
POEMS syndrome
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1] Associate Editor(s)-in-Chief: Sabawoon Mirwais, M.B.B.S, M.D.[2] Syed Hassan A. Kazmi BSc, MD [3]
Synonyms and keywords: Crow-Fukase syndrome; Takatsuki disease; PEP syndrome
Overview
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1] Associate Editor(s)-in-Chief: Syed Hassan A. Kazmi BSc, MD [2]Sabawoon Mirwais, M.B.B.S, M.D.[3]
Overview
POEMS syndrome is a rare medical syndrome named for its main clinically recognizable features: Polyneuropathy (peripheral nerve damage), Organomegaly (abnormal enlargement of organs), Endocrinopathy (damage to hormone-producing glands)/Edema, M-protein (an abnormal antibody) and Skin abnormalities (including hyperpigmentation and hypertrichosis). In 1938, Ilya Mark Scheinker, a Russian neurologist and neuropathologist described a patient with a solitary plasmacytoma, sensorimotor polyneuropathy, and localized patches of thickened and deeply pigmented skin. In 1956, R. S. Crow published two case reports of myelomatosis with peripheral neuritis and other striking features. In 1977, Iwashita et al described a patient who had an osteosclerotic myeloma accompanied by sensorimotor polyneuropathy, skinhyperipigmentation, edema, hypertrichosis, gynecomastia, and white nails. In 1980, Bardwick et al proposed the acronym ‘POEMS’ to represent a syndrome characterized by polyneuropathy, organomegaly, endocrinopathy, M protein, and skin changes. POEMS syndrome is a para-neoplastic syndrome characterized by multi-organ system dysfunction, monoclonal plasma cell proliferation and demyelinating inflammatory polyneuropathy. The lambda component of immunoglobulin light chains is thought to be overproduced in POEMS syndrome secondary to monoclonal plasma cell proliferation. Bone marrow studies of patients suffering from POEMS syndrome shows lymphoid aggregates rimmed by monotypic or polytypic plasma cells. The monoclonal gammopathy or overproduction of lambda light chain stimulates the monocyte/macrophage system to produce various proinflammatory cytokines. such as interleukin-1, interleukin-6, interleukin-12, vascular endothelial growth factor (VEGF) and TNF-Alpha. Transforming growth factor beta (TGF-beta), an inhbitory cytokine is thought to be underproduced in patients suffering from POEMS syndrome leading to a storm of proinflammatory cytokines which drive the disease process. The overproduction of this IL-6 may be related to some of the clinical features seen in POEMS syndrome such as gammopathy, elevated C-Reactive protein (CRP) and thrombocytosis. The mesangial proliferation and membranoproliferative glomerulonephritis (MPGN) seen in POEMS syndrome is thought to be secondary to increased production of platelet-derived growth factor(PDGF) and fibroblast growth factor beta (FGF-β) have been implicated in mesangial cell proliferation. The neovascularization induced by VEGF leads to increased vascular permeability. Since the increased production of VEGF is unchecked due to the plasma cell dyscrasia, the consequence is an unregulated extravasation of intravascular fluid into the extravascular compartment. resulting in edema. POEMS syndrome is known to be associated multiple myeloma (osteosclerotic type), Castleman’s disease, plasmacytoma, monoclonal gammopathy of undetermined significance (MGUS), pulmonary hypertension, restrictive lung disease, thrombophilia, cardiac amyloidosis and papilledema. There are no known and well established causes of POEMS syndrome. Marked activation of the pro-inflammatory cytokines and weak or decreased TGF beta 1 action can play a role in the disease pathogenesis. The precise incidence of POEMS syndrome is difficult to determine and we have no well established data to quote. The median age at presentation has been 51 years with the majority of the patients comprising of males. A mediansurvival of 165 months has also been recorded. The precise incidence of POEMS syndrome is difficult to determine due to the complexity of the syndrome presentation and we have no well established data regarding the incidence. Prevalence of POEMS syndrome in Japan is reported to be about 0.3/100,000. There is no racial predilection to POEMS syndrome. There is no well established data regarding the gender predilection of POEMS syndrome. Data from Japan shows a male predilection of 2.5:1. The majority of POEMS syndrome cases have been reported in Japan and China. According to the The International Myeloma Working Group, the diagnosis of POEMS syndrome may be established if both mandatory criteria, one major and one minor criteria are fulfilled. Mandatory criteria include presence of polyneuropathy and a monoclonal plasma cell proliferative disorder. Major criteria include presence of sclerotic bone lesions or mixed sclerotic/lytic lesions, presence of Castleman’s disease and elevated serum VEGF levels. Minor criteria include presence of organomegaly, extravascular volume overload, endocrinopathy, skin changes, papilledema, thrombocytosis and polycythemia. Patients suffering from POEMS syndrome may have variable presentation and can present a diagnostic challenge for the clinician due to non-specific symptomology. Common symptoms of POEMS syndrome include numbness, tingling and weakness affecting extremities, fatigue, generalized pain in the body, foot drop, blurred vision, peripheral edema, dyspnea and hyperpigmentation. Less common symptoms include muscle weakness, diplopia, ocular pain and ascites. Laboratory findings consistent with the diagnosis of POEMS syndrome include increased serum VEGF level, increased number of thrombocytes, increased number of erythrocytes, elevated cerebrospinal fluid (CSF) protein content, increased number of leukocytes, low levels of IgG lambda or IgA lambda M-protein in the serum, and increased number of plasma cells in the bone marrow. An x-ray may be helpful in the diagnosis of POEMS syndrome. Findings on an x-ray suggestive of POEMS syndrome include osteolytic bone lesions, pleural effusion, increased cardiac silhouette (secondary to pericardial effusion), and ascites. CT scan may be helpful in the diagnosis of POEMS syndrome. Findings on CT scan suggestive of POEMS syndrome include bone lesions, lymphadenopathy, hepatomegaly, splenomegaly, pleural effusion, pericardial effusion, and ascites. MRI may be helpful in the diagnosis of POEMS syndrome. Findings on MRI suggestive of POEMS syndrome include diffuse lumbosacral nerve root enhancement, bone lesions. Echocardiography/ultrasound may be helpful in the diagnosis of POEMS syndrome. Findings on echocardiography/ultrasound suggestive of POEMS syndrome include pericardial effusion, left ventricular hypertrophy with moderately impaired systolic function, pulmonary hypertension, seroperitoneum, and hepatosplenomegaly. CT scan may be helpful in the diagnosis of POEMS syndrome. Findings on CT scan suggestive of POEMS syndrome include bone lesions, lymphadenopathy, hepatomegaly, splenomegaly, pleural effusion, pericardial effusion, and ascites. MRI may be helpful in the diagnosis of POEMS syndrome. Findings on MRI suggestive of POEMS syndrome include diffuse lumbo–sacral nerve root enhancement and bone lesions. (18)F-FDG PET/CT is an adequate tool for evaluation, diagnosis, and monitoring of the pathology. (18)F-FDG PET/CT may be helpful in the diagnosis of POEMS syndrome. Findings suggestive of POEMS syndrome include mixed bone lesions, lymphadenopathy, hepatosplenomegaly, and serous cavity effusions. Fluorescein angiography may reveal unilateral pooling of fluid consistent with cystoid macular edema. Optical coherence tomography (OCT) may show loss of retinal nerve fiber layer thickness. Other diagnostic studies that can help in making the diagnosis of POEMS syndrome include nerve conduction study, electromyograpy, fundoscopy, serum plasma electrophoresis and immunofixation electrophoresis, visual field testing, and pulmonary function test. Patients with isolated bone lesion without bone marrow clonal plasma cells involvement can be treated with radiotherapy. Patients with a disseminated disease (more bone lesions and/or bone marrow plasmacytosis) are the candidates for systemic therapy. Systemic therapy includes corticosteroids, autologous stem cell transplantation (ASCT), induction therapy, alkylator-based therapy, thalidomide, lenalidomide, bortezomib, and bevacizumab. Surgical intervention is not recommended for the management of POEMS syndrome. There are no established measures for the primary prevention of POEMS syndrome. There are no established measures for the secondary prevention of POEMS syndrome.
Historical Perspective
In 1938, Ilya Mark Scheinker, a Russian neurologist and neuropathologist described a patient with a solitary plasmacytoma, sensorimotor polyneuropathy, and localized patches of thickened and deeply pigmented skin. In 1956, R. S. Crow published two case reports of myelomatosis with peripheral neuritis and other striking features. In 1977, Iwashita et al described a patient who had an osteosclerotic myeloma accompanied by sensorimotor polyneuropathy, skinhyperipigmentation, edema, hypertrichosis, gynecomastia, and white nails. In 1980, Bardwick et al proposed the acronym ‘POEMS’ to represent a syndrome characterized by polyneuropathy, organomegaly, endocrinopathy, M protein, and skin changes.
Pathophysiology
POEMS syndrome is an acronym, where the ‘P’ stands for polyneuropathy, ‘O’ for organomegaly (specifically of the liver and spleen), ‘E’ for endocrinopathy, ‘M’ for immunoglobulin (para-protein or M-protein) and ‘S’ for skin changes. POEMS syndrome is a para-neoplastic syndrome characterized by multi-organ system dysfunction, monoclonal plasma cell proliferation and demyelinating inflammatory polyneuropathy. The lambda component of immunoglobulin light chains is thought to be overproduced in POEMS syndrome secondary to monoclonal plasma cell proliferation. Bone marrow studies of patients suffering from POEMS syndrome shows lymphoid aggregates rimmed by monotypic or polytypic plasma cells. The monoclonal gammopathy or overproduction of lambda light chain stimulates the monocyte/macrophage system to produce various proinflammatory cytokines. such as interleukin-1, interleukin-6, interleukin-12, vascular endothelial growth factor (VEGF) and TNF-Alpha. Transforming growth factor beta (TGF-beta), an inhbitory cytokine is thought to be underproduced in patients suffering from POEMS syndrome leading to a storm of proinflammatory cytokines which drive the disease process. The overproduction of this IL-6 may be related to some of the clinical features seen in POEMS syndrome such as gammopathy, elevated C-Reactive protein (CRP) and thrombocytosis. The mesangial proliferation and membranoproliferative glomerulonephritis (MPGN) seen in POEMS syndrome is thought to be secondary to increased production of platelet-derived growth factor(PDGF) and fibroblast growth factor beta (FGF-β) have been implicated in mesangial cell proliferation. The neovascularization induced by VEGF leads to increased vascular permeability. Since the increased production of VEGF is unchecked due to the plasma cell dyscrasia, the consequence is an unregulated extravasation of intravascular fluid into the extravascular compartment. resulting in edema. POEMS syndrome is known to be associated multiple myeloma (osteosclerotic type), Castleman’s disease, plasmacytoma, monoclonal gammopathy of undetermined significance (MGUS), pulmonary hypertension, restrictive lung disease, thrombophilia, cardiac amyloidosis and papilledema. The most potent risk factor leading to the development of POEMS syndrome is multiple myeloma of osteosclerotic type.
