
Cardiogenic shock
For patient information, click here.
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: João André Alves Silva, M.D. [2] Ahmed Elsaiey, MBBCH [3], Syed Musadiq Ali M.B.B.S.[4]
Overview
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Mohammad Salih, MD. João André Alves Silva, M.D. [2] Syed Musadiq Ali M.B.B.S.[3]
Overview
Acute cardiac hemodynamic instability may result from disorders that impair function of the myocardium, valves, conduction system, or pericardium, either in isolation or in combination. CS is pragmatically defined as a state in which ineffective cardiac output caused by a primary cardiac disorder results in both clinical and biochemical manifestations of inadequate tissue perfusion. The clinical presentation is typically characterized by persistent hypotensionunresponsive to volume replacement and is accompanied by clinical features of end-organ hypoperfusion requiring intervention with pharmacological or mechanical support. Although not mandated, objective hemodynamic parameters for CS can help confirm the diagnosis and enable comparison across cohorts and clinical trials. Definitions in clinical practice guidelines and operationalized definitions used in the SHOCK (Should We Emergently Revascularize Occluded Coronaries for Cardiogenic Shock) and IABP-SHOCK II (Intraaortic Balloon Pump in Cardiogenic Shock II) trials.Before the routine use of early revascularization, MI-associated CS had an in-hospital mortality exceeding 80%. A registry trial of 250 patients with acute MI described the association between bedside physical examination (Killip classification) for the assessment of heart failure (HF) and the risk of mortality. Patients with Killip class IV (CS) had a mortality of 81%. Subsequently, the Diamond and Forrester classification using right-sided heart catheterization described the role of cardiac hemodynamics in stratifying risk after acute MI in the prereperfusion era. Patients in Diamond and Forrester subgroup IV with a pulmonary capillary wedge pressure (PCWP) >18 mm Hg and a cardiac index (CI) <2.2 L·min−1·m−2, indicative of CS, had a mortality of 51%. Treatment efforts to reduce mortality initially focused on improvement of hemodynamic parameters by mechanical devices. The intra-aortic balloon pump (IABP), introduced in a registry cooperative trial, decreased systolic blood pressure (SBP), increased diastolic blood pressure, and modestly but significantly increased CI. Nevertheless, mortality remained virtually unchanged, with only 15 survivors among 87 patients (83% mortality). The early reperfusion era did not affect outcomes for shock complicating acute MI. Fibrinolysis was effective for patients with ST-segment–elevation MI (STEMI) in general, but it is less clear if fibrinolysis reduces mortality in those with CS.The first major breakthrough in CS treatment was achieved by the randomized SHOCK trial. Although an early invasive strategy coupled with percutaneous coronary intervention (PCI) or coronary artery bypass grafting (CABG) did not reduce 30-day mortality (the primary outcome of the trial), a significant mortality reduction emerged at 6 and 12 months that persisted at longer-term follow-up. Subsequent registries confirmed the survival advantage of early revascularization. Further efforts to reduce CS mortality have been directed toward improvements in MCS devices. The largest randomized trial in patients with acute MI complicated by CS did not show a benefit with routine IABP placement in addition to revascularization. As a result, there has been a decrease in the use of IABPs in clinical practice and a downgrading in guideline recommendations. Recently, other percutaneous MCS devices have shown promise in the treatment of CS, but more data from randomized clinical trials are needed.
Historical Perspective
The term “cardiogenic shock” is thought to have first arisen in 1942 with Stead who, after studying a series of two patients, described them as having a “shock of cardiac origin“. This designation would later be rephrased as “cardiogenic shock“. However, the clinical features of cardiogenic shock had first been described by Herrick, in 1912, who noticed in severe coronary artery disease patients a profound weakness, a rapid pulse, pulmonary rales, faint cardiac tones, cyanosis and dyspnea. Despite its still high incidence and mortality nowadays, cardiogenic shock has seen its impact decreased throughout the years. Particularly since the 1970’s, when the mortality rate for this condition was about 80-90%, these values have been decreasing since then, particularly due to the earlier diagnosis and better management of CS, with more effective reperfusion techniques]]. Today the its mortality rate is about 50%. .Before the routine use of early revascularization, MI-associated CS had an in-hospital mortality exceeding 80%. A registry trial of 250 patients with acute MI described the association between bedside physical examination (Killip classification) for the assessment of heart failure (HF) and the risk of mortality. Patients with Killip class IV (CS) had a mortality of 81%. Subsequently, the Diamond and Forrester classification using right-sided heart catheterization described the role of cardiac hemodynamics in stratifying risk after acute MI in the prereperfusion era. Patients in Diamond and Forrester subgroup IV with a pulmonary capillary wedge pressure (PCWP) >18 mm Hg and a cardiac index (CI) <2.2 L·min−1·m−2, indicative of CS, had a mortality of 51%. Treatment efforts to reduce mortality initially focused on improvement of hemodynamic parameters by mechanical devices. The intra-aortic balloon pump (IABP), introduced in a registry cooperative trial, decreased systolic blood pressure (SBP), increased diastolic blood pressure, and modestly but significantly increased CI. Nevertheless, mortality remained virtually unchanged, with only 15 survivors among 87 patients (83% mortality). The early reperfusion era did not affect outcomes for shock complicating acute MI. Fibrinolysis was effective for patients with ST-segment–elevation MI (STEMI) in general, but it is less clear if fibrinolysis reduces mortality in those with CS.The first major breakthrough in CS treatment was achieved by the randomized SHOCK trial.
Classification
The Society for Cardiovascular Angiography and Intervention (SCAI) developed an expert consensus statement, endorsed by multiple relevant societies, proposing a novel CS classification scheme, which categorizes patients with or at risk of CS into worsening stages of hemodynamic compromise for the purposes of facilitating patient care and research. The SCAI CS classification consensus statement describes 5 stages of CS, each of which may have an “A” modifier signifying the occurrence of cardiac arrest (CA). This classification schema was developed based on expert consensus opinion and its ability to discriminate among levels of mortality risk in critically ill patients remains to be established. The goal of this study was to examine the construct validity of the SCAI CS staging schema by demonstrating the ability of a simple functional classification of SCAI shock stages at the time of cardiac intensive care unit (CICU) admission to predict mortality in CICU patients.The purpose of the classification schema is to assist in clear communication among clinicians and researchers regarding the patient’s current clinical status, recognizing that CS encompasses a spectrum, including those at high risk of developing shock from myocardial dysfunction to those who develop hemodynamic collapse and cardiac arrest. The CS classification schema includes five stages of shock labeled A through E. The authors categorized patients in three domains, including laboratory findings, physical exams findings, and hemodynamics. When cardiac arrest has occurred the modifier (A) is added to stage classification (i.e. stage CA).
Pathophysiology
The pathophysiology of cardiogenic shock is complex and not fully understood. Ischemia to the myocardium causes derangement to both systolic and diastolic left ventricular function, resulting in a profound depression of myocardial contractility. This, in turn, leads to a potentially catastrophic and vicious spiral of reduced cardiac output and low blood pressure, perpetuating further coronary ischemia and impairment of contractility. Several physiologic compensatory processes ensue. These include:The activation of the sympathetic system leading to peripheral vasoconstriction which may improve coronary perfusion at the cost of increased afterload, and Tachycardia which increases myocardial oxygen demand and subsequently worsens myocardial ischemia.These compensatory mechanisms are subsequently counteracted by pathologic vasodilation that occurs from the release of potent systemic inflammatory markers such as interleukin-1, tumor necrosis factor a, and interleukin-6. Additionally, higher levels of nitric oxide and peroxynitrite are released, which also contribute to pathologic vasodilation and are known to be cardiotoxic. Unless interrupted by adequate treatment measures, this self-perpetuating cycle leads to global hypoperfusion and the inability to effectively meet the metabolic demands of the tissues, progressing to multiorgan failure and eventually death.
Causes
The most common cause of cardiogenic shock is acute myocardial infarction with left ventricular dysfunction. Less commonly, right ventricular myocardial infarction can lead to cardiogenic shock. Other causes of cardiogenic shock include mechanical injuries such as acute valvular regurgitation or rupture, free wall rupture, and ventricular septum rupture.
Epidemiology and Demographics
In defiance of the historic numbers of mortality from cardiogenic shock of 80% to 90%, in the modern era, this type of shock comprises a mortality risk of around 50%, in the face of the diagnostic and treatment techniques, which have greatly been developed in recent years. Depending on the demographic and clinical factors, this risk can range from 10% to 80%. The incidence of cardiogenic shock among patients with acute MI is approximately 5% to 10%. Because atherosclerosis and myocardial infarction are both more frequent among males, cardiogenic shock is more common in this gender. However, because women tend to present with acute myocardial infarction at a later age, along with the fact that they have a greater chance of having multivessel coronary artery disease when they first develop symptoms, a greater proportion of women with acute MI develop cardiogenic shock.
Risk Factors
The identification of high-risk groups for developing cardiogenic shock and its promoting factors is mandatory for the improvement of the survival rate of these patients. This will facilitate the providing of adequate therapeutic measures and the avoidance of others which would otherwise lead to iatrogenic shock. Considering that the most common cause of cardiogenic shock is acute coronary syndrome, either with or without persistent ST-segment elevation, these patients are at higher risk and will benefit highly from these measures.
Natural history, Complications and Prognosis
Cardiogenic shock (CS) is a clinical condition, defined as a state of systemic hypoperfusion originated in cardiac failure, in the presence of adequate intravascular volume, typically followed by hypotension, which leads to insufficient ability to meet oxygen and nutrient demands of organs and other peripheral tissues.It may range from mild to severe hypoperfusion and may be defined in terms of hemodynamic parameters, which according to most studies, means a state in which systolic blood pressure is persistently < 90 mm Hg or < 80 mm Hg, for longer than 1 hour, with adequate or elevated left and right ventricular filling pressures that does not respond to isolated fluid administration, is secondary to cardiac failure and occurs with signs of hypoperfusion (oliguria, cool extremities, cyanosis and altered mental status) or a cardiac index of < 2.2 L/min/m² (on inotropic, vasopressor or circulatory device support) or < 1.8-2.2 L/min/m² (off support) and pulmonary artery wedge pressure > 18 mm Hg. In the presence of CS, a pathological cycle develops in which ischemia, the initial aggression, leads to myocardial dysfunction. This will affect parameters like the cardiac output, stroke volume and myocardial perfusion thereby worsening the ischemia. The body will then initiate a series of compensatory mechanisms, such as sympathetic stimulation of the heart and activation of the renin/angiotensin/aldosterone system, trying to overcome the cardiac aggression, however, this will ultimately lead to a downward spiral worsening of the ischemia. Inflammatory mediators, originated in the infarcted area, will also intervene at some point causing myocardial depression, decreasing contractility and worsening hypotension. Lactic acidosis will also develop, resulting from the poor tissue perfusion, that is responsible for a shift in metabolism to glycolysis, which will further depress the myocardium, thereby worsening the clinical scenario. CS has several risk factors which will contribute to the progression of the condition. Depending on these underlying factors and in concordance to the pathological mechanism responsible for the development of CS, the patient will have higher or lower probability of developing complications, of which the most common are cardiac, renal and pulmonary. The presence of certain risk factors and the etiology behind the shock will dictate the outcome of the condition. Despite the decreasing incidence and mortality rate seen throughout recent years, CS is still associated with a poor prognosis, particularly in elderly patients.
Diagnosis
Attending to the catastrophic outcome of cardiogenic shock in a very short time span, its diagnosis must be reached as early as possible in order for proper therapy to be started. This period until diagnosis and treatment initiation is particularly important in the case of cardiogenic shock since the mortality rate of this condition complicating acute-MI is very high, along with the fact that the ability to revert the damage caused, through reperfusion techniques, declines considerably with diagnostic delays. Therefore and due to the unstable state of these patients, the diagnostic evaluations are usually performed as supportive measures are initiated. The diagnostic measures should start with the proper history and physical examination, including blood pressure measurement, followed by an EKG, echocardiography, chest x-ray and collection of blood samples for evaluation. The physician should keep in mind the common features of shock, irrespective of the type of shock, in order to avoid delays in the diagnosis. Although not all shock patients present in the same way, these features include: abnormal mental status, cool extremities, clammy skin, manifestations of hypoperfusion, such as hypotension and oliguria, as well as evidence of metabolic acidosis on the blood results.
History and Symptoms
The presenting symptoms of cardiogenic shock are variable. The most common clinical manifestations of shock, such as hypotension, altered mental status, oliguria, and cold, clammy skin, can be seen in patients with cardiogenic shock. History plays a very important role in understanding the etiology of the shock and thus helps in the management of cardiogenic shock.The patient should also be assessed for cardiac risk factors: Diabetes mellitus, Tobacco smoking, Hypertension, Hyperlipidemia, A family history of premature coronary artery disease, Age older than 45 in men and older than 55 in women, Physical inactivity.
Physical Examination
Physical examination findings in patients with cardiogenic shock include the following: Altered mental status, cyanosis, cold and clammy skin, mottled extremities Peripheral pulses are faint, rapid and sometimes irregular if there is an underlying arrhythmia, Jugular venous distension, Diminished heart sounds, S3 or S4, may be present, murmurs in the presence of valvular disorders such as mitral regurgitation or aortic stenosis, Pulmonary vascular congestion may be associated with rales Peripheral edema may be present in the setting of fluid overload.
Laboratory Finding
Biomarkers of cardiac myonecrosis are useful to gauge the severity of acute underlying myocardial injury in conditions such as fulminant myocarditis. In ACS, cardiac troponin is noted to be elevated and has a rise-and-fall pattern consistent with acute ischemic injury. A mismatch between the degree of segmental dysfunction on imaging and troponin release may be noted in the setting of stunned/hibernating myocardium or when presentation is significantly delayed after the ischemic insult. Myocardial necrosis biomarker levels may provide an idea of the extent of myocardial injury, whereas serial measurements are useful in assessing early washout after successful reperfusion and in estimating the amount of cardiac necrosis. Natriuretic peptides are significantly elevated in the setting of acute HF culminating in CS and are associated with mortality in MI-associated CS. Oxygen-carrying capacity is the product of cardiac output and the oxygen content of blood. Thus, an ineffective CI will result in inadequate peripheral tissue oxygen delivery. Elevated arterial lactic acid levels are nonspecifically indicative of tissue hypoxia but are associated with mortality in CS.The pathogenesis of lactate production in CS is uncertain, although impaired oxygen delivery, stress-induced hyperlactatemia, and impaired clearance are likely contributors. A peripheral oxygen demand-delivery mismatch will result in low central venous oxygen measurements. A mixed venous oxygen saturation sample is ideally obtained from the distal port of a pulmonary artery catheter (PAC) and is a reflection of oxygen saturation from blood returning to the heart via the superior and inferior vena cava, as well as the coronary sinus. Serial measurements of arterial lactate and mixed venous oxygen saturation levels may be helpful to temporally monitor responses to therapeutic interventions. Arterial blood gas measurements also permit the assessment of [[arterial] oxygenation and ventilation, as well as metabolic and respiratory acid-base disorders. Acute kidney injury, which is reflected by a rise in serum creatinine and a potential reduction in urinary output, in the setting of CS may indicate renal hypoperfusion and is associated with poor outcomes. It should be noted that novel renal biomarkers such as neutrophil gelatinase–associated lipocalcin, kidney injury molecule 1, and cystatin C were not more effective than standard evaluation with serum creatinine for assessing risk. Acute ischemic or congestive liver injury can occur in the setting of CS and manifests as a marked elevation in serum aspartate aminotransferase, alanine aminotransferase, serum bilirubin, and lactate dehydrogenase levels, often accompanied by an increase in prothrombin time with a peak at 24 to 72 hours that subsequently recovers to baseline within 5 to 10 days, and a ratio of alanine aminotransferase to lactate dehydrogenase of <1.5. This should be differentiated from chronic to subacute elevation of liver function abnormalities in the setting of venous congestion resulting from right-sided HF.
Electrocardiogram
An electrocardiogram may be useful in distinguishing cardiogenic shock from septic shock or neurogenic shock. A diagnosis of cardiogenic shock is suggested by the presence of ST segment changes, new left bundle branch block or signs of a cardiomyopathy. Cardiac arrhythmias may also be present.
Chest X-ray
The chest x ray will show pulmonary edema, pulmonary vascular redistribution, enlarged hila, kerley’s B lines, and bilateral pleural effusions in patients with left ventricular failure. In contrast, a pneumonia may be present in the patient with septic shock.Chest x-ray provides information on cardiac size and pulmonary congestion and may suggest alternative pathogeneses such as aortic dissection, pericardial effusion, pneumothorax, esophageal perforation, or pulmonary embolism. The test enables clinicians to confirm the position of the endotracheal tube and the position of supportive devices, including temporary pacing wires.
Echocardiography
Echocardiography is an important imaging modality for the evaluation of the patient with cardiogenic shock. This test will allow the identification of certain characteristics that, when complemented by a proper medical history and physical examination, will likely prompt to the diagnosis. These may include: poor wall motion, papillary muscle rupture, pseudoaneurysms, ventricular septal defects, among others. The echocardiographic findings may also suggest or rule out a different diagnosis. The test will provide information about the overall hemodynamic status of the heart as well, which may reveal to be vital in order to plan further measures and predict the outcome. Transthoracic and transesophageal (in the case of inadequate visibility) echocardiography is increasingly used for non-invasive hemodynamic assessment and monitoring in the ICU setting. Using echocardiography, it is possible to assess preload, fluid responsiveness, systolic and diastolic cardiac function, and calculate cardiac output, intravascular and intra-cardiac pressures. It is the golden standard in the initial hemodynamic assessment and should be used as complementary tool in invasively monitored patients in the case of new circulatory or respiratory failure. Echocardiography is indispensable in the management of shock patients and is extremely powerful diagnostic role for the cardiac abnormalities (pericardial effusion and tamponade, acute cor pulmonale and acute or chronic valvular disorders) as a cause for hemodynamic instability. It is the most important and suitable method for assessment of right ventricular function, for diagnosis of septic cardiomyopathy and cardiac causes of weaning failure.
CT Scan
The CT scan is usually not recommended as an initial imaging study, when evaluating patients with cardiogenic shock. However, it may be helpful in certain situations, such as: aortic dissection, pulmonary emboli and internal hemorrhage, this last one more related to hypovolemic shock.
MRI
New non-invasive imaging techniques such as cardiovascular magnetic resonance (CMR) imaging promise the non-invasive diagnosis of myocarditis which can be the cause of cardiogenic shock. Considering the hallmarks of acute and chronic myocarditis (accumulation of inflammatory cells; swelling, necrosis and/or apoptosis of cardiomyocytes; increase in extracellular space and water content; myocardial remodelling with fibrotic tissue replacement), an imaging modality such as CMR that enables non-invasive detection of changes in myocardial tissue composition is highly valuable and welcome.
Other Diagnostic Studies
The Swan-ganz catheter, right heart catheter or pulmonary artery catheter has been gradually replaced by echocardiography with color Doppler throughout the years, however, it is still common practice in some centers. It may be used for different situations, such as: confirming the diagnosis of cardiogenic shock following clinical evaluation, ensuring adequacy of filling pressures, establishing the relationship between these filling pressures and cardiac output as well as helping in possible adjustments in therapy. It is still a very important tool for the assessment of hemodynamic parameters, such as cardiac power and stroke work index, which are important data for short-term prognosis.It may also be helpful in distinguishing cardiogenic shock from septic shock and in optimizing the patient’s left ventricular filling pressures. The presence of significant V waves (greatly exceeding the pulmonary capillary wedge pressure) on the pulmonary artery tracing suggests either acute mitral regurgitation or a ventricular septal defect. The revascularization procedure may consist of percutaneous coronary intervention procedure or coronary artery bypass graft surgery. Patients who have undergone reperfusion procedures with either percutaneous coronary intervention or fibrinolytic therapy, experiencing new symptoms, should also be evaluated for failure of the initial treatment.
Medical Therapy
Cardiogenic shock is a medical emergency, rescusitive measures should be initiated immediately while the underlying etiology of the cardiogenic shock is promptly investigated. Myocardial infarction (MI) is the most common cause of cardiogenic shock, and when present, prompt revascularization should be performed. Other causes, such as free wall rupture, acute valvular abnormality, or left ventricular septum rupture, may require more invasive interventions. The management plan of cardiogenic shock includes the initiation of resuscitation and general measures, optimization of the blood pressure (pharmacological therapy or mechanical therapy when hypotension is refractory to inotrope and vasopressors), reperfusion or revascularization, and hemodynamic monitoring and stabilization. Urgent revascularization is a priority over hemodynamic monitoring in MI patients with cardiogenic shock and should not be delayed. The first line strategy for reperfusion is percutaneous coronary intervention which is preffered over coronary artery bypass graft (CABG), when PCI or CABG can not be perfomed, fibrinolytic therapy is indicated in the absence of any contraindications.
Surgery
Cardiogenic shock is considered an emergency and irrespectively to the therapeutic approach, the target goal of any therapy is prompt revascularization of ischemic myocardium. This should be achieved in the shortest timespan possible. There are two major categories of treatment for cardiogenic shock, the medical/conservative approach and the interventional approach. The ideal treatment combines both mechanisms, in which medical therapy, after restored filling pressures, allows hemodynamical stabilization of the patient, until interventional methods, that contribute to the reversal of the process leading to the shock state, may performed. The interventional approach may include PCI or coronary artery bypass graft surgery (CABG) and in both techniques the goal is not only reperfusion of the occluded coronary artery, but also prevention of vessel reoclusion. If there is no access to a cardiac catheterization facility, nor the possibility of transferring the patient to one within 90 minutes, then immediately thrombolytic therapy should be considered. Other important factors to increase the chances of a better outcome are: mechanical ventilation, in order to improve tissue oxygenation, and close monitoring of the therapeutic dosages, particularly of vasoactive drugs, since these have been associated with excess mortality due to toxicity effects.Also, it is recommended invasive hemodynamic monitoring, in order to monitor and guide the effects of the therapy as well as the overall status of the patient. The success of reperfusion is usually suggested by the relief of symptoms, restoration of hemodynamic parameters and electrical stability, as well as the reduction of at least 50% in the ST-segment on the EKG, in the case of a STEMI.
