
Membranous glomerulonephritis
For patient information page, click here
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor-In-Chief: Syed Ahsan Hussain, M.D.[2] Cafer Zorkun, M.D., Ph.D. [3] Syed Hassan A. Kazmi BSc, MD [4] Jogeet Singh Sekhon, M.D. [5]
Synonyms and keywords: Extramembranous glomerulopathy; Heymann nephritis; idiopathic membranous glomerulonephritis; idiopathic membranous nephropathy; membranous glomerulonephropathy; membranous glomerulopathy; membranous nephropathy; nephropathy, membranous
Overview
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Syed Ahsan Hussain, M.D.[2]
Overview
Historical Perspective
Membranous glomerulonephritis was first discovered by David Jones, renal pathologist from Syracuse University in New York, in 1957.
Classification
There is no established system for the classification of MGN. however it can be divided in two groups based on etiology of MGN.
Pathophysiology
Membranous glomerulonephritis is caused by immune complex formation in the glomerulus. The immune complexes are formed by binding of antibodies to antigens in the glomerular basement membrane. The antigens damage the basement membrane and activates the immune response. The immune complex serves as an activator that triggers a response from the complement system. PLA2R antigen detected within immune deposits by immunofluorescence of the biopsy specimen. Formation of the immune complex. Immune complex formation results in release of cytokines which release membrane attack complex C5-C9. Release of C5-C9 lead to injury of podocyte which causes loss of glomerular permeablity. The damage to podocyte reults in proteinuria.
Causes
The main causes of Membranous Glomerulonephritis are Infectious causes like Hepatitis B, drugs like captopril and autoimmune diseases like systemic lupus erythematosus.
Differentiating Hereditary pancreatitis from Other Diseases
MGN must be differentiated from other diseases that cause proteinuria, weight loss, and renal failure, such as MPGN, MCD, and FSGC.
Epidemiology and Demographics
The incidence rate of membranous glomerulonephritis is 27 per 100.000. The prevalence rate of membranous glomerulonephritis is 690 per 100,000. The prevalence of membranous glomerulonephritis is approximately 690 per 100,000 individuals worldwide. In 2001, the mortality rate of membranous glomerulonephritis is approximately 380 per 100,000. The incidence of membranous glomerulonephritis increases with age; the median age at diagnosis is 40 years. Membranous glomerulopathy usually affects individuals of the caucasian race and chinese population. Membranous glomerulonephritis affects men and women equally. Membranous glomerulonephritis tends to affect Caucasian population and Chinese population.
Risk Factors
The most common risk factors of membranous glomerulonephritis include SLE and drugs like captopril, penicilliamine.
Screening
There is insufficient evidence to recommend routine screening for membranous glomerulonephritis.
Natural History, Complications, and Prognosis
The symptoms of membranous glomerulonephritis usually develop in the fourth decade of life in males. Approximately 5-30% patients with MN have spontanous remission. Common complications of membranous glomerulonephritis include renal failure, hypertension, proteinuria, dyslipidemia, hypercoagulable state leading to thromboembolism, Increased risk of infection. Prognosis is generally good, and 1 year mortality rate of patients with membranous glomerulonephritis is approximately 0.38%. The presence of proteinuria and baseline renal insuffiency are associated with a particularly poor prognosis among patients with membranous glomerulonephritis. Membranous glomerulonephritis caused by NSAIDS is associated with the most favorable prognosis.
Diagnosis
Diagnostic Criteria
The most efficient and sensitive test is ANA, ds-DNA antibodies specific test that is utilized for diagnosis of membranous glomerulonephritis. The gold standard test for the diagnosis of biopsy.
History and Symptoms
The hallmark of membranous glomerulonephritis is nephrotic syndrome. A positive history of forthy urine and headache are suggestive of membranous glomerulonephritis.
Physical Examination
Common physical examination findings of membranous glomerulonephritis include edematous feets and headache.
Laboratory Findings
The major laboratory workup includes blood workup, auto-immune workup and urine workup.
Electrocardiogram
There are no ECG findings associated with membranous glomerulonephritis.
X-ray
There are no x-ray findings associated with membranous glomerulonephritis.
Ultrasound
There are no echocardiography and ultrasound findings associated with membranous glomerulonephritis.
CT scan
There are no CT scan findings associated with membranous glomerulonephritis.
MRI
There are no MRI findings associated with membranous glomerulonephritis.
Other Imaging Findings
There are no other imaging findings associated with membranous glomerulonephritis
Other Diagnostic Studies
The patients with compromised renal functions are indicated for biopsy
Treatment
Medical Therapy
Pharmacologic medical therapy is recommended among patients who has infectious, autoimmune causes of membranous glomerulonephritis. The drugs like prednisone and cyclophospamide are recomended for the treatment of autoimmune cause of membranous glomerulonephritis. Drug like Angiotensin receptor inhibitior (ACEi) is recomended for managment of hypertension.
Surgery
Surgery is not the first-line treatment option for patients with MGN. Surgery is usually reserved for patients requiring renal transplant.
Primary Prevention
Vaccine against heptatis B and treatment of hepatitis C can be preventive for membranous glomerulopathy.
Secondary Prevention
Early detection and treatment of hepatitis C can be preventive for developing membranous glomerulopathy. Safe sexual practice can prevent the risk of HIV which can eventually decreases the risk of MN. Safe sexual practice can prevent the risk of syphilis which can be preventive the risk of MN.
References
Historical Perspective
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Syed Ahsan Hussain, M.D.[2]
Overview
Membranous glomerulonephritis was first discovered by David Jones, renal pathologist from Syracuse University in New York, in 1957
Historical Perspective
Discovery
Following is the course of events that lead to important discoveries in spectrum of membranous glomerulonephritis:[1][2]
- Membranous glomerulonephritis (MGN) was first discovered by David Jones, renal pathologist from Syracuse University in New York, in 1957
- in 1929 Bell introduced the term membranous glomerulonephritis to differentiate the membranous glomerulonephritis with nephrotic syndrome.
References
Classification
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Syed Ahsan Hussain, M.D.[2]
Overview
There is no established system for the classification of membranous glomerulonephritis (MGN).
Classification
There is no established system for the classification of membranous glomerulonephritis (MGN).
References
Pathophysiology
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Syed Ahsan Hussain, M.D.[2] Pervaiz Laghari, MD[3]
Overview
Membranous glomerulonephritis is caused by immune complex formation in the glomerulus. The immune complexes are formed by binding of antibodies to antigens in the glomerular basement membrane. The antigens damage the basement membrane and activates the immune response. The immune complex serves as an activator that triggers a response from the complement system. .PLA2R antigen detected within immune deposits by immunofluorescence of the biopsy specimen. Formation of the immune complex. Immune complex formation results in release of cytokines which release membrane attack complex C5-C9. Release of C5-C9 lead to injury of podocyte which causes loss of glomerular permeablity. The damage to podocyte reults in proteinuria.
Pathophysiology
- The membranous glomerulonephritis is a result of multiple changes, which are:[1][2][3][4][5][6][7]
- Membranous glomerulonephritis is caused by immune complex formation in the glomerulus.
