
Adenocarcinoma of the lung
For patient information click here
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Shanshan Cen, M.D. [2]
Synonyms and keywords: Lung adenocarcinoma, Pulmonary adenocarcinoma, Adenocarcinoma of lung
Overview
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Trusha Tank, M.D.[2], Sudarshana Datta, MD [3], Shanshan Cen, M.D. [4]
Overview
Adenocarcinoma of the lung is a common histological form of lung cancer. Adenocarcinoma of the lung may be classified according to WHO into 8 subtypes: Lepidic, acinar, papillary, micropapillary, solid, colloid, fetal, enteric adenocarcinoma. Adenocarcinoma of the lung may be classified according to IASLC/ATS/ERS into 3 main types: adenocarcinoma in situ, minimally invasive adenocarcinoma, invasive adenocarcinoma. On gross pathology, peripheral multifocal lesions is the characteristic finding of adenocarcinoma of the lung. On microscopic histopathological analysis, nuclear atypia, eccentrically placed nuclei, abundant cytoplasm, and conspicuous nucleoli are characteristic findings of adenocarcinoma of the lung. Genes involved in the pathogenesis of adenocarcinoma of the lung include EGFR, HER2, KRAS, ALK, and BRAF. Common risk factors in the development of adenocarcinoma of the lung include smoking, family history of lung cancer, high levels of air pollution, radiation therapy to the chest, radon gas, asbestos, occupational exposure to chemical carcinogens, and previous lung disease. The incidence of adenocarcinoma of the lung is approximately 22.1 per 100,000 individuals worldwide. Adenocarcinoma of the lung affects men and women equally. Patients of all age groups may develop adenocarcinoma of the lung. Common symptoms of adenocarcinoma of the lung include dyspnea, hemoptysis, chronic coughing, chest pain, cachexia, dysphonia, and paraneoplastic syndromes. Adenocarcinoma of the lung may be classified into several subtypes based on TNM and UICC staging system. The predominant therapy for adenocarcinoma of the lung is surgical resection. Adjunctive chemotherapy, radiation therapy, and target therapy may be required. Common complications of adenocarcinoma of the lung include breathing difficulties, pneumonia, pleural effusion, metastasis, and Horner’s syndrome. The prognosis of adenocarcinoma of the lung varies with the staging of tumor; Stage IA have the most favorable prognosis. The presence of metastasis is associated with a particularly poor prognosis.
Classification
Adenocarcinoma of the lung may be classified according to WHO into 5 subtypes: mixed, acinar, papillary, bronchioloalveolar carcinoma, and solid adenocarcinoma. Adenocarcinoma of the lung may be classified according to IASLC/ATS/ERS into 6 subtypes: pre-invasive lesions, atypical adenomatous hyperplasia, adenocarcinoma in situ, minimally invasive adenocarcinoma, invasive adenocarcinoma, and variants of invasive adenocarcinoma. Adenocarcinoma of the lung may be classified into several subtypes based on TNM and UICC staging system.
Pathophysiology
On gross pathology, peripheral multifocal lesions is the characteristic finding of adenocarcinoma of the lung. On microscopic histopathological analysis, nuclear atypia, eccentrically placed nuclei, abundant cytoplasm, and conspicuous nucleoli are characteristic findings of adenocarcinoma of the lung. Genes involved in the pathogenesis of adenocarcinoma of the lung include EGFR, HER2, KRAS, ALK, and BRAF.
Cause
Adenocarcinoma of the lung may caused by genetic mutations, including EGFR (7p11), KRAS (12p12), BRAF (7q34), and PIK3CA (3q26).
Differential Diagnosis
Adenocarcinoma of the lung must be differentiated from atypical adenomatous hyperplasia of the lung, adenocarcinoma in situ, squamous cell carcinoma of the lung, small cell carcinoma of the lung, malignant mesothelioma, and metastatic adenocarcinoma.
Epidemiology and Demographics
The incidence of adenocarcinoma of the lung is approximately 22.1 per 100,000 individuals worldwide. Adenocarcinoma of the lung affects men and women equally. Patients of all age groups may develop adenocarcinoma of the lung.
Risk Factors
Common risk factors in the development of adenocarcinoma of the lung include smoking, family history of lung cancer, high levels of air pollution, radiation therapy to the chest, radon gas, asbestos, occupational exposure to chemical carcinogens, and previous lung disease.
Screening
According to the clinical practice guideline by the U.S. Preventive Services Task Force (USPSTF), screening for lung cancer by low-dose computed tomography (LDCT) is recommended every year among smokers and former smokers who are between 55 to 80 years old and who have smoked 30 pack-years or more and either continue to smoke or have quit within the past 15 years (grade B recommendation). According to the clinical practice guideline issued by the American College of Chest Physicians (CHEST) in 2013, screening for lung cancer by low-dose CT (LDCT) is recommended every year among smokers and former smokers who are age 55 to 74 and who have smoked for 30 pack-years or more and either continue to smoke or have quit within the past 15 years.
Natural history, Complications, and Prognosis
Common complications of adenocarcinoma of the lung include breathing difficulties, pneumonia, pleural effusion, metastasis, and Horner’s syndrome. The prognosis of adenocarcinoma of the lung varies with the staging of tumor; Stage IA have the most favorable prognosis. The presence of metastasis is associated with a particularly poor prognosis.
Diagnosis
Diagnostic Study of Choice
Biopsy is helpful in the diagnosis of adenocarcinoma of the lung.
History and Symptoms
Common symptoms of adenocarcinoma of the lung include dyspnea, hemoptysis, chronic coughing, chest pain, cachexia, dysphonia, and paraneoplastic syndromes.
Physical Examination
Common physical examination findings of adenocarcinoma of the lung include tachypnea, decreased breath sounds, and lethargy.
Laboratory Findings
Electrocardiogram
X Ray
Chest x-ray may be helpful in the diagnosis of adenocarcinoma of the lung. Findings on x-ray suggestive of adenocarcinoma of the lung include mass, widening of the mediastinum, atelectasis, consolidation, and pleural effusion.
Echocardiography and Ultrasound
Ultrasound may be helpful in the diagnosis of pleural effusion among patients with adenocarcinoma of the lung.
CT
Chest CT scan may be helpful in the diagnosis of adenocarcinoma of the lung. Finding on CT scan suggestive of adenocarcinoma of the lung is a lung nodule with a rounded or irregular region of increased attenuation.
MRI
There are no MRI findings associated with adenocarcinoma of the lung.
Other Imaging Findings
Other diagnostic studies for adenocarcinoma of the lung include bone scintigraphy, PET scan, and pulmonary ventilation/perfusion scan.
Other Diagnostic Studies
Other diagnostic studies for adenocarcinoma of the lung include molecular testing and endoscopy.
Treatment
Medical Therapy
The predominant therapy for adenocarcinoma of the lung is surgical resection. Adjunctive chemotherapy, radiation therapy, and target tharapy may be required.
Interventions
Surgery
Surgery is the mainstay of treatment for adenocarcinoma of the lung.
Primary Prevention
Effective measures for the primary prevention of adenocarcinoma of the lung include smoking cessation, eliminating secondhand smoke, reducing or eliminating exposure to radon, and reducing or eliminating occupational exposure to lung carcinogens.
Secondary Prevention
References
Historical Perspective
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief:
Overview
Prior to the introduction of cigarette smoking and industrial carcinogens, lung cancer was thought to be a rare disease. Of all tumors detected upon autopsy, lung cancer accounted for only 1% of cancers in the 1800s. Majority of the cases of lung cancer were associated with occupational hazards due to radon exposure. The association between lung cancer and smoking was not defined until the mid-20th century.
Historical Perspective
The historical data on lung cancer is described below:[1][2][3][4][5][6][7][8]
- Majority of the cases of lung cancer were associated with occupational hazards. Death among miners was reported to be caused by Bergkrankheit (mountain sickness).
- During World war 1, cigarette smoking gained popularity because the soldiers used to smoke in trenches to relieve stress, so did the civilians and the women at home. General John J.(“Black Jack”) Pershing reportedly stated: “You ask me what it is we need to win this war. I answer tobacco as much as bullets.”
- In 1924, radon gas was first reported to be a prominent cause of lung cancer among miners.
- In 1929, German physician, Fritz Lickint published a paper and suggested that lung cancer patients were likely to be smokers.
- In 1929, German physician, Fritz Lickint launched anti-tobacco campaign in Germany.
- In the 1930s, clinicians started suspecting the association between cigarette smoking and lung cancer due to an increased number of cases.
- The association between lung cancer and smoking was not defined until the mid-20th century. The first reports between lung cancer and smoking were often confounded by gender, given that men were more likely to be smokers compared to women.
- In the 1950s, Doll and Hill in England provided additional corroboration for a causal association between smoking and lung cancer.
- In the 1950s, Cuyler Hammond and Ernest Wynder in the U.S provided additional corroboration for a causal association between smoking and lung cancer.
- In 1961, the first case of adenocarcinoma of the lung was reported.
- The 1969 Springer Handbook of Special Pathology is considered to be the landmark publication that highlighted the role of smoking in the development of lung cancer in over 25 pages.
- In 1969, the first surgeon general warning was issued suggesting cigarette smoking to be a hazard for lung cancer.
- In the 1980s, cisplatin-based chemotherapy emerged and demonstrated modest efficacy in the reduction of tumor related symptoms and improvement of quality of life.
References
- ↑ Witschi H (2001). “A short history of lung cancer”. Toxicological Sciences : an Official Journal of the Society of Toxicology. 64 (1): 4–6. PMID 11606795. Retrieved 2011-12-09. Unknown parameter
|month=ignored (help) - ↑ Hecht SS (1999). “Tobacco smoke carcinogens and lung cancer”. J. Natl. Cancer Inst. 91 (14): 1194–210. PMID 10413421.
- ↑ Kluger, R. (1996). Ashes to ashes: America’s hundred-year cigarette war, the public health, and the unabashed triumph of Philip Morris. New York: Alfred A. Knopf.
- ↑ Proctor, Robert (2000). The Nazi war on cancer. Princeton, N.J. Oxford: Princeton University Press. ISBN 978-0691070513.
- ↑ Morabia, Alfredo (2012). “Quality, originality, and significance of the 1939 “Tobacco consumption and lung carcinoma” article by Mueller, including translation of a section of the paper”. Preventive Medicine. 55 (3): 171–177. doi:10.1016/j.ypmed.2012.05.008. ISSN 0091-7435.
- ↑ Mueller F. Tabakmissbrauch und Lungencarcinom. Z. Krebsforsch. 1939;49:57–85.
- ↑ Wynder, E. L. (1994). Prevention and cessation of tobacco use: Obstacles and challenges. J. Smoking-Related Dis. 5(Suppl. 1), 3–8.
- ↑ Hanspeter Witschi ITEH and Department of Molecular Biosciences, School of Veterinary Medicine, University of California, Davis, California 95616
Classification
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Trusha Tank, M.D.[2]Shanshan Cen, M.D. [3] Sudarshana Datta, MD [4]
Overview
Adenocarcinoma of the lung may be classified according to WHO into many sub-types. Adenocarcinoma of the lung may be classified according to IASLC/ATS/ERS into pre-invasive lesions, atypical adenomatous hyperplasia, adenocarcinoma in situ, minimally invasive adenocarcinoma, invasive adenocarcinoma, and variants of invasive adenocarcinoma.
Classification
- Adenocarcinomas are highly heterogeneous tumors.