Primary Prevention
The most common causes of cardiogenic shock remain MI. The American College of Cardiology and American Heart Association, in collaboration with the Canadian Cardiovascular Society, have issued an update of the 2004 guideline for the management of patients with ST-segment elevation myocardial infarction. The American Academy of Family Physicians endorses and accepts this guideline as its policy. Early recognition and prompt initiation of reperfusion therapy remains the cornerstone of management of ST-segment elevation myocardial infarction. Aspirin should be given to symptomatic patients. Beta blockers should be used cautiously in the acute setting because they may increase the risk of cardiogenic shock and death. The combination of clopidogrel and aspirin is indicated in patients who have had ST-segment elevation myocardial infarction. A stepped care approach to analgesia for musculoskeletal pain in patients with coronary heart disease is provided. Cyclooxygenase inhibitors and nonsteroidal anti-inflammatory drugs increase mortality risk and should be avoided. Primary prevention is important to reduce the burden of heart disease.
Secondary Prevention
Secondary prevention includes early detection and halting the progression of established but asymptomatic disease. For CAD, this includes taking measures to prevent cardiovascular symptoms (e.g., dyspnea), damage (e.g., ventricular dysfunction), and events (e.g., acute coronary syndromes). However, once such symptoms, damage, or events occur, it is too late for secondary prevention.
Historical Perspective
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: João André Alves Silva, M.D. [2] Syed Musadiq Ali M.B.B.S.[3]
Overview
The term “cardiogenic shock” is thought to have first arisen in 1942 with Stead who, after studying a series of two patients, described them as having a “shock of cardiac origin”. This designation would later be rephrased as “cardiogenic shock”.However, the clinical features of cardiogenic shock had first been described by Herrick, in 1912, who noticed in severe coronary artery disease patients a profound weakness, a rapid pulse, pulmonary rales, faint cardiac tones, cyanosis and dyspnea.Despite its still high incidence and mortality nowadays, cardiogenic shock has seen its impact decreased throughout the years. Particularly since the 1970’s, when the mortality rate for this condition was about 80-90%, these values have been decreasing since then, particularly due to the earlier diagnosis and better management of CS, with more effective reperfusion techniques. Today the its mortality rate is about 50%.
Historical perspective
- Posttraumatic syndrome was first decribed by the Greek physicians, Hippocrates and Galen.
- The term shock would only be introduced in 1743 by the English physician Clarke, after the mistranslation of the work of French surgeon Henri Fraçois Le Dran, who in 1737 had written “A Treatise of of Reflections Drawn from Experience with Gunshot Wounds”, in which he had described the term “choc” as a result of a severe impact or jolt.
- Clarke defined it as a sudden deterioration of a patient’s condition following a severe trauma.
- The concept would then be spread by Edwin A. Moses, who in 1867 used it in his “A Practical Treatise on Shock after Operations and Injuries”, defining it as an “effect on the animal system, produced by violent injuries from any cause, or from violent mental emotions”.[1]
- The term “cardiogenic shock” is thought to have first arisen in 1942 with Stead who, after studying a series of two patients, described them as having a “shock of cardiac origin”.
- This designation would later be rephrased as “cardiogenic shock”.[2] However, the clinical features of cardiogenic shock had first been described by Herrick, in 1912, who noticed in severe coronary artery disease patients a profound weakness, a rapid pulse, pulmonary rales, faint cardiac tones, cyanosis and dyspnea.[3]
- In 1967, after studying a series of 250 patients with acute MI, Killip and Kimball proposed a clinical classification of hemodynamic status, which included 4 classes and that is still in widespread use:[4]
- I – no clinical signs of heart failure
- II – S3 gallop and/or basilar rales on lung auscultation and/or elevated JVP
- III – Pulmonary edema
- IV – Cardiogenic shock
- Throughout the years the outcome of cardiogenic shock has been improving, with a decrease in mortality seen particularly during the 1990’s.
- According to the studies, from 1975 to 1990, the in-hospital mortality from this condition averaged 77%. Between 1993 and 1995 this percentage declined to 61%, reaching about 59% in 1997.
- For this decrease, revascularization techniques along with an aggressive approach to shock have contributed greatly.[5][6]
References
- ↑ Parrillo, Joseph (2013). Critical care medicine principles of diagnosis and management in the adult. Philadelphia, PA: Elsevier/Saunders. ISBN 0323089291.
- ↑ Stead, Eugene A. (1942). “SHOCK SYNDROME PRODUCED BY FAILURE OF THE HEART”. Archives of Internal Medicine. 69 (3): 369. doi:10.1001/archinte.1942.00200150002001. ISSN 0003-9926.
- ↑ Herrick, James B. (1912). “CLINICAL FEATURES OF SUDDEN OBSTRUCTION OF THE CORONARY ARTERIES”. Journal of the American Medical Association. LIX (23): 2015. doi:10.1001/jama.1912.04270120001001. ISSN 0002-9955.
- ↑ Killip T, Kimball JT (1967). “Treatment of myocardial infarction in a coronary care unit. A two year experience with 250 patients”. Am J Cardiol. 20 (4): 457–64. PMID 6059183.
- ↑ Goldberg, Robert J.; Samad, Navid A.; Yarzebski, Jorge; Gurwitz, Jerry; Bigelow, Carol; Gore, Joel M. (1999). “Temporal Trends in Cardiogenic Shock Complicating Acute Myocardial Infarction”. New England Journal of Medicine. 340 (15): 1162–1168. doi:10.1056/NEJM199904153401504. ISSN 0028-4793.
- ↑ Hochman JS, Sleeper LA, Webb JG, Sanborn TA, White HD, Talley JD; et al. (1999). “Early revascularization in acute myocardial infarction complicated by cardiogenic shock. SHOCK Investigators. Should We Emergently Revascularize Occluded Coronaries for Cardiogenic Shock”. N Engl J Med. 341 (9): 625–34. doi:10.1056/NEJM199908263410901. PMID 10460813.
Classification
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Mohammad Salih, MD. João André Alves Silva, M.D. [2] Syed Musadiq Ali M.B.B.S.[3]
Overview
The Society for Cardiovascular Angiography and Intervention (SCAI) developed an expert consensus statement, endorsed by multiple relevant societies, proposing a novel CS classification scheme, which categorizes patients with or at risk of CS into worsening stages of hemodynamic compromise for the purposes of facilitating patient care and research. The SCAI CS classification consensus statement describes 5 stages of CS, each of which may have an “A” modifier signifying the occurrence of cardiac arrest (CA). This classification schema was developed based on expert consensus opinion and its ability to discriminate among levels of mortality risk in critically ill patients remains to be established. The goal of this study was to examine the construct validity of the SCAI CS staging schema by demonstrating the ability of a simple functional classification of SCAI shock stages at the time of cardiac intensive care unit (CICU) admission to predict mortality in CICU patients.The purpose of the classification schema is to assist in clear communication among clinicians and researchers regarding the patient’s current clinical status, recognizing that CS encompasses a spectrum, including those at high risk of developing shock from myocardial dysfunction to those who develop hemodynamic collapse and cardiac arrest. The CS classification schema includes five stages of shock labeled A through E. The authors categorized patients in three domains, including laboratory findings, physical exams findings, and hemodynamics. When cardiac arrest has occurred the modifier (A) is added to stage classification (i.e. stage CA).
Classification
- Here is a brief description of each stage, including the domains of patient characteristics that you can expect to find when your patient is each stage.[1][2]
Stage A or “At Risk”
- Patient identified at risk of developing, but is not yet displaying signs or symptoms of CS
- Diagnoses such as non-ST elevated myocardial infarction, ST elevated myocardial infarction (especially in the anterior wall distribution or large infarcts), and decompensated heart failure (both systolic and diastolic)
- Physical exam, laboratory, and hemodynamics are within normal limits.
Stage B or “Beginning CS”
- Also referred to as pre-shock or compensated shock
- Patient with relative hypotension (SBP < 90 mm Hg or mean arterial pressure [MAP] < 60 mm Hg or drop in MAP of > 30 mm Hg from baseline) or tachycardia (pulse > 100 bpm) without hypoperfusion
- Physical exam findings may include elevated jugular vein distension (JVP), rales in lung fields, warm skin with strong distal pulses, normal mentation
- Laboratory findings may include normal lactate, minimal renal function impairment, and elevated brain natriuretic peptide (BNP)
- Hemodynamic findings include relative hypotension, tachycardia, normal cardiac index (≥ 2.2 L/min/m2) and pulmonary arterial (PA) oxygen saturation ≥ 65%.
Stage C or “Classic CS”
- Patient with hypotension and signs of hypoperfusion that require various interventions (inotropes, pressor, mechanical support, or extracorporeal membrane oxygenation [ECMO])
- Physical exam findings may include distressed/panicked appearance, ashen/mottled/ dusky skin color, extensive rales in lung fields, cold/clammy skin temperature, altered mentation, decreased urine output (< 30 mL/h)
- Laboratory findings may include lactate ≥ 2 mmol/L, decreased renal function (creatinine doubling or > 50% drop in glomerular filtration rate [GFR])
- Hemodynamic findings may include SBP <90 mm Hg or MAP < 60 mm Hg or drop in MAP > 30 mm Hg from baseline and devices/medications utilized to maintain adequate SBP, *cardiac index < 2.2 L/min/m2, pulmonary artery capillary wedge pressure (PCWP) > 15 mm Hg, cardiac power output ≤ 0.6 W/m2.
Stage D or “Deteriorating or Doom CS”
- Patient who fail to stabilize after at least 30 minutes of initial treatment methods
- Treatment efforts are escalated, including the addition of multiple pressors; mechanical circulatory support may be initiated
- Physical exam, laboratory, and hemodynamic findings are similar to those found in stage C, but deteriorating.
Stage E or “Extremis”
- Patient with circulatory collapse, possibly with cardiac arrest with ongoing cardiopulmonary resuscitation (CPR) and/or ECMO
- Patient requires multiple interventions (mechanical ventilation, defibrillation) and assistance from multiple clinicians
- Physical exam findings may include near pulselessness, severe hypotension, lethal cardiac disturbances (pulseless electrical activity [PEA], ventricular tachycardia, ventricular fibrillation)
- Laboratory findings may include lactate ≥ 5 mmol/L and pH ≤ 7
- Hemodynamic findings include no SBP without resuscitation, PEA or ventricular arrythmias, hypotension despite maximum medical interventions.
In cardiogenic shock, the root abnormality is the inability of the heart to pump out enough blood to maintain normal organ perfusion and blood pressure. However, this failure may be due to different factors, which allow us to classify cardiogenic shock into two categories:[3][4][5]
- Intrinsic – this includes the conditions affecting the heart or the structures that allow it to function properly. In this category, the affected structures may be: the myocardial muscle, responsible to pump out the blood; the heart valves allowing the blood in and out of the heart chambers; the conduction system, responsible for the transmission of the electrical signals that allow the myocardium to contract in a coordinated fashion or, a combination of the previous. Examples of such factors are: myocardial infarction, mitral regurgitation and electrolyte imbalances.
- Compressive – this includes the conditions in which an otherwise “healthy heart” is prevented from working properly and pumping the blood through the vascular system, by a mechanism not related to it. The degree of impact that an extrinsic factor must have on the heart will depend on the overall “health status” of this last one. An “healthy heart” might take a more aggressive outside influence without compromising its function, while a heart already weakened by another disease, such as atherosclerosis, might fail more promptly. An example of such factor is cardiac tamponade.
Often times both factors are affecting the heart‘s ability to perform its function, at which times it might be hard to identify clearly the underlying mechanism of the cardiogenic shock.[6]
References
- ↑ . doi:10.1016/j.jacc.2019.07.07. Missing or empty
|title=(help) - ↑ van Diepen, Sean; Katz, Jason N.; Albert, Nancy M.; Henry, Timothy D.; Jacobs, Alice K.; Kapur, Navin K.; Kilic, Ahmet; Menon, Venu; Ohman, E. Magnus; Sweitzer, Nancy K.; Thiele, Holger; Washam, Jeffrey B.; Cohen, Mauricio G. (2017). “Contemporary Management of Cardiogenic Shock: A Scientific Statement From the American Heart Association”. Circulation. 136 (16). doi:10.1161/CIR.0000000000000525. ISSN 0009-7322.
- ↑ Longo, Dan L. (Dan Louis) (2012). Harrison’s principles of internal medici. New York: McGraw-Hill. ISBN 978-0-07-174889-6.
- ↑ Myers, Jeffrey (2002). Principles of pathophysiology and emergency medical care. Albany: Delmar/Thomson Learning. ISBN 978-0766825482.
- ↑ Kheng CP, Rahman NH (July 2012). “The use of end-tidal carbon dioxide monitoring in patients with hypotension in the emergency department”. Int J Emerg Med. 5 (1): 31. doi:10.1186/1865-1380-5-31. PMC 3585511. PMID 22828152.
- ↑ Myers, Jeffrey (2002). Principles of pathophysiology and emergency medical care. Albany: Delmar/Thomson Learning. ISBN 978-0766825482.
Pathophysiology
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Mohammad Salih, MD. João André Alves Silva, M.D. [2] Syed Musadiq Ali M.B.B.S.[3]
Overview
The pathophysiology of cardiogenic shock is complex and not fully understood. Ischemia to the myocardium causes derangement to both systolic and diastolic left ventricular function, resulting in a profound depression of myocardial contractility. This, in turn, leads to a potentially catastrophic and vicious spiral of reduced cardiac output and low blood pressure, perpetuating further coronary ischemia and impairment of contractility. Several physiologic compensatory processes ensue. These include:The activation of the sympathetic system leading to peripheral vasoconstriction which may improve coronary perfusion at the cost of increased afterload, and Tachycardia which increases myocardial oxygen demand and subsequently worsens myocardial ischemia.These compensatory mechanisms are subsequently counteracted by pathologic vasodilation that occurs from the release of potent systemic inflammatory markers such as interleukin-1, tumor necrosis factor a, and interleukin-6. Additionally, higher levels of nitric oxide and peroxynitrite are released, which also contribute to pathologic vasodilation and are known to be cardiotoxic. Unless interrupted by adequate treatment measures, this self-perpetuating cycle leads to global hypoperfusion and the inability to effectively meet the metabolic demands of the tissues, progressing to multiorgan failure and eventually death.
Pathophysiology
- The most common insult for cardiogenic shock is left ventricular pump failure in the setting of acute myocardial infarction.
- It usually takes a considerable area of infarcted myocardium (around 40%) to lead to cardiogenic shock.
- A smaller infarct may also originate this condition in a patient with a previously compromised ventricle function.
- There may also be other etiologies, other parts of the circulatory system may contribute, either alone or in combination, with inadequate compensation, or additional defects for this shock of cardiac origin, such as:[1]
- Systolic Left Ventricular Dysfunction – acute myocardial infarction, CHF, Cardiomyopathy, Coronary artery bypass grafting, Myocarditis, Myocardial contusion and Hypophosphatemia
- Diastolic Left Ventricular Dysfunction – Ischemia
- Obstruction of Left Ventricular Outflow, with Increased Afterload – Aortic stenosis, Hypertrophic Cardiomyopathy, Coarctation of the Aorta and Malignant Hypertension
- Reversal of flow into the left ventricle – Acute aortic insufficiency and endocarditis
- Inadequate left ventricular filling due to mechanical causes – Tamponade and pulmonary embolism
- Inadequate left ventricular filling due to inadequate filling time – Tachycardia and tachycardia-mediated cardiomyopathy
- Conduction abnormalities – Atrioventricular block and sinus bradycardia
- Mechanical defect – VSD and left ventricle free wall rupture
- Right ventricular failure – Pulmonary embolism and hypoxic pulmonary vasoconstriction[1]
The downward “Spiral” of Cardiogenic shock
- Cardiac dysfunction in patients with cardiogenic shock is usually initiated by myocardial infarction or ischemia.
- The myocardial dysfunction resulting from ischemia worsens that ischemia, creating a downward spiral.
- When a critical mass of left ventricular myocardium is ischemic or necrotic and fails to pump, stroke volume and cardiac output decrease.
- Myocardial perfusion, which depends on the pressure gradient between the coronary arterial system and the left ventricle.
- The duration of diastole, is compromised by hypotension and tachycardia. Which in turn, exacerbates ischemia.
- The increased ventricular diastolic pressures caused by pump failure further reduce coronary perfusion pressure, and the additional wall stress elevates myocardial oxygen requirements, further worsening ischemia.
- Decreased cardiac output also compromises systemic perfusion, which can lead to lactic acidosis and further compromise of systolic performance.
- The pathologic process begins with myocardial ischemia leading to an abnormal function of the cardiac muscle.
- This abnormality worsens the initial ischemia, which then deteriorates even further the ventricular function, creating the so called “downward spiral”.[2]
- When ischemia reaches a point that the left ventricular myocardium fails to pump properly, parameters like stroke volume and cardiac output will therefore decrease.
- The pressure gradient produced between the pressure within the coronary arteries and the left ventricle, along with the duration of the diastole, dictate myocardial perfusion.
- This will be compromised by the hypotension and the tachycardia, worsening the myocardial ischemia and the perfusion of other vital organs.
- The fact that the heart is the only organ that benefits from a low blood pressure, as afterload decreases, makes these hemodynamical changes both beneficial and detrimental.
- The pump failure will then decrease the ability to push the blood out of the ventricle, thereby increasing the ventricular diastolic pressures.
- This will not only reduce the coronary perfusion pressure, as it will also increase the ventricle wall stress, so that the myocardial oxygen requirements will also raise, consequently propagating the ischemia.[2][1][3]
- cardiac pump failure and hypoperfusion of the peripheral tissues is that this last one, leads to the release of catecholamines.
- Catecholamines such as norepinephrine, will increase the heart‘s contractility and peripheral blood flow, by causing constriction of arterioles, together with angiotensin II, to maintain perfusion, however, this will also increase the heart‘s oxygen demand and have proarrhythmic and myocardiotoxic consequences.
- The increased SVR coupled with the low cardiac output will lead to an even more pronounced reduction of tissue perfusion.[1]
- The ischemia generated by all these processes increases the diastolic stiffness of the ventricle wall and this, along with the left ventricular dysfunction, will increase the left atrial pressure. The increased left atrial pressure will propagate through the pulmonary veins, generating pulmonary congestion, which by decreasing oxygen exchanges, leads to hypoxia.
- The hypoxia will further worsen the ischemia of the myocardium and the pulmonary congestion will propagate its effect through the pulmonary arteries to the right ventricle, hence jeopardizing its performance.
- Once myocardial function is affected, the body will put in motion compensatory mechanisms to try to increase the cardiac output. These include:[4]
- Tachycardia and increased contractility through sympathetic stimulation
- Activation of the renin/angiotensin/aldosterone system, leading to fluid retention and consequently increased preload
- These compensatory mechanisms eventually become maladaptive seeing that:[1][5]
- Tachycardia and increased contractility will increase cardiac muscle oxygen demand, thereby exacerbating the initial ischemia;
- Vasoconstriction, as a response to impaired cardiac output, in order to try to maintain coronary artery perfusion and systemic blood pressure (SVR) increases myocardial afterload, leading to an impairment in myocardial performance and an increase in its oxygen demand, worsening ischemia;
- The activation of the neurohormonal cascade will promote retention of water and sodium, in order to compensate for the hypotension and improve perfusion, yet this will also exacerbate pulmonary edema.
- The prolonged systemic hypoperfusion and hypoxia will cause a shift in cellular metabolism, prioritizing glycolysis, leading to a state of lactic acidosis, which jeopardizes contractility and systolic performance, thereby affecting the previously described system.
- All these factors affecting oxygen demand and cardiac performance create a vicious cycle that if not interrupted, may eventually lead to death.
- The therapeutic approach to cardiogenic shock focuses in disrupting this cycle.[6]
- The area of original infarct, remote territories may also exhibit some kind of myocardial damage, called myocardial stunning.
- Myocardial stunning is the name given the myocardium which remains dysfunctional even though the restoration to normal perfusion.
- The pathophysiology of myocardial stunning is multifactorial and involves calcium overload in the sarcolemma and diastolic dysfunction, as well as the release of myocardial depressant substances.
- This calcium overload is responsible for the activation of proteases called calpains. These and other proteases will be responsible for the degradation of myofilaments, which will decrease the response to calcium, thereby explaining the temporary myocardial dysfunction after reperfusion.
- Areas of stunned myocardium may remain stunned after revascularization due to the need to resynthetize new myofilaments.[7]
- These regions retain contractile reserve and usually respond to inotropic stimulation.
- Stunned myocardium, hibernating myocardium does respond earlier to revascularization since myocardial cells remain viable and when reperfused, calcium levels normalize.[8][9][10]
Right Ventricle Myocardial Infarction
- 5% of the cases but represents as high mortality rate as left ventricular shock.
- The right ventricular regions more commonly affected by infarction are the inferior and inferior-posterior walls.
- The coronary arteries frequently occluded in this setting are the right coronary artery, or the left circumflex coronary artery, in a left dominant system.[11][12] Patients with right coronary artery occlusion, in a right dominant system, are at higher risk of developing papillary muscle rupture and therefore undergoing valvular heart disease, such as mitral regurgitation.[12][13][14]
- Right ventricle failure may affect left ventricular performance by several means:[15][16]
- Decrease in right ventricular output leading to a decrease in left ventricular filling thereby affecting overall cardiac output;
- Increased right ventricular telediastolic pressure, leading to a shifting of the interventricular septum into the left ventricle, therefore jeopardizing left ventricular filling and systolic function.
