
Amenorrhea
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Eiman Ghaffarpasand, M.D. [2]
Synonyms and keywords:Primary amenorrhea, Secondary amenorrhea, Functional amenorrhea, Hypothalamic amenorrhea, Menstrual cycle pause.
Overview
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Eiman Ghaffarpasand, M.D. [2]
Overview
The first descriptions about disturbances in menstrual cycle are found in Papyrus Ebres [named after the Egyptologist Georg M. Ebers (1837-1898)], from New Kingdom period (1450-1550 B.C.). Amenorrhea may be classified according to etiology into three subtypes, including primary amenorrhea, secondary amenorrhea, and functional amenorrhea. Primary amenorrhea is basically refers to a young girl who have not experienced menarche, at all. Secondary amenorrhea reflects a woman who had ordinary menstruation cycles, experiencing at least 3 months of absence of menstruation cycle. Functional amenorrhea is a subtype of the amenorrhea caused by exaggerated different lifestyles. Primary and secondary amenorrhea are distinguished solely based on history. Mainly the pathophysiology of amenorrhea is described in many categories, include hypothalamic, pituitary, thyroid, adrenal, ovarian, uterine, and vaginal pathogenesis. About 25 various genes, in 3 different group of Kallmann syndrome related genes, hypothalamus–pituitary–gonadal (HPG) axis related genes, and obesity related genes, play role in amenorrhea. Common causes of amenorrhea include breastfeeding, pregnancy, menopause, and stress. Primary amenorrhea must be differentiated from other diseases that cause lack of menstrual cycle, such as Mullerian agenesis, 3-beta-hydroxysteroid dehydrogenase type 2 deficiency, androgen insensitivity syndrome, Kallmann syndrome, Turner syndrome, and 17-alpha-hydroxylase deficiency. In contrast, secondary amenorrhea must be differentiated from other diseases that cause menstrual cycle arrest, such as primary ovarian insufficiency, hypothyroidism, hyperprolactinemia, polycystic ovary syndrome, and Asherman’s syndrome. The prevalence of amenorrhea is approximately 3,000 to 4,000 per 100,000 individuals worldwide. The most common risk factor in the development of primary amenorrhea is chromosomal disorder and the most common risk factor in the development of secondary amenorrhea is breastfeeding. If left untreated, all of patients with amenorrhea may progress to develop infertility and osteoporosis. Common complications of amenorrhea are based on the background disease that induced it. Prognosis is generally excellent and the mortality rate of patients with amenorrhea is approximately less than 1%, generally in amenorrhea due to brain lesions. The initial laboratory tests for evaluating amenorrhea are pregnancy test, thyroid stimulating hormone (TSH), follicle stimulating hormone (FSH), and prolactin (PRL). Second line laboratory tests include free and total testosterone, dehydroepiandrosterone sulfate (DHEAS), and also progesterone challenge test. There are no echocardiography findings associated with amenorrhea. However, an echocardiography may be helpful in the diagnosis of the diseases that can cause amenorrhea, such as Turner syndrome. Findings on an echocardiography suggestive of Turner syndrome include bicuspid aortic valve, elongation of transverse aortic arch, coarctation of aorta, and partial anomalous pulmonary venous return (PAPVR). There are no ultrasound findings associated with amenorrhea. However, an ultrasound may be helpful in the diagnosis of the diseases that can cause amenorrhea, such as polycystic ovary syndrome (PCOS), premature ovarian insufficiency, androgen insensitivity syndrome, 17-alpha hydroxylase deficiency, and also anatomic genital defects. Pharmacologic medical therapy is recommended among patients with hypothalamic causes, pituitary causes, ovarian insufficiency, and chronic anovulation. The general principle of the treatment in amenorrhea is sex hormone replacement therapy, with suitable forms of estrogen and progesterone. The mainstay of treatment for amenorrhea is medical therapy. Surgery is usually reserved for patients with either hypothalamus or pituitary tumors, Turner syndrome, and genital anatomical defects (imperforate hymen or transverse vaginal septum). The surgical treatment for hypothalamus or pituitary tumors is tumor resection via endoscopic transsphenoidal surgery. Ovaries have to be excised in Turner syndrome to prevent malignant transformation. Small incision is the main surgery for imperforate hymen and septal excision is the main treatment for transverse vaginal septum.
Historical Perspective
The ancient Egyptian belief honored “menstrual blood” as life-giving. The Mesopotamian mother goddess, named Ninhursag, is believed to have created mankind from loam and her “blood of life“. The first descriptions about disturbances in menstrual cycle are found in Papyrus Ebres [named after the Egyptologist Georg M. Ebers (1837-1898)], from New Kingdom period (1450-1550 B.C.E). They described the patients as a “women who suffers from the side of her pubic region as an irregularity of her menstruation“. In 1907, British Medical Journal, released an article about different types of treatments (mostly herbal and conservative) for amenorrhea. In 1911, some researchers evaluate the therapeutic methods presented 4 years ago and make some suggestions to manage amenorrhea better. The term amenorrhea is derived from Greek language [a = negative, men = month, rhoia = flow], means lack of menstruation cycle in a woman.
Classification
Amenorrhea may be classified according to etiology into three subtypes, including primary amenorrhea, secondary amenorrhea, and functional amenorrhea. Primary amenorrhea is basically refers to a young girl who have not experienced menarche, at all, classified as hypergonadotropic hypogonadism, hypogonadotropic hypogonadism, and eugonadotropic state. Secondary amenorrhea reflects a woman who had normal menstruation cycles, experiencing at least 3 months of absence of menstruation cycle. It is classified as polycystic ovary syndrome, hypothalamic–pituitary dysfunction, hypothalamic–pituitary failure, and ovarian failure. Functional amenorrhea is a subtype of the amenorrhea caused by exaggerated different lifestyles, classified as stress, weight loss, and exercise related groups.
Pathophysiology
Amenorrhea is defined as absence of menstrual cycle. The pathophysiology of amenorrhea include hypothalamic, pituitary, thyroid, adrenal, ovarian, uterine, and vaginal causes. About 25 different genes are involved in the pathogenesis of amenorrhea such as 3 different groups of Kallmann syndrome related genes, hypothalamus–pituitary–gonadal (HPG) axis related genes, and obesity related genes. On gross pathology, normal endometrium is the characteristic findings of amenorrhea. Patients of amenorrhea from craniopharyngioma have cystic mass filled with motor oil-like fluid on gross pathology. On microscopic histopathological analysis, craniopharyngioma presents as trabecular squamous epithelium surrounded by palisaded columnar epithelium, small-to-medium sized cells with moderate amount of basophilic cytoplasm, bland nuclei, and calcifications. On microscopic histopathological analysis, pituitary adenoma as a cause of amenorrhea presents as loss of fibrous stroma and nested cells of normal anterior pituitary (based on the type of adenoma).
Causes
Common causes of amenorrhea are breastfeeding, pregnancy, menopause, and stress. Common causes of primary amenorrhea are craniopharyngioma, idiopathic gonadotropin deficiency, Kallmann’s syndrome, Mayer-Rokitansky-Hauser Syndrome, Mullerian dysgenesis, and outflow tract disorders. Common causes of secondary amenorrhea are craniocerebral trauma, curettage, Cushing’s syndrome, depression, diabetes mellitus, and drug side effects. Common causes of functional amenorrhea are stress, rapid weight loss, and excessive exercise.
Differentiating Amenorrhea from Other Diseases
As amenorrhea manifests in a variety of clinical forms, differentiation must be established in accordance with the particular subtype. Primary amenorrhea must be differentiated from other diseases that cause lack of menstrual cycle, such as Mullerian agenesis, 3-beta-hydroxysteroid dehydrogenase type 2 deficiency, androgen insensitivity syndrome, Kallmann syndrome, Turner syndrome, and 17-alpha-hydroxylase deficiency. In contrast, secondary amenorrhea must be differentiated from other diseases that cause menstrual cycle arrest, such as primary ovarian insufficiency, hypothyroidism, hyperprolactinemia, polycystic ovary syndrome, and Asherman’s syndrome.
Epidemiology and Demographics
The incidence of primary amenorrhea is approximately 3,000 cases per 100,000 individuals, mostly due to hypothalamic amenorrhea. The incidence of secondary amenorrhea is approximately 3,300 per 100,000 individuals. The prevalence of amenorrhea is approximately 3,000 to 4,000 per 100,000 individuals worldwide. The prevalence of amenorrhea was estimated to be 13,400 cases per 100,000 female athletes. The mortality rate of amenorrhea is less than 1%, and seen in patients of pituitary macroadenomas or generally brain lesions which cause amenorrhea. Primary amenorrhea is initially diagnosed among adolescents, 16 years of age. There is no racial predilection for amenorrhea. Commonly, females in developed countries experience puberty and menarche earlier than females of developing countries. This can be attributed to nutritional and socioeconomic situation but since the age of diagnosis of primary amenorrhea is based on the society’s mean age of puberty onset and menarche, there is not any difference between developing and developed countries in terms of prevalence of amenorrhea.
Risk Factors
The most common risk factor in the development of primary amenorrhea is chromosomal disorder and the most common risk factor in the development of secondary amenorrhea is breastfeeding. Common risk factors in the development of amenorrhea include risk factors related to hypothalamus, pituitary, ovaries, and also functional amenorrhea. Most common hypothalamic risk factors are Kallmann syndrome and chronic disorders. Most common pituitary risk factors are hyperprolactinemia and pituitary microadenoma.
Screening
According to the US Preventive Services Task Force (USPSTF), there is insufficient evidence to recommend routine screening for amenorrhea.
Natural History, Complications, and Prognosis
If left untreated, all of patients with amenorrhea may progress to develop infertility and osteoporosis. Common complications of amenorrhea are based on the background disease that induced it. Prognosis is generally excellent and the mortality rate of patients with amenorrhea is approximately less than 1%, generally in brain lesions.
Diagnosis
Diagnostic Criteria
There are no established criteria for the diagnosis of amenorrhea. Diagnosis is based on delayed or absent menstrual cycle.
History and Symptoms
The hallmark of primary amenorrhea is lack of menarche 15 years of age, while other secondary sexual characteristics are already appeared; or lack of menarche after 5 years of thelarche, if it is occurred before 10 years of age. The hallmark of secondary amenorrhea is menstrual cycle interruption for at least 3 months, however was regular before; or menstrual cycle interruption for at least 6 months, however was irregular before.
Physical Examination
Physical examination of patients with amenorrhea is based on underlying disease. The presence of hirsutism and acne on physical examination is diagnostic of polycystic ovary disease. The presence of galactorrhea and vision loss on physical examination is diagnostic of hyperprolactinemia (prolactinoma). The presence of bulging in vulva and imperforated hymen on physical examination is highly suggestive of imperforate hymen.
Laboratory Findings
The initial laboratory tests for evaluating amenorrhea are pregnancy test, thyroid stimulating hormone (TSH), follicle stimulating hormone (FSH), and prolactin (PRL). Second line laboratory tests include free and total testosterone, dehydroepiandrosterone sulfate (DHEAS), and also progesterone challenge test.
Electrocardiogram
There are no ECG findings associated with amenorrhea.
X-ray
There are no X-ray findings associated with amenorrhea, exclusively. There are no X-ray findings associated with most common causes of amenorrhea, like polycystic ovary syndrome (PCOS) and premature ovarian failure. However, an X-ray may be helpful in the diagnosis of delayed puberty.
Echocardiography/Ultrasound
There are no echocardiography findings associated with amenorrhea. However, an echocardiography may be helpful in the diagnosis of the diseases that can cause amenorrhea, such as Turner syndrome. Findings on an echocardiography suggestive of Turner syndrome include bicuspid aortic valve, elongation of transverse aortic arch, coarctation of aorta, and partial anomalous pulmonary venous return (PAPVR). There are no ultrasound findings associated with amenorrhea. However, an ultrasound may be helpful in the diagnosis of the diseases that can cause amenorrhea, such as polycystic ovary syndrome (PCOS), premature ovarian insufficiency, androgen insensitivity syndrome, 17-alpha hydroxylase deficiency, and also anatomic genital defects.
CT scan
There are no CT scan findings associated with amenorrhea. However, a CT scan may be helpful in the diagnosis of the diseases that can cause amenorrhea, such as Turner syndrome, androgen insensitivity syndrome and also anatomic genital defects.
MRI
There are no MRI findings associated with amenorrhea. However, a MRI may be helpful in the diagnosis of the diseases that can cause amenorrhea, such as polycystic ovary syndrome (PCOS), androgen insensitivity syndrome, anatomic genital defects, and also pituitary adenoma.
Other Imaging Findings
Hysterosalpingography (HSG) may be helpful in the diagnosis of the anatomic defects that can cause amenorrhea. Findings on a hysterosalpingography diagnostic of Asherman syndrome include multiple irregular linear (or lacunar) filling defects showing intrauterine adhesion, inability to distend the endometrial cavity, and totally non-filled uterine mostly in severe cases. Testicular scan can diagnosis the intra-abdominal or inguinal testes in androgen insensitivity syndrome.
Other Diagnostic Studies
Karyotyping is used to diagnose amenorrhea caused by chromosomal disorders, such as Turner syndrome. University of Pennsylvania Smell Identification Test (UPSIT), consist of microencapsulated odorants released by scratching standardized odor-impregnated questionnaires, is used to detect hyposmia or anosmia in Kallmann syndrome.
Treatment
Medical Therapy
Pharmacologic medical therapy is recommended among patients with hypothalamic causes, pituitary causes, ovarian insufficiency, and chronic anovulation. The general principle of the treatment in amenorrhea is sex hormone replacement therapy, mostly with suitable forms of estrogen and progesterone.
Surgery
The mainstay of treatment for amenorrhea is medical therapy. Surgery is usually reserved for patients with either hypothalamus or pituitary tumors, Turner syndrome, and genital anatomical defects (imperforate hymen or transverse vaginal septum). The surgical treatment for hypothalamus or pituitary tumors is tumor resection via endoscopic transsphenoidal surgery. Ovaries have to be excised in Turner syndrome to prevent malignant transformation. Small incision is the main surgery for imperforate hymen and septal excision is the main treatment for transverse vaginal septum.
Primary Prevention
Based on US Preventive Services Task Force (USPTSF), there are no established measures for the primary prevention of amenorrhea.
Secondary Prevention
Effective measures for the secondary prevention of functional hypothalamic amenorrhea include oral contraceptive pills (OCPs), androgen therapy, recombinant insulin like growth factor 1 (IGF-1), recombinant leptin, bisphosphonates, and increasing calorie intake.
References
Historical Perspective
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Eiman Ghaffarpasand, M.D. [2]
Overview
The ancient Egyptian belief honored “menstrual blood” as life-giving. The Mesopotamian mother goddess, named Ninhursag, is believed to have created mankind from loam and her “blood of life“. The first description on disturbances in menstrual cycle can be found in Papyrus Ebres [named after the Egyptologist Georg M. Ebers (1837-1898)], from New Kingdom period (1450-1550 B.C.E). They described the patients as a “women who suffers from the side of her pubic region as an irregularity of her menstruation“. In 1907, British Medical Journal, released an article about different types of treatments (mostly herbal and conservative) for amenorrhea. These treatment options were further evaluated in 1911 and led to a better approach in the management of amenorrhea. The term amenorrhea is derived from Greek language [a = negative, men = month, rhoia = flow], means lack of menstruation cycle in a woman.