- Several major histological sub-types are currently recognized by the WHO and IASLC/ATS/ERS classification systems.[1][2][3]
- The IASLC/ATS/ERS lung adenocarcinoma histological classification system was proposed in 2011.[4]
- According to this new classification, tumor size ≤ 3 cm with pure lepidic pattern, but without lymphatic, vascular, and pleural invasion or tumor necrosis, was defined as adenocarcinoma in situ (AIS).
- If tumor size ≤ 3 cm with a lepidic predominant pattern and contained ≤ 5 mm stromal invasion, it was defined as minimally invasive adenocarcinoma (MIA).
- If tumor had > 5 mm stromal invasion, it was defined as an invasive adenocarcinoma.
- The WHO histological classification of adenocarcinoma is following:[5][6]
| WHO Classification of Lung Tumors | |
|---|---|
| Histological type | Subtype |
| Epithelial Tumors | |
| Adenocarcinoma |
|
References
- ↑ Van Schil, P. E.; Asamura, H; Rusch, V. W.; Mitsudomi, T; Tsuboi, M; Brambilla, E; Travis, W. D. (2012). “Surgical implications of the new IASLC/ATS/ERS adenocarcinoma classification”. European Respiratory Journal. 39 (2): 478–86. doi:10.1183/09031936.00027511. PMID 21828029.
- ↑ Travis, W. D.; Brambilla, E; Van Schil, P; Scagliotti, G. V.; Huber, R. M.; Sculier, J. P.; Vansteenkiste, J; Nicholson, A. G. (2011). “Paradigm shifts in lung cancer as defined in the new IASLC/ATS/ERS lung adenocarcinoma classification”. European Respiratory Journal. 38 (2): 239–43. doi:10.1183/09031936.00026711. PMID 21804158.
- ↑ Vazquez, M; Carter, D; Brambilla, E; Gazdar, A; Noguchi, M; Travis, W. D.; Huang, Y; Zhang, L; Yip, R; Yankelevitz, D. F.; Henschke, C. I.; International Early Lung Cancer Action Program Investigators (2009). “Solitary and multiple resected adenocarcinomas after CT screening for lung cancer: Histopathologic features and their prognostic implications”. Lung Cancer. 64 (2): 148–54. doi:10.1016/j.lungcan.2008.08.009. PMC 2849638. PMID 18951650.
- ↑ . doi:10.3978/j.issn.2072-1439.2014.09.13. Missing or empty
|title=(help) - ↑ Travis, William (2004). Pathology and genetics of tumours of the lung, pleura, thymus, and heart. Lyon: IARC Press. ISBN 9283224183.
- ↑ “www.jto.org”.
Pathophysiology
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Trusha Tank, M.D.[2], Shanshan Cen, M.D. [3], Sudarshana Datta, MD [4]
Overview
Adenocarcinoma is the most common type of lung cancer found in non-smokers and is usually seen as a peripheral lesion in the lungs. In the past several years, many genetic and environmental factors have been identified as causative factors for lung cancer. Individual susceptibility, active smoking, radon exposure, exposure to high pollution levels, asbestos exposure, occupational or environmental exposure to particular agents, and carcinogens contribute to the development of adenocarcinoma of the lung. Hydrocarbons cause damage to the DNA and form DNA adducts. Genes involved in the pathogenesis of adenocarcinoma of the lung include EGFR, HER2, KRAS, ALK, and BRAF. On gross pathology, peripheral multifocal single or multiple solid firm yellow-white nodule or mass which may invade into the pleura and cause pleural retraction/puckering. Adenocarcinoma usually does not form a cavitary lesion. It may present as a diffuse pleural thickening resembling malignant mesothelioma. On microscopic histopathological analysis, nuclear atypia, eccentrically placed nuclei, abundant cytoplasm, and conspicuous nucleoli are characteristic findings of adenocarcinoma of the lung.
Pathophysiology
Pathogenesis
- Adenocarcinoma is the most common type of lung cancer found in non-smokers and is usually seen as a peripheral lesion in the lungs, as compared to centrally located tumors such as small cell lung cancer and squamous cell lung cancer.[1][2]
- Lung cancer pathogenesis can be understood with the help of the following hypotheses:[3][4][5]
- Familial Lung Cancer:
- 6q23–25 locus has been identified as a susceptibility gene for familial lung cancer.
- Multistep Tumorigenesis:
- Tumors of organs such as skin, lung, and colon are developed through a process called multistep tumorigenesis.[6]
- As with other epithelial malignancies, lung cancers are believed to arise from preneoplastic or precursor lesions in the respiratory mucosa.
- Multistep tumorigenesis is the development of tumor through a series of progressive pathologic events such as preneoplastic or precursor lesions with corresponding genetic and epigenetic aberrations.
- Hyperplasia, squamous metaplasia, squamous dysplasia, and carcinoma in situ (CIS) comprise changes in the large airways that precede or accompany invasive squamous cell carcinoma of the lung.
- Multistep tumorigenesis explains pathogenesis of centrally located squamous cell carcinoma of the lung very well but fails to explain pathogenesis of large cell lung carcinomas, lung adenocarcinomas, and small cell lung cancer.
- Accumulation of Molecular Abnormalities:
- Another theory for pathogenesis of lung cancer is the accumulation of molecular abnormalities beyond a certain threshold point, rather than the sequence of alterations.
- There are no known preneoplastic lesions for the most common type of neuroendocrine lung tumors and small cell carcinoma of the lung,
- Atypical adenomatous hyperplasia (AAH) is the only sequence of morphologic change identified leading to the development of invasive adenocarcinoma of the lung.
- Pathogenesis of lung cancer is thought to be the result of both step-wise, sequence-specific and multistage molecular pathogenesis and accumulation and combination of genetic and epigenetic abnormalities.
Field of Injury and Field Cancerization
- Preneoplastic lung lesions frequently extend throughout the respiratory epithelium, indicating a field effect in which much of the respiratory epithelium has been mutagenized, presumably from exposure to tobacco-related carcinogens.[7][8][9]
- Epithelial cells lining the entire respiratory tract that have been exposed to smoking show molecular alterations that may signify the onset of lung cancers, a paradigm known as the “airway field of injury”.
- Premalignant airway fields in the molecular pathogenesis of lung cancer:
- Smoking induces widespread molecular alterations, such as gene expression changes in exposed epithelia throughout the respiratory tract.
- The airway field of injury can be seen in smokers with or without lung cancer and is highly relevant for the identification of markers for minimally invasive and early detection of lung cancer.
- The adjacent airway field of carcinoma represents the field in normal appearing airways adjacent to lung tumors.
- It has been suggested that in this adjacent field of tumor, there is closer molecular genealogy between lung cancers and airways that are in closest proximity to the tumors compared with airways that are more distant from the tumors.
- The progression of the molecular airway field of injury to preneoplasia and lung malignancy is still not clear.
- Molecular changes involved in the development of the airway field of injury and changes mediating progression of this field to lung preneoplasia may help the identification of early markers for lung cancer detection and chemoprevention.
- Underlying lung disease such as COPD, idiopathic pulmonary fibrosis and tuberculosis may exacerbate also trigger the process.
Genetics
Molecular Pathogenesis of Adenocarcinoma of the Lung
- Somatic copy number alterations affect a large fraction of the cancer cell genome and are also associated with lung cancer.[10][11][12][13][14]
- Copy-number gain of chromosome 5p has been identified as the most frequent alteration in lung adenocarcinoma followed by chromosome 3q.
- The Kirsten rat sarcoma viral oncogene (KRAS) pathway is commonly found in smokers.[15]
- Mutation in epidermal growth factor receptor (EGFR), particularly in-frame deletions are associated with never-smoking status, female gender, and East Asian ethnicity.[16]
- Focal amplifications of 14q13·3 are also frequent in adenocarcinoma of the lung, region coding for NKX2–1 (TTF1), a transcription factor crucial for development of the lung, thyroid, and brain.
- RBM10 mutation is more prevalent in men.
- Mutation in MGA, coding for a Max-interacting protein, which functions as a transcriptional repressor capable of blocking MYC-dependent transformation.[17]
- Some of the other recurrent somatic copy number alterations in lung adenocarcinoma include:
| Mutations | TP53, KRAS, EGFR, NF1, BRAF, MET, RIT |
| Fusions | ALK, ROS1, RET |
| SCNAs | Gains: NKX2-1, TERT, EGFR, MET, KRAS, ERBB2, MDM2 |
| Pathway alterations | RTK/RAS/RAF
mTOR, JAK-STAT, DNA repair, cell cycle regulation, epigenetic deregulation |
Environment
- Although genetics play a significant role in the pathogenesis of lung cancer, it is thought that exposure to environmental risk factors plays an equally important role in the development of lung cancer.
- The main causes of lung cancer include carcinogens (such as those present in tobacco smoke), ionizing radiation, and viral infections.
- Chronic exposure results in cumulative alterations to the DNA in the tissue lining the bronchi of the lungs (the bronchial epithelium).
- Irreversible DNA changes following exposure to carcinogens are directly associated with the development of lung cancer.[19]
Smoking
- Cigarette smoking is a leading cause of lung cancer.[20][21][22]
- Cigarette smoke contains over 60 known carcinogens including radioisotopes from the radon decay sequence, nitrosamine, and benzopyrene.
- Nicotine is thought to reduce the immune response to malignant growths in exposed tissue.
- The length of time an individual smokes, as well as the amount, significantly increases the person’s chance of developing lung cancer.
- Among individuals who stopped smoking, the risk of lung cancer steadily decreases as lung tissue repairs itself and as contaminant particles are eliminated from the lungs.
- It is thought that the risk of lung cancer among persons with a history of smoking (even when stopped) is always higher than those who never smoked.
Radon Gas
The association of radon gas exposure to lung cancer is described below.[23][24]
- Radon is a colorless and odorless gas generated by the breakdown of radioactive radium (decay product of uranium) found in the Earth’s crust. The radiation decay products ionize genetic material, causing mutations that sometimes turn cancerous.
- Radon exposure is the second major cause of lung cancer following smoking.
- The mechanism of lung damage following radon exposure is not thought to be due to the radon gas itself, but due to the short-lived alpha decay products that cause cellular damage and DNA mutations.
Asbestos
- Asbestos exposure is associated with many lung diseases, including lung cancer.[25]
- Tiny asbestos fibers are released into the air are breathed into the lungs. The fibers become lodged in the lungs and are stuck for an indefinite amount of time. They can eventually lead to scarring and inflammation.
Viruses
- Viruses known to be associated with the development of lung cancer in animals and humans include:[26][27][28][29][30][31]
- These viruses may affect the cell cycle and inhibit apoptosis, allowing uncontrolled cell division.
- HIV has also been thought to increase the risk of developing lung cancer. Although the mechanism is unknown, HIV is thought to be associated with a state of chronic lung inflammation that may potentiate cellular damage and DNA mutations.
Infection and Inflammation
- There may be a correlation between general inflammation of lung tissue and the development of lung cancers.[31]
- Neutrophils are released in response to bacterial infection and are considered to be the initial responders during inflammation.
- The hypothesis is that neutrophils may activate reactive oxygen or nitrogen species, which can bind to DNA and lead to genomic alterations. Accordingly, inflammation may be thought of as an initiator or promoter of lung cancer development. Also, tissue repair from inflammation is associated with cellular proliferation. During cellular proliferation there may be errors in chromosomal replication that can cause further DNA mutation.
- Angiogenesis, a significant process during tumor growth, may be promoted by chronic states of inflammation, which often require increased blood flow to sites of inflammation.
Gross Pathology

(Source: Libre pathology
- Adenocarcinoma of the lung may be preceded by morphological changes such as atypical adenomatous hypertrophy (AAH) in peripheral airway cells.