- The immune complexes are formed by binding of antibodies to antigens in the glomerular basement membrane.
- The antigens damage the basement membrane and activates the immune response.
- The immune complex serves as an activator that triggers a response from the complement system.
Phospholipase A2 receptor
- The M-type PLA2R is the major antigen in human idiopathic membranous glomerulonephritis. It is expressed in glomerular podocytes.T
- here was no colocalization of PLA2R in secondary membranous glomerulonephritis biopsies
- .PLA2R antigen detected within immune deposits by immunofluorescence of the biopsy specimen. Formation of the immune complex.
- Immune complex formation results in release of cytokines which release membrane attack complex C5-C9.
- Release of C5-C9 lead to injury of podocyte which causes loss of glomerular permeablity.
- The damage to podocyte reults in proteinuria.
| HLA susceptibility 1 | Environmental factors | ||||||||||||||||||||||||||||
| Variant of PLA2R1 on podocyte surface | |||||||||||||||||||||||||||||
| Innate immunity activation and inflammation dendritic cell sense epitope of PLA2R1 and present them for adaptive immunity | |||||||||||||||||||||||||||||
| Production of auto-immune antibody IgG4/IgG1 which attach them self to epitope on podocyte surface | |||||||||||||||||||||||||||||
| In Situ formation and shedding of subepithelial immune complex | |||||||||||||||||||||||||||||
| Which lead to cytokine release oxygen derivative release membrane attack complex C5-C9 | |||||||||||||||||||||||||||||
| Podocyte injury by apoptosis altered lectin cytoskeleton loss of silt pore integrity loss of glomerular permeability proteinuria | |||||||||||||||||||||||||||||
Genetics
- Single-nucleotide polymorphisms (SNPs) at two loci that are highly associated with idiopathic membranous glomerulonephritis.[5][6]
- The two loci are within the genes for the PLA2R on chromosome 2q24.
- The human leukocyte antigen (HLA) complex class II alpha chain 1A (”HLA-DQA1”) on chromosome 6p21.
- The PLA2R has been identified as a major antigen in idiopathic membranous glomerulonephritis.
Associated Conditions
Consitions associated with membranous glomerulonephritis include:[8]
- Hepatitis B
- Hepatitis C
- Congenital Syphilis
- Systemic Lupus Erythematosis
- Malignancy
Gross Pathology
- On gross pathology examination there is no characteristic findings present
Microscopic Pathology
Microscopic pathologic findings characteristic of membranous glomerulonephritis include:[1][2]
- Early biopsies may be normal.
- Later: uniform diffuse capillary wall thickening without hypercellularity, no mesangial sclerosis and inflammatory cells.
- Proximal convoluted tubules: hyaline droplets, reflecting protein reabsorption.
- Membrane thickening and narrow capillary lumina.
- Mesangial sclerosis and glomerulosclerosis.
Immunofluorescence
- Granular diffuse peripheral deposits, usually IgG and C3, also C5b–C9 and occasionally IgM or IgA.
- C4d immunostaining may be diagnostic.
The microscopic,immunofluorscence and electron microscopic features are listed in the following table:[1][2]
| Stage | Glomerular Basement Membrane | Immunofluorescence | Electron Microscopy |
|---|---|---|---|
| Stage 1 | Normal or slightly thickned BM | Fine granular IgG, C3 | Scattered small subepithelial electron dense deposits no foot effacement |
| Stage 2 | Moderately thickened BM with spikes and vacuolization | Granular IgG, C3 | Diffuse spikes due to subepithelial deposits, diffuse foot process effacement |
| Stage 3 | Moderately thickened BM residual spikes and vacuoles | Chain like appearance IF, coarsely granular IgG, C3 | Intramembraneous deposits, spikes, neomembrane formation and diffuse foot process effacement |
| Stage 4 | Markedly thick GBM, few spikes, vacoules and glomerulosclerosis | Focal IgG, C3 | Sclerotic GBM, few deposits and lacunae |
-
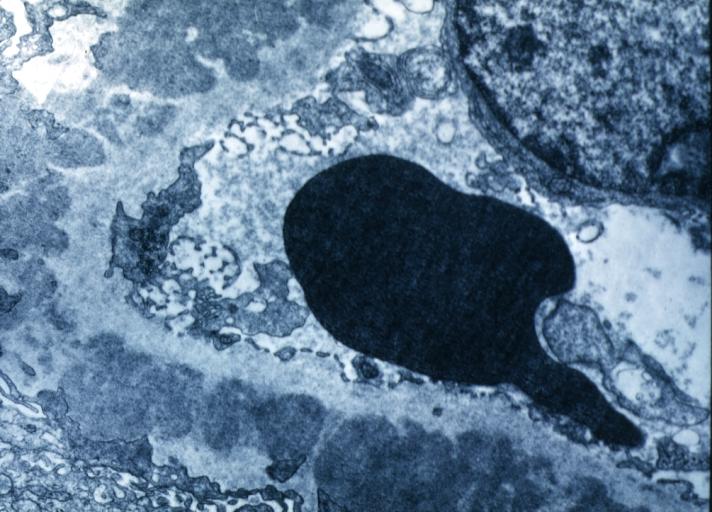 Membranous Glomerulonephritis: Electron micrography. An excellent example to show thickened basement membrane and immune complexes.
Membranous Glomerulonephritis: Electron micrography. An excellent example to show thickened basement membrane and immune complexes. -
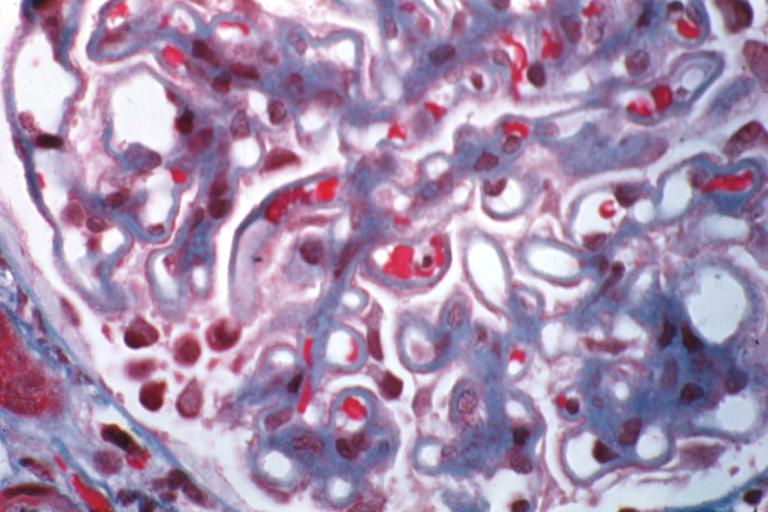 Membranous Glomerulonephritis: Micro trichrome high mag excellent to show thickened capillary basement membranes
Membranous Glomerulonephritis: Micro trichrome high mag excellent to show thickened capillary basement membranes -
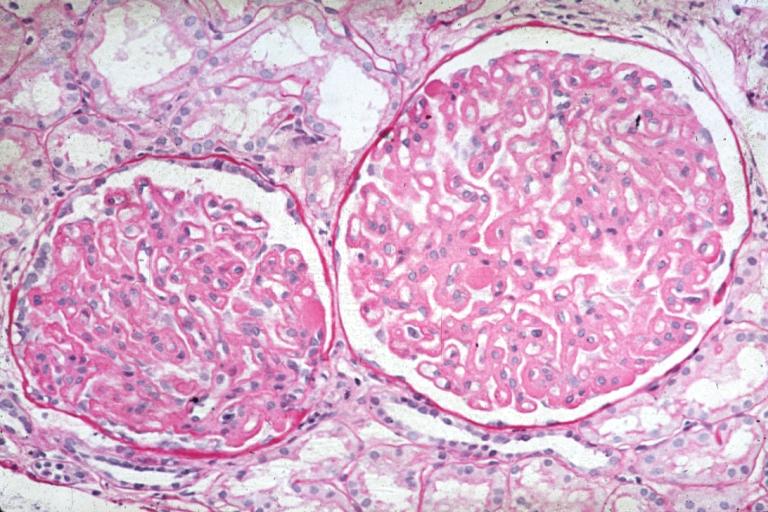 Membranous Glomerulonephritis: Micro PAS high mag excellent example of this lesion
Membranous Glomerulonephritis: Micro PAS high mag excellent example of this lesion -
 Membranous Glomerulonephritis: Micro PAS med mag
Membranous Glomerulonephritis: Micro PAS med mag




References
- ↑ 1.0 1.1 1.2 Cybulsky AV, Quigg RJ, Salant DJ (October 2005). “Experimental membranous nephropathy redux”. Am. J. Physiol. Renal Physiol. 289 (4): F660–71. doi:10.1152/ajprenal.00437.2004. PMC 1325222. PMID 16159900.
