002). Uveitis: a global perspective. Ocular Immunology and Inflammation, 10(4), 263–279. https://doi.org/10.1076/ocii.10.4.263.15592
- ↑ Bro, T., & Tallstedt, L. (2020). Epidemiology of uveitis in a region of southern Sweden. Acta Ophthalmologica, 98(1), 32–35. https://doi.org/10.1111/aos.14130
- ↑ London, N. J., Garg, S. J., Moorthy, R. S., & Cunningham, E. T. (2013). Drug-induced uveitis. Journal of Ophthalmic Inflammation and Infection, 3(1), 43. https://doi.org/10.1186/1869-5760-3-43
- ↑ Hu, J., Vu, J. T., Hong, B., & Gottlieb, C. (2020). Uveitis and cystoid macular oedema secondary to topical prostaglandin analogue use in ocular hypertension and open angle glaucoma. The British Journal of Ophthalmology, 104(8), 1040–1044. https://doi.org/10.1136/bjophthalmol-2019-315280
- ↑ Rodriguez, A., Calonge, M., Pedroza-Seres, M., Akova, Y. A., Messmer, E. M., D’Amico, D. J., & Foster, C. S. (1996). Referral patterns of uveitis in a tertiary eye care center. Archives of Ophthalmology, 114(5), 593–599. https://doi.org/10.1001/archopht.1996.01100130585016
- ↑ Guo, X., Chen, Z., & Xing, Y. (2021). Immune-mediated uveitis and lifestyle factors: A review. Ophthalmic Research, 64(5), 687–695. https://doi.org/10.1159/000518496
- ↑ Bai, Y.-C., Wang, C.-Y., Lin, C.-L., Lai, J.-N., & Wei, J. C.-C. (2021). Association between air pollution and the risk of uveitis: A nationwide, population-based cohort study. Frontiers in Immunology, 12, 613893. https://doi.org/10.3389/fimmu.2021.613893
- ↑ Liba, T., Gorenshtein, A., Leibovitch, L., Gepstein, R., Machinski, E., & Segal, O. (2025). Epidemiological characterization of uveitis in Japan: A systematic review. Ocular Immunology and Inflammation, 33(7), 1086–1095. https://doi.org/10.1080/09273948.2025.2452193
- ↑ Das, D., Bhattacharjee, H., Bhattacharyya, P. K., Jain, L., Panicker, M. J., Das, K., & Deka, A. C. (2009). Pattern of uveitis in North East India: a tertiary eye care center study. Indian Journal of Ophthalmology, 57(2), 144–146. https://doi.org/10.4103/0301-4738.45506
- ↑ Wakabayashi, T., Morimura, Y., Miyamoto, Y., & Okada, A. A. (2003). Changing patterns of intraocular inflammatory disease in Japan. Ocular Immunology and Inflammation, 11(4), 277–286. https://doi.org/10.1076/ocii.11.4.277.18260
- ↑ Çakar Özdal, M. P., Yazici, A., Tüfek, M., & Öztürk, F. (2014). Epidemiology of uveitis in a referral hospital in Turkey. Turkish Journal of Medical Sciences, 44(2), 337–342. https://doi.org/10.3906/sag-1302-132
- ↑ Engelhard, S. B., Patel, V., & Reddy, A. K. (2015). Intermediate uveitis, posterior uveitis, and panuveitis in the Mid-Atlantic USA. Clinical Ophthalmology (Auckland, N.Z.), 9, 1549–1555. https://doi.org/10.2147/OPTH.S89428
- ↑ Dick, A. D., Tundia, N., Sorg, R., Zhao, C., Chao, J., Joshi, A., & Skup, M. (2016). Risk of ocular complications in patients with noninfectious intermediate uveitis, posterior uveitis, or panuveitis. Ophthalmology, 123(3), 655–662. https://doi.org/10.1016/j.ophtha.2015.10.028
- ↑ Saari, K. M., Päivönsalo-Hietanen, T., Vaahtoranta-Lehtonen, H., Tuominen, J., & Sillanpää, M. (1995). Epidemiology of endogenous uveitis in south-western Finland. Acta Ophthalmologica Scandinavica, 73(4), 345–349. https://doi.org/10.1111/j.1600-0420.1995.tb00040.x
- ↑ 32.0 32.1 Agrawal RV, Murthy S, Sangwan V, et al; Current approach in diagnosis and management of anterior uveitis. Indian J Ophthalmol. 2010 Jan-Feb;58(1):11-9. doi: 10.4103/0301-4738.58468.
