
Aortic dissection
For patient information, click here
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor-In-Chief: Cafer Zorkun, M.D., Ph.D. [2] Sahar Memar Montazerin, M.D.[3] Laith Adnan Allaham, M.D.[4]
Synonyms and keywords: Leaking aneurysm; dissecting aortic aneurysm; aneurysm, dissecting, aorta; aortic aneurysm – dissecting
Overview
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor-In-Chief: Cafer Zorkun, M.D., Ph.D. [2] Sahar Memar Montazerin, M.D.[3]
Overview
Dr. Frank Nicholls described the first case of aortic dissection in 1761. Later, in 1819, Dr. René Laennec used the term dissecting aneurysm for the first time. The first successful surgical intervention for aortic dissection was done by Dr. Cooley and Dr. Creech in 1954. In 1965, Dr. DeBakey suggested the first classification system for aortic dissection. In 1970, a group of surgeons suggested the simplified classification system of Stanford. In 1996, an international, referral center was registered for acute aortic dissection with the goal of registering patients’ presentation, treatment, and outcome. This registry provides information of more than 1500 patients with acute aortic dissection and may be used as a resource for this disorder. In 2006, another international registry was established in Germany for acute aortic dissection type A (AADA) with the goal of collecting patients’ information for structured follow-up. This registry with more than 2000 patients is now the largest database on AADA worldwide. Several different classification systems have been used to describe aortic dissections. The systems commonly in use are either based on either the anatomy of the dissection (proximal, distal) or the duration of onset of symptoms (acute, chronic) prior to presentation. DeBakey and Stanford’s systems are commonly used classification systems for aortic dissection. European society of cardiology defined another classification system for aortic dissection in 2014. Aortic dissection begins as a tear in the aortic wall in > 95% of patients. The tear is usually transverse, extends through the intima and halfway through the media and involves ~50% of the aortic circumference. An inherent weakness in the tunica media layer predisposes patients to develop a tear in the intima layer. Two thirds of dissections originate in the ascending aorta, and 20% are in the proximal descending aorta. Age-related changes due to atherosclerosis and uncontrolled hypertension are associated with spontaneous dissection, while blunt trauma injury and sudden deceleration in a motor vehicle accident is a major cause of aortic dissection. Aortic dissection is a life threatening entity that must be distinguished from other life threatening entities such as cardiac tamponade, cardiogenic shock, myocardial infarction, and pulmonary embolism. An aortic aneurysm is not synonymous with aortic dissection. Aneurysms are defined as a localized permanent dilation of the aorta to a diameter > 50% of normal. The incidence of aortic dissection is approximately 6 per 100,000 individuals worldwide.The incidence of aortic dissection increases with age, with a mean age of 63 years. Men are more commonly affected by aortic dissection than women. However, the prognosis tends to be worse in women due to unusual presentations. There is no racial predilection to aortic dissection. However, non-white race is associated with worse prognosis. The 30-days mortality rate of aortic dissection type A and B is approximately 47% and 13%, respectively. Common risk factors in the development of aortic dissection include aging, atherosclerosis, diabetes, hypertension and trauma. Less common risk factors include bicuspid aortic valve, cocaine abuse, coarctation of the aorta, cystic medial necrosis, a history of collagen vascular disoders, giant cell arteritis, heart surgery, pseudoxanthoma elasticum, Turner’s syndrome, tertiary syphilis and the third trimester of pregnancy. Screening guidelines state that an EKG should be obtained for all patients who present with symptoms suspicious for aortic dissection. A chest x-ray should be obtained for patients determined to be in low-risk, and moderate-risk categories, and for patients in high-risk categories, TEE, CT Angiography or MRI Angiography should be obtained. The symptoms of aortic dissection usually develop in the fifth decade of life and start with symptoms such as sudden onset chest/back pain. If left untreated, patients with aortic dissection may progress to develop aortic regurgitation, myocardial ischemia, and cardiac tamponade. The complications of aortic dissection include but not limited to aortic rupture, pericardial tamponade, myocardial ischemia, compression of nearby organs and etc. Aortic dissection carries a poor prognosis. Mortality rate differs based on the type of dissection and is higher in type A compared to type B (25% versus 12%). The diagnostic work-up of aortic dissection is highly dependent on the pretest probability of the patients as well as their hemodynamic status. In hemodynamically unstable patients, transesophageal echocardiography has the greatest value. CT scan, MRI, and transesophageal echocardiography have been observed to have similar reliability in the diagnosis of aortic dissection. However, CT and MRI have been preferred modality for assessing the extension and branch involvement in aortic dissection and diagnosing other types of acute aortic syndrome other than dissection as well as traumatic aortic lesions. History of patients with aortic dissection may be positive for factors such as connective tissue disease, known aortic valve disease, recent heart surgery, Known thoracic aortic aneurysm, and family history of the aortic disease. Sudden onset chest/back pain is the most common symptom of aortic dissection. Pain may be of sharp, ripping, tearing, and knife-like quality. Aortic dissection is commonly associated with varying blood pressure (pseudohypotension or hypertension or hypotension), wide pulse pressure (if the aortic root is involved causing aortic insufficiency), tachycardia, pulsus paradoxus, swollen face due to superior vena cava compression (superior vena cava syndrome). Radial-radial delay or radio-femoral delay (deficit) in pulse can be seen in patients depending on the location of dissection. Pulse deficit is commonly seen in females. In proximal dissections involving aortic root, aortic insufficiency is a complication, and on physical examination an early diastolic decrescendo murmur, which is best heard in the right second intercostal space is noted. There is no particular laboratory findings for the diagnosis of aortic dissection. Possible laboratory findings associated with aortic dissection may include troponin elevation, CK-MB elevation, hematuria, and etc. There has been reports of using a smooth muscle myosin heavy chain immunoassay to help diagnose aortic dissection. EKG findings in aortic dissection are usually non-specific. Possible findings include non-specific ST-segment changes, atrioventricular block (second degree), left ventricular hypertrophy, and sinus bradycardia. It worth mentioning that ECG may lead to a delay in the diagnosis. Since clinicians usually follow the diagnosis of coronary artery disease due to its higher prevalence. Chest x-ray may be helpful in the diagnosis of aortic dissection. Findings suggestive of aortic dissection on x-ray include widening of mediastinum, wide aortic contour, tracheal deviation, aortic kinking, and displacement of previous aortic calcification. Chest x-ray has limited sensitivity (64%) and specificity (86%) in the diagnosis of aortic diseases. It also worth mentioning that a normal chest x-ray may not rule out the diagnosis of aortic dissection. A CT scan can be used to diagnose aortic dissection if neither a TEE nor MRI is available in a timely fashion, or if there is a contraindication to their performance. An example would be after hours in an emergency room setting. If the results of the CT scan are non-diagnostic, then TEE or MRI should be performed to confirm the diagnosis. MRI is the imaging modality of choice in the assessment of longstanding aortic disease in a patient who has chronic chest pain who is hemodynamically stable or for the evaluation of a chronic dissection. Type A dissections of the proximal aorta are generally managed with the operative repair. The repair can be done via open surgery vs endovascular repair depending on the extent of dissection. Type B dissections of the descending aorta are generally managed medically. Even patients who are undergoing operative repair require optimal medical management. The two goals in the medical management of aortic dissection are to reduce blood pressure and to reduce the oscillatory shear on the wall of the aorta (the shear-force dP/dt or force of ejection of blood from the left ventricle). The target blood pressure should be a mean arterial pressure (MAP) of 60 to 75 mm Hg. Aortic dissection is the only hypertensive emergency where target BP is less than 120/80 within the first four hours of presentation. Ideally, the target is to control the heart rate to less than 60 per minute. The first line of agents are beta-blockers, esmolol continuous infusion is used preferably as it is short-acting and works for blood pressure as well as heart rate. IV Labetalol or PO propranolol or metoprolol can also be used. The addition of other IV continuous nitroprusside can also be used. Cyanide toxicity is a concern when nitroprusside is used for more than 24 hours. Any dissection that involves the ascending aorta is considered a surgical emergency, and urgent surgical consultation is recommended. There is a 90% 3-month mortality among patients with a proximal aortic dissection who do not undergo surgery. These patients can rapidly develop acute aortic insufficiency (AI), tamponade or myocardial infarction (MI).
Historical Perspective
Dr. Frank Nicholls described the first case of aortic dissection in 1761. Later, in 1819, Dr. René Laennec used the term dissecting aneurysm for the first time. The first successful surgical intervention for aortic dissection was done by Dr. Cooley and Dr. Creech in 1954. In 1965, Dr. DeBakey suggested the first classification system for aortic dissection. In 1970, a group of surgeons suggested the simplified classification system of Stanford. In 1996, an international, referral center was registered for acute aortic dissection with the goal of registering patients’ presentation, treatment, and outcome. This registry provides information of more than 1500 patients with acute aortic dissection and may be used as a resource for this disorder. In 2006, another international registry was established in Germany for acute aortic dissection type A (AADA) with the goal of collecting patients’ information for structured follow-up. This registry with more than 2000 patients is now the largest database on AADA worldwide.
Classification
Several different classification systems have been used to describe aortic dissections. The systems commonly in use are either based on either the anatomy of the dissection (proximal, distal) or the duration of onset of symptoms (acute, chronic) prior to presentation. DeBakey and Stanford’s systems are commonly used classification systems for aortic dissection. European society of cardiology defined another classification system for aortic dissection in 2014.
Pathophysiology
Aortic dissection begins as a tear in the aortic wall in > 95% of patients. The tear is usually transverse, extends through the intima and halfway through the media and involves ~50% of the aortic circumference. An inherent weakness in the tunica media layer predisposes patients to develop a tear in the intima layer. Two thirds of dissections originate in the ascending aorta, and 20% are in the proximal descending aorta.
Causes
Age-related changes due to atherosclerosis and uncontrolled hypertension are associated with spontaneous dissection, while blunt trauma injury and sudden deceleration in a motor vehicle accident is a major cause of aortic dissection.
Differentiating Aortic Dissection from other Diseases
Aortic dissection is a life threatening entity that must be distinguished from other life threatening entities such as cardiac tamponade, cardiogenic shock, myocardial infarction, and pulmonary embolism. An aortic aneurysm is not synonymous with aortic dissection. Aneurysms are defined as a localized permanent dilation of the aorta to a diameter > 50% of normal.
Epidemiology and Demographics
The incidence of aortic dissection is approximately 6 per 100,000 individuals worldwide.The incidence of aortic dissection increases with age, with a mean age of 63 years. Men are more commonly affected by aortic dissection than women. However, the prognosis tends to be worse in women due to unusual presentations. There is no racial predilection to aortic dissection. However, non-white race is associated with worse prognosis. The 30-days mortality rate of aortic dissection type A and B is approximately 47% and 13%, respectively.
Risk Factors
Common risk factors in the development of aortic dissection include aging, atherosclerosis, diabetes, hypertension and trauma. Less common risk factors include bicuspid aortic valve, cocaine abuse, coarctation of the aorta, cystic medial necrosis, a history of collagen vascular disoders, giant cell arteritis, heart surgery, pseudoxanthoma elasticum, Turner’s syndrome, tertiary syphilis and the third trimester of pregnancy.
Screening
Screening guidelines state that an EKG should be obtained for all patients who present with symptoms suspicious for aortic dissection. A chest x-ray should be obtained for patients determined to be in low-risk, and moderate-risk categories, and for patients in high-risk categories, TEE, CT Angiography or MRI Angiography should be obtained.
Natural History, Complications and Prognosis
The symptoms of aortic dissection usually develop in the fifth decade of life and start with symptoms such as sudden onset chest/back pain. If left untreated, patients with aortic dissection may progress to develop aortic regurgitation, myocardial ischemia, and cardiac tamponade. The complications of aortic dissection include but not limited to aortic rupture, pericardial tamponade, myocardial ischemia, compression of nearby organs and etc. Aortic dissection carries a poor prognosis. Mortality rate differs based on the type of dissection and is higher in type A compared to type B (25% versus 12%).
Diagnosis
Diagnostic Study of Choice
The diagnostic work-up of aortic dissection is highly dependent on the pretest probability of the patients as well as their hemodynamic status. In hemodynamically unstable patients, transesophageal echocardiography has the greatest value. CT scan, MRI, and transesophageal echocardiography have been observed to have similar reliability in the diagnosis of aortic dissection. However, CT and MRI have been preferred modality for assessing the extension and branch involvement in aortic dissection and diagnosing other types of acute aortic syndrome other than dissection as well as traumatic aortic lesions.
History and Symptoms
History of patients with aortic dissection may be positive for factors such as connective tissue disease, known aortic valve disease, recent heart surgery, Known thoracic aortic aneurysm, and family history of the aortic disease. Sudden onset chest/back pain is the most common symptom of aortic dissection. Pain may be of sharp, ripping, tearing, and knife-like quality.
Physical Examination
Aortic dissection is commonly associated with varying blood pressure (pseudohypotension or hypertension or hypotension), wide pulse pressure (if the aortic root is involved causing aortic insufficiency), tachycardia, pulsus paradoxus, swollen face due to superior vena cava compression (superior vena cava syndrome). Radial-radial delay or radio-femoral delay (deficit) in pulse can be seen in patients depending on the location of dissection. Pulse deficit is commonly seen in females. In proximal dissections involving aortic root, aortic insufficiency is a complication, and on physical examination an early diastolic decrescendo murmur, which is best heard in the right second intercostal space is noted.
Laboratory Findings
There is no particular laboratory findings for the diagnosis of aortic dissection. Possible laboratory findings associated with aortic dissection may include troponin elevation, CK-MB elevation, hematuria, and etc. There has been reports of using a smooth muscle myosin heavy chain immunoassay to help diagnose aortic dissection.
Electrocardiogram
EKG findings in aortic dissection are usually non-specific. Possible findings include non-specific ST-segment changes, atrioventricular block (second degree), left ventricular hypertrophy, and sinus bradycardia. It worth mentioning that ECG may lead to a delay in the diagnosis. Since clinicians usually follow the diagnosis of coronary artery disease due to its higher prevalence.
Imaging in Acute Aortic Dissection
There are a wide variety of imaging studies that can be used to diagnose aortic dissection, but in general, transesophageal imaging is the imaging modality of choice in the acutely ill patient and CT Angiography, MRI is the imaging modality of choice in the assessment of longstanding aortic disease in a patient who has chronic chest pain who is hemodynamically stable or for the evaluation of a chronic dissection.
Chest X-ray
Chest x-ray may be helpful in the diagnosis of aortic dissection. Findings suggestive of aortic dissection on x-ray include widening of mediastinum, wide aortic contour, tracheal deviation, aortic kinking, and displacement of previous aortic calcification. Chest x-ray has limited sensitivity (64%) and specificity (86%) in the diagnosis of aortic diseases. It also worth mentioning that a normal chest x-ray may not rule out the diagnosis of aortic dissection.
CT
A CT scan can be used to diagnose aortic dissection if neither a TEE nor MRI is available in a timely fashion, or if there is a contraindication to their performance. An example would be after hours in an emergency room setting. If the results of the CT scan are non-diagnostic, then TEE or MRI should be performed to confirm the diagnosis.
MRI
MRI is the imaging modality of choice in the assessment of longstanding aortic disease in a patient who has chronic chest pain who is hemodynamically stable or for the evaluation of a chronic dissection.
Echocardiography
The echocardiographic changes diagnostic of aortic dissection include Intimal flaps in the aorta obstruction of a false lumen, intimal calcification displacement toward the center of the lumen, separation of intimal layers from the thrombus, and shearing of different wall layers during aortic pulsation. The sensitivity and specificity of transthoracic echocardiography vary based on the type of dissection and are usually lower for the diagnosis of distally located aortic dissection. Echocardiography may also show severe pleural effusion, which is suggestive of the development of cardiac tamponade. Transesophageal echocardiography may be useful in the diagnosis of aortic dissection in patients in whom transthoracic echocardiography has limited efficacy. Prolapse of intimal flap through the aortic valve seen in transesophageal echocardiography is diagnostic of aortic dissection complicated by aortic regurgitation. Sensitivity is usually higher (99%). However, it has limited usage in the diagnosis of dissections involving the distal portion of ascending aorta.
Treatment
Medical Therapy
Type A dissections of the proximal aorta are generally managed with the operative repair. The repair can be done via open surgery vs endovascular repair depending on the extent of dissection. Type B dissections of the descending aorta are generally managed medically. Even patients who are undergoing operative repair require optimal medical management. The two goals in the medical management of aortic dissection are to reduce blood pressure and to reduce the oscillatory shear on the wall of the aorta (the shear-force dP/dt or force of ejection of blood from the left ventricle). The target blood pressure should be a mean arterial pressure (MAP) of 60 to 75 mmHg. Aortic dissection is the only hypertensive emergency where target BP is less than 120/80 within the first four hours of presentation. Ideally, the target is to control the heart rate to less than 60 per minute. The first line of agents are beta-blockers, esmolol continuous infusion is used preferably as it is short-acting and works for blood pressure as well as heart rate. IV Labetalol or PO propranolol or metoprolol can also be used. The addition of other IV continuous nitroprusside can also be used.Cyanide toxicity is a concern when nitroprusside is used for more than 24 hours.
Surgery
Any dissection that involves the ascending aorta is considered a surgical emergency, and urgent surgical consultation is recommended. There is a 90% 3-month mortality among patients with a proximal aortic dissection who do not undergo surgery. These patients can rapidly develop acute aortic insufficiency (AI), tamponade or myocardial infarction (MI).
Secondary Prevention
Proper treatment and control of hardening of the arteries (atherosclerosis) and high blood pressure may reduce risk of aortic dissection. It is very important for patients at risk for dissection to tightly control their blood pressure. Taking safety precautions to prevent injuries can help prevent dissections. Many cases of aortic dissection cannot be prevented. If diagnosed with Marfan or Ehlers-Danlos syndrome, regular follow-up is advisable.
Historical Perspective
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Sahar Memar Montazerin, M.D.[2]
Overview
Dr. Frank Nicholls described the first case of aortic dissection in 1761. Later, in 1819, Dr. René Laennec used the term dissecting aneurysm for the first time. First successful surgical intervention for aortic dissection was done by Dr. Cooley and Dr. Creech in 1954. In 1965, Dr. DeBakey suggested the first classification system for aortic dissection. In 1970, a group of surgeons suggested the simplified classification system of Stanford. In 1996, an international, referral center was registered for acute aortic dissection with the goal of registering patients presentation, treatment, and outcome. This registry provides information of more than 1500 patients with acute aortic dissection and may be used as a resource for this disorder. In 2006, another international registry was established in Germany for acute aortic dissection type A (AADA) with the goal of collecting patients information for structured follow-up. This registry of more than 2000 patients is now the largest database on AADA worldwide.
Historical Perspective
Discovery
- In 1761, Dr. Frank Nicholls described the first case of aortic dissection.[1]
- In 1965, Dr. DeBakey suggested the first classification system for aortic dissection.[2]
Landmark Events in the Development of Treatment Strategies
- First successful surgical intervention for aortic dissection was done by Dr. Cooley and Dr. Creech in 1954.[3]
- In 1970, a group of surgeons suggested the simplified classification system of Stanford.[4]
- In 1996, an international, referral center was registered for acute aortic dissection with the goal of registering patients presentation, treatment, and outcome. This registry provides information of more than 1500 patients with acute aortic dissection and may be used as a resource for this disorder.[5]
- In 2006, another international registry was established in Germany for acute aortic dissection type A (AADA) with the goal of collecting patients information for structured follow-up. This registry of more than 2000 patients is now the largest database on AADA worldwide.[6][7]
Impact on Cultural History
- In 1819, Dr. René Laennec used the term dissecting aneurysm for the first time.[8]
Famous Cases
The following are the famous cases of aortic dissection:[9]
- George II, King of England
- Dr. Michael DeBakey
References
- ↑ “LI. Observations concerning the body of his late Majesty, October 26, 1760”. Philosophical Transactions of the Royal Society of London. 52: 265–275. 1761. doi:10.1098/rstl.1761.0052. ISSN 0261-0523.