Historical Perspective
Amenorrhea historical perspective
| Believed to create mankind from loam and her “blood of life“ Ninhursag Mesopotamian mother goddess | |||||||||||||||||||||||||||
| First descriptions about disturbances in menstrual cycle Papyrus Ebres, from New Kingdom period (1450-1550 B.C.E) Named after the Egyptologist Georg M. Ebers (1837-1898) | |||||||||||||||||||||||||||
| First definition of amenorrhea “woman suffering in her abdomen, so that the menstrual discharge can not leave her” Papyrus Edwin Smith, from 2900 B.C.E Named after an American antiques dealer (1822-1906) | |||||||||||||||||||||||||||
| Description of secondary amenorrhea in severe cachexia due to chronic peptic ulcer William Brinton, a British physician In 1855 | |||||||||||||||||||||||||||
| Suggestion of Permanganate of Potash for treatment of psychosis associated amenorrhea Maury Deas, a British physician In 1885 | |||||||||||||||||||||||||||
| Description of secondary amenorrhea with brain mass lesion Jollye, a British physician In 1894 | |||||||||||||||||||||||||||
| Release an article about treatments (mostly herbal and conservative) for amenorrhea British Medical Journal In 1907 | |||||||||||||||||||||||||||
| First description of pituitary gland as a regulator of gonads‘ stem cell Crowe, a Canadian physician In 1910 | |||||||||||||||||||||||||||
| First description of hypophysis, pituitary stalk, and centres above medulla oblongata as the pituitary gland controlling systems Bernhard Aschner, an Austrian endocrinologist In 1912 | |||||||||||||||||||||||||||
| Initiation of puberty and gonads enlargement by implanting animals’ pituitary glands into other animals (mice, cats, and rabbits) Philip Smith, an American endocrinologist In 1926 | Puberty induction by implanting adult humans’ or cows’ pituitary glands into some immature animals Bernhard Zondek, a Israeli gynecologist In 1926 | ||||||||||||||||||||||||||
| First revealing that pituitary gland secrets “prolan A” and “prolan B” as major controllers of the sexual life Bernhard Zondek, a Israeli gynecologist In 1929 | |||||||||||||||||||||||||||
| First presentation of sexual characteristics regression in mature animals and failure of sexual maturation in immature animals, both after excision of pituitary gland Philip Smith, an American endocrinologist In 1930 | First description of prolan A and prolan B roles in sexual cycle, leading to secretion of “fuliculin” and “lutein“ Bernhard Zondek, a Israeli gynecologist In 1930 | ||||||||||||||||||||||||||
| First naming fuliculin and lutein as follicle stimulating factor and luteinizing factor, respectively Fevold, an American zoologist In 1931 | |||||||||||||||||||||||||||
- The ancient Egyptian belief honored menstrual blood as life-giving. The Mesopotamian mother goddess, named Ninhursag, is believed to have created mankind from loam and her “blood of life“.[1]
- The first description on disturbances in menstrual cycle can be found in Papyrus Ebres [named after the Egyptologist Georg M. Ebers (1837-1898)], from New Kingdom period (1450-1550 B.C.E). They described the patients as a “women who suffers from the side of her pubic region as an irregularity of her menstruation“.[2][3]
- In Papyrus Edwin Smith [named after an American antiques dealer (1822-1906)], from 2900 B.C.E, first definition of amenorrhea presents as “woman suffering in her abdomen, so that the menstrual discharge can not leave her”. There are also herbal treatment options for this condition in the Papyrus.[4]
- The term amenorrhea is derived from Greek language [a = negative, men = month, rhoia = flow]. The opposite is the normal menstrual period.
- Historically, the term amenorrhea has been often used as a euphemism for “unwanted pregnancy” and many traditional treatments for this condition were in fact abortifacients.
- In 1855, William Brinton, a British physician, presented a woman with secondary amenorrhea caused by severe cachexia due to chronic peptic ulcer disease.[5]
- In 1885, Maury Deas, a British physician, suggested Permanganate of Potash as a treatment option for psychosis associated amenorrhea.[6]
- In 1894, Jollye, a British physician, described a girl with secondary amenorrhea along with some symptoms reflecting brain mass lesion.[7]
- In 1910, Crowe, a Canadian physician, was the first to describe pituitary gland as a regulator of gonadal stem cell.[8]
- In 1912, Bernhard Aschner, an Austrian endocrinologist, found gonadal control by pituitary gland is regulated by another superior center in the brain. He suggested hypophysis, pituitary stalk, and centers superior to the medulla oblongata as the controlling centers. Their dysfunction leads to hypopituitarism as well as hypogonadism.[9]
- In 1926, Philip Smith, an American endocrinologist, experienced and approved that implanting animals’ pituitary gland into other animals (mice, cats, and rabbits) leads to initiation of puberty and enlargement of gonads.[10]
- In 1926, Bernhard Zondek, a Israeli gynecologist, had the same experience, injecting adult humans’ or cows’ pituitary gland into immature animals and witnessing the rapid rush of their puberty process.[11]
- In 1929, Bernhard Zondek, a Israeli gynecologist, identified that, pituitary gland secretes two major hormones, that controls sexual life and maintains the species. He named them as “prolan A” and “prolan B“, named after the Latin word “prole” which means “descendant“.[12]
- In 1930, Philip Smith, an American endocrinologist, suggested that excision of pituitary gland in immature animals can lead to failure of sexual maturation; whereas in mature animals excision can lead to gonadal atrophy, regression of sexual characteristics, and infertility.[13]
- In 1930, Bernhard Zondek, a Israeli gynecologist, found prolan A is responsible for follicular growth stimulation and prolan B is responsible for ovulation induction and corpus luteum formation. Zondek also described that prolan A and B together induce the hormone “fuliculin” from gonads, while prolan B alone induce both fuliculin and “lutein” hormones.[14]
- In 1931, Fevold, an American zoologist, named fuliculin and lutein as follicle stimulating factor and luteinizing factor respectively.[15]
Landmark Events in the Development of Treatment Strategies
- In 1907, British Medical Journal, released an article about different types of treatments (mostly herbal and conservative) for amenorrhea.[16]
- In 1911, researchers further evaluated the therapeutic methods (described in 1907) and suggested better management of amenorrhea.[17]
References
- ↑ “Menstruation in ancient Egypt, by Petra Habiger, at the Museum of Menstruation and Women’s Health”.
- ↑ Sigerist, Henry (1951). A history of medicine. New York: Oxford. ISBN 9780195001020.
- ↑ “Reorganized text”. JAMA Otolaryngol Head Neck Surg. 141 (5): 428. 2015. doi:10.1001/jamaoto.2015.0540. PMID 25996397.
- ↑ Breasted, James (1930). The Edwin Smith surgical papyrus, published in facsimile and hieroglyphic transliteration with translation and commentary in two volumes. Chicago, Ill: University of Chicago, Oriental Institute. ISBN 0-918986-73-7.
- ↑ Brinton W (1856). “ROYAL FREE HOSPITAL. ULCER OF THE STOMACH, COMPLICATED WITH AMENORRHOEA, TREATED SUCCESSFULLY”. Assoc Med J. 4 (158): 22–4. PMC 2439376. PMID 20741224.
- ↑ Deas PM (1885). “Note on the Use of Permanganate of Potash in Cases of Insanity Associated with Amenorrhoea”. Br Med J. 1 (1268): 778–9. PMC 2256047. PMID 20751231.
- ↑ Jollye FW (1894). “A Case of Amenorrhoea with Brain Symptoms”. Br Med J. 1 (1747): 1354–5. PMC 2404280. PMID 20754906.
- ↑ Crowe, SJ (1910). Experimental hypophysectomy (Bulletin of the Johns Hopkins Hospital). Johns Hopkins Hospital: Johns Hopkins Press. ASIN B00088F464.
- ↑ Aschner, Bernhard (1912). “Ueber die Beziehungen zwischen Hypophysis und Genitale”. Archiv für Gynaekologie. 97 (2): 200–228. doi:10.1007/BF01726121. ISSN 0003-9128.
- ↑ Smith, P. E. (1926). “Hastening Development of Female Genital System by Daily Homoplastic Pituitary Transplants”. Experimental Biology and Medicine. 24 (2): 131–132. doi:10.3181/00379727-24-3260. ISSN 1535-3702.
- ↑ Zondek, Bernhard (1926). “Ueber die Funktion des Ovariums”. Zeitschr Geburtsh Gynäkol. 90: 327.
- ↑ Zondek, Bernhard (1929). “Weitere Untersuchungen zur Darstellung, Biologie und Klinik des Hypophysenvorderlappen-Hormons (Prolan)”. Klinische Wochenschrift. 8 (4): 157–159. doi:10.1007/BF01748589. ISSN 0023-2173.
- ↑ Steelman, Sanford L.; Pohley, Florence M. (1953). “ASSAY OF THE FOLLICLE STIMULATING HORMONE BASED ON THE AUGMENTATION WITH HUMAN CHORIONIC GONADOTROPIN”. Endocrinology. 53 (6): 604–616. doi:10.1210/endo-53-6-604. ISSN 0013-7227.
- ↑ Zondek, Bernhard (1930). “über die Hormone des Hypophysenvorderlappens”. Klinische Wochenschrift. 9 (6): 245–248. doi:10.1007/BF01765181. ISSN 0023-2173.
- ↑ Fevold, HL; Hisaw, FL; Leonard, SL (1931). “The gonad stimulating and the luteinizing hormones of the anterior lobe of the hypophesis”. American Journal of Physiology–Legacy Content. 97 (2): 291–301. ISSN 0002-9513.
- ↑ “The Composition Of Certain Secret Remedies. VIII. “Female Medicines” on JSTOR”.
- ↑ “THE COMPOSITION OF CERTAIN SECRET REMEDIES : PREPARATIONS FOR AMENORRHOEA AND OTHER WOMEN’S COMPLAINTS”. Br Med J. 2 (2635): 32–7. 1911. PMC 2331498. PMID 20765710.
]]
Classification
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Eiman Ghaffarpasand, M.D. [2]
Overview
Amenorrhea can be classified on the basis of etiology into three subtypes, including primary amenorrhea, secondary amenorrhea, and functional amenorrhea. Primary amenorrhea can also be classified on the basis of HPG (hypothalamic-pituitary-gonadal) axis function into hypergonadotropic hypogonadism, hypogonadotropic hypogonadism, and eugonadotropic state. Secondary amenorrhea reflects an absence of menstrual cycle for at least 3 months in a woman with normal menstruation cycles in the past. Secondary amenorrhea can be classified based on pathology into polycystic ovary syndrome, hypothalamic–pituitary dysfunction, hypothalamic–pituitary failure, and ovarian failure. Functional (hypothalamic) amenorrhea is a subtype of the amenorrhea seen in patients with erratic lifestyle and can be classified on the basis of etiology into stress, weight loss, and exercise related amenorrhea.
Classification
- Amenorrhea may be classified according to etiology into three subtypes:
- Primary amenorrhea
- Secondary amenorrhea
- Functional amenorrhea
- Each of the subtypes of amenorrhea has their own classifications, as following:
| Amenorrhea classification | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Lifestyle etiology | Lack of menarche | Mensturation absence more than 3 months | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Functional amenorrhea | Secondary amenorrhea | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Stress related | Weight loss related | Exercise related | Polycystic ovary syndrome | Hypothalamic–pituitary dysfunction | Hypothalamic–pituitary failure | Ovarian failure | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Primary amenorrhea | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Present uterus | Absent uterus | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Hypergonadotropic hypogonadism | Hypogonadotropic hypogonadism | Eugonadotropic | Mullerian agenesis | Androgen insensitivity | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Primary amenorrhea
- Primary amenorrhea refers to an adolescent girl who have never experienced menarche. Primary amenorrhea is defined as one of the followings:[1][2][3]
- Normal secondary sexual characteristics and absence of menarche by 15 years of age.
- Lack of secondary sexual characteristics and absence of menarche by 14 years of age.
- Lack of menarche five years after initial breast development (thelarche).
- An important aspect of classification in patients with primary amenorrhea is the presence or absence of uterus.
- If uterus is present, primary amenorrhea can be classified based on plasma level of follicle stimulating hormone (FSH) and luteinizing hormone (LH), into hypergonadotropic hypogonadism (elevated FSH and LH), hypogonadotropic hypogonadism (decreased FSH and LH), and eugonadotropic state (normal FSH and LH).
- Patients with absent uterus can be classified into mullerian agenesis or androgen insensitivity.
Secondary amenorrhea
- Secondary amenorrhea is more common than primary amenorrhea. Secondary amenorrhea is defined as one of the followings:
- Absence of menstrual cycle for at least 3 months in a woman with normal menstrual cycle in the past.
- Absence of menstrual cycle for at least 9 months in a woman with a history of oligomenorrhea.
- Secondary amenorrhea can be classified based on pathology into polycystic ovary syndrome, hypothalamic–pituitary dysfunction, hypothalamic–pituitary failure, and ovarian failure.[1][4][5]
Functional amenorrhea
- Functional (hypothalmic) amenorrhea is a subtype of the amenorrhea seen in patients with erratic lifestyle and can be classified on the basis of etiology into stress, weight loss, and exercise related amenorrhea.[6]
- Functional amenorrhea is defined as absence of menstrual cycle for 6 months from disturbances in hypothalamic-pituitary-ovarian axis, and without any anatomical or organic pathology.[7]
- Generally, the primary factor that causes functional amenorrhea is lack of gonadotropin releasing hormone (GnRH) pulsatility.[8]
References
- ↑ 1.0 1.1 “Current evaluation of amenorrhea”. Fertil. Steril. 90 (5 Suppl): S219–25. 2008. doi:10.1016/j.fertnstert.2008.08.038. PMID 19007635.
- ↑ Fritz, Marc (2011). Clinical gynecologic endocrinology and infertility. Philadelphia: Wolters Kluwer Health/Lippincott Williams & Wilkins. ISBN 9780781779685.
- ↑ Euling SY, Herman-Giddens ME, Lee PA, Selevan SG, Juul A, Sørensen TI, Dunkel L, Himes JH, Teilmann G, Swan SH (2008). “Examination of US puberty-timing data from 1940 to 1994 for secular trends: panel findings”. Pediatrics. 121 Suppl 3: S172–91. doi:10.1542/peds.2007-1813D. PMID 18245511.
- ↑ Reindollar, Richard H.; Novak, Michael; Tho, Sandra P.T.; McDonough, Paul G. (1986). “Adult-onset amenorrhea: A study of 262 patients”. American Journal of Obstetrics and Gynecology. 155 (3): 531–541. doi:10.1016/0002-9378(86)90274-7. ISSN 0002-9378.
- ↑ Reindollar RH, Byrd JR, McDonough PG (1981). “Delayed sexual development: a study of 252 patients”. Am. J. Obstet. Gynecol. 140 (4): 371–80. PMID 7246652.
- ↑ Meczekalski B, Podfigurna-Stopa A, Warenik-Szymankiewicz A, Genazzani AR (2008). “Functional hypothalamic amenorrhea: current view on neuroendocrine aberrations”. Gynecol. Endocrinol. 24 (1): 4–11. doi:10.1080/09513590701807381. PMID 18224538.
- ↑ Liu JH, Bill AH (2008). “Stress-associated or functional hypothalamic amenorrhea in the adolescent”. Ann. N. Y. Acad. Sci. 1135: 179–84. doi:10.1196/annals.1429.027. PMID 18574223.
- ↑ Gordon, Catherine M. (2010). “Functional Hypothalamic Amenorrhea”. New England Journal of Medicine. 363 (4): 365–371. doi:10.1056/NEJMcp0912024. ISSN 0028-4793.
Pathophysiology
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Eiman Ghaffarpasand, M.D. [2]
Overview
Amenorrhea is defined as absence of menstrual cycle. The causes of amenorrhea include hypothalamic, pituitary, thyroid, adrenal, ovarian, uterine, and vaginal. About 25 different genes are involved in the pathogenesis of amenorrhea including 3 different groups of Kallmann syndrome related genes, hypothalamus–pituitary–gonadal (HPG) axis related genes, and obesity related genes. On gross pathology, normal endometrium is the characteristic findings of amenorrhea. Patients of amenorrhea from Craniopharyngioma as have cystic mass filled with motor oil-like fluid on gross pathology. On microscopic histopathological analysis, craniopharyngioma presents as trabecular squamous epithelium surrounded by palisaded columnar epithelium, small-to-medium sized cells with moderate amount of basophilic cytoplasm, bland nuclei, and calcifications. On microscopic histopathological analysis, pituitary adenoma as a cause of amenorrhea presents as loss of fibrous stroma and nested cells of normal anterior pituitary (based on the type of adenoma).
Pathophysiology
Physiology of normal puberty
Menarche and Menstruation
- The mean age for onset of menstruation is 12.43 years in US. About 80% of females experience menarche between 11 and 13.75 years of age.[1]
- Almost all (98%) of females experience menarche by the age of 15.[2]
- Gonadotropin releasing hormone (GnRH) is the main factor in puberty onset.
- GnRH is secreted by the neurosecretory neurons of hypothalamus into the hypophysial portal system, from where it is transferred to anterior pituitary gland.
- GnRH stimulates production and secretion of follicle stimulating hormone (FSH) and luteinizing hormone (LH).
- During puberty the amplitude and frequency of GnRH pulses is significantly increased.