Ventricular Septal and Free Wall Rupture
- Ventricular septal rupture and free wall rupture, which constitute two entities of cardiac rupture, represent the second most common cause of death in patients with acute myocardial infarction, during hospital stay.[17][18][19]
- Ventricular septal rupture in the SHOCK registry, it accounted for 4.6% of the cases of cardiogenic shock.[20]
- The most recent registries show that ventricular septal rupture generally develops within the first 16 to 24 hours post-MI and has the following characteristics:[21][22][23][24][25][12][26][12][27][28]
- According to the SHOCK trial data, this type of rupture had 55% of mortality rate within the first 30 days.[28] Free wall rupture may also be classified as simple or complex. It may occur either on the anterior or the lateral and posterior left ventricular walls.[28][17] These last two are thought to rupture easier, however, because of the higher proportion of anterior MIs, they are seen less frequently.[12]
- The rupture may present with different types of courses:
- Acute – the patient generally feels acute onset of chest pain, developing cardiac tamponade, hemodynamical collapse and sudden death. Because of the rapid course of this type, it is usually not controlled with current therapies.[29][30]
- Subacute – this type generally results in smaller and contained ruptures. These may be stabilized by the formation of a clot or fibrinous pericardial adhesions for a short period of time. Therapeutical measures must be applied urgently.[31][24]
- Chronic – less frequently associated with cardiogenic shock.
Inflammation and Hemodynamics
- Studies like the SHOCK trial show that not all patients follow this classic paradigm, since:[32][33][34]
- The range of elevation of systemic vascular resistance in this trial was wide, suggesting that the compensatory vasoconstriction wasn’t a rule in every patient;
- The mean ejection fraction was also moderately decreased in this trial, showing that other mechanisms besides cardiac failure were present;
- Some of the patients had leukocytosis and fever, which along with the decreased systemic vascular resistance suggested SIRS.
- These facts have introduced the concept that myocardial infarction may cause SIRS and that inflammation plays an important part in the development and persistence of cardiogenic shock, contributing to myocardial dysfunction and vasodilation.
- The possibility of developing SIRS raises with the increasing permanence in cardiogenic shock.[1][35][36]
- At the time of the cardiac injury, the myocardium releases into circulation cytokines, particularly during the first 24 to 72 hours after the MI. *These will induce the enzyme nitric oxide synthase, thereby increasing the level of nitric oxide, which will be responsible for vasodilation and worsening of hypotension, further jeopardizing left ventricle performance.[37][38][39][40][41][42] NO may also form a toxic radical, called peroxynitrite, when combined with superoxide, affecting myocardial contractility.[43]
- Among these released cytokines during cardiogenic shock, are interleukin-6 and tumor necrosis factor.
- IL-6,is specific cytokine is correlated with the degree of organ failure and therefore mortality.[44]
- These inflammatory mediators, among other actions, are responsible for the release of BNP, which makes the levels of BNP good markers, not only for the level of inflammation, but also to evaluate hemodynamic decompensation.[45]
- Other circulatory factors, such as procalcitonin, complement and CRP, have been reported in some studies to contribute to the development of SIRS in cardiogenic shock.[46][47]
- Besides the aforementioned macrocirculatory changes in cardiogenic shock, which may also be seen in septic shock, it is important to mention that microcirculatory abnormalities, caused in part by the inflammatory cascades, play an important part in the pathogenesis of organ failure as well.[48][49][50]
Iatrogenic Cardiogenic Shock
- An important number of patients in cardiogenic shock complicating myocardial infarction (around 3/4), develop it after hospital admission.[51][52]
- In some of these patients, it is reported that the development of shock, particularly in high risk patients, is related to the use of certain classes of medications, used to treat the MI. These include:[53][54][55][56]
- Beta-blockers
- ACE inhibitors
- Morphine
- Diuretics (As a cause or aggravating factor. This is due to the fact that pulmonary edema is a common complication of cardiogenic shock, leading to a decrease of circulating plasma volume, particularly in patients with prior heart failure.
- After the administration of high-dose diuretics, the plasma volume will further decline)
- Excess fluid administration (In the case of right ventricular myocardial infarction, the excess volume loading in these patients may also contribute to the development of shock)
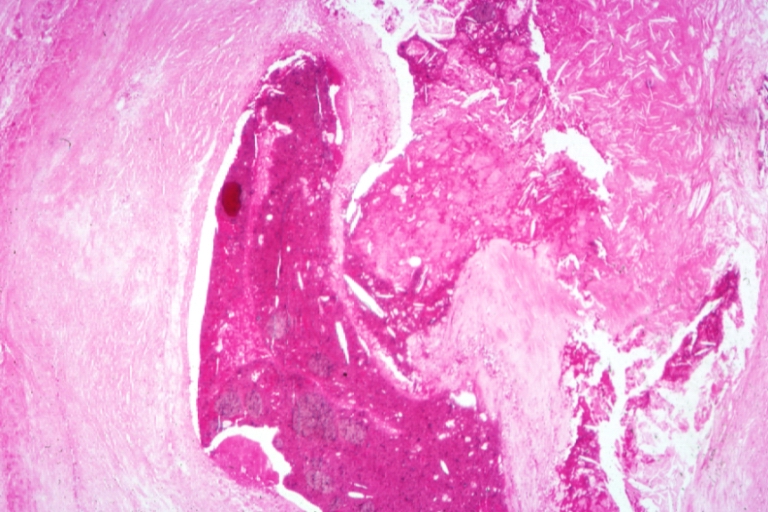
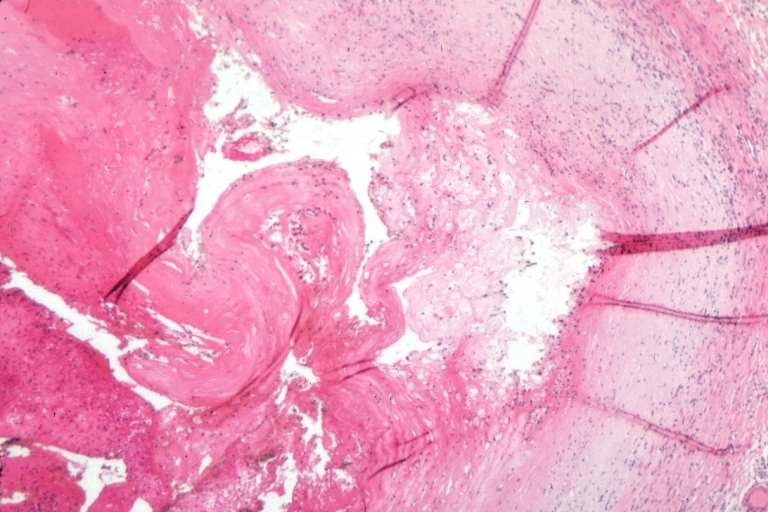
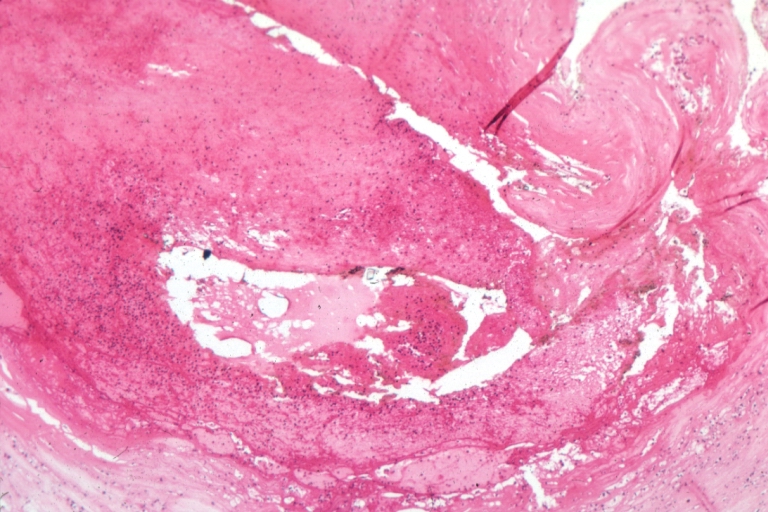
Histopathological Findings Of myocardial infarction and plaque rupture
http://www.peir.net Images courtesy of Professor Peter Anderson DVM PhD and published with permission © PEIR, University of Alabama at Birmingham, Department of Pathology]
-
 Coronary artery: Atherosclerosis: Micro H&E med mag; A good example of plaque rupture with thrombosis.
Coronary artery: Atherosclerosis: Micro H&E med mag; A good example of plaque rupture with thrombosis. -
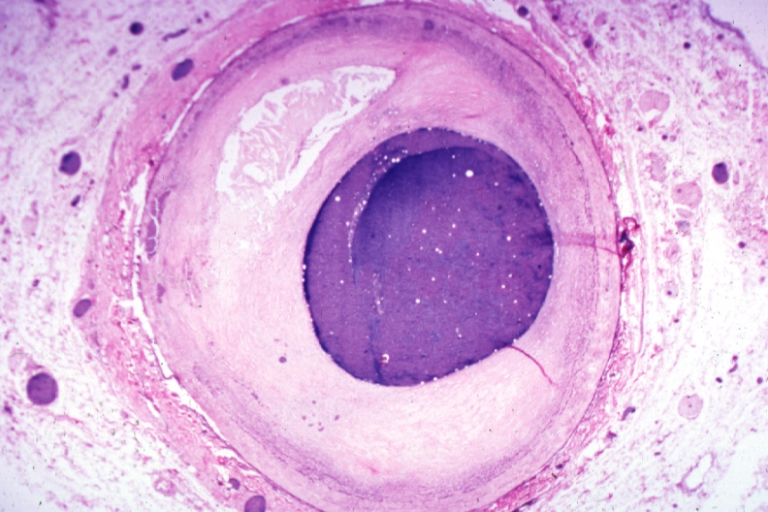
 Right coronary artery: Ruptured Plaque: Micro low mag H&E; Ruptured plaque with foam cell lesion (near rupture site).
Right coronary artery: Ruptured Plaque: Micro low mag H&E; Ruptured plaque with foam cell lesion (near rupture site).


-
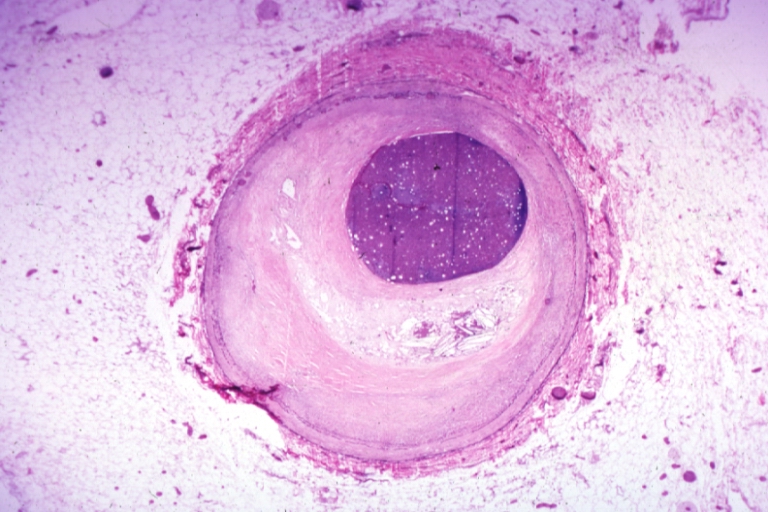
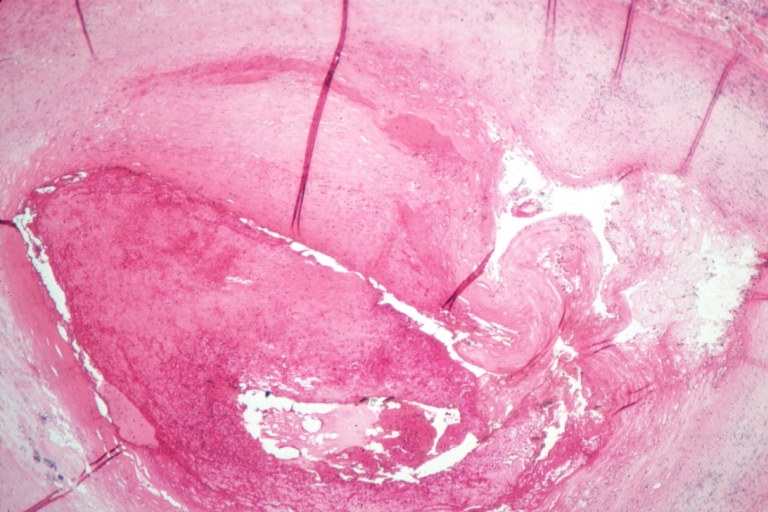 Right coronary artery: Atherosclerosis Plaque Ruptured with Thrombus: Micro low mag H&E; an excellent view of ruptured plaque with thrombus and some old fibrin in it.
Right coronary artery: Atherosclerosis Plaque Ruptured with Thrombus: Micro low mag H&E; an excellent view of ruptured plaque with thrombus and some old fibrin in it. -
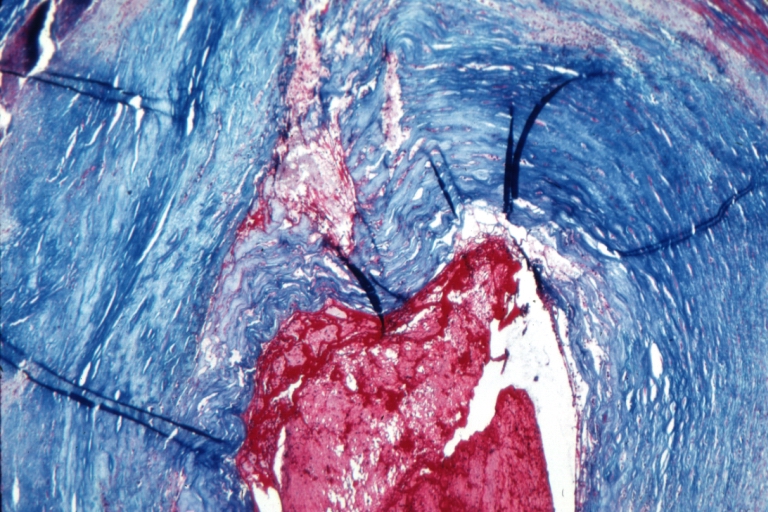 Right coronary artery: Atherosclerosis Plaque Ruptured with Thrombus: Micro low mag trichrome.
Right coronary artery: Atherosclerosis Plaque Ruptured with Thrombus: Micro low mag trichrome.


-
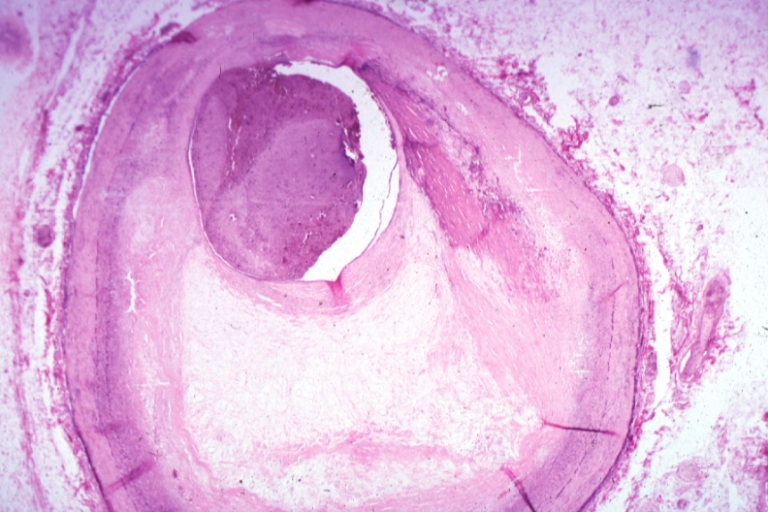
 Right coronary artery: Atherosclerosis Plaque Ruptured: Micro low mag H&E; large plaque with hemorrhage; (an excellent example of hemorrhage).
Right coronary artery: Atherosclerosis Plaque Ruptured: Micro low mag H&E; large plaque with hemorrhage; (an excellent example of hemorrhage). -
 Coronary artery: Atherosclerosis: Micro H&E low mag injected artery fairly typical uncomplicated atheromatous plaque
Coronary artery: Atherosclerosis: Micro H&E low mag injected artery fairly typical uncomplicated atheromatous plaque


-
 Coronary artery: Atherosclerosis: Micro H&E low mag, injected artery has typical fibrous plaque with small hemorrhage in atheroma.
Coronary artery: Atherosclerosis: Micro H&E low mag, injected artery has typical fibrous plaque with small hemorrhage in atheroma. -
 Coronary artery: Atherosclerosis: Micro H&E low mag, injected artery is a very good example of marked lumen stenosis due to typical fibrous plaque with calcification
Coronary artery: Atherosclerosis: Micro H&E low mag, injected artery is a very good example of marked lumen stenosis due to typical fibrous plaque with calcification


References
- ↑ 1.0 1.1 1.2 1.3 1.4 1.5 Reynolds, H. R.; Hochman, J. S. (2008). “Cardiogenic Shock: Current Concepts and Improving Outcomes”. Circulation. 117 (5): 686–697. doi:10.1161/CIRCULATIONAHA.106.613596. ISSN 0009-7322.
- ↑ 2.0 2.1 Hollenberg SM, Kavinsky CJ, Parrillo JE (1999). “Cardiogenic shock”. Ann Intern Med. 131 (1): 47–59. PMID 10391815.
- ↑ Hasdai, David. (2002). Cardiogenic shock : diagnosis and treatmen. Totowa, N.J.: Humana Press. ISBN 1-58829-025-5.
- ↑ Hasdai, David. (2002). Cardiogenic shock : diagnosis and treatmen. Totowa, N.J.: Humana Press. ISBN 1-58829-025-5.
- ↑ Hasdai, David. (2002). Cardiogenic shock : diagnosis and treatmen. Totowa, N.J.: Humana Press. ISBN 1-58829-025-5.
- ↑ Hasdai, David. (2002). Cardiogenic shock : diagnosis and treatmen. Totowa, N.J.: Humana Press. ISBN 1-58829-025-5.
- ↑ Bolli R, Marbán E (1999). “Molecular and cellular mechanisms of myocardial stunning”. Physiol Rev. 79 (2): 609–34. PMID 10221990.
- ↑ Hasdai, David. (2002). Cardiogenic shock : diagnosis and treatmen. Totowa, N.J.: Humana Press. ISBN 1-58829-025-5.
- ↑ Bolli R (1998). “Basic and clinical aspects of myocardial stunning”. Prog Cardiovasc Dis. 40 (6): 477–516. PMID 9647607.
- ↑ Marban E (1991). “Myocardial stunning and hibernation. The physiology behind the colloquialisms”. Circulation. 83 (2): 681–8. PMID 1991384.
- ↑ Isner JM, Roberts WC (1978). “Right ventricular infarction complicating left ventricular infarction secondary to coronary heart disease. Frequency, location, associated findings and significance from analysis of 236 necropsy patients with acute or healed myocardial infarction”. Am J Cardiol. 42 (6): 885–94. PMID 153103.
- ↑ 12.0 12.1 12.2 12.3 12.4 Ng, R.; Yeghiazarians, Y. (2011). “Post Myocardial Infarction Cardiogenic Shock: A Review of Current Therapies”. Journal of Intensive Care Medicine. 28 (3): 151–165. doi:10.1177/0885066611411407. ISSN 0885-0666.
- ↑ Reeder GS (1995). “Identification and treatment of complications of myocardial infarction”. Mayo Clin Proc. 70 (9): 880–4. doi:10.1016/S0025-6196(11)63946-3. PMID 7643642.
- ↑ Lavie CJ, Gersh BJ (1990). “Mechanical and electrical complications of acute myocardial infarction”. Mayo Clin Proc. 65 (5): 709–30. PMID 2190052.
- ↑ Jacobs AK, Leopold JA, Bates E, Mendes LA, Sleeper LA, White H; et al. (2003). “Cardiogenic shock caused by right ventricular infarction: a report from the SHOCK registry”. J Am Coll Cardiol. 41 (8): 1273–9. PMID 12706920.
- ↑ Brookes, C.; Ravn, H.; White, P.; Moeldrup, U.; Oldershaw, P.; Redington, A. (1999). “Acute Right Ventricular Dilatation in Response to Ischemia Significantly Impairs Left Ventricular Systolic Performance”. Circulation. 100 (7): 761–767. doi:10.1161/01.CIR.100.7.761. ISSN 0009-7322.
- ↑ 17.0 17.1 Figueras J, Alcalde O, Barrabés JA, Serra V, Alguersuari J, Cortadellas J; et al. (2008). “Changes in hospital mortality rates in 425 patients with acute ST-elevation myocardial infarction and cardiac rupture over a 30-year period”. Circulation. 118 (25): 2783–9. doi:10.1161/CIRCULATIONAHA.108.776690. PMID 19064683.
- ↑ Becker RC, Gore JM, Lambrew C, Weaver WD, Rubison RM, French WJ; et al. (1996). “A composite view of cardiac rupture in the United States National Registry of Myocardial Infarction”. J Am Coll Cardiol. 27 (6): 1321–6. PMID 8626938.
- ↑ Becker RC, Hochman JS, Cannon CP, Spencer FA, Ball SP, Rizzo MJ; et al. (1999). “Fatal cardiac rupture among patients treated with thrombolytic agents and adjunctive thrombin antagonists: observations from the Thrombolysis and Thrombin Inhibition in Myocardial Infarction 9 Study”. J Am Coll Cardiol. 33 (2): 479–87. PMID 9973029.
- ↑ Hochman JS, Buller CE, Sleeper LA, Boland J, Dzavik V, Sanborn TA; et al. (2000). “Cardiogenic shock complicating acute myocardial infarction–etiologies, management and outcome: a report from the SHOCK Trial Registry. SHould we emergently revascularize Occluded Coronaries for cardiogenic shocK?”. J Am Coll Cardiol. 36 (3 Suppl A): 1063–70. PMID 10985706.
- ↑ Thompson CR, Buller CE, Sleeper LA, Antonelli TA, Webb JG, Jaber WA; et al. (2000). “Cardiogenic shock due to acute severe mitral regurgitation complicating acute myocardial infarction: a report from the SHOCK Trial Registry. SHould we use emergently revascularize Occluded Coronaries in cardiogenic shocK?”. J Am Coll Cardiol. 36 (3 Suppl A): 1104–9. PMID 10985712.