- ↑ DEBAKEY ME, HENLY WS, COOLEY DA, MORRIS GC, CRAWFORD ES, BEALL AC (January 1965). “SURGICAL MANAGEMENT OF DISSECTING ANEURYSMS OF THE AORTA”. J. Thorac. Cardiovasc. Surg. 49: 130–49. PMID 14261867.
- ↑ De Bakey, Michael E.; Cooley, Denton A.; Creech, Oscar (1955). “Surgical Considerations of Dissecting Aneurysm of the Aorta”. Annals of Surgery. 142 (4): 586–612. doi:10.1097/00000658-195510000-00005. ISSN 0003-4932.
- ↑ Daily, Pat O.; Trueblood, H. Ward; Stinson, Edward B.; Wuerflein, Robert D.; Shumway, Norman E. (1970). “Management of Acute Aortic Dissections”. The Annals of Thoracic Surgery. 10 (3): 237–247. doi:10.1016/S0003-4975(10)65594-4. ISSN 0003-4975.
- ↑ Hagan, Peter G.; Nienaber, Christoph A.; Isselbacher, Eric M.; Bruckman, David; Karavite, Dean J.; Russman, Pamela L.; Evangelista, Arturo; Fattori, Rossella; Suzuki, Toru; Oh, Jae K.; Moore, Andrew G.; Malouf, Joseph F.; Pape, Linda A.; Gaca, Charlene; Sechtem, Udo; Lenferink, Suzanne; Deutsch, Hans Josef; Diedrichs, Holger; Marcos y Robles, Jose; Llovet, Alfredo; Gilon, Dan; Das, Sugata K.; Armstrong, William F.; Deeb, G. Michael; Eagle, Kim A. (2000). “The International Registry of Acute Aortic Dissection (IRAD)”. JAMA. 283 (7): 897. doi:10.1001/jama.283.7.897. ISSN 0098-7484.
- ↑ Conzelmann, L.O.; Krüger, T.; Hoffmann, I.; Rylski, B.; Easo, J.; Oezkur, M.; Kallenbach, K.; Dapunt, O.; Karck, M.; Weigang, E. (2011). “Deutsches Register für akute Aortendissektion Typ A (GERAADA)”. Herz. 36 (6): 513–524. doi:10.1007/s00059-011-3512-x. ISSN 0340-9937.
- ↑ Weigang, E.; Rylski, B.; Krüger, T.; Easo, J.; Conzelmann, L.O.; Karck, M.; Boening, A. (2016). “German Registry for Acute Aortic Dissection Type A: Structure, Results, and Future Perspectives”. The Thoracic and Cardiovascular Surgeon. 65 (02): 077–084. doi:10.1055/s-0036-1572436. ISSN 0171-6425.
- ↑ Criado FJ (2011). “Aortic dissection: a 250-year perspective”. Tex Heart Inst J. 38 (6): 694–700. PMC 3233335. PMID 22199439.
- ↑ Leonard, J C (1979). “Thomas Bevill Peacock and the early history of dissecting aneurysm”. BMJ. 2 (6184): 260–262. doi:10.1136/bmj.2.6184.260. ISSN 0959-8138.
Classification
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor-In-Chief: Cafer Zorkun, M.D., Ph.D. [2] Sahar Memar Montazerin, M.D.[3]
Overview
Several different classification systems have been used to describe aortic dissections. The systems commonly in use are either based on either the anatomy of the dissection (proximal, distal) or the duration of onset of symptoms (acute, chronic) prior to presentation. DeBakey and Stanford systems are the commonly used classification systems for aortic dissection. European society of cardiology defined another classification system for aortic dissection in 2014.
Classification
- Several classification systems have been suggested for the description of aortic dissection.[1][2][3][4]
- The commonly used classifications for aortic dissection are either based on the timing of the symptoms or the anatomy of the dissection.
- DeBakey and Stanford systems are the commonly used classification systems for aortic dissection.
DeBakey Classification System
The DeBakey system classifies aortic dissection based on anatomy of the aorta. It classifies the dissection according to the intimal tear location.[5]
- Type I – Intimal tear is located in ascending aorta, spreads at least to the aortic arch and often beyond it distally.
- Type II –Intimal tear is located and limited to the ascending aorta.
- Type III – Intimal tear is located in descending aorta, rarely extends proximally.
- Type III A: Dissection limited to the descending thoracic aorta
- Type III B: Dissection extended below the diaphragm

|

|

| |
| Percentage | 60 % | 10-15 % | 25-30 % |
| Type | DeBakey I | DeBakey II | DeBakey III |
| Stanford A | Stanford B | ||
| Proximal | Distal | ||
| Classification of aortic dissection | |||
Stanford Classification System
Stanford classification system is based on the involvement of ascending aorta.[6]
- A = Type I and II DeBakey
- B = Type III Debakey

- Aortic dissection may be classified according to the timing of symptom presentation to the following:
- Acute (<14 days)
- Sub-acute (15-90 days)
- Chronic (>90 days)
References
- ↑ Nienaber CA, Eagle KA (August 2003). “Aortic dissection: new frontiers in diagnosis and management: Part I: from etiology to diagnostic strategies”. Circulation. 108 (5): 628–35. doi:10.1161/01.CIR.0000087009.16755.E4. PMID 12900496.
- ↑ Tsai TT, Nienaber CA, Eagle KA (December 2005). “Acute aortic syndromes”. Circulation. 112 (24): 3802–13. doi:10.1161/CIRCULATIONAHA.105.534198. PMID 16344407.
- ↑ DEBAKEY ME, HENLY WS, COOLEY DA, MORRIS GC, CRAWFORD ES, BEALL AC (January 1965). “SURGICAL MANAGEMENT OF DISSECTING ANEURYSMS OF THE AORTA”. J. Thorac. Cardiovasc. Surg. 49: 130–49. PMID 14261867.
- ↑ Daily PO, Trueblood HW, Stinson EB, Wuerflein RD, Shumway NE (September 1970). “Management of acute aortic dissections”. Ann. Thorac. Surg. 10 (3): 237–47. doi:10.1016/s0003-4975(10)65594-4. PMID 5458238.
- ↑ DeBakey ME, Henly WS, Cooley DA, Morris GC Jr, Crawford ES, Beall AC Jr. Surgical management of dissecting aneurysms of the aorta. J Thorac Cardiovasc Surg 1965;49:130-49. PMID 14261867.
- ↑ Daily PO, Trueblood HW, Stinson EB, Wuerflein RD, Shumway NE. Management of acute aortic dissections. Ann Thorac Surg 1970;10:237-47. PMID 5458238.
Pathophysiology
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Cafer Zorkun, M.D., Ph.D. [2] Sahar Memar Montazerin, M.D.[3]
Overview
Aortic dissection begins as a tear in the aortic wall in > 95% of patients. The tear is usually transverse, extends through the intima and halfway through the media and involves ~50% of the aortic circumference. Two thirds of dissections originate in the ascending aorta, and 20% are in the proximal descending aorta.
Pathophysiology
Normal Anatomy of the Aorta

Pathogenesis
Initial Intimal Tear
- Aortic dissection begins as a tear in the aortic wall in > 95% of patients.
- It is usually transverse, extends through the intima and halfway through the media and involves ~50% of the aortic circumference.
Location of Dissections
- The initial tear is usually within 100 mm of the aortic valve.
- 65% of dissections originate in the ascending aorta, distal to the aortic valve and coronary ostia
- 10% arise in the transverse aortic arch
- 20% in the proximal descending aorta
- 5% in the more distal descending aorta
Propagation of the Intimal Tear
In an aortic dissection, blood penetrates the intima and enters the media layer. The high pressure rips the tissue of the media apart, allowing more blood to enter. This can propagate along the length of the aorta for a variable distance, dissecting either towards or away from the heart or both.
Once a tear develops, blood then passes into the media, and a false lumen is dissected in the outer layer of aortic media involving ~50% of the aortic circumference. This false lumen can enlarge, and compress the true lumen, as well as extend proximally or distally and occlude aortic branches. For some unknown reason, the right lateral wall of the ascending aorta is the most common site for dissection. The right coronary artery can become occluded as a result of this propagation.
Separating the false lumen from the true lumen is a layer of intimal tissue. This tissue is known as the intimal flap. As blood flows down the false lumen, it may cause secondary tears in the intima. Through these secondary tears, the blood can re-enter the true lumen.
Aortic Dissection in the Absence of an Intimal Tear
In about 13% of aortic dissections, there is no evidence of an intimal tear. It is believed that in these cases the inciting event is an intramural hematoma (caused by hemorrhage within the media). Since there is no direct connection between the true lumen and the false lumen in these cases, it is difficult to diagnose an aortic dissection by aortography if the etiology is an intramural hematoma. An aortic dissection secondary to an intramural hematoma should be treated the same as one caused by an intimal tear.
An aortic intramural hematoma can form when the vasa vasorum ruptures into the aortic wall. This is distinguished from dissection by the lack of an intimal tear. This disorder parallels aortic dissection in terms of prognosis when the ascending aorta or aortic arch is involved, and rapid surgical intervention is indicated. Involvement of the descending aorta, however, carries a better prognosis than dissection, and outcome tends to be similar with medical or surgical therapy.
Genetics
Genes involved in the pathogenesis of aortic dissection include:[1][2]
- FBN1 (fibrillin-1)
- LOX (lysyl oxidase)
- MYH11 (smooth muscle myosin heavy chain 11)
- ACTA2 (smooth muscle α-actin 2)
- MYLK (myosin light chain kinase)
- PRKG1 (protein kinase cGMP-dependent type 1)
- COL3A1 (α-1 procollagen, type III)
- TGFBR1 (TGF-β receptor type I)
- TGFBR2 (TGF-β receptor type II)
- TGFB2
- SMAD3 (mothers against decapentaplegic drosophila homolog 3)
Associated Conditions
Conditions associated with aortic dissection include:[1]
- Aortic aneurysm
- Smooth muscle dysfunction syndrome
- Marfan syndrome
- Vascular Ehlers-Danlos syndrome
- Loeys-Dietz syndromes
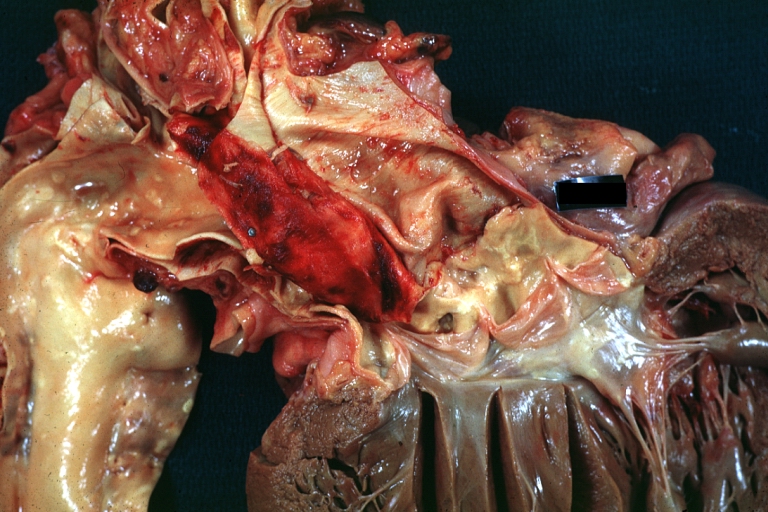
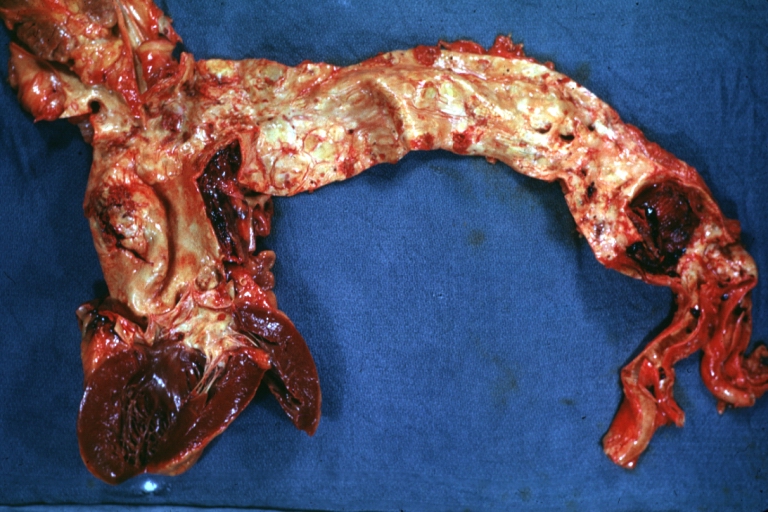
Gross Pathology
-
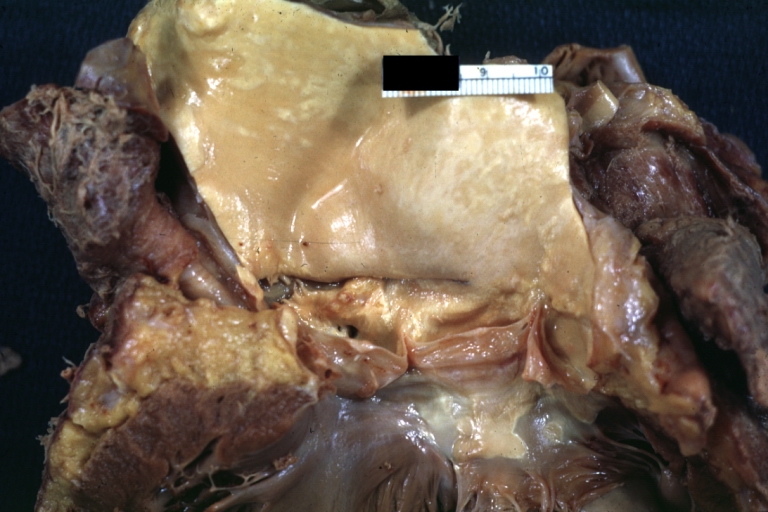
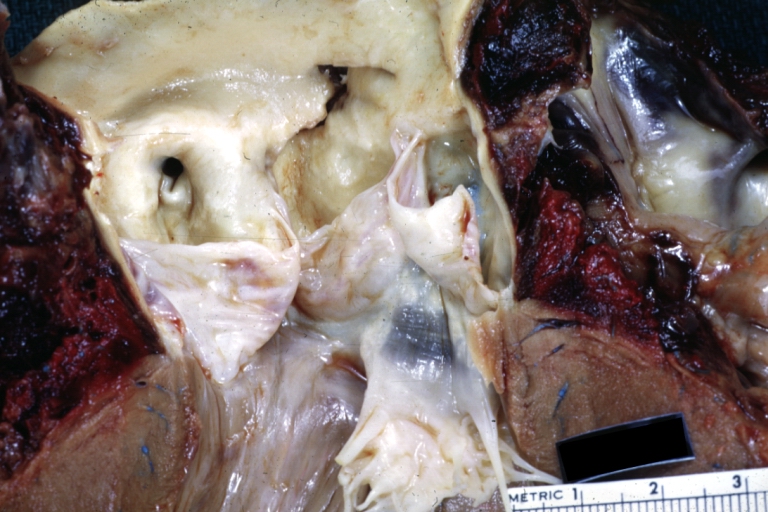
 Dissecting Aneurysm: Gross fixed tissue external view of heart aortic arch and descending aorta showing dilated first and second portion of arch from anterior projection.
Dissecting Aneurysm: Gross fixed tissue external view of heart aortic arch and descending aorta showing dilated first and second portion of arch from anterior projection. -
-



-
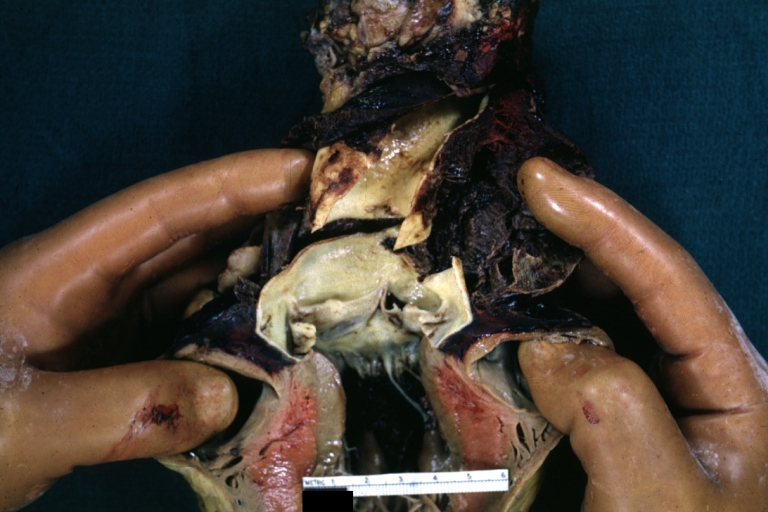
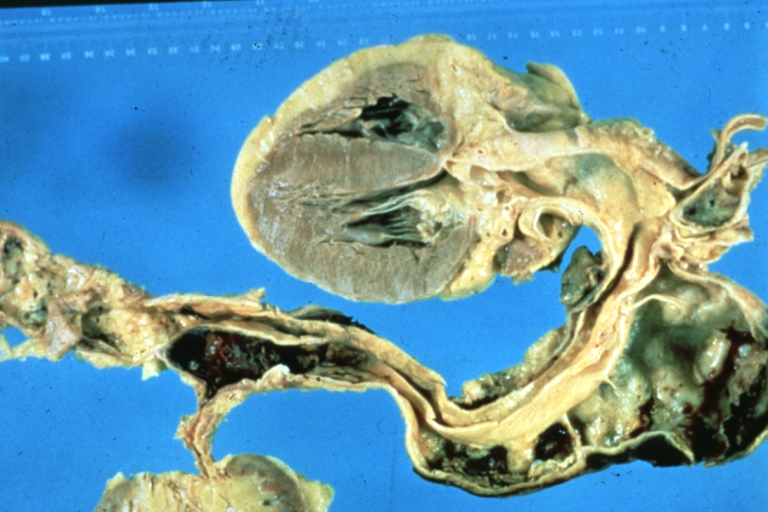
 Dissecting Aneurysm: Gross very good example dissected channel has been opened.
Dissecting Aneurysm: Gross very good example dissected channel has been opened. -
 Dissecting Aneurysm: Gross external view good appearance from adventitia.
Dissecting Aneurysm: Gross external view good appearance from adventitia. -
 Dissecting Aneurysm: Gross opened false channel.
Dissecting Aneurysm: Gross opened false channel.



-
 Dissecting Aneurysm: Gross good example dissection beginning at third portion aortic arch.
