
The WikiDoc Living Textbook of Cardiology
Click Here For A Complete Listing Of All Chapters In The Living Textbook Of Cardiology In Alphabetical Order
Click Here For Status Update Of Cardiology
ANATOMY
| Organ System Project |
|---|
| Topics |
| Leaders & Members |
| Meetings’ Summary |
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1] Associate Editor(s)-in-Chief: Huda A. Karman, M.D.
System leader: Sahar Memar Montazerin, M.D.
Status Updates
| Resident survival guide Progress | |
|---|---|
| Completed | 50 |
| In progress | 0 |
| Remaining | 1 |
| Primary care chapter Progress | |
| Completed | 1 |
| In progress | 6 |
| Remaining | 6 |
Primary Care Topics
Status Updates
| Progress | |
|---|---|
| Completed | 84 |
| In progress | 48 |
| Remaining | 0 |
List of Chapters Requiring Content
In progress chapters
| Category | Chapters that need content | Assignment Status | Scholar’s name | Coach name | Completion Status | Review status | Reviewer name |
|---|---|---|---|---|---|---|---|
| Cardiovascular system | |||||||
| Aortic regurgitation | Assigned | Mohammed Salih | Ali | In progress | |||
| Arrhythmogenic right ventricular cardiomyopathy | Assigned | Huda | In progress | ||||
| Atherosclerosis | Assigned | Niloofar | In progress | ||||
| AV nodal reentrant tachycardia | Assigned | Ramyar | In progress | ||||
| Cardiac transplant | Assigned | Ifrah Fatima | Sogand | In progress | |||
| Cardiopulmonary resuscitation | Assigned | Amir Bagheri | Farima | In progress | |||
| Cardioversion | Assigned | Sara hadadi | In progress | ||||
| Collateral circulation | Assigned | Mydah | Elsaiey,Ahmed | In progress | |||
| Coronary artery bypass grafting | Assigned | Nidhi Kanwar | Sahar | In progress | |||
| Dextrocardia | Assigned | Scott | Fahimeh | In progress | |||
| Heart transplantation associated arrhythmias | Assigned | Syed Rizvi | Aditya | In progress | |||
| Holter monitor | Assigned | Rinky | Abdelrahman | In progress | |||
| Hyperkalemia | Assigned | Huda | In progress | ||||
| Hypokalemia | Assigned | Alieh Behjat | Mandana | ||||
| Infra-Hisian Block | Assigned | Sara | In progress | ||||
| Junctional rhythm | Assigned | Ahmed | In progress | ||||
| Mycotic aneurysm | Assigned | Krishna | In progress | ||||
| Oculofaciocardiodental syndrome | Assigned | Arash | Niloofar | In progress | |||
| Pacemaker syndrome | Assigned | Tayyaba, Mohammed Salih | Ali | In progress | |||
| Paradoxical embolism | Assigned | Hira Rehman | Roukoz | In progress | |||
| Paradoxical septal motion | Assigned | Mitra | Sogand | In progress | |||
| Parkes Weber syndrome | Assigned | Saud Khan | Inactive | ||||
| Paroxysmal supraventricular tachycardia | Assigned | Noha Elzeiny | Homa | In progress | |||
| Palpitation | Assigned | Akash Daswaney | Homa | In progress | |||
| Persistent juvenile T-wave pattern | Assigned | Zaida | Farima | In progress | |||
| Peripartum cardiomyopathy | Assigned | Nabeel ahmad | Inactive | ||||
| Persistent truncus arteriosus | Assigned | Fahime | In progress | ||||
| Premature ventricular contraction | Assigned | Radwa | Homa | In progress | |||
| Post-infarction conduction abnormalities | Assigned | Hamid Parsa | Ramyar | In progress | |||
| Postural orthostatic tachycardia syndrome | Assigned | Saud Khan | Mahshid, Sahar | Inactive | |||
| PR interval alternans | Assigned | Sogand’s scholar | In progress | ||||
| Pulmonary atresia | Assigned | Muhammad Waqas | In progress | ||||
| Pulmonary valve | Assigned | Mohammed Salih | Ali | – | |||
| Pulmonary valve stenosis | Assigned | Mohammed Salih | Ali | – | |||
| P wave alternans | Assigned | Ahmed | – | ||||
| Reperfusion injury | Assigned | Shivam Single | Sara | In progress | |||
| Right ventricular outflow obstruction | Assigned | Mohemmed Salih | Ali | – | |||
| Spontaneous coronary artery dissection | Assigned | Mohammed aboali | Inactive | ||||
| Short QT syndrome | Assigned | Sumanth | Huda | In progress | |||
| Sudden infant death syndrome | Assigned | Krishna | In progress | ||||
| Transcatheter aortic valve implantation | Assigned | Sogand | In progress | ||||
| Thoracic aortic aneurysm | Assigned | Mohammed Salih | Ali | – | |||
| Ventricular Assist device | Assigned | Tayebah Choudhary | Ali | In progress | |||
| Ventricular tachycardia | Assigned | Aisha Adigun | Homa | In progress | |||
| Wolff-Parkinson White syndrome | Assigned | Sara Zand | Fahime | In progress |
Completed chapters
| Category | Chapters that need content | Assignment Status | Scholar’s name | Coach name | Completion Status | Review status | Reviewer name |
|---|---|---|---|---|---|---|---|
| CVS | Abdominal aortic aneurysm | Assigned | Ramyar | Complete | In progress | ||
| Acute coronary syndromes | Assigned | Sabawoon | Complete | Completed | Nicholas Menzel | ||
| Acute aortic syndrome | Assigned | Sahar | Complete | In progress | |||
| Aortic dissection | Assigned | Sahar | Complete | In progress | |||
| Aortic intramural hematoma | Assigned | Cafer Zorkon | Complete | In progress | |||
| Aortic stenosis | Assigned | Mandana | Complete | In progress | |||
| Artificial pacemaker | Assigned | Javaria Anwer | Farima | Complete | In progress | ||
| Atrial fibrillation | Assigned | Hasan | Complete | In progress | |||
| Atrial septal defect | Assigned | Ifeoma | Complete | In progress | |||
| Beri Beri | Assigned | Abdelrahman | Complete | In progress | |||
| Bifascicular block | Assigned | Shadi Ebr | Sahar | Complete | In progress | ||
| Blalock-Taussig shunt | Assigned | Usman Ali Akbar | Sara Mohsin | Complete | Completed | Sara Mohsin | |
| Brugada syndrome | Assigned | Sogand | Complete | In progress | |||
| Bundle branch block (LP) | Assigned | Maneesha | Complete | In progress | |||
| Cardiac amyloidosis | Assigned | Sabawoon | Complete | In progress | |||
| Cardiac tamponade | Assigned | Ramyar | Complete | In progress | |||
| Cardiac fibrosis | Assigned | Niloofar | Complete | In progress | |||
| Cardiogenic shock | Assigned | Ali | Complete | In progress | |||
| Cardiac transplantation | Assigned | Ifrah Fatima | Sogand | Complete | In progress | ||
| Catecholaminergic polymorphic ventricular tachycardia (CPVT) | Assigned | Mounika | Krishna | Complete | In progress | ||
| Chagas disease | Assigned | Huda | Complete | In progress | |||
| Congenital heart block | Assigned | Sogand | Complete | In progress | |||
| Constrictive pericarditis | Assigned | Huda | Complete | In progress | |||
| Cyanotic heart disease | Assigned | Fahime | Complete | In progress | |||
| Dressler’s syndrome | Assigned | Abdelrahman | Complete | In progress | |||
| Ebstein’s anomaly | Assigned | Maneesha | Complete | In progress | |||
| Eisenmenger’s syndrome | Assigned | Abdelrahman | Complete | In progress | |||
| Endocardial cushion defect | Assigned | Aditya | Complete | In progress | |||
| Endocarditis | Assigned | Fahime | Complete | In progress | |||
| Dilated cardiomyopathy | Assigned | Abdelrahman | Complete | In progress | |||
| First degree AV block | Assigned | Ahmed | Complete | In progress | |||
| Heart Failure | Assigned | Hasan | Complete | In progress | |||
| Heart in Kawasaki disease | Assigned | Sabawoon | Complete | In progress | |||
| HIV induced pericarditis | Assigned | Ramyar | Complete | In progress | |||
| Holiday heart syndrome | Assigned | Apeksha Gupta | Aditya | Complete | In progress | ||
| Hypertrophic obstructive cardiomyopathy | Assigned | Soroush | Complete | In progress | |||
| Kawasaki disease | Assigned | Fahime | Complete | In progress | |||
| Jervel Lange Nielson Syndrome | Assigned | Krishna | Complete | In progress | |||
| Libman-Sacks endocarditis | Assigned | Sara | Complete | In progress | |||
| Long QT syndrome (LQTS) | Assigned | Krishna | Complete | In progress | |||
| Lown-Ganong-Levine syndrome | Assigned | Usman Ali Akbar | Sara Mohsin | Complete | English reviewed | Sara Mohsin | |
| Loeffler endocarditis | Assigned | Soroush | Complete | In progress | |||
| Mitral stenosis | Assigned | Aditya | Complete | In progress | |||
| Myocardial abscess | Assigned | Ali | Complete | In progress | |||
| Myocarditis | Assigned | Homa | Complete | In progress | |||
| Myxoma | Assigned | Sogand | Complete | In progress | |||
| Myxomatous degeneration | Assigned | Ali | Complete | In progress | |||
| Nonbacterial thrombotic endocarditis | Assigned | Homa | Complete | In progress | |||
| Obesity cardiomyopathy | Assigned | Soroush | Complete | In progress | |||
| Paget-Schroetter disease | Assigned | Anahita Deylamshahi | Krishna | Complete | In progress | ||
| Parasystole | Assigned | Mohammed Salih | Complete | In progress | |||
| Paroxysmal AV block | Assigned | Akash Daswaney | Homa | Complete | In progress | ||
| Patent ductus arteriosus | Assigned | Ramyar | Complete | In progress | |||
| Patent foramen ovale | Assigned | Ifoma | Complete | In progress | |||
| Penetrating atherosclerotic aortic ulcer | Assigned | Sahar | Complete | In progress | |||
| Pentalogy of Fallot | Assigned | Abdulkareem Lukan | Sahar | Complete | In progress | ||
| Pericardial effusion | Assigned | Abdelrahman | Complete | In progress | |||
| Post-cardiac injury syndrome | Assigned | Ibtisam Ashraf | Sahar | Complete | In progress | ||
| Post myocardial infarction pericarditis | Assigned | Mandana | Complete | In progress | |||
| Postpericardiotomy syndrome | Assigned | Niloofar | Complete | In progress | |||
| Pericarditis | Assigned | Homa | Complete | In progress | |||
| Pre-excitation syndrome | Assigned | Shivam Singla | Sara Mohsin | Complete | Needs English Review | Sara Mohsin | |
| Premature atrial contraction | Assigned | Amandeep | Complete | In progress | |||
| Prinzmetal’s angina | Assigned | Amandeep | Complete | In progress | |||
| Restrictive Cardiomyopathy | Assigned | Maneesha | Complete | In progress | |||
| Rheumatic heart disease | Assigned | Huda | Complete | In progress | |||
| 2nd degree heart block | Assigned | Ahmed | Complete | In progress | |||
| Sick sinus syndrome | Assigned | Sahar | Complete | In progress | |||
| Supraventricular tachycardia | Assigned | Abdelrahman | Complete | In progress | |||
| Tetralogy of Fallot | Assigned | Fahime | Complete | In progress | |||
| Third degree AV block | Assigned | Qasim Khurshid | Maneesha | Complete | In progress | ||
| Transesophageal echocardiography | Assigned | Shakiba Hassanzadeh | Ahmed | Complete | In progress | ||
| Transposition of great arteries | Assigned | Aditya | Complete | In progress | |||
| Tricuspid atresia | Assigned | Sara Zand | Fahime | Complete | In progress | ||
| Tricuspid regurgitation | Assigned | Krishna | Complete | In progress | |||
| Timothys syndrome | Assigned | Krishna | Complete | In progress | |||
| Tuberculous pericarditis | Assigned | Fahime | Complete | In progress | |||
| Ventricular septal defect | Assigned | Huda | Complete | In progress | |||
| Ventricular fibrillation | Assigned | Sahar | Complete | In progress | |||
| Long QT syndrome | Assigned | Complete | In progress | ||||
| Angina pectoris | Assigned | Complete | In progress | ||||
| Mitral regurgitation | Assigned | Complete | In progress | ||||
| Pulmonary valve regurgitation | Assigned | Javaria | Complete | In progress | |||
| Preoperative cardiac risk assessment | Assigned | Complete | In progress | ||||
| Percutaneous coronary intervention | Assigned | Complete | In progress | ||||
| Multifocal atrial tachycardia | Assigned | Sara Mohsin | Complete |
Cardiovascular Anatomy
Arteries | Coronary arteries | Head and Neck | Upper Limbs | Torso-Chest | Torso-Abdomen | Lower Limbs | All
Veins | Head and Neck | Upper Extremity | Torso | Lower Extremity
Atria | Atria | Left atrium | Right atrium | Interatrial septum | Musculi pectinati
Ventricles | Ventricles | Left ventricle | Right ventricle | Interventricular septum | Trabeculae carneae | Chordae tendinae | Papillary muscle
Valves | Valves | Aortic valve | Mitral valve | Pulmonic valve | Tricuspid valve | Cusps
Grooves | Coronary/atrioventricular | Interatrial | Anterior interventricular | Posterior interventricular
Surfaces | Sternocostal | Diaphragmatic
Right heart | Vena cavae | Coronary sinus | Right atrium | Right auricle | Fossa ovalis | Limbus of fossa ovalis | Crista terminalis | Valve of the inferior vena cava | Valve of the coronary sinus | Tricuspid valve | Right ventricle | Conus arteriosus | Moderator band/septomarginal trabecula | Pulmonary valve | Pulmonary artery | Pulmonary circulation
Left heart | Pulmonary veins | Left atrium | Left Auricle | Mitral valve | Left ventricle | Aortic valve | Aortic sinus | Aorta | Systemic circulation
Pericardium | Pericardium | Fibrous pericardium | Serous pericardium | Pericardial cavity | Epicardium/visceral layer | Pericardial sinus
Myocardium | Myocardium | Endocardium | Cardiac skeleton | Fibrous trigone | Fibrous rings
Conduction system | Conduction system | Cardiac pacemaker | SA node | AV node | Bundle of His | Purkinje fibers
PHYSIOLOGY
Cardiovascular Physiology
Volumes | Preload | Afterload | End-systolic volume | End-diastolic volume | Frank-Starling law of the heart | Cardiac output
Interactions | Wiggers diagram | Pressure volume diagram
Tropism | Chronotropy | Dromotropy | Inotropy
Hemodynamics | Hemodynamics | Baroreflexes | Kinin-kallikrein system | Renin-angiotensin system | Vasoconstrictors | Vasodilators | Compliance | Vascular resistance
Conduction | Electrical conduction system of the heart | Cardiac action potential
Cardiopulmonary | Respiratory physiology | Blood | Pulmonary circulation | Perfusion (Q) | Hypoxic pulmonary vasoconstriction | Pulmonary shunt | Ventilation/perfusion scan | ventilation/perfusion ratio (V/Q) | Zones of the lung | Gas exchange | Pulmonary gas pressures | Alveolar gas equation | Hemoglobin | Oxygen-haemoglobin dissociation curve | 2,3-DPG | Bohr effect | Haldane effect | Carbonic anhydrase | Chloride shift | Oxyhemoglobin | Respiratory quotient | Arterial blood gas | Diffusion capacity | Dlco
DEVELOPMENTAL BIOLOGY
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Assistant Editor(s)-in-Chief: Rim Halaby
Key Words
Listed in alphabetical order:
- Angiotensin
- Aortic body
- Autoregulation
- Baroreceptor
- Baroreflex
- Blood pressure
- Blood vessel
- Cardiac action potential
- Cardiac output
- Cardiac pacemaker
- Carotid body
- Central venous pressure
- Chronotropic
- Compliance
- Diastolic pressure
- Dromotropic
- Ejection fraction
- Electrical conduction system of the heart
- Electrocardiogram
- End-diastolic volume
- End-systolic volume
- Fick’s law of diffusion
- Frank-Starling law of the heart
- Heart
- Heart rate
- Inotropic
- Juxtaglomerular apparatus
- Mean arterial pressure
- Microcirculation
- Poiseuille’s law
- Pressure volume diagram
- Pulse pressure
- Renin
- Renin-angiotensin system
- Skeletal-muscle pump
- Starling equation
- Stroke volume
- Systolic pressure
- Total peripheral resistance
- Wiggers diagram
Cardiovascular Development
Arteries | Dorsal aorta | Aortic arches | Vitelline arteries | Ductus arteriosus | Umbilical artery
Veins | Cardinal veins | Ducts of Cuvier | Vitelline veins | Ductus venosus | Umbilical vein
Heart Development | Primitive heart tube | Truncus arteriosus | Bulbus cordis | Primitive ventricle | Primitive atrium | Sinus venosus | Septum primum | Ostium primum | Ostium secundum | Septum secundum | Foramen ovale | Endocardial cushions | Septum intermedium | Aorticopulmonary septum | Atrial canal
BASIC SCIENCE
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]
Overview
The heart is the first functional organ in a vertebrate embryo. There are 5 stages to heart development.
Specification of cardiac precursor cells

The lateral plate mesoderm delaminates to form two layers: the dorsal somatic (parietal) mesoderm and the ventral splanchnic (visceral) mesoderm. The heart precursor cells come from the two regions of the splanchnic mesoderm called the cardiogenic mesoderm. These cells can differentiate into endocardium which lines the heart chamber and valves and the myocardium which forms the musculature of the ventricles and the atria.
The heart cells are specified in anterior mesoderm by proteins such as Dickkopf-1, Nodal, and Cerberus secreted by the anterior endoderm. Whether Dickkopf-1 and Nodal act directly on the cardiac mesoderm is the subject of research, but it seems that at least they act indirectly by stimulating the production of additional factors from the anterior endoderm. These early signals are essential for heart formation such that removal of the anterior endoderm blocks heart formation. Anterior endoderm is also sufficient to stimulate heart differientation since it can induce non-cardiogenic mesoderm from more posterior positions in the embryo to form heart.
The secretion of Wnt inhibitors (such as Cerberus, Dickkopf and Crescent) by the anterior endoderm also prevents Wnt3a and Wnt8 secreted by the neural tube from inhibiting heart formation. The notochord secretes BMP antagonists (Chordin and Noggin) to prevent formation of cardiac mesoderm in inappropriate places.
Other cardiogenic signals such as BMP and FGF activate the expression of cardiac specific transcription factors such as homeodomain protein Nkx2.5. Nkx2.5 activates a number of downstream transcription factors (such as MEF2 and GATA) which activate the expression of cardiac muscle specific proteins. Mutations in Nkx2.5 result in heart development defects and congenital heart malformations.
Migration of cardiac precursor cells and fusion of the primordia

The cardiac precursor cells migrate anteriorly towards the midline and fuse into a single heart tube. Fibronectin in the extracellular matrix directs this migration. If this migration event is blocked, cardia bifida results where the two heart primordia remain separated. During fusion, the heart tube is patterned along the anterior/posterior axis for the various regions and chambers of the heart.
Heart looping

The heart tube undergoes right-ward looping to change from anterior/posterior polarity to left/right polarity. The detailed mechanism is unknown however the looping requires the asymmetrically localized transcription factor Pitx2. It is possible that the asymmetry is caused by the clockwise rotation of cilia in dispersing this transcription factor. Looping also depends on heart specific proteins activated by Nkx2.5 such as Hand1, Hand2, and Xin.
Heart chamber formation

The cell fates of the heart chambers are characterized before heart looping but can not be distinguished until after looping. Hand1 is localized to the left ventricle while Hand2 is localized to the right ventricle.
Septation and valve formation
Proper positioning and function of the valves is critical for chamber formation and proper blood flow. The endocardial cushion serves as a makeshift valve until then.
Embryofetal Heart Rates