- ↑ 2.0 2.1 2.2 Nangaku M, Shankland SJ, Couser WG (May 2005). “Cellular response to injury in membranous nephropathy”. J. Am. Soc. Nephrol. 16 (5): 1195–204. doi:10.1681/ASN.2004121098. PMID 15800119.
- ↑ Cunningham PN, Quigg RJ (May 2005). “Contrasting roles of complement activation and its regulation in membranous nephropathy”. J. Am. Soc. Nephrol. 16 (5): 1214–22. doi:10.1681/ASN.2005010096. PMID 15800113.
- ↑ Kanigicherla D, Gummadova J, McKenzie EA, Roberts SA, Harris S, Nikam M, Poulton K, McWilliam L, Short CD, Venning M, Brenchley PE (May 2013). “Anti-PLA2R antibodies measured by ELISA predict long-term outcome in a prevalent population of patients with idiopathic membranous nephropathy”. Kidney Int. 83 (5): 940–8. doi:10.1038/ki.2012.486. PMID 23364522.
- ↑ 5.0 5.1 Debiec H, Ronco P (February 2011). “PLA2R autoantibodies and PLA2R glomerular deposits in membranous nephropathy”. N. Engl. J. Med. 364 (7): 689–90. doi:10.1056/NEJMc1011678. PMID 21323563.
- ↑ 6.0 6.1 Hoxha E, Kneißler U, Stege G, Zahner G, Thiele I, Panzer U, Harendza S, Helmchen UM, Stahl RA (October 2012). “Enhanced expression of the M-type phospholipase A2 receptor in glomeruli correlates with serum receptor antibodies in primary membranous nephropathy”. Kidney Int. 82 (7): 797–804. doi:10.1038/ki.2012.209. PMID 22673885.
- ↑ Svobodova B, Honsova E, Ronco P, Tesar V, Debiec H (July 2013). “Kidney biopsy is a sensitive tool for retrospective diagnosis of PLA2R-related membranous nephropathy”. Nephrol. Dial. Transplant. 28 (7): 1839–44. doi:10.1093/ndt/gfs439. PMID 23223223.
- ↑ Wasserstein AG (April 1997). “Membranous glomerulonephritis”. J. Am. Soc. Nephrol. 8 (4): 664–74. PMID 10495797.
References
Causes
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Syed Ahsan Hussain, M.D.[2]
Overview
The main causes of membranous glomerulonephritis are infections like hepatitis B, hepatitis C, HIV, syphilis, leprosy, drugs like captopril, penicilliamine, autoimmune diseases like systemic lupus erythematosus, Guillian-Barre nephropathy and neoplastic diseases like non-hodgkin`s lymphoma, chronic lymphocytic leukemia, occasionally hodgkin`s lymphoma.
Causes:
Life-threatening Causes
Common Causes
Infectious Causes
Drugs and toxicity
- The causes related to drug and toxicity are given below:[1]
- Penicilliamine
- Captopril (high doses)
- Nonsteroidal anti-inflammatory drugs
Neoplastic causes:
Less common causes:
Infectious causes:
Drug and toxicity:
Neoplastic disease
- The neoplastic causes are given below:[1]
- Carcinoma ( lung, breast, stomach, colon, esophagus, melanoma, renal cell, neuroblastoma, carotid body)
Miscellaneous
- The other causes are given below[1]:
- Diabetes Mellitus
- Sickle cell anemia
- Sarcoidosis
- Weber-christian disease
- Dermatitis herpetiformis
- Bullous pemphigoid
- Mysthenia gravis
- Guillian-Barre nephropathy
Causes by Organ System
| Cardiovascular | No underlying causes |
| Chemical/Poisoning | Volatile hydrocarbons |
| Dental | No underlying causes |
| Dermatologic | Bullous pemphigoid |
| Drug Side Effect | Captopril, Penicilliamine |
| Ear Nose Throat | No underlying causes |
| Endocrine | Diabetes mellitus, Hashimoto`s thyroiditis |
| Environmental | No underlying causes |
| Gastroenterologic | No underlying causes |
| Genetic | Weber-christian disease |
| Hematologic | Sickle cell anemia |
| Iatrogenic | No underlying causes |
| Infectious Disease | Hepatitis B, Hepatitis C, secondary and congenital syphilis, HIV nephropathy, Schistosomiasis, Leprosy, Hydatid disease, Loaiasis (filaria), Quartan malaria |
| Musculoskeletal/Orthopedic | Rheumatoid arthritis |
| Neurologic | Guillain-Barre nephropathy, Myasthenia gravis |
| Nutritional/Metabolic | No underlying causes |
| Obstetric/Gynecologic | No underlying causes |
| Oncologic | Non-Hodgkin`s Lymphoma, Chronic Lymphocytic Leukemia, Hodgkin`s Lymphoma |
| Ophthalmologic | No underlying causes |
| Overdose/Toxicity | Captopril, Gold, Penicilliamine |
| Psychiatric | No underlying causes |
| Pulmonary | Sarcoidosis |
| Renal/Electrolyte | No underlying causes |
| Rheumatology/Immunology/Allergy | Rheumatoid arthritis, Mysthenia gravis, Primary biliary cirrhosis, Guillain-Barre nephropathy, Systemic lupus erythematosis |
| Sexual | No underlying causes |
| Trauma | No underlying causes |
| Urologic | No underlying causes |
| Miscellaneous | No underlying causes |
Causes in Alphabetical Order
List the causes of the disease in alphabetical order:[1][2][3]
- Bullous pemphigoid
- Captopril
- Dermatitis herpetiformis
- Diabetes Mellitus
- Formaldehyde
- Guillain-Barre nephropathy
- Hashimoto`s thyroiditis
- Hepatitis B
- Hepatitis C
- Hydatid disease
- HIV
- Leprosy
- Loaiasis (filaria)
- Lymphoproliferative (non-hodgkin`s lymphoma, chronic lymphocytic leukemia, occasionally hodgkin`s lymphoma)
- Mysthenia gravis
- Nonsteroidal anti-inflammatory drugs
- Penicilliamine
- Primary biliary cirrhosis
- Quartan malaria
- Sarcoidosis
- Systemic lupus erythematosus
- Sickle cell anemia
- Schistosomiasis
- Syphilis (Secondary and congenital)
- Weber-christian disease
- Volatile hydrocarbons
References
- ↑ 1.0 1.1 1.2 1.3 1.4 1.5 1.6 Wasserstein AG (April 1997). “Membranous glomerulonephritis”. J. Am. Soc. Nephrol. 8 (4): 664–74. PMID 10495797.