Dissecting Aneurysm: Gross good example dissection beginning at third portion aortic arch. -
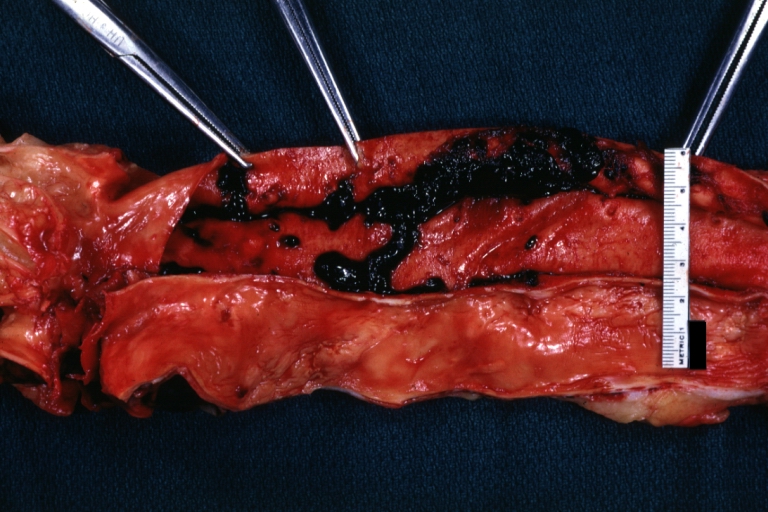
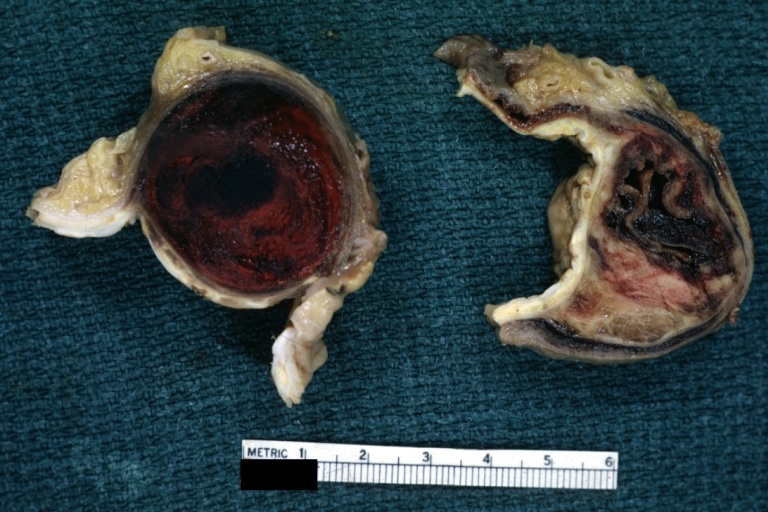 Dissecting Aneurysm: Gross cross sections showing thrombus in false lumen. True lumen has been opened longitudinally.
Dissecting Aneurysm: Gross cross sections showing thrombus in false lumen. True lumen has been opened longitudinally. -
 Dissecting Aneurysm: Gross shows origin just above aortic valve false channel shown in descending thoracic aorta (very good example).
Dissecting Aneurysm: Gross shows origin just above aortic valve false channel shown in descending thoracic aorta (very good example).



-
 Dissecting Aneurysm: Gross, an excellent example, starting just above the aortic valve with reflection of aorta to show the dissection tract and some thrombus
Dissecting Aneurysm: Gross, an excellent example, starting just above the aortic valve with reflection of aorta to show the dissection tract and some thrombus -
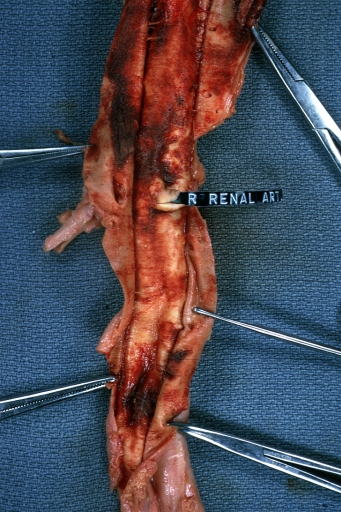
 Dissecting Aneurysm: Gross shows dilated aorta with extensive atherosclerosis dissection is seen, a small abdominal aorta atherosclerotic aneurysm is present good for association of dilation with dissection
Dissecting Aneurysm: Gross shows dilated aorta with extensive atherosclerosis dissection is seen, a small abdominal aorta atherosclerotic aneurysm is present good for association of dilation with dissection -
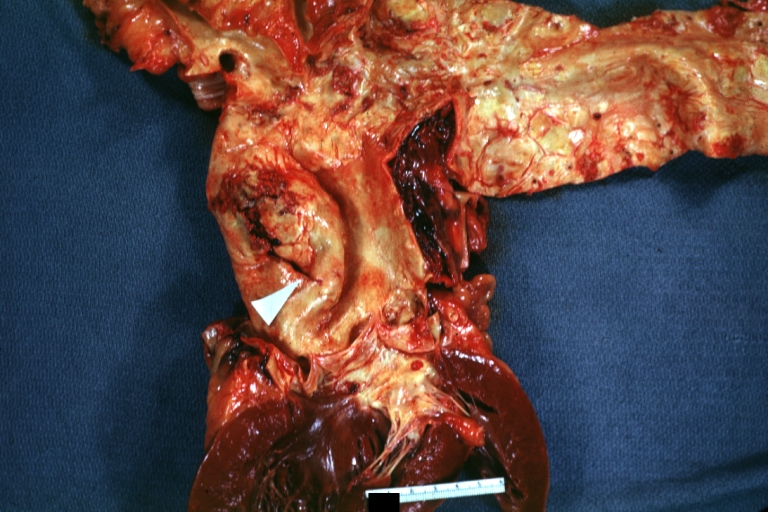 Dissecting Aneurysm: Gross arrow points to start of dissection in first portion aortic arch good but not the best example shows dilation
Dissecting Aneurysm: Gross arrow points to start of dissection in first portion aortic arch good but not the best example shows dilation -
 Dissecting Aneurysm: Gross, very good to show start of dissection above aortic valve and blood in false channel.
Dissecting Aneurysm: Gross, very good to show start of dissection above aortic valve and blood in false channel.




-
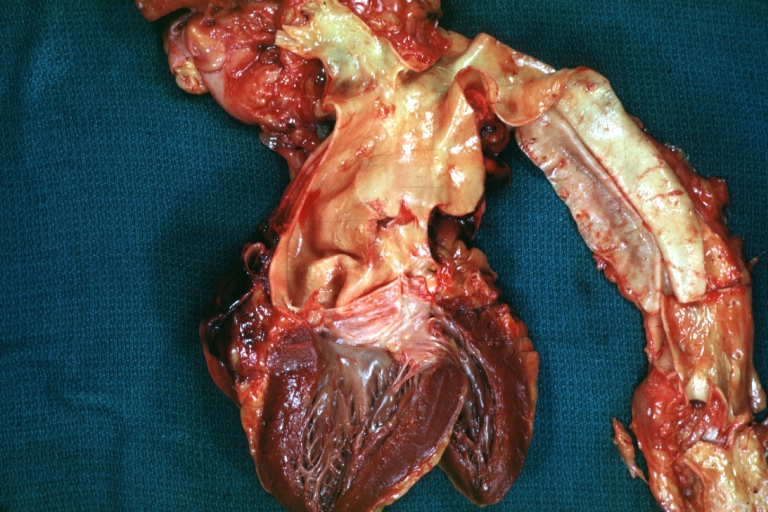
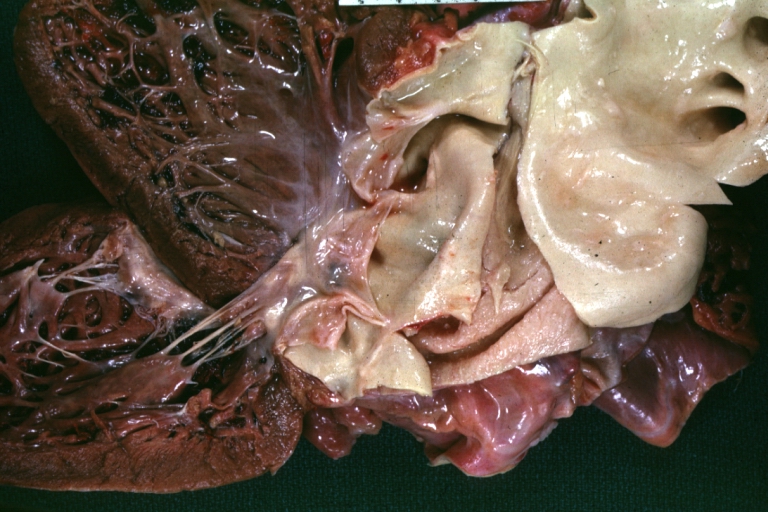
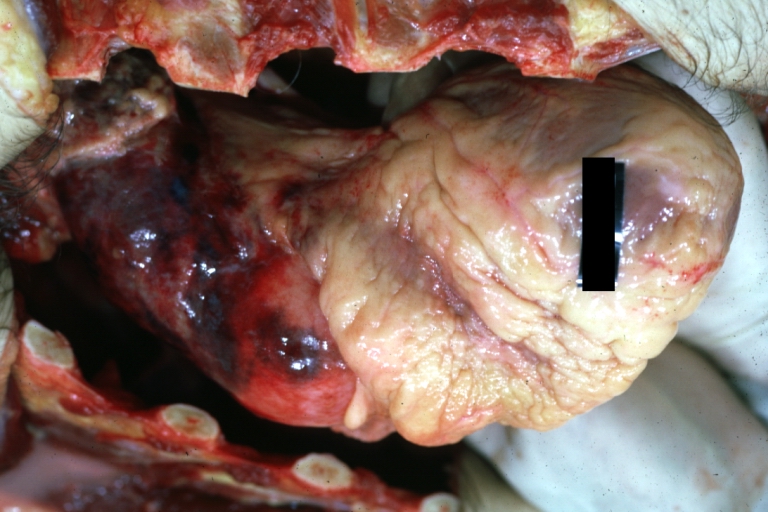
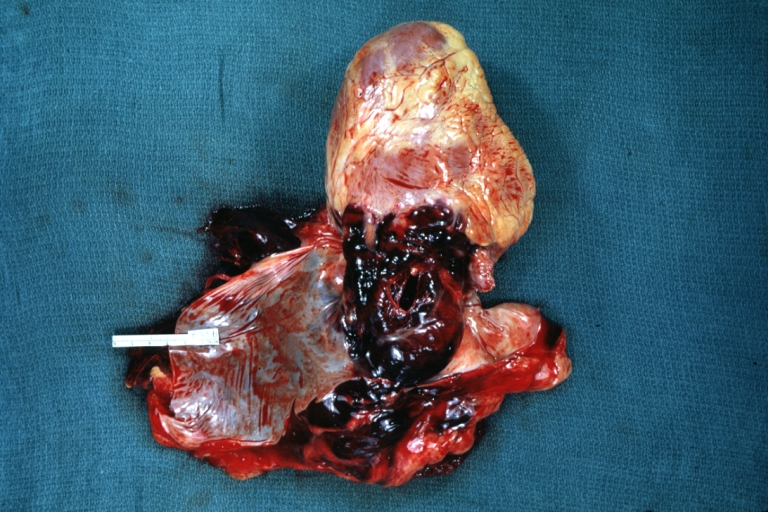 Dissecting Aneurysm: Gross, heart with root of aorta to show hemorrhage into pericardium (a very good example).
Dissecting Aneurysm: Gross, heart with root of aorta to show hemorrhage into pericardium (a very good example). -
-

-
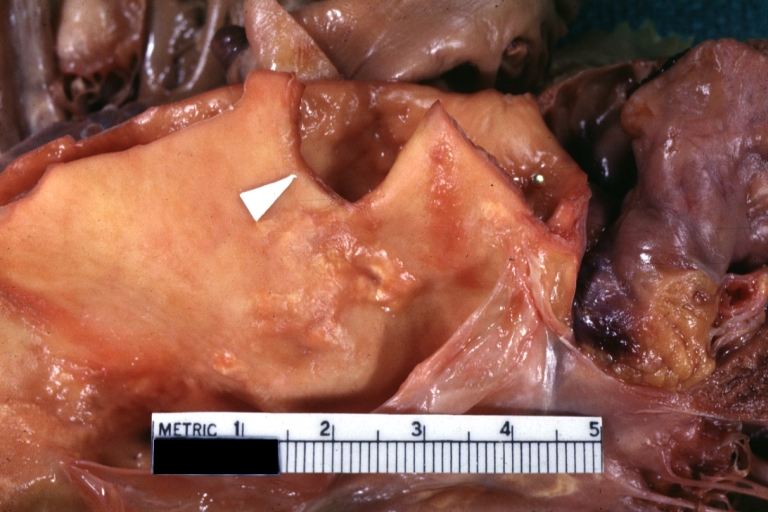
 Dissecting Aneurysm: Gross good example angular tear above aortic valve.
Dissecting Aneurysm: Gross good example angular tear above aortic valve.




-
 Dissecting Aneurysm: Gross good example of typical angular tear above aortic valve.
Dissecting Aneurysm: Gross good example of typical angular tear above aortic valve. -
 Dissecting Aneurysm: Gross, rather well shown dissection in first portion of the aortic arch
Dissecting Aneurysm: Gross, rather well shown dissection in first portion of the aortic arch -
 Dissecting Aneurysm: Gross, rather well shown dissection in first portion of the aortic arch
Dissecting Aneurysm: Gross, rather well shown dissection in first portion of the aortic arch -








-
 Dissecting Aneurysm: Gross, coagulum of blood in false channel
Dissecting Aneurysm: Gross, coagulum of blood in false channel -
 Dissecting Aneurysm: Gross, aortic valve area dissection (well shown, typical lesion)
Dissecting Aneurysm: Gross, aortic valve area dissection (well shown, typical lesion) -
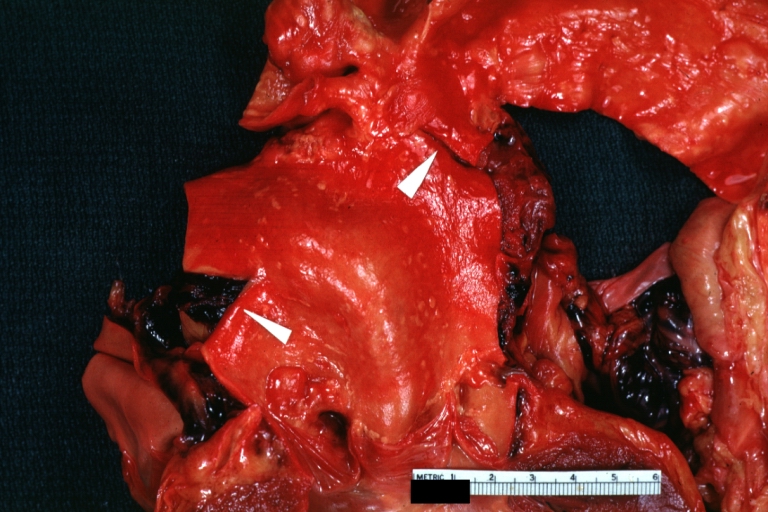
 Dissecting Aneurysm: Gross, external view of heart and first portion of aortic arch, annuloaortic ectasia, hemorrhage beneath adventitia is evidence of dissection
Dissecting Aneurysm: Gross, external view of heart and first portion of aortic arch, annuloaortic ectasia, hemorrhage beneath adventitia is evidence of dissection -
 Dissecting Aneurysm in a patient with Marfan’s syndrome
Dissecting Aneurysm in a patient with Marfan’s syndrome




-
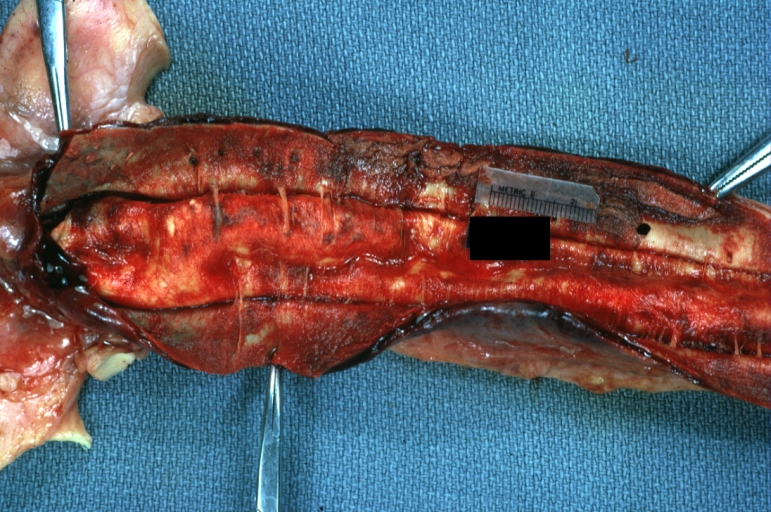
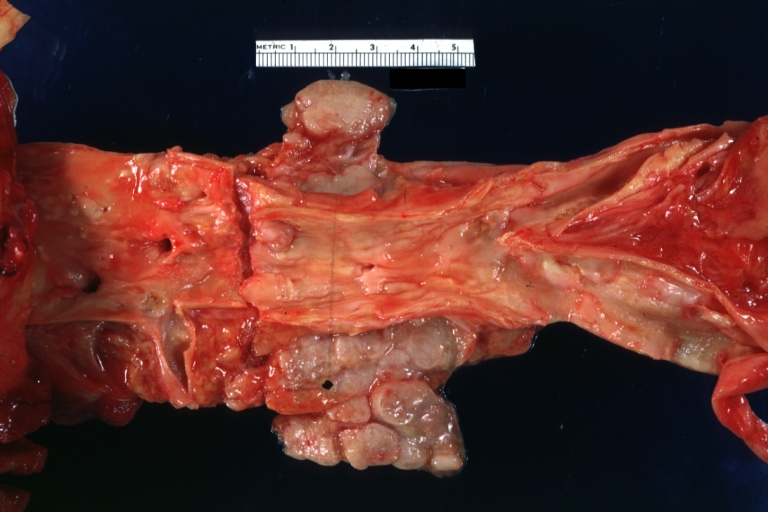
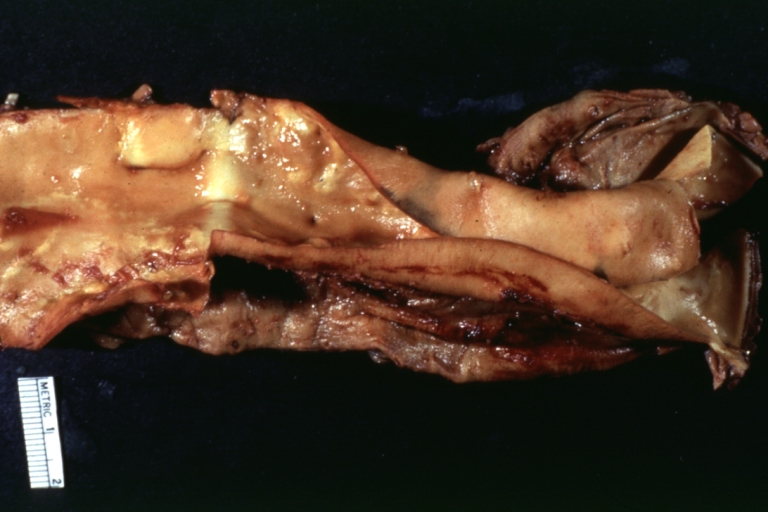
 Dissecting Aneurysm: Gross, fixed tissue, descending thoracic segment dissection opened to show the false channel. The true surface is also visible
Dissecting Aneurysm: Gross, fixed tissue, descending thoracic segment dissection opened to show the false channel. The true surface is also visible -
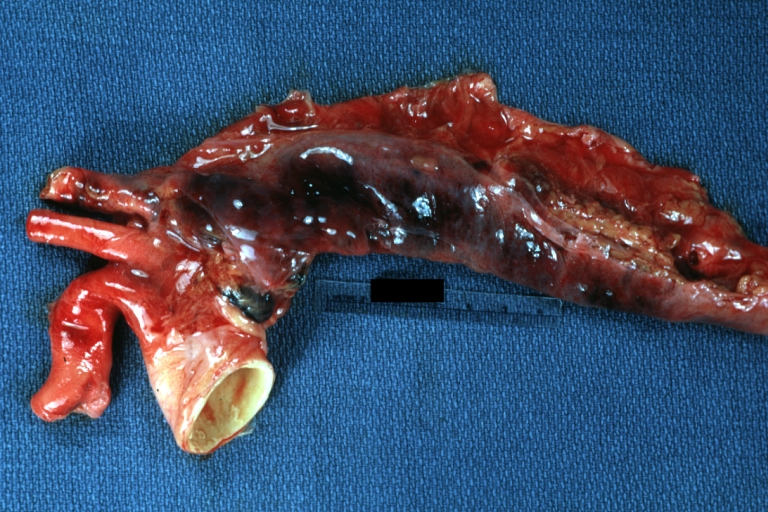
 Dissecting Aneurysm: Gross natural color descending aorta opened into false channel
Dissecting Aneurysm: Gross natural color descending aorta opened into false channel -
 Dissecting Aneurysm: Gross natural color close-up view of aortic valve and proximal aortic arch with ruptured intima rather good illustration of this lesion
Dissecting Aneurysm: Gross natural color close-up view of aortic valve and proximal aortic arch with ruptured intima rather good illustration of this lesion -
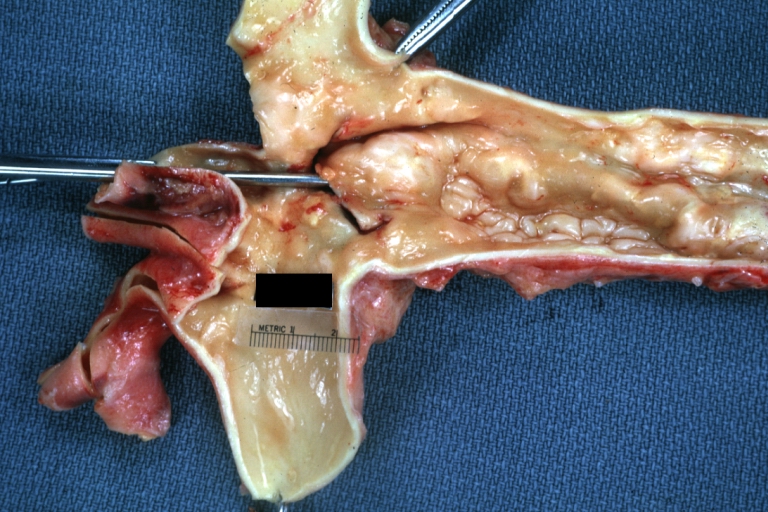
 Dissecting Aneurysm Chronic: Gross natural color first portion of aortic arch with intimal rent well shown with healed margins and view into false channel that shows a surface looking like atherosclerosis which is known to develop in a chronic dissection
Dissecting Aneurysm Chronic: Gross natural color first portion of aortic arch with intimal rent well shown with healed margins and view into false channel that shows a surface looking like atherosclerosis which is known to develop in a chronic dissection -






Microscopic Pathology
 |
References
- ↑ 1.0 1.1 Pinard, Amélie; Jones, Gregory T.; Milewicz, Dianna M. (2019). “Genetics of Thoracic and Abdominal Aortic Diseases”. Circulation Research. 124 (4): 588–606. doi:10.1161/CIRCRESAHA.118.312436. ISSN 0009-7330.