Causes
There are no known and well established causes of POEMS syndrome. Marked activation of the pro-inflammatory cytokines and weak or decreased TGF beta 1 action can play a role in the disease pathogenesis.
Differential Diagnosis
The diagnosis of POEMS syndrome presents a diagnostic challenge for the physician. A thorough examination of organ systems should be attempted in order to reach a confirmed diagnosis. POEMS syndrome should be differentiated from other conditions presenting as a polyneuropathy (metabolic syndrome, vitamin B12 deficiency, Guillain-Barre syndrome, chronic inflammatory demyelinating polyneuropathy and multifocal motor polyneuropathy), organomegaly with lymphadenopathy (malaria, leshmaniasis or kala-azar, infective hepatitis, chronic myelogenous leukemia, lymphoma, primary amyloidosis, Gaucher’s disease), endocrinopathy (hypogonadism, hypothyroidism, hypopituitarism), monoclonal plasma cell proliferation (multiple myeloma, monoclonal gammopathy of undetermined significance, plasmacytoma), mixed lytic/sclerotic bone lesions (osteomalacia, osteogenesis imperfecta) and skin changes.
Epidemiology and Demographics
The precise incidence of POEMS syndrome is difficult to determine and we have no well established data to quote. The median age at presentation has been 51 years with the majority of the patients comprising of males. A mediansurvival of 165 months has also been recorded. The precise incidence of POEMS syndrome is difficult to determine due to the complexity of the syndrome presentation and we have no well established data regarding the incidence. Prevalence of POEMS syndrome in Japan is reported to be about 0.3/100,000. There is no racial predilection to POEMS syndrome. There is no well established data regarding the gender predilection of POEMS syndrome. Data from Japan shows a male predilection of 2.5:1. The majority of POEMS syndrome cases have been reported in Japan and China.
Risk Factors
The most potent risk factor leading to the development of POEMS syndrome is multiple myeloma of osteosclerotic type.
Screening
There is insufficient evidence to recommend routine screening for POEMS syndrome.
Natural History, Complications, and Prognosis
POEMS syndrome presents as a chronic progressive polyneuropathy. Patients may have coexisting multi-organ system disorders. The neuropathy is usually symmetrical and ascending. Endocrinopathy, present in majority of cases, involves hypogonadism, hypothyroidism, and abnormalities of the pituitary–adrenal axis. If left untreated, patients suffering from POEMS syndrome may become wheel chair bound. Complications of POEMS syndrome include renal failure, pulmonary hypertension, pathologic fractures, ischemic stroke, restrictive lung disease, polycythemia, thrombocytosis, papilledema, and myocardial infarction. 3, 5, and 10 year overall survival (OS) for patients newly diagnosed with POEMS syndrome is 87.7%, 84.1%, and 77%. Age >50 years, pulmonary hypertension, pleural effusion, and estimated glomerular filtration rate <30 ml/min/1.73 m2 were associated with inferior overall survival in the derivation cohort, with the use of multivariate Cox regression model based on randomized sample splitting of 362 patients. Low albumin (defined as<3.2 g/dl) at diagnosis and failure to achieve a complete hematologic response to first-line therapy can be independent risk factors for progression-free survival (PFS). Improvement of plasma cell dyscrasia leads to improvement or marked reduction in other abnormalities. Neuropathy, stroke, and myocardial infarction are the most common causes of death in POEMS syndrome.
Diagnosis
Diagnostic Study of Choice
According to the The International Myeloma Working Group, the diagnosis of POEMS syndrome may be established if both mandatory criteria, one major and one minor criteria are fulfilled. Mandatory criteria include presence of polyneuropathy and a monoclonal plasma cell proliferative disorder. Major criteria include presence of sclerotic bone lesions or mixed sclerotic/lytic lesions, presence of Castleman’s disease and elevated serum VEGF levels. Minor criteria include presence of organomegaly, extravascular volume overload, endocrinopathy, skin changes, papilledema, thrombocytosis and polycythemia.
History and Symptoms
Patients suffering from POEMS syndrome may have variable presentation and can present a diagnostic challenge for the clinician due to non-specific symptomology. Common symptoms of POEMS syndrome include numbness, tingling and weakness affecting extremities, fatigue, generalized pain in the body, foot drop, blurred vision, peripheral edema, dyspnea and hyperpigmentation. Less common symptoms include muscle weakness, diplopia, ocular pain and ascites.
Physical Examination
Common physical examination findings of POEMS syndrome include, organomegaly (hepatomegaly, splenomegaly), peripheral edema/anasarca, ascites, mixed lytic/sclerotic bone lesions, papilledema, skin hyperpigmentation and lymphadenopathy.
Laboratory Findings
Laboratory findings consistent with the diagnosis of POEMS syndrome include increased serum VEGF level, increased number of thrombocytes, increased number of erythrocytes, elevated cerebrospinal fluid (CSF) protein content, increased number of leukocytes, low levels of IgG lambda or IgA lambda M-protein in the serum, and increased number of plasma cells in the bone marrow.
Electrocardiogram
There are no ECG findings associated with POEMS syndrome.
X-ray
An x-ray may be helpful in the diagnosis of POEMS syndrome. Findings on an x-ray suggestive of POEMS syndrome include osteolytic bone lesions, pleural effusion, increased cardiac silhouette (secondary to pericardial effusion), and ascites.
Echocardiography and Ultrasound
Echocardiography/ultrasound may be helpful in the diagnosis of POEMS syndrome. Findings suggestive of POEMS syndrome include pericardial effusion, left ventricular hypertrophy with moderately impaired systolic function, pulmonary hypertension, seroperitoneum, and hepatosplenomegaly.
CT Scan
CT scan may be helpful in the diagnosis of POEMS syndrome. Findings on CT scan suggestive of POEMS syndrome include bone lesions, lymphadenopathy, hepatomegaly, splenomegaly, pleural effusion, pericardial effusion, and ascites.
MRI
MRI may be helpful in the diagnosis of POEMS syndrome. Findings on MRI suggestive of POEMS syndrome include diffuse lumbo–sacral nerve root enhancement and bone lesions.
Other Imaging Findings
(18)F-FDG PET/CT is an adequate tool for evaluation, diagnosis, and monitoring of the pathology. (18)F-FDG PET/CT may be helpful in the diagnosis of POEMS syndrome. Findings suggestive of POEMS syndrome include mixed bone lesions, lymphadenopathy, hepatosplenomegaly, and serous cavity effusions. Fluorescein angiography may reveal unilateral pooling of fluid consistent with cystoid macular edema. Optical coherence tomography (OCT) may show loss of retinal nerve fiber layer thickness.
Other Diagnostic Studies
Other diagnostic studies that can help in making the diagnosis of POEMS syndrome include nerve conduction study, electromyograpy, fundoscopy, serum plasma electrophoresis and immunofixation electrophoresis, visual field testing, and pulmonary function test.
Treatment
Medical Therapy
Patients with isolated bone lesion without bone marrow clonal plasma cells involvement can be treated with radiotherapy. Patients with a disseminated disease (more bone lesions and/or bone marrow plasmacytosis) are the candidates for systemic therapy. Systemic therapy includes corticosteroids, autologous stem cell transplantation (ASCT), induction therapy, alkylator-based therapy, thalidomide, lenalidomide, bortezomib, and bevacizumab.
Surgery
Surgical intervention is not recommended for the management of POEMS syndrome.
Primary Prevention
There are no established measures for the primary prevention of POEMS syndrome.
Secondary Prevention
There are no established measures for the secondary prevention of POEMS syndrome.
Historical Perspective
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]Associate Editor(s)-in-Chief: Sabawoon Mirwais, M.B.B.S, M.D.[2]
Overview
In 1938, Ilya Mark Scheinker, a Russian neurologist and neuropathologist described a patient with a solitary plasmacytoma, sensorimotor polyneuropathy, and localized patches of thickened and deeply pigmented skin. In 1956, R. S. Crow published two case reports of myelomatosis with peripheral neuritis and other striking features. In 1977, Iwashita et al described a patient who had an osteosclerotic myeloma accompanied by sensorimotor polyneuropathy, skin hyperipigmentation, edema, hypertrichosis, gynecomastia, and white nails. In 1980, Bardwick et al proposed the acronym ‘POEMS’ to represent a syndrome characterized by polyneuropathy, organomegaly, endocrinopathy, M protein, and skin changes.
Historical Perspective
Discovery
- In 1938, Ilya Mark Scheinker, a Russian neurologist and neuropathologist described a patient with a solitary plasmacytoma, sensorimotor polyneuropathy, and localized patches of thickened and deeply pigmented skin.[1][2]
- POEMS syndrome has been recognized by various names over the years, such as osteosclerotic myeloma, Crow-Fukase syndrome, PEP syndrome, and Takatsuki syndrome.[1]
- In 1956, R. S. Crow published two case reports of myelomatosis with peripheral neuritis and other striking features.[3]
- In 1977, Iwashita et al described a patient who had an osteosclerotic myeloma accompanied by sensorimotor polyneuropathy, skin hyperipigmentation, edema, hypertrichosis, gynecomastia, and white nails.[4]
- In 1980, Bardwick et al proposed the acronym ‘POEMS’ to represent a syndrome characterized by polyneuropathy, organomegaly, endocrinopathy, M protein, and skin changes.[5]
Synonyms of POEMS syndrome
- Crow-Fukase syndrome[6]
- Osteosclerotic myeloma[7]
- PEP syndrome[8]
- Polyneuropathy–organomegaly–endocrinopathy–M protein–skin lesions[9]
- Shimpo syndrome[10]
- Takatsuki syndrome[11]
References
- ↑ 1.0 1.1 Dispenzieri, A. (2002). “POEMS syndrome: definitions and long-term outcome”. Blood. 101 (7): 2496–2506. doi:10.1182/blood-2002-07-2299. ISSN 0006-4971.
- ↑ Scheinker I. Myelom und Nervensystem: über eine bisher nicht beschriebene mit eigentümlichen Hautveränderungen einhergehende Polyneuritis bei einem plasmazellulären myelom des Sternums. Dtsch Z Nervenheilkd 1938; 147: 247
- ↑ CROW RS (October 1956). “Peripheral neuritis in myelomatosis”. Br Med J. 2 (4996): 802–4. PMC 2035359. PMID 13364332.