- AAH is a parenchymal lesion that arises in the alveoli close to terminal and respiratory bronchioles.
- AAH lesions are small and usually show incidental histological findings.
- They may be detected grossly, especially if they are 0.5 cm or larger.
- AAH is characterized by an alveolar structure lined by rounded, cuboidal, or low columnar cells.
- On gross pathology, peripheral multifocal lesions are characteristic findings in patients with adenocarcinoma of the lung.[32]
- Single or multiple solid firm yellow-white nodule or mass which may invade into the pleura and cause pleural retraction/puckering.
- Adenocarcinoma usually does not form a cavitary lesion.
- Adenocarcinoma may present as a diffuse pleural thickening resembling malignant mesothelioma.
Microscopic Pathology
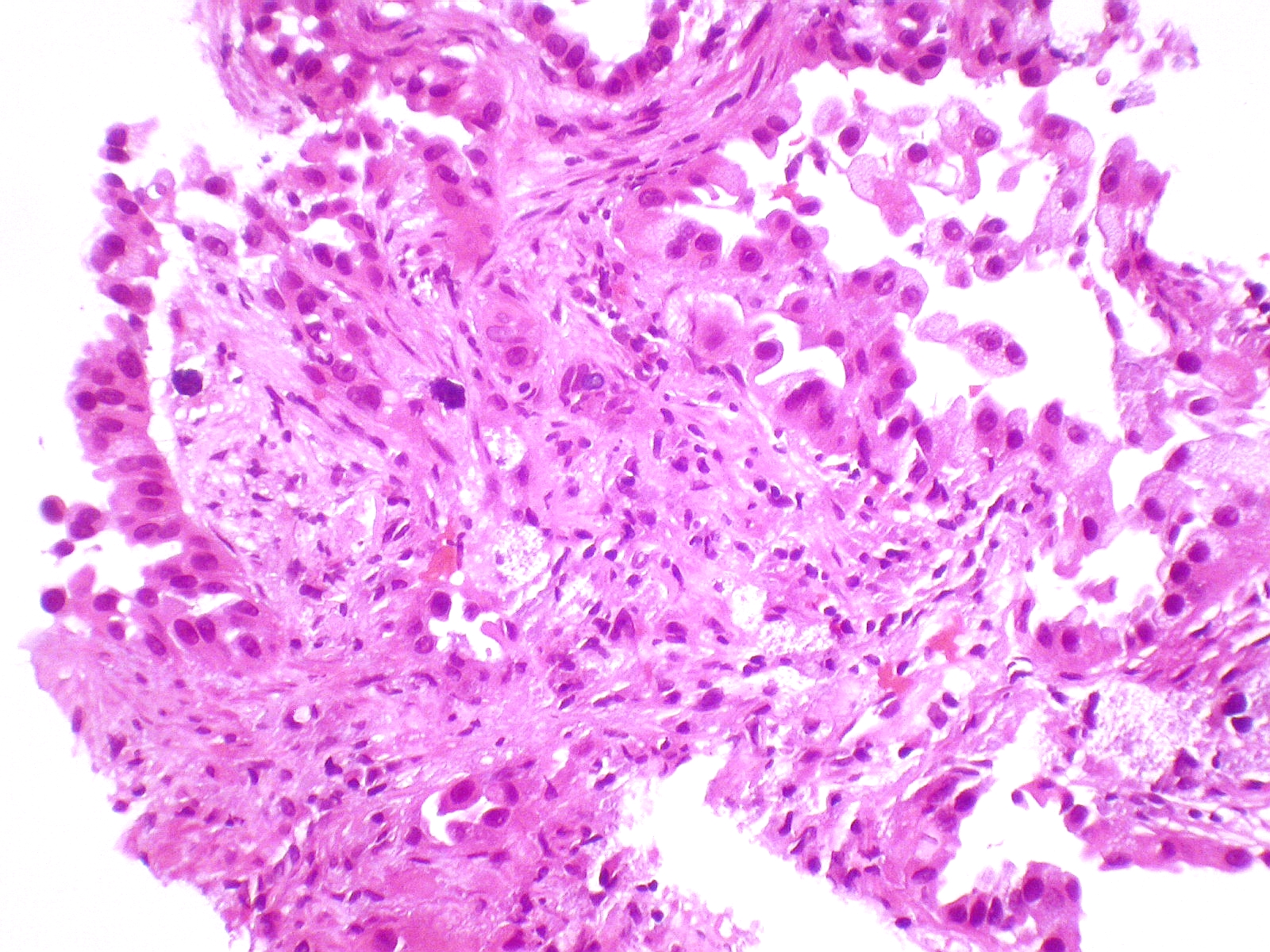
On microscopic histopathological analysis, nuclear atypia, eccentrically placed nuclei, abundant cytoplasm, and conspicuous nucleoli are characteristic findings of adenocarcinoma of the lung.
- Atypical adenomatous hyperplasia (AAH) is the precursor of peripheral adenocarcinomas. It consists of well demarcated columnar or cuboidal cells with the following features:[33][34]
- Varying degrees of cytologic atypia
- Hyperchromasia
- Pleomorphism
- Prominent nucleoli
- As adenocarcinoma is a derivative of mucus producing glands in the lungs, it tends to stain mucin positive.
- Based on differentiation, the tumor may be:
- Well differentiated (low grade): Normal appearance.
- Poorly differentiated (high grade): Abnormal glandular appearance with a positive mucin stain.
Histological Sub-types
- The IASLC/ATS/ERS lung adenocarcinoma histologic classification system was proposed in the Journal of Thoracic Oncology in 2011.[35]
- According to this new classification, tumor size ≤3 cm with pure lepidic pattern, but without lymphatic, vascular, pleural invasion or tumor necrosis was defined as adenocarcinoma in situ (AIS).
- If tumor size ≤3 cm with a lepidic predominant pattern and contained ≤5 mm stromal invasion it was defined as minimally invasive adenocarcinoma (MIA).
- If tumor had >5 mm stromal invasion it was defined as an invasive adenocarcinoma.
- Histologically adenocarcinoma is divided in to following subtypes:[36][37][38][39][40][41]
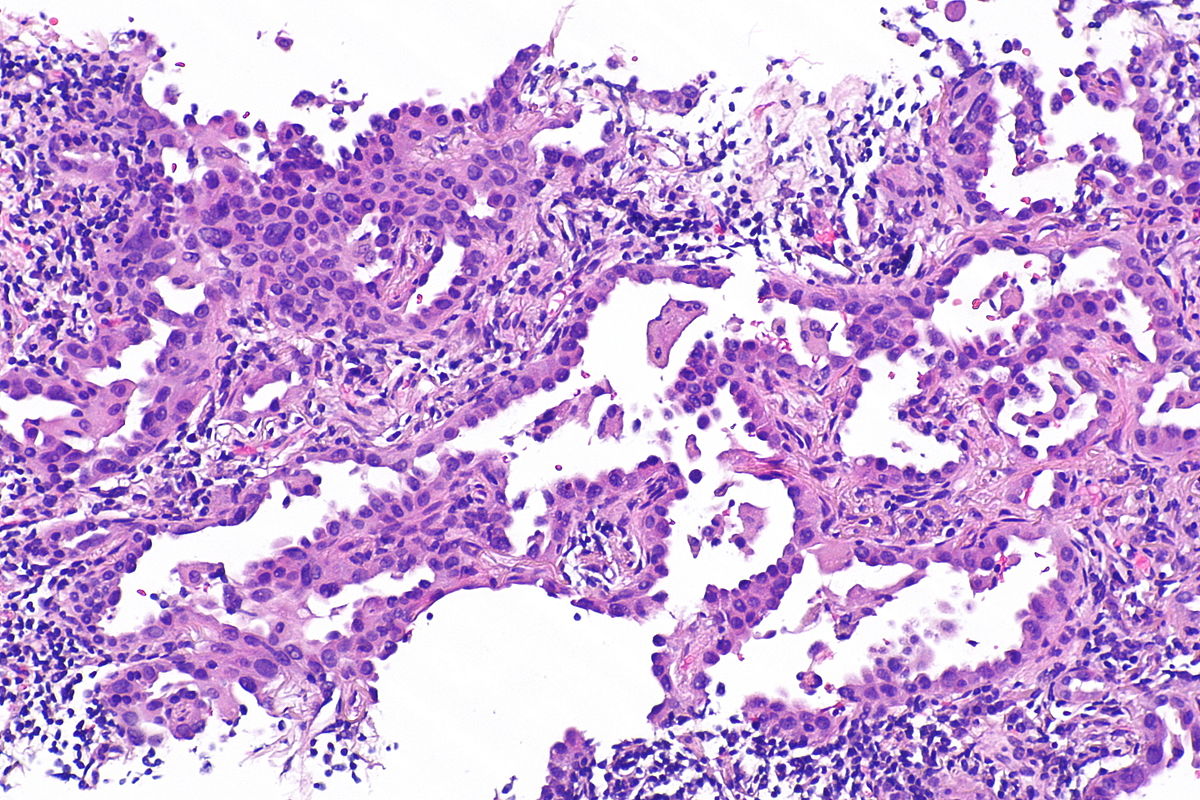
- Lepidic Adenocarcinoma:
Micrograph showing an invasive carcinoma with a few areas of lepidic growth lining alveoli.
Source: Pathology outlines- Lepidic growth adenocarcinoma is defined as tumor cells proliferating along the surface of intact alveolar walls without stromal or vascular invasion pathologically.
- Solitary adenocarcinomas with pure lepidic growth, termed “AIS” has 100% disease-specific survival, if the lesion is completely resected.
- Acinar Adenocarcinoma:
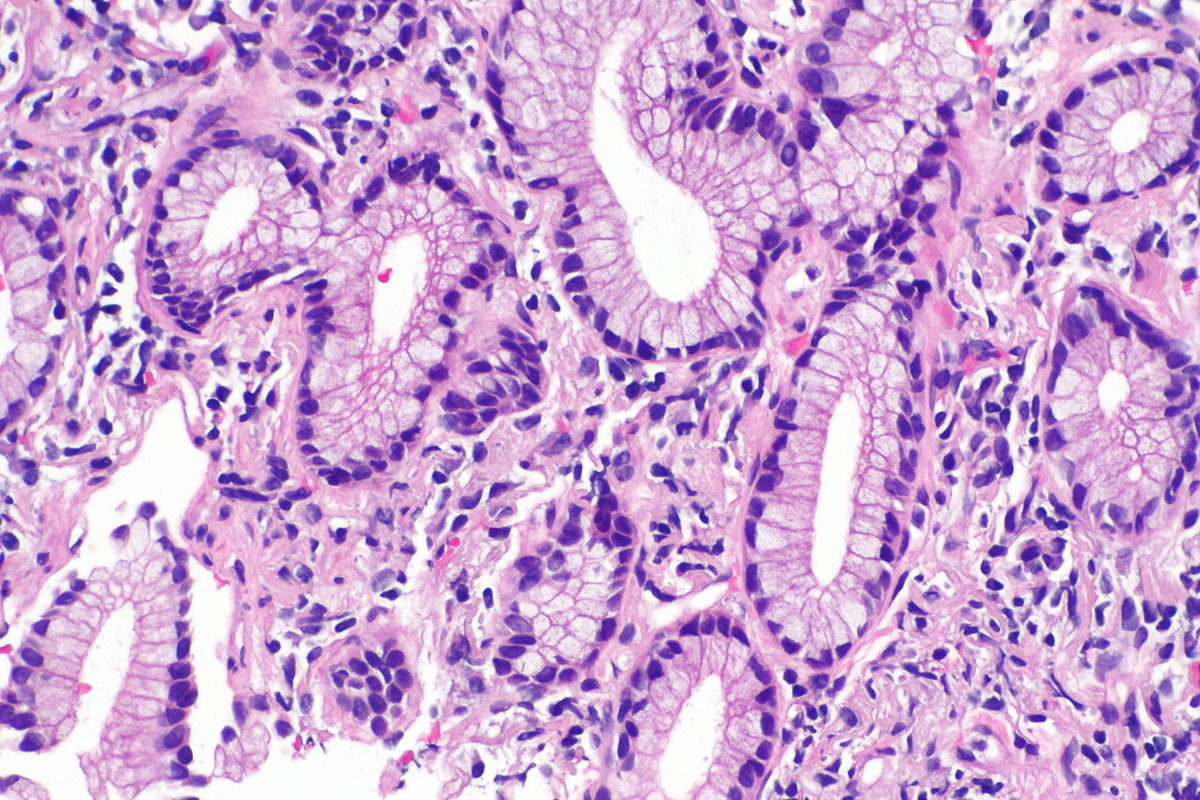
Micrograph showing an adenocarcinoma of the lung (acinar pattern), H&E stain.
