
Endocarditis
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-In-Chief: Fahimeh Shojaei, M.D., Maliha Shakil, M.D. [2], Cafer Zorkun, M.D., Ph.D. [3]; Michael W. Tempelhof M.D., Dima Nimri, M.D. [4]
Synonyms and keywords: Infective Endocarditis (IE); Subacute bacterial endocarditis (SBE); Acute bacterial endocarditis; Fungal endocarditis; Nosocomial infective endocarditis; Intravenous drug abuse endocarditis; Intravenous drug abuse infective endocarditis; Prosthetic valve endocarditis; Endocardial infection; Native valve endocarditis; HACEK endocarditis; Bloodstream infection
Overview
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor-in-Chief: Maliha Shakil, M.D. [2] Cafer Zorkun, M.D., Ph.D. [3] Kosar Doraghi, M.D.[4]
Overview
Endocarditis is an inflammation of the inner layer of the heart, the endocardium. It usually involves the heart valves. While acute bacterial endocarditis is caused by an infection with a virulent organism such as Staphylococcus aureus, group A or other beta-hemolytic streptococci, subacute bacterial endocarditis is an indolent infection with less virulent organisms such as streptococcus viridans. Patients with unexplained fever for more than 48 hours and who are at high risk for infective endocarditis and patients among whom valve regurgitation is newly diagnosed should undergo a diagnostic workup to rule out endocarditis. The diagnosis of endocarditis depends on a thorough history and physical exam as well as on the results of the blood cultures and the findings on transthoracic echocardiogram or transesophageal echocardiogram. The modified Duke criteria is used to establish the diagnosis of endocarditis. Endocarditis is initially treated with empiric antibiotic therapy until the causative agent is identified.
Historical Perspective
Endocarditis was first described in 1554. The inflammatory process associated with endocarditis was discovered in 1799. Vegetations were first discovered to be associated with endocarditis in 1806.
Classification
Endocarditis may be classified based on the underlying pathophysiology of the process (infective vs. non-infective), the onset of the disease (acute vs. subacute or short incubation vs. long incubation), results of the cultures (culture-positive vs. culture-negative), the nature of the valve (native vs. prosthetic) and the valve affected (aortic, mitral, or tricuspid valve).
Pathophysiology
The pathogenesis of infective endocarditis includes valvular damage, altered and turbulent flow, bacteremia, and lack of blood supply to the valves. Damaged endothelium becomes a site for attachment of infectious agents in infectious endocarditis. Nonbacterial thrombotic endocarditis is related to hypercoagulable states such as pregnancy or systemic bacterial infection. The characteristic lesion of endocarditis is vegetation. Vegetations are composed of fibrin, inflammatory cells, platelets, and microorganisms.
Causes
The majority of cases of infective endocarditis are due to bacteria. Common causes of infective endocarditis include Streptococcus viridans, Staphylococci, and Enterococcus.
Differentiating Endocarditis From Other Diseases
Endocarditis must be differentiated from other causes of a fever of unknown origin (FUO) such as pulmonary embolism, deep vein thrombosis, lymphoma, drug fever, cotton fever, and disseminated granulomatosis.
Risk Factors
Common risk factors for endocarditis include prosthetic heart valves, valvular heart disease, congenital heart disease, intravenous drug use, age-related degenerative valvular lesions, immunosuppression, and colon cancer.
Epidemiology and Demographics
The incidence of native valve infective endocarditis is approximately 1.7-6.2 cases per 100,000 individuals per year in the United States and Europe. The prevalence of infective endocarditis among IV drug users ranges from 10 to 15%. The incidence of endocarditis increases with age; the median age of patients is 47 to 69 years. There is an increased incidence of infective endocarditis in persons 65 years of age and older. Males are more commonly affected with endocarditis than females. The male to female ratio is approximately 1.7:1.
Natural History, Complications, and Prognosis
If left untreated, patients with endocarditis may progress to develop congestive heart failure. Complications of endocarditis can occur as a result of the locally destructive effects of the infection. These complications include perforation of valve leaflets causing congestive heart failure, abscesses, and disruption of the heart’s conduction system. Endocarditis may also cause embolization to the brain (causing a stroke), to the coronary artery (causing a heart attack), to the lung (causing pulmonary embolism), to the spleen (causing a splenic infarct), and to the kidney (causing a renal infarct). Prognosis of endocarditis is generally poor and the overall mortality rate for both native and prosthetic valve endocarditis ranges from 20-25%. The mortality rate for right-sided endocarditis in injection drug users is approximately 10%. The 5 year survival rate for native valve endocarditis is 70-80% and 50-80% for prosthetic valve endocarditis.
Diagnosis
Diagnostic Criteria
The Duke criteria can be used to establish the diagnosis of endocarditis. The Duke clinical criteria for infective endocarditis require either: Two major criteria, or one major and three minor criteria, or five minor criteria.
History and Symptoms
Common symptoms of endocarditis include fever, chills, new onset of murmur, anorexia, malaise, weight loss, and back pain.
Physical Examination
Common signs on physical examination of endocarditis include fever, rigors, osler’s nodes, janeway lesions and evidence of embolization. Aortic insufficiency with a wide pulse pressure, mitral regurgitation or tricuspid regurgitation may be present depending upon the valve that is infected.
Laboratory Tests
Two blood cultures should be ordered when infective endocarditis is suspected. Laboratory findings consistent with the diagnosis of endocarditis include elevated white blood cell count, erythrocyte sedimentation rate, rheumatoid factor, and elevated BUN and creatinine if glomerulonephritis is present.
Chest x-ray
On chest x-ray, right sided endocarditis is characterized by pleural effusions, multiple round densities, and cavitary multilobar infiltrates.
Electrocardiography
On EKG, endocarditis may be characterized by conduction abnormalities, low QRS voltage, ST elevation, heart block, ventricular tachycardia, and supraventricular tachycardia. The EKG may show ST elevation in the presence of embolization of a vegetation or clot down the coronary artery.
Cardiac MRI
Findings on cardiac MRI suggestive of infective endocarditis include valvular vegetations, valvular and perivalvular damage, and vascular endothelial involvement.
CT Scan
CT scans may be helpful in the diagnosis of endocarditis. CT scan findings suggestive of endocarditis include vegetations, paravalvular abscesses, and pseudoaneurysms.
Echocardiography
Echocardiography may be diagnostic of endocarditis. Echocardiography allows detection of microbial vegetations and the degree of valvular dysfunction. Findings on transthoracic and transesophageal echocardiogram diagnostic of endocarditis include vegetations, valvular regurgitation, pseudoaneurysms, paravalvular abscess, and fistulas.
Treatment
Medical Therapy
Antimicrobial therapy is the mainstay of therapy for endocarditis. Empiric antimicrobial therapy depends on the nature of the valve (native vs. prosthetic) and the onset of endocarditis following valve implantation (less than 1 year vs. more than 1 year). In patients with endocarditis, antithrombotic therapy may be administered when needed. The prothrombin time must be carefully monitored as anticoagulants may cause or worsen hemorrhage in patients with endocarditis. Heparin administration should be avoided if possible.