- ↑ 33.0 33.1 Guly CM, Forrester JV; Investigation and management of uveitis. BMJ. 2010 Oct 13;341:c4976. doi: 10.1136/bmj.c4976
- ↑ 34.0 34.1 Gutteridge IF, Hall AJ; Acute anterior uveitis in primary care. Clin Exp Optom. 2007 Mar;90(2):70-82.
- ↑ 35.0 35.1 Patient Info UK and European Guidelines(2016)http://patient.info/doctor/uveitis-pro#ref-1
- ↑ Thorne, J. E., Suhler, E., Skup, M., Tari, S., Macaulay, D., Chao, J., & Ganguli, A. (2016). Prevalence of noninfectious uveitis in the United States: A claims-based analysis. JAMA Ophthalmology, 134(11), 1237–1245. https://doi.org/10.1001/jamaophthalmol.2016.3229
- ↑ Yeung, I. Y. L., Popp, N. A., & Chan, C.-C. (2015). The role of sex in uveitis and ocular inflammation. International Ophthalmology Clinics, 55(3), 111–131. https://doi.org/10.1097/IIO.0000000000000072
Risk Factors
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Tarek Nafee, M.D. [2]
Overview
A history of cigarette smoking is associated with all etiologies and subtypes of uveitis.[1] Some underlying causes have specific potent risk factors for developing uveitis such as seronegative spondyloarthropathies, immunosuppression, sarcoidosis, and juvenile idiopathic arthritis.[2]
Risk Factors
A history of smoking is associated with all etiologies and subtypes of uveitis.[1] Some underlying causes may have potent risk factors for developing uveitis such as:[2]
- Acute posterior multifocal placoid pigment epitheliopathy: HLA-B27 or HLA-DR2 alleles, preceding viral illness, underlying vasculitis
- CMV retinitis: HIV, CD4 count <50, severe immunosuppression, localized ocular immunosuppression
- Necrotizing herpitic retinitis: Immunosuppression
- Punctuate inner choroidopathy: Myopia in females, age 18 to 40
- Sarcoid uveitis: African American race, age<50
- Autoimmune scleritis: Female gender, age 40-60 years
- Sympathetic ophthalmia: Ocular trauma with delayed closing of the wound
- Acute anterior uveitis: HLA-B27 allele, ankylosing spondylitis, psoraitic arthritis
- TINU syndrome: Female gender
- Vogt-Koyanagi-Harada syndrome: Hispanic or Japanese race, HLA-DR1 and HLA-DR4 alleles
- Drug-induced uveitis: Use of rifabutin, cidofovir, bisphosphonates, sulfonamides, moxifloxacin, metipranolol, brimonidine, prostaglandin analogues, or flurbiprofen
References
- ↑ 1.0 1.1 Lin P, Loh AR, Margolis TP, Acharya NR (2010). “Cigarette smoking as a risk factor for uveitis”. Ophthalmology. 117 (3): 585–90. doi:10.1016/j.ophtha.2009.08.011. PMC 2830339. PMID 20036011.
- ↑ 2.0 2.1 American Academy of Ophthalmology EyeWiki (2015-2016)http://eyewiki.aao.org/Category:Uveitis
Screening
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Tarek Nafee, M.D. [2]
Overview
There is insufficient evidence to recommend routine screening for uveitis for the general population. For patients diagnosed with or suspected of having juvenile idiopathic arthritis (JIA), screening guidelines have been recommended by the American Academy of Pediatrics (AAP) and the British Society of Paediatrics and Rheumatology (BSPAR).[1][2]
Screening
There is insufficient evidence to recommend routine screening for uveitis for the general population.[3] For patients diagnosed with, or suspected of having juvenile idiopathic arthritis (JIA), screening guidelines have been recommended based on the AAP, Cincinnati Children’s Hospital, and the BSPAR. Screening for uveitis in children with JIA is recommended as follows:
- Patients should be referred at the time of diagnosis or suspicion of JIA, and a slit lamp ophthalmologic examination be performed within one month to 6 weeks of referral. It is recommended that after the initial screening examination, regular follow-up screenings be maintained based on risk category and classification.