Source: Libre pathology- Acinar pattern comprises infiltrating round to oval glands lined by tumor cells.
- Irregular-shaped glands.
- Malignant cells: Hyperchromatic nuclei, fibroblastic stroma.
- Sometimes the glandular cells and lumina may contain mucin.
- Papillary Adenocarcinoma:
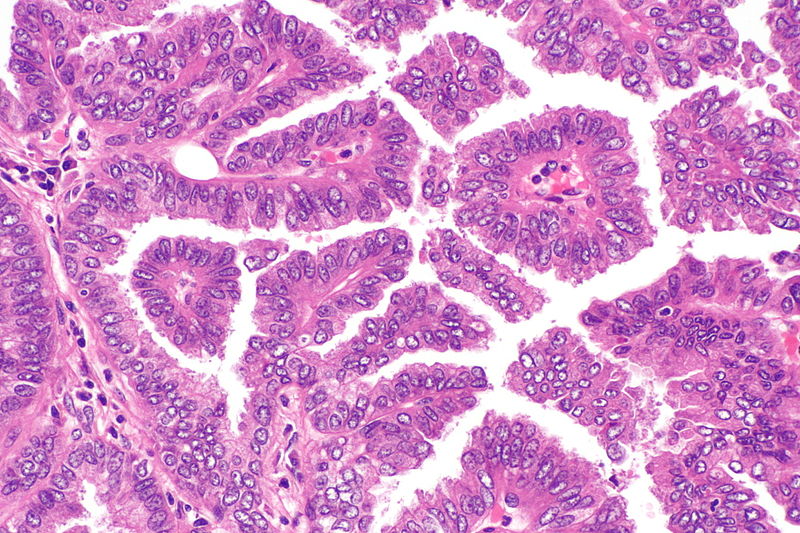
Micrograph showing papillary adenocarcinoma of the lung
Source: Libre pathology- The papillary pattern is composed of glandular tumour cells growing along fibrovascular cores.
- Papillae, necrosis, surrounding invasion, cuboidal to columnar epithelial lining, mucinous or non-mucinous.
- Lung adenocarcinomas with papillary growth show 2 types of papillary architecture:
- True papillary type: Papillae containing a layered glandular epithelium surrounded by fibrovascular core.
- Micropapillary type: The papillary tufts lack a central fibrovascular core and extensively shed within alveolar spaces.
- Micropapillary adenocarcinoma:
- The papillary tufts lack a central fibrovascular core and extensively shed within alveolar spaces.
- Micropapillary growth has been associated with an aggressive clinical course compared with traditional papillary adenocarcinoma.
- Micropapillary adenocarcinoma (MPA) may be often diagnosed at a high stage in nonsmokers, with intralobar satellites.
- Micropapillary adenocarcinoma frequently metastasizes to the contralateral lung, mediastinal lymph nodes, bone, and adrenal glands, with high mortality.
- Solid Adenocarcinoma:
- Cohesive cell cluster in a nest-like pattern without acinar polarity are the hallmark of the solid growth pattern.
- Solid adenocarcinoma consists of sheets of tumor cells with abundant cytoplasm and mostly vesicular nuclei with several conspicuous nucleoli.
- No acinar, papillary, or lepidic patterns are seen and there was no suggestion of mucin in tumor cell cytoplasm.
- Invasive Mucinous Adenocarcinoma:
Micrograph of mucinous adenocarcinoma of the lung, H&E stain.
Source: Libre pathology- Mixed invasive mucinous: Invasive mucinous adenocarcinoma demonstrates areas with lepidic, acinar, and papillary patterns.
- Fibrotic focus that contains invasive tumor with a desmoplastic stroma.
- The tumor consists of columnar cells filled with abundant mucin in the apical cytoplasm and shows small, basally oriented nuclei.
- Nonmucinous adenocarcinoma
- Mixed invasive mucinous: Invasive mucinous adenocarcinoma demonstrates areas with lepidic, acinar, and papillary patterns.
- Colloid Adenocarcinoma:
- This tumor consists of abundant pools of mucin growing within and distending airspaces.
- Well differentiated mucinous glandular epithelium along the surface of fibrous septa and within the pools of mucin.
- Tumor cells may be very inconspicuous.
- The surface of the fibrous wall may be lined by well-differentiated cuboidal or columnar mucinous epithelium.
- Fetal Adenocarcinoma:
- Fetal adenocarcinoma consists of malignant glandular cells growing in tubules and papillary structures with endometrioid morphology.
- Some tumor cells have prominent clear cytoplasm, and squamoid morules are present.
- Enteric Adenocarcinoma:
- Consists of an adenocarcinoma that morphologically resembles colonic adenocarcinoma with back-to-back angulated acinar structures.
- The tumor cells are cuboidal to columnar with nuclear pseudostratification.
- The tumor stains strongly for CDX-2.
- Minimally Invasive Adenocarcinoma (MIA)
- Nonmucinous (MIA):
- Mucinous (MIA):
- Mucinous MIA consists of a tumor showing lepidic growth and a small (0.5 cm) area of invasion.
- The tumor cells consist of mucinous columnar cells and pale cytoplasm resembling goblet cells growing mostly in a lepidic pattern along the surface of alveolar walls.
- The tumor invades the areas of stromal fibrosis in an acinar pattern.
- Low grade differentiation.
- Preinvasive Lesions
- Atypical adenomatous hyperplasia (AAH): Consists of atypical pneumocytes proliferating along alveolar walls.
- Non invasive.
- The slightly atypical pneumocytes are cuboidal and show gaps between the cells.
- Nuclei are hyperchromatic and may present with nuclear enlargement and multinucleation.
- Adenocarcinoma in situ (AIS)
- Nonmucinous (AIS): Tumor grows purely with a lepidic pattern.
- No foci of invasion or scarring is seen.
- It shows atypical pneumocytes proliferating along the thickened, but preserved, alveolar walls.
- Mucinous AIS: Consists of a nodular proliferation of mucinous columnar cells growing in a purely lepidic pattern.
- Although there is a small central scar, no stromal or vascular invasion is seen.
- The tumor cells consist of cuboidal to columnar cells with abundant apical mucin and small, basally oriented nuclei.
- Nonmucinous (AIS): Tumor grows purely with a lepidic pattern.
- Atypical adenomatous hyperplasia (AAH): Consists of atypical pneumocytes proliferating along alveolar walls.
- Lepidic Adenocarcinoma:




References
- ↑ Travis WD, Travis LB, Devesa SS (January 1995). “Lung cancer”. Cancer. 75 (1 Suppl): 191–202. doi:10.1002/1097-0142(19950101)75:1+<191::AID-CNCR2820751307>3.0.CO;2-Y. PMID 8000996.
- ↑ Mitchell, Richard Sheppard; Kumar, Vinay; Abbas, Abul K.; Fausto, Nelson. “Chapter 13, box on morphology of adenocarcinoma”. Robbins Basic Pathology (8th ed.). Philadelphia: Saunders. ISBN 1-4160-2973-7.
- ↑ Kanwal, Madiha; Ding, Xiao-Ji; Cao, Yi (2017). “Familial risk for lung cancer”. Oncology Letters. 13 (2): 535–542. doi:10.3892/ol.2016.5518. ISSN 1792-1074.
- ↑ Kadara, H.; Scheet, P.; Wistuba, I. I.; Spira, A. E. (2016). “Early Events in the Molecular Pathogenesis of Lung Cancer”. Cancer Prevention Research. 9 (7): 518–527. doi:10.1158/1940-6207.CAPR-15-0400. ISSN 1940-6207.
- ↑ Raso, Maria Gabriela; Wistuba, Ignacio I. (2007). “Molecular Pathogenesis of Early-Stage Non-small Cell Lung Cancer and a Proposal for Tissue Banking to Facilitate Identification of New Biomarkers”. Journal of Thoracic Oncology. 2 (7): S128–S135. doi:10.1097/JTO.0b013e318074fe42. ISSN 1556-0864.
- ↑ Wistuba II, Gazdar AF (2006). “Lung cancer preneoplasia”. Annu Rev Pathol. 1: 331–48. doi:10.1146/annurev.pathol.1.110304.100103. PMID 18039118.
- ↑ Devarakonda, Siddhartha; Morgensztern, Daniel; Govindan, Ramaswamy (2015). “Genomic alterations in lung adenocarcinoma”. The Lancet Oncology. 16 (7): e342–e351. doi:10.1016/S1470-2045(15)00077-7. ISSN 1470-2045.
- ↑ Kadara H, Scheet P, Wistuba II, Spira AE (July 2016). “Early Events in the Molecular Pathogenesis of Lung Cancer”. Cancer Prev Res (Phila). 9 (7): 518–27. doi:10.1158/1940-6207.CAPR-15-0400. PMID 27006378.
- ↑ Auerbach, Oscar; Stout, A. P.; Hammond, E. Cuyler; Garfinkel, Lawrence (1961). “Changes in Bronchial Epithelium in Relation to Cigarette Smoking and in Relation to Lung Cancer”. New England Journal of Medicine. 265 (6): 253–267. doi:10.1056/NEJM196108102650601. ISSN 0028-4793.
- ↑ Stewart, Bernard (2014). World cancer report 2014. Lyon, France Geneva, Switzerland: International Agency for Research on Cancer,Distributed by WHO Press, World Health Organization. ISBN 9283204298.
- ↑ Soda M, Choi YL, Enomoto M, Takada S, Yamashita Y, Ishikawa S; et al. (2007). “Identification of the transforming EML4-ALK fusion gene in non-small-cell lung cancer”. Nature. 448 (7153): 561–6. doi:10.1038/nature05945. PMID 17625570.
- ↑ Davies KD, Le AT, Theodoro MF, Skokan MC, Aisner DL, Berge EM; et al. (2012). “Identifying and targeting ROS1 gene fusions in non-small cell lung cancer”. Clin Cancer Res. 18 (17): 4570–9. doi:10.1158/1078-0432.CCR-12-0550. PMC 3703205. PMID 22919003.
- ↑ Stewart, Bernard (2014). World cancer report 2014. Lyon, France Geneva, Switzerland: International Agency for Research on Cancer,Distributed by WHO Press, World Health Organization. ISBN 9283204298.