2023 ESC Guidelines for the management of endocarditis ESC Clinical Practice Guidelines (DO NOT EDIT)
New recommendations (DO NOT EDIT)[1]
Recommendations for antibiotic prophylaxis in patients with cardiovascular diseases undergoing oro-dental procedures at increased risk of infective endocarditis (DO NOT EDIT)
| Class I |
| “1. (General prevention measures are recommended in individuals at high and intermediate risk of IE) (Level of Evidence: C)“[2] |
| ”2. (Antibiotic prophylaxis is recommended in patients with ventricular assist devices) (Level of Evidence: C)“[3] |
| Class IIb |
| “1. (Antibiotic prophylaxis may be considered in recipients of heart transplant) (Level of Evidence: C)” |
Recommendations for infective endocarditis prevention in high-risk patients (DO NOT EDIT)
| Class IIb |
| “1. (Systemic antibiotic prophylaxis may be considered for
high-risk patients undergoing an invasive diagnostic or therapeutic procedure of the respiratory, gastrointestinal, genitourinary tract, skin, or musculoskeletal systems) (Level of Evidence: C)” |
Recommendations for infective endocarditis prevention in cardiac procedures (DO NOT EDIT)
| Class I |
| “1. (Optimal pre-procedural aseptic measures of the site of implantation is recommended to prevent CIED infections.) (Level of Evidence: B)” |
| ”2. (Surgical standard aseptic measures are recommended during the insertion and manipulation of catheters in the catheterization laboratory environment) (Level of Evidence: C)” |
| Class II |
| “1. (Antibiotic prophylaxis covering for common skin flora including Enterococcus spp. and S. aureus should be considered before TAVI and other transcatheter valvular procedures) (Level of Evidence: C)” |
Recommendations for the role of echocardiography in infective endocarditis (DO NOT EDIT)
| Class I |
| “1. (TOE is recommended when the patient is stable before switching from intravenous to oral antibiotic therapy) (Level of Evidence: B)” |
Recommendations for the role of computed tomography, nuclear imaging, and magnetic resonance in infective endocarditis (DO NOT EDIT)
| Class I |
| “1. (Cardiac CTA is recommended in patients with possible NVE to detect valvular lesions and confirm the diagnosis of IE) (Level of Evidence: B)” |
| ”2. ([18F]FDG-PET/CT(A) and cardiac CTA are recommended in possible PVE to detect valvular lesions and confirm the diagnosis of IE.) (Level of Evidence: B)” |
| Class IIb |
| “1. ([18F]FDG-PET/CT(A) may be considered in possible CIED-related IE to confirm the diagnosis of IE.) (Level of Evidence: B)” |
| Class I |
| “1. (Cardiac CTA is recommended in NVE and PVE to diagnose paravalvular or periprosthetic complications if echocardiography is inconclusive.) (Level of Evidence: B)” |
| ”2. (Brain and whole-body imaging (CT, [18F]FDG-PET/CT, and/or MRI) are recommended in symptomatic patients with NVE and PVE to detect peripheral lesions or add minor diagnostic criteria) (Level of Evidence: B)” |
| Class II |
| “1. (WBC SPECT/CT should be considered in patients with high clinical suspicion of PVE when echocardiography is negative or inconclusive and when PET/CT is unavailable) (Level of Evidence: C)” |
| Class IIb |
| “1. (Brain and whole-body imaging (CT, [18F]FDG-PET/ CT, and MRI) in NVE and PVE may be considered for screening of peripheral lesions in asymptomatic patients) (Level of Evidence: B)” |
Recommendations for outpatient antibiotic treatment of infective endocarditis (DO NOT EDIT)
| Class II |
| “1. (Outpatient parenteral antibiotic treatment should be considered in patients with left-sided IE caused by Streptococcus spp., E. faecalis, S. aureus, or CoNS who were receiving appropriate i.v. antibiotic treatment for at least 10 days (or at least 7 days after cardiac surgery), are clinically stable, and who do not show signs of abscess formation or valve abnormalities requiring surgery on TOE) (Level of Evidence: A)” |
| Class III |
| “1. (Outpatient parenteral antibiotic treatment is not recommended in patients with IE caused by highly difficult-to-treat microorganisms, liver cirrhosis (Child–Pugh B or C), severe cerebral nervous system emboli, untreated large extracardiac abscesses, heart valve complications, or other severe conditions requiring surgery, severe post-surgical complications, and in PWID-related IE.) (Level of Evidence: C)” |
Recommendations for the treatment of neurological complications of infective endocarditis (DO NOT EDIT)
| Class IIb |
| “1. (In embolic stroke, mechanical thrombectomy may be considered if the expertise is available in a timely manner) (Level of Evidence: C)” |
| Class III |
| “1. (Thrombolytic therapy is not recommended in embolic stroke due to IE) (Level of Evidence: C)” |
Recommendations for pacemaker implantation in patients with complete atrioventricular block and infective endocarditis (DO NOT EDIT)
| Class II |
| “1. (Immediate epicardial pacemaker implantation should be considered in patients undergoing surgery for valvular IE and complete AVB if one of the following predictors of persistent AVB is present: pre-operative conduction abnormality, S. aureus infection, aortic root abscess, tricuspid valve involvement, or previous valvular surgery) (Level of Evidence: C)” |
Recommendations for patients with musculoskeletal manifestations of infective endocarditis (DO NOT EDIT)
| Class I |
| “1. (MRI or PET/CT is recommended in patients with suspected spondylodiscitis and vertebral osteomyelitis complicating IE) (Level of Evidence: C)” |
| ”2. (TTE/TOE is recommended to rule out IE in patients with spondylodiscitis and/or septic arthritis with positive blood cultures for typical IE microorganisms) (Level of Evidence: C)” |
| Class II |
| “1. (More than 6-week antibiotic therapy should be considered in patients with osteoarticular IE-related lesions caused by difficult-to-treat microorganisms, such as S. aureus or Candida spp., and/or complicated with severe vertebral destruction or abscesses) (Level of Evidence: C)” |
Recommendations for pre-operative coronary anatomy assessment in patients requiring surgery for infective endocarditis (DO NOT EDIT)
| Class I |
| “1. (In haemodynamically stable patients with aortic valve vegetations who require cardiac surgery and are high risk of CAD, a high-resolution multislice coronary CTA is recommended) (Level of Evidence: B)” |
| ”2. (Invasive coronary angiography is recommended in patients requiring heart surgery who are high risk of CAD, in the absence of aortic valve vegetations.) (Level of Evidence: C)” |
| Class II |
| “1. (In emergency situations, valvular surgery without pre-operative coronary anatomy assessment regardless of CAD risk should be considered.) (Level of Evidence: C)” |
| Class IIb |
| “1. (Invasive coronary angiography may be considered despite the presence of aortic valve vegetations in selected patients with known CAD or at high risk of significant obstructive CAD.) (Level of Evidence: C)” |
Indications and timing of cardiac surgery after neurological complications in active infective endocarditis (DO NOT EDIT)
| Class II |
| “1. (In patients with intracranial haemorrhage and unstable clinical status due to HF, uncontrolled infection, or persistent high embolic risk, urgent or emergency surgery should be considered weighing the likelihood of a meaningful neurological outcome.) (Level of Evidence: C)” |
Recommendations for post-discharge follow-up (DO NOT EDIT)
| Class I |
| “1. (Patient education on the risk of recurrence and preventive measures, with emphasis on dental health, and based on the individual risk profile, is recommended during follow-up.) (Level of Evidence: C)” |
| ”2. (Addiction treatment for patients following PWID-related IE is recommended) (Level of Evidence: C)” |
| Class II |
| “1. (Cardiac rehabilitation including physical exercise training should be considered in clinically stable patients based on an individual assessment.) (Level of Evidence: C)” |
| Class IIb |
| “1. (Psychosocial support may be considered to be integrated in follow-up care, including screening for anxiety and depression, and referral to relevant psychological treatment.) (Level of Evidence: C)” |
Recommendations for prosthetic valve endocarditis (DO NOT EDIT)
| Class I |
| “1. (Surgery is recommended for early PVE (within 6 months of valve surgery) with new valve replacement and complete debridement) (Level of Evidence: C)” |
Recommendations for cardiovascular implanted electronic device-related infective endocarditis (DO NOT EDIT)
| Class I |
| “1. (Complete system extraction without delay is recommended in patients with definite CIED-related IE under initial empirical antibiotic therapy.) (Level of Evidence: B)” |
| Class II |
| “1. (Extension of antibiotic treatment of CIED-related endocarditis to (4–)6 weeks following device extraction should be considered in the presence of septic emboli or prosthetic valves.) (Level of Evidence: C)” |
| Class IIb |
| “1. (Use of an antibiotic envelope may be considered in select high-risk patients undergoing CIED reimplantation to reduce risk of infection) (Level of Evidence: B)” |
| “1. (In non-S. aureus CIED-related endocarditis without valve involvement or lead vegetations, and if follow-up blood cultures are negative without septic emboli, 2 weeks of antibiotic treatment may be considered following device extraction.) (Level of Evidence: C)” |
| Class III |
| “1. (Removal of CIED after a single positive blood culture, with no other clinical evidence of infection, is not recommended) (Level of Evidence: C)” |
Recommendations for the surgical treatment of right-sided infective endocarditis (DO NOT EDIT)
| Class II |
| “1. (Tricuspid valve repair should be considered instead of valve replacement, when possible.) (Level of Evidence: B)” |
| ”2. (Surgery should be considered in patients with right-sided IE who are receiving appropriate antibiotic therapy and present persistent bacteraemia/sepsis after at least 1 week of appropriate antibiotic therapy.) (Level of Evidence: C)” |
| ”3. (Prophylactic placement of an epicardial pacing lead should be considered at the time of tricuspid valve surgical procedures) (Level of Evidence: C)” |
| Class II |
| “1. (Debulking of right intra-atrial septic masses by aspiration may be considered in select patients who are high risk of surgery.) (Level of Evidence: C)” |