The human heart beats more than 3.5 billion times in an average lifetime.
The human embryonic heart begins beating approximately 21 days after conception, or five weeks after the last normal menstrual period (LMP), which is the date normally used to date pregnancy. The human heart begins beating at a rate near the mother’s, about 75-80 beats per minute (BPM). The embryonic heart rate (EHR) then accelerates linearly for the first month of beating, peaking at 165-185 BPM during the early 7th week, (early 9th week after the LMP). This acceleration is approximately 3.3 BPM per day, or about 10 BPM every three days, an increase of 100 BPM in the first month.[1]
After peaking at about 9.2 weeks after the LMP, it decelerates to about 150 BPM (+/-25 BPM) during the 15th week after the LMP. After the 15th week the deceleration slows reaching an average rate of about 145 (+/-25 BPM) BPM at term. The regression formula which describes this acceleration before the embryo reaches 25 mm in crown-rump length or 9.2 LMP weeks is:
Age in days = EHR(0.3)+6
There is no difference in male and female heart rates before birth.[2]
References
- ↑ http://www.obgyn.net/us/us.asp?page=/us/cotm/0001/ehr2000
- ↑ Terry J. DuBose http://www.obgyn.net/english/pubs/features/dubose/ehr-age.htm Sex, Heart Rate and Age]
Template:Developmental biology Template:Development of circulatory system
Cardiovascular Biochemistry
Molecular Biology | Biochemistry | Organic Chemistry | Enzymes | Immunology
DIAGNOSTIC MODALITIES IN CARDIOLOGY
The Patient History in Cardiovascular Disease
Chest Pain | Claudication | Cough | Dyspnea | Orthopnea | Palpitations | Paroxysmal Nocturnal Dyspnea | Pedal Edema
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]
The cardinal symptoms of cardiac disease are shown below. Click on the link in blue to read about a component of the patient history in detail.
Discomfort in the chest which can be squeezing, a heaviness, a tightness, a burning or an aching.
Recurring burning, aching, fatigue, or heaviness in the leg muscles with predictable level of walking, that resolves with a predictable duration of rest.
- Cough is defined as being a reflex explosive expiration that promotes the removal of secretions and foreign particles from the lungs, while preventing aspiration
- Coughing can take on two forms:
- Nonproductive
- Productive
- A cough can either be chronic or acute (coughing lasting less than three weeks)
- The production of sputum is important when assessing a cough
- The quality, quantity and circumstances of the sputum production surrounding the coughing episodes are also important
Dyspnea is an uncomfortable awareness of breathing, shortness of breath, or difficulty or distress in breathing. It is often associated with cardiac or pulmonary disease.
Orthopnea is dyspnea which occurs when lying flat, causing the person to have to sleep propped up in bed or sitting in a chair. Orthopnea is generally a symptom of heart failure. It can also occur in those with asthma and chronic bronchitis, as well as those with sleep apnea or panic disorder. The condition is often due to left ventricular failure and/or pulmonary edema. It is also associated with Polycystic Liver Disease. Patients with orthopnea often complain of waking up suddenly during the night ‘unable to breathe’ if they have slipped down from their pillows into the supine position. They may run to the window to ‘get some air’. It is commonly measured according to the number of pillows needed to prop the patient up to enable breathing (Example: “3 pillow orthopnea”). See also: Paroxysmal Nocturnal Dyspnea which means that a patient wakes up short of breath.
Paroxysmal nocturnal dyspnea (PND) is a medical symptom wherein people with congestive heart failure develop difficulties breathing after lying flat. PND commonly occurs several hours after a person with heart failure has fallen asleep. PND resolves quickly once a person awakens and sits upright.
PND is caused by increasing amounts of fluid entering the lung during sleep and filling the small, air-filled sacs (alveoli) in the lung responsible for absorbing oxygen from the atmosphere. This fluid typically rests in the legs during the day when the individual is walking around and redistributes throughout the body (including the lungs) when recumbent. PND is a sign of severe heart failure
The Physical Examination in Cardiovascular Disease
The Pulse | The Neck | The Heart | Lungs | The Extremities
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]
The cardinal symptoms of cardiac disease are shown below. Click on the link in blue to read about a component of the patient history in detail.
The Electrocardiogram
Intervals | PR Interval | QRS Interval | QT Interval | T Wave | U Wave
Hypertrophy | Electrocardiographic Findings in LVH | Electrocardiographic Findings in Right Ventricular Hypertrophy (RVH) | Biventricular Hypertrophy
Bundle Branch Block | LBBB | LAHB | RBBB | Trifascicular block
Atrial Arrhythmias | Premature Atrial Contractions (PACs) | Ectopic Atrial Rhythm | Paroxysmal Atrial Tachycardia (PAT) | Paroxysmal Atrial Tachycardia (PAT) with Block | Multifocal Atrial Tachycardia (MAT) | Atrial Flutter | Atrial Fibrillation
Ventricular Arrhythmias | Differential Diagnosis of Tachycardia with a Wide QRS Complex | Accelerated Idioventricular Rhythm | Ventricular Parasystole | Premature Ventricular Contractions | Ventricular Tachycardia Including Torsades De Pointes and Polymorphic Ventricular Tachycardia
Conduction Abnormalities | First Degree AV Block | Second Degree AV Block | Complete or Third-Degree AV Block | Concealed conduction | AV Junctional Rhythms | Wolff-Parkinson-White Syndrome
Electrocardiographic Abnormalities in Different Disease States | The EKG in the Patient with an Atrial Septal Defect (ASD) | EKG Changes of Hypothermia | EKG Abnormalities in CNS Disease | The EKG of Cardiac Transplantation | The EKG in a Patient with a Pacemaker | Electrocardiography of Traumatic Heart Disease
Drug Effects on the EKG | Digitalis | Quinidine | Procainamide | Disopyramide | Lidocaine | Tocainide and Mexiletine | Phenytoin | Encainide, Flecainide and Propafenone | β-blockers | Amiodarone | Bretylium | Ca Channel Blockers | Adenosine | Phenothiazines | Tricyclic Antidepressants | Lithium
EKG in Electrolyte Disturbances | The EKG in Hyperkalemia | The EKG in Hypokalemia | The EKG in Hypercalcemia | The EKG in Hypocalcemia | Nonspecific ST-Segment and T-Wave Changes
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Assistant Editor-in-Chief: Rim Halaby
Fundamentals of EKG
Basic Principles of Interpretation of an EKG
- Introduction to EKG
- How to read an EKG
- Normal sinus rhythm
- QRS axis and voltage
- Overall overview on electrocardiography
EKG Complexes
EKG Intervals
Abnormal Findings on the EKG
- Delta wave
- H wave
- K wave
- Low QRS voltage
- Nonspecific ST-segment and T-wave changes
- NSSTW changes
- Osborn wave
- P wave alternans
- Poor R wave progression
- PR interval alternans
- QRS complex alternans
- QT prolongation
- Retrograde P wave
- Sine wave pattern
- T wave alternans
- T wave inversion
- Tombstone ST elevation
- U wave
Conduction System
Tachyarrhythmias
Atrial Arrhythmias
- Atrial fibrillation
- Atrial flutter
- Ectopic atrial rhythm
- Multifocal atrial tachycardia (MAT)
- Paroxysmal atrial tachycardia (PAT) with block
- Premature atrial contractions (PAC)
- Sinus tachycardia
- Supraventricular tachycardia
- Wandering atrial pacemaker
Ventricular Arrhythmias
- Accelerated idioventricular rhythm
- Ventricular fibrillation
- Ventricular parasystole
- Ventricular tachycardia
- Wide complex tachycardias
Bradycardia and Conduction Abnormalities
- Sinus bradycardia
- First degree AV block
- Second degree AV block
- Complete or third-degree AV block
- Concealed conduction
- AV junctional rhythms
- Wolff-Parkinson-White syndrome
- Left bundle branch block
- Right bundle branch block
- Trifascicular block
EKG Findings in Diseases
Cardiac Hypertrophy and Dilatation
- Left ventricular hypertrophy (LVH)
- Right ventricular hypertrophy (RVH)
- Biventricular hypertrophy
- Left atrial enlargement
- Right atrial enlargement
- Biatrial enlargement
Acute Myocardial Infarction
Pre-excitation Syndromes
Cardiomyopathies
Congenital Heart Diseases
- Dextrocardia
- Atrial septal defect
- Ventricular septal defect
- Tetralogy of Fallot
- The heart in conjoined twins
- Congenital heart block
Inherited Diseases
Other Heart Diseases
EKG in Other Disease States
EKG Abnormalities in Electrolyte Disturbances
EKG Abnormalities in Normal Pregnancy (Physiological Changes)
- Left axis deviation
- Right axis deviation
- Q wave in lead III
- T wave inversion
- Increased R/S ratio in V1 and V2
- ST-segment depression (usually after anesthesia for C-section)
Drug Effects on the EKG
- Adenosine
- Amiodarone
- β-blockers
- Bretylium
- Calcium channel blockers
- Digitalis
- Disopyramide
- Encainide
- Flecainide
- Lidocaine
- Lithium
- Phenothiazines
- Phenytoin
- Procainamide
- Propafenone
- Quinidine
- Tocainide
- Tricyclic antidepressants
Technical Issues and Potential Errors in Interpretation
- EKG Artifacts
- EKG lead placement errors
- EKG in a patient with a pacemaker
- EKG in athletes
- Persistent juvenile T-wave pattern
- Postprandial EKG changes
Additional Information
Exercise Stress Testing
Editor(s)-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Ernest Gervino, Ph.D.; Brenna Southern, M.D.; Kapil Kumar, M.D.; Bruce D. Nearing, Ph.D.; Richard L. Verrier, Ph.D.
To read more about Exercise Tolerance Test Time as an Endpoint for Clinical Trials Evaluating Therapies for Refractory Angina, click here.
Overview
An exercise stress test (EST) is an evaluation modality used in cardiology in which the ability of the heart to respond to stress, either actually induced by exercise or stimulated by pharmacologic maneuvers, is measured in a controlled clinical setting. The image created by its recording is known as an electrocardiogram or ECG.
The test is typically included in the initial evaluation of suspected ischemic heart disease, and as a prognostic indicator after myocardial infarction.[1]
Exercise EKG
Strengths:
- Low cost
- Short duration
- Functional status evaluation
- High sensitivity in 3 VD or left main disease
- Useful prognostic information
Limitations:
- Sub-optimal sensitivity in the detection of single vessel disease (50%), 85% in the presence of three vessel disease
- In all patients, overall sensitivity 68%, specificity 77%
- Beta blocker use is associated with a higher rate of false negatives (fail to achieve rate pressure product)
- Non diagnostic in patients with abnormal baseline EKG (dig, LVH, WPW)
- Poor specificity in certain patient populations: premenopausal women, LVH, dig, IVCD, hypokalemia, hyperventilation, severe hypertension, resting ST abnormalities
- The negative predictive value in women of low to intermediate risk is high, the positive predictive value in men is high
- Need to achieve > 85% of maximum heart rate for maximizing accuracy
- Its main values lies in excluding CAD in patients with a low pre-test probability of CAD based on gender and age.
Stress Radionuclide Myocardial Perfusion Imaging
Strengths:
- Simultaneous evaluation of perfusion and function with gated SPECT
- Higher sensitivity and specificity than exercise EKG: For exercise or pharmacologic SPECT imaging with Tl or Tc, in patients with chest pain the sensitivity for the detection of CAD is 85% to 90%. Specificity for excluding CAD is in the 90% range. Good in patients with LVH, dig, IVCD etc. ST segment depression response higher rate pressure product than does a perfusion abnormality with tracers. Therefore they are more sensitive. Adding stress perfusion imaging to the exercise ECG stress test greatly assists in differentiating true positive from false positive ETT ST segment depression. For single vessel disease, the sensitivity is 25% higher with SPECT imaging compared with exercise testing. The sensitivity for detecting 3VD with exercise SPECT is 95% to 100%.
- High specificity with Tc labeled agents: Half life is shorter than Tl, therefore dose is higher, therefore image is brighter and better. Also allows gated assessment of LV thickening.
- Studies can be performed in almost all patients
- Significant additional prognostic information, can quantitate LV function
- Comparable accuracy with pharmacologic stress testing
- Viability and ischemia when assessed simultaneously
- Quantitative image analysis
Limitations:
- Suboptimal specificity with thallium imaging, with a high false positive rate in many labs, particularly among women and obese patients.
- Long procedure time with Tc agents, higher costs than ETT
- Radiation exposure
- Poor images in obese patients
- Pharmacologic stress testing: sensitivity and specificity are similar for persantine and adenosine. Dobutamine is used in those patients with a history of bronchospasm, or for those patients who have consumed coffee before the procedure. Pharmacologic testing is the preferred method in patients with LBBB.
- Women with chest pain who are referred for exercise or pharmacologic stress testing benefit the most from the enhanced accuracy of Tc imaging. Both Tl and Tc had a sensitivity of about 70%, but the specificity rose to 92% with Tc. Most labs now use Tc because of its improved specificity, the ability to gait the images and assess regional wall thickening. Mild non reversible defects that show preserved systolic thickening usually represent attenuation artifacts, however, if there is abnormal wall thickening, then this is most likely scar.
Exercise/Pharmacologic Stress Echocardiography
Strengths:
- Higher sensitivity and specificity than exercise EKG: Metanalysis showed sensitivity of 84%, specificity 86%. Marked variation across trials though, highly operator dependent. If the max heart rate is < 85% of age predicted, then sensitivity drops to 42%. Sensitivity is 10% lower in women than in men, specificity is the same across genders. In women with single vessel disease the sensitivity was only 40%, if there was 2 or 3 vessel disease, this number increased to 60%.
- Additional prognostic value over exercise EKG
- Dobutamine stress has higher sensitivity than does pharmacologic stress
- Time to complete examination is short
- Identification of co-existent structural cardiac abnormalities (valvular disease)
- Simultaneous evaluation of perfusion with contrast agents
- Relatively lower costs than with other techniques
- No radiation
Limitations:
- Decreased sensitivity for the detection of single vessel disease or mild stenosis with post exercise imaging
- Inability to image the entire ventricle in some patients
- Highly operator dependent in the analysis of images
- No quantitative image analysis
- Poor windows in patients with COPD
- Infarct zone ischemia less well detected
Comparison of exercise SPECT imaging and Exercise Echocardiography
- Both have a higher sensitivity and specificity than regular exercise EKG testing
- Both provide functional information that EKG testing does not
- Both provide information about myocardial viability, which the angiogram does not
Strengths of Stress ECHO over SPECT
Noninvasive, safe and repeatable, no radiation exposure, quick, little sophisticated equipment and portable, low costs, can identify co-existing valvular heart disease
Limitations of Stress ECHO over SPECT
Images are difficult to obtain at peak exercise, an ischemic response is required to observe wall motion abnormalities, wall motion can recover quickly in the presence of mild ischemia, detection of residual ischemia is difficult in an akinetic wall zone, the technique is highly operator dependent, good quality images were only acquired in 70% of cases.
Strengths of SPECT over stress ECHO
Does not require an ischemic response to be abnormal, just requires an abnormality in flow reserve, sensitivity is slightly higher by about 8-10 percentage points (mostly because the ability to detect single vessel disease or mild stenoses of 50-70% is not as good with stress Echo), can see defects in areas that contain scar and viable myocardium, acquisition of images is not operator dependent, in virtually 100% of patients diagnostic images are obtained, with Tc simultaneous assessment of perfusion and function is obtained, resting LV ejection fraction can be obtained, vasodilator SPECT has significantly higher sensitivity than vasodilator stress ECHO, dobutamine ECHO is associated with higher sensitivity and specificity than vasodilator ECHO.
Limitations of SPECT imaging in relation to stress ECHO
Longer imaging protocols, greater expense of equipment, must inject and store radiopharmaceuticals, inability to visualize the heart in real time, lower spatial resolution than ECHO, higher costs to patients.
In general, the sensitivity is lower for stress ECHO while the specificity is higher.
Prognosis
Exercise Tolerance Testing
- 1 mm or more of horizontal or downsloping ST depression is associated with a poor prognosis
- Failure to achieve 6 METS is associated with an elevated mortality rate over the next 2.5 years.
- Failure of heart rate to rise is associated with higher mortality, even after adjusting for perfusion defects.
- Failure to reach 85% of age adjusted max HR is associated with a RR of 1.85 in mortality.
- Limitation of ETT is the fact that the magnitude of ST depression is not strongly associated with the extent of CAD
- Exercise testing alone has excellent prognostic ability among patients with atypical chest pain or non anginal pain who have a normal EKG at baseline. If these patients have a normal ETT, the prognosis is excellent.
Stress Myocardial Perfusion
- The following are associated with a poor prognosis:
- 20% of the LV is a perfusion defect
- Defects in more than one distribution suggestive of multivessel CAD
- A large number of non reversible defects
- Transient LV cavitary dilation
- Increased lung uptake
- Resting LVEF of < 40%
- Normal thallium: Mortality 1% per year
- Normal Tc: annual mortality 0.6%, 12 fold higher if there is a Tc defect
- The positive predictive value of stress myocardial perfusion imaging and stress ECHO is low: That is the percentage of people who die or sustain an MI is low among patients with abnormal findings. On the other hand the negative predictive value is high and exceeds 95%.
Non Invasive Risk Stratification According to the ACC Appropriate Use Criteria
| “ |
High-Risk (greater than 3% annual mortality rate)1. Severe resting left ventricular dysfunction (LVEF less than 35%) 2. High-risk treadmill score (score less than or equal to 11) 3. Severe exercise left ventricular dysfunction (exercise LVEF less than 35%) 4. Stress-induced large perfusion defect (particularly if anterior) 5. Stress-induced multiple perfusion defects of moderate size 6. Large, fixed perfusion defect with LV dilation or increased lung uptake (thallium-201) 7. Stress-induced moderate perfusion defect with LV dilation or increased lung uptake (thallium-201) 8. Echocardiographic wall motion abnormality (involving greater than two segments) developing at low dose of dobutamine (less than or equal to 10 mg/kg/min) or at a low heart rate (less than 120 beats/min) 9. Stress echocardiographic evidence of extensive ischemia Intermediate-Risk (1% to 3% annual mortality rate)1. Mild/moderate resting left ventricular dysfunction (LVEF equal to 35% to 49%) 2. Intermediate-risk treadmill score (11 less than score less than 5) 3. Stress-induced moderate perfusion defect without LV dilation or increased lung intake (thallium-201) 4. Limited stress echocardiographic ischemia with a wall motion abnormality only at higher doses of dobutamine involving less than or equal to two segments Low-Risk (less than 1% annual mortality rate)1. Low-risk treadmill score (score greater than or equal to 5) 2. Normal or small myocardial perfusion defect at rest or with stress* 3. Normal stress echocardiographic wall motion or no change of limited resting wall motion abnormalities during stress* |
” |
Techniques used to Assess Myocardial Viability
Tl Imaging:
Rest and delayed redistribution is the most common radionuclide method used to assess viability. Uptake of Tl is related not only to blood flow, but also to membrane integrity. Myocardial stunning or hibernation does not result in a reduction in Tl extraction as long as the sarcolemmal membrane does not sustain irreversible ischemic damage. 60 to 70% of asynergistic segments will show > a 50% improvement after revascularization.
Tc Imaging:
Same as above, as usual a better signal with Tc, can also assess regional wall thickening. If thickening is present, then viability is likely.
PET:
- Considered by many to be the gold standard. Can be used to assess perfusion and metabolism simultaneously. If there is mismatch in perfusion and metabolism, then the tissue is viable. If there is a match, then there is scar.
- Dobutamine: Enhanced systolic contractility with low dose dobutamine is associated with recovery.
Emergent Stress Testing in Young People
Stress testing has frequently been used to assess adult patients with suspected or known coronary artery disease (CAD) based on pre-test probability. Pre-test probability is the assessment of a patient and their likelihood of CAD based on clinical history and symptoms. Stress testing to diagnose myocardial ischemic syndrome is usually indicated only in patients with an intermediate pre-test probability.[3]
The average age of a patient who undergoes a stress test is typically between 45-60 years. Increasing age is one of many positive risk factors for CAD. However, there have been several cases in which young adults and adolescents have presented with chest pain and were found to have had a myocardial infarction (MI). [4] Since chest pain can be a complaint among children, the question becomes whether or not an emergent stress test is needed.
The most common reason for stress testing is chest pain. All patients who present with acute or chronic chest pain need to be evaluated to determine the course or urgency of further non-invasive vs. invasive testing. Inpatient stress testing can be done if a recent MI or an acute unstable coronary syndrome has been excluded.
Among children presenting with chest pain, the symptoms often tend to be benign. [5] Given the fact that the majority of children have no probable cardiac risk factors, their pre-test probability is already very low. Yet there are several conditions that can cause ischemic chest pain and other cardiac abnormalities so a thorough careful history and physical examination should always be performed. The presenting symptom can be secondary to congenital defects as well as acquired diseases. Kawasaki disease has a common manifestation of coronary artery aneurysms which can progress to coronary stenosis. [6] Acute MI is one of the main causes of death in children with Kawasaki disease. Another acquired condition is sickle cell disease in which children can frequently present with chest pain, have an MI and have normal coronary arteries. [7] Other issues that could cause ischemic chest pain are coronary vasospasm, pericarditis or myocarditis, cocaine use, or other conditions causing anatomic congenital cardiovascular abnormalities.
Acute symptoms in children should be dealt with accordingly to rule out an MI, congenital defects or diseases. Based on above indications, an emergent stress test may not be warranted. To help determine the etiology of the symptom, ECG, echocardiogram, MRI, cardiac enzymes, drug screening, blood testing for hypercoagulability and coronary angiograms may be more useful. Or for chronic chest pain associated with exertion, an outpatient stress test could also be helpful.
Whether or not stress testing is emergent in children should again be considered similarly to adult emergent stress testing. Comprehensive assessment of acute or chronic problems and the consideration of the child’s pre-test probability being significantly low are compelling points that an emergent stress test may not be necessary.
T Wave Alternans for Risk Stratification during Exercise Stress Testing
Across the past decade, a sizeable body of evidence has been amassed indicating that measurement of T wave alternans (TWA), a beat-to-beat fluctuation in the morphology of the T wave, during exercise is useful in assessing risk for life-threatening arrhythmias.
TWA is a marker of repolarization instability and an indicator of a vulnerable myocardial substrate. This electrocardiographic phenomenon parallels the beat-to-beat oscillation of action potential duration (APD) at the level of cardiac myocytes. The cellular mechanism has been linked primarily to an aberration in intracellular calcium, which results in fluctuation of calcium transients from one beat to the next. This oscillation in APD can be solely a temporal event (concordant alternans) or both a temporal and spatial occurrence (discordant alternans). Discordant alternans has the potential to create steep repolarization gradients leading to transient unidirectional block, a pre-requisite for reentrant arrhythmias [8] [9]
Until recently, TWA analysis has largely involved frequency-domain based spectral analysis. The spectral method (SM) requires provocative testing to raise and plateau the heart rate. The level of TWA detected is in the range of a few microvolts and thus cannot be observed by visual inspection. SM is the first and most widely studied commercially available algorithm (Cambridge Heart, Inc.). It employs a fast Fourier transformation of the electrocardiogram (ECG) across 128 consecutive beats into the frequency domain and employs specialized electrodes to minimize noise. The power of the spectrum at 0.5 cycle per beat (occurring on every other beat) between the JT segment is defined as the alternans power. An alternans level (Valt) >1.9 μV, greater than 3 times the standard deviation of noise (k score), and sustained for at least one minute at stable heart rates <110 beats per minute is considered a positive test, indicating that TWA is present. A negative test is defined as one that has a Valt of <1.9 μV at a heart rate >105 bpm without significant noise or premature beats. Tests that do not strictly meet the positive or negative test definitions are referred to as indeterminate [10] and occur in 20 to 40% of all cases. Most recent studies using SM have grouped positive and indeterminate tests together as “abnormal” or “non-negative,” since the risk of death or sustained ventricular arrhythmias in patients with indeterminate tests due to patient factors is as high as that of patients with positive tests. [11]
A recently developed, FDA cleared commercial method (GE Healthcare, Inc.) is time domain modified moving average (MMA) developed at Beth Israel Deaconess Medical Center (Nearing and Verrier 2002). This technique was developed to circumvent the stationarity requirements of SM, which mandates stabilization of heart rate for several minutes given the fast Fourier transform. The requirement for specialized electrodes is also eliminated through the use of advanced noise reduction algorithms. The MMA method separates odd and even beats into separate bins and creates median templates for both the odd and even complexes every 15 seconds. [12] These templates are then superimposed and the entire JT segment is analyzed for alternation. The peak difference between the odd and even median complexes at any point within the JT segment is defined as the TWA value. These templates of superimposed complexes may be examined visually to verify TWA presence and magnitude. Noise measurements are in part derived from mismatch of the median templates outside of the JT segment. The moving average allows control of the influence of new incoming complexes on the median templates with an adjustable update factor. A lower update factor provides greater sensitivity in detecting transient surges in TWA.
Results from SM and MMA are highly comparable, although the TWA values reported with the MMA algorithm are consistently larger by a factor of 4 to 10. This difference is mainly attributable to the fact that SM reports the average TWA level across the entire JT segment for 128 beats that is above the noise level, while MMA method reports the peak TWA level at any point within the JT segment for each 15-second beat stream, with the noise level reported separately.
The majority of clinical studies focusing on TWA as a risk stratification tool have enrolled CAD patients with EF 40% and employed the SM. In 2005, Gehi and colleagues [13] conducted a meta-analysis of 19 prospective studies of exercise-based TWA testing with SM that enrolled a total of 2608 patients. The majority of these patients had CAD, and half had depressed EF, but only a small percentage had a history of ventricular arrhythmias. Positive TWA test results conveyed an average 3.77-fold risk of future ventricular tachyarrhythmic events when compared to patients with negative TWA test results. The negative predictive value (NPV) of TWA was 97.2%. However, its positive predictive value (PPV) was quite poor, generally <30% for all subgroups.
By virtue of its excellent NPV, TWA testing has been presented as a means of identifying those patients who are least likely to experience a future ventricular tachyarrhythmic event and thus least likely to benefit from ICD implantation.
Only one large prospective observational trial has investigated TWA in a broader population. The incidence of SCD in this subgroup of patients, however, is relatively low; rendering it even more difficult to identify those most likely to benefit from ICD implantation even though the absolute number of SCD events is higher in this population than in those with depressed EF. [14] Nieminen and coworkers (2007) provided evidence that TWA is also suitable as a screening tool in the general population of patients with preserved ejection fraction and can be performed during routine exercise stress testing. They applied the MMA method in 1037 consecutive patients referred for exercise testing and reported that TWA 65μV recorded in the precordial leads predicted all-cause death (RR= 3.3), cardiovascular mortality (RR=6.0), and sudden cardiac death (RR=7.4) across the 44 ±7 month follow-up. The analysis window was restricted to heart rates 125 beats/min in order to minimize the effects of noise.
Most recently, the REFINE study [15] enrolled 322 post-MI patients with ejection fraction 50% and measured TWA at 10 to 14 weeks. Spectral analysis was performed during the specialized exercise protocol, and MMA was employed during post-exercise recovery. Exner and colleagues (2007) determined that the predictivity of the spectral and MMA methods for TWA analysis is similar, with hazard ratios in the range of 2.75-2.94 for cardiac death or arrest during 47 months following the index event. Combining the TWA test results with heart rate turbulence, a noninvasive marker of autonomic tone, accurately predicted risk of cardiac death or arrest with a hazard ratio of 5.2 and identified the majority of patients destined to suffer serious events.
Collectively, sound scientific and clinical evidence support the utility of TWA testing for sudden death risk stratification during exercise. With the advent of time-domain based TWA analysis, this measurement can be performed seamlessly during the course of routine clinical exercise stress testing as well as ambulatory ECG monitoring. While TWA testing has been focused largely on guiding ICD implantation for primary prevention, there may be a greater role for TWA analysis in screening the broader, low-risk population and for evaluating the effectiveness of medical therapy.
Since sudden cardiac death results from diverse pathologic mechanisms, involving derangements in myocardial substrate and altered autonomic function, it is unlikely that any single parameter will adequately represent the complex factors that lead to lethal ventricular arrhythmias. Therefore, it will be valuable to examine whether combinations of several risk stratification parameters may be more effective than any individual parameter as observed in the REFINE study.[16]
Related chapters
- Electrocardiogram
- Cardiology
- Myocardial infarction
- Emergent Stress Testing in Young People [2]
- T Wave Alternans for Risk Stratification during Exercise Stress Testing [3]
Additional Resources
- Modified Gervino Protocol
- Emergent Stress Testing in Young People [4]
- T Wave Alternans for Risk Stratification during Exercise Stress Testing [5]
References
- ↑ Sabatine, Marc (February 15, 2000). Pocket Medicine. Lippincott Williams & Wilkins. pp. 256 pages.
- ↑ 2008.10.005 J. Am. Coll. Cardiol. 2009;53;530-553.
- ↑ Gibbons, RJ, Balady, GJ, Bricker, JT, et al. ACC/AHA 2002 guideline update for exercise testing: summary article: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation 2002; 106:1883.
- ↑ Kocis, KC. Chest pain in pediatrics. Pediatr Clin North Am 1999; 46:189.
- ↑ Lane, JR, Ben-Shachar, G. Myocardial Infarction in Healthy Adolescents. Pediatrics 2007; 120 No.4: 938
- ↑ Taubert, KA, Shulman, ST. Kawasaki Disease. Am Fam Physician 1999; 59 No.11: 3093
- ↑ Martin, CR, Johnson, CS, Cobb, C, et al. Myocardial infarction in sickle cell disease. J Natl Med Assoc 1996; 88:428.
- ↑ Narayan SM: T-wave alternans and the susceptibility to ventricular arrhythmias. J Am Coll Cardiol 2006, 47: 269-281.
- ↑ Nearing BD, Verrier RL: Tracking heightened cardiac electrical instability by computing interlead heterogeneity of T-wave morphology. J Appl Physiol 2003, 95:2265-2272.
- ↑ Bloomfield DM, Hohnloser SH, Cohen RJ: Interpretation and classification of microvolt T wave alternans tests. J Cardiovasc Electrophysiol 2002, 13:502-512.
- ↑ Kaufman ES, Bloomfield DM, Steinman RC, et al: “Indeterminate” microvolt T-wave alternans tests predict high risk of death or sustained ventricular arrhythmias in patients with left ventricular dysfunction. J Am Coll Cardiol 2006, 48:1399-1404.
- ↑ Nearing BD, Verrier RL: Modified moving average method for T-wave alternans analysis with high accuracy to predict ventricular fibrillation. J Appl Physiol 2002, 92:541-549.
- ↑ Gehi AK, Stein RH, Metz LD, Gomes JA: Microvolt T-wave alternans for the risk stratification of ventricular tachyarrhythmic events: a meta-analysis. J Am Coll Cardiol 2005, 46:75-82.
- ↑ Huikuri HV, Castellanos A, Myerburg RJ: Sudden death due to cardiac arrhythmias. N Engl J Med 2001, 345:1473-1482.
- ↑ Exner DV, Kavanagh KM, Slawnych MP, et al, for the REFINE Investigators: Noninvasive Risk Assessment Early After a Myocardial Infarction. The Risk Estimation Following Infarction, Noninvasive Evaluation (REFINE) Study. J Am Coll Cardiol 2007, 50:2275-84.
- ↑ Kumar K, Kwaku KF, Verrier RL. Treatment Options for Patients with Coronary Artery Disease Identified as High-Risk by T-Wave Alternans Testing. In: Current Treatment Options in Cardiovascular Medicine 2008, in press.
Cardiac Electrophysiology
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Assistant Editor(s)-in-Chief: Rim Halaby; Serge Korjian
Overview
- Cardiac electrophysiology (also referred to as clinical cardiac electrophysiology , or electrophysiology) is the science of the mechanisms, functions, and performance of the electrical activities of specific regions of the heart.
- The normal electrical conduction in the heart allows the impulse that is generated by the sinoatrial node (SA node) of the heart to be propagated to (and stimulate) the myocardium (Cardiac muscle). The myocardium contracts after stimulation. It is the ordered stimulation of the myocardium that allows efficient contraction of the heart, thereby allowing blood to be pumped throughout the body.
Cardiac Conduction System
- Proper cardiac function heavily depends on the ability of the cardiomyocytes to receive and propagate an electrical impulse allowing the heart to contract.
- These impulses, known as action potentials, originate and travel through the cardiac conduction system.
- A time-ordered propagation of the electrical impulse through the myocardium allows efficient contraction of all four chambers of the heart, starting with the atria pumping the blood toward the ventricles, followed by the ventricles which contribute to the pulmonary and systemic circulation.
The Components of the Cardiac Conduction System:
- The sinus (sinoatrial) node
- The internodal tracts
- The atrioventricular (AV) node
- The His/AV bundle
- The right and left bundle branches,
- The Purkinje fibers.
The Direction of Propagation of the Action Potential:
- The initial cardiac impulse, produced by pacemaker cells, originates in the sinoatrial (SA) node at the intersection of the right atrium and the superior vena cava.
- This action potential is the trigger of every cardiac cycle, initiating the atrial then ventricular contractions; it is henceforth responsible for the rhythmic beating of the heart.
- This action potential then propagates as a wave of depolarization through the internodal tracts initiating atrial contraction and then converging at the AV node.
- The convergence occurs because, in a normal heart, the AV node is the only electrical connection between the atria and the ventricles.
- The conduction of this potential is delayed at the AV node mainly due to the slower depolarization in these cells.
- This delay is represented as the PR interval of the ECG.
- The electrical impulse then moves to the ventricles by means of the AV or His bundle located in the superior portion of the interventricular septum.
- It then continues moving apically and propagating through both [[]]ventricles via the right and left bundle branches, and the Purkinje fibers.[1][2][3][4]
-
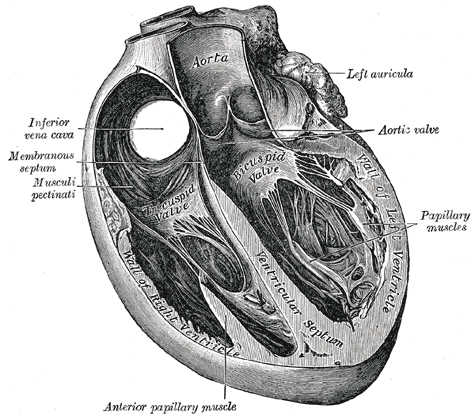 Section of the heart showing the ventricular septum.
Section of the heart showing the ventricular septum. -
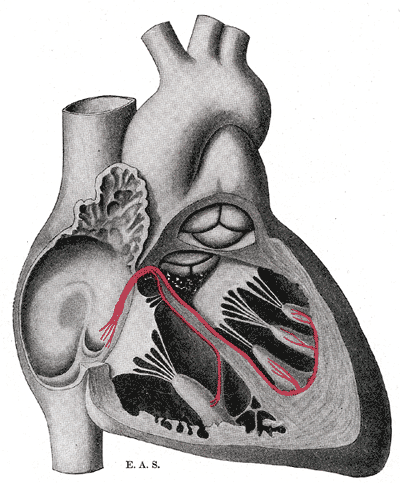 Schematic representation of the atrioventricular bundle of His.
Schematic representation of the atrioventricular bundle of His.


- Similarly to skeletal muscle cells which are also striated muscles, the cardiomyocytes contract in response to a rapid alteration in the cell membrane’s potential.
- However, the cardiomyocytes differ from skeletal muscle cells by three important variations that are essential for cardiac function:
- 1) They can self-generate a change in cell membrane potential.
- 2) The action potential can be transmitted directly from cell to cell.
- 3) The action potentials have a significantly longer duration.
The Resting Membrane Potential
- All cells including cardiomyocytes have a resting membrane potential that is maintained assuming there is no electrical charge crossing the membrane from the intracellular towards the extracellular milieu or vice versa.
- This potential is estimated to be –80 to –90 mV.
- The most crucial ions that determine this resting potential are:
- Sodium (Na+)
- Calcium (Ca2+)
- Potassium (K+)
- Sodium (Na+) and calcium (Ca2+) are most present in the interstitial fluid, while potassium (K+) is more present in intracellularly.
- These ions are lipid insoluble which prevents them from crossing the lipid bilayer or the cell membrane.
- Alternatively, ions cross via specific protein structures in the cell membrane that may be either: ion channels, ion pumps, or ion exchangers.
- These transmembrane proteins are highly specific and allow only one type of ion to pass through which allows good maintenance of the membrane potential.
- Ion channels can be opened, inactivated or closed depending on complex factors that modulate their activity.
The Cardiac Action Potential
- The cardiac contraction action potential is divided into 5 phases.
Phase 0: Depolarization
- The initial rapid increase in the transmembrane potential from -80mV to approximately +30mV constitutes the Phase 0 or the depolarization phase.
- This depolarization results from a rapid increase in the membrane permeability to Na+ ions via opening of voltage-dependent fast Na+ channels allowing Na+ ions to move intracellularly according to their electrochemical gradient.
- Following the conduction of an action potential, a recovery phase is attained where a large number of Na+ channels are inactivated, preventing the conduction of a second action potential.
- When the membrane is fully repolarized, these channels are reactivated and allow the conduction of the following action potential.
Phase I: Initial Repolarization
- The phase I of the action potential, known as the initial rapid repolarization ensues, resulting from K+ and Cl- ion flux across the membrane.
- This forms the notch seen in the action potential following the depolarization.
Phase II: Plateau
- Phase II, almost exclusive to cardiomyocytes, represents a plateau in the membrane potential as an outcome of the equilibrium between Ca2+ influx and K+ outflow.
- The channels responsible for this Ca2+ influx are known as the L-type calcium channels, which are activated rapidly when the membrane potential reaches -50mV, but are slowly inactivated thereafter.
- Throughout this plateau phase, few Na+ channels also remain active.
- These are Na+/Ca2+ exchangers that allow 1 ion of calcium to move outside the cell for every 3 molecules of sodium moving inside the cell.
Phase III: Repolarization
- The third phase, also known as rapid repolarization, depicts the restoration of a resting membrane potential.
- It is initiated by inactivation of the L-type calcium channels and an increase in K+ outflow.
- This change in potassium across the membrane is related to 3 K+ currents:
- 1) Inwardly rectifying K+ current (IK1) à Produces the resting membrane potential
- 2) Transient outward K+ current (ITO) à Accounts for initial part of repolarization
- 3) Delayed outward K+ current (IK) à Responsible for final part of repolarization
- After repolarization has occurred, intracellular Na+ and extracellular K+ are rearranged via the Na+/K+ ATPase pump.
- The ATPase moves 3 sodium ions out for every 2 potassium ions moved intracellularly.
- Equilibrium of ions across the membrane is also achieved via the Na+/Ca2+ exchangers.
Phase IV: Diastolic depolarization
- The phase IV of the action potential is characterized by a diastolic depolarization that is both spontaneous and slow.
- This phase provides cardiac cells with features of automaticity.
- In a normal functioning heart, only the sinoatrial node is able to reach a threshold potential during phase IV making it the pacemaker of the heart.
- Nevertheless other cells including those in the AV node, the His bundle, and the Purkinje fibers are able to reach a threshold and fire automatically if they are not suppressed by the SA node, which is true in some disease entities.
The factors responsible for the initial diastolic depolarization in the SA node are:
- Inward Ca2+ current
- Delayed outward K+ current
- IF Currents – Inward sodium-potassium currents activated if membrane repolarizes below the If threshold
- T-type Ca2+ channel – Releases calcium from internal stores
The rate of impulse generation by the SA node is determined by 3 factors:
- 1) The slope of diastolic depolarization
- 2) The maximal diastolic potential
- 3) The threshold potential
- All these factors are controlled by the autonomic nervous system allowing for the modulation of the rate of SA node firing and subsequently the heart rate.[1][5][3][4]
Electrophysiology Studies and Therapeutic Modalities
Overview
- An electrophysiologic study is a term used to describe a number of invasive (intracardiac) and non-invasive recording of spontaneous electrical activity as well as of cardiac responses to programmed electrical stimulation.
- These studies are performed to assess arrhythmias, elucidate symptoms, evaluate abnormal electrocardiograms, assess risk of developing arrhythmias in the future, and design treatment.
- These procedures increasingly include therapeutic methods (typically radiofrequency ablation) in addition to diagnostic and prognostic procedures.
- Other therapeutic modalities employed in this field include antiarrhythmic drug therapy and implantation of pacemakers and implantable cardioverter-defibrillators.
- A specialist in cardiac electrophysiology is known as a cardiac electrophysiologist, or (more commonly) simply an electrophysiologist. Cardiac electrophysiology is considered a subspecialty of cardiology, and in most countries requires two or more years of fellowship training beyond a general cardiology fellowship. They are trained to perform interventional cardiac EP procedures as well as surgical device implantations.
Diagnostic Testing
- Ambulatory electrocardiographic monitoring (Holter recording and interpretation; loop recording and interpretation)
- Tilt table testing
- Signal-averaged electrocardiogram (SAECG) interpretation, also referred to as “late potentials” reading
- Electrophysiologic study (EPS)
- Pacing and recording electrodes are inserted either in the esophagus (intra-esophageal EPS) or, through blood vessels, directly into the heart chambers (intra-cardiac EPS) in order to measure electrical properties of the heart. In addition, intra-cardiac EPS electrically stimulates the heart and induces arrhythmias for diagnostic purposes (“programmed electrical stimulation”).
Medical Treatment
Electrophysiologists play a role in:
- The initial administration and monitoring of the effect of drugs for treatment of heart rhythm disorders
- The management of severe or life threatening arrhythmias
- The management of arrythmias requiring multiple drugs use
Catheter Ablation
- Ablation therapy is the catheter based creation of lesions in the heart with radiofrequency energy, cryotherapy (destructive freezing), or ultrasound energy in order to cure or control arrhythmias (see radiofrequency ablation). Ablation is usually performed during the same procedure as the electrophysiology study which induces and confirms the diagnosis of the arrhythmia for which ablation therapy is sought.
Non-complex ablation
- It includes ablation for arrhythmias such as: AV nodal reentrant tachycardia, accessory pathway mediated tachycardia and atrial flutter.
- This procedure is usually performed using intracardiac catheters , fluoroscopy (a real-time X-ray camera), and electrical recordings from the inside of the heart.
Complex ablation
- It includes ablation for arrhythmias such as: multifocal atrial tachycardia, atrial fibrillation, and ventricular tachycardia.
- In addition to the apparatus used for a “non-complex” ablation, these procedures often make use of sophisticated computer mapping systems to localize the source of the abnormal rhythm and to direct delivery of ablation lesions.
Surgical Procedures: Pacemaker and Defibrillator Implantation and Follow Up
- Implantation of single and dual chamber pacemakers and defibrillators
- Implantation of “biventricular” pacemakers and defibrillators for patients with congestive heart failure
- Implantation of loop recorders (implanted ECG recorders for long term monitoring of ECG to allow for diagnosis of an arrhythmia)
- Clinical follow up and reprogramming of implanted devices
Abnormalities in Cardiac Electrophysiology
- Mechanism of Arrhythmias
- Diseases of the Conduction System and Bradyarrhythmias
- Narrow Complex Tachycardias
- Wide Complex Tachycardias
- Ventricular Tachyarrhythmias, Cardiac Arrest and Sudden Cardiac Death
- Arrhythmias in Pregnancy
Treatment Modalities for Arrhythmia
- Antiarrhythmic Medications
- Indications for Pacemakers
- Indications for an ICD
- Cardiac Resynchronization Therapy
- Catheter ablation
See also
- Clinical cardiac electrophysiology
- Electrical conduction system of the heart
- Electrocardiogram (EKG)
- Basic Principles of ECG Interpretation
- Electrophysiologic study
- Cardiology
- Cardiac arrhythmia
External links
References
- ↑ 1.0 1.1 David E. Mohrman, L. J. (2010). Cardiovascular Physiology, 7e. The McGraw-Hill Companies, Inc.
- ↑ Kim E. Barrett, S. B. (2012). Ganong’s Review of Medical Physiology, 24e . The McGraw-Hill Companies, Inc.
- ↑ 3.0 3.1 Olson, E. N. (2004). A decade of discoveries in cardiac biology. Nature Medicine, 467 – 474.
- ↑ 4.0 4.1 Valentin Fuster, R. A. (2011). Hurst’s The Heart, 13e. The McGraw-Hill Companies, Inc.
- ↑ Kim E. Barrett, S. B. (2012). Ganong’s Review of Medical Physiology, 24e . The McGraw-Hill Companies, Inc.
Cardiac Biomarkers
Creatine Kinase | Cytokines and their receptors | Lipoprotein-associated phospholipase A2 (Lp-PLA2) | Metalloproteinases (MMPs) | Natriuretic peptides | Prothrombin fragment 1.2 (F1.2) | Prothrombin time (PT) | Soluble CD40 ligand (sCD40L) | Thrombus precursor protein (TpP) | Von Willebrand factor (vWF) | White blood cell (WBC) count
An Overview of Cardiac Imaging
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; David E. Winchester M.D. M.S.
This chapter presents a brief overview of cardiac imaging techniques. For a detailed discussion of each of the imaging technoloies, please view the chapter on that imaging technology.
Assessment of LV function
- Least expensive, most versatile.
- Portable, immediately available
- Preferred initial technique to diagnose heart muscle disease of unknown etiology.
- Regional thickening can be assessed on ECHO and not other techniques and this is a better marker of regional function than is regional wall motion (cant be seen on nuclear or angio studies, MRI can assess though)
- ECHO is not as good at assessing quantitative ejection fraction (SPECT, angio, RVG are better at this).
- More sensitive than EKG in diagnosis of LVH.
- Excellent in estimating LV mass
- Good for quantitating LV and RV EFs. Excellent for following the wall motion in patients treated with chemotherapeutic agents.
- Good for wall motion.
- In MI does not tell you about infarct expansion, MR, LV thrombus, regional thickening abnormalities.
- Permits evaluation of regional thickening, global LV function and myocardial perfusion.
- Good regional and global cardiac function.
- With contrast agents, good perfusion data
- Superior for congenital, aortic disease, anomalous coronary arteries, and RV dysplasia
- Cost benefit ratios of echo and nuclear make them superior for LV function assessment
- May be best technique for quantitating LV mass
- As a research tool may be useful in the assessment of LV remodeling
- Gold standard in the assessment of wall motion but not in the assessment of wall thickening.
- LVEF and absolute volumes are highly reproducible
- LVH and LV mass are better quantitated with echo and MRI
- Left to right shunts are most accurately quantitated with cardiac cath over echo and MRI
Techniques to Assess CAD and Prognosis
- Strengths
- Low cost
- Short duration
- Functional status evaluation
- High sensitivity in 3 VD or left main disease
- Useful prognostic information
- Limitations
- Suboptimal sensitivity in the detection of single vessel disease (50%), 85% in the presence of three vessel disease
- In all patients, overall sensitivity 68%, specificity 77%
- Beta blocker use is associated with a higher rate of false negatives (fail to achieve rate pressure product)
- Non diagnostic in patients with abnormal baseline EKG (dig, LVH, WPW)
- Poor specificity in certain patient populations: premenopausal women, LVH, dig, IVCD, hypokalemia, hyperventilation, severe hypertension, resting ST abnormalities
- The negative predictive value in women of low to intermediate risk is high, the positive predictive value in men is high
- Need to achieve > 85% of maximum heart rate for maximizing accuracy
- Its main values lies in excluding CAD in patients with a low pre test probability of CAD based on gender and age.
- Strengths
- Simultaneous evaluation of perfusion and function with gated SPECT
- Higher sensitivity and specificity than exercise EKG: For exercise or pharmacologic SPECT imaging with Tl or Tc, in patients with chest pain the sensitivity for the detection of CAD is 85% to 90%. Specificity for excluding CAD is in the 90% range. Good in patients with LVH, dig, IVCD etc. ST depression response higher rate pressure product than does a perfusion abnormality with tracers. Therefore they are more sensitive. Adding stress perfusion imaging to the exercise ECG stress test greatly assists in differentiating true positive from false positive ETT ST segment depression. For single vessel disease, the sensitivity is 25% higher with SPECT imaging compared with exercise testing. The sensitivity for detecting 3VD with exercise SPECT is 95% to 100%.
- High specificity with Tc labeled agents: Half life is shorter than Tl, therefore dose is higher, therefore image is brighter and better. Also allows gated assessment of LV thickening.
- Studies can be performed in almost all patients
- Significant additional prognostic information, can quantitate LV function
- Comparable accuracy with pharmacologic stress testing
- Viability and ischemia when assessed simultaneously
- Quantitative image analysis
- Limitations
- Suboptimal specificity with thallium imaging, with a high false positive rate in many labs, particularly among women and obese patients.
- Long procedure time with Tc agents, higher costs than ETT
- Radiation exposure
- Poor images in obese patients
- Pharmacologic stress testing: sensitivity and specificity are similar for persantine and adenosine. Dobutamine is used in those patients with a history of bronchospasm, or for those patients who have consumed coffee before the procedure. Pharmacologic testing is the preferred method in patients with LBBB.
- Women with chest pain who are referred for exercise or pharmacologic stress testing benefit the most from the enhanced accuracy of Tc imaging. Both Tl and Tc had a sensitivity of about 70%, but the specificity rose to 92% with Tc. Most labs now use Tc because of its improved specificity, the ability to gait the images and assess regional wall thickening. Mild non reversible defects that show preserved systolic thickening usually represent attenuation artifacts, however, if there is abnormal wall thickening, then this is most likely scar.
- Strengths
- Higher sensitivity and specificity than exercise EKG: Metanalysis showed sensitivity of 84%, specificity 86%. Marked variation across trials though, highly operator dependent. If the max heart rate is < 85% of age predicted, then sensitivity drops to 42%. Sensitivity is 10% lower in women than in men, specificity is the same across genders. In women with single vessel disease the sensitivity was only 40%, if there was 2 or 3 vessel disease, this number increased to 60%.
- Additional prognostic value over exercise EKG
- Dobutamine stress has higher sensitivity than does pharmacologic stress
- Time to complete examination is short
- Identification of co-existent structural cardiac abnormalities (valvular disease)
- Simultaneous evaluation of perfusion with contrast agents
- Relatively lower costs than with other techniques
- No radiation
- Limitations
- Decreased sensitivity for the detection of single vessel disease or mild stenosis with post exercise imaging
- Inability to image the entire ventricle in some patients
- Highly operator dependent in the analysis of images
- No quantitative image analysis
- Poor windows in patients with COPD
- Infarct zone ischemia less well detected
Comparison of exercise SPECT imaging and Exercise Echocardiography
- Both have a higher sensitivity and specificity than regular exercise EKG testing
- Both provide functional information that EKG testing does not
- Both provide information about myocardial viability, which the angiogram does not
Strengths of Stress ECHO over SPECT
- Noninvasive, safe and repeatable, no radiation exposure, quick, little sophisticated equipment and portable, low costs, can identify co-existing valvular heart disease
Limitations of Stress ECHO over SPECT
- Images are difficult to obtain at peak exercise, an ischemic response is required to observe wall motion abnormalities, wall motion can recover quickly in the presence of mild ischemia, detection of residual ischemia is difficult in an akinetic wall zone, the technique is highly operator dependent, good quality images were only acquired in 70% of cases.
Strengths of SPECT over stress ECHO
- Does not require an ischemic response to be abnormal, just requires an abnormality in flow reserve, sensitivity is slightly higher by about 8-10 percentage points (mostly because the ability to detect single vessel disease or mild stenoses of 50-70% is not as good with stress Echo), can see defects in areas that contain scar and viable myocardium, acquisition of images is not operator dependent, in virtually 100% of patients diagnostic images are obtained, with Tc simultaneous assessment of perfusion and function is obtained, resting LV ejection fraction can be obtained, vasodilator SPECT has significantly higher sensitivity than vasodilator stress ECHO, dobutamine ECHO is associated with higher sensitivity and specificity than vasodilator ECHO.
Limitations of SPECT imaging in relation to stress ECHO
- Longer imaging protocols, greater expense of equipment, must inject and store radiopharmaceuticals, inability to visualize the heart in real time, lower spatial resolution than ECHO, higher costs to patients.
In general, the sensitivity is lower for stress ECHO while the specificity is higher.
Prognosis
Exercise Tolerance Testing
- 1 mm or more of horizontal or downsloping ST depression is associated with a poor prognosis
- Failure to achieve 6 METS is associated with an elevated mortality rate over the next 2.5 years.
- Failure of heart rate to rise is associated with higher mortality, even after adjusting for perfusion defects.
- Failure to reach 85% of age adjusted max HR is associated with a RR of 1.85 in mortality.
- Limitation of ETT is the fact that the magnitude of ST depression is not strongly associated with the extent of CAD
- Exercise testing alone has excellent prognostic ability among patients with atypical chest pain or non anginal pain who have a normal EKG at baseline. If these patients have a normal ETT, the prognosis is excellent.
Nuclear Stress Myocardial Perfusion
- Nuclear Stress Myocardial Perfusion Imaging, often abbreviated MPI or MPS, is a technique for measuring perfusion of myocardial tissue using externally injected radioactive tracers. Photons, or positrons emitted from these tracers are then detected with specialized imaging equipment and software. The most common methods are single photon emission computed tomography (SPECT) and positron emission tomography (PET). SPECT can be performed with radiotracers based on thallium or technetium 99-m. PET is commonly performed with rubidium-82, although some centers use ammonia (NH3) or radiolabeled oxygen in water. Cardiac PET with fluorodeoxyglucose (FDG) is useful for other investigations such as evaluation of infections, sarcoidosis activity, and viability/hibernation. Flurpiridaz, is a PET tracer based on fluorine-18 (F-18) and was approved for use by the FDA in 2025.
- The following are associated with a poor prognosis:
- 20% of the LV is a perfusion defect
- Defects in more than one distribution suggestive of multivessel CAD
- A large number of non reversible defects
- Transient LV cavitary dilation
- Increased lung uptake
- Resting LVEF of < 40%
- Normal thallium: Mortality 1% per year
- Normal Tc: annual mortality 0.6%, 12 fold higher if there is a Tc defect
- The positive predictive value of stress myocardial perfusion imaging and stress ECHO is low: That is the percentage of people who die or sustain an MI is low among patients with abnormal findings. On the other hand the negative predictive value is high and exceeds 95%.
Techniques used to Assess Myocardial Viability
- Tl Imaging
- Rest and delayed redistribution is the most common radionuclide method used to assess viability. Uptake of Tl is related not only to blood flow, but also to membrane integrity. Myocardial stunning or hibernation does not result in a reduction in Tl extraction as long as the sarcolemmal membrane does not sustain irreversible ischemic damage. 60 to 70% of asynergistic segments will show > a 50% improvement after revascularization.
- Tc Imaging
- Same as above, as usual a better signal with Tc, can also assess regional wall thickening. If thickening is present, then viability is likely.
- PET
- Considered by many to be the gold standard. Can be used to assess perfusion and metabolism simultaneously. If there is mismatch in perfusion and metabolism, then the tissue is viable. If there is a match, then there is scar.
Dobutamine: Enhanced systolic contractility with low dose dobutamine is associated with recovery.
The Chest X Ray in Cardiovascular Disease
Editors-in-Chief: Eli V. Gelfand, M.D.[1], and Matthew W. Parker, M.D.[2] (Beth Israel Deaconess Medical Center, Harvard Medical School)
Overview
The plain film radiograph of the chest is the most commonly performed radiologic test, with approximately 150 million performed in the USA every year, accounting for 45% of all radiologic exams chestxraydotcom. Chest radiography is widely available, inexpensive, and carries low risk to the patient being examined. Therefore it is often the first test to image the heart and great vessels in patients with suspected cardiovascular disease, although much of the information about the cardiovascular system obtained from a chest x-ray is indirect and non-specific.
The test is performed by placing an x-ray film (or digital detector) parallel to the chest wall and then exposing the film to x-rays generated from a source on the opposite side of the patient’s body. The standard views most useful for evaluating cardiovascular structures are the postero-anterior (PA) view, in which the film is placed anterior to the chest and x-rays travel through the patient from posterior to anterior before reaching the film, and the antero-posterior (AP) view, in which the film is against the patient’s back and the x-ray generator is anterior to the patient’s body. The PA view places the heart closer to the x-ray film, resulting in less x-ray scatter and a more accurate representation of the cardiac size, but the AP view is often advantageous because it does not require any active participation from the patient and can be performed with a portable x-ray generator; that is, the film cartridge can be placed in bed behind a patient too unstable to travel to the radiology exam room and stand up in front of the x-ray apparatus. Because the plain-film is a 2-dimensional projection of the body, a lateral view, when feasible, is required to determine the location of structures along the AP axis of the body.
Normal cardiovascular anatomy on a chest radiograph