- ↑ Weir, Barbara A.; Woo, Michele S.; Getz, Gad; Perner, Sven; Ding, Li; Beroukhim, Rameen; Lin, William M.; Province, Michael A.; Kraja, Aldi; Johnson, Laura A.; Shah, Kinjal; Sato, Mitsuo; Thomas, Roman K.; Barletta, Justine A.; Borecki, Ingrid B.; Broderick, Stephen; Chang, Andrew C.; Chiang, Derek Y.; Chirieac, Lucian R.; Cho, Jeonghee; Fujii, Yoshitaka; Gazdar, Adi F.; Giordano, Thomas; Greulich, Heidi; Hanna, Megan; Johnson, Bruce E.; Kris, Mark G.; Lash, Alex; Lin, Ling; Lindeman, Neal; Mardis, Elaine R.; McPherson, John D.; Minna, John D.; Morgan, Margaret B.; Nadel, Mark; Orringer, Mark B.; Osborne, John R.; Ozenberger, Brad; Ramos, Alex H.; Robinson, James; Roth, Jack A.; Rusch, Valerie; Sasaki, Hidefumi; Shepherd, Frances; Sougnez, Carrie; Spitz, Margaret R.; Tsao, Ming-Sound; Twomey, David; Verhaak, Roel G. W.; Weinstock, George M.; Wheeler, David A.; Winckler, Wendy; Yoshizawa, Akihiko; Yu, Soyoung; Zakowski, Maureen F.; Zhang, Qunyuan; Beer, David G.; Wistuba, Ignacio I.; Watson, Mark A.; Garraway, Levi A.; Ladanyi, Marc; Travis, William D.; Pao, William; Rubin, Mark A.; Gabriel, Stacey B.; Gibbs, Richard A.; Varmus, Harold E.; Wilson, Richard K.; Lander, Eric S.; Meyerson, Matthew (2007). “Characterizing the cancer genome in lung adenocarcinoma”. Nature. 450 (7171): 893–898. doi:10.1038/nature06358. ISSN 0028-0836.
- ↑ Rodenhuis S, Slebos RJ, Boot AJ, Evers SG, Mooi WJ, Wagenaar SS, van Bodegom PC, Bos JL (October 1988). “Incidence and possible clinical significance of K-ras oncogene activation in adenocarcinoma of the human lung”. Cancer Res. 48 (20): 5738–41. PMID 3048648.
- ↑ Imielinski M, Berger AH, Hammerman PS, Hernandez B, Pugh TJ, Hodis E, Cho J, Suh J, Capelletti M, Sivachenko A, Sougnez C, Auclair D, Lawrence MS, Stojanov P, Cibulskis K, Choi K, de Waal L, Sharifnia T, Brooks A, Greulich H, Banerji S, Zander T, Seidel D, Leenders F, Ansén S, Ludwig C, Engel-Riedel W, Stoelben E, Wolf J, Goparju C, Thompson K, Winckler W, Kwiatkowski D, Johnson BE, Jänne PA, Miller VA, Pao W, Travis WD, Pass HI, Gabriel SB, Lander ES, Thomas RK, Garraway LA, Getz G, Meyerson M (September 2012). “Mapping the hallmarks of lung adenocarcinoma with massively parallel sequencing”. Cell. 150 (6): 1107–20. doi:10.1016/j.cell.2012.08.029. PMC 3557932. PMID 22980975.
- ↑ Hurlin, Peter J.; Huang, Jie (2006). “The MAX-interacting transcription factor network”. Seminars in Cancer Biology. 16 (4): 265–274. doi:10.1016/j.semcancer.2006.07.009. ISSN 1044-579X.
- ↑ Devarakonda S, Morgensztern D, Govindan R (July 2015). “Genomic alterations in lung adenocarcinoma”. Lancet Oncol. 16 (7): e342–51. doi:10.1016/S1470-2045(15)00077-7. PMID 26149886.
- ↑ Dela Cruz CS, Tanoue LT, Matthay RA (2011). “Lung cancer: epidemiology, etiology, and prevention”. Clin. Chest Med. 32 (4): 605–44. doi:10.1016/j.ccm.2011.09.001. PMC 3864624. PMID 22054876.
- ↑ Morabia, Alfredo (2012). “Quality, originality, and significance of the 1939 “Tobacco consumption and lung carcinoma” article by Mueller, including translation of a section of the paper”. Preventive Medicine. 55 (3): 171–177. doi:10.1016/j.ypmed.2012.05.008. ISSN 0091-7435.
- ↑ Hecht, S (Oct 2003). “Tobacco carcinogens, their biomarkers and tobacco-induced cancer”. Nature Reviews. Cancer. Nature Publishing Group. 3 (10): 733–744. doi:10.1038/nrc1190. PMID 14570033. Retrieved 2007-08-10.
- ↑ Peto R, R (2006). Mortality from smoking in developed countries 1950–2000: Indirect estimates from National Vital Statistics. Oxford University Press. ISBN 0-19-262535-7. Retrieved 2007-08-10. Unknown parameter
|coauthors=ignored (help) - ↑ Catelinois, O (May 2006). “Lung Cancer Attributable to Indoor Radon Exposure in France: Impact of the Risk Models and Uncertainty Analysis”. Environmental Health Perspectives. National Institute of Environmental Health Science. 114 (9): 1361–1366. doi:10.1289/ehp.9070. PMID 16966089. Retrieved 2007-08-10. Unknown parameter
|coauthors=ignored (help) - ↑ University of Minnesota.http://enhs.umn.edu/hazards/hazardssite/radon/radonmolaction.html#Anchor-Molecular-23240/
- ↑ Järvholm, Bengt; Åström, Evelina (2014). “The Risk of Lung Cancer After Cessation of Asbestos Exposure in Construction Workers Using Pleural Malignant Mesothelioma as a Marker of Exposure”. Journal of Occupational and Environmental Medicine. 56 (12): 1297–1301. doi:10.1097/JOM.0000000000000258. ISSN 1076-2752.
- ↑ Leroux, C (Mar–Apr 2007). “Jaagsiekte Sheep Retrovirus (JSRV): from virus to lung cancer in sheep”. Veterinary Research. 38 (2): 211–228. PMID 17257570. Unknown parameter
|coauthors=ignored (help) - ↑ Palmarini, M (November 2001). “Retrovirus-induced ovine pulmonary adenocarcinoma, an animal model for lung cancer”. Journal of the National Cancer Institute. Oxford University Press. 93 (21): 1603–1614. PMID 11698564. Retrieved 2007-08-11. Unknown parameter
|coauthors=ignored (help) - ↑ Cheng, YW (Apr 2001). “The association of human papillomavirus 16/18 infection with lung cancer among nonsmoking Taiwanese women”. Cancer Research. American Association for Cancer Research. 61 (7): 2799–2803. PMID 11306446. Retrieved 2007-08-11. Unknown parameter
|coauthors=ignored (help) - ↑ Zheng, H (May 2007). “Oncogenic role of JC virus in lung cancer”. Journal of Pathology. 212 (3): 306–315. PMID 17534844. Unknown parameter
|coauthors=ignored (help) - ↑ Giuliani, L (Sep 2007). “Detection of oncogenic viruses (SV40, BKV, JCV, HCMV, HPV) and p53 codon 72 polymorphism in lung carcinoma”. Lung Cancer. 57 (3): 273–281. PMID 17400331. Unknown parameter
|coauthors=ignored (help) - ↑ 31.0 31.1 Eric A Engels.11/30/11. Inflammation in the development of lung cancer:epidemiological evidence.Expert Review of Anticancer Therapy.Apr.2008.p605
- ↑ Adenocarcinoma of the lung. Librepathology 2015. http://librepathology.org/wiki/index.php/File:Adenocarcinoma_%283950819000%29.jpg
- ↑ Kumar, Vinay (2007). Robbins basic pathology. Philadelphia, PA: Saunders/Elsevier. ISBN 1416029737.
- ↑ Stewart, Bernard (2014). World cancer report 2014. Lyon, France Geneva, Switzerland: International Agency for Research on Cancer,Distributed by WHO Press, World Health Organization. ISBN 9283204298.
- ↑ . doi:10.3978/j.issn.2072-1439.2014.09.13. Missing or empty
|title=(help) - ↑ Travis, William (2004). Pathology and genetics of tumours of the lung, pleura, thymus, and heart. Lyon: IARC Press. ISBN 9283224183.
- ↑ “www.jto.org”.
- ↑ Travis WD, Brambilla E, Noguchi M, Nicholson AG, Geisinger K, Yatabe Y, Ishikawa Y, Wistuba I, Flieder DB, Franklin W, Gazdar A, Hasleton PS, Henderson DW, Kerr KM, Nakatani Y, Petersen I, Roggli V, Thunnissen E, Tsao M (May 2013). “Diagnosis of lung adenocarcinoma in resected specimens: implications of the 2011 International Association for the Study of Lung Cancer/American Thoracic Society/European Respiratory Society classification”. Arch. Pathol. Lab. Med. 137 (5): 685–705. doi:10.5858/arpa.2012-0264-RA. PMID 22913371.
- ↑ Iwata H (September 2016). “Adenocarcinoma containing lepidic growth”. J Thorac Dis. 8 (9): E1050–E1052. doi:10.21037/jtd.2016.08.78. PMID 27747060.
- ↑ Jones KD (December 2013). “Whence lepidic?: the history of a Canadian neologism”. Arch. Pathol. Lab. Med. 137 (12): 1822–4. doi:10.5858/arpa.2013-0144-HP. PMID 23937575.
- ↑ Lin, Gengpeng; Xie, Canmao (2017). “PUB070 Acinar-Predominant Pattern Correlates with Poorer Outcome in Invasive Mucinous Adenocarcinoma of the Lung”. Journal of Thoracic Oncology. 12 (1): S1489. doi:10.1016/j.jtho.2016.11.2040. ISSN 1556-0864.
Causes
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Shanshan Cen, M.D. [2]
Overview
Genetic mutations are primarily responsible for the development of adenocarcinoma of the lung. Genetic mutations of EGFR (7p11), KRAS (12p12), BRAF (7q34), and PIK3CA (3q26) play a major role in the pathogenesis of adenocarcinoma.
Causes
- EGFR (7p11)
- KRAS (12p12)
- BRAF (7q34)
- PIK3CA (3q26)
- ERBB2 (17q12)
- Translocation EML4/ALK
- Tyrosine kinase fusions
- ALK (2p23), ROS1 (6q22), and RET (10q11)
References
- ↑ Stewart, Bernard (2014). World cancer report 2014. Lyon, France Geneva, Switzerland: International Agency for Research on Cancer,Distributed by WHO Press, World Health Organization. ISBN 9283204298.
- ↑ Stewart, Bernard (2014). World cancer report 2014. Lyon, France Geneva, Switzerland: International Agency for Research on Cancer,Distributed by WHO Press, World Health Organization. ISBN 9283204298.
- ↑ Soda M, Choi YL, Enomoto M, Takada S, Yamashita Y, Ishikawa S; et al. (2007). “Identification of the transforming EML4-ALK fusion gene in non-small-cell lung cancer”. Nature. 448 (7153): 561–6. doi:10.1038/nature05945. PMID 17625570.
- ↑ Davies KD, Le AT, Theodoro MF, Skokan MC, Aisner DL, Berge EM; et al. (2012). “Identifying and targeting ROS1 gene fusions in non-small cell lung cancer”. Clin Cancer Res. 18 (17): 4570–9. doi:10.1158/1078-0432.CCR-12-0550. PMC 3703205. PMID 22919003.
Differentiating Adenocarcinoma of the Lung from other Diseases
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Shanshan Cen, M.D. [2]
Overview
Adenocarcinoma of the lung must be differentiated from atypical adenomatous hyperplasia of the lung, adenocarcinoma in situ, squamous cell carcinoma of the lung, small cell carcinoma of the lung, malignant mesothelioma, and metastatic adenocarcinoma.