- GnRH secretion is regulated by certain neurotransmitters in brain, such as dopamine, endogenous opioids, norepinephrine, gamma amino butyric acid (GABA), and corticotropin releasing hormone (CRH). Alteration in level and function of these neurotransmitters may lead to specific types of amenorrhea. For example stress, exercise, and malnutrition affects CRH, β-endorphin, and dopamine, respectively.[3]
- After the onset of puberty, the negative feedback on GnRH is removed.
- Pulsatile secretion of GnRH induce LH and FSH production which finally lead to ovulation.
- In the absence of fertilisation, the ovarian follicle is turned into corpus luteum. Endometrium proliferates through estrogen release from corpus luteum. Withdrawal of progesterone from estrogen-mediated proliferated endometrium results in menstrual bleeding.
Hypothalamic-pituitary-ovarian (HPO) axis maturation
- After activation of the HPO axis during second trimester of pregnancy, the level of gonadotropins rises from mid to term pregnancy. After cessation of placental hormone feedback, FSH and LH increases again slightly to mild secondary peak.
- Before puberty, negative feedback from adrenal androgens keep the gonadotropins in low plasma level.[4]
- Right before puberty, the sensitivity of hypothalamus to negative feedback from adrenal androgens is decreased. This leads to increased production of GnRH from hypothalamus and make it possible for GnRH to be raised in magnitude and frequency to induce an increase in LH and FSH.[5]
- The complete maturation of HPO axis takes around 5-7 years from the onset of menstruation. Generally, during the first two years of menstruation, the cycles are mostly anovulatory due to immature HPO axis.
Pathogenesis
- Amenorrhea is defined as the absence of menstrual cycle.[3]
- Primary amenorrhea is the absence of menstrual cycle by 16 years of age, in the presence of normal growth and secondary sexual characteristics.
- Secondary amenorrhea reflects absence of menstrual cycle for at least 3 months in a woman with normal menstruation cycles in the past.
- The pathophysiology of amenorrhea is multifactorial and include hypothalamic, pituitary, thyroid, adrenal, ovarian, uterine, and vaginal causes.
Hypothalamic pathogenesis
- The most common cause of amenorrhea in adolescents are hypothalamic disorders and is known as hypothalamic amenorrhea.
- During the initial 2-3 years after the onset of menarche, the HPO axis is still under development. Immature HPO axis may lead to anovulatory cycles which can cause abnormalities in menstrual cycles.
- The most common cause of amenorrhea after 2-3 years of onset of puberty include eating disorders, excessive exercise, medications, and psychosocial stress.[6][7]
- Leptin plays an important role in energy consumption, body composition, food intake along with sexual maturation and reproductive improvement.
- It is assumed that leptin plays a role in the development of hypothalamic amenorrhea.
- Leptin receptors are in close relationship with hypothalamus and it is postulated that leptin regulates GnRH production and secretion.
- Patients with anorexia nervosa or excessive exercise have amenorrhea from down-regulation of leptin receptors, which can be elevated by refeeding.[8][9][10]
- Leptin level in cachexic patients will increase after gaining appropriate weight in patients without amenorrhea, but will remain low in patients with amenorrhea.[11][12]
- It has been observed that leptin levels in amenorrheic athletes are low as compared to non-athletes women or athletes with regular menses.[13][14]
- Administration of recombinant leptin for 3 months in women with conditions such as hypothalamic amenorrhea, excessive exercises or weight loss has been associated with an increased level of LH, FSH, and estradiol leading to ovulatory cycles.[15]
- Antipsychotic drugs and other medications that have an inhibitory effect on dopamine D2 receptor lead to an increased level of prolactin. Higher levels of prolactin suppress pulsatile GnRH secretion and block positive feedback of estradiol on hypothalamus, leading to disruption of HPO axis.[16]
- Stress and strenuous activities like other metabolic or cardiovascular responses are regulated through corticotropin releasing hormone (CRH), secreted by paraventricular nuclei of hypothalamus. CRH induce the release of β-endorphin, an endogenous opioid. Both CRH and β-endorphin suppress GnRH release. On the other hand, glucocorticoids suppress LH production from pituitary and also estrogen/progesterone from ovaries.[17]
- Kallmann syndrome, a genetic disorder caused by KAL gene mutation, has disturbance in migration of olfactory nerves along with GnRH neurons. Lack of GnRH leads to absence of secondary sexual characteristics and amenorrhea.[18]
Pituitary pathogenesis
- Prolactinoma is one of the most common anterior pituitary tumors. Prolactinoma leads to increased prolactin secretion and along with the tumor’s mass effect may cause suppression of GnRH.
- The second most common tumor in the suprasellar region is craniopharyngioma. The tumor leads to LH and FSH disturbances, which may cause amenorrhea.[19]
Thyroid pathogenesis
- In hypothyroidism, the main mechanism that can lead to amenorrhea is the influence of thyrotropin releasing hormone (TRH) on lactotroph cells, increasing prolactin levels. Since the TRH is increased in hypothyroidism, it leads to functional hyperprolactinemia. The increase in prolactin may suppress the GnRH pulsatility and lead to amenorrhea.[20]
- In hyperthyroidism, the mechanism of amenorrhea is not clear. It is assumed that increased level of sex hormone binding globulins (SHBGs) in hyperthyroidism may lead to increased levels of androgens and estrogen. Conclusively, the LH surge become absent and amenorrhea happens.[21]
Adrenal pathogenesis
- Congenital adrenal hyperplasia (CAH) is a group of genetic enzyme deficiencies in adrenal gland. Most common is the defect in 21-hydroxylase enzyme, which leads to decrease in the level of aldosterone and cortisol. To overcome the hormone deficiencies, CRH production is increased by the hypothalamus. As described earlier, increased level of CRH may suppress GnRH and lead to amenorrhea.[22]
- Cushing syndrome has an increased level of cortisol, that can directly inhibit HPO axis and lead to amenorrhea.
Ovarian pathogenesis
- In polycystic ovary syndrome (PCOS) insulin resistance leads to increased androgen production (insulin reduces the SHBG circulating in plasma, causing increased testosterone). In ovaries, increased stimulation from GnRH leads to increased production of 17-hydroxy progesterone and cytochrome P450c17 which promotes androgens biosynthesis.[23][24] Finally, the pulsatility of GnRH will be disrupted leading to amenorrhea .[25]
- Primary ovarian insufficiency is multifactorial and leads to ovarian failure and decrease in estrogen which leads to amenorrhea. (In galactosemia, it is assumed that galactose and its metabolites are toxic to ovarian tissue.)[26]
Uterine pathogenesis
- The main pathogenesis of amenorrhea in androgen insensitivity syndrome is the absence of uterus. The patient is genotypically male, 46 XY; but with absent sexual characteristics due to lack of functional effect of androgen hormones on their receptors.
- One of the acquired conditions that can lead to amenorrhea is Asherman syndrome. The basis of Asherman syndrome is any condition that can alter the normal histology of endometrium, such as scarring from surgical procedure or adhesion from severe infection.
- Mayer-Rokitansky-Kuster-Hauser syndrome is complete agenesis of uterine, blind ended vagina. The lack of uterine and endometrium is the main pathogenesis of amenorrhea. The main reason of uterine agenesis is overactivation of anti-mullerian hormone in embryogenesis period.[27] Cervical agenesis also follow the similar process.
- Imperforated hymen, transverse vaginal septum, and vaginal agenesis are other anatomical disorders of female reproductive system that can lead to amenorrhea.[28]
Genetics
The major genes in amenorrhea
| Groups | Gene | Other name(s) | OMIM number | Chromosome | Function | Other related disorders |
|---|---|---|---|---|---|---|
| Kallmann syndrome
and Isolated hypogonadotropic hypogonadism[29] |
KAL1 | KAL1, anosmin-1 | 308700 | Xp22.3 |
|
|
| FGFR1 | KAL2 | 136350 | 8q12 |
|
| |
| PROKR2 | KAL3 | 607123 | 20p13 |
|
||
| PROK2 | KAL4 | 607002 | 3p21.1 | |||
| CHD7 | KAL5 | 608892 | 8q12.1 |
|
| |
| FGF8 | KAL6 | 600483 | 10q24 |
|
| |
| GPR54 | KISS1R | 604161 | 19p13.3 |
|
– | |
| KISS1 | KISS1, kisspeptin1 | 603286 | 1q32 |
|
– | |
| HS6ST1 | – | 604846 | 2q21 |
|
– | |
| TAC3 | NKB | 162330 | 12q13–q21 |
|
||
| TACR3 | NK3R | 152332 | 4q25 | |||
| GnRH1 | – | 152760 | 8p21–8p11.2 |
|
| |
| GnRHR | – | 138850 | 4q21.2 |
|
||
| NELF | – | 608137 | 9q34.3 | – | ||
| EBF2 | – | 609934 | 8p21.2 |
|
– | |
| HPG axis development | DAX1 | NR0B | 300473 | Xp21.2 |
|
|
| SF-1 | NR5A1 | 184757 | 9q33.3 |
|
||
| HESX-1 | RPX | 601802 | 3p14.3 |
|
| |
| LHX3 | LIM3 | 600577 | 9q34.3 |
|
| |
| PROP-1 | – | 601538 | 5q35.3 |
|
| |
| Obesity related
hypogonadotropic hypogonadism |
LEP | OB | 164160 | 7q32.1 |
|
|
| LEPR | OBR | 601007 | 1p31.3 | |||
| PC1 | NEC1 | 162150 | 5q15 |
|
| |
|
Abbreviations (alphabetic): | ||||||
Kisspeptin system (KISS1R and KISS1)
- The GPR54 gene, also called KISS1R, with Online Mendelian Inheritance in Man (OMIM) number of 604161 is on chromosome 19p13.3. The KISS1 gene, also known as kisspeptin1, with OMIM number of 603286 is on chromosome 1q32.
- Kisspeptin and related G-protein coupled receptor (KISS1R or GPR54) have key roles in the regulation of GnRH secretion. The GnRH secretion has to be pulsatile to stimulate gonadotropins. Kisspeptins are encoded by KISS1 gene, neuropeptides secreted from hypothalamus nuclei. It has been observed that patients with idiopathic hypogonadotropic hypogonadism have KISS1 receptor (GPR54) inactivating gene mutations.[30][31]
- By the time of onset of puberty, the KISS1 genes become activated through neuroanatomical and functional changes from environmental triggers, critical for brain sexual maturation and hypothalamic–pituitary–gonadal axis (HPG axis) activation with pulsatile GnRH.[32]
- Along HPG axis neurons, gamma-aminobutyric acid is inhibitory and glutamate is excitatory neurotransmitters. In related KNDy neurons in arcuate nucleus, the materials secreted are included kisspeptin, neurokinin B, and dynorphin A. Before puberty begins, inhibitory dynorphin A is the dominant element; decreased by stimulatory effect of neurokinin B, when puberty started. Conclusively, kisspeptin and GnRH/LH are increased.[33]
Kallmann syndrome 1 (KAL1)
- The KAL1 gene, also called anosmin-1, with OMIM number of 308700 is on chromosome Xp22.3, and encodes an extracellular matrix glycoprotein.
- Anosmin-1 is expressed at five weeks of gestation in forebrain near olfactory bulbs and stimulate the afferent fibers projections around it.[34]
- X-linked Kallmann syndrome is directly associated with KAL1 deletion. It is assumed to result in an absence of olfactory fibers along with disrupted migration of GnRH neurons, that are supposed to from migrated olfactory placode.[35]
- Male patient with KAL1 mutation would have central hypogonadism and anosmia/hyposmia. Additionally, the more diseases are assumed to relate with KAL1 gene, such as midline facial defects (cleft lip and/or cleft palate), short metacarpals, renal agenesis, sensorineural hearing loss, bimanual synkinesis, oculomotor abnormalities, and cerebellar ataxia.[36]
Fibroblast growth factor receptor 1 and fibroblast growth factor 8 (FGFR1 and FGF8)
- The FGFR1 gene, also called KAL2, with OMIM number of 136350 is on chromosome 8q12, encode a receptor tyrosine kinase protein. The FGF8 gene, also called KAL6, is on chromosome 10q24.
- FGFR1 pathway is assumed to be the main role in embryogenesis, homeostasis, and wound healing. FGF8 plays a critical role in the primary generation of neural tissue.[37]
- On the other hand, interaction between FGFR1, FGF8, and heparan sulfate helps the olfactory bulb to become differentiated and developed and also facilitates GnRH neurons in migration and function.[38]
- Dominant deletion mutation of FGFR1 gene is associated with a 30% decrease in hypothalamic GnRH neurons.[39] Other defects related to FGFR1 includes cleft palate or lip, dental agenesis and bimanual synkinesis.[36]
Heparan sulfate 6-O-sulphotransferase 1 (HS6ST1)
- The HS6ST1 gene with OMIM number of 604846 is on chromosome 2q21 has been found to be mutated in hypogonadism.[40]
- The modifications of heparan sulfate polysaccharides in extracellular matrix have some role in FGFR–FGF and also anosmin1–cell membrane interactions.[41][42]
- This gene may be mutated in both Kallmann syndrome and idiopathic hypogonadism resulting in various courses, disruption pf frequency of GnRH secretion, and/or GnRH deficiencies.[40]
Prokineticin 2 and prokineticin 2 receptor (PROK2 and PROKR2)
- The PROK2 and PROKR2 genes, also called KAL4 and KAL3, with OMIM numbers of 607002 and 607123 are on chromosomes 3p21.1 and 20p13, respectively. They are believed to be a cause of Kallmann syndrome.
- PROKR2 is a G protein coupled receptor (GPCR), has a major role in olfactory bulb development; and its mutation may lead to severe gonadal atrophy.[43]
- In prokineticin system, there are two receptors (PROKR1 and PROKR2) and two ligands (PROK1 and PROK2). PROK1 and its receptor (PROKR1) have some role in gastrointestinal system motility. PROK2 and PROKR2 are parts of neuroendocrine system, located in arcuate nucleus, olfactory tract, and suprachiasmatic nucleus.[44]
- The mutated versions of PROK2 and PROKR2 could lead to decrease GnRH production and hypogonadism. Other disorders caused by PROK2 and PROKR2 mutations include fibrous dysplasia, sleep disorder, severe obesity, synkinesis, and epilepsy.[45]
Tachykinin 3 and tachykinin 3 receptor (TAC3 and TACR3)
- The TAC3 and TACR3 genes, also called neurokinin B (NKB) and neurokinin 3 receptor (NK3R), with OMIM numbers of 162330 and 152332, are on chromosomes 12q13–q21 and 4q25, respectively.[46]
- It is postulated that the normal function of TAC3/TACR3 system is necessary for an intact HPG axis and its development during puberty. On the other hand, TAC3/TACR3 system disturbance may cause micropenis and cryptorchidism in males, showing the major role of TAC3/TACR3 in fetal gonadotropins secretion.[47]
- TACR3 encoded protein (NK3R) is GPCR, initially produced in central nervous system. The major mechanism, through which the mutated gene may lead to neuroendocrine disturbance and delayed puberty, is not yet discovered completely.[48]
- TAC3 encoded protein (NKB) is produced in arcuate nucleus of hypothalamus and play an important role in GnRH secretion. Kisspeptin is also produced and secreted in arcuate nucleus, whereas, both of them are inhibited by estrogen. It may be considered that kisspeptin and NKB have identical roles in diverting negative feedback from sex hormones to GnRH. Their mutation has been shown to be related with hypogonadism.
Gonadotropin releasing hormone and its receptor (GnRH1 and GnRHR)
- The GnRH1 and GnRHR genes with OMIM numbers of 152760 and 138850 are on chromosomes 8p21–8p11.2 and 4q21.2, respectively.[49]
- In HPG axis, GnRH is one of the most effective elements; therefore, a defect could directly influence the axis and slow down the progress.
- The GnRHR gene is also responsible for gonadal normal functions and its mutation could lead to hypogonadism and delayed puberty. The mutation in GnRHR has also been associated with conditions such as atrophic gonads along with low LH/FSH and sex hormones, sexual puberty disturbance, inability to conceive, and failure to impact from exogenous GnRH.[50]
- GnRH1 and GnRHR genes have variable expression and cause a spectrum of symptoms, from fertile eunuch syndrome and partial idiopathic hypogonadotropic hypogonadism to complete GnRH resistance (i.e., characterized by cryptorchidism), microphallus, very low LH/FSH, and delayed puberty.[51]
- The other disorders that have been found to be related to GnRH mutation are tooth maturation and biomineralization.[52]
Chromodomain helicase DNA-binding protein 7 (CHD7)
- The CHD7 gene, also called as KAL5, with OMIM number of 608892 is on chromosome 8q12.1.