Fig. 1. PA Chest X-ray of a Normal Adult. Because the heart and other structures in the mediastinum have similar densities, there are only modest differences in their x-ray appearance. Thus, the most reliable information about the heart and vascular structures comes from the interfaces where they meet the aerated lung fields. Prior knowledge of the cardiovascular anatomy allows the interpreter to approximate the location of the heart structures and great vessels:

Fig. 2. PA Projections of Right Heart Stuctures. SVC is superior vena cava; PA are the pulmonary arteries, right and left; RA is right atrium; RV is right ventricle; and IVC is the approximate position of the inferior vena cava. The venae cavae are poorly visualized with plain film x-ray, however, the right border of the mediastinum is generally accepted as the right border of the SVC, which should not extend laterally beyond the right border of the heart in a normal individual. The RV is an anterior structure, so it is superimposed on the RA and left ventricule. Additionally, the interventricular septum lies obliquely in the body, so that its projection in this diagram is arbitrary.

Fig. 3. PA Projections of the Left Heart Structures. Ao is the aortic arch, which then continues as the descending aorta, indicated by the dotted line. LAu is the auricle of the left atrium, which itself sits posteriorly at the base of the heart. PV are the pulmonary veins converging on the left atrium. LV is the left ventricle, which is partially posterior to the right ventricle.
Specific cardiovascular abnormalities on chest radiograph
- Cardiac chamber dilation and hypertrophy
– Left ventricular hypertrophy
– Left atrial enlargement:

This radiograph of a patient with mitral stenosis shows a prominent left atrial appendage caused by pressure overload of the left atrium.
– Right ventricular/bi-ventricular hypertrophy
- Abnormalities of pulmonary vasculature
– mitral stenosis, pulmonary hypertension
– examples of upper lobe vascular redistribution,
– Cardiogenic Pulmonary Edema

Radiograph of patient with congestive heart failure, showing pulmonary edema with Kerley lines and perihilar engorgement.
– pericardial effusion


First image, above, shows a patient with an enlarged, globular cardio-mediastinal silhouette representing a large pericardial effusion and a large right-sided pleural effusion one month after aortic valve replacement. The second image is the same patient after pericardiocentesis, which yielded one liter of pericardial fluid, and thoracentesis.
– Tetralogy – patent ductus arteriosus – coarctation of aorta – atrial septal defect – Eisenmenger syndrome
– Situs Inversus

This patient has situs inversus; the viscera including the heart developed in mirror-image fashion relative to their usual positions in the body. This can occur sporadically or as part of Kartagener’s syndrome.
Cardiac fluoroscopy
- Cardiac fluoroscopy: Indications and procedural description
Further online resources
- Chest Imaging Tutorial at Michigan State University Department of Radiology
- Case-Based Introduction to Chest X-rays at the University of Liverpool School of Medicine.
- Overview of a systematic approach to reading Chest Radiographs at Everything2.
- Patient information about chest radiography from the American College of Radiology.
References
Echocardiography
Editor(s)-In-Chief: C. Michael Gibson M.S., M.D. [1] Phone:617-525-6884 ; Eli V. Gelfand, M.D. [2]
Overview
Echocardiography
- Echocardiography (echo) is a test that uses sound waves to create a moving picture of your heart. The picture shows how well your heart is working and its size and shape. There are several types of echo, including stress echo.
- Stress echo can show whether you have decreased blood flow to your heart, a sign of coronary heart disease. Another type of echo is transesophageal (tranz-ih-sof-uh-JEE-ul) echo, or TEE.
- TEE provides a view of the back of the heart. For this test, a sound wave wand is put on the end of a special tube. The tube is gently passed down your throat and into your esophagus (the passage leading from your mouth to your stomach). Because this passage is right behind the heart,
General Principles of Echocardiography
- Basic physical principles of ultrasound
- Quantification of pressure gradients
- Echocardiographic evaluation of ventricular dyssynchrony
- Echocardiography terminology
- Guidelines for echocardiography
Principal Echocardiographic Modalities
- Transthoracic echo (TTE): standard views and measurements
- Transesophageal echocardiography (TEE): standard views
- M-mode echo: principles and classic findings
- Doppler echocardiography
- Tissue Doppler imaging
- Contrast echocardiography
- Stress echocardiography
- Three-dimensional echocardiography
- Myocardial contrast echocardiography
- Intraoperative echocardiography
Echocardiographic Diagnosis and Evaluation of Specific Cardiovascular Disorders
- Echo in emergencies
- Echo in coronary artery disease
- Echo in pericardial diseases: effusion, cardiac tamponade, constriction
- Echo in dilated cardiomyopathies
- Echo in hypertrophic cardiomyopathy
- Echo in restrictive cardiomyopathies
- Echo in pulmonary hypertension
- Echo in pulmonary embolism
- Endocarditis (TTE and TEE)
- Echo in patients with atrial fibrillation
- Echo in cardiac tumors and masses
- Echo in diseases of the aorta
- Echo in congenital heart disease
- Echo in non-cardiac systemic disease
Miscellaneous
References
Nuclear Cardiology
Section editor: Eli V. Gelfand, M.D. (Beth Israel Deaconess Medical Center, Harvard Medical School) [1]
General overview of Nuclear Cardiology
- Basic physical principles of single-photon emission computed tomography (SPECT)
- Basic physical principles of positron emission tomography (PET)
- Commonly used radiopharmaceuticals
- Selecting appropriate candidates for myocardial perfusion imaging
- Standard exercise stress protocols
- Standard pharmacologic stress protocols
- Imaging protocols
- Combining myocardial perfusion imaging with coronary CT
- Radionuclide angiography
- Molecular imaging and related novel technologies
Clinical use of stress myocardial perfusion imaging (MPI)
- ACCF/ASNC appropriateness criteria for SPECT-MPI (2005)
- ACC/AHA guidelines for cardiac radionuclide imaging (2003)
Coronary Disease
- Assessment of patients presenting with chest pain to the Emergency Department
- Detection of CAD
- Management, risk assessment and prognosis of patients with chronic CAD
- Detection of acute MI
- Risk assessment of patients following ST-elevation MI
- Risk assessment of patients following non-ST elevation acute coronary syndrome
Heart Failure
- Assessment of LV systolic function
- Assessment of etiology of heart failure
- Detection of CAD in patients with heart failure
- Determination of myocardial viability
Specific patient populations
- Patients with an “uninterpretable” resting ECG
- Elderly patients
- Asymptomatic patients with diabetes
- Patients following up after a coronary calcium screening
- Patients before and after coronary revascularization
- Patients undergoing elective noncardiac surgery
Coronary Angiography
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]
Synonyms and keywords: coronary arteriography, cardiac arteriography, cardiac angiogram, coronary angio, coronary artery angio, coronary cath, cardiac cath
General Principles
- Overview
- Historical perspective
- Contraindications
- Appropriate Use Criteria for Revascularization
- Complications
- Technique
- Film Quality
Coronary Anatomy and Projection Angles
Normal Coronary Anatomy
- Coronary arteries
- Left coronary artery | Left main coronary artery | Left anterior descending artery | Left circumflex artery | Ramus intermedius
- Right coronary artery
- Coronary artery dominance
Coronary Anatomic Variants
Projection Angles
Assessment of Perfusion
How to Assess Epicardial Coronary Blood Flow
- TIMI flow grade (TFG): TIMI flow grade 0 | TIMI flow grade 1 | TIMI flow grade 2 | TIMI flow grade 3
- TIMI frame count (TFC)
- Pulsatile flow
- Deceleration
How to Assess Myocardial Perfusion
- TIMI myocardial perfusion grade (TMPG): TIMI myocardial perfusion grade 0 | TIMI myocardial perfusion grade 0.5 | TIMI myocardial perfusion grade 1 | TIMI myocardial perfusion grade 2 | TIMI myocardial perfusion grade 3
Assessment of Lesion Morphology
Lesion Complexity
Thrombus Grades
- TIMI thrombus grade: TIMI thrombus grade 0 | TIMI thrombus grade 1 | TIMI thrombus grade 2 | TIMI thrombus grade 3 | TIMI thrombus grade 4 | TIMI thrombus grade 5 | TIMI thrombus grade 6
Lesion Morphology
- Quantitative angiography
- Definitions of Preprocedural Lesion Morphology
- Irregular lesion
- Disease extent
- Arterial foreshortening
- Infarct related artery (Culprit lesion)
- Restenosis
- Degenerated saphenous vein graft
- Collaterals
- Coronary artery ulceration
- Coronary artery aneurysm
- Coronary artery bifurcation
- Coronary artery trifurcation
- Technique
- Quantification of LV Function
- Quantification of Mitral Regurgitation
- Left Ventricular Ejection Fraction Assessment by Visual Estimation
Vein and Arterial Bypass Graft
Performing Diagnostic Catheterization
Risks stratification and benefits of PCI | Conscious Sedation | Preparation of the Patient for Diagnostic Catheterization | Technical Aspects of the Cardiac Catheterization Laboratory | Obtaining Venous and Arterial Access | Equipment Used in Diagnostic Cardiac Catheterizaiton | Hemodynamic Assessment in the Cardiac Catheterization Laboratory | Radiation Safety
Therapeutic Catheterization
Therapeutic procedures | Advances in catheter based physical treatments
PCI in Specific Lesion Types
Classification of the Lesion | The Calcified Lesion | The Ostial Lesion | The Angulated or Tortuous Lesion | The Bifurcation Lesion | The Long Lesion | The Bridge Lesion | Vasospasm | The Chronic Total Occlusion | Multivessel Disease | Distal Anastomotic Lesions | Left Main Intervention | The Thrombotic Lesion
PCI Complications
Vessel Perforation | Dissection | Distal Embolization | No-reflow | Abrupt Closure | Restenosis | Late Acquired Stent Malapposition | Loss of Side Branch | Multiple Complications | Coronary stent thrombosis | Slow flow | Pulsatile flow | Deceleration | Ectasia | Intimal flap | Staining | Coronary air embolism
Cardiovascular Magnetic Resonance Imaging (CMR)
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-In-Chief: Eli V. Gelfand, M.D.[2]; Caitlin J. Harrigan [3]
Overview
- CMR-Related Definitions
- ACCF/ACR/SCCT/SCMR/ASNC/NASCI/SCAI/SIR 2006 Appropriateness Criteria for Cardiac Magnetic Resonance Imaging
- ACR Practice Guideline for the Performance and Interpretation of Cardiac Magnetic Resonance Imaging (MRI)
- Basic MRI Physics
- CMR Image Acquisition Protocols
- Standard Image Orientation
- Normal Cardiac Anatomy as Viewed by CMR
- Contrast CMR
- Cine CMR
- Myocardial Tagging
- Flow Quantification by CMR
- CMR in Valvular Heart Disease
ACC/AHA Guidelines- ACCF/ACR/AHA/NASCI/SCMR 2010 Expert Consensus Document on Cardiovascular Magnetic Resonance[1] (DO NOT EDIT)
| “ |
CMR may be used for assessing individuals with valvular heart disease in which evaluation of valvular stenosis, regurgitation, para- or perivalvular masses, perivalvular complications of infectious processes, or prosthetic valve disease are needed. CMR may be useful in identifying serial changes in LV volumes or mass in patients with valvular dysfunction. |
” |
- CMR in Dilated Cardiomyopathy, Hypertrophic cardiomyopathy, myocarditis, amyloidosis, other infiltrative heart diseases and arrhythmogenic right ventricular dysplasia
ACC/AHA Guidelines- ACCF/ACR/AHA/NASCI/SCMR 2010 Expert Consensus Document on Cardiovascular Magnetic Resonance[1] (DO NOT EDIT)
| “ |
CMR may be used for assessment of patients with LV dysfunction or hypertrophy or suspected forms of cardiac injury not related to ischemic heart disease. When the diagnosis is unclear, CMR may be considered to identify the etiology of cardiac dysfunction in patients presenting with heart failure, including
|
” |
- CMR in Cardiac Masses
ACC/AHA Guidelines- ACCF/ACR/AHA/NASCI/SCMR 2010 Expert Consensus Document on Cardiovascular Magnetic Resonance[1] (DO NOT EDIT)
| “ |
CMR may be used for clinical evaluation of cardiac masses, extracardiac structures, and involvement and characterization of masses in the differentiation of tumors from thrombi. |
” |
- CMR in Pericardial Disease
ACC/AHA Guidelines- ACCF/ACR/AHA/NASCI/SCMR 2010 Expert Consensus Document on Cardiovascular Magnetic Resonance[1] (DO NOT EDIT)
| “ |
CMR may be used as a noninvasive imaging modality to diagnose patients with suspected pericardial disease. CMR can provide a comprehensive structural and functional assessment of the pericardium as well as evaluate the physiological consequences of pericardial constriction. |
” |
- CMR in Congenital heart Disease
ACC/AHA Guidelines- ACCF/ACR/AHA/NASCI/SCMR 2010 Expert Consensus Document on Cardiovascular Magnetic Resonance[1] (DO NOT EDIT)
| “ |
CMR may be used for assessing cardiac structure and function, blood flow, and cardiac and extracardiac conduits in individuals with simple and complex congenital heart disease. Specifically, CMR can be used to identify and characterize congenital heart disease, to assess the magnitude or quantify the severity of intracardiac shunts or extracardiac conduit blood flow, to evaluate the aorta, and to assess the pathological and physiologic consequences of congenital heart disease on left and right atrial and ventricular function and anatomy. |
” |
- CMR in Athlete’s Heart
- Coronary MRI
- Peripheral Vascular MRA
- Atherosclerosis/Plaque Imaging with CMR
- CMR Risk Factors: NSF
- CMR in Heart failure
ACC/AHA Guidelines- ACCF/ACR/AHA/NASCI/SCMR 2010 Expert Consensus Document on Cardiovascular Magnetic Resonance[1] (DO NOT EDIT)
| “ |
CMR may be used for assessment of LV and RV size and morphology, systolic and diastolic function, and for characterizing myocardial tissue for the purpose of understanding the etiology of LV systolic or diastolic dysfunction. The writing committee recognizes the potential capabilities of spectroscopic techniques for acquiring metabolic information of the heart when evaluating individuals with heart failure. |
” |
- CMR in Coronary artery disease
ACC/AHA Guidelines- ACCF/ACR/AHA/NASCI/SCMR 2010 Expert Consensus Document on Cardiovascular Magnetic Resonance[1] (DO NOT EDIT)
| “ |
CMR may be used for identifying coronary artery anomalies and aneurysms and for determining coronary artery patency. In specialized centers, CMR may be uniquely useful in identifying patients with multivessel coronary artery disease without exposure to ionizing radiation or iodinated contrast medium. |
” |
- CMR in Ischemic heart disease
ACC/AHA Guidelines- ACCF/ACR/AHA/NASCI/SCMR 2010 Expert Consensus Document on Cardiovascular Magnetic Resonance[1] (DO NOT EDIT)
| “ |
The combination of CMR stress perfusion, function, and LGE allows the use of CMR as a primary form of testing for
Assessment of LV wall motion after low-dose dobutamine in patients with resting akinetic LV wall segments is useful for identifying patients who will develop improvement in LV systolic function after coronary arterial revascularization. The writing committee recognizes the potential advantages of spectroscopic techniques for identifying early evidence of myocardial ischemia that may or may not be evident using existing non-CMR methods. Myocardial infarction/scar LGE-CMR may be used for identifying the extent and location of myocardial necrosis in individuals suspected of having or possessing chronic or acute ischemic heart disease. |
” |
- CMR in Myocardial infarction
ACC/AHA Guidelines- ACCF/ACR/AHA/NASCI/SCMR 2010 Expert Consensus Document on Cardiovascular Magnetic Resonance[1] (DO NOT EDIT)
| “ |
LGE-CMR may be used for identifying the extent and location of myocardial necrosis in individuals suspected of having or possessing chronic or acute ischemic heart disease. |
” |
- CMR in Pulmonary angiography
ACC/AHA Guidelines- ACCF/ACR/AHA/NASCI/SCMR 2010 Expert Consensus Document on Cardiovascular Magnetic Resonance[1] (DO NOT EDIT)
| “ |
CE-MRA may be used in patients with a strong suspicion of pulmonary embolism in whom the results of other tests are equivocal or for whom iodinated contrast material or ionizing radiation are relatively contraindicated. The writing committee agrees that data in the literature are insufficient to recommend where pulmonary CE-MRA should fit into a diagnostic pathway for pulmonary embolism. |
” |
- CMR in atrial fibrillation
ACC/AHA Guidelines- ACCF/ACR/AHA/NASCI/SCMR 2010 Expert Consensus Document on Cardiovascular Magnetic Resonance[1] (DO NOT EDIT)
| “ |
CMR may be used for assessing left atrial structure and function in patients with atrial fibrillation. The writing committee recognizes that evolving techniques utilizing LGE may have high utility for identifying evidence of fibrotic tissue within the atrial wall or an adjoining structure. Standardization of protocols and further studies are needed to determine if CMR provides a reliable effective method for detecting thrombi in the left atrial appendage in patients with atrial fibrillation. CMR is recommended for identifying pulmonary vein anatomy prior to or after electrophysiology procedures without need for patient exposure to ionizing radiation. |
” |
- CMR in peripheral arterial disease
ACC/AHA Guidelines- ACCF/ACR/AHA/NASCI/SCMR 2010 Expert Consensus Document on Cardiovascular Magnetic Resonance[1] (DO NOT EDIT)
| “ | CMR recommendations for PAD are in agreement with current guidelines and appropriate use criteria.
CMR for PAD
Level of Evidence: A). CMR of the extremities may be considered
(Class IIb, Level of Evidence: B); and
IIb, Level of Evidence: B). Additionally, MRA of the lower extremities is appropriate for patients with claudication. |
” |
- CMR in Carotid artery disease
ACC/AHA Guidelines- ACCF/ACR/AHA/NASCI/SCMR 2010 Expert Consensus Document on Cardiovascular Magnetic Resonance[1] (DO NOT EDIT)
| “ |
CMR may be used for defining the location and extent of carotid arterial stenoses. |
” |
- CMR in thoracic aortic disease
ACC/AHA Guidelines- ACCF/ACR/AHA/NASCI/SCMR 2010 Expert Consensus Document on Cardiovascular Magnetic Resonance[1] (DO NOT EDIT)
| “ |
CMR of thoracic aortic disease CMR may be used for defining the location and extent of aortic aneurysms, erosions, ulcers, dissections; evaluating postsurgical processes involving the aorta and surrounding structures, and aortic size blood flow and cardiac cycle–dependent changes in area. |
” |
- CMR in renal artery disease
ACC/AHA Guidelines- ACCF/ACR/AHA/NASCI/SCMR 2010 Expert Consensus Document on Cardiovascular Magnetic Resonance[1] (DO NOT EDIT)
| “ |
CMR may be used for evaluating renal arterial stenoses and quantifying renal arterial blood flow. CE-MRA indicates contrast-enhanced magnetic resonance angiography; CMR, cardiovascular magnetic resonance; ECG, electrocardiogram; LGE, late gadolinium enhancement; LV, left ventricular; RV, right ventricular; MRA, magnetic resonance angiography; and PAD, peripheral arterial |
” |
References
- ↑ 1.00 1.01 1.02 1.03 1.04 1.05 1.06 1.07 1.08 1.09 1.10 1.11 1.12 1.13 1.14 American College of Cardiology Foundation Task Force on Expert Consensus Documents. Hundley WG, Bluemke DA, Finn JP, Flamm SD, Fogel MA; et al. (2010). “ACCF/ACR/AHA/NASCI/SCMR 2010 expert consensus document on cardiovascular magnetic resonance: a report of the American College of Cardiology Foundation Task Force on Expert Consensus Documents”. Circulation. 121 (22): 2462–508. doi:10.1161/CIR.0b013e3181d44a8f. PMC 3034132. PMID 20479157.
CT Angiography
Editors-In-Chief: Joanna J. Wykrzykowska, MD; Alexander Morss, MD; Roger J. Laham, MD; Melvin Clouse, MD
Overview
- CT angiography is emerging as the imaging modality of choice to rule out significant coronary artery disease in patients with low pretest probablity of disease. Good negative predictive value of the test (Garcia et al., 2006) promises to obviate the need for cardiac catheterization in patients with atypical chest pain
- The entire coronary tree can be examine in one breath hold
- Temporal resolution is 100 ms allowing for almost motion free imaging in the diastolic phase
- Spatial resolution is determined by the so called pitch=travel/x-ray beam width which currently ranges between 0.25-0.5 mm
- 64 slice/detector scanner can cover in a helical fashion 12.5 cm in 5 secs; new 256 detector MDCT will allow single beat aquisition thereby reducing any motion artifact and reducing the radiation dose
- As the technology improves with new post-processing software MDCT may allow for non-invasive screening for in-stent restenosis, especially after left main stenting
Role of Electron Beam Computer Tomography and Calcium score
- Electron Beam CT was developped in the 1980s
- It is performed before coronary CTA and if calcium score is above 1000, the CTA postion of the exam is aborted, due to inerpretable results
- EBCT and calcium score correlated with overall atherosclerosis burden and high calcium scores confer a 10 fold risk of future coronary events
- It is an independent risk factor of the Framingham Health Study Risk Score
- More importantly, calcium score progression on serial EBCT in the same patient confers the highest risk of future cardiac events
- Basic calcium score is calculated by simply adding the calcified areas slices by slice in each coronary artery examined
Basic principles of Multislice Computer Tomographic Imaging
Imaging of the coronary arteries
- Patient preparation (heart rate and breath hold)
- Upper heart rate limits are 65 beats/min and thus beta-blockers IV and/or po need to be administered to achieve an optimal heart rate
- Usual protocol is to give 100 mg of metoprolol for HR> 65 1 hour before the scan
- For frequent PVCs IV lidocaine can be considered
- If the patient has a pacer that should be interrogated before the scan
- Usually 80 cc of contrast dye are needed for coronary imaging and 100 cc for SVG grafts with a 40-50 cc saline flush
- The scan is triggered when a selected area in the aorta reaches a peak signal in Hounsfield Units (HU)
- ECG gating
- Spatial and Temporal resolution
- Basics of reconstruction: diagnostic qualty of the images largely depends on chosing the reconstruction time within the cardiac cycle; usually 60-70% of the RR interval is chosen
- axial images are usually not used primarily for detection of coronary stenosis but maybe used to confirm the findings from maximum intensity projections
- MPR = multiplanar recoonstructions
- MIP = maximum intensity projections: simulate three different cardiac catheter projections: MIP planes reconstructed along the atria-ventricular groove to create in the left anterior oblique projection show the left circumfelx and right coronary artery; MIP reconstruction along the interventricular groove in the right anterior oblique projection show the left anterior descending artery
- VRT = volume rendering technique
- Hounsfield units:
- Water = 0
- Air and Bone = 1000
- Image processing and Post-processing
- Results from the 16 slice MDCT:
” Accuracy of 16-row Multidetector Computed Tomography for the Assessment of Coronary Artery Stenosis.”
This randomized trial of 238 patients assessed 1629 coronary segments, of which 71% were evaluable. Detection of > 50% stenosis in the evaluable segments had a sensitivity: 89% specificity: 65% and 54% in a patient-based analysis positive predictive value: 13% negative predictive value: 99%
High percentage of non-evaluable segments and false positive results (low specificity and positive predictive value) in this study lead to the conclusion that MDCT 16 should not be used routinely for angiographic assessment. The main reasons for inability to evaluate the segments were respiratory or cardiac motion, excessive calcification, poor opacification and small vessel size (< 2 mm). This is after beta-blocker administration to optimize the heart rate and after exclusion of patients with calcium scores > 600. There were 10 false negative results. Out of the patients with non-evaluable segments 38% were found to have significant coronary artery disease on angiography (Garcia MJ et al. for the CATSCAN Study Investigators; JAMA 2006).
The multicenter trial Coronary Evaluation using 64-Row Multi-detector CT Angiography completed recently will show us the accuracy of 64-slice scanner in identifying significant stenosis.
Special issues in imaging coronary arteries
- Stents: The major limitation of the MDCT has been in imaging of coronary stents due to partial volume effects and beam hardening. Accuracy of stent lumen analysis by the 4 and 16 slice scanner has been quite limited. However with sharp kernels and post-processing software on 64 slice scanners, stents 3.0 mm and greater appear to be possible to adequately evaluate.
Follow up of patients after multivessel stenting would greatly benefit from CTA technology. Particularly that in stent restenosis presents as non-ST elevation MI in 20% of cases. Recently published papers suggest that the technology may have improved accuracy. Cademartini et al. (JACC, 2007) evaluated 182 patients with previously placed stents. Only 14 segments in that study were unevaluable (7%).Of the 20 stents with significant in-stent restenosis by angiography, 19 were correctly identified by MDCT. This gave overall: sensitivity: 95% specificity: 93% positive predictive value: 63% negative predictive value: 99% To achieve these results tube voltage of 120 KeV was used and a sharp convulition kernel as well as particular window settings. While the readers were blinded to the angiographi results, they were aware of prior stenting history (? type of stent). Most importantly, unlike in the previous trials stents <3.0 mm, = 3.0 mm and >3.0 mm had comparable assessability and the rate of false positives was the same across the stent sizes. The trial did not comment specifically on stent type as predictor of assessability. We know from prior investigations that stents with thick struts and closed-cell stents such as Cypher stents tend to be more difficult to assess that thinner strut cobalt chromium or Taxus stents. These promising results await verification in a larger multicenter trial.
- Left main stents
- Bypass-grafts
- Chronic total occlusions and planning of interventions
Other applications
- Perfusion imaging
- Valvular disease
- LV function
Radiation dose, image quality and other considerations
For 16 detector multi slice CTs the radiation dose is 8 m Sev which is 2-3 times that of coronary cardiac catheterization and comparable to the nuclear imaging dose. This is reduced with 64 slice scanner and will be further reduced with dual source and 256 detector scanners.
Similarly, given the 5 second acquisition rate for 256 slices scanners, contrast bolus dose will be further reduced to 40-60 ml.
Positron Emission Tomography
CARDIAC DISEASE STATES

