
Chickenpox
Template:DiseaseDisorder infobox
For patient information click here
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1] Aravind Reddy Kothagadi M.B.B.S[2]
Synonyms and keywords: Varicella zoster; Chicken pox; VZV
Overview
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]
Associate Editor(s)-in-Chief:
Michael Maddaleni, B.S.
Aravind Reddy Kothagadi M.B.B.S[2]
Overview
Chickenpox is the common name for varicella zoster, and it is classically one of the childhood infectious diseases caught by and survived by almost every child. It is one of the most contagious infectious diseases. The affected child or adult may develop hundreds of itchy, fluid-filled blisters that burst and form crusts. Chickenpox is caused by varicella-zoster virus, a member of the herpes virus family. The same virus also causes shingles (herpes zoster) in adults. There is no racial or sexual predilection for chickenpox. Only symptomatic treatment is advised for chickenpox except in immunocompromised patients.
Historical Perspective
Chickenpox was first described by Razi, an Iranian physician. In the mid-1500s, Giovanni Filippo described it in more detail. In 1767, William Heberden from England, differentiated chickenpox from smallpox. The live attenuated vaccine for chickenpox was introduced in 1974.
Classification
There is no established classification system for chickenpox.
Pathophysiology
Chickenpox is a highly contagious disease contracted by the inhalation of aerosolized nasopharyngeal secretions droplets or through direct contact with the vesicles from an infected host. It takes from 10 to 21 days after exposure to a person with chickenpox or shingles for someone to develop chickenpox. Viral proliferation occurs in regional lymph nodes of the upper respiratory tract leading to viremia. Viremia is characterized by diffuse viral invasion of capillary endothelial cells and the epidermis. VZV infection of cells of the malpighian layer produces both intercellular and intracellular edema, resulting in the characteristic vesicles.
Causes
Chickenpox is caused by the varicella-zoster virus, also known as human herpes virus 3 (HHV-3), one of the eight herpes viruses known to affect humans. Transmission of the disease from an infected individual occurs by droplet transmission of nasopharyngeal secretions and contact with vesicle fluid from the skin lesions.
Differentiating Chickenpox from other Diseases
Different rash-like conditions can be confused with chickenpox and are thus included in its differential diagnosis. There are many active considerations that need to be ruled out to diagnose chickenpox. The one exception to this is Smallpox.
Epidemiology and Demographics
Chickenpox is an endemic disease spread mainly by the respiratory route. Cases are observed all through the year but mostly in the winter and early spring. In tropical regions, cases of varicella infection have been reported to be more common among adults than children.
Risk Factors
Risk factors which increase the likelihood of contracting chickenpox are people without a history of chickenpox in the past, individuals who are not immunized against chickenpox, newborns, especially those born prematurely, less than 1 month or born to mothers who never contracted chickenpox prior to pregnancy, immunocompromised individuals, cancer patients and the use of immunosuppressant drugs.
Screening
According to Center for Disease Control and Prevention (CDC), there is insufficient evidence to recommend routine screening among general population. Children are vaccinatedagainst chickenpox and most adults generally may have been infected with VZV in their early years. Screening is recommended for specific populations which include, healthcare workers, pregnant women, newborns, HIV/AIDS patients and for people prior to organ transplantation.
Natural History, Complications and Prognosis
If left untreated, skin irritation from repeatedly scratching chickenpox sores allows the bacteria to invade the skin resulting in cellulitis. In some cases, varicella infection can spread to the lungs causing pneumonia and can be proven fatal. The disease is usually mild, although serious complications sometimes occur. Two of the most common complications are bacterial infections of the skin and soft tissues in children and pneumonia in adults. Primary varicella is a common childhood disease in the western countries. Anyone who has recovered from chickenpox may develop shingles; even children can get shingles. Chickenpox is rarely fatal (usually from varicella pneumonia), with pregnant women and those with a suppressed immune systems being more at risk. Pregnant women not known to be immune and who come into contact with chickenpox may need urgent treatment as the virus can cause serious problems for the baby. This is less of an issue after 20 weeks.
Diagnosis
History and Symptoms
Patient with chickenpox presents with the characteristic rash and numerous spread out of lesions. Symptoms usually start as low-grade fever and skin manifestations appear by 1-2 days. Rash initially appears on the head, trunk and then spreads to the rest of the body with intense pruritus, headache, malaise, anorexia, cough, coryza, tiredness and loss of appetite.
Physical Examination
The diagnosis of varicella is primarily made by clinical findings. In a non-immunized individual with the appropriate appearing rash occurring in “crops”, no further investigation would normally be undertaken. For further investigation, examination of the fluid within the vesicles, or by testing blood for evidence of an acute immunologic response. Vesicle fluid can be examined with a tzanck smear, or better with examination for the direct fluorescent antibody. The fluid can also be “cultured”, whereby attempts are made to grow the virus from a fluid sample. Blood tests can be used to identify a response to acute infection (IgM) or previous infection and subsequent immunity (IgG). Prenatal diagnosis of fetal varicella infection can be performed using ultrasound, though a delay of 5 weeks following primary maternal infection is advised. A PCR (DNA) test of the mother’s amniotic fluid can also be performed, though the risk of spontaneous abortion due to the amniocentesis procedure is higher than the risk of the baby developing fetal varicella syndrome.
Laboratory Findings
Diagnosis of chickenpox is usually based upon signs and symptoms of the affected individual. Laboratory tests are not routinely used to diagnose active cases of chickenpox and shingles, which are caused by the varicella zoster virus (VZV). Children are nowadays vaccinated and most adults generally may have been infected with VZV in their early years. Hence, general population screening is not done usually. Anyhow, testing for VZV or for the antibodies produced in response to VZV infection may be performed in when required for screening purposes. Also, screening may be advised for newborns, pregnant women, prior to organ transplantation, and in those with HIV/AIDS. Testing may be used to determine if someone has been previously exposed to varicella zoster virus either through past infection or had received vaccination and has developed immunity to the disease.
Chest X Ray
Pneumonia, as a complication of chickenpox, rarely occurs in children, but occurs in about one-fifth of adults. Chest x-ray shows cloudiness throughout the lungs, caused by acute pneumonia following chickenpox.
CT scan
CT Scan has a minimal diagnostic value in diagnosing chickenpox unless complications arise such as in varicella pneumonia.
MRI
There are no MRI findings associated with chickenpox.
Ultrasound
There are no ultrasound findings associated with chickenpox.
Other Imaging Findings
There are no other specific imaging findings for chickenpox.
Other Diagnostic Studies
There are no additional diagnostic findings for chickenpox.
Treatment
Medical Therapy
Chickenpox usually doesn’t require any medical therapy in otherwise healthy individuals. Only symptomatic treatment is usually prescribed to ease the discomfort. The complexity of the therapy grows when many risk factors are involved.
Surgery
Surgical intervention is not recommended for the management of chickenpox.
Primary Prevention
Vaccination is recommended for children as well as adults who haven’t been vaccinated previously to prevent chickenpox. Two doses of varicella vaccine are recommended for children who never have contracted chickenpox at the following intervals. The first dose is recommended between 12-15 months of age. The second dose is recommended around 4-6 years of age and also it may be given earlier if the gap between the doses is at least three months from the first dose. In adults, a vaccine is recommended for people who are 13 years of age or older. There should be a gap of at least 28 days between the two doses.
Secondary Prevention
There are several things that can be done at home to help relieve the symptoms and prevent skin infections. Calamine lotion and colloidal oatmeal baths may help relieve some of the itching. Keeping fingernails trimmed short may help prevent skin infections caused by scratching blisters.
References
Historical Perspective
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1];Associate Editor(s)-in-Chief: Seyedmahdi Pahlavani, M.D. [2]
Overview
Chickenpox was first described by Razi, an Iranian physician. In the mid-1500s, Giovanni Filippo described it in more details. The live attenuated vaccine for chickenpox was introduced in 1974.
Historical Perspective
- In the late 800’s and early 900’s AD, Muhammad Ibn Zakariya Razi, also known as Razi, reported some of the first known information on chickenpox and noted the differences between measles and smallpox.[1]
- In the 1500s, Giovanni Filippo, an Italian anatomist, described Varicella (chickenpox) for the first time.
- In the 1600s, Richard Morton, an English physician described chickenpox as a mild form of smallpox.
- In 1767, William Heberden from England, differentiated chickenpox from smallpox.
- In 1974, the live attenuated vaccine for chickenpox was developed.
- In 1995, the varicella vaccine was licensed and introduced.
References
- ↑ Weller, T. H. (1996). “Varicella: Historical Perspective And Clinical Overview”. Journal of Infectious Diseases. 174 (Supplement 3): S306–S309. doi:10.1093/infdis/174.Supplement_3.S306. ISSN 0022-1899.
Classification
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1];Associate Editor(s)-in-Chief: Seyedmahdi Pahlavani, M.D. [2]
Overview
There is no established classification system for chickenpox.
Classification
There is no established classification system for chickenpox.
References
Pathophysiology
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1] Associate Editor(s)-in-Chief: Aravind Reddy Kothagadi M.B.B.S[2]
Overview
Chickenpox is a highly contagious disease contracted by the inhalation of aerosolized nasopharyngeal secretions or through direct contact with the vesicles from an infected host. Chicken pox has an incubation period of 10-21 days. Viral proliferation occurs in regional lymph nodes of the upper respiratory tract leading to viremia. Viremia is characterized by diffuse viral invasion of capillary endothelial cells and the epidermis. VZV infection of cells of the malpighian layer produces both intercellular and intracellular edema, resulting in the characteristic vesicles.
Pathophysiology
Chickenpox is contracted by the inhalation of aerosolized nasopharyngeal secretions from an infected host. The highly contagious nature of VZV explains the epidemics of chickenpox that spread through schools, as one child who is infected quickly spreads the virus to many classmates.
Transmission
- The mode of transmission is by inhalation of aerosolized nasopharyngeal secretions from an infected host.[1]
- Chickenpox can also be spread from people with shingles by direct contact.
- Viral shedding occurs 1-2 days prior to development of the rash and continues until all their chickenpox blisters have formed scabs.
- Nosocomial transmission of Varicella-zoster virus (VZV) has also been reported.[2]
Incubation Period
- The incubation period of chickenpox is typically from 14 to 16 days. However, the interval may vary from 10 to 21 days.[3]
- The infectivity period begins 48 hours prior to the appearance of the rash and lasts till crusts appear.
Dissemination
- After initial inhalation of contaminated aerosolized droplets, the virus infects the conjunctivae and the mucosae of the upper respiratory tract.