- CHD7 gene mutation results in autosomal dominant CHARGE syndrome, which is a combination of hypogonadism and Kallmann syndrome, and includes:[53]
- Coloboma
- Heart anomalies
- Choanal Atresia
- Retardation
- Genital anomalies
- Ear anomalies
- Screening for CHD7 gene mutation may be done in patients with hypogonadism or Kallmann syndrome with specific features such as semicircular canal hypoplasia or aplasia, dysmorphic ears, and deafness.
Nasal embryonic LH-releasing hormone factor (NELF)
- The NELF gene with OMIM number of 608137 is on chromosome 9q34.3; present mostly in nervous tissues specifically during fetal development and may be found in olfactory bulb and pituitary LH releasing cells.
- The most common function is in olfactory axons and GnRH neurons, before and during neuron migration in the developmental process.[54]
Early B-cell factor 2 (EBF2)
- The EBF2 gene with OMIM number of 609934 is on chromosome 8p21.2; mostly expressed in mice osteoblasts and osteoclast cells.[55]
- EBF2 gene plays an effective role in HPG axis. Mutation in EBF2 gene can result in disruption of HPG axis, leading to secondary hypogonadism.[56]
DSS-AHC on the X-chromosome 1 (DAX1)
- The DAX1 gene, also called nuclear receptor 0B (NR0B), with OMIM number of 300473 is on chromosome Xp21.2, and expressed in all members of HPG axis (hypothalamus, pituitary, and gonads).[57]
- During the spermatogenesis and steroidogenesis, both sertoli and leydig cells have increased expression of DAX1 gene. It is assumed that during puberty, the peak expression of DAX1 is observed.[58]
- Other disease that can be caused by DAX1 mutation is congenital adrenal cortex hypoplasia.[59]
Steroidogenic factor 1 (SF1)
- The SF1 gene, also called nuclear receptor 5A1 (NR5A1), with OMIM number of 184757 is on chromosome 9q33.3, has some role in reproduction, steroidogenesis, and sexual differentiation.
- It is mainly expressed in sertoli and leydig cells, and plays an important role in steroidogenesis and spermatogenesis. The SF1 is believed to have an increase in expression from childhood until adolescence, and is dominantly expressed by leydig cells in puberty.[58]
- Other diseases that may be caused by SF1 mutation include male pseudohermaphroditism, Denys-Drash syndrome, and also hypospadias.[60]
Homeobox gene 1 (HESX1)
- The HESX1 gene, also called Rathke pouch homeobox (RPX), with OMIM number of 601802 is on chromosome 3p14.3, initially expressed during embryogenesis and help the formation of Rathke pouch and anterior pituitary.[61]
- HESX1 gene has an important role in pituitary development and midfacial differentiation. Mutation may lead to pituitary hypoplasia and decreased level of all anterior pituitary hormones.[62]
- Other disorders resulting from HESX1 mutation include septo optic dysplasia, reduced prosencephalon, anophthalmia, microphthalmia, defective olfactory development, Rathke pouch bifurcations, and abnormalities in the corpus callosum, hippocampus, and septum pellucidum.[61]
LIM homeobox gene 3 (LHX3)
- The LHX3 gene, also called LIM3, with OMIM number of 600577 is on chromosome 9q34.3, mainly expressed in developing anterior pituitary gland.[63]
- LHX3 gene function is important in development of pituitary gland and pituitary hormones secretion. Mutation in the LHX3 gene may result in combined pituitary hormone deficiency (CPHD).[64]
- LHX3 gene mutation may also result in neonatal hypoglycemia, short neck with limited rotation, mild sensorineural hearing loss, skin laxity, and skeletal abnormalities.[63]
PROP paired-like homeobox 1 (PROP1)
- The PROP1 gene with OMIM number of 601538 is on chromosome 5q35.3, with a role in developing anterior pituitary gland and associated cells such as gonadotrophs, thyrotrophs, somatotrophs, and lactotrophs.[65]
- Mutated PROP1 gene can lead to deficiency of LH, FSH, GH, TSH, and prolactin. Decreased level of LH and FSH may also delay or inhibit the onset of puberty.[66]
- Pituitary hormones have a vital role in regulating other endocrine organs via TRH, ACTH, FSH or LH and a mutation in PROP1 gene can lead to thyroid dysfunctions, growth retardation, and libido/lactation problems.
Leptin and leptin receptor (LEP and LEPR)
- The LEP and LEPR genes, also called OB and OBR, with OMIM numbers of 164160 and 601007 are on chromosomes 7q32.1 and 1p31.3, respectively; with a major role in modulation of body weight.
- These genes are believed to carry the message of onset of puberty. Recent studies have shown that recombinant leptin injection in female mice may result in puberty and cure their maturation (secondary sexual characteristics) problems.[67]
- It has been observed that leptin levels increase by 50% just before the onset of puberty and during puberty.[68]
- Mutation in LEP and LEPR genes may result in dysfunctional hematopoiesis, angiogenesis, wound healing, and the immune or inflammatory response.
Proprotein convertase 1 (PC1)
- The PC1 gene, also known as neuroendocrine convertase 1 (NEC1), with OMIM number of 162150 is on chromosome 5q15, and regulates neuroendocrine pathway.
- PC1 gene has a dominant role in proopiomelanocortin (POMC) cleavage. PC1 gene also has a role in processing proinsulin and proglucagon in pancreas.[69]
- Recent studies have shown that PC1 gene mutation and hypogonadotropic hypogonadism may result in extreme childhood obesity, abnormal glucose homeostasis, hypocortisolism, elevated plasma proinsulin, and POMC concentrations.[70]
Makorin RING-finger protein 3 (MKRN3)
- Newly discovered MKRN3 gene has a role in ubiquitination and cell signaling. The gene family proteins are majorly expressed in fetal brain during development, especially in arcuate nucleus.
- The process of gene amplification is on its peak after birth, which gradually declines with time, and finally rises again with onset of puberty. Thus MKRN3 gene is believed to be one of the factors in onset of puberty, along with kisspeptins and neurokinin B.[71]
Estrogen receptor α (ESR1)
- Estrogen receptor mutations are very rare, and were reported in a case report of delayed puberty.[72]
- Estradiol promotes breast maturation and provides negative feedback to hypothalamus and pituitary, by means of estrogen receptor α (encoded by ESR1 gene).[73]
- Female mice with mutated ESR1 gene have hypoplastic uterus with hemorrhage, multicystic ovary without corpus luteum; which is make them infertile.[74]
Associated Conditions
The associated conditions that are related to amenorrhea, are as following:[75]
Gross Pathology

- On gross pathology, normal endometrium in proliferative or luteal phases are characteristic findings of amenorrhea.
- In cases of amenorrhea which are secondary to other causes, the related gross pathology would be seen.
- Craniopharyngioma on gross pathology presents as cystic mass filled with motor oil-like fluid.[76]
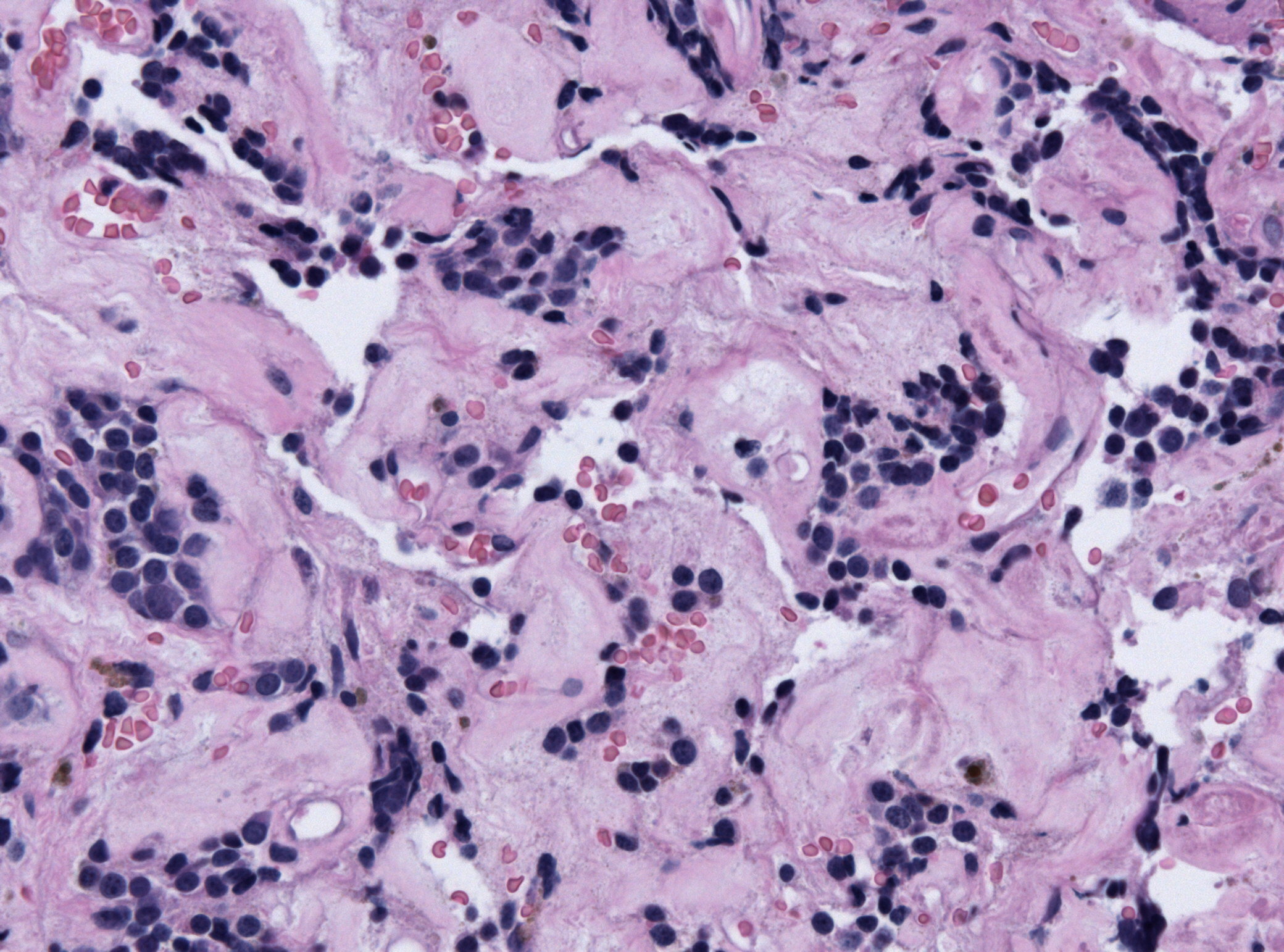
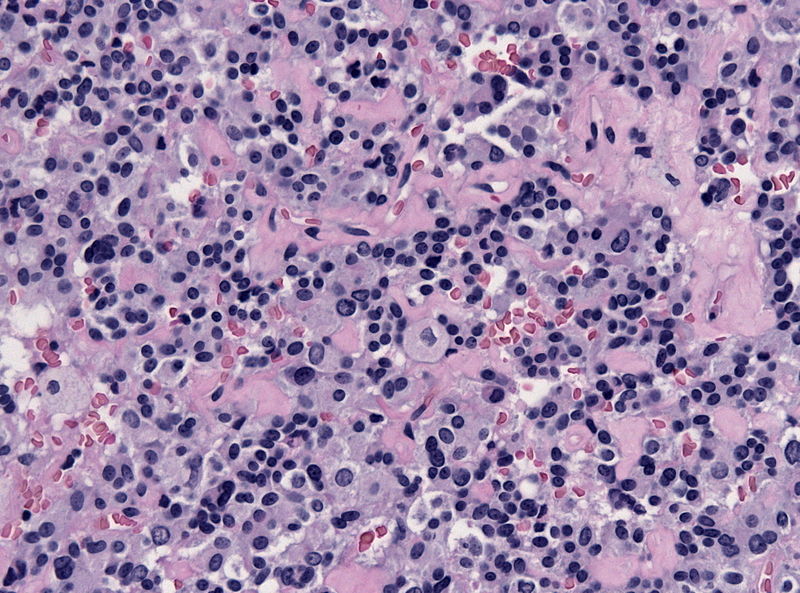
Microscopic Pathology
- On microscopic histopathological analysis, craniopharyngioma as a cause of amenorrhea will have the following features:
- Trabecular squamous epithelium surrounded by palisaded columnar epithelium
- Small-to-medium sized cells with moderate amount of basophilic cytoplasm
- Bland nuclei
- Calcifications
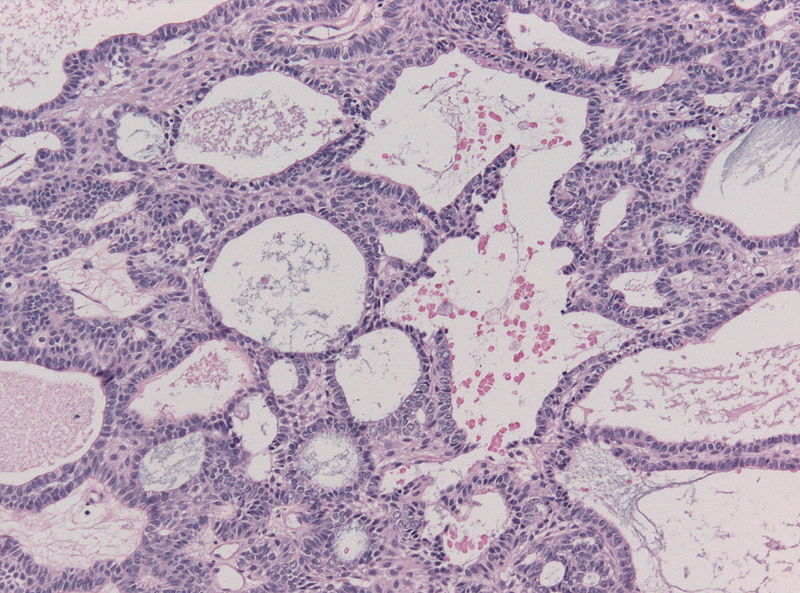
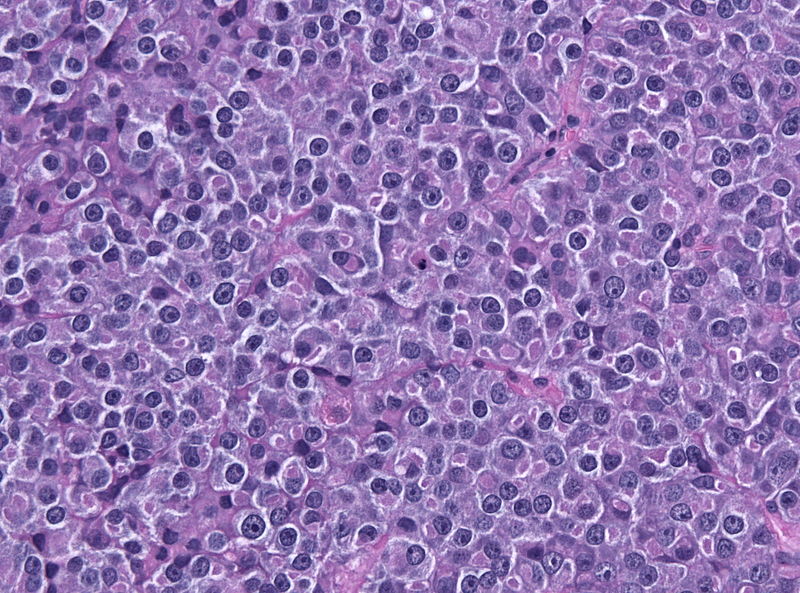
- On microscopic histopathological analysis, pituitary adenoma as a cause of amenorrhea will have the following features:
- Loss of fibrous stroma
- Nested cells of normal anterior pituitary (based on the type of adenoma)
-
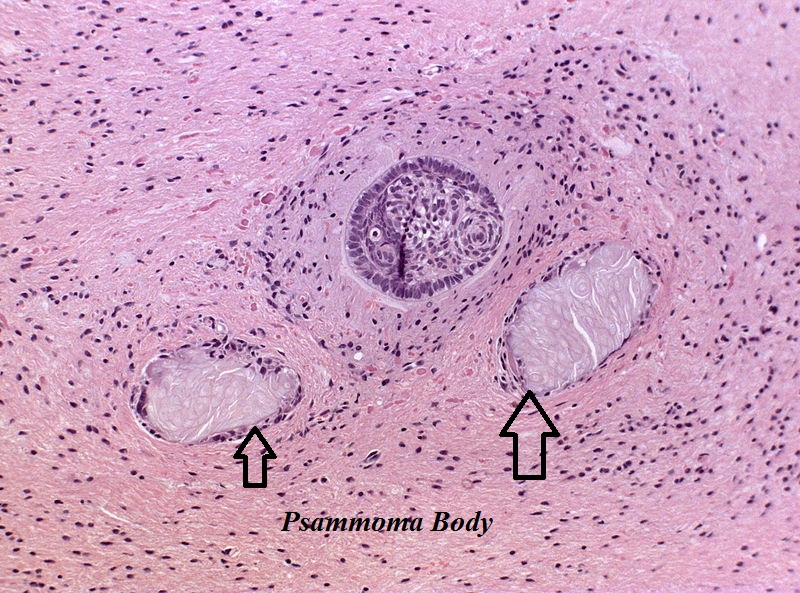 Craniopharyngioma; with psammoma bodies – by Jensflorian source: Librepathology
Craniopharyngioma; with psammoma bodies – by Jensflorian source: Librepathology -
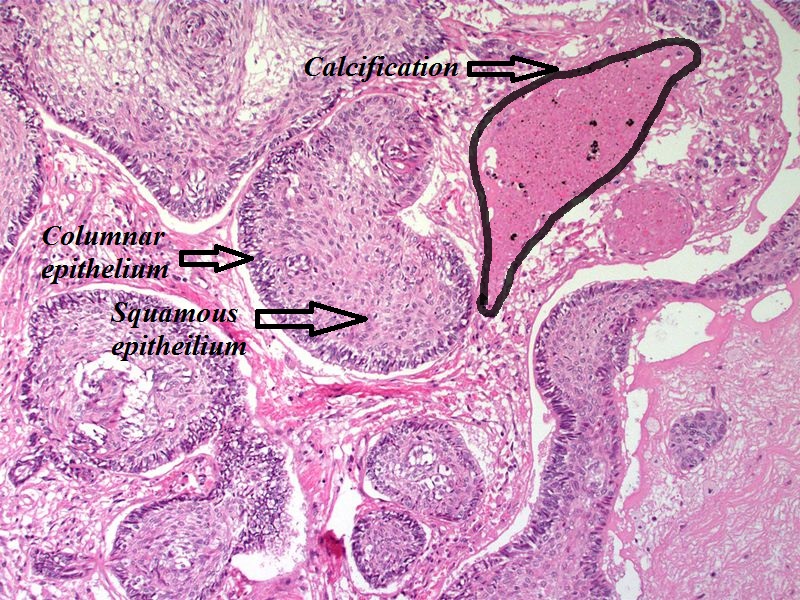 Craniopharyngioma; with calcification and two types of epithelium – by Sarahkayb source: Librepathology
Craniopharyngioma; with calcification and two types of epithelium – by Sarahkayb source: Librepathology -
 Craniopharyngioma; multicystic texture – by Jensflorian source: Librepathology
Craniopharyngioma; multicystic texture – by Jensflorian source: Librepathology -
 Pituitary adenoma of lactotroph cells (prolactin producing) – by Jensflorian source: Librepathology
Pituitary adenoma of lactotroph cells (prolactin producing) – by Jensflorian source: Librepathology -
 Pituitary adenoma of lactotroph cells (prolactin producing) regression after treatment – by Jensflorian source: Librepathology
Pituitary adenoma of lactotroph cells (prolactin producing) regression after treatment – by Jensflorian source: Librepathology -
 Pituitary adenoma of thyrotroph cells (TSH producing) – by Jensflorian source: Librepathology
Pituitary adenoma of thyrotroph cells (TSH producing) – by Jensflorian source: Librepathology






References
- ↑ Chumlea WC, Schubert CM, Roche AF, Kulin HE, Lee PA, Himes JH, Sun SS (2003). “Age at menarche and racial comparisons in US girls”. Pediatrics. 111 (1): 110–3. PMID 12509562.