2023 Recommendations for antibiotic prophylaxis in patients with cardiovascular diseases undergoing oro-dental procedures at increased risk for infective endocarditis (DO NOT EDIT)
| Class I |
| “1. (General prevention measures are recommended in individuals at high and intermediate risk for IE.) (Level of Evidence: C)” |
| ”2. (Antibiotic prophylaxis is recommended in patients with previous IE.) (Level of Evidence: B)” |
| ”3. (Antibiotic prophylaxis is recommended in patients with surgically implanted prosthetic valves and with any material used for surgical cardiac valve repair.) (Level of Evidence: C)” |
| ”2. (Antibiotic prophylaxis is recommended in patients with transcatheter implanted aortic and pulmonary valvular prostheses.) (Level of Evidence: C)” |
| ”2. (Antibiotic prophylaxis is recommended in patients with untreated cyanotic CHD, and patients treated with surgery or transcatheter procedures with post-operative palliative shunts, conduits, or other prostheses. After surgical repair, in the absence of residual defects or valve prostheses, antibiotic prophylaxis is recommended only for the first 6 months after the procedure.) (Level of Evidence: C)” |
| ”2. (Antibiotic prophylaxis is recommended in patients with ventricular assist devices.) (Level of Evidence: C)” |
| Class Ila |
| “1. (Antibiotic prophylaxis should be considered in patients with transcatheter mitral and tricuspid valve repair.) (Level of Evidence: C)” |
| Class Ilb |
| “1. (Antibiotic prophylaxis may be considered in recipients of heart transplant.) (Level of Evidence: C)” |
| Class III |
| “1. (Antibiotic prophylaxis is not recommended in other patients at low risk for IE.) (Level of Evidence: C)” |
2023 ESC Guidelines Recommendations for Prophylactic antibiotic regime for high-risk dental procedures

2023 ESC Guidelines Recommendations for Diagnostic Procedures of rare causes of blood culture-negative infective endocarditis

Recommendations for infective endocarditis prevention in high-risk patients (DO NOT EDIT)
| Class I | “1. (Antibiotic prophylaxis is recommended in dental extractions, oral surgery procedures, and procedures requiring manipulation of the gingival or periapical region of the teeth.) (Level of Evidence: B)” |
| Class IIb |
| “1. (Systemic antibiotic prophylaxis may be considered for high-riskc patients undergoing an invasive diagnostic or therapeutic procedure of the respiratory, gastrointestinal, genitourinary tract, skin, or musculoskeletal systems.) (Level of Evidence: C)” |
Recommendations for infective endocarditis prevention in cardiac procedures (DO NOT EDIT)
| Class I |
| “1. (Pre-operative screening for nasal carriage of S. aureus is recommended before elective cardiac surgery or transcatheter valve implantation to treat carriers.) (Level of Evidence: A)” |
| ”2. (Peri-operative antibiotic prophylaxis is recommended before placement of a CIED.) (Level of Evidence: A)” |
| ”3. (Optimal pre-procedural aseptic measures of the site of implantation is recommended to prevent CIED infections.) (Level of Evidence: B)” |
| ”3. (Periprocedural antibiotic prophylaxis is recommended in patients undergoing surgical or transcatheter implantation of a prosthetic valve, intravascular prosthetic, or other foreign material.) (Level of Evidence: B)” |
| ”3. (Surgical standard aseptic measures are recommended during the insertion and manipulation of catheters in the catheterization laboratory environment.) (Level of Evidence: C)” |
| Class IIa |
| ”2. (Elimination of potential sources of sepsis (including of dental origin) should be considered ≥2 weeks before implantation of a prosthetic valve or other intracardiac or intravascular foreign material, except in urgent procedures.) (Level of Evidence: C)” |
| ”2. (Antibiotic prophylaxis covering for common skin flora including Enterococcus spp. and S. aureus should be considered before TAVI and other transcatheter valvular procedures.) (Level of Evidence: C)” |
| Class III |
| “1. (Systematic skin or nasal decolonization without screening for S. aureus is not recommended.) (Level of Evidence: C)” |
Recommendations for the Endocarditis Team Recommendations (DO NOT EDIT)
| Class I |
| “1. (Diagnosis and management of patients with complicated IE are recommended to be performed at an early stage in a Heart Valve Centre, with immediate surgical facilities and an Endocarditis Team’ to improve the outcomes.) (Level of Evidence: B)” |
| ”2. (For patients with uncomplicated IE managed in a Referring Centre, early and regular communication between the local and the Heart Valve Centre endocarditis teams is recommended to improve the outcomes of the patients.) (Level of Evidence: B)” |
Recommendations for the role of echocardiography in infective endocarditis (DO NOT EDIT)
| Class I |
| “1. (TTE is recommended as the first-line imaging modality in suspected IE.) (Level of Evidence: B)” |
| ”2. (TOE is recommended in all patients with clinical suspicion of IE and a negative or non-diagnostic TTE.) (Level of Evidence: B)” |
| ”3. (TOE is recommended in patients with clinical suspicion of IE, when a prosthetic heart valve or an intracardiac device is present.) (Level of Evidence: B)” |
| ”3. (Repeating TTE and/or TOE within 5–7 days is recommended in cases of initially negative or inconclusive examination when clinical suspicion of IE remains high.) (Level of Evidence: C)” |
| ”3. (TOE is recommended in patients with suspected IE, even in cases with positive TTE, except in isolated right-sided native valve IE with good quality TTE examination and unequivocal echocardiographic findings.) (Level of Evidence: C)” |
| Class IIa |
| ”2. (Performing an echocardiography should be considered in S. aureus, E. faecalis, and some Streptococcus spp. bacteraemia.) (Level of Evidence: C)” |
| Class I |
| “1. (Repeating TTE and/or TOE is recommended as soon as a new complication of IE is suspected (new murmur, embolism, persisting fever and bacteraemia, HF, abscess, AVB) (Level of Evidence: B)” |
| ”2. (TOE is recommended when patient is stable before switching from intravenous to oral antibiotic therapy.) (Level of Evidence: B)” |
| Class IIa |
| ”2. (During follow-up of uncomplicated IE, repeat TTE and/ or TOE should be considered to detect new silent complications. The timing of repeat TTE and/or TOE depends on the initial findings, type of microorganism, and initial response to therapy.) (Level of Evidence: B)” |
| Class I |
| “1. (Intra-operative echocardiography is recommended in all cases of IE requiring surgery) (Level of Evidence: C)” |
| ”2. (TTE and/or TOE are recommended at completion of antibiotic therapy for evaluation of cardiac and valve morphology and function in patients with IE who did not undergo heart valve surgery.) (Level of Evidence: C)” |
Recommendations for the role of computed tomography, nuclear imaging, and magnetic resonance in infective endocarditis (DO NOT EDIT)
| Class I |
| “1. (Cardiac CTA is recommended in patients with possible NVE to detect valvular lesions and confirm the diagnosis of IE) (Level of Evidence: B)” |
| ”2. ( 18F FDG-PET/CT(A) and cardiac CTA are recommended in possible PVE to detect valvular lesions and confirm the diagnosis of IE) (Level of Evidence: B)” |
| ”3. (Cardiac CTA is recommended in NVE and PVE to diagnose paravalvular or periprosthetic complications if echocardiography is inconclusive.) (Level of Evidence: B)” |
| ”3. (Brain and whole-body imaging (CT, 18F FDG-PET/ CT, and/or MRI) are recommended in symptomaticc patients with NVE and PVE to detect peripheral lesions or add minor diagnostic criteria) (Level of Evidence: B)” |
| Class IIa |
| “1. (WBC SPECT/CT should be considered in patients with high clinical suspicion of PVE when echocardiography is negative or inconclusive and when PET/CT is unavailable.) (Level of Evidence: C)” |
| Class IIb |
| “1. (18F FDG-PET/CT(A) may be considered in possible CIED-related IE to confirm the diagnosis of IE) (Level of Evidence: B)” |
| ”2. (Brain and whole-body imaging (CT, [18F]FDG-PET/ CT, and MRI) in NVE and PVE may be considered for screening of peripheral lesions in asymptomatic patients) (Level of Evidence: B)” |
Definitions of the 2023 European Society of Cardiology modified diagnostic criteria of infective endocarditis (DO NOT EDIT)


Recommendations for antibiotic treatment of infective endocarditis due to oral streptococci and Streptococcus gallolyticus group (DO NOT EDIT)
Penicillin-susceptible oral streptococci and Streptococcus gallolyticus group (DO NOT EDIT)
Standard treatment: 4-week duration in NVE or 6-week duration in PVE (DO NOT EDIT)
| Class I |
| “1. (In patients with IE due to oral streptococci and S. gallolyticus group, penicillin G, amoxicillin, or ceftriaxone are recommended for 4 (in NVE) or 6 weeks (in PVE), using the following doses: *Adult antibiotic dosage and route
Penicillin G 12–18 millionc U/day i.v. either in 4–6 doses or continuously Amoxicillin 100–200 mg/kg/day i.v. in 4–6 doses Ceftriaxone 2 g/day i.v. in 1 dose
Penicillin G 200 000 U/kg/day i.v. in 4–6 divided doses Amoxicillin 100–200c mg/kg/day i.v. in 4–6 doses Ceftriaxone 100 mg/kg/day i.v. in 1 dose) (Level of Evidence: B)” |
Standard treatment: 2-week duration (not applicable to PVE) (DO NOT EDIT)
| Class I |
| “1. (2-week treatment with penicillin G, amoxicillin, ceftriaxone combined with gentamicin is recommended only for the treatment of non-complicated NVE due to oral streptococci and S. gallolyticus in patients with normal renal function using the following doses: *Adult antibiotic dosage and route
Penicillin G 12–18 millionc U/day i.v. either in 4–6 doses or continuously, Amoxicillin 100–200 mg/kg/day i.v. in 4–6 doses, Ceftriaxone 2 g/day i.v. in 1 dose, Gentamicind 3 mg/kg/day i.v. or i.m. in 1 dose.
Penicillin G 200 000 U/kg/day i.v. in 4–6 divided doses, Amoxicillin 100–200 mg/kg/dayc i.v. in 4–6 doses , Ceftriaxone 100 mg/kg i.v. in 1 dose, Gentamicind 3 mg/kg/day i.v. or i.m. in 1 dose or 3 equally divided doses) (Level of Evidence: B)” |
Allergy to beta-lactams (DO NOT EDIT)
| Class I |
| “1. (In patients allergic to beta-lactams and with IE due to oral streptococci and S. gallolyticus, vancomycin for 4 weeks in NVE or for 6 weeks in PVE is recommended using the following doses: *Adult antibiotic dosage and route
Vancomycine 30 mg/kg/day i.v. in 2 doses.