- Viral proliferation occurs in regional lymph nodes of the upper respiratory tract 2-4 days after initial infection, and is followed by primary viremia.
Pathogenesis
- Viral replication occurs in the liver, spleen, followed by a secondary viremia 14-16 days post infection. Secondary viremia is characterized by diffuse viral invasion of capillary endothelial cells and the epidermis.
- VZV infection of cells of the malpighian layer produces both intercellular and intracellular edema, resulting in the characteristic vesicles.
- Exposure to VZV initiates the production of host immunoglobulin G (IgG), immunoglobulin M (IgM), and immunoglobulin A (IgA) antibodies; IgG antibodies persist for life and confer immunity.
- After primary infection, VZV then remains latent in the dorsal ganglion cells of the sensory nerves.
- Reactivation of VZV results in the clinically distinct syndrome of herpes zoster (shingles).
Genetics
There is no genetic predisposition associated with chickenpox. Similarities in sibling response to varicella vaccine are supportive of the hypothesis that genetic factors play a role in the antibody response to the varicella vaccine.[4]
Associated Conditions
- Red eye in chickenpox: varicella-related acute anterior uveitis[6]
Gross Pathology
Rash findings
The typical rash in chickenpox may show the following findings:
- Superficial
- Unilocular
- Umblicated
- Area of inflammation around rash
- Pleomorphism (papules, vesicles and crusts may be seen simultaneously at the same area)
Microscopic Pathology
Rash findings
Skin lesions in chickenpox may show the following findings:
- Multi-nucleated giant cells
- Steel-gray nuclei with accentuation of nucleoplasm at their periphery
- Necrosis
- Acantholysis
- Vascular dilation
-
![Transmission electron micrograph (TEM) of a Varicella (Chickenpox) Virus. From Public Health Image Library (PHIL). [7]](https://www.wikidoc.org/images/f/fa/VZV14.jpeg) Transmission electron micrograph (TEM) of a Varicella (Chickenpox) Virus. From Public Health Image Library (PHIL). [7]
Transmission electron micrograph (TEM) of a Varicella (Chickenpox) Virus. From Public Health Image Library (PHIL). [7] -
![Various viruses from the Herpesviridae family seen using an electron micrograph. From Public Health Image Library (PHIL). [7]](https://www.wikidoc.org/images/7/76/VZV13.jpeg) Various viruses from the Herpesviridae family seen using an electron micrograph. From Public Health Image Library (PHIL). [7]
Various viruses from the Herpesviridae family seen using an electron micrograph. From Public Health Image Library (PHIL). [7] -
![photomicrograph reveals some of the cytoarchitectural histopathologic changes which you’d find in a human skin tissue specimen that included a chickenpox, or varicella zoster virus lesion (500x mag). From Public Health Image Library (PHIL). [7]](https://www.wikidoc.org/images/e/e2/VZV09.jpeg) photomicrograph reveals some of the cytoarchitectural histopathologic changes which you’d find in a human skin tissue specimen that included a chickenpox, or varicella zoster virus lesion (500x mag). From Public Health Image Library (PHIL). [7]
photomicrograph reveals some of the cytoarchitectural histopathologic changes which you’d find in a human skin tissue specimen that included a chickenpox, or varicella zoster virus lesion (500x mag). From Public Health Image Library (PHIL). [7] -
![Hematoxylin-eosin (H&E)-stained photomicrograph reveals some of the cytoarchitectural histopathologic changes found in a human skin tissue specimen that included a varicella zoster virus lesion (50x mag). From Public Health Image Library (PHIL). [7]](https://www.wikidoc.org/images/f/fa/VZV08.jpeg) Hematoxylin-eosin (H&E)-stained photomicrograph reveals some of the cytoarchitectural histopathologic changes found in a human skin tissue specimen that included a varicella zoster virus lesion (50x mag). From Public Health Image Library (PHIL). [7]
Hematoxylin-eosin (H&E)-stained photomicrograph reveals some of the cytoarchitectural histopathologic changes found in a human skin tissue specimen that included a varicella zoster virus lesion (50x mag). From Public Health Image Library (PHIL). [7] -
![Hematoxylin-eosin (H&E)-stained photomicrograph reveals some of the cytoarchitectural histopathologic changes found in a human skin tissue specimen that included a varicella zoster virus lesion (50x mag). From Public Health Image Library (PHIL). [7]](https://www.wikidoc.org/images/3/3d/VZV07.jpeg) Hematoxylin-eosin (H&E)-stained photomicrograph reveals some of the cytoarchitectural histopathologic changes found in a human skin tissue specimen that included a varicella zoster virus lesion (50x mag). From Public Health Image Library (PHIL). [7]
Hematoxylin-eosin (H&E)-stained photomicrograph reveals some of the cytoarchitectural histopathologic changes found in a human skin tissue specimen that included a varicella zoster virus lesion (50x mag). From Public Health Image Library (PHIL). [7] -
![Hematoxylin-eosin (H&E)-stained photomicrograph reveals some of the cytoarchitectural histopathologic changes found in a human skin tissue specimen that included a varicella zoster virus lesion (500x mag). From Public Health Image Library (PHIL). [7]](https://www.wikidoc.org/images/3/3d/VZV06.jpeg) Hematoxylin-eosin (H&E)-stained photomicrograph reveals some of the cytoarchitectural histopathologic changes found in a human skin tissue specimen that included a varicella zoster virus lesion (500x mag). From Public Health Image Library (PHIL). [7]
Hematoxylin-eosin (H&E)-stained photomicrograph reveals some of the cytoarchitectural histopathologic changes found in a human skin tissue specimen that included a varicella zoster virus lesion (500x mag). From Public Health Image Library (PHIL). [7] -
![Hematoxylin-eosin (H&E)-stained photomicrograph reveals some of the cytoarchitectural histopathologic changes found in a human skin tissue specimen that included a varicella zoster virus lesion (1200x mag). From Public Health Image Library (PHIL). [7]](https://www.wikidoc.org/images/8/84/VZV04.jpeg) Hematoxylin-eosin (H&E)-stained photomicrograph reveals some of the cytoarchitectural histopathologic changes found in a human skin tissue specimen that included a varicella zoster virus lesion (1200x mag). From Public Health Image Library (PHIL). [7]
Hematoxylin-eosin (H&E)-stained photomicrograph reveals some of the cytoarchitectural histopathologic changes found in a human skin tissue specimen that included a varicella zoster virus lesion (1200x mag). From Public Health Image Library (PHIL). [7]
![Transmission electron micrograph (TEM) of a Varicella (Chickenpox) Virus. From Public Health Image Library (PHIL). [7]](https://www.wikidoc.org/index.php/File%3AVZV14.jpeg)
![Various viruses from the Herpesviridae family seen using an electron micrograph. From Public Health Image Library (PHIL). [7]](https://www.wikidoc.org/index.php/File%3AVZV13.jpeg)
![photomicrograph reveals some of the cytoarchitectural histopathologic changes which you’d find in a human skin tissue specimen that included a chickenpox, or varicella zoster virus lesion (500x mag). From Public Health Image Library (PHIL). [7]](https://www.wikidoc.org/index.php/File%3AVZV09.jpeg)
![Hematoxylin-eosin (H&E)-stained photomicrograph reveals some of the cytoarchitectural histopathologic changes found in a human skin tissue specimen that included a varicella zoster virus lesion (50x mag). From Public Health Image Library (PHIL). [7]](https://www.wikidoc.org/index.php/File%3AVZV08.jpeg)
![Hematoxylin-eosin (H&E)-stained photomicrograph reveals some of the cytoarchitectural histopathologic changes found in a human skin tissue specimen that included a varicella zoster virus lesion (50x mag). From Public Health Image Library (PHIL). [7]](https://www.wikidoc.org/index.php/File%3AVZV07.jpeg)
![Hematoxylin-eosin (H&E)-stained photomicrograph reveals some of the cytoarchitectural histopathologic changes found in a human skin tissue specimen that included a varicella zoster virus lesion (500x mag). From Public Health Image Library (PHIL). [7]](https://www.wikidoc.org/index.php/File%3AVZV06.jpeg)
![Hematoxylin-eosin (H&E)-stained photomicrograph reveals some of the cytoarchitectural histopathologic changes found in a human skin tissue specimen that included a varicella zoster virus lesion (1200x mag). From Public Health Image Library (PHIL). [7]](https://www.wikidoc.org/index.php/File%3AVZV04.jpeg)
References
- ↑ Straus SE, Ostrove JM, Inchauspé G, Felser JM, Freifeld A, Croen KD; et al. (1988). “NIH conference. Varicella-zoster virus infections. Biology, natural history, treatment, and prevention”. Ann Intern Med. 108 (2): 221–37. PMID 2829675.
- ↑ Leclair JM, Zaia JA, Levin MJ, Congdon RG, Goldmann DA (1980). “Airborne transmission of chickenpox in a hospital”. N Engl J Med. 302 (8): 450–3. doi:10.1056/NEJM198002213020807. PMID 7351951.
- ↑ Heininger U, Seward JF (2006). “Varicella”. Lancet. 368 (9544): 1365–76. doi:10.1016/S0140-6736(06)69561-5. PMID 17046469.
- ↑ Klein NP, Fireman B, Enright A, Ray P, Black S, Dekker CL (2007). “A role for genetics in the immune response to the varicella vaccine”. Pediatr. Infect. Dis. J. 26 (4): 300–5. doi:10.1097/01.inf.0000257454.74513.07. PMID 17414391.
- ↑ 5.0 5.1 Muthu, Valliappan; M.B., Adarsh; Kumar, P. Sathish; Varma, Subhash; Malhotra, Pankaj (2013). “Varicella zoster virus-related pancytopenia”. International Journal of Infectious Diseases. 17 (12): e1264. doi:10.1016/j.ijid.2013.06.010. ISSN 1201-9712.
- ↑ Johnston NR (2010). “Red eye in chickenpox: varicella-related acute anterior uveitis in a child”. BMJ Case Rep. 2010. doi:10.1136/bcr.01.2010.2678. PMC 3029245. PMID 22778248.
- ↑ 7.0 7.1 7.2 7.3 7.4 7.5 7.6 “Public Health Image Library (PHIL)”.
Causes
For information about primary infection with VZV, visit chicken pox.
For information about reactivation of primary VZV infection, visit shingles.
For information about congenital Varicella Syndrome, click here.
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]
Overview
Varicella zoster virus or varicella-zoster virus (VZV) is one of eight herpes viruses known to infect humans and vertebrates. VZV only affects humans, and commonly causes chickenpox in children, teens and young adults and herpes zoster (shingles) in adults and rarely in children. VZV is known by many names, including chickenpox virus, varicella virus, zoster virus, and human herpesvirus type 3 (HHV-3).