- ↑ “Menstruation in Girls and Adolescents: Using the Menstrual Cycle as a Vital Sign – ACOG”.
- ↑ 3.0 3.1 Golden NH, Carlson JL (2008). “The pathophysiology of amenorrhea in the adolescent”. Ann. N. Y. Acad. Sci. 1135: 163–78. doi:10.1196/annals.1429.014. PMID 18574222.
- ↑ Apter D (1997). “Development of the hypothalamic-pituitary-ovarian axis”. Ann. N. Y. Acad. Sci. 816: 9–21. PMID 9238251.
- ↑ Boyar RM, Rosenfeld RS, Kapen S, Finkelstein JW, Roffwarg HP, Weitzman ED, Hellman L (1974). “Human puberty. Simultaneous augmented secretion of luteinizing hormone and testosterone during sleep”. J. Clin. Invest. 54 (3): 609–18. doi:10.1172/JCI107798. PMC 301594. PMID 4852310.
- ↑ Wiksten-Almströmer M, Hirschberg AL, Hagenfeldt K (2007). “Menstrual disorders and associated factors among adolescent girls visiting a youth clinic”. Acta Obstet Gynecol Scand. 86 (1): 65–72. doi:10.1080/00016340601034970. PMID 17230292.
- ↑ Perkins RB, Hall JE, Martin KA (2001). “Aetiology, previous menstrual function and patterns of neuro-endocrine disturbance as prognostic indicators in hypothalamic amenorrhoea”. Hum. Reprod. 16 (10): 2198–205. PMID 11574516.
- ↑ Hebebrand J, Muller TD, Holtkamp K, Herpertz-Dahlmann B (2007). “The role of leptin in anorexia nervosa: clinical implications”. Mol. Psychiatry. 12 (1): 23–35. doi:10.1038/sj.mp.4001909. PMID 17060920.
- ↑ Grinspoon S, Gulick T, Askari H, Landt M, Lee K, Anderson E, Ma Z, Vignati L, Bowsher R, Herzog D, Klibanski A (1996). “Serum leptin levels in women with anorexia nervosa”. J. Clin. Endocrinol. Metab. 81 (11): 3861–3. doi:10.1210/jcem.81.11.8923829. PMID 8923829.
- ↑ Haas V, Onur S, Paul T, Nutzinger DO, Bosy-Westphal A, Hauer M, Brabant G, Klein H, Müller MJ (2005). “Leptin and body weight regulation in patients with anorexia nervosa before and during weight recovery”. Am. J. Clin. Nutr. 81 (4): 889–96. PMID 15817868.
- ↑ Misra M, Miller KK, Almazan C, Ramaswamy K, Aggarwal A, Herzog DB, Neubauer G, Breu J, Klibanski A (2004). “Hormonal and body composition predictors of soluble leptin receptor, leptin, and free leptin index in adolescent girls with anorexia nervosa and controls and relation to insulin sensitivity”. J. Clin. Endocrinol. Metab. 89 (7): 3486–95. doi:10.1210/jc.2003-032251. PMID 15240636.
- ↑ Katzman DK, Golden NH, Neumark-Sztainer D, Yager J, Strober M (2000). “From prevention to prognosis: clinical research update on adolescent eating disorders”. Pediatr. Res. 47 (6): 709–12. PMID 10832726.
- ↑ Thong FS, McLean C, Graham TE (2000). “Plasma leptin in female athletes: relationship with body fat, reproductive, nutritional, and endocrine factors”. J. Appl. Physiol. 88 (6): 2037–44. PMID 10846016.
- ↑ Weimann E, Blum WF, Witzel C, Schwidergall S, Böhles HJ (1999). “Hypoleptinemia in female and male elite gymnasts”. Eur. J. Clin. Invest. 29 (10): 853–60. PMID 10583427.
- ↑ Welt, Corrine K.; Chan, Jean L.; Bullen, John; Murphy, Robyn; Smith, Patricia; DePaoli, Alex M.; Karalis, Aspasia; Mantzoros, Christos S. (2004). “Recombinant Human Leptin in Women with Hypothalamic Amenorrhea”. New England Journal of Medicine. 351 (10): 987–997. doi:10.1056/NEJMoa040388. ISSN 0028-4793.
- ↑ Wieck A, Haddad PM (2003). “Antipsychotic-induced hyperprolactinaemia in women: pathophysiology, severity and consequences. Selective literature review”. Br J Psychiatry. 182: 199–204. PMID 12611781.
- ↑ Magiakou MA, Mastorakos G, Webster E, Chrousos GP (1997). “The hypothalamic-pituitary-adrenal axis and the female reproductive system”. Ann. N. Y. Acad. Sci. 816: 42–56. PMID 9238254.
- ↑ Seminara SB, Hayes FJ, Crowley WF (1998). “Gonadotropin-releasing hormone deficiency in the human (idiopathic hypogonadotropic hypogonadism and Kallmann’s syndrome): pathophysiological and genetic considerations”. Endocr. Rev. 19 (5): 521–39. doi:10.1210/edrv.19.5.0344. PMID 9793755.
- ↑ Karavitaki N, Cudlip S, Adams CB, Wass JA (2006). “Craniopharyngiomas”. Endocr. Rev. 27 (4): 371–97. doi:10.1210/er.2006-0002. PMID 16543382.
- ↑ Koutras DA (1997). “Disturbances of menstruation in thyroid disease”. Ann. N. Y. Acad. Sci. 816: 280–4. PMID 9238278.
- ↑ Poppe K, Velkeniers B, Glinoer D (2007). “Thyroid disease and female reproduction”. Clin. Endocrinol. (Oxf). 66 (3): 309–21. doi:10.1111/j.1365-2265.2007.02752.x. PMID 17302862.
- ↑ Speiser, Phyllis W.; White, Perrin C. (2003). “Congenital Adrenal Hyperplasia”. New England Journal of Medicine. 349 (8): 776–788. doi:10.1056/NEJMra021561. ISSN 0028-4793.
- ↑ Gilling-Smith C, Story H, Rogers V, Franks S (1997). “Evidence for a primary abnormality of thecal cell steroidogenesis in the polycystic ovary syndrome”. Clin. Endocrinol. (Oxf). 47 (1): 93–9. PMID 9302378.
- ↑ Ehrmann DA, Barnes RB, Rosenfield RL (1995). “Polycystic ovary syndrome as a form of functional ovarian hyperandrogenism due to dysregulation of androgen secretion”. Endocr. Rev. 16 (3): 322–53. doi:10.1210/edrv-16-3-322. PMID 7671850.
- ↑ Pastor CL, Griffin-Korf ML, Aloi JA, Evans WS, Marshall JC (1998). “Polycystic ovary syndrome: evidence for reduced sensitivity of the gonadotropin-releasing hormone pulse generator to inhibition by estradiol and progesterone”. J. Clin. Endocrinol. Metab. 83 (2): 582–90. doi:10.1210/jcem.83.2.4604. PMID 9467578.
- ↑ Kaufman FR, Kogut MD, Donnell GN, Goebelsmann U, March C, Koch R (1981). “Hypergonadotropic hypogonadism in female patients with galactosemia”. N. Engl. J. Med. 304 (17): 994–8. doi:10.1056/NEJM198104233041702. PMID 6782485.
- ↑ Varner RE, Younger JB, Blackwell RE (1985). “Müllerian dysgenesis”. J Reprod Med. 30 (6): 443–50. PMID 4020785.
- ↑ Edmonds DK (2003). “Congenital malformations of the genital tract and their management”. Best Pract Res Clin Obstet Gynaecol. 17 (1): 19–40. PMID 12758224.
- ↑ Bonomi, Marco; Libri, Domenico Vladimiro; Guizzardi, Fabiana; Guarducci, Elena; Maiolo, Elisabetta; Pignatti, Elisa; Asci, Roberta; Persani, Luca (2011). “New understandings of the genetic basis of isolated idiopathic central hypogonadism”. Asian Journal of Andrology. 14 (1): 49–56. doi:10.1038/aja.2011.68. ISSN 1008-682X.
- ↑ de Roux N, Genin E, Carel JC, Matsuda F, Chaussain JL, Milgrom E (2003). “Hypogonadotropic hypogonadism due to loss of function of the KiSS1-derived peptide receptor GPR54”. Proc. Natl. Acad. Sci. U.S.A. 100 (19): 10972–6. doi:10.1073/pnas.1834399100. PMC 196911. PMID 12944565.
- ↑ Seminara, Stephanie B.; Messager, Sophie; Chatzidaki, Emmanouella E.; Thresher, Rosemary R.; Acierno, James S.; Shagoury, Jenna K.; Bo-Abbas, Yousef; Kuohung, Wendy; Schwinof, Kristine M.; Hendrick, Alan G.; Zahn, Dirk; Dixon, John; Kaiser, Ursula B.; Slaugenhaupt, Susan A.; Gusella, James F.; O’Rahilly, Stephen; Carlton, Mark B.L.; Crowley, William F.; Aparicio, Samuel A.J.R.; Colledge, William H. (2003). “TheGPR54Gene as a Regulator of Puberty”. New England Journal of Medicine. 349 (17): 1614–1627. doi:10.1056/NEJMoa035322. ISSN 0028-4793.
- ↑ Kaur KK, Allahbadia G, Singh M (2012). “Kisspeptins in human reproduction-future therapeutic potential”. J Assist Reprod Genet. 29 (10): 999–1011. doi:10.1007/s10815-012-9856-1. PMC 3492584. PMID 23015158.
- ↑ Uenoyama, Yoshihisa; Tsukamura, Hiroko; Maeda, Kei-ichiro (2014). “KNDy neuron as a gatekeeper of puberty onset”. Journal of Obstetrics and Gynaecology Research. 40 (6): 1518–1526. doi:10.1111/jog.12398. ISSN 1341-8076.
- ↑ Hardelin JP, Julliard AK, Moniot B, Soussi-Yanicostas N, Verney C, Schwanzel-Fukuda M, Ayer-Le Lievre C, Petit C (1999). “Anosmin-1 is a regionally restricted component of basement membranes and interstitial matrices during organogenesis: implications for the developmental anomalies of X chromosome-linked Kallmann syndrome”. Dev. Dyn. 215 (1): 26–44. doi:10.1002/(SICI)1097-0177(199905)215:1<26::AID-DVDY4>3.0.CO;2-D. PMID 10340754.
- ↑ Schwanzel-Fukuda M, Bick D, Pfaff DW (1989). “Luteinizing hormone-releasing hormone (LHRH)-expressing cells do not migrate normally in an inherited hypogonadal (Kallmann) syndrome”. Brain Res. Mol. Brain Res. 6 (4): 311–26. PMID 2687610.
- ↑ 36.0 36.1 Trarbach EB, Silveira LG, Latronico AC (2007). “Genetic insights into human isolated gonadotropin deficiency”. Pituitary. 10 (4): 381–91. doi:10.1007/s11102-007-0061-7. PMID 17624596.
- ↑ González-Martínez D, Kim SH, Hu Y, Guimond S, Schofield J, Winyard P, Vannelli GB, Turnbull J, Bouloux PM (2004). “Anosmin-1 modulates fibroblast growth factor receptor 1 signaling in human gonadotropin-releasing hormone olfactory neuroblasts through a heparan sulfate-dependent mechanism”. J. Neurosci. 24 (46): 10384–92. doi:10.1523/JNEUROSCI.3400-04.2004. PMID 15548653.
- ↑ Hébert JM, Lin M, Partanen J, Rossant J, McConnell SK (2003). “FGF signaling through FGFR1 is required for olfactory bulb morphogenesis”. Development. 130 (6): 1101–11. PMID 12571102.
- ↑ Tsai PS, Moenter SM, Postigo HR, El Majdoubi M, Pak TR, Gill JC, Paruthiyil S, Werner S, Weiner RI (2005). “Targeted expression of a dominant-negative fibroblast growth factor (FGF) receptor in gonadotropin-releasing hormone (GnRH) neurons reduces FGF responsiveness and the size of GnRH neuronal population”. Mol. Endocrinol. 19 (1): 225–36. doi:10.1210/me.2004-0330. PMID 15459253.
- ↑ 40.0 40.1 Tornberg J, Sykiotis GP, Keefe K, Plummer L, Hoang X, Hall JE, Quinton R, Seminara SB, Hughes V, Van Vliet G, Van Uum S, Crowley WF, Habuchi H, Kimata K, Pitteloud N, Bülow HE (2011). “Heparan sulfate 6-O-sulfotransferase 1, a gene involved in extracellular sugar modifications, is mutated in patients with idiopathic hypogonadotrophic hypogonadism”. Proc. Natl. Acad. Sci. U.S.A. 108 (28): 11524–9. doi:10.1073/pnas.1102284108. PMC 3136273. PMID 21700882.