- ↑ Iwashita H, Ohnishi A, Asada M, Kanazawa Y, Kuroiwa Y (July 1977). “Polyneuropathy, skin hyperpigmentation, edema, and hypertrichosis in localized osteosclerotic myeloma”. Neurology. 27 (7): 675–81. PMID 559975.
- ↑ Bardwick PA, Zvaifler NJ, Gill GN, Newman D, Greenway GD, Resnick DL (July 1980). “Plasma cell dyscrasia with polyneuropathy, organomegaly, endocrinopathy, M protein, and skin changes: the POEMS syndrome. Report on two cases and a review of the literature”. Medicine (Baltimore). 59 (4): 311–22. PMID 6248720.
- ↑ https://rarediseases.org/rare-diseases/poems-syndrome/
- ↑ https://rarediseases.org/rare-diseases/poems-syndrome/
- ↑ https://rarediseases.org/rare-diseases/poems-syndrome/
- ↑ https://rarediseases.org/rare-diseases/poems-syndrome/
- ↑ https://rarediseases.org/rare-diseases/poems-syndrome/
- ↑ https://rarediseases.org/rare-diseases/poems-syndrome/
Pathophysiology
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1] Associate Editor(s)-in-Chief: Syed Hassan A. Kazmi BSc, MD [2]
Overview
POEMS syndrome is an acronym, where the ‘P’ stands for polyneuropathy, ‘O’ for organomegaly (specifically of the liver and spleen), ‘E’ for endocrinopathy, ‘M’ for immunoglobulin (para-protein or M-protein) and ‘S’ for skin changes. POEMS syndrome is a para-neoplastic syndrome characterized by multi-organ system dysfunction, monoclonal plasma cell proliferation and demyelinating inflammatory polyneuropathy. The lambda component of immunoglobulin light chains is thought to be overproduced in POEMS syndrome secondary to monoclonal plasma cell proliferation. Bone marrow studies of patients suffering from POEMS syndrome shows lymphoid aggregates rimmed by monotypic or polytypic plasma cells. The monoclonal gammopathy or overproduction of lambda light chain stimulates the monocyte/macrophage system to produce various proinflammatory cytokines. such as interleukin-1, interleukin-6, interleukin-12, vascular endothelial growth factor (VEGF) and TNF-Alpha. Transforming growth factor beta (TGF-beta), an inhbitory cytokine is thought to be underproduced in patients suffering from POEMS syndrome leading to a storm of proinflammatory cytokines which drive the disease process. The overproduction of this IL-6 may be related to some of the clinical features seen in POEMS syndrome such as gammopathy, elevated C-Reactive protein (CRP) and thrombocytosis. The mesangial proliferation and membranoproliferative glomerulonephritis (MPGN) seen in POEMS syndrome is thought to be secondary to increased production of platelet-derived growth factor (PDGF) and fibroblast growth factor beta (FGF-β) have been implicated in mesangial cell proliferation. The neovascularization induced by VEGF leads to increased vascular permeability. Since the increased production of VEGF is unchecked due to the plasma cell dyscrasia, the consequence is an unregulated extravasation of intravascular fluid into the extravascular compartment. resulting in edema. POEMS syndrome is known to be associated multiple myeloma (osteosclerotic type), Castleman’s disease, plasmacytoma, monoclonal gammopathy of undetermined significance (MGUS), pulmonary hypertension, restrictive lung disease, thrombophilia, cardiac amyloidosis and papilledema.
Pathophysiology
POEMS syndrome is an acronym, where the ‘P’ stands for polyneuropathy, ‘O’ for organomegaly, ‘E’ for endocrinopathy, ‘M’ for immunoglobulin (para-protein or M-protein) and ‘S’ for skin changes. POEMS syndrome is a para-neoplastic syndrome characterized by multi-organ system dysfunction, monoclonal plasma cell proliferation and demyelinating inflammatory polyneuropathy.[1]
Pathogenesis
Monoclonal Plasma Cell Proliferation
- POEMS syndrome is associated with plasma cell dyscrasia in which there is monoclonal proliferation of plasma cells. The plasma cells are involved in antibody production under physiological conditions via reorganization of immunoglobulin heavy and light chains.
- The lambda component of immunoglobulin light chains is thought to be overproduced in POEMS syndrome secondary to monoclonal plasma cell proliferation.[2]
- Bone marrow studies of patients suffering from POEMS syndrome shows lymphoid aggregates rimmed by monotypic or polytypic plasma cells.
- Diffuse infiltration of light chain restricted plasma cells leads to development of predominantly sclerotic bone lesions. This is in contrast with myeloma patients where there is a predominance of lytic bone lesions. The bony lesions are primarily restricted to the axial and proximal appendicular skeleton.[3][4][5]
- The monoclonal gammopathy or overproduction of lambda light chain stimulates the monocyte/macrophage system to produce various proinflammatory cytokines.
Cytokine Storm
- The monoclonal plasma cell proliferation in POEMS syndrome is thought to play a major role in overproduction of numerous pro-angiogenic and pro-inflammatory cytokines.
- The hypercytokinetic state induced in patients of POEMS syndrome is thought to drive the disease process. The following cytokines are overproduced:[6]
Role of Interleukin-6 , Interleukin-12 and TNF-Alpha
- Interleukin- 6 is overproduced in patients with POEMS syndrome. IL-6 is a pro-inflammatory cytokine involved in maturation of B-cells into antibody producing plasma cells, induction of acute phase reactants and thrombopoeisis.[11][12][13] The overproduction of this cytokine may be related to some of the clinical features seen in POEMS syndrome such as gammopathy, elevated C-Reactive protein (CRP) and thrombocytosis.[14][15]
- Interleukin-1 beta and interleukin-6 both are also involved in increased production of VEGF in POEMS syndrome.[16]
Upregulation of VEGF production
- VEGF is a pro-angiogenic cytokine that promotes neovascularization. It is thought to be overproduced in POEMS syndrome and can serve as a marker of disease activity in these patients.
- VEGF is expressed by osteoblasts, chondrocytes, macrophages, tumor cells (including plasma cells) and megakaryocytes.
- VEGF165 is the isoform of VEGF that is overexpressed in POEMS syndrome.
- Increased VEGF could account for the organomegaly, edema, skin hemangiomata, and possibly the occasional mesangioproliferative changes found on renal biopsy.
- Since VEGF is expressed by osteoblasts and has a role in osteoblastic differentiation, the bone condensation (sclerosis) seen in POEMS syndrome may also be partly attributed to increased circulating VEGF levels.[17]
- The mesangial proliferation and membranoproliferative glomerulonephritis (MPGN) seen in POEMS syndrome is thought to be secondary to increased production of platelet-derived growth factor (PDGF), transforming growth factor beta (TGF-β), and fibroblast growth factor beta (FGF-β) have been implicated in mesangial cell proliferation. It has been suggested that FGF-β participates in the initiation, PDGF in the maintenance, and TGF-β (an inhibitory cytokine) in the resolution of the proliferation.[18]
Neovascularization and Edema
- The neovascularization induced by VEGF leads to increased vascular permeability. Since the increased production of VEGF is unchecked due to the plasma cell dyscrasia, the consequence is an unregulated extravasation of intravascular fluid into the extravascular compartment.
- As a result, there is accumulation of fluid in the extracellular compartment and the resultant edema seen in patients of POEMS syndrome.
Alteration of Blood-Nerve Barrier and Secondary Axonal Degenration
- Unregulated neovascularization also leads to disruption of the blood-nerve barrier in the peripheral nervous system (PNS), which subsequently results in endoneural edema. The edema compresses the nerves and eventually leads to secondary axonal degeneration.
Associated Conditions
POEMS syndrome is known to be associated with the following conditions:[19]
- Multiple myeloma (osteosclerotic type)
- Castleman’s disease
- Plasmacytoma
- Monoclonal gammopathy of undetermined significance (MGUS).
- Pulmonary hypertension
- Restrictive lung disease
- Thrombophilia
- Cardiac amyloidosis
- Papilledema
- Necrotizing autoimmune myopathy[20]
Gross Pathology
- POEMS syndrome is known to cause organomegaly, specially of the liver and spleen.
- A normal liver is less than 16 cm on ultrasound evaluation. Hepatomegaly may be found during physical examination or on imaging studies. Imaging is more accurate in determining liver size.[21][22]

Microscopic Pathology
- POEMS syndrome is most often associated with multiple myeloma.
- On microscopic histopathological analysis, multiple myeloma is characterized by the following:[23]
- Abundant eosinophilic cytoplasm
- Eccentrically placed nucleus
- Clock face morphology of the nucleus due to chromatin clumps around the edges
- Russell bodies which are eosinophilic, large (10-15 micrometres), homogenous immunoglobulin-containing inclusions
- Dutcher bodies which are PAS stain +ve intranuclear crystalline rods
- Shown below is a series of microscopic images seen in multiple myeloma:
-
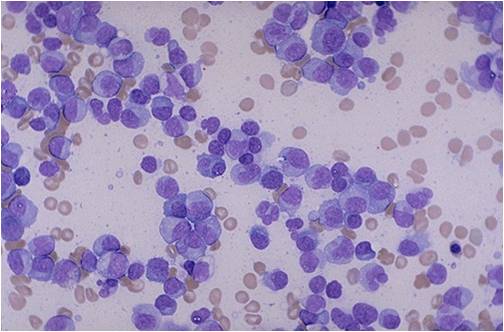 Bone marrow aspiration in multiple myeloma.
Bone marrow aspiration in multiple myeloma.
(Image courtesy of Melih Aktan M.D.) -
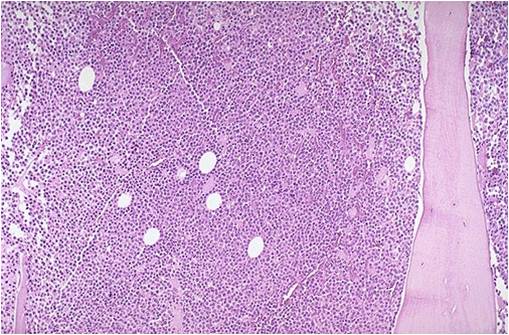 Bone marrow biopsy in multiple myeloma.
Bone marrow biopsy in multiple myeloma.