Differentiating Adenocarcinoma of the Lung from other Diseases
Adenocarcinoma of the lung must be differentiated from:[1]
- Atypical adenomatous hyperplasia of the lung
- Adenocarcinoma in situ
- Squamous cell carcinoma of the lung
- Small cell carcinoma of the lung
- Malignant mesothelioma
- Metastatic adenocarcinoma
- Colorectal adenocarcinoma
- Breast adenocarcinoma
- Invasive ductal carcinoma of the breast
- Invasive lobular carcinoma
- Amyloidosis
- Pulmonary tuberculosis
- Non-Hodgkin’s lymphoma (NHL)
- Hodgkin’s lymphoma
- Thymoma
- Tracheal tumors
- Thyroid mass
- Arteriovenous malformation
- Wegener’s granulomatosis
- Sarcoidosis
- Lung abscess[2]
- Pneumonia
- Fungal infection
- Chronic eosinophilic pneumonia[3]
Differentiating Lung Cancer from Other Diseases
Lung cancer must be differentiated from other cavitary lung lesions. The table below summarizes the differentiation:
| Causes of
lung cavities |
Differentiating Features | Differentiating radiological findings | Diagnosis
confirmation |
|---|---|---|---|
|
|
| |
|
|
|
|
|
|
| |
|
|
|
|
|
|
| |
|
|
| |
|
|
||
|
|
| |
|
|
|
The following table summarizes the differentiation of various lung tumors based on histological and topographical features:[17]
| Abrevations:
HPV: human papillomavirus; CEA: Carcino embryogenic antigen; TTF1: Thyroid transcription factor-1; EMA: Epithelial membrane antigen; CK: Cyto keratin; CD: Cluster differentiation; NCAM: Neural Cell Differentiation Molecule; MMP’s: Mettaloprotineases matrix ; GFAP: Glial fibrocilliary acid protein | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Benign Lung Tumors[18] | ||||||||||
| Benign lung tumor | Risk/Epidemiology | Pleuripotent cells | Topography | Gross | Histology | Immunohistochemistry | Imaging | Metastasis | ||
| Papilloma[19] | Squamous cell papilloma |
|
|
|
|
|
| |||
| Glandular papilloma |
|
|
|
|
|
|
| |||
| Adenoma[20] | Alveolar adenoma |
|
|
|
|
|
|
| ||
| Papillary adenoma[21] |
|
|
|
|
|
|
|
| ||
| Mucinous cystadenoma |
|
|
|
|
|
|
|
| ||
| Malignant Lung Tumors[22] | ||||||||||
| Variants of lung carcinoma | Risk Factors/Epidemiology | Pleuripotent cell | Topography | Gross | Histology | Immunohistochemistry | Imaging | Metastasis | ||
| Squamous cell carcinoma (SCC)[23] | Papillary |
|
|
|
|
|
|
|||
| Clear cell |
| |||||||||
| Basaloid |
| |||||||||
| Small cell carcinoma[24] |
|
|
|
|
|
| ||||
| Adenocarcinoma[25][26][27] | Acinar adenocarcinoma |
|
|
|
|
|
Aerogenous spread is characteristic
| |||
| Papillary adenocarcinoma |
| |||||||||
| Bronchio-alveolar carcinoma | Non-mucinous | |||||||||
| Mucinous |
| |||||||||
| Mixed non-mucinous and mucinous or indeterminate |
| |||||||||
| Solid adenocarcinoma with mucin production | Fetal adenocarcinoma |
| ||||||||
| Mucinous (“colloid”) carcinoma |
| |||||||||
| Mucinous cystadenocarcinoma |
| |||||||||
| Signet ring adenocarcinoma |
| |||||||||
| Clear cell adenocarcinoma |
| |||||||||
| Variants of lung carcinoma | Risk Factors/Epidemiology | Pleuripotent cell | Topography | Gross | Histology | Immunohistochemistry | Imaging | Metastasis | ||
| Large cell carcinoma[28] | Basaloid large cell carcinoma of the lung |
|
|
|
|
|
|
| ||
| Clear cell carcinoma of the lung | ||||||||||
| Lymphoepithelioma-like carcinoma of the lung |
| |||||||||
| Large-cell lung carcinoma with rhabdoid phenotype |
| |||||||||
| Mixed type |
| |||||||||
| Variants of lung carcinoma | Risk Factors/Epidemiology | Pleuripotent cell | Topography | Gross | Histology | Immunohistochemistry | Imaging | Metastasis | ||
| Sarcomatoid carcinoma[29] | Carcinosarcoma |
|
|
|
|
|
|
|||
| Spindle cell carcinoma |
|
|||||||||
| Giant cell carcinoma |
| |||||||||
| Pleomorphic carcinoma |
| |||||||||
| Pulmonary blastoma |
|
| ||||||||
| Variants of lung carcinoma | Risk Factors/Epidemiology | Pleuripotent cell | Topography | Gross | Histology | Immunohistochemistry | Imaging | Metastasis | ||
| Carcinoid tumor[30] | Typical carcinoid
Atypical carcinoid |
|
|
|
|
|
|
|||
| Salivary gland tumors[31] | Mucoepidermoid carcinoma |
|
|
|
|
|
|
| ||
| Adenoid cystic carcinoma |
|
|
|
|
|
|||||
| Epithelial-myoepithelial carcinoma |
|
|
|
|
|
|||||
| Variants of lung carcinoma | Risk Factors/Epidemiology | Pleuripotent cell | Topography | Gross | Histology | Immunohistochemistry | Imaging | Metastasis | ||
| Preinvasive lesions[32] | Squamous carcinoma in situ |
|
|
|
|
|
||||
| Atypical adenomatous hyperplasia |
|
|
|
|
| |||||
| Diffuse idiopathic pulmonary neuroendocrine cell hyperplasia |
|
|
|
| ||||||
| Variants of lung carcinoma | Risk Factors/Epidemiology | Pleuripotent cell | Topography | Gross | Histology | Immunohistochemistry | Imaging | Metastasis | ||
| Mesenchymal tumors[33] | Epithelioid haemangioendothelioma / Angiosarcoma |
|
|
|
|
|
||||
| Pleuropulmonary blastoma |
|
|
|
|
|
|||||
| Chondroma |
|
|
|
|
|
|
|
| ||
| Congenital peribronchial myofibroblastic tumor |
|
|
|
|
|
| ||||
| Diffuse pulmonary lymphangiomatosis |
|
|
|
|
|
| ||||
| Inflammatory myofibroblastic tumor |
|
|
|
|
|
| ||||
| Pulmonary artery sarcoma |
|
|
|
|
|
|
| |||
| Pulmonary vein sarcoma |
|
|
|
| ||||||
The following table summarizes the differentiation of lung cancer from other disease entities with similar presentation.[4][5][7][34][15]
| Disease | Clinical features
Signs & symptoms |
Radiological Findings | Characterstic feature | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Fever | Cough | Hemoptysis | Dyspnea | Chest pain | Weight loss | Night sweats | |||||
| High-grade | Low grade | Productive | Dry | ||||||||
| Acute Lung abscess | + | – | + | – | – | – | + | – | – |
|
|
| Malignancy | – | + | – | + | + | – | – | + | + |
|
|
| Pulmonary Tuberculosis | + | – | + | – | + | – | – | – | + |
|
|
| Necrotizing Pneumonia | + | – | + | + | – | + | – | – |
|
| |
| Empyema | + | – | + | – | + | + | + | – | – |
|
|
| Bronchiectasis | – | – | + | – | + | – | – | – | – |
|
|
| Wegners granulomatosis | – | – | + | + | + | – | – | – |
| ||
| Sarcoidosis | + | – | + | – | + | – | – | + | + |
|
|
| Rheumatoid nodule | – | – | – | – | – | + | – | + | – |
|
|
| Langerhans cell Histiocytosis | – | – | – | – | – | + | + | + | – |
|
|
| Bronchiolitis obliterans | – | – | + | – | + | + | + | – | – |
|
|
References
- ↑ Adenocarcinoma of the lung. Librepathology 2015. http://librepathology.org/wiki/index.php/Adenocarcinoma_of_the_lung
- ↑ Kamiya K, Yoshizu A, Misumi Y, Hida N, Okamoto H, Yoshida S (2011). “[Lung abscess which needed to be distinguished from lung cancer; report of a case]”. Kyobu Geka. 64 (13): 1204–7. PMID 22242302.
- ↑ Matsuoka T, Uematsu H, Iwakiri S, Itoi K (2013). “[Chronic eosinophilic pneumonia presenting as a solitary nodule, suspicious of lung cancer;report of a case]”. Kyobu Geka. 66 (10): 941–3. PMID 24008649.
- ↑ 4.0 4.1 4.2 Chaudhuri MR (1973). “Primary pulmonary cavitating carcinomas”. Thorax. 28 (3): 354–66. PMC 470041. PMID 4353362.
- ↑ 5.0 5.1 Mouroux J, Padovani B, Elkaïm D, Richelme H (1996). “Should cavitated bronchopulmonary cancers be considered a separate entity?”. Ann. Thorac. Surg. 61 (2): 530–2. doi:10.1016/0003-4975(95)00973-6. PMID 8572761.
- ↑ Onn A, Choe DH, Herbst RS, Correa AM, Munden RF, Truong MT, Vaporciyan AA, Isobe T, Gilcrease MZ, Marom EM (2005). “Tumor cavitation in stage I non-small cell lung cancer: epidermal growth factor receptor expression and prediction of poor outcome”. Radiology. 237 (1): 342–7. doi:10.1148/radiol.2371041650. PMID 16183941.
- ↑ 7.0 7.1 7.2 Langford CA, Hoffman GS (1999). “Rare diseases.3: Wegener’s granulomatosis”. Thorax. 54 (7): 629–37. PMC 1745525. PMID 10377211.
- ↑ Lee KS, Kim TS, Fujimoto K, Moriya H, Watanabe H, Tateishi U, Ashizawa K, Johkoh T, Kim EA, Kwon OJ (2003). “Thoracic manifestation of Wegener’s granulomatosis: CT findings in 30 patients”. Eur Radiol. 13 (1): 43–51. doi:10.1007/s00330-002-1422-2. PMID 12541109.
- ↑ Baughman RP, Teirstein AS, Judson MA, Rossman MD, Yeager H, Bresnitz EA, DePalo L, Hunninghake G, Iannuzzi MC, Johns CJ, McLennan G, Moller DR, Newman LS, Rabin DL, Rose C, Rybicki B, Weinberger SE, Terrin ML, Knatterud GL, Cherniak R (2001). “Clinical characteristics of patients in a case control study of sarcoidosis”. Am. J. Respir. Crit. Care Med. 164 (10 Pt 1): 1885–9. doi:10.1164/ajrccm.164.10.2104046. PMID 11734441.
- ↑ Brauner MW, Grenier P, Mompoint D, Lenoir S, de Crémoux H (1989). “Pulmonary sarcoidosis: evaluation with high-resolution CT”. Radiology. 172 (2): 467–71. doi:10.1148/radiology.172.2.2748828. PMID 2748828.
- ↑ Murphy J, Schnyder P, Herold C, Flower C (1998). “Bronchiolitis obliterans organising pneumonia simulating bronchial carcinoma”. Eur Radiol. 8 (7): 1165–9. doi:10.1007/s003300050527. PMID 9724431.