- ↑ Verhagen, Judith M.A.; Kempers, Marlies; Cozijnsen, Luc; Bouma, Berto J.; Duijnhouwer, Anthonie L.; Post, Jan G.; Hilhorst-Hofstee, Yvonne; Bekkers, Sebastiaan C.A.M.; Kerstjens-Frederikse, Wilhelmina S.; van Brakel, Thomas J.; Lambermon, Eric; Wessels, Marja W.; Loeys, Bart L.; Roos-Hesselink, Jolien W.; van de Laar, Ingrid M.B.H. (2018). “Expert consensus recommendations on the cardiogenetic care for patients with thoracic aortic disease and their first-degree relatives”. International Journal of Cardiology. 258: 243–248. doi:10.1016/j.ijcard.2018.01.145. ISSN 0167-5273.
- ↑ Case courtesy of Wikimedia Commons
Causes
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Vendhan Ramanujam M.B.B.S [2] Sahar Memar Montazerin, M.D.[3]
Overview
Atherosclerosis and hypertension are associated with spontaneous aortic dissection, while blunt trauma and sudden deceleration in a motor vehicle accident are major causes of traumatic aortic dissection.
Causes
Common Causes
The most common causes of aortic dissection include:[1][2][3][4][5]
- Atherosclerosis
- Chest trauma
- Chronic hypertension
- Complication of cardiac procedures
- Connective tissue disorders
- Vasculitis
Causes by Organ System
- For more information on potential risk factors for the development of aortic dissection click here.
References
- ↑ Penn JL, Martindale JL, Milne LW, Marill KA (2015). “Aortic dissection associated with blunt chest trauma diagnosed by elevated D-dimer”. Int J Surg Case Rep. 10: 76–9. doi:10.1016/j.ijscr.2015.03.027. PMC 4429846. PMID 25805614.
- ↑ Weissmann-Brenner A, Schoen R, Divon MY (2004). “Aortic dissection in pregnancy”. Obstet Gynecol. 103 (5 Pt 2): 1110–3. doi:10.1097/01.AOG.0000124984.82336.43. PMID 15121626.
- ↑ Brooke V, Goswami S, Mohanty A, Kasi PM (2012). “Aortic dissection and renal failure in a patient with severe hypothyroidism”. Case Rep Med. 2012: 842562. doi:10.1155/2012/842562. PMC 3399550. PMID 22829842.
- ↑ “Classification of diabetic retinopathy from fluorescein angiograms. ETDRS report number 11. Early Treatment Diabetic Retinopathy Study Research Group”. Ophthalmology. 98 (5 Suppl): 807–22. 1991. PMID 2062514.
- ↑ Cury M, Zeidan F, Lobato AC (2013). “Aortic disease in the young: genetic aneurysm syndromes, connective tissue disorders, and familial aortic aneurysms and dissections”. Int J Vasc Med. 2013: 267215. doi:10.1155/2013/267215. PMC 3557640. PMID 23401778.
- ↑ Larson, Eric W.; Edwards, William D. (1984). “Risk factors for aortic dissection: A necropsy study of 161 cases”. The American Journal of Cardiology. 53 (6): 849–855. doi:10.1016/0002-9149(84)90418-1. ISSN 0002-9149.
- ↑ Januzzi, James L; Isselbacher, Eric M; Fattori, Rossella; Cooper, Jeanna V; Smith, Dean E; Fang, Jianming; Eagle, Kim A; Mehta, Rajendra H; Nienaber, Christoph A; Pape, Linda A (2004). “Characterizing the young patient with aortic dissection: results from the international registry of aortic dissection (IRAD)”. Journal of the American College of Cardiology. 43 (4): 665–669. doi:10.1016/j.jacc.2003.08.054. ISSN 0735-1097.
- ↑ “Correspondence”. The Annals of Thoracic Surgery. 67 (2): 593. 1999. doi:10.1016/S0003-4975(99)00037-5. ISSN 0003-4975.
- ↑ Losenno, Katie L.; Goodman, Robert L.; Chu, Michael W. A. (2012). “Bicuspid Aortic Valve Disease and Ascending Aortic Aneurysms: Gaps in Knowledge”. Cardiology Research and Practice. 2012: 1–16. doi:10.1155/2012/145202. ISSN 2090-8016.
- ↑ Senaha S, Uezu T, Shimoji M, Akasaki M (March 2015). “[Stanford type B aortic dissection associated with coarctation of the aorta]”. Kyobu Geka (in Japanese). 68 (3): 184–7. PMID 25743550.
- ↑ Dioguardi GS, Pimenta J, Knoplich J, Ghorayeb N, Ramos LR, Giannini SD (June 1994). “[Risk factors for cardiovascular diseases in physicians. Preliminary data from the VIDAM Project of the Paulista Medical Association]”. Arq. Bras. Cardiol. (in Portuguese). 62 (6): 383–8. PMID 7826227.
- ↑ Caglayan, Ahmet Okay; Dundar, Munis (2009). “Inherited diseases and syndromes leading to aortic aneurysms and dissections”. European Journal of Cardio-Thoracic Surgery. 35 (6): 931–940. doi:10.1016/j.ejcts.2009.01.006. ISSN 1010-7940.
- ↑ “Acute aortic dissection: pathogenesis, risk factors and diagnosis”. Swiss Medical Weekly. 147 (3334). 2017. doi:10.4414/smw.2017.14489. ISSN 1424-7860.
- ↑ Increased maternal cardiovascular mortality associated with pregnancy in women with Turner syndrome.
Differentiating Aortic Dissection from other Diseases
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]Associate Editor(s)-in-Chief: Sahar Memar Montazerin, M.D.[2]Cafer Zorkun, M.D., Ph.D. [3]
Overview
Aortic dissection is a life threatening entity that must be distinguished from other life threatening entities such as cardiac tamponade, cardiogenic shock, myocardial infarction, and pulmonary embolism. An aortic aneurysm is not synonymous with aortic dissection. Aneurysms are defined as a localized permanent dilation of the aorta to a diameter > 50% of normal.
Differentiating Aortic Dissection from other Diseases
- Aortic intramural hematoma
- Penetrating atherosclerotic aortic ulcer
- Aortic regurgitation
- Aortic stenosis
- Cardiac tamponade
- Cardiogenic shock
- Gastroenteritis
- Hemorrhagic shock
- Hernias
- Hypertensive emergencies
- Hypovolemic shock
- Mechanical back pain
- Myocardial infarction
- Myocarditis
- Myopathies
- Pancreatitis
- Pericarditis
- Peripheral vascular injuries
- Pleural effusion
- Pulmonary embolism
- Thoracic outlet syndrome
Differentiating Aortic Dissection from other Diseases on the Basis of Chest Pain
The following table outlines the major differential diagnoses of Chest Pain..[1][2][3][4][5][6][7][8][9][10][11][12][13][14][15][16][17][18][19][20][21][22][23][24][25][26][27][28][29][30][31][32][33][34][35][36]
Abbreviations: ABG (arterial blood gas); ACE (angiotensin converting enzyme); BMI (body mass index); CBC (complete blood count); CSF (cerebrospinal fluid); CXR (chest X-ray); ECG (electrocardiogram); FEF (forced expiratory flow rate); FEV1 (forced expiratory volume); FVC (forced vital capacity); JVD (jugular vein distention); MCV (mean corpuscular volume); Plt (platelet); RV (residual volume); SIADH (syndrome of inappropriate antidiuretic hormone); TSH (thyroid stimulating hormone); Vt (tidal volume); WBC (white blood cell); Coronary CT angiography (CCTA); multidetector row scanners (MDCT); Cardiovascular magnetic resonance — CMRI; Myocardial perfusion imaging (MPI); single-photon emission CT (SPECT); Positron emission tomography (PET) scanning; Magnetic resonance (MR) angiography, Computed tomographic (CT) angiography, and Transesophageal echocardiography (TEE), late gadolinium enhancement (LGE); right ventricular hypertrophy (RVH), right atrial enlargement (RAE), functional tricuspid regurgitation (TR), Pulmonary artery systolic pressure (PASP; adenosine deaminase (ADA); Serum amyloid A (SAA), soluble interleukin-2 receptor (sIL2R); High-resolution CT (HRCT) scanning
| Differentials on the basis of Etiology | Disease | Clinical manifestations | Diagnosis | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Symptoms | Risk factors | Physical exam | Lab Findings | EKG | Imaging | Gold standard | |||||||||
| Onset | Duration | Quality of Pain | Cough | Fever | Dyspnea | Weight loss | Associated Features | ||||||||
| Stable Angina[37] | Sudden (acute) | 2-10 minutes |
|
– | – | +/- | – |
|
|
|
|
|
|||
| Unstable Angina[38][39][40] | Acute | 10-20 minutes |
|
– | – | + | – |
|
|
|
| ||||
| Myocardial Infarction[1][2][3][4] | Acute | Commonly > 20 minutes |
|
– | – | + | – |
|
|
|
|
| |||
| Cardiac | Vasospastic/ Prinzmetal/ Variant Angina[41][42] | Gradual in onset and offset | Episodic, gradual in onset and offset |
|
– | – | + | – |
|
|
|
|
|||
| Aortic Dissection[43][44] | Sudden severe progressive pain (common) or chronic (rare) | Variable |
|
– | – | + | – |
|
|
|
|
|
| ||
| Aortic intramural hematoma | Sudden severe progressive pain (common) or chronic (rare) | Variable |
|
– | – | + | – |
|
|
|
|
|
| ||
| Penetrating atherosclerotic aortic ulcer[45][46][47] | Sudden severe pain | Variable |
|
– | – | + | – |
|
_ |
_ |
|
| |||
| Pericarditis[48][49][50] | Acute or subacute | May last for hours to days |
|
+ | + | + | – |
|
|
|
|
||||
| Pericardial Tamponade[51][52] | Acute or subacute | May last for hours to days |
|
+/- | + | + | – |
|
EKG findings:
|
|
|||||
| Myocarditis[53][54][55] | Acute or subacute | Variable |
|
+/- | + | + | – |
|
|
|
|
||||
| Hypertrophic cardiomyopathy[56][57][58] | Acute or subacute | Variable | Typical or atypical chest pain | – | – | + | – |
|
|
|
Non-specific |
|
|
Genetic testing for HCM | |
| Stress (takotsubo) | Acute | Commonly > 20 minutes |
|
– | – | + | – |
|
Stress |
|
|
|
|||
| Aortic Stenosis[63][64][65] | Acute, recurrent episodes of angina | 2-10 minutes |
|
– | – | + | – |
|
|
|
|
|
|||
| Heart Failure[66][67][68] | Subacute or chronic | Variable |
|
+ | +/- | + | + | Dyslipidemia, hypertension, smoking, family history of premature disease, and diabetes |
|
|
|
||||
| Differentials on the basis of Etiology | Disease | Clinical manifestations | Diagnosis | ||||||||||||
| Symptoms | Risk factors | Physical exam | Lab Findings | EKG | Imaging | Gold standard | |||||||||
| Onset | Duration | Quality of Pain | Cough | Fever | Dyspnea | Weight loss | Associated Features | ||||||||
| Pulmonary | Pulmonary Embolism[69][70] | Acute | May last minutes to hours |
|
+ | +/- | + | – |
|
Hormone replacement therapy
Cancer Oral contraceptive pills Stroke Pregnancy Postpartum Prior history of VTE Thrombophilia |
|
|
|
||
| Spontaneous Pneumothorax[71][72] | Acute | May last minutes to hours |
|
– | – | + | – |
|
|
|
|
|
| ||
| Tension Pneumothorax[73][74] | Acute | May last minutes to hours |
|
– | – | + | – |
|
|
|
|
||||
| Pneumonia[75][76][77] | Acute or chronic | Variable |
|
+ | + | + | +/- |
|
|
|
|
|
|||
| Tracheitis/ Bronchitis[78][79][80][81] | Acute | Variable |
|
+ | + | + | – |
|
|
||||||
| Pleuritis | Acute or subacute or chronic | May last minutes to hours |
|
+ | + | + | – |
|
|
|
|
|
|||
| Pulmonary Hypertension[82][83][84] | Acute or subacute or chronic | Variable |
|
+ | – | + | – |
|
|
|
|
|
|||
| Pleural Effusion[85][86][87] | Acute or subacute or chronic | Variable |
|
+ | +/- | + | +/- |
|
|
|
|
||||
| Asthma & COPD[88][89][90][91] | Acute or subacute or chronic | Variable |
|
+ | +/- | + | +/- |
|
|
|
|||||
| Pulmonary Malignancy[92][93][94][95] | Chronic | Variable |
|
+ | +/- | + | + |
|
|
|
|
||||
| Sarcoidosis[96][97][98][99] | Chronic | Days to week |
|
+ | – | + | + |
|
|
|
|
|
|
| |
| Acute chest syndrome (Sickle cell anemia)[100][101][102] | Acute | May last minutes to hours |
|
+ | +/- | + | – |
|
|
|
|
|
— | ||
| Differentials on the basis of Etiology | Disease | Clinical manifestations | Diagnosis | ||||||||||||
| Symptoms | Risk factors | Physical exam | Lab Findings | EKG | Imaging | Gold standard | |||||||||
| Onset | Duration | Quality of Pain | Cough | Fever | Dyspnea | Weight loss | Associated Features | ||||||||
| Gastrointestinal | GERD, Peptic Ulcer[103][104][105] | Acute |
|
|
+/- | – | – | +/- |
|
|
|
|
|
| |
| Diffuse Esophageal Spasm[106][107][108][109] | Acute |
|
|
+ | – | +/- | +/- |
|
— | — |
|
|
|
||
| Esophagitis[110][111][112] | Acute | Variable |
|
+ | + | – | +/- |
|
|
|
|||||
| Eosinophilic Esophagitis[113][114][115][116][117][118] | Chronic | Variable |
|
+ | – | – | – |
|
|
|
|
| |||
| Esophageal Perforation[6] | Acute | Minutes to hours |
|
– | +/- | + | – |
|
|
|
|
|
| ||
| Mediastinitis[119][120][121][122] | Acute, Chronic | Variable |
|
+/- | + | + | – |
|
|
|
|
|
|
CT scan | |
| Cholelithiasis[123][124][125][126] | Acute, subacute | Minutes to hours |
|
– | +/- | – | – |
|
•Clinical acute cholangitis •A serum bilirubin greater than 4 mg/dL (68 micromol/L) |
|
|
|
|
Endoscopic ultrasound and MECP | |
| Pancreatitis[127][128][129][130][131] | Acute, Chronic | Variable |
|
– | + | + | +/- |
|
|
|
|
| |||
| Sliding Hiatal Hernia[132][133][134] | Acute | Variable |
|
+ | – | + | – |
|
|
|
|
|
|
| |
| Musculoskeletal | Costosternal syndromes (costochondritis)[135][136][137][138] | Acute, subacute | Days to weeks |
|
– | + | – | – |
|
|
|
|
|
|
Pain by palpation of tender areas |
| Lower rib pain syndromes[139] | Chronic | Variable |
|
– | – | + | – |
|
— |
|
|
|
|
— | |
| Sternalis syndrome | Chronic | Variable | Pressure like pain
|
– | – | – | – |
|
|
|
|
|
| ||
| Tietze’s syndrome[140] | Acute | Weeks | Pressure like pain over
|
– | – | – | – |
|
|
|
|
|
|
| |
| Xiphoidalgia[141] | Acute | Variable | Pressure like pain over
|
– | – | – | – |
|
|
|
|
|
|
| |
| Spontaneous sternoclavicular subluxation[142] | Acute, Chronic | Variable | Aching pain over Sternoclavicular joint | – | – | – | – |
|
|
|
|
|
|
| |
| Differentials on the basis of Etiology | Disease | Clinical manifestations | Diagnosis | ||||||||||||
| Symptoms | Risk factors | Physical exam | Lab workup | EKG | Imaging | Gold standard | |||||||||
| Onset | Duration | Quality of Pain | Cough | Fever | Dyspnea | Weight loss | Associated Features | ||||||||
| Rheumatic | Fibromyalgia[143][144][145] | Chronic | Variable | – | – | + | – | — |
|
|
|
— | — | ||
| Rheumatoid arthritis[146] | Chronic | Years | Symmetrical joint pain in
|
– | + | – | + |
|
|
|
|
|
|
— | |
| Ankylosing spondylitis[147][148][149][150] | Chronic | Years | Intermittent pain in
|
– | – | – | – |
|
|
|
|
|
|
| |
| Psoriatic arthritis[149] | Chronic | Years | Asymmetrical intermittent pain in
|
– | – | – | – |
|
|
Non specific |
|
|
| ||
| Sternocostoclavicular hyperostosis (SAPHO syndrome)[149][151][152][153][154] | Chronic | Years | Recurrent and multifocal pain in
Sternoclavicular joint |
– | + | – | – |
|
Positive family history of:
|
|
|
|
|
| |
| Systemic lupus erythematosus[155] [156][157] | Chronic | Years | +/- | + | + | + |
|
|
|
| |||||
| Relapsing polychondritis[158] | Chronic | Years | Intermittent pain in: | + | + | + | + |
|
|
|
|
|
| ||
| Psychiatric | Panic attack/ Disorder[159][7][160] | Acute or subacute or chronic | Variable | Variable | + | – | + | – |
|
|
|
|
|
|
— |
|
Others |
Substance abuse | Acute (hours) | Minutes to hours | Pressure like pain in the center of chest | + | + | + | + |
|
|
|
|
— |
| |
| Herpes Zoster[164][165][166] | Acute or Chronic | Variable | Burning pain on
|
– | + | – | – |
|
|
|
|
|
|
| |
References
- ↑ 1.0 1.1 Svavarsdóttir AE, Jónasson MR, Gudmundsson GH, Fjeldsted K (June 1996). “Chest pain in family practice. Diagnosis and long-term outcome in a community setting”. Can Fam Physician. 42: 1122–8. PMC 2146490. PMID 8704488.