- ↑ Ibrahimi OA, Zhang F, Hrstka SC, Mohammadi M, Linhardt RJ (2004). “Kinetic model for FGF, FGFR, and proteoglycan signal transduction complex assembly”. Biochemistry. 43 (16): 4724–30. doi:10.1021/bi0352320. PMID 15096041.
- ↑ Hudson ML, Kinnunen T, Cinar HN, Chisholm AD (2006). “C. elegans Kallmann syndrome protein KAL-1 interacts with syndecan and glypican to regulate neuronal cell migrations”. Dev. Biol. 294 (2): 352–65. doi:10.1016/j.ydbio.2006.02.036. PMID 16677626.
- ↑ Matsumoto S, Yamazaki C, Masumoto KH, Nagano M, Naito M, Soga T, Hiyama H, Matsumoto M, Takasaki J, Kamohara M, Matsuo A, Ishii H, Kobori M, Katoh M, Matsushime H, Furuichi K, Shigeyoshi Y (2006). “Abnormal development of the olfactory bulb and reproductive system in mice lacking prokineticin receptor PKR2”. Proc. Natl. Acad. Sci. U.S.A. 103 (11): 4140–5. doi:10.1073/pnas.0508881103. PMC 1449660. PMID 16537498.
- ↑ Li M, Bullock CM, Knauer DJ, Ehlert FJ, Zhou QY (2001). “Identification of two prokineticin cDNAs: recombinant proteins potently contract gastrointestinal smooth muscle”. Mol. Pharmacol. 59 (4): 692–8. PMID 11259612.
- ↑ Cole LW, Sidis Y, Zhang C, Quinton R, Plummer L, Pignatelli D, Hughes VA, Dwyer AA, Raivio T, Hayes FJ, Seminara SB, Huot C, Alos N, Speiser P, Takeshita A, Van Vliet G, Pearce S, Crowley WF, Zhou QY, Pitteloud N (2008). “Mutations in prokineticin 2 and prokineticin receptor 2 genes in human gonadotrophin-releasing hormone deficiency: molecular genetics and clinical spectrum”. J. Clin. Endocrinol. Metab. 93 (9): 3551–9. doi:10.1210/jc.2007-2654. PMC 2567850. PMID 18559922.
- ↑ Topaloglu AK, Reimann F, Guclu M, Yalin AS, Kotan LD, Porter KM, Serin A, Mungan NO, Cook JR, Imamoglu S, Akalin NS, Yuksel B, O’Rahilly S, Semple RK (2009). “TAC3 and TACR3 mutations in familial hypogonadotropic hypogonadism reveal a key role for Neurokinin B in the central control of reproduction”. Nat. Genet. 41 (3): 354–358. doi:10.1038/ng.306. PMC 4312696. PMID 19079066.
- ↑ Pinto FM, Almeida TA, Hernandez M, Devillier P, Advenier C, Candenas ML (2004). “mRNA expression of tachykinins and tachykinin receptors in different human tissues”. Eur. J. Pharmacol. 494 (2–3): 233–9. doi:10.1016/j.ejphar.2004.05.016. PMID 15212980.
- ↑ Semple RK, Topaloglu AK (2010). “The recent genetics of hypogonadotrophic hypogonadism – novel insights and new questions”. Clin. Endocrinol. (Oxf). 72 (4): 427–35. doi:10.1111/j.1365-2265.2009.03687.x. PMID 19719764.
- ↑ Bouligand J, Ghervan C, Tello JA, Brailly-Tabard S, Salenave S, Chanson P, Lombès M, Millar RP, Guiochon-Mantel A, Young J (2009). “Isolated familial hypogonadotropic hypogonadism and a GNRH1 mutation”. N. Engl. J. Med. 360 (26): 2742–8. doi:10.1056/NEJMoa0900136. PMID 19535795.
- ↑ Wu S, Wilson MD, Busby ER, Isaac ER, Sherwood NM (2010). “Disruption of the single copy gonadotropin-releasing hormone receptor in mice by gene trap: severe reduction of reproductive organs and functions in developing and adult mice”. Endocrinology. 151 (3): 1142–52. doi:10.1210/en.2009-0598. PMID 20068010.
- ↑ Silveira LF, MacColl GS, Bouloux PM (2002). “Hypogonadotropic hypogonadism”. Semin. Reprod. Med. 20 (4): 327–38. doi:10.1055/s-2002-36707. PMID 12536356.
- ↑ Tiong J, Locastro T, Wray S (2007). “Gonadotropin-releasing hormone-1 (GnRH-1) is involved in tooth maturation and biomineralization”. Dev. Dyn. 236 (11): 2980–92. doi:10.1002/dvdy.21332. PMID 17948256.
- ↑ Kim HG, Kurth I, Lan F, Meliciani I, Wenzel W, Eom SH, Kang GB, Rosenberger G, Tekin M, Ozata M, Bick DP, Sherins RJ, Walker SL, Shi Y, Gusella JF, Layman LC (2008). “Mutations in CHD7, encoding a chromatin-remodeling protein, cause idiopathic hypogonadotropic hypogonadism and Kallmann syndrome”. Am. J. Hum. Genet. 83 (4): 511–9. doi:10.1016/j.ajhg.2008.09.005. PMC 2561938. PMID 18834967.
- ↑ Kramer PR, Wray S (2000). “Novel gene expressed in nasal region influences outgrowth of olfactory axons and migration of luteinizing hormone-releasing hormone (LHRH) neurons”. Genes Dev. 14 (14): 1824–34. PMC 316793. PMID 10898796.
- ↑ Corradi A, Croci L, Broccoli V, Zecchini S, Previtali S, Wurst W, Amadio S, Maggi R, Quattrini A, Consalez GG (2003). “Hypogonadotropic hypogonadism and peripheral neuropathy in Ebf2-null mice”. Development. 130 (2): 401–10. PMID 12466206.
- ↑ Trarbach EB, Baptista MT, Garmes HM, Hackel C (2005). “Molecular analysis of KAL-1, GnRH-R, NELF and EBF2 genes in a series of Kallmann syndrome and normosmic hypogonadotropic hypogonadism patients”. J. Endocrinol. 187 (3): 361–8. doi:10.1677/joe.1.06103. PMID 16423815.
- ↑ Guo W, Burris TP, McCabe ER (1995). “Expression of DAX-1, the gene responsible for X-linked adrenal hypoplasia congenita and hypogonadotropic hypogonadism, in the hypothalamic-pituitary-adrenal/gonadal axis”. Biochem. Mol. Med. 56 (1): 8–13. PMID 8593542.
- ↑ 58.0 58.1 Kojima Y, Sasaki S, Hayashi Y, Umemoto Y, Morohashi K, Kohri K (2006). “Role of transcription factors Ad4bp/SF-1 and DAX-1 in steroidogenesis and spermatogenesis in human testicular development and idiopathic azoospermia”. Int. J. Urol. 13 (6): 785–93. doi:10.1111/j.1442-2042.2006.01403.x. PMID 16834661.
- ↑ Zanaria E, Muscatelli F, Bardoni B, Strom TM, Guioli S, Guo W, Lalli E, Moser C, Walker AP, McCabe ER (1994). “An unusual member of the nuclear hormone receptor superfamily responsible for X-linked adrenal hypoplasia congenita”. Nature. 372 (6507): 635–41. doi:10.1038/372635a0. PMID 7990953.
- ↑ Nachtigal MW, Hirokawa Y, Enyeart-VanHouten DL, Flanagan JN, Hammer GD, Ingraham HA (1998). “Wilms’ tumor 1 and Dax-1 modulate the orphan nuclear receptor SF-1 in sex-specific gene expression”. Cell. 93 (3): 445–54. PMID 9590178.
- ↑ 61.0 61.1 Dattani MT, Martinez-Barbera JP, Thomas PQ, Brickman JM, Gupta R, Mårtensson IL, Toresson H, Fox M, Wales JK, Hindmarsh PC, Krauss S, Beddington RS, Robinson IC (1998). “Mutations in the homeobox gene HESX1/Hesx1 associated with septo-optic dysplasia in human and mouse”. Nat. Genet. 19 (2): 125–33. doi:10.1038/477. PMID 9620767.
- ↑ Thomas PQ, Dattani MT, Brickman JM, McNay D, Warne G, Zacharin M, Cameron F, Hurst J, Woods K, Dunger D, Stanhope R, Forrest S, Robinson IC, Beddington RS (2001). “Heterozygous HESX1 mutations associated with isolated congenital pituitary hypoplasia and septo-optic dysplasia”. Hum. Mol. Genet. 10 (1): 39–45. PMID 11136712.
- ↑ 63.0 63.1 Rajab A, Kelberman D, de Castro SC, Biebermann H, Shaikh H, Pearce K, Hall CM, Shaikh G, Gerrelli D, Grueters A, Krude H, Dattani MT (2008). “Novel mutations in LHX3 are associated with hypopituitarism and sensorineural hearing loss”. Hum. Mol. Genet. 17 (14): 2150–9. doi:10.1093/hmg/ddn114. PMID 18407919.
- ↑ Netchine I, Sobrier ML, Krude H, Schnabel D, Maghnie M, Marcos E, Duriez B, Cacheux V, Moers A, Goossens M, Grüters A, Amselem S (2000). “Mutations in LHX3 result in a new syndrome revealed by combined pituitary hormone deficiency”. Nat. Genet. 25 (2): 182–6. doi:10.1038/76041. PMID 10835633. Vancouver style error: initials (help)
- ↑ Duquesnoy P, Roy A, Dastot F, Ghali I, Teinturier C, Netchine I, Cacheux V, Hafez M, Salah N, Chaussain JL, Goossens M, Bougnères P, Amselem S (1998). “Human Prop-1: cloning, mapping, genomic structure. Mutations in familial combined pituitary hormone deficiency”. FEBS Lett. 437 (3): 216–20. PMID 9824293.
- ↑ Wu W, Cogan JD, Pfäffle RW, Dasen JS, Frisch H, O’Connell SM, Flynn SE, Brown MR, Mullis PE, Parks JS, Phillips JA, Rosenfeld MG (1998). “Mutations in PROP1 cause familial combined pituitary hormone deficiency”. Nat. Genet. 18 (2): 147–9. doi:10.1038/ng0298-147. PMID 9462743.
- ↑ Chehab FF, Lim ME, Lu R (1996). “Correction of the sterility defect in homozygous obese female mice by treatment with the human recombinant leptin”. Nat. Genet. 12 (3): 318–20. doi:10.1038/ng0396-318. PMID 8589726.
- ↑ Mantzoros CS, Flier JS, Rogol AD (1997). “A longitudinal assessment of hormonal and physical alterations during normal puberty in boys. V. Rising leptin levels may signal the onset of puberty”. J. Clin. Endocrinol. Metab. 82 (4): 1066–70. doi:10.1210/jcem.82.4.3878. PMID 9100574.
- ↑ Jansen E, Ayoubi TA, Meulemans SM, Van de Ven WJ (1995). “Neuroendocrine-specific expression of the human prohormone convertase 1 gene. Hormonal regulation of transcription through distinct cAMP response elements”. J. Biol. Chem. 270 (25): 15391–7. PMID 7797529.
- ↑ Jackson RS, Creemers JW, Ohagi S, Raffin-Sanson ML, Sanders L, Montague CT, Hutton JC, O’Rahilly S (1997). “Obesity and impaired prohormone processing associated with mutations in the human prohormone convertase 1 gene”. Nat. Genet. 16 (3): 303–6. doi:10.1038/ng0797-303. PMID 9207799.
- ↑ Hughes, Ieuan A. (2013). “Releasing the Brake on Puberty”. New England Journal of Medicine. 368 (26): 2513–2515. doi:10.1056/NEJMe1306743. ISSN 0028-4793.
- ↑ Quaynor, Samuel D.; Stradtman, Earl W.; Kim, Hyung-Goo; Shen, Yiping; Chorich, Lynn P.; Schreihofer, Derek A.; Layman, Lawrence C. (2013). “Delayed Puberty and Estrogen Resistance in a Woman with Estrogen Receptor α Variant”. New England Journal of Medicine. 369 (2): 164–171. doi:10.1056/NEJMoa1303611. ISSN 0028-4793.
- ↑ Christian CA, Glidewell-Kenney C, Jameson JL, Moenter SM (2008). “Classical estrogen receptor alpha signaling mediates negative and positive feedback on gonadotropin-releasing hormone neuron firing”. Endocrinology. 149 (11): 5328–34. doi:10.1210/en.2008-0520. PMC 2584581. PMID 18635656.
- ↑ Lubahn DB, Moyer JS, Golding TS, Couse JF, Korach KS, Smithies O (1993). “Alteration of reproductive function but not prenatal sexual development after insertional disruption of the mouse estrogen receptor gene”. Proc. Natl. Acad. Sci. U.S.A. 90 (23): 11162–6. PMC 47942. PMID 8248223.
- ↑ Invalid
<ref>tag; no text was provided for refs namedPalmertDunkel2012 - ↑ Fernandez-Miranda JC, Gardner PA, Snyderman CH, Devaney KO, Strojan P, Suárez C, Genden EM, Rinaldo A, Ferlito A (2012). “Craniopharyngioma: a pathologic, clinical, and surgical review”. Head Neck. 34 (7): 1036–44. doi:10.1002/hed.21771. PMID 21584897.
Causes
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Eiman Ghaffarpasand, M.D. [2], Kiran Singh, M.D. [3]
Overview
Common causes of amenorrhea are breastfeeding, pregnancy, menopause, and stress. Common causes of primary amenorrhea are craniopharyngioma, idiopathic gonadotropin deficiency, Kallmann’s Syndrome, Mayer-Rokitansky-Hauser Syndrome, Mullerian dysgenesis, and outflow tract disorders. Common causes of secondary amenorrhea are craniocerebral trauma, curettage, Cushing’s Syndrome, depression, diabetes mellitus, and drug side effects. Common causes of functional amenorrhea are stress, rapid weight loss, and excessive exercise.
Causes
Life Threatening Causes
Life-threatening causes include conditions which may result in death or permanent disability within 24 hours if left untreated. There are no life-threatening causes of amenorrhea, however complications resulting from untreated amenorrhea are common.