(Image courtesy of Melih Aktan M.D.) -
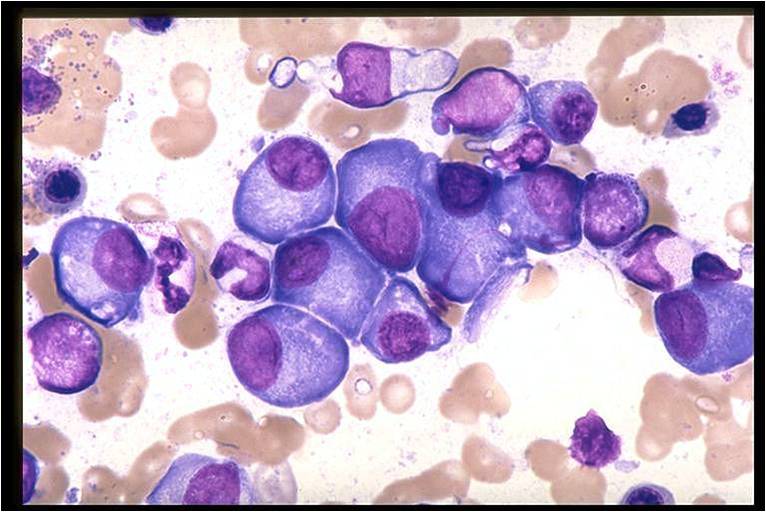 Bone marrow in multiple myeloma.
Bone marrow in multiple myeloma.
(Image courtesy of Melih Aktan M.D.) -
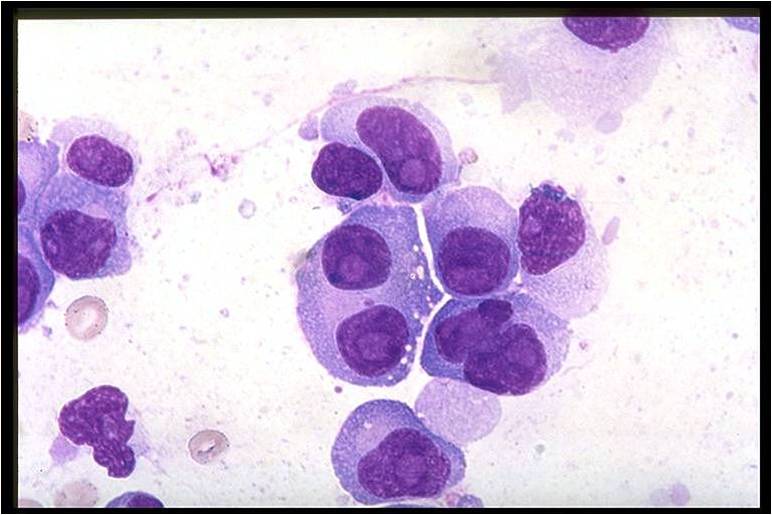 Bone marrow in multiple myeloma.
Bone marrow in multiple myeloma.
(Image courtesy of Melih Aktan M.D.) -
![Multiple myeloma slide with intermediate magnification[23]](https://www.wikidoc.org/images/4/40/Multiple_myeloma_intermed_mag.jpg) Multiple myeloma slide with intermediate magnification[23]
Multiple myeloma slide with intermediate magnification[23] -
![Multiple myeloma slide with high magnification[23]](https://www.wikidoc.org/images/d/d5/Multiple_myeloma.jpg) Multiple myeloma slide with high magnification[23]
Multiple myeloma slide with high magnification[23] -
![Multiple myeloma slide with russell bodies[23]](https://www.wikidoc.org/images/a/ad/Russell_bodies.jpg) Multiple myeloma slide with russell bodies[23]
Multiple myeloma slide with russell bodies[23]




![Multiple myeloma slide with intermediate magnification[23]](https://www.wikidoc.org/index.php/File%3AMultiple_myeloma_intermed_mag.jpg)
![Multiple myeloma slide with high magnification[23]](https://www.wikidoc.org/index.php/File%3AMultiple_myeloma.jpg)
![Multiple myeloma slide with russell bodies[23]](https://www.wikidoc.org/index.php/File%3ARussell_bodies.jpg)
References
- ↑ Aggarwal S, Goulatia RK, Sood A, Prasad K, Ahuja GK, Mitchell MJ, Kumar A (August 1990). “POEMS syndrome: a rare variety of plasma cell dyscrasia”. AJR Am J Roentgenol. 155 (2): 339–41. doi:10.2214/ajr.155.2.2115264. PMID 2115264.
- ↑ Wang C, Su W, Zhang W, Di Q, Duan MH, Ji W, Cao XX, Zhou DB, Li J (July 2014). “Serum immunoglobulin free light chain and heavy/light chain measurements in POEMS syndrome”. Ann. Hematol. 93 (7): 1201–6. doi:10.1007/s00277-014-2019-y. PMID 24482101.
- ↑ Bardwick PA, Zvaifler NJ, Gill GN, Newman D, Greenway GD, Resnick DL (July 1980). “Plasma cell dyscrasia with polyneuropathy, organomegaly, endocrinopathy, M protein, and skin changes: the POEMS syndrome. Report on two cases and a review of the literature”. Medicine (Baltimore). 59 (4): 311–22. PMID 6248720.
- ↑ Nakanishi T, Sobue I, Toyokura Y, Nishitani H, Kuroiwa Y, Satoyoshi E, Tsubaki T, Igata A, Ozaki Y (June 1984). “The Crow-Fukase syndrome: a study of 102 cases in Japan”. Neurology. 34 (6): 712–20. PMID 6539431.
- ↑ Resnick D, Greenway GD, Bardwick PA, Zvaifler NJ, Gill GN, Newman DR (July 1981). “Plasma-cell dyscrasia with polyneuropathy, organomegaly, endocrinopathy, M-protein, and skin changes: the POEMS syndrome. Distinctive radiographic abnormalities”. Radiology. 140 (1): 17–22. doi:10.1148/radiology.140.1.7244223. PMID 7244223.
- ↑ “Elevated levels of interleukin-1 beta (IL-1 beta) and IL-6 in serum and increased production of IL-1 beta mRNA in lymph nodes of patients with polyneuropathy, organomegaly, endocrinopathy, M protein, and skin changes (POEMS) syndrome | Blood Journal”.
- ↑ Mandler RN, Kerrigan DP, Smart J, Kuis W, Villiger P, Lotz M (June 1992). “Castleman’s disease in POEMS syndrome with elevated interleukin-6”. Cancer. 69 (11): 2697–703. PMID 1571900.
- ↑ Kanai K, Sawai S, Sogawa K, Mori M, Misawa S, Shibuya K, Isose S, Fujimaki Y, Noto Y, Sekiguchi Y, Nasu S, Nakaseko C, Takano S, Yoshitomi H, Miyazaki M, Nomura F, Kuwabara S (August 2012). “Markedly upregulated serum interleukin-12 as a novel biomarker in POEMS syndrome”. Neurology. 79 (6): 575–82. doi:10.1212/WNL.0b013e318263c42b. PMID 22843279.
- ↑ Koike H, Iijima M, Mori K, Yamamoto M, Hattori N, Watanabe H, Tanaka F, Doyu M, Sobue G (October 2008). “Neuropathic pain correlates with myelinated fibre loss and cytokine profile in POEMS syndrome”. J. Neurol. Neurosurg. Psychiatry. 79 (10): 1171–9. doi:10.1136/jnnp.2007.135681. PMID 18356256.
- ↑ Watanabe O, Arimura K, Kitajima I, Osame M, Maruyama I (March 1996). “Greatly raised vascular endothelial growth factor (VEGF) in POEMS syndrome”. Lancet. 347 (9002): 702. PMID 8596427.
- ↑ Yoshizaki K, Nakagawa T, Kaieda T, Muraguchi A, Yamamura Y, Kishimoto T (March 1982). “Induction of proliferation and Ig production in human B leukemic cells by anti-immunoglobulins and T cell factors”. J. Immunol. 128 (3): 1296–301. PMID 6799573.
- ↑ Muraguchi A, Hirano T, Tang B, Matsuda T, Horii Y, Nakajima K, Kishimoto T (February 1988). “The essential role of B cell stimulatory factor 2 (BSF-2/IL-6) for the terminal differentiation of B cells”. J. Exp. Med. 167 (2): 332–44. PMC 2188837. PMID 3258006.
- ↑ Gauldie J, Richards C, Harnish D, Lansdorp P, Baumann H (October 1987). “Interferon beta 2/B-cell stimulatory factor type 2 shares identity with monocyte-derived hepatocyte-stimulating factor and regulates the major acute phase protein response in liver cells”. Proc. Natl. Acad. Sci. U.S.A. 84 (20): 7251–5. PMC 299269. PMID 2444978.
- ↑ Hitoshi S, Okazawa H, Shimizu J, Suzuki K, Sakuta M (July 1991). “[A case of Crow-Fukase syndrome with increased serum interleukin-6]”. Rinsho Shinkeigaku (in Japanese). 31 (7): 730–3. PMID 1786657.
- ↑ Mandler RN, Kerrigan DP, Smart J, Kuis W, Villiger P, Lotz M (June 1992). “Castleman’s disease in POEMS syndrome with elevated interleukin-6”. Cancer. 69 (11): 2697–703. PMID 1571900.
- ↑ Soubrier, Martin; Dubost, Jean-Jacques; Serre, Anne Françhise; Ristori, Jean-Michel; Sauvezie, Bernard; Cathebras, Pascal; Piette, Jean-Charles; Chapman, Antoine; Authier, François-Jérôme; Gherardi, Romain K. (1997). “Growth factors in POEMS syndrome: Evidence for a marked increase in circulating vascular endothelial growth factor”. Arthritis & Rheumatism. 40 (4): 786–787. doi:10.1002/art.1780400430. ISSN 0004-3591.
- ↑ “Vascular Endothelial Growth Factor, a Potent and Selective Angiogenic Agent”.
- ↑ “HarvardKey Login”.
- ↑ Pei G, Yang D, Sun J, Luo Y, Yan J, Chen Y (2015). “Cardiac Involvement in a Patient With POEMS Syndrome Detected Using Cardiac Magnetic Resonance Imaging”. Int Heart J. 56 (5): 571–3. doi:10.1536/ihj.15-038. PMID 26346518.
- ↑ Gremain V, Litrowski N, Boulard C, Marguet F, Courville P, Zarnitsky C, Langlois V (January 2018). “Necrotizing autoimmune myopathy associated with POEMS syndrome report”. QJM. 111 (1): 49–50. doi:10.1093/qjmed/hcx197. PMID 29088446.
- ↑ Sapira JD, Williamson DL (1979). “How big is the normal liver?”. Arch Intern Med. 139 (9): 971–3. PMID 475535.