- ↑ Crenshaw BS, Granger CB, Birnbaum Y, Pieper KS, Morris DC, Kleiman NS; et al. (2000). “Risk factors, angiographic patterns, and outcomes in patients with ventricular septal defect complicating acute myocardial infarction. GUSTO-I (Global Utilization of Streptokinase and TPA for Occluded Coronary Arteries) Trial Investigators”. Circulation. 101 (1): 27–32. PMID 10618300.
- ↑ Radford MJ, Johnson RA, Daggett WM, Fallon JT, Buckley MJ, Gold HK; et al. (1981). “Ventricular septal rupture: a review of clinical and physiologic features and an analysis of survival”. Circulation. 64 (3): 545–53. PMID 7020978.
- ↑ 24.0 24.1 Skehan JD, Carey C, Norrell MS, de Belder M, Balcon R, Mills PG (1989). “Patterns of coronary artery disease in post-infarction ventricular septal rupture”. Br Heart J. 62 (4): 268–72. PMC 1277362. PMID 2803872.
- ↑ SWITHINBANK JM (1959). “Perforation of the interventricular septum in myocardial infarction”. Br Heart J. 21: 562–6. PMC 1017615. PMID 13836145.
- ↑ Cohn, Lawrence (2012). Cardiac surgery in the adult. New York: McGraw-Hill Medical. ISBN 978-0-07-163310-9.
- ↑ Oliva PB, Hammill SC, Edwards WD (1993). “Cardiac rupture, a clinically predictable complication of acute myocardial infarction: report of 70 cases with clinicopathologic correlations”. J Am Coll Cardiol. 22 (3): 720–6. PMID 8354804.
- ↑ 28.0 28.1 28.2 Slater J, Brown RJ, Antonelli TA, Menon V, Boland J, Col J; et al. (2000). “Cardiogenic shock due to cardiac free-wall rupture or tamponade after acute myocardial infarction: a report from the SHOCK Trial Registry. Should we emergently revascularize occluded coronaries for cardiogenic shock?”. J Am Coll Cardiol. 36 (3 Suppl A): 1117–22. PMID 10985714.
- ↑ Figueras J, Cortadellas J, Soler-Soler J (2000). “Left ventricular free wall rupture: clinical presentation and management”. Heart. 83 (5): 499–504. PMC 1760810. PMID 10768896.
- ↑ Cohn, Lawrence (2012). Cardiac surgery in the adult. New York: McGraw-Hill Medical. ISBN 007163312X.
- ↑ Cohn, Lawrence (2012). Cardiac surgery in the adult. New York: McGraw-Hill Medical. ISBN 007163312X.
- ↑ Hochman JS, Sleeper LA, Webb JG, Sanborn TA, White HD, Talley JD; et al. (1999). “Early revascularization in acute myocardial infarction complicated by cardiogenic shock. SHOCK Investigators. Should We Emergently Revascularize Occluded Coronaries for Cardiogenic Shock”. N Engl J Med. 341 (9): 625–34. doi:10.1056/NEJM199908263410901. PMID 10460813.
- ↑ Picard MH, Davidoff R, Sleeper LA, Mendes LA, Thompson CR, Dzavik V; et al. (2003). “Echocardiographic predictors of survival and response to early revascularization in cardiogenic shock”. Circulation. 107 (2): 279–84. PMID 12538428.
- ↑ Kohsaka S, Menon V, Lowe AM, Lange M, Dzavik V, Sleeper LA; et al. (2005). “Systemic inflammatory response syndrome after acute myocardial infarction complicated by cardiogenic shock”. Arch Intern Med. 165 (14): 1643–50. doi:10.1001/archinte.165.14.1643. PMID 16043684.
- ↑ Hochman, J. S. (2003). “Cardiogenic Shock Complicating Acute Myocardial Infarction: Expanding the Paradigm”. Circulation. 107 (24): 2998–3002. doi:10.1161/01.CIR.0000075927.67673.F2. ISSN 0009-7322.
- ↑ Brunkhorst FM, Clark AL, Forycki ZF, Anker SD (1999). “Pyrexia, procalcitonin, immune activation and survival in cardiogenic shock: the potential importance of bacterial translocation”. Int J Cardiol. 72 (1): 3–10. PMID 10636626.
- ↑ Hasdai, David. (2002). Cardiogenic shock : diagnosis and treatmen. Totowa, N.J.: Humana Press. ISBN 1-58829-025-5.
- ↑ Neumann, F.-J.; Ott, I.; Gawaz, M.; Richardt, G.; Holzapfel, H.; Jochum, M.; Schomig, A. (1995). “Cardiac Release of Cytokines and Inflammatory Responses in Acute Myocardial Infarction”. Circulation. 92 (4): 748–755. doi:10.1161/01.CIR.92.4.748. ISSN 0009-7322.
- ↑ Shah, A (2000). “Inducible nitric oxide synthase and cardiovascular disease”. Cardiovascular Research. 45 (1): 148–155. doi:10.1016/S0008-6363(99)00316-8. ISSN 0008-6363.
- ↑ Feng Q, Lu X, Jones DL, Shen J, Arnold JM (2001). “Increased inducible nitric oxide synthase expression contributes to myocardial dysfunction and higher mortality after myocardial infarction in mice”. Circulation. 104 (6): 700–4. PMID 11489778.
- ↑ Cotter G, Kaluski E, Blatt A, Milovanov O, Moshkovitz Y, Zaidenstein R; et al. (2000). “L-NMMA (a nitric oxide synthase inhibitor) is effective in the treatment of cardiogenic shock”. Circulation. 101 (12): 1358–61. PMID 10736276.
- ↑ Kaluski E, Hendler A, Blatt A, Uriel N (2006). “Nitric oxide synthase inhibitors in post-myocardial infarction cardiogenic shock–an update”. Clin Cardiol. 29 (11): 482–8. PMID 17133844.
- ↑ Ferdinandy P, Danial H, Ambrus I, Rothery RA, Schulz R (2000). “Peroxynitrite is a major contributor to cytokine-induced myocardial contractile failure”. Circ Res. 87 (3): 241–7. PMID 10926876.
- ↑ Geppert A, Dorninger A, Delle-Karth G, Zorn G, Heinz G, Huber K (2006). “Plasma concentrations of interleukin-6, organ failure, vasopressor support, and successful coronary revascularization in predicting 30-day mortality of patients with cardiogenic shock complicating acute myocardial infarction”. Crit Care Med. 34 (8): 2035–42. doi:10.1097/01.CCM.0000228919.33620.D9. PMID 16775569.
- ↑ Rudiger A, Gasser S, Fischler M, Hornemann T, von Eckardstein A, Maggiorini M (2006). “Comparable increase of B-type natriuretic peptide and amino-terminal pro-B-type natriuretic peptide levels in patients with severe sepsis, septic shock, and acute heart failure”. Crit Care Med. 34 (8): 2140–4. doi:10.1097/01.CCM.0000229144.97624.90. PMID 16763507.
- ↑ Granger CB, Mahaffey KW, Weaver WD, Theroux P, Hochman JS, Filloon TG; et al. (2003). “Pexelizumab, an anti-C5 complement antibody, as adjunctive therapy to primary percutaneous coronary intervention in acute myocardial infarction: the COMplement inhibition in Myocardial infarction treated with Angioplasty (COMMA) trial”. Circulation. 108 (10): 1184–90. doi:10.1161/01.CIR.0000087447.12918.85. PMID 12925454.
- ↑ APEX AMI Investigators. Armstrong PW, Granger CB, Adams PX, Hamm C, Holmes D; et al. (2007). “Pexelizumab for acute ST-elevation myocardial infarction in patients undergoing primary percutaneous coronary intervention: a randomized controlled trial”. JAMA. 297 (1): 43–51. doi:10.1001/jama.297.1.43. PMID 17200474.
- ↑ De Backer D, Creteur J, Dubois MJ, Sakr Y, Vincent JL (2004). “Microvascular alterations in patients with acute severe heart failure and cardiogenic shock”. Am Heart J. 147 (1): 91–9. PMID 14691425.
- ↑ De Backer D, Creteur J, Preiser JC, Dubois MJ, Vincent JL (2002). “Microvascular blood flow is altered in patients with sepsis”. Am J Respir Crit Care Med. 166 (1): 98–104. PMID 12091178.
- ↑ Trzeciak S, Dellinger RP, Parrillo JE, Guglielmi M, Bajaj J, Abate NL; et al. (2007). “Early microcirculatory perfusion derangements in patients with severe sepsis and septic shock: relationship to hemodynamics, oxygen transport, and survival”. Ann Emerg Med. 49 (1): 88–98, 98.e1–2. doi:10.1016/j.annemergmed.2006.08.021. PMID 17095120.
- ↑ Babaev A, Frederick PD, Pasta DJ, Every N, Sichrovsky T, Hochman JS; et al. (2005). “Trends in management and outcomes of patients with acute myocardial infarction complicated by cardiogenic shock”. JAMA. 294 (4): 448–54. doi:10.1001/jama.294.4.448. PMID 16046651.
- ↑ Jeger, R. V. (2006). “Emergency revascularization in patients with cardiogenic shock on admission: a report from the SHOCK trial and registry”. European Heart Journal. 27 (6): 664–670. doi:10.1093/eurheartj/ehi729. ISSN 0195-668X.
- ↑ Meine TJ, Roe MT, Chen AY, Patel MR, Washam JB, Ohman EM; et al. (2005). “Association of intravenous morphine use and outcomes in acute coronary syndromes: results from the CRUSADE Quality Improvement Initiative”. Am Heart J. 149 (6): 1043–9. doi:10.1016/j.ahj.2005.02.010. PMID 15976786.
- ↑ “ISIS-4: a randomised factorial trial assessing early oral captopril, oral mononitrate, and intravenous magnesium sulphate in 58,050 patients with suspected acute myocardial infarction. ISIS-4 (Fourth International Study of Infarct Survival) Collaborative Group”. Lancet. 345 (8951): 669–85. 1995. PMID 7661937.
- ↑ “Indications for ACE inhibitors in the early treatment of acute myocardial infarction: systematic overview of individual data from 100,000 patients in randomized trials. ACE Inhibitor Myocardial Infarction Collaborative Group”. Circulation. 97 (22): 2202–12. 1998. PMID 9631869.
- ↑ Chen ZM, Pan HC, Chen YP, Peto R, Collins R, Jiang LX; et al. (2005). “Early intravenous then oral metoprolol in 45,852 patients with acute myocardial infarction: randomised placebo-controlled trial”. Lancet. 366 (9497): 1622–32. doi:10.1016/S0140-6736(05)67661-1. PMID 16271643. Review in: ACP J Club. 2006 May-Jun;144(3):58-9 Review in: Evid Based Med. 2006 Jun;11(3):82-3
Causes
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: João André Alves Silva, M.D. [2] Syed Musadiq Ali M.B.B.S.[3]
Overview
The most common cause of cardiogenic shock is acute myocardial infarction with left ventricular dysfunction. Less commonly, right ventricular myocardial infarction can lead to cardiogenic shock. Other causes of cardiogenic shock include mechanical injuries such as acute valvular regurgitation or rupture, free wall rupture, and ventricular septum rupture.
Causes
Life Threatening Causes
Cardiogenic Shock is a life-threatening condition and must be treated as such irrespective of the causes. Life-threatening conditions may result in death or permanent disability within 24 hours if left untreated.
Common Causes
The most common causes of cardiogenic shock remain:[1]
However, other likewise important causes must be identified. These may be classified according to their nature into:
- Arrhythmic
- Mechanical
- Acute mitral regurgitation (papillary muscle rupture, chordae tendinae rupture)[6]
- Free wall rupture
- Hypertrophic cardiomyopathy[7]
- Obstruction to left ventricular filling (mitral stenosis, left atrial myxoma)
- Obstruction to left ventricular outflow tract (aortic stenosis, hypertrophic obstructive cardiomyopathy)
- Ventricular septal defect
- Myopathic
- Pharmacologic
Causes by Organ System
Causes in Alphabetical Order
Causes of Cardiogenic Shock Classified According to Underlying Pathophysiologic Mechanism
Systolic Left Ventricular Dysfunction
- Hypophosphatemia as can be seen in the refeeding syndrome)
- Septic shock with myocardial depression
Diastolic Left Ventricular Dysfunction
- Subendocardial ischemia
- Excess wall stress
Obstruction of Left Ventricular Outflow and Increased After Load
Reversal of Flow into the Left Ventricle
- Aortic insufficiency
- Endocarditis
- Aortic dissection
- Chordal rupture, from degenerative disease or trauma[13]
Inadequate Left Ventricular Filling due to Mechanical Causes
Inadequate Left Ventricular Filling due to Inadequate Filling Time
Conduction Abnormalities
Mechanical Defect
- Ventricular septal defect (VSD)
- Ruptured chordae
- Myocardial rupture of the left ventricular free wall
Right Ventricular Failure
Iatrogenic
- Excess administration of vasodilators and venodilators
- Apical balloon syndrome or Takotsubo cardiomyopathy[14]
Miscellaneous
References
- ↑ Reynolds, H. R.; Hochman, J. S. (2008). “Cardiogenic Shock: Current Concepts and Improving Outcomes”. Circulation. 117 (5): 686–697. doi:10.1161/CIRCULATIONAHA.106.613596. ISSN 0009-7322.
- ↑ Acharya D (2018). “Predictors of Outcomes in Myocardial Infarction and Cardiogenic Shock”. Cardiol Rev. 26 (5): 255–266. doi:10.1097/CRD.0000000000000190. PMC 6082598. PMID 29300230.
- ↑ Sánchez Marteles M, Urrutia A (March 2014). “[Acute heart failure: acute cardiogenic pulmonary edema and cardiogenic shock]”. Med Clin (Barc) (in Spanish; Castilian). 142 Suppl 1: 14–9. doi:10.1016/S0025-7753(14)70077-6. PMID 24930078.
- ↑ Kang S, An S, Yu HM, Kim J, Kim SH, Kim HJ, Chung SM (November 2013). “Cardiogenic shock accompanied by dynamic left ventricular outflow tract obstruction and myocardial bridging after transient complete atrioventricular block mimicking ST-elevation myocardial infarction: a case report”. BMC Res Notes. 6: 478. doi:10.1186/1756-0500-6-478. PMC 3874663. PMID 24252345.
- ↑ Eldar M, Sievner Z, Goldbourt U, Reicher-Reiss H, Kaplinsky E, Behar S (July 1992). “Primary ventricular tachycardia in acute myocardial infarction: clinical characteristics and mortality. The SPRINT Study Group”. Ann. Intern. Med. 117 (1): 31–6. doi:10.7326/0003-4819-117-1-31. PMID 1596045.
- ↑ Burton LV, Beier K. PMID 29763151. Missing or empty
|title=(help) - ↑ Sherrid MV, Swistel DG, Balaran S (December 2018). “Apical Ballooning and Cardiogenic Shock in Obstructive Hypertrophic Cardiomyopathy”. CASE (Phila). 2 (6): 243. doi:10.1016/j.case.2018.07.009. PMC 6302028. PMID 30582082.
- ↑ Mathew V, Misgar RA, Ghosh S, Mukhopadhyay P, Roychowdhury P, Pandit K, Mukhopadhyay S, Chowdhury S (2011). “Myxedema coma: a new look into an old crisis”. J Thyroid Res. 2011: 493462. doi:10.4061/2011/493462. PMC 3175396. PMID 21941682.
- ↑ Binaghi G, Congia D, Cossa S, Massidda S, Pasqualucci D, Pilo F, Serra E, Angelucci E, Porcu M (2018). “Cardiogenic Shock during First Infusion of Anthracycline Chemotherapy in a Patient with Hodgkin Lymphoma: An Unusual Event”. Cardiology. 139 (1): 7–10. doi:10.1159/000480291. PMID 29041005.
- ↑ Kleber FX, Sabin GV, Winter UJ, Reindl I, Beil S, Wenzel M, Fischer M, Doering W (August 1997). “Angiotensin-converting enzyme inhibitors in preventing remodeling and development of heart failure after acute myocardial infarction: results of the German multicenter study of the effects of captopril on cardiopulmonary exercise parameters (ECCE)”. Am. J. Cardiol. 80 (3A): 162A–167A. doi:10.1016/s0002-9149(97)00474-8. PMID 9293972.
- ↑ Mark AL (January 1983). “The Bezold-Jarisch reflex revisited: clinical implications of inhibitory reflexes originating in the heart”. J. Am. Coll. Cardiol. 1 (1): 90–102. doi:10.1016/s0735-1097(83)80014-x. PMID 6826948.
- ↑ Cárdenes León A, Gallardo Santos E, Prada Osorio R, López Pérez M, Martín Lorenzo PL (December 2017). “Cardiogenic Shock and Cardiac Tamponade in the Context of Influenza A Myopericarditis”. Rev Esp Cardiol (Engl Ed). 70 (12): 1149–1151. doi:10.1016/j.rec.2017.01.031. PMID 28454888.
- ↑ Hasdai, David. (2002). Cardiogenic shock : diagnosis and treatmen. Totowa, N.J.: Humana Press. ISBN 1-58829-025-5.
- ↑ Gianni, M. (2006). “Apical ballooning syndrome or takotsubo cardiomyopathy: a systematic review”. European Heart Journal. 27 (13): 1523–1529. doi:10.1093/eurheartj/ehl032. ISSN 0195-668X.
Differentiating Cardiogenic shock from other Diseases
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: João André Alves Silva, M.D. [2] Syed Musadiq Ali M.B.B.S.[3] Ramyar Ghandriz MD[4]
Overview
Shock is a clinical syndrome resulting from the hypoperfusion of the tissues. Regardless of the underlying cause, this hypoperfusion leads to the failure to meet tissues’ nutritional and oxygen needs, causing cellular dysfunction. The affected tissues lead to the production and release of inflammatory mediators that will further jeopardize perfusion through changes in the vasculature. The results of these changes are organ failure and death if treatment in not timely applied. According to the underlying cause, there will be different types of shock, which will have similar presentations. It is mandatory to determine the underlying cause of the condition so that proper treatment may be started. Cardiogenic shock is a clinical condition, defined as a state of systemic hypoperfusion originated in cardiac failure, in the presence of adequate intravascular volume, typically followed by hypotension, which leads to insufficient ability to meet oxygen and nutrient demands of organs and other peripheral tissues. It may range from mild to severe hypoperfusion and may be defined in terms of hemodynamic parameters, which according to most studies, means a state in which systolic blood pressure is persistently < 90 mm Hg or < 80 mm Hg, for longer than 1 hour, with adequate or elevated left and right ventricular filling pressures that does not respond to isolated fluid administration, is secondary to cardiac failure and occurs with signs of hypoperfusion (oliguria, cool extremities, cyanosis and altered mental status) or a cardiac index of < 2.2 L/min/m² (on inotropic, vasopressor or circulatory device support) or < 1.8-2.2 L/min/m² (off support) and pulmonary artery wedge pressure > 18 mm Hg.
Differential Diagnosis
Depending on the author and the source used there will be different ways of organizing the types of shock. Sometimes it might be difficult to differentiate, from the clinical standpoint, two types of shock since components of each type may combine in a single patient. The clinical presentation of shock is usually the result of a complexity of processes, such as the sympathetic and endocrine responses to hypoperfusion, along with manifestations of organ failure. Patients who present with signs and symptoms of hypoperfusion following a diagnosed or suspected myocardial infarction, are commonly suffering a cardiogenic shock as a complication of the MI. However, other clinical scenarios, not related to acute MI, may present similarly:[1][2]
-
- More than a simple loss of intravascular volume, hypovolemic shock is a dynamic process in which the responses to the initial insult, and the period of time during which they are in practice, will dictate the response to treatment and therefore the outcome. Several causes may be in the origin of this type of shock, including: hemorrhage, dehydration, GI or urinary losses and severe venodilation (in the setting of other conditions). There is a relationship between the clinical status of the patient and the amount of circulating blood volume, the signs may include pallor, cool extremities, tachycardia and tachypnea, oliguria and decreased consciousness. Compensatory mechanisms are responsible for tolerating initial blood loss, however they begin to fail after about 20-25% of blood has been lost. This tolerance will be dictated mostly by the previous cardiac reserve of the patient, along with the velocity of loss of intravascular volume[3][4].
- When comparing hypovolemic and cardiogenic shock (most commonly complicating acute-MI) some specific clinical signs of shock will be similar, however, others will be different, particularly signs of CHF, such as the presence of distended jugular and peripheral veins, presence of an S3 sound and pulmonary edema on the cardiogenic type.
- When comparing hemodynamic data, similarities include: decreased cardiac index, stroke volume index, cardiac output, mixed venous oxygen saturation and increased difference in arteriovenous O2 saturation and SVR.
Differences to be noted include:
- <math>\mbox{Shock index} = \frac{heart\ rate}{systolic\ blood\ pressure}</math>
Other measures include: decreased ventricular preload, ventricular diastolic volumes and pressures, pulmonary wedge pressure and central venous pressure.
- When treating hypovolemic shock it’s mandatory to rule out cardiogenic cause because part of the treatment for hypovolemic shock, urgent intravascular volume replacement, may further jeopardize the cardiac condition in the cardiogenic form.
-
- This form of shock results from an obstruction to the flow of blood through the cardiovascular system, including the vessels and the heart. Therefore, different causes may give rise to this condition, such as: tension pneumothorax, pulmonary emboli, pericardial tamponade and constrictive pericarditis.[5] As in other types of shock, the clinical response will be heavily dictated by the timespan during which the insult develops and urgent therapy must be applied[6][7].
- To evaluate the hemodynamics of obstructive shock it is important to know the underlying etiology of the shock, since different causes will present with different hemodynamic values. One example of cause of obstructive shock is cardiac tamponade, which, similarly to the cardiogenic form, will likely present with: decreased cardiac index, stroke volume, stroke work, mixed venous oxygen saturation and increased difference in arteriovenous O2 saturation, right and left ventricular diastolic pressures, pulmonary artery diastolic pressure, serum lactate and CVP. Other causes may be observed on the table below.