Vancomycine 30 mg/kg/day i.v. in 2 or 3 equally divided doses) (Level of Evidence: C)” |
Oral streptococci and Streptococcus gallolyticus group susceptible, increased exposure or resistant to penicillin (DO NOT EDIT)
| Class I |
| “1. (In patients with NVE due to oral streptococci and S. gallolyticus, penicillin G, amoxicillin, or ceftriaxone for 4 weeks in combination with gentamicin for 2 weeks is recommended using the following doses: *Adult antibiotic dosage and route
Penicillin G 24 million U/day i.v. either in 4–6 doses or continuously, Amoxicillin 12 g/day i.v. in 6 doses, Ceftriaxone 2 g/day i.v. in 1 dose, Gentamicin 3 mg/kg/day i.v. or i.m. in 1 dose) (Level of Evidence: B)” |
”2. (In patients with PVE due to oral streptococci and S. gallolyticus, penicillin G, amoxicillin, or ceftriaxone for 6 weeks combined with gentamicin for 2 weeks is recommended using the following doses:
Penicillin G 24 million U/day i.v. either in 4–6 doses or continuously, Amoxicillin 12 g/day i.v. in 6 doses, Ceftriaxone 2 g/day i.v. in 1 dose, Gentamicind 3 mg/kg/day i.v. or i.m. in 1 dose) (Level of Evidence: B)” |
Sources
- 2023 ESC Guidelines for the management of endocarditis
Developed by the task force on the management of endocarditis of the European Society of Cardiology (ESC) Endorsed by the European Association for Cardio-Thoracic Surgery (EACTS) and the European Association of Nuclear Medicine (EANM)
Surgery
Surgical removal of the valve is necessary for patients who fail to clear micro-organisms from their blood in response to antibiotic therapy, or in patients who develop cardiac failure resulting from destruction of a valve by infection. A removed valve is usually replaced with an artificial valve which may either be mechanical (metallic) or obtained from an animal such as a pig; the latter are termed bioprosthetic valves. Surgical treatment of endocarditis involves excision of all infected valve tissue, drainage and debridement of abscess cavities, repair or replacement of damaged valves, and repair of any associated pathology such as fistulas or septal defects.
Prevention
Prevention of infective endocarditis can be achieved through the administration of antibiotic prophylaxis to high risk subjects who are undergoing high risk procedures. The choice of antibiotic prophylaxis depends on whether the subject can tolerate oral intake or not, as well as on whether patient has allergy to penicillin or not.
References
- ↑ Delgado V, Ajmone Marsan N, de Waha S, Bonaros N, Brida M, Burri H; et al. (2023). “2023 ESC Guidelines for the management of endocarditis”. Eur Heart J. 44 (39): 3948–4042. doi:10.1093/eurheartj/ehad193. PMID 37622656 Check
|pmid=value (help). - ↑ Habib G, Erba PA, Iung B, Donal E, Cosyns B, Laroche C; et al. (2019). “Clinical presentation, aetiology and outcome of infective endocarditis. Results of the ESC-EORP EURO-ENDO (European infective endocarditis) registry: a prospective cohort study”. Eur Heart J. 40 (39): 3222–3232. doi:10.1093/eurheartj/ehz620. PMID 31504413.
- ↑ Maeda K, Hirai Y, Nashi M, Yamamoto S, Taniike N, Takenobu T (2022). “Clinical features and antimicrobial susceptibility of oral bacteria isolated from the blood cultures of patients with infective endocarditis”. J Dent Sci. 17 (2): 870–875. doi:10.1016/j.jds.2021.09.023. PMC 9201522 Check
|pmc=value (help). PMID 35756779 Check|pmid=value (help).
Historical Perspective
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Cafer Zorkun, M.D., Ph.D. [2] Maliha Shakil, M.D. [3]
Overview
Endocarditis was first described in 1554. The inflammatory process associated with endocarditis was discovered in 1799. Vegetations were first discovered to be associated with endocarditis in 1806.
Historical Perspective
Discovery
Important landmarks in the history of endocarditis include the following:[1][2][3][4]
- In 1554: Earliest report of endocarditis in medical books.
- In 1669: Accurately description of tricuspid valve endocarditis.
- In 1646: Description of unusual “outgrowths” from autopsy of a patient with endocarditis; detected murmurs by placing a hand on patient’s chest.
- In 1708: Description of unusual structures in entrance of aorta.
- In 1715: Description of abnormality in aortic valve and mitral valve.
- In 1749: Description of valvular lesions.
- In 1769: Link between infectious disease and endocarditis established; association with spleen observed.
- In 1784: Intracardiac abnormalities accurately drawn.
- In 1797: Relationship between rheumatism and heart disease established.
- In 1799: Inflammatory process associated with endocarditis described.
- In 1806: Described unusual structures in the heart as “vegetations,” syphilitic virus as a causative agent of endocarditis, and theory of antiviral treatment of endocarditis.
- In 1809: Vegetations were described as not “outgrowths” or “buds” but particles adhering to the heart wall.
- In 1816: Invention of cylindrical stethoscope used to listen to heart murmurs; the link between venereal disease and endocarditis dismissed.
- In 1832: Laennec’s observations observed.
- In 1835-40: Named endocardium and endocarditis; described symptoms; herbal tea and bloodletting described as treatment regimen; the link between acute rheumatoid arthritis and endocarditis established.
- In 1852: Consequences of embolization of vegetations throughout body described. Described cutaneous nodules (named “Osler’s nodes” by Libman).
- In 1858-71: Examined fibrin vegetation associated with endocarditis by microscope; coined term “embolism;” discussed role of bacteria, vibrios, and micrococci in endocarditis.
- In 1861: Virchow’s theory on emboli described.
- In 1862: Granulations or foreign elements in blood and valves described.
- In 1868-70: Described infected arterial blood as originating from the heart; proposed scarlet fever as a cause of endocarditis.
- In 1869: Established “parasites” on skin transported to the heart and attached to endocardium; named Mycosis endocarditis.
- In 1872: Microorganisms in vegetations of endocarditis are described.
- In 1878: All cases of endocarditis were infectious in origin.
- In 1878: Combined experimental physiology and infection to produce an animal model of endocarditis in rabbit; noted valve had to be damaged before bacteria grafted onto the valve.
- In 1878: Micrococci enter vessels that valves were fitted into; valves exposed to abnormal mechanical attacks over long period created favorable niche for bacterial colonization.
- In 1879: Virchow’s student; employed early animal model of endocarditis.
- In 1879: Proposed etiology of endocarditis was based on infectious model and treatment should focus on eliminating “parasitic infection”
- In 1880: Working with Pasteur, proposed use of routine blood cultures.
- In 1881-86: Believed endocarditis could appear during various infections; noted translocation of respiratory pathogen from pulmonary lesion to valve through blood.
- In 1883: Believed microorganisms were result, not cause, of endocarditis.
- In 1884: Named disease “infective endocarditis“.
- In 1886: Demonstrated various bacteria introduced to bloodstream could cause endocarditis on valve that had previous lesion.
- In 1885: Synthesized work of others relating to endocarditis.
- In 1899: Described streptococcal, staphylococcal, pneumococcal, and gonococcal endocarditis.
- In 1903: First described “endocarditis lenta”.
- In 1909: Credited by Osler as first to observe cutaneous nodes (named “Osler’s nodes” by Libman) in patients with endocarditis.
- In 1909: Analyzed 150 cases of endocarditis and published diagnostic criteria relating to signs and symptoms.
- In 1910: Described initial classification scheme to include “subacute endocarditis,” with clinical signs/symptoms; absolute diagnosis required blood cultures.
- In 1981: Beth Israel criteria based on strict case definitions described.
- In 1994: New criteria utilizing specific echocardiographic findings.
- In 1995: Antibiotic treatment of adults with infective endocarditis caused by streptococci, enterococci, staphylococci, and HACEK microorganisms described.
- In 1996: Modified Duke Criteria to allow serologic diagnosis of Coxiella burnetii.
- In 1997: Guidelines for preventing bacterial endocarditis established.
- In 1997: Modifications to Duke criteria for clinical diagnosis of native valve and prosthetic valve endocarditis suggested: Analysis of 118 pathologically proven cases.
- In 1998: Guidelines for antibiotic treatment of streptococcal, enterococcal, and staphylococcal endocarditis established.
- In 1998: Antibiotic treatment of infective endocarditis due to viridans streptococci, enterococci, and other streptococci established; recommendations for surgical treatment of endocarditis.
- In 2000: Updated and modified Duke Criteria.
- In 2002: Duke Criteria to include a molecular diagnosis of causal agents.
- In 2001-3: Etiology of Bartonella spp., Tropheryma whipplei, and Coxiella burnetii in endocarditis described.
References
- ↑ Millar BC, Moore JE (2004). “Emerging issues in infective endocarditis”. Emerg Infect Dis. 10 (6): 1110–6. doi:10.3201/eid1006.030848. PMC 3323180. PMID 15207065.
- ↑ Grinberg M, Solimene MC (2011). “Historical aspects of infective endocarditis”. Rev Assoc Med Bras (1992). 57 (2): 228–33. doi:10.1590/s0104-42302011000200023. PMID 21537712.
- ↑ Contrepois, Alain (2012). “Towards a history of infective endocarditis”. Medical History. 40 (1): 25–54. doi:10.1017/S0025727300060658. ISSN 0025-7273.
- ↑ Sordelli C, Fele N, Mocerino R, Weisz SH, Ascione L, Caso P; et al. (2019). “Infective Endocarditis: Echocardiographic Imaging and New Imaging Modalities”. J Cardiovasc Echogr. 29 (4): 149–155. doi:10.4103/jcecho.jcecho_53_19. PMC 7011492 Check
|pmc=value (help). PMID 32089994 Check|pmid=value (help).
Classification
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1] ; Associate Editor(s)-in-Chief: Maliha Shakil, M.D. [2]
Overview
Endocarditis may be classified based on the underlying pathophysiology of the process (infective vs. non-infective), the onset of the disease (acute vs. subacute or short incubation vs. long incubation), results of the cultures (culture-positive vs. culture-negative), the nature of the valve (native vs. prosthetic) and the valve affected (aortic, mitral, or tricuspid valve).