- ↑ Niederau C, Sonnenberg A, Müller JE, Erckenbrecht JF, Scholten T, Fritsch WP (1983). “Sonographic measurements of the normal liver, spleen, pancreas, and portal vein”. Radiology. 149 (2): 537–40. doi:10.1148/radiology.149.2.6622701. PMID 6622701.
- ↑ 23.0 23.1 23.2 23.3 Multiple myeloma. Librepathology (2015)http://www.wikidoc.org/index.php?title=Multiple_myeloma_pathophysiology&action=edit§ion=1 Accessed on September, 20th 2015
Causes
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Sabawoon Mirwais, M.B.B.S, M.D.[2]
Overview
There are no known and well established causes of POEMS syndrome. Marked activation of the pro-inflammatory cytokines and weak or decreased TGF beta 1 action can play a role in the disease pathogenesis.
Causes
- There are no known and well established causes of POEMS syndrome.
- Some studies suggest that marked activation of the pro-inflammatory cytokines (IL-1 beta, IL-6, and TNF-alpha) play a role in the disease pathogenesis.[1]
- Weak or even decreased (TGF beta 1) antagonistic reaction insufficient to counteract the noxious effects of cytokines can also result in this syndrome.[1]
References
Differentiating POEMS syndrome from other Diseases
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1] Associate Editor(s)-in-Chief: Syed Hassan A. Kazmi BSc, MD [2]
Overview
The diagnosis of POEMS syndrome presents a diagnostic challenge for the physician. A thorough examination of organ systems should be attempted in order to reach a confirmed diagnosis. POEMS syndrome should be differentiated from other conditions presenting as a polyneuropathy (metabolic syndrome, vitamin B12 deficiency, Guillain-Barre syndrome, chronic inflammatory demyelinating polyneuropathy and multifocal motor polyneuropathy), organomegaly with lymphadenopathy (malaria, leshmaniasis or kala-azar, infective hepatitis, chronic myelogenous leukemia, lymphoma, primary amyloidosis, Gaucher’s disease), endocrinopathy (hypogonadism, hypothyroidism, hypopituitarism), monoclonal plasma cell proliferation (multiple myeloma, monoclonal gammopathy of undetermined significance, plasmacytoma), mixed lytic/sclerotic bone lesions (osteomalacia, osteogenesis imperfecta) and skin changes.
Differentiating POEMS Syndrome From Other Diseases
The diagnosis of POEMS syndrome presents a diagnostic challenge for the physician. A thorough examination of organ systems should be attempted in order to reach a confirmed diagnosis. POEMS syndrome should be differentiated from other conditions presenting as a polyneuropathy, organomegaly, endocrinopathy, monoclonal plasma cell proliferation, mixed lytic/sclerotic bone lesions and skin changes. The differentials include the following:
| Organ System Involvement | Differential Diagnosis | Causes | Clinical Features | Laboratory Findings | Gold Standard Test | Therapy | |
|---|---|---|---|---|---|---|---|
| P = Polyneuropathy | POEMS syndrome (Demyelinating)[1] |
|
|
||||
| Metabolic Syndrome (Axonal pathology)[8] |
|
|
|
||||
| Vitamin Deficiencies (Axonal Pathology)[10] |
|
|
|
| |||
| Guillain-Barre Syndrome (Demyelinating)[16] |
|
|
|
||||
| Chronic Inflammatory Demyelinating Polyneuropathy (CIDP) (Mixed axonal and demyelinatiing)[24][25] |
|
|
|
||||
| Multifocal Motor Neuropathy[35] |
|
||||||
| Organ System Involvement | Differential Diagnosis | Causes | Features | Laboratory Findings | Gold Standard Test | Therapy | |
| O = Organomegaly (Hepatosplenomegaly and Lymphadenopathy) | Malaria[37][38][39] |
|
|
| |||
| Kala-azar[40][41] |
|
|
|
||||
| Infective Hepatitis[42][43] |
|
|
|||||
| Chronic Myelogenous Leukemia (CML)[44][45][46][47][48][49][50][51][52][51] |
|
|
|||||
| Lymphoma |
|
|
|||||
| Primary (AL) Amyloidosis[54][55] |
|
|
|
||||
| Gaucher’s Disease[61] |
|
|
|
|
|||
| Organ System Involvement | Differential Diagnosis | Causes | Features | Laboratory Findings | Gold Standard Test | Therapy | |
| E = Endocrinopathy (Hypogonadism, Hypothyroidism, Hypopituitarism) | Hypogonadism[62][63] | Primary Hypogonadism (Hypergonadotrophic) |
|
|
|
||
| Secondary Hypogonadism (Hypogonadotrophic) |
| ||||||
| Hypothyroidism[64][65] | Primary Hypothyroidism |
|
|
||||
| Secondary Hypothyroidism |
|
||||||
| Tertiary Hypothyroidism |
|
||||||
| Hypopituitarism[66][67] | Congenital |
|
|
|
|
| |
| Acquired |
| ||||||
| Organ System Involvement | Differential Diagnosis | Causes | Features | Laboratory Findings | Gold Standard Test | Therapy | |
| M = M-protein ( Hematological Abnormality/Plasma Cell Dyscrasias) | Multiple myeloma[68][69][70] |
|
|
|
AND
|
| |
| Monoclonal gammopathy of undetermined significance (MGUS)[71] |
|
|
AND
AND
|
| |||
| Asymptomatic Plasma Cell Myeloma |
|
|
OR
AND/OR
AND
|
| |||
| Plasmacytoma |
|
|
|
|
| ||
| Bone Lesions | Osteoporosis |
|
|
|
|
| |
| Osteomalacia[72] |
|
|
|
|
| ||
| Osteogenesis imperfecta |
|
|
|
|
| ||
| Skin Changes | Scurvy |
|
| ||||
Other Differentials
POEMS syndrome must also be differentiated from other similar conditions which lead to multiple endocrine disorders such as autoimmune polyendocrine syndrome, Hirata syndrome, Kearns–Sayre syndrome and Wolfram syndromes.[73][74][75][76][77]
| Disease | Addison’s disease | Type 1 diabetes mellitus | Hypothyroidism | Other disorders present |
|---|---|---|---|---|
| POEMS syndrome | + | Less common | Less common | Hypoparathyroidism Candidiasis Hypogonadism |
| APS type 2 | + | + | + | Hypogonadism Malabsorption |
| APS type 3 | – | + | + | Malabsorption |
| Thymoma | + | – | + | Myasthenia gravis Cushing syndrome |
| Chromosomal abnormalities (Turner syndrome, Down’s syndrome) |
– | + | + | Cardiac dysfunction |
| Kearns–Sayre syndrome | – | + | – | Myopathy Hypoparathyroidism Hypogonadism |
| Wolfram syndrome | – | + | – | Diabetes insipidus Optic atrophy Deafness |
| POEMS syndrome | – | + | – | Polyneuropathy Hypogonadism Plasma cell dyscrasias |
References
- ↑ Gherardi RK, Bélec L, Soubrier M, Malapert D, Zuber M, Viard JP, Intrator L, Degos JD, Authier FJ (February 1996). “Overproduction of proinflammatory cytokines imbalanced by their antagonists in POEMS syndrome”. Blood. 87 (4): 1458–65. PMID 8608236.
- ↑ 2.0 2.1 Nozza A (2017). “POEMS SYNDROME: an Update”. Mediterr J Hematol Infect Dis. 9 (1): e2017051. doi:10.4084/MJHID.2017.051. PMC 5584767. PMID 28894560.
- ↑ 3.0 3.1 3.2 Bardwick PA, Zvaifler NJ, Gill GN, Newman D, Greenway GD, Resnick DL (July 1980). “Plasma cell dyscrasia with polyneuropathy, organomegaly, endocrinopathy, M protein, and skin changes: the POEMS syndrome. Report on two cases and a review of the literature”. Medicine (Baltimore). 59 (4): 311–22. PMID 6248720.
- ↑ 4.0 4.1 4.2 4.3 4.4 Takatsuki K, Sanada I (September 1983). “Plasma cell dyscrasia with polyneuropathy and endocrine disorder: clinical and laboratory features of 109 reported cases”. Jpn. J. Clin. Oncol. 13 (3): 543–55. PMID 6315993.
- ↑ Nobile-Orazio E, Terenghi F, Giannotta C, Gallia F, Nozza A (March 2009). “Serum VEGF levels in POEMS syndrome and in immune-mediated neuropathies”. Neurology. 72 (11): 1024–6. doi:10.1212/01.wnl.0000344569.13496.ff. PMID 19289745.
- ↑ Güneş HN, Bilecenoğlu NT, Şener U, Yoldaş TK (April 2015). “POEMS syndrome with peripheral and central nervous system demyelination: case report”. Neurologist. 19 (4): 101–3. doi:10.1097/NRL.0000000000000017. PMID 25888197.
- ↑ “IMWG | International Myeloma Working Group (IMWG) Criteria for the Diagnosis of Multiple Myeloma”.
- ↑ Schreiber AK, Nones CF, Reis RC, Chichorro JG, Cunha JM (April 2015). “Diabetic neuropathic pain: Physiopathology and treatment”. World J Diabetes. 6 (3): 432–44. doi:10.4239/wjd.v6.i3.432. PMID 25897354.
- ↑ “Diagnosis and classification of diabetes mellitus”. Diabetes Care. 33 Suppl 1: S62–9. January 2010. doi:10.2337/dc10-S062. PMID 20042775.
- ↑ Ekabe CJ, Kehbila J, Abanda MH, Kadia BM, Sama CB, Monekosso GL (January 2017). “Vitamin B12 deficiency neuropathy; a rare diagnosis in young adults: a case report”. BMC Res Notes. 10 (1): 72. doi:10.1186/s13104-017-2393-3. PMID 28129784.
- ↑ Doi T, Kawata T, Tadano N, Iijima T, Maekawa A (February 1989). “Effect of vitamin B12 deficiency on S-adenosylmethionine metabolism in rats”. J. Nutr. Sci. Vitaminol. 35 (1): 1–9. PMID 2738712.
- ↑ Berg RL, Shaw GR (February 2013). “Laboratory evaluation for vitamin B12 deficiency: the case for cascade testing”. Clin Med Res. 11 (1): 7–15. doi:10.3121/cmr.2012.1112. PMID 23262189.
- ↑ Lindenbaum J, Savage DG, Stabler SP, Allen RH (June 1990). “Diagnosis of cobalamin deficiency: II. Relative sensitivities of serum cobalamin, methylmalonic acid, and total homocysteine concentrations”. Am. J. Hematol. 34 (2): 99–107. PMID 2339684.