- ↑ 2.0 2.1 Klinkman MS, Stevens D, Gorenflo DW (April 1994). “Episodes of care for chest pain: a preliminary report from MIRNET. Michigan Research Network”. J Fam Pract. 38 (4): 345–52. PMID 8163958.
- ↑ 3.0 3.1 Bösner S, Becker A, Haasenritter J, Abu Hani M, Keller H, Sönnichsen AC, Karatolios K, Schaefer JR, Seitz G, Baum E, Donner-Banzhoff N (2009). “Chest pain in primary care: epidemiology and pre-work-up probabilities”. Eur J Gen Pract. 15 (3): 141–6. doi:10.3109/13814780903329528. PMID 19883149.
- ↑ 4.0 4.1 Ebell MH (March 2011). “Evaluation of chest pain in primary care patients”. Am Fam Physician. 83 (5): 603–5. PMID 21391528.
- ↑ von Kodolitsch Y, Schwartz AG, Nienaber CA (October 2000). “Clinical prediction of acute aortic dissection”. Arch. Intern. Med. 160 (19): 2977–82. PMID 11041906.
- ↑ 6.0 6.1 Pate JW, Walker WA, Cole FH, Owen EW, Johnson WH (May 1989). “Spontaneous rupture of the esophagus: a 30-year experience”. Ann. Thorac. Surg. 47 (5): 689–92. PMID 2730190.
- ↑ 7.0 7.1 Fleet RP, Dupuis G, Marchand A, Burelle D, Beitman BD (October 1994). “Panic disorder, chest pain and coronary artery disease: literature review”. Can J Cardiol. 10 (8): 827–34. PMID 7954018.
- ↑ Bass C, Chambers JB, Kiff P, Cooper D, Gardner WN (December 1988). “Panic anxiety and hyperventilation in patients with chest pain: a controlled study”. Q. J. Med. 69 (260): 949–59. PMID 3270082.
- ↑ Evans DW, Lum LC (January 1977). “Hyperventilation: An important cause of pseudoangina”. Lancet. 1 (8004): 155–7. PMID 64694.
- ↑ Ros E, Armengol X, Grande L, Toledo-Pimentel V, Lacima G, Sanz G (July 1997). “Chest pain at rest in patients with coronary artery disease. Myocardial ischemia, esophageal dysfunction, or panic disorder?”. Dig. Dis. Sci. 42 (7): 1344–53. PMID 9246027.
- ↑ Ben Freedman S, Tennant CC (April 1998). “Panic disorder and coronary artery spasm”. Med. J. Aust. 168 (8): 376–7. PMID 9594945.
- ↑ Smoller JW, Pollack MH, Wassertheil-Smoller S, Jackson RD, Oberman A, Wong ND, Sheps D (October 2007). “Panic attacks and risk of incident cardiovascular events among postmenopausal women in the Women’s Health Initiative Observational Study”. Arch. Gen. Psychiatry. 64 (10): 1153–60. doi:10.1001/archpsyc.64.10.1153. PMID 17909127.
- ↑ Mehta NJ, Khan IA (November 2002). “Cardiac Munchausen syndrome”. Chest. 122 (5): 1649–53. PMID 12426266.
- ↑ Swap CJ, Nagurney JT (November 2005). “Value and limitations of chest pain history in the evaluation of patients with suspected acute coronary syndromes”. JAMA. 294 (20): 2623–9. doi:10.1001/jama.294.20.2623. PMID 16304077.
- ↑ Marcus GM, Cohen J, Varosy PD, Vessey J, Rose E, Massie BM, Chatterjee K, Waters D (January 2007). “The utility of gestures in patients with chest discomfort”. Am. J. Med. 120 (1): 83–9. doi:10.1016/j.amjmed.2006.05.045. PMID 17208083.
- ↑ Verdon F, Burnand B, Herzig L, Junod M, Pécoud A, Favrat B (September 2007). “Chest wall syndrome among primary care patients: a cohort study”. BMC Fam Pract. 8: 51. doi:10.1186/1471-2296-8-51. PMC 2072948. PMID 17850647.
- ↑ Davies HA, Jones DB, Rhodes J, Newcombe RG (December 1985). “Angina-like esophageal pain: differentiation from cardiac pain by history”. J. Clin. Gastroenterol. 7 (6): 477–81. PMID 4086742.
- ↑ Panju AA, Hemmelgarn BR, Guyatt GH, Simel DL (October 1998). “The rational clinical examination. Is this patient having a myocardial infarction?”. JAMA. 280 (14): 1256–63. PMID 9786377.
- ↑ Berger JP, Buclin T, Haller E, Van Melle G, Yersin B (March 1990). “Right arm involvement and pain extension can help to differentiate coronary diseases from chest pain of other origin: a prospective emergency ward study of 278 consecutive patients admitted for chest pain”. J. Intern. Med. 227 (3): 165–72. PMID 2313224.
- ↑ Yelland MJ (September 2001). “Back, chest and abdominal pain. How good are spinal signs at identifying musculoskeletal causes of back, chest or abdominal pain?”. Aust Fam Physician. 30 (9): 908–12. PMID 11676323.
- ↑ Chan S, Maurice AP, Davies SR, Walters DL (October 2014). “The use of gastrointestinal cocktail for differentiating gastro-oesophageal reflux disease and acute coronary syndrome in the emergency setting: a systematic review”. Heart Lung Circ. 23 (10): 913–23. doi:10.1016/j.hlc.2014.03.030. PMID 24791662.
- ↑ Henrikson CA, Howell EE, Bush DE, Miles JS, Meininger GR, Friedlander T, Bushnell AC, Chandra-Strobos N (December 2003). “Chest pain relief by nitroglycerin does not predict active coronary artery disease”. Ann. Intern. Med. 139 (12): 979–86. PMID 14678917.
- ↑ Pryor DB, Harrell FE, Lee KL, Califf RM, Rosati RA (November 1983). “Estimating the likelihood of significant coronary artery disease”. Am. J. Med. 75 (5): 771–80. PMID 6638047.
- ↑ Buntinx F, Knockaert D, Bruyninckx R, de Blaey N, Aerts M, Knottnerus JA, Delooz H (December 2001). “Chest pain in general practice or in the hospital emergency department: is it the same?”. Fam Pract. 18 (6): 586–9. PMID 11739341.
- ↑ Tierney WM, Roth BJ, Psaty B, McHenry R, Fitzgerald J, Stump DL, Anderson FK, Ryder KW, McDonald CJ, Smith DM (July 1985). “Predictors of myocardial infarction in emergency room patients”. Crit. Care Med. 13 (7): 526–31. PMID 4006491.
- ↑ Sequist TD, Marshall R, Lampert S, Buechler EJ, Lee TH (November 2006). “Missed opportunities in the primary care management of early acute ischemic heart disease”. Arch. Intern. Med. 166 (20): 2237–43. doi:10.1001/archinte.166.20.2237. PMID 17101942.
- ↑ Norell M, Lythall D, Coghlan G, Cheng A, Kushwaha S, Swan J, Ilsley C, Mitchell A (January 1992). “Limited value of the resting electrocardiogram in assessing patients with recent onset chest pain: lessons from a chest pain clinic”. Br Heart J. 67 (1): 53–6. PMC 1024701. PMID 1739527.
- ↑ Law K, Elley R, Tietjens J, Mann S (July 2006). “Troponin testing for chest pain in primary healthcare: a survey of its use by general practitioners in New Zealand”. N. Z. Med. J. 119 (1238): U2082. PMID 16868579.
- ↑ Wilhelmsen L, Rosengren A, Hagman M, Lappas G (July 1998). ““Nonspecific” chest pain associated with high long-term mortality: results from the primary prevention study in Göteborg, Sweden”. Clin Cardiol. 21 (7): 477–82. PMID 9669056.
- ↑ Ruigómez A, Rodríguez LA, Wallander MA, Johansson S, Jones R (April 2006). “Chest pain in general practice: incidence, comorbidity and mortality”. Fam Pract. 23 (2): 167–74. doi:10.1093/fampra/cmi124. PMID 16461444.
- ↑ Robinson JG, Wallace R, Limacher M, Sato A, Cochrane B, Wassertheil-Smoller S, Ockene JK, Blanchette PL, Ko MG (December 2006). “Elderly women diagnosed with nonspecific chest pain may be at increased cardiovascular risk”. J Womens Health (Larchmt). 15 (10): 1151–60. doi:10.1089/jwh.2006.15.1151. PMID 17199456.
- ↑ Geraldine McMahon C, Yates DW, Hollis S (February 2008). “Unexpected mortality in patients discharged from the emergency department following an episode of nontraumatic chest pain”. Eur J Emerg Med. 15 (1): 3–8. doi:10.1097/MEJ.0b013e32827b14cd. PMID 18180659.
- ↑ Yelland M, Cayley WE, Vach W (March 2010). “An algorithm for the diagnosis and management of chest pain in primary care”. Med. Clin. North Am. 94 (2): 349–74. doi:10.1016/j.mcna.2010.01.011. PMID 20380960.
- ↑ Wang WH, Huang JQ, Zheng GF, Wong WM, Lam SK, Karlberg J, Xia HH, Fass R, Wong BC (June 2005). “Is proton pump inhibitor testing an effective approach to diagnose gastroesophageal reflux disease in patients with noncardiac chest pain?: a meta-analysis”. Arch. Intern. Med. 165 (11): 1222–8. doi:10.1001/archinte.165.11.1222. PMID 15956000.
- ↑ Borzecki AM, Pedrosa MC, Prashker MJ (March 2000). “Should noncardiac chest pain be treated empirically? A cost-effectiveness analysis”. Arch. Intern. Med. 160 (6): 844–52. PMID 10737285.
- ↑ Wertli MM, Ruchti KB, Steurer J, Held U (November 2013). “Diagnostic indicators of non-cardiovascular chest pain: a systematic review and meta-analysis”. BMC Med. 11: 239. doi:10.1186/1741-7015-11-239. PMC 4226211. PMID 24207111.
- ↑ Fihn SD, Gardin JM, Abrams J, Berra K, Blankenship JC, Dallas AP, Douglas PS, Foody JM, Gerber TC, Hinderliter AL, King SB, Kligfield PD, Krumholz HM, Kwong RY, Lim MJ, Linderbaum JA, Mack MJ, Munger MA, Prager RL, Sabik JF, Shaw LJ, Sikkema JD, Smith CR, Smith SC, Spertus JA, Williams SV, Anderson JL (December 2012). “2012 ACCF/AHA/ACP/AATS/PCNA/SCAI/STS guideline for the diagnosis and management of patients with stable ischemic heart disease: a report of the American College of Cardiology Foundation/American Heart Association task force on practice guidelines, and the American College of Physicians, American Association for Thoracic Surgery, Preventive Cardiovascular Nurses Association, Society for Cardiovascular Angiography and Interventions, and Society of Thoracic Surgeons”. Circulation. 126 (25): e354–471. doi:10.1161/CIR.0b013e318277d6a0. PMID 23166211.
- ↑ Tatum JL, Jesse RL, Kontos MC, Nicholson CS, Schmidt KL, Roberts CS, Ornato JP (January 1997). “Comprehensive strategy for the evaluation and triage of the chest pain patient”. Ann Emerg Med. 29 (1): 116–25. PMID 8998090.
- ↑ Ornato JP (August 1999). “Chest pain emergency centers: improving acute myocardial infarction care”. Clin Cardiol. 22 (8 Suppl): IV3–9. PMID 10492848.
- ↑ Gibler WB (August 1995). “Evaluation of chest pain in the emergency department”. Ann. Intern. Med. 123 (4): 315, author reply 317–8. PMID 7611601.
- ↑ PRINZMETAL M, KENNAMER R, MERLISS R, WADA T, BOR N (September 1959). “Angina pectoris. I. A variant form of angina pectoris; preliminary report”. Am. J. Med. 27: 375–88. PMID 14434946.
- ↑ Kaski JC, Crea F, Meran D, Rodriguez L, Araujo L, Chierchia S, Davies G, Maseri A (December 1986). “Local coronary supersensitivity to diverse vasoconstrictive stimuli in patients with variant angina”. Circulation. 74 (6): 1255–65. PMID 3779913.
- ↑ Takagi H, Ando T, Umemoto T (November 2017). “Meta-Analysis of Circadian Variation in the Onset of Acute Aortic Dissection”. Am. J. Cardiol. 120 (9): 1662–1666. doi:10.1016/j.amjcard.2017.07.067. PMID 28847596.
- ↑ Kojima S, Sumiyoshi M, Nakata Y, Daida H (March 2002). “Triggers and circadian distribution of the onset of acute aortic dissection”. Circ. J. 66 (3): 232–5. PMID 11922269.
- ↑ Eggebrecht, Holger; Baumgart, Dietrich; Schmermund, Axel; Herold, Ulf; Hunold, Peter; Jakob, Heinz; Erbel, Raimund (2003). “Penetrating atherosclerotic ulcer of the aorta: treatment by endovascular stent-graft placement”. Current Opinion in Cardiology. 18 (6): 431–435. doi:10.1097/00001573-200311000-00002. ISSN 0268-4705.
- ↑ Bossone, Eduardo; LaBounty, Troy M; Eagle, Kim A (2018). “Acute aortic syndromes: diagnosis and management, an update”. European Heart Journal. 39 (9): 739–749d. doi:10.1093/eurheartj/ehx319. ISSN 0195-668X.
- ↑ DeMartino, Randall R.; Sen, Indrani; Huang, Ying; Bower, Thomas C.; Oderich, Gustavo S.; Pochettino, Alberto; Greason, Kevin; Kalra, Manju; Johnstone, Jill; Shuja, Fahad; Harmsen, W. Scott; Macedo, Thanila; Mandrekar, Jay; Chamberlain, Alanna M.; Weiss, Salome; Goodney, Philip P.; Roger, Veronique (2018). “Population-Based Assessment of the Incidence of Aortic Dissection, Intramural Hematoma, and Penetrating Ulcer, and Its Associated Mortality From 1995 to 2015”. Circulation: Cardiovascular Quality and Outcomes. 11 (8). doi:10.1161/CIRCOUTCOMES.118.004689. ISSN 1941-7713.
- ↑ Imazio M, Demichelis B, Parrini I, Giuggia M, Cecchi E, Gaschino G, Demarie D, Ghisio A, Trinchero R (March 2004). “Day-hospital treatment of acute pericarditis: a management program for outpatient therapy”. J. Am. Coll. Cardiol. 43 (6): 1042–6. doi:10.1016/j.jacc.2003.09.055. PMID 15028364.
- ↑ Troughton RW, Asher CR, Klein AL (February 2004). “Pericarditis”. Lancet. 363 (9410): 717–27. doi:10.1016/S0140-6736(04)15648-1. PMID 15001332.
- ↑ Spodick DH (March 2003). “Acute pericarditis: current concepts and practice”. JAMA. 289 (9): 1150–3. PMID 12622586.
- ↑ Ewart W (March 1896). “Practical Aids in the Diagnosis of Pericardial Effusion, in Connection with the Question as to Surgical Treatment”. Br Med J. 1 (1838): 717–21. PMC 2406464. PMID 20756103.
- ↑ Adler Y, Charron P, Imazio M, Badano L, Barón-Esquivias G, Bogaert J, Brucato A, Gueret P, Klingel K, Lionis C, Maisch B, Mayosi B, Pavie A, Ristić AD, Sabaté Tenas M, Seferovic P, Swedberg K, Tomkowski W, Achenbach S, Agewall S, Al-Attar N, Angel Ferrer J, Arad M, Asteggiano R, Bueno H, Caforio AL, Carerj S, Ceconi C, Evangelista A, Flachskampf F, Giannakoulas G, Gielen S, Habib G, Kolh P, Lambrinou E, Lancellotti P, Lazaros G, Linhart A, Meurin P, Nieman K, Piepoli MF, Price S, Roos-Hesselink J, Roubille F, Ruschitzka F, Sagristà Sauleda J, Sousa-Uva M, Uwe Voigt J, Luis Zamorano J (November 2015). “2015 ESC Guidelines for the diagnosis and management of pericardial diseases: The Task Force for the Diagnosis and Management of Pericardial Diseases of the European Society of Cardiology (ESC)Endorsed by: The European Association for Cardio-Thoracic Surgery (EACTS)”. Eur. Heart J. 36 (42): 2921–64. doi:10.1093/eurheartj/ehv318. PMID 26320112.
- ↑ Dec GW, Palacios IF, Fallon JT, Aretz HT, Mills J, Lee DC, Johnson RA (April 1985). “Active myocarditis in the spectrum of acute dilated cardiomyopathies. Clinical features, histologic correlates, and clinical outcome”. N. Engl. J. Med. 312 (14): 885–90. doi:10.1056/NEJM198504043121404. PMID 3974674.
- ↑ Caforio AL, Calabrese F, Angelini A, Tona F, Vinci A, Bottaro S, Ramondo A, Carturan E, Iliceto S, Thiene G, Daliento L (June 2007). “A prospective study of biopsy-proven myocarditis: prognostic relevance of clinical and aetiopathogenetic features at diagnosis”. Eur. Heart J. 28 (11): 1326–33. doi:10.1093/eurheartj/ehm076. PMID 17493945.
- ↑ Ukena C, Mahfoud F, Kindermann I, Kandolf R, Kindermann M, Böhm M (April 2011). “Prognostic electrocardiographic parameters in patients with suspected myocarditis”. Eur. J. Heart Fail. 13 (4): 398–405. doi:10.1093/eurjhf/hfq229. PMID 21239404.
- ↑ Elliott PM, Kaski JC, Prasad K, Seo H, Slade AK, Goldman JH, McKenna WJ (July 1996). “Chest pain during daily life in patients with hypertrophic cardiomyopathy: an ambulatory electrocardiographic study”. Eur. Heart J. 17 (7): 1056–64. PMID 8809524.
- ↑ Pasternac A, Noble J, Streulens Y, Elie R, Henschke C, Bourassa MG (April 1982). “Pathophysiology of chest pain in patients with cardiomyopathies and normal coronary arteries”. Circulation. 65 (4): 778–89. PMID 7199403.
- ↑ Webb JG, Sasson Z, Rakowski H, Liu P, Wigle ED (January 1990). “Apical hypertrophic cardiomyopathy: clinical follow-up and diagnostic correlates”. J. Am. Coll. Cardiol. 15 (1): 83–90. PMID 2295747.
- ↑ Sharkey SW, Lesser JR, Zenovich AG, Maron MS, Lindberg J, Longe TF, Maron BJ (February 2005). “Acute and reversible cardiomyopathy provoked by stress in women from the United States”. Circulation. 111 (4): 472–9. doi:10.1161/01.CIR.0000153801.51470.EB. PMID 15687136.
- ↑ Krishnamoorthy P, Garg J, Sharma A, Palaniswamy C, Shah N, Lanier G, Patel NC, Lavie CJ, Ahmad H (July 2015). “Gender Differences and Predictors of Mortality in Takotsubo Cardiomyopathy: Analysis from the National Inpatient Sample 2009-2010 Database”. Cardiology. 132 (2): 131–136. doi:10.1159/000430782. PMID 26159108.