- ↑ 12.0 12.1 Al-Ghanem S, Al-Jahdali H, Bamefleh H, Khan AN (2008). “Bronchiolitis obliterans organizing pneumonia: pathogenesis, clinical features, imaging and therapy review”. Ann Thorac Med. 3 (2): 67–75. doi:10.4103/1817-1737.39641. PMC 2700454. PMID 19561910.
- ↑ Cordier JF, Loire R, Brune J (1989). “Idiopathic bronchiolitis obliterans organizing pneumonia. Definition of characteristic clinical profiles in a series of 16 patients”. Chest. 96 (5): 999–1004. PMID 2805873.
- ↑ Lee KS, Kullnig P, Hartman TE, Müller NL (1994). “Cryptogenic organizing pneumonia: CT findings in 43 patients”. AJR Am J Roentgenol. 162 (3): 543–6. doi:10.2214/ajr.162.3.8109493. PMID 8109493.
- ↑ 15.0 15.1 Suri HS, Yi ES, Nowakowski GS, Vassallo R (2012). “Pulmonary langerhans cell histiocytosis”. Orphanet J Rare Dis. 7: 16. doi:10.1186/1750-1172-7-16. PMC 3342091. PMID 22429393.
- ↑ Moore AD, Godwin JD, Müller NL, Naidich DP, Hammar SP, Buschman DL, Takasugi JE, de Carvalho CR (1989). “Pulmonary histiocytosis X: comparison of radiographic and CT findings”. Radiology. 172 (1): 249–54. doi:10.1148/radiology.172.1.2787035. PMID 2787035.
- ↑ Erasmus JJ, Connolly JE, McAdams HP, Roggli VL (2000). “Solitary pulmonary nodules: Part I. Morphologic evaluation for differentiation of benign and malignant lesions”. Radiographics. 20 (1): 43–58. doi:10.1148/radiographics.20.1.g00ja0343. PMID 10682770.
- ↑ Gümüştaş S, Inan N, Akansel G, Ciftçi E, Demirci A, Ozkara SK (June 2012). “Differentiation of malignant and benign lung lesions with diffusion-weighted MR imaging”. Radiol Oncol. 46 (2): 106–13. doi:10.2478/v10019-012-0021-3. PMC 3472932. PMID 23077446.
- ↑ Maxwell RJ, Gibbons JR, O’Hara MD (January 1985). “Solitary squamous papilloma of the bronchus”. Thorax. 40 (1): 68–71. PMC 459982. PMID 3969658.
- ↑ Shiota Y, Matsumoto H, Sasaki N, Taniyama K, Hashimoto S, Sueishi K (1998). “Solitary bronchioloalveolar adenoma of the lung”. Respiration. 65 (6): 483–5. doi:10.1159/000029319. PMID 9817965.
- ↑ Kanchustambham V, Saladi S, Patolia S, Mahmoud Assaf S, Stoeckel D (March 2017). “A Rare Case of a Benign Primary Pleomorphic Adenoma of the Lung”. Cureus. 9 (3): e1069. doi:10.7759/cureus.1069. PMC 5375953. PMID 28409070.
- ↑ Kelley LC, Puette M, Langheinrich KA, King B (November 1994). “Bovine pulmonary blastomas: histomorphologic description and immunohistochemistry”. Vet. Pathol. 31 (6): 658–62. doi:10.1177/030098589403100605. PMID 7863581.
- ↑ Roth E, Smidt D (January 1970). “[Studies on early ejaculate collection using electroejaculation in German improved land-swines and Goettinger miniature pigs]”. Berl. Munch. Tierarztl. Wochenschr. (in German). 83 (1): 7–11. PMID 5528918.
- ↑ Jackman DM, Johnson BE (2005). “Small-cell lung cancer”. Lancet. 366 (9494): 1385–96. doi:10.1016/S0140-6736(05)67569-1. PMID 16226617.
- ↑ Mitchell, Richard Sheppard; Kumar, Vinay; Abbas, Abul K.; Fausto, Nelson. “Chapter 13, box on morphology of adenocarcinoma”. Robbins Basic Pathology (8th ed.). Philadelphia: Saunders. ISBN 1-4160-2973-7.
- ↑ Soda M, Choi YL, Enomoto M, Takada S, Yamashita Y, Ishikawa S; et al. (2007). “Identification of the transforming EML4-ALK fusion gene in non-small-cell lung cancer”. Nature. 448 (7153): 561–6. doi:10.1038/nature05945. PMID 17625570.
- ↑ Adenocarcinoma of the lung. Librepathology 2015. http://librepathology.org/wiki/index.php/File:Adenocarcinoma_%283950819000%29.jpg
- ↑ Rossi G, Mengoli MC, Cavazza A, Nicoli D, Barbareschi M, Cantaloni C, Papotti M, Tironi A, Graziano P, Paci M, Stefani A, Migaldi M, Sartori G, Pelosi G (January 2014). “Large cell carcinoma of the lung: clinically oriented classification integrating immunohistochemistry and molecular biology”. Virchows Arch. 464 (1): 61–8. doi:10.1007/s00428-013-1501-6. PMID 24221342.
- ↑ Huang SY, Shen SJ, Li XY (October 2013). “Pulmonary sarcomatoid carcinoma: a clinicopathologic study and prognostic analysis of 51 cases”. World J Surg Oncol. 11: 252. doi:10.1186/1477-7819-11-252. PMC 3850921. PMID 24088577.
- ↑ Dahabreh J, Stathopoulos GP, Koutantos J, Rigatos S (March 2009). “Lung carcinoid tumor biology: treatment and survival”. Oncol. Rep. 21 (3): 757–60. PMID 19212636.
- ↑ Elnayal A, Moran CA, Fox PS, Mawlawi O, Swisher SG, Marom EM (July 2013). “Primary salivary gland-type lung cancer: imaging and clinical predictors of outcome”. AJR Am J Roentgenol. 201 (1): W57–63. doi:10.2214/AJR.12.9579. PMC 3767141. PMID 23789697.
- ↑ Greenberg AK, Yee H, Rom WN (2002). “Preneoplastic lesions of the lung”. Respir. Res. 3: 20. PMC 107849. PMID 11980589.
- ↑ Koenigkam-Santos M, Sommer G, Puderbach M, Safi S, Schnabel PA, Kauczor HU, Heussel CP (April 2014). “Primary intrathoracic malignant mesenchymal tumours: computed tomography features of a rare group of chest neoplasms”. Insights Imaging. 5 (2): 237–44. doi:10.1007/s13244-013-0306-0. PMC 3999366. PMID 24407922.
- ↑ Langford CA, Hoffman GS (1999). “Rare diseases.3: Wegener’s granulomatosis”. Thorax. 54 (7): 629–37. PMC 1745525. PMID 10377211.
Epidemiology and Demographics
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Shanshan Cen, M.D. [2]
Overview
The incidence of adenocarcinoma of the lung is approximately 22.1 per 100,000 individuals worldwide. Adenocarcinoma of the lung affects men and women equally. Patients of all age groups may develop adenocarcinoma of the lung.
Epidemiology and Demographics
Incidence
- The incidence of adenocarcinoma of the lung is approximately 22.1 per 100,000 individuals worldwide.[1]
Prevalence
- Presently, adenocarcinoma is the most common histological subtype of lung cancer as it accounts for forty percent of all lung cancers.[1]
- It is more common in individuals who smoke fewer than 100 cigarettes in their lifetimes.
- To view more epidemiological information among patients of lung cancer, please click Here.
Age
Gender
- Adenocarcinoma of the lung affects men and women equally.[2]
Developed Countries
- Adenocarcinoma of the lung is more common in developed countries and is currently the most common subtype in lifelong nonsmokers and smokers.[1]
References
- ↑ 1.0 1.1 1.2 Adenocarcinoma of the lung. Wikipedia 2015. https://en.wikipedia.org/wiki/Adenocarcinoma_of_the_lung#Epidemiology
- ↑ 2.0 2.1 Paris C, Clement-Duchene C, Vignaud JM, Gislard A, Stoufflet A, Bertrand O; et al. (2010). “Relationships between lung adenocarcinoma and gender, age, smoking and occupational risk factors: A case-case study”. Lung Cancer. 68 (2): 146–53. doi:10.1016/j.lungcan.2009.06.007. PMID 19586681.
Risk Factors
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Shanshan Cen, M.D. [2]
Overview
Common risk factors in the development of adenocarcinoma of the lung are smoking, family history of lung cancer, high levels of air pollution, radiation therapy to the chest, radon gas, asbestos, occupational exposure to chemical carcinogens, and previous lung disease.
Risk Factors
- Common risk factors in the development of adenocarcinoma of the lung include smoking, family history of lung cancer, radiation therapy to the chest and asbestos exposure.
Common Risk Factors
- Common risk factors in the development of adenocarcinoma of the lung may be occupational, environmental, or constitutional.
- Common risk factors in the development of adenocarcinoma of the lung include:[1]
- Smoking[2][3]
- Second-hand smoke[4][5]
- Family history of lung cancer
- High levels of air pollution
- Radiation therapy to the chest
- Radon gas
- Asbestos
- High levels of arsenic in drinking water
- Occupational exposure to chemical carcinogens
- Previous lung disease
- Indoor burning of coal
- Weakened immune system
- Lupus
- Pre-existing scars
- Pre-existing wounds
- Inflammation
Smoking
- Cigarette smoking is the leading cause of lung cancer.
- Both active and passive smoking are associated with increased risk of lung cancer.
- The risk of lung cancer is associated with increased quantity as well as increased duration of smoking.
- There is no evidence to suggest that smoking low-tar cigarettes lowers the risk.
- Recently introduced e-cigarrettes, which were thought to be risk-free were recently demonstrated to be also associated with a significantly increased risk of lung cancer due to the presence of formaldehyde.[6]
- Smoking accounts for 87% of lung cancer cases in the US. The lag period between smoking and death due to lung cancer is 20 years.[7]
Second-hand smoke
- Second-hand smoke is exhaled by smokers. It is also known as involuntary, passive smoking or environmental tobacco smoke (ETS).[8]
- Acitvely inhaled smoke and second-hand smoke contain the same chemicals.
- Exposure to second-hand smoke increases risk of developing lung cancer.
- Second-hand smoke is a major risk factor for lung cancer among non-smokers.
- Even small amounts of exposure to second hand smoke is considered unsafe.[9]
Air Pollution
- Emissions from automobiles, factories and power plants may increase predisposition of individuals to lung cancer.[10]
- Individual components of air pollution which include diesel engine exhaust, particulate matter, benzene, and some polycyclic aromatic hydrocarbons (PAHs) are considered particularly harmful in individuals.[11]
Family History of Lung Cancer
- Family history of lung cancer may increase the risk of developing lung cancer in individuals.[12]
- First-degree relatives of lung cancer patients are always considered high-risk.
Radiation Therapy to the Chest
- DNA mutations and cellular damage due to radiation therapy may increase individual predisposition to lung cancer.
- Previous exposure to ionizing radiation may increase individual risk of developing lung cancer.
- Radiation therapy for Hodgkin lymphoma or breast cancer is associated with development of lung cancer.
Radon Exposure
- Radon exposure increases the risk of lung cancer. Radon is the leading cause of lung cancer in non-smokers and the second leading cause of lung cancer in smokers.
- Radon comes from the natural breakdown of uranium in rocks and soil and may reach unsafe levels in enclosed, poorly ventilated homes or buildings due to seepage into the basement.
- The risk of developing lung cancer depends on degree of exposure, duration of exposure and smoking history. The risk is much higher in smokers.
Asbestos Exposure[13]
- The risk of asbestos exposure is highest for miners or those involved in manufacturing.
