
Myxoma
For patient information click here
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Sogand Goudarzi, MD [2] Maria Fernanda Villarreal, M.D. [3]Cafer Zorkun, M.D., Ph.D. [4] Ahmad Al Maradni, M.D. [5]
Synonyms and keywords:Atrial myxoma; Intracardiac myxoma; Cardiac myxoma; Myxoma of the heart; Heart myxoma; Left atrial myxoma; Right atrial myxoma
Overview
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Sogand Goudarzi, MD [2]Maria Fernanda Villarreal, M.D. [3]Cafer Zorkun, M.D., Ph.D. [4]Ahmad Al Maradni, M.D. [5]
Overview
A myxoma (Myxo- = Latin for mucus) is the most common primary tumor of the heart. Cardiac myxoma was first described in 1845. In 1951, Prichard described a kind of microscopic endocardial structure of the atrial septum, which was suggested to be associated with cardiac myxoma. Clarence Crafoord, a Swedish cardiovascular surgeon successfully removed a cardiac myxoma for the first time in 1954. Before 1951, cardiac myxoma diagnosis was made only at post-mortem examination. In 1959, the first M-mode echocardiogram of a left atrial myxoma was reported. Cardiac myxomas are classified by the WHO histological classification of tumors of the heart “Benign tumors and tumor-like lesions” and categorized into a type of pluripotent mesenchymal tumor. Cardiac myxoma arises from remnants of subendocardial vasoformative reserve cells, which are primitive mesenchymal cells that are normally involved in the supportive structure of the endocardium. Myxomas are usually located in the fossa ovalis and endocardium of the atrial septum. Some symptoms of myxoma may be associated with the release of interleukin 6 (IL-6). On gross pathology, a gelatinous, irregular surface that fills the left atrium is the characteristic finding of myxoma. A common histopathological finding is the Gamna-Gandy Bodies that consist of fibrosis and deposition of iron pigments. The main cause of cardiac myxoma remains unknown. However, in some cases like inherited myxomatosis, there is a strong relation with genetic mutations of PRKAR1A gene. Cardiac myxoma should be differentiated from other benign and malignant primary heart tumors including papillary fibroelastoma, lipoma, rhabdomyoma, and cardiac metastasis. Cardiac myxomas are the most common primary cardiac tumor in adults, with a reported prevalence of 0.03% in general population. The incidence of cardiac myxoma is about 1/ 100,000 per year. The majority of patients with cardiac myxoma are diagnosed between 30 to 60 years; children are rarely affected. Females are more commonly affected with cardiac myxoma than men. The female-to-male ratio is approximately 1.8 to 1. Cardiac myxomas represent 78% of heart tumors. Common risk factors in the development of myxoma are female gender and genetic predisposition. In some cases, right atrial myxoma has been associated with tricuspid stenosis and atrial fibrillation. If left untreated, cardiac myxoma progression occurs slowly. The overlap of various phenomena such as thrombosis, hemorrhage, or fragmentation may influence tumor growth, detachment, and consequently embolism. Constitutional symptoms, such as: weight loss, fatigue, weakness are often the initial clinical onset of cardiac myxoma, and may resemble those from endocarditis. Metastases are uncommon in cardiac myxoma. Since the majority of the cardiac myxomas are left-sided, it may progress to develop mitral valve obstruction or systemic embolic events, such as stroke. Whereas, right atrial myxomas may obstruct the tricuspid valve and can present as right sided heart failure. Approximately 20% of patients with cardiac myxoma are asymptomatic. Overall, clinical features of cardiac myxoma are associated with the size of the tumor, location, size, and mobility. There is no single diagnostic study of choice for myxoma. Myxoma may be diagnosed based on clinical presentation and detecting the cardiac mass. Symptoms associated with cardiac myxomas are typically due to the effect of the mass of the tumor obstructing the normal blood flow within the heart chambers. Left atrial myxoma symptoms may mimic mitral stenosis, while right atrial myxomas rarely produce symptoms until they have grown to be at least 13 cm wide. General symptoms may also mimic those of infective endocarditis. Cardiac myxoma symptoms may occur at any time, but most often they tend to occur with changes in body position. Common symptoms include: chest pain, palpitation, dizziness, syncope and dyspnea on exertion. There are no specific physical findings for cardiac myxoma. The auscultatory presence of a “tumor plop” (which is caused by the obstruction of the mitral valve orifice by the tumor) on physical examination is highly suggestive of cardiac myxoma. Common physical examination findings of cardiac myxoma include systolic or diastolic murmurs (depending on size, mobility, and location of the tumor). Laboratory findings consistent with cardiac myxoma are generally non-specific, results often demonstrate anemia, leukocytosis and elevated erythrocyte sedimentation rate. On chest x-ray, cardiac myxoma is characterized by normal results and in some cases a calcification overlying the heart. On CT scan, cardiac myxoma is characterized by low attenuation and areas of dystrophic calcification in cardiac chambers. CT scan may be helpful in the diagnosis of cardiac myxoma because it provides better soft-tissue contrast than echocardiography, and it can also differentiate calcification and fat, and may allow tissue diagnosis of some masses such as lipomas. On Magnetic Resonance Imaging (MRI) or Cardiac Magnetic Resonance (CMR), cardiac myxoma is characterized by a soft tissue mass within the cardiac chambers isointense to skeletal muscle. This imaging modality plays an important role in the evaluation of cardiac masses and is of great value when echocardiographic findings are suboptimal or when the lesion has an atypical location or appearance. The echocardiogram is the initial modality and most useful diagnostic imaging study in cardiac myxoma. On cardiac ultrasound, cardiac myxoma is characterized by the presence of a heterogeneous pedunculated mass that is commonly located in the left atrium. Echocardiography allows for evaluation assessment of tumor mobility, as it often protrudes through valve flaps. As a testing modality, two-dimensional echocardiography is often coupled with other modalities (such as, Doppler echocardiography) to detect vascular abnormalities that frequently occur in cardiac myxomas. Another diagnostic study for cardiac myxoma is cardiac angiography, which often demonstrates contrast media-enhanced tumor vasculature. There is no known medical therapy for cardiac myxomas. Surgery is the mainstay of treatment for cardiac myxoma. The feasibility of surgery depends on the patient hemodynamic stability at diagnosis. Cardiac myxoma surgery has operative mortality around 0 to 3%, depending on risk factors or mechanical damage to a heart valve, as well as adhesion of the tumor to valve leaflets. The short and long-term prognosis is generally regarded as excellent.
Historical Perspective
Cardiac myxoma was first described in 1845. In 1951, Prichard described a kind of microscopic endocardial structure of the atrial septum, which was suggested to be associated with cardiac myxoma. Clarence Crafoord, a Swedish cardiovascular surgeon successfully removed a cardiac myxoma for the first time in 1954. Before 1951, cardiac myxoma diagnosis was made only at post-mortem examination. In 1959, the first M-mode echocardiogram of a left atrial myxoma was reported.
Classification
Cardiac myxomas are classified by the WHO histological classification of tumors of the heart “Benign tumors and tumor-like lesions” and categorized into a type of pluripotent mesenchymal tumor.
Pathophysiology
Cardiac myxoma arises from remnants of subendocardial vasoformative reserve cells, which are primitive mesenchymal cells that are normally involved in the supportive structure of the endocardium. Myxomas are usually located in the fossa ovalis and endocardium of the atrial septum
Some symptoms of myxoma may be associated with the release of interleukin 6 (IL-6). On gross pathology, a gelatinous, irregular surface that fills the left atrium is the characteristic finding of myxoma. A common histopathological finding is the Gamna-Gandy Bodies that consist of fibrosis and deposition of iron pigments.
Causes
The main cause of cardiac myxoma remains unknown. However, in some cases like inherited myxomatosis, there is a strong relation with genetic mutations of PRKAR1A gene.
Differentiating Myxoma from other Diseases
Cardiac myxoma should be differentiated from other benign and malignant primary heart tumors including papillary fibroelastoma, lipoma, rhabdomyoma, and cardiac metastasis.
Epidemiology and Demographics
Cardiac myxomas are the most common primary cardiac tumor in adults, with a reported prevalence of 0.03% in general population. The incidence of cardiac myxoma is about 1/ 100,000 per year. The majority of patients with cardiac myxoma are diagnosed between 30 to 60 years; children are rarely affected. Females are more commonly affected with cardiac myxoma than men. The female-to-male ratio is approximately 1.8 to 1. Cardiac myxomas represent 78% of heart tumors.
Risk Factors
Common risk factors in the development of myxoma are female gender and genetic predisposition. In some cases, right atrial myxoma has been associated with tricuspid stenosis and atrial fibrillation.