- ↑ Berg RL, Shaw GR (February 2013). “Laboratory evaluation for vitamin B12 deficiency: the case for cascade testing”. Clin Med Res. 11 (1): 7–15. doi:10.3121/cmr.2012.1112. PMC 3573090. PMID 23262189.
- ↑ Lane LA, Rojas-Fernandez C (2002). “Treatment of vitamin b(12)-deficiency anemia: oral versus parenteral therapy”. Ann Pharmacother. 36 (7–8): 1268–72. doi:10.1345/aph.1A122. PMID 12086562.
- ↑ Winer JB (December 2001). “Guillain Barré syndrome”. MP, Mol. Pathol. 54 (6): 381–5. PMC 1187127. PMID 11724912.
- ↑ Rees JH, Gregson NA, Hughes RA (November 1995). “Anti-ganglioside GM1 antibodies in Guillain-Barré syndrome and their relationship to Campylobacter jejuni infection”. Ann. Neurol. 38 (5): 809–16. doi:10.1002/ana.410380516. PMID 7486873.
- ↑ Winer JB, Hughes RA, Anderson MJ, Jones DM, Kangro H, Watkins RP (May 1988). “A prospective study of acute idiopathic neuropathy. II. Antecedent events”. J. Neurol. Neurosurg. Psychiatry. 51 (5): 613–8. PMC 1033063. PMID 3404161.
- ↑ Yuki N, Koga M (October 2006). “Bacterial infections in Guillain-Barré and Fisher syndromes”. Curr. Opin. Neurol. 19 (5): 451–7. doi:10.1097/01.wco.0000245367.36576.e9. PMID 16969154.
- ↑ Kimura J (April 1978). “Proximal versus distal slowing of motor nerve conduction velocity in the Guillain-Barré syndrome”. Ann. Neurol. 3 (4): 344–50. doi:10.1002/ana.410030412. PMID 666277.
- ↑ Winer JB (December 2001). “Guillain Barré syndrome”. MP, Mol. Pathol. 54 (6): 381–5. PMC 1187127. PMID 11724912.
- ↑ “Randomised trial of plasma exchange, intravenous immunoglobulin, and combined treatments in Guillain-Barré syndrome. Plasma Exchange/Sandoglobulin Guillain-Barré Syndrome Trial Group”. Lancet. 349 (9047): 225–30. January 1997. PMID 9014908.
- ↑ “Plasmapheresis and acute Guillain-Barré syndrome. The Guillain-Barré syndrome Study Group”. Neurology. 35 (8): 1096–104. August 1985. PMID 4022342.
- ↑ “Chronic Inflammatory Demyelinating Polyradiculoneuropathy: Clinical Characteristics, Course, and Recommendations for Diagnostic Criteria | JAMA Neurology | JAMA Network”.
- ↑ “onlinelibrary.wiley.com”.
- ↑ Milner P, Lovelidge CA, Taylor WA, Hughes RA (July 1987). “P0 myelin protein produces experimental allergic neuritis in Lewis rats”. J. Neurol. Sci. 79 (3): 275–85. PMID 2440998.
- ↑ Gabriel CM, Gregson NA, Hughes RA (May 2000). “Anti-PMP22 antibodies in patients with inflammatory neuropathy”. J. Neuroimmunol. 104 (2): 139–46. PMID 10713353.
- ↑ Bouchard C, Lacroix C, Planté V, Adams D, Chedru F, Guglielmi JM, Said G (February 1999). “Clinicopathologic findings and prognosis of chronic inflammatory demyelinating polyneuropathy”. Neurology. 52 (3): 498–503. PMID 10025777.
- ↑ Yan WX, Archelos JJ, Hartung HP, Pollard JD (September 2001). “P0 protein is a target antigen in chronic inflammatory demyelinating polyradiculoneuropathy”. Ann. Neurol. 50 (3): 286–92. PMID 11558784.
- ↑ Barohn RJ, Kissel JT, Warmolts JR, Mendell JR (August 1989). “Chronic inflammatory demyelinating polyradiculoneuropathy. Clinical characteristics, course, and recommendations for diagnostic criteria”. Arch. Neurol. 46 (8): 878–84. PMID 2757528.
- ↑ Barohn RJ, Kissel JT, Warmolts JR, Mendell JR (August 1989). “Chronic inflammatory demyelinating polyradiculoneuropathy. Clinical characteristics, course, and recommendations for diagnostic criteria”. Arch. Neurol. 46 (8): 878–84. PMID 2757528.
- ↑ Dimachkie MM, Barohn RJ (June 2013). “Chronic inflammatory demyelinating polyneuropathy”. Curr Treat Options Neurol. 15 (3): 350–66. doi:10.1007/s11940-013-0229-6. PMC 3987657. PMID 23564314.
- ↑ “onlinelibrary.wiley.com”.
- ↑ Koski CL, Baumgarten M, Magder LS, Barohn RJ, Goldstein J, Graves M, Gorson K, Hahn AF, Hughes RA, Katz J, Lewis RA, Parry GJ, van Doorn P, Cornblath DR (February 2009). “Derivation and validation of diagnostic criteria for chronic inflammatory demyelinating polyneuropathy”. J. Neurol. Sci. 277 (1–2): 1–8. doi:10.1016/j.jns.2008.11.015. PMID 19091330.
- ↑ Robbins, Nathaniel M; Lawson, Victoria (2018). “The Potential Misdiagnosis of Multifocal Motor Neuropathy as Amyotrophic Lateral Sclerosis—A Case Series”. US Neurology. 14 (2): 102. doi:10.17925/USN.2018.14.2.102. ISSN 1758-4000.
- ↑ “European Federation of Neurological Societies/Peripheral Nerve Society guideline on management of multifocal motor neuropathy. Report of a joint task force of the European Federation of Neurological Societies and the Peripheral Nerve Society–first revision”. J. Peripher. Nerv. Syst. 15 (4): 295–301. December 2010. doi:10.1111/j.1529-8027.2010.00290.x. PMID 21199100.
- ↑ Bartoloni A, Zammarchi L (2012). “Clinical aspects of uncomplicated and severe malaria”. Mediterr J Hematol Infect Dis. 4 (1): e2012026. doi:10.4084/MJHID.2012.026. PMID 22708041.
- ↑ Tangpukdee N, Duangdee C, Wilairatana P, Krudsood S (June 2009). “Malaria diagnosis: a brief review”. Korean J. Parasitol. 47 (2): 93–102. doi:10.3347/kjp.2009.47.2.93. PMID 19488414.
- ↑ White NJ (September 1996). “The treatment of malaria”. N. Engl. J. Med. 335 (11): 800–6. doi:10.1056/NEJM199609123351107. PMID 8703186.
- ↑ Aggarwal P, Handa R, Singh S, Wali JP (1999). “Kala-azar–new developments in diagnosis and treatment”. Indian J Pediatr. 66 (1): 63–71. PMID 10798038.
- ↑ Torres-Guerrero E, Quintanilla-Cedillo MR, Ruiz-Esmenjaud J, Arenas R (2017). “Leishmaniasis: a review”. F1000Res. 6: 750. doi:10.12688/f1000research.11120.1. PMID 28649370.
- ↑ Liang TJ (May 2009). “Hepatitis B: the virus and disease”. Hepatology. 49 (5 Suppl): S13–21. doi:10.1002/hep.22881. PMC 2809016. PMID 19399811.
- ↑ Li HC, Lo SY (June 2015). “Hepatitis C virus: Virology, diagnosis and treatment”. World J Hepatol. 7 (10): 1377–89. doi:10.4254/wjh.v7.i10.1377. PMC 4450201. PMID 26052383.
- ↑ National Cancer Institute. Physician Data Query Database 2015.http://www.cancer.gov/types/leukemia/hp/cml-treatment-pdq#section/_19
- ↑ Jabbour E, Kantarjian H (May 2014). “Chronic myeloid leukemia: 2014 update on diagnosis, monitoring, and management”. Am. J. Hematol. 89 (5): 547–56. doi:10.1002/ajh.23691. PMID 24729196.
- ↑ Thompson PA, Kantarjian HM, Cortes JE (October 2015). “Diagnosis and Treatment of Chronic Myeloid Leukemia in 2015”. Mayo Clin. Proc. 90 (10): 1440–54. doi:10.1016/j.mayocp.2015.08.010. PMC 5656269. PMID 26434969.
- ↑ Faderl S, Talpaz M, Estrov Z, Kantarjian HM (August 1999). “Chronic myelogenous leukemia: biology and therapy”. Ann. Intern. Med. 131 (3): 207–19. PMID 10428738.
- ↑ Canadian Cancer Society.2015.http://www.cancer.ca/en/cancer-information/cancer-type/leukemia-chronic-myelogenous-cml/treatment/chronic/?region=ab
- ↑ Tefferi A (2006). “Classification, diagnosis and management of myeloproliferative disorders in the JAK2V617F era”. Hematology Am Soc Hematol Educ Program: 240–245. PMID 17124067.
- ↑ Canadian Cancer Society.2015.http://www.cancer.ca/en/cancer-information/cancer-type/leukemia-chronic-myelogenous-cml/signs-and-symptoms/?region=ab
- ↑ 51.0 51.1 Thompson PA, Kantarjian HM, Cortes JE (October 2015). “Diagnosis and Treatment of Chronic Myeloid Leukemia in 2015”. Mayo Clin. Proc. 90 (10): 1440–54. doi:10.1016/j.mayocp.2015.08.010. PMC 5656269. PMID 26434969.
- ↑ Wang YL, Bagg A, Pear W, Nowell PC, Hess JL (October 2001). “Chronic myelogenous leukemia: laboratory diagnosis and monitoring”. Genes Chromosomes Cancer. 32 (2): 97–111. PMID 11550277.
- ↑ Zahra K, Ben Fredj W, Ben Youssef Y, Zaghouani H, Chebchoub I, Zaier M, Badreddine S, Braham N, Sennana H, Khelif A (2012). “Chronic myeloid leukemia as a secondary malignancy after lymphoma in a child. A case report and review of the literature”. Onkologie. 35 (11): 690–3. doi:10.1159/000343952. PMID 23147546.
- ↑ Real de Asúa D, Costa R, Galván JM, Filigheddu MT, Trujillo D, Cadiñanos J (2014). “Systemic AA amyloidosis: epidemiology, diagnosis, and management”. Clin Epidemiol. 6: 369–77. doi:10.2147/CLEP.S39981. PMC 4218891. PMID 25378951.