- ↑ Templin C, Ghadri JR, Diekmann J, Napp LC, Bataiosu DR, Jaguszewski M, Cammann VL, Sarcon A, Geyer V, Neumann CA, Seifert B, Hellermann J, Schwyzer M, Eisenhardt K, Jenewein J, Franke J, Katus HA, Burgdorf C, Schunkert H, Moeller C, Thiele H, Bauersachs J, Tschöpe C, Schultheiss HP, Laney CA, Rajan L, Michels G, Pfister R, Ukena C, Böhm M, Erbel R, Cuneo A, Kuck KH, Jacobshagen C, Hasenfuss G, Karakas M, Koenig W, Rottbauer W, Said SM, Braun-Dullaeus RC, Cuculi F, Banning A, Fischer TA, Vasankari T, Airaksinen KE, Fijalkowski M, Rynkiewicz A, Pawlak M, Opolski G, Dworakowski R, MacCarthy P, Kaiser C, Osswald S, Galiuto L, Crea F, Dichtl W, Franz WM, Empen K, Felix SB, Delmas C, Lairez O, Erne P, Bax JJ, Ford I, Ruschitzka F, Prasad A, Lüscher TF (September 2015). “Clinical Features and Outcomes of Takotsubo (Stress) Cardiomyopathy”. N. Engl. J. Med. 373 (10): 929–38. doi:10.1056/NEJMoa1406761. PMID 26332547.
- ↑ Bybee KA, Kara T, Prasad A, Lerman A, Barsness GW, Wright RS, Rihal CS (December 2004). “Systematic review: transient left ventricular apical ballooning: a syndrome that mimics ST-segment elevation myocardial infarction”. Ann. Intern. Med. 141 (11): 858–65. PMID 15583228.
- ↑ Green SJ, Pizzarello RA, Padmanabhan VT, Ong LY, Hall MH, Tortolani AJ (April 1985). “Relation of angina pectoris to coronary artery disease in aortic valve stenosis”. Am. J. Cardiol. 55 (8): 1063–5. PMID 3984868.
- ↑ Silaruks S, Clark D, Thinkhamrop B, Sia B, Buxton B, Tonkin A (2001). “Angina pectoris and coronary artery disease in severe isolated valvular aortic stenosis”. Heart Lung Circ. 10 (1): 14–23. doi:10.1046/j.1444-2892.2001.00060.x. PMID 16352020.
- ↑ Munt B, Legget ME, Kraft CD, Miyake-Hull CY, Fujioka M, Otto CM (February 1999). “Physical examination in valvular aortic stenosis: correlation with stenosis severity and prediction of clinical outcome”. Am. Heart J. 137 (2): 298–306. doi:10.1053/hj.1999.v137.95496. PMID 9924164.
- ↑ Anker SD, Sharma R (September 2002). “The syndrome of cardiac cachexia”. Int. J. Cardiol. 85 (1): 51–66. PMID 12163209.
- ↑ Horwich TB, Kalantar-Zadeh K, MacLellan RW, Fonarow GC (May 2008). “Albumin levels predict survival in patients with systolic heart failure”. Am. Heart J. 155 (5): 883–9. doi:10.1016/j.ahj.2007.11.043. PMID 18440336.
- ↑ Breathett K, Allen LA, Udelson J, Davis G, Bristow M (October 2016). “Changes in Left Ventricular Ejection Fraction Predict Survival and Hospitalization in Heart Failure With Reduced Ejection Fraction”. Circ Heart Fail. 9 (10). doi:10.1161/CIRCHEARTFAILURE.115.002962. PMC 5082710. PMID 27656000.
- ↑ Stein PD, Beemath A, Matta F, Weg JG, Yusen RD, Hales CA, Hull RD, Leeper KV, Sostman HD, Tapson VF, Buckley JD, Gottschalk A, Goodman LR, Wakefied TW, Woodard PK (October 2007). “Clinical characteristics of patients with acute pulmonary embolism: data from PIOPED II”. Am. J. Med. 120 (10): 871–9. doi:10.1016/j.amjmed.2007.03.024. PMC 2071924. PMID 17904458.
- ↑ “Value of the ventilation/perfusion scan in acute pulmonary embolism. Results of the prospective investigation of pulmonary embolism diagnosis (PIOPED)”. JAMA. 263 (20): 2753–9. 1990. PMID 2332918.
- ↑ Bense L, Wiman LG, Hedenstierna G (September 1987). “Onset of symptoms in spontaneous pneumothorax: correlations to physical activity”. Eur J Respir Dis. 71 (3): 181–6. PMID 3678419.
- ↑ Seow A, Kazerooni EA, Pernicano PG, Neary M (February 1996). “Comparison of upright inspiratory and expiratory chest radiographs for detecting pneumothoraces”. AJR Am J Roentgenol. 166 (2): 313–6. doi:10.2214/ajr.166.2.8553937. PMID 8553937.
- ↑ Stark P, Leung A (1996). “Effects of lobar atelectasis on the distribution of pleural effusion and pneumothorax”. J Thorac Imaging. 11 (2): 145–9. PMID 8820023.
- ↑ Jalli R, Sefidbakht S, Jafari SH (April 2013). “Value of ultrasound in diagnosis of pneumothorax: a prospective study”. Emerg Radiol. 20 (2): 131–4. doi:10.1007/s10140-012-1091-7. PMID 23179505.
- ↑ File TM (December 2003). “Community-acquired pneumonia”. Lancet. 362 (9400): 1991–2001. doi:10.1016/S0140-6736(03)15021-0. PMID 14683661.
- ↑ Mandell LA, Wunderink RG, Anzueto A, Bartlett JG, Campbell GD, Dean NC, Dowell SF, File TM, Musher DM, Niederman MS, Torres A, Whitney CG (March 2007). “Infectious Diseases Society of America/American Thoracic Society consensus guidelines on the management of community-acquired pneumonia in adults”. Clin. Infect. Dis. 44 Suppl 2: S27–72. doi:10.1086/511159. PMID 17278083.
- ↑ Musher DM, Thorner AR (October 2014). “Community-acquired pneumonia”. N. Engl. J. Med. 371 (17): 1619–28. doi:10.1056/NEJMra1312885. PMID 25337751.
- ↑ Conley SF, Beste DJ, Hoffmann RG (May 1993). “Measles-associated bacterial tracheitis”. Pediatr. Infect. Dis. J. 12 (5): 414–5. PMID 8327305.
- ↑ Salamone FN, Bobbitt DB, Myer CM, Rutter MJ, Greinwald JH (December 2004). “Bacterial tracheitis reexamined: is there a less severe manifestation?”. Otolaryngol Head Neck Surg. 131 (6): 871–6. doi:10.1016/j.otohns.2004.06.708. PMID 15577783.
- ↑ Hopkins A, Lahiri T, Salerno R, Heath B (October 2006). “Changing epidemiology of life-threatening upper airway infections: the reemergence of bacterial tracheitis”. Pediatrics. 118 (4): 1418–21. doi:10.1542/peds.2006-0692. PMID 17015531.
- ↑ Liston SL, Gehrz RC, Siegel LG, Tilelli J (August 1983). “Bacterial tracheitis”. Am. J. Dis. Child. 137 (8): 764–7. PMID 6869336.
- ↑ Mesquita SM, Castro CR, Ikari NM, Oliveira SA, Lopes AA (March 2004). “Likelihood of left main coronary artery compression based on pulmonary trunk diameter in patients with pulmonary hypertension”. Am. J. Med. 116 (6): 369–74. doi:10.1016/j.amjmed.2003.11.015. PMID 15006585.
- ↑ Rich S, McLaughlin VV, O’Neill W (October 2001). “Stenting to reverse left ventricular ischemia due to left main coronary artery compression in primary pulmonary hypertension”. Chest. 120 (4): 1412–5. PMID 11591592.
- ↑ Kawut SM, Silvestry FE, Ferrari VA, DeNofrio D, Axel L, Loh E, Palevsky HI (March 1999). “Extrinsic compression of the left main coronary artery by the pulmonary artery in patients with long-standing pulmonary hypertension”. Am. J. Cardiol. 83 (6): 984–6, A10. PMID 10190427.
- ↑ Feinsilver SH, Barrows AA, Braman SS (October 1986). “Fiberoptic bronchoscopy and pleural effusion of unknown origin”. Chest. 90 (4): 516–9. PMID 3757561.
- ↑ Collins TR, Sahn SA (June 1987). “Thoracocentesis. Clinical value, complications, technical problems, and patient experience”. Chest. 91 (6): 817–22. PMID 3581930.
- ↑ Venekamp LN, Velkeniers B, Noppen M (2005). “Does ‘idiopathic pleuritis’ exist? Natural history of non-specific pleuritis diagnosed after thoracoscopy”. Respiration. 72 (1): 74–8. doi:10.1159/000083404. PMID 15753638.
- ↑ Kuempel ED, Wheeler MW, Smith RJ, Vallyathan V, Green FH (August 2009). “Contributions of dust exposure and cigarette smoking to emphysema severity in coal miners in the United States”. Am. J. Respir. Crit. Care Med. 180 (3): 257–64. doi:10.1164/rccm.200806-840OC. PMID 19423717.
- ↑ Lamprecht B, McBurnie MA, Vollmer WM, Gudmundsson G, Welte T, Nizankowska-Mogilnicka E, Studnicka M, Bateman E, Anto JM, Burney P, Mannino DM, Buist SA (April 2011). “COPD in never smokers: results from the population-based burden of obstructive lung disease study”. Chest. 139 (4): 752–763. doi:10.1378/chest.10-1253. PMC 3168866. PMID 20884729.
- ↑ Rennard S, Decramer M, Calverley PM, Pride NB, Soriano JB, Vermeire PA, Vestbo J (October 2002). “Impact of COPD in North America and Europe in 2000: subjects’ perspective of Confronting COPD International Survey”. Eur. Respir. J. 20 (4): 799–805. PMID 12412667.
- ↑ Badgett RG, Tanaka DJ, Hunt DK, Jelley MJ, Feinberg LE, Steiner JF, Petty TL (February 1993). “Can moderate chronic obstructive pulmonary disease be diagnosed by historical and physical findings alone?”. Am. J. Med. 94 (2): 188–96. PMID 8430714.
- ↑ Kocher F, Hilbe W, Seeber A, Pircher A, Schmid T, Greil R, Auberger J, Nevinny-Stickel M, Sterlacci W, Tzankov A, Jamnig H, Kohler K, Zabernigg A, Frötscher J, Oberaigner W, Fiegl M (February 2015). “Longitudinal analysis of 2293 NSCLC patients: a comprehensive study from the TYROL registry”. Lung Cancer. 87 (2): 193–200. doi:10.1016/j.lungcan.2014.12.006. PMID 25564398.
- ↑ Hyde L, Hyde CI (March 1974). “Clinical manifestations of lung cancer”. Chest. 65 (3): 299–306. PMID 4813837.
- ↑ Chute CG, Greenberg ER, Baron J, Korson R, Baker J, Yates J (October 1985). “Presenting conditions of 1539 population-based lung cancer patients by cell type and stage in New Hampshire and Vermont”. Cancer. 56 (8): 2107–11. PMID 2992757.
- ↑ Hiraki A, Ueoka H, Takata I, Gemba K, Bessho A, Segawa Y, Kiura K, Eguchi K, Yoneda T, Tanimoto M, Harada M (March 2004). “Hypercalcemia-leukocytosis syndrome associated with lung cancer”. Lung Cancer. 43 (3): 301–7. doi:10.1016/j.lungcan.2003.09.006. PMID 15165088.
- ↑ Ungprasert P, Carmona EM, Utz JP, Ryu JH, Crowson CS, Matteson EL (February 2016). “Epidemiology of Sarcoidosis 1946-2013: A Population-Based Study”. Mayo Clin. Proc. 91 (2): 183–8. doi:10.1016/j.mayocp.2015.10.024. PMC 4744129. PMID 26727158.
- ↑ Baughman RP, Teirstein AS, Judson MA, Rossman MD, Yeager H, Bresnitz EA, DePalo L, Hunninghake G, Iannuzzi MC, Johns CJ, McLennan G, Moller DR, Newman LS, Rabin DL, Rose C, Rybicki B, Weinberger SE, Terrin ML, Knatterud GL, Cherniak R (November 2001). “Clinical characteristics of patients in a case control study of sarcoidosis”. Am. J. Respir. Crit. Care Med. 164 (10 Pt 1): 1885–9. doi:10.1164/ajrccm.164.10.2104046. PMID 11734441.
- ↑ Rizzato G, Tinelli C (2005). “Unusual presentation of sarcoidosis”. Respiration. 72 (1): 3–6. doi:10.1159/000083392. PMID 15753626.
- ↑ Rizzato G, Palmieri G, Agrati AM, Zanussi C (June 2004). “The organ-specific extrapulmonary presentation of sarcoidosis: a frequent occurrence but a challenge to an early diagnosis. A 3-year-long prospective observational study”. Sarcoidosis Vasc Diffuse Lung Dis. 21 (2): 119–26. PMID 15281433.
- ↑ Vichinsky EP, Styles LA, Colangelo LH, Wright EC, Castro O, Nickerson B (March 1997). “Acute chest syndrome in sickle cell disease: clinical presentation and course. Cooperative Study of Sickle Cell Disease”. Blood. 89 (5): 1787–92. PMID 9057664.
- ↑ Castro O, Brambilla DJ, Thorington B, Reindorf CA, Scott RB, Gillette P, Vera JC, Levy PS (July 1994). “The acute chest syndrome in sickle cell disease: incidence and risk factors. The Cooperative Study of Sickle Cell Disease”. Blood. 84 (2): 643–9. PMID 7517723.
- ↑ Vichinsky EP, Neumayr LD, Earles AN, Williams R, Lennette ET, Dean D, Nickerson B, Orringer E, McKie V, Bellevue R, Daeschner C, Manci EA (June 2000). “Causes and outcomes of the acute chest syndrome in sickle cell disease. National Acute Chest Syndrome Study Group”. N. Engl. J. Med. 342 (25): 1855–65. doi:10.1056/NEJM200006223422502. PMID 10861320.
- ↑ Vakil N, van Zanten SV, Kahrilas P, Dent J, Jones R (August 2006). “The Montreal definition and classification of gastroesophageal reflux disease: a global evidence-based consensus”. Am. J. Gastroenterol. 101 (8): 1900–20, quiz 1943. doi:10.1111/j.1572-0241.2006.00630.x. PMID 16928254.
- ↑ Vakil NB, Traxler B, Levine D (August 2004). “Dysphagia in patients with erosive esophagitis: prevalence, severity, and response to proton pump inhibitor treatment”. Clin. Gastroenterol. Hepatol. 2 (8): 665–8. PMID 15290658.
- ↑ Giannini EG, Zentilin P, Dulbecco P, Vigneri S, Scarlata P, Savarino V (February 2008). “Management strategy for patients with gastroesophageal reflux disease: a comparison between empirical treatment with esomeprazole and endoscopy-oriented treatment”. Am. J. Gastroenterol. 103 (2): 267–75. doi:10.1111/j.1572-0241.2007.01659.x. PMID 18289194.
- ↑ Katz PO, Dalton CB, Richter JE, Wu WC, Castell DO (April 1987). “Esophageal testing of patients with noncardiac chest pain or dysphagia. Results of three years’ experience with 1161 patients”. Ann. Intern. Med. 106 (4): 593–7. PMID 3826958.
- ↑ Kahrilas PJ (May 2010). “Esophageal motor disorders in terms of high-resolution esophageal pressure topography: what has changed?”. Am. J. Gastroenterol. 105 (5): 981–7. doi:10.1038/ajg.2010.43. PMC 2888528. PMID 20179690.
- ↑ Pandolfino JE, Ghosh SK, Rice J, Clarke JO, Kwiatek MA, Kahrilas PJ (January 2008). “Classifying esophageal motility by pressure topography characteristics: a study of 400 patients and 75 controls”. Am. J. Gastroenterol. 103 (1): 27–37. doi:10.1111/j.1572-0241.2007.01532.x. PMID 17900331.
- ↑ Kahrilas PJ, Ghosh SK, Pandolfino JE (2008). “Esophageal motility disorders in terms of pressure topography: the Chicago Classification”. J. Clin. Gastroenterol. 42 (5): 627–35. doi:10.1097/MCG.0b013e31815ea291. PMC 2895002. PMID 18364587.
- ↑ Bott S, Prakash C, McCallum RW (August 1987). “Medication-induced esophageal injury: survey of the literature”. Am. J. Gastroenterol. 82 (8): 758–63. PMID 3605035.
- ↑ Parfitt JR, Jayakumar S, Driman DK (September 2008). “Mycophenolate mofetil-related gastrointestinal mucosal injury: variable injury patterns, including graft-versus-host disease-like changes”. Am. J. Surg. Pathol. 32 (9): 1367–72. PMID 18763324.
- ↑ Jaspersen D (March 2000). “Drug-induced oesophageal disorders: pathogenesis, incidence, prevention and management”. Drug Saf. 22 (3): 237–49. PMID 10738847.
- ↑ Kapel RC, Miller JK, Torres C, Aksoy S, Lash R, Katzka DA (May 2008). “Eosinophilic esophagitis: a prevalent disease in the United States that affects all age groups”. Gastroenterology. 134 (5): 1316–21. doi:10.1053/j.gastro.2008.02.016. PMID 18471509.
- ↑ Straumann A, Rossi L, Simon HU, Heer P, Spichtin HP, Beglinger C (March 2003). “Fragility of the esophageal mucosa: a pathognomonic endoscopic sign of primary eosinophilic esophagitis?”. Gastrointest. Endosc. 57 (3): 407–12. doi:10.1067/mge.2003.123. PMID 12612531.
- ↑ Straumann A, Bussmann C, Zuber M, Vannini S, Simon HU, Schoepfer A (May 2008). “Eosinophilic esophagitis: analysis of food impaction and perforation in 251 adolescent and adult patients”. Clin. Gastroenterol. Hepatol. 6 (5): 598–600. doi:10.1016/j.cgh.2008.02.003. PMID 18407800.
- ↑ Prasad GA, Alexander JA, Schleck CD, Zinsmeister AR, Smyrk TC, Elias RM, Locke GR, Talley NJ (October 2009). “Epidemiology of eosinophilic esophagitis over three decades in Olmsted County, Minnesota”. Clin. Gastroenterol. Hepatol. 7 (10): 1055–61. doi:10.1016/j.cgh.2009.06.023. PMC 3026355. PMID 19577011.
- ↑ Prasad GA, Talley NJ, Romero Y, Arora AS, Kryzer LA, Smyrk TC, Alexander JA (December 2007). “Prevalence and predictive factors of eosinophilic esophagitis in patients presenting with dysphagia: a prospective study”. Am. J. Gastroenterol. 102 (12): 2627–32. doi:10.1111/j.1572-0241.2007.01512.x. PMID 17764492.
- ↑ Desai TK, Stecevic V, Chang CH, Goldstein NS, Badizadegan K, Furuta GT (June 2005). “Association of eosinophilic inflammation with esophageal food impaction in adults”. Gastrointest. Endosc. 61 (7): 795–801. PMID 15933677.
- ↑ Loyd JE, Tillman BF, Atkinson JB, Des Prez RM (September 1988). “Mediastinal fibrosis complicating histoplasmosis”. Medicine (Baltimore). 67 (5): 295–310. PMID 3045478.
- ↑ Feigin DS, Eggleston JC, Siegelman SS (January 1979). “The multiple roentgen manifestations of sclerosing mediastinitis”. Johns Hopkins Med J. 144 (1): 1–8. PMID 762913.
- ↑ Garrett HE, Roper CL (December 1986). “Surgical intervention in histoplasmosis”. Ann. Thorac. Surg. 42 (6): 711–22. PMID 3539049.
- ↑ Sherrick AD, Brown LR, Harms GF, Myers JL (August 1994). “The radiographic findings of fibrosing mediastinitis”. Chest. 106 (2): 484–9. PMID 7774324.
- ↑ Fitzgerald JE, White MJ, Lobo DN (April 2009). “Courvoisier’s gallbladder: law or sign?”. World J Surg. 33 (4): 886–91. doi:10.1007/s00268-008-9908-y. PMID 19190960.
- ↑ Yang MH, Chen TH, Wang SE, Tsai YF, Su CH, Wu CW, Lui WY, Shyr YM (July 2008). “Biochemical predictors for absence of common bile duct stones in patients undergoing laparoscopic cholecystectomy”. Surg Endosc. 22 (7): 1620–4. doi:10.1007/s00464-007-9665-2. PMID 18000708.