Natural History, Complications and Prognosis
If left untreated, cardiac myxoma progression occurs slowly. The overlap of various phenomena such as thrombosis, hemorrhage, or fragmentation may influence tumor growth, detachment, and consequently embolism. Constitutional symptoms, such as: weight loss, fatigue, weakness are often the initial clinical onset of cardiac myxoma, and may resemble those from endocarditis. Metastases are uncommon in cardiac myxoma.
Since the majority of the cardiac myxomas are left-sided, it may progress to develop mitral valve obstruction or systemic embolic events, such as stroke. Whereas, right atrial myxomas may obstruct the tricuspid valve and can present as right sided heart failure. Approximately 20% of patients with cardiac myxoma are asymptomatic. Overall, clinical features of cardiac myxoma are associated with the size of the tumor, location, size, and mobility.
Diagnosis
Diagnostic Study of Choice
There is no single diagnostic study of choice for myxoma. Myxoma may be diagnosed based on clinical presentation and detecting the cardiac mass.
History and Symptoms
Symptoms associated with cardiac myxomas are typically due to the effect of the mass of the tumor obstructing the normal blood flow within the heart chambers. Left atrial myxoma symptoms may mimic mitral stenosis, while right atrial myxomas rarely produce symptoms until they have grown to be at least 13 cm wide. General symptoms may also mimic those of infective endocarditis. Cardiac myxoma symptoms may occur at any time, but most often they tend to occur with changes in body position. Common symptoms include: chest pain, palpitation, dizziness, syncope and dyspnea on exertion.
Physical Examination
There are no specific physical findings for cardiac myxoma. The auscultatory presence of a “tumor plop” (which is caused by the obstruction of the mitral valve orifice by the tumor) on physical examination is highly suggestive of cardiac myxoma. Common physical examination findings of cardiac myxoma include systolic or diastolic murmurs (depending on size, mobility, and location of the tumor).
Laboratory Findings
Laboratory findings consistent with cardiac myxoma are generally non-specific, results often demonstrate anemia, leukocytosis and elevated erythrocyte sedimentation rate.
Chest X-ray
On chest x-ray, cardiac myxoma is characterized by normal results and in some cases a calcification overlying the heart.
CT Scan
On CT scan, cardiac myxoma is characterized by low attenuation and areas of dystrophic calcification in cardiac chambers. CT scan may be helpful in the diagnosis of cardiac myxoma because it provides better soft-tissue contrast than echocardiography, and it can also differentiate calcification and fat, and may allow tissue diagnosis of some masses such as lipomas.
MRI
On Magnetic Resonance Imaging (MRI) or Cardiac Magnetic Resonance (CMR), cardiac myxoma is characterized by a soft tissue mass within the cardiac chambers isointense to skeletal muscle. This imaging modality plays an important role in the evaluation of cardiac masses and is of great value when echocardiographic findings are suboptimal or when the lesion has an atypical location or appearance.
Echocardiography
The echocardiogram is the initial modality and most useful diagnostic imaging study in cardiac myxoma. On cardiac ultrasound, cardiac myxoma is characterized by the presence of a heterogeneous pedunculated mass that is commonly located in the left atrium. Echocardiography allows for evaluation assessment of tumor mobility, as it often protrudes through valve flaps. As a testing modality, two-dimensional echocardiography is often coupled with other modalities (such as, Doppler echocardiography) to detect vascular abnormalities that frequently occur in cardiac myxomas.
Other Diagnostic Studies
Another diagnostic study for cardiac myxoma is cardiac angiography, which often demonstrates contrast media-enhanced tumor vasculature.
Treatment
Medical Therapy
There is no known medical therapy for cardiac myxomas.
Surgery
Surgery is the mainstay of treatment for cardiac myxoma. The feasibility of surgery depends on the patient hemodynamic stability at diagnosis. Cardiac myxoma surgery has operative mortality around 0 to 3%, depending on risk factors or mechanical damage to a heart valve, as well as adhesion of the tumor to valve leaflets. The short and long-term prognosis is generally regarded as excellent.
References
Historical Perspective
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]Associate Editor(s)-in-Chief: Sogand Goudarzi, MD [2] Maria Fernanda Villarreal, M.D. [3]
Overview
Cardiac myxoma was first described in 1845. In 1951, Prichard described a kind of microscopic endocardial structure of the atrial septum, which was suggested to be associated with cardiac myxoma. Clarence Crafoord, a Swedish cardiovascular surgeon successfully removed a cardiac myxoma for the first time in 1954. Before 1951, cardiac myxoma diagnosis was made only at post-mortem examination.
Historical perspective
- In 1951, Prichard described a kind of microscopic endocardial structure of the atrial septum, which was suggested to be related to cardiac myxoma.[2]
- In 1951, intracardiac myxoma was recognized by angiography for the first time. Before 1951, cardiac myxoma diagnosis was made only at autopsy.[3]
- In 1959, the first M-mode echocardiogram was used to diagnose a left atrial myxoma.[4]
- In 2000, gene mutation PRKAR1A was first identified in the pathogenesis of cardiac myxoma syndromes, such as; LAMB (lentigines, atrial myxoma, mucocutaneous myxomas and blue nevi), NAME (nevi, atrial myxoma, mucinosis of the skin, and endocrine overactivity), and Carney complex (myxomas, spotty skin pigmentation and endocrine overactivity).[5][6].
Landmark Events in the Development of Treatment Strategies
- In 1954, Clarence Crafoord (1899 – 1984), a Swedish cardiovascular surgeon, successfully removed a cardiac myxoma for the first time. This case also represents the first extirpation of a cardiac tumor on cardiopulmonary support.[7][8]
References
- ↑ King TW. On simple vascular growths in the left auricle of the heart. Lancet 1845; 2:428-9
- ↑ Amano J, Kono T, Wada Y, Zhang T, Koide N, Fujimori M, Ito K (2003). “Cardiac myxoma: its origin and tumor characteristics”. Ann Thorac Cardiovasc Surg. 9 (4): 215–21. PMID 13129418.
- ↑ Guhathakurta S, Riordan JP (2000). “Surgical treatment of right atrial myxoma”. Tex Heart Inst J. 27 (1): 61–3. PMC 101023. PMID 10830633.
- ↑ Pinede L, Duhaut P, Loire R (2001). “Clinical presentation of left atrial cardiac myxoma. A series of 112 consecutive cases”. Medicine (Baltimore). 80 (3): 159–72. PMID 11388092.
- ↑ Carney JA, Hruska LS, Beauchamp GD, Gordon H (1986). “Dominant inheritance of the complex of myxomas, spotty pigmentation, and endocrine overactivity”. Mayo Clin. Proc. 61 (3): 165–72. PMID 3945116.
- ↑ Mabuchi T, Shimizu M, Ino H, Yamguchi M, Terai H, Fujino N, Nagata M, Sakata K, Inoue M, Yoneda T, Mabuchi H (2005). “PRKAR1A gene mutation in patients with cardiac myxoma”. Int. J. Cardiol. 102 (2): 273–7. doi:10.1016/j.ijcard.2004.05.053. PMID 15982496.
- ↑ Chitwood WR (1992). “Clarence Crafoord and the first successful resection of a cardiac myxoma”. Ann. Thorac. Surg. 54 (5): 997–8. PMID 1417305.
- ↑ Chitwood WR (November 1992). “Clarence Crafoord and the first successful resection of a cardiac myxoma”. Ann. Thorac. Surg. 54 (5): 997–8. doi:10.1016/0003-4975(92)90676-u. PMID 1417305.
Classification
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1] Associate Editor(s)-in-Chief: Sogand Goudarzi, MD [2] Maria Fernanda Villarreal, M.D. [3]
Overview
Cardiac myxomas are classified by the World Health Organization (WHO) histological classification of tumors of the heart, as “Benign tumors and tumor-like lesions” and categorized into a type of pluripotent mesenchymal tumor.
Classification
- Based on the location and biological behavior of symptoms, cardiac myxomas may be classified into two groups: typical and atypical.[1]
- Typical:
- atypical.
- In atypical cases, presentation is usually early and multicentricity is more common. They are more frequently located on the right side of the heart (38%), or in the left ventricle (5%). There is also recurrence after surgical excision (12%–22%) and an association with other conditions, such as the Carney complex.[2]
- Cardiac myxomas are anatomically distributed, as following:[2]
- Atria (95%)
- Left (75%)
- Right (20%)
- Ventricles (5%)
- Atria (95%)
- There is no established histological differentiation between both type of cardiac myxomas (typical and atypical).[5]
References
- ↑ Nina, Vinícius JS; Silva, Nathalia AC; Gaspar, Shirlyne FD; Rapôso, Thaísa L; Ferreira, Eduardo C; Nina, Rachel VAH; Lages, Joyce S; Silva, Fernando ACC; Filho, Natalino Salgado (2012). “Atypical size and location of a right atrial myxoma: a case report”. Journal of Medical Case Reports. 6 (1). doi:10.1186/1752-1947-6-26. ISSN 1752-1947.