VZV infects the nerves and causes a wide variety of symptoms. After the primary infection (chickenpox), the virus goes dormant in the nerves, including the cranial nerve ganglia, dorsal root ganglia, and autonomic ganglia. Many years after the patient has recovered from chickenpox, VZV can reactivate to cause a number of neurologic conditions.[1]
Human disease
Primary Varicella Zoster Virus infection results in chickenpox (varicella), which may result in complications including encephalitis or pneumonia (either direct viral pneumonia or secondary bacterial pneumonia). Even when clinical symptoms of chickenpox have resolved, VZV remains dormant in the nervous system of the infected person (virus latency), in the trigeminal and dorsal root ganglia.[2]
In about 10–20% of cases, VZV reactivates later in life, producing a disease known as shingles or herpes zoster. VZV can also infect the central nervous system, with a 2013 article reporting an incidence rate of 1.02 cases per 100 000 inhabitants in Switzerland, and an annual incidence rate of 1.8 cases per 100,000 inhabitants in Sweden.[3] For comparison, Amyotrophic lateral sclerosis (ALS) has an annual incidence rate of 0.2 to 2.4 per 100,000 population in industrialized countries. [4]
Other serious complications of varicella zoster infection include postherpetic neuralgia, Mollaret’s meningitis, zoster multiplex, and inflammation of arteries in the brain leading to stroke,[5] myelitis, herpes ophthalmics, or zoster sine herpete. In Ramsay Hunt syndrome, VZV affects the geniculate ganglion resulting in lesions that follow specific branches of the facial nerve. Symptoms may include painful blisters on the tongue and ear along with one sided facial weakness and hearing loss.
Recent advances in research and diagnosis
Until the mid-1990s, infectious complications of the CNS caused by VZV reactivation were regarded as rare. The presence of rash, as well as specific neurological symptoms, were required to diagnose a CNS infection caused by VZV. Since 2000, PCR testing has become more widely used, and the number of diagnosed cases of CNS infection has increased. [6]
Classic textbook descriptions state that VZV reactivation in the CNS is restricted to immunocompromised individuals and the elderly, however, recent studies have found that most patients are immunocompetent, and less than 60 years old. Old references cite vesicular rash as a characteristic finding, however, recent studies have found that the rash is only present in 45% of cases. [7] In addition, systemic inflammation is not as reliable an indicator as previously thought: the mean level of C-reactive protein and mean white blood cell count is within the normal range in patients with VZV meningitis. [8] MRI and CT scans are usually normal in cases of VZV reactivation in the CNS. CSF pleocytosis, previously thought to be a strong indicator of VZV encephalitis, was absent in half of a group of patients diagnosed with VZV encephalitis by PCR. [9]
The frequency of CNS infections presented at the emergency room of a community hospital is not negligible, so a means of diagnosing cases is needed. PCR is not a foolproof method of diagnosis, but because so many other indicators have turned out to not be reliable in diagnosing VZV infections in the CNS, screening for VZV by PCR is recommended. Negative PCR does not rule out VZV involvement, but a positive PCR can be used for diagnosis, and appropriate treatment started (for example, antivirals can be prescribed rather than antibiotics). [10]
The introduction of DNA analysis techniques has shown some complications of varicella-zoster to be more common than previously thought. For example, sporadic meningoencephalitis (ME) caused by varicella-zoster was regarded as a rare disease, mostly related to childhood chickenpox. However, meningoencephalitis caused by varicella-zoster is increasingly recognized as a predominant cause of ME among immunocompetent adults in non-epidemic circumstances.[11]
Diagnosis of complications of varicella-zoster, particularly in cases where the disease reactivates after years or decades of latency, are difficult. A rash (shingles) can be present or absent. Symptoms vary, and there is significant overlap in symptoms with herpes-simplex symptoms.[11]
Although DNA analysis techniques such as Polymerase Chain Reaction can be used to look for DNA of herpesviruses in spinal fluid or blood, the results may be negative, even in cases where other definitive symptoms exist.[12] Notwithstanding these limitations, the use of PCR has resulted in an advance in the state of the art in our understanding of herpesviruses, including VZV, during the 1990s and 2000s. For example, in the past, clinicians believed that encephalitis was caused by herpes simplex and that patients always died or developed serious long term function problems. People were diagnosed at autopsy or by brain biopsy. Brain biopsy is not undertaken lightly: it is reserved only for serious cases that cannot be diagnosed by less invasive methods. For this reason, knowledge of these herpes virus conditions was limited to severe cases. DNA techniques have made it possible to diagnose “mild” cases, caused by VZV or HSV, in which the symptoms include fever, headache, and altered mental status. Mortality rates in treated patients are decreasing.[11]
Morphology
VZV is closely related to the herpes simplex viruses (HSV), sharing much genome homology. The known envelope glycoproteins (gB, gC, gE, gH, gI, gK, gL) correspond with those in HSV; however, there is no equivalent of HSV gD. VZV also fails to produce the LAT (latency-associated transcripts) that play an important role in establishing HSV latency (herpes simplex virus). VZV virions are spherical and 180–200 nm in diameter. Their lipid envelope encloses the 100 nm nucleocapsid of 162 hexameric and pentameric capsomers arranged in an icosahedral form. Its DNA is a single, linear, double-stranded molecule, 125,000 nt long. The capsid is surrounded by a number of loosely associated proteins known collectively as the tegument; many of these proteins play critical roles in initiating the process of virus reproduction in the infected cell. The tegument is in turn covered by a lipid envelope studded with glycoproteins that are displayed on the exterior of the virion, each approximately 8 nm long.
Genome
The genome was first sequenced in 1986.[13] It is a linear duplex DNA molecule, a laboratory strain has 124,884 base pairs. The genome has 2 predominant isomers, depending on the orientation of the S segment, P (prototype) and IS (inverted S) which are present with equal frequency for a total frequency of 90-95%. The L segment can also be inverted resulting in a total of four linear isomers (IL and ILS). This is distinct from HSV’s equiprobable distribution, and the discriminatory mechanism is not known. A small percentage of isolated molecules are circular genomes, about which little is known. (It is known that HSV circularizes on infection.) There are at least 70 open reading frames in the genome.
There are at least five clades of this virus.[14] Clades 1 and 3 include European/North American strains; clade 2 are Asian strains, especially from Japan; and clade 5 appears to be based in India. Clade 4 includes some strains from Europe but its geographic origins need further clarification.
Evolution
Commonality with HSV1 and HSV2 indicates a common ancestor, five genes do not have corresponding HSV genes. Relation with other human herpes viruses is less strong, but many homologous and conserved gene blocks are still found.
There are five principal clades (1-5) and four genotypes that do not fit into these clades.[15] The current distribution of these clades is Asia (clades 1, 2, and 5) and Europe (clades 1, 3 and 4). Allocation of VZV strains to clades required a sequence of the whole virus genome. Practically all molecular epidemiological data on global VZV strain distribution obtained with the targeted sequencing of selected regions.
Phylogenetic analysis of VZV genomic sequences resolves wild-type strains into 9 genotypes (E1, E2, J, M1, M2, M3, M4, VIII and IX).[16][17] Complete sequences for M3 and M4 strains are unavailable, but targeted analyses of representative strains suggest they are stable, circulating VZV genotypes. Sequence analysis of VZV isolates identified both shared and specific markers for every genotype and validated a unified VZV genotyping strategy. Despite high genotype diversity no evidence for intra-genotypic recombination was observed. Five of seven VZV genotypes were reliably discriminated using only four single nucleotide polymorphisms (SNP) present in ORF22, and the E1 and E2 genotypes were resolved using SNP located in ORF21, ORF22 or ORF50. Sequence analysis of 342 clinical varicella and zoster specimens from 18 European countries identified the following distribution of VZV genotypes: E1, 221 (65%); E2, 87 (25%); M1, 20 (6%); M2, 3 (1%); M4, 11 (3%). No M3 or J strains were observed.[16] Of 165 clinical varicella and zoster isolates from Australia and New Zealand typed using this approach, 67 of 127 eastern Australian isolates were E1, 30 were E2, 16 were J, 10 were M1, and 4 were M2; 25 of 38 New Zealand isolates were E1, 8 were E2, and 5 were M1.[18]
The mutation rate for synonymous and nonsynonymous mutation rates among the herpesviruses have been estimated at 1 × 10−7 and 2.7 × 10−8 mutations/site/year, respectively, based on the highly conserved gB gene.[19]
Vaccination
A live attenuated VZV Oka/Merck strain vaccine is available and is marketed in the United States under the trade name Varivax. It was developed by Merck, Sharp & Dohme in the 1980s from the Oka strain virus isolated and attenuated by Michiaki Takahashi and colleagues in the 1970s. It was submitted to the US Food and Drug Administration for approval in 1990 and was approved in 1995. Since then, it has been added to the recommended vaccination schedules for children in Australia, the United States, and many other countries. Varicella vaccination has raised concerns in some that the immunity induced by the vaccine may not be lifelong, possibly leaving adults vulnerable to more severe disease as the immunity from their childhood immunization wanes. Vaccine coverage in the United States in the population recommended for vaccination is approaching 90%, with concomitant reductions in the incidence of varicella cases and hospitalizations and deaths due to VZV. So far, clinical data has proved that the vaccine is effective for over 10 years in preventing varicella infection in healthy individuals and when breakthrough infections do occur, illness is typically mild.[20] In 2007, the ACIP recommended a second dose of vaccine before school entry to ensure the maintenance of high levels of varicella immunity.[21]
In 2006, the United States Food and Drug Administration approved Zostavax for the prevention of shingles. Zostavax is a more concentrated formulation of the Varivax vaccine, designed to elicit an immune response in older adults whose immunity to VZV wanes with advancing age. A systematic review by the Cochrane Library shows that Zostavax reduces the incidence of shingles by almost 50%.[22]
See also
Gallery
-