Editor-in-Chief: Thomas F. Heston, MD, PhD
Overview
Positron emission tomography (PET) is a nuclear medicine medical imaging technique which produces a three-dimensional image or map of functional processes in the body. The concept of emission and transmission tomography was introduced by David Kuhl and Roy Edwards in the late 1950’s. Their work later led to the design and construction of several tomographic instruments at the University of Pennsylvania. The technique was further developed by Michel (Michael) Ter-Pogossian, Michael E. Phelps and others at the Washington University School of Medicine [1][2]
Description
How a PET scan is conducted
To conduct the scan, a short-lived radioactive tracer isotope, which decays by emitting a positron, which also has been chemically incorporated into a metabolically active molecule, is injected into the living subject (usually into blood circulation). There is a waiting period while the metabolically active molecule becomes concentrated in tissues of interest; then the research subject or patient is placed in the imaging scanner. The molecule most commonly used for this purpose is fluorodeoxyglucose (FDG), a sugar, for which the waiting period is typically an hour.
How the scanner operates
As the radioisotope undergoes positron emission decay (also known as positive beta decay), it emits a positron, the antimatter counterpart of an electron. After travelling up to a few millimeters the positron encounters and annihilates with an electron, producing a pair of annihilation (gamma) photons moving in almost opposite directions. These are detected when they reach a scintillator material in the scanning device, creating a burst of light which is detected by photomultiplier tubes or silicon avalanche photodiodes (Si APD). The technique depends on simultaneous or coincident detection of the pair of photons; photons which do not arrive in pairs (i.e., within a few nanoseconds) are ignored.
The most significant fraction of electron-positron decays result in two 511 keV gamma photons being emitted at almost 180 degrees to each other; hence it is possible to localize their source along a straight line of coincidence (also called formally the “line of response” or LOR). In practice the LOR has a finite width as the emitted photons are not exactly 180 degrees apart. If the recovery time of detectors is in the picosecond range rather than the 10’s of nanosecond range, it is possible to calculate the single point on the LOR at which an annihilation event originated, by measuring the “time of flight” of the two photons. This technology is not yet common, but it is available on some new systems [1]. More commonly, a technique much like the reconstruction of computed tomography (CT) and single photon emission computed tomography (SPECT) data is used, although the data set collected in PET is much poorer than CT, so reconstruction techniques are more difficult (see section below on image reconstruction of PET). Using statistics collected from tens-of-thousands of coincidence events, a set of simultaneous equations for the total activity of each parcel of tissue along many LORs can be solved by a number of techniques, and thus a map of radioactivities as a function of location for parcels or bits of tissue (“voxels”), may be constructed and plotted. The resulting map shows the tissues in which the molecular probe has become concentrated, and can be interpreted by a nuclear medicine physician or radiologist in the context of the patient’s diagnosis and treatment plan.
-
 Schematic view of a detector block and ring of a PET scanner (here: Siemens ECAT Exact HR+)
Schematic view of a detector block and ring of a PET scanner (here: Siemens ECAT Exact HR+) -
 Schema of a PET acquisition process
Schema of a PET acquisition process


PET scans are increasingly read alongside CT or magnetic resonance imaging (MRI) scans, the combination (co-registration”) giving both anatomic and metabolic information (i.e., what the structure is, and what it is doing biochemically). Because PET imaging is most useful in combination with anatomical imaging, such as CT, modern PET scanners are now available with integrated high-end multi-detector-row CT scanners. Because the two scans can be performed in immediate sequence during the same session, with the patient not changing position between the two types of scans, the two sets of images are more-precisely registered, so that areas of abnormality on the PET imaging can be more perfectly correlated with anatomy on the CT images. This is very useful in showing detailed views of moving organs or structures with higher amounts of anatomical variation, such as are more likely to occur outside the brain.
How PET scanning is used
PET is both a medical and research tool. It is used heavily in clinical oncology (medical imaging of tumors and the search for metastases), and for clinical diagnosis of certain diffuse brain diseases such as those causing various types of dementias. PET is also an important research tool to map normal human brain and heart function.
PET is also used in pre-clinical studies using animals, where it allows repeated investigations into the same subjects. This is particularly valuable in cancer research, as it results in an increase in the statistical quality of the data (subjects can act as their own control) and substantially reduces the numbers of animals required for a given study.
Alternative methods of scanning include x-ray computed tomography (CT), magnetic resonance imaging (MRI) and functional magnetic resonance imaging (fMRI), ultrasound and single photon emission computed tomography (SPECT).
While some imaging scans such as CT and MRI isolate organic anatomic changes in the body, PET scanners, like SPECT are capable of detecting areas of molecular biology detail (even prior to anatomic change). The PET scanner does this via the use of radiolabelled molecular probes that have different rates of uptake, depending on the type and function of tissue involved. The changing of regional blood flow in various anatomic structures (as a measure of the injected positron emitter) can be visualized and relatively quantified with a PET scan.
PET imaging is best performed using a dedicated PET scanner. However, it is possible to acquire PET images using a conventional dual-head gamma camera fitted with a coincidence detector. The quality of gamma-camera PET is considerably lower, and acquisition is slower. However, for institutions with low demand for PET, this may allow on-site imaging, instead of referring patients to another center, or relying on a visit by a mobile scanner.
-
 Maximum intensity projection (MIP) of a typical F-18 FDG wholebody PET acquisition
Maximum intensity projection (MIP) of a typical F-18 FDG wholebody PET acquisition -
 PET scan of the human brain.
PET scan of the human brain.