- ↑ Prat F, Meduri B, Ducot B, Chiche R, Salimbeni-Bartolini R, Pelletier G (March 1999). “Prediction of common bile duct stones by noninvasive tests”. Ann. Surg. 229 (3): 362–8. PMC 1191701. PMID 10077048.
- ↑ Tse F, Barkun JS, Barkun AN (September 2004). “The elective evaluation of patients with suspected choledocholithiasis undergoing laparoscopic cholecystectomy”. Gastrointest. Endosc. 60 (3): 437–48. PMID 15332044.
- ↑ Dickson AP, Imrie CW (October 1984). “The incidence and prognosis of body wall ecchymosis in acute pancreatitis”. Surg Gynecol Obstet. 159 (4): 343–7. PMID 6237447.
- ↑ Yadav D, Agarwal N, Pitchumoni CS (June 2002). “A critical evaluation of laboratory tests in acute pancreatitis”. Am. J. Gastroenterol. 97 (6): 1309–18. doi:10.1111/j.1572-0241.2002.05766.x. PMID 12094843.
- ↑ Fortson MR, Freedman SN, Webster PD (December 1995). “Clinical assessment of hyperlipidemic pancreatitis”. Am. J. Gastroenterol. 90 (12): 2134–9. PMID 8540502.
- ↑ Lecesne R, Taourel P, Bret PM, Atri M, Reinhold C (June 1999). “Acute pancreatitis: interobserver agreement and correlation of CT and MR cholangiopancreatography with outcome”. Radiology. 211 (3): 727–35. doi:10.1148/radiology.211.3.r99jn08727. PMID 10352598.
- ↑ Stimac D, Miletić D, Radić M, Krznarić I, Mazur-Grbac M, Perković D, Milić S, Golubović V (May 2007). “The role of nonenhanced magnetic resonance imaging in the early assessment of acute pancreatitis”. Am. J. Gastroenterol. 102 (5): 997–1004. doi:10.1111/j.1572-0241.2007.01164.x. PMID 17378903.
- ↑ Weston AP (October 1996). “Hiatal hernia with cameron ulcers and erosions”. Gastrointest. Endosc. Clin. N. Am. 6 (4): 671–9. PMID 8899401.
- ↑ Bredenoord AJ, Weusten BL, Timmer R, Smout AJ (February 2006). “Intermittent spatial separation of diaphragm and lower esophageal sphincter favors acidic and weakly acidic reflux”. Gastroenterology. 130 (2): 334–40. doi:10.1053/j.gastro.2005.10.053. PMID 16472589.
- ↑ Kahrilas PJ, Kim HC, Pandolfino JE (2008). “Approaches to the diagnosis and grading of hiatal hernia”. Best Pract Res Clin Gastroenterol. 22 (4): 601–16. doi:10.1016/j.bpg.2007.12.007. PMC 2548324. PMID 18656819.
- ↑ Wolf E, Stern S (February 1976). “Costosternal syndrome: its frequency and importance in differential diagnosis of coronary heart disease”. Arch. Intern. Med. 136 (2): 189–91. PMID 1247350.
- ↑ Fam AG, Smythe HA (September 1985). “Musculoskeletal chest wall pain”. CMAJ. 133 (5): 379–89. PMC 1346531. PMID 4027804.
- ↑ Bösner S, Becker A, Hani MA, Keller H, Sönnichsen AC, Karatolios K, Schaefer JR, Haasenritter J, Baum E, Donner-Banzhoff N (August 2010). “Chest wall syndrome in primary care patients with chest pain: presentation, associated features and diagnosis”. Fam Pract. 27 (4): 363–9. doi:10.1093/fampra/cmq024. PMID 20406787.
- ↑ Zaruba RA, Wilson E (June 2017). “IMPAIRMENT BASED EXAMINATION AND TREATMENT OF COSTOCHONDRITIS: A CASE SERIES”. Int J Sports Phys Ther. 12 (3): 458–467. PMC 5455195. PMID 28593100.
- ↑ Scott EM, Scott BB (July 1993). “Painful rib syndrome–a review of 76 cases”. Gut. 34 (7): 1006–8. PMC 1374244. PMID 8344569.
- ↑ Aeschlimann A, Kahn MF (1990). “Tietze’s syndrome: a critical review”. Clin. Exp. Rheumatol. 8 (4): 407–12. PMID 1697801.
- ↑ LIPKIN M, FULTON LA, WOLFSON EA (October 1955). “The syndrome of the hypersensitive xiphoid”. N. Engl. J. Med. 253 (14): 591–7. doi:10.1056/NEJM195510062531403. PMID 13266001.
- ↑ van Holsbeeck M, van Melkebeke J, Dequeker J, Pennes DR (September 1992). “Radiographic findings of spontaneous subluxation of the sternoclavicular joint”. Clin. Rheumatol. 11 (3): 376–81. PMID 1458785.
- ↑ Almansa C, Wang B, Achem SR (March 2010). “Noncardiac chest pain and fibromyalgia”. Med. Clin. North Am. 94 (2): 275–89. doi:10.1016/j.mcna.2010.01.002. PMID 20380956.
- ↑ Disla E, Rhim HR, Reddy A, Karten I, Taranta A (November 1994). “Costochondritis. A prospective analysis in an emergency department setting”. Arch. Intern. Med. 154 (21): 2466–9. PMID 7979843.
- ↑ Wise CM, Semble EL, Dalton CB (February 1992). “Musculoskeletal chest wall syndromes in patients with noncardiac chest pain: a study of 100 patients”. Arch Phys Med Rehabil. 73 (2): 147–9. PMID 1543409.
- ↑ Rodríguez-Henríquez P, Solano C, Peña A, León-Hernández S, Hernández-Díaz C, Gutiérrez M, Pineda C (July 2013). “Sternoclavicular joint involvement in rheumatoid arthritis: clinical and ultrasound findings of a neglected joint”. Arthritis Care Res (Hoboken). 65 (7): 1177–82. doi:10.1002/acr.21958. PMID 23335586.
- ↑ Ramonda R, Lorenzin M, Lo Nigro A, Vio S, Zucchetta P, Frallonardo P, Campana C, Oliviero F, Modesti V, Punzi L (September 2012). “Anterior chest wall involvement in early stages of spondyloarthritis: advanced diagnostic tools”. J. Rheumatol. 39 (9): 1844–9. doi:10.3899/jrheum.120107. PMID 22798267.
- ↑ Wendling D, Prati C, Demattei C, Loeuille D, Richette P, Dougados M (July 2013). “Anterior chest wall pain in recent inflammatory back pain suggestive of spondyloarthritis. data from the DESIR cohort”. J. Rheumatol. 40 (7): 1148–52. doi:10.3899/jrheum.121460. PMID 23678156.
- ↑ 149.0 149.1 149.2 Jurik AG (1992). “Seronegative anterior chest wall syndromes. A study of the findings and course at radiography”. Acta Radiol Suppl. 381: 1–42. PMID 1488919.
- ↑ Guglielmi G, Cascavilla A, Scalzo G, Salaffi F, Grassi W (2009). “Imaging of sternocostoclavicular joint in spondyloarthropaties and other rheumatic conditions”. Clin. Exp. Rheumatol. 27 (3): 402–8. PMID 19604431.
- ↑ Saghafi M, Henderson MJ, Buchanan WW (February 1993). “Sternocostoclavicular hyperostosis”. Semin. Arthritis Rheum. 22 (4): 215–23. PMID 8484129.
- ↑ Magrey M, Khan MA (October 2009). “New insights into synovitis, acne, pustulosis, hyperostosis, and osteitis (SAPHO) syndrome”. Curr Rheumatol Rep. 11 (5): 329–33. PMID 19772827.
- ↑ Colina M, Govoni M, Orzincolo C, Trotta F (June 2009). “Clinical and radiologic evolution of synovitis, acne, pustulosis, hyperostosis, and osteitis syndrome: a single center study of a cohort of 71 subjects”. Arthritis Rheum. 61 (6): 813–21. doi:10.1002/art.24540. PMID 19479702.
- ↑ Carneiro S, Sampaio-Barros PD (May 2013). “SAPHO syndrome”. Rheum. Dis. Clin. North Am. 39 (2): 401–18. doi:10.1016/j.rdc.2013.02.009. PMID 23597971.
- ↑ Turner-Stokes L, Turner-Warwick M (April 1982). “Intrathoracic manifestations of SLE”. Clin Rheum Dis. 8 (1): 229–42. PMID 6749397.
- ↑ Hunder GG, McDuffie FC, Hepper NG (March 1972). “Pleural fluid complement in systemic lupus erythematosus and rheumatoid arthritis”. Ann. Intern. Med. 76 (3): 357–63. PMID 5015911.
- ↑ Porcel JM, Ordi-Ros J, Esquerda A, Vives M, Madroñero AB, Bielsa S, Vilardell-Tarrés M, Light RW (2007). “Antinuclear antibody testing in pleural fluid for the diagnosis of lupus pleuritis”. Lupus. 16 (1): 25–7. doi:10.1177/0961203306074470. PMID 17283581.
- ↑ Chopra R, Chaudhary N, Kay J (May 2013). “Relapsing polychondritis”. Rheum. Dis. Clin. North Am. 39 (2): 263–76. doi:10.1016/j.rdc.2013.03.002. PMID 23597963.
- ↑ Fleet RP, Martel JP, Lavoie KL, Dupuis G, Beitman BD (2000). “Non-fearful panic disorder: a variant of panic in medical patients?”. Psychosomatics. 41 (4): 311–20. doi:10.1176/appi.psy.41.4.311. PMID 10906353.
- ↑ Simpson RJ, Kazmierczak T, Power KG, Sharp DM (August 1994). “Controlled comparison of the characteristics of patients with panic disorder”. Br J Gen Pract. 44 (385): 352–6. PMC 1238951. PMID 8068393.
- ↑ Grant BF, Goldstein RB, Saha TD, Chou SP, Jung J, Zhang H, Pickering RP, Ruan WJ, Smith SM, Huang B, Hasin DS (August 2015). “Epidemiology of DSM-5 Alcohol Use Disorder: Results From the National Epidemiologic Survey on Alcohol and Related Conditions III”. JAMA Psychiatry. 72 (8): 757–66. doi:10.1001/jamapsychiatry.2015.0584. PMC 5240584. PMID 26039070.
- ↑ Cosci F, Schruers KR, Abrams K, Griez EJ (June 2007). “Alcohol use disorders and panic disorder: a review of the evidence of a direct relationship”. J Clin Psychiatry. 68 (6): 874–80. PMID 17592911.
- ↑ George DT, Nutt DJ, Dwyer BA, Linnoila M (February 1990). “Alcoholism and panic disorder: is the comorbidity more than coincidence?”. Acta Psychiatr Scand. 81 (2): 97–107. PMID 2183544.
- ↑ Dworkin RH, Johnson RW, Breuer J, Gnann JW, Levin MJ, Backonja M, Betts RF, Gershon AA, Haanpaa ML, McKendrick MW, Nurmikko TJ, Oaklander AL, Oxman MN, Pavan-Langston D, Petersen KL, Rowbotham MC, Schmader KE, Stacey BR, Tyring SK, van Wijck AJ, Wallace MS, Wassilew SW, Whitley RJ (January 2007). “Recommendations for the management of herpes zoster”. Clin. Infect. Dis. 44 Suppl 1: S1–26. doi:10.1086/510206. PMID 17143845.
- ↑ Oxman MN (December 1995). “Immunization to reduce the frequency and severity of herpes zoster and its complications”. Neurology. 45 (12 Suppl 8): S41–6. PMID 8545018.
- ↑ Jumaan AO, Yu O, Jackson LA, Bohlke K, Galil K, Seward JF (June 2005). “Incidence of herpes zoster, before and after varicella-vaccination-associated decreases in the incidence of varicella, 1992-2002”. J. Infect. Dis. 191 (12): 2002–7. doi:10.1086/430325. PMID 15897984.
Epidemiology and Demographics
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor-In-Chief: Sahar Memar Montazerin, M.D.[2] Cafer Zorkun, M.D., Ph.D. [3]
Overview
The incidence of aortic dissection is approximately 6 per 100,000 individuals worldwide.The incidence of aortic dissection increases with age, with a mean age of 63 years. Men are more commonly affected by aortic dissection than women. However, the prognosis tends to be worse in women due to unusual presentations. There is no racial predilection to aortic dissection. However, non-white race is associated with worse prognosis. The 30-days mortality rate of aortic dissection type A and B is approximately 47% and 13%, respectively.
Epidemiology and Demographics
Incidence
Age
Race
- There is no racial predilection to aortic dissection. However, non-white race is associated with worse prognosis.[4]
Gender
- Men are more commonly affected by aortic dissection than women. However, the prognosis tends to be worse in women due to unusual presentations.[2]
Mortality rate
- The 30-days mortality rate of aortic dissection type A and B is approximately 47% and 13% affected individuals, respectively.[1]
References
- ↑ 1.0 1.1 Howard, Dominic P.J.; Banerjee, Amitava; Fairhead, Jack F.; Perkins, Jeremy; Silver, Louise E.; Rothwell, Peter M. (2013). “Population-Based Study of Incidence and Outcome of Acute Aortic Dissection and Premorbid Risk Factor Control”. Circulation. 127 (20): 2031–2037. doi:10.1161/CIRCULATIONAHA.112.000483. ISSN 0009-7322.
- ↑ 2.0 2.1 Olsson, Christian; Thelin, Stefan; Ståhle, Elisabeth; Ekbom, Anders; Granath, Fredrik (2006). “Thoracic Aortic Aneurysm and Dissection”. Circulation. 114 (24): 2611–2618. doi:10.1161/CIRCULATIONAHA.106.630400. ISSN 0009-7322.
- ↑ “Correspondence”. The Annals of Thoracic Surgery. 67 (2): 593. 1999. doi:10.1016/S0003-4975(99)00037-5. ISSN 0003-4975.
- ↑ Harris, Donald; Klyushnenkova, Elena; Kalsi, Richa; Garrido, Danon; Bhardwaj, Abhishek; Rabin, Joseph; Toursavadkohi, Shahab; Diaz, Jose; Crawford, Robert (2016). “Non-White Race Is an Independent Risk Factor for Hospitalization for Aortic Dissection”. Ethnicity & Disease. 26 (3): 363. doi:10.18865/ed.26.3.363. ISSN 1945-0826.
Risk Factors
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Cafer Zorkun, M.D., Ph.D. [2]; Raviteja Guddeti, M.B.B.S. [3] Sahar Memar Montazerin, M.D.[4]
Overview
Common risk factors in the development of aortic dissection include aging, atherosclerosis, diabetes, hypertension and trauma. Less common risk factors include bicuspid aortic valve, cocaine abuse, coarctation of the aorta, cystic medial necrosis, a history of collagen vascular disoders, giant cell arteritis, heart surgery, pseudoxanthoma elasticum, Turner’s syndrome, tertiary syphilis and the third trimester of pregnancy.
Risk Factors
Common risk factors in the development of aortic dissection include:[1][2][3]
- Aging with the highest incidence in individuals who are 50 to 70 years old
- Atherosclerosis and its associated risk factors like diabetes
- Bicuspid aortic valve especially important in ascending aorta dissection[4]
- The risk of dissection in individuals with bicuspid aortic valve is not associated with the degree of stenosis of the valve.
- Chest trauma including blunt trauma and iatrogenic (for example during cardiac catheterization or due to an intra-aortic balloon pump)
- Coarctation of the aorta[5]
Less Common Risk Factors
Less common risk factors in the development of aortic dissection include:[6][7][8][9]
- Cocaine abuse
- Cystic medial necrosis
- Deceleration trauma most commonly causes aortic rupture, not dissection
- Diabetes
- A history of collagen vascular disorders such as:
- Familial hypercholesterolemia
- Giant cell arteritis
- Heart surgery particularly aortic valve replacement
- Hypertension most frequently in those with type III dissection
- Male gender
- Preexisting aortic aneurysm
- Preexisting aortic valve disease
- Prior aortic aneurysm repair
- Prior aortic dissection
- Prior aortic dissection repair
- Pseudoxanthoma elasticum
- Tertiary syphilis
- Tetralogy of Fallot
- Third trimester of pregnancy
- Turner’s syndrome due to aortic root dilatation in this syndrome
- Vasculitis (inflammation (rarely)
2010 ACCF/AHA/AATS/ACR/ASA/SCA/SCAI/SIR/STS/SVM Guidelines for the Diagnosis and Management of Patients With Thoracic Aortic Disease (DO NOT EDIT)[10]
Estimation of Pretest Risk of Thoracic Aortic Dissection (DO NOT EDIT)[10]
| Class I |
| “1. Providers should routinely evaluate any patient presenting with complaints that may represent acute thoracic aortic dissection to establish a pretest risk of disease that can then be used to guide diagnostic decisions. This process should include specific questions about medical history, family history, and pain features as well as a focused examination to identify findings that are associated with aortic dissection, including: |
a. High-risk conditions and historical features[11] (Level of Evidence: B):
|
| b. High-risk chest, back, or abdominal pain features[12][11][13][14][15][16][17](Level of Evidence: B): |
c. High-risk examination features[12][18][13][17][19][20][21] (Level of Evidence: B):
|
| “2. Patients presenting with sudden onset of severe chest, back, and/or abdominal pain, particularly those less than 40 years of age, should be questioned about a history and examined for physical features of Marfan syndrome, Loeys-Dietz syndrome, vascular Ehlers-Danlos syndrome, Turner syndrome, or other connective tissue disorders associated with thoracic aortic disease.[11] (Level of Evidence: B)” |
| “3. Patients presenting with sudden onset of severe chest, back, and/or abdominal pain should be questioned about a history of aortic pathology in immediate family members as there is a strong familial component to acute thoracic aortic disease.[11] (Level of Evidence: B)” |
| “4. Patients presenting with sudden onset of severe chest, back, and/or abdominal pain should be questioned about recent aortic manipulation (surgical or catheter-based) or a known history of aortic valvular disease, as these factors predispose to acute aortic dissection. (Level of Evidence: C)” |
| “5. In patients with suspected or confirmed aortic dissection who have experienced a syncopal episode, a focused examination should be performed to identify associated neurologic injury or the presence of pericardial tamponade. (Level of Evidence: C)” |
| “6. All patients presenting with acute neurologic complaints should be questioned about the presence of chest, back, and/or abdominal pain and checked for peripheral pulse deficits as patients with dissection related neurologic pathology are less likely to report thoracic pain than the typical aortic dissection patient.[20] |
References
- ↑ Larson, Eric W.; Edwards, William D. (1984). “Risk factors for aortic dissection: A necropsy study of 161 cases”. The American Journal of Cardiology. 53 (6): 849–855. doi:10.1016/0002-9149(84)90418-1. ISSN 0002-9149.
- ↑ Januzzi, James L; Isselbacher, Eric M; Fattori, Rossella; Cooper, Jeanna V; Smith, Dean E; Fang, Jianming; Eagle, Kim A; Mehta, Rajendra H; Nienaber, Christoph A; Pape, Linda A (2004). “Characterizing the young patient with aortic dissection: results from the international registry of aortic dissection (IRAD)”. Journal of the American College of Cardiology. 43 (4): 665–669. doi:10.1016/j.jacc.2003.08.054. ISSN 0735-1097.
- ↑ “Correspondence”. The Annals of Thoracic Surgery. 67 (2): 593. 1999. doi:10.1016/S0003-4975(99)00037-5. ISSN 0003-4975.
- ↑ Losenno, Katie L.; Goodman, Robert L.; Chu, Michael W. A. (2012). “Bicuspid Aortic Valve Disease and Ascending Aortic Aneurysms: Gaps in Knowledge”. Cardiology Research and Practice. 2012: 1–16. doi:10.1155/2012/145202. ISSN 2090-8016.
- ↑ Senaha S, Uezu T, Shimoji M, Akasaki M (March 2015). “[Stanford type B aortic dissection associated with coarctation of the aorta]”. Kyobu Geka (in Japanese). 68 (3): 184–7. PMID 25743550.