Common Causes
- Breastfeeding
- Menopause
- Pregnancy
- Stress
- Turner syndrome
- Excessive exercise
- Dieting
- Obesity
- Hyperthyroidism
- Hypothyroidism
Less Common Causes
- Androgen insensitivity syndrome (testicular feminization)
- Autoimmune disorders
- Autoimmune oophoritis (in myasthenia gravis, thyroiditis, or vitiligo)
- Aneurysms of the pituitary
- Cachexia
- Chronic disorders
- Chemotherapy (e.g., high-dose alkylating drugs)
- Congenital adrenal virilism
- Cushing syndrome
- Drug abuse
- Drug-induced virilization
- Androgens
- Antidepressants
- Danazol
- High-dose progestins
- Eating disorders
- Genetic disorder
- Congenital gonadotropin-releasing hormone deficiency
- GnRH receptor gene mutations
- Prader-Willi syndrome
- Congenital thymic aplasia
- Fragile X syndrome
- Idiopathic accelerated ovarian follicular atresia
- Gestational trophoblastic disease
- Gonadal dysgenesis
- HIV infection
- Hyperprolactinemia
- Idiopathic hypogonadotropic hypogonadism
- Infiltrative disorders of the pituitary
- Isolated gonadotropin deficiency
- Immunodeficiency
- Infiltrative disorders of the hypothalamus
- Irradiation to the pelvis
- Irradiation to the hypothalamus
Causes by Organ System
Causes in Alphabetical Order
- 5-alpha-reductase deficiency
- 18p minus syndrome
- Achard-Thiers syndrome
- Acromegaly
- Addison’s disease
- Adrenal cortex tumours
- Adrenal gland disorders
- Adrenocortical hyperplasia
- Agenesis of lower vagina
- Ahumada-del castillo syndrome
- Alcoholism
- Anemia
- Androgen insensitivity syndrome
- Anorexia nervosa [1]
- Anovulation
- Anterior pituitary failure
- Antidepressants
- Antipsychotics
- Anxiety
- Arrhenoblastoma
- Asherman syndrome
- Autoimmune adrenalitis
- Autoimmune hepatitis
- Autoimmune oophoritis
- Bearn-Kunkel syndrome
- Brain tumor
- Breastfeeding
- Bulimia
- C21-hydroxylase deficiency
- Celiac disease
- Cervical closure
- Chemotherapy
- Chiari-Frommel syndrome
- Chromosome 15q duplication syndrome
- Chromosome 17p, partial deletion
- Chronic alcohol poisoning
- Chronic illness
- Chronic renal failure
- Climate change
- Combined oral contraceptive pill
- Complications from D&C procedure
- Congenital adrenal hyperplasia
- Conn syndrome
- Constitutional delay of puberty
- Corpus luteum cyst
- Cortisone reductase deficiency
- Cranial irradiation
- Craniopharyngioma
- Cretinism
- Cushing syndrome
- Cushing’s disease
- Cyclophosphamide
- Cystic fibrosis
- Defect in SRY gene
- Denys-Drash syndrome
- Depression
- Diabetes mellitus
- Dietetic deficiency
- Down’s syndrome
- Dystrophia adipose-genitalis
- Eating disorders[2]
- Ectopic pregnancy [3]
- Emotional turmoil
- Empty sella syndrome
- Endometrial scarring
- Epirubicin
- Ethanol
- Excessive exercise
- Exogenous androgen use
- Female athlete syndrome[4]
- FGFR1 mutation
- Fluoxymesterone
- Forbes-Albright syndrome
- Frasier syndrome
- Fröhlich’s syndrome
- FSH receptor deficiency
- Galactorrhea
- Galactorrhoea-hyperprolactinaemia
- Galactose-1-phosphate uridyltransferase deficiency
- Germinoma
- Glioma
- GnRH deficiency
- Gonadal dysgenesis
- Granulosa cell tumor
- Grief
- Hematometra
- Hemosiderosis
- Heart disease
- Hematocolpos
- Hematosalpinx
- Hepatocellular carcinoma
- Hodgkin’s disease
- Hydatidiform mole
- Hyperprolactinaemia
- Hyperthyroidism
- Hypogonadism
- Hypogonadotropic hypogonadism
- Hypokalaemic distal renal tubular acidosis
- Hypopituitarism
- Hypothalamic tumor
- Hypothyroidism
- Hysterectomy
- Imperforate hymen
- Incomplete androgen insensitivity
- Inflammatory bowel disease
- Insanity
- Kal1 mutation
- Kallmann syndrome
- Laron syndrome
- Laurence-Moon-Biedl syndrome
- Lead poisoning
- Leukemia
- Liver cirrhosis
- Low weight
- Malabsorption syndrome
- Malnutrition
- Masculinization disorders
- Mayer-Rokitansky syndrome
- Medroxyprogesterone acetate
- Meningioma
- Menopause
- Metoclopramide
- Mercury poisoning
- Morphine poisoning
- Mullerian aplasia
- Mullerian dysgenesis
- Multiple endocrine neoplasia type 1
- Mumps
- Myxoedema
- Nandrolone
- Nephritis
- Obesity
- Oral contraceptives
- Ovarian cancer
- Ovarian failure
- Ovarian insufficiency due to FSH resistance
- Ovarian insufficiency, familial
- Ovarioleukodystrophy
- Ovary damage
- Panhypopituitarism
- Perimenopause
- Pituitary apoplexy
- Pituitary dwarfism
- Pituitary infarct
- Pituitary tumour
- Polycystic ovary syndrome
- Prader-Willi syndrome
- Pregnancy
- Premature ovarian failure
- Primary affective disorder
- PROKR2 mutation
- Prolactinoma
- Proprotein convertase 1/3 deficiency
- Pseudoamenorrhea
- Pseudocyesis
- Pseudohermaphroditism, female
- Radiotherapy
- Rapid weight loss
- Reproductive disorders
- Sheehan syndrome
- Simmonds’ disease
- Spironolactone
- Stanozolol
- Stein-Leventhal Syndrome
- Stress
- Systemic lupus erythematosus
- Testicular feminization syndrome
- Testosterone
- Tetrasomy X
- Thyrotoxicosis
- Traumatic brain injury
- Triple X syndrome
- Tubal ligationsyndrome
- Tuberculosis
- Turner syndrome
- Underweight
- Uterine aplasia
- Vaginal agenesis
- Vaginal closure
- Vaginal septum
- Virilizing ovarian tumor
- Vitamin A embryopathy
- Weight gain
- Werner syndrome
- XY female
Causes Based on Classification
- 17 beta-hydroxysteroid dehydrogenase deficiency
- Agonadism
- Anorexia Nervosa
- Anovulation
- Complete androgen insenstivity syndrome
- Constitutional bradygenesis
- Constitutional delay of puberty
- Diabetes Mellitus
- Early infantile brain damage
- Gonadal dysgenesis
- Homozygous adrenogenital syndrome
- Hymenal atresia
- Hyperandrogenism
- Hypothalamic and pituitary tumors
- Idiopathic gonadotropin deficiency
- Kallmann’s Syndrome
- Mayer-Rokitansky-Hauser Syndrome
- Mullerian dysgenesis
- Outflow tract disorders
- Pituitary insufficiency
- Polycystic Ovary Syndrome
- Post-hormonal contraceptive amenorrhea
- Severe systemic diseases
- Swyer’s Syndrome
- Testicular feminization
- Trauma
- Turner’s Syndrome
- Uterine atresia
- Uterine hypoplasia
- Vaginal atresia / gynatresia
Secondary Amenorrhea
- 5-alpha-reductase deficiency
- Addiction
- Addison’s Disease
- Adrenocortical insuffiency
- Adrenal tumors
- Asherman’s Syndrome
- Autoimmune diseases
- Body building (use of androgens)
- Castration (radiation or surgical)
- Central nervous system (CNS) tumor
- Cervical stenosis
- Change of environment
- Complete and incomplete androgen insensitivity
- Congenital adrenal hyperplasia
- Craniocerebral trauma
- Curettage
- Cushing’s Syndrome
- Depression
- Diabetes Mellitus
- Drug Side Effect (Chlorpromazine, Desogestrel and Ethinyl Estradiol, Docetaxel, Epirubicin hydrochloride, Ethynodiol diacetate and ethinyl estradiol, Fluoxymesterone, Histrelin, Iloperidone, Loxapine, Medroxyprogesterone, Norgestimate and Ethinyl estradiol, Norgestrel and Ethinyl estradiol, Sertraline, Methyltestosterone, Olanzapine, Pramipexole, Prochlorperazine, Tiagabine, and Trifluoperazine)
- Encephalitis
- Enzymatic defects in testosterone biosynthesis
- Exposure to maternal androgens in utero
- Extreme obesity
- During chemotherapy
- Gonadotropin deficiency in tumors
- Hormone-active ovarian tumor
- Hermaphroditism
- Heterozygous adrenogenital syndrome
- Hyperprolactinemia
- Hyperthyroidism
- Hypothyroidism
- Hysterectomy
- Imprisonment
- Meningitis
- Mullerian anomalies
- Myotonic dystrophy
- Pituitary insufficiency
- Polycystic ovary syndrome
- Post-hormonal contraception
- Post-infection (mumps and severe pelvic inflammatory disease)
- Post-operative gonadotropin deficiency
- Pregnancy
- Premature menopause
- Prolactinoma
- Radiation
- Sheehan’s Syndrome
- Testicular feminization
- Transsexuality when taking androgens
- Turner’s Syndrome
- Uterine cavity sclerosis
- Uterine Schistosomiasis
- Abortion
- Severe generalized infections of the pelvis
- Post uterine surgery
- Overzealous or repeated uterine curettage
- Tuberculosis endometritis
Functional amenorrhea
- Stress
- Eating disorders
- Excessive exercise
- Weight loss
References
- ↑ Abed J, Judeh H, Abed E, Kim M, Arabelo H, Gurunathan R (2014). ““Fixing a heart”: the game of electrolytes in anorexia nervosa”. Nutr J. 13: 90. doi:10.1186/1475-2891-13-90. PMC 4168120. PMID 25192814.
- ↑ Andersen AE, Ryan GL (2009). “Eating disorders in the obstetric and gynecologic patient population”. Obstet Gynecol. 114 (6): 1353–67. doi:10.1097/AOG.0b013e3181c070f9. PMID 19935043.
- ↑ Shaikh NB, Shaikh S, Shaikh F (2014). “A clinical study of ectopic pregnancy”. J Ayub Med Coll Abbottabad. 26 (2): 178–81. PMID 25603672.
- ↑ Hobart JA, Smucker DR (2000). “The female athlete triad”. Am Fam Physician. 61 (11): 3357–64, 3367. PMID 10865930.
- ↑ Sailer, Christian, Wasner, Susanne. Differential Diagnosis Pocket. Hermosa Beach, CA: Borm Bruckmeir Publishing LLC, 2002:77 ISBN 1591032016
Differentiating Amenorrhea from other Diseases
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Eiman Ghaffarpasand, M.D. [2], Mehrian Jafarizade, M.D [3]
Overview
As amenorrhea manifests in a variety of clinical forms, differentiation must be established in accordance with the particular subtype. Primary amenorrhea must be differentiated from other diseases that cause lack of menstrual cycle, such as Mullerian agenesis, 3-beta-hydroxysteroid dehydrogenase type 2 deficiency, androgen insensitivity syndrome, Kallmann syndrome, Turner syndrome, and 17-alpha-hydroxylase deficiency. In contrast, secondary amenorrhea must be differentiated from other diseases that cause menstrual cycle arrest, such as primary ovarian insufficiency, hypothyroidism, hyperprolactinemia, polycystic ovary syndrome, and Asherman’s syndrome.
Differentiating Diseases with Amenorrhea from each other
As amenorrhea manifests in a variety of clinical forms, differentiation must be established in accordance with the particular subtype. Primary amenorrhea must be differentiated from other diseases that cause lack of menstrual cycle, such as Mullerian agenesis, 3-beta-hydroxysteroid dehydrogenase type 2 deficiency, androgen insensitivity syndrome, Kallmann syndrome, Turner syndrome, and 17-alpha-hydroxylase deficiency. In contrast, secondary amenorrhea must be differentiated from other diseases that cause menstrual cycle arrest, such as primary ovarian insufficiency, hypothyroidism, hyperprolactinemia, polycystic ovary syndrome, and Asherman’s syndrome.
| Group | Diseases | Laboratory Findings | Physical Examination | Other Findings | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Estrogen | Progesterone | GnRH | LH | FSH | Androgen | TSH | T4 | PRL | Karyotype | Externl genitalia | Breast development | Pubic hair | Uterus | |||
| Primary amenorrhea | Mullerian agenesis[1] | Nl | Nl | Nl | Nl | Nl | Nl | Nl | Nl | Nl | 46 XX | Nl | + | + | – | |
| 3-beta-hydroxysteroid dehydrogenase type 2 deficiency | Nl | Nl | Nl | Nl | Nl | ↓ | Nl | Nl | Nl | 46 XX | Clitoromegaly | -/+ | + | + | ||
| Androgen insensitivity syndrome[2] | Nl | Nl | ↓ | ↑ | Nl | ↑↑ | Nl | Nl | Nl | 46 XY | Nl | + | + | – | ||
| Kallmann syndrome[3] | ↓ | ↓ | ↓↓ | ↓ | ↓ | ↓ | Nl | Nl | Nl | 46 XX | Nl | – | – | + | ||
| Turner syndrome[4] | ↓↓ | ↓ | ↑ | ↑ | ↑ | Nl | Nl | Nl | Nl | 45 XO | Nl | +/- | + | + |
| |
| 17-alpha-hydroxylase deficiency | ↓ | Nl | ↑ | ↑ | ↑ | ↓ | Nl | Nl | Nl | 46 XY | Infantilism | – | – | – | ||
| Secondary amenorrhea | Primary ovarian insufficiency[5] | ↓↓ | ↓ | ↑ | ↑ | ↑ | Nl | Nl | Nl | Nl | 46 XX | Nl | + | + | + | |
| Hypothyroidism[6] | Nl | Nl | Nl | Nl | Nl | ↑ | ↑↑ | ↓↓ | Nl | 46 XX | Nl | + | + | + |
| |
| Hyperprolactinemia[7] | ↓ | ↓ | ↓ | ↓ | ↓ | ↓ | Nl | Nl | ↑ | 46 XX | Nl | + | + | + | ||
| Polycystic ovary syndrome[8] | ↓↓ | ↓↓ | ↑ | ↑ | ↑ | ↑ | Nl | Nl | Nl | 46 XX | Nl | + | + | + | ||
| Asherman’s syndrome[9] | Nl | Nl | Nl | Nl | Nl | Nl | Nl | Nl | Nl | 46 XX | Nl | + | + | + | ||
References
- ↑ Folch M, Pigem I, Konje JC (2000). “Müllerian agenesis: etiology, diagnosis, and management”. Obstet Gynecol Surv. 55 (10): 644–9. PMID 11023205.
- ↑ “Current evaluation of amenorrhea”. Fertil. Steril. 82 (1): 266–72. 2004. doi:10.1016/j.fertnstert.2004.02.098. PMID 15237040.
- ↑ Albanese A, Stanhope R (1995). “Investigation of delayed puberty”. Clin. Endocrinol. (Oxf). 43 (1): 105–10. PMID 7641400.
- ↑ Sybert VP, McCauley E (2004). “Turner’s syndrome”. N. Engl. J. Med. 351 (12): 1227–38. doi:10.1056/NEJMra030360. PMID 15371580.
- ↑ Nelson LM (2009). “Clinical practice. Primary ovarian insufficiency”. N. Engl. J. Med. 360 (6): 606–14. doi:10.1056/NEJMcp0808697. PMC 2762081. PMID 19196677.
- ↑ Kalro BN (2003). “Impaired fertility caused by endocrine dysfunction in women”. Endocrinol. Metab. Clin. North Am. 32 (3): 573–92. PMID 14575026.
- ↑ Pickett CA (2003). “Diagnosis and management of pituitary tumors: recent advances”. Prim. Care. 30 (4): 765–89. PMID 15024895.
- ↑ “ACOG practice bulletin clinical management guidelines for obstetrician-gynecologists. Number 40, November 2002”. Obstet Gynecol. 100 (5 Pt 1): 1045–50. 2002. PMID 12434783.
- ↑ Fritz, Marc (2011). Clinical gynecologic endocrinology and infertility. Philadelphia: Wolters Kluwer Health/Lippincott Williams & Wilkins. ISBN 978-0781779685.
Epidemiology and Demographics
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Eiman Ghaffarpasand, M.D. [2]
Overview
The incidence of primary amenorrhea is approximately 3,000 cases per 100,000 individuals, mostly due to hypothalamic amenorrhea. The incidence of secondary amenorrhea is approximately 3,300 per 100,000 individuals in Sweden. The prevalence of amenorrhea is approximately 3,000 to 4,000 per 100,000 individuals worldwide. The prevalence of amenorrhea was estimated to be 13,400 cases per 100,000 female athletes in Oslo marathon games. The case-fatality rate/mortality rate of amenorrhea is less than 1%, and seen in patients of pituitary macroadenomas or generally brain lesions which cause amenorrhea. Primary amenorrhea is usually first diagnosed among adolescents (around 16 years of age). There is no racial predilection for amenorrhea. Commonly, females in developed countries experience puberty and menarche earlier than females of developing countries. This can be attributed to nutritional and socioeconomic situation but since the age of diagnosis of primary amenorrhea is based on the society’s mean age of puberty onset and menarche, there is not any difference between developing and developed countries in terms of prevalence of amenorrhea.