-
- The hallmark of this form of shock is the decrease of peripheral resistance. This may be present in a series of conditions that may lead to distributive shock, such as: sepsis, anaphylaxis, toxic shock syndrome and adrenal crisis.
- When compared to cardiogenic shock it presents with similarities, such as: decreased cardiac index, left and right ventricular stroke work and increased serum lactate. The differences reside in: overall decreased of SVR, which after fluid resuscitation may become elevated, ventricular filling pressure, difference in arteriovenous O2 saturation and increase of mixed venous oxygen saturation. It is important to note that, unlike cardiogenic and other types of shock, in the distributive kind there is an increase in venous oxygen saturation which, despite the increased O2 demand, might be due to the increased total body perfusion, that is responsible for diminishing the effectiveness of individual tissue perfusion[8][9][10].
| Type of Shock | Etiology | CO | SVR | PCWP | CVP | SVO2 | RVS | RVD | PAS | PAD |
| Cardiogenic | Acute Ventricular Septal Defect | ↓↓ | ↑ | N — ↑ | ↑↑ | ↑ — ↑↑ | N — ↑ | ↑ | N — ↑ | N — ↑ |
| Acute Mitral Regurgitation | ↓↓ | ↑ | ↑↑ | ↑ — ↑↑ | ↓ | ↑ | N — ↑ | ↑ | ↑ | |
| Myocardial Dysfunction | ↓↓ | ↑ | ↑↑ | ↑↑ | ↓ | N — ↑ | N — ↑ | N — ↑ | ↑ | |
| Right Ventricular Infarction | ↓↓ | ↑ | N — ↓ | ↑↑ | ↓ | ↓ — ↑ | ↑ | ↓ — ↑ | ↓ — ↑ | |
| Obstructive | Pulmonary Embolism | ↓↓ | ↑ | N — ↓ | ↑↑ | ↓ | ↓ — ↑ | ↑ | ↓ — ↑ | ↓ — ↑ |
| Cardiac Tamponade | ↓ — ↓↓ | ↑ | ↑↑ | ↑↑ | ↓ | N — ↑ | ↑ | N — ↑ | N — ↑ | |
| Distributive | Septic Shock | N — ↑↑ | ↓ — ↓↓ | N — ↓ | N — ↓ | ↑ — ↑↑ | N — ↓ | N — ↓ | ↓ | ↓ |
| Anaphylactic Shock | N — ↑↑ | ↓ — ↓↓ | N — ↓ | N — ↓ | ↑ — ↑↑ | N — ↓ | N — ↓ | ↓ | ↓ | |
| Hypovolemic | Volume Depletion | ↓↓ | ↑ | ↓↓ | ↓↓ | ↓ | N — ↓ | N — ↓ | ↓ | ↓ |
The following table outlines the major differential diagnoses of Shock on the basis of clinical manifestations..[13][14][15][16][17][18][19][20][21][22][23][24][25][26][27][28][29][30][31][32][33][34][35][36][37][38][39][40][41][42][43][44][45][46][47][48]
Abbreviations: ABG (arterial blood gas); ACE (angiotensin converting enzyme); BMI (body mass index); CBC (complete blood count); CSF (cerebrospinal fluid); CXR (chest X-ray); ECG (electrocardiogram); FEF (forced expiratory flow rate); FEV1 (forced expiratory volume); FVC (forced vital capacity); JVD (jugular vein distention); MCV (mean corpuscular volume); Plt (platelet); RV (residual volume); SIADH (syndrome of inappropriate antidiuretic hormone); TSH (thyroid stimulating hormone); Vt (tidal volume); WBC (white blood cell); Coronary CT angiography (CCTA); multidetector row scanners (MDCT); Cardiovascular magnetic resonance — CMRI; Myocardial perfusion imaging (MPI); single-photon emission CT (SPECT); Positron emission tomography (PET) scanning; Magnetic resonance (MR) angiography, Computed tomographic (CT) angiography, and Transesophageal echocardiography (TEE), late gadolinium enhancement (LGE); right ventricular hypertrophy (RVH), right atrial enlargement (RAE), functional tricuspid regurgitation (TR), Pulmonary artery systolic pressure (PASP; adenosine deaminase (ADA); Serum amyloid A (SAA), soluble interleukin-2 receptor (sIL2R); High-resolution CT (HRCT) scanning
| Differentials on the basis of Etiology | Disease | Clinical manifestations | Diagnosis | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Symptoms | Risk factors | Physical exam | Lab Findings | EKG | Imaging | Gold standard | |||||||||
| Onset | Duration | Quality of Pain | Cough | Fever | Dyspnea | Weight loss | Associated Features | ||||||||
| Myocardial Infarction[13][14][15][16] | Acute | Commonly > 20 minutes |
|
– | – | + | – |
|
|
|
|
| |||
| Cardiac | |||||||||||||||
| Aortic Dissection[49][50] | Sudden severe progressive pain (common) or chronic (rare) | Variable |
|
– | – | + | – |
|
|
|
|
|
| ||
| Aortic intramural hematoma | Sudden severe progressive pain (common) or chronic (rare) | Variable |
|
– | – | + | – |
|
|
|
|
|
| ||
| Penetrating atherosclerotic aortic ulcer[51][52][53] | Sudden severe pain | Variable |
|
– | – | + | – |
|
_ |
_ |
|
| |||
| Pericardial Tamponade[54][55] | Acute or subacute | May last for hours to days |
|
+/- | + | + | – |
|
EKG findings:
|
|
|||||
| Myocarditis[56][57][58] | Acute or subacute | Variable |
|
+/- | + | + | – |
|
|
|
|
||||
| Hypertrophic cardiomyopathy[59][60][61] | Acute or subacute | Variable | Typical or atypical chest pain | – | – | + | – |
|
|
|
Non-specific |
|
|
Genetic testing for HCM | |
| Stress (takotsubo) | Acute | Commonly > 20 minutes |
|
– | – | + | – |
|
Stress |
|
|
|
|||
| Aortic Stenosis[66][67][68] | Acute, recurrent episodes of angina | 2-10 minutes |
|
– | – | + | – |
|
|
|
|
|
|||
| Heart Failure[69][70][71] | Subacute or chronic | Variable |
|
+ | +/- | + | + | Dyslipidemia, hypertension, smoking, family history of premature disease, and diabetes |
|
|
|
||||
| Differentials on the basis of Etiology | Disease | Clinical manifestations | Diagnosis | ||||||||||||
| Symptoms | Risk factors | Physical exam | Lab Findings | EKG | Imaging | Gold standard | |||||||||
| Onset | Duration | Quality of Pain | Cough | Fever | Dyspnea | Weight loss | Associated Features | ||||||||
| Pulmonary | Pulmonary Embolism[72][73] | Acute | May last minutes to hours |
|
+ | +/- | + | – |
|
Hormone replacement therapy
Cancer Oral contraceptive pills Stroke Pregnancy Postpartum Prior history of VTE Thrombophilia |
|
|
|
||
| Spontaneous Pneumothorax[74][75] | Acute | May last minutes to hours |
|
– | – | + | – |
|
|
|
|
|
| ||
| Tension Pneumothorax[76][77] | Acute | May last minutes to hours |
|
– | – | + | – |
|
|
|
|
||||
| Pleural Effusion[78][79][80] | Acute or subacute or chronic | Variable |
|
+ | +/- | + | +/- |
|
|
|
|
||||
| Acute chest syndrome (Sickle cell anemia)[81][82][83] | Acute | May last minutes to hours |
|
+ | +/- | + | – |
|
|
|
|
|
— | ||
| Differentials on the basis of Etiology | Disease | Clinical manifestations | Diagnosis | ||||||||||||
| Symptoms | Risk factors | Physical exam | Lab Findings | EKG | Imaging | Gold standard | |||||||||
| Onset | Duration | Quality of Pain | Cough | Fever | Dyspnea | Weight loss | Associated Features | ||||||||
| Gastrointestinal | Perforated Peptic Ulcer[84][85][86] | Acute |
|
|
+/- | – | – | +/- |
|
|
|
|
|
| |
| Esophagitis[87][88][89] | Acute | Variable |
|
+ | + | – | +/- |
|
|
|
|||||
| Esophageal Perforation[18] | Acute | Minutes to hours |
|
– | +/- | + | – |
|
|
|
|
|
| ||
| Mediastinitis[90][91][92][93] | Acute, Chronic | Variable |
|
+/- | + | + | – |
|
|
|
|
|
|
CT scan | |
| Pancreatitis[94][95][96][97][98] | Acute, Chronic | Variable |
|
– | + | + | +/- |
|
|
|
|
| |||
| IBD[99] | Acute, Chronic | Variable |
|
– | + | + | + |
|
|
|
|
|
|
| |
References
- ↑ Longo, Dan L. (Dan Louis) (2012). Harrison’s principles of internal medici. New York: McGraw-Hill. ISBN 978-0-07-174889-6.
- ↑ Parrillo, Joseph (2013). Critical care medicine principles of diagnosis and management in the adult. Philadelphia, PA: Elsevier/Saunders. ISBN 0323089291.
- ↑ Lier H, Bernhard M, Hossfeld B (March 2018). “[Hypovolemic and hemorrhagic shock]”. Anaesthesist (in German). 67 (3): 225–244. doi:10.1007/s00101-018-0411-z. PMID 29404656.
- ↑ Kobayashi L, Costantini TW, Coimbra R (December 2012). “Hypovolemic shock resuscitation”. Surg. Clin. North Am. 92 (6): 1403–23. doi:10.1016/j.suc.2012.08.006. PMID 23153876.
- ↑ “Shock: Shock and Fluid Resuscitation: Merck Manual Professional”.
- ↑ Pich H, Heller AR (May 2015). “[Obstructive shock]”. Anaesthesist (in German). 64 (5): 403–19. doi:10.1007/s00101-015-0031-9. PMID 25994928.
- ↑ Dababneh E, Siddique MS. PMID 28613734. Missing or empty
|title=(help) - ↑ Smith N, Lopez RA, Silberman M. PMID 29261964. Missing or empty
|title=(help) - ↑ Alyeşil C, Doğan NÖ, Özturan İU, Güney S (June 2017). “Distributive Shock in the Emergency Department: Sepsis, Anaphylaxis, or Capillary Leak Syndrome?”. J Emerg Med. 52 (6): e229–e231. doi:10.1016/j.jemermed.2017.01.012. PMID 28238385.
- ↑ Brown SG (May 2007). “The pathophysiology of shock in anaphylaxis”. Immunol Allergy Clin North Am. 27 (2): 165–75, v. doi:10.1016/j.iac.2007.03.003. PMID 17493496.
- ↑ Parrillo, Joseph E.; Ayres, Stephen M. (1984). Major issues in critical care medicine. Baltimore: William Wilkins. ISBN 0-683-06754-0.
- ↑ Judith S. Hochman, E. Magnus Ohman (2009). Cardiogenic Shock. Wiley-Blackwell. ISBN 9781405179263.
- ↑ 13.0 13.1 Svavarsdóttir AE, Jónasson MR, Gudmundsson GH, Fjeldsted K (June 1996). “Chest pain in family practice. Diagnosis and long-term outcome in a community setting”. Can Fam Physician. 42: 1122–8. PMC 2146490. PMID 8704488.
- ↑ 14.0 14.1 Klinkman MS, Stevens D, Gorenflo DW (April 1994). “Episodes of care for chest pain: a preliminary report from MIRNET. Michigan Research Network”. J Fam Pract. 38 (4): 345–52. PMID 8163958.
- ↑ 15.0 15.1 Bösner S, Becker A, Haasenritter J, Abu Hani M, Keller H, Sönnichsen AC, Karatolios K, Schaefer JR, Seitz G, Baum E, Donner-Banzhoff N (2009). “Chest pain in primary care: epidemiology and pre-work-up probabilities”. Eur J Gen Pract. 15 (3): 141–6. doi:10.3109/13814780903329528. PMID 19883149.
- ↑ 16.0 16.1 Ebell MH (March 2011). “Evaluation of chest pain in primary care patients”. Am Fam Physician. 83 (5): 603–5. PMID 21391528.
- ↑ von Kodolitsch Y, Schwartz AG, Nienaber CA (October 2000). “Clinical prediction of acute aortic dissection”. Arch. Intern. Med. 160 (19): 2977–82. PMID 11041906.
- ↑ 18.0 18.1 Pate JW, Walker WA, Cole FH, Owen EW, Johnson WH (May 1989). “Spontaneous rupture of the esophagus: a 30-year experience”. Ann. Thorac. Surg. 47 (5): 689–92. PMID 2730190.
- ↑ Fleet RP, Dupuis G, Marchand A, Burelle D, Beitman BD (October 1994). “Panic disorder, chest pain and coronary artery disease: literature review”. Can J Cardiol. 10 (8): 827–34. PMID 7954018.
- ↑ Bass C, Chambers JB, Kiff P, Cooper D, Gardner WN (December 1988). “Panic anxiety and hyperventilation in patients with chest pain: a controlled study”. Q. J. Med. 69 (260): 949–59. PMID 3270082.
- ↑ Evans DW, Lum LC (January 1977). “Hyperventilation: An important cause of pseudoangina”. Lancet. 1 (8004): 155–7. PMID 64694.
- ↑ Ros E, Armengol X, Grande L, Toledo-Pimentel V, Lacima G, Sanz G (July 1997). “Chest pain at rest in patients with coronary artery disease. Myocardial ischemia, esophageal dysfunction, or panic disorder?”. Dig. Dis. Sci. 42 (7): 1344–53. PMID 9246027.
- ↑ Ben Freedman S, Tennant CC (April 1998). “Panic disorder and coronary artery spasm”. Med. J. Aust. 168 (8): 376–7. PMID 9594945.
- ↑ Smoller JW, Pollack MH, Wassertheil-Smoller S, Jackson RD, Oberman A, Wong ND, Sheps D (October 2007). “Panic attacks and risk of incident cardiovascular events among postmenopausal women in the Women’s Health Initiative Observational Study”. Arch. Gen. Psychiatry. 64 (10): 1153–60. doi:10.1001/archpsyc.64.10.1153. PMID 17909127.
- ↑ Mehta NJ, Khan IA (November 2002). “Cardiac Munchausen syndrome”. Chest. 122 (5): 1649–53. PMID 12426266.
- ↑ Swap CJ, Nagurney JT (November 2005). “Value and limitations of chest pain history in the evaluation of patients with suspected acute coronary syndromes”. JAMA. 294 (20): 2623–9. doi:10.1001/jama.294.20.2623. PMID 16304077.
- ↑ Marcus GM, Cohen J, Varosy PD, Vessey J, Rose E, Massie BM, Chatterjee K, Waters D (January 2007). “The utility of gestures in patients with chest discomfort”. Am. J. Med. 120 (1): 83–9. doi:10.1016/j.amjmed.2006.05.045. PMID 17208083.
- ↑ Verdon F, Burnand B, Herzig L, Junod M, Pécoud A, Favrat B (September 2007). “Chest wall syndrome among primary care patients: a cohort study”. BMC Fam Pract. 8: 51. doi:10.1186/1471-2296-8-51. PMC 2072948. PMID 17850647.
- ↑ Davies HA, Jones DB, Rhodes J, Newcombe RG (December 1985). “Angina-like esophageal pain: differentiation from cardiac pain by history”. J. Clin. Gastroenterol. 7 (6): 477–81. PMID 4086742.
- ↑ Panju AA, Hemmelgarn BR, Guyatt GH, Simel DL (October 1998). “The rational clinical examination. Is this patient having a myocardial infarction?”. JAMA. 280 (14): 1256–63. PMID 9786377.
- ↑ Berger JP, Buclin T, Haller E, Van Melle G, Yersin B (March 1990). “Right arm involvement and pain extension can help to differentiate coronary diseases from chest pain of other origin: a prospective emergency ward study of 278 consecutive patients admitted for chest pain”. J. Intern. Med. 227 (3): 165–72. PMID 2313224.
- ↑ Yelland MJ (September 2001). “Back, chest and abdominal pain. How good are spinal signs at identifying musculoskeletal causes of back, chest or abdominal pain?”. Aust Fam Physician. 30 (9): 908–12. PMID 11676323.
- ↑ Chan S, Maurice AP, Davies SR, Walters DL (October 2014). “The use of gastrointestinal cocktail for differentiating gastro-oesophageal reflux disease and acute coronary syndrome in the emergency setting: a systematic review”. Heart Lung Circ. 23 (10): 913–23. doi:10.1016/j.hlc.2014.03.030. PMID 24791662.
- ↑ Henrikson CA, Howell EE, Bush DE, Miles JS, Meininger GR, Friedlander T, Bushnell AC, Chandra-Strobos N (December 2003). “Chest pain relief by nitroglycerin does not predict active coronary artery disease”. Ann. Intern. Med. 139 (12): 979–86. PMID 14678917.
- ↑ Pryor DB, Harrell FE, Lee KL, Califf RM, Rosati RA (November 1983). “Estimating the likelihood of significant coronary artery disease”. Am. J. Med. 75 (5): 771–80. PMID 6638047.
- ↑ Buntinx F, Knockaert D, Bruyninckx R, de Blaey N, Aerts M, Knottnerus JA, Delooz H (December 2001). “Chest pain in general practice or in the hospital emergency department: is it the same?”. Fam Pract. 18 (6): 586–9. PMID 11739341.
- ↑ Tierney WM, Roth BJ, Psaty B, McHenry R, Fitzgerald J, Stump DL, Anderson FK, Ryder KW, McDonald CJ, Smith DM (July 1985). “Predictors of myocardial infarction in emergency room patients”. Crit. Care Med. 13 (7): 526–31. PMID 4006491.
- ↑ Sequist TD, Marshall R, Lampert S, Buechler EJ, Lee TH (November 2006). “Missed opportunities in the primary care management of early acute ischemic heart disease”. Arch. Intern. Med. 166 (20): 2237–43. doi:10.1001/archinte.166.20.2237. PMID 17101942.
- ↑ Norell M, Lythall D, Coghlan G, Cheng A, Kushwaha S, Swan J, Ilsley C, Mitchell A (January 1992). “Limited value of the resting electrocardiogram in assessing patients with recent onset chest pain: lessons from a chest pain clinic”. Br Heart J. 67 (1): 53–6. PMC 1024701. PMID 1739527.
- ↑ Law K, Elley R, Tietjens J, Mann S (July 2006). “Troponin testing for chest pain in primary healthcare: a survey of its use by general practitioners in New Zealand”. N. Z. Med. J. 119 (1238): U2082. PMID 16868579.
- ↑ Wilhelmsen L, Rosengren A, Hagman M, Lappas G (July 1998). ““Nonspecific” chest pain associated with high long-term mortality: results from the primary prevention study in Göteborg, Sweden”. Clin Cardiol. 21 (7): 477–82. PMID 9669056.
- ↑ Ruigómez A, Rodríguez LA, Wallander MA, Johansson S, Jones R (April 2006). “Chest pain in general practice: incidence, comorbidity and mortality”. Fam Pract. 23 (2): 167–74. doi:10.1093/fampra/cmi124. PMID 16461444.
- ↑ Robinson JG, Wallace R, Limacher M, Sato A, Cochrane B, Wassertheil-Smoller S, Ockene JK, Blanchette PL, Ko MG (December 2006). “Elderly women diagnosed with nonspecific chest pain may be at increased cardiovascular risk”. J Womens Health (Larchmt). 15 (10): 1151–60. doi:10.1089/jwh.2006.15.1151. PMID 17199456.
- ↑ Geraldine McMahon C, Yates DW, Hollis S (February 2008). “Unexpected mortality in patients discharged from the emergency department following an episode of nontraumatic chest pain”. Eur J Emerg Med. 15 (1): 3–8. doi:10.1097/MEJ.0b013e32827b14cd. PMID 18180659.
- ↑ Yelland M, Cayley WE, Vach W (March 2010). “An algorithm for the diagnosis and management of chest pain in primary care”. Med. Clin. North Am. 94 (2): 349–74. doi:10.1016/j.mcna.2010.01.011. PMID 20380960.
- ↑ Wang WH, Huang JQ, Zheng GF, Wong WM, Lam SK, Karlberg J, Xia HH, Fass R, Wong BC (June 2005). “Is proton pump inhibitor testing an effective approach to diagnose gastroesophageal reflux disease in patients with noncardiac chest pain?: a meta-analysis”. Arch. Intern. Med. 165 (11): 1222–8. doi:10.1001/archinte.165.11.1222. PMID 15956000.
- ↑ Borzecki AM, Pedrosa MC, Prashker MJ (March 2000). “Should noncardiac chest pain be treated empirically? A cost-effectiveness analysis”. Arch. Intern. Med. 160 (6): 844–52. PMID 10737285.
- ↑ Wertli MM, Ruchti KB, Steurer J, Held U (November 2013). “Diagnostic indicators of non-cardiovascular chest pain: a systematic review and meta-analysis”. BMC Med. 11: 239. doi:10.1186/1741-7015-11-239. PMC 4226211. PMID 24207111.
- ↑ Takagi H, Ando T, Umemoto T (November 2017). “Meta-Analysis of Circadian Variation in the Onset of Acute Aortic Dissection”. Am. J. Cardiol. 120 (9): 1662–1666. doi:10.1016/j.amjcard.2017.07.067. PMID 28847596.
- ↑ Kojima S, Sumiyoshi M, Nakata Y, Daida H (March 2002). “Triggers and circadian distribution of the onset of acute aortic dissection”. Circ. J. 66 (3): 232–5. PMID 11922269.
- ↑ Eggebrecht, Holger; Baumgart, Dietrich; Schmermund, Axel; Herold, Ulf; Hunold, Peter; Jakob, Heinz; Erbel, Raimund (2003). “Penetrating atherosclerotic ulcer of the aorta: treatment by endovascular stent-graft placement”. Current Opinion in Cardiology. 18 (6): 431–435. doi:10.1097/00001573-200311000-00002. ISSN 0268-4705.