- ↑ 2.0 2.1 2.2 2.3 Reichert, LJ; Koene, RA; Wetzels, JF (1998). “Prognostic factors in idiopathic membranous nephropathy”. American Journal of Kidney Diseases. 31 (1): 1–11. doi:10.1053/ajkd.1998.v31.pm9428445. ISSN 0272-6386.
- ↑ 3.0 3.1 3.2 Troyanov, S.; Roasio, L.; Pandes, M.; Herzenberg, A.M.; Cattran, D.C. (2006). “Renal pathology in idiopathic membranous nephropathy: A new perspective”. Kidney International. 69 (9): 1641–1648. doi:10.1038/sj.ki.5000289. ISSN 0085-2538.
Differentiating Membranous glomerulonephritis from other Diseases
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Mehrian Jafarizade, M.D [2], Syed Hassan A. Kazmi BSc, MD [3]
Overview
MGN must be differentiated from other diseases that cause proteinuria, weight loss, and renal failure, such as MPGN, MCD, and FSGC.
Differentiating Membranous Glomerulonephritis From Other Diseases
The various types of glomerular diseases should be differentiated from each other based on associations, presence of pitting edema, hematuria, hypertension, hemoptysis, oliguria, peri-orbital edema, hyperlipidemia, type of antibodies, light and electron microscopic features. The following table differentiates between various types of glumerular diseases:
| Glomerular diseases | Disease | History and Symtoms | Laboratory Findings | Pathology | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| History | Systemic symptoms | Hemeturia | Proteinuria | Hypertension | Pitting edema | Oliguria | Nephrotic features | Nephritic features | Hyperlipidemia and hypercholesterolemia | Auto-antibodies,
Complements |
Light microscope | Electron microscope | Immunoflourescence pattern | |||
| Acute Nephritic Syndromes | Poststreptococcal Glomerulonephritis[1][2][3] |
|
+/- | + | +/- | +/- | +/- | +/- | +/- | +/- |
|
|
| |||
| Renal disease due to Subacute Bacterial Endocarditis, or cardiac shunt (Atrioventricular)[4][5] |
|
+/- | + | +/- | +/- | +/- | +/- | +/- | +/- |
|
|
|
| |||
| Lupus Nephritis[6] |
|
|
+/- | + | +/- | +/- | +/- | +/- | +/- | +/- |
|
|
|
| ||
| Antiglomerular Basement Membrane Disease (Goodpasture’s syndrome)[7][8] |
|
|
+ | + | + | + | + | + | – | – | Diffuse thickening of the glomerular basement membrane with absence of sub-epithelial and sub-endothelial deposits |
| ||||
| IgA Nephropathy[9][10] |
|
|
+ | +/- | + | +/- | + | – | + | – |
|
|
|
| ||
| Disease | History | Systemic symptoms | Hemeturia | Proteinuria | Hypertension | Pitting edema | Oliguria | Nephrotic features | Nephritic features | Hyperlipidemia and hypercholesterolemia | Auto-antibodies,
Complements |
Light microscope | Electron microscope | Immunoflourescence pattern | ||
| ANCA Small-Vessel Vasculitis[11][12] | Granulomatosis with Polyangiitis (Wegener’s)[13][14][15] |
|
|
+ | + | + | +/- | + | – | + | – |
|
|
| ||
| Microscopic Polyangiitis[16] | +/- |
|
+ | + | + | + | + | + | – |
| ||||||
| Churg-Strauss Syndrome[17] | +/- | + | + | + | + | + | + | – |
| |||||||
| Membranoproliferative Glomerulonephritis[18][19] |
|
+ | + | + | +/- | + | + | – | – | – |
|
| ||||
| Henoch-Schönlein purpura [20] |
|
|
+ | + | + | +/- | + | + | – | – | – |
|
|
| ||
| Disease | History | Systemic symptoms | Hemeturia | Proteinuria | Hypertension | Pitting edema | Oliguria | Nephrotic features | Nephritic features | Hyperlipidemia and hypercholesterolemia | Auto-antibodies,
Complements |
Light microscope | Electron microscope | Immunoflourescence pattern | ||
| Cryoglobulinemia[21] | Patients having cryoglobulinemia may have positive history of:
|
Pulmonary symptoms:
Cutaneous symptoms: Gastrointestinal symptoms:
General symptoms:
|
+/- | + | +/- | + | +/- | +/- | +/- | +/- | +/- |
|
| |||
| Nephrotic Syndrome | Minimal Change Disease[22][23] |
|
– | + | – | + | +/- | + | – | + |
|
|
– | |||
| Focal Segmental Glomerulosclerosis[24][25][26] |
|
– | + | – | + | +/- | + | – | + |
|
|
– | ||||
| Membranous Glomerulonephritis[27][28] |
|
– | + | – | + | +/- | + | – | + | Immune complex deposition |
|
Immune complex GN, granular deposite | ||||
| Diabetic Nephropathy[29][30][31][32][33][34][35][36][37][38] | For more information on diabetes click here. | – | + | – | + | +/- | + | – | + |
|
|
– | ||||
| Disease | History | Systemic symptoms | Hemeturia | Proteinuria | Hypertension | Pitting edema | Oliguria | Nephrotic features | Nephritic features | Hyperlipidemia and hypercholesterolemia | Auto-antibodies,
Complements |
Light microscope | Electron microscope | Immunoflourescence pattern | ||
| Glomerular Deposition Diseases | Light Chain Deposition Disease[39] |
|
– | – | + | – | + | +/- | + | – | + | – |
|
|
| |
| Renal Amyloidosis[40][41][42][43] |
|
– | + | – | + | +/- | + | – | + | – |
|
|
| |||
| Fibrillary-Immunotactoid Glomerulopathy[44] | – | +/- | + | +/- | +/- | +/- | + | +/- | +/- | – |
|
|
| |||
| Fabry’s Disease[45][46][47] |
|
|
– | + | – | + | +/- | + | – | + | – |
|
|
– | ||
| Basement Membrane Syndrome | Alport’s Syndrome[48][49][50][51][52][53] |
|
Auditary:
Occular problems:
|
– | + | – | + | +/- | + | – | + | – |
|
|
| |