Radioisotopes used in PET
Radionuclides used in PET scanning are typically isotopes with short half lives such as carbon-11 (~20 min), nitrogen-13 (~10 min), oxygen-15 (~2 min), and fluorine-18 (~110 min). Due to their short half lives, the radionuclides must be produced in a cyclotron which is not too far away in delivery-time to the PET scanner. These radionuclides are incorporated into compounds normally used by the body such as glucose, water or ammonia and then injected into the body to trace where they become distributed. Such labelled compounds are known as radiotracers.
Limitations of PET
PET as a technique for scientific investigation in humans is limited by the need for clearance by ethics committees to inject radioactive material into participants. The minimization of radiation dose to the subject is an attractive feature of the use of short-lived radionuclides. Besides its established role as a diagnostic technique, PET has an expanding role as a method to assess the response to therapy, in particular, cancer therapy (e.g. Young et al. 1999), where the risk to the patient from lack of knowledge about disease progress is much greater than the risk from the test radiation.
Limitations to the widespread use of PET arise from the high costs of cyclotrons needed to produce the short-lived radionuclides for PET scanning and the need for specially adapted on-site chemical synthesis apparatus to produce the radiopharmaceuticals. Few hospitals and universities are capable of maintaining such systems, and most clinical PET is supported by third-party suppliers of radiotracers which can supply many sites simultaneously. This limitation restricts clinical PET primarily to the use of tracers labelled with F-18, which has a half life of 110 minutes and can be transported a reasonable distance before use, or to rubidium-82, which can be created in a portable generator and is used for myocardial perfusion studies. Nevertheless, in recent years a few on-site cyclotrons with integrated shielding and hot labs have begun to accompany PET units to remote hospitals. The presence of the small on-site cyclotron promises to expand in the future as the cyclotrons shrink in response to the high cost of isotope transportation to remote PET machines [3]
Because the half-life of F-18 is about two hours, the prepared dose of a radiopharmaceutical bearing this radionuclide will undergo multiple half-lives of decay during the working day. This necessitates frequent recalibration of the remaining dose (determination of activity per unit volume) and careful planning with respect to patient scheduling.
Image reconstruction in PET
The raw data collected by a PET scanner are a list of ‘coincidence events’ representing near-simultaneous detection of annihilation photons by a pair of detectors. Each coincidence event represents a line in space connecting the two detectors along which the positron emission occurred.
Coincidence events can be grouped into projections images, called sinograms. The sinograms are sorted by the angle of each view and tilt, the latter in 3D case images. The sinogram images are analogous to the projections captured by computed tomography (CT) scanners, and can be reconstructed in a similar way. However, the statistics of the data is much worse than those obtained through transmission tomography. A normal PET data set has millions of counts for the whole acquisition, while the CT can reach a few billion counts. Furthermore, PET data suffer from scatter and random events much more dramatically than CT data does.
In practice, considerable pre-processing of the data is required – correction for random coincidences, estimation and subtraction of scattered photons, detector dead-time correction (after the detection of a photon, the detector must “cool down” again) and detector-sensitivity correction (for both inherent detector sensitivity and changes in sensitivity due to angle of incidence).
Filtered back projection (FBP) has been frequently used to reconstruct images from the projections. This algorithm has the advantage of being simple while having a low requirement for computing resources. However, shot noise in the raw data is prominent in the reconstructed images and areas of high tracer uptake tend to form streaks across the image.
Iterative expectation-maximization algorithms are now the preferred method of reconstruction. The advantage is a better noise profile and resistance to the streak artifacts common with FBP, but the disadvantage is higher computer resource requirements.
Attenuation correction: As different LORs must traverse different thicknesses of tissue, the photons are attenuated differentially. The result is that structures deep in the body are reconstructed as having falsely low tracer uptake. Contemporary scanners can estimate attenuation using integrated x-ray CT equipment, however earlier equipment offered a crude form of CT using a gamma ray (positron emitting) source and the PET detectors.
While attenuation corrected images are generally more faithful representations, the correction process is itself susceptible to significant artifacts. As a result, both corrected and uncorrected images are always reconstructed and read together.
2D/3D reconstruction: Early PET scanners had only a single ring of detectors, hence the acquisition of data and subsequent reconstruction was restricted to a single transverse plane. More modern scanners now include multiple rings, essentially forming a cylinder of detectors.
There are two approaches to reconstructing data from such a scanner: 1) treat each ring as a separate entity, so that only coincidences within a ring are detected, the image from each ring can then be reconstructed individually (2D reconstruction), or 2) allow coincidences to be detected between rings as well as within rings, then reconstruct the entire volume together (3D).
3D techniques have better sensitivity (because more coincidences are detected and used) and therefore less noise, but are more sensitive to the effects of scatter and random coincidences, as well as requiring correspondingly greater computer resources.
More detailed applications list
PET is a valuable technique for some diseases and disorders, because it is possible to target the radio-chemicals used for particular bodily functions.
- Oncology: PET scanning with the tracer fluorine-18 (F-18) fluorodeoxyglucose (FDG), called FDG-PET, is widely used in clinical oncology. This tracer is a glucose analog that is taken up by glucose-using cells and phosphorylated by hexokinase (whose mitochondrial form is greatly elevated in rapidly-growing malignant tumours). A typical dose of FDG used in an oncological scan is 200-400 MBq for an adult human. Because the oxygen atom which is replaced by F-18 to generate FDG is required for the next step in glucose metabolism in all cells, no further reactions occur in FDG. Furthermore, most tissues (with the notable exception of liver and kidneys) cannot remove the phosphate added by hexokinase. This means that FDG is trapped in any cell which takes it up, until it decays, since phosphorylated sugars, due to their ionic charge, cannot exit from the cell. This results in intense radiolabeling of tissues with high glucose uptake, such as the brain, the liver, and most cancers. As a result, FDG-PET can be used for diagnosis, staging, and monitoring treatment of cancers, particularly in Hodgkin’s disease, non Hodgkin’s lymphoma, and lung cancer. Many other types of solid tumors will be found to be very highly labeled on a case-by-case basis– a fact which becomes especially useful in searching for tumor metastasis, or for recurrence after a known highly-active primary tumor is removed. Because individual PET scans are more expensive than “conventional” imaging with computed tomography (CT) and magnetic resonance imaging (MRI), expansion of FDG-PET in cost-constrained health services will depend on proper health technology assessment; this problem is a difficult one because structural and functional imaging often cannot be directly compared, as they provide different information. Oncology scans using FDG make up over 90% of all PET scans in current practice.
- Neurology: PET neuroimaging is based on an assumption that areas of high radioactivity are associated with brain activity. What is actually measured indirectly is the flow of blood to different parts of the brain, which is generally believed to be correlated, and has been measured using the tracer oxygen-15. However, because of its 2-minute half-life O-15 must be piped directly from a medical cyclotron for such uses, and this is difficult. In practice, since the brain is normally a rapid user of glucose, and since brain pathologies such as Alzheimer’s disease greatly decrease brain metabolism of both glucose and oxygen in tandem, standard FDG-PET of the brain, which measures regional glucose use, may also be successfully used to differentiate Alzheimer’s disease from other dementing processes, and also to make early diagnosis of Alzheimer’s disease. The advantage of FDG-PET for these uses is its much wider availability.
Several radiotracers (i.e. radioligands) have been developed for PET that are ligands for specific neuroreceptor subtypes (e.g. dopamine D2, serotonin 5-HT1A, etc.), transporters (such as [(11)C]McN5652, [(11)C]DASB or other novel tracer ligands for serotonin in this case), or enzyme substrates (e.g. 6-FDOPA for the AADC enzyme). These agents permit the visualization of neuroreceptor pools in the context of a plurality of neuropsychiatric and neurologic illnesses. A novel probe developed at the University of Pittsburgh termed PIB (Pittsburgh Compound-B) permits the visualization of amyloid plaques in the brains of Alzheimer’s patients. This technology could assist clinicians in making a positive clinical diagnosis of AD pre-mortem and aid in the development of novel anti-amyloid therapies.
- Cardiology, atherosclerosis and vascular disease study: In clinical cardiology, FDG-PET can identify so-called “hibernating myocardium“, but its cost-effectiveness in this role versus SPECT is unclear. Recently, a role has been suggested for FDG-PET imaging of atherosclerosis to detect patients at risk of stroke [2].
- Neuropsychology / Cognitive neuroscience: To examine links between specific psychological processes or disorders and brain activity.
- Psychiatry: Numerous compounds that bind selectively to neuroreceptors of interest in biological psychiatry have been radiolabeled with C-11 or F-18. Radioligands that bind to dopamine receptors (D1,D2, reuptake transporter), serotonin receptors (5HT1A, 5HT2A, reuptake transporter) opioid receptors (mu) and other sites have been used successfully in studies with human subjects. Studies have been performed examining the state of these receptors in patients compared to healthy controls in schizophrenia, substance abuse, mood disorders and other psychiatric conditions.
- Pharmacology: In pre-clinical trials, it is possible to radiolabel a new drug and inject it into animals. The uptake of the drug, the tissues in which it concentrates, and its eventual elimination, can be monitored far more quickly and cost effectively than the older technique of killing and dissecting the animals to discover the same information. PET scanners for rats and apes are marketed for this purpose. The technique is still generally too expensive for the veterinary medicine market, however, so very few pet PET scans are done. Drug occupancy at the purported site of action can also be inferred indirectly by competition studies between unlabeled drug and radiolabeled compounds known apriori to bind with specificity to the site.
PET scan safety
PET scanning is non-invasive, but it does involve exposure to ionizing radiation. The total dose of radiation is small, however, usually around 7 mSv. This can be compared to 2.2 mSv average annual background radiation in the UK, 0.02 mSv for a chest x-ray, up to 8 mSv for a CT scan of the chest, 2-6 mSv per annum for aircrew (data from UK National Radiological Protection Board).
Availability
In Canada, availability varies from province to province [3]. In Ontario, PET scan costs are not covered under the government-funded public health system (OHIP), but scans are available from a few public and private facilities at a cost equivalent of approximately $2500 USD. [4]
See also
References
- ↑ Simon Cherry, et al. Physics in Nuclear Medicine. Saunders Publishing. 2003. p.3
- ↑ Phelps ME, Hoffman EJ, Mullani NA, Ter-Pogossian MM. “Application of annihilation coincidence detection to transaxial reconstruction tomography.” Journal of Nuclear Medicine. 1975; 16(3):210-24.
- ↑ http://www.medicalimagingmag.com/issues/articles/2003-07_05.asp
Additional Resources
- Young H, Baum R, Cremerius U; et al. (1999). “Measurement of clinical and subclinical tumour response using [18F]-fluorodeoxyglucose and positron emission tomography: review and 1999 EORTC recommendations”. European Journal of Cancer. 35 (13): 1773–1782.
- Bustamante E. and Pedersen P.L. (1977). “High aerobic glycolysis of rat hepatoma cells in culture: role of mitochondrial hexokinase”. Proceedings of the National Academy of Sciences USA. 74 (9): 3735–3739.
- Klunk WE, Engler H, Nordberg A, Wang Y, Blomqvist G, Holt DP, Bergstrom M, Savitcheva I, Huang GF, Estrada S, Ausen B, Debnath ML, Barletta J, Price JC, Sandell J, Lopresti BJ, Wall A, Koivisto P, Antoni G, Mathis CA, and Langstrom B. (2004). “Imaging brain amyloid in Alzheimer’s disease with Pittsburgh Compound-B”. Annals of Neurology. 55 (3): 306–319.
da:Positronemissionstomografi de:Positronen-Emissions-Tomographie eo:Pozitrona Emisia Tomografio fa:پت اسکن gl:PET is:PET-skanni it:Tomografia ad emissione di positroni he:PET hu:Pozitron emissziós tomográfia nl:Positronemissietomografie no:Positronemisjonstomografi fi:Positroniemissiotomografia sv:Positronemissionstomografi
The Genetic Basis of Heart Disease
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]
Overview
The following is a list of genetic disorders and their origins. Besides, most disorders are a code that indicates the type of fertilization and the chromosome involved.
- P – Point mutation, or any insertion/deletion entirely inside one gene
- D – Deletion of a gene or genes
- C – Whole chromosome extra, missing, or both – see chromosomal aberrations
- T – Trinucleotide repeat disorders – gene is extended in length
Common disorders
| Disorder | Mutation | Chromosome |
|---|---|---|
| 22q11.2 deletion syndrome | D | 22q |
| Angelman syndrome | DCP | 15 |
| Canavan disease | 17p | |
| Celiac disease | ||
| Charcot-Marie-Tooth disease | ||
| Color blindness | P | X |
| Cri du Chat | D | 5 |
| Cystic fibrosis | P | 7q |
| Down syndrome | C | 21 |
| Duchenne muscular dystrophy | D | Xp |
| Hemophilia | P | X |
| Klinefelter syndrome | C | X |
| Neurofibromatosis | 17q/22q/? | |
| Phenylketonuria | P | 12q |
| Prader-Willi syndrome | DC | 15 |
| Sickle-cell disease | P | 11p |
| Spina bifida | P | 1 |
| Tay-Sachs disease | P | 15 |
| Turner syndrome | C | X |
0–9
| Disorder | Mutation | Chromosome |
|---|---|---|
| 18p deletion syndrome | D | 18p |
| 21-hydroxylase deficiency | 6p21.3 | |
| 45,X see Turner syndrome |
C | X |
| 47,XX,+21 see Down syndrome |
C | 21 |
| 47,XXX see triple X syndrome |
C | X |
| 47,XXY see Klinefelter syndrome |
C | X |
| 47,XY,+21 see Down syndrome |
C | 21 |
| 47,XYY syndrome | C | Y |
| 5-ALA dehydratase-deficient porphyria see ALA dehydratase deficiency |
||
| 5-aminolaevulinic dehydratase deficiency porphyria see ALA dehydratase deficiency |
||
| 5p deletion syndrome see Cri du chat |
D | 5p |
| 5p- syndrome see Cri du chat |
D | 5p |
A
B
C
D
E
| Disorder | Mutation | Chromosome |
|---|---|---|
| Early-Onset familial alzheimer disease (EOFAD) see Alzheimer disease#type 1 see Alzheimer disease#type 3 see Alzheimer disease#type 4 |
||
| EDS see Ehlers-Danlos syndrome |
||
| Ehlers-Danlos syndrome | ||
| Ekman-Lobstein disease see osteogenesis imperfecta |
||
| Entrapment neuropathy see hereditary neuropathy with liability to pressure palsies |
||
| Epiloia see tuberous sclerosis |
||
| EPP see erythropoietic protoporphyria |
||
| Erythroblastic anemia see beta thalassemia |
||
| Erythrohepatic protoporphyria see erythropoietic protoporphyria |
||
| Erythroid 5-aminolevulinate synthetase deficiency see X-linked sideroblastic anemia |
||
| Erythropoietic porphyria see congenital erythropoietic porphyria |
||
| erythropoietic protoporphyria | ||
| Erythropoietic uroporphyria see congenital erythropoietic porphyria |
||
| Eye cancer see retinoblastoma FA – Friedreich ataxia see Friedreich ataxia |
F
G
| Disorder | Mutation | Chromosome |
|---|---|---|
| G6PD deficiency |
||
| Galactokinase deficiency disease see galactosemia |
||
| Galactose-1-phosphate uridyl-transferase deficiency disease see galactosemia |
||
| galactosemia | ||
| Galactosylceramidase deficiency disease see Krabbe disease |
||
| Galactosylceramide lipidosis see Krabbe disease |
||
| galactosylcerebrosidase deficiency see Krabbe disease |
||
| galactosylsphingosine lipidosis see Krabbe disease |
||
| GALC deficiency see Krabbe disease |
||
| GALT deficiency see galactosemia |
||
| Gaucher disease | ||
| Gaucher-like disease see pseudo-Gaucher disease |
||
| GBA deficiency see Gaucher disease type 1 |
||
| GD see Gaucher’s disease |
||
| Genetic brain disorders | ||
| genetic emphysema see alpha-1 antitrypsin deficiency |
||
| genetic hemochromatosis see hemochromatosis |
||
| Giant cell hepatitis, neonatal see Neonatal hemochromatosis |
||
| GLA deficiency see Fabry disease |
||
| Glioblastoma, retinal see retinoblastoma |
||
| Glioma, retinal see retinoblastoma |
||
| globoid cell leukodystrophy (GCL, GLD) see Krabbe disease |
||
| globoid cell leukoencephalopathy see Krabbe disease |
||
| Glucocerebrosidase deficiency see Gaucher disease |
||
| Glucocerebrosidosis see Gaucher disease |
||
| Glucosyl cerebroside lipidosis see Gaucher disease |
||
| Glucosylceramidase deficiency see Gaucher disease |
||
| Glucosylceramide beta-glucosidase deficiency see Gaucher disease |
||
| Glucosylceramide lipidosis see Gaucher disease |
||
| Glyceric aciduria see hyperoxaluria, primary |
||
| Glycine encephalopathy see Nonketotic hyperglycinemia |
||
| Glycolic aciduria see hyperoxaluria, primary |
||
| GM2 gangliosidosis, type 1 see Tay-Sachs disease |
||
| Goiter-deafness syndrome see Pendred syndrome |
||
| Graefe-Usher syndrome see Usher syndrome |
||
| Gronblad-Strandberg syndrome see pseudoxanthoma elasticum |
||
| Guenther porphyria see congenital erythropoietic porphyria |
||
| Gunther disease see congenital erythropoietic porphyria |
| Disorder | Mutation | Chromosome |
|---|---|---|
| Haemochromatosis see hemochromatosis |
||
| Hallgren syndrome see Usher syndrome |
||
| Hb S disease see sickle cell anemia |
||
| HCH see hypochondroplasia |
||
| HCP see hereditary coproporphyria |
||
| Head and brain malformations | ||
| Hearing disorders and deafness | ||
| Hearing problems in children | ||
| HEF2A see hemochromatosis#type 2 |
||
| HEF2B see hemochromatosis#type 2 |
||
| Hematoporphyria see porphyria |
||
| Heme synthetase deficiency see erythropoietic protoporphyria |
||
| Hemochromatoses see hemochromatosis |
||
| hemochromatosis | ||
| hemoglobin M disease see methemoglobinemia#beta-globin type |
||
| Hemoglobin S disease see sickle cell anemia |
||
| hemophilia | ||
| HEP see hepatoerythropoietic porphyria |
||
| hepatic AGT deficiency see hyperoxaluria, primary |
||
| hepatoerythropoietic porphyria | ||
| Hepatolenticular degeneration syndrome see Wilson disease |
||
| Hereditary arthro-ophthalmopathy see Stickler syndrome |
||
| Hereditary coproporphyria | ||
| Hereditary dystopic lipidosis see Fabry disease |
||
| Hereditary hemochromatosis (HHC) see hemochromatosis |
||
| Hereditary iron-loading anemia see X-linked sideroblastic anemia |
||
| Hereditary motor and sensory neuropathy see Charcot-Marie-Tooth disease |
||
| Hereditary motor neuronopathy see spinal muscular atrophy |
||
| Hereditary motor neuronopathy, type V see distal spinal muscular atrophy, type V |
||
| Hereditary Multiple Exostoses | ||
| Hereditary nonpolyposis colorectal cancer | DNA mismatch repair dysfunction usually in MSH2 and MLH1 genes | usually chromosomes 2 and 3 |
| Hereditary periodic fever syndrome see Mediterranean fever, familial |
||
| Hereditary Polyposis Coli see familial adenomatous polyposis |
||
| Hereditary pulmonary emphysema see alpha-1 antitrypsin deficiency |
||
| Hereditary resistance to activated protein C see factor V Leiden thrombophilia |
||
| Hereditary sensory and autonomic neuropathy type III see familial dysautonomia |
||
| Hereditary spastic paraplegia see infantile-onset ascending hereditary spastic paralysis |
||
| Hereditary spinal ataxia see Friedreich ataxia |
||
| Hereditary spinal sclerosis see Friedreich ataxia |
||
| Herrick’s anemia see sickle cell anemia |
||
| Heterozygous OSMED see Weissenbacher-Zweymüller syndrome |
||
| Heterozygous otospondylomegaepiphyseal dysplasia see Weissenbacher-Zweymüller syndrome |
||
| HexA deficiency see Tay-Sachs disease |
||
| Hexosaminidase A deficiency see Tay-Sachs disease |
||
| Hexosaminidase alpha-subunit deficiency (variant B) see Tay-Sachs disease |
||
| HFE-associated hemochromatosis see hemochromatosis |
||
| HGPS see Hutchinson-Gilford progeria syndrome |
||
| Hippel-Lindau disease see von Hippel-Lindau disease |
||
| HLAH see hemochromatosis |
||
| HMN V see distal spinal muscular atrophy, type V |
||
| HMSN see Charcot-Marie-Tooth disease |
||
| HNPCC see hereditary nonpolyposis colorectal cancer |
||
| HNPP see hereditary neuropathy with liability to pressure palsies |
||
| homocystinuria | ||
| Homogentisic acid oxidase deficiency see alkaptonuria |
||
| Homogentisic acidura see alkaptonuria |
||
| Homozygous porphyria cutanea tarda see hepatoerythropoietic porphyria |
||
| HP1 see hyperoxaluria, primary |
||
| HP2 see hyperoxaluria, primary |
||
| HPA see hyperphenylalaninemia |
||
| HPRT – Hypoxanthine-guanine phosphoribosyltransferase deficiency see Lesch-Nyhan syndrome |
||
| HSAN type III see familial dysautonomia |
||
| HSAN3 see familial dysautonomia |
||
| HSN-III see familial dysautonomia |
||
| Human dermatosparaxis see Ehlers-Danlos syndrome#dermatosparaxis type |
||
| Huntington disease | T | gene IT-15 on chromosome 4 |
| Huntington’s disease see Huntington disease |
||
| Hutchinson-Gilford progeria syndrome | ||
| Hyperandrogenism, nonclassic type, due to 21-hydroxylase deficiency see 21-hydroxylase deficiency |
||
| Hyperchylomicronemia, familial see lipoprotein lipase deficiency, familial |
||
| hyperglycinemia with ketoacidosis and leukopenia see propionic acidemia |
||
| Hyperlipoproteinemia type I see lipoprotein lipase deficiency, familial |
||
| hyperoxaluria, primary | ||
| hyperphenylalaninemia see hyperphenylalaninemia |
||
| hyperphenylalaninemia | ||
| Hypochondrodysplasia see hypochondroplasia |
||
| hypochondrogenesis | ||
| hypochondroplasia | ||
| Hypochromic anemia see X-linked sideroblastic anemia |
||
| Hypocupremia, congenital see Menkes syndrome |
||
| hypoxanthine phosphoribosyltransferse (HPRT) deficiency see Lesch-Nyhan syndrome |
I
| Disorder | Mutation | Chromosome |
|---|---|---|
| IAHSP see infantile-onset ascending hereditary spastic paralysis |
||
| idiopathic hemochromatosis see hemochromatosis, type 3 |
||
| Idiopathic neonatal hemochromatosis see hemochromatosis, neonatal |
||
| Idiopathic pulmonary hypertension see primary pulmonary hypertension |
||
| Immune system disorders see X-linked severe combined immunodeficiency |
||
| Incontinentia Pigmenti | P | Xq28 |
| Infantile cerebral Gaucher’s disease see Gaucher disease type 2 |
||
| Infantile Gaucher disease see Gaucher disease type 2 |
||
| infantile-onset ascending hereditary spastic paralysis | ||
| Infertility | ||
| inherited emphysema see alpha-1 antitrypsin deficiency |
||
| Inherited human transmissible spongiform encephalopathies see prion disease |
||
| inherited tendency to pressure palsies see hereditary neuropathy with liability to pressure palsies |
||
| Insley-Astley syndrome see otospondylomegaepiphyseal dysplasia |
||
| Intermittent acute porphyria syndrome see acute intermittent porphyria |
||
| Intestinal polyposis-cutaneous pigmentation syndrome see Peutz-Jeghers syndrome |
||
| IP see incontinentia pigmenti |
||
| Iron storage disorder see hemochromatosis |
||
| Isodicentric 15 see idic15 |
Inv dup | 15q11-14 |
| Isolated deafness see nonsyndromic deafness |
J
| Disorder | Mutation | Chromosome |
|---|---|---|
| Jackson-Weiss syndrome | ||
| JH see Haemochromatosis#type 2 |
||
| Joubert syndrome | ||
| JPLS see Juvenile Primary Lateral Sclerosis |
ALS2 | |
| juvenile amyotrophic lateral sclerosis see Amyotrophic lateral sclerosis#type 2 |
||
| Juvenile gout, choreoathetosis, mental retardation syndrome see Lesch-Nyhan syndrome |
||
| juvenile hyperuricemia syndrome see Lesch-Nyhan syndrome |
||
| JWS see Jackson-Weiss syndrome |
K
| Disorder | Mutation | Chromosome |
|---|---|---|
| KD see X-linked spinal-bulbar muscle atrophy |
||
| Kennedy disease see X-linked spinal-bulbar muscle atrophy |
||
| Kennedy spinal and bulbar muscular atrophy see X-linked spinal-bulbar muscle atrophy |
||
| Kerasin histiocytosis see Gaucher disease |
||
| Kerasin lipoidosis see Gaucher disease |
||
| Kerasin thesaurismosis see Gaucher disease |
||
| ketotic glycinemia see propionic acidemia |
||
| ketotic hyperglycinemia see propionic acidemia |
||
| Kidney diseases see hyperoxaluria, primary |
||
| Kinky hair syndrome see Menkes syndrome |
||
| Klinefelter syndrome | ||
| Klinefelter’s syndrome see Klinefelter syndrome |
||
| Kniest dysplasia | ||
| Krabbe disease |
L
M
N
O
| Disorder | Mutation | Chromosome |
|---|---|---|
| Ochronosis see alkaptonuria |
||
| Ochronotic arthritis see alkaptonuria |
||
| OI see osteogenesis imperfecta |
||
| OSMED see otospondylomegaepiphyseal dysplasia |
||
| osteogenesis imperfecta | ||
| Osteopsathyrosis see osteogenesis imperfecta |
||
| Osteosclerosis congenita see achondroplasia |
||
| Oto-spondylo-megaepiphyseal dysplasia see otospondylomegaepiphyseal dysplasia |
||
| otospondylomegaepiphyseal dysplasia | ||
| Oxalosis see hyperoxaluria, primary |
||
| Oxaluria, primary see hyperoxaluria, primary |
P
R
| Disorder | Mutation | Chromosome |
|---|---|---|
| Rb see retinoblastoma |
||
| Recklinghausen disease, nerve see neurofibromatosis 1 |
||
| Recurrent polyserositis see Mediterranean fever, familial |
||
| Retinal disorders | ||
| Retinitis pigmentosa-deafness syndrome see Usher syndrome |
||
| retinoblastoma | ||
| Rett syndrome | ||
| RFALS type 3 see Amyotrophic lateral sclerosis#type 2 |
||
| Ricker syndrome see Myotonic dystrophy#type 2 |
||
| Riley-Day syndrome see familial dysautonomia |
||
| Roussy-Levy syndrome see Charcot-Marie-Tooth disease |
||
| RSTS see Rubinstein-Taybi syndrome |
||
| RTS see Rett syndrome see Rubinstein-Taybi syndrome |
||
| RTT see Rett syndrome |
||
| Rubinstein-Taybi syndrome |
S
T
U
| Disorder | Mutation | Chromosome |
|---|---|---|
| UDP-galactose-4-epimerase deficiency disease see galactosemia |
||
| UDP glucose 4-epimerase deficiency disease see galactosemia |
||
| UDP glucose hexose-1-phosphate uridylyltransferase deficiency see galactosemia |
||
| Ullrich-Noonan syndrome see Noonan syndrome |
||
| Ullrich-Turner syndrome see Turner syndrome |
||
| Undifferentiated deafness see nonsyndromic deafness |
||
| UPS deficiency see acute intermittent porphyria |
||
| Urinary bladder cancer see bladder cancer |
||
| UROD deficiency see porphyria cutanea tarda |
||
| Uroporphyrinogen decarboxylase deficiency see porphyria cutanea tarda |
||
| Uroporphyrinogen synthase deficiency see acute intermittent porphyria |
||
| UROS deficiency see congenital erythropoietic porphyria |
||
| Usher syndrome | ||
| UTP hexose-1-phosphate uridylyltransferase deficiency see galactosemia |
V
| Disorder | Mutation | Chromosome |
|---|---|---|
| Van Bogaert-Bertrand syndrome see Canavan disease |
||
| Van der Hoeve syndrome see osteogenesis imperfecta#Type I |
||
| variegate porphyria | ||
| Velocardiofacial syndrome see 22q11.2 deletion syndrome |
D | 22q |
| VHL syndrome see von Hippel-Lindau disease |
||
| Vision impairment and blindness see Alstrom syndrome |
||
| Von Bogaert-Bertrand disease see Canavan disease |
||
| von Hippel-Lindau disease | ||
| Von Recklenhausen-Applebaum disease see hemochromatosis |
||
| von Recklinghausen disease see neurofibromatosis 1 |
||
| VP see variegate porphyria |
||
| Vrolik disease see osteogenesis imperfecta |
W
| Disorder | Mutation | Chromosome |
|---|---|---|
| Waardenburg syndrome | ||
| WD – Wilson’s disease see Wilson disease |
||
| Weissenbacher-Zweymüller syndrome | ||
| Wilson disease | ||
| Wilson’s disease see Wilson disease |
||
| Wolff Periodic disease see Mediterranean fever, familial |
||
| WZS see Weissenbacher-Zweymüller syndrome |
X
Y
| Disorder | Mutation | Chromosome |
|---|---|---|
| YY syndrome see 47,XYY syndrome |
hu:Genetikai betegségek listája nl:Lijst van erfelijke aandoeningen
Congenital Heart Disease
Click on Show on the right to expand:
For patient information, click here
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-In-Chief: Priyamvada Singh, MBBS [2] Assistant Editor(s)-In-Chief: Kristin Feeney, B.S. [3]
Synonyms and keywords: CHD; cardiac malformation
Congenital heart disease (CHD) is the most common type of birth defect, accounting for about 1% of all cases [4]. Although mild cases of CHD are not detected until after discharge, most of the critical CHD cases are identified soon after birth requiring surgery or catheter-based intervention in the first year of life. CHD is broadly classified into three major groups, namely, cyanotic CHD, ductal-dependent CHD and critical CHD. Cyanotic CHD involves defects that lead to mixing of deoxygenated blood into the systemic circulation. Ductal-dependent CHD relies on the patency of the ductus arteriosus for supply of blood to the pulmonary or systemic outflow which allows adequate mixing between the parallel circulations. Lesions requiring surgery or catheter-based intervention in the first year of life are referred to as critical CHD which includes ductal-dependent and cyanotic lesions, as well as forms of CHD that, although not requiring surgery in the neonatal period, do necessitate intervention in the first year of life, such as a big ventricular septal defect or an atrioventricular canal defect (or atrioventricular septal defect).
Aortic stenosis | Atrial septal defect (ASD) | Atrial septal defect sinus venosus | Atrioventricular canal | Atrioventricular septal defect (AVSD) | Bicuspid aortic valve | Brugada syndrome | Cardiomyopathy | Coarctation of the aorta (CoA) | dextro-Transposition of the great arteries (d-TGA) | Dextrocardia | Ebstein’s anomaly | Hypoplastic left heart syndrome (HLHS) | Hypoplastic right heart syndrome | Interrupted aortic arch (IAA) | levo-Transposition of the great arteries (l-TGA) | Lutembacher’s syndrome | Mitral stenosis | Ostium primum | Ostium secundum | Partial anomalous pulmonary venous connection (PAPVC) | Patent ductus arteriosus (PDA) | Pulmonary atresia | Pulmonary stenosis | Septum primum | Subaortic stenosis | Tetralogy of Fallot (ToF) | Total anomalous pulmonary venous connection (TAPVC) | Tricuspid atresia | Truncus arteriosus | Ventricular septal defect (VSD)
Diagnosis
Diagnostic Criteria | History and Symptoms | Physical Examination | Laboratory Findings | Electrocardiogram | Chest X Ray | MRI | CT | Echocardiography | Prenatal Ultrasound | Other Imaging Findings
Treatment
Medical Therapy | Surgery | Prevention | Outcomes | Reproduction
Case Studies
Related Chapters
Cardiac Disease in Pregnancy
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-In-Chief: Cafer Zorkun, M.D., Ph.D. [2]; Anjan K. Chakrabarti, M.D. [3]; Lakshmi Gopalakrishnan, M.B.B.S. [4]
Diagnosis
History and Symptoms | Physical Examination | Electrocardiogram | Exercise Testing | Radiation Exposure | Chest X Ray | Echocardiography | MRI | CT | Pulmonary artery catheterization | Cardiac catheterization | Cardiac Ablation
Treatment
Cardiovascular Drug Therapy During Pregnancy | Labor and delivery | Resuscitation in Late Pregnancy
Prevention
Contraindications to pregnancy
Cardiac Conditions Associated with Complications
I. Pre-existing Cardiac Disease
II. Valvular Heart Disease
III. Cardiomyopathy
IV. Cardiac diseases that may develop During Pregnancy
External Links
Cardiac Diseases in AIDS
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Raviteja Guddeti, M.B.B.S. [2]
Diagnosis
History and Symptoms | Physical Examination | Laboratory Findings | Electrocardiogram | Chest X Ray | Echocardiography | Other Imaging Findings | Other Diagnostic Studies
Treatment
Medical Therapy | Surgery | Prevention | Cost-Effectiveness of Therapy | Future or Investigational Therapies
Case Studies
Diseases of the Pericardium
For patient information, click here.
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Homa Najafi, M.D.[2]Varun Kumar, M.B.B.S.; Cafer Zorkun, M.D., Ph.D. [3]
Synonyms and keywords:acute pericarditis, chronic pericarditis, idiopathic pericarditis, recurrent pericarditis, chronic effusive pericarditis, chronic constrictive pericarditis, inflammation of the pericardium, pericardial inflammation, inflammation of the pericardial sac, serous pericarditis, purulent pericarditis, hemorrhagic pericarditis, fibrinous pericarditis, caseous pericarditis, bacterial pericarditis, viral pericarditis, fungal pericarditis, parasitic pericarditis, autoimmune pericarditis, neoplastic pericarditis, metabolic pericarditis, traumatic pericarditis, iatrogenic pericarditis, drug-related pericarditis, postoperative pericarditis, post-operative pericarditis, post-surgery pericarditis, postsurgery pericarditis, acute recurrent pericarditis, radiation induced pericarditis, radiation-induced pericarditis, uremic pericarditis, radiation induced constrictive pericarditis, children pericarditis, pericarditis in children
HIV | Post-MI | Post-pericardiotomy | Radiation | Tuberculosis | Uremia | Malignancy
Pericardial Effusion | Cardiac Tamponade | Constrictive Pericarditis
Diagnosis
History and Symptoms | Physical Examination | Laboratory Findings | Electrocardiogram | EKG Examples | Chest X Ray | MRI | CT | Echocardiography | Other Imaging Findings
Treatment
Medical Therapy | Pericardiocentesis | Pericardial Window | Pericardial Stripping | Treatment Related Videos
Case Studies
Related Chapters
Trauma and the Heart
For patient information, click here
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Maryam Hadipour, M.D.[2]
Synonyms and keywords: Commotion of the heart
Diagnosis
History and Symptoms | Physical Examination | Laboratory Findings | Electrocardiogram | Echocardiography or Ultrasound | Other Imaging Findings | Other Diagnostic Studies
Treatment
Medical Therapy | Primary Prevention | Secondary Prevention | Cost-Effectiveness of Therapy | Future or Investigational Therapies
Case Studies
Template:Injuries, other than fractures, dislocations, sprains and strains
de:Herzverletzung
Diseases of the Valvular Structures
Aortic Stenosis | Aortic Regurgitation | Mitral Stenosis | Mitral Regurgitation | Mitral Valve Prolapse | Pulmonic Regurgitation | Pulmonic Stenosis | Tricuspid Valve Prolapse | Tricuspid Regurgitation | Tricuspid Stenosis | Infective Endocarditis
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]
Diseases of the Myocardium
Cardiomegaly | Cardiomyopathy | Congestive Heart Failure | Left Ventricular Hypertrophy | Myocarditis
Cardiac Arrhythmias
VASCULAR MEDICINE
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Assistant Editor(s)-in-Chief: Rim Halaby; Serge Korjian
Overview
- Cardiac electrophysiology (also referred to as clinical cardiac electrophysiology , or electrophysiology) is the science of the mechanisms, functions, and performance of the electrical activities of specific regions of the heart.
- The normal electrical conduction in the heart allows the impulse that is generated by the sinoatrial node (SA node) of the heart to be propagated to (and stimulate) the myocardium (Cardiac muscle). The myocardium contracts after stimulation. It is the ordered stimulation of the myocardium that allows efficient contraction of the heart, thereby allowing blood to be pumped throughout the body.
Cardiac Conduction System
- Proper cardiac function heavily depends on the ability of the cardiomyocytes to receive and propagate an electrical impulse allowing the heart to contract.
- These impulses, known as action potentials, originate and travel through the cardiac conduction system.
- A time-ordered propagation of the electrical impulse through the myocardium allows efficient contraction of all four chambers of the heart, starting with the atria pumping the blood toward the ventricles, followed by the ventricles which contribute to the pulmonary and systemic circulation.
The Components of the Cardiac Conduction System:
- The sinus (sinoatrial) node
- The internodal tracts
- The atrioventricular (AV) node
- The His/AV bundle
- The right and left bundle branches,
- The Purkinje fibers.
The Direction of Propagation of the Action Potential:
- The initial cardiac impulse, produced by pacemaker cells, originates in the sinoatrial (SA) node at the intersection of the right atrium and the superior vena cava.
- This action potential is the trigger of every cardiac cycle, initiating the atrial then ventricular contractions; it is henceforth responsible for the rhythmic beating of the heart.
- This action potential then propagates as a wave of depolarization through the internodal tracts initiating atrial contraction and then converging at the AV node.
- The convergence occurs because, in a normal heart, the AV node is the only electrical connection between the atria and the ventricles.
- The conduction of this potential is delayed at the AV node mainly due to the slower depolarization in these cells.
- This delay is represented as the PR interval of the ECG.
- The electrical impulse then moves to the ventricles by means of the AV or His bundle located in the superior portion of the interventricular septum.
- It then continues moving apically and propagating through both [[]]ventricles via the right and left bundle branches, and the Purkinje fibers.[1][2][3][4]
-
Section of the heart showing the ventricular septum.
-
Schematic representation of the atrioventricular bundle of His.
- Similarly to skeletal muscle cells which are also striated muscles, the cardiomyocytes contract in response to a rapid alteration in the cell membrane’s potential.
- However, the cardiomyocytes differ from skeletal muscle cells by three important variations that are essential for cardiac function:
- 1) They can self-generate a change in cell membrane potential.
- 2) The action potential can be transmitted directly from cell to cell.
- 3) The action potentials have a significantly longer duration.
The Resting Membrane Potential
- All cells including cardiomyocytes have a resting membrane potential that is maintained assuming there is no electrical charge crossing the membrane from the intracellular towards the extracellular milieu or vice versa.
- This potential is estimated to be –80 to –90 mV.
- The most crucial ions that determine this resting potential are:
- Sodium (Na+)
- Calcium (Ca2+)
- Potassium (K+)
- Sodium (Na+) and calcium (Ca2+) are most present in the interstitial fluid, while potassium (K+) is more present in intracellularly.
- These ions are lipid insoluble which prevents them from crossing the lipid bilayer or the cell membrane.
- Alternatively, ions cross via specific protein structures in the cell membrane that may be either: ion channels, ion pumps, or ion exchangers.
- These transmembrane proteins are highly specific and allow only one type of ion to pass through which allows good maintenance of the membrane potential.
- Ion channels can be opened, inactivated or closed depending on complex factors that modulate their activity.
The Cardiac Action Potential
- The cardiac contraction action potential is divided into 5 phases.
Phase 0: Depolarization
- The initial rapid increase in the transmembrane potential from -80mV to approximately +30mV constitutes the Phase 0 or the depolarization phase.
- This depolarization results from a rapid increase in the membrane permeability to Na+ ions via opening of voltage-dependent fast Na+ channels allowing Na+ ions to move intracellularly according to their electrochemical gradient.
- Following the conduction of an action potential, a recovery phase is attained where a large number of Na+ channels are inactivated, preventing the conduction of a second action potential.
- When the membrane is fully repolarized, these channels are reactivated and allow the conduction of the following action potential.
Phase I: Initial Repolarization
- The phase I of the action potential, known as the initial rapid repolarization ensues, resulting from K+ and Cl- ion flux across the membrane.
- This forms the notch seen in the action potential following the depolarization.
Phase II: Plateau
- Phase II, almost exclusive to cardiomyocytes, represents a plateau in the membrane potential as an outcome of the equilibrium between Ca2+ influx and K+ outflow.
- The channels responsible for this Ca2+ influx are known as the L-type calcium channels, which are activated rapidly when the membrane potential reaches -50mV, but are slowly inactivated thereafter.
- Throughout this plateau phase, few Na+ channels also remain active.
- These are Na+/Ca2+ exchangers that allow 1 ion of calcium to move outside the cell for every 3 molecules of sodium moving inside the cell.
Phase III: Repolarization
- The third phase, also known as rapid repolarization, depicts the restoration of a resting membrane potential.
- It is initiated by inactivation of the L-type calcium channels and an increase in K+ outflow.
- This change in potassium across the membrane is related to 3 K+ currents:
- 1) Inwardly rectifying K+ current (IK1) à Produces the resting membrane potential
- 2) Transient outward K+ current (ITO) à Accounts for initial part of repolarization
- 3) Delayed outward K+ current (IK) à Responsible for final part of repolarization
- After repolarization has occurred, intracellular Na+ and extracellular K+ are rearranged via the Na+/K+ ATPase pump.
- The ATPase moves 3 sodium ions out for every 2 potassium ions moved intracellularly.
- Equilibrium of ions across the membrane is also achieved via the Na+/Ca2+ exchangers.
Phase IV: Diastolic depolarization
- The phase IV of the action potential is characterized by a diastolic depolarization that is both spontaneous and slow.
- This phase provides cardiac cells with features of automaticity.
- In a normal functioning heart, only the sinoatrial node is able to reach a threshold potential during phase IV making it the pacemaker of the heart.
- Nevertheless other cells including those in the AV node, the His bundle, and the Purkinje fibers are able to reach a threshold and fire automatically if they are not suppressed by the SA node, which is true in some disease entities.
The factors responsible for the initial diastolic depolarization in the SA node are:
- Inward Ca2+ current
- Delayed outward K+ current
- IF Currents – Inward sodium-potassium currents activated if membrane repolarizes below the If threshold
- T-type Ca2+ channel – Releases calcium from internal stores
The rate of impulse generation by the SA node is determined by 3 factors:
- 1) The slope of diastolic depolarization
- 2) The maximal diastolic potential
- 3) The threshold potential
- All these factors are controlled by the autonomic nervous system allowing for the modulation of the rate of SA node firing and subsequently the heart rate.[1][5][3][4]
Electrophysiology Studies and Therapeutic Modalities
Overview
- An electrophysiologic study is a term used to describe a number of invasive (intracardiac) and non-invasive recording of spontaneous electrical activity as well as of cardiac responses to programmed electrical stimulation.
- These studies are performed to assess arrhythmias, elucidate symptoms, evaluate abnormal electrocardiograms, assess risk of developing arrhythmias in the future, and design treatment.
- These procedures increasingly include therapeutic methods (typically radiofrequency ablation) in addition to diagnostic and prognostic procedures.
- Other therapeutic modalities employed in this field include antiarrhythmic drug therapy and implantation of pacemakers and implantable cardioverter-defibrillators.
- A specialist in cardiac electrophysiology is known as a cardiac electrophysiologist, or (more commonly) simply an electrophysiologist. Cardiac electrophysiology is considered a subspecialty of cardiology, and in most countries requires two or more years of fellowship training beyond a general cardiology fellowship. They are trained to perform interventional cardiac EP procedures as well as surgical device implantations.
Diagnostic Testing
- Ambulatory electrocardiographic monitoring (Holter recording and interpretation; loop recording and interpretation)
- Tilt table testing
- Signal-averaged electrocardiogram (SAECG) interpretation, also referred to as “late potentials” reading
- Electrophysiologic study (EPS)
- Pacing and recording electrodes are inserted either in the esophagus (intra-esophageal EPS) or, through blood vessels, directly into the heart chambers (intra-cardiac EPS) in order to measure electrical properties of the heart. In addition, intra-cardiac EPS electrically stimulates the heart and induces arrhythmias for diagnostic purposes (“programmed electrical stimulation”).
Medical Treatment
Electrophysiologists play a role in:
- The initial administration and monitoring of the effect of drugs for treatment of heart rhythm disorders
- The management of severe or life threatening arrhythmias
- The management of arrythmias requiring multiple drugs use
Catheter Ablation
- Ablation therapy is the catheter based creation of lesions in the heart with radiofrequency energy, cryotherapy (destructive freezing), or ultrasound energy in order to cure or control arrhythmias (see radiofrequency ablation). Ablation is usually performed during the same procedure as the electrophysiology study which induces and confirms the diagnosis of the arrhythmia for which ablation therapy is sought.
Non-complex ablation
- It includes ablation for arrhythmias such as: AV nodal reentrant tachycardia, accessory pathway mediated tachycardia and atrial flutter.
- This procedure is usually performed using intracardiac catheters , fluoroscopy (a real-time X-ray camera), and electrical recordings from the inside of the heart.
Complex ablation
- It includes ablation for arrhythmias such as: multifocal atrial tachycardia, atrial fibrillation, and ventricular tachycardia.
- In addition to the apparatus used for a “non-complex” ablation, these procedures often make use of sophisticated computer mapping systems to localize the source of the abnormal rhythm and to direct delivery of ablation lesions.
Surgical Procedures: Pacemaker and Defibrillator Implantation and Follow Up
- Implantation of single and dual chamber pacemakers and defibrillators
- Implantation of “biventricular” pacemakers and defibrillators for patients with congestive heart failure
- Implantation of loop recorders (implanted ECG recorders for long term monitoring of ECG to allow for diagnosis of an arrhythmia)
- Clinical follow up and reprogramming of implanted devices
Abnormalities in Cardiac Electrophysiology
- Mechanism of Arrhythmias
- Diseases of the Conduction System and Bradyarrhythmias
- Narrow Complex Tachycardias
- Wide Complex Tachycardias
- Ventricular Tachyarrhythmias, Cardiac Arrest and Sudden Cardiac Death
- Arrhythmias in Pregnancy
Treatment Modalities for Arrhythmia
- Antiarrhythmic Medications
- Indications for Pacemakers
- Indications for an ICD
- Cardiac Resynchronization Therapy
- Catheter ablation
See also
- Clinical cardiac electrophysiology
- Electrical conduction system of the heart
- Electrocardiogram (EKG)
- Basic Principles of ECG Interpretation
- Electrophysiologic study
- Cardiology
- Cardiac arrhythmia
External links
References
- ↑ 1.0 1.1 David E. Mohrman, L. J. (2010). Cardiovascular Physiology, 7e. The McGraw-Hill Companies, Inc.
- ↑ Kim E. Barrett, S. B. (2012). Ganong’s Review of Medical Physiology, 24e . The McGraw-Hill Companies, Inc.
- ↑ 3.0 3.1 Olson, E. N. (2004). A decade of discoveries in cardiac biology. Nature Medicine, 467 – 474.
- ↑ 4.0 4.1 Valentin Fuster, R. A. (2011). Hurst’s The Heart, 13e. The McGraw-Hill Companies, Inc.
- ↑ Kim E. Barrett, S. B. (2012). Ganong’s Review of Medical Physiology, 24e . The McGraw-Hill Companies, Inc.
Vascular Medicine
Editor-in-Chief: Amjad AlMahameed, MD, MPH, RPVI, FACP. Beth Israel Decaoness Medical Center and Harvard Medical School. Boston, USA
Vascular medicine is a rapidly advancing discipline that is concerned with the study of the the blood vessels and their diseases. It encompasses the evaluation and treatment of the following disease states:
- Arterial disease, such as carotid, renal, mesenteric and other peripheral (limb) arterial abnormalities, including acute and chronic syndromes as well as long-term complications.
- Diseases of the veins, such as varicose veins, thrombophlebitis, venous thromboembolic disease (DVT and PE) and its long-term sequelae.
- Diseases of the lymphatics, such as lymphedema.
- Associated medical disorders, such as hypercholesterolemia, hypertension, diabetes.
- Nonatherosclerotic vascular disease, such as vasculitidis, thromboangiitis obliterans (Buerger’s disease), fibromuscular dysplasia, pernio, atheromatous embolization, HIV and other vasculopathies.
- The appropriate use of noninvasive and invasive assessment and management of these problems
Arterial Diseases
Occlusive Disease
Peripheral Arterial Disease of the Lower Extremities
Peripheral Arterial Disease of the Upper Extremities
Extracranial Carotid Artery Stenosis
Mesenteric Artery Stenosis
Iliac and Popliteal Aneurysms
Splenic, Renal, and mesenteric aneurysms
Acute Aortic Syndromes
Intramural Hematoma
Penetrating Ulcer of the Aorta
Occlusive Aortic Disease
Nonatherosclerotic Vascular Syndromes
Vasculitidis
Buerger’s Disease
Cold-Induced Vasculopathies
Pernio
Atheromatous embolization
Other Arteriopathies
Complications of Vascular Access
Pseudoaneurysms
Arterial-Venous Fistula
Retroperitoneal Hematomas
Venous Disease
Venous Thromboembolic Disease
Acute Deep Venous Thrombosis
Post-Phlebetic Syndrome
Lymphatic Disease
The Vascular Laborartory
Introduction to Vascular Ultrasounds Physics
Criteria for Mesenteric Stenosis
Ankle Brachial Index and Segmental Blood Pressure Measurement
Arterial Duplex of the Peripheral Arteries
Graft Surveillance
Venous Ultrasounds
Diseases of the Aorta
Editor-in-Chief: Amjad AlMahameed, MD, MPH, RPVI, FACP. Beth Israel Decaoness Medical Center and Harvard Medical School. Boston, USA
The term aneurysm is derived from the Greek word (aneurysmos) meaning dilatation. The most common site for true arterial aneurysms is the infra-renal aorta. A true aneurysm is a circumscribed dilatation of the three layers of vessel wall with a diameter increase of at least 50% compared to that of the proximal segment (i.e., the the dilated segment is 1.5 times that of the adjacent proximal segment). Ectasia, on the other hand, is a mild dilatation (luminal diameter increased by <50%) that is due to age-related degenerative changes in the vessel wall. Pheotypically, aneurysms are further classified as fusiform (symmetric involvement of the entire aortic circumference) or saccular (focal outpouching of part of the vessel wall). While most aneurysms are silent, a variety of symptoms and life-threatening complications can occur. Timely diagnosis and treatment of aortic aneurysms is critical.
Thoracic aortic aneurysms (TAAs) encompass all aneurysms the aorta between the aortic root and the crura of the diaphragm. The aortic root and the ascending vthoracic aorta are the most common sites of TAAs (60%), followed by the descending thoracic aorta (40%). Involvement of the aortic arch and/or extension of a TAA into the abdominal aorta (AA) (so called thoracoabdominal aneurysms) are relatively uncommon subsets (each encountered in 10% of cases or less).
TAAs are relatively uncommon with an estimated incidence between 6 and 10 new aneurysms per 100,000 person-years. TAAs are usually diagnosed after the sixth decade of life and they typically expand slowly (approximately 0.1-0.2 cm/year). The risk of rupture is closely related to aneurysm size (3% for TAAs <4 cm and 7% for >6 cm). These bioepidemiological characteristics support the current stand that screening for TAA is not recommended in the general population. Certain population substrates, such as those with history of Marfan syndrome, Turner syndrome, Ehlers-Danlos type IV syndrome, familial thoracic aortic disease syndromes, and patients with bicuspid aortic valve should have imaging study to screen for TAAs.
Since the abdominal aorta tends to be about 2 cm in diameter, a true AAA measures >3.0 cm. However, studies showed that the normal diameter varies depending on the patient’s age, sex, height, weight, race, body surface area, and baseline blood pressure. Hence, using a diameter ratio (> 1.5 the proximal segment) may be more accurate, particularly in smaller people such as women and those of short stature.
Peripheral Arterial Disease
For patient information on this page, click here
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor-In-Chief: Cafer Zorkun, M.D., Ph.D. [2] Kiran Singh, M.D. [3]
Synonyms and keywords: Peripheral vascular disease; peripheral artery occlusive disease; PVD; PAOD; PAD; acute limb ischemia; chronic limb ischemia; claudication
Diagnosis
History and Symptoms | Physical Examination | Laboratory Findings | Electrocardiogram | Chest X Ray | CT | MRI | Ultrasound | Other Imaging Findings | Other Diagnostic Studies
Treatment
Medical Therapy | Surgery | Primary Prevention | Guidelines for Management
Case Studies
Subclavian Artery Disease
Renovascular Disease
Aortoiliac Disease
Sytemic Arterial Hypertension
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Sara Zand, M.D.[2] Usama Talib, BSc, MD [3] Hafiz M. Ahmed, M.D.[4]
Synonyms and keywords: Blood pressure; hypertension; high blood pressure; systolic blood pressure; essential hypertension
Overview
Hypertension is a major risk factor for cardiovascular disease and a major public health problem. The prevalence of hypertension increased among the united states due to changing The previous cut-off 140/90 mmHg (the previous 2003 threshold from the Joint National Committee (JNC) 7 guideline 3) to a lower threshold of greater than or equal to 130/80 mmHg. Hypertension is a leading cause of mortality worldwide. More than half of hypertensive patients are not aware of the disorder and some diagnosed patients do not take the medication. The new guideline recommends considering the average of reading BP≥ 2 visits office. Home blood pressure monitoring (HBPM) and ambulatory blood pressure monitoring (ABPM) are better than clinic or home blood pressure readings to determine masked hypertension or white coat hypertension out of the office[1].
Historical Perspective
- Hypertension was first discovered by Scipione Riva-Rocci, an Italian physician, in 1896 following the invention of the cuff-based mercury sphygmomanometer and measurement of the peak systolic blood pressure by noting the cuff pressure at which the radial pulse was no longer palpable.
- In 1905, the sound after cuff deflation of sphygmomanometer was first identified by Russian physician Nikolai.
- Between 1910 and 1914, essential hypertension and malignant hypertension were described.
Classification
Hypertension classified based on presence of underlying disorders into two groups:[2][3]
- Chronic hypertension, also called primary hypertension or essential hypertension, (90-95%)
- Gradually rising in blood pressure
- History of environmental exposure (weight gain, high-sodium diet, decreased physical activity, job change leading increased travel, excessive consumption of alcohol
- Family history of hypertension
- Secondary hypertension, (5%), due to underlying disorder
- BP lability, suddenly rising BP with pallor and dizziness (pheochromocytoma)
- Snoring, hypersomnolence (obstructive sleep apnea)
- Prostatism (chronic kidney disease due to post-renal urinary tract obstruction)
- Muscle cramps, weakness (hypokalemia from primary aldosteronism or secondary aldosteronism due to renovascular disease)
- Weight loss, palpitations, heat intolerance (hyperthyroidism)
- Edema, fatigue, frequent urination (kidney disease or kidney failure)
- History of coarctation repair (residual hypertension associated with coarctation)
- Central obesity, facial rounding, easy bruisability (Cushing syndrome)
- Medication or substance use (alcohol, NSAIDS, cocaine, amphetamines)
- Absence of family history of hypertension
- Resistant hypertension is defined as a higher level of BP above the goal in spite of concurrent use of three antihypertensive drugs including a long-acting calcium channel blocker, angiotensin-converting enzyme inhibitor or angiotensin receptor blocker, and a diuretic and requires ≥ medications.[4]
- Refractory hypertension is explained as failing to control hypertension with at least five classes of antihypertensive drugs including long-acting thiazide-type diuretic, such as chlorthalidone, and a mineralocorticoid receptor antagonist, such as spironolactone.
Comparison between two guidelines of hypertension
| Hypertension Guidline | 2017 ACC/AHA | 2018 ESC/ESH |
|---|---|---|
| Definition of hypertension (mmHg) | ≥130/80 | ≥140/90 |
| Normal blood pressure range (mmHg) |
|
|
| Hypertension stage (mmHg) |
|
|
| Age specific blood pressure targets(9mmHg) |
|
|
2017/ACC/AHA Guideline of hypertension
- Hypertension can be classified based on the guideline into 2 stages:
| Blood pressure category | Systolic blood pressure | Diastolic blood pressure |
|---|---|---|
| Normal | <120/80 mmHg | <80 mmHg |
| Elevated | 120-129 mmHg | <80 mmHg |
| Stage 1 hypertension | 130–139 mm Hg | 80–89 mm Hg |
| Stage 2 hypertension | ≥140 mm Hg | ≥90 mm Hg |
Pathophysiology
- The pathogenesis of hypertension is characterized by a malfunction in the renin-angiotensin-aldosterone system (RAAS), natriuretic peptides ,endothelium, sympathetic nervous system (SNS),immune system.
- Allelic variants of several genes have been associated with the development of primary hypertension.
- Endothelial dysfunction and increased TGF-B was shown in salt sensitivity patients lead to increased systolic blood pressure 10 mmHg following ingestion of 5 gr salt.[5]
Causes
Common causes of hypertension include:[2]
- Genetic susceptibility
- Hypertension is a Polygenic disorder
- Findings of 25 rare mutations,120 single-nucleotide polymorphisms in hypertensive patients
- Monogenic forms of hypertension in conditions such as: Glucocorticoid-remediable aldosteronism, Liddle syndrome, Gordon’s syndrome
- Association between high blood pressure and older age with increased defects in the gene
Environmental exposure
- Direct relationship between body mass index and BP
- Strong relationship between waist-to hip ratio, distribution of central fat and BP
- Relation between obesity at a young age with further hypertension
- Sodium intake
- Inverse relation between physical fitness and physical activity with BP
- Modest exercise activity reduces the risk of BP
| Pharmacological causes of hypertension |
Management: |
| |
| |
|
|
| |
| |
| |
|
|
| |
| |
| |
|
|
|
Differentiating hypertension from other Diseases
- Differential diagnosis of hypertension includes:[6]
| Differentiating hypertension | Explanation |
|---|---|
| Isolated systolic hypertension | |
| Isolated diastolic hypertension |
|
| Masked hypertension | |
| White coat hypertension |
|
| Severe hypertension |
|
| Malignant hypertension (emergency hypertension) |
|
Epidemiology and Demographics
- The prevalence of hypertension is approximately 45,600 per 100,000 individuals worldwide.
- Between the years 2000-2002, the incidence of hypertension was estimated to be 5680 for whites, 8490 for African-Americans, 6570 for Hispanics, and 5220 for Chinese cases per 100,000 individuals in United States.[10]
Age
- Hypertension is more commonly observed among elderly patients
Gender
Race
- Hypertension usually affects individuals of the black race, Asians and Hispanic Americans.
Risk Factors
- Common risk factors in the development of hypertension are:
- Diabetes mellitus
- Family history of hypertension
- Dyslipidemia
- Increased age
- Obesity
- Low socioeconomic state
- Physical inactivity/low fitness
- Male sex
- Unhealthy diet
- Obstructive sleep apnea
- Psychological stress
- Common risk factors associated with resistant hypertension include:
- Older age
- Obesity
- CKD
- Black race
- DM
| Modifiable risk factors | Fixed risk factors |
|---|---|
| |
Natural History, Complications and Prognosis
- The patients with primary hypertension usually remain asymptomatic. [2]
- The clinical features of secondary hypertension dependent on the characteristics of an underlying disorder.[11]
- If hypertension left untreated, 33% of patients with hypertension may progress to developheart attack and stroke.[12]
- Common complications of resistant hypertension include MI, stroke, ESRD, and death that are 2-7 times higher compared with patients without resistant hypertension.
- Prognosis is generally poor without treatment, and the 10 year mortality rate of patients with hypertension is approximately 11%.
Diagnosis
Diagnostic Criteria
- The diagnosis of hypertension is made when at least three of the following diagnostic criteria are met:[2]
- Accurate measurement of BP
- Assessment of cardiovascular risk
- Assessment about secondary hypertension
Abbreviations:
SBP: Systolic blood pressure;
DBP: Diastolic blood pressure;
BP: Blood pressure
| Blood pressure measurement | Definition |
|---|---|
| Systolic blood pressure (SBP) | First Korotkoff sound |
| Diastolic blood pressure(DBP) | Fifth Korotkoff sound |
| Pulse pressure | SBP minus DBP |
| Mean arterial pressure | DBP plus one third pulse pressure |
| Mid- blood pressure | (SBP+DBP) divided by 2 |
| Arm circumference | cuff size |
|---|---|
| 22-26 cm | Small adult |
| 27-34 cm | Adult |
| 35-44 cm | Large adult |
| 45-52 cm | Adult thigh |
| Key steps for accurate blood pressure measurement | Educations |
|---|---|
| Properly prepare the patient | |
| Using proper technique |
|
| Taking proper measurement |
|
| Documentation of reading blood pressure |
|
| Average the reading |
|
| Providing blood pressure reading to patient |
| New onset or uncontrolled hypertension in adult | |||||||||||||||||||||||||||||||||||||||||||||||||
* Drug resistance hypertension
| |||||||||||||||||||||||||||||||||||||||||||||||||
| Yes | No | ||||||||||||||||||||||||||||||||||||||||||||||||
| Screening for secondary hypertension | No need for screening | ||||||||||||||||||||||||||||||||||||||||||||||||
Abbreviations:
ABPM: Ambulatory blood pressure monitoring;
HBPM: Home blood pressure monitoring;
BP: Blood pressure
| Office BP≥130/80 mm Hg, but < 160/100 mmHg after 3 months of life style modification, suspected white coat hypertension | |||||||||||||||||||
| Daytime ABPM or HBPM, BP<130/80 mmHg | |||||||||||||||||||
YES
| NO
| ||||||||||||||||||
Abbreviations:
ABPM: Ambulatory blood pressure monitoring;
HBPM: Home blood pressure monitoring;
BP: Blood pressure
| Office BP: 120-129/<80 mmHg after 3 months of lifestyle modification, suspected masked hypertension | |||||||||||||||||||
| Daytime ABPM or HBPM, BP≥130/80 mm Hg | |||||||||||||||||||
Yes
| NO
| ||||||||||||||||||
Abbreviations:
ABPM: Ambulatory blood pressure monitoring;
HBPM: Home blood pressure monitoring;
BP: Blood pressure
| Recommendations for masked hypertension and white coat hypertension : (Class IIa, Level of Evidence B) |
|
❑ Screening for white-coat hypertension in patients with systolic blood pressure 130-160 mmHg and diastolic blood pressure 80-110 mmHg by using ABPM or HBPM before the diagnosis of hypertension |
| (Class IIa, Level of Evidence C) |
|
❑ Periodic monitoring of blood pressure with ABPM or HBPM for detection of transient or sustained hypertension inwhite coat hypertension |
| (Class IIa, Level of Evidence C) |
|
❑ Finding of white coat hypertension by HBPM and ABPM in high office blood pressure in spite of receiving treatment, is recommended |
| (Class IIa, Level of Evidence B) |
|
❑ Finding of mask hypertension by HBPM or ABPM in-office blood pressure 120-129 /75-79 mmHg |
| (Class IIb, Level of Evidence C) |
|
❑ Finding of white coat hypertension by HBPM or ABPM if office blood pressure is 10 mmHg higher than normal in spite of receiving multiple medications |
| 2017 ACC/AHA Guideline |
Screening for Primary adlostronism: |
|
|
History and Symptoms
- Primary hypertensive patients are usually asymptomatic.
- Symptoms related to underlying causes of secondary hypertension may include the following:
- Palpitation
- Headache
- Sweeting
- Abdominal pain
- Urinary symptoms
- Muscle cramps
- Abdominal mass
- Skin lesions
- Edema
Physical Examination
- Patients with primary hypertension usually are asymptomatic.
- In secondary hypertension physical examination may be remarkable for :
- Arterial bruit
- Irregular pulses, Tachycardia, Absent femoral pulses
- Fine tremor
- Acute abdominal pain, abdominal mass
- Skin stigmata, Violaceous striae
- Hirsutism
- Warm skin, moist skin, Skin pallor
- Central obesity
- Moon face
- Dorsal and supraclavicular fat pads
- Loss of normal nocturnal blood pressure fall
- Orthostatic hypotension
- Periorbital puffiness,Coarse skin, Cold skin, Slow movement,Goiter
- continuous murmur over back or chest
- Abdominal bruit
| Conditions | Physical examination |
|---|---|
| Renal parenchymal disease | |
| Renovascular disease |
|
| Primary aldosteronism | |
| Obstructive sleep apnea |
|
| Drug or alcohol induced | |
| Pheochromocytoma/paraganglioma | |
| Cushing syndrome | |
| Hypothyroidism | |
| Hyperthyroidism | |
| Coarctation of aorta |
|
| Congenital adrenal hyperplasia |
|
| Acromegaly |
Laboratory Findings
- Basic laboratory test should be taken in patients with the diagnosis of hypertension include:
- Fasting blood sugar
- Complete blood count
- Lipid profile
- Serum creatinine with eGFR
- Serum sodium, potassium, calcium
- Thyroid-stimulating hormone
- Urinalysis
- Optional laboratory test in hypertensive patients include:
- Uric acid
- Urinary albumin to creatinine ratio
Electrocardiogram
- An ECG may be helpful in the diagnosis of left ventricular hypertrophy associated hypertension. Findings on an ECG suggestive of left ventricular hypertrophy include
- Cornell criteria: R wave in aVL + S wave in V3> 28 millimeters in males or greater than 20 mm in females
- Modified Cornell Criteria: R wave in aVL> 12 mm
- Sokolow-Lyon Criteria: S wave in V1 + R wave in V5 or V6> 35mm
- Romhilt-Estes: If the score equals 4, LVH is present with 30% to 54% sensitivity. If the score is greater than 5, LVH is present with 83% to 97% specificity.
- The amplitude of the largest R or S in limb leads ≥ 20 mm = 3 points
- The amplitude of S in V1 or V2 ≥ 30 mm = 3 points
- The amplitude of R in V5 or V6 ≥ 30 mm = 3 points
- ST and T wave changes opposite QRS without digoxin = 3 points
- ST and T wave changes opposite QRS with digoxin = 1 point
- Left Atrial Enlargement = 3 points
- Left Axis Deviation = 2 points
- QRS duration ≥ 90 ms = 1 point
- Intrinsicoid deflection in V5 or V6 > 50 ms = 1 point
Chest X-ray
- Finding on a chest x-ray associated target organ damage in hypertension include widening aortic knob.[13]
- Ascending aorta dilation and increased cardiothoracic ratio may be associated with hypertension.
Echocardiography or Ultrasound
Echocardiography may be helpful in the diagnosis of complications of hypertension, which include left ventricular hypertrophy (LVH), left ventricular (LV) diastolic dysfunction and left atrial dilation.
CT scan
- CT scan may be helpful in the diagnosis of underlying causes of secondary hypertension such as hyperaldosteronism, pheochromocytoma, hyperparathyroidism, aortic coarctation.[11]
- CT scan may also show the complication of hypertension including:
MRI
- Cardiac MRI is a reliable tool in the diagnosis of hypertensive heart disease by evaluation of left ventricular hypertrophy, left ventricular mass, biventricular function, valvular disease, inflammation and stress myocardial perfusion-fibrosis.[14]
Other Imaging Findings
- There are no other imaging findings associated with hypertension.
Other Diagnostic Studies
- There are no other diagnostic studies associated with hypertension.
Treatment
Treatment Goal
For all adults with confirmed hypertension, the recommended target is <130/80 mm Hg. For high-risk patients (10-year CVD risk ≥7.5% by PREVENT), achieving SBP <120 mm Hg is encouraged to reduce major adverse events. [15]
Medical Therapy
- The mainstay of treatment for hypertension is: Initiation of treatment with one or more of three classes of first-line BP lowering agents:[15]
- Calcium channel blocker (CCB)
- Renin-angiotensin-converting enzyme inhibitors (ACEI or ARB)
- Thiazide-like diuretic
- Beta-blockers are not first-line for hypertension unless specific comorbidities (e.g., coronary heart disease, heart failure with reduced ejection fraction) are present.
- Second-line lowering BP agents are used in resistant hypertension or specific conditions
- For Stage 2 hypertension (BP ≥140/90 mm Hg), initiation of antihypertensive therapy with two first-line agents of different classes, ideally in a single-pill combination, is recommended to improve blood pressure control and medication adherence.
- The mainstay of therapy for resistant hypertension is:
- Improving medications adherence
- Diagnosis and treatment of the causes of secondary hypertension
- Adding spironolactone or hydralazine or minoxidil to first line therapy (CCBs, inhibitors of RAS, chlorthalidone)
- Renal Denervation may be reasonable as an adjunct in select patients
| Treatment strategy | |||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Nomal BP (BP<120/80 mmHg) | Elevated BP (BP120-129/<80mmHg) | Stage1 hypertension (BP 130-139/80-89mmHg) | Stage 2 hypertension (BP≥ 140/90 | ||||||||||||||||||||||||||||||||||||||||||||||||||||
| Lifestyle modifications | Non-pharmocological therapy (class1) | 10-year cardiovascular disease (CVD) risk ≥7.5% by PREVENT | Non-pharmacological therapy and BP lowering medication | ||||||||||||||||||||||||||||||||||||||||||||||||||||
| Reevaulation in 1 year (class 2a) | Reevaulation in 3-6 months (class 1) | No, non-pharmocological therapy (class1) | Yes, non-pharmacological therapy and BP lowering medication | ||||||||||||||||||||||||||||||||||||||||||||||||||||
| Reevaulation in 3-6 months (class 1) | Reevaulation in 1 months (class 1) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||
| BP goal reached | |||||||||||||||||||||||||||||||||||||||||||||||||||||||
| No, evaluation and optimization the adherence to medical therapy | Yes, Reevaulation in 3-6 months(class 1) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Intensification of medical therapy | |||||||||||||||||||||||||||||||||||||||||||||||||||||||
| First line of treatment | Drug / Dosage (mg/day) / Frequency | Comments |
|---|---|---|
| Thiazide or thiazidetype diuretics |
|
|
| ACE inhibitors |
|
|
| ARB |
|
|
| CCB—dihydropyridines |
|
|
| CCB—nondihydropyridines |
|
|
| Second line of treatment | Drug_ Dosage(mg/day)_ Frequency | Comments |
| Diuretics—loop |
|
|
| Diuretics—potassium sparing |
|
|
| Diuretics—aldosterone antagonists |
|
|
| Betablocker–cardioselective |
|
|
| Betablocker-cardioselective and vasodilatory |
|
|
| Beta blockers—noncardioselective |
|
|
| Beta blockers—intrinsic sympathomimetic activity |
|
|
| Beta blockers—combined alpha-beta receptor |
|
|
| Direct renin inhibitor |
|
|
| Alpha-1 blockers |
|
|
| Central alpha2-agonist and other centrally acting drugs |
|
|
| Direct vasodilators |
|
|
| Class I, Level of evidence:A |
| In patients with atherosclerotic renal artery stenosis, medical therapy is recommended |
| Class IIb, Level of evidence:C |
| Revascularization (percutaneous renal artery angioplasty and/ or stent placement) indicates in patients with refractory hypertension, worsening
renal function, intractable heart failure, nonatherosclerotic disease (fibromuscular dysplasia) |
| Class IIb, Level of evidence:B |
| The effectiveness of continuous positive airway pressure (CPAP) to decrease blood pressure in patients with obstructive sleep apnea and hypertension is not verified |
Surgery
- Surgical procedure may be performed for patients with secondary hypertension such as coarctation of aorta, primary aldosteronism.
- Renal Denervation may be reasonable as an adjunct in select patients with resistant hypertension or drug intolerance, but requires evaluation by a multidisciplinary team.
Prevention
- Effective measures for the primary prevention of hypertension include:[15]
- Weight loss: Sustained ≥5% reduction in body weight or ≥3 kg/m² reduction in BMI. Expect ~1 mmHg SBP drop per 1 kg lost
- Healthy diet: A diet rich in fruits, vegetables, whole grains, low-fat dairy products, reduced content of saturated and total fat
- Reduced intake of dietary sodium: Target <2300 mg/day, with ideal limit <1500 mg/day
- Enhanced intake of dietary potassium: 3500–5000 mg/d by ideally intaking rich diet with potassium, or moderate supplementation (<80 mmol/day)
- Use of salt substitutes: Replace regular table/cooking salt with potassium-based salt substitutes. Avoid in CKD or with potassium-sparing drugs
- Reduced alcohol intake: Abstinence is optimal for BP control. If consumed, reduce intake by >50% to ≤1 drink/day for women or ≤2 drinks/day for men
- Physical activity: Aerobic ( 90–150 min/week), dynamic resistance (90–150 min/week), Isometric resistance (4 × 2 min handgrip, 1 min rest between exercises, 3 sessions per week)
- Stress reduction: Transcendental meditation (2 × 20 min/day) or device-guided slow breathing (<10 breaths/min for 15 min/day) may be reasonable adjuncts to lifestyle modification
- Once diagnosed and treated, patients with hypertension are followed-up every month for evaluation of medication adherence and response to treatment.
References
- ↑ Karnjanapiboonwong A, Anothaisintawee T, Chaikledkaew U, Dejthevaporn C, Attia J, Thakkinstian A (2020). “Diagnostic performance of clinic and home blood pressure measurements compared with ambulatory blood pressure: a systematic review and meta-analysis”. BMC Cardiovasc Disord. 20 (1): 491. doi:10.1186/s12872-020-01736-2. PMC 7681982 Check
|pmc=value (help). PMID 33225900 Check|pmid=value (help). - ↑ 2.0 2.1 2.2 2.3 Whelton, Paul K.; Carey, Robert M.; Aronow, Wilbert S.; Casey, Donald E.; Collins, Karen J.; Dennison Himmelfarb, Cheryl; DePalma, Sondra M.; Gidding, Samuel; Jamerson, Kenneth A.; Jones, Daniel W.; MacLaughlin, Eric J.; Muntner, Paul; Ovbiagele, Bruce; Smith, Sidney C.; Spencer, Crystal C.; Stafford, Randall S.; Taler, Sandra J.; Thomas, Randal J.; Williams, Kim A.; Williamson, Jeff D.; Wright, Jackson T. (2018). “2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines”. Hypertension. 71 (6). doi:10.1161/HYP.0000000000000065. ISSN 0194-911X.
- ↑ Aronow, Wilbert S. (2017). “Drug-induced causes of secondary hypertension”. Annals of Translational Medicine. 5 (17): 349–349. doi:10.21037/atm.2017.06.16. ISSN 2305-5839.
- ↑ Carey, Robert M.; Calhoun, David A.; Bakris, George L.; Brook, Robert D.; Daugherty, Stacie L.; Dennison-Himmelfarb, Cheryl R.; Egan, Brent M.; Flack, John M.; Gidding, Samuel S.; Judd, Eric; Lackland, Daniel T.; Laffer, Cheryl L.; Newton-Cheh, Christopher; Smith, Steven M.; Taler, Sandra J.; Textor, Stephen C.; Turan, Tanya N.; White, William B. (2018). “Resistant Hypertension: Detection, Evaluation, and Management: A Scientific Statement From the American Heart Association”. Hypertension. 72 (5). doi:10.1161/HYP.0000000000000084. ISSN 0194-911X.
- ↑ Oparil S, Acelajado MC, Bakris GL, Berlowitz DR, Cífková R, Dominiczak AF, Grassi G, Jordan J, Poulter NR, Rodgers A, Whelton PK (March 2018). “Hypertension”. Nat Rev Dis Primers. 4: 18014. doi:10.1038/nrdp.2018.14. PMC 6477925. PMID 29565029.
- ↑ McEvoy, John W.; Daya, Natalie; Rahman, Faisal; Hoogeveen, Ron C.; Blumenthal, Roger S.; Shah, Amil M.; Ballantyne, Christie M.; Coresh, Josef; Selvin, Elizabeth (2020). “Association of Isolated Diastolic Hypertension as Defined by the 2017 ACC/AHA Blood Pressure Guideline With Incident Cardiovascular Outcomes”. JAMA. 323 (4): 329. doi:10.1001/jama.2019.21402. ISSN 0098-7484.
- ↑ Franklin, Stanley S.; O’Brien, Eoin; Staessen, Jan A. (2016). “Masked hypertension: understanding its complexity”. European Heart Journal: ehw502. doi:10.1093/eurheartj/ehw502. ISSN 0195-668X.
- ↑ Franklin, Stanley S.; Thijs, Lutgarde; Hansen, Tine W.; O’Brien, Eoin; Staessen, Jan A. (2013). “White-Coat Hypertension”. Hypertension. 62 (6): 982–987. doi:10.1161/HYPERTENSIONAHA.113.01275. ISSN 0194-911X.
- ↑ Rubin, Sébastien; Cremer, Antoine; Boulestreau, Romain; Rigothier, Claire; Kuntz, Sophie; Gosse, Philippe (2019). “Malignant hypertension”. Journal of Hypertension. 37 (2): 316–324. doi:10.1097/HJH.0000000000001913. ISSN 0263-6352.
- ↑ Carson AP, Howard G, Burke GL, Shea S, Levitan EB, Muntner P (June 2011). “Ethnic differences in hypertension incidence among middle-aged and older adults: the multi-ethnic study of atherosclerosis”. Hypertension. 57 (6): 1101–7. doi:10.1161/HYPERTENSIONAHA.110.168005. PMID 21502561.
- ↑ 11.0 11.1 Siddiqui, Mohammed Azfar; Mittal, Pardeep K.; Little, Brent P.; Miller, Frank H.; Akduman, Ece Isin; Ali, Kamran; Sartaj, Sara; Moreno, Courtney C. (2019). “Secondary Hypertension and Complications: Diagnosis and Role of Imaging”. RadioGraphics. 39 (4): 1036–1055. doi:10.1148/rg.2019180184. ISSN 0271-5333.
- ↑ Fihaya, Faris Yuflih; Sofiatin, Yulia; Ong, Paulus Anam; Sukandar, Hadyana; Roesli, Rully M.A. (2015). “Prevalence of Hypertension and Its Complications in Jatinangor 2014”. Journal of Hypertension. 33: e35. doi:10.1097/01.hjh.0000469851.39188.36. ISSN 0263-6352.
- ↑ Rayner, B (2004). “The chest radiographA useful investigation in the evaluation of hypertensive patients”. American Journal of Hypertension. 17 (6): 507–510. doi:10.1016/j.amjhyper.2004.02.012. ISSN 0895-7061.
- ↑ Mavrogeni, Sophie; Katsi, Vasiliki; Vartela, Vasiliki; Noutsias, Michel; Markousis-Mavrogenis, George; Kolovou, Genovefa; Manolis, Athanasios (2017). “The emerging role of Cardiovascular Magnetic Resonance in the evaluation of hypertensive heart disease”. BMC Cardiovascular Disorders. 17 (1). doi:10.1186/s12872-017-0556-8. ISSN 1471-2261.
- ↑ 15.0 15.1 15.2 Writing Committee Members*, Jones, D. W., Ferdinand, K. C., Taler, S. J., Johnson, H. M., Shimbo, D., Abdalla, M., Altieri, M. M., Bansal, N., Bello, N. A., Bress, A. P., Carter, J., Cohen, J. B., Collins, K. J., Commodore-Mensah, Y., Davis, L. L., Egan, B., Khan, S. S., Lloyd-Jones, D. M., … Williamson, J. D. (2025). 2025 AHA/ACC/AANP/AAPA/ABC/ACCP/ACPM/AGS/AMA/ASPC/NMA/PCNA/SGIM guideline for the Prevention, Detection, Evaluation and Management of High Blood Pressure in Adults: A report of the American college of cardiology/American heart association joint committee on clinical practice guidelines. Circulation, 152(11), e114–e218. https://doi.org/10.1161/CIR.0000000000001356
Hypotension
For patient information click here
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Cafer Zorkun, M.D., Ph.D. [2]
Synonyms and keywords: low blood pressure; blood pressure low, systemic.
Diagnosis
History and Symptoms | Physical Examination | Laboratory Findings | Electrocardiogram | Chest X Ray | CT | MRI | Echocardiography or Ultrasound | Other Imaging Findings | Other Diagnostic Studies
Treatment
Medical Therapy | Surgery | Primary Prevention | Secondary Prevention | Cost-Effectiveness of Therapy | Future or Investigational Therapies
Case Studies
Primary Cardiac Tumors
For patient information click here
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-In-Chief: Cafer Zorkun, M.D., Ph.D. [2]; Varun Kumar, M.B.B.S. Syed Hassan A. Kazmi BSc, MD [3]
Primary cardiac tumors | Secondary cardiac tumors
Diagnosis
Staging | History and Symptoms | Physical Examination | Laboratory Findings | Electrocardiogram | Chest X Ray | CT | MRI | Echocardiography | Other Imaging Findings | Other Diagnostic Studies
Treatment
Medical Therapy | Surgery | Primary Prevention | Secondary Prevention | Cost-Effectiveness of Therapy | Future or Investigational Therapies
Case Studies
Case #1 | Case #2: Cardiac lymphoma
Related Chapters
The Heart in Oncologic Disease
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]
Associate Editor-In-Chief: Cafer Zorkun, M.D., Ph.D. [2]
Imaging
CT
Labeled images below are courtesy of RadsWiki and copylefted.
- Atrial Myxoma
-
 Atrial Myxoma
Atrial Myxoma -
 Atrial Myxoma
Atrial Myxoma -
 Atrial Myxoma
Atrial Myxoma