Classification
Endocarditis may be classified into 8 subtypes based on:[1][2][3]
| Classification criterion | Subgroups |
|---|---|
|
|
|
|
|
|
|
|
References
- ↑ Ortiz C, López J, García H, Sevilla T, Revilla A, Vilacosta I; et al. (2014). “Clinical classification and prognosis of isolated right-sided infective endocarditis”. Medicine (Baltimore). 93 (27): e137. doi:10.1097/MD.0000000000000137. PMC 4602814. PMID 25501052.
- ↑ Fernández Guerrero ML, González López JJ, Goyenechea A, Fraile J, de Górgolas M (2009). “Endocarditis caused by Staphylococcus aureus: A reappraisal of the epidemiologic, clinical, and pathologic manifestations with analysis of factors determining outcome”. Medicine (Baltimore). 88 (1): 1–22. doi:10.1097/MD.0b013e318194da65. PMID 19352296.
- ↑ Selton-Suty C, Doco-Lecompte T, Freysz L, Chometon F, Duhoux F, Blangy H; et al. (2008). “[Non-valvular cardiac devices endocarditis]”. Ann Cardiol Angeiol (Paris). 57 (2): 81–7. doi:10.1016/j.ancard.2008.02.005. PMID 18402924.
Pathophysiology
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1] Associate Editor(s)-in-Chief: Maliha Shakil, M.D. [2]
Overview
The pathogenesis of infective endocarditis includes valvular damage, altered and turbulent flow, bacteremia, and lack of blood supply to the valves. Damaged endothelium becomes a site for attachment of infectious agents in infectious endocarditis. Nonbacterial thrombotic endocarditis is related to hypercoagulable states such as pregnancy or systemic bacterial infection. The characteristic lesion of endocarditis is vegetation. Vegetations are composed of fibrin, inflammatory cells, platelets, and microorganisms.
Pathophysiology
Pathogenesis
Infective Endocarditis
- The pathogenesis of infective endocarditis includes:
| Pathogenic Factors | Mechanism |
|---|---|
|
|
|
|
|
|
Nonbacterial Thrombotic Endocarditis
- The exact pathogenesis of nonbacterial thrombotic endocarditis is not completely understood.
- Nonbacterial thrombotic endocarditis (NBTE), also called marantic endocarditis is most commonly found on previously undamaged valves.
- The vegetations in nonbacterial thrombotic endocarditis are sterile and small.
- The vegetations mostly aggregate at the edges of the valve or the cusps.
- We can divide the pathogenesis pathway of nonbacterial endocarditis into to phase:
- Initiating phase
- Immune complexes:[1][2]
- Circulating immune complexes and complement deposition can initiate the process.
- The example for this initiating factor in libman sacks endocarditis in lupus patients.
- Hypoxia:[3][4]
- Some studies demonstrated that hypoxia may lead to tissue factor activation.
- Higher tissue factor level has an association with higher rate of endocarditis.
- Other studies implies that the rate of endocarditis is higher in smokers and patients with chronic lung disease and possibly hypoxia.
- Hypercoagulability:[5][6]
- There is an association between hypercoagulable state and clotting factor abnormalities with initiation of nonbacterial thrombotic endocarditis.
- There is an association between hypercoagulable state and clotting factor abnormalities with initiation of nonbacterial thrombotic endocarditis.
- Carcinomatosis:[7]
- The association between cancer and nonbacterial thrombotic endocarditis is well established.
- In most of the cases of cancer related endocarditis we have abnormal activity of tissue factor.
- Tissue factor may be secreted from promyelocytic leukaemia cells.
- Tissue factor may be expressed on the surface of adenocarcinoma cells which leads to increased expression of tissue factor by endothelial cells.
- Immune complexes:[1][2]
- Verrucae formation
- Initiating phase
Genetics
Genes involved in the pathogenesis of infective endocarditis include:[8]
- Interleukin-6 c.471+870G>A
- Interleukin-1b c.315C>T
- Selectin-E c.-19 GT
Genes involved in the pathogenesis of nonbacterial thrombotic endocarditis include:[9]
- Homozygous for the C677T mutation of the methylenetetrahydrofolate reductase gene which leads to hyperhomocysteinemia.
Associated Conditions
Conditions associated with endocarditis include:
- Prosthetic heart valves[10]
- Valvular heart disease (mitral valve prolapse is the most common valvular lesion that predisposes to endocarditis)[11][12]
- Intravenous drug abuse[13]
- Intracardiac devices, such as implantable cardioverter-defibrillators[14]
- Hemodialysis[15]
- Congenital heart disease[16]
- History of rheumatic heart disease[17]
- Diabetes mellitus[18][19]
- Colon cancer[20]
- Hypercoagulable state such as pregnancy and systemic bacterial infection [21][22]
- Malignancy especially mucin-producing adenocarcinomas (most commonly associated with pancreatic adenocarcinomas)[23]
- Systemic lupus erythematosus[24]
Gross Pathology
On gross pathology, characteristic findings of endocarditis are:
| Endocarditis Subtype | Features on Gross Pathology |
| Infective Endocarditis |
|
|---|---|
| Nonbacterial Thrombotic Endocarditis |
|
Microscopic Pathology
On microscopic histopathological, characteristic findings of endocarditis are:
- Vegetation:
- Vegetations are composed of fibrin, inflammatory cells, platelets, and microorganisms.[25]
| Endocarditis Subtype | Features on Histopathological Microscopic Analysis |
| Infective Endocarditis |
|
|---|---|
| Nonbacterial Thrombotic Endocarditis |
|
-
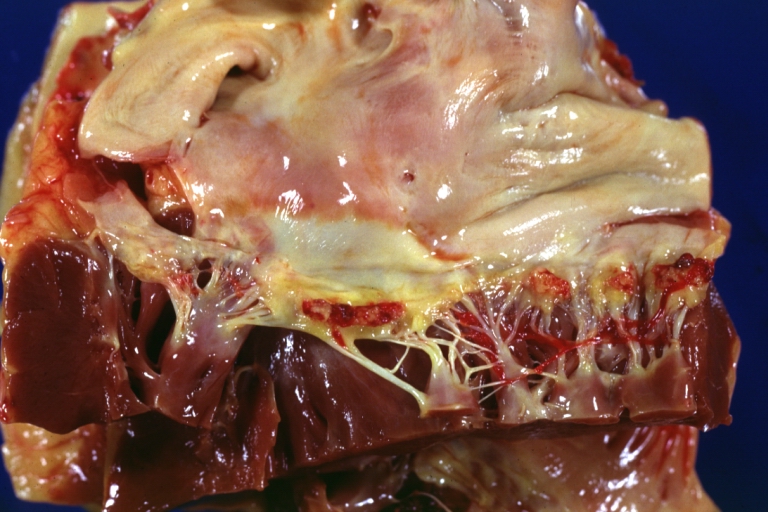 Heart; Breast intraductal papilloma metastasis. Thrombotic Nonbacterial Endocarditis (Infected): Gross mitral valve natural color vegetations well-illustrated these were secondarily infected with staphylococcus case of 8-year survival breast intraductal papillary adenocarcinoma with extensive metastases. Aortic valve also involved.
Heart; Breast intraductal papilloma metastasis. Thrombotic Nonbacterial Endocarditis (Infected): Gross mitral valve natural color vegetations well-illustrated these were secondarily infected with staphylococcus case of 8-year survival breast intraductal papillary adenocarcinoma with extensive metastases. Aortic valve also involved. -
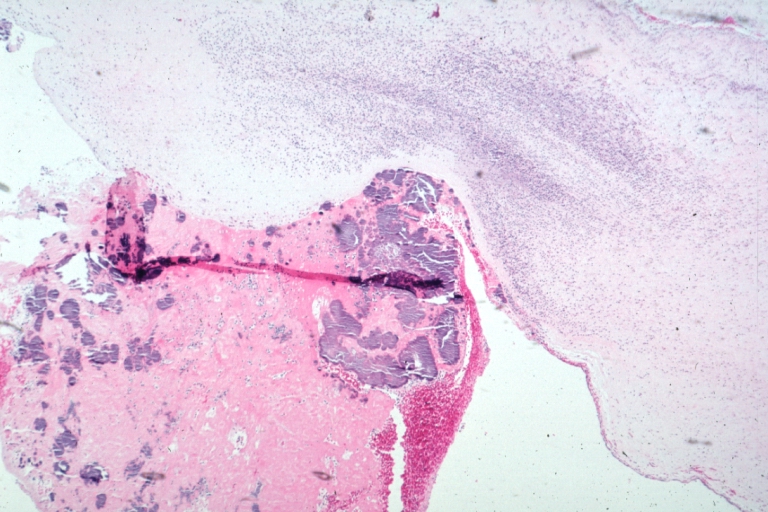 Nonbacterial Thrombotic Endocarditis Infected: Micro low mag H&E fibrin vegetation with masses of staphylococci and inflammatory cells in valve secondarily infected case 8-year survival breast papillary intraductal adenocarcinoma with extensive metastases gross is aortic valve lesions.
Nonbacterial Thrombotic Endocarditis Infected: Micro low mag H&E fibrin vegetation with masses of staphylococci and inflammatory cells in valve secondarily infected case 8-year survival breast papillary intraductal adenocarcinoma with extensive metastases gross is aortic valve lesions.


Videos
{{#ev:youtube|gk7cpP2ymOs}} {{#ev:youtube|BiNulEFh6rU}}
References
- ↑ Ford PM, Ford SE, Lillicrap DP (April 1988). “Association of lupus anticoagulant with severe valvular heart disease in systemic lupus erythematosus”. J. Rheumatol. 15 (4): 597–600. PMID 3135393.