- ↑ Misumi Y, Ando Y (July 2014). “[Classification of amyloidosis]”. Brain Nerve (in Japanese). 66 (7): 731–7. PMID 24998818.
- ↑ Bilginer Y, Akpolat T, Ozen S (August 2011). “Renal amyloidosis in children”. Pediatr. Nephrol. 26 (8): 1215–27. doi:10.1007/s00467-011-1797-x. PMC 3119800. PMID 21360109.
- ↑ Khoor A, Colby TV (February 2017). “Amyloidosis of the Lung”. Arch. Pathol. Lab. Med. 141 (2): 247–254. doi:10.5858/arpa.2016-0102-RA. PMID 28134587.
- ↑ Palladini G, Perfetti V, Obici L, Caccialanza R, Semino A, Adami F, Cavallero G, Rustichelli R, Virga G, Merlini G (April 2004). “Association of melphalan and high-dose dexamethasone is effective and well tolerated in patients with AL (primary) amyloidosis who are ineligible for stem cell transplantation”. Blood. 103 (8): 2936–8. doi:10.1182/blood-2003-08-2788. PMID 15070667.
- ↑ Wechalekar AD, Goodman HJ, Lachmann HJ, Offer M, Hawkins PN, Gillmore JD (January 2007). “Safety and efficacy of risk-adapted cyclophosphamide, thalidomide, and dexamethasone in systemic AL amyloidosis”. Blood. 109 (2): 457–64. doi:10.1182/blood-2006-07-035352. PMID 16990593.
- ↑ Skinner M, Sanchorawala V, Seldin DC, Dember LM, Falk RH, Berk JL, Anderson JJ, O’Hara C, Finn KT, Libbey CA, Wiesman J, Quillen K, Swan N, Wright DG (January 2004). “High-dose melphalan and autologous stem-cell transplantation in patients with AL amyloidosis: an 8-year study”. Ann. Intern. Med. 140 (2): 85–93. PMID 14734330.
- ↑ Stirnemann J, Belmatoug N, Camou F, Serratrice C, Froissart R, Caillaud C, Levade T, Astudillo L, Serratrice J, Brassier A, Rose C, Billette de Villemeur T, Berger MG (February 2017). “A Review of Gaucher Disease Pathophysiology, Clinical Presentation and Treatments”. Int J Mol Sci. 18 (2). doi:10.3390/ijms18020441. PMID 28218669.
- ↑ Carnegie C (2004). “Diagnosis of hypogonadism: clinical assessments and laboratory tests”. Rev Urol. 6 Suppl 6: S3–8. PMC 1472884. PMID 16985909.
- ↑ Dandona P, Rosenberg MT (May 2010). “A practical guide to male hypogonadism in the primary care setting”. Int. J. Clin. Pract. 64 (6): 682–96. doi:10.1111/j.1742-1241.2010.02355.x. PMID 20518947.
- ↑ Kostoglou-Athanassiou I, Ntalles K (April 2010). “Hypothyroidism – new aspects of an old disease”. Hippokratia. 14 (2): 82–7. PMID 20596261.
- ↑ Koulouri O, Moran C, Halsall D, Chatterjee K, Gurnell M (December 2013). “Pitfalls in the measurement and interpretation of thyroid function tests”. Best Pract. Res. Clin. Endocrinol. Metab. 27 (6): 745–62. doi:10.1016/j.beem.2013.10.003. PMID 24275187.
- ↑ Kim SY (December 2015). “Diagnosis and Treatment of Hypopituitarism”. Endocrinol Metab (Seoul). 30 (4): 443–55. doi:10.3803/EnM.2015.30.4.443. PMID 26790380.
- ↑ Prabhakar VK, Shalet SM (April 2006). “Aetiology, diagnosis, and management of hypopituitarism in adult life”. Postgrad Med J. 82 (966): 259–66. doi:10.1136/pgmj.2005.039768. PMID 16597813.
- ↑ “Multiple Myeloma | NEJM”.
- ↑ Palumbo A, Chanan-Khan A, Weisel K, Nooka AK, Masszi T, Beksac M, Spicka I, Hungria V, Munder M, Mateos MV, Mark TM, Qi M, Schecter J, Amin H, Qin X, Deraedt W, Ahmadi T, Spencer A, Sonneveld P (August 2016). “Daratumumab, Bortezomib, and Dexamethasone for Multiple Myeloma”. N. Engl. J. Med. 375 (8): 754–66. doi:10.1056/NEJMoa1606038. PMID 27557302.
- ↑ Rajkumar SV, Kumar S (January 2016). “Multiple Myeloma: Diagnosis and Treatment”. Mayo Clin. Proc. 91 (1): 101–19. doi:10.1016/j.mayocp.2015.11.007. PMC 5223450. PMID 26763514.
- ↑ Kyle RA, Rajkumar SV (September 2006). “Monoclonal gammopathy of undetermined significance”. Br. J. Haematol. 134 (6): 573–89. doi:10.1111/j.1365-2141.2006.06235.x. PMID 16938117.
- ↑ Allen SC, Raut S (November 2004). “Biochemical recovery time scales in elderly patients with osteomalacia”. J R Soc Med. 97 (11): 527–30. doi:10.1258/jrsm.97.11.527. PMID 15520146.
- ↑ Sherer Y, Bardayan Y, Shoenfeld Y (1997). “Thymoma, thymic hyperplasia, thymectomy and autoimmune diseases (Review)”. Int. J. Oncol. 10 (5): 939–43. PMID 21533467.
- ↑ Nozza, Andrea (2017). “POEMS SYNDROME: AN UPDATE”. Mediterranean Journal of Hematology and Infectious Diseases. 9 (1): e2017051. doi:10.4084/mjhid.2017.051. ISSN 2035-3006.
- ↑ Maceluch JA, Niedziela M (2006). “The clinical diagnosis and molecular genetics of kearns-sayre syndrome: a complex mitochondrial encephalomyopathy”. Pediatr Endocrinol Rev. 4 (2): 117–37. PMID 17342029.
- ↑ Rigoli L, Di Bella C (2012). “Wolfram syndrome 1 and Wolfram syndrome 2”. Curr. Opin. Pediatr. 24 (4): 512–7. doi:10.1097/MOP.0b013e328354ccdf. PMID 22790102.
- ↑ Husebye, Eystein S.; Anderson, Mark S. (2010). “Autoimmune Polyendocrine Syndromes: Clues to Type 1 Diabetes Pathogenesis”. Immunity. 32 (4): 479–487. doi:10.1016/j.immuni.2010.03.016. ISSN 1074-7613.
Epidemiology and Demographics
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Sabawoon Mirwais, M.B.B.S, M.D.[2]
Overview
The precise incidence of POEMS syndrome is difficult to determine and we have no well established data to quote. The median age at presentation has been 51 years with the majority of the patients comprising of males. A median survival of 165 months has also been recorded. The precise incidence of POEMS syndrome is difficult to determine due to the complexity of the syndrome presentation and we have no well established data regarding the incidence. Prevalence of POEMS syndrome in Japan is reported to be about 0.3 per 100,000 individuals. There is no racial predilection to POEMS syndrome. There is no well established data regarding the gender predilection of POEMS syndrome. Data from Japan shows a male predilection of 2.5:1. The majority of POEMS syndrome cases have been reported in Japan and China.
Epidemiology and Demographics
Incidence
The precise incidence of POEMS syndrome is difficult to determine due to the complexity of the syndrome presentation and we have no well established data regarding the incidence.
Prevalence
Prevalence of POEMS syndrome in Japan is reported to be about 0.3 per 100,000 individuals.[1]
Age
The median age at presentation is 51 years.[2]
Race
There is no racial predilection to POEMS syndrome.[3][4][5]
Gender
- There is no well established data regarding the gender predilection of POEMS syndrome.
- Data from Japan shows a male predilection of 2.5:1.[6]
Region
The majority of POEMS syndrome cases have been reported in Japan and China.[3][4][5]
References
- ↑ https://www.orpha.net/consor/cgi-bin/OC_Exp.php?Lng=GB&Expert=2905
- ↑ Dispenzieri A, Kyle RA, Lacy MQ, Rajkumar SV, Therneau TM, Larson DR, Greipp PR, Witzig TE, Basu R, Suarez GA, Fonseca R, Lust JA, Gertz MA (April 2003). “POEMS syndrome: definitions and long-term outcome”. Blood. 101 (7): 2496–506. doi:10.1182/blood-2002-07-2299. PMID 12456500.
- ↑ 3.0 3.1 Yuan M, Chen W, Zhou H, Xiao Z, Wang W, Wang W, Yin X, Xu L (2016). “Kennedy Disease Misdiagnosed as Polyneuropathy, Organomegaly, Endocrinopathy, Monoclonal Gammopathy, and Skin Changes (POEMS) Syndrome: A Case Report”. Med Princ Pract. 25 (3): 286–9. doi:10.1159/000442822. PMC 5588369. PMID 26618536.
- ↑ 4.0 4.1 Tang LM, Chen ST, Cheng SY, Lyu RK (1995). “POEMS syndrome in Chinese”. Eur. Neurol. 35 (6): 349–53. doi:10.1159/000117159. PMID 8591803.
- ↑ 5.0 5.1 Romas E, Storey E, Ayers M, Byrne E (July 1992). “Polyneuropathy, organomegaly, endocrinopathy, M-protein and skin change (POEMS) syndrome with IgG kappa paraproteinemia”. Pathology. 24 (3): 217–20. PMID 1437299.
- ↑ https://www.orpha.net/consor/cgi-bin/OC_Exp.php?Lng=GB&Expert=2905
Risk Factors
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1] Associate Editor(s)-in-Chief: Syed Hassan A. Kazmi BSc, MD [2]
Overview
The most potent risk factor leading to the development of POEMS syndrome is multiple myeloma of osteosclerotic type.