For access to the complete American guideline,click here.[2]
For access to the complete British guideline,click here.[1]
References
- ↑ 1.0 1.1 Sen ES, Dick AD, Ramanan AV (2015). “Uveitis associated with juvenile idiopathic arthritis”. Nat Rev Rheumatol. 11 (6): 338–48. doi:10.1038/nrrheum.2015.20. PMID 25825278.
- ↑ 2.0 2.1 Cassidy J, Kivlin J, Lindsley C, Nocton J, Section on Rheumatology. Section on Ophthalmology (2006). “Ophthalmologic examinations in children with juvenile rheumatoid arthritis”. Pediatrics. 117 (5): 1843–5. doi:10.1542/peds.2006-0421. PMID 16651348.
- ↑ U.S. Preventative Services Task Force Recommendations (2016)http://www.uspreventiveservicestaskforce.org/BrowseRec/Index/browse-recommendations
Natural History, Complications and Prognosis
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Tarek Nafee, M.D. [2]
Overview
If left untreated, uveitis can progress to permanent vision loss. Complications of uveitis include cataracts, glaucoma, macular edema, and retinal detachment. With appropriate treatment, most attacks of anterior uveitis resolve within days to weeks, however, relapses are common. Inflammation related to posterior uveitis may last from months to years and may cause permanent vision damage, even with treatment.[1][2][3][4][5]
Natural History
If left untreated, uveitis can progress to permanent vision loss. Uveitis is estimated to be responsible for approximately 10% of the blindness in the western world.[3][4][5]
Complications
Possible complications of uveitis include:[6][7]
Prognosis
The prognosis of uveitis varies with the subtype, etiology, severity, duration and responsiveness to treatment.
- The following are favorable prognostic factors:[8][9][10][11][12][13][14][15][16][17]
- Rapid initiation of corticosteroid treatment
- Good initial visual acuity
- Good response to standard medical therapy
- The following are poor prognostic factors:[8][9][10][11][12][13][14][15][16][17]
- Chronic disease course
- Posterior or intermediate uveitis
- Lack of response to standard medical therapy
- Complications of uveitis
- Poor initial visual acuity
- Isolated ocular uveitis (no underlying systemic disease)
With appropriate treatment, most attacks of anterior uveitis resolve within days to weeks, however, relapses are common. Inflammation related to posterior uveitis may last from months to years and may cause permanent vision damage, even with treatment.[1][2]
References
- ↑ 1.0 1.1 MedlinePlus Medical Encyclopedia Uveitis(2014)https://medlineplus.gov/ency/article/001005.htm
- ↑ 2.0 2.1 Patient Trusted Medical Information and Support (2016)http://patient.info/health/uveitis-leaflet
- ↑ 3.0 3.1 McCluskey PJ, Towler HM, Lightman S (2000). “Management of chronic uveitis”. BMJ. 320 (7234): 555–8. PMC 1117601. PMID 10688564.
- ↑ 4.0 4.1 Rothova A, Suttorp-van Schulten MS, Frits Treffers W, Kijlstra A (1996). “Causes and frequency of blindness in patients with intraocular inflammatory disease”. Br J Ophthalmol. 80 (4): 332–6. PMC 505460. PMID 8703885.
- ↑ 5.0 5.1 Nussenblatt RB (1990). “The natural history of uveitis”. Int Ophthalmol. 14 (5–6): 303–8. PMID 2249907.
- ↑ Dick AD, Tundia N, Sorg R, Zhao C, Chao J, Joshi A; et al. (2016). “Risk of Ocular Complications in Patients with Noninfectious Intermediate Uveitis, Posterior Uveitis, or Panuveitis”. Ophthalmology. 123 (3): 655–62. doi:10.1016/j.ophtha.2015.10.028. PMID 26712559.