- ↑ Williams, Ralph (1980). Immune complexes in clinical and experimental medicine. Cambridge, Mass: Harvard University Press. ISBN 978-0674444386.
- ↑ Nakanishi K, Tajima F, Nakata Y, Osada H, Ogata K, Kawai T, Torikata C, Suga T, Takishima K, Aurues T, Ikeda T (October 1998). “Tissue factor is associated with the nonbacterial thrombotic endocarditis induced by a hypobaric hypoxic environment in rats”. Virchows Arch. 433 (4): 375–9. doi:10.1007/s004280050262. PMID 9808440.
- ↑ Truskinovsky AM, Hutchins GM (April 2001). “Association between nonbacterial thrombotic endocarditis and hypoxigenic pulmonary diseases”. Virchows Arch. 438 (4): 357–61. doi:10.1007/s004280000372. PMID 11355169.
- ↑ MACDONALD RA, ROBBINS SL (February 1957). “The significance of nonbacterial thrombotic endocarditis: an autopsy and clinical study of 78 cases”. Ann. Intern. Med. 46 (2): 255–73. doi:10.7326/0003-4819-46-2-255. PMID 13403513.
- ↑ Sack GH, Levin J, Bell WR (January 1977). “Trousseau’s syndrome and other manifestations of chronic disseminated coagulopathy in patients with neoplasms: clinical, pathophysiologic, and therapeutic features”. Medicine (Baltimore). 56 (1): 1–37. PMID 834136.
- ↑ Gralnick HR, Abrell E (January 1973). “Studies of the procoagulant and fibrinolytic activity of promyelocytes in acute promyelocytic leukaemia”. Br. J. Haematol. 24 (1): 89–99. doi:10.1111/j.1365-2141.1973.tb05730.x. PMID 4577065.
- ↑ Weinstock M, Grimm I, Dreier J, Knabbe C, Vollmer T (2014). “Genetic variants in genes of the inflammatory response in association with infective endocarditis”. PLoS ONE. 9 (10): e110151. doi:10.1371/journal.pone.0110151. PMC 4192365. PMID 25299518.
- ↑ Durante-Mangoni E, Iossa D, Nappi F, Utili R (March 2011). “Inherited hyper-homocysteinemia as a cause of nonbacterial thrombotic endocarditis”. J. Heart Valve Dis. 20 (2): 232–3. PMID 21560828.
- ↑ Arvay A, Lengyel M (1988). “Incidence and risk factors of prosthetic valve endocarditis”. Eur J Cardiothorac Surg. 2 (5): 340–6. PMID 3272238.
- ↑ Mylonakis E, Calderwood SB (2001). “Infective endocarditis in adults”. N Engl J Med. 345 (18): 1318–30. doi:10.1056/NEJMra010082. PMID 11794152.
- ↑ Corrigall, Denton; Bolen, James; Hancock, E.William; Popp, Richard L. (1977). “Mitral valve prolapse and infective endocarditis”. The American Journal of Medicine. 63 (2): 215–222. doi:10.1016/0002-9343(77)90235-2. ISSN 0002-9343.
- ↑ Sousa, C.; Botelho, C.; Rodrigues, D.; Azeredo, J.; Oliveira, R. (2012). “Infective endocarditis in intravenous drug abusers: an update”. European Journal of Clinical Microbiology & Infectious Diseases. 31 (11): 2905–2910. doi:10.1007/s10096-012-1675-x. ISSN 0934-9723.
- ↑ Sohail, Muhammad R.; Uslan, Daniel Z.; Khan, Akbar H.; Friedman, Paul A.; Hayes, David L.; Wilson, Walter R.; Steckelberg, James M.; Jenkins, Sarah M.; Baddour, Larry M. (2008). “Infective Endocarditis Complicating Permanent Pacemaker and Implantable Cardioverter-Defibrillator Infection”. Mayo Clinic Proceedings. 83 (1): 46–53. doi:10.4065/83.1.46. ISSN 0025-6196.
- ↑ Mccarthy, James T.; Steckelberg, James M. (2000). “Infective Endocarditis in Patients Receiving Long-term Hemodialysis”. Mayo Clinic Proceedings. 75 (10): 1008–1014. doi:10.4065/75.10.1008. ISSN 0025-6196.
- ↑ Knirsch, Walter; Nadal, David (2011). “Infective endocarditis in congenital heart disease”. European Journal of Pediatrics. 170 (9): 1111–1127. doi:10.1007/s00431-011-1520-8. ISSN 0340-6199.
- ↑ Strom BL, Abrutyn E, Berlin JA, Kinman JL, Feldman RS, Stolley PD, Levison ME, Korzeniowski OM, Kaye D (November 1998). “Dental and cardiac risk factors for infective endocarditis. A population-based, case-control study”. Ann. Intern. Med. 129 (10): 761–9. doi:10.7326/0003-4819-129-10-199811150-00002. PMID 9841581.
- ↑ Lin CJ, Chua S, Chung SY, Hang CL, Tsai TH (June 2019). “Diabetes Mellitus: An Independent Risk Factor of In-Hospital Mortality in Patients with Infective Endocarditis in a New Era of Clinical Practice”. Int J Environ Res Public Health. 16 (12). doi:10.3390/ijerph16122248. PMC 6617149 Check
|pmc=value (help). PMID 31242695. - ↑ Chirillo F, Bacchion F, Pedrocco A, Scotton P, De Leo A, Rocco F, Valfrè C, Olivari Z (May 2010). “Infective endocarditis in patients with diabetes mellitus”. J. Heart Valve Dis. 19 (3): 312–20. PMID 20583393.
- ↑ Lazarovitch, T.; Shango, M.; Levine, M.; Brusovansky, R.; Akins, R.; Hayakawa, K.; Lephart, P. R.; Sobel, J. D.; Kaye, K. S.; Marchaim, D. (2012). “The relationship between the new taxonomy of Streptococcus bovis and its clonality to colon cancer, endocarditis, and biliary disease”. Infection. 41 (2): 329–337. doi:10.1007/s15010-012-0314-x. ISSN 0300-8126.
- ↑ “THE SIGNIFICANCE OF NONBACTERIAL THROMBOTIC ENDOCARDITIS: AN AUTOPSY AND CLINICAL STUDY OF 78 CASES”. Annals of Internal Medicine. 46 (2): 255. 1957. doi:10.7326/0003-4819-46-2-255. ISSN 0003-4819.
- ↑ Horwitz, Charles A.; Ward, Patrick C.J. (1971). “Disseminated intravascular coagulation, nonbacterial thrombotic endocarditis and adult pulmonary hyaline membranes-an interrelated triad?”. The American Journal of Medicine. 51 (2): 272–280. doi:10.1016/0002-9343(71)90245-2. ISSN 0002-9343.
- ↑ Min, Kyung-Whan; Gyorkey, Ferene; Sato, Clifford (1980). “Mucin-producing adenocarcinomas and nonbacterial thrombotic endocarditis. Pathogenetic role of tumor mucin”. Cancer. 45 (9): 2374–2382. doi:10.1002/1097-0142(19800501)45:9<2374::AID-CNCR2820450923>3.0.CO;2-J. ISSN 0008-543X.
- ↑ Moyssakis, Ioannis; Tektonidou, Maria G.; Vasilliou, Vassilios A.; Samarkos, Michael; Votteas, Vassilios; Moutsopoulos, Haralampos M. (2007). “Libman-Sacks Endocarditis in Systemic Lupus Erythematosus: Prevalence, Associations, and Evolution”. The American Journal of Medicine. 120 (7): 636–642. doi:10.1016/j.amjmed.2007.01.024. ISSN 0002-9343.
- ↑ Mylonakis E, Calderwood SB (2001). “Infective endocarditis in adults”. N Engl J Med. 345 (18): 1318–30. doi:10.1056/NEJMra010082. PMID 11794152.
Causes
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Ahmed Zaghw, M.D. [2] Ogheneochuko Ajari, MB.BS, MS [3]
Overview
The majority of cases of infective endocarditis are due to bacteria. Common causes of infective endocarditis include Streptococcus viridans, Staphylococci, and Enterococcus.
Causes
Common Causes
- Staphylococcus aureus[1]
- Streptococcus viridans
- Coagulase negative Staphylococci
- Candida albicans
- Clostridium septicum
- Enterococcus
- HACEK organisms
- Pseudomonas
- Streptococcus bovis
- Streptococcus pneumoniae
Causes by Organ System
Epidemiological Clues in Etiological Diagnosis of Culture-Negative Endocarditis[2]
| Epidemiological features | Common Microorganism(s) |
|---|---|
| |
| |
| |
| |
| |
| |
| |
References
- ↑ Murdoch, DR; et al. (9 March 2009). “Clinical presentation, etiology, and outcome of infective endocarditis in the 21st century: the International Collaboration on Endocarditis-Prospective Cohort Study”. Archives of Internal Medicine. 169 (5): 463–73. doi:10.1001/archinternmed.2008.603. PMC 3625651. PMID 19273776.