- ↑ 2.0 2.1 2.2 Grebenc ML, Rosado de Christenson ML, Burke AP, Green CE, Galvin JR (2000). “Primary cardiac and pericardial neoplasms: radiologic-pathologic correlation”. Radiographics. 20 (4): 1073–103, quiz 1110–1, 1112. doi:10.1148/radiographics.20.4.g00jl081073. PMID 10903697.
- ↑ Amano J, Nakayama J, Yoshimura Y, Ikeda U (2013). “Clinical classification of cardiovascular tumors and tumor-like lesions, and its incidences”. Gen Thorac Cardiovasc Surg. 61 (8): 435–47. doi:10.1007/s11748-013-0214-8. PMC 3732772. PMID 23460447.
- ↑ Wold LE, Lie JT (1980). “Cardiac myxomas: a clinicopathologic profile”. Am. J. Pathol. 101 (1): 219–40. PMC 1903582. PMID 7446701.
- ↑ McCarthy PM, Piehler JM, Schaff HV, Pluth JR, Orszulak TA, Vidaillet HJ, Carney JA (1986). “The significance of multiple, recurrent, and “complex” cardiac myxomas”. J. Thorac. Cardiovasc. Surg. 91 (3): 389–96. PMID 3951243.
Pathophysiology
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1] Associate Editor(s)-in-Chief: Sogand Goudarzi, MD [2] Maria Fernanda Villarreal, M.D. [3]Cafer Zorkun, M.D., Ph.D. [4]Ahmad Al Maradni, M.D. [5]
Overview
Cardiac myxoma is a benign intracavitary endocardial mass that represents the most common primary tumor of the heart. Myxoma cells are characterized by undifferentiated mesenchymal cells, which potentially differentiate into many tissues such as blood vessels, glandular structures, and bones. The primary distribution of cardiac myxoma is the left atrium (75%) of the heart; regularly, they tend to be located in the fossa ovalis and endocardium of the atrial septum.
Pathogenesis
Pathogenesis
- Cardiac myxoma arises from remnants of subendocardial vasoformative reserve cells, which are primitive mesenchymal cells that are normally involved in the supportive structure of the endocardium.[1][2][3][4][5]
- The exact pathogenesis of cardiac myxoma is not fully understood.[5]
- It is thought that cardiac myxoma is produced by the neoplastic theory, dysembryoplastic theory, histopathogenesis of glandular cells in myxoma or the thrombotic theory.[6][7]
- The site of tumor attachment, normally the foramen ovale, is considered to be consistent with an origin from multipotent mesenchymal cells or from embryonic rests.[8]
Genetics
- Sporadic cardiac myxomas and familial forms are related with several chromosome and gene alterations which involve cardiac development.[9]
- Inherited myxomas are usually present in Carney complex.[9]
- The development of Carney complex is a result of PRKAR1A gene inactivation mutation that is associated with chromosome 17q24.2-q24.3.[9]
- The gene 17q24.2-q24.3 plays an important role in cardiac development and myxomagenesis. The expression of PRKAR1A causes myxomatous changes in the endocardium.[9]
- The encoded protein of PRKAR1A is a type 1A regulatory subunit of protein kinase A.Inactivating germline mutations of this gene are found in 70% of people with Carney complex.[10]
- Less commonly, the molecular pathogenesis of Carney complex is a variety of genetic changes at chromosome 2p16.[11]
- Both types of Carney complex are autosomal dominant.
- Despite dissimilar genetics, there appears to be no phenotypic difference between PRKAR1A and chromosome 2p16 mutations.[12]
Associated Conditions
- The Carney complex is characterized by myxomatous neoplasms (cardiac, endocrine, cutaneous, and neural), and a host of pigmented lesions of the skin and mucosae, including the rarely occurring epitheloid blue nevus.[13][14][15]
- Approximately 7% of all cardiac myxomas are associated with Carney complex.[16]
Gross Pathology
- On gross pathology, external appearance, consistency size, and weight are extremely variable findings of cardiac myxoma.[17]
- Tumor consistency depends on the quantity and distribution of fibrous tissue and calcification (it can be smooth, lobulated, friable or gelatinous).
- Myxomas are usually described as having a gelatinous, irregular surface.
- Myxomas that have an irregular consistency are more likely to form surface thrombi and embolize.[18]
- Morphologically, these lesions tend to be attached to the endocardium by a broad-based pedunculated stalk.[8]
- In some cases, the attachment to the endocardium can also be without a clear stalk, or sessile.[8]
- Cardiac myxomas are non-invasive tumors, thus there is no infiltration to underlying tissues.[19]
- Cardiac myxomas are intracavitary tumors.
- The distribution is normally within the interatrial septum or adjacent to foramen ovale (75%).
- However, they can also be found in other cardiac chambers, such as right atrium (15%), ventricles (2%) or cardiac valves (rare).
- Large cardiac myxomas are usually located in fossa ovalis.[5]
- The size of the tumor varies from 0.6 to 12 cm, with a mean weight of 40 g.
- Images shown below are courtesy of Professor Peter Anderson DVM PhD and published with permission © PEIR, University of Alabama at Birmingham, Department of Pathology
-
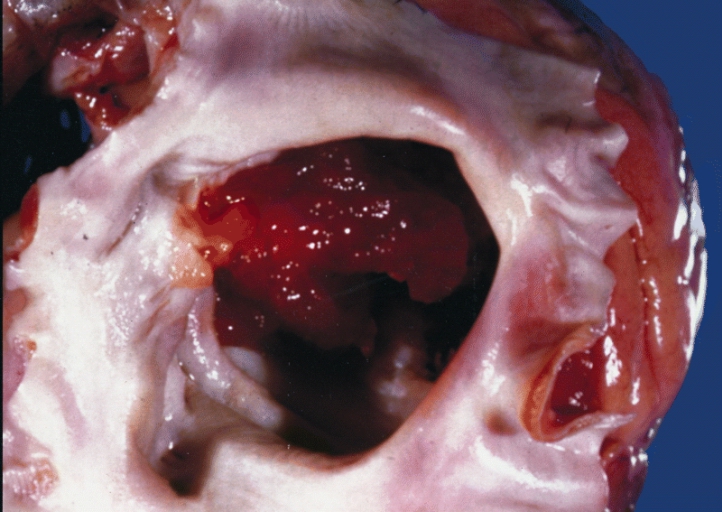 A gelatinous tumor is attached by a narrow pedicle to the atrial septum. The myxoma has an irregular surface and nearly fills the left atrium
A gelatinous tumor is attached by a narrow pedicle to the atrial septum. The myxoma has an irregular surface and nearly fills the left atrium -
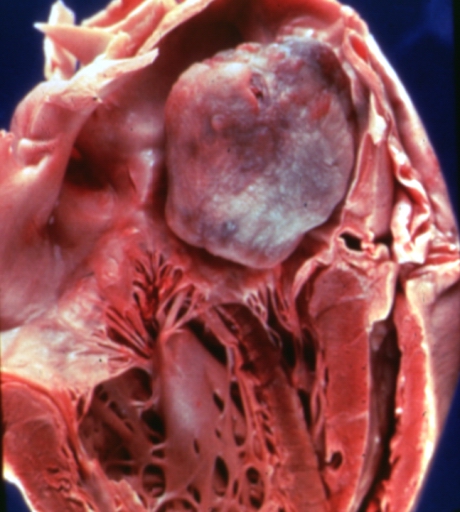 Left atrial myxoma