- Cardiac Rhabdomyosarcoma
-
 Cardiac Rhabdomyosarcoma
Cardiac Rhabdomyosarcoma -
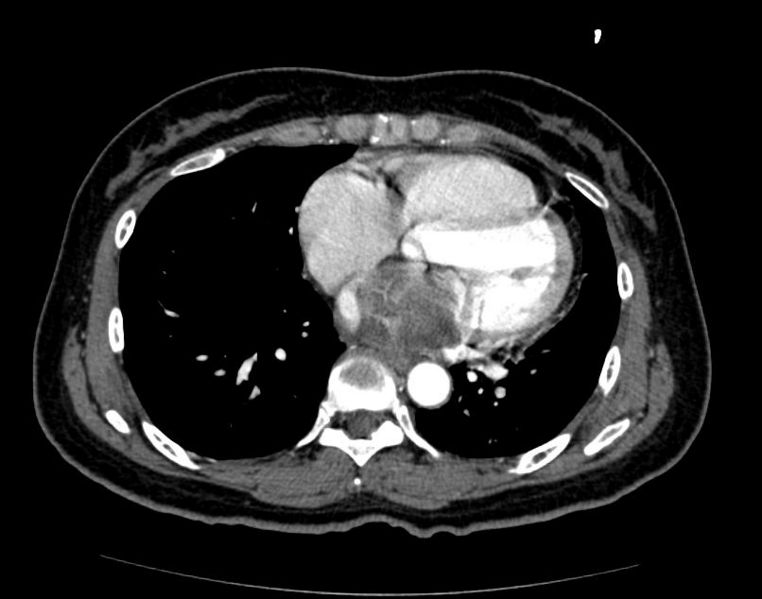 Cardiac Rhabdomyosarcoma
Cardiac Rhabdomyosarcoma -
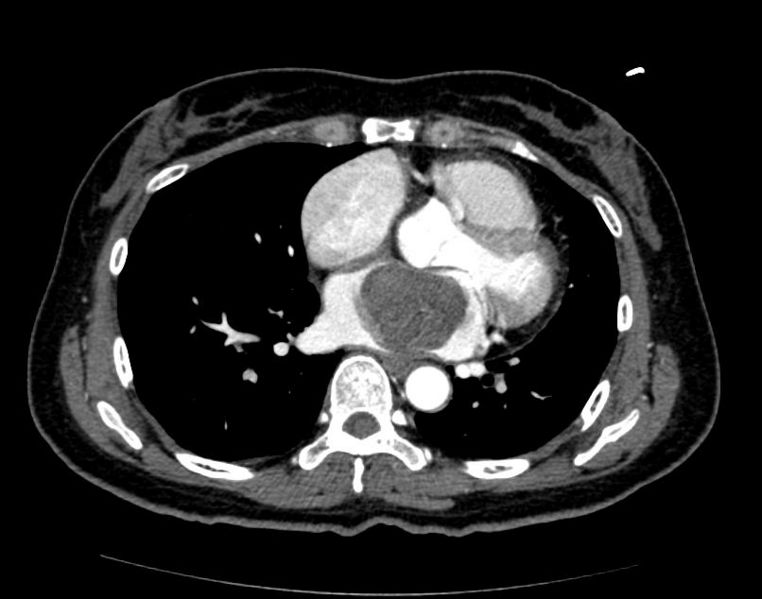 Cardiac Rhabdomyosarcoma
Cardiac Rhabdomyosarcoma



Pathological Findings
Image shown below is courtesy of Professor Peter Anderson DVM PhD and published with permission. © PEIR, University of Alabama at Birmingham, Department of Pathology
-
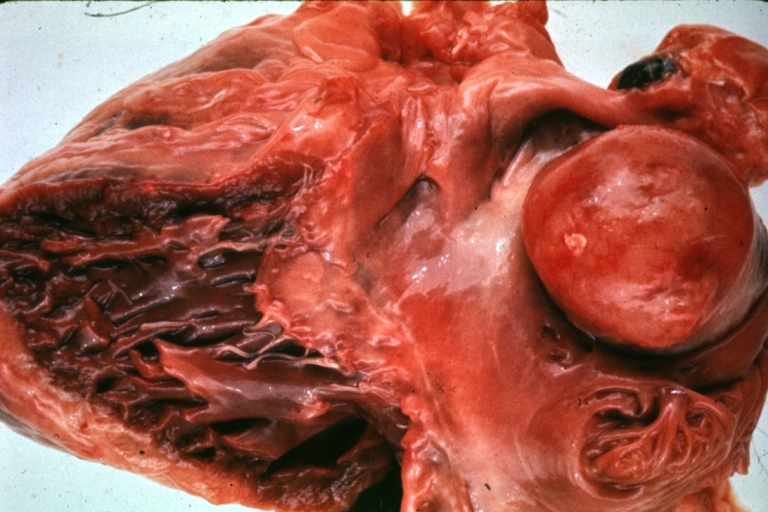 HEART: Metastatic Tumor: Gross very unusual large metastatic carcinoid in right atrium
HEART: Metastatic Tumor: Gross very unusual large metastatic carcinoid in right atrium -
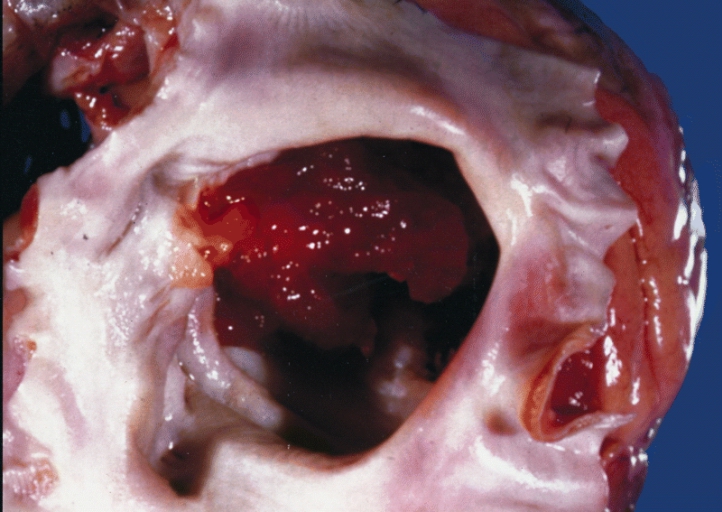 Cardiac Myxoma A gelatinous tumor is attached by a narrow pedicle to the atrial septum. The myxoma has an irregular surface and nearly fills the left atrium.
Cardiac Myxoma A gelatinous tumor is attached by a narrow pedicle to the atrial septum. The myxoma has an irregular surface and nearly fills the left atrium.


-
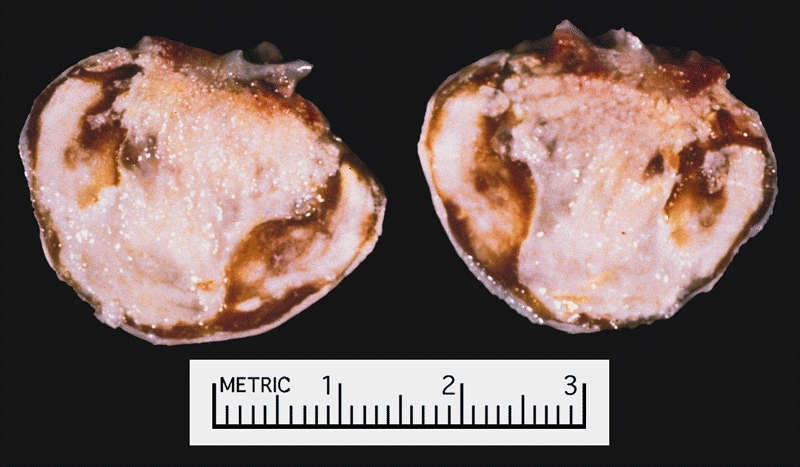 Cardiac Myxoma There was a calcified right atrial mass on the X ray of a 47-year-old man. Resection demonstrated a smooth-surfaced tumor. The gritty material seen microscopically on cut section was calcified and ossified myxoma.
Cardiac Myxoma There was a calcified right atrial mass on the X ray of a 47-year-old man. Resection demonstrated a smooth-surfaced tumor. The gritty material seen microscopically on cut section was calcified and ossified myxoma. -
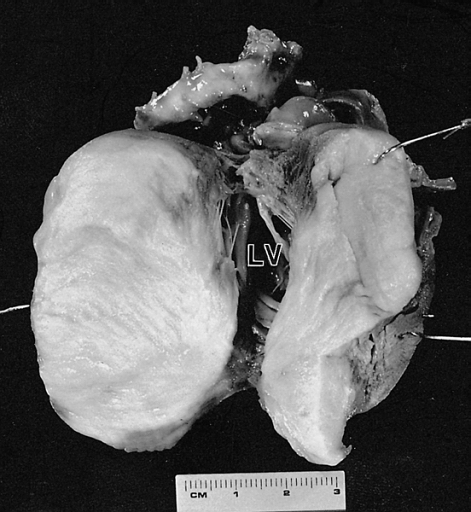 Cardiac Fibroma Cut surface of the tumor shown in figure 6-2. The left ventricular (LV) cavity is present behind the mass. The patient was a 4-month-old child who died suddenly without a previous medical history.
Cardiac Fibroma Cut surface of the tumor shown in figure 6-2. The left ventricular (LV) cavity is present behind the mass. The patient was a 4-month-old child who died suddenly without a previous medical history.


-
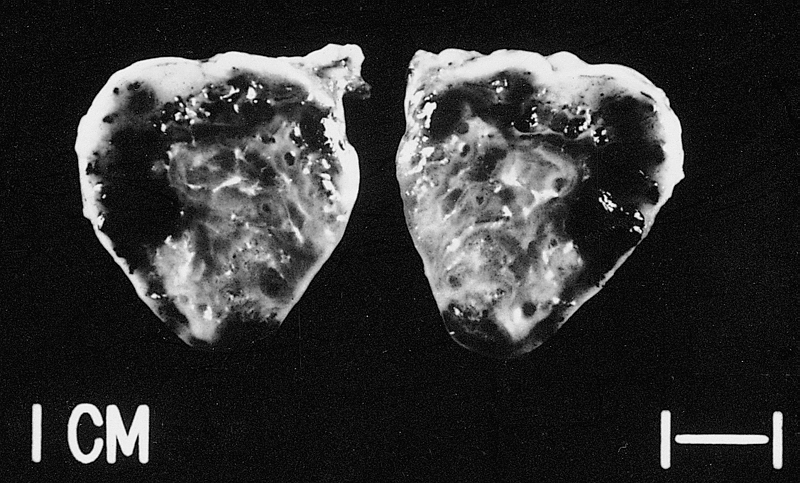 This tumor was resected from the right atrium of a 1-year-old boy with pericardial effusions. Note areas of hemorrhage and dilated vessels. The patient was well 49 months postoperatively.
This tumor was resected from the right atrium of a 1-year-old boy with pericardial effusions. Note areas of hemorrhage and dilated vessels. The patient was well 49 months postoperatively. -
 Papillary fibroelastomas are often on the arterial surface and may project into the coronary ostium, causing ostial occlusion. This tumor is in the noncoronary sinus.
Papillary fibroelastomas are often on the arterial surface and may project into the coronary ostium, causing ostial occlusion. This tumor is in the noncoronary sinus.