- ↑ Baddour, LM.; Wilson, WR.; Bayer, AS.; Fowler, VG.; Bolger, AF.; Levison, ME.; Ferrieri, P.; Gerber, MA.; Tani, LY. (2005). “Infective endocarditis: diagnosis, antimicrobial therapy, and management of complications: a statement for healthcare professionals from the Committee on Rheumatic Fever, Endocarditis, and Kawasaki Disease, Council on Cardiovascular Disease in the Young, and the Councils on Clinical Cardiology, Stroke, and Cardiovascular Surgery and Anesthesia, American Heart Association: endorsed by the Infectious Diseases Society of America”. Circulation. 111 (23): e394–434. doi:10.1161/CIRCULATIONAHA.105.165564. PMID 15956145. Unknown parameter
|month=ignored (help)
Differentiating Endocarditis for other Disorders
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1] Associate Editor(s)-in-Chief: Maliha Shakil, M.D. [2]
Overview
Endocarditis must be differentiated from other causes of a fever of unknown origin (FUO) such as pulmonary embolism, deep vein thrombosis, lymphoma, drug fever, cotton fever, and disseminated granulomatoses.[1]
Differential Diagnosis
Endocarditis must be differentiated from other causes of a fever of unknown origin such as:[1]
- Lymphoma
- Pulmonary embolism
- Deep vein thrombosis
- Drug fever
- Cotton fever
- Disseminated granulomatoses such as tuberculosis, histoplasmosis, coccidioidomycosis, blastomycosis, and sarcoidosis
Drug Fever
A drug fever will resolve with discontinuation of the offending agent. There may be elevated urine eosinophils and a peripheral eosinophilia as well.
Cotton Fever
The symptoms of cotton fever resemble those of sepsis and patients may be initially misdiagnosed upon admission to a hospital. However sepsis is a serious medical condition which can lead to death, whereas cotton fever, if left alone, will usually resolve itself spontaneously within 12-24 hours. Symptoms usually appear with 10-20 minutes after injection and in addition to fever may include headaches, malaise, chills, nausea and tachycardia. The fever itself usually reaches 38.5 – 40.3°C (101 – 105°F) within the first hour.[2]
Table 1; Differentiating psittacosis from other diseases
| Clinical feature | Cough | Sputum | Dyspnea | Sore throat | Headache | Confusion | Diarrhea | Chest radiograph changes | Hyponatremia | Leukopenia | Abnormal Liver function tests | Treatment |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Psittacosis | ++ | – | + | – | +++ | + | Minimal |
|
– | + | – | Doxycycline |
| C.pneumoniae pneumonia | + | + | + | +++ | ++ | + | – |
|
– | – | – | Doxycycline, Azithromycin |
| M. pneumoniae pneumonia | ++ | ++ | ++ | – | – | – | – |
|
– | – | + | Doxycycline |
| L. Pneumophila infection | + | +++ | +++ | – | + | ++ | + | Often Multifocal | ++ | + | ++ | Doxycycline |
| Influenza | ++ | ++ | ++ | ++ | ++ | +/- | +/- |
|
– | – | – | zanamivir, oseltamivir, |
| Endocarditis | ++ | ++ | + | – | – | – | – |
bases bilaterally |
– | +/- | +/- | Vancomycin |
| Coxiella burnetii infection | ++ | – | + | +/- | – | +/- | Minimal |
|
– | +/- | =/- | Doxycycline |
| Leptospirosis | ++ | + | ++ | + | + | ++ | – |
|
+++ | Doxycycline, azithromycin, amoxicillin | ||
| Brucellosis | ++ | – | + | – | ++ | + | – |
|
-/+ | +/- | +/- | Doxycycline, rifampin |
Key;
+, occurs in some cases
++, occurs in many cases,
+++, occurs frequently
References
- ↑ 1.0 1.1 Hirschmann JV (1997). “Fever of unknown origin in adults”. Clin Infect Dis. 24 (3): 291–300, quiz 301-2. PMID 9114175.
- ↑ Harrison DW, Walls RM (1990). ““Cotton fever”: a benign febrile syndrome in intravenous drug abusers”. J Emerg Med. 8 (2): 135–9. PMID 2362114.
Risk Factors
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1] Associate Editor(s)-in-Chief: Maliha Shakil, M.D. [2]
Overview
Common risk factors for endocarditis include prosthetic heart valves, valvular heart disease, congenital heart disease, intravenous drug use, age-related degenerative valvular lesions, immunosuppression, and colon cancer.
Risk Factors
Common risk factors in the development of infective endocarditis are:
- Prosthetic heart valves[1]
- Valvular heart disease (mitral valve prolapse is the most common valvular lesion that predisposes to endocarditis)[2][3]
- Intravenous drug abuse[4]
- Intracardiac devices, such as implantable cardioverter-defibrillators[5]
- Age-related degenerative valvular lesions
- Hemodialysis[6]
- Congenital heart disease[7]
- History of rheumatic heart disease[8]
- Diabetes mellitus[9][10]
- Colon cancer[11]
Common risk factors in the development of nonbacterial thrombotic endocarditis include:
- Hypercoagulable state such as pregnancy and systemic bacterial infection [12][13]
- Malignancy especially mucin-producing adenocarcinomas (most commonly associated with pancreatic adenocarcinomas)[14]
- Systemic lupus erythematosus[15]
Epidemiological Clues in Etiological Diagnosis of Culture-Negative Endocarditis[16]
| Epidemiological features | Common Microorganism(s) |
|---|---|
| |
| |
| |
| |
| |
| |
| |
References
- ↑ Arvay A, Lengyel M (1988). “Incidence and risk factors of prosthetic valve endocarditis”. Eur J Cardiothorac Surg. 2 (5): 340–6. PMID 3272238.
- ↑ Mylonakis E, Calderwood SB (2001). “Infective endocarditis in adults”. N Engl J Med. 345 (18): 1318–30. doi:10.1056/NEJMra010082. PMID 11794152.
- ↑ Corrigall, Denton; Bolen, James; Hancock, E.William; Popp, Richard L. (1977). “Mitral valve prolapse and infective endocarditis”. The American Journal of Medicine. 63 (2): 215–222. doi:10.1016/0002-9343(77)90235-2. ISSN 0002-9343.
- ↑ Sousa, C.; Botelho, C.; Rodrigues, D.; Azeredo, J.; Oliveira, R. (2012). “Infective endocarditis in intravenous drug abusers: an update”. European Journal of Clinical Microbiology & Infectious Diseases. 31 (11): 2905–2910. doi:10.1007/s10096-012-1675-x. ISSN 0934-9723.
- ↑ Sohail, Muhammad R.; Uslan, Daniel Z.; Khan, Akbar H.; Friedman, Paul A.; Hayes, David L.; Wilson, Walter R.; Steckelberg, James M.; Jenkins, Sarah M.; Baddour, Larry M. (2008). “Infective Endocarditis Complicating Permanent Pacemaker and Implantable Cardioverter-Defibrillator Infection”. Mayo Clinic Proceedings. 83 (1): 46–53. doi:10.4065/83.1.46. ISSN 0025-6196.
- ↑ Mccarthy, James T.; Steckelberg, James M. (2000). “Infective Endocarditis in Patients Receiving Long-term Hemodialysis”. Mayo Clinic Proceedings. 75 (10): 1008–1014. doi:10.4065/75.10.1008. ISSN 0025-6196.
- ↑ Knirsch, Walter; Nadal, David (2011). “Infective endocarditis in congenital heart disease”. European Journal of Pediatrics. 170 (9): 1111–1127. doi:10.1007/s00431-011-1520-8. ISSN 0340-6199.
- ↑ Strom BL, Abrutyn E, Berlin JA, Kinman JL, Feldman RS, Stolley PD, Levison ME, Korzeniowski OM, Kaye D (November 1998). “Dental and cardiac risk factors for infective endocarditis. A population-based, case-control study”. Ann. Intern. Med. 129 (10): 761–9. doi:10.7326/0003-4819-129-10-199811150-00002. PMID 9841581.
- ↑ Lin CJ, Chua S, Chung SY, Hang CL, Tsai TH (June 2019). “Diabetes Mellitus: An Independent Risk Factor of In-Hospital Mortality in Patients with Infective Endocarditis in a New Era of Clinical Practice”. Int J Environ Res Public Health. 16 (12). doi:10.3390/ijerph16122248. PMC 6617149 Check
|pmc=value (help). PMID 31242695. - ↑ Chirillo F, Bacchion F, Pedrocco A, Scotton P, De Leo A, Rocco F, Valfrè C, Olivari Z (May 2010). “Infective endocarditis in patients with diabetes mellitus”. J. Heart Valve Dis. 19 (3): 312–20. PMID 20583393.
- ↑ Lazarovitch, T.; Shango, M.; Levine, M.; Brusovansky, R.; Akins, R.; Hayakawa, K.; Lephart, P. R.; Sobel, J. D.; Kaye, K. S.; Marchaim, D. (2012). “The relationship between the new taxonomy of Streptococcus bovis and its clonality to colon cancer, endocarditis, and biliary disease”. Infection. 41 (2): 329–337. doi:10.1007/s15010-012-0314-x. ISSN 0300-8126.
- ↑ “THE SIGNIFICANCE OF NONBACTERIAL THROMBOTIC ENDOCARDITIS: AN AUTOPSY AND CLINICAL STUDY OF 78 CASES”. Annals of Internal Medicine. 46 (2): 255. 1957. doi:10.7326/0003-4819-46-2-255. ISSN 0003-4819.
- ↑ Horwitz, Charles A.; Ward, Patrick C.J. (1971). “Disseminated intravascular coagulation, nonbacterial thrombotic endocarditis and adult pulmonary hyaline membranes-an interrelated triad?”. The American Journal of Medicine. 51 (2): 272–280. doi:10.1016/0002-9343(71)90245-2. ISSN 0002-9343.