Left atrial myxoma -
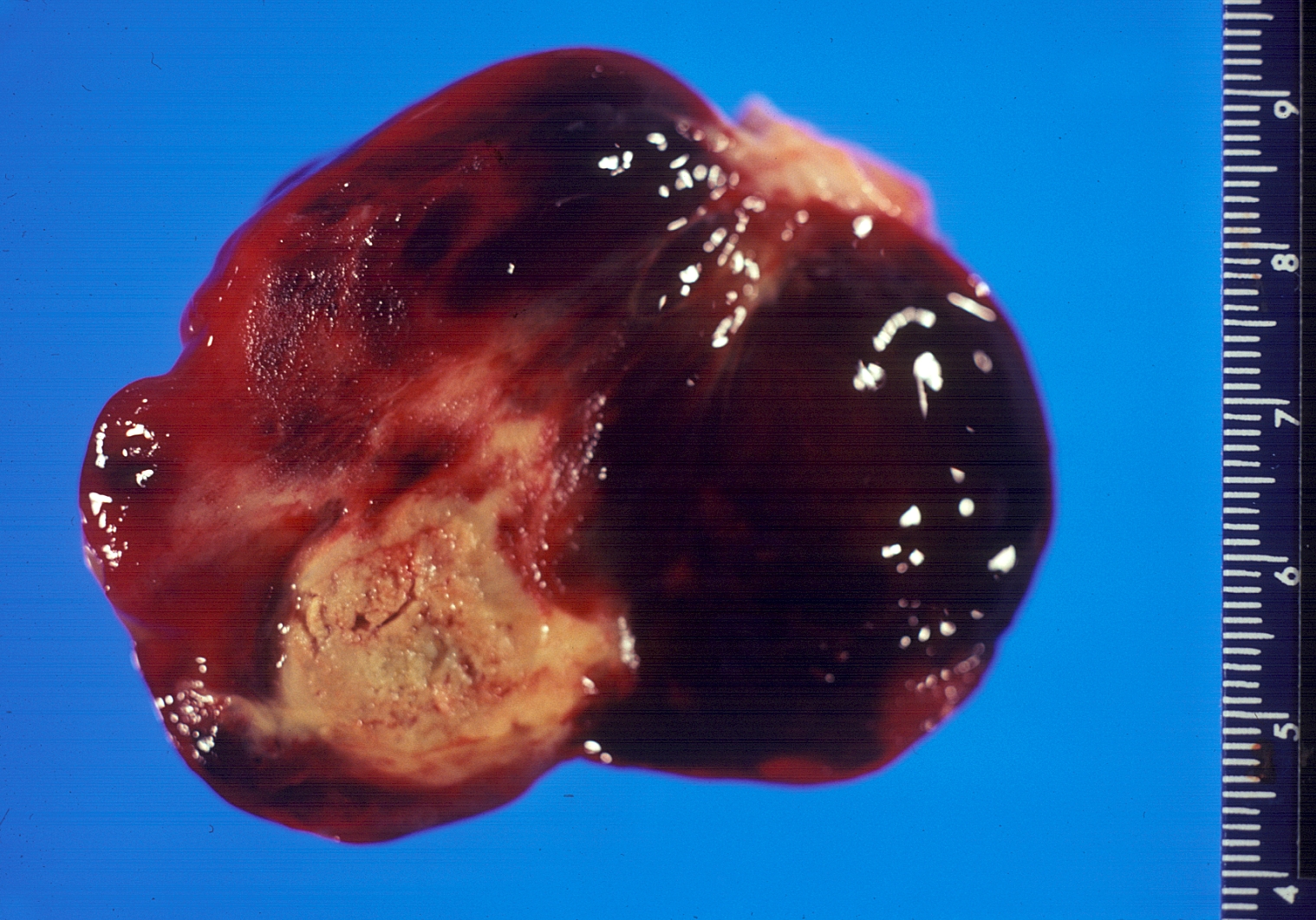 Gross pathology atrial myxoma: myxomas are brownish or white and are frequently covered with thrombus
Gross pathology atrial myxoma: myxomas are brownish or white and are frequently covered with thrombus



Microscopic Pathology
- On microscopic histopathological analysis, myxoma cells have an ovoid nucleus with large nucleoli, abundant eosinophilic cytoplasm, and indistinct cell borders.[20]
- They are usually arranged in perivascular ring structures (typically, infiltrated by lymphocytes and macrophages).[17]
- The Gamna-Bodies which consist of fibrosis and deposition of iron pigments are a characteristic finding of myxoma tumors.[17]
- Other frequent histological findings, are hemosiderin within the histiocytes, thrombosis, fibrosis and calcifications.[17]
- In some cases, extramedullary hematopoiesis is present and mucin-producing glands can be also seen in the base of the tumor.[17]
- The extracellular matrix forms an alcian blue-positive myxoid stroma, composed of variable amounts of proteoglycans, elastin and collagen.[17]
 |
 |
 |
 |
 |
Immunohistochemistry
- Cardiac myxoma cells exhibit immuno-reactivity mainly for calretinin (75–100%) followed by vimentin (>50%), NOTCH1, alpha-1 antichymotrypsin and plakophilin- 2.[21]
- Calretinin plays an important role in the discrimination of mural thrombi and papillary fibroelastoma.[21]
- Another immunohistochemical marker, survivin (an apoptosis inhibitor) has been detected to play an important role in the development and growth of cardiac myxomas.[22]
| Features | Description |
|---|---|
| General aspects | |
| Genetics | |
| Gross Pathology |
|
| Micropathology |
|
| Inmunohistochemistry |
|
References
- ↑ Bulkley BH, Hutchins GM (1979). “Atrial myxomas: a fifty year review”. Am. Heart J. 97 (5): 639–43. PMID 433739.
- ↑ Grebenc ML, Rosado de Christenson ML, Burke AP, Green CE, Galvin JR (2000). “Primary cardiac and pericardial neoplasms: radiologic-pathologic correlation”. Radiographics. 20 (4): 1073–103, quiz 1110–1, 1112. doi:10.1148/radiographics.20.4.g00jl081073. PMID 10903697.
- ↑ Roscher AA, Kato NS, Quan H, Padmanabhan M (1996). “Intra-atrial myxomas, clinical-pathologic correlation based on two case studies including historical review”. J Cardiovasc Surg (Torino). 37 (6 Suppl 1): 131–7. PMID 10064365.
- ↑ Acebo E, Val-Bernal JF, Gómez-Román JJ (2001). “Prichard’s structures of the fossa ovalis are not histogenetically related to cardiac myxoma”. Histopathology. 39 (5): 529–35. PMID 11737312.
- ↑ 5.0 5.1 5.2 Grebenc ML, Rosado de Christenson ML, Burke AP, Green CE, Galvin JR (2000). “Primary cardiac and pericardial neoplasms: radiologic-pathologic correlation”. Radiographics. 20 (4): 1073–103, quiz 1110–1, 1112. doi:10.1148/radiographics.20.4.g00jl081073. PMID 10903697.
- ↑ Orlandi A, Ciucci A, Ferlosio A, Genta R, Spagnoli LG, Gabbiani G (2006). “Cardiac myxoma cells exhibit embryonic endocardial stem cell features”. J. Pathol. 209 (2): 231–9. doi:10.1002/path.1959. PMID 16508920.
- ↑ Amano J, Kono T, Wada Y, Zhang T, Koide N, Fujimori M, Ito K (2003). “Cardiac myxoma: its origin and tumor characteristics”. Ann Thorac Cardiovasc Surg. 9 (4): 215–21. PMID 13129418.
- ↑ 8.0 8.1 8.2 Reynen K (1995). “Cardiac myxomas”. N. Engl. J. Med. 333 (24): 1610–7. doi:10.1056/NEJM199512143332407. PMID 7477198.
- ↑ 9.0 9.1 9.2 9.3 Sun Y, Chen X, Sun J, Wen X, Liu X, Zhang Y, Hoffman AR, Hu JF, Gao Y (2015). “A Novel Inherited Mutation in PRKAR1A Abrogates PreRNA Splicing in a Carney Complex Family”. Can J Cardiol. 31 (11): 1393–401. doi:10.1016/j.cjca.2015.05.018. PMID 26416542.
- ↑ Correa R, Salpea P, Stratakis CA (October 2015). “Carney complex: an update”. Eur. J. Endocrinol. 173 (4): M85–97. doi:10.1530/EJE-15-0209. PMC 4553126. PMID 26130139.
- ↑ Stratakis, Constantine A.; Kirschner, Lawrence S.; Carney, J. Aidan (2001). “Clinical and Molecular Features of the Carney Complex: Diagnostic Criteria and Recommendations for Patient Evaluation”. The Journal of Clinical Endocrinology & Metabolism. 86 (9): 4041–4046. doi:10.1210/jcem.86.9.7903. ISSN 0021-972X.
- ↑ Stratakis, Constantine A.; Kirschner, Lawrence S.; Carney, J. Aidan (2001). “Clinical and Molecular Features of the Carney Complex: Diagnostic Criteria and Recommendations for Patient Evaluation”. The Journal of Clinical Endocrinology & Metabolism. 86 (9): 4041–4046. doi:10.1210/jcem.86.9.7903. ISSN 0021-972X.
- ↑ Carney JA, Gordon H, Carpenter PC, Shenoy BV, Go VL. The complex of myxomas, spotty pigmentation, and endocrine overactivity. Medicine (Baltimore). 1985;64(4):270-83.
- ↑ Iglesias C, Torrelo A, Colmenero I, Mediero IG, Zambrano A, Requenca L. Isolated multiple congential epithelioid blue naevus. British Journal of Dermatology 2005;152:391-393.
- ↑ Gaissmaier et al. (letter and response) Carney Complex. Circulation 1999;100 (25); e150 http://circ.ahajournals.org/cgi/reprint/100/25/e150
- ↑ Reynen, K. (1995). “Cardiac Myxomas”. New England Journal of Medicine. 333 (24): 1610–1617. doi:10.1056/NEJM199512143332407. PMID 7477198.
- ↑ 17.0 17.1 17.2 17.3 17.4 17.5 Di Vito A, Mignogna C, Donato G (2015). “The mysterious pathways of cardiac myxomas: a review of histogenesis, pathogenesis and pathology”. Histopathology. 66 (3): 321–32. doi:10.1111/his.12531. PMID 25297937.