![Transmission electron micrograph of varicella-zoster virions from vesicle fluid of patient with chickenpox. From Public Health Image Library (PHIL). [23]](https://www.wikidoc.org/images/b/b7/VZV15.jpeg) Transmission electron micrograph of varicella-zoster virions from vesicle fluid of patient with chickenpox. From Public Health Image Library (PHIL). [23]
Transmission electron micrograph of varicella-zoster virions from vesicle fluid of patient with chickenpox. From Public Health Image Library (PHIL). [23] -
![Electron micrographs of Variola, Varicella and Vaccinia virions. From Public Health Image Library (PHIL). [23]](https://www.wikidoc.org/images/a/a3/Chickenpox38.jpeg) Electron micrographs of Variola, Varicella and Vaccinia virions. From Public Health Image Library (PHIL). [23]
Electron micrographs of Variola, Varicella and Vaccinia virions. From Public Health Image Library (PHIL). [23] -
Transmission electron micrograph (TEM) of a Varicella (Chickenpox) Virus. From Public Health Image Library (PHIL). [23]
-
Various viruses from the Herpesviridae family seen using an electron micrograph. From Public Health Image Library (PHIL). [23]
-
photomicrograph reveals some of the cytoarchitectural histopathologic changes which you’d find in a human skin tissue specimen that included a chickenpox, or varicella zoster virus lesion (500x mag). From Public Health Image Library (PHIL). [23]
-
Hematoxylin-eosin (H&E)-stained photomicrograph reveals some of the cytoarchitectural histopathologic changes found in a human skin tissue specimen that included a varicella zoster virus lesion (50x mag). From Public Health Image Library (PHIL). [23]
-
Hematoxylin-eosin (H&E)-stained photomicrograph reveals some of the cytoarchitectural histopathologic changes found in a human skin tissue specimen that included a varicella zoster virus lesion (50x mag). From Public Health Image Library (PHIL). [23]
-
Hematoxylin-eosin (H&E)-stained photomicrograph reveals some of the cytoarchitectural histopathologic changes found in a human skin tissue specimen that included a varicella zoster virus lesion (500x mag). From Public Health Image Library (PHIL). [23]
-
![Hematoxylin-eosin (H&E)-stained photomicrograph reveals some of the cytoarchitectural histopathologic changes found in a human skin tissue specimen that included a varicella zoster virus lesion (1200x mag). From Public Health Image Library (PHIL). [23]](https://www.wikidoc.org/images/1/14/VZV05.jpeg) Hematoxylin-eosin (H&E)-stained photomicrograph reveals some of the cytoarchitectural histopathologic changes found in a human skin tissue specimen that included a varicella zoster virus lesion (1200x mag). From Public Health Image Library (PHIL). [23]
Hematoxylin-eosin (H&E)-stained photomicrograph reveals some of the cytoarchitectural histopathologic changes found in a human skin tissue specimen that included a varicella zoster virus lesion (1200x mag). From Public Health Image Library (PHIL). [23] -
Hematoxylin-eosin (H&E)-stained photomicrograph reveals some of the cytoarchitectural histopathologic changes found in a human skin tissue specimen that included a varicella zoster virus lesion (1200x mag). From Public Health Image Library (PHIL). [23]
-
![From Public Health Image Library (PHIL). [23]](https://www.wikidoc.org/images/7/72/VZV03.jpeg)
-
![This image depicts three mounted chickenpox scabs seen from the side. From Public Health Image Library (PHIL). [23]](https://www.wikidoc.org/images/1/1f/VZV02.jpeg) This image depicts three mounted chickenpox scabs seen from the side. From Public Health Image Library (PHIL). [23]
This image depicts three mounted chickenpox scabs seen from the side. From Public Health Image Library (PHIL). [23] -
![Back of boy who had manifested the maculopapular rash that was determined to be chickenpox, also known as varicella-zoster virus (VZV). From Public Health Image Library (PHIL). [23]](https://www.wikidoc.org/images/f/fd/VZV01.jpeg) Back of boy who had manifested the maculopapular rash that was determined to be chickenpox, also known as varicella-zoster virus (VZV). From Public Health Image Library (PHIL). [23]
Back of boy who had manifested the maculopapular rash that was determined to be chickenpox, also known as varicella-zoster virus (VZV). From Public Health Image Library (PHIL). [23] -
![Chickenpox lesions on the skin of this patient's left breast and arm on day 6 of the illness. From Public Health Image Library (PHIL). [23]](https://www.wikidoc.org/images/9/95/Chickenpox36.jpeg) Chickenpox lesions on the skin of this patient’s left breast and arm on day 6 of the illness. From Public Health Image Library (PHIL). [23]
Chickenpox lesions on the skin of this patient’s left breast and arm on day 6 of the illness. From Public Health Image Library (PHIL). [23] -
![Chickenpox lesions on the skin of this patient's back and buttocks at day 6 of the illness. From Public Health Image Library (PHIL). [23]](https://www.wikidoc.org/images/8/8e/Chickenpox35.jpeg) Chickenpox lesions on the skin of this patient’s back and buttocks at day 6 of the illness. From Public Health Image Library (PHIL). [23]
Chickenpox lesions on the skin of this patient’s back and buttocks at day 6 of the illness. From Public Health Image Library (PHIL). [23] -
![Chickenpox lesions on the skin of this patient's breasts, arms, and torso at day 6 of the illness. From Public Health Image Library (PHIL). [23]](https://www.wikidoc.org/images/7/71/Chickenpox34.jpeg) Chickenpox lesions on the skin of this patient’s breasts, arms, and torso at day 6 of the illness. From Public Health Image Library (PHIL). [23]
Chickenpox lesions on the skin of this patient’s breasts, arms, and torso at day 6 of the illness. From Public Health Image Library (PHIL). [23] -
![Patient with cervical skin lesions caused by chickenpox. From Public Health Image Library (PHIL). [23]](https://www.wikidoc.org/images/c/c7/Chickenpox33.jpeg) Patient with cervical skin lesions caused by chickenpox. From Public Health Image Library (PHIL). [23]
Patient with cervical skin lesions caused by chickenpox. From Public Health Image Library (PHIL). [23] -
![4-month old infant with skin lesions on his brow ridge due to chickenpox. From Public Health Image Library (PHIL). [23]](https://www.wikidoc.org/images/0/03/Chickenpox32.jpeg) 4-month old infant with skin lesions on his brow ridge due to chickenpox. From Public Health Image Library (PHIL). [23]
4-month old infant with skin lesions on his brow ridge due to chickenpox. From Public Health Image Library (PHIL). [23] -
![Patient had presented with chickenpox demonstrating the typical rash on day eight. From Public Health Image Library (PHIL). [23]](https://www.wikidoc.org/images/8/84/Chickenpox29.jpeg) Patient had presented with chickenpox demonstrating the typical rash on day eight. From Public Health Image Library (PHIL). [23]
Patient had presented with chickenpox demonstrating the typical rash on day eight. From Public Health Image Library (PHIL). [23] -
![Patient developed palatal mucosal lesions due to chickenpox. From Public Health Image Library (PHIL). [23]](https://www.wikidoc.org/images/1/18/Chickenpox28.jpeg) Patient developed palatal mucosal lesions due to chickenpox. From Public Health Image Library (PHIL). [23]
Patient developed palatal mucosal lesions due to chickenpox. From Public Health Image Library (PHIL). [23] -
![Vaccine recipient developed a secondary herpes infection adjacent to the vaccination site. From Public Health Image Library (PHIL). [23]](https://www.wikidoc.org/images/3/3e/Chickenpox27.jpeg) Vaccine recipient developed a secondary herpes infection adjacent to the vaccination site. From Public Health Image Library (PHIL). [23]
Vaccine recipient developed a secondary herpes infection adjacent to the vaccination site. From Public Health Image Library (PHIL). [23] -
![Pustulovesicular rash represents a generalized herpes outbreak due to the Varicella-zoster virus (VZV) pathogen. From Public Health Image Library (PHIL). [23]](https://www.wikidoc.org/images/6/6e/Chickenpox26.jpeg) Pustulovesicular rash represents a generalized herpes outbreak due to the Varicella-zoster virus (VZV) pathogen. From Public Health Image Library (PHIL). [23]
Pustulovesicular rash represents a generalized herpes outbreak due to the Varicella-zoster virus (VZV) pathogen. From Public Health Image Library (PHIL). [23] -
![Case of chickenpox. From Public Health Image Library (PHIL). [23]](https://www.wikidoc.org/images/e/e2/Chickenpox24.jpeg) Case of chickenpox. From Public Health Image Library (PHIL). [23]
Case of chickenpox. From Public Health Image Library (PHIL). [23] -
![Case of chickenpox. From Public Health Image Library (PHIL). [23]](https://www.wikidoc.org/images/6/6c/Chickenpox23.jpeg) Case of chickenpox. From Public Health Image Library (PHIL). [23]
Case of chickenpox. From Public Health Image Library (PHIL). [23] -
![Case of chickenpox. From Public Health Image Library (PHIL). [23]](https://www.wikidoc.org/images/5/5a/Chickenpox22.jpeg) Case of chickenpox. From Public Health Image Library (PHIL). [23]
Case of chickenpox. From Public Health Image Library (PHIL). [23] -
![Chickenpox lesions on a patient’s back, which were displaying the characteristic “cropping” distribution, or manifesting themselves in clusters. From Public Health Image Library (PHIL). [23]](https://www.wikidoc.org/images/4/47/Chickenpox21.jpeg) Chickenpox lesions on a patient’s back, which were displaying the characteristic “cropping” distribution, or manifesting themselves in clusters. From Public Health Image Library (PHIL). [23]
Chickenpox lesions on a patient’s back, which were displaying the characteristic “cropping” distribution, or manifesting themselves in clusters. From Public Health Image Library (PHIL). [23] -
![Posterior view of a hospitalized man's neck, back and shoulders, who’d been assigned a bed in a smallpox ward, due to an initially misdiagnosed illness, which turned out to be chickenpox. From Public Health Image Library (PHIL). [23]](https://www.wikidoc.org/images/e/e9/Chickenpox20.jpeg) Posterior view of a hospitalized man’s neck, back and shoulders, who’d been assigned a bed in a smallpox ward, due to an initially misdiagnosed illness, which turned out to be chickenpox. From Public Health Image Library (PHIL). [23]
Posterior view of a hospitalized man’s neck, back and shoulders, who’d been assigned a bed in a smallpox ward, due to an initially misdiagnosed illness, which turned out to be chickenpox. From Public Health Image Library (PHIL). [23] -
![View of a patient’s thighs and upper legs, who’d been diagnosed with chickenpox. From Public Health Image Library (PHIL). [23]](https://www.wikidoc.org/images/2/21/Chickenpox19.jpeg) View of a patient’s thighs and upper legs, who’d been diagnosed with chickenpox. From Public Health Image Library (PHIL). [23]
View of a patient’s thighs and upper legs, who’d been diagnosed with chickenpox. From Public Health Image Library (PHIL). [23] -
![Pathologic changes seen on the surface of the right unilateral side of this elderly male patient’s tongue and chin, represent a herpes outbreak due to the Varicella-zoster virus (VZV) pathogen. From Public Health Image Library (PHIL). [23]](https://www.wikidoc.org/images/b/b8/Chickenpox18.jpeg) Pathologic changes seen on the surface of the right unilateral side of this elderly male patient’s tongue and chin, represent a herpes outbreak due to the Varicella-zoster virus (VZV) pathogen. From Public Health Image Library (PHIL). [23]