- ↑ Min, Kyung-Whan; Gyorkey, Ferene; Sato, Clifford (1980). “Mucin-producing adenocarcinomas and nonbacterial thrombotic endocarditis. Pathogenetic role of tumor mucin”. Cancer. 45 (9): 2374–2382. doi:10.1002/1097-0142(19800501)45:9<2374::AID-CNCR2820450923>3.0.CO;2-J. ISSN 0008-543X.
- ↑ Moyssakis, Ioannis; Tektonidou, Maria G.; Vasilliou, Vassilios A.; Samarkos, Michael; Votteas, Vassilios; Moutsopoulos, Haralampos M. (2007). “Libman-Sacks Endocarditis in Systemic Lupus Erythematosus: Prevalence, Associations, and Evolution”. The American Journal of Medicine. 120 (7): 636–642. doi:10.1016/j.amjmed.2007.01.024. ISSN 0002-9343.
- ↑ Baddour, LM.; Wilson, WR.; Bayer, AS.; Fowler, VG.; Bolger, AF.; Levison, ME.; Ferrieri, P.; Gerber, MA.; Tani, LY. (2005). “Infective endocarditis: diagnosis, antimicrobial therapy, and management of complications: a statement for healthcare professionals from the Committee on Rheumatic Fever, Endocarditis, and Kawasaki Disease, Council on Cardiovascular Disease in the Young, and the Councils on Clinical Cardiology, Stroke, and Cardiovascular Surgery and Anesthesia, American Heart Association: endorsed by the Infectious Diseases Society of America”. Circulation. 111 (23): e394–434. doi:10.1161/CIRCULATIONAHA.105.165564. PMID 15956145. Unknown parameter
|month=ignored (help)
Epidemiology and Demographics
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1] Associate Editor(s)-in-Chief: Maliha Shakil, M.D. [2]
Overview
The incidence of native valve infective endocarditis is approximately 1.7-6.2 cases per 100,000 individuals per year in the United States and Europe. The prevalence of infective endocarditis among IV drug users ranges from 10 to 15%.The incidence of endocarditis increases with age; the median age of patients is 47 to 69 years. There is an increased incidence of infective endocarditis in persons 65 years of age and older. Males are more commonly affected with endocarditis than females. The male to female ratio is approximately 1.7:1.
Epidemiology and Demographics
Incidence
- The incidence of native valve infective endocarditis is approximately 1.7-6.2 cases per 100,000 individuals per year in the United States and Europe.[1]
Age
- The incidence of infective endocarditis increases with age; the median age of patients is 47 to 69 years.
- There is an increased incidence of infective endocarditis in persons 65 years of age and older.
- The incidence of nonbacterial thrombotic endocarditis increases with age; the median age of patients is 40 to 70 years.[2]
Gender
- Males are more commonly affected with endocarditis than females.[1]
- The male to female ratio is approximately 1.7:1.
References
- ↑ 1.0 1.1 Mylonakis E, Calderwood SB (2001). “Infective endocarditis in adults”. N Engl J Med. 345 (18): 1318–30. doi:10.1056/NEJMra010082. PMID 11794152.
- ↑ MACDONALD RA, ROBBINS SL (February 1957). “The significance of nonbacterial thrombotic endocarditis: an autopsy and clinical study of 78 cases”. Ann. Intern. Med. 46 (2): 255–73. doi:10.7326/0003-4819-46-2-255. PMID 13403513.
Natural History, Complications, and Prognosis
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1] Associate Editor(s)-in-Chief: Maliha Shakil, M.D. [2]
Overview
If left untreated, patients with endocarditis may progress to develop congestive heart failure. Complications of endocarditis can occur as a result of the locally destructive effects of the infection. These complications include perforation of valve leaflets causing congestive heart failure, abscesses, and disruption of the heart’s conduction system. Endocarditis may also cause embolization to the brain (causing a stroke), to the coronary artery (causing a heart attack), to the lung (causing pulmonary embolism), to the spleen (causing a splenic infarct), and to the kidney (causing a renal infarct). Prognosis of endocarditis is generally poor and the overall mortality rate for both native and prosthetic valve endocarditis ranges from 20-25%. The mortality rate for right-sided endocarditis in injection drug users is approximately 10%. The 5-year survival rate for native valve endocarditis is 70-80% and 50-80% for prosthetic valve endocarditis.
Natural History
- If left untreated, patients with endocarditis may progress to develop congestive heart failure.[1]
Complications
Complications of infective endocarditis include:[1][2]
Cardiac
- Murmur
- A new aortic diastolic murmur suggests dilatation of the aortic annulus or eversion, rupture, or fenestration of an aortic leaflet
- The sudden onset of a loud mitral pansystolic murmur suggests rupture of chordae tendineae or fenestration of a mitral valve leaflet
- Congestive heart failure
- Cardiac rhythm disturbances including AV block
- Pericarditis (uncommon)
Cutaneous
- Petechiae of the conjunctiva, oropharynx, skin, and legs
- Linear subungual splinter haemorrhages of the lower or middle nail bed
- Osler’s nodes
- Janeway lesions
Musculoskeletal
- Myalgias
- Arthralgias
- Arthritis
- Low back pain
- Rheumatoid factor is elevated in up to 50% of patients with endocarditis for >6 weeks
- Clubbing of fingers is present in < 15% of patients
Ocular
- Petechial hemorrhages
- Flame-shaped hemorrhages
- Roth’s spots
- Cotton-wool exudates in the retina
Embolic
- Significant arterial emboli occur in 30%–50% of patients, causing the following:
- Stroke
- Monocular blindness
- Acute abdominal pain, ileus, and melena
- Pain and gangrene in the extremities
- CNS emboli are common
- Coronary emboli, often asymptomatic, can cause myocardial infarction
- Pulmonary emboli are common in right-sided endocarditis, causing pulmonary infarcts or focal pneumonitis
Splenic
- Splenomegaly is observed in 15%–30% of patients
- Splenic infarcts occur in up to 40% of patients
- Splenic abscesses occur in ~ 5% of patients
Renal
- Microscopic hematuria occurs in ~ 50% of patients
- Embolic renal infarction
- Diffuse membranoproliferative glomerulonephritis
Mycotic Aneurysms
Occur in any artery in 2%–8% of patients, causing the following:
- Pain or headache
- Pulsatile mass
- Fever
- Sudden expanding hematoma
- Signs of major blood loss
Neurologic
- Neurologic complications occur in 25%–40% of cases
- Strokes caused by cerebral embolisms in ~15% of cases, causing the following:
- Altered level of consciousness
- Seizures
- Fluctuating focal neurologic signs
- Cerebral aneurysms occur in 1%–5% of cases, causing the following:
- Headache
- Focal signs
- Acute intracerebral or subarachnoid hemorrhage caused by rupture
- Mild meningeal irritation resulting from slow leakage
- Brain abscesses may occur in acute endocarditis caused by Staphylococcus aureus
- Seizures
Monitoring for Complications of Infectious Endocarditis
Among those patients at high risk, careful monitoring should be undertaken to detect the early development of complications such as:
- Valvular dysfunction, usual insufficiency of the mitral or aortic valves
- Myocardial or septal abscesses
- Congestive heart failure
- Metastatic infection
- Embolic phenomenon
Prognosis
- The prognosis of endocarditis is generally poor and the overall mortality rate for both native and prosthetic valve endocarditis ranges from 20-25%.
- The mortality rate for right-sided endocarditis in injection drug users is approximately 10%.[1]
- The 5-year survival rate for native valve endocarditis is 70-80% and 50-80% for prosthetic valve endocarditis.[2]
References
- ↑ 1.0 1.1 1.2 Mylonakis E, Calderwood SB (2001). “Infective endocarditis in adults”. N Engl J Med. 345 (18): 1318–30. doi:10.1056/NEJMra010082. PMID 11794152. Unknown parameter
|http://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=ignored (help) - ↑ 2.0 2.1 Baddour Larry M., Wilson Walter R., Bayer Arnold S., Fowler Vance G. Jr, Bolger Ann F., Levison Matthew E., Ferrieri Patricia, Gerber Michael A., Tani Lloyd Y., Gewitz Michael H., Tong David C., Steckelberg James M., Baltimore Robert S., Shulman Stanford T., Burns Jane C., Falace Donald A., Newburger Jane W., Pallasch Thomas J., Takahashi Masato, Taubert Kathryn A. (2005). “Infective Endocarditis: Diagnosis, Antimicrobial Therapy, and Management of Complications: A Statement for Healthcare Professionals From the Committee on Rheumatic Fever, Endocarditis, and Kawasaki Disease, Council on Cardiovascular Disease in the Young, and the Councils on Clinical Cardiology, Stroke, and Cardiovascular Surgery and Anesthesia, American Heart Association-Executive Summary: Endorsed by the Infectious Diseases Society of America”. Circulation. 111 (23): 3167–84. PMID 15956145.
Diagnosis
Diagnosis
Diagnostic Criteria | History and Symptoms | Physical Examination and Signs | Laboratory Findings | Chest X Ray | Electrocardiogram | Cardiac MRI | CT | Echocardiography
Treatment
Treatment
Medical Therapy | | Surgery | Antithrombotic Therapy | Primary Prevention | Secondary Prevention
2014 AHA/ACC Guideline for the Management of Patients With Valvular Heart Disease
2014 AHA/ACC Guideline for the Management of Patients With Valvular Heart Disease
Diagnosis and Follow-up | Endocarditis Medical Therapy Guidelines | Endocarditis Intervention Guidelines
Looking for the patient version?
© 2026 MyEClinic – IFTM Institut für Telematik in der Medizin GmbH