- ↑ He DK, Zhang YF, Liang Y, Ye SX, Wang C, Kang B; et al. (2015). “Risk factors for embolism in cardiac myxoma: a retrospective analysis”. Med Sci Monit. 21: 1146–54. doi:10.12659/MSM.893855. PMC 4418206. PMID 25900256.
- ↑ Yoon DH, Roberts W (2002). “Sex distribution in cardiac myxomas”. Am. J. Cardiol. 90 (5): 563–5. PMID 12208428.
- ↑ Vaideeswar P, Butany JW (2008). “Benign cardiac tumors of the pluripotent mesenchyme”. Semin Diagn Pathol. 25 (1): 20–8. PMID 18350919.
- ↑ 21.0 21.1 Acebo E, Val-Bernal JF, Gómez-Roman JJ (2001). “Thrombomodulin, calretinin and c-kit (CD117) expression in cardiac myxoma”. Histol. Histopathol. 16 (4): 1031–6. PMID 11642722.
- ↑ Lin YS, Jung SM, Wu HH, Shiu TF, Tzai FC, Chu JJ, Lin PJ, Chu PH (2011). “Survivin expression in cardiac myxoma”. Chang Gung Med J. 34 (4): 360–6. PMID 21880190.
Causes
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1];Associate Editor(s)-in-Chief: Sogand Goudarzi, MD [2] Maria Fernanda Villarreal, M.D. [3]
Overview
The cause of cardiac myxoma has not been identifie. However, in some cases like inherited myxomatosis there is a strong relation with genetic mutations of PRKAR1A gene.
Disease name] may be caused by [cause1], [cause2], or [cause3].
OR
Common causes of [disease] include [cause1], [cause2], and [cause3].
OR
The most common cause of [disease name] is [cause 1]. Less common causes of [disease name] include [cause 2], [cause 3], and [cause 4].
OR
The cause of [disease name] has not been identified. To review risk factors for the development of [disease name], click here.
Causes
Life-threatening Causes
- Life-threatening causes include conditions which may result in death or permanent disability within 24 hours if left untreated. There are no life-threatening causes of disease name, however complications resulting from untreated disease name is common.
- Life-threatening causes of [symptom/manifestation] include [cause1], [cause2], and [cause3].[1]
- [Cause] is a life-threatening cause of [disease].
Common Causes
Common causes of [disease name] may include:[2]
- [Cause1]
- [Cause2]
- [Cause3]
OR
- [Disease name] is caused by an infection with [pathogen name].
- [Pathogen name] is caused by [pathogen name].
Less Common Causes
Less common causes of [disease name] include:
- [Cause1]
- [Cause2]
- [Cause3]
Genetic Causes
- [Disease name] is caused by a mutation in the [gene name] gene.
Causes by Organ System
| Cardiovascular | No underlying causes |
| Chemical/Poisoning | No underlying causes |
| Dental | No underlying causes |
| Dermatologic | No underlying causes |
| Drug Side Effect | No underlying causes |
| Ear Nose Throat | No underlying causes |
| Endocrine | No underlying causes |
| Environmental | No underlying causes |
| Gastroenterologic | No underlying causes |
| Genetic | No underlying causes |
| Hematologic | No underlying causes |
| Iatrogenic | No underlying causes |
| Infectious Disease | No underlying causes |
| Musculoskeletal/Orthopedic | No underlying causes |
| Neurologic | No underlying causes |
| Nutritional/Metabolic | No underlying causes |
| Obstetric/Gynecologic | No underlying causes |
| Oncologic | No underlying causes |
| Ophthalmologic | No underlying causes |
| Overdose/Toxicity | No underlying causes |
| Psychiatric | No underlying causes |
| Pulmonary | No underlying causes |
| Renal/Electrolyte | No underlying causes |
| Rheumatology/Immunology/Allergy | No underlying causes |
| Sexual | No underlying causes |
| Trauma | No underlying causes |
| Urologic | No underlying causes |
| Miscellaneous | No underlying causes |
Causes in Alphabetical Order
List the causes of the disease in alphabetical order:
- Cause 1
- Cause 2
- Cause 3
- Cause 4
- Cause 5
- Cause 6
- Cause 7
- Cause 8
- Cause 9
- Cause 10
Causes
- There are no established causes for cardiac myxoma.[3][4][5][6]
- About 10% of cardiac myxomas are familial.
- Inherited myxomatosis is caused by a mutation in the PRKAR1A gene.
References
- ↑ Wells, Samuel A.; Pacini, Furio; Robinson, Bruce G.; Santoro, Massimo (2013). “Multiple Endocrine Neoplasia Type 2 and Familial Medullary Thyroid Carcinoma: An Update”. The Journal of Clinical Endocrinology & Metabolism. 98 (8): 3149–3164. doi:10.1210/jc.2013-1204. ISSN 0021-972X.
- ↑ SULLIVAN AW, HAND JR (September 1958). “Seminoma of the testis following mumps orchitis with atrophy; report of a case”. Portland Clin Bull. 12 (2): 17–26. PMID 13578776.
- ↑ Messina F, Romano P, Crosca S (2015). “Atrial myxomas and different clinical presentations”. Int. J. Cardiol. doi:10.1016/j.ijcard.2015.08.063. PMID 26442965.
- ↑ Amano J, Kono T, Wada Y, Zhang T, Koide N, Fujimori M, Ito K (2003). “Cardiac myxoma: its origin and tumor characteristics”. Ann Thorac Cardiovasc Surg. 9 (4): 215–21. PMID 13129418.
- ↑ Amano J, Kono T, Wada Y, Zhang T, Koide N, Fujimori M, Ito K (August 2003). “Cardiac myxoma: its origin and tumor characteristics”. Ann Thorac Cardiovasc Surg. 9 (4): 215–21. PMID 13129418.
- ↑ Messina, F.; Romano, P.; Crosca, S. (2016). “Atrial myxomas and different clinical presentations”. International Journal of Cardiology. 203: 1136–1137. doi:10.1016/j.ijcard.2015.08.063. ISSN 0167-5273.
Differentiating Myxoma from other Diseases
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Syed Hassan A. Kazmi BSc, MD [2]Cafer Zorkun, M.D., Ph.D. [3] Ahmad Al Maradni, M.D. [4] Maria Fernanda Villarreal, M.D. [5]
Overview
Cardiac myxoma should be differentiated from other benign and malignant primary heart tumors including papillary fibroelastoma, lipoma, rhabdomyoma, and cardiac metastasis. Primarily, cardiac myxoma should be differentiated from other diseases that cause mitral valve obstruction and embolic events, such as thrombi or endocarditis.
Differentiating Myxoma from other Diseases
Cardiac myxoma should be differentiated from other cardiac tumors that present as a cardiac mass. The following are the differentials:[1][2][3][4][5][6][7][8][9][10][11][12][13][14][15][16][17][18][19][20][21][22][23][24][25][26][27][28][29][30][31][32][33][34][35][36][37][38][39][40][41][42][43][44][45][46][47][48]
| Site of Tumor | Malignant Potential | Type of Tumor | Tissue of Origin | Age of Presentation | Location | Morphology | Signs and Symptoms | MRI Findings | ||
|---|---|---|---|---|---|---|---|---|---|---|
| Systemic Manifestations | Cardiac Manifestations | Embolic Manifestations | ||||||||
| Primary Cardiac Tumor | Primary Benign | Myxoma |
|
|
|
|
|
| ||
| Rhabdomyoma |
|
|
|
|
| |||||
| Fibroma |
|
|
|
| ||||||
| Fibroelastoma |
|
|
|
|
| |||||
| Hemangioma |
|
|
|
|
| |||||
| Lipoma |
|
|
|
|
| |||||
| Paraganglioma |
|
|
|
|
|
|
|
| ||
| Atrioventricular Node Tumor |
|
|
|
|
|
| ||||
| Lipomatous hypertrophy of the interatrial septum |
|
|
|
|
– |
| ||||
| Primary Malignant | Fibrosarcoma |
|
|
|
|
|
| |||
| Angiosarcoma |
|
|
|
| ||||||
| Rhabdomyosarcoma |
|
|
|
| ||||||
| Lymphoma |
|
|
|
|
| |||||
| Secondary Cardiac Tumor | Metastastatic Malignant | Metastasis |
|
|
|
|
| |||
- Differential diagnosis of intracardiac masses requires histological analysis and a direct assessment of the specific location (endocardial, myocardial, and pericardial). The table below summarizes the findings that differentiate cardiac myxoma from other conditions that are also intracavitary cardiac masses and cause embolic events:
| Disease | Findings |
|---|---|
| Papillary fibroelastoma | Is a rare benign primary tumor of the heart that typically involves one of the valves of the heart. Presents with syncope, chest pain, myocardial infarction, stroke and sudden cardiac death. They are the third most common type of primary tumor of the heart. There is a slightly increased male predilection.[49][50] |
| Lipoma | Also known as “Lipomatous hypertrophy (LHIS)” is a very rare benign primary cardiac neoplasm. It is the proliferation of mature adipocytes. Lipomas are typically found in adult patients but can affect all ages. A common clinical feature is arrythmias.[51] |
| Rhabdomyoma | Is the most common primary cardiac tumor in children. It is conformed from hamartomatous accumulation of the striated cardiomyocytes. Rhabdomyomas occur with more frequency in the myocardium of the left ventricle or in the interventricular septum. Is commonly associated with tuberous sclerosis, and congenital defects of the heart.[52] |
| Thrombus | Intracardiac thrombi, can occur when there is an elevated risk of blood clots developing, such as: atrial fibrillation (atrial thrombi predominate), mitral stenosis, heart valve replacement and myocardial infarction (ventricular thrombus formation).[53] |
| Metastasis | Secondary malignant tumor of the heart, arising by lymphatic or hematogenous spread of a primary neoplasm. Presents with dyspnea, congestive heart failure, hypotension and malignant pericardial effusion. Any primary malignancy may metastasize to the heart, however, lung cancer is among the most common.[54] |
References
- ↑ Hartig I, Kraatz EG, Beurich HW, Moosig F (2014). “[Atrial myxoma with clinical signs of systemic inflammatory disease.]”. Z Rheumatol. doi:10.1007/s00393-013-1347-y. PMID 24599357.