Pathologic changes seen on the surface of the right unilateral side of this elderly male patient’s tongue and chin, represent a herpes outbreak due to the Varicella-zoster virus (VZV) pathogen. From Public Health Image Library (PHIL). [23] -
![Viewed from above, this image depicts a smallpox scab (left), and chickenpox scab (right) as a demonstration in comparative morphology. From Public Health Image Library (PHIL). [23]](https://www.wikidoc.org/images/a/ae/Chickenpox17.jpeg) Viewed from above, this image depicts a smallpox scab (left), and chickenpox scab (right) as a demonstration in comparative morphology. From Public Health Image Library (PHIL). [23]
Viewed from above, this image depicts a smallpox scab (left), and chickenpox scab (right) as a demonstration in comparative morphology. From Public Health Image Library (PHIL). [23] -
![Close-up of a maculopapular rash that was diagnosed as a crop of chickenpox lesions. From Public Health Image Library (PHIL). [23]](https://www.wikidoc.org/images/a/a8/Chickenpox16.jpeg) Close-up of a maculopapular rash that was diagnosed as a crop of chickenpox lesions. From Public Health Image Library (PHIL). [23]
Close-up of a maculopapular rash that was diagnosed as a crop of chickenpox lesions. From Public Health Image Library (PHIL). [23] -
![Lateral view of a 4 month-old infant’s face with a single varicella-zoster, otherwise known as chickenpox. From Public Health Image Library (PHIL). [23]](https://www.wikidoc.org/images/4/45/Chickenpox15.png) Lateral view of a 4 month-old infant’s face with a single varicella-zoster, otherwise known as chickenpox. From Public Health Image Library (PHIL). [23]
Lateral view of a 4 month-old infant’s face with a single varicella-zoster, otherwise known as chickenpox. From Public Health Image Library (PHIL). [23] -
![This anteroposterior (AP) radiograph revealed bilateral pulmonary infiltrates throughout the entirety of each lung field in the case of a child with leukemia, as well as chickenpox pneumonia. From Public Health Image Library (PHIL). [23]](https://www.wikidoc.org/images/0/0f/Chickenpox06.jpeg) This anteroposterior (AP) radiograph revealed bilateral pulmonary infiltrates throughout the entirety of each lung field in the case of a child with leukemia, as well as chickenpox pneumonia. From Public Health Image Library (PHIL). [23]
This anteroposterior (AP) radiograph revealed bilateral pulmonary infiltrates throughout the entirety of each lung field in the case of a child with leukemia, as well as chickenpox pneumonia. From Public Health Image Library (PHIL). [23] -
![Image depicts three mounted chickenpox scabs seen from the side revealing the superficiality of these scabs when morphologically compared to a smallpox scab. From Public Health Image Library (PHIL). [23]](https://www.wikidoc.org/images/0/09/Chickenpox04.jpeg) Image depicts three mounted chickenpox scabs seen from the side revealing the superficiality of these scabs when morphologically compared to a smallpox scab. From Public Health Image Library (PHIL). [23]
Image depicts three mounted chickenpox scabs seen from the side revealing the superficiality of these scabs when morphologically compared to a smallpox scab. From Public Health Image Library (PHIL). [23] -
![Volar surface of a patient’s left forearm, including the palmar surface of the left hand upon which you’ll note classic maculopapular rash of chickenpox. From Public Health Image Library (PHIL). [23]](https://www.wikidoc.org/images/0/09/Chickenpox03.jpeg) Volar surface of a patient’s left forearm, including the palmar surface of the left hand upon which you’ll note classic maculopapular rash of chickenpox. From Public Health Image Library (PHIL). [23]
Volar surface of a patient’s left forearm, including the palmar surface of the left hand upon which you’ll note classic maculopapular rash of chickenpox. From Public Health Image Library (PHIL). [23] -
![Right lateral surface of a patient’s right lower leg and foot with classic maculopapular rash of chickenpox. From Public Health Image Library (PHIL). [23]](https://www.wikidoc.org/images/5/50/Chickenpox02.jpeg) Right lateral surface of a patient’s right lower leg and foot with classic maculopapular rash of chickenpox. From Public Health Image Library (PHIL). [23]
Right lateral surface of a patient’s right lower leg and foot with classic maculopapular rash of chickenpox. From Public Health Image Library (PHIL). [23] -
![Bilateral pulmonary infiltrates throughout the entirety of each lung field in the case of a child with leukemia, as well as chickenpox pneumonia. From Public Health Image Library (PHIL). [23]](https://www.wikidoc.org/images/5/55/Chickenpox05.jpeg) Bilateral pulmonary infiltrates throughout the entirety of each lung field in the case of a child with leukemia, as well as chickenpox pneumonia. From Public Health Image Library (PHIL). [23]
Bilateral pulmonary infiltrates throughout the entirety of each lung field in the case of a child with leukemia, as well as chickenpox pneumonia. From Public Health Image Library (PHIL). [23]
![Transmission electron micrograph of varicella-zoster virions from vesicle fluid of patient with chickenpox. From Public Health Image Library (PHIL). [23]](https://www.wikidoc.org/index.php/File%3AVZV15.jpeg)
![Electron micrographs of Variola, Varicella and Vaccinia virions. From Public Health Image Library (PHIL). [23]](https://www.wikidoc.org/index.php/File%3AChickenpox38.jpeg)
![Hematoxylin-eosin (H&E)-stained photomicrograph reveals some of the cytoarchitectural histopathologic changes found in a human skin tissue specimen that included a varicella zoster virus lesion (1200x mag). From Public Health Image Library (PHIL). [23]](https://www.wikidoc.org/index.php/File%3AVZV05.jpeg)
![From Public Health Image Library (PHIL). [23]](https://www.wikidoc.org/index.php/File%3AVZV03.jpeg)
![This image depicts three mounted chickenpox scabs seen from the side. From Public Health Image Library (PHIL). [23]](https://www.wikidoc.org/index.php/File%3AVZV02.jpeg)
![Back of boy who had manifested the maculopapular rash that was determined to be chickenpox, also known as varicella-zoster virus (VZV). From Public Health Image Library (PHIL). [23]](https://www.wikidoc.org/index.php/File%3AVZV01.jpeg)
![Chickenpox lesions on the skin of this patient's left breast and arm on day 6 of the illness. From Public Health Image Library (PHIL). [23]](https://www.wikidoc.org/index.php/File%3AChickenpox36.jpeg)
![Chickenpox lesions on the skin of this patient's back and buttocks at day 6 of the illness. From Public Health Image Library (PHIL). [23]](https://www.wikidoc.org/index.php/File%3AChickenpox35.jpeg)
![Chickenpox lesions on the skin of this patient's breasts, arms, and torso at day 6 of the illness. From Public Health Image Library (PHIL). [23]](https://www.wikidoc.org/index.php/File%3AChickenpox34.jpeg)
![Patient with cervical skin lesions caused by chickenpox. From Public Health Image Library (PHIL). [23]](https://www.wikidoc.org/index.php/File%3AChickenpox33.jpeg)
![4-month old infant with skin lesions on his brow ridge due to chickenpox. From Public Health Image Library (PHIL). [23]](https://www.wikidoc.org/index.php/File%3AChickenpox32.jpeg)
![Patient had presented with chickenpox demonstrating the typical rash on day eight. From Public Health Image Library (PHIL). [23]](https://www.wikidoc.org/index.php/File%3AChickenpox29.jpeg)
![Patient developed palatal mucosal lesions due to chickenpox. From Public Health Image Library (PHIL). [23]](https://www.wikidoc.org/index.php/File%3AChickenpox28.jpeg)
![Vaccine recipient developed a secondary herpes infection adjacent to the vaccination site. From Public Health Image Library (PHIL). [23]](https://www.wikidoc.org/index.php/File%3AChickenpox27.jpeg)
![Pustulovesicular rash represents a generalized herpes outbreak due to the Varicella-zoster virus (VZV) pathogen. From Public Health Image Library (PHIL). [23]](https://www.wikidoc.org/index.php/File%3AChickenpox26.jpeg)
![Case of chickenpox. From Public Health Image Library (PHIL). [23]](https://www.wikidoc.org/index.php/File%3AChickenpox24.jpeg)
![Case of chickenpox. From Public Health Image Library (PHIL). [23]](https://www.wikidoc.org/index.php/File%3AChickenpox23.jpeg)
![Case of chickenpox. From Public Health Image Library (PHIL). [23]](https://www.wikidoc.org/index.php/File%3AChickenpox22.jpeg)
![Chickenpox lesions on a patient’s back, which were displaying the characteristic “cropping” distribution, or manifesting themselves in clusters. From Public Health Image Library (PHIL). [23]](https://www.wikidoc.org/index.php/File%3AChickenpox21.jpeg)
![Posterior view of a hospitalized man's neck, back and shoulders, who’d been assigned a bed in a smallpox ward, due to an initially misdiagnosed illness, which turned out to be chickenpox. From Public Health Image Library (PHIL). [23]](https://www.wikidoc.org/index.php/File%3AChickenpox20.jpeg)
![View of a patient’s thighs and upper legs, who’d been diagnosed with chickenpox. From Public Health Image Library (PHIL). [23]](https://www.wikidoc.org/index.php/File%3AChickenpox19.jpeg)
![Pathologic changes seen on the surface of the right unilateral side of this elderly male patient’s tongue and chin, represent a herpes outbreak due to the Varicella-zoster virus (VZV) pathogen. From Public Health Image Library (PHIL). [23]](https://www.wikidoc.org/index.php/File%3AChickenpox18.jpeg)
![Viewed from above, this image depicts a smallpox scab (left), and chickenpox scab (right) as a demonstration in comparative morphology. From Public Health Image Library (PHIL). [23]](https://www.wikidoc.org/index.php/File%3AChickenpox17.jpeg)
![Close-up of a maculopapular rash that was diagnosed as a crop of chickenpox lesions. From Public Health Image Library (PHIL). [23]](https://www.wikidoc.org/index.php/File%3AChickenpox16.jpeg)
![This anteroposterior (AP) radiograph revealed bilateral pulmonary infiltrates throughout the entirety of each lung field in the case of a child with leukemia, as well as chickenpox pneumonia. From Public Health Image Library (PHIL). [23]](https://www.wikidoc.org/index.php/File%3AChickenpox06.jpeg)
![Image depicts three mounted chickenpox scabs seen from the side revealing the superficiality of these scabs when morphologically compared to a smallpox scab. From Public Health Image Library (PHIL). [23]](https://www.wikidoc.org/index.php/File%3AChickenpox04.jpeg)
![Volar surface of a patient’s left forearm, including the palmar surface of the left hand upon which you’ll note classic maculopapular rash of chickenpox. From Public Health Image Library (PHIL). [23]](https://www.wikidoc.org/index.php/File%3AChickenpox03.jpeg)
![Right lateral surface of a patient’s right lower leg and foot with classic maculopapular rash of chickenpox. From Public Health Image Library (PHIL). [23]](https://www.wikidoc.org/index.php/File%3AChickenpox02.jpeg)
![Bilateral pulmonary infiltrates throughout the entirety of each lung field in the case of a child with leukemia, as well as chickenpox pneumonia. From Public Health Image Library (PHIL). [23]](https://www.wikidoc.org/index.php/File%3AChickenpox05.jpeg)
References
- ↑ “The protean neurologic manifestations of varicella-zoster virus infection”. Cleveland Clinic Journal of Medicine. July 2007.