- ↑ Maini R, O’Sullivan J, Reddy A, Watson S, Edelsten C (2004). “The risk of complications of uveitis in a district hospital cohort”. Br J Ophthalmol. 88 (4): 512–7. PMC 1772087. PMID 15031168.
- ↑ 8.0 8.1 Chee SP, Jap A, Bacsal K (2009). “Prognostic factors of Vogt-Koyanagi-Harada disease in Singapore”. Am J Ophthalmol. 147 (1): 154–161.e1. doi:10.1016/j.ajo.2008.07.044. PMID 18834575.
- ↑ 9.0 9.1 Sheu SJ, Kou HK, Chen JF (2003). “Prognostic factors for Vogt-Koyanagi-Harada disease”. J Chin Med Assoc. 66 (3): 148–54. PMID 12779034.
- ↑ 10.0 10.1 Al-Kharashi AS, Aldibhi H, Al-Fraykh H, Kangave D, Abu El-Asrar AM (2007). “Prognostic factors in Vogt-Koyanagi-Harada disease”. Int Ophthalmol. 27 (2–3): 201–10. doi:10.1007/s10792-007-9062-9. PMID 17435968.
- ↑ 11.0 11.1 Lobo A, Barton K, Minassian D, du Bois RM, Lightman S (2003). “Visual loss in sarcoid-related uveitis”. Clin Experiment Ophthalmol. 31 (4): 310–6. PMID 12880455.
- ↑ 12.0 12.1 Maleki A, Cao JH, Silpa-Archa S, Foster CS (2016). “VISUAL OUTCOME AND POOR PROGNOSTIC FACTORS IN ISOLATED IDIOPATHIC RETINAL VASCULITIS”. Retina. doi:10.1097/IAE.0000000000001019. PMID 26991648.
- ↑ 13.0 13.1 Bollemeijer JG, Wieringa WG, Missotten TO, Meenken I, ten Dam-van Loon NH, Rothova A; et al. (2016). “Clinical Manifestations and Outcome of Syphilitic Uveitis”. Invest Ophthalmol Vis Sci. 57 (2): 404–11. doi:10.1167/iovs.15-17906. PMID 26848879.
- ↑ 14.0 14.1 Cheon JH, Kim WH (2015). “An update on the diagnosis, treatment, and prognosis of intestinal Behçet’s disease”. Curr Opin Rheumatol. 27 (1): 24–31. doi:10.1097/BOR.0000000000000125. PMID 25405821.
- ↑ 15.0 15.1 Abu El-Asrar AM, Al Tamimi M, Hemachandran S, Al-Mezaine HS, Al-Muammar A, Kangave D (2013). “Prognostic factors for clinical outcomes in patients with Vogt-Koyanagi-Harada disease treated with high-dose corticosteroids”. Acta Ophthalmol. 91 (6): e486–93. doi:10.1111/aos.12127. PMID 23575246.
- ↑ 16.0 16.1 Wolf MD, Lichter PR, Ragsdale CG (1987). “Prognostic factors in the uveitis of juvenile rheumatoid arthritis”. Ophthalmology. 94 (10): 1242–8. PMID 3684202.
- ↑ 17.0 17.1 Al-Mansour YS, Al-Rajhi AA, Al-Dhibi H, Abu El-Asrar AM (2010). “Clinical features and prognostic factors in Fuchs’ uveitis”. Int Ophthalmol. 30 (5): 501–9. doi:10.1007/s10792-010-9379-7. PMID 20496098.
Diagnosis
Diagnosis
History and Symptoms | Physical Examination | Laboratory Findings | X ray | CT | MRI | Ultrasound | Other Imaging Findings | Other Diagnostic Studies
Treatment
Treatment
Medical therapy | Surgery | Primary Prevention | Secondary Prevention | Cost Effectiveness of Therapy | Future or Investigational Therapies
Related Chapters
Related Chapters
External Links
External Links
Looking for the patient version?
© 2026 MyEClinic – IFTM Institut für Telematik in der Medizin GmbH