- ↑ Mankad R, Herrmann J (December 2016). “Cardiac tumors: echo assessment”. Echo Res Pract. 3 (4): R65–R77. doi:10.1530/ERP-16-0035. PMC 5292983. PMID 27600455.
- ↑ Zaragoza-Macias E, Zaragosa-Macias E, Chen MA, Gill EA (February 2012). “Real time three-dimensional echocardiography evaluation of intracardiac masses”. Echocardiography. 29 (2): 207–19. doi:10.1111/j.1540-8175.2011.01627.x. PMID 22283202.
- ↑ Larrieu AJ, Jamieson WR, Tyers GF, Burr LH, Munro AI, Miyagishima RT, Gerein AN, Allen P (March 1982). “Primary cardiac tumors: experience with 25 cases”. J. Thorac. Cardiovasc. Surg. 83 (3): 339–48. PMID 7062746.
- ↑ Molina JE, Edwards JE, Ward HB (August 1990). “Primary cardiac tumors: experience at the University of Minnesota”. Thorac Cardiovasc Surg. 38 Suppl 2: 183–91. doi:10.1055/s-2007-1014064. PMID 2237900.
- ↑ Tazelaar HD, Locke TJ, McGregor CG (October 1992). “Pathology of surgically excised primary cardiac tumors”. Mayo Clin. Proc. 67 (10): 957–65. PMID 1434856.
- ↑ Sarjeant JM, Butany J, Cusimano RJ (2003). “Cancer of the heart: epidemiology and management of primary tumors and metastases”. Am J Cardiovasc Drugs. 3 (6): 407–21. doi:10.2165/00129784-200303060-00004. PMID 14728061.
- ↑ St John Sutton MG, Mercier LA, Giuliani ER, Lie JT (June 1980). “Atrial myxomas: a review of clinical experience in 40 patients”. Mayo Clin. Proc. 55 (6): 371–6. PMID 7382545.
- ↑ Pinede L, Duhaut P, Loire R (May 2001). “Clinical presentation of left atrial cardiac myxoma. A series of 112 consecutive cases”. Medicine (Baltimore). 80 (3): 159–72. PMID 11388092.
- ↑ Reynen K (December 1995). “Cardiac myxomas”. N. Engl. J. Med. 333 (24): 1610–7. doi:10.1056/NEJM199512143332407. PMID 7477198.
- ↑ Javed A, Zalawadiya S, Kovach J, Afonso L (March 2014). “Aortic valve myxoma at the extreme age: a review of literature”. BMJ Case Rep. 2014. doi:10.1136/bcr-2013-202689. PMC 3962858. PMID 24642215.
- ↑ Lee VH, Connolly HM, Brown RD (August 2007). “Central nervous system manifestations of cardiac myxoma”. Arch. Neurol. 64 (8): 1115–20. doi:10.1001/archneur.64.8.1115. PMID 17698701.
- ↑ Carney JA, Gordon H, Carpenter PC, Shenoy BV, Go VL (July 1985). “The complex of myxomas, spotty pigmentation, and endocrine overactivity”. Medicine (Baltimore). 64 (4): 270–83. PMID 4010501.
- ↑ McAllister HA, Hall RJ, Cooley DA (February 1999). “Tumors of the heart and pericardium”. Curr Probl Cardiol. 24 (2): 57–116. PMID 10028128.
- ↑ Klarich KW, Enriquez-Sarano M, Gura GM, Edwards WD, Tajik AJ, Seward JB (September 1997). “Papillary fibroelastoma: echocardiographic characteristics for diagnosis and pathologic correlation”. J. Am. Coll. Cardiol. 30 (3): 784–90. PMID 9283541.
- ↑ Tamin SS, Maleszewski JJ, Scott CG, Khan SK, Edwards WD, Bruce CJ, Oh JK, Pellikka PA, Klarich KW (June 2015). “Prognostic and Bioepidemiologic Implications of Papillary Fibroelastomas”. J. Am. Coll. Cardiol. 65 (22): 2420–9. doi:10.1016/j.jacc.2015.03.569. PMID 26046736.
- ↑ Gowda RM, Khan IA, Nair CK, Mehta NJ, Vasavada BC, Sacchi TJ (September 2003). “Cardiac papillary fibroelastoma: a comprehensive analysis of 725 cases”. Am. Heart J. 146 (3): 404–10. doi:10.1016/S0002-8703(03)00249-7. PMID 12947356.
- ↑ Beghetti M, Gow RM, Haney I, Mawson J, Williams WG, Freedom RM (December 1997). “Pediatric primary benign cardiac tumors: a 15-year review”. Am. Heart J. 134 (6): 1107–14. PMID 9424072.
- ↑ Smythe JF, Dyck JD, Smallhorn JF, Freedom RM (November 1990). “Natural history of cardiac rhabdomyoma in infancy and childhood”. Am. J. Cardiol. 66 (17): 1247–9. PMID 2239731.
- ↑ Jacobs JP, Konstantakos AK, Holland FW, Herskowitz K, Ferrer PL, Perryman RA (November 1994). “Surgical treatment for cardiac rhabdomyomas in children”. Ann. Thorac. Surg. 58 (5): 1552–5. PMID 7979700.
- ↑ Elbardissi AW, Dearani JA, Daly RC, Mullany CJ, Orszulak TA, Puga FJ, Schaff HV (September 2008). “Survival after resection of primary cardiac tumors: a 48-year experience”. Circulation. 118 (14 Suppl): S7–15. doi:10.1161/CIRCULATIONAHA.107.783126. PMID 18824772.
- ↑ Basu S, Folliguet T, Anselmo M, Greengart A, Sabado M, Cunningham JN, Jacobowitz IJ (April 1994). “Lipomatous hypertrophy of the interatrial septum”. Cardiovasc Surg. 2 (2): 229–31. PMID 8049952.
- ↑ Simpson L, Kumar SK, Okuno SH, Schaff HV, Porrata LF, Buckner JC, Moynihan TJ (June 2008). “Malignant primary cardiac tumors: review of a single institution experience”. Cancer. 112 (11): 2440–6. doi:10.1002/cncr.23459. PMID 18428209.
- ↑ Vander Salm TJ (April 2000). “Unusual primary tumors of the heart”. Semin. Thorac. Cardiovasc. Surg. 12 (2): 89–100. PMID 10807431.
- ↑ Petersen CD, Robinson WA, Kurnick JE (1976). “Involvement of the heart and pericardium in the malignant lymphomas”. Am. J. Med. Sci. 272 (2): 161–5. PMID 1008078.
- ↑ Ragland MM, Tak T (March 2006). “The role of echocardiography in diagnosing space-occupying lesions of the heart”. Clin Med Res. 4 (1): 22–32. PMC 1447535. PMID 16595790.
- ↑ Miguel CE, Bestetti RB (June 2011). “Primary cardiac lymphoma”. Int. J. Cardiol. 149 (3): 358–63. doi:10.1016/j.ijcard.2010.02.016. PMID 20227122.
- ↑ Grebenc ML, Rosado de Christenson ML, Burke AP, Green CE, Galvin JR (2000). “Primary cardiac and pericardial neoplasms: radiologic-pathologic correlation”. Radiographics. 20 (4): 1073–103, quiz 1110–1, 1112. doi:10.1148/radiographics.20.4.g00jl081073. PMID 10903697.