- ↑ Steiner I (2007). “The neurotropic herpes viruses: herpes simplex and varicella-zoster”. Lancet Neurol. 6 (11): 1015–28. doi:10.1016/S1474-4422(07)70267-3. PMID 17945155. Unknown parameter
|coauthors=ignored (help) - ↑ “Infection of the central nervous system caused by varicella zoster virus reactivation: a retrospective case series study”. International Journal of Infectious Diseases. July 2013.
- ↑ “Mapping amyotrophic lateral sclerosis lake risk factors across northern New England”. International Journal of Health Geographics. 2014.
- ↑ “The varicella zoster virus vasculopathies: clinical, CSF, imaging, and virologic features”. Neurology. March 2008.
- ↑ “Infection of the central nervous system caused by varicella zoster virus reactivation: a retrospective case series study”. International Journal of Infectious Diseases. July 2013.
- ↑ “Infection of the central nervous system caused by varicella zoster virus reactivation: a retrospective case series study”. International Journal of Infectious Diseases. July 2013.
- ↑ “Clinical Features of Viral Meningitis in Adults: Significant Differences in Cerebrospinal Fluid Findings among Herpes Simplex Virus, Varicella Zoster Virus, and Enterovirus Infections” (PDF). Clinical Infectious Diseases, the Infectious Diseases Society of America. 2008.
- ↑ “Infection of the central nervous system caused by varicella zoster virus reactivation: a retrospective case series study”. International Journal of Infectious Diseases. July 2013.
- ↑ “Infection of the central nervous system caused by varicella zoster virus reactivation: a retrospective case series study”. International Journal of Infectious Diseases. July 2013.
- ↑ 11.0 11.1 11.2 “Varicella zoster vs. herpes simplex meningoencephalitis in the PCR era. A single center study”. Journal of the Neurological Sciences. August 2011.
- ↑ “Recurrent Herpes Simplex Virus Type 2 Meningitis: A Case Report of Mollaret’s Meningitis” (PDF). Jpn. J. Infect. Dis. July 2002.
- ↑ Davison AJ, Scott JE (1986) The complete DNA sequence of varicella-zoster virus. J Gen Virol 67:1759-1816
- ↑ Template:Cite doi
- ↑ Template:Cite doi
- ↑ 16.0 16.1 PMID 19019403 (PMID 19019403)
Citation will be completed automatically in a few minutes. Jump the queue or expand by hand - ↑ Template:Cite doi
- ↑ Template:Cite doi
- ↑ McGeoch DJ, Cook S (1994) Molecular phylogeny of the alphaherpesvirinae subfamily and a proposed evolutionary timescale. J Mol Biol 238:9-22
- ↑ “Prevention of varicella: Recommendations of the Advisory Committee on Immunization Practices (ACIP). Centers for Disease Control and Prevention”. MMWR Recomm Rep. 45 (RR–11): 1–36. July 1996. PMID 8668119.
- ↑ Marin M (June 2007). “Prevention of varicella: recommendations of the Advisory Committee on Immunization Practices (ACIP)”. MMWR Recomm Rep. 56 (RR–4): 1–40. PMID 17585291. Unknown parameter
|coauthors=ignored (help) - ↑ Gagliardi AM, Gomes Silva BN, Torloni MR, Soares BG (2012). Gagliardi, Anna MZ, ed. “Vaccines for preventing herpes zoster in older adults”. Cochrane Database Syst Rev. 10: CD008858. doi:10.1002/14651858.CD008858.pub2. PMID 23076951.
- ↑ 23.00 23.01 23.02 23.03 23.04 23.05 23.06 23.07 23.08 23.09 23.10 23.11 23.12 23.13 23.14 23.15 23.16 23.17 23.18 23.19 23.20 23.21 23.22 23.23 23.24 23.25 23.26 23.27 23.28 23.29 23.30 23.31 23.32 23.33 23.34 23.35 23.36 “Public Health Image Library (PHIL)”.
External links
- “Varicella (Chickenpox) Vaccination” Centers for Disease Control and Prevention (CDC)
Differentiating Chickenpox from other Diseases
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Michael Maddaleni, B.S. João André Alves Silva, M.D. [2] Aravind Reddy Kothagadi M.B.B.S[3]
Overview
Chickenpox must be differentiated from various rash-causing conditions like Coxsackievirus, Stevens-Johnson syndrome (SJS), measles, rubella, Rocky mountain spotted fever and syphilis.
Differentiating Chickenpox from other Diseases
Chickenpox must be differentiated from other diseases presenting with diffuse papulovesicular rash in a febrile patient. The various conditions that should be differentiated from chickenpox include:[1][2][3][4][5][6][7]
Common conditions to be differentiated from chickenpox:
| Common Conditions | Features |
|---|---|
| Coxsackievirus |
|
| Stevens-Johnson syndrome |
|
| Kawasaki disease |
|
| Measles |
|
| Syphilis | It commonly presents with gneralized systemic symptoms such as malaise, fatigue, headache and fever. Skin eruptions may be subtle and asymptomatic It is classically described as:
|
| Rubella |
|
| Cytomegalovirus |
|
| Meningococcemia |
|
| Meningitis |
|
| Rocky Mountain spotted fever |
|
| Molluscum contagiosum |
|
| Mononucleosis |
|
Less common conditions to be differentiated from chickenpox:
| Less Common Diseases | Features |
|---|---|
| Atypical measles |
|
| Parvovirus B19 |
|
| Rickettsial pox | |
| Toxic erythema | |
| Monkeypox |
|
| Rat-bite fever | |
| Scarlet fever |
|
Differentiating chickenpox infection in immunocompromised host
Varicella Zoster virus infection is common among immunocompromised patients who are at high risk for other fungal, bacterial, and viral infections. It should be differentiated from the following diseases, which may present as confusion, fever and headache in immunocompromised patients:
| Disease | Differentiating signs and symptoms | Differentiating tests |
|---|---|---|
| CNS lymphoma[8] |
|
|
| Disseminated tuberculosis[9] |
|
|
| Aspergillosis[10] |
|
|
| Cryptococcosis |
|
|
| Chagas disease[11] |
|
|
| CMV infection[12] |
|
|
| HSV infection[13] |
|
|
| Varicella Zoster infection[14] |
|
|
| Brain abscess[15][16] |
|
|
| Progressive multifocal leukoencephalopathy[17] |
|
Oral lesions to be differentiated from chicken pox:
Oral lesions caused by chickenpox must be differentiated from other diseases presenting with pain and blistering within the mouth (gingivostomatitis and glossitis). The differentials include:
| Disease | Presentation | Risk Factors | Diagnosis | Affected Organ Systems | Important features | Picture |
|---|---|---|---|---|---|---|
| Coxsackie virus |
|
|

| |||
| Chicken pox |
|
|
|
|

| |
| Measles |
|
|
|
|

| |
| Herpangina |
|
|
|
|
|
 |
| Primary herpetic gingivostomatitis[20] |
|
|
|
|
|
|
| Oral Candidiasis |
|
|
Localized candidiasis
Invasive candidasis |
|
 |

| Disease | Presentation | Risk Factors | Diagnosis | Affected Organ Systems | Important features | Picture |
|---|---|---|---|---|---|---|
| Diseases predominantly affecting the oral cavity | ||||||
| Oral Candidiasis |
|
|
|
Localized candidiasis
Invasive candidasis |
|
|
| Herpes simplex oral lesions |
|
|
|
|
 | |
| Aphthous ulcers |
|
|
|
|
|
 |
| Squamous cell carcinoma |
|
|
 | |||
| Leukoplakia |
|
|
|
|
 | |
| Melanoma |
|
|
|
|
 | |
| Fordyce spots |
|
|
|
|
 | |
| Burning mouth syndrome |
|
|
||||
| Torus palatinus |
|
 | ||||
| Diseases involving oral cavity and other organ systems | ||||||
| Behcet’s disease |
|
|
|
 | ||
| Crohn’s disease |
|
|
|
|||
| Agranulocytosis |
|
|
||||
| Syphilis[24] |
|
|
|
 | ||
| Coxsackie virus |
|
|
| |||
| Chicken pox |
|
|
|
|
 | |
| Measles |
|
|
|
 | ||
References
- ↑ Hartman-Adams H, Banvard C, Juckett G (2014). “Impetigo: diagnosis and treatment”. Am Fam Physician. 90 (4): 229–35. PMID 25250996.
- ↑ Mehta N, Chen KK, Kroumpouzos G (2016). “Skin disease in pregnancy: The approach of the obstetric medicine physician”. Clin Dermatol. 34 (3): 320–6. doi:10.1016/j.clindermatol.2016.02.003. PMID 27265069.
- ↑ Moore, Zack S; Seward, Jane F; Lane, J Michael (2006). “Smallpox”. The Lancet. 367 (9508): 425–435. doi:10.1016/S0140-6736(06)68143-9. ISSN 0140-6736.
- ↑ Ibrahim F, Khan T, Pujalte GG (2015). “Bacterial Skin Infections”. Prim Care. 42 (4): 485–99. doi:10.1016/j.pop.2015.08.001. PMID 26612370.
- ↑ Ramoni S, Boneschi V, Cusini M (2016). “Syphilis as “the great imitator”: a case of impetiginoid syphiloderm”. Int J Dermatol. 55 (3): e162–3. doi:10.1111/ijd.13072. PMID 26566601.