| Disease | History | Systemic symptoms | Hemeturia | Proteinuria | Hypertension | Pitting edema | Oliguria | Nephrotic features | Nephritic features | Hyperlipidemia and hypercholesterolemia | Auto-antibodies,
Complements |
Light microscope | Electron microscope | Immunoflourescence pattern | ||
| Thin Basement Membrane Disease[54][55] |
|
– | – | + | -/+ | – | -/+ | – | -/+ | – | – | – | Diffuse thinning of the glomerular basement membranes (GBM) | – | ||
| Nail-Patella Syndrome[56][57] |
|
|
+ | + | – | – | – | – | – | – | – |
|
|
| ||
| Glomerular-Vascular Syndromes | Hypertensive Nephrosclerosis[58] | Chronic hypertension |
|
+/- | +/- | + | +/- | +/- | +/- | – | +/- | – | ||||
| Cholesterol Emboli[59] |
|
|
+/- | +/- | + | +/- | +/- | +/- | – | +/- | – |
|
|
| ||
| Disease | History | Systemic symptoms | Hemeturia | Proteinuria | Hypertension | Pitting edema | Oliguria | Nephrotic features | Nephritic features | Hyperlipidemia and hypercholesterolemia | Auto-antibodies,
Complements |
Light microscope | Electron microscope | Immunoflourescence pattern | ||
| Sickle Cell Disease[60] |
|
|
+/- | +/- | +/- | – | – | – | – | – | – |
| ||||
| Thrombotic Microangiopathies[61] | Click for more information on Thrombotic Microangiopathies. | + | +/- | + | +/- | +/- | +/- | – | – | – |
|
|
| |||
| Antiphospholipid Antibody Syndrome [62][63][64] |
|
|
+ | +/- | + | +/- | +/- | +/- | – | – | – |
|
|
| ||
Some infectious diseases such as HIV, HBV, HCV, syphilis, leprosy, malaria, and schistosomiasis may cause glomerular diseases.
References
- ↑ GERMUTH FG (1953). “A comparative histologic and immunologic study in rabbits of induced hypersensitivity of the serum sickness type”. J Exp Med. 97 (2): 257–82. PMC 2136196. PMID 13022878.
- ↑ Germuth FG, Senterfit LB, Dreesman GR (1972). “Immune complex disease. V. The nature of the circulating complexes associated with glomerular alterations in the chronic BSA-rabbit system”. Johns Hopkins Med J. 130 (6): 344–57. PMID 5031005.
- ↑ Radhakrishnan J, Cattran DC (2012). “The KDIGO practice guideline on glomerulonephritis: reading between the (guide)lines–application to the individual patient”. Kidney Int. 82 (8): 840–56. doi:10.1038/ki.2012.280. PMID 22895519.
- ↑ Neugarten J, Baldwin DS (August 1984). “Glomerulonephritis in bacterial endocarditis”. Am. J. Med. 77 (2): 297–304. PMID 6380288.
- ↑ Arze RS, Rashid H, Morley R, Ward MK, Kerr DN (January 1983). “Shunt nephritis: report of two cases and review of the literature”. Clin. Nephrol. 19 (1): 48–53. PMID 6831779.
- ↑ Weening JJ, D’Agati VD, Schwartz MM, Seshan SV, Alpers CE, Appel GB, Balow JE, Bruijn JA, Cook T, Ferrario F, Fogo AB, Ginzler EM, Hebert L, Hill G, Hill P, Jennette JC, Kong NC, Lesavre P, Lockshin M, Looi LM, Makino H, Moura LA, Nagata M (February 2004). “The classification of glomerulonephritis in systemic lupus erythematosus revisited”. Kidney Int. 65 (2): 521–30. doi:10.1111/j.1523-1755.2004.00443.x. PMID 14717922.
- ↑ Bolton WK (November 1996). “Goodpasture’s syndrome”. Kidney Int. 50 (5): 1753–66. PMID 8914046.
- ↑ Mathew TH, Hobbs JB, Kalowski S, Sutherland PW, Kincaid-Smith P (February 1975). “Goodpasture’s syndrome: normal renal diagnostic findings”. Ann. Intern. Med. 82 (2): 215–8. PMID 1090223.
- ↑ Suzuki H, Kiryluk K, Novak J, Moldoveanu Z, Herr AB, Renfrow MB, Wyatt RJ, Scolari F, Mestecky J, Gharavi AG, Julian BA (October 2011). “The pathophysiology of IgA nephropathy”. J. Am. Soc. Nephrol. 22 (10): 1795–803. doi:10.1681/ASN.2011050464. PMC 3892742. PMID 21949093.
- ↑ Wyatt RJ, Julian BA (June 2013). “IgA nephropathy”. N. Engl. J. Med. 368 (25): 2402–14. doi:10.1056/NEJMra1206793. PMID 23782179.
- ↑ Higgins RM, Goldsmith DJ, Connolly J, Scoble JE, Hendry BM, Ackrill P, Venning MC (January 1996). “Vasculitis and rapidly progressive glomerulonephritis in the elderly”. Postgrad Med J. 72 (843): 41–4. PMC 2398323. PMID 8746284.
- ↑ Jennette JC (March 2003). “Rapidly progressive crescentic glomerulonephritis”. Kidney Int. 63 (3): 1164–77. doi:10.1046/j.1523-1755.2003.00843.x. PMID 12631105.
- ↑ Renaudineau Y, Le Meur Y (October 2008). “Renal involvement in Wegener’s granulomatosis”. Clin Rev Allergy Immunol. 35 (1–2): 22–9. doi:10.1007/s12016-007-8066-6. PMID 18172777.
- ↑ Weiss MA, Crissman JD (October 1984). “Renal biopsy findings in Wegener’s granulomatosis: segmental necrotizing glomerulonephritis with glomerular thrombosis”. Hum. Pathol. 15 (10): 943–56. PMID 6384024.
- ↑ Pagnoux C (March 2008). “[Wegener’s granulomatosis and microscopic polyangiitis]”. Rev Prat (in French). 58 (5): 522–32. PMID 18524109.
- ↑ Chung SA, Seo P (August 2010). “Microscopic polyangiitis”. Rheum. Dis. Clin. North Am. 36 (3): 545–58. doi:10.1016/j.rdc.2010.04.003. PMC 2917831. PMID 20688249.
- ↑ Sinico RA, Di Toma L, Maggiore U, Tosoni C, Bottero P, Sabadini E, Giammarresi G, Tumiati B, Gregorini G, Pesci A, Monti S, Balestrieri G, Garini G, Vecchio F, Buzio C (May 2006). “Renal involvement in Churg-Strauss syndrome”. Am. J. Kidney Dis. 47 (5): 770–9. doi:10.1053/j.ajkd.2006.01.026. PMID 16632015.