- ↑ Grinda JM, Couetil JP, Chauvaud S, D’Attellis N, Berrebi A, Fabiani JN, Deloche A, Carpentier A (January 1999). “Cardiac valve papillary fibroelastoma: surgical excision for revealed or potential embolization”. J. Thorac. Cardiovasc. Surg. 117 (1): 106–10. PMID 9869763.
- ↑ Webb DW, Thomas RD, Osborne JP (March 1993). “Cardiac rhabdomyomas and their association with tuberous sclerosis”. Arch. Dis. Child. 68 (3): 367–70. PMC 1793857. PMID 8466239.
- ↑ Yoshitake I, Hata M, Sezai A, Niino T, Unosawa S, Shimura K, Kasamaki Y, Minami K (September 2009). “Cardiac angiosarcoma with cardiac tamponade diagnosed as a ruptured aneurysm of the sinus valsalva”. Jpn. J. Clin. Oncol. 39 (9): 612–5. doi:10.1093/jjco/hyp044. PMID 19493870.
- ↑ Parissis H, Akbar MT, Young V (October 2010). “Primary leiomyosarcoma of the right atrium: a case report and literature update”. J Cardiothorac Surg. 5: 80. doi:10.1186/1749-8090-5-80. PMC 2964688. PMID 20939891.
- ↑ Gulati G, Sharma S, Kothari SS, Juneja R, Saxena A, Talwar KK (2004). “Comparison of echo and MRI in the imaging evaluation of intracardiac masses”. Cardiovasc Intervent Radiol. 27 (5): 459–69. doi:10.1007/s00270-004-0123-4. PMID 15383848.
- ↑ Narin B, Arman A, Arslan D, Simşek M, Narin A (February 2010). “Assessment of cardiac masses: magnetic resonance imaging versus transthoracic echocardiography”. Anadolu Kardiyol Derg. 10 (1): 69–74. PMID 20150010.
- ↑ “academic.oup.com”.
- ↑ Ismail I, Al-Khafaji K, Mutyala M, Aggarwal S, Cotter W, Hakim H, Khosla S, Arora R (2015). “Cardiac lipoma”. J Community Hosp Intern Med Perspect. 5 (5): 28449. doi:10.3402/jchimp.v5.28449. PMC 4612478. PMID 26486106.
- ↑ D’Souza J, Shah R, Abbass A, Burt JR, Goud A, Dahagam C (January 2017). “Invasive Cardiac Lipoma: a case report and review of literature”. BMC Cardiovasc Disord. 17 (1): 28. doi:10.1186/s12872-016-0465-2. PMC 5237479. PMID 28088193.
- ↑ Yadav, Pradeep K.; Baquero, Giselle A.; Malysz, Jozef; Kelleman, John; Gilchrist, Ian C. (2014). “Cardiac Paraganglioma”. Circulation: Cardiovascular Interventions. 7 (6): 851–856. doi:10.1161/CIRCINTERVENTIONS.114.001856. ISSN 1941-7640.
- ↑ Tahir M, Noor SJ, Herle A, Downing S (2009). “Right atrial paraganglioma: a rare primary cardiac neoplasm as a cause of chest pain”. Tex Heart Inst J. 36 (6): 594–7. PMC 2801953. PMID 20069088.
- ↑ Hamilton BH, Francis IR, Gross BH, Korobkin M, Shapiro B, Shulkin BL, Deeb CM, Orringer MB (January 1997). “Intrapericardial paragangliomas (pheochromocytomas): imaging features”. AJR Am J Roentgenol. 168 (1): 109–13. doi:10.2214/ajr.168.1.8976931. PMID 8976931.
- ↑ Shih, Wei-Jen; McCullough, Scott; Smith, Mary (1993). “Diagnostic imagings for primary cardiac fibrosarcoma”. International Journal of Cardiology. 39 (2): 157–161. doi:10.1016/0167-5273(93)90028-F. ISSN 0167-5273.
- ↑ Arai T, Kurashima C, Wada S, Chida K, Ohkawa S (November 1998). “Histological evidence for cell proliferation activity in cystic tumor (endodermal heterotopia) of the atrioventricular node”. Pathol. Int. 48 (11): 917–23. PMID 9832064.
- ↑ Wolf PL, Bing R (November 1965). “The smallest tumor which causes sudden death”. JAMA. 194 (6): 674–5. PMID 5897246.
- ↑ Burke AP, Anderson PG, Virmani R, James TN, Herrera GA, Ceballos R (October 1990). “Tumor of the atrioventricular nodal region. A clinical and immunohistochemical study”. Arch. Pathol. Lab. Med. 114 (10): 1057–62. PMID 2222148.
- ↑ Burke A, Tavora F (April 2016). “The 2015 WHO Classification of Tumors of the Heart and Pericardium”. J Thorac Oncol. 11 (4): 441–52. doi:10.1016/j.jtho.2015.11.009. PMID 26725181.
- ↑ Tran, Thao T; Starnes, Vaughn; Wang, Xuedong; Getzen, James; Ross, Brian D (2009). “Cardiovascular magnetics resonance diagnosis of cystic tumor of the atrioventricular node”. Journal of Cardiovascular Magnetic Resonance. 11 (1): 13. doi:10.1186/1532-429X-11-13. ISSN 1532-429X.
- ↑ Tatli, Servet; O’Gara, Patrick Thomas; Lambert, Jarvis; Kwong, Raymond; Byrne, John Gerald; Yucel, E. Kent (2004). “MRI of Atypical Lipomatous Hypertrophy of the Interatrial Septum”. American Journal of Roentgenology. 182 (3): 598–600. doi:10.2214/ajr.182.3.1820598. ISSN 0361-803X.
- ↑ Saboo, Sachin S.; Krajewski, Katherine M.; Zukotynski, Katherine; Howard, Stephanie; Jagannathan, Jyothi P.; Hornick, Jason L.; Ramaiya, Nikhil (2012). “Imaging Features of Primary and Secondary Adult Rhabdomyosarcoma”. American Journal of Roentgenology. 199 (6): W694–W703. doi:10.2214/AJR.11.8213. ISSN 0361-803X.
- ↑ Papillary fibroelastoma of the heart. Dr Craig Hacking et al http://radiopaedia.org/articles/papillary-fibroelastoma-of-the-heart Accessed on November 24, 2015
- ↑ Papillary fibroelastoma .Wikipedia https://en.wikipedia.org/wiki/Papillary_fibroelastoma Accessed on November 24, 2015
- ↑ Lipoma. Dr Craig Hacking et al . Radiopedia. http://radiopaedia.org/articles/cardiac-lipoma Accessed on November 24, 2015
- ↑ Rhabdomyoma. Wikipedia.https://en.wikipedia.org/wiki/Rhabdomyoma Accessed on November 24, 2015
- ↑ Intracardiac thrombi. Dr Craig Hacking et al. Radiopedia.http://radiopaedia.org/articles/intracardiac-thrombi Accessed on November 24, 2015
- ↑ Secondary cardiac neoplasm. Radiopedia.http://radiopaedia.org/articles/secondary-cardiac-neoplasms Accessed on November 24, 2015
Epidemiology and Demographics
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1] Associate Editor(s)-in-Chief: Maria Fernanda Villarreal, M.D. [2]Ahmad Al Maradni, M.D. [3]
Overview
Cardiac myxoma is a rare disease with a reported prevalence of 0.03% in general population. The incidence of cardiac myxoma is about 1/ 100,000 per year. The majority of patients with cardiac myxoma are diagnosed between 30 to 60 years; children are rarely affected. Females are more commonly affected with cardiac myxoma than men. The female-to-male ratio is approximately 1.8 to 1. Cardiac myxomas represent 78% of heart tumors.
Epidemiology and Demographics
Prevalence
- The prevalence of cardiac myxoma is reported as 0.03% in general population.[1][2]
Incidence
Age
- The mean age of patients at diagnosis is 50 years, most patients are between 30-60 age range.[3]
- Cardiac myxomas are rare in children. However, in the pediatric population cardiac myxomas are more likely to be related with familial forms such as the (Carney complex).[4]
Gender
- Females are more commonly affected with cardiac myxoma than men. The female-to-male ratio is approximately 1.8 to 1.[5]
- Patients with Carney complex, tend to be younger and male.[5]
References
- ↑ 1.0 1.1 Walpot J, Shivalkar B, Rodrigus I, Pasteuning WH, Hokken R (2010). “Atrial myxomas grow faster than we think”. Echocardiography. 27 (10): E128–31. doi:10.1111/j.1540-8175.2010.01186.x. PMID 20545988.
- ↑ Grebenc ML, Rosado de Christenson ML, Burke AP, Green CE, Galvin JR (2000). “Primary cardiac and pericardial neoplasms: radiologic-pathologic correlation”. Radiographics. 20 (4): 1073–103, quiz 1110–1, 1112. doi:10.1148/radiographics.20.4.g00jl081073. PMID 10903697.