Risk Factors
The most potent risk factor leading to the development of POEMS syndrome is multiple myeloma of osteosclerotic type. Other risk factors include the following:
References
Natural History, Complications and Prognosis
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]Associate Editor(s)-in-Chief: Syed Hassan A. Kazmi BSc, MD [2]Sabawoon Mirwais, M.B.B.S, M.D.[3]
Overview
POEMS syndrome presents as a chronic progressive polyneuropathy. Patients may have coexisting multi-organ system disorders. The neuropathy is usually symmetrical and ascending. Endocrinopathy, present in majority of cases, involves hypogonadism, hypothyroidism, and abnormalities of the pituitary–adrenal axis. If left untreated, patients suffering from POEMS syndrome may become wheel chair bound. Complications of POEMS syndrome include renal failure, pulmonary hypertension, pathologic fractures, ischemic stroke, restrictive lung disease, polycythemia, thrombocytosis, papilledema, and myocardial infarction. 3, 5, and 10 year overall survival (OS) for patients newly diagnosed with POEMS syndrome is 87.7%, 84.1%, and 77%. Age >50 years, pulmonary hypertension, pleural effusion, and estimated glomerular filtration rate <30 ml/min/1.73 m2 were associated with inferior overall survival in the derivation cohort, with the use of multivariate Cox regression model based on randomized sample splitting of 362 patients. Low albumin (defined as<3.2 g/dl) at diagnosis and failure to achieve a complete hematologic response to first-line therapy can be independent risk factors for progression-free survival (PFS). Improvement of plasma cell dyscrasia leads to improvement or marked reduction in other abnormalities. Neuropathy, stroke, and myocardial infarction are the most common causes of death in POEMS syndrome.
Natural History, Complications, and Prognosis
Natural History
- POEMS syndrome typically presents as a chronic progressive polyneuropathy with both sensory and motor disability, the motor component is usually present to a greater degree than the sensory component of the disease.[1]
- Many patients may have coexisting multi-organ system disorders such as organomegaly (liver, spleen and lymph nodes), edema, endocrinopathy (pituitary, thyroid, adrenal glands), thrombocytosis, polycythemia, pulmonary hypertension, an M-spike (M protein or para-protein, may be IgA lambda component, IgG lambda component or light chain lambda component) and skin changes. The skin changes include angiomata, hyperpigmentation, hypertrichosis.[2]
- The neuropathy is usually symmetrical and ascending, with either insidious or rapidly progressing onset. Sensory neuropathy precedes motor dysfunction and pin-prick and vibratory sensations are typically affected.
- The endocrinopathy is present in a majority of cases of POEMS syndrome. Almost all patients exhibiting endocrinopathy have hyperestrogenemia. The increased levels of estrogen may be the cause of hypogonadism and impotence seen in male patients. Hypogonadism, hypothyroidism, and abnormalities of the pituitary–adrenal axis are noted in order of descending frequency.[3][4]
- POEMS syndrome may also lead to glomerular disease (membranoproliferative glomerulonephritis) eventually resulting in renal failure.
- If left untreated, patients suffering from POEMS syndrome may become wheel chair bound.
Complications
- Patients suffering from POEMS syndrome may develop the following complications:
Prognosis
- The median survival of patients with POEMS syndrome is 165 months.[15]
- 3, 5, and 10 year overall survival (OS) for patients newly diagnosed with POEMS syndrome is 87.7%, 84.1%, and 77%.[16]
- Age >50 years, pulmonary hypertension, pleural effusion, and estimated glomerular filtration rate <30 ml/min/1.73 m2 were associated with inferior overall survival in the derivation cohort, with the use of multivariate Cox regression model based on randomized sample splitting of 362 patients.[16][17][18][9][19]
- Low albumin (defined as<3.2 g/dl) at diagnosis and failure to achieve a complete hematologic response to first-line therapy can be independent risk factors for progression-free survival (PFS).[16][20]
- Papilledema, decreased diffusing capacity of the lung for carbon monoxide (DLCO) and treatment with corticosteroids alone are also related to poor prognosis.[21]
- Improvement of plasma cell dyscrasia leads to improvement or marked reduction in other abnormalities.
- Neuropathy, stroke and myocardial infarction are the most common causes of death in POEMS syndrome.
References
- ↑ Mauermann ML (February 2018). “The Peripheral Neuropathies of POEMS Syndrome and Castleman Disease”. Hematol. Oncol. Clin. North Am. 32 (1): 153–163. doi:10.1016/j.hoc.2017.09.012. PMID 29157616.
- ↑ Dispenzieri A (August 2012). “POEMS syndrome: update on diagnosis, risk-stratification, and management”. Am. J. Hematol. 87 (8): 804–14. doi:10.1002/ajh.23288. PMID 22806697.
- ↑ Gandhi GY, Basu R, Dispenzieri A, Basu A, Montori VM, Brennan MD (July 2007). “Endocrinopathy in POEMS syndrome: the Mayo Clinic experience”. Mayo Clin. Proc. 82 (7): 836–42. doi:10.4065/82.7.836. PMID 17605964.
- ↑ Caimari F, Keddie S, Lunn MP, D’Sa S, Baldeweg SE (September 2018). “Prevalence and course of endocrinopathy in POEMS syndrome”. J. Clin. Endocrinol. Metab. doi:10.1210/jc.2018-01516. PMID 30239770.
- ↑ Modesto-Segonds A, Rey JP, Orfila C, Huchard G, Suc JM (May 1995). “Renal involvement in POEMS syndrome”. Clin. Nephrol. 43 (5): 342–5. PMID 7634552.
- ↑ Brewis MJ, Church AC, Peacock AJ, Thomson S, Tighe J, Johnson MK (December 2014). “Pulmonary hypertension in POEMS syndrome: resolution following radiotherapy”. Pulm Circ. 4 (4): 732–5. doi:10.1086/678553. PMID 25610609.
- ↑ Shibuya K, Misawa S, Horikoshi T, Kanai K, Isose S, Nasu S, Sekiguchi Y, Noto Y, Fujimaki Y, Nakaseko C, Kuwabara S (2011). “Detection of bone lesions by CT in POEMS syndrome”. Intern. Med. 50 (13): 1393–6. PMID 21720058.
- ↑ Fu FW, Rao J, Zheng YY, Wang HL, Yang JG, Zheng GQ (October 2017). “Ischemic stroke in patients with POEMS syndrome: a case report and comprehensive analysis of literature”. Oncotarget. 8 (51): 89406–89424. doi:10.18632/oncotarget.20131. PMID 29179528.
- ↑ 9.0 9.1 Allam JS, Kennedy CC, Aksamit TR, Dispenzieri A (April 2008). “Pulmonary manifestations in patients with POEMS syndrome: a retrospective review of 137 patients”. Chest. 133 (4): 969–74. doi:10.1378/chest.07-1800. PMID 18198255.
- ↑ Naddaf E, Dispenzieri A, Mandrekar J, Mauermann ML (October 2015). “Thrombocytosis distinguishes POEMS syndrome from chronic inflammatory demyelinating polyneuropathy”. Muscle Nerve. 52 (4): 658–9. doi:10.1002/mus.24768. PMID 26179010.
- ↑ Decker P, Galland J, Risse J, Claudin M, Mohamed S, Perrot A, Wahl D (February 2018). “[A POEMS syndrome revealed by a blue toe syndrome]”. Rev Med Interne (in French). 39 (2): 127–129. doi:10.1016/j.revmed.2017.09.005. PMID 29288001.
- ↑ Schulz W, Domenico D, Nand S (March 1989). “POEMS syndrome associated with polycythemia vera”. Cancer. 63 (6): 1175–8. PMID 2537136.
- ↑ Kumar S, Sharma S (March 2015). “Polyneuropathy, organomegaly, endocrinopathy, M-protein and skin changes (POEMS syndrome): a paraneoplastic syndrome”. Oxf Med Case Reports. 2015 (3): 237–40. doi:10.1093/omcr/omv023. PMID 26634133.
- ↑ Manning WJ, Goldberger AL, Drews RE, Goldstein BJ, Matheson JK, Rabinowe SL, Trentham DE, Landsberg L (December 1992). “POEMS syndrome with myocardial infarction: observations concerning pathogenesis and review of the literature”. Semin. Arthritis Rheum. 22 (3): 151–61. PMID 1295088.
- ↑ Dispenzieri A, Kyle RA, Lacy MQ, Rajkumar SV, Therneau TM, Larson DR, Greipp PR, Witzig TE, Basu R, Suarez GA, Fonseca R, Lust JA, Gertz MA (April 2003). “POEMS syndrome: definitions and long-term outcome”. Blood. 101 (7): 2496–506. doi:10.1182/blood-2002-07-2299. PMID 12456500.
- ↑ 16.0 16.1 16.2 Wang C, Huang XF, Cai QQ, Cao XX, Duan MH, Cai H, Zhou DB, Li J (January 2017). “Prognostic study for overall survival in patients with newly diagnosed POEMS syndrome”. Leukemia. 31 (1): 100–106. doi:10.1038/leu.2016.168. PMID 27338259.
- ↑ Clegg A, Young J, Iliffe S, Rikkert MO, Rockwood K (March 2013). “Frailty in elderly people”. Lancet. 381 (9868): 752–62. doi:10.1016/S0140-6736(12)62167-9. PMC 4098658. PMID 23395245.
- ↑ Lesprit P, Godeau B, Authier FJ, Soubrier M, Zuber M, Larroche C, Viard JP, Wechsler B, Gherardi R (March 1998). “Pulmonary hypertension in POEMS syndrome: a new feature mediated by cytokines”. Am. J. Respir. Crit. Care Med. 157 (3 Pt 1): 907–11. doi:10.1164/ajrccm.157.3.9707095. PMID 9517610.
- ↑ Li J, Tian Z, Zheng HY, Zhang W, Duan MH, Liu YT, Cao XX, Zhou DB (March 2013). “Pulmonary hypertension in POEMS syndrome”. Haematologica. 98 (3): 393–8. doi:10.3324/haematol.2012.073031. PMC 3659947. PMID 22983590.
- ↑ Kourelis TV, Buadi FK, Gertz MA, Lacy MQ, Kumar SK, Kapoor P, Go RS, Lust JA, Hayman SR, Rajkumar V, Zeldenrust SR, Russell SJ, Dingli D, Lin Y, Leung N, Hwa YL, Gonsalves W, Kyle RA, Dispenzieri A (May 2016). “Risk factors for and outcomes of patients with POEMS syndrome who experience progression after first-line treatment”. Leukemia. 30 (5): 1079–85. doi:10.1038/leu.2015.344. PMID 26669974.
- ↑ Cui R, Yu S, Huang X, Zhang J, Tian C, Pu C (January 2014). “Papilloedema is an independent prognostic factor for POEMS syndrome”. J. Neurol. 261 (1): 60–5. doi:10.1007/s00415-013-7143-4. PMID 24141729.
Diagnosis
Diagnosis
Diagnostic Criteria | History and Symptoms | Physical Examination | Laboratory Findings | Chest X Ray | CT | MRI | Echocardiography or Ultrasound | Other Imaging Findings | Other Diagnostic Studies
Treatment
Treatment
Medical Therapy | Surgery | Cost-Effectiveness of Therapy | Future or Investigational Therapies
Looking for the patient version?
© 2026 MyEClinic – IFTM Institut für Telematik in der Medizin GmbH