- ↑ Alchi B, Jayne D (August 2010). “Membranoproliferative glomerulonephritis”. Pediatr. Nephrol. 25 (8): 1409–18. doi:10.1007/s00467-009-1322-7. PMC 2887509. PMID 19908070.
- ↑ Davis AE, Schneeberger EE, Grupe WE, McCluskey RT (May 1978). “Membranoproliferative glomerulonephritis (MPGN type I) and dense deposit disease (DDD) in children”. Clin. Nephrol. 9 (5): 184–93. PMID 657595.
- ↑ Jennette JC, Falk RJ (July 1994). “The pathology of vasculitis involving the kidney”. Am. J. Kidney Dis. 24 (1): 130–41. PMID 8023818.
- ↑ Fogo AB, Lusco MA, Najafian B, Alpers CE (February 2016). “AJKD Atlas of Renal Pathology: Cryoglobulinemic Glomerulonephritis”. Am. J. Kidney Dis. 67 (2): e5–7. doi:10.1053/j.ajkd.2015.12.007. PMID 26802335.
- ↑ Saha TC, Singh H (November 2006). “Minimal change disease: a review”. South. Med. J. 99 (11): 1264–70. doi:10.1097/01.smj.0000243183.87381.c2. PMID 17195422.
- ↑ Saleem MA, Kobayashi Y (2016). “Cell biology and genetics of minimal change disease”. F1000Res. 5. doi:10.12688/f1000research.7300.1. PMC 4821284. PMID 27092244.
- ↑ Rosenberg AZ, Kopp JB (March 2017). “Focal Segmental Glomerulosclerosis”. Clin J Am Soc Nephrol. 12 (3): 502–517. doi:10.2215/CJN.05960616. PMC 5338705. PMID 28242845.
- ↑ Jefferson JA, Shankland SJ (September 2014). “The pathogenesis of focal segmental glomerulosclerosis”. Adv Chronic Kidney Dis. 21 (5): 408–16. doi:10.1053/j.ackd.2014.05.009. PMC 4149756. PMID 25168829.
- ↑ Gephardt GN, Tubbs RR, Popowniak KL, McMahon JT (October 1986). “Focal and segmental glomerulosclerosis. Immunohistologic study of 20 renal biopsy specimens”. Arch. Pathol. Lab. Med. 110 (10): 902–5. PMID 2429634.
- ↑ Lai WL, Yeh TH, Chen PM, Chan CK, Chiang WC, Chen YM, Wu KD, Tsai TJ (February 2015). “Membranous nephropathy: a review on the pathogenesis, diagnosis, and treatment”. J. Formos. Med. Assoc. 114 (2): 102–11. doi:10.1016/j.jfma.2014.11.002. PMID 25558821.
- ↑ Wasserstein AG (April 1997). “Membranous glomerulonephritis”. J. Am. Soc. Nephrol. 8 (4): 664–74. PMID 10495797.
- ↑ Drummond K, Mauer M, International Diabetic Nephropathy Study Group (2002). “The early natural history of nephropathy in type 1 diabetes: II. Early renal structural changes in type 1 diabetes”. Diabetes. 51 (5): 1580–7. PMID 11978659.
- ↑ Hørlyck A, Gundersen HJ, Osterby R (1986). “The cortical distribution pattern of diabetic glomerulopathy”. Diabetologia. 29 (3): 146–50. PMID 3699305.
- ↑ Alpers CE, Hudkins KL (2011). “Mouse models of diabetic nephropathy”. Curr Opin Nephrol Hypertens. 20 (3): 278–84. doi:10.1097/MNH.0b013e3283451901. PMC 3658822. PMID 21422926.
- ↑ Kimmelstiel P, Wilson C (1936). “Intercapillary Lesions in the Glomeruli of the Kidney”. Am J Pathol. 12 (1): 83–98.7. PMC 1911022. PMID 19970254.
- ↑ Alpers CE, Biava CG (1989). “Idiopathic lobular glomerulonephritis (nodular mesangial sclerosis): a distinct diagnostic entity”. Clin Nephrol. 32 (2): 68–74. PMID 2766585.
- ↑ Toyoda M, Najafian B, Kim Y, Caramori ML, Mauer M (2007). “Podocyte detachment and reduced glomerular capillary endothelial fenestration in human type 1 diabetic nephropathy”. Diabetes. 56 (8): 2155–60. doi:10.2337/db07-0019. PMID 17536064.
- ↑ Najafian B, Crosson JT, Kim Y, Mauer M (2006). “Glomerulotubular junction abnormalities are associated with proteinuria in type 1 diabetes”. J Am Soc Nephrol. 17 (4 Suppl 2): S53–60. doi:10.1681/ASN.2005121342. PMID 16565248.
- ↑ Najafian B, Kim Y, Crosson JT, Mauer M (2003). “Atubular glomeruli and glomerulotubular junction abnormalities in diabetic nephropathy”. J Am Soc Nephrol. 14 (4): 908–17. PMID 12660325.
- ↑ Najafian B, Alpers CE, Fogo AB (2011). “Pathology of human diabetic nephropathy”. Contrib Nephrol. 170: 36–47. doi:10.1159/000324942. PMID 21659756.
- ↑ Najafian B, Alpers CE, Fogo AB (2011). “Pathology of human diabetic nephropathy”. Contrib Nephrol. 170: 36–47. doi:10.1159/000324942. PMID 21659756.
- ↑ Hutchison CA, Cockwell P, Stringer S, Bradwell A, Cook M, Gertz MA, Dispenzieri A, Winters JL, Kumar S, Rajkumar SV, Kyle RA, Leung N (June 2011). “Early reduction of serum-free light chains associates with renal recovery in myeloma kidney”. J. Am. Soc. Nephrol. 22 (6): 1129–36. doi:10.1681/ASN.2010080857. PMC 3103732. PMID 21511832.
- ↑ Baker KR, Rice L (2012). “The amyloidoses: clinical features, diagnosis and treatment”. Methodist Debakey Cardiovasc J. 8 (3): 3–7. PMC 3487569. PMID 23227278.
- ↑ Gillmore JD, Hawkins PN (October 2013). “Pathophysiology and treatment of systemic amyloidosis”. Nat Rev Nephrol. 9 (10): 574–86. doi:10.1038/nrneph.2013.171. PMID 23979488.
- ↑ Jerzykowska S, Cymerys M, Gil LA, Balcerzak A, Pupek-Musialik D, Komarnicki MA (2014). “Primary systemic amyloidosis as a real diagnostic challenge – case study”. Cent Eur J Immunol. 39 (1): 61–6. doi:10.5114/ceji.2014.42126. PMC 4439975. PMID 26155101.
- ↑ Pepys MB (2006). “Amyloidosis”. Annu. Rev. Med. 57: 223–41. doi:10.1146/annurev.med.57.121304.131243. PMID 16409147.
- ↑ Korbet SM, Schwartz MM, Lewis EJ (March 1991). “Immunotactoid glomerulopathy”. Am. J. Kidney Dis. 17 (3): 247–57. PMID 1996564.
- ↑ Alroy J, Sabnis S, Kopp JB (June 2002). “Renal pathology in Fabry disease”. J. Am. Soc. Nephrol. 13 Suppl 2: S134–8. PMID 12068025.