- Studies have shown that the combination of smoking and asbestos exposure is extremely hazardous.
Exposure to Other Chemical Carcinogens[14]
Exposure to chemical carcinogens may be particularly harmful and predispose to the development of lung adenocarcinoma.
- Arsenic and inorganic arsenic compounds
- Beryllium and beryllium compounds
- Cadmium and cadmium compounds
- Chemicals used in rubber manufacturing, iron and steel founding and painting
- Chloromethyl ethers and bischloromethylether
- Chromium (VI) compounds
- Cobalt-tungsten carbide
- Diesel engine exhaust
- Mustard gas
- Polycyclic aromatic hydrocarbons (PAHs)
- Radioactive ores such as uranium and plutonium
- Silica dust and crystalline silica
- Some nickel compounds
Less Common Risk Factors
- Less common risk factors in the development of adenocarcinoma of the lung include:[15]
- Marijuana use
- Indoor burning of wood
- High-temperature frying
- Meat diet
- Physical inactivity
- Occupational exposure to certain chemicals
- Occupational exposure to vinyl chloride, dioxin, cobalt-tungsten carbide, or strong inorganic acid mists
- Removal of both ovaries
References
- ↑ Lung cancer. Canadian Cancer Society 2015. http://www.cancer.ca/en/cancer-information/cancer-type/lung/risks/?region=ab#Outdoor_air_pollution
- ↑ CDC (Dec 1986). “1986 Surgeon General’s report: the health consequences of involuntary smoking”. CDC. PMID 3097495. Retrieved 2007-08-10.
* National Research Council (1986). Environmental tobacco smoke: measuring exposures and assessing health effects. National Academy Press. ISBN 0-309-07456-8.
* Template:Cite paper
* California Environmental Protection Agency (1997). “Health effects of exposure to environmental tobacco smoke”. Tobacco Control. 6 (4): 346–353. PMID 9583639. Retrieved 2007-08-10.
* CDC (Dec 2001). “State-specific prevalence of current cigarette smoking among adults, and policies and attitudes about secondhand smoke—United States, 2000”. Morbidity and Mortality Weekly Report. CDC. 50 (49): 1101–1106. PMID 11794619. Retrieved 2007-08-10.
* Alberg, AJ (Jan 2003). “Epidemiology of lung cancer”. Chest. American College of Chest Physicians. 123 (S1): 21S–49S. PMID 12527563. Retrieved 2007-08-10. Unknown parameter|coauthors=ignored (help) - ↑ Boffetta, P (Oct 1998). “Multicenter case-control study of exposure to environmental tobacco smoke and lung cancer in Europe”. Journal of the National Cancer Institute. Oxford University Press. 90 (19): 1440–1450. PMID 9776409. Retrieved 2007-08-10. Unknown parameter
|coauthors=ignored (help) - ↑ “Report of the Scientific Committee on Tobacco and Health”. Department of Health. Mar 1998. Retrieved 2007-07-09.
* Hackshaw, AK (Jun 1998). “Lung cancer and passive smoking”. Statistical Methods in Medical Research. 7 (2): 119–136. PMID 9654638. - ↑ Template:Cite paper
- ↑ Jensen RP, Luo W, Pankow JF, Strongin RM, Peyton DH (2015). “Hidden formaldehyde in e-cigarette aerosols”. N Engl J Med. 372 (4): 392–4. doi:10.1056/NEJMc1413069. PMID 25607446.
- ↑ Samet, JM (May 1988). “Cigarette smoking and lung cancer in New Mexico”. American Review of Respiratory Disease. 137 (5): 1110–1113. PMID 3264122. Unknown parameter
|coauthors=ignored (help) - ↑ Lung cancer. Canadian Cancer Society 2015. http://www.cancer.ca/en/cancer-information/cancer-type/lung/risks/?region=ab#Outdoor_air_pollution
- ↑ Lung cancer. Canadian Cancer Society 2015. http://www.cancer.ca/en/cancer-information/cancer-type/lung/risks/?region=ab#Outdoor_air_pollution
- ↑ Parent, ME (Jan 2007). “Exposure to diesel and gasoline engine emissions and the risk of lung cancer”. American Journal of Epidemiology. 165 (1): 53–62. PMID 17062632. Unknown parameter
|coauthors=ignored (help) - ↑ Lung cancer. Canadian Cancer Society 2015. http://www.cancer.ca/en/cancer-information/cancer-type/lung/risks/?region=ab#Outdoor_air_pollution
- ↑ Lung cancer. Canadian Cancer Society 2015. http://www.cancer.ca/en/cancer-information/cancer-type/lung/risks/?region=ab#Outdoor_air_pollution
- ↑ Lung cancer. Canadian Cancer Society 2015. http://www.cancer.ca/en/cancer-information/cancer-type/lung/risks/?region=ab#Outdoor_air_pollution
- ↑ Lung cancer. Canadian Cancer Society 2015. http://www.cancer.ca/en/cancer-information/cancer-type/lung/risks/?region=ab#Outdoor_air_pollution
- ↑ Lung cancer. Canadian Cancer Society 2015. http://www.cancer.ca/en/cancer-information/cancer-type/lung/risks/?region=ab#Outdoor_air_pollution
Screening
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Shanshan Cen, M.D. [2]
Overview
According to the U.S. Preventive Services Task Force (USPSTF), screening for lung cancer by low-dose computed tomography (LDCT) is recommended every year among smokers and former smokers who are between 55 to 80 years old and who have smoked 30 pack-years or more and either continue to smoke or have quit within the past 15 years (grade B recommendation). According to the clinical practice guideline issued by the American College of Chest Physicians (CHEST) in 2013, screening for lung cancer by low-dose CT (LDCT) is recommended every year among smokers and former smokers who are age 55 to 74 and who have smoked for 30 pack-years or more and either continue to smoke or have quit within the past 15 years.
Screening
Guidelines
- According to the U.S. Preventive Services Task Force (USPSTF), screening for lung cancer by low-dose computed tomography (LDCT) is recommended every year among smokers and former smokers who are between 55 to 80 years old and who have smoked 30 pack-years or more and either continue to smoke or have quit within the past 15 years (grade B recommendation).[1]
- According to the American College of Chest Physicians (CHEST) in 2013, screening for lung cancer by low-dose CT (LDCT) is recommended every year among smokers and former smokers who are age 55 to 74 and who have smoked for 30 pack-years or more and either continue to smoke or have quit within the past 15 years.[2]
Strategies[3]
- Advantages:
- There is evidence that screening 55 to 74 year old smokers of 30 or more pack-years or former smokers, who have quit within the last 15 years, reduces lung cancer mortality by 20% and all-cause mortality by 6.7%.
- Diasdvantages:
- At least 98% of all positive low-dose helical computed tomography screening exams do not result in a lung cancer diagnosis.
- False-positive exams may result in unnecessary invasive diagnostic procedures.
- Chest x-ray and/or sputum cytology:
- Advantages:
- Screening with chest x-ray and/or sputum cytology has no role in reducing mortality from lung cancer in the general population.
- Disadvantages:
- False positive exams
- At least 95% of all positive chest x-ray screening exams do not result in a lung cancer diagnosis.
- False-positive exams result in unnecessary invasive diagnostic procedures.
References
- ↑ Lung Cancer Screening. U.S. Preventive Services Task Force 2015. http://www.uspreventiveservicestaskforce.org/Page/Document/UpdateSummaryFinal/lung-cancer-screening Accessed on December 20, 2015
- ↑ Detterbeck FC, Mazzone PJ, Naidich DP, Bach PB (2013). “Screening for Lung Cancer: Diagnosis and Management of Lung Cancer, 3rd ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines”. Chest. 143 (5 Suppl): e78S–92S. doi:10.1378/chest.12-2350. PMID 23649455. Summary in JournalWatch
- ↑ Lung Cancer Screening. National Cancer Institute 2015. http://www.cancer.gov/types/lung/hp/lung-screening-pdq Accessed on December 20, 2015
Natural history, Complications, and Prognosis
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Shanshan Cen, M.D. [2]
Overview
Common complications of adenocarcinoma of the lung include breathing difficulties, pneumonia, pleural effusion, metastasis, and Horner’s syndrome. The prognosis of adenocarcinoma of the lung varies with the staging of tumor; stage IA have the most favorable prognosis. The presence of metastasis is associated with a particularly poor prognosis.
Natural History
- The majority of lung cancers present with advanced disease because the symptoms tend to occur later in the course of the disease.[1]
- The patient experiences non-specific symptoms such as cough, hemoptysis, dyspnea, chest pain, dysphonia, dysphagia, lack of appetite, weight loss, and fatigue from 3 weeks to 3 months before seeking medical attention.
- During the 3 weeks to 3 months course, the tumor cell may double 20 times.[1]
- In more advanced disease, the tumor may spread to other organs such as the spinal cord, brain, and bone.
- Patients with metastasis may develop symptoms such as leg weakness, paresthesias, bladder dysfunction, seizures, hemiplegia, cranial nerve palsies, confusion, personality changes, skeletal pain, and pleuritic pain.[1]
- Once the cancer spreads to the other organs, it is most likely to be fatal.
Complications
- Cancer growth in the airway may obstruct airflow, leading to breathing difficulties. Accumulation of secretions behind the blockage predisposes patients to pneumonia.
- Pleural effusion:
- Lung cancer may cause fluid to build up in the lungs which may lead to breathing difficulties.
- Metastasis:
- Lung cancer metastasizes to are the bones, liver, brain, and adrenal glands.
- Horner’s syndrome:
- Tumors in the apex of the lung, known as Pancoast tumors, may invade the local part of the sympathetic nervous system, leading to altered sweating patterns and eye muscle problems (Horner’s syndrome).[3]
Prognosis
- The prognosis of adenocarcinoma of the lung varies with the staging of tumor; Stage IA have the most favorable prognosis.
- The presence of metastasis is associated with a particularly poor prognosis.
Survival rate by stage[4]
| Stage | 5-year survival rate |
|---|---|
| IA | 49% |
| IB | 45% |
| IIA | 30% |
| IIB | 31% |
| IIIA | 14% |
| IIIB | 5% |
| IV | 1% |
References
- ↑ 1.0 1.1 1.2 Leary, A (2012). Lung cancer a multidisciplinary approach. Chichester, West Sussex, UK Ames, Iowa: Wiley-Blackwell. ISBN 9781405180757.
- ↑ Lung cancer complications. Mayo Clinic 2015. http://www.mayoclinic.org/diseases-conditions/lung-cancer/basics/complications/con-20025531 Accessed on December 20, 2015
- ↑ Jones, DR (Jul 1998). “Pancoast tumors of the lung”. Current Opinion in Pulmonary Medicine. 4 (4): 191–197. PMID 10813231. Unknown parameter
|coauthors=ignored (help) - ↑ Lung cancer. Canadian Cancer Society 2015. http://www.cancer.ca/en/cancer-information/cancer-type/lung/prognosis-and-survival/survival-statistics/?region=ab
Diagnosis
Diagnosis
Diagnostic study of choice | History and Symptoms | Physical Examination | Laboratory Findings | Electrocardiogram | X Ray Findings | Echocardiography and Ultrasound | CT-Scan Findings | MRI Findings | Other Imaging Findings | Other Diagnostic Studies
Treatment
Treatment
Medical Therapy | Interventions | Surgery | Primary Prevention | Secondary Prevention | Cost-Effectiveness of Therapy | Future or Investigational Therapies
Looking for the patient version?
© 2026 MyEClinic – IFTM Institut für Telematik in der Medizin GmbH