Epidemiology and Demographics
Incidence
- The incidence of primary amenorrhea is approximately 3,000 per 100,000 individuals, mostly due to hypothalamic amenorrhea.[1]
- The incidence of secondary amenorrhea is approximately 3,300 per 100,000 individuals.[2]
- The incidence of genital abnormality in patients with amenorrhea is about 15% (15,000 per each 100,000 individuals).[3]
- 10% of primary amenorrhea cases are caused by Mullerian agenesis, 10,000 cases per 100,000 cases.[4]
- Androgen insensitivity syndrome accounts for 5% cases of primary amenorrhea, 1.7 cases per 100,000 of population.[5]
- Anatomic defects incidences are including imperforate hymen of 100 in 100,000 women and transverse vaginal septum of 1.25 in 100,000 individuals.[4]
- Among the women with fragile X syndrome, 16,000 cases per 100,000 individuals would experience amenorrhea.[6]
- The incidence of Mayer-Rokitansky-Küster-Hauser syndrome is approximately 20 per 100,000 individuals.[7]
- The incidence of Kallmann syndrome is approximately 2.5 per 100,000 girls.[8]
- The incidence of Turner syndrome is approximately 40 per 100,000 live female births.[9]
- The incidence of premature ovarian insufficiency is approximately 100 per 100,000 under 30 years, 400 per 100,000 around 35 years, and 1000 per 100,000 at 40 years of age.[10]
Prevalence
- The prevalence of amenorrhea is approximately 3,000 to 4,000 per 100,000 individuals worldwide.[11][12]
- In Oslo marathon games, the prevalence of amenorrhea was estimated to be 13,400 cases per 100,000 female athletes.[13]
- The prevalence of both primary and secondary amenorrhea is estimated to be 10-15 cases annually, in highly specialized referral centres.[3][4]
- Premature ovarian failure prevalence among women is 1,000 to 5,000 per 100,000 individuals.[14]
- Prevalence of oligomenorrhea and amenorrhea among polycystic ovary syndrome patients are 76% and 24%, respectively.[15]
- The prevalence of weight related amenorrhea is approximately 1,000 to 5,000 per 100,000 individuals.[16]
- Hyperprolactinemia prevalence among patients with primary amenorrhea is about 1%.[17]
Case-fatality rate/Mortality rate
- The case-fatality rate/mortality rate of amenorrhea is approximately below 1%, due to pituitary macroadenomas or generally brain lesions which cause amenorrhea.
Age
- Patients of all age groups may develop secondary amenorrhea, before menopause.
- The incidence of premature ovarian insufficiency is approximately 100 per 100,000 under 30 years, 400 per 100,000 around 35 years, and 1000 per 100,000 at 40 years of age.[10]
- Primary amenorrhea is usually first diagnosed among adolescence (around 16 years of age).
Race
- There is no racial predilection to amenorrhea.
- Menarche usually occurs earlier in non-Hispanic black girls compared to girls of the white race.
- Whereas, menarche in Mexican American girls is slightly earlier than girls of the white race.[18]
Region
- The incidence of secondary amenorrhea is approximately 3,300 per 100,000 individuals in Sweden. 0.7% of studied population have amenorrhea secondary to oral contraceptives.[2]
- In Oslo marathon games, the prevalence of amenorrhea was estimated to be 13,400 cases per 100,000 individuals.[13]
Developed Countries vs. Developing Countries
- Majority of times, girls from developed countries experience the puberty and menarche earlier than developing countries, due to nutritional and socioeconomic situation. But, since the diagnosing age of primary amenorrhea is based on society’s mean age of puberty onset and menarche, there is not any difference between developing and developed countries in prevalence of amenorrhea.[18]
References
- ↑ Rosenfield RL (1990). “Clinical review 6: Diagnosis and management of delayed puberty”. J. Clin. Endocrinol. Metab. 70 (3): 559–62. doi:10.1210/jcem-70-3-559. PMID 2407749.
- ↑ 2.0 2.1 Pettersson F, Fries H, Nillius SJ (1973). “Epidemiology of secondary amenorrhea. I. Incidence and prevalence rates”. Am. J. Obstet. Gynecol. 117 (1): 80–6. PMID 4722382.
- ↑ 3.0 3.1 “Current evaluation of amenorrhea”. Fertil. Steril. 90 (5 Suppl): S219–25. 2008. doi:10.1016/j.fertnstert.2008.08.038. PMID 19007635.
- ↑ 4.0 4.1 4.2 “Current evaluation of amenorrhea”. Fertil. Steril. 86 (5 Suppl 1): S148–55. 2006. doi:10.1016/j.fertnstert.2006.08.013. PMID 17055812.
- ↑ Doody KM, Carr BR (1990). “Amenorrhea”. Obstet. Gynecol. Clin. North Am. 17 (2): 361–87. PMID 2234749.
- ↑ Allingham-Hawkins DJ, Babul-Hirji R, Chitayat D, Holden JJ, Yang KT, Lee C, Hudson R, Gorwill H, Nolin SL, Glicksman A, Jenkins EC, Brown WT, Howard-Peebles PN, Becchi C, Cummings E, Fallon L, Seitz S, Black SH, Vianna-Morgante AM, Costa SS, Otto PA, Mingroni-Netto RC, Murray A, Webb J, Vieri F (1999). “Fragile X premutation is a significant risk factor for premature ovarian failure: the International Collaborative POF in Fragile X study–preliminary data”. Am. J. Med. Genet. 83 (4): 322–5. PMC 3728646. PMID 10208170.
- ↑ Fedele L, Bianchi S, Tozzi L, Borruto F, Vignali M (1996). “A new laparoscopic procedure for creation of a neovagina in Mayer-Rokitansky-Kuster-Hauser syndrome”. Fertil. Steril. 66 (5): 854–7. PMID 8893702.
- ↑ Dodé C, Hardelin JP (2009). “Kallmann syndrome”. Eur. J. Hum. Genet. 17 (2): 139–46. doi:10.1038/ejhg.2008.206. PMC 2986064. PMID 18985070.
- ↑ Nielsen J, Wohlert M (1991). “Chromosome abnormalities found among 34,910 newborn children: results from a 13-year incidence study in Arhus, Denmark”. Hum. Genet. 87 (1): 81–3. PMID 2037286.
- ↑ 10.0 10.1 Timmreck LS, Reindollar RH (2003). “Contemporary issues in primary amenorrhea”. Obstet. Gynecol. Clin. North Am. 30 (2): 287–302. PMID 12836721.
- ↑ Bachmann GA, Kemmann E (1982). “Prevalence of oligomenorrhea and amenorrhea in a college population”. Am. J. Obstet. Gynecol. 144 (1): 98–102. PMID 7114117.
- ↑ Pettersson F, Fries H, Nillius SJ (1973). “Epidemiology of secondary amenorrhea. I. Incidence and prevalence rates”. Am. J. Obstet. Gynecol. 117 (1): 80–6. PMID 4722382.
- ↑ 13.0 13.1 Tomten SE (1996). “Prevalence of menstrual dysfunction in Norwegian long-distance runners participating in the Oslo Marathon games”. Scand J Med Sci Sports. 6 (3): 164–71. PMID 8827845.
- ↑ Jones GS, De Moraes-Ruehsen M (1969). “A new syndrome of amenorrhae in association with hypergonadotropism and apparently normal ovarian follicular apparatus”. Am. J. Obstet. Gynecol. 104 (4): 597–600. PMID 5786709.
- ↑ Bili H, Laven J, Imani B, Eijkemans MJ, Fauser BC (2001). “Age-related differences in features associated with polycystic ovary syndrome in normogonadotrophic oligo-amenorrhoeic infertile women of reproductive years”. Eur. J. Endocrinol. 145 (6): 749–55. PMID 11720900.
- ↑ Laughlin GA, Dominguez CE, Yen SS (1998). “Nutritional and endocrine-metabolic aberrations in women with functional hypothalamic amenorrhea”. J. Clin. Endocrinol. Metab. 83 (1): 25–32. doi:10.1210/jcem.83.1.4502. PMID 9435412.
- ↑ Patel SS, Bamigboye V (2007). “Hyperprolactinaemia”. J Obstet Gynaecol. 27 (5): 455–9. doi:10.1080/01443610701406125. PMID 17701788.
- ↑ 18.0 18.1 Chumlea WC, Schubert CM, Roche AF, Kulin HE, Lee PA, Himes JH, Sun SS (2003). “Age at menarche and racial comparisons in US girls”. Pediatrics. 111 (1): 110–3. PMID 12509562.
Risk Factors
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Eiman Ghaffarpasand, M.D. [2]
Overview
The most common risk factor in the development of primary amenorrhea include chromosomal disorders and the most common risk factor in the development of secondary amenorrhea is breastfeeding. Common risk factors in the development of amenorrhea include risk factors related to hypothalamus, pituitary, ovaries, and also functional amenorrhea. Most common hypothalamic risk factors are Kallmann syndrome and chronic disorders. Most common pituitary risk factors are hyperprolactinemia and pituitary microadenoma.
Risk Factors
- The most common risk factor in the development of primary amenorrhea is chromosomal disorder and the most common risk factor in the development of secondary amenorrhea is breastfeeding.
- Common risk factors in the development of amenorrhea include risk factors related to hypothalamus, pituitary, ovaries, and also functional amenorrhea. The risk factors in the development of amenorrhea, in an order from most common to least common, are as following:[1][2]
Hypothalamic risk factors
- Kallmann syndrome
- Chronic disorders
- Congenital gonadotropin-releasing hormone deficiency
- Irradiation to the hypothalamus
- Infiltrative disorders of the hypothalamus
- Tumors of the hypothalamus
- Tumors of the brain
- Traumatic brain injury
Pituitary risk factors
- Isolated gonadotropin deficiency
- Postpartum pituitary necrosis (Sheehan syndrome)
- Traumatic brain injury
- Aneurysms of the pituitary
Gonadal risk factors
- Androgen insensitivity syndrome (testicular feminization)
- Autoimmune disorders
- Autoimmune oophoritis (in myasthenia gravis, thyroiditis, or vitiligo)
- Chemotherapy (e.g., high-dose alkylating drugs)
- Congenital adrenal virilism
- Gestational trophoblastic disease
- Drug-induced virilization
- Androgens
- Antidepressants
- Danazol
- High-dose progestins
- Prader-Willi syndrome
- Fragile X syndrome
- Idiopathic accelerated ovarian follicular atresia
Anatomical defects risk factors
- Family history of anatomical defects
- Radiation within pregnancy
- Dilation and curettage (D & C)
- Prior complicated Cesarean section
- Severe pelvic inflammatory disease (PID)-induced adhesion
- Uterus scarring
Functional amenorrhea risk factors
Miscellaneous
High risk sports in female athletes
- Cross country
- Ballet
- Track and Field
- Swimming
- Cycling
- Rowing
- Diving
- Figure skating
- Gymnastics
- All other intense and strenuous sports
References
- ↑ “Current evaluation of amenorrhea”. Fertil. Steril. 90 (5 Suppl): S219–25. 2008. doi:10.1016/j.fertnstert.2008.08.038. PMID 19007635.
- ↑ Golden NH, Carlson JL (2008). “The pathophysiology of amenorrhea in the adolescent”. Ann. N. Y. Acad. Sci. 1135: 163–78. doi:10.1196/annals.1429.014. PMID 18574222.
Screening
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Eiman Ghaffarpasand, M.D. [2]
Overview
According to the US Preventive Services Task Force (USPSTF), there is insufficient evidence to recommend routine screening for amenorrhea.
Screening
- According to the US Preventive Services Task Force (USPSTF), there is insufficient evidence to recommend routine screening for amenorrhea.
References
Natural History, Complications and Prognosis
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Eiman Ghaffarpasand, M.D. [2]
Overview
If left untreated, patients with amenorrhea may progress to develop infertility and osteoporosis. Common complications of amenorrhea are based on underlying disorder that induce amenorrhea. Prognosis is generally excellent and the mortality rate of patients with amenorrhea is approximately less than 1%, generally in patients with brain lesions.
Natural History, Complications, and Prognosis
Natural History
- If left untreated, all patients of amenorrhea may progress to develop infertility and osteoporosis.
- The majority of cases woth amenorrhea are result of four conditions, which include polycystic ovary syndrome, hypothalamic amenorrhea, hyperprolactinemia, and ovarian failure.
- Polycystic ovary syndrome (PCOS), if left untreated can lead to heart disease from elevated cholesterol and increased levels of androgens. Long periods of not having menstrual cycles leads to unopposed exposure of endometrium to estrogen, can result in endometrial cancer.[1]
- In functional (hypothalamic) amenorrhea, the patient usually reports normal regular cycles in the past, with sudden interruption of menstrual cycles for more than 3 months. There is almost always a history of weight loss (severe), excessive exercise, or drastic emotional stress prior to cessation of menstruation.[2]
- Premature ovarian failure presents with menopause before the age of 40 and elevated levels of gonadotropins. In the age group of 41 to 44 years, it is called pre-menopause. Patients of premature ovarian failure generally have a family history of ovarian failure.[3]
- Amenorrhea from hyperprolactinemia can be caused by prolactin overproduction or dopamine suppression, and is mostly seen in middle aged women.[4]
Complications
- Common complications of amenorrhea are based on the underlying disorder inducing amenorrhea. The majority of amenorrhea cases are caused by four conditions, which include polycystic ovary syndrome, hypothalamic amenorrhea, hyperprolactinemia, and ovarian failure.
- Common complications of amenorrhea from PCOS include:
- Hyperprolactinemia leads to galactorrhea, decreased libido, and pregnancy complications. In cases with prolactinoma, massive enlargement of the tumor may affect vision and pituitary function. It may also cause osteopenia and osteoporosis in pre-menopausal women.[5]
- Common complications of premature ovarian failure include infertility, osteoporosis, depression/anxiety, cardiac disease, and dementia.[6]
- Patients with hypothalamic (functional) amenorrhea experience various complications, such as infertility, decrease in bone mineral density (BMD), increased risk for fracture, along with cardiovascular and psychological complicatons.[2]
- The most important complication of premature ovarian failure is infertility, that is preventable to some extent with appropriate therapies. Bone loss and psychiatric disorders are other complications.[7]
Prognosis
- Prognosis is generally excellent and the mortality rate of patients with amenorrhea is approximately less than 1%.
- Among patients of androgen insensitivity syndrome there is an increased risk of testicular cancer, and surveillance is needed appropriate intervals.
- Prognosis of polycystic ovary syndrome (PCOS) is generally good. Long term dietary management and exercise along with metformin therapy decreases the cardiovascular and pregnancy complications in the future.[8]
- Prognosis is excellent for hyperprolactinemia due to microprolactinoma. Depending on the size of the tumor and the extent of tumor resection, the rate of recurrence may range from 20% to 50%. The majority of recurrent prolactinomas develop within the first 5 years.[9]
References
- ↑ Palomba S, Santagni S, Falbo A, La Sala GB (2015). “Complications and challenges associated with polycystic ovary syndrome: current perspectives”. Int J Womens Health. 7: 745–63. doi:10.2147/IJWH.S70314. PMC 4527566. PMID 26261426.
- ↑ 2.0 2.1 Meczekalski B, Katulski K, Czyzyk A, Podfigurna-Stopa A, Maciejewska-Jeske M (2014) Functional hypothalamic amenorrhea and its influence on women’s health. J Endocrinol Invest 37 (11):1049-56. DOI:10.1007/s40618-014-0169-3 PMID: 25201001
- ↑ Vegetti W, Marozzi A, Manfredini E, Testa G, Alagna F, Nicolosi A, Caliari I, Taborelli M, Tibiletti MG, Dalprà L, Crosignani PG (2000). “Premature ovarian failure”. Mol. Cell. Endocrinol. 161 (1–2): 53–7. PMID 10773392.
- ↑ Mattei AM, Severini V, Crosignani PG (1991). “Natural history of hyperprolactinemia”. Ann. N. Y. Acad. Sci. 626: 130–6. PMID 2058949.
- ↑ Sanfilippo JS (1999). “Implications of not treating hyperprolactinemia”. J Reprod Med. 44 (12 Suppl): 1111–5. PMID 10649820.
- ↑ “Premature ovarian failure – Symptoms and causes – Mayo Clinic”.
- ↑ Nelson LM (2009). “Clinical practice. Primary ovarian insufficiency”. N Engl J Med. 360 (6): 606–14. doi:10.1056/NEJMcp0808697. PMC 2762081. PMID 19196677.
- ↑ Hart R (2007). “Polycystic ovarian syndrome–prognosis and treatment outcomes”. Curr. Opin. Obstet. Gynecol. 19 (6): 529–35. doi:10.1097/GCO.0b013e3282f10e22. PMID 18007129.
- ↑ http://www.niddk.nih.gov/health-information/health-topics/endocrine/prolactinoma/Pages/fact-sheet.aspx
Diagnosis
Diagnosis
History and Symptoms | Physical Examination | Laboratory Findings | Electrocardiogram | X-Ray Findings | Echocardiography and Ultrasound | CT-Scan Findings | MRI Findings | Other Diagnostic Studies | Other Imaging Findings
Treatment
Treatment
Medical Therapy | Surgery | Primary Prevention | Secondary Prevention | Cost-Effectiveness of Therapy | Future or Investigational Therapies
Looking for the patient version?
© 2026 MyEClinic – IFTM Institut für Telematik in der Medizin GmbH