- ↑ Siminelakis S, Kakourou A, Kakourou A, Batistatou A, Batistatou A, Sismanidis S, Sismanidis S, Ntoulia A, Tsakiridis K, Syminelaki T, Syminelaki T, Apostolakis E, Apostolakis E, Zarogoulidis P, Tsiouda T, Katsikogiannis N, Kougioumtzi I, Dryllis G, Machairiotis N, Mpakas A, Beleveslis T, Zarogoulidis K (March 2014). “Thirteen years follow-up of heart myxoma operated patients: what is the appropriate surgical technique?”. J Thorac Dis. 6 Suppl 1: S32–8. doi:10.3978/j.issn.2072-1439.2013.10.21. PMC 3966159. PMID 24672697.
- ↑ Arciniegas E, Hakimi M, Farooki ZQ, Truccone NJ, Green EW (1980). “Primary cardiac tumors in children”. J. Thorac. Cardiovasc. Surg. 79 (4): 582–91. PMID 7359937.
- ↑ 5.0 5.1 Yoon DH, Roberts W (2002). “Sex distribution in cardiac myxomas”. Am. J. Cardiol. 90 (5): 563–5. PMID 12208428.
Risk Factors
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Sogand Goudarzi, MD [2], Maria Fernanda Villarreal, M.D. [3], Ahmad Al Maradni, M.D. [4]
Overview
Common risk factors in the development of myxoma are female gender and genetic predisposition. In some cases, right atrial myxoma has been associated with tricuspid stenosis and atrial fibrillation.
Risk Factors
- Common risk factors in the development of myxoma are:[1]
- Female gender
- Genetic predisposition (Carney complex)
- In some cases, right atrial myxoma has been associated with tricuspid stenosis and atrial fibrillation.
- Risk factors for the embolism in myxoma include the following:[2]
- Tumor location
- Macroscopic appearance
- Platelet volume
- High platelet count
References
- ↑ Hasan, Mustajab; Abdelmaseih, Ramy; Faluk, Mohammed; Chacko, Jay; Nasser, Hesham (2020). “Atrial Myxoma, a Rare Cause of Sudden Cardiac Death: A Case Report and Review of Literature”. Cureus. doi:10.7759/cureus.6704. ISSN 2168-8184.
- ↑ He DK, Zhang YF, Liang Y, Ye SX, Wang C, Kang B; et al. (2015). “Risk factors for embolism in cardiac myxoma: a retrospective analysis”. Med Sci Monit. 21: 1146–54. doi:10.12659/MSM.893855. PMC 4418206. PMID 25900256.
Natural History, Complications and Prognosis
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1] Associate Editor(s)-in-Chief: Ahmad Al Maradni, M.D. [2]Maria Fernanda Villarreal, M.D. [3]
Overview
If left untreated, cardiac myxoma progression occurs slowly. The overlap of various phenomena such as thrombosis, hemorrhage, or fragmentation may influence tumor growth, detachment, and consequently embolism. Complications that can develop as a result of myxoma are: arrhythmias, pulmonary edema, peripheral emboli, metastasis, blockage of the mitral heart valve. The survival rates after 5-years are 83% for benign heart tumors.
Natural History
- If left untreated, cardiac myxoma progression occurs slowly. The overlap of various phenomena such as thrombosis, hemorrhage, or fragmentation may influence tumor growth, detachment, and consequently embolism..[1][2]
- Constitutional symptoms, such as: weight loss, fatigue, and weakness are often the initial clinical presentation of cardiac myxoma patients, and may resemble those from endocarditis.[3]
- Metastases are very uncommon in cardiac myxoma.[4]
- Overall, clinical features of cardiac myxoma are associated with the tumor size, location, and mobility.[5]
- Approximately 20% of patients with cardiac myxoma are asymptomatic.[6]
- Since the majority of the cardiac myxomas are left sided, it may progress to develop mitral valve obstruction or systemic embolic events, such as stroke.[7]
- Whereas, right atrial myxomas may obstruct the tricuspid valve and can present as right sided heart failure.[8]
Complications
Complications are common. Some of the complications that may develop as a result of myxoma are:[9][10][11]
- Peripheral emboli
- Blockage of the mitral heart valve
- Syncope
- Arrhythmias
- Pulmonary edema
- Metastasis
- Sudden death
- Fusiform cerebral aneurysms
Prognosis
Depending on the complications derivated from the cardiac myxoma at the time of diagnosis (embolic event or valve obstruction) the prognosis may vary. However with no complications, the prognosis is generally regarded as favorable after surgery. Recurrence rates (either locally or elsewhere in the heart) reported in 1-3% of cases. In atypical cases the rate is much higher (12-22%). The survival rates after 5-years are 83% for benign heart tumors.[1]
References
- ↑ 1.0 1.1 Hoffmeier A, Sindermann JR, Scheld HH, Martens S (2014). “Cardiac tumors–diagnosis and surgical treatment”. Dtsch Arztebl Int. 111 (12): 205–11. doi:10.3238/arztebl.2014.0205. PMC 3983698. PMID 24717305.
- ↑ Markel ML, Waller BF, Armstrong WF (1987). “Cardiac myxoma. A review”. Medicine (Baltimore). 66 (2): 114–25. PMID 3547010.
- ↑ Singhal P, Luk A, Rao V, Butany J (January 2014). “Molecular basis of cardiac myxomas”. Int J Mol Sci. 15 (1): 1315–37. doi:10.3390/ijms15011315. PMC 3907871. PMID 24447924.
- ↑ Wan, Yan; Du, Hai; Zhang, Lei; Guo, Shuang; Xu, Li; Li, Yuanyuan; He, Hui; Zhou, Lian; Chen, Yunping; Mao, Ling; Jin, Huijuan; Hu, Bo (2019). “Multiple cerebral metastases and metastatic aneurysms in patients with left atrial Myxoma: a case report”. BMC Neurology. 19 (1). doi:10.1186/s12883-019-1474-4. ISSN 1471-2377.
- ↑ Burke A, Virmani R. Tumors of the Heart and Great Vessels. Amer Registry of Pathology; 1996.
- ↑ Thyagarajan, Braghadheeswar; Kumar, Monisha Priyadarshini; Patel, Shil; Agrawal, Abhinav (2017). “Extracardiac manifestations of atrial myxomas”. Journal of the Saudi Heart Association. 29 (1): 37–43. doi:10.1016/j.jsha.2016.07.003. ISSN 1016-7315.
- ↑ Lyaker, MichaelR; Tulman, DavidB; Dimitrova, GalinaT; Pin, RichardH; Papadimos, ThomasJ (2013). “Arterial embolism”. International Journal of Critical Illness and Injury Science. 3 (1): 77. doi:10.4103/2229-5151.109429. ISSN 2229-5151.
- ↑ Thyagarajan, Braghadheeswar; Kumar, Monisha Priyadarshini; Patel, Shil; Agrawal, Abhinav (2017). “Extracardiac manifestations of atrial myxomas”. Journal of the Saudi Heart Association. 29 (1): 37–43. doi:10.1016/j.jsha.2016.07.003. ISSN 1016-7315.
- ↑ Cina SJ, Smialek JE, Burke AP, Virmani R, Hutchins GM (1996). “Primary cardiac tumors causing sudden death: a review of the literature”. Am J Forensic Med Pathol. 17 (4): 271–81. doi:10.1097/00000433-199612000-00001. PMID 8947350.
- ↑ Wang Z, Chen S, Zhu M, Zhang W, Zhang H, Li H; et al. (2016). “Risk prediction for emboli and recurrence of primary cardiac myxomas after resection”. J Cardiothorac Surg. 11: 22. doi:10.1186/s13019-016-0420-4. PMC 4736655. PMID 26832806.
- ↑ Guk HS, Lee S, Jeong HB, Ju W, Choi JS, Lee YS (2019). “Recurrent Embolic Stroke Associated with Long-Latency Relapsing Cardiac Myxoma”. J Clin Neurol. 15 (4): 591–593. doi:10.3988/jcn.2019.15.4.591. PMC 6785467 Check
|pmc=value (help). PMID 31591856.
Diagnosis
Diagnosis
Staging | History and Symptoms | Physical Examination | Laboratory Findings | Electrocardiogram | Chest X Ray | CT | MRI | Echocardiography or Ultrasound | Other Imaging Findings | Other Diagnostic Studies
Treatment
Treatment
Medical Therapy | Surgery | Cost-Effectiveness of Therapy | Future or Investigational Therapies
References
References
- ↑ Image courtesy of Radswiki Radiopaedia (original file here).Creative Commons BY-SA-NC
Looking for the patient version?
© 2026 MyEClinic – IFTM Institut für Telematik in der Medizin GmbH