- ↑ Bossone, Eduardo; LaBounty, Troy M; Eagle, Kim A (2018). “Acute aortic syndromes: diagnosis and management, an update”. European Heart Journal. 39 (9): 739–749d. doi:10.1093/eurheartj/ehx319. ISSN 0195-668X.
- ↑ DeMartino, Randall R.; Sen, Indrani; Huang, Ying; Bower, Thomas C.; Oderich, Gustavo S.; Pochettino, Alberto; Greason, Kevin; Kalra, Manju; Johnstone, Jill; Shuja, Fahad; Harmsen, W. Scott; Macedo, Thanila; Mandrekar, Jay; Chamberlain, Alanna M.; Weiss, Salome; Goodney, Philip P.; Roger, Veronique (2018). “Population-Based Assessment of the Incidence of Aortic Dissection, Intramural Hematoma, and Penetrating Ulcer, and Its Associated Mortality From 1995 to 2015”. Circulation: Cardiovascular Quality and Outcomes. 11 (8). doi:10.1161/CIRCOUTCOMES.118.004689. ISSN 1941-7713.
- ↑ Ewart W (March 1896). “Practical Aids in the Diagnosis of Pericardial Effusion, in Connection with the Question as to Surgical Treatment”. Br Med J. 1 (1838): 717–21. PMC 2406464. PMID 20756103.
- ↑ Adler Y, Charron P, Imazio M, Badano L, Barón-Esquivias G, Bogaert J, Brucato A, Gueret P, Klingel K, Lionis C, Maisch B, Mayosi B, Pavie A, Ristić AD, Sabaté Tenas M, Seferovic P, Swedberg K, Tomkowski W, Achenbach S, Agewall S, Al-Attar N, Angel Ferrer J, Arad M, Asteggiano R, Bueno H, Caforio AL, Carerj S, Ceconi C, Evangelista A, Flachskampf F, Giannakoulas G, Gielen S, Habib G, Kolh P, Lambrinou E, Lancellotti P, Lazaros G, Linhart A, Meurin P, Nieman K, Piepoli MF, Price S, Roos-Hesselink J, Roubille F, Ruschitzka F, Sagristà Sauleda J, Sousa-Uva M, Uwe Voigt J, Luis Zamorano J (November 2015). “2015 ESC Guidelines for the diagnosis and management of pericardial diseases: The Task Force for the Diagnosis and Management of Pericardial Diseases of the European Society of Cardiology (ESC)Endorsed by: The European Association for Cardio-Thoracic Surgery (EACTS)”. Eur. Heart J. 36 (42): 2921–64. doi:10.1093/eurheartj/ehv318. PMID 26320112.
- ↑ Dec GW, Palacios IF, Fallon JT, Aretz HT, Mills J, Lee DC, Johnson RA (April 1985). “Active myocarditis in the spectrum of acute dilated cardiomyopathies. Clinical features, histologic correlates, and clinical outcome”. N. Engl. J. Med. 312 (14): 885–90. doi:10.1056/NEJM198504043121404. PMID 3974674.
- ↑ Caforio AL, Calabrese F, Angelini A, Tona F, Vinci A, Bottaro S, Ramondo A, Carturan E, Iliceto S, Thiene G, Daliento L (June 2007). “A prospective study of biopsy-proven myocarditis: prognostic relevance of clinical and aetiopathogenetic features at diagnosis”. Eur. Heart J. 28 (11): 1326–33. doi:10.1093/eurheartj/ehm076. PMID 17493945.
- ↑ Ukena C, Mahfoud F, Kindermann I, Kandolf R, Kindermann M, Böhm M (April 2011). “Prognostic electrocardiographic parameters in patients with suspected myocarditis”. Eur. J. Heart Fail. 13 (4): 398–405. doi:10.1093/eurjhf/hfq229. PMID 21239404.
- ↑ Elliott PM, Kaski JC, Prasad K, Seo H, Slade AK, Goldman JH, McKenna WJ (July 1996). “Chest pain during daily life in patients with hypertrophic cardiomyopathy: an ambulatory electrocardiographic study”. Eur. Heart J. 17 (7): 1056–64. PMID 8809524.
- ↑ Pasternac A, Noble J, Streulens Y, Elie R, Henschke C, Bourassa MG (April 1982). “Pathophysiology of chest pain in patients with cardiomyopathies and normal coronary arteries”. Circulation. 65 (4): 778–89. PMID 7199403.
- ↑ Webb JG, Sasson Z, Rakowski H, Liu P, Wigle ED (January 1990). “Apical hypertrophic cardiomyopathy: clinical follow-up and diagnostic correlates”. J. Am. Coll. Cardiol. 15 (1): 83–90. PMID 2295747.
- ↑ Sharkey SW, Lesser JR, Zenovich AG, Maron MS, Lindberg J, Longe TF, Maron BJ (February 2005). “Acute and reversible cardiomyopathy provoked by stress in women from the United States”. Circulation. 111 (4): 472–9. doi:10.1161/01.CIR.0000153801.51470.EB. PMID 15687136.
- ↑ Krishnamoorthy P, Garg J, Sharma A, Palaniswamy C, Shah N, Lanier G, Patel NC, Lavie CJ, Ahmad H (July 2015). “Gender Differences and Predictors of Mortality in Takotsubo Cardiomyopathy: Analysis from the National Inpatient Sample 2009-2010 Database”. Cardiology. 132 (2): 131–136. doi:10.1159/000430782. PMID 26159108.
- ↑ Templin C, Ghadri JR, Diekmann J, Napp LC, Bataiosu DR, Jaguszewski M, Cammann VL, Sarcon A, Geyer V, Neumann CA, Seifert B, Hellermann J, Schwyzer M, Eisenhardt K, Jenewein J, Franke J, Katus HA, Burgdorf C, Schunkert H, Moeller C, Thiele H, Bauersachs J, Tschöpe C, Schultheiss HP, Laney CA, Rajan L, Michels G, Pfister R, Ukena C, Böhm M, Erbel R, Cuneo A, Kuck KH, Jacobshagen C, Hasenfuss G, Karakas M, Koenig W, Rottbauer W, Said SM, Braun-Dullaeus RC, Cuculi F, Banning A, Fischer TA, Vasankari T, Airaksinen KE, Fijalkowski M, Rynkiewicz A, Pawlak M, Opolski G, Dworakowski R, MacCarthy P, Kaiser C, Osswald S, Galiuto L, Crea F, Dichtl W, Franz WM, Empen K, Felix SB, Delmas C, Lairez O, Erne P, Bax JJ, Ford I, Ruschitzka F, Prasad A, Lüscher TF (September 2015). “Clinical Features and Outcomes of Takotsubo (Stress) Cardiomyopathy”. N. Engl. J. Med. 373 (10): 929–38. doi:10.1056/NEJMoa1406761. PMID 26332547.
- ↑ Bybee KA, Kara T, Prasad A, Lerman A, Barsness GW, Wright RS, Rihal CS (December 2004). “Systematic review: transient left ventricular apical ballooning: a syndrome that mimics ST-segment elevation myocardial infarction”. Ann. Intern. Med. 141 (11): 858–65. PMID 15583228.
- ↑ Green SJ, Pizzarello RA, Padmanabhan VT, Ong LY, Hall MH, Tortolani AJ (April 1985). “Relation of angina pectoris to coronary artery disease in aortic valve stenosis”. Am. J. Cardiol. 55 (8): 1063–5. PMID 3984868.
- ↑ Silaruks S, Clark D, Thinkhamrop B, Sia B, Buxton B, Tonkin A (2001). “Angina pectoris and coronary artery disease in severe isolated valvular aortic stenosis”. Heart Lung Circ. 10 (1): 14–23. doi:10.1046/j.1444-2892.2001.00060.x. PMID 16352020.
- ↑ Munt B, Legget ME, Kraft CD, Miyake-Hull CY, Fujioka M, Otto CM (February 1999). “Physical examination in valvular aortic stenosis: correlation with stenosis severity and prediction of clinical outcome”. Am. Heart J. 137 (2): 298–306. doi:10.1053/hj.1999.v137.95496. PMID 9924164.
- ↑ Anker SD, Sharma R (September 2002). “The syndrome of cardiac cachexia”. Int. J. Cardiol. 85 (1): 51–66. PMID 12163209.
- ↑ Horwich TB, Kalantar-Zadeh K, MacLellan RW, Fonarow GC (May 2008). “Albumin levels predict survival in patients with systolic heart failure”. Am. Heart J. 155 (5): 883–9. doi:10.1016/j.ahj.2007.11.043. PMID 18440336.
- ↑ Breathett K, Allen LA, Udelson J, Davis G, Bristow M (October 2016). “Changes in Left Ventricular Ejection Fraction Predict Survival and Hospitalization in Heart Failure With Reduced Ejection Fraction”. Circ Heart Fail. 9 (10). doi:10.1161/CIRCHEARTFAILURE.115.002962. PMC 5082710. PMID 27656000.
- ↑ Stein PD, Beemath A, Matta F, Weg JG, Yusen RD, Hales CA, Hull RD, Leeper KV, Sostman HD, Tapson VF, Buckley JD, Gottschalk A, Goodman LR, Wakefied TW, Woodard PK (October 2007). “Clinical characteristics of patients with acute pulmonary embolism: data from PIOPED II”. Am. J. Med. 120 (10): 871–9. doi:10.1016/j.amjmed.2007.03.024. PMC 2071924. PMID 17904458.
- ↑ “Value of the ventilation/perfusion scan in acute pulmonary embolism. Results of the prospective investigation of pulmonary embolism diagnosis (PIOPED)”. JAMA. 263 (20): 2753–9. 1990. PMID 2332918.
- ↑ Bense L, Wiman LG, Hedenstierna G (September 1987). “Onset of symptoms in spontaneous pneumothorax: correlations to physical activity”. Eur J Respir Dis. 71 (3): 181–6. PMID 3678419.
- ↑ Seow A, Kazerooni EA, Pernicano PG, Neary M (February 1996). “Comparison of upright inspiratory and expiratory chest radiographs for detecting pneumothoraces”. AJR Am J Roentgenol. 166 (2): 313–6. doi:10.2214/ajr.166.2.8553937. PMID 8553937.
- ↑ Stark P, Leung A (1996). “Effects of lobar atelectasis on the distribution of pleural effusion and pneumothorax”. J Thorac Imaging. 11 (2): 145–9. PMID 8820023.
- ↑ Jalli R, Sefidbakht S, Jafari SH (April 2013). “Value of ultrasound in diagnosis of pneumothorax: a prospective study”. Emerg Radiol. 20 (2): 131–4. doi:10.1007/s10140-012-1091-7. PMID 23179505.
- ↑ Feinsilver SH, Barrows AA, Braman SS (October 1986). “Fiberoptic bronchoscopy and pleural effusion of unknown origin”. Chest. 90 (4): 516–9. PMID 3757561.
- ↑ Collins TR, Sahn SA (June 1987). “Thoracocentesis. Clinical value, complications, technical problems, and patient experience”. Chest. 91 (6): 817–22. PMID 3581930.
- ↑ Venekamp LN, Velkeniers B, Noppen M (2005). “Does ‘idiopathic pleuritis’ exist? Natural history of non-specific pleuritis diagnosed after thoracoscopy”. Respiration. 72 (1): 74–8. doi:10.1159/000083404. PMID 15753638.
- ↑ Vichinsky EP, Styles LA, Colangelo LH, Wright EC, Castro O, Nickerson B (March 1997). “Acute chest syndrome in sickle cell disease: clinical presentation and course. Cooperative Study of Sickle Cell Disease”. Blood. 89 (5): 1787–92. PMID 9057664.
- ↑ Castro O, Brambilla DJ, Thorington B, Reindorf CA, Scott RB, Gillette P, Vera JC, Levy PS (July 1994). “The acute chest syndrome in sickle cell disease: incidence and risk factors. The Cooperative Study of Sickle Cell Disease”. Blood. 84 (2): 643–9. PMID 7517723.
- ↑ Vichinsky EP, Neumayr LD, Earles AN, Williams R, Lennette ET, Dean D, Nickerson B, Orringer E, McKie V, Bellevue R, Daeschner C, Manci EA (June 2000). “Causes and outcomes of the acute chest syndrome in sickle cell disease. National Acute Chest Syndrome Study Group”. N. Engl. J. Med. 342 (25): 1855–65. doi:10.1056/NEJM200006223422502. PMID 10861320.
- ↑ Vakil N, van Zanten SV, Kahrilas P, Dent J, Jones R (August 2006). “The Montreal definition and classification of gastroesophageal reflux disease: a global evidence-based consensus”. Am. J. Gastroenterol. 101 (8): 1900–20, quiz 1943. doi:10.1111/j.1572-0241.2006.00630.x. PMID 16928254.
- ↑ Vakil NB, Traxler B, Levine D (August 2004). “Dysphagia in patients with erosive esophagitis: prevalence, severity, and response to proton pump inhibitor treatment”. Clin. Gastroenterol. Hepatol. 2 (8): 665–8. PMID 15290658.
- ↑ Giannini EG, Zentilin P, Dulbecco P, Vigneri S, Scarlata P, Savarino V (February 2008). “Management strategy for patients with gastroesophageal reflux disease: a comparison between empirical treatment with esomeprazole and endoscopy-oriented treatment”. Am. J. Gastroenterol. 103 (2): 267–75. doi:10.1111/j.1572-0241.2007.01659.x. PMID 18289194.
- ↑ Bott S, Prakash C, McCallum RW (August 1987). “Medication-induced esophageal injury: survey of the literature”. Am. J. Gastroenterol. 82 (8): 758–63. PMID 3605035.
- ↑ Parfitt JR, Jayakumar S, Driman DK (September 2008). “Mycophenolate mofetil-related gastrointestinal mucosal injury: variable injury patterns, including graft-versus-host disease-like changes”. Am. J. Surg. Pathol. 32 (9): 1367–72. PMID 18763324.
- ↑ Jaspersen D (March 2000). “Drug-induced oesophageal disorders: pathogenesis, incidence, prevention and management”. Drug Saf. 22 (3): 237–49. PMID 10738847.
- ↑ Loyd JE, Tillman BF, Atkinson JB, Des Prez RM (September 1988). “Mediastinal fibrosis complicating histoplasmosis”. Medicine (Baltimore). 67 (5): 295–310. PMID 3045478.
- ↑ Feigin DS, Eggleston JC, Siegelman SS (January 1979). “The multiple roentgen manifestations of sclerosing mediastinitis”. Johns Hopkins Med J. 144 (1): 1–8. PMID 762913.
- ↑ Garrett HE, Roper CL (December 1986). “Surgical intervention in histoplasmosis”. Ann. Thorac. Surg. 42 (6): 711–22. PMID 3539049.
- ↑ Sherrick AD, Brown LR, Harms GF, Myers JL (August 1994). “The radiographic findings of fibrosing mediastinitis”. Chest. 106 (2): 484–9. PMID 7774324.
- ↑ Dickson AP, Imrie CW (October 1984). “The incidence and prognosis of body wall ecchymosis in acute pancreatitis”. Surg Gynecol Obstet. 159 (4): 343–7. PMID 6237447.
- ↑ Yadav D, Agarwal N, Pitchumoni CS (June 2002). “A critical evaluation of laboratory tests in acute pancreatitis”. Am. J. Gastroenterol. 97 (6): 1309–18. doi:10.1111/j.1572-0241.2002.05766.x. PMID 12094843.
- ↑ Fortson MR, Freedman SN, Webster PD (December 1995). “Clinical assessment of hyperlipidemic pancreatitis”. Am. J. Gastroenterol. 90 (12): 2134–9. PMID 8540502.
- ↑ Lecesne R, Taourel P, Bret PM, Atri M, Reinhold C (June 1999). “Acute pancreatitis: interobserver agreement and correlation of CT and MR cholangiopancreatography with outcome”. Radiology. 211 (3): 727–35. doi:10.1148/radiology.211.3.r99jn08727. PMID 10352598.
- ↑ Stimac D, Miletić D, Radić M, Krznarić I, Mazur-Grbac M, Perković D, Milić S, Golubović V (May 2007). “The role of nonenhanced magnetic resonance imaging in the early assessment of acute pancreatitis”. Am. J. Gastroenterol. 102 (5): 997–1004. doi:10.1111/j.1572-0241.2007.01164.x. PMID 17378903.
- ↑ Colbert, James F.; Schmidt, Eric P.; Faubel, Sarah; Ginde, Adit A. (2017). “Severe Sepsis Outcomes Among Hospitalizations With Inflammatory Bowel Disease”. SHOCK. 47 (2): 128–131. doi:10.1097/SHK.0000000000000742. ISSN 1073-2322.
Epidemiology and Demographics
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: João André Alves Silva, M.D. [2] Syed Musadiq Ali M.B.B.S.[3]
Overview
In defiance of the historic numbers of mortality from cardiogenic shock of 80% to 90%, in the modern era, this type of shock comprises a mortality risk of around 50%, in the face of the diagnostic and treatment techniques, which have greatly been developed in recent years. Depending on the demographic and clinical factors, this risk can range from 10% to 80%. The incidence of cardiogenic shock among patients with acute MI is approximately 5% to 10%. Because atherosclerosis and myocardial infarction are both more frequent among males, cardiogenic shock is more common in this gender. However, because women tend to present with acute myocardial infarction at a later age, along with the fact that they have a greater chance of having multivessel coronary artery disease when they first develop symptoms, a greater proportion of women with acute MI develop cardiogenic shock.
Epidemiology and Demographics
Incidence
- Higher incidence of CS are observed in women, Asian/Pacific Islanders, and patients aged >75 years[1].
- The incidence of CS has increased in recent years, while the reason for increasing incidence is unclear, improved diagnosis and better access to care are both likely contributory.
- The in‐hospital mortality has improved[2].
- The 6‐ to 12‐month mortality in cardiogenic shock has remained unchanged at ≈50% over the past 2 decades[3].
- Survivors of MI‐associated CS have an 18.6% risk of 30‐day readmission after discharge, with a median time of 10 days.
- The risk of readmission is slightly lower among patients with STEMI versus NSTEMI. The most common causes of readmission are congestive heart failure and new myocardial infarction.
Prevalence
- prevalence of CS between 1997 and 2012, was 600 per 100,000. Over the 15‐year study period, the prevalence of CS increased to 700 per 100,000.
- Female sex, low socioeconomic status, mechanical circulatory support (MCS) device placement, atrial fibrillation, and ventricular tachycardia are predictors of readmission[4].
- With the improvements made in the time for diagnosis and therapeutic measures offered for acute myocardial infarction, in which increasing rates of use of primary PCI in recent years have a major role, the once very stable incidence of cardiogenic shock in this group of patients is finally declining.[5]
- Cardiogenic shock is still an important complication in 5-8% of patients presenting with ST elevation myocardial infarction[6][7] and 2.5% of those with non ST elevation myocardial infarction.[8][9]
- The high incidence of left ventricular dysfunction following myocardial infarction, cardiogenic shock due to right ventricle failure (incidence of 2.8%) has as high mortality risk as shock following left ventricle failure.[10]
- According to the SHOCK registry, both groups of patients benefit equally from revascularization procedures.[11]
Age
- Multicentre hospital‐based registries and surveys in the USA and Europe have shown the typical patient with CS to be >70 years of age.
- CS patients to the ICU has increased over time in patients aged ≤65 years (from 44% to 51%), but remained relatively unchanged above this age (from 52% to 51%).
- Also according to this registry, the 3 and 6 year survival rates of the group who underwent early revascularization were 41.4% and 32.8% respectively.[12]
Race
- There is no racial predilection to CS.
Sex
- Female sex, although initially classified as an independent predictor of outcome,[13] studies have revealed that this assumption wasn’t true.[14][15][16]
Cardiogenic shock has shown to have greater incidence and mortality rate in certain classes of patients:
- The time course evaluated by the GUSTO-I trial showed that, of the 41.000 patients with acute MI treated with fibrinolytic therapy, 0.8% were in shock on admission, an additional 5.3% developed shock after admission as a sudden event or as a gradual fall in blood pressure, and approximately 50% of the patients who developed shock after admission.[17]
- The increase in the use of primary PCI, as the main reperfusion strategy for MI, over thrombolysis, has also contributed to the decrease in the incidence of CHF.[18][19] Back in the prereperfusion era, the 30-day mortality for acute MI complicated by cardiogenic shock was about 80%. This number went down to 58%, according to the GUSTO I registry, in patients who were treated with thrombolysis.[20]
- Recently, improvements in mortality have been shown and confirmed, as by the GRACE registry, which studied a group of patients from 1999 to 2006, and that demonstrated a 24% decline in cardiogenic shock complicating acute MI, with the use of PCI reperfusion.[21]
References
- ↑ Kolte D, Khera S, Aronow WS, Mujib M, Palaniswamy C, Sule S, Jain D, Gotsis W, Ahmed A, Frishman WH, Fonarow GC (January 2014). “Trends in incidence, management, and outcomes of cardiogenic shock complicating ST-elevation myocardial infarction in the United States”. J Am Heart Assoc. 3 (1): e000590. doi:10.1161/JAHA.113.000590. PMC 3959706. PMID 24419737.
- ↑ “Contemporary Management of Cardiogenic Shock: A Scientific Statement From the American Heart Association | Circulation”.
- ↑ 3.0 3.1 Hochman JS, Sleeper LA, Webb JG, Sanborn TA, White HD, Talley JD, Buller CE, Jacobs AK, Slater JN, Col J, McKinlay SM, LeJemtel TH (August 1999). “Early revascularization in acute myocardial infarction complicated by cardiogenic shock. SHOCK Investigators. Should We Emergently Revascularize Occluded Coronaries for Cardiogenic Shock”. N. Engl. J. Med. 341 (9): 625–34. doi:10.1056/NEJM199908263410901. PMID 10460813.