- ↑ Dioguardi GS, Pimenta J, Knoplich J, Ghorayeb N, Ramos LR, Giannini SD (June 1994). “[Risk factors for cardiovascular diseases in physicians. Preliminary data from the VIDAM Project of the Paulista Medical Association]”. Arq. Bras. Cardiol. (in Portuguese). 62 (6): 383–8. PMID 7826227.
- ↑ Caglayan, Ahmet Okay; Dundar, Munis (2009). “Inherited diseases and syndromes leading to aortic aneurysms and dissections”. European Journal of Cardio-Thoracic Surgery. 35 (6): 931–940. doi:10.1016/j.ejcts.2009.01.006. ISSN 1010-7940.
- ↑ “Acute aortic dissection: pathogenesis, risk factors and diagnosis”. Swiss Medical Weekly. 147 (3334). 2017. doi:10.4414/smw.2017.14489. ISSN 1424-7860.
- ↑ Increased maternal cardiovascular mortality associated with pregnancy in women with Turner syndrome.
- ↑ 10.0 10.1 Hiratzka LF, Bakris GL, Beckman JA, Bersin RM, Carr VF, Casey DE; et al. (2010). “2010 ACCF/AHA/AATS/ACR/ASA/SCA/SCAI/SIR/STS/SVM guidelines for the diagnosis and management of patients with Thoracic Aortic Disease: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines, American Association for Thoracic Surgery, American College of Radiology, American Stroke Association, Society of Cardiovascular Anesthesiologists, Society for Cardiovascular Angiography and Interventions, Society of Interventional Radiology, Society of Thoracic Surgeons, and Society for Vascular Medicine”. Circulation. 121 (13): e266–369. doi:10.1161/CIR.0b013e3181d4739e. PMID 20233780.
- ↑ 11.0 11.1 11.2 11.3 Hagan PG, Nienaber CA, Isselbacher EM, Bruckman D, Karavite DJ, Russman PL, Evangelista A, Fattori R, Suzuki T, Oh JK, Moore AG, Malouf JF, Pape LA, Gaca C, Sechtem U, Lenferink S, Deutsch HJ, Diedrichs H, Marcos y Robles J, Llovet A, Gilon D, Das SK, Armstrong WF, Deeb GM, Eagle KA (February 2000). “The International Registry of Acute Aortic Dissection (IRAD): new insights into an old disease”. JAMA. 283 (7): 897–903. doi:10.1001/jama.283.7.897. PMID 10685714.
- ↑ 12.0 12.1 Coady MA, Davies RR, Roberts M, Goldstein LJ, Rogalski MJ, Rizzo JA, Hammond GL, Kopf GS, Elefteriades JA (April 1999). “Familial patterns of thoracic aortic aneurysms”. Arch Surg. 134 (4): 361–7. doi:10.1001/archsurg.134.4.361. PMID 10199307.
- ↑ 13.0 13.1 von Kodolitsch Y, Schwartz AG, Nienaber CA (October 2000). “Clinical prediction of acute aortic dissection”. Arch. Intern. Med. 160 (19): 2977–82. doi:10.1001/archinte.160.19.2977. PMID 11041906.
- ↑ Mészáros I, Mórocz J, Szlávi J, Schmidt J, Tornóci L, Nagy L, Szép L (May 2000). “Epidemiology and clinicopathology of aortic dissection”. Chest. 117 (5): 1271–8. doi:10.1378/chest.117.5.1271. PMID 10807810.
- ↑ Spittell PC, Spittell JA, Joyce JW, Tajik AJ, Edwards WD, Schaff HV, Stanson AW (July 1993). “Clinical features and differential diagnosis of aortic dissection: experience with 236 cases (1980 through 1990)”. Mayo Clin. Proc. 68 (7): 642–51. doi:10.1016/s0025-6196(12)60599-0. PMID 8350637.
- ↑ Mehta RH, O’Gara PT, Bossone E, Nienaber CA, Myrmel T, Cooper JV, Smith DE, Armstrong WF, Isselbacher EM, Pape LA, Eagle KA, Gilon D (August 2002). “Acute type A aortic dissection in the elderly: clinical characteristics, management, and outcomes in the current era”. J. Am. Coll. Cardiol. 40 (4): 685–92. doi:10.1016/s0735-1097(02)02005-3. PMID 12204498.
- ↑ 17.0 17.1 Klompas M (May 2002). “Does this patient have an acute thoracic aortic dissection?”. JAMA. 287 (17): 2262–72. doi:10.1001/jama.287.17.2262. PMID 11980527.
- ↑ Januzzi JL, Isselbacher EM, Fattori R, Cooper JV, Smith DE, Fang J, Eagle KA, Mehta RH, Nienaber CA, Pape LA (February 2004). “Characterizing the young patient with aortic dissection: results from the International Registry of Aortic Dissection (IRAD)”. J. Am. Coll. Cardiol. 43 (4): 665–9. doi:10.1016/j.jacc.2003.08.054. PMID 14975480.
- ↑ Armstrong WF, Bach DS, Carey LM, Froehlich J, Lowell M, Kazerooni EA (December 1998). “Clinical and echocardiographic findings in patients with suspected acute aortic dissection”. Am. Heart J. 136 (6): 1051–60. doi:10.1016/s0002-8703(98)70162-0. PMID 9842019.
- ↑ 20.0 20.1 Gaul C, Dietrich W, Friedrich I, Sirch J, Erbguth FJ (February 2007). “Neurological symptoms in type A aortic dissections”. Stroke. 38 (2): 292–7. doi:10.1161/01.STR.0000254594.33408.b1. PMID 17194878.
- ↑ Roberts WC, Ko JM, Moore TR, Jones WH (August 2006). “Causes of pure aortic regurgitation in patients having isolated aortic valve replacement at a single US tertiary hospital (1993 to 2005)”. Circulation. 114 (5): 422–9. doi:10.1161/CIRCULATIONAHA.106.622761. PMID 16864725.
Screening
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Aarti Narayan, M.B.B.S [2]; Raviteja Guddeti, M.B.B.S. [3]; Laith Adnan Allaham, M.D.[4]
Overview
Screening guidelines state that an EKG should be obtained for all patients who present with symptoms suspicious for aortic dissection. A chest x ray should be obtained in patients determined to be at low-risk and moderate-risk. In patients in high-risk categories, TEE, CT or MRI should be obtained.
Screening
2010 ACCF/AHA/AATS/ACR/ASA/SCA/SCAI/SIR/STS/SVM Guidelines for the Diagnosis and Management of Patients With Thoracic Aortic Disease (DO NOT EDIT)[1]
| Class I |
| “1. An electrocardiogram should be obtained on all patients who present with symptoms that may represent acute thoracic aortic dissection. |
| a. Given the relative infrequency of dissection-related coronary artery occlusion, the presence of ST-segment elevation suggestive of myocardial infarction should be treated as a primary cardiac event without delay for definitive aortic imaging unless the patient is at high risk for aortic dissection.[2][3] (Level of Evidence: B)” |
| “2. The role of chest x-ray in the evaluation of possible thoracic aortic disease should be directed by the patient’s pretest risk of disease as follows: |
| a. Intermediate risk: Chest x-ray should be performed on all intermediate-risk patients, as it may establish a clear alternate diagnosis that will obviate the need for definitive aortic imaging. (Level of Evidence: C) |
| b. Low risk: Chest x-ray should be performed on all low-risk patients, as it may either establish an alternative diagnosis or demonstrate findings that are suggestive of thoracic aortic disease, indicating the need for urgent definitive aortic imaging. (Level of Evidence: C)” |
| “3. Urgent and definitive imaging of the aorta using transesophageal echocardiogram, computed tomographic imaging, or magnetic resonance imaging is recommended to identify or exclude thoracic aortic dissection in patients at high risk for the disease by initial screening.[4][5][6][7][8][9][10] (Level of Evidence: B)” |
| Class III (No Benefit) |
| “1. A negative chest x-ray should not delay definitive aortic imaging in patients determined to be high risk for aortic dissection by initial screening. (Level of Evidence: C)” |
Genetic Syndromes of Familial Thoracic Aortic Aneurysms and Dissections (DO NOT EDIT) [1]
| Class IIa |
| “1. Sequencing of the ACTA2 gene is reasonable in patients with a family history of thoracic aortic aneurysms and/or dissections to determine if ACTA2 mutations are responsible for the inherited predisposition.[11][12][13][14][15][16] (Level of Evidence: B)” |
| Class IIb |
| “1. Sequencing of other genes known to cause familial thoracic aortic aneurysms and/or dissection (TGFBR1, TGFBR2, MYH11) may be considered in patients with a family history and clinical features associated with mutations in these genes.[11][12][13][14][15][16] (Level of Evidence: B)” |
| “2. If one or more first-degree relatives of a patient with known thoracic aortic aneurysm and/or dissection are found to have thoracic aortic dilatation, aneurysm, or dissection, then referral to a geneticist may be considered. (Level of Evidence: C)” |
References
- ↑ 1.0 1.1 Hiratzka LF, Bakris GL, Beckman JA; et al. (2010). “2010 ACCF/AHA/AATS/ACR/ASA/SCA/SCAI/SIR/STS/SVM guidelines for the diagnosis and management of patients with Thoracic Aortic Disease: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines, American Association for Thoracic Surgery, American College of Radiology, American Stroke Association, Society of Cardiovascular Anesthesiologists, Society for Cardiovascular Angiography and Interventions, Society of Interventional Radiology, Society of Thoracic Surgeons, and Society for Vascular Medicine”. Circulation. 121 (13): e266–369. doi:10.1161/CIR.0b013e3181d4739e. PMID 20233780. Unknown parameter
|month=ignored (help) - ↑ Hagan PG, Nienaber CA, Isselbacher EM; et al. (2000). “The International Registry of Acute Aortic Dissection (IRAD): new insights into an old disease”. JAMA. 283 (7): 897–903. PMID 10685714. Unknown parameter
|month=ignored (help) - ↑ Klompas M (2002). “Does this patient have an acute thoracic aortic dissection?”. JAMA. 287 (17): 2262–72. PMID 11980527. Unknown parameter
|month=ignored (help) - ↑ Yoshida S, Akiba H, Tamakawa M; et al. (2003). “Thoracic involvement of type A aortic dissection and intramural hematoma: diagnostic accuracy–comparison of emergency helical CT and surgical findings”. Radiology. 228 (2): 430–5. doi:10.1148/radiol.2282012162. PMID 12819341. Unknown parameter
|month=ignored (help) - ↑ Sommer T, Fehske W, Holzknecht N; et al. (1996). “Aortic dissection: a comparative study of diagnosis with spiral CT, multiplanar transesophageal echocardiography, and MR imaging”. Radiology. 199 (2): 347–52. PMID 8668776. Unknown parameter
|month=ignored (help) - ↑ Zeman RK, Berman PM, Silverman PM; et al. (1995). “Diagnosis of aortic dissection: value of helical CT with multiplanar reformation and three-dimensional rendering”. AJR Am J Roentgenol. 164 (6): 1375–80. PMID 7754876. Unknown parameter
|month=ignored (help) - ↑ Shiga T, Wajima Z, Apfel CC, Inoue T, Ohe Y (2006). “Diagnostic accuracy of transesophageal echocardiography, helical computed tomography, and magnetic resonance imaging for suspected thoracic aortic dissection: systematic review and meta-analysis”. Arch. Intern. Med. 166 (13): 1350–6. doi:10.1001/archinte.166.13.1350. PMID 16831999. Unknown parameter
|month=ignored (help) - ↑ Nienaber CA, von Kodolitsch Y, Nicolas V; et al. (1993). “The diagnosis of thoracic aortic dissection by noninvasive imaging procedures”. N. Engl. J. Med. 328 (1): 1–9. doi:10.1056/NEJM199301073280101. PMID 8416265. Unknown parameter
|month=ignored (help) - ↑ Erbel R, Engberding R, Daniel W, Roelandt J, Visser C, Rennollet H (1989). “Echocardiography in diagnosis of aortic dissection”. Lancet. 1 (8636): 457–61. PMID 2563839. Unknown parameter
|month=ignored (help) - ↑ Börner N, Erbel R, Braun B, Henkel B, Meyer J, Rumpelt J (1984). “Diagnosis of aortic dissection by transesophageal echocardiography”. Am. J. Cardiol. 54 (8): 1157–8. PMID 6496346. Unknown parameter
|month=ignored (help) - ↑ 11.0 11.1 Pannu H, Fadulu VT, Chang J, Lafont A, Hasham SN, Sparks E; et al. (2005). “Mutations in transforming growth factor-beta receptor type II cause familial thoracic aortic aneurysms and dissections”. Circulation. 112 (4): 513–20. doi:10.1161/CIRCULATIONAHA.105.537340. PMID 16027248.
- ↑ 12.0 12.1 Guo DC, Pannu H, Tran-Fadulu V, Papke CL, Yu RK, Avidan N; et al. (2007). “Mutations in smooth muscle alpha-actin (ACTA2) lead to thoracic aortic aneurysms and dissections”. Nat Genet. 39 (12): 1488–93. doi:10.1038/ng.2007.6. PMID 17994018.
- ↑ 13.0 13.1 Zhu L, Vranckx R, Khau Van Kien P, Lalande A, Boisset N, Mathieu F; et al. (2006). “Mutations in myosin heavy chain 11 cause a syndrome associating thoracic aortic aneurysm/aortic dissection and patent ductus arteriosus”. Nat Genet. 38 (3): 343–9. doi:10.1038/ng1721. PMID 16444274.
- ↑ 14.0 14.1 Loeys BL, Schwarze U, Holm T, Callewaert BL, Thomas GH, Pannu H; et al. (2006). “Aneurysm syndromes caused by mutations in the TGF-beta receptor”. N Engl J Med. 355 (8): 788–98. doi:10.1056/NEJMoa055695. PMID 16928994.
- ↑ 15.0 15.1 Stheneur C, Collod-Béroud G, Faivre L, Gouya L, Sultan G, Le Parc JM; et al. (2008). “Identification of 23 TGFBR2 and 6 TGFBR1 gene mutations and genotype-phenotype investigations in 457 patients with Marfan syndrome type I and II, Loeys-Dietz syndrome and related disorders”. Hum Mutat. 29 (11): E284–95. doi:10.1002/humu.20871. PMID 18781618.
- ↑ 16.0 16.1 Guo DC, Papke CL, Tran-Fadulu V, Regalado ES, Avidan N, Johnson RJ; et al. (2009). “Mutations in smooth muscle alpha-actin (ACTA2) cause coronary artery disease, stroke, and Moyamoya disease, along with thoracic aortic disease”. Am J Hum Genet. 84 (5): 617–27. doi:10.1016/j.ajhg.2009.04.007. PMC 2680995. PMID 19409525.
Natural History, Complications and Prognosis
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor-In-Chief: Cafer Zorkun, M.D., Ph.D. [2] Sahar Memar Montazerin, M.D.[3]
Overview
The symptoms of aortic dissection usually develop in the fifth decade of life and start with symptoms such as sudden onset chest/back pain. If left untreated, patients with aortic dissection may progress to develop aortic regurgitation, myocardial ischemia, and cardiac tamponade. The complications of aortic dissection include but not limited to aortic rupture, pericardial tamponade, myocardial ischemia, compression of nearby organs and etc. Aortic dissection carries a poor prognosis. Mortality rate differs based on the type of dissection and is higher in type A compared to type B (25% versus 12%).
Natural History, Complications, and Prognosis
Natural History
- The symptoms of aortic dissection usually develop in the fifth decade of life and start with symptoms such as sudden onset chest/back pain.[1]
- If left untreated, patients with aortic dissection may progress to develop aortic regurgitation, myocardial ischemia, and cardiac tamponade.
Complications
The complications of aortic dissection include:[2][3][4][5][6][7]
Cardiovascualr Complications
- Aortic rupture
- Pericardial tamponade
- Acute aortic regurgitation
- Myocardial ischemia
- Thoracic aortic aneurysm
- Renal ischemia
- Superior mesenteric artery dissection and resultant visceral ischemia
- Pleural effusion
- Claudication due to an extension of the dissection into the iliac arteries
Neurologic Complications
- Ischemic cerebrovascular accident (CVA) due to dissection into the head vessels
- Hemiplegia due to dissection into the spinal arteries
- Hemianesthesia due to dissection into the spinal arteries
Compression of Nearby Organs
- Superior vena cava syndrome due to compression of the superior vena cava
- Horner syndrome (compression of the superior cervical ganglia)
- Dysphagia due to (compression of the esophagus)
- Stridor and wheezing (compression of the airway)
- Hemoptysis (compression of and erosion into the bronchus)
- Vocal cord paralysis and hoarseness (compression of the recurrent laryngeal nerve)
Prognosis
- Aortic dissection carries a poor prognosis.[8]
- Mortality rate differs based on the type of dissection and is higher in type A compared to type B (25% versus 12%).
References
- ↑ Juang, Derek; Braverman, Alan C.; Eagle, Kim (2008). “Aortic Dissection”. Circulation. 118 (14). doi:10.1161/CIRCULATIONAHA.108.799908. ISSN 0009-7322.
- ↑ Cambria, Richard P.; Brewster, David C.; Gertler, Jonathan; Moncure, Ashby C.; Gusberg, Richard; Tilson, M.David; Darling, R.Clement; Hammond, Grahme; Megerman, Joseph; Abbott, William M. (1988). “Vascular complications associated with spontaneous aortic dissection”. Journal of Vascular Surgery. 7 (2): 199–209. doi:10.1016/0741-5214(88)90137-1. ISSN 0741-5214.
- ↑ Fadahunsi, Opeyemi; Romeo, Michael (2014). “Cardiac tamponade – presentation of type A aortic dissection”. Journal of Community Hospital Internal Medicine Perspectives. 4 (5): 25449. doi:10.3402/jchimp.v4.25449. ISSN 2000-9666.
- ↑ Cai, Jingjing; Cao, Yu; Yuan, Hong; Yang, Kan; Zhu, Yuan-Shan (2012). “Inferior myocardial infarction secondary to aortic dissection associated with bicuspid aortic valve”. Journal of Cardiovascular Disease Research. 3 (2): 138–142. doi:10.4103/0975-3583.95370. ISSN 0975-3583.
- ↑ Siegelman, Stanley S.; Sprayregen, Seymour; Strasberg, Zeno; Attai, Lari A.; Robinson, George (1970). “Aortic Dissection and the Left Renal Artery”. Radiology. 95 (1): 73–78. doi:10.1148/95.1.73. ISSN 0033-8419.
- ↑ Blanco, M.; Díez-Tejedor, E.; Larrea, J. L.; Ramírez, U. (1999). “Neurologic complications of type I aortic dissection”. Acta Neurologica Scandinavica. 99 (4): 232–235. doi:10.1111/j.1600-0404.1999.tb07352.x. ISSN 0001-6314.
- ↑ Arata, Kenichi; Imagama, Itsumi; Shigehisa, Yoshiya; Mukaihara, Kousuke; Toyokawa, Kenji; Matsuba, Tomoyuki; Imoto, Yutaka (2015). “Aortic Fenestration for Type B Chronic Aortic Dissection Complicated with Lower Limb Malperfusion Induced by Walking Exercise”. Annals of Vascular Diseases. 8 (1): 29–32. doi:10.3400/avd.cr.14-00101. ISSN 1881-641X.
- ↑ “Correspondence”. The Annals of Thoracic Surgery. 67 (2): 593. 1999. doi:10.1016/S0003-4975(99)00037-5. ISSN 0003-4975.
Diagnosis
Diagnosis
History and Symptoms | Physical Examination | Laboratory Findings | Electrocardiogram | Imaging in Aortic Dissection | Chest X Ray | CT | MRI | Echocardiography | Aortography | Coronary Angiography | Other Diagnostic Studies
Looking for the patient version?
© 2026 MyEClinic – IFTM Institut für Telematik in der Medizin GmbH