- ↑ Meikle PJ, Hopwood JJ, Clague AE, Carey WF (1999). “Prevalence of lysosomal storage disorders”. JAMA : the Journal of the American Medical Association. 281 (3): 249–54. PMID 9918480. Unknown parameter
|month=ignored (help) - ↑ Branton MH, Schiffmann R, Sabnis SG; et al. (2002). “Natural history of Fabry renal disease: influence of alpha-galactosidase A activity and genetic mutations on clinical course”. Medicine. 81 (2): 122–38. PMID 11889412. Unknown parameter
|month=ignored (help) - ↑ McCarthy PA, Maino DM (2000). “Alport syndrome: a review”. Clin Eye Vis Care. 12 (3–4): 139–150. PMID 11137428.
- ↑ Chugh KS, Sakhuja V, Agarwal A, Jha V, Joshi K, Datta BN; et al. (1993). “Hereditary nephritis (Alport’s syndrome)–clinical profile and inheritance in 28 kindreds”. Nephrol Dial Transplant. 8 (8): 690–5. PMID 8414153.
- ↑ Chugh KS, Sakhuja V, Agarwal A, Jha V, Joshi K, Datta BN; et al. (1993). “Hereditary nephritis (Alport’s syndrome)–clinical profile and inheritance in 28 kindreds”. Nephrol Dial Transplant. 8 (8): 690–5. PMID 8414153.
- ↑ McCarthy PA, Maino DM (2000). “Alport syndrome: a review”. Clin Eye Vis Care. 12 (3–4): 139–150. PMID 11137428.
- ↑ Amari F, Segawa K, Ando F (1994). “Lens coloboma and Alport-like glomerulonephritis”. Eur J Ophthalmol. 4 (3): 181–3. PMID 7819734.
- ↑ Govan JA (1983). “Ocular manifestations of Alport’s syndrome: a hereditary disorder of basement membranes?”. Br J Ophthalmol. 67 (8): 493–503. PMC 1040106. PMID 6871140.
- ↑ Savige J, Rana K, Tonna S, Buzza M, Dagher H, Wang YY (2003). “Thin basement membrane nephropathy”. Kidney Int. 64 (4): 1169–78. doi:10.1046/j.1523-1755.2003.00234.x. PMID 12969134. Unknown parameter
|month=ignored (help) - ↑ Hou P, Chen Y, Ding J, Li G, Zhang H (2007). “A novel mutation of COL4A3 presents a different contribution to Alport syndrome and thin basement membrane nephropathy”. Am. J. Nephrol. 27 (5): 538–44. doi:10.1159/000107666. PMID 17726307.
- ↑ Najafian B, Smith K, Lusco MA, Alpers CE, Fogo AB (October 2017). “AJKD Atlas of Renal Pathology: Nail-Patella Syndrome-Associated Nephropathy”. Am. J. Kidney Dis. 70 (4): e19–e20. doi:10.1053/j.ajkd.2017.08.001. PMID 28941488.
- ↑ Guidera KJ, Satterwhite Y, Ogden JA, Pugh L, Ganey T (1991). “Nail patella syndrome: a review of 44 orthopaedic patients”. J Pediatr Orthop. 11 (6): 737–42. PMID 1960197.
- ↑ Hughson MD, Puelles VG, Hoy WE, Douglas-Denton RN, Mott SA, Bertram JF (July 2014). “Hypertension, glomerular hypertrophy and nephrosclerosis: the effect of race”. Nephrol. Dial. Transplant. 29 (7): 1399–409. doi:10.1093/ndt/gft480. PMC 4071048. PMID 24327566.
- ↑ Lusco MA, Najafian B, Alpers CE, Fogo AB (April 2016). “AJKD Atlas of Renal Pathology: Cholesterol Emboli”. Am. J. Kidney Dis. 67 (4): e23–4. doi:10.1053/j.ajkd.2016.02.034. PMID 27012950.
- ↑ Wesson DE (June 2002). “The initiation and progression of sickle cell nephropathy”. Kidney Int. 61 (6): 2277–86. doi:10.1046/j.1523-1755.2002.00363.x. PMID 12028473.
- ↑ Lusco MA, Fogo AB, Najafian B, Alpers CE (December 2016). “AJKD Atlas of Renal Pathology: Thrombotic Microangiopathy”. Am. J. Kidney Dis. 68 (6): e33–e34. doi:10.1053/j.ajkd.2016.10.006. PMID 27884283.
- ↑ Jayakody Arachchillage D, Greaves M (2014). “The chequered history of the antiphospholipid syndrome”. Br J Haematol. 165 (5): 609–17. doi:10.1111/bjh.12848. PMID 24684307.
- ↑ Jayakody Arachchillage D, Greaves M (2014). “The chequered history of the antiphospholipid syndrome”. Br J Haematol. 165 (5): 609–17. doi:10.1111/bjh.12848. PMID 24684307.
- ↑ Popa A, Voinea L, Pop M, Stana D, Dascalu AM, Alexandrescu C; et al. (2008). “[Primary antiphospholipid syndrome]”. Oftalmologia. 52 (1): 13–7. PMID 18714484.
Epidemiology and Demographics
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Syed Ahsan Hussain, M.D.[2]
Overview
The incidence rate of membranous glomerulonephritis is 27 per 100.000. The prevalence rate of membranous glomerulonephritis is 690 per 100,000. The prevalence of membranous glomerulonephritis is approximately 690 per 100,000 individuals worldwide. In 2001, the mortality rate of membranous glomerulonephritis is approximately 380 per 100,000. The incidence of membranous glomerulonephritis increases with age; the median age at diagnosis is 40 years. Membranous glomerulopathy usually affects individuals of the caucasian race and chinese population. Membranous glomerulonephritis affects men and women equally. Membranous glomerulonephritis tends to affect Caucasian population and Chinese population.
Epidemiology and Demographics
Incidence
- The incidence of membranous glomerulopathy is approximately 27 per 100,000 individuals worldwide.[1]
Prevalence
- The prevalence of membranous glomerulonephritis is approximately 690 per 100,000 individuals worldwide.[1][3]
Mortality rate
- In 2001, the mortality rate of membranous glomerulonephritis is approximately 380 per 100,000[1][3][4]
Age
- Patients of all age groups may develop membranous glomerulonephritis
- The incidence of membranous glomerulonephritis increases with age; the median age at diagnosis is 40 years[5]
Race
- Membranous glomerulopathy usually affects individuals of the caucasian race and chinese population.[3][5]
Gender
- Membranous glomerulonephritis affects men and women equally.[3]
Region
References
- ↑ 1.0 1.1 1.2 1.3 McGrogan, A.; Franssen, C. F. M.; de Vries, C. S. (2010). “The incidence of primary glomerulonephritis worldwide: a systematic review of the literature”. Nephrology Dialysis Transplantation. 26 (2): 414–430. doi:10.1093/ndt/gfq665. ISSN 0931-0509.