- ↑ “Prevalence, Causes, and Predictors of 30‐Day Readmissions Following Hospitalization With Acute Myocardial Infarction Complicated By Cardiogenic Shock: Findings From the 2013–2014 National Readmissions Database | Journal of the American Heart Association”.
- ↑ Hasdai, David. (2002). Cardiogenic shock : diagnosis and treatmen. Totowa, N.J.: Humana Press. ISBN 1-58829-025-5.
- ↑ Fox KA, Anderson FA, Dabbous OH, Steg PG, López-Sendón J, Van de Werf F; et al. (2007). “Intervention in acute coronary syndromes: do patients undergo intervention on the basis of their risk characteristics? The Global Registry of Acute Coronary Events (GRACE)”. Heart. 93 (2): 177–82. doi:10.1136/hrt.2005.084830. PMC 1861403. PMID 16757543.
- ↑ Babaev A, Frederick PD, Pasta DJ, Every N, Sichrovsky T, Hochman JS; et al. (2005). “Trends in management and outcomes of patients with acute myocardial infarction complicated by cardiogenic shock”. JAMA. 294 (4): 448–54. doi:10.1001/jama.294.4.448. PMID 16046651.
- ↑ 8.0 8.1 Hasdai D, Harrington RA, Hochman JS, Califf RM, Battler A, Box JW; et al. (2000). “Platelet glycoprotein IIb/IIIa blockade and outcome of cardiogenic shock complicating acute coronary syndromes without persistent ST-segment elevation”. J Am Coll Cardiol. 36 (3): 685–92. PMID 10987585.
- ↑ Thom T, Haase N, Rosamond W, Howard VJ, Rumsfeld J, Manolio T; et al. (2006). “Heart disease and stroke statistics–2006 update: a report from the American Heart Association Statistics Committee and Stroke Statistics Subcommittee”. Circulation. 113 (6): e85–151. doi:10.1161/CIRCULATIONAHA.105.171600. PMID 16407573.
- ↑ Jacobs AK, Leopold JA, Bates E, Mendes LA, Sleeper LA, White H; et al. (2003). “Cardiogenic shock caused by right ventricular infarction: a report from the SHOCK registry”. J Am Coll Cardiol. 41 (8): 1273–9. PMID 12706920.
- ↑ Hochman, Judith S; Buller, Christopher E; Sleeper, Lynn A; Boland, Jean; Dzavik, Vladimir; Sanborn, Timothy A; Godfrey, Emilie; White, Harvey D; Lim, John; LeJemtel, Thierry (2000). “Cardiogenic shock complicating acute myocardial infarction—etiologies, management and outcome: a report from the SHOCK Trial Registry”. Journal of the American College of Cardiology. 36 (3): 1063–1070. doi:10.1016/S0735-1097(00)00879-2. ISSN 0735-1097.
- ↑ Hochman JS, Sleeper LA, Webb JG, Dzavik V, Buller CE, Aylward P; et al. (2006). “Early revascularization and long-term survival in cardiogenic shock complicating acute myocardial infarction”. JAMA. 295 (21): 2511–5. doi:10.1001/jama.295.21.2511. PMC 1782030. PMID 16757723. [http://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi? dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=17080971 Review in: ACP J Club. 2006 Nov-Dec;145(3):59]
- ↑ Klein LW, Shaw RE, Krone RJ, Brindis RG, Anderson HV, Block PC; et al. (2005). “Mortality after emergent percutaneous coronary intervention in cardiogenic shock secondary to acute myocardial infarction and usefulness of a mortality prediction model”. Am J Cardiol. 96 (1): 35–41. doi:10.1016/j.amjcard.2005.02.040. PMID 15979429.
- ↑ 14.0 14.1 Zeymer U, Vogt A, Zahn R, Weber MA, Tebbe U, Gottwik M; et al. (2004). “Predictors of in-hospital mortality in 1333 patients with acute myocardial infarction complicated by cardiogenic shock treated with primary percutaneous coronary intervention (PCI); Results of the primary PCI registry of the Arbeitsgemeinschaft Leitende Kardiologische Krankenhausärzte (ALKK)”. Eur Heart J. 25 (4): 322–8. doi:10.1016/j.ehj.2003.12.008. PMID 14984921.
- ↑ Wong SC, Sleeper LA, Monrad ES, Menegus MA, Palazzo A, Dzavik V; et al. (2001). “Absence of gender differences in clinical outcomes in patients with cardiogenic shock complicating acute myocardial infarction. A report from the SHOCK Trial Registry”. J Am Coll Cardiol. 38 (5): 1395–401. PMID 11691514.
- ↑ Antoniucci D, Migliorini A, Moschi G, Valenti R, Trapani M, Parodi G; et al. (2003). “Does gender affect the clinical outcome of patients with acute myocardial infarction complicated by cardiogenic shock who undergo percutaneous coronary intervention?”. Catheter Cardiovasc Interv. 59 (4): 423–8. doi:10.1002/ccd.10573. PMID 12891599.
- ↑ Holmes DR, Bates ER, Kleiman NS, Sadowski Z, Horgan JH, Morris DC; et al. (1995). “Contemporary reperfusion therapy for cardiogenic shock: the GUSTO-I trial experience. The GUSTO-I Investigators. Global Utilization of Streptokinase and Tissue Plasminogen Activator for Occluded Coronary Arteries”. J Am Coll Cardiol. 26 (3): 668–74. PMID 7642857.
- ↑ Goldberg, R. J.; Spencer, F. A.; Gore, J. M.; Lessard, D.; Yarzebski, J. (2009). “Thirty-Year Trends (1975 to 2005) in the Magnitude of, Management of, and Hospital Death Rates Associated With Cardiogenic Shock in Patients With Acute Myocardial Infarction: A Population-Based Perspective”. Circulation. 119 (9): 1211–1219. doi:10.1161/CIRCULATIONAHA.108.814947. ISSN 0009-7322.
- ↑ Giglioli C, Margheri M, Valente S, Comeglio M, Lazzeri C, Chechi T; et al. (2006). “Timing, setting and incidence of cardiovascular complications in patients with acute myocardial infarction submitted to primary percutaneous coronary intervention”. Can J Cardiol. 22 (12): 1047–52. PMC 2568965. PMID 17036099.
- ↑ Topol, Eric (2007). Textbook of cardiovascular medicine. Philadelphia: Lippincott Williams & Wilkins. ISBN 0781770122.
- ↑ Fox KA, Steg PG, Eagle KA, Goodman SG, Anderson FA, Granger CB; et al. (2007). “Decline in rates of death and heart failure in acute coronary syndromes, 1999-2006”. JAMA. 297 (17): 1892–900. doi:10.1001/jama.297.17.1892. PMID 17473299.
- ↑ Hasdai D, Holmes DR, Califf RM, Thompson TD, Hochman JS, Pfisterer M; et al. (1999). “Cardiogenic shock complicating acute myocardial infarction: predictors of death. GUSTO Investigators. Global Utilization of Streptokinase and Tissue-Plasminogen Activator for Occluded Coronary Arteries”. Am Heart J. 138 (1 Pt 1): 21–31. PMID 10385759.
- ↑ Shindler DM, Palmeri ST, Antonelli TA, Sleeper LA, Boland J, Cocke TP; et al. (2000). “Diabetes mellitus in cardiogenic shock complicating acute myocardial infarction: a report from the SHOCK Trial Registry. SHould we emergently revascularize Occluded Coronaries for cardiogenic shocK?”. J Am Coll Cardiol. 36 (3 Suppl A): 1097–103. PMID 10985711.
- ↑ Holmes, D. R.; Berger, P. B.; Hochman, J. S.; Granger, C. B.; Thompson, T. D.; Califf, R. M.; Vahanian, A.; Bates, E. R.; Topol, E. J. (1999). “Cardiogenic Shock in Patients With Acute Ischemic Syndromes With and Without ST-Segment Elevation”. Circulation. 100 (20): 2067–2073. doi:10.1161/01.CIR.100.20.2067. ISSN 0009-7322.
- ↑ Jacobs, Alice K; French, John K; Col, Jacques; Sleeper, Lynn A; Slater, James N; Carnendran, Louis; Boland, Jean; Jiang, Xianjiao; LeJemtel, Thierry; Hochman, Judith S (2000). “Cardiogenic shock with non-ST-segment elevation myocardial infarction: a report from the SHOCK Trial Registry”. Journal of the American College of Cardiology. 36 (3): 1091–1096. doi:10.1016/S0735-1097(00)00888-3. ISSN 0735-1097.
Risk Factors
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: João André Alves Silva, M.D. [2] Syed Musadiq Ali M.B.B.S.[3]
Overview
The identification of high-risk groups for developing cardiogenic shock and its promoting factors is mandatory for the improvement of the survival rate of these patients. This will facilitate the providing of adequate therapeutic measures and the avoidance of others which would otherwise lead to iatrogenic shock. Considering that the most common cause of cardiogenic shock is acute coronary syndrome, either with or without persistent ST-segment elevation, these patients are at higher risk and will benefit highly from these measures.
Risk Factors
Common Risk Factors
According to several studies and considering that left ventricular dysfunction is the most common cause of developing cardiogenic shock following myocardial infarction, the most common risk factors for this condition include:
- Older age (> 65 years)[1] For every 10 years of age, the risk is 47% greater.[2]
- Female sex, although some studies do not consider female sex as an independent predictor of poor outcome[3]
- Prior myocardial infarction (MI)[3]
- Prior angina[3]
- Peripheral vascular disease[3]
- Left ventricular ejection fraction < 35%[1]
- Moderate to severe mitral regurgitation[4]
- Larger infarct area (estimated by serial cardiac markers)[1]
- Diabetes mellitus[1]
- Impaired fasting glucose[5]
- ST elevation[6]
- ST depression[6]
- Q waves (EKG evidence of prior myocardial infarction)[6]
- According to the analysis of PURSUIT trial database[7] in Non-ST-segment elevation myocardial infarction patients who received eptifibatide saw their 30-day mortality risk reduced by 50%. In this trial, risk factors for development of cardiogenic shock like age and presence of ST depression in the initial EKG, in patients with Non-ST-segment elevation myocardial infarction, was also noted.
- Left bundle branch block[8]
- History of hypertension[9][10]
- Heart failure on admission[9][10]
- Multivessel coronary artery disease[9][10]
- Early use of beta blockers in large infarcts[9][10]
- In certain cases, excessive use of diuretics causing depletion of intravascular volume[11]
- Systolic blood pressure < 120 mm Hg[9][10]
- Sinus tachycardia[9][10]
- Heart rate < 60 bpm[12]
- Physical findings of hypoperfusion at time of diagnosis, such as altered state of consciousness or cold and clammy skin[13]
- Oliguria[13]
- Cardiogenic shock on admission[14]
- Timespan between symptom onset and when reperfusion is restored[15]
Specific Risk Factors
According to the etiology of the shock post-myocardial infarction, the different risk factors may have different importances in each cause:[16]
- Right Ventricular Infarction
- Younger age
- Generally no history of previous MI
- Generally single-vessel coronary disease
- Less likely anterior wall myocardial infarction
- Volume overloading[17][18]
- Acute Mitral Regurgitation
- Female gender
- Older age
- Diabetes mellitus
- Underlying cerebrovascular disease
- Common preexisting symptomatic coronary artery disease[19]
- Ventricular Septal Rupture
- Male gender[20]
- Mean age of presentation of 62.5 years[21]
- Common history of myocardial infarction[22][23]
- History of systemic hypertension prior to myocardial infarction[24]
- Free-Wall Rupture/Tamponade
- Female gender
- Age greater than 55 years[25][26]
- History of hypertension
- Larger infarct area
- Delayed or incomplete revascularization[24][27][28]
- No history of myocardial infarction[24][26]
- Single vessel coronary artery disease[24][26]
References
- ↑ 1.0 1.1 1.2 1.3 Hands, Mark E.; Rutherford, John D.; Muller, James E.; Davies, Glenn; Stone, Peter H.; Parker, Corette; Braunwald, Eugene (1989). “The in-hospital development of cardiogenic shock after myocardial infarction: Incidence, predictors of occurrence, outcome and prognostic factors”. Journal of the American College of Cardiology. 14 (1): 40–46. doi:10.1016/0735-1097(89)90051-X. ISSN 0735-1097.
- ↑ Hasdai D, Califf RM, Thompson TD, Hochman JS, Ohman EM, Pfisterer M; et al. (2000). “Predictors of cardiogenic shock after thrombolytic therapy for acute myocardial infarction”. J Am Coll Cardiol. 35 (1): 136–43. PMID 10636271.
- ↑ 3.0 3.1 3.2 3.3 Leor J, Goldbourt U, Reicher-Reiss H, Kaplinsky E, Behar S (1993). “Cardiogenic shock complicating acute myocardial infarction in patients without heart failure on admission: incidence, risk factors, and outcome. SPRINT Study Group”. Am J Med. 94 (3): 265–73. PMID 8452150.
- ↑ Picard MH, Davidoff R, Sleeper LA, Mendes LA, Thompson CR, Dzavik V; et al. (2003). “Echocardiographic predictors of survival and response to early revascularization in cardiogenic shock”. Circulation. 107 (2): 279–84. PMID 12538428.
- ↑ Zeller M, Cottin Y, Brindisi MC, Dentan G, Laurent Y, Janin-Manificat L; et al. (2004). “Impaired fasting glucose and cardiogenic shock in patients with acute myocardial infarction”. Eur Heart J. 25 (4): 308–12. doi:10.1016/j.ehj.2003.12.014. PMID 14984919.
- ↑ 6.0 6.1 6.2 Hathaway WR, Peterson ED, Wagner GS, Granger CB, Zabel KM, Pieper KS; et al. (1998). “Prognostic significance of the initial electrocardiogram in patients with acute myocardial infarction. GUSTO-I Investigators. Global Utilization of Streptokinase and t-PA for Occluded Coronary Arteries”. JAMA. 279 (5): 387–91. PMID 9459474.
- ↑ Hasdai D, Harrington RA, Hochman JS, Califf RM, Battler A, Box JW; et al. (2000). “Platelet glycoprotein IIb/IIIa blockade and outcome of cardiogenic shock complicating acute coronary syndromes without persistent ST-segment elevation”. J Am Coll Cardiol. 36 (3): 685–92. PMID 10987585.
- ↑ Sgarbossa EB, Pinski SL, Topol EJ, Califf RM, Barbagelata A, Goodman SG; et al. (1998). “Acute myocardial infarction and complete bundle branch block at hospital admission: clinical characteristics and outcome in the thrombolytic era. GUSTO-I Investigators. Global Utilization of Streptokinase and t-PA [tissue-type plasminogen activator] for Occluded Coronary Arteries”. J Am Coll Cardiol. 31 (1): 105–10. PMID 9426026.
- ↑ 9.0 9.1 9.2 9.3 9.4 9.5 Reynolds, H. R.; Hochman, J. S. (2008). “Cardiogenic Shock: Current Concepts and Improving Outcomes”. Circulation. 117 (5): 686–697. doi:10.1161/CIRCULATIONAHA.106.613596. ISSN 0009-7322.
- ↑ 10.0 10.1 10.2 10.3 10.4 10.5 Hasdai, David; Califf, Robert M.; Thompson, Trevor D.; Hochman, Judith S.; Ohman, E.Magnus; Pfisterer, Matthias; Bates, Eric R.; Vahanian, Alec; Armstrong, Paul W.; Criger, Douglas A.; Topol, Eric J.; Holmes, David R. (2000). “Predictors of cardiogenic shock after thrombolytic therapy for acute myocardial infarction”. Journal of the American College of Cardiology. 35 (1): 136–143. doi:10.1016/S0735-1097(99)00508-2. ISSN 0735-1097.
- ↑ Hasdai, David. (2002). Cardiogenic shock : diagnosis and treatmen. Totowa, N.J.: Humana Press. ISBN 1-58829-025-5.
- ↑ Antman, EM.; Hand, M.; Armstrong, PW.; Bates, ER.; Green, LA.; Halasyamani, LK.; Hochman, JS.; Krumholz, HM.; Lamas, GA. (2008). “2007 focused update of the ACC/AHA 2004 guidelines for the management of patients with ST-elevation myocardial infarction: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines”. J Am Coll Cardiol. 51 (2): 210–47. doi:10.1016/j.jacc.2007.10.001. PMID 18191746. Unknown parameter
|month=ignored (help) - ↑ 13.0 13.1 Hasdai D, Holmes DR, Califf RM, Thompson TD, Hochman JS, Pfisterer M; et al. (1999). “Cardiogenic shock complicating acute myocardial infarction: predictors of death. GUSTO Investigators. Global Utilization of Streptokinase and Tissue-Plasminogen Activator for Occluded Coronary Arteries”. Am Heart J. 138 (1 Pt 1): 21–31. PMID 10385759.
- ↑ Jeger RV, Harkness SM, Ramanathan K, Buller CE, Pfisterer ME, Sleeper LA; et al. (2006). “Emergency revascularization in patients with cardiogenic shock on admission: a report from the SHOCK trial and registry”. Eur Heart J. 27 (6): 664–70. doi:10.1093/eurheartj/ehi729. PMID 16423873.
- ↑ Ortolani P, Marzocchi A, Marrozzini C, Palmerini T, Saia F, Serantoni C; et al. (2006). “Clinical impact of direct referral to primary percutaneous coronary intervention following pre-hospital diagnosis of ST-elevation myocardial infarction”. Eur Heart J. 27 (13): 1550–7. doi:10.1093/eurheartj/ehl006. PMID 16707549.
- ↑ Ng, R.; Yeghiazarians, Y. (2011). “Post Myocardial Infarction Cardiogenic Shock: A Review of Current Therapies”. Journal of Intensive Care Medicine. 28 (3): 151–165. doi:10.1177/0885066611411407. ISSN 0885-0666.
- ↑ Hasdai, David. (2002). Cardiogenic shock : diagnosis and treatmen. Totowa, N.J.: Humana Press. ISBN 1-58829-025-5.
- ↑ Brookes, C.; Ravn, H.; White, P.; Moeldrup, U.; Oldershaw, P.; Redington, A. (1999). “Acute Right Ventricular Dilatation in Response to Ischemia Significantly Impairs Left Ventricular Systolic Performance”. Circulation. 100 (7): 761–767. doi:10.1161/01.CIR.100.7.761. ISSN 0009-7322.
- ↑ Tcheng JE, Jackman JD, Nelson CL, Gardner LH, Smith LR, Rankin JS; et al. (1992). “Outcome of patients sustaining acute ischemic mitral regurgitation during myocardial infarction”. Ann Intern Med. 117 (1): 18–24. PMID 1596043.
- ↑ SANDERS RJ, KERN WH, BLOUNT SG (1956). “Perforation of the interventricular septum complicating myocardial infarction; a report of eight cases, one with cardiac catheterization”. Am Heart J. 51 (5): 736–48. PMID 13302144.
- ↑ Skillington PD, Davies RH, Luff AJ, Williams JD, Dawkins KD, Conway N; et al. (1990). “Surgical treatment for infarct-related ventricular septal defects. Improved early results combined with analysis of late functional status”. J Thorac Cardiovasc Surg. 99 (5): 798–808. PMID 2329817.
- ↑ Hutchins GM (1979). “Rupture of the interventricular septum complicating myocardial infarction: pathological analysis of 10 patients with clinically diagnosed perforations”. Am Heart J. 97 (2): 165–73. PMID 760447.
- ↑ Daggett WM, Buckley MJ, Akins CW, Leinbach RC, Gold HK, Block PC; et al. (1982). “Improved results of surgical management of postinfarction ventricular septal rupture”. Ann Surg. 196 (3): 269–77. PMC 1352596. PMID 7114934.
- ↑ 24.0 24.1 24.2 24.3 Mann JM, Roberts WC (1988). “Rupture of the left ventricular free wall during acute myocardial infarction: analysis of 138 necropsy patients and comparison with 50 necropsy patients with acute myocardial infarction without rupture”. Am J Cardiol. 62 (13): 847–59. PMID 3052010.
- ↑ Bates RJ, Beutler S, Resnekov L, Anagnostopoulos CE (1977). “Cardiac rupture–challenge in diagnosis and management”. Am J Cardiol. 40 (3): 429–37. PMID 331926.
- ↑ 26.0 26.1 26.2 Figueras J, Curos A, Cortadellas J, Sans M, Soler-Soler J (1995). “Relevance of electrocardiographic findings, heart failure, and infarct site in assessing risk and timing of left ventricular free wall rupture during acute myocardial infarction”. Am J Cardiol. 76 (8): 543–7. PMID 7677073.
- ↑ Lewis AJ, Burchell HB, Titus JL (1969). “Clinical and pathologic features of postinfarction cardiac rupture”. Am J Cardiol. 23 (1): 43–53. PMID 5380841.
- ↑ Dellborg M, Held P, Swedberg K, Vedin A (1985). “Rupture of the myocardium. Occurrence and risk factors”. Br Heart J. 54 (1): 11–6. PMC 481840. PMID 4015910.