- ↑ Kimura U, Yokoyama K, Hiruma M, Kano R, Takamori K, Suga Y (2015). “Tinea faciei caused by Trichophyton mentagrophytes (molecular type Arthroderma benhamiae ) mimics impetigo : a case report and literature review of cases in Japan”. Med Mycol J. 56 (1): E1–5. doi:10.3314/mmj.56.E1. PMID 25855021.
- ↑ CEDEF (2012). “[Item 87–Mucocutaneous bacterial infections]”. Ann Dermatol Venereol. 139 (11 Suppl): A32–9. doi:10.1016/j.annder.2012.01.002. PMID 23176858.
- ↑ Gerstner ER, Batchelor TT (2010). “Primary central nervous system lymphoma”. Arch. Neurol. 67 (3): 291–7. doi:10.1001/archneurol.2010.3. PMID 20212226.
- ↑ von Reyn CF, Kimambo S, Mtei L, Arbeit RD, Maro I, Bakari M, Matee M, Lahey T, Adams LV, Black W, Mackenzie T, Lyimo J, Tvaroha S, Waddell R, Kreiswirth B, Horsburgh CR, Pallangyo K (2011). “Disseminated tuberculosis in human immunodeficiency virus infection: ineffective immunity, polyclonal disease and high mortality”. Int. J. Tuberc. Lung Dis. 15 (8): 1087–92. doi:10.5588/ijtld.10.0517. PMID 21740673.
- ↑ Latgé JP (1999). “Aspergillus fumigatus and aspergillosis”. Clin. Microbiol. Rev. 12 (2): 310–50. PMC 88920. PMID 10194462.
- ↑ Rassi A, Rassi A, Marin-Neto JA (2010). “Chagas disease”. Lancet. 375 (9723): 1388–402. doi:10.1016/S0140-6736(10)60061-X. PMID 20399979.
- ↑ Emery VC (2001). “Investigation of CMV disease in immunocompromised patients”. J. Clin. Pathol. 54 (2): 84–8. PMC 1731357. PMID 11215290.
- ↑ Bustamante CI, Wade JC (1991). “Herpes simplex virus infection in the immunocompromised cancer patient”. J. Clin. Oncol. 9 (10): 1903–15. doi:10.1200/JCO.1991.9.10.1903. PMID 1919640.
- ↑ Hambleton S (2005). “Chickenpox”. Curr. Opin. Infect. Dis. 18 (3): 235–40. PMID 15864101.
- ↑ Alvis Miranda H, Castellar-Leones SM, Elzain MA, Moscote-Salazar LR (2013). “Brain abscess: Current management”. J Neurosci Rural Pract. 4 (Suppl 1): S67–81. doi:10.4103/0976-3147.116472. PMC 3808066. PMID 24174804.
- ↑ Patel K, Clifford DB (2014). “Bacterial brain abscess”. Neurohospitalist. 4 (4): 196–204. doi:10.1177/1941874414540684. PMC 4212419. PMID 25360205.
- ↑ Tan CS, Koralnik IJ (2010). “Progressive multifocal leukoencephalopathy and other disorders caused by JC virus: clinical features and pathogenesis”. Lancet Neurol. 9 (4): 425–37. doi:10.1016/S1474-4422(10)70040-5. PMC 2880524. PMID 20298966.
- ↑ 18.0 18.1 Feikin DR, Lezotte DC, Hamman RF, Salmon DA, Chen RT, Hoffman RE (2000). “Individual and community risks of measles and pertussis associated with personal exemptions to immunization”. JAMA. 284 (24): 3145–50. PMID 11135778.
- ↑ 19.0 19.1 Ratnam S, West R, Gadag V, Williams B, Oates E (1996). “Immunity against measles in school-aged children: implications for measles revaccination strategies”. Can J Public Health. 87 (6): 407–10. PMID 9009400.
- ↑ Kolokotronis, A.; Doumas, S. (2006). “Herpes simplex virus infection, with particular reference to the progression and complications of primary herpetic gingivostomatitis”. Clinical Microbiology and Infection. 12 (3): 202–211. doi:10.1111/j.1469-0691.2005.01336.x. ISSN 1198-743X.
- ↑ Chauvin PJ, Ajar AH (2002). “Acute herpetic gingivostomatitis in adults: a review of 13 cases, including diagnosis and management”. J Can Dent Assoc. 68 (4): 247–51. PMID 12626280.
- ↑ Ann M. Gillenwater, Nadarajah Vigneswaran, Hanadi Fatani, Pierre Saintigny & Adel K. El-Naggar (2013). “Proliferative verrucous leukoplakia (PVL): a review of an elusive pathologic entity!”. Advances in anatomic pathology. 20 (6): 416–423. doi:10.1097/PAP.0b013e3182a92df1. PMID 24113312. Unknown parameter
|month=ignored (help) - ↑ Andrès E, Zimmer J, Affenberger S, Federici L, Alt M, Maloisel F. (2006). “Idiosyncratic drug-induced agranulocytosis: Update of an old disorder”. Eur J Intern Med. 17 (8): 529–35. Text “pmid 17142169” ignored (help)
- ↑ title=”By Internet Archive Book Images [No restrictions], via Wikimedia Commons” href=”https://commons.wikimedia.org/wiki/File:A_manual_of_syphilis_and_the_venereal_diseases%2C_(1900)_(14595882378).jpg“
- ↑ “Dermatology Atlas”.
Epidemiology and Demographics
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Aravind Reddy Kothagadi M.B.B.S[2]
Overview
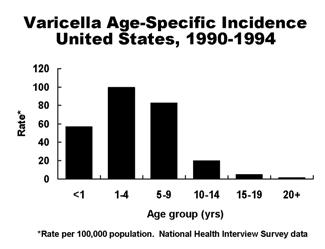
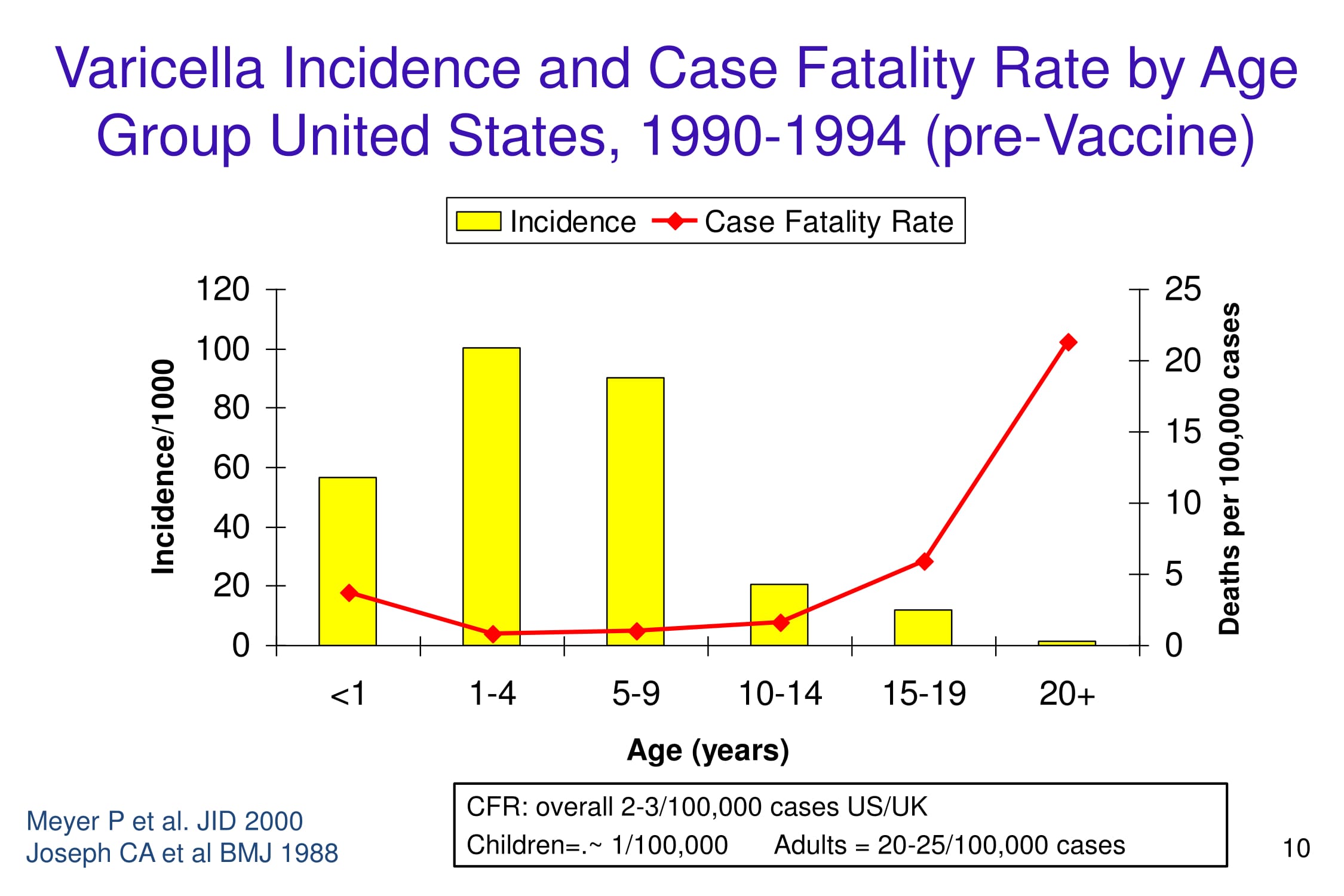
The incidence of chickenpox varies among various age groups. Varicella commonly affects children less than 10 years of age with the highest incidence among children 1-4 years of age. The incidence of chickenpox for children between 0 to 4 years of age is 5234 per 100,000 individuals. Between the years 1990-1994, the case fatality rate of chickenpox in the US/UK was 2-3 per 100,000 individuals. In developed countries, chickenpox causes around 3 deaths per 100,000 individuals.
Epidemiology
Incidence
The incidence of chickenpox varies among various age groups. The incidence rates per 100,000 persons in each age group were as follow:
- For age groups 0 to 4 years 5234 per 100,000 individuals
- For age groups 5 to 9 years 4132 per 100,000 individuals
- For age groups 10 to 14 years 1404 per 100,000 individuals
- For age groups 15 to 19 years 610 per 100,000 individuals
- For age groups >20 years 175 per 100,000 individuals
The rates of incidence of chickenpox declines for older age groups.[1]

Case Fatality Rate
Between the years 1990-1994, case fatality rate in the US/UK is 2-3 per 100,000.
- The case fatality rate among children was 1 per 100,000.