References
External Links
See Also
Endocrine Disease and the Heart
Hyperthyroidism | Hypothyroidism | Hypoparathyroidism | Acromegaly
Renal Disease and the Heart
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]
Associate Editor-In-Chief: Cafer Zorkun, M.D., Ph.D. [2]
Overview
An estimated 10 to 20 million people have chronic kidney disease (CKD). While many will never develop kidney failure, others will, joining more than 400,000 people annually treated with dialysis or a kidney transplant. Cardiovascular disorders accounts for half of all deaths among people with kidney failure.
- Cardiovascular disease accounts for more than half of all deaths among people with renal failure.
- Even early or mild kidney disease places a person at higher risk of acute coronary syndromes and heart failure, as well as cardiovascular disease related death.
- Hypertension (high blood pressure) and diabetes are major risk factors for chronic kidney disease and heart disease. The development of chronic kidney disease in persons with diabetes or hypertension further increases the risk of developing cardiovascular disease.
- Hypertension increases the risk of cardiovascular disease, and severe hypertension can cause extensive and rapidly progressive kidney damage. Newer medications that better control blood pressure, however, can slow the rate of kidney damage only by about 50 percent.
- In comparison, death from cardiovascular disease is 10 to 30 times more likely in dialysis patients.
- Kidney disease by itself increases the risk of cardiovascular disease, even with concurrent diabetes, hypertension and high cholesterol.
- Numerous studies reported that kidney disease accelerates heart disease, even before the kidneys are damaged to the point of needing dialysis or transplantation.
Clinical Trials
A pair of epidemiology studies confirmed that chronic kidney disease independently increases the risk of developing cardiovascular disease, even among people with early kidney disease and after considering other risk factors such as diabetes, hypertension and high cholesterol.
The National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK) funded study followed more than 1.1 million adults from the Kaiser Permanente Renal Registry in San Francisco for nearly 3 years; average age was 52 years. The investigators found that when kidney function (GFR) dropped, the risk of death, cardiovascular events such as heart disease and stroke, and hospitalization increased. Compared to patients whose GFR was at least 60 (ml per min. per 1.73 m2):
- The increased risk of death ranged from 17 percent in those whose GFR was between 45 and 59 to about 600 percent in those whose GFR was less than 15
- The increased risk of CVD events ranged from 43 percent in those whose GFR was between 45 and 59 to 343 percent in those whose GFR was less than 15,
- The increased risk of hospitalization ranged from 14 percent in those whose GFR was between 45 and 59 to 315 percent in those whose GFR was less than 15.
The industry-funded VALIANT study related CKD to deaths from CVD in a 2-year drug-treatment trial of more than 14,500 heart-attack patients. The researchers found death rates ranging from 14.1 percent in patients whose GFR was at least 75 to 45.5 percent in those whose GFR was less than 45.
The investigators attribute the increased risk of death from CVD in part to complications of kidney disease, including anemia, oxidative stress, changes in calcium and phosphate regulation, inflammation, and conditions promoting clotting. The researchers also suggest that other kidney-related factors such as protein in the urine and elevated blood levels of both homocysteine and uric acid may increase the risk of CVD and death. Furthermore, they found that common CVD therapies such as aspirin and beta-blockers were “curiously underused” in CKD patients with lower kidney function, perhaps inspired by a fatalist mind-set that may be a self-fulfilling prophecy.
Renal Cell Carcinoma and Heart
-
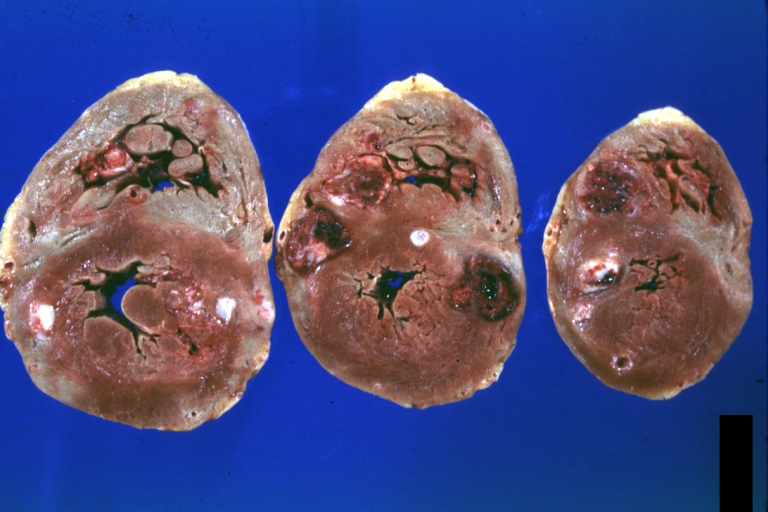 HEART: Metastatic Carcinoma: Gross natural color horizontal slices ventricles large metastatic renal cell carcinoma
HEART: Metastatic Carcinoma: Gross natural color horizontal slices ventricles large metastatic renal cell carcinoma -
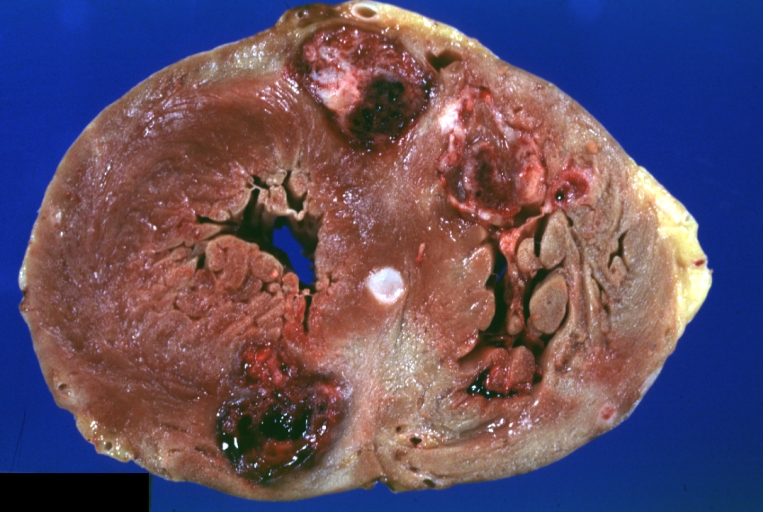 HEART: Metastatic Carcinoma: Gross natural color close-up of horizontal section ventricles with large hemorrhagic lesions (an excellent photo) in large metastatic renal cell carcinoma.
HEART: Metastatic Carcinoma: Gross natural color close-up of horizontal section ventricles with large hemorrhagic lesions (an excellent photo) in large metastatic renal cell carcinoma. -
 HEART: Metastatic Carcinoma: Gross fixed tissue, color, large lesions, primer is renal cell carcinoma.
HEART: Metastatic Carcinoma: Gross fixed tissue, color, large lesions, primer is renal cell carcinoma. -
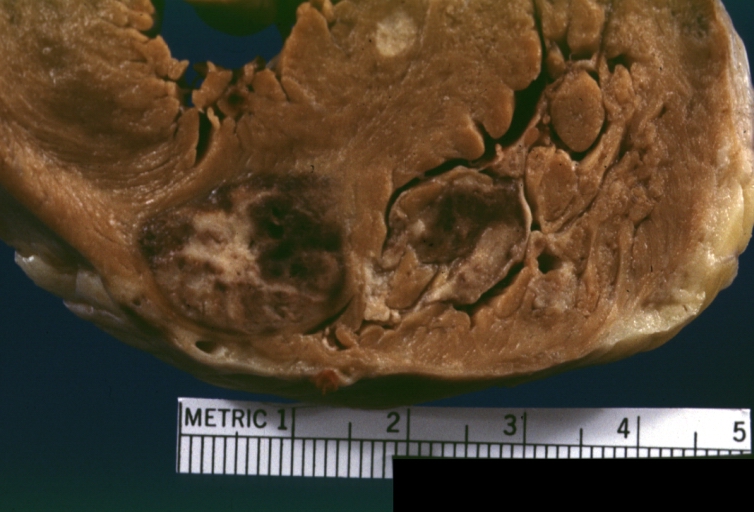 HEART: Metastatic Carcinoma: Gross fixed tissue, color, an excellent close-up of large hemorrhagic lesions primary is kidney
HEART: Metastatic Carcinoma: Gross fixed tissue, color, an excellent close-up of large hemorrhagic lesions primary is kidney




Source
- National Institute of Health
Autoimmune/Rheumatologic Disease and the Heart
Ankylosing Spondylitis | Antiphospholipid Syndrome | Behçet | Chagas | Crohn | Essential Mixed Cryoglobulinemia | Juvenile Idiopathic Arthritis | Kawasaki | Lupus | Mixed Connective Tissue Disorder | Polyarteritis Nodosa | Polychondritis | Polymyositis & Dermatomyositis | Psoriasis | Rheumatoid Arthritis | Scleroderma | Sarcoidosis | Takayasu | Temporal Arteritis | Ulcerative Colitis | Wegener’s Granulomatosis | Wilson
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor in Chief: Cafer Zorkun, M.D., Ph.D. [2]
Overview
The cardiovascular manifestations of underlying autoimmune diseases may go unrecognized and this may contribute to excess morbidity and mortality in these patients. [1] Below is a list of autoimmune diseases which may have cardiovascular manifestations.