Natural History, Complications and Prognosis
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: James Nasr[2]
Cardiogenic shock natural history, complications and prognosis
Overview
Cardiogenic shock is a time-sensitive, high-mortality syndrome characterized by impaired cardiac output, systemic hypoperfusion, and progressive end-organ dysfunction. Its clinical course is best understood as a continuum rather than a fixed state, ranging from preshock to classic, deteriorating, and refractory shock. Prognosis is determined by the cause of shock, SCAI shock stage, lactate trajectory, hemodynamic severity, cardiac arrest status, comorbidity burden, and the development of multiorgan failure.[1][2][3]
Major complications include multiorgan failure, acute kidney injury, hepatic injury, neurologic injury after cardiac arrest, bleeding and vascular complications from invasive support, respiratory failure, arrhythmias, secondary infection, and coagulopathy. Although short-term mortality remains high, survivors also face substantial long-term risks, including recurrent heart failure, renal dysfunction, neurocognitive impairment, frailty, rehospitalization, and reduced quality of life.[4][5]
Natural history
Cardiogenic shock is a dynamic clinical syndrome rather than a binary event. The clinical course may progress from preshock to classic shock, deteriorating shock, and refractory shock, corresponding broadly to SCAI shock stages B through E.[1][2]
The typical trajectory begins with impaired stroke volume and reduced cardiac output, followed by systemic tissue hypoperfusion, rising lactate, progressive end-organ dysfunction, and, if uncorrected, multiorgan failure.[3][4] In acute myocardial infarction-related cardiogenic shock, shock may be present at admission or may develop during hospitalization; therefore, patients with early or less severe shock require serial reassessment rather than one-time staging.[6]
Serial SCAI staging has prognostic value. In the Cardiogenic Shock Working Group registry, progression of any SCAI stage from baseline to 24 hours was associated with higher unadjusted in-hospital mortality than improvement, and progression to SCAI stage E at 24 hours was associated with very high mortality.[6] Notably, baseline SCAI stage B patients had higher unadjusted mortality than stage C patients in this registry (28.3% vs. 22.0%; P=0.017), likely reflecting higher rates of stage escalation from stage B; mortality was 33.8% for stage D and 59.6% for stage E.[6]
Complications
| Complication | Clinical significance | Prognostic implication |
|---|---|---|
| Multiorgan failure | Hallmark complication of advanced cardiogenic shock; may involve renal, hepatic, respiratory, neurologic, hematologic, and metabolic systems. | Strongly associated with in-hospital mortality; mortality rises with each additional failing organ system.[7] |
| Acute kidney injury | May result from low renal perfusion, renal venous congestion, inflammation, contrast exposure, and progression to acute tubular necrosis. In the DanGer Shock trial, renal replacement therapy was administered to 41.9% of patients treated with a microaxial flow pump and 26.7% of patients receiving standard care (relative risk, 1.98; 95% CI, 1.27 to 3.09).[8] In the dedicated renal substudy using RIFLE criteria, acute kidney injury occurred in 61% of the microaxial flow pump group and 45% of the control group; all patients alive at 180 days were free of renal replacement therapy.[9] | Need for renal replacement therapy is consistently associated with worse survival. |
| Hepatic injury | Hypoxic hepatitis is commonly defined as aminotransferase elevation greater than 20 times the upper limit of normal and has been reported in approximately 18% of patients with acute myocardial infarction-related cardiogenic shock.[3] Congestive hepatopathy from elevated right-sided filling pressures may coexist. | Marked aminotransferase elevation and worsening synthetic function indicate severe systemic hypoperfusion. |
| Neurologic injury | Most common after preceding cardiac arrest; includes hypoxic-ischemic brain injury and coma. | Major determinant of death and long-term disability, especially after out-of-hospital cardiac arrest.[10] |
| Bleeding and vascular complications | Occur particularly with mechanical circulatory support, large-bore arterial access, anticoagulation, and antiplatelet therapy. In the primary DanGer Shock publication, moderate or severe bleeding by GUSTO criteria occurred in 21.8% of patients treated with a microaxial flow pump and 11.9% of patients receiving standard care; limb ischemia occurred in 5.6% and 1.1%, respectively.[8] | Bleeding, limb ischemia, and vascular injury may limit therapy and increase morbidity. |
| Respiratory failure | May result from pulmonary edema, impaired oxygen delivery, acute respiratory distress syndrome, or need for airway protection after cardiac arrest. | Worsens tissue hypoxia and may increase right ventricular afterload. |
| Arrhythmia | Includes ventricular tachycardia, ventricular fibrillation, bradyarrhythmias, and high-grade atrioventricular block. | May precipitate shock, worsen established shock, or represent a terminal mode of death.[11] |
| Sepsis and secondary infection | May occur during prolonged critical illness, invasive device support, indwelling catheter use, and gut barrier dysfunction. | Adds distributive physiology and may convert isolated cardiogenic shock into mixed shock. |
| Coagulopathy and disseminated intravascular coagulation | May occur with systemic inflammation, liver dysfunction, shock-induced endothelial injury, or extracorporeal support. | Increases bleeding and thrombotic risk. |
Short-term prognosis
Cardiogenic shock remains a high-mortality syndrome despite contemporary reperfusion, critical care, vasoactive support, and mechanical circulatory support. In acute myocardial infarction-related cardiogenic shock, contemporary 30-day mortality is approximately 30% to 50%, depending on case mix, shock severity, cardiac arrest status, and treatment strategy.[12][4]
Etiology influences early mortality. Among 8,974 patients with cardiogenic shock, in-hospital mortality was 48% in mixed-cause shock, 41% in acute myocardial infarction-related shock, 31% in new heart failure, 31% in secondary causes, and 25% in acute-on-chronic heart failure-related shock.[12][13] A 2026 meta-analysis of 29 studies including 497,368 patients found higher short-term mortality in acute myocardial infarction-related cardiogenic shock than in heart failure-related cardiogenic shock (odds ratio, 1.58; 95% CI, 1.06 to 2.37).[14]
In a single-center registry, heart failure-related cardiogenic shock had lower in-hospital mortality than acute myocardial infarction-related cardiogenic shock (23.9% vs. 39.3%) and lower 1-year mortality (42.6% vs. 52.9%), with similar 30-day readmission rates.[15]
SCAI stage strongly stratifies hospital mortality. In the initial Mayo Clinic validation cohort, the unadjusted odds of hospital mortality increased stepwise from SCAI stage B through stage E compared with stage A.[16] Using Cardiogenic Shock Working Group-defined criteria, in-hospital mortality also rises across SCAI stages B, C, D, and E.[2]
Long-term prognosis
Long-term mortality remains substantial among survivors of cardiogenic shock. In a population-based study of 9,789 consecutive patients with acute myocardial infarction complicated by cardiogenic shock, mortality was 40.9% at 1 year and 58.9% at 5 years, with no clear plateau in mortality up to 10 years after admission.[5]
Among hospital survivors of acute myocardial infarction-related cardiogenic shock who undergo revascularization, long-term survival may be substantially better than early mortality statistics suggest; however, the highest post-discharge risk is concentrated in the early recovery period.[5] In patients aged 65 years or older who survived hospitalization for acute myocardial infarction-related cardiogenic shock, excess post-discharge mortality was concentrated in the first 60 days after discharge; after this period, mortality was similar to patients without cardiogenic shock.[17]
Survivors require structured follow-up for residual ventricular dysfunction, recurrent heart failure, arrhythmia risk, renal dysfunction, frailty, cognitive impairment, and psychosocial sequelae.[18][19]
Predictors of mortality
| Prognostic domain | Adverse predictors | Clinical interpretation |
|---|---|---|
| Shock severity | Higher baseline SCAI stage; maximum SCAI stage during hospitalization; worsening SCAI stage over the first 24 to 72 hours | Serial worsening is more informative than a single baseline assessment.[6] |
| Cardiac arrest status | Out-of-hospital cardiac arrest; in-hospital cardiac arrest; persistent coma or anoxic brain injury | Cardiac arrest increases mortality across SCAI stages and changes the dominant mode of death.[16][10] |
| Hemodynamics | Low mean arterial pressure, low cardiac index, elevated right atrial pressure, low cardiac power output, low cardiac power index, low pulmonary artery pulsatility index, low central venous oxygen saturation | Cardiac power output is a strong hemodynamic marker of mortality. The SHOCK trial registry identified cardiac power output ≤0.53 W as the threshold most accurately predicting in-hospital mortality, with sensitivity and specificity of 0.66 and positive predictive value of 58%.[20] In a post-hoc analysis of two prospective studies, clinically relevant 24-hour hemodynamic thresholds associated with poor outcomes included mean arterial pressure less than 70 mm Hg, cardiac index 1.8 L/min/m² or less, cardiac power index less than 0.27 W/m², and central venous oxygen saturation less than 70%.[21] |
| Lactate and lactate clearance | Elevated baseline lactate, persistently elevated lactate, rising lactate, impaired lactate clearance | Lactate trajectory is more informative than a single value. In IABP-SHOCK II post-hoc analysis, 8-hour lactate was the strongest lactate-based mortality predictor, with an optimal cutoff of 3.1 mmol/L. In the Altshock-2 registry, 24-hour lactate had higher predictive accuracy than baseline lactate; reported optimal cutoffs were 3.2 mmol/L at baseline and 1.7 mmol/L at 24 hours.[22][23] |
| Acid-base and metabolic injury | Systemic pH ≤7.2, severe metabolic acidosis, hyperglycemia | Reflects advanced tissue hypoperfusion and impaired metabolic reserve. |
| End-organ injury | Acute kidney injury, need for dialysis, hepatic injury, respiratory failure, multiorgan failure | Organ failure burden is a major determinant of mortality.[7] |
| Patient factors | Older age, diabetes mellitus, prior myocardial infarction, prior percutaneous coronary intervention, prior coronary artery bypass grafting, frailty | These factors reduce physiologic reserve and increase treatment risk. |
| Comorbidity burden | Higher aggregate comorbidity burden | Comorbidity burden independently modifies mortality risk across SCAI stages and may be most influential in early or preshock states.[24] |
| Treatment course | Prolonged vasopressor requirement, inability to restore perfusion, need for escalation of mechanical circulatory support | Suggests persistent or refractory shock physiology. |
Lactate clearance
Lactate clearance is an important dynamic marker of recovery from cardiogenic shock. Failure of lactate to fall after restoration of macrocirculatory targets suggests persistent tissue hypoperfusion, impaired clearance, or progression to hemometabolic shock.[3]
The SCAI Door-to-Lactate Clearance initiative proposes serial lactate measurement at 2- to 3-hour intervals and lactate clearance within 24 hours as a quality metric and prognostic marker in cardiogenic shock, analogous to door-to-balloon time in ST-elevation myocardial infarction.[25] A secondary analysis of the CardShock registry found that a 50% relative reduction in lactate at 24 hours was predictive of improved survival.[25]
Prognostic scoring systems
Several cardiogenic shock-specific prognostic tools have been externally validated, but no single score should replace serial bedside reassessment, hemodynamic evaluation, and multidisciplinary clinical judgment.
| Score | Population | Components or domains | Main use |
|---|---|---|---|
| CardShock score | Mixed cardiogenic shock populations | Age greater than 75 years, confusion at presentation, prior myocardial infarction or coronary artery bypass grafting, acute coronary syndrome etiology, reduced left ventricular ejection fraction, arterial lactate, and estimated glomerular filtration rate | Early mortality risk stratification |
| Cardiogenic Shock Score | Mixed cardiogenic shock populations | Age, sex, acute myocardial infarction-related cardiogenic shock etiology, systolic blood pressure, heart rate, pH, lactate, glucose, and cardiac arrest | Mortality risk stratification; reported discrimination was higher than IABP-SHOCK II and CardShock in its derivation and validation study.[26] |
| IABP-SHOCK II score | Acute myocardial infarction-related cardiogenic shock | Age greater than 73 years, prior stroke, admission glucose greater than 191 mg/dL, creatinine greater than 1.36 mg/dL, lactate greater than 5.0 mmol/L, and post-PCI TIMI flow less than 3 | Mortality risk stratification after AMI-CS |
| SHOCK trial and registry score | Acute myocardial infarction-related cardiogenic shock | Derived from SHOCK trial-era clinical and hemodynamic predictors | Prognostic assessment in AMI-CS populations |
| ENCOURAGE score | Patients receiving venoarterial extracorporeal membrane oxygenation | Clinical and laboratory variables before or at VA-ECMO initiation | Mortality prediction in VA-ECMO-supported shock |
| SAVE score | Patients receiving extracorporeal life support | Pre-extracorporeal support clinical variables | Survival prediction after extracorporeal support |
A systematic review and meta-analysis of prognostic scores in cardiogenic shock found no statistically significant difference between scores overall, although the CardShock score had the highest pooled discrimination and best calibration among the evaluated tools.[27] No consensus currently mandates use of a specific prognostic score to determine initiation of temporary mechanical circulatory support.[3][12]
Modes of death
In the Critical Care Cardiology Trials Network registry, most in-hospital deaths among patients with cardiogenic shock were cardiovascular, and persistent cardiogenic shock was the dominant specific mode of death.[11] Other modes of death include arrhythmia, anoxic brain injury, respiratory failure, and multiorgan failure.[11][10]
Timing of death varies by mechanism. Primary cardiac death may occur early, whereas death from neurologic injury or multiorgan failure often occurs later during the hospitalization.[10] Patients with preceding cardiac arrest are more likely to die from anoxic brain injury or arrhythmia than patients without cardiac arrest.[11]
Prognosis in older adults
Older age is associated with higher mortality in cardiogenic shock and is associated with increased vulnerability to frailty, bleeding, renal injury, delirium, functional decline, and complications of invasive support.[28] In older adults, prognosis should be assessed using shock severity, reversibility of the underlying cardiac process, neurologic status, comorbidity burden, frailty, pre-illness functional status, and patient goals rather than chronologic age alone.[28]
Survivorship and quality of life
Survivors of cardiogenic shock may experience persistent heart failure, recurrent hospitalization, chronic kidney disease, neurocognitive impairment after cardiac arrest, physical deconditioning, anxiety, depression, and reduced quality of life.[18][19] Post-discharge care should emphasize recovery of ventricular function when possible, optimization of guideline-directed medical therapy, rehabilitation, assessment for implantable cardioverter-defibrillator or cardiac resynchronization therapy when indicated, and evaluation for advanced heart failure therapies in selected patients.[19]
References
- ↑ 1.0 1.1 Baran DA, Grines CL, Bailey S; et al. (2019). “SCAI Clinical Expert Consensus Statement on the Classification of Cardiogenic Shock”. Catheterization and Cardiovascular Interventions. 94 (1): 29–37. doi:10.1002/ccd.28329.
- ↑ 2.0 2.1 2.2 Kapur NK, Kanwar M, Sinha SS; et al. (2022). “Criteria for Defining Stages of Cardiogenic Shock Severity”. Journal of the American College of Cardiology. 80 (3): 185–198. doi:10.1016/j.jacc.2022.04.049.
- ↑ 3.0 3.1 3.2 3.3 3.4 Lüsebrink E, Binzenhöfer L, Adamo M; et al. (2024). “Cardiogenic Shock”. Lancet. 404 (10466): 2006–2020. doi:10.1016/S0140-6736(24)01818-X.
- ↑ 4.0 4.1 4.2 Samsky MD, Morrow DA, Proudfoot AG; et al. (2021). “Cardiogenic Shock After Acute Myocardial Infarction: A Review”. JAMA. 326 (18): 1840–1850. doi:10.1001/jama.2021.18323.
- ↑ 5.0 5.1 5.2 Sterling LH, Fernando SM, Talarico R; et al. (2023). “Long-Term Outcomes of Cardiogenic Shock Complicating Myocardial Infarction”. Journal of the American College of Cardiology. 82 (10): 985–995. doi:10.1016/j.jacc.2023.06.026.
- ↑ 6.0 6.1 6.2 6.3 Ton VK, Li S, John K; et al. (2024). “Serial Shock Severity Assessment Within 72 Hours After Diagnosis: A Cardiogenic Shock Working Group Report”. Journal of the American College of Cardiology. doi:10.1016/j.jacc.2024.04.069.
- ↑ 7.0 7.1 Vallabhajosyula S, Dunlay SM, Prasad A; et al. (2019). “Acute Noncardiac Organ Failure in Acute Myocardial Infarction With Cardiogenic Shock”. Journal of the American College of Cardiology. 73 (14): 1781–1791. doi:10.1016/j.jacc.2019.01.053.
- ↑ 8.0 8.1 Møller JE, Engstrøm T, Jensen LO; et al. (2024). “Microaxial Flow Pump or Standard Care in Infarct-Related Cardiogenic Shock”. The New England Journal of Medicine. 390 (15): 1382–1393. doi:10.1056/NEJMoa2312572.
- ↑ Zweck E, Hassager C, Beske RP; et al. (2024). “Microaxial Flow Pump Use and Renal Outcomes in Infarct-Related Cardiogenic Shock: A Secondary Analysis of the DanGer Shock Trial”. Circulation. 150 (25): 1990–2003. doi:10.1161/CIRCULATIONAHA.124.072370.
- ↑ 10.0 10.1 10.2 10.3 Davodian LW, Larsen JKP, Povlsen AL; et al. (2022). “Timing and Causes of Death in Acute Myocardial Infarction Complicated by Cardiogenic Shock (From the RETROSHOCK Cohort)”. The American Journal of Cardiology. 171: 15–22. doi:10.1016/j.amjcard.2022.01.050.
- ↑ 11.0 11.1 11.2 11.3 Berg DD, Singal S, Palazzolo M; et al. (2024). “Modes of Death in Patients With Cardiogenic Shock in the Cardiac Intensive Care Unit: A Report From the Critical Care Cardiology Trials Network”. Journal of Cardiac Failure. 30 (5): 728–733. doi:10.1016/j.cardfail.2024.01.012.
- ↑ 12.0 12.1 12.2 Thiele H, Hassager C (2026). “Cardiogenic Shock”. The New England Journal of Medicine. 394 (1): 62–77. doi:10.1056/NEJMra2312086.
- ↑ Zweck E, Kanwar M, Li S; et al. (2023). “Clinical Course of Patients in Cardiogenic Shock Stratified by Phenotype”. JACC: Heart Failure. 11 (10): 1304–1315. doi:10.1016/j.jchf.2023.05.007.
- ↑ Yilmaz MB, Kilic ME, Biegus J; et al. (2026). “Acute Myocardial Infarction Versus Acute Decompensated Heart Failure in Cardiogenic Shock: A Systematic Review and Meta-Analysis of Clinical Phenotypes and Mortality”. European Journal of Heart Failure. doi:10.1093/ejhf/xuag186.
- ↑ Sinha SS, Rosner CM, Tehrani BN; et al. (2022). “Cardiogenic Shock From Heart Failure Versus Acute Myocardial Infarction: Clinical Characteristics, Hospital Course, and 1-Year Outcomes”. Circulation: Heart Failure. 15 (6): e009279. doi:10.1161/CIRCHEARTFAILURE.121.009279.
- ↑ 16.0 16.1 Jentzer JC, van Diepen S, Barsness GW; et al. (2019). “Cardiogenic Shock Classification to Predict Mortality in the Cardiac Intensive Care Unit”. Journal of the American College of Cardiology. 74 (17): 2117–2128. doi:10.1016/j.jacc.2019.07.077.
- ↑ Shah RU, de Lemos JA, Wang TY; et al. (2016). “Post-Hospital Outcomes of Patients With Acute Myocardial Infarction With Cardiogenic Shock: Findings From the NCDR”. Journal of the American College of Cardiology.
- ↑ 18.0 18.1 Hall EJ, Agarwal S, Cullum CM; et al. (2025). “Survivorship After Cardiogenic Shock”. Circulation. 151 (3): 257–271. doi:10.1161/CIRCULATIONAHA.124.068203.
- ↑ 19.0 19.1 19.2 Blumer V, Sinha SS, Carnicelli AP; et al. (2026). “Cardiogenic Shock Survivorship: A Multidisciplinary Approach Across the Continuum of Care”. Journal of the American College of Cardiology. doi:10.1016/j.jacc.2026.02.5080.
- ↑ Fincke R, Hochman JS, Lowe AM; et al. (2004). “Cardiac Power Is the Strongest Hemodynamic Correlate of Mortality in Cardiogenic Shock: A Report From the SHOCK Trial Registry”. Journal of the American College of Cardiology. 44 (2): 340–348. doi:10.1016/j.jacc.2004.03.060.
- ↑ Levy B, Curtiaud A, Duarte K; et al. (2025). “Association Between Mean Hemodynamic Variables During the First 24 h and Outcomes in Cardiogenic Shock: Identification of Clinically Relevant Thresholds”. Critical Care. 29 (1): 137. doi:10.1186/s13054-025-05356-0.
- ↑ IABP-SHOCK II post-hoc lactate analysis. Eight-hour lactate and mortality prediction in acute myocardial infarction-related cardiogenic shock.
- ↑ Pagnesi M, Riccardi M, Sacco A; et al. (2025). “Lactate Values and Mortality in Patients With Cardiogenic Shock: Insights From the Altshock-2 Registry”. Critical Care Medicine. doi:10.1097/CCM.0000000000006738.
- ↑ Sundermeyer et al. Comorbidity burden and mortality modification across SCAI shock stages. Journal of the American College of Cardiology. 2025.
- ↑ 25.0 25.1 Naidu SS, Nathan S, Basir MB; et al. (2025). “SCAI Door to Lactate Clearance (SCAI DLC) Cardiogenic Shock Initiative: Definition, Hypothesis, and Call to Action”. Journal of the Society for Cardiovascular Angiography & Interventions. 4 (11): 103996. doi:10.1016/j.jscai.2025.103996.
- ↑ Beer BN, Jentzer JC, Weimann J; et al. (2022). “Early Risk Stratification in Patients With Cardiogenic Shock Irrespective of the Underlying Cause – the Cardiogenic Shock Score”. European Journal of Heart Failure. 24 (4): 657–667. doi:10.1002/ejhf.2449.
- ↑ Ng et al. Prognostic scores in cardiogenic shock: systematic review and meta-analysis. Critical Care Medicine. 2025.
- ↑ 28.0 28.1 Blumer V, Kanwar MK, Barnett CF; et al. (2024). “Cardiogenic Shock in Older Adults: A Focus on Age-Associated Risks and Approach to Management: A Scientific Statement From the American Heart Association”. Circulation. 149 (14): e1051–e1065. doi:10.1161/CIR.0000000000001214.
Diagnosis
Diagnosis
Diagnostic Evaluation | History and Symptoms | Physical Examination | Laboratory Findings | Electrocardiogram | Chest X Ray | CT | MRI | Echocardiography or Ultrasound | Other Imaging Findings | Other Diagnostic Studies
Treatment
Treatment
Medical Therapy | Surgery | Primary Prevention | Secondary Prevention | Cost-Effectiveness of Therapy | Future or Investigational Therapies
Looking for the patient version?
© 2026 MyEClinic – IFTM Institut für Telematik in der Medizin GmbH