- In 2008 the case fatality rate in Brazil estimated case fatality rate is 4 per 100,000. [2]
- In 2000 the case fatality rate in Guinea Bissau was approximately 129 per 100,000 cases, 50 times higher than US/UK.
- In 1970, the case fatality rate in India among adults was 52 per 100,000 cases, 20 times higher than US/UK.
- Worldwide, the case fatality rate among adults was 20-25 per 100,000. [2]

Demographics
Age
- The prevalence of chicken pox decreases with age.
- Varicella commonly affects children less than 10 years of age with the highest incidence among children 1-4 years of age.


Gender
- The prevalence and incidence of chickenpox generally do not vary by gender.
- Chickenpox is more prevalent in females between the ages of 15 – 24 as compared to males.[3]
Race
- There is no racial predilection for chickenpox.
Developed Countries
The epidemiology and demographics of chickenpox in developed countries are as follows:[2]
- Incidence
- 1500 – 1600 per 100,000 persons per year
- Case-fatality rate
- 3 deaths per 100,000 cases
Gallery
-
-
-
-
-
-
![Varicella cases and states reporting, United States, 1972-1996. From Public Health Image Library (PHIL). [4]](https://www.wikidoc.org/images/2/26/Chickenpox40.jpeg) Varicella cases and states reporting, United States, 1972-1996. From Public Health Image Library (PHIL). [4]
Varicella cases and states reporting, United States, 1972-1996. From Public Health Image Library (PHIL). [4]

![Varicella cases and states reporting, United States, 1972-1996. From Public Health Image Library (PHIL). [4]](https://www.wikidoc.org/index.php/File%3AChickenpox40.jpeg)
References
- ↑ Choo PW, Donahue JG, Manson JE, Platt R (1995). “The epidemiology of varicella and its complications”. J. Infect. Dis. 172 (3): 706–12. PMID 7658062.
- ↑ 2.0 2.1 2.2 “www.who.int” (PDF).
- ↑ Fleming DM, Cross KW, Cobb WA, Chapman RS (2004). “Gender difference in the incidence of shingles”. Epidemiol. Infect. 132 (1): 1–5. PMC 2870070. PMID 14979582.
- ↑ “Public Health Image Library (PHIL)”.
Risk Factors
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1] Michael Maddaleni, B.S. Aravind Reddy Kothagadi M.B.B.S[2]
Overview
Risk factors which increase the likelihood of contracting chickenpox include, people without a history of chickenpox in the past, individuals who are not immunized against chickenpox, newborns, especially those born prematurely (less than 1 month or born to mothers who never contracted chickenpox prior to pregnancy), immunocompromised individuals, cancer patients and the use of immunosuppressant drugs.
Risk Factors
Risk factors which increase the likelihood of contracting chickenpox are as follows: [1][2]
- No history of chickenpox
- Not immunized for varicella
- Newborns, preterms and infants born to unsensitized mothers
- Pregnancy
- Infants born at less than 28 weeks gestation or who weigh less than or equal to 1000 grams regardless of maternal immune status.
- Immunodeficient states:
- Cancer patients
- Use of immunosuppressant drugs
References
- ↑ Leung TF, Chik KW, Li CK, Lai H, Shing MM, Chan PK, Lee V, Yuen PM (2000). “Incidence, risk factors and outcome of varicella-zoster virus infection in children after haematopoietic stem cell transplantation”. Bone Marrow Transplant. 25 (2): 167–72. doi:10.1038/sj.bmt.1702119. PMID 10673675.
- ↑ Miller GG, Dummer JS (2007). “Herpes simplex and varicella zoster viruses: forgotten but not gone”. Am. J. Transplant. 7 (4): 741–7. doi:10.1111/j.1600-6143.2006.01718.x. PMID 17391119.
Screening
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1] Associate Editor(s)-in-Chief: Aravind Reddy Kothagadi M.B.B.S[2]
Overview
According to Center for Disease Control and Prevention (CDC), there is insufficient evidence to recommend routine screening among general population. Children are vaccinated against chickenpox and most adults generally may have been infected with VZV in their early years. Screening is recommended for specific populations which include, healthcare workers, pregnant women, newborns, HIV/AIDS patients and for people prior to organ transplantation.
Screening
- According to Center for Disease Control and Prevention (CDC), there is insufficient evidence to recommend routine screening among general population.
- Children are vaccinated and most adults generally may have been infected with VZV in their early years. Hence, screening for general population is not recommended. Testing for VZV or for the antibodies produced in response to VZV infection may be performed when required.
Screening Varicella in specific populations
- Screening tests are recommended for people without symptoms, who are at higher risk of acquiring chickenpox. The specific groups in which screening for chickenpox is recommended include:[1]
- Healthcare workers
- Pregnant women
- Newborns
- HIV/AIDS patients
- Potential organ transplant recepients
- Blood tests are done to measure the levels of antibodies in the blood, which indicates whether the individual has developed an immunity to chickenpox from previous infection or a missed immunization.
- Testing for VZV or for the antibodies produced in response to VZV infection may be performed for screening purposes. Also, screening may be advised for newborns, pregnant women, prior to organ transplantation, and in those with HIV/AIDS.
Antenatal screening
- Routine antenatal varicella screening of all pregnant women with negative or indeterminate varicella histories is not cost-effective. It could be cost-effective in groups of women with increased exposure risk.[3]
Screening in Healthcare Workers
- A study shows that 26% to 55% of healthcare workers with no history of chickenpox and who test negative for antibody against varicella require vaccination. Hence, in healthcare facilities, varicella screening and vaccination should be offered to all healthcare workers.[4]
References
- ↑ “Chickenpox and Shingles Tests: The Test”.
- ↑ “Prevention of Varicella: Recommendations of the Advisory Committee on Immunization Practices (ACIP)”.
- ↑ Glantz JC, Mushlin AI (1998). “Cost-effectiveness of routine antenatal varicella screening”. Obstet Gynecol. 91 (4): 519–28. PMID 9540934.
- ↑ Chong CY, Lim SH, Ng WY, Tee N, Lin RV (2004). “Varicella screening and vaccination for healthcare workers at KK Women’s and Children’s Hospital”. Ann. Acad. Med. Singap. 33 (2): 243–7. PMID 15098642.
Natural History, Complications and Prognosis
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1] Associate Editor(s)-in-Chief: Aravind Reddy Kothagadi M.B.B.S[2]
Overview
Primary varicella presents with pruritic macules, papules, vesicles, pustules, and crusts, usually on the back, chest, face, and abdomen. Reactivation of the virus can present as shingles. Common complications of chickenpox are bacterial infections of the skin and soft tissues in children and pneumonia in adults. Chickenpox is rarely fatal. Pregnant women and immunocompromised patients are at a higher risk of developing varicella pneumonia.
Natural History
If left untreated, in healthy children varicella manifestations develop within 15 days post exposure and typically present as: [1]
- Generalized vesicular rash develops within 24 hours
- Fever
- Malaise
- Pharyngitis
- Loss of appetite
Complications
The disease is usually mild, although serious complications sometimes occur. Two of the most common complications are bacterial infections of the skin and soft tissues in children and pneumonia in adults.[2][3][1]
Complications in Immunocompetent
Common complications associated with chickenpox in immunocompetent individuals include:[2][4][5][3][6][7]
- Toxic shock syndrome
- Viral pneumonia
- Zoster paresis
- Post-herpetic neuralgia)
- VZV meningoencephalitis
- VZV vasculopathy
- VZV and giant cell arteritis
- VZV-induced stromal keratitis
- Necrotizing fasciitis
- Septicemia
- Osteomyelitis
- Bacterial pneumonia
- Cerebellar ataxia
- Encephalitis
- Hemorrhagic conditions
- Septic arthritis
Complications in Immunocompromised
Common complications associated with chickenpox in immunosupressed individuals include:
- Hemorrhagic complications
- Febrile purpura
- Malignant chickenpox with purpura (mortality rate of greater than 70%)
- Anaphylactoid purpura
Prognosis
- Chickenpox is rarely fatal except if the patient develops varicella pneumonia.
- Prognosis in the immunocompromised is poor.
- Varicella zoster virus remains dormant in nerves which can be reactivated later in life, resulting in shingles. It is most commonly seen in the immunocompromised and the elderly.
References
- ↑ 1.0 1.1 Straus SE, Ostrove JM, Inchauspé G, Felser JM, Freifeld A, Croen KD; et al. (1988). “NIH conference. Varicella-zoster virus infections. Biology, natural history, treatment, and prevention”. Ann Intern Med. 108 (2): 221–37. PMID 2829675.
- ↑ 2.0 2.1 Gnann JW (2002). “Varicella-zoster virus: atypical presentations and unusual complications”. J Infect Dis. 186 Suppl 1: S91–8. doi:10.1086/342963. PMID 12353193.
- ↑ 3.0 3.1 Marin M, Watson TL, Chaves SS, Civen R, Watson BM, Zhang JX; et al. (2008). “Varicella among adults: data from an active surveillance project, 1995-2005”. J Infect Dis. 197 Suppl 2: S94–S100. doi:10.1086/522155. PMID 18419417.
- ↑ Laupland KB, Davies HD, Low DE, Schwartz B, Green K, McGeer A (2000). “Invasive group A streptococcal disease in children and association with varicella-zoster virus infection. Ontario Group A Streptococcal Study Group”. Pediatrics. 105 (5): E60. PMID 10799624.
- ↑ de Benedictis FM, Osimani P (2008). “Necrotising fasciitis complicating varicella”. Arch Dis Child. 93 (7): 619. doi:10.1136/adc.2008.141994. PMID 18567772.
- ↑ Gershon AA, Breuer J, Cohen JI, Cohrs RJ, Gershon MD, Gilden D; et al. (2015). “Varicella zoster virus infection”. Nat Rev Dis Primers. 1: 15016. doi:10.1038/nrdp.2015.16. PMC 5381807. PMID 27188665.
- ↑ Clark P, Davidson D, Letts M, Lawton L, Jawadi A (2003). “Necrotizing fasciitis secondary to chickenpox infection in children”. Can J Surg. 46 (1): 9–14. PMC 3211661. PMID 12585787.
Diagnosis
Diagnosis
History and Symptoms | Physical Examination | Laboratory Findings | Chest X Ray | Other Diagnostic Studies
Treatment
Treatment
Medical Therapy | Primary Prevention | Secondary Prevention | Cost-Effectiveness of Therapy | Future or Investigational Therapies
Looking for the patient version?
© 2026 MyEClinic – IFTM Institut für Telematik in der Medizin GmbH