List of Autoimmune Diseases Associated with Heart Disease in Some Studies
Diseases listed below in alphabetical order: [2] [3] [4] [5] [6] [7] [8] [9] [10] [11] [12] [13] [14] [15]
The Heart in Ankylosing Spondylitis
The Heart in Antiphospholipid Syndrome
The Heart in Essential Mixed Cryoglobulinemia
The Heart in Grave’s Disease (Overactive Thyroid)
The Heart in Guillain Barre Syndrome
The Heart in Hashimoto’s Thyroiditis (Underactive Thyroid)
The Heart in Juvenile Rheumatoid Arthritis
The Heart in Köhlmeier-Degos Disease
The Heart in Mixed Connective Tissue Disorders
The Heart in Polyarteritis Nodosa
The Heart in Polymyositis and Dermatomyositis
The Heart in Progressive Systemic Sclerosis (Scleroderma)
The Heart in Reiter’s Syndrome
The Heart in Rheumatoid Arthritis
The Heart in Sjögren’s Syndrome
The Heart in Systemic Lupus Erythematosus (SLE)
The Heart in Takayasu Arteritis
The Heart in Temporal Arteritis / Giant Cell Arteritis
The Heart in Ulcerative colitis
The Heart in Wegener’s Granulomatosis
References
- ↑ Matucci – Cerinic M, Seferovic PM. Heart involvement in autoimmune rheumatic diseases: the ‘‘phantom of the opera’’. Rheumatology 2006; 45:iv1–iv3
- ↑ ACP Medicine, 2007, Dale D C, Federman D D
- ↑ Braunwald’s Heart Disease 8th Ed, 2007, Libby P
- ↑ Mayo Clinic Cardiology, Concise Textbook, 3rd edition, 2007
- ↑ Hurst’s The Heart, Fuster V, 12th edition 2008
- ↑ NMS Medicine, 6th Edition, 2008
- ↑ Oxford Textbook of Medicine 4th edition (March 2003)
- ↑ Harris: Kelley’s Textbook of Rheumatology, 7th ed. 2005
- ↑ Robbins and Cotran PATHOLOGIC BASIS OF DISEASE, 7th Edition, 2005
- ↑ Washington Manual of Medical Therapeutics, The, 32nd Edition, 2007
- ↑ Cecil Textbook of Medicine, 23rd Edition, 2007
- ↑ Harrison’s Principals of Internal Medicine, 16th Edition, 2005
- ↑ Myocarditis, From Bench to Bedside, Cooper L T, 2003
- ↑ Endovascular Aneurysm Repair, From Bench to Bedside, Marty B. 2005
- ↑ Asherson R A. Pediatrics in Systemic Autoimmune Diseases, First edition, 2008
Pulmonary Embolism
For patient information, click here
For economy class syndrome, click here
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1] The APEX Trial Investigators; Associate Editor(s)-in-Chief: Cafer Zorkun, M.D., Ph.D. [2]; Rim Halaby, M.D. [3]
Synonyms and keywords: PE; lung blood clot; blood clot-lung; embolism-pulmonary
Diagnosis
Diagnostic Approach | Assessment of Clinical Probability and Risk Scores | Assessment of Probability of Subsequent VTE and Risk Scores | History and Symptoms | Physical Examination | Laboratory Findings | Arterial Blood Gas Analysis | D-dimer | Biomarkers | Electrocardiogram | Chest X Ray | Ventilation/Perfusion Scan | Echocardiography | Compression Ultrasonography | CT | MRI
Treatment
Treatment Approach | Medical Therapy | IVC Filter | Pulmonary Thrombectomy | Pulmonary Thromboendarterectomy | Discharge Care and Long Term Treatment | Prevention | Cost-Effectiveness of Therapy | Future or Investigational Therapies
Follow-Up
Special Scenarios
Trials
Case Studies
Related Chapters
Pulmonary Hypertension
For patient information click here
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Assistant Editor(s)-in-Chief: José Eduardo Riceto Loyola Junior, M.D.[2], Ralph Matar, Lisa Prior, Ann Slater, R.N., Rim Halaby, Mohamed Moubarak, M.D. [3]
Synonyms and keywords: Hypertensive pulmonary vascular disease; pulmonary arterial hypertension; PAH; hypertensive pulmonary vascular disease; Ayerza syndrome; Ayerza’s syndrome; Ayerza-Arrilaga syndrome
Diagnosis
Diagnostic Study of Choice | History & Symptoms | Physical Examination | Laboratory Findings | Electrocardiography | Chest x-ray | CT | MRI | Echocardiography or Ultrasound | Right heart catheterization | Other Diagnostic Studies
Treatment
Medical Therapy | Surgery | Primary Prevention | Secondary Prevention | Cost-Effectiveness of Therapy | Future or Investigational Therapies
Case Studies
External links
Cor Pulmonale
For the WikiPatient page for this topic, click here
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Jad Z Al Danaf, Rim Halaby
Synonyms and keywords: Cor pulmonale; right ventricular failure; RV failure
Diagnosis
History and Symptoms | Physical Examination | Laboratory Findings | Electrocardiogram | Chest X Ray | CT | MRI | Echocardiography
Treatment
Medical Therapy | Surgery | Primary Prevention | Secondary Prevention | Cost-Effectiveness of Therapy | Future or Investigational Therapies
Case Studies
Pre-Operative Clearance
HEMOCARDIOLOGY
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor-In-Chief: Mohammed A. Sbeih, M.D. [2]; Kashish Goel,M.D.
Please click here for Preoperative Cardiac Risk Assessment
For a printable checklist for pre-operative cardiac work up click here
Overview
The goal of the preoperative clearance (Preoperative medical assessment) is to assess the patient’s general medical condition in order to identify any unrecognized co-morbid diseases and optimize the patient’s state for the procedure. The preoperative medical assessment helps the doctors to decide if the patient is suitable for the proposed surgery according to the patient’s risk category, also it helps them to identify the factors that may reduce the patient’s risk for complications and provide the best possible recommendations for the post-operative care. Preoperative clearance usually starts by identifying the type of surgery to be performed and the risk category of the patient who needs this surgery.
Perioperative risk of death
Patients can be divided into different risk categories based on the basis of their preoperative medical assessment. This helps the doctors to decide if the patient is suitable for the proposed surgery or procedure, and identify the factors that may reduce the patient risk. There are many factors that may influence the risk of perioperative complications, including death.
- Anesthesia
- Although the modern anesthesia is safe, the risk of surgical complications varies according to the type of anesthesia (general or regional).
- The patient’s factors and surgical factors are more important risk predictors for post operative complications.
- The American society of anesthesiologists (ASA) classification is a predictor of perioperative mortality. It also predicts cardiac and pulmonary morbidity.
- ASA classification
Class Systemic disturbance Mortality rate 1 Healthy patient with no disease outside of the surgical process <0.03% 2 Mild-to-moderate systemic disease caused by the surgical condition or by other pathologic processes 0.2% 3 Severe disease process which limits activity but is not incapacitating 1.2% 4 Severe incapacitating disease process that is a constant threat to life 8% 5 Moribund patient not expected to survive 24 hours with or without an operation 34% E Suffix to indicate an emergency surgery for any class Increased
- Type of surgery
- Perioperative risk of complications varies according to the type of surgery.
- Patient age
- Emergency procedures
- In emergency procedures the risk of complications may increases two to four times, or even more than that in elderly patients.
- Pulmonary factors
- There are several pulmonary factors that may increase the risk of complications in surgical patients, these may include:
- Cigarete smoking.[3]
- Respiratory diseases.
- Abnormal chest x-ray or phisical examination findings.
- Thoracic or upper abdominal surgery.
- Morbid obesity.
- Age over 60.
- Cardiac factors
- There are several cardiac factors that may increase the risk of complications in surgical patients, these may include:
- History of prosthetic valves.
- History of rheumatic fever.
- Congestive heart failure.
- Arrhithmia.
Preoperative patient questionnaire
In general, the overall risk of surgery is extremely low in healthy individuals.
History
- The patient should be asked about his age. Some studies found a small increased risk of surgery with advanced age of the patient. The mortality rate for most surgical procedures increases linearly with age due to increasing numbers of comorbidities with advancing age.
- The patient should be asked if he had a history of:
- Heart diseases,irregular heart beat, murmurs or rheumatic fever as a child.
- Pulmonary diseases, such as asthma, bronchitis, or emphysema.
- Chest pain, angina, or chest tightness.
- Hypertension or hypotension.
- Shortness of breath, cough.
- Liver diseases, jaundice or hepatitis.
- Gastrointestinal problems or indigestion.
- Diabetes.
- Thyroid problems.
- Kidney problems.
- Weakness or numbness in the extremities.
- Seizures or blackouts.
- Bleeding disorders.
- Blood clotting abnormality.
- Arthritis or joint pain.
- The patient should be asked about:
- Any allergies for food or medication.
- A list of any medications he is currently taking, including over-the-counter medications and steroidal compounds. Nonsteroidal anti-inflammatory drugs are associated with :an increased risk of perioperative bleeding.
- Any other medical conditions in the past.
- Any previous surgeries or anesthesia.
- pregnancy state.
- Any problems with a previous surgery due to anesthesia.
- The patient should be asked when did he last eat or drink on the day of surgery.
- The patient should be asked about his height and weight. Studies showed that obesity is not a risk factor for most adverse postoperative outcomes, with the exception of :deep venous thrombosis and pulmonary embolism. However, some cardiac surgery studies have shown higher complication rates for obese patients, such as prolonged hospital stay, wound infections and prolonged mechanical ventilation [4] [5].
- The patient should be asked about his exercise capacity, patients with unlimited exercise tolerance generally have a low risk of postoperative complications. Those patients :can walk two blocks on level ground without symptoms,
- The patient should be asked if he smokes cigarettes, how many packs per day and for how many years.[3]
- The patient should be asked if he drinks alcohol. There is increased risk for postoperative complications in patients who misuse alcohol on a regular basis.[6]
- The patient should be asked about his family history.
Preoperative laboratory testing
The American society of anesthesiologists recommends against routine preoperative laboratory testing in the absence of clinical indications [7]. In specific circumstances, selective testing may be appropriate, such as in patients with underlying diseases or risk factors that would increase their risk for surgical complications. Also in specific high risk surgical procedures, these tests should be done. If there is no significant change in the clinical condition of the patient, it may be safe to use test results that were performed within the past four months. These tests include:
1. Complete blood count (CBC): Anemia maybe presents in asymptomatic patients and it is common following major surgery. Postoperative mortality maybe predicted by the preoperative hemoglobin level [8]. CBC test should be done for:
- Patients 65 years of age or older.
- Patients who are undergoing major surgery.
- Young patients who undergoing major surgery with the expectation to result in significant blood loss.
- Patients with a history that suggests anemia.
2. Renal function test (RFT): Serum creatinine concentration should be ordered for patients over the age of 50 undergoing intermediate or high risk surgeries, also it should be ordered if hypotension is likely, or when nephrotoxic medications will be used. Mild to moderate renal impairment is usually asymptomatic. Dosage adjustment of some medications may be needed if the patient has renal insufficiency.
3. Electrolytes: It is not recommended to be done routinely if the patient does not have a history of electrolytes abnormality.
4. Blood glucose: Diabetes increases the operative risk in patients undergoing vascular surgery or coronary artery bypass grafting [9][10]. Routine measurement of blood glucose is not recommended for healthy patients before the surgery, since some studies showed that unexpected abnormal blood glucose results do not often influence perioperative management [1][11].
5. Liver function tests (LFT): It is not recommended to do this test routinely unless the patient has a history of liver disease [12].
6. Hemostasis tests: It is not recommended to do prothrombin time (PT) or Partial thromboplastin time (PTT) blood tests routinely unless the patient has bleeding disorder or an unusual bleeding tendency [12]. Some doctors have suggested to test all patients who undergoing intermediate to high risk surgeries. This avoids the chance that clinicians may forget to ask the patients about their bleeding history. The bleeding time is not useful in assessing the risk of perioperative hemorrhage [12][13].
7. Urinalysis: It is usually done to detect any urinary tract infection which has the potential to cause wound infection after the surgery [14], especially with prosthetic surgery. If the test is positive, the patient should be treated with antibiotics and proceed with surgery without delay. Some studies showed that there is no reduction in the risk of postoperative wound infection if the patient treated with antibiotics before the surgery, and so, it is not indicated to test for Urinary tract infection before the surgery for every patient [15][16].
8. Pregnancy testing: Pregnant women may need specific perioperative management, this includes specific anesthetic teqniques. An elective surgery may be cancelled or postponed in pregnant women. The American society of anesthesiologists recommends that clinicians consider pregnancy testing for all woman of childbearing age [7]. Many institutions require pregnancy testing for all reproductive age women before surgery.
9. Electrocardiogram (EKG): This should be done to detect any recent myocardial infarction (MI) which known to be associated with increased surgical morbidity and mortality [1], also it may be important as a baseline to be compared with the one postoperatively. In general, EKG alone may be a poor indicator of postoperative cardiac complications. The 2007 American college of cardiology/American heart association (ACC/AHA) Guidelines on perioperative cardiovascular evaluation states that ECG is not useful in asymptomatic patients undergoing low risk procedures [17]. Also, the European Society of Cardiology 2009 preoperative guidelines do not recommend ECG in patients without risk factors [18]. According to the 2007 ACC/AHA guidelines the 12-lead ECG are recommended for the following patients:
- Patients who are scheduled to undergo vascular surgery and have at least one of the following clinical risk factors:
- Ischemic heart disease.
- Compensated or prior heart failure.
- Cerebrovascular disease.
- Diabetes.
- Renal insufficiency.
- It is less strongly recommended to perform an ECG for patients scheduled to undergo vascular surgery with no clinical risk factors.
- Patients who are scheduled to undergo intermediate-risk surgery with known cardiovascular disease, peripheral artery disease, or cerebrovascular disease.It is less strongly recommended to perform an ECG for patients scheduled to undergo intermediate-risk surgery with at least one clinical risk factor.
10. Chest radiograph (Chest x-ray): Its not recommended to do this test routinely before the operations in healthy patients, many studies showed that an abnormal chest x-ray findings may occur frequently, especially in elderly persons [19]. According to the American College of Physicians (ACP), if there is a suspicion of cardiopulmonary disease from the patient’s history or physical examination, then this test should be done, also in those older than 50 years of age who are undergoing abdominal aortic aneurysm surgery or upper abdominal/thoracic surgery [20]. The American heart association (AHA) recommends preoperative chest x-ray for patients with morbid obesity (BMI ≥40 kg/m2)[21].
11. Pulmonary function test (PFT): This test only recommended for patients who have dyspnea or other abnormal respiratory clinical findings such as decreased breath sounds, prolonged expiratory phase, rales, rhonchi, or wheezes [22].
Thromboembolism prophylaxis
Orthopedic surgery
For knee of hip arthroplasty
- The CRISTAL trial found more benefit (mainly from reducing distal DVTs) from Enoxaparin than aspirin (aspirin 100 mg daily or enoxaparin 40 mg daily for 35 days after hip replacement and 14 days after knee replacement)[23].
- However shorter therapy,After an initial 5 days of rivaroxaban, 9 days of aspirin or rivaroxaban may similarly reduce thromboembolism according to the EPCAT II trial[24].
For knee arthroscopy
- Evidence from trials conflicts:
- Low molecular weight heparin did not prevent thromboembolism in the POT-KAST trial trial published in 2017[25]. There was no routine imaging for outcomes in this study. Average age of patients was 56. The patients were not routinely imaged for thromboembolism.
- In comparing their negative results to the two positive studies below, the POT-KAST authors noted “…in both trials, all the participants underwent ultrasonographic screening for venous thromboembolism, at which time questions were asked about possible signs and symptoms. This clearly does not reflect the method for identification of symptomatic venous thromboembolism that is used in general clinical practice and has therefore led to overestimation of the incidences.”
- Rivaroxaban once-daily rivaroxaban (10 mg) for .seven days may be better than placebo at preventing thromboembolism in the ERIKA trial published in 2016[26]. Average age of patients was 46. All patients received colour-coded Doppler ultrasonography (CCDU) after seven days.
- Low molecular weight heparin did prevent thromboembolism as compared to compression stockings in a trial published in 2008[27]. In this trial, “All patients had bilateral, whole-leg, color-coded Doppler ultrasonography at the end of prophylaxis (8 or 15 days).”
- Low molecular weight heparin did not prevent thromboembolism in the POT-KAST trial trial published in 2017[25]. There was no routine imaging for outcomes in this study. Average age of patients was 56. The patients were not routinely imaged for thromboembolism.
- For systematic reviews:
- The Cochrane Collaboration concludes “There is moderate- to low-certainty evidence of no benefit from the use of LMWH, aspirin or rivaroxaban in reducing this small risk of PE or symptomatic DVT. There is very low-certainty evidence that LMWH use may reduce the risk of asymptomatic DVT when compared to no treatment but it is uncertain how this directly relates to incidence of DVT or PE in healthy patients”[28]
External links
http://www.askdrwiki.com/mediawiki/index.php?title=Preoperative_Clearance
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2146059/
http://circ.ahajournals.org/content/116/17/e418.full.pdf+html
References
- ↑ 1.0 1.1 1.2 Goldman L, Caldera DL, Nussbaum SR, Southwick FS, Krogstad D, Murray B; et al. (1977). “Multifactorial index of cardiac risk in noncardiac surgical procedures”. N Engl J Med. 297 (16): 845–50. doi:10.1056/NEJM197710202971601. PMID 904659.
- ↑ Linn BS, Linn MW, Wallen N (1982). “Evaluation of results of surgical procedures in the elderly”. Ann Surg. 195 (1): 90–6. PMC 1352408. PMID 7055387.
- ↑ 3.0 3.1 Jones R, Nyawo B, Jamieson S, Clark S (2011). “Current smoking predicts increased operative mortality and morbidity after cardiac surgery in the elderly”. Interact Cardiovasc Thorac Surg. 12 (3): 449–53. doi:10.1510/icvts.2010.239863. PMID 21097455.
- ↑ Yap CH, Zimmet A, Mohajeri M, Yii M (2007). “Effect of obesity on early morbidity and mortality following cardiac surgery”. Heart Lung Circ. 16 (1): 31–6. doi:10.1016/j.hlc.2006.09.007. PMID 17161973.
- ↑ Kuduvalli M, Grayson AD, Oo AY, Fabri BM, Rashid A (2002). “Risk of morbidity and in-hospital mortality in obese patients undergoing coronary artery bypass surgery”. Eur J Cardiothorac Surg. 22 (5): 787–93. PMID 12414047.
- ↑ Tønnesen H, Nielsen PR, Lauritzen JB, Møller AM (2009). “Smoking and alcohol intervention before surgery: evidence for best practice”. Br J Anaesth. 102 (3): 297–306. doi:10.1093/bja/aen401. PMID 19218371.
- ↑ 7.0 7.1 American Society of Anesthesiologists Task Force on Preanesthesia Evaluation (2002). “Practice advisory for preanesthesia evaluation: a report by the American Society of Anesthesiologists Task Force on Preanesthesia Evaluation”. Anesthesiology. 96 (2): 485–96. PMID 11818784.
- ↑ Mathew A, Devereaux PJ, O’Hare A, Tonelli M, Thiessen-Philbrook H, Nevis IF; et al. (2008). “Chronic kidney disease and postoperative mortality: a systematic review and meta-analysis”. Kidney Int. 73 (9): 1069–81. doi:10.1038/ki.2008.29. PMID 18288098.
- ↑ Eagle KA, Coley CM, Newell JB, Brewster DC, Darling RC, Strauss HW; et al. (1989). “Combining clinical and thallium data optimizes preoperative assessment of cardiac risk before major vascular surgery”. Ann Intern Med. 110 (11): 859–66. PMID 2655519.
- ↑ Higgins TL, Estafanous FG, Loop FD, Beck GJ, Blum JM, Paranandi L (1992). “Stratification of morbidity and mortality outcome by preoperative risk factors in coronary artery bypass patients. A clinical severity score”. JAMA. 267 (17): 2344–8. PMID 1564774.
- ↑ Velanovich V (1991). “The value of routine preoperative laboratory testing in predicting postoperative complications: a multivariate analysis”. Surgery. 109 (3 Pt 1): 236–43. PMID 2000554.
- ↑ 12.0 12.1 12.2 Smetana GW, Macpherson DS (2003). “The case against routine preoperative laboratory testing”. Med Clin North Am. 87 (1): 7–40. PMID 12575882.
- ↑ Peterson P, Hayes TE, Arkin CF, Bovill EG, Fairweather RB, Rock WA; et al. (1998). “The preoperative bleeding time test lacks clinical benefit: College of American Pathologists’ and American Society of Clinical Pathologists’ position article”. Arch Surg. 133 (2): 134–9. PMID 9484723.
- ↑ Koulouvaris P, Sculco P, Finerty E, Sculco T, Sharrock NE (2009). “Relationship between perioperative urinary tract infection and deep infection after joint arthroplasty”. Clin Orthop Relat Res. 467 (7): 1859–67. doi:10.1007/s11999-008-0614-8. PMC 2690738. PMID 19009324.
- ↑ Lawrence VA, Kroenke K (1988). “The unproven utility of preoperative urinalysis. Clinical use”. Arch Intern Med. 148 (6): 1370–3. PMID 3377621.
- ↑ Ollivere BJ, Ellahee N, Logan K, Miller-Jones JC, Allen PW (2009). “Asymptomatic urinary tract colonisation predisposes to superficial wound infection in elective orthopaedic surgery”. Int Orthop. 33 (3): 847–50. doi:10.1007/s00264-008-0573-4. PMC 2903079. PMID 18521600.
- ↑ Fleisher LA, Beckman JA, Brown KA, Calkins H, Chaikof EL, Fleischmann KE; et al. (2009). “2009 ACCF/AHA focused update on perioperative beta blockade incorporated into the ACC/AHA 2007 guidelines on perioperative cardiovascular evaluation and care for noncardiac surgery: a report of the American college of cardiology foundation/American heart association task force on practice guidelines”. Circulation. 120 (21): e169–276. doi:10.1161/CIRCULATIONAHA.109.192690. PMID 19884473.
- ↑ Task Force for Preoperative Cardiac Risk Assessment and Perioperative Cardiac Management in Non-cardiac Surgery. European Society of Cardiology (ESC). Poldermans D, Bax JJ, Boersma E, De Hert S; et al. (2009). “Guidelines for pre-operative cardiac risk assessment and perioperative cardiac management in non-cardiac surgery”. Eur Heart J. 30 (22): 2769–812. doi:10.1093/eurheartj/ehp337. PMID 19713421.
- ↑ García-Miguel FJ, Serrano-Aguilar PG, López-Bastida J (2003). “Preoperative assessment”. Lancet. 362 (9397): 1749–57. PMID 14643127.
- ↑ Smetana GW, Lawrence VA, Cornell JE, American College of Physicians (2006). “Preoperative pulmonary risk stratification for noncardiothoracic surgery: systematic review for the American College of Physicians”. Ann Intern Med. 144 (8): 581–95. PMID 16618956. Review in: ACP J Club. 2006 Sep-Oct;145(2):37
- ↑ Poirier P, Alpert MA, Fleisher LA, Thompson PD, Sugerman HJ, Burke LE; et al. (2009). “Cardiovascular evaluation and management of severely obese patients undergoing surgery: a science advisory from the American Heart Association”. Circulation. 120 (1): 86–95. doi:10.1161/CIRCULATIONAHA.109.192575. PMID 19528335.
- ↑ Lawrence VA, Dhanda R, Hilsenbeck SG, Page CP (1996). “Risk of pulmonary complications after elective abdominal surgery”. Chest. 110 (3): 744–50. PMID 8797421.
- ↑ CRISTAL Study Group. Sidhu VS, Kelly TL, Pratt N, Graves SE, Buchbinder R; et al. (2022). “Effect of Aspirin vs Enoxaparin on Symptomatic Venous Thromboembolism in Patients Undergoing Hip or Knee Arthroplasty: The CRISTAL Randomized Trial”. JAMA. 328 (8): 719–727. doi:10.1001/jama.2022.13416. PMC 9399863 Check
|pmc=value (help). PMID 35997730 Check|pmid=value (help). - ↑ Anderson DR, Dunbar M, Murnaghan J, Kahn SR, Gross P, Forsythe M; et al. (2018). “Aspirin or Rivaroxaban for VTE Prophylaxis after Hip or Knee Arthroplasty”. N Engl J Med. 378 (8): 699–707. doi:10.1056/NEJMoa1712746. PMID 29466159.
- ↑ van Adrichem RA, Nemeth B, Algra A, le Cessie S, Rosendaal FR, Schipper IB; et al. (2017). “Thromboprophylaxis after Knee Arthroscopy and Lower-Leg Casting”. N Engl J Med. 376 (6): 515–525. doi:10.1056/NEJMoa1613303. PMID 27959702.
- ↑ Camporese G, Bernardi E, Noventa F, Bosco M, Monteleone G, Santoro L; et al. (2016). “Efficacy of Rivaroxaban for thromboprophylaxis after Knee Arthroscopy (ERIKA). A phase II, multicentre, double-blind, placebo-controlled randomised study”. Thromb Haemost. 116 (2): 349–55. doi:10.1160/TH16-02-0118. PMID 27075710.
- ↑ Camporese G, Bernardi E, Prandoni P, Noventa F, Verlato F, Simioni P; et al. (2008). “Low-molecular-weight heparin versus compression stockings for thromboprophylaxis after knee arthroscopy: a randomized trial”. Ann Intern Med. 149 (2): 73–82. doi:10.7326/0003-4819-149-2-200807150-00003. PMID 18626046. Review in: ACP J Club. 2008 Dec 16;149(6):10
- ↑ Perrotta C, Chahla J, Badariotti G, Ramos J (2020). “Interventions for preventing venous thromboembolism in adults undergoing knee arthroscopy”. Cochrane Database Syst Rev. 5: CD005259. doi:10.1002/14651858.CD005259.pub4. PMC 7202465 Check
|pmc=value (help). PMID 32374919 Check|pmid=value (help).
The Role of the Coagulation System in Heart Disease
CORONARY ARTERY DISEASE
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]
Associate Editor-In-Chief: Cafer Zorkun, M.D., Ph.D. [2]
Overview
The fibrinolytic system dissolved intravascular clots as a result of plasmin, an enzyme that digests fibrin. Plasminogen, an inactive precursor, is converted in plasmin. Plasmin is a relatively nonspecific protease – it digests fibrin clots and other plasma proteins, including some coagulating factors. Tissue plasminogen activator (t-PA) is released from endothelial cells in response of various signals, including stasis produced by vascular occlusion.
Therapy with thrombolytic drugs tends to dissolve both pathological thrombi and fibrin deposits in sites of vascular injury.
Platelets provide the initial hemostatic plug at sites of vascular injury. They also participate in reactions that lead to atherosclerosis and pathological thrombosis. Antagonists of platelet function thus have been used in attempt to prevent thrombosis and to alter the natural progress of athrosclerotic vascular disease.
Hemostasis is the cessation of blood loss from the damaged vessel. First platelets adhere to the injured regions of blood vessel, they aggregate to form of primary hemostatic plug. Platelets stimulate local activation of plasma coagulation factors, leading to generation of fibrin clot that reinforces the platelet aggregate. Thrombosis is a pathological process in which platelets aggregate and/or fibrin clot occludes a blood vessel. Arterial thrombosis may result in ischemic necrosis of the tissue supplied by the artery. Venous thrombosis may cause tissue drained by the vein to become edematous and inflamed. Thrombosis of a deep vein may be complicated by pulmonary embolism.
Platelet aggregation and coagulation normally do not occur within an intact blood vessel. Thrombosis is prevented by several regulatory mechanisms that require a normal vascular endothelium. Prostacyclin (PGI-2), a metabolite of arachidonic acid, is synthesized by endothelial cells, and inhibits platelets aggregation and secretion. Antithrombin is a plasma protein that inhibits coagulation factors. Heparan sulfate synthesized by endothelial cells stimulate the activity of antithrombin. Protein C in combination with protein S degrade coagulating cofactors Va and VIIIa and diminishes the rates of activation of prothrombin and factor X.
A number of studies have clearly shown the association of increased plasma fibrinogen levels with cardiovascular disease. Interestingly, preliminary results from the Bezafibrate Infarction Prevention (BIP) study have pointed out that the reduction of the increased fibrinogen levels in CAD patients could decrease the incidence of cardiac death and ischemic stroke. The substantial variability of plasma fibrinogen levels owing to a number of factors including the assay used, socioeconomic and metabolic factors, etc. limit the wide application of this coagulation factor as a risk factor in every-day clinical practice. It should be mentioned that smoking cessation, weight loss, regular exercise,moderate alcohol consumption and fibrates can significantly reduce plasma fibrinogen levels.[1] [2] [3] [4] [5] [6] [7] [8] [9] [10]
Several other factors participating in blood coagulation have been associated with CVD risk,including factor VII levels, plasminogen activator inhibitor (PAI-1) and increased platelet aggregation. Compelling evidence from randomized controlled trials now exists on the beneficial effect of antiplatelet agents (mainly aspirin) in the prevention of cardiovascular events in patients with established vascular disease. However, there is no unequivocal evidence on the beneficial effect of aspirin in the primary prevention of CVD taking into account the long-term risks of therapy. It should be mentioned that in well-controlled treated hypertensive patients, as well as in men at particularly high risk, aspirin results in a significant decrease in cardiovascular events. [11] [12] [13] [14] [15] [16]
References
- ↑ Kannel, W. B., Wolf, P. A., Castelli, W. P. et al. (1987).Fibrinogen and risk of cardiovascular disease. JAMA,258, 1183-1186
- ↑ Ernst, E. and Resch, K. L. (1993). Fibrinogen as a cardiovascular risk factor: a meta-analysis and review of the literature. Ann. Intern. Med., 118, 956-963
- ↑ Behar, S. (1999). Lowering fibrinogen levels clinical update. BIP Study Group. Bezafibrate infarction Prevention. Blood Coagul. Fibrinolysis, 10, 41-43
- ↑ Barasch, E., Benderly, M., Graff, E. et al. (1995).Plasma fibrinogen levels and their correlates in 6457coronary heart disease patients. The Bezafibrate Infarction Prevention (BIP) Study. J. Clin.Epidemiol., 48, 757-765
- ↑ Brunner, E., Smith, G. D., Marmot, M. et al. (1996).Childhood social circumstances and psychological and behavioural factors as determinants of plasma fibrinogen. Lancet, 347, 1008-1013
- ↑ Muldoon, M. F., Herbert, T. B., Patterson, S. M. et al.(1995). Effects of acute psychological stress on serum lipid levels, hemo concentration, and blood viscosity.Arch. Intern. Med., 155, 615-620
- ↑ Meade, T. W., North, W. R., Chakrabarti, R. et al.(1977). Population-based distributions of haemostatic variables. Br. Med. Bull., 33, 283-288
- ↑ Ernst, E. and Resch, K. L. (1995). Therapeutic interventions to lower plasma fibrinogen concentration. Eur. Heart J., 16 (Suppl A), 47-53
- ↑ Mikhailidis, D. P., Ganotakis, E. S., Spyropoulos, K.A. et al. (1998). Prothrombotic and lipoprotein variables in patients attending a cardiovascular risk management clinic: response to ciprofibrate or lifestyle advice. Int. Angiol., 17, 225-233
- ↑ Papadakis, J. A., Ganotakis, E. S., Jagroop, I. A. et al.(1999). Effect of hypertension and its treatment on lipid, lipoprotein (a), fibrinogen, and bilirubin levels in patients referred for dyslipidemia. Am. J.Hypertens., 12, 673-681
- ↑ Pazzucconi, F., Mannucci, L., Mussoni, L. et al.(1992). Bezafibrate lowers plasma lipids, fibrinogen and platelet aggregability in hypertriglyceridemia.Eur. J. Clin. Pharmacol., 43, 219-223
- ↑ Meade, T. W. Jr (1992). Fibrinogen and other clotting factors in cardiovascular disease. In: Francis, R. B. Jr(Ed), Atherosclerotic Vascular Disease, Hemostasis, and Endothelial Function. Marcel Dekker, New York, 1-32
- ↑ Junker, R., Heinrich, J., Schulte, H. et al. (1997).Coagulation factor VII and the risk of coronary heart disease in healthy men. Arterioscler. Thromb. Vasc.Biol., 17, 1539-1544
- ↑ Elwwood, P. C., Renaud, S., Sharp, D. S. et al.(1991). Ischaemic heart disease and platelet aggregation. The Caerphilly Collaborative Heart disease Study. Circulation, 83, 38-44
- ↑ Hennekens, C. H. (1999). Update on aspirin in the treatment and prevention of cardiovascular disease.Am. Heart J., 137, 9-13
- ↑ Hansson, L., Zanchetti, A., Carruthers, S. G. et al. for the HOT Study Group (1998). Effects of intensive blood pressure lowering and low-dose aspirin inpatients with hypertension: principal results of the Hypertension Optimal Treatment (HOT) Randomized Trial. Lancet, 351, 1755-1762
Atherosclerosis Prevention and Risk Factor Modification
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]
Overview
Prevention of coronary heart disease can be divided into primary prevention aimed at preventing an initial episode or manifestion of the disease, and secondary prevention aimed at preventing a second episode in a patient with coronary artery disease or a coronary artery disease equivalent. It is critical to perform risk factor assessment to identify optimal candidates for primary prevention and secondary prevention of coronary artery disease.
Main Chapters
References
Chronic Stable Angina
Introduction | Definition | Historical Perspective | Epidemiology | Pathophysiology | Presentation | Recognition of Clinical Subsets | Risk Factors | Diagnosis | Differential Diagnosis of Chest Pain | Treatment | Prognosis | Rehabilitation | Prevention
For patient information, click here
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-In-Chief: Cafer Zorkun, M.D., Ph.D. [2]; Vijay Kunadian, M.D., Ph.D.; Smita Kohli, M.D.; Lakshmi Gopalakrishnan, M.B.B.S., Aysha Aslam, M.B.B.S[3]
Synonyms and keywords: Stenocardia; angina pectoris; angor pectoris
Classification
Classic: Chronic Stable Angina
Atypical: Walk through Angina | Mixed Angina | Nocturnal Angina | Postprandial Angina | Cardiac Syndrome X | Vasospastic Angina
ECG/Chest X-Ray | Rest LV Function | Exercise Treadmill Test | Stress Imaging in Patients who are Able to Exercise | Stress Imaging in Patients who are Unable to Exercise | Coronary Angiography
Diagnosis
History and Symptoms | Physical Examination | Test Selection Guideline for the Individual Basis | Laboratory Findings | Electrocardiography | Exercise ECG | Chest X-Ray | Myocardial Perfusion Scintigraphy with Pharmacologic Stress | Myocardial Perfusion Scintigraphy with Thallium | Echocardiography | Exercise Echocardiography | Positron Emission Tomography | Ambulatory ST Segment Monitoring | Electron Beam Tomography | Cardiac Magnetic Resonance Imaging | Coronary Angiography
- Anti-platelet Agents: Aspirin | Dipyridamole | Clopidogrel
- Anti-anginal Agents: Nitrates | Beta Blockers | Calcium Channel Blockers | Potassium Channel Openers | Newer Anti-anginal Agents
Revascularization: PCI | CABG | Guidelines for Revascularization | PCI vs Medical Therapy | CABG vs Medical Therapy | PCI and CABG versus Medical Therapy | PCI vs CABG
Alternative Therapies for Refractory Angina: Transmyocardial Revascularization (TMR) | Spinal Cord Stimulation (SCS) | Enhanced External Counter Pulsation (EECP) | ACC/AHA Guidelines for Alternative Therapies in patients with Refractory Angina
Discharge Care
Patient Follow-Up | Rehabilitation
Secondary Prevention
Overview | Smoking Cessation | Weight Management | Physical Activity | Lipid Management | BP Control | Diabetes Control | Influenza Vaccination | ACC/AHA Guidelines for Cardiovascular Risk Factor Reduction
Guidelines for Asymptomatic Patients
Noninvasive Testing in Asymptomatic Patients | Coronary Angiography in Asymptomatic Patients | Pharmacotherapy to Prevent MI and Death in Asymptomatic Patients
Case Studies
Related Chapters
Unstable Angina
For patient information, click here
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-In-Chief: Cafer Zorkun, M.D., Ph.D. [2]; Varun Kumar, M.B.B.S.; Lakshmi Gopalakrishnan, M.B.B.S.; Smita Kohli, M.D.; Neil Gheewala, M.D. [3]; Bryan Piccirillo, B.S., M.D.
Synonyms and keywords: Angina at rest; rest angina; progressive angina; crescendo angina; accelerating angina; new-onset angina; pre-infarction angina; unstable angina pectoris; UAP; UA; new-onset angina; angina – unstable
Unstable Angina | Non-ST Elevation Myocardial Infarction
Special Groups
Women | Diabetic Patients | Post CABG Patients | Elderly | Chronic Kidney Disease | Substance Abusers | Prinzmetal’s Angina | Cardiovascular Syndrome X
Diagnosis
History and Symptoms | Physical Examination | Blood Studies | Biomarkers | Electrocardiogram | Chest X Ray | Echocardiography | Coronary Angiography
Immediate Management: Overview | Oxygen | Nitrates | Analgesics | Beta Blockers | Calcium Channel Blocker | Renin-Angiotensin-Aldosterone Inhibitors
Antithrombin Therapy: Overview | Unfractionated Heparin | Low Molecular Weight Heparin | Direct Thrombin Inhibitors | Factor Xa Inhibitors | Long Term Anticoagulation
Antiplatelet Agents: Antiplatelet Therapy Recommendations | Aspirin | Thienopyridines | Glycoprotein IIb/IIIa Inhibitor | Additional Management Considerations
Mechanical Reperfusion: Initial Conservative Versus Initial Invasive Strategies | PCI | CABG
Complications of Bleeding and Transfusion: Overview | Incidence | Definitions | Predictors and Causes of Bleeding | Blood Transfusions | Prognosis | Prevention | Recommendations
Discharge Care: Medical Regimen | Post-Discharge Follow-Up | Cardiac Rehabilitation
Long-Term Medical Therapy and Secondary Prevention: Overview | Convalescent and Long-Term Antiplatelet Therapy | Beta Blockers | Inhibition Of The Renin-Angiotensin-Aldosterone System | Nitroglycerin Therapy | Calcium Channel Blockers | Warfarin Therapy | Lipid Management | Blood Pressure Control | Smoking Cessation | Weight Management | Physical Activity | Patient Education | Influenza | Depression | Nonsteroidal Anti-Inflammatory Drugs | Hormone Therapy | Antioxidant Vitamins and Folic Acid | Quality Care and Outcomes
Future or Investigational Therapies
Contraindicated medications
Unstable angina is considered an absolute contraindication to the use of the following medications:
Case Studies
Related Chapters
- Acute Coronary Syndrome Risk Stratification
- Chronic stable angina
- Non ST Elevation Myocardial Infarction
- ST Elevation Myocardial Infarction
- Coronary Heart Disease
- PCI
External Links
- Clinical Trial Results: An up to date resource of Cardiovascular Research
- Risk Assessment Tool for Estimating Your 10-year Risk of Having a Heart Attack – based on information of the Framingham Heart Study, from the United States National Heart, Lung and Blood Institute
Non ST Elevation Myocardial Infarction
For patient information, click here
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-In-Chief: Cafer Zorkun, M.D., Ph.D. [2]; Varun Kumar, M.B.B.S.; Lakshmi Gopalakrishnan, M.B.B.S.; Smita Kohli, M.D.; Neil Gheewala, M.D. [3]; Bryan Piccirillo, B.S., M.D.
Synonyms and keywords: Angina at rest; rest angina; progressive angina; crescendo angina; accelerating angina; new-onset angina; pre-infarction angina; unstable angina pectoris; UAP; UA; new-onset angina; angina – unstable
Unstable Angina | Non-ST Elevation Myocardial Infarction
Special Groups
Women | Diabetic Patients | Post CABG Patients | Elderly | Chronic Kidney Disease | Substance Abusers | Prinzmetal’s Angina | Cardiovascular Syndrome X
Diagnosis
History and Symptoms | Physical Examination | Blood Studies | Biomarkers | Electrocardiogram | Chest X Ray | Echocardiography | Coronary Angiography
Immediate Management: Overview | Oxygen | Nitrates | Analgesics | Beta Blockers | Calcium Channel Blocker | Renin-Angiotensin-Aldosterone Inhibitors
Antithrombin Therapy: Overview | Unfractionated Heparin | Low Molecular Weight Heparin | Direct Thrombin Inhibitors | Factor Xa Inhibitors | Long Term Anticoagulation
Antiplatelet Agents: Antiplatelet Therapy Recommendations | Aspirin | Thienopyridines | Glycoprotein IIb/IIIa Inhibitor | Additional Management Considerations
Mechanical Reperfusion: Initial Conservative Versus Initial Invasive Strategies | PCI | CABG
Complications of Bleeding and Transfusion: Overview | Incidence | Definitions | Predictors and Causes of Bleeding | Blood Transfusions | Prognosis | Prevention | Recommendations
Discharge Care: Medical Regimen | Post-Discharge Follow-Up | Cardiac Rehabilitation
Long-Term Medical Therapy and Secondary Prevention: Overview | Convalescent and Long-Term Antiplatelet Therapy | Beta Blockers | Inhibition Of The Renin-Angiotensin-Aldosterone System | Nitroglycerin Therapy | Calcium Channel Blockers | Warfarin Therapy | Lipid Management | Blood Pressure Control | Smoking Cessation | Weight Management | Physical Activity | Patient Education | Influenza | Depression | Nonsteroidal Anti-Inflammatory Drugs | Hormone Therapy | Antioxidant Vitamins and Folic Acid | Quality Care and Outcomes
Future or Investigational Therapies
Contraindicated medications
Unstable angina is considered an absolute contraindication to the use of the following medications:
Case Studies
Related Chapters
- Acute Coronary Syndrome Risk Stratification
- Chronic stable angina
- Non ST Elevation Myocardial Infarction
- ST Elevation Myocardial Infarction
- Coronary Heart Disease
- PCI
External Links
- Clinical Trial Results: An up to date resource of Cardiovascular Research
- Risk Assessment Tool for Estimating Your 10-year Risk of Having a Heart Attack – based on information of the Framingham Heart Study, from the United States National Heart, Lung and Blood Institute
ST Elevation Myocardial Infarction
Overview | Epidemiology and Demographics | Pathophysiology of Reperfusion | Risk Factors | Pathophysiology | Triggers | Classification
Diagnosis | Symptoms | Physical Examination | Electrocardiogram | Cardiac Markers | Coronary Angiography | Histopathology
Treatment | Pre-Hospital Care | Initial Care | Thrombolytic Therapy | Primary Percutaneous Coronary Intervention | Rescue Percutaneous Coronary Intervention | Facilitated Percutaneous Coronary Intervention | Coronary Artery Bypass Graft Surgery | Barriers to Implementing Clinical Guidelines
ST Elevation Myocardial Infarction Arrhythmia Monitoring | Secondary Prevention | Complications | Prognosis | ST Elevation Myocardial Infarction | Cardiac Rehabilitation
For patient information click here
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1] Arzu Kalayci, M.D. [2]
Synonyms and keywords: AMI, STEMI, heart attack, MI, myocardial infarct, acute MI, coronary, coronary thrombosis
Anterior myocardial infarction | Inferior myocardial infarction | Right ventricular myocardial infarction | Posterior myocardial infarction | Lateral myocardial infarction
Pathophysiology of Vessel Occlusion | Pathophysiology of Reperfusion | Gross Pathology | Histopathology
Diagnosis
Diagnostic Criteria | History and Symptoms | Physical Examination | Laboratory Findings | Electrocardiogram | EKG Examples | Chest X Ray | Cardiac MRI | Echocardiography | Coronary Angiography
Treatment
Oxygen | Nitrates | Analgesics | Aspirin | Beta Blockers | Antithrombins | The coronary care unit | The step down unit | STEMI and Out-of-Hospital Cardiac Arrest
Pharmacologic Reperfusion | Reperfusion Therapy (Overview of Fibrinolysis and Primary PCI) | Fibrinolysis
Mechanical Reperfusion | The importance of reducing Door-to-Balloon times | Primary PCI | Adjunctive and Rescue PCI | Rescue PCI | Facilitated PCI | Adjunctive PCI | CABG | Management of Patients Who Were Not Reperfused | Assessing Success of Reperfusion
Antithrombin Therapy | Antithrombin therapy | Unfractionated heparin | Low Molecular Weight Heparinoid Therapy | Direct Thrombin Inhibitor Therapy | Factor Xa Inhibition | DVT prophylaxis | Long term anticoagulation
Antiplatelet Agents | Aspirin | Thienopyridine Therapy | Glycoprotein IIbIIIa Inhibition
Other Initial Therapy | Inhibition of the Renin-Angiotensin-Aldosterone System | Magnesium Therapy | Glucose Control | Calcium Channel Blocker Therapy | Lipid Management
Long-Term Medical Therapy and Secondary Prevention
Overview | Inhibition of the Renin-Angiotensin-Aldosterone System | Cardiac Rehabilitation | Pacemaker Implantation | Long Term Anticoagulation | Implantable Cardioverter Defibrillator
Case Studies
Case #1 | Case #2 | Case #3 | Case #4 | Case #5
Disclaimer
Any recommendations found on these pages are for education use only. WikiDoc is not a substitute for a licensed healthcare provider. Please see the disclaimers page for important information regarding limitations of the information found here.
The Living Guidelines
PHARMACOTHERAPY
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]
Associate Editor-In-Chief: Cafer Zorkun, M.D., Ph.D. [2]
Any recommendations found on these pages are for education use only. WikiDoc is not a substitute for a licensed healthcare provider. Please see the disclaimers page for important information regarding limitations of the information found here. In suggesting edits to the guidelines, WikiDoc suggests that the following classification scheme be used. Read more about the classification scheme used by the ACC / AHA Guidelines Committee here.
Cardiovascular Pharmacotherapy
Adrenergic Agonists
Adrenergic Agonists Overview
Direct Acting | Dobutamine | Dopamine | Epinephrine | Formoterol | Isoproterenol | Metaproterenol | Methoxamine | Norepinephrine | Phenylephrine | Salmeterol | Tamsulosin | Terbutaline
Indirect Acting | Amphetamine | Tyramine
Mixed Action | Ephedrine
Angiotensin-Renin Inhibitors (C09)
ACE Inhibitor Overview | Benazepril | Captopril | Enalapril | Fosinopril | Lisinopril | Perindopril | Quinapril | Ramipril | Spirapril | Trandolapril
Angiotensin II receptor antagonist Overview | Candesartan | Eprosartan | Irbesartan | Losartan | Olmesartan | Tasosartan | Telmisartan | Valsartan
Renin Inhibitors Overview | Aliskiren | Remikiren
Antiarrhythmic agents
Antiarrhythmic Agents Overview (C01B)
Class Ia | Ajmaline | Disopyramide | Prajmaline | Procainamide | Quinidine | Sparteine
Class Ib | Aprindine | Lidocaine | Mexiletine | Tocainide
Class Ic | Encainide | Flecainide | Lorcainide | Moricizine | Propafenone
Class II | Propranolol | Metoprolol | Nadolol | Atenolol | Acebutolol | Pindolol see Beta blockers (C07)
Class III | Amiodarone | Bretylium tosylate | Bunaftine | Dofetilide | Ibutilide | Sotalol
Class IV | Verapamil | Diltiazem see Calcium channel blockers (C08)
Class V | Adenosine | Atropine | Digoxin
Anticoagulants
Anticoagulants Overview
Vitamin K Antagonists Overview | Acenocoumarol | Clorindione | Coumatetralyl | Dicumarol (Dicoumarol) | Diphenadione | Ethyl biscoumacetate | Phenprocoumon | Phenindione | Tioclomarol | Warfarin
Antihypertensives and Diuretics
Antihypertensive Overview (C02) and Diuretic Overview (C03)
Sympatholytic Agents Overview (including Alpha Blockers Overview)
- Centrally Acting Antiadrenergics Overview | Clonidine | Guanfacine | Methyldopa | Moxonidine | Rescinnamine | Reserpine | Rilmenidine
- Ganglionic Blocker Overview / Nicotinic Antagonist Overview | Mecamylamine | Trimethaphan
- Peripherally acting/Antiadrenergics | Prazosin | Guanethidine | Indoramin | Doxazosin
Vasodilators Overview | Diazoxide | Hydralazine | Minoxidil | Nitroprusside | Phentolamine
Other antihypertensives
- Serotonin Antagonist Overview |Ketanserin
- Endothelin Receptor Antagonist Overview | Bosentan | Ambrisentan | Sitaxsentan
Low ceiling diuretics
- Thiazide Overview | Bendroflumethiazide | Chlorothiazide | Hydrochlorothiazide
- Non-thiazides | Chlortalidone | Indapamide | Quinethazone | Mersalyl | Metolazone | Theobromine | Cicletanine
High ceiling diuretics
- Loop Diuretic Overview | Bumetanide | Furosemide | Torasemide)
- Potassium-Sparing Diuretics Overview
- Epithelial Sodium Channel Overview |Amiloride | Triamterene)
- Aldosterone Antagonist Overview |Spironolactone | Eplerenone | Potassium canrenoate | Canrenone
Antiplatelet Agents
Glycoprotein IIb/IIIa Inhibitors Overview | Abciximab | Eptifibatide | Tirofiban
ADP Receptor Antagonists | Clopidogrel | Ticlopidine | Prasugrel
Prostaglandin Analogues Overview | Beraprost | Prostacyclin | Iloprost | Treprostinil
Other Antiplatelet Agents Acetylsalicylic acid/Aspirin | Aloxiprin | Ditazole | Carbasalate calcium | Cloricromen | Dipyridamole | Indobufen | Picotamide | Triflusal
Antithrombins
Direct Thrombin Inhibitors Overview | Argatroban | Bivalirudin | Dabigatran | Desirudin | Hirudin | Lepirudin | Melagatran | Ximelagatran
Indirect Thrombin Inhibitors
- Heparins | Danaparoid | Heparin | Sulodexide
- Low Molecular Weight Heparins | Bemiparin | Dalteparin | Enoxaparin | Nadroparin | Parnaparin | Reviparin | Tinzaparin
Other Antithrombotics | Defibrotide | Dermatan sulfate | Fondaparinux | Rivaroxaban
Non-Medicinal Antithrombins Overview | Citrate | EDTA | Oxalate
Beta Blockers
Non-selective β antagonists | Metipranolol | Nadolol | Oxprenolol | Penbutolol | Pindolol | Propranolol | Timolol | Sotalol
β1 antagonists (cardioselective) | Atenolol | Acebutolol | Betaxolol | Bisoprolol | Esmolol | Metoprolol | Nebivolol
Mixed α1/β antagonists | Carvedilol | Labetalol
Calcium Channel Blockers
Calcium Channel Blocker Overview
Class I Phenylalkylamines (C08DA) | Verapamil
Class II Dihydropyridines (C08CA) | Amlodipine | Felodipine | Isradipine | Lacidipine | Lercanidipine | Nicardipine | Nifedipine | Nimodipine | Nisoldipine
Class III Benzothiazepines (C08DB) | Diltiazem
Cardiac Glycosides
Cardiac Glycoside Overview (C01A)
Digitalis Glycosides Overview | Acetyldigitoxin | Acetyldigoxin | Digitalis leaves | Digitoxin | Digoxin | Lanatoside C | Deslanoside | Metildigoxin | Gitoformate
Scilla Glycosides Overview | Proscillaridin
Strophantus Glycosides Overview | G-strophanthin | Cymarin
Other Cardiac Glycosides | Peruvoside
Cardiac Stimulants Excluding Cardiac Glycosides
Cardiac stimulants excluding cardiac glycosides (C01C)
Adrenergic Overview and Dopaminergic Overview agents | Etilefrine | Isoprenaline | Norepinephrine | Dopamine | Norfenefrine | Phenylephrine | Dobutamine | Oxedrine | Metaraminol | Methoxamine | Mephentermine | Dimetofrine | Prenalterol | Dopexamine | Gepefrine | Ibopamine | Midodrine | Octopamine | Fenoldopam | Cafedrine | Arbutamine | Theodrenaline | Epinephrine
Phosphodiesterase Inhibitors Overview (PDE3I) | Amrinone | Milrinone | Enoximone | Bucladesine
Other cardiac stimulants | Angiotensinamide | Xamoterol | Levosimendan
Fibrinolytics
Alteplase | Reteplase | Tenecteplase | Streptokinase, Urokinase | Saruplase | Anistreplase
Hypolipidemic Agents
Statins Overview | Atorvastatin | Cerivastatin | Fluvastatin | Lovastatin | Mevastatin | Pitavastatin | Pravastatin | Rosuvastatin | Simvastatin
Fibrates Overview | Clofibrate | Bezafibrate | Aluminium clofibrate | Gemfibrozil | Fenofibrate | Simfibrate | Ronifibrate | Ciprofibrate | Etofibrate | Clofibride
Bile Acid Sequestrant Overview | Colestyramine | Colestipol | Colextran | Colesevelam
Niacin and Derivatives | Niceritrol | Niacin | Nicofuranose | Aluminium nicotinate | Nicotinyl alcohol | Acipimox
Other | Dextrothyroxine | Probucol | Tiadenol | Benfluorex | Meglutol | Omega-3-triglycerides | Magnesium pyridoxal 5-phosphate glutamate | Policosanol | Ezetimibe
Nitrates
Nitrates Overview | Glyceryl trinitrate | Isosorbide dinitrate | Isosorbide mononitrate | Molsidomine | Pentaerythritol tetranitrate
Pulmonary Artery Hypertension
Medications used in the management of pulmonary arterial hypertension Overview (B01, C02)
Prostacyclin Overview | Beraprost | Epoprostenol | Iloprost | Treprostinil
Endothelin Receptor Antagonists Overview | Ambrisentan | Bosentan | Sitaxsentan
PDE5 Inhibitors Overview | Sildenafil | Tadalafil | Vardenafil
Adjunctive therapy | Calcium channel blockers | Diuretics | Digoxin | Oxygen therapy | Warfarin
Vasodilators
Quinolone Vasodilators Overview | Flosequinan
Other Vasodilators | Heptaminol | Molsidomine | Nicorandil | Nesiritide
INTERVENTIONAL CARDIOLOGY
Interventional Cardiology
Diagnostic Catheterization | Risk Stratification and the Benefits of PCI vs Medical Therapy | Conscious Sedation | Preparation of the Patient for Diagnostic Catheterization | Technical Aspects of the Cardiac Catheterization Laboratory | Obtaining Venous and Arterial Access | Equipment Used in Diagnostic Cardiac Catheterizaiton | Hemodynamic Assessment in the Cardiac Catheterization Laboratory | Radiation Safety
Assesement of coronary lesions | Coronary Fractional Flow Reserve (FFR)) | Coronary flow reserve(CFR) | Intravascular ultrasound (IVUS)
PCI | Preparation of the Patient for Percutaneous Coronary Intervention (PCI) | Percutaneous Coronary Intervention (PCI): Basic Principles and Guidelines | Equipment Used in Percutaneous Coronary Intervention | Pharmacotherapy to Support PCI | Antiplatelet therapy | Antithrombotic therapy | Angiography and PCI in Special Patient Populations | Management Of Specific Lesion Types | High Risk Percutaneous Coronary Intervention (PCI) | Vascular Closure Devices | Post PCI Medical Management of the Interventional Patient | Complications During and Following Cardiac Catheterization and Percutaneous Coronary Intervention | Coronary stent thrombosis
PCI in Specific Populations and Lesion Types
- Assessment of Lesion Complexity and Morphology Using Coronary Lesion Classification Systems
- Angiographically Visible Thrombus
- The Calcified Leison
- The Ostial Lesion
- The Angulated or Tortuous Lesion
- Management of the Bifurcation Lesion
- The Long Lesion
- Management of a Coronary Bridge Lesion and Kinks
- Management of Coronary Vasospasm
- The Chronic Total Occlusion (CTO)
- Intervention in Small Vessels
- Intervention in Diffusely Diseased Vessels
- Intervention in Saphenous Vein Grafts (SVG)
- Intervention in the LIMA
- Intervention in the RIMA
- Intervention in a Free Radial and other Conduits
- Multivessel Intervention
- PCI in the Patient with Restenosis
- Management of the Patient with Stent Thrombosis
- Treatment of Distal Anastomotic Lesions
- Coronary Artery Perforation
- Left Main Intervention
- Management of the Thrombotic Lesion
High Risk PCI | PCI in the Patient in Cardiogenic Shock | PCI in the Patient Requiring CPR and Refractory Ventricular Arrhythmias | PCI in the Patient with Severely Depressed Ventricular Function | PCI in the Patient with Critical Valve Stenosis | PCI in the Sole Remaining Conduit | PCI in the Unprotected Left Main Patient | Adjuncts for High Risk Percuatenous Coronary Intervention
Mechanical circulatory support | Mechanical circulatory support | Intra-aortic balloon pump | Ventricular assist devices
Other TopicsNon Coronary Interventions in the Cardiac Catheterization Laboratory | Transfusion in ACS management | Revascularization in the “No Option” Patient
Cardiac Surgery
Vascular Surgery
BIOSTATISTICS
COST EFFECTIVENESS AND QUALITY OF LIFE
Template:WH Template:WikiDoc Sources
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]
Diagnostic Catheterization | Risk Stratification and the Benefits of PCI vs Medical Therapy | Conscious Sedation | Preparation of the Patient for Diagnostic Catheterization | Technical Aspects of the Cardiac Catheterization Laboratory | Obtaining Venous and Arterial Access | Equipment Used in Diagnostic Cardiac Catheterizaiton | Hemodynamic Assessment in the Cardiac Catheterization Laboratory | Radiation Safety
Therapeutic Catheterization | Therapeutic procedures | Advances in catheter based physical treatments
Coronary angiography | Overview | Historical Perspective | Contraindications | Appropriate use criteria for revascularization | Complications | Technique | Film Quality
Coronary Anatomy and Projection Angles | Normal Coronary Anatomy | Coronary arteries | Left coronary artery | Left main coronary artery | Left anterior descending artery | Left circumflex artery | Ramus intermedius | Right coronary artery | Coronary artery dominance | Coronary Anatomic Variants | Separate ostia | Anomalous origins of the coronary arteries | Coronary artery fistula | Projection Angles | Standard angiographic views | Left coronary artery | Right coronary artery
Assessment of Epicardial Coronary Blood Flow | TIMI flow grade (TFG) | TIMI flow grade 0 | TIMI flow grade 1 | TIMI flow grade 2 | TIMI flow grade 3 | TIMI frame count (TFC) | Pulsatile flow | Deceleration
Assessment of Myocardial Perfusion | TIMI myocardial perfusion grade (TMPG) | TIMI myocardial perfusion grade 0 | TIMI myocardial perfusion grade 0.5 | TIMI myocardial perfusion grade 1 | TIMI myocardial perfusion grade 2 | TIMI myocardial perfusion grade 3
Assessment of Coronary Lesions | Coronary Fractional Flow Reserve (FFR)) | Coronary flow reserve(CFR) | Intravascular ultrasound (IVUS) | Lesion Complexity | ACC-AHA characteristics of type A, B, and C coronary lesions | SCAI Lesion Classification System
Thrombus Grades | TIMI thrombus grade | TIMI thrombus grade 0 | TIMI thrombus grade 1 | TIMI thrombus grade 2 | TIMI thrombus grade 3 | TIMI thrombus grade 4 | TIMI thrombus grade 5 | TIMI thrombus grade 6 | Lesion Morphology | Quantitative angiography | Definitions of Preprocedural Lesion Morphology | Irregular lesion | Disease extent | Arterial foreshortening | Infarct related artery (Culprit lesion) | Restenosis | Degenerated saphenous vein graft | Collaterals | Coronary artery ulceration | Coronary artery aneurysm | Coronary artery bifurcation | Coronary artery trifurcation
PCI | Preparation of the Patient for Percutaneous Coronary Intervention (PCI) | Percutaneous Coronary Intervention (PCI): Basic Principles and Guidelines | Equipment Used in Percutaneous Coronary Intervention | Pharmacotherapy to Support PCI | Antiplatelet therapy | Antithrombotic therapy | Angiography and PCI in Special Patient Populations | Management Of Specific Lesion Types | High Risk Percutaneous Coronary Intervention (PCI) | Vascular Closure Devices | Post PCI Medical Management of the Interventional Patient | Complications During and Following Cardiac Catheterization and Percutaneous Coronary Intervention | Coronary stent thrombosis
PCI in Specific Populations and Lesion Types
- Assessment of Lesion Complexity and Morphology Using Coronary Lesion Classification Systems
- Angiographically Visible Thrombus
- The Calcified Leison
- The Ostial Lesion
- The Angulated or Tortuous Lesion
- Management of the Bifurcation Lesion
- The Long Lesion
- Management of a Coronary Bridge Lesion and Kinks
- Management of Coronary Vasospasm
- The Chronic Total Occlusion (CTO)
- Intervention in Small Vessels
- Intervention in Diffusely Diseased Vessels
- Intervention in Saphenous Vein Grafts (SVG)
- Intervention in the LIMA
- Intervention in the RIMA
- Intervention in a Free Radial and other Conduits
- Multivessel Intervention
- PCI in the Patient with Restenosis
- Management of the Patient with Stent Thrombosis
- Treatment of Distal Anastomotic Lesions
- Coronary Artery Perforation
- Left Main Intervention
- Management of the Thrombotic Lesion
High Risk PCI | PCI in the Patient in Cardiogenic Shock | PCI in the Patient Requiring CPR and Refractory Ventricular Arrhythmias | PCI in the Patient with Severely Depressed Ventricular Function | PCI in the Patient with Critical Valve Stenosis | PCI in the Sole Remaining Conduit | PCI in the Unprotected Left Main Patient | Adjuncts for High Risk Percuatenous Coronary Intervention
Mechanical circulatory support | Mechanical circulatory support | Intra-aortic balloon pump | Ventricular assist devices | Artificial heart
PCI Complications | Vessel Perforation | Dissection | Distal Embolization | No-reflow | Abrupt Closure | Restenosis | Late Acquired Stent Malapposition | Loss of Side Branch | Multiple Complications | Coronary stent thrombosis | Slow flow | Pulsatile flow | Deceleration | Ectasia | Intimal flap | Staining | Coronary air embolism
Left Ventriculography | Technique | Quantification of LV Function | Quantification of Mitral Regurgitation
Other TopicsNon Coronary Interventions in the Cardiac Catheterization Laboratory | Transfusion in ACS management | Revascularization in the “No Option” Patient
Looking for the patient version?
© 2026 MyEClinic – IFTM Institut für Telematik in der Medizin GmbH