- ↑ Cattran DC, Brenchley PE (March 2017). “Membranous nephropathy: integrating basic science into improved clinical management”. Kidney Int. 91 (3): 566–574. doi:10.1016/j.kint.2016.09.048. PMID 28065518.
- ↑ 3.0 3.1 3.2 3.3 3.4 Debiec H, Ronco P (July 2014). “Immunopathogenesis of membranous nephropathy: an update”. Semin Immunopathol. 36 (4): 381–97. doi:10.1007/s00281-014-0423-y. PMID 24715030.
- ↑ Xu X, Wang G, Chen N, Lu T, Nie S, Xu G, Zhang P, Luo Y, Wang Y, Wang X, Schwartz J, Geng J, Hou FF (December 2016). “Long-Term Exposure to Air Pollution and Increased Risk of Membranous Nephropathy in China”. J. Am. Soc. Nephrol. 27 (12): 3739–3746. doi:10.1681/ASN.2016010093. PMC 5118492. PMID 27365535.
- ↑ 5.0 5.1 5.2 Tang, Lijun; Yao, Jing; Kong, Xianglei; Sun, Qing; Wang, Zunsong; Zhang, Ying; Wang, Ping; Liu, Yipeng; Li, Wenbin; Cui, Meiyu; Zhen, Junhui; Xu, Dongmei (2017). “Increasing prevalence of membranous nephropathy in patients with primary glomerular diseases: A cross-sectional study in China”. Nephrology. 22 (2): 168–173. doi:10.1111/nep.12739. ISSN 1320-5358.
Risk Factors
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Syed Ahsan Hussain, M.D.[2]
Overview
The most common risk factors of membranous glomerulonephritis include SLE and drugs like captopril, penicilliamine.
Risk Factors
Common Risk Factors
- The most common risk factors of membranous glomerulonephritis includes:[1][2][3]
- Gold
- Penicilliamine
- Captopril
- Systemic Lupus Erythematousis
Less Common Risk Factors
References
- ↑ 1.0 1.1 Wasserstein AG (April 1997). “Membranous glomerulonephritis”. J. Am. Soc. Nephrol. 8 (4): 664–74. PMID 10495797.
- ↑ Reichert, LJ; Koene, RA; Wetzels, JF (1998). “Prognostic factors in idiopathic membranous nephropathy”. American Journal of Kidney Diseases. 31 (1): 1–11. doi:10.1053/ajkd.1998.v31.pm9428445. ISSN 0272-6386.
- ↑ Troyanov, S.; Roasio, L.; Pandes, M.; Herzenberg, A.M.; Cattran, D.C. (2006). “Renal pathology in idiopathic membranous nephropathy: A new perspective”. Kidney International. 69 (9): 1641–1648. doi:10.1038/sj.ki.5000289. ISSN 0085-2538.
- ↑ Reichert, LJ; Koene, RA; Wetzels, JF (1998). “Prognostic factors in idiopathic membranous nephropathy”. American Journal of Kidney Diseases. 31 (1): 1–11. doi:10.1053/ajkd.1998.v31.pm9428445. ISSN 0272-6386.
Screening
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Syed Ahsan Hussain, M.D.[2]
Overview
There is insufficient evidence to recommend routine screening for membranous glomerulonephritis.
Screening
There is insufficient evidence to recommend routine screening for membranous glomerulonephritis.
References
Natural History, Complications and Prognosis
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Syed Ahsan Hussain, M.D.[2]
Overview
The symptoms of membranous glomerulonephritis usually develop in the fourth decade of life in males. Approximately 5-30% patients with MN have spontanous remission. Common complications of membranous glomerulonephritis include renal failure, hypertension, proteinuria, dyslipidemia, hypercoagulable state leading to thromboembolism, Increased risk of infection. Prognosis is generally good, and 1 year mortality rate of patients with membranous glomerulonephritis is approximately 0.38%. The presence of proteinuria and baseline renal insuffiency are associated with a particularly poor prognosis among patients with membranous glomerulonephritis. Membranous glomerulonephritis caused by NSAIDS is associated with the most favorable prognosis.
Natural History
- The natural history of membranous glomerulonephritis (MN) is given below:[1][2]
- The symptoms of MN usually develop in the fourth decade of life in males.
- The presence of symptoms of MN young female is suggestive of lupus.
- Approximately 5-30% patients with MN have spontanous remission.
Complications
- Common complications of membranous glomerulonepharitis include:[3][4]
- Renal failure
- Symptoms associated with the nephrotic syndrome:
- Hypercoagulable state leading to thromboembolism
- Increased risk of infection
Prognosis
- The prognostic factors of membranous glomerulonephritis are given below:[5][6]
- Prognosis is generally good, and 1 year mortality rate of patients with membranous glomerulonephritis is approximately 0.38%.
- Depending on the extent of the membranous glomerulonephritis at the time of diagnosis, the prognosis may vary. However, the prognosis is generally regarded as good.
- The presence of proteinuria and baseline renal insuffiency are associated with a particularly poor prognosis among patients with membranous glomerulonephritis.
- Membranous glomerulonephritis caused by NSAIDS is associated with the most favorable prognosis.
- The prognosis of membranous glomerulonephritis associated with hepatitis B has less favorable prognosis.
References
- ↑ Kerjaschki D (2000). “Pathogenetic concepts of membranous glomerulopathy (MGN)”. J. Nephrol. 13 Suppl 3: S96–100. PMID 11132040.
- ↑ Schieppati A, Mosconi L, Perna A, Mecca G, Bertani T, Garattini S, Remuzzi G (July 1993). “Prognosis of untreated patients with idiopathic membranous nephropathy”. N. Engl. J. Med. 329 (2): 85–9. doi:10.1056/NEJM199307083290203. PMID 8510707.
- ↑ Debiec H, Ronco P (July 2014). “Immunopathogenesis of membranous nephropathy: an update”. Semin Immunopathol. 36 (4): 381–97. doi:10.1007/s00281-014-0423-y. PMID 24715030.
- ↑ Barbour S, Reich H, Cattran D (2013). “Short-term complications of membranous nephropathy”. Contrib Nephrol. 181: 143–51. doi:10.1159/000349976. PMID 23689576.
- ↑ Wasserstein AG (April 1997). “Membranous glomerulonephritis”. J. Am. Soc. Nephrol. 8 (4): 664–74. PMID 10495797.
- ↑ McGrogan, A.; Franssen, C. F. M.; de Vries, C. S. (2010). “The incidence of primary glomerulonephritis worldwide: a systematic review of the literature”. Nephrology Dialysis Transplantation. 26 (2): 414–430. doi:10.1093/ndt/gfq665. ISSN 0931-0509.
Diagnosis
Diagnosis
History and Symptoms | Physical Examination | Laboratory Findings | Renal Biopsy | Light Microscopy | CT | Immunofluorescence Microscopy | Ultrasound | Other Imaging Findings | Other Diagnostic Studies
Treatment
Treatment
Medical Therapy | Surgery | Primary Prevention | Secondary Prevention | Cost-Effectiveness of Therapy | Future or Investigational Therapies
Looking for the patient version?
© 2026 MyEClinic – IFTM Institut für Telematik